current concept of management gastric carcinoma
TRANSCRIPT

Current concepts in Current concepts in management of gastric management of gastric
carcinomacarcinoma
Prof. R.N.MangualProf. R.N.Mangual
Prof.&Head of the Dept. of surgeryProf.&Head of the Dept. of surgeryM.K.C.G.Medical CollegeM.K.C.G.Medical CollegeBerhampur,OrissaBerhampur,Orissa

THE MAGNITUDE OF PROBLEM
Adenocarcinoma of Stomach 2nd Common cause of cancer death 10% of all new cancer death.
Poor prognosis : Incidence = Mortality. Geographical variation. Highest incidence in Japan - 90/1,00,000 High incidence Chili, Costa Rica, Hungary, Portugal,
Singapore, Romania. US decreased mortality - 15/1,00,000 India : Kashmir - 36/1,00,000
Chennai - 15/1,00,000Bangalore - 10.6/1,00,000

ANNUAL INCIDENCE IN THE ANNUAL INCIDENCE IN THE WORLDWORLD
Male – about 600,000Male – about 600,000 Female – about 330,000Female – about 330,000 Age standard incidence – Age standard incidence –
10.4(F) - 22.0(M)/ 100,000 10.4(F) - 22.0(M)/ 100,000 Male deaths – 445,000 or age standardized Male deaths – 445,000 or age standardized
mortality rate of 16.3/100,000mortality rate of 16.3/100,000

THE CHANGING SCENARIO
Incidence Worldwide ↓ Incidence of proximal gastric cancer ↑. Incidence distal gastric cancer ↓. Proximal gastric cancer ↑↑ in UK,
Netherland. Natural history unchanged with obscure
symptoms. Delayed presentation.

Incidence of cardia tumourIncidence of cardia tumour
England & wales(1977-England & wales(1977-1998) Newnham et al1998) Newnham et al
Male- Male- 2.02.0→5.4/100,000→5.4/100,000
Female- Female- 0.6→1.4/100,0000.6→1.4/100,000
U.S.A(1974-1994) U.S.A(1974-1994)
Devessa et alDevessa et al Reported simillar resultReported simillar result ↑ ↑ cardia tumour cardia tumour
-2.1→3.3/100,000-2.1→3.3/100,000 ↓ ↓ non cardia tumour – non cardia tumour –
5.1→3.7/100,0005.1→3.7/100,000
In Japan similar result reported1963-90

WHAT GOES WRONGMen are at risk -2:1 and 3:2 Age :Peak : 7th to 8th Decade
> 40 – Intestinal variant Younger : More aggressive diffuse type.
Environmental Influence on migrant population.Exposure to environmental factor in early life.
Social, cultural, occupational and dietary factors have influence on the incidence on Gastric Cancer.

TWO VIEWSTWO VIEWS
A tailored therapeutic approach for A tailored therapeutic approach for every every individual patientsindividual patients based on pre operative based on pre operative staging, with adequate knowledge of location staging, with adequate knowledge of location and type of tumour is the key to success.and type of tumour is the key to success.
A thorough pre operative staging with A thorough pre operative staging with adequate knowledge of prognostic factors and adequate knowledge of prognostic factors and anatomy will be helpful for choosing the anatomy will be helpful for choosing the optimal therapeutic option in optimal therapeutic option in individual individual situation.situation.

ANATOMY OF THE STOMACH

ANTERIOR VIEW

POSTERIOR VIEW

PERIGASTRIC LYMPHATICS

Japanese concept of stomachJapanese concept of stomach

LAYERS OF THE STOMACH

Commonly encountered G.C.Commonly encountered G.C.
Early gastric cancer (E.G.C.)Early gastric cancer (E.G.C.) Resectable G.C.Resectable G.C. Potential resectable G.C.Potential resectable G.C. Unresectable gastric Ca.Unresectable gastric Ca. G.E. Junction Ca.G.E. Junction Ca. Distal G.C.Distal G.C. Proximal G.C.Proximal G.C.

