intramucosal carcinoma of the gastric antrum complicating
TRANSCRIPT

J Clin Pathol 1983;36:1071-1075
Intramucosal carcinoma of the gastric antrumcomplicating Menetrier's diseaseGORDON M WOOD, CHRISTINE BATES, RICHARD C BROWN, MONTY S LOSOWSKY
From the Departments ofMedicine and Pathology, St James's University Hospital, Beckett Street, Leeds LS97TF
SUMMARY A 48-year-old man presented with haematemesis and was found to have Menetrier'sdisease. Three and a half years later early gastric cancer was detected at routine follow-upendoscopy. This is the first report of the development of early gastric cancer during follow-up in a
case of Menetrier's disease. It is probable that patients with Menetrier's disease are at increasedrisk of gastric cancer, and should have regular endoscopic follow-up with gastric biopsy.
The controversy over the possibility that Menetrier'sdisease predisposes to gastric cancer is assuminggreater importance now that more cases of Mene-trier's disease are managed without gastric resec-tion.We report a patient who developed an early gas-
tric cancer three and a half years after Menetrier'sdisease was first diagnosed, and review presentknowledge of the relationship between the twoconditions.
Case report
The patient first presented with haematemesis at theage of 48 yr. He had had mild non-specific dyspepsiafor many years. There were no abnormal findings onexamination, apart from melaena. Barium mealdemonstrated large mucosal folds along the greatercurvature of the stomach and poor mucosal coatingwith barium, due to copious mucus secretion. Theradiological diagnosis was a greater curve gastriccarcinoma. Gastroscopy showed that the enlargedfolds on the greater curve were composed of thick-ened, oedematous gastric mucosa with superficialerosions. The endoscopic diagnosis was Menetrier'sdisease with a superimposed erosive gastritis.
Histological sections of gastric mucosal biopsiesshowed an unusually abundant gastric mucosa, withdisruption and loss of continuity of the muscularismucosae. The glands were lined by mucous cells andsome showed cystic dilatation; parietal cells werealso present indicating body mucosa. The superficialmucosa was infiltrated by lymphocytes and neu-
Accepted for publication 20 April 1983
trophils (Fig. 1). The histological diagnosis wasMenetrier's disease with a chronic superficial gas-tritis. There was no evidence of neoplastic change.The patiept had no further gastrointestinal bleed-
ing during this first admission. He continued to havemild dyspepsia with little relief from antacids.Twelve months later he suffered an extensiveinferior myocardial infarction. After a further 13months, he was readmitted with epigastric pain andmelaena. Gastroscopy again showed large folds ofmucosa in the fundus and body of the stomach. Asbefore, there were scattered mucosal erosions, someof which were bleeding. Biospy of the gastric antrumshowed a chronic superficial gastritis with no evi-dence of neoplasia. Cimetidine was commenced at adose of 1 g/day with rapid symptomatic relief andthe patient was followed by regular endoscopy.
After four months treatment with cimetidine, theerosions had healed but large gastric folds were stillpresent. There was no further change at follow-upendoscopy 11 months later. On this occasion thebody and antrum were again biopsied. The bodymucosa showed similar features to the first biopsydescribed above. There was no evidence of malig-nant change. Two of the five antral biopsies, how-ever, showed large hyperchromatic, pleomorphicepithelial cells with occasional mitotic figures, theappearances being those of gastric adenocarcinoma.The patient was readmitted to hospital andcimetidine was discontinued. Examination revealedno abnormal findings and investigations included aserum albumin of 43 g/l, a basal acid output of 0-19mmollh and peak acid output of 18-8 mmol/h afterpentagastrin. Double contrast barium mealconfirmed coarse gastric mucosal folds along the
1071
copyright. on 3 January 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1071 on 1 Septem
ber 1983. Dow
nloaded from

1072
greater curve with a thickened stomach wall but noabnormality was found in the antrum (Fig. 2).At laparotomy the abdominal viscera appeared
normal, apart from the stomach which had a normalserosa but a grossly thickened and lumpy wall. Atwo-thirds Polya gastrectomy was performed. Thepatient had a satisfactory convalescence apart froman episode of multifocal ventricular ectopic beats inthe immediate post-operative period. He remainswell 18 months later. Follow-up gastroscopy andbiopsy of the gastric remnant has shown no evidenceof recurrent carcinoma.
