ct scans of the head: a neurologist’s perspective lara cooke january 15, 2009
TRANSCRIPT

CT Scans of the Head:A Neurologist’s Perspective
CT Scans of the Head:A Neurologist’s Perspective
Lara CookeJanuary 15, 2009

ObjectivesObjectives
• At the end of this session, residents should be able to:• Identify key anatomic structures on CT• Apply an approach to reading a CT of the head• List reasons to image a patient with headache• Identify CT signs of raised ICP, early ischemia• Describe the clinical presentation of dural sinus
thrombosis• Distinguish between intracranial hemorrhages

General Principles of the CT
General Principles of the CT
• CT is basically a specialized X-Ray• We talk about “density” or
“attenuation”• The image is a measure of
absorption of X-rays through different angles through a given tissue and then transformed mathematically

What is hyperdense vs hypodense on CT?
What is hyperdense vs hypodense on CT?
• Bone (dense calcium) (1000 HU)• Metal• Acute (but not hyperacute) blood (56-76
HU) • Thrombosis• Grey matter>white matter (30, 20 HU)• CSF (0 HU)• Fat (-30-100 HU)• Air (-1000)

General Principles:General Principles:
• Are there any fractures?• Use bone windows• Look around the orbits, skull base, zygoma
• Remember to look at the sinuses (frontal, maxillary, ethmoid, sphenoid, mastoid air cells)• Should be black & full of air--look for
hyperdense fluid levels, thickening of mucosa, cysts….especially when the patient complains of headache

BonesBones
Fracture

SinusesSinuses
Sphenoid Maxillary
Frontal
Ethmoid

General PrinciplesGeneral Principles
• Look at the dura• Is there anything ‘extra’ between the
brain and the skull?• Hygroma• Blood• Tumor• Air

Things between skull & brain that shouldn’t be there
Things between skull & brain that shouldn’t be there
Hygroma
MeningiomaSubduralhematoma
PneumocephalyEpidural hematoma

General PrinciplesGeneral Principles
• Look at the brain:• Grey-white differentiation• Basal ganglia• Internal capsule• Corona radiata• Is there blood? Is there edema? Is
there CSF due to encephalomalacia/cysts? Is there a mass?

GW DifferentiationAnatomic StructuresGW Differentiation
Anatomic StructuresAnterior horn of lateral ventriclecaudate
Internalcapsule(post. limb)
lentiform
Pineal gland3rd ventricle
thalamus
Sylvian fissure
Insular ribbon

General PrinciplesGeneral Principles
• Look at the spaces• Ventricles:
• Can you see all the ventricles?• Is there hydrocephalus?
• Cisterns• Are the normal spaces around the brainstem still
visible?
• Dural Sinuses• Can you see them?• Are they thicker or brighter than usual?

CaseCase
• 43 yo woman with headache x 3 weeks
• Presents to hospital with double vision
• Low grade fever• On examination, weakness of EOM
of left eye, mild proptosis, red eye

What do you see?What do you see?
Sphenoidsinusitis

CT is good at showing…CT is good at showing…
• Bony abnormalities• Acute blood• Large masses (and small enhancing
masses if contrast is given)• Calcified intracranial abnormalities• Edema• Large intracranial aneurysms (now we
have CTA which is very good at this!!!)• stroke

CT might miss…CT might miss…• Subacute subdural (isodense to brain)• Isodense tumors/infections with little mass
effect/edema associated• Small aneurysms• Vasculitis• Vascular malformations• Dural sinus thrombosis• Lesions in the posterior fossa• Demyelination/white matter disease• Stroke• Meningeal processes• Diffuse axonal injury

Yield of CT for headacheYield of CT for headache
• CT is generally low yield if a thorough neurologic exam is normal (including LOC/mentation)
• CT is higher yield with focal findings, decreased LOC
• In typical migraine with normal exam, yield is 0.18%

