cross contamination and infection control · cross contamination and infection control ... label...
TRANSCRIPT
Cross Contamination and Infection Control
Presented by: Onnicah D. Matuka
National Health Laboratory Services
National Institute for Occupational Health
PO Box 4788, Johannesburg, 2000, RSA
Practice No.: 5200296
Switchboard: + 27 (0) 11 712 6400
Website: http://www.nhls.ac.za
http://www.nioh.ac.za
DoL Shopsteward Workshop (KZN): 10 November 2015
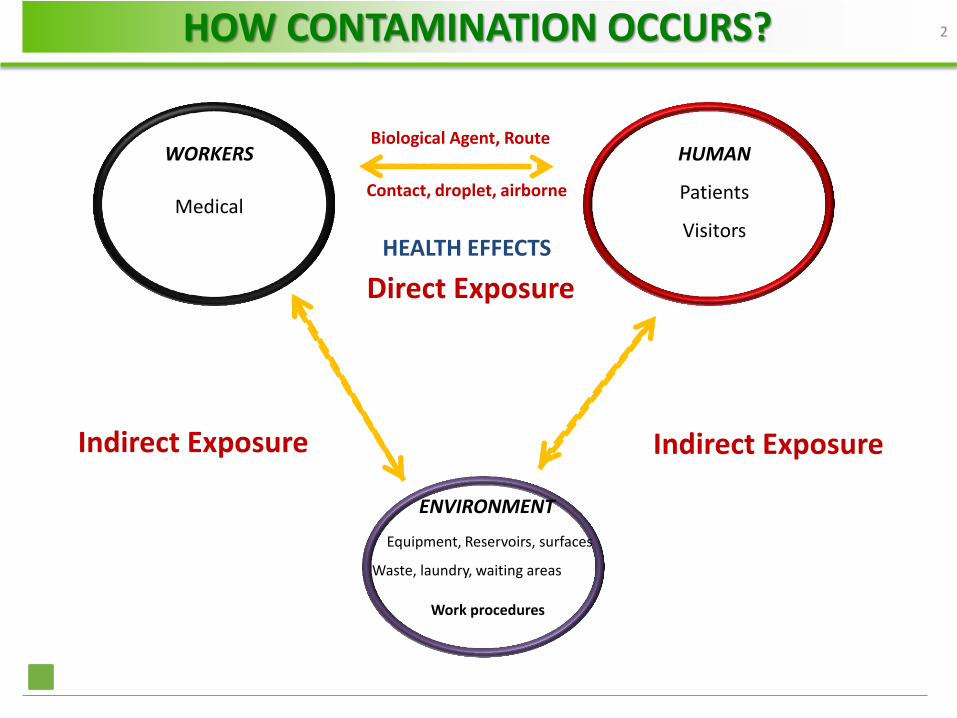
ENVIRONMENT
Equipment, Reservoirs, surfaces
Waste, laundry, waiting areas
Work procedures
HUMAN
Patients
Visitors
WORKERS
Medical HEALTH EFFECTS
Contact, droplet, airborne
Biological Agent, Route
Indirect Exposure
Direct Exposure
Indirect Exposure
HOW CONTAMINATION OCCURS? 2

Skin
Respiratory
tract
Gastro-
intestinal
tract
Mode of transmission
Vector
Ingestion
Inhalation
Contact
Site of entry
Needlesticks
TRANSMISSION ROUTES 3
Basic measures of IC (i.e. standard precautions)
Education and training of HCWs
Protection of HCWs (i.e. Immunization)
Identification of hazards and minimizing the risks
Routine practices (e.g. aseptic techniques)
NB. Must include support staff (cleaners, waste, laundry, porters)