The gastrectomy specimen was opened along thegreater curvature which measured 24 cm in length.Large folds of mucosa up to 1 cm wide were presentin the body and fundus and were most prominentalong the greater curve. The antrum was macroscop-ically normal apart from slight nodularity of themucosa (Fig. 3). Histologically, the body of the
4
IL
ffi~~~~TP
Fig. 1 Original gastroscopic biopsy showing gastricmucosa with disruption ofmuscularis mucosae, cysticglands lined by mucous cells and a superficial infitrate oflymphocytes and neutrophils. Haematoxylin and eosin x80.
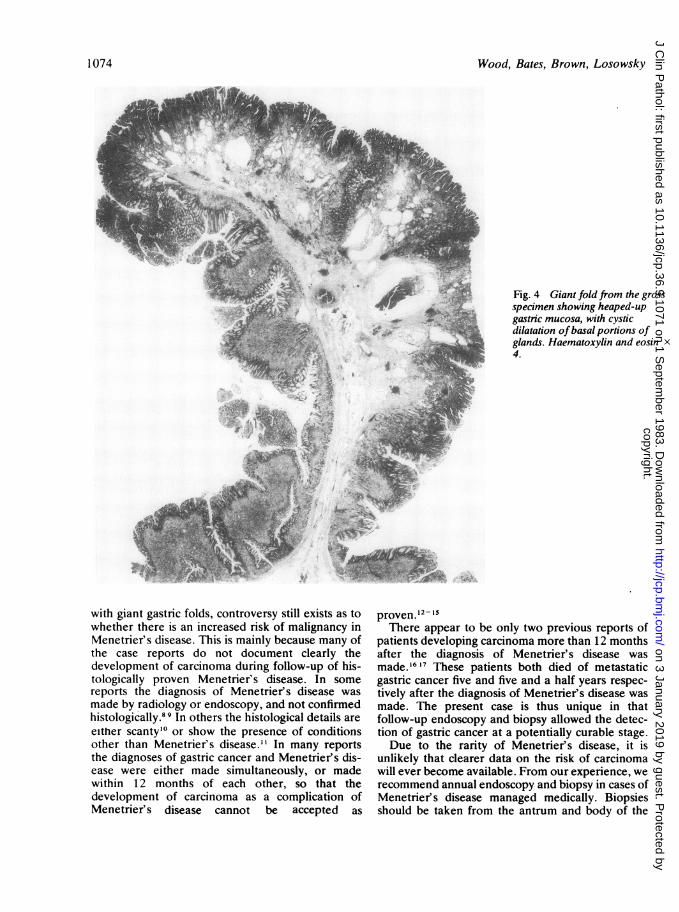
Wood, Bates, Brown, Losowskystomach showed features of advanced Menetrier'sdisease. The gastric mucosa was heaped up, forminggiant rugae (Fig. 4). The glands were long andstraight with the usual complement of gastric andparietal cells, but in many areas cystic dilatation ofthe, basal portion of the glands had occurred. Inplaces, the glands herniated through the muscularismucosae which was frayed and disrupted. Meta-plasia of the epithelium to mucus-secreting gobletcells had occurred in the cystic portions of theglands. Plasma cells and polymorphonuclear leuco-cytes were present throughout the lamina propriabut they were especially prominent in the superficialareas. Nine blocks were taken from the body of thestomach with no evidence of malignancy. One blockout of 15 taken from the gastric antrum showedintramucosal carcinoma, spreading superficially.There was no invasion beyond the lamina propria(Fig. 5). Fourteen lymph nodes were examined andfound to be free of metastatic deposits. The antralmucosa in the area of carcinomatous change alsoshowed features of Menetrier's disease with cysticglands, superficial inflammation and disrupted mus-cularis mucosae but the mucosa itself was relativelythin. Other sections from the antrum showed similarfeatures of the disease which were less marked,though inflammation of the lamina propria wasnoted in all areas. A few small areas of intestinalmetaplasia were observed.