Normal CTNormal CT
Maxillary sinusair-fluidlevel
Brainstem-medulla

Normal CTNormal CT
Superior ophthalmic vein
Temporal lobe
Mastoid air cells
Cerebellum
Sphenoid sinus
4th ventricle
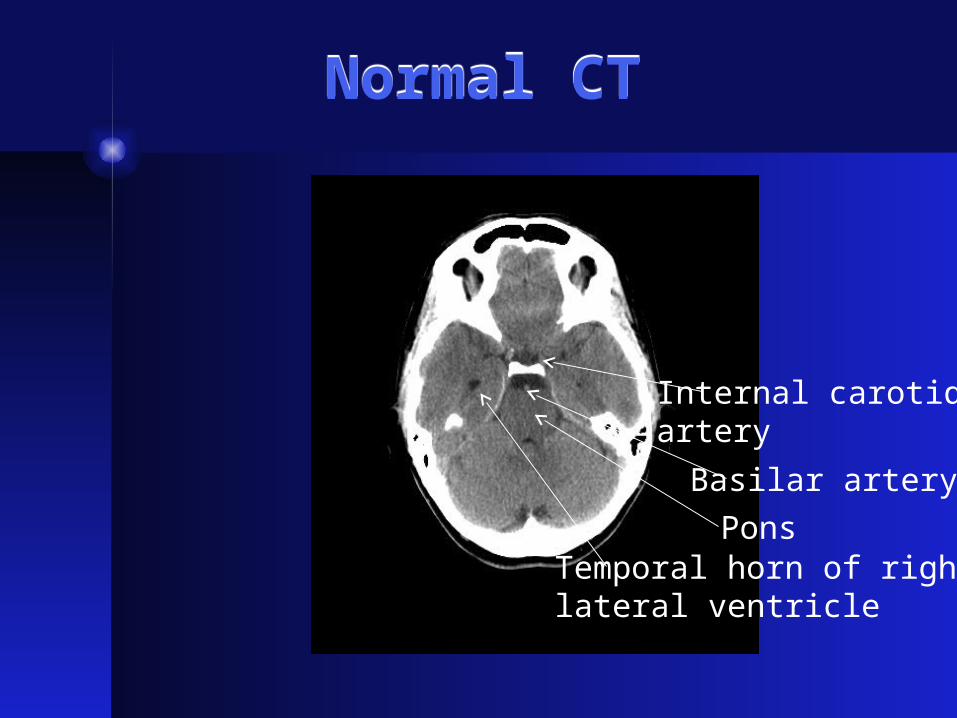
Normal CTNormal CT
Internal carotidartery
Basilar artery
PonsTemporal horn of rightlateral ventricle

Normal CTNormal CT
Left MCA
Suprasellar cistern
Cerebral aqueduct

Normal CTNormal CT
Cerebral peduncleInterpedulcular cistern

Normal CTNormal CTAnterior hornof left lateralventricle
Caudate
Lentiform
Posterior limbof internalcapsule
Thalamus3rd ventricleSylvian fissure
Insular ribbon

Normal CTNormal CT

Normal CTNormal CT
Falx cerebrei
Superior sagittal sinus


Normal or Not Normal?Normal or Not Normal?

Normal or not normal?Normal or not normal?

Normal or Not Normal?Normal or Not Normal?
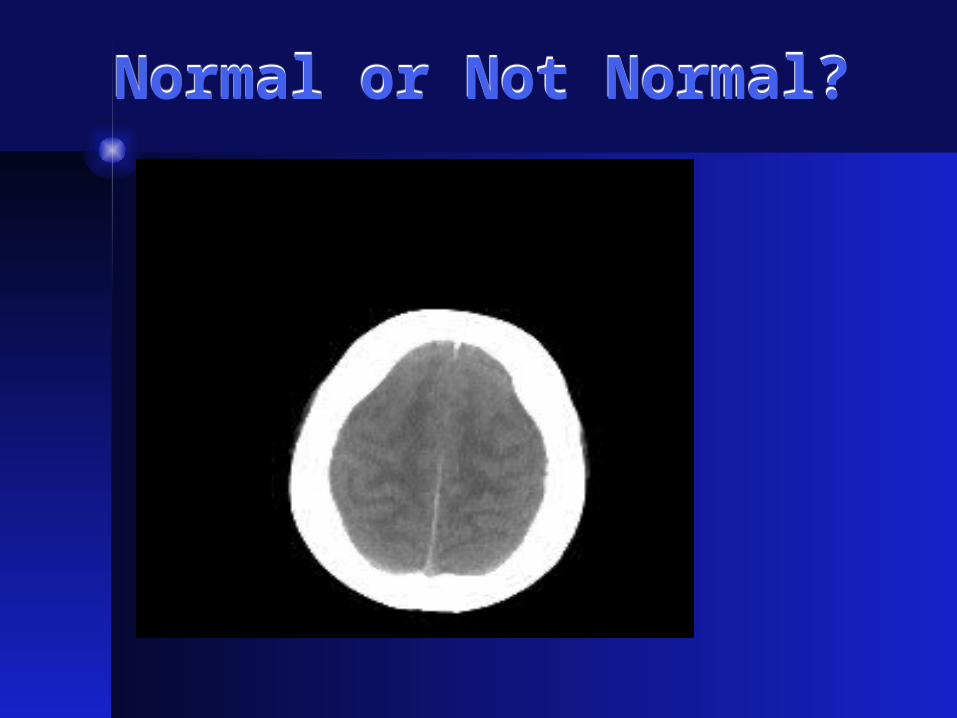
Normal or Not Normal?Normal or Not Normal?