Early Gastric Ca.Early Gastric Ca.
Early gastric cancer is defined as tumour Early gastric cancer is defined as tumour confined to mucosa and sub mucosa confined to mucosa and sub mucosa irrespective of lymph node involvementirrespective of lymph node involvement . (Gotala. (Gotala et et
al, gastric cancer 2000)al, gastric cancer 2000)
???????????? Diagnosed 15%-30% Korea, in West-16%, Diagnosed 15%-30% Korea, in West-16%,
Japan- 50%, USA- 20%Japan- 50%, USA- 20% 5 Yr survival:- N0 – 97%,N2 – 77%(> +3 LN)5 Yr survival:- N0 – 97%,N2 – 77%(> +3 LN)

The treatment protocol varies from Submucosal The treatment protocol varies from Submucosal resection to D2 dissection with gastrectomy resection to D2 dissection with gastrectomy depending on size and depth of the tumour.depending on size and depth of the tumour.
Size of T < 30 mm -- Size of T < 30 mm -- ↓ L.N. invasion↓ L.N. invasion Depth 300 Depth 300 μμm infiltration – D1 and D2 m infiltration – D1 and D2
recommended.recommended. Sm 1 → 2% L.N.Sm 1 → 2% L.N. Sm 2 → 12% L.N.Sm 2 → 12% L.N. Sm 3 → 20 % L.N.Sm 3 → 20 % L.N.

H.Pylori & Gastric carcinoma

Japanese Endoscopic Society Classification

Diagnostic modalities & pre- Diagnostic modalities & pre- operative stagingoperative staging
Upper G.I. endoscopy with 6-8 sites of biopsy. *Upper G.I. endoscopy with 6-8 sites of biopsy. * Endoscopic. U.S.G. *Endoscopic. U.S.G. * Virtual endoscopyVirtual endoscopy Abdominal ultrasonography *Abdominal ultrasonography * Abdominal contrast C.T. for LN evaluation & distant Abdominal contrast C.T. for LN evaluation & distant
metastasismetastasis M.R.I. & PET Scan.M.R.I. & PET Scan. Diagnostic & staging laparoscopy *Diagnostic & staging laparoscopy *



MULTIPE SECONDARIES IN MULTIPE SECONDARIES IN LIVERLIVER




T.N.M. StagingT.N.M. Staging TXTX Primary tumor cannot be assessedPrimary tumor cannot be assessed T0T0 No evidence of primary tumorNo evidence of primary tumor TisTis Carcinoma in situ: intraepithelial tumor without invasion Carcinoma in situ: intraepithelial tumor without invasion
of the lamina propria of the lamina propria T1 Tumor invades lamina propria or submucosaT1 Tumor invades lamina propria or submucosa T2T2 Tumor invades muscularis propria or subserosa*Tumor invades muscularis propria or subserosa* T2aT2a Tumor invades muscularis propriaTumor invades muscularis propria T2bT2b Tumor invades subserosaTumor invades subserosa T3T3 Tumor penetrates serosa (visceral peritoneum) without Tumor penetrates serosa (visceral peritoneum) without
invasion of adjacent structures**,***invasion of adjacent structures**,*** T4T4 Tumor invades adjacent structures**,***Tumor invades adjacent structures**,***

Definition of American Joint Committee on Cancer/International Union Against Cancer T stage based on depth of penetration of the gastric wall.

Regional Lymph Nodes (N)Regional Lymph Nodes (N)
NX Regional lymph node(s) cannot be NX Regional lymph node(s) cannot be assessed assessed
N0 No regional lymph node metastasis*N0 No regional lymph node metastasis* N1 Metastasis in 1 to 6 regional lymph nodesN1 Metastasis in 1 to 6 regional lymph nodes N2 Metastasis in 7 to 15 regional lymph N2 Metastasis in 7 to 15 regional lymph
nodes nodes N3 Metastasis in more than 15 regional N3 Metastasis in more than 15 regional
lymph nodes lymph nodes

Distant Metastasis (M)Distant Metastasis (M)
MX Distant metastasis cannot be assessedMX Distant metastasis cannot be assessed M0 No distant metastasisM0 No distant metastasis M1 Distant metastasisM1 Distant metastasis