INFECTION CONTROL PROGRAMME 4
Contact with blood and body fluids
HIV, Hepatitis B and Hepatitis C
Workers are at high risk of exposure
Sharps injuries (needles &scalpels)
Splashes (eyes and mouth)
Prevention: Hand hygiene & safety engineered devices
Don’t recap needles after use
Use sharp containers
BLOODBORNE PATHOGENS 5
Waste management
Segregate waste (sharps & boxes)
Sharps containers readily available
Don’t compress garbage bags by hand
Hold waste bags away from body
Transport waste in a dedicated trolley
Store waste in areas with restricted access
PREVENTION OF BLOODBORNE DISEASES 6
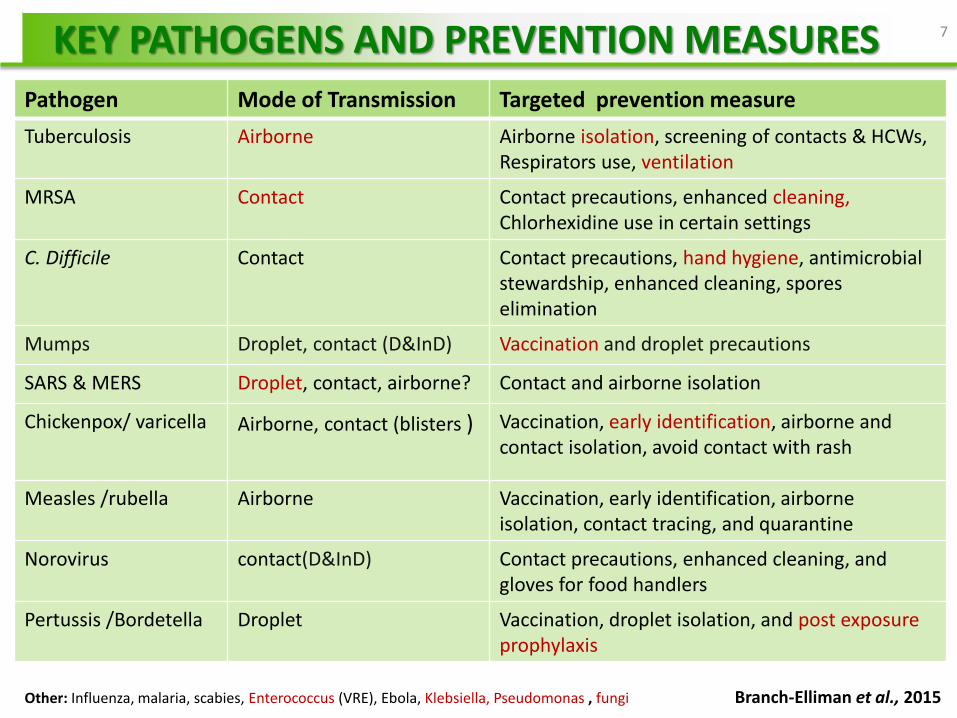
Pathogen Mode of Transmission Targeted prevention measure
Tuberculosis Airborne Airborne isolation, screening of contacts & HCWs, Respirators use, ventilation
MRSA Contact Contact precautions, enhanced cleaning, Chlorhexidine use in certain settings
C. Difficile Contact Contact precautions, hand hygiene, antimicrobial stewardship, enhanced cleaning, spores elimination
Mumps Droplet, contact (D&InD) Vaccination and droplet precautions
SARS & MERS Droplet, contact, airborne? Contact and airborne isolation
Chickenpox/ varicella Airborne, contact (blisters ) Vaccination, early identification, airborne and contact isolation, avoid contact with rash