Raised Intracranial Pressure: What to look for
Raised Intracranial Pressure: What to look for
• Loss of basal cisterns• Loss of suprasellar cistern
(unilateral or bilateral)• Loss of sulcal/gyral pattern• Loss of grey-white differentiation• Enlarged “trapped ventricles”• Slit-like ventricles

Valproic Acid OverdoseValproic Acid Overdose

Valproic Acid OverdoseValproic Acid Overdose

Posterior FossaPosterior Fossa

Posterior Fossa Day 3Posterior Fossa Day 3

When not to do an LPWhen not to do an LP

Raised ICPRaised ICP
• Do not do an LP if: • you suspect raised ICP• You see a mass or structural lesion with
mass effect (e.g. hematoma)• You see mass effect (displaced structures
like the falx, uncus, ventricles)• You cannot see the basal cisterns• You see hydrocephalus• You have not done a CT, there are neuro
findings/altered LOC and you work in a tertiary care centre where this test is readily available

When should you image a headache patient?
When should you image a headache patient?
When should you order CT for headache?
When should you order CT for headache?
• Any unexplained neurologic signs• Altered LOC• New headache type in an older
patient• Change in pattern of previous
headache• Progressive headache• Thunderclap headache• Refractory headache

Headache Red Flags…CT please!
Headache Red Flags…CT please!
• Abnormal neuro exam• Headache worst on waking in a.m.• Headache waking patient from sleep• Progressive headache• Worse with valsalva• Worse supine than upright • Abrupt onset headache• Other condition predisposing to CNS
disease (immune suppressed, cancer, clotting disorder, anticoagulants, recent trauma, etc)


35 yo man, assaulted with pipe35 yo man, assaulted with pipe
Intracerebralhemorrhage
Epiduralhematoma
Subarachnoidhemorrhage
Obliteration of ant horn of Rlateral ventricle

assaultassault
Midline shift

66 yo man with subacute onset of language difficulty
66 yo man with subacute onset of language difficulty
Hypodense mass
Edema
Midline shift

wetwet
Ring enhancing

47 yo man with RA and vertigo47 yo man with RA and vertigo
Cerebellarhemorrhage

CaseCase
• 39 yo man with polycystic kidney disease
• CT head was done for headache• Normal neuro exam

What do you see?What do you see?
Small hyperdenselesion
CaseCase
• 18 yo girl with a history of ITP• Presents with bizarre behaviour,
difficulty walking and headache• On exam appears ‘indifferent’ to her
‘state’• Moves both sides well with
encouragement• Left side ‘lags’ behind when she
gets off bed

CTCT
Enlarged corticalveins

MRV & MRIMRV & MRI

Dural Sinus ThrombosisDural Sinus Thrombosis
• May present with chronic progressive headache
• May present with thunderclap headache
• May or may not have abnormal neurosigns

Predisposing FactorsPredisposing Factors
• OCP +/-smoking• Pregnancy/post-partum• Clotting disorder (APA, ACA, Pr C, ATIII,
S deficiencies, Factor V Leiden, cancer, IBD, nephrotic syndrome)
• Dehydration• Local occlusion by trauma/tumor• Infection (meningitis, mastoiditis,
sinusitis, dental abscess)

What you might see on CTWhat you might see on CT
• Nothing at all• Hyperdense/misshapen/thickened dural
sinus or cortical vein• Hyperdense/empty delta (empty on
enhanced CT) (do not hang your hat on this to r/o DST)
• Venous infarct (wedge shaped, grey-white junction, associated hemorrhage, deeper white matter, non-arterial territory
• May be bilateral• Diffuse edema/raised ICP

DSTDST
• Often missed• 25% don’t have predisposing
factors• Ask yourself if this is a possibility
whenever you want to scan a patient for headache
• Remember the redflags• Remember to look at the fundi

Case IICase II
• 89 yo woman with progressive confusion and intermittent spells lasting 10-20 min of word-finding difficulties
• Headache for two weeks--moderate, dull, holocephalic
• 1) additional history you would like?• 2) do you want to do a CT?