STAGE GROUPING STAGE GROUPING Stage 0 Tis N0 M0Stage 0 Tis N0 M0 Stage IA T1 N0 M0Stage IA T1 N0 M0 Stage IB T1 N1 M0Stage IB T1 N1 M0 T2a/b N0 M0T2a/b N0 M0 Stage II T1 N2 M0Stage II T1 N2 M0 T2a/b N1 M0T2a/b N1 M0 T3 N0 M0T3 N0 M0 Stage IIIA T2a/b N2 M0Stage IIIA T2a/b N2 M0 T3 N1 M0T3 N1 M0 T4 N0 M0T4 N0 M0 Stage IIIB T3 N2 M0Stage IIIB T3 N2 M0
Stage IV T4 N1-3 M0Stage IV T4 N1-3 M0 T1-3 N3 M0T1-3 N3 M0 Any T Any N M1Any T Any N M1

Four types of T.N.M.classifications : Four types of T.N.M.classifications :
Clinical classification, designated cTNM or Clinical classification, designated cTNM or TNM TNM
Pathologic classification, designated pTNM Pathologic classification, designated pTNM
Retreatment classification, designated rTNM Retreatment classification, designated rTNM
Autopsy classification, designated aTNM Autopsy classification, designated aTNM

SURGICAL MANAGEMENTSURGICAL MANAGEMENT
OBJECTIVES :-OBJECTIVES :- 1.1. The optimal surgical management is The optimal surgical management is
tailored to the extent and location of the tailored to the extent and location of the tumour.tumour.
2.2. Aggressive resection is justified in absence Aggressive resection is justified in absence of distant metastasis.of distant metastasis.
3.3. Extent of resection determines the Extent of resection determines the microscopic tumour free margin( 6cm Away)microscopic tumour free margin( 6cm Away)

SURGICAL OPTIONSSURGICAL OPTIONS1.G.E. Junction & - Total gastrectomy ± S.P1.G.E. Junction & - Total gastrectomy ± S.P
cardiac end T cardiac end T -Prox.gastrectomy ± S.P -Prox.gastrectomy ± S.P
2.Mid third T 2.Mid third T Total gastrectomy ± S.P Total gastrectomy ± S.P
3.Distal T 3.Distal T -Near total gastrectomy± S.P-Near total gastrectomy± S.P
-Total gastrectomy ± S.P-Total gastrectomy ± S.P
-Partial gastrectomy ±S.P-Partial gastrectomy ±S.P
Intestinal type Intestinal type –– 3c.m. margin clearance 3c.m. margin clearance
Diffuse type Diffuse type –– 5c.m. margin clearance 5c.m. margin clearance

Total Vs. Proximal gastric resectionTotal Vs. Proximal gastric resection
Norwegian stomach cancer trial Norwegian stomach cancer trial →→
TYPESTYPES MORTALITYMORTALITY MORBIDITYMORBIDITY
PROXIMAL PROXIMAL GASTRIC GASTRIC RESECTIONRESECTION
52%52% 16%16%
TOTAL TOTAL GASTRIC GASTRIC RESECTIONRESECTION
38%38% 8%8%

R status of tumour resectionR status of tumour resection
Described by Hermanek 1994 of tumour status Described by Hermanek 1994 of tumour status after resection.after resection.
R0 – Microscopically margin negative ,no R0 – Microscopically margin negative ,no gross or microscopic tumour remains in the gross or microscopic tumour remains in the tumour bed (complete resection).tumour bed (complete resection).
R1 – Macroscopic clearance of tumour but R1 – Macroscopic clearance of tumour but microscopic margins are positive.microscopic margins are positive.
R2 – Gross residual tumour remains.R2 – Gross residual tumour remains.

Extent of lymph node dissectionExtent of lymph node dissection
D1 = Perigastric nodes (station 1-6)D1 = Perigastric nodes (station 1-6) D1+/Over D1 = D1 plus L.N. of D2 safely D1+/Over D1 = D1 plus L.N. of D2 safely
removed without splenectomy or removed without splenectomy or pancreatectomypancreatectomy
D2 = Common hepatic, left gastric, coeliac & D2 = Common hepatic, left gastric, coeliac & splenic L.N.(7-11)splenic L.N.(7-11)
D3 = Hepato-duodenal ligament & root of the D3 = Hepato-duodenal ligament & root of the mesentery (12-16)mesentery (12-16)
D4 = D3 + para-aortic LN dissection D4 = D3 + para-aortic LN dissection