Measles /rubella Airborne Vaccination, early identification, airborne isolation, contact tracing, and quarantine
Norovirus contact(D&InD) Contact precautions, enhanced cleaning, and gloves for food handlers
Pertussis /Bordetella Droplet Vaccination, droplet isolation, and post exposure prophylaxis
Other: Influenza, malaria, scabies, Enterococcus (VRE), Ebola, Klebsiella, Pseudomonas , fungi Branch-Elliman et al., 2015
KEY PATHOGENS AND PREVENTION MEASURES 7
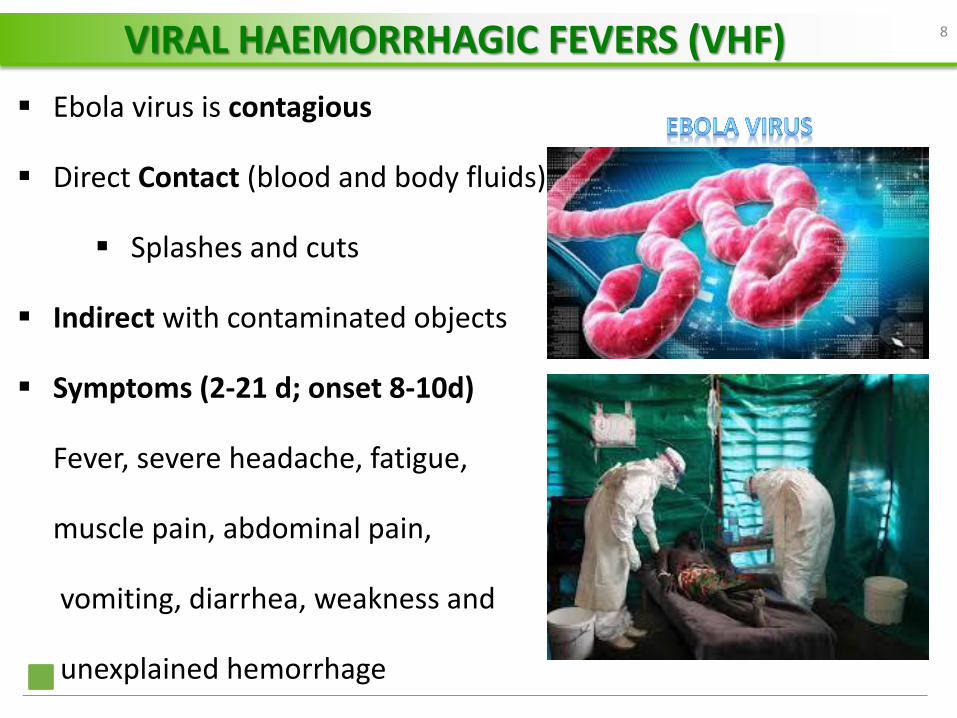
Ebola virus is contagious
Direct Contact (blood and body fluids)
Splashes and cuts
Indirect with contaminated objects
Symptoms (2-21 d; onset 8-10d)
Fever, severe headache, fatigue,
muscle pain, abdominal pain,
vomiting, diarrhea, weakness and
unexplained hemorrhage
VIRAL HAEMORRHAGIC FEVERS (VHF) 8
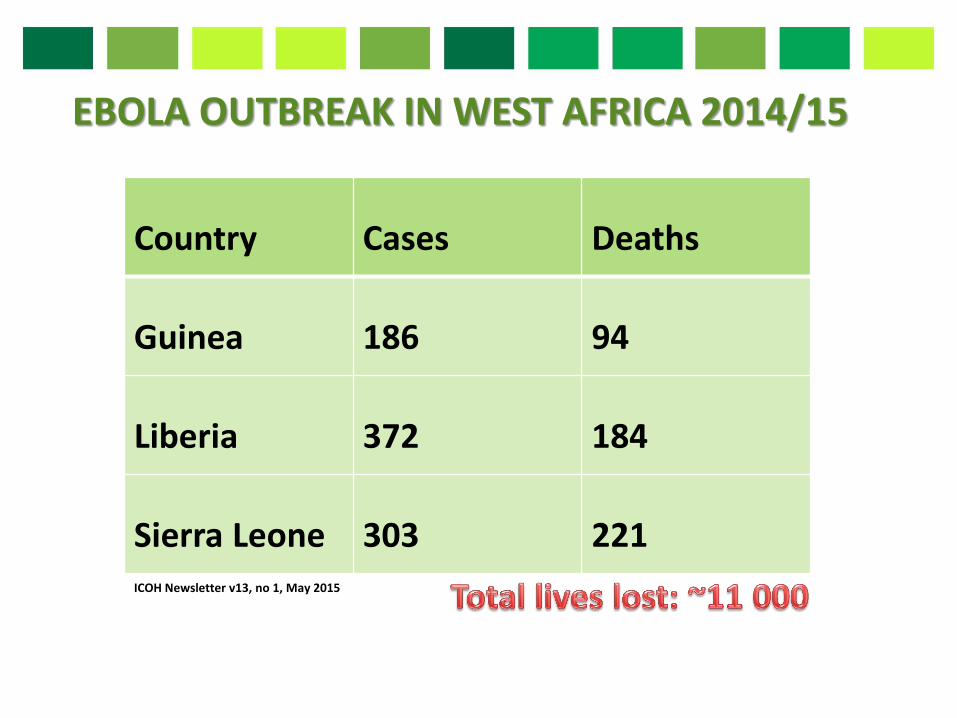
EBOLA OUTBREAK IN WEST AFRICA 2014/15
Country Cases Deaths
Guinea 186 94
Liberia 372 184
Sierra Leone 303 221 ICOH Newsletter v13, no 1, May 2015
Public and Occupational health problem
2nd highest infection rate - 22 high burden states
9th highest annual incidence rate (834/100 000)
Prevention and Control