Acute on chronicSDH

Key Points:Key Points:
• Older people are at risk due to atrophy + tearing of bridging veins
• Ask about anticoagulants• Ask about recent minor trauma• Scan older people who have new
headache• Scan people with ‘TIAs’

Small SDH


Acute on chronicSDH

CaseCase
• 29 yo male involved in a bar-fight this evening
• Punched in the head - brief LOC then went home with his girlfriend
• Brought in 2 hours later with progressive decrease in LOC
• On exam, comatose, right pupil sluggish
• Do you want to do a scan?

Management?Management?
Epidural hematoma


Epidural hematoma
Acute on chronicSDH
Midline shift

Epidural hematoma

CaseCase
• 55 yo man fell off of a stool and struck head on concrete floor
• Had had some EtOH• Wife brought him in because he had some
slurred speech and inappropriate behaviour• Headache• On exam, smells like EtOH. Slurred speech.
Behaviour inappropriate. Nil focal.• What do you want to do?

Subarachnoidhemorrhage

Blood follows the pattern of gyri/sulci
Blood follows the pattern of gyri/sulci
Subarachnoidhemorrhage

“Pentagon Sign”“Pentagon Sign”
Subarachnoidhemorrhage

Pentagon sign + hydrocephalusPentagon sign + hydrocephalus
Temporal horn oflateral ventricle

CaseCase
• 40 y.o. man with new onset mild incoordination of the Left hand & behavioural change
• What do you want to know?
• What do you want to do?

Hypodense region& loss of G-W in M1
Loss of lentiformnucleus

Early Ischemic Changes: Clues to Stroke
Early Ischemic Changes: Clues to Stroke
• ASPECTS
• Out of 10
• M1, M2, M3, M4, M5, M6
• Caudate
• Lentiform nucleus
• Internal capsule
• Insular ribbon
• Also, look at MCA

ASPECT ScoreASPECT Score
• M1,2,3, IC, L, C

ASPECTSASPECTS
• M4-6

Looking for strokeLooking for stroke
• Time is brain
• Stroke more than 12 hours old begins to look quite hypodense (dark) in the affected arterial territory
• Acutely, there ARE subtle signs--which may alter likelihood of getting TPa and risk of hemorrhage

Subtle findingsSubtle findings
• Look at:• Grey-white differentiation• Presence/loss of sulcal/gyral pattern• Compare side to side - stroke is usually
unilateral--so you have a built-in comparator• Look for hyper dense, asymmetric, vessels• Look for loss of signal in deep structures (basal
ganglia, thalami, internal capsule)• Know the basics of vascular anatomy

80 yo man with dysphasia x 3hrs80 yo man with dysphasia x 3hrs
Loss of insularribbon
Loss of G-WDifferentiationIn M1, M2, M3

Same scan, superiorlySame scan, superiorly
Loss of GWdifferentiationin M4, M5, M6

12 hrs later12 hrs later


CaseCase
• 68 yo man with DMII, htn.
• Woke up with left-sided weakness, leg more than hand.

What do you see?What do you see?
HypodenseRegion - ACA

CaseCase
• 43 yo waiter
• Binge drinking
• Awoke at 4 am feeling nauseated/headache
• Awoke at noon unable to get out of bed
• Discovered by his mother & brought to hospital

Holiday HeartHoliday Heart

Monday morningMonday morning
CaseCase
• 28 yo woman, 2 days post partum
• Headache, left-sided, nausea, vomiting, photophobia, phonophobia, worsening with routine activity.
• What else do you want to know?What do you want to do?

What do you see?What do you see?

CaseCase
• Pt 3 weeks post-partum develps severe headache and left leg paresthesias
• Throbbing pain, photophobia, phonophobia, nausea, x 4 days
• Worse with valsalva & lying down

Post-Partum PatientPost-Partum Patient

CaseCase
• 43 yo man works at packing plant
• Developed acute onset of headache and left-sided weakness
• One exam, normal power on left, but complete sensory loss to all modalities and mild neglect
• PMHx; htn, DM
• Ran out of BP meds 2 months earlier

Left sensory loss & neglectLeft sensory loss & neglect
Thalamic ICH

Acute vertigo, N/V, then coma in 80 yo hypertensive man
Acute vertigo, N/V, then coma in 80 yo hypertensive man
Cerebellarhemorrhage

Hypertensive HemorrhagesHypertensive Hemorrhages
• Basal ganglia (putamen>caudate)
• Thalamus
• Pons
• Cerebellum
• Centrum semiovale
• Intraventricular (from basal ganglia)