D1 D2

D2D1
DISTAL RADICAL GASTRECTOMY

D2D1
GASTRECTOMY FOR TUMOURS OF THE BODY

TOTAL GASTRECTOMY FOR TUMOURS OF THE UPPER THIRD

D1 Vs D2 resectionD1 Vs D2 resection
In terms of survival the meta analysis shows In terms of survival the meta analysis shows no statistically significant difference between no statistically significant difference between D1 & D2 groups- weighed 5 Yr SR was 42.6% D1 & D2 groups- weighed 5 Yr SR was 42.6% for D2 &41% for D1.for D2 &41% for D1.
But the patient with TNM stage 2 and Stage 3a But the patient with TNM stage 2 and Stage 3a also exhibited trends to higher rate of 11 Yr also exhibited trends to higher rate of 11 Yr SR after D2 surgery -37% Vs 23% (p = 0.1)for SR after D2 surgery -37% Vs 23% (p = 0.1)for stage 2 & 22% Vs 4% (p=0.38)for stage 3a.stage 2 & 22% Vs 4% (p=0.38)for stage 3a.

A sub group analysis shows that patient with A sub group analysis shows that patient with N2 group of LN ,who had D2 resection N2 group of LN ,who had D2 resection exhibited exhibited ↑ ↑ long term survival rate of 21% long term survival rate of 21% compared with 0% in D1 resection.compared with 0% in D1 resection.
A long battle between East & West.A long battle between East & West.



G.E.JUNCTION CLEARANCE

PROXIMAL GASTRECTOMYPROXIMAL GASTRECTOMY

D2 RESECTIOND2 RESECTION

TOTAL GASTRECTOMY

DISTAL GASTRECTOMY
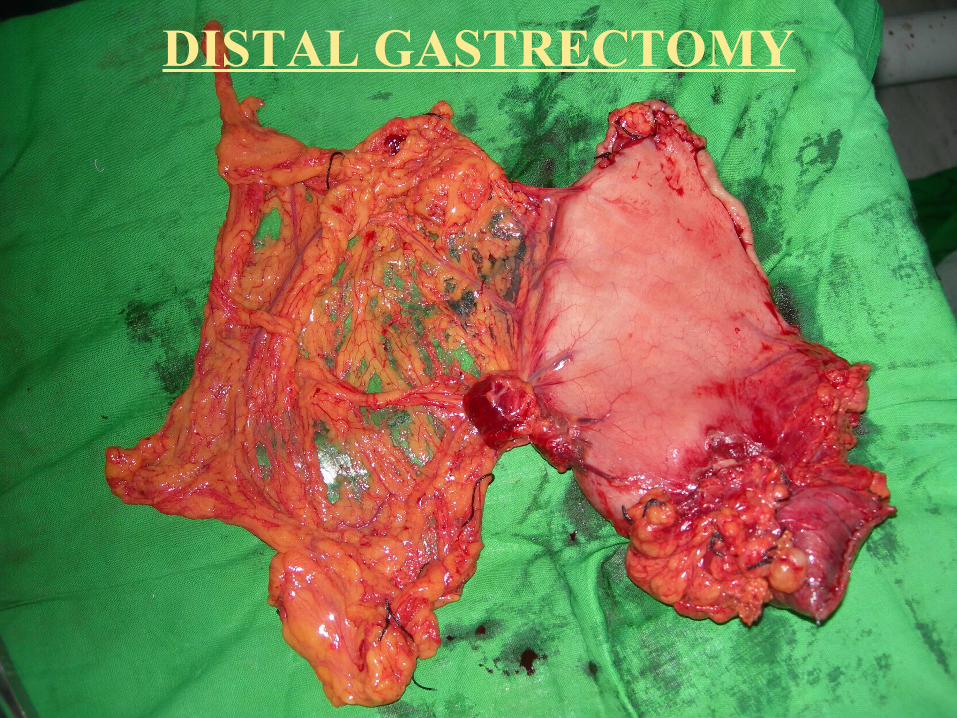
DISTAL GASTRECTOMY

UNRESECTABLE G.C.
Impact of resection marginImpact of resection margin
In margin positive, there is significant In margin positive, there is significant ↓ ↓ of OS.of OS. Memorial Sloan-Kettering cancer centre Memorial Sloan-Kettering cancer centre
( MSKCC) recommends resection ( MSKCC) recommends resection ≥ ≥ 6 cm 6 cm away from primary tumour.away from primary tumour.
5-20 % positive margin found in most of the 5-20 % positive margin found in most of the series.series.
Dutch Gastric Cancer Trial –reports +ve Dutch Gastric Cancer Trial –reports +ve margin in 6% ( n =61/694)margin in 6% ( n =61/694)