TUBERCULOSIS IN SA 10
Detection & case isolation
HCWs must wear respirators
Install Ventilation
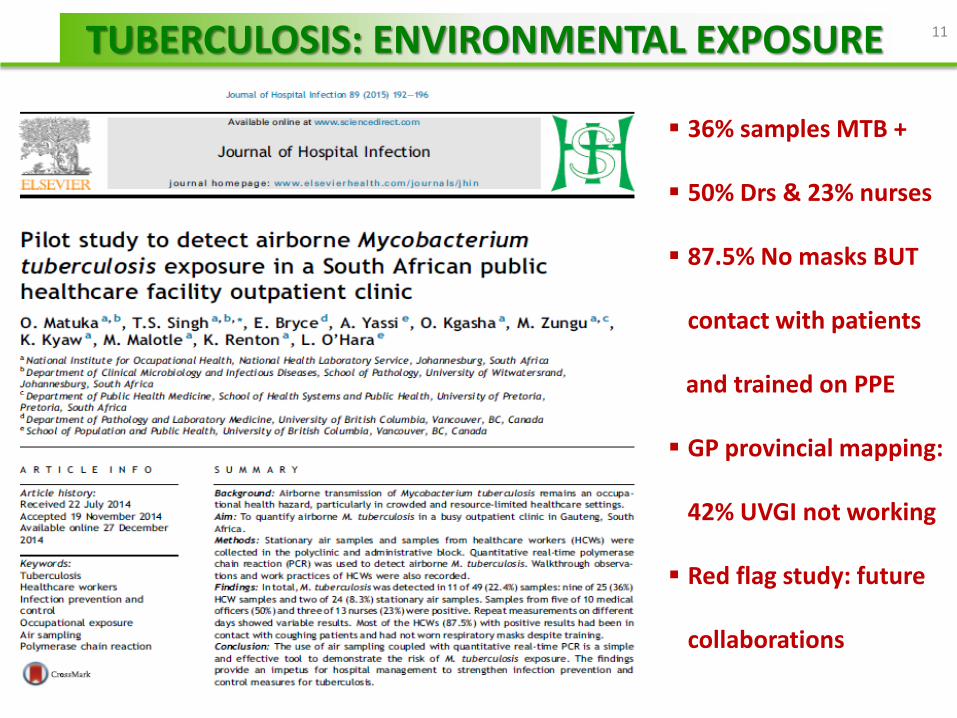
36% samples MTB +
50% Drs & 23% nurses
87.5% No masks BUT
contact with patients
and trained on PPE
GP provincial mapping:
42% UVGI not working
Red flag study: future
collaborations
TUBERCULOSIS: ENVIRONMENTAL EXPOSURE 11
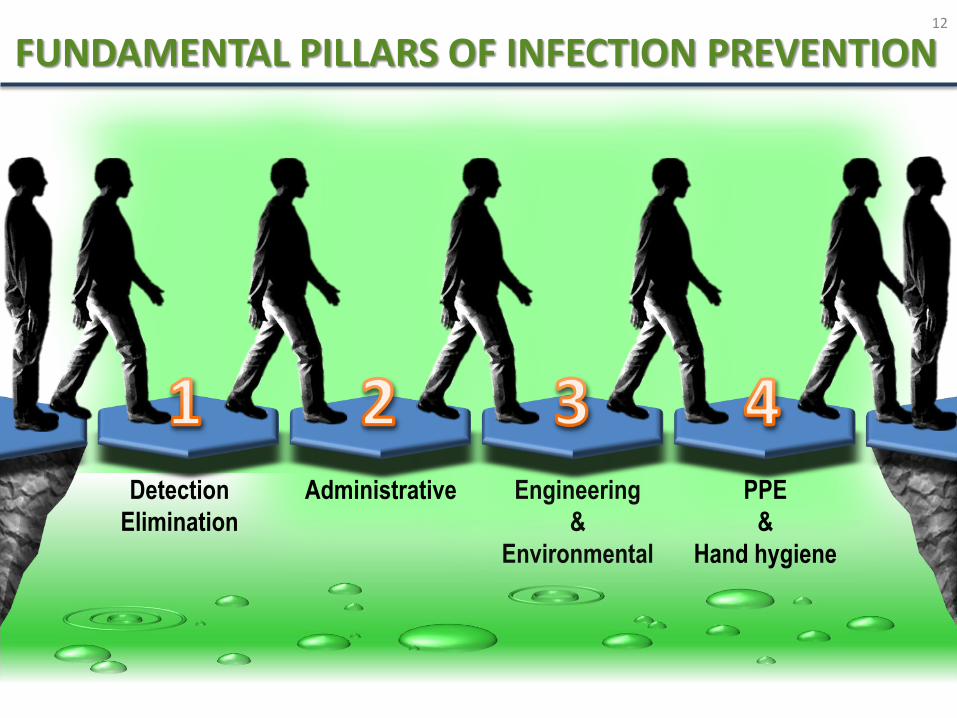
Detection
Elimination
Administrative Engineering
&
Environmental
PPE
&
Hand hygiene
12
FUNDAMENTAL PILLARS OF INFECTION PREVENTION
Public awareness campaigns or media attention
Screening for possible exposure (e.g. travel)
Identify key symptoms at healthcare facility
Diagnostic testing for “flagged” cases
Isolate suspicious cases
Notify the laboratory and authorities (IP)
Detection | Elimination
CASE DETECTION AND IDENTIFICATION
Policies and procedures to prevent transmission of MOs within the HC facility
Safe working practices to minimize the risk of exposure
Safe Disposal and Disinfection
Specific Emergency procedures (spills & incidences)
Administrative
Screening of high risk areas and Isolation
Vaccination is effective for Infection control
ADMINISTRATIVE PROCEDURES
Handle laundry carefully, hidden sharps may be present