CaseCase
• 68 yo RHD woman found wandering at work, speaking incoherently.
• PMHx: Htn, gout
• Discontinued BP meds one month ago

AphasiaAphasia

CaseCase
• 70 yo woman developed severe headache & confusion
• On examination, has receptive aphasia & mild expressive problems
• Right visual field abnormality (homonymous hemianopia)
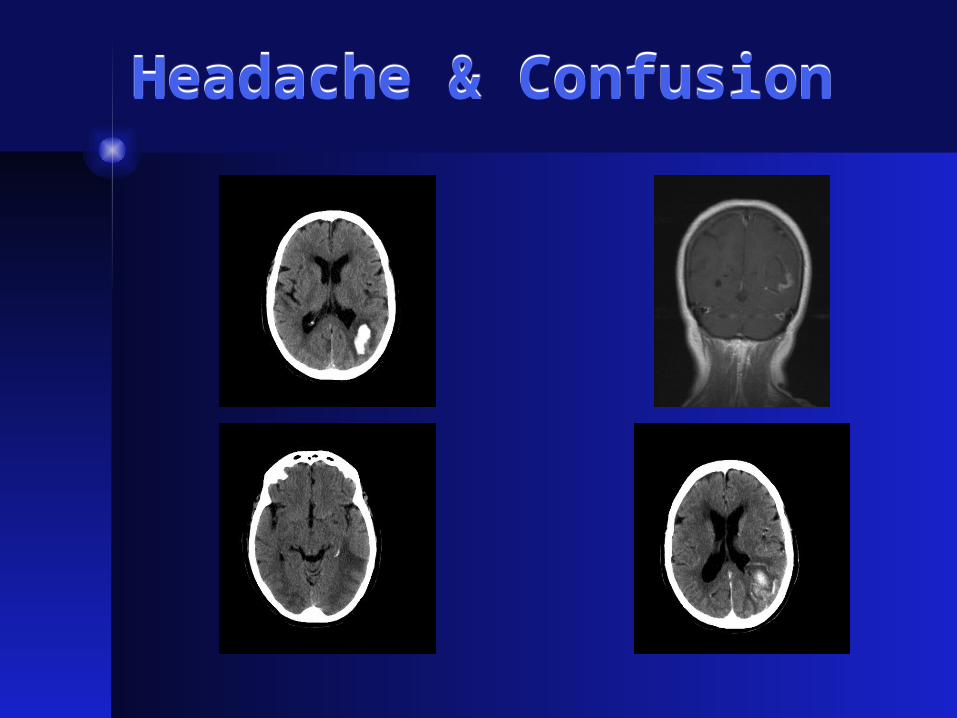
Headache & ConfusionHeadache & Confusion

CaseCase
• 65 yo man with gradual onset of left-sided weakness, now has decreased LOC.

??

CaseCase
• 49 yo woman with known breast cancer
• Presents with complaints of problems seeing
• Has L visual field defect

??
Multiple hyperdensefoci
Edema

CaseCase
• 65 yo man with colon Ca
• Presents with word finding difficulties and headache.
• Onset was acute.

??

Take-Home MessagesTake-Home Messages
- don’t LP if you think ICP might be up- Remember to look at more than
parenchyma: Bones, dura, sinuses, cisterns, ventricles, and dural sinuses
- Look for normal anatomy: grey-white margin, basal ganglia, insula, internal capsule
- Chronic blood is not bright--may be isodense, and therefore subtle

Messages about HeadacheMessages about Headache
• If there are focal findings, decreased LOC or red flag features: SCAN
• Ask yourself if this could be a dural sinus thrombosis
• Do LP query SAH, encephalitis, meningitis• Do not LP if you’re not sure about the CT• Do not LP without a CT in a tertiary care
centre (caveat--some clinical judgement here)

Messages about StrokeMessages about Stroke
• Compare side to side
• Changes may be present under 3 hours
• Image your TIA patients (sometimes they have something else--eg. SDH)
• A normal CT means better prognosis
• Early subtle signs mean more damaged tissue, greater risk of hemorrhage
• Time is brain

Tests that sometimes don’t happen, but should….
Tests that sometimes don’t happen, but should….
• If you think there may be a neuro problem, be sure to always do these parts of the CNS exam--otherwise you may miss the boat:• Look at the discs (don’t be shy about dilating)
• Check fields
• Look at nasolabial folds & forehead
• Look for drift
• Check toes
• Check for sensory extinction
• Walk your patient

I don’t know what the heck this is…
I don’t know what the heck this is…