Locoregional failure rateLocoregional failure rate
AuthorAuthor Stomach Stomach remnant %remnant %
Anastomosis Anastomosis %%
Lymph Lymph Node %Node %
Gunderson Gunderson et alet al
55 %55 % 26 %26 % 43 %43 %
Landry et alLandry et al 21 %21 % 26 %26 % 8 %8 %
Lim et alLim et al 1 %1 % 5 %5 %
D`Angelica D`Angelica et alet al
12 %12 % 18 %18 % 28 %28 %

Median survival rateMedian survival rate
The presence of a positive margin had lost The presence of a positive margin had lost significance in the patients > 5 node positive.significance in the patients > 5 node positive.
Aggressive locoregional clearance does not Aggressive locoregional clearance does not make difference of OS.make difference of OS.
In R0 + Chemoradiation - MS=19.3 monthsIn R0 + Chemoradiation - MS=19.3 months In R1 + Chemoradiation – MS = 16.2 monthsIn R1 + Chemoradiation – MS = 16.2 months In R2 + Chemoradiation – MS = 9.2 monthsIn R2 + Chemoradiation – MS = 9.2 months

Adjuvant chemotherapyAdjuvant chemotherapy
A single agent + R0 , does not show any survival A single agent + R0 , does not show any survival benefit.benefit.
1. R0+ FAM(315) no benefit of OS and RR1. R0+ FAM(315) no benefit of OS and RR 2. FAMT2. FAMTxx widely used claims better result 56% widely used claims better result 56%
response rate, response rate, Klein et alKlein et al ,phase 2,EORTC ,phase 2,EORTC 3. EAP (1980)- RR=64%, MS=9 months, CR=21% in 3. EAP (1980)- RR=64%, MS=9 months, CR=21% in
advanced Gastric cancer. MSKCC trial claims FAMTadvanced Gastric cancer. MSKCC trial claims FAMTxx Vs EAP no apparent difference, EAP is more toxic.Vs EAP no apparent difference, EAP is more toxic.
4. ELF –Etoposide, leucovorin and 5FU (1991) MS 4. ELF –Etoposide, leucovorin and 5FU (1991) MS 11 months, RR= 53%, less toxic, EORTC phase 2 11 months, RR= 53%, less toxic, EORTC phase 2 trial similar results.trial similar results.

Adjuvant chemotherapyAdjuvant chemotherapy
5. ECF –Epirubucin, cisplatin, 5FU RR= 71%, 5. ECF –Epirubucin, cisplatin, 5FU RR= 71%, CR=12%, in advanced gastric cancer. (Royal CR=12%, in advanced gastric cancer. (Royal Marsden hospital report)Marsden hospital report)
Italian group study of digestive tract cancer for GC Italian group study of digestive tract cancer for GC claims 5FU cisplatin and epirubicin (weekly) claims claims 5FU cisplatin and epirubicin (weekly) claims RR= 62%, CR=17%, MS= 11months.RR= 62%, CR=17%, MS= 11months.
FAM 2( 7 cycles), EORTC phase 2(314) randomized FAM 2( 7 cycles), EORTC phase 2(314) randomized with surgery alone in stage 2 & 3, 5 year SR 70%with surgery alone in stage 2 & 3, 5 year SR 70%(stage 2), 32%(stage 3), DFS (stage 2), 32%(stage 3), DFS ↑ but more toxic.↑ but more toxic.

Adjuvant RadiotherapyAdjuvant Radiotherapy
Although the complete surgical resection is Although the complete surgical resection is potentially curative in early stage, locoregional potentially curative in early stage, locoregional recurrence remains frustrating problem in the recurrence remains frustrating problem in the patient presenting with more advanced stage , patient presenting with more advanced stage , T3-4, N1-2(60% in serosal involvement)T3-4, N1-2(60% in serosal involvement)
INT(0116) trial demonstrates improvement in INT(0116) trial demonstrates improvement in DFS and OS with post-operative DFS and OS with post-operative chemoradiation than with surgery alone.chemoradiation than with surgery alone.