Discussion
The patient described above had the clinical,radiological and endoscopic features of Menetrier'sdisease when he first presented.' 2 The serum albu-min is usually low in this condition but is more than35 g/l in 20% of cases.' Gastric biopsies at that timeshowed typical histological changes of the disease,with hypertrophy of the gastric glands and cysticdilatation of their basal portions, replacement ofparietal cells by mucus cells and a moderateinflammatory infiltrate in the lamina propria.'-3 Thebiopsies were adequate to make a confident diag-nosis of Menetrier's disease as they included themuscularis mucosae. Full-thickness biopsies fromthe gastrectomy specimen later confirmed this con-clusion and also demonstrated microscopc featuresof Menetrier's disease in the antrum; gross antralinvolvement in this condition is rare but has beendescribed.45 No other cause for giant gastric foldswas found. There is thus no doubt that this patienthad Menetrier's disease when he first presented witha haematemesis.Carcinoma was found in antral biopsies taken
three and a half years after the original diagnosis ofMenetrier's disease, and early gastric cancer was
copyright. on 3 January 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1071 on 1 Septem
ber 1983. Dow
nloaded from

Intramucosal carcinoma of the gastric antrum complicating Menetrier's disease
Fig. 2 The double contrastbarium meal shows giant folds onthe greater curvature ofthe body ofthe stomach but the antrumappears normal.
confirmed in the gastrectomy specimen. Althoughearly gastric cancer may remain confined to themucosa for 3-4 yr,6 we had taken antral biopsies ontwo occasions during follow-up in our patient, withno evidence of malignancy. We therefore believe itto be very likely that early gastric cancer developedafter Menetrier's disease in this case.
When Menetrier first described "polyadenomesen nappe", he considered the lesion to be benign,but wrote "... . it does have affinity with a moremalignant state and these lesions may be trans-formed into epitheliomas and cancers".' Althoughthere have been more than 30 subsequent casereports of gastric carcinoma found in association
- W . ,Fig. 3 The gastrectomy specimenopened along the greater curveshowing giant folds in the body ofthe stomach with sparing of theantrum. The arrow indicates thesite of the intramucosal carcinoma.
1073
i
copyright. on 3 January 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1071 on 1 Septem
ber 1983. Dow
nloaded from
Wood, Bates, Brown, Losowsky
Fig. 4 Giant fold from the grossspecimen showing heaped-upgastric mucosa, with cysticdilatation ofbasal portions ofglands. Haematoxylin and eosin x4.
with giant gastric folds, controversy still exists as towhether there is an increased risk of malignancy inMenetrier's disease. This is mainly because many ofthe case reports do not document clearly thedevelopment of carcinoma during follow-up of his-tologically proven Menetrier's disease. In somereports the diagnosis of Menetrier's disease wasmade by radiology or endoscopy, and not confirmedhistologically.8 9 In others the histological details areeither scanty'° or show the presence of conditionsother than Menetrier's disease." In many reportsthe diagnoses of gastric cancer and Menetrier's dis-ease were either made simultaneously, or madewithin 12 months of each other, so that thedevelopment of carcinoma as a complication ofMenetrier's disease cannot be accepted as
proven."2- '5There appear to be only two previous reports of
patients developing carcinoma more than 12 monthsafter the diagnosis of Menetrier's disease wasmade.'6'7 These patients both died of metastaticgastric cancer five and five and a half years respec-tively after the diagnosis of Menetrier's disease wasmade. The present case is thus unique in thatfollow-up endoscopy and biopsy allowed the detec-tion of gastric cancer at a potentially curable stage.Due to the rarity of Menetrier's disease, it is
unlikely that clearer data on the risk of carcinomawill ever become available. From our experience, werecommend annual endoscopy and biopsy in cases ofMenetrier' s disease managed medically. Biopsiesshould be taken from the antrum and body of the
1 074
copyright. on 3 January 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1071 on 1 Septem
ber 1983. Dow
nloaded from

Intramucosal carcinoma of the gastric antrum complicating Menetrier's disease
4L~~~~~~e9~~~ ,. *.r
4,~~~~~~~~~V
a
Fig. 5 Low power view (a) and high power view (b) ofthe antral biopsy from the gastrectomy specimen demonstratingintramucosal carcinoma spreading superficially and features ofMenetrier's disease. Haematoxylin and eosin (a) x 80 (b) x200.