Radiotherapy is limited, due to its position Radiotherapy is limited, due to its position near vital organs like kidney spinal cord, near vital organs like kidney spinal cord, pancreas, liver & bowel.pancreas, liver & bowel.
Stomach itself is highly sensitive, tends to Stomach itself is highly sensitive, tends to bleed and ulcerate with EBRT.bleed and ulcerate with EBRT.

NEO ADJUVANT RADIOTHERAPYNEO ADJUVANT RADIOTHERAPY
For down staging, neo-adjuvant For down staging, neo-adjuvant chemoradiation is useful as claimed by chemoradiation is useful as claimed by multicentric trials.multicentric trials.
1. n = 32 – Docetaxel + Cisplatin – followed 1. n = 32 – Docetaxel + Cisplatin – followed by EBRT neo-adjuvant by EBRT neo-adjuvant → claims 14(pCR), 10 → claims 14(pCR), 10 microscopic residual tumour. (microscopic residual tumour. (Mauer & Mauer & Ferguson 2000)Ferguson 2000)
2. 5FU + EBRT (neo-adjuvant)→ pCR (5/34), 2. 5FU + EBRT (neo-adjuvant)→ pCR (5/34), pPR (18/36) less encouraging. ( pPR (18/36) less encouraging. ( Mansfiled Mansfiled 20002000))

3. 5FU + Leucovorin & Cisplatin followed by 3. 5FU + Leucovorin & Cisplatin followed by 45Gy of RT with concurrent 5FU, patients 45Gy of RT with concurrent 5FU, patients demonstrating a pCR & pPR had longer demonstrating a pCR & pPR had longer median survival than those with outmedian survival than those with out neo-adjuvant therapy. MS= 63.9 month Vs neo-adjuvant therapy. MS= 63.9 month Vs 12.6 month p = 0.03 (12.6 month p = 0.03 (Ajani and Mansfield Ajani and Mansfield 2004).2004).
Unfortunately the majority of study claims Unfortunately the majority of study claims neoadjuvant RT as sole modality, has no neoadjuvant RT as sole modality, has no survival benefit.survival benefit.

Intraoperative radiotherapy (IORT)Intraoperative radiotherapy (IORT)
Phase 2, RTOG (Radiation therapy oncology group) Phase 2, RTOG (Radiation therapy oncology group) in 27 patients of IORT (12.5-16.5Gy)+ EBRT (post in 27 patients of IORT (12.5-16.5Gy)+ EBRT (post Op) claims 23 patients, 2 year SR 47%.Op) claims 23 patients, 2 year SR 47%.
Takahashi & AbeTakahashi & Abe in 1986, Japan randomized 211 in 1986, Japan randomized 211 patient IORT (25- 40 Gy) Vs surgery alone claims patient IORT (25- 40 Gy) Vs surgery alone claims ↑ ↑ in 5 Yr SR with IORT.in 5 Yr SR with IORT.
Chen & SongChen & Song 1994, China randomized stage 3 & 4 1994, China randomized stage 3 & 4 patients for surgery with IORT Vs surgery alone patients for surgery with IORT Vs surgery alone claims ↑ in SR only in stage 3.claims ↑ in SR only in stage 3.
Sindelar & Tepper et alSindelar & Tepper et al in 1993 , NCI in 1993 , NCI (National Cancer institute) claims no survival (National Cancer institute) claims no survival benefit with IORT, but improvement in local benefit with IORT, but improvement in local recurrence (44% Vs 92%, p < 0.001).recurrence (44% Vs 92%, p < 0.001).
Still it needs to define the role of IORT in Still it needs to define the role of IORT in gastric carcinoma.gastric carcinoma.

NEOADJUVANT CHEMOTHERAPYNEOADJUVANT CHEMOTHERAPY
This is a new area of interest to discuss the This is a new area of interest to discuss the result of phase 3 trial ( MAGIC ) performed by result of phase 3 trial ( MAGIC ) performed by British MRC, ECF given pre & post Op. Vs British MRC, ECF given pre & post Op. Vs surgery alone.surgery alone.
The data placed before ASCO (American The data placed before ASCO (American society of clinical oncology) 2003 in Spring society of clinical oncology) 2003 in Spring meeting. meeting.
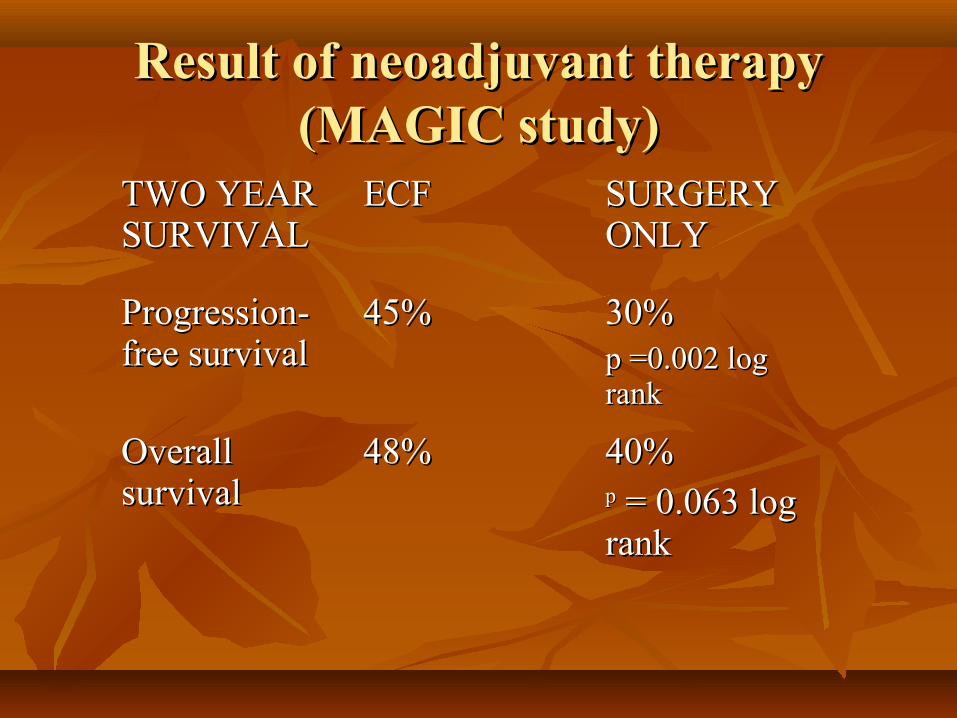
Result of neoadjuvant therapy Result of neoadjuvant therapy (MAGIC study)(MAGIC study)
TWO YEAR TWO YEAR SURVIVALSURVIVAL
ECFECF SURGERY SURGERY ONLYONLY
Progression-Progression-free survivalfree survival
45%45% 30% 30% p =0.002 log p =0.002 log rankrank
Overall Overall survivalsurvival
48%48% 40%40%
pp = 0.063 log = 0.063 log rankrank

MAGIC trial results MAGIC trial results (on curative (on curative resection and downstaging of tumour)resection and downstaging of tumour)
ECFECF SURGERY SURGERY ONLYONLY
No. of cases No. of cases having surgeryhaving surgery
212 (85%)212 (85%) 232 (95%)232 (95%)
Median time to Median time to surgerysurgery
99 days99 days 14 days14 days
Proportion of R0 Proportion of R0 curative resectioncurative resection
79%79% 69%69%
Proportion of –Proportion of –T3/T4 tumour T3/T4 tumour
49%49% 64%64%

The data presented in ASCO 2003 was not The data presented in ASCO 2003 was not encouraging, but data presented in ASCO encouraging, but data presented in ASCO MAY 2005 was significant and shows MAY 2005 was significant and shows statistical improvement with ECFstatistical improvement with ECF
The result of MAGIC study including the The result of MAGIC study including the ↓ ↓ of of T size some evidence of increase of rate of R0 T size some evidence of increase of rate of R0 resection and resection and ↑ ↑ of OS rate clearly indicated of OS rate clearly indicated that there is some potential important clinical that there is some potential important clinical benefit for neoadjuvant chemotherapy.benefit for neoadjuvant chemotherapy.

Post Operative ChemoradiationPost Operative Chemoradiation
SWOG 9006/INT 0116 trial of US in 7 Yr SWOG 9006/INT 0116 trial of US in 7 Yr follow up (n = 603) in stage IIIa, stage IIIb and follow up (n = 603) in stage IIIa, stage IIIb and stage IV with 5FU with Leucovorin followed stage IV with 5FU with Leucovorin followed by radiotherapy 4500 cGy with rest 2 cycles of by radiotherapy 4500 cGy with rest 2 cycles of chemotherapy with an observe arm.chemotherapy with an observe arm.
Claims significant improvement of DFS and Claims significant improvement of DFS and OS with acceptable toxicity in long term OS with acceptable toxicity in long term treatment protocol.treatment protocol.