stomach, and should be taken both from areas ofstomach macroscopically affected by the Menetrier'sdisease and from apparently normal mucosa.Patients who have had partial gastric resections forMenetrier's disease should be followed-up similarly.No cases have yet been described of gastric car-cinoma developing in the gastric stump after surgeryfor Menetrier's disease, though the publishedfollow-up data is scanty.
References
'Scharschmidt BF. The natural history of hypertrophic gas-tropathy (Menetrier's disease). Am J Med 1977;63:644-52.
2 Cooper BT, Chadwick VS. Menetrier's Disease. In: Baron JH,Moody FG, eds. Foregut. London: Butterworth & Co,1981: 141-91.
3Butz WC. Giant hypertrophic gastritis. Gastroenterology1960;39: 183-90.
4 Steigmann F, Hyman S, Kannapel WL. Large gastric rugae:benign or malignant. Gdstroenterology 1957;32:72-84.
'Moeller DD, Dunn GD, Laing RR, Klotz AP. Hypertrophic gas-tropathy and carcinoma of the stomach. Gastrointest Endosc1970;16: 159-63.
6 Okabe H. Growth of early gastric cancer. In: Murakami T, ed.Early gastric cancer. Gann 1971;11:67-79.
'Menetrier P. Des polyadenomes gastriques et de leurs rapportsavec le cancer de l'estomac. Arch Physiol Norm Pathol1888;1:32-55; 236-62.
Texter EC, Legerton CW, Reeves RJ, Smith AG, Ruffin JM.Coexistent carcinoma of the stomach and hypertrophic gas-
tritis. Report of a case with review of the literature. Gastroen-terology 1953;24:579-86.
Matzner MJ, Raab AP, Spear PW. Benign giant gastric rugaecomplicated by submucosal gastric carcinoma. Gastroenterol-ogy 1951;18:296-302.
'° Palumbo LT, Rugtiv GM, Cross KR. Giant hypertrophic gas-tritis: its surgical and pathological significance. Ann Surg1951 ;134:259-67.
"Mills GP. Multiple polyps of the stomach (gastritis polyposa)with report of a case. Br J Surg 1922;10:226-31.
2 Stamatakis JD. Menetrier's disease and carcinoma of thestomach. Proc R Soc Med 1976;69:264-5.
3 Vazquez ME, Vazquez IJL, Campo MJ, Valbuena RL.Gastropatia hipertrofica-hiperplasica (enfermedad deMenetrier) asociada a carcinoma gastrico superficial:presentacion de un caso. Rev Esp Enferm Apar Dig (Madrid)1978;54: 173-82.
4 Rubin RG, Fink H. Giant hypertrophy of the gastric mucosaassociated with carcinoma of the stomach. Am J Gastroenterol1967;47:379-88.
"Sanner CJ, Saltzman DA, Mueller JC. Polypoid gastritis. Reportof a case associated with gastric adenocarcinoma and review ofthe literature. Am J Dig Dis 1978;23:19s-24s.
"Chusid EL, Hirsch RL, Colcher H. Spectrum of hypertrophicgastropathy. Arch Intern Med 1964;114:621-8.
"Von Loewenthal M, Steinitz H, Friedlander E. Gastritis hyper-trophica gigantea und magenkarzinom. Gastroenterologia(Basel) 1960;93:133-44.
Requests for reprints to: Dr GM Wood, Department ofMedicine, St James's University Hospital, Leeds LS9 7TF,England.
1 075
copyright. on 3 January 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.9.1071 on 1 Septem
ber 1983. Dow
nloaded from