SWOG9008/INT0116 resultsSWOG9008/INT0116 results
Chemoradiation Chemoradiation ControlControl
No. of casesNo. of cases 281 281 275275
Disease free Disease free median survivalmedian survival
30(months)30(months) 19(months)19(months)
Overall median Overall median survivalsurvival
35(months)35(months) 28(months)28(months)

Why Japanese trials claims better ?Why Japanese trials claims better ?
1. Aggressive screening procedure1. Aggressive screening procedure
2. Japanese believe in more radical surgery D2 & D3.2. Japanese believe in more radical surgery D2 & D3.
3. Most of the series starts early post Op 3. Most of the series starts early post Op chemotherapy.chemotherapy.
4. Japanese BMI is less than in west.4. Japanese BMI is less than in west.
5. Specialized centers and highly skilled hands.5. Specialized centers and highly skilled hands.
6. The incidence of GC is more distal and intestinal to 6. The incidence of GC is more distal and intestinal to the west more proximal. the west more proximal.
7. Japanese patients are younger and less obese.7. Japanese patients are younger and less obese.

PROGNOSTIC FACTORSPROGNOSTIC FACTORS
The prognosis is unpredictable even after a The prognosis is unpredictable even after a complete resection R0, there occurs loco-complete resection R0, there occurs loco-regional failure for which adjuvant chemo regional failure for which adjuvant chemo radiation is sought.radiation is sought.
Definitely the prognosis depends upon Definitely the prognosis depends upon location, depth of infiltration, extent and location, depth of infiltration, extent and histopathological behavior, not excluding the histopathological behavior, not excluding the nodal status & distant metastasis.nodal status & distant metastasis.

It taxes surgeon’s skill & ability, with different It taxes surgeon’s skill & ability, with different protocols of belief with institutional facility & protocols of belief with institutional facility & community drive for early diagnosis.community drive for early diagnosis.
Patient without systemic metastasis or Patient without systemic metastasis or peritoneal dissemination R0 (complete micro peritoneal dissemination R0 (complete micro & macroscopic resection) is the most & macroscopic resection) is the most independent prognostic factor.independent prognostic factor.
In pTNM of specimen , the number of In pTNM of specimen , the number of positive LN is, another prognostic factor.positive LN is, another prognostic factor.

5 out of 15 positive LN 5 out of 15 positive LN → Unfavorable→ Unfavorable Ichikura & OguwaIchikura & Oguwa et alet al -2003(Japan) suggest -2003(Japan) suggest
30 LN for histopathological study. If 20-3030 LN for histopathological study. If 20-30//30 30 negative → Favorable. If 9-19/30 LN negative, negative → Favorable. If 9-19/30 LN negative, it is unfavorable.it is unfavorable.
The Japanese concept regarding prognosis is The Japanese concept regarding prognosis is different to West which includes PHNS different to West which includes PHNS (peritoneum, liver, node, serosa) & CMA (peritoneum, liver, node, serosa) & CMA (location) system i.e. systemic involvement (location) system i.e. systemic involvement with anatomical location of the with anatomical location of the tumourtumour..

One should rememberOne should remember
1)1) 6 cm margin clearance of tumour is recommended.6 cm margin clearance of tumour is recommended.2)2) Clearance of N1 & N2 group of LN is essential.Clearance of N1 & N2 group of LN is essential.3)3) Resection of greater & lesser omentum is Resection of greater & lesser omentum is
necessary.necessary.4)4) Splenopancreatectomy only on indicated cases.Splenopancreatectomy only on indicated cases.5)5) For proximal lesion varying length of esophagus For proximal lesion varying length of esophagus
should be excised.should be excised.6)6) Judicious decision should be taken for total, Judicious decision should be taken for total,
proximal & distal gastrectomy.proximal & distal gastrectomy.7)7) All patient should receive All patient should receive chemoradiationchemoradiation..

MAY GOD BLESS YOUMAY GOD BLESS YOU