Isolate contaminated laundry and bag separately
Place wet laundry in leak-proof bags
Label and Colour code contaminated laundry bags
Send directly to laundry, DO NOT rinse or sort in patient areas
Minimize agitation to avoid aerosolization of microbes
HANDLING CONTAMINATED LAUNDRY 15
Restrict access to the area
Wear PPE and gather the needed tools
Wipe up and dispose visible material
Decontaminate using fresh disinfectant (2% Jik-10min)
Clean and decontaminate all equipment
CLEANING UP SPILLS 16
HVAC systems
HEPA filters
Negative pressure
Dilution rate (6-12 ACH)
Install in risky areas (RA)
Isolation rooms and waiting areas
Critical care, operating rooms and transplant rooms
PPE must be worn (airborne precaution) Engineering | Environmental
Isolation rooms: prevent airborne pathogens transmission
Natural ventilation is superior to mechanical
Natural ventilation have more than Double ACH
Patients have low risk of TB acquisition after exposure
Natural ventilation is cost effective than mechanical
Haiti : 2 open air hospitals reduce respiratory infections
UVGI lamps or fixtures
Kimmelman, 2014
Escombe et al, 2007
VENTILATION: NATURAL VS MECHANICAL 18

Photograph courtesy: CSIR
Lack of maintenance
Poor installations
Effectiveness
Inferior designs
Dose Rec: 20 mW/m³ Photograph courtesy: CSIR
UVGI FIXTURES 19
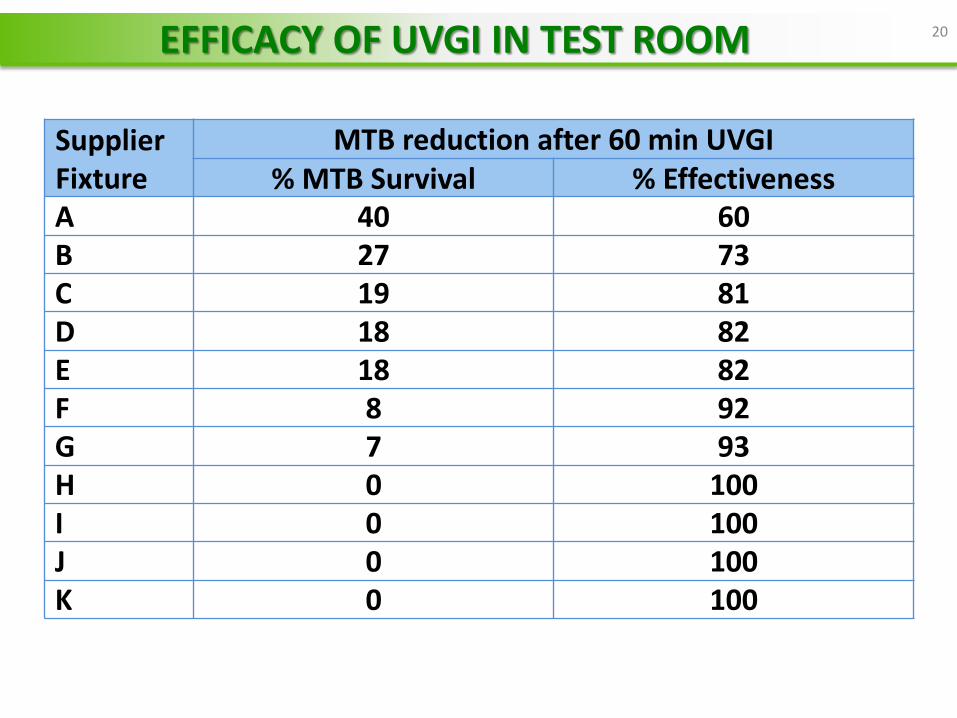
Supplier Fixture
MTB reduction after 60 min UVGI
% MTB Survival % Effectiveness
A 40 60 B 27 73 C 19 81 D 18 82 E 18 82 F 8 92 G 7 93 H 0 100 I 0 100 J 0 100 K 0 100
EFFICACY OF UVGI IN TEST ROOM 20
Water systems, cooling towers, showers
L. pneumophila
Pneumonia and Pontiac fever (“flu-like”)
Prevention Strategy
Water system maintenance ( Temp. & ClO2)
PPE (respirators) not a feasible measure of prevention – Mitigation is Environmental
Engineering | Environmental
LEGIONELLA OUTBREAKS
MERS survive up to 2 days
Calciviruses (e.g. norovirus)
Resistant to standard disinfectants
Transferred to food (at least 7d)
Prevention Strategy
MDR- H202 vapour (Pasaretti et al., 2013)
C.dificille H202 deep cleaning
(Best et al., 2014)
ENVIRONMENTAL PERSISTENT AGENTS 22
GOWNS and GLOVES
Pathogens transmitted by contact
Skin protection -blood & body fluids
GOGGLES: Eye splashes, Blood splatter
RESPIRATORS AND MASKS:
Reduce risk of inhaling or spreading aerosols
Other: Aprons, boots, hair and shoe covers PPE | Hand hygiene
PERSONAL PROTECTIVE EQUIPMENT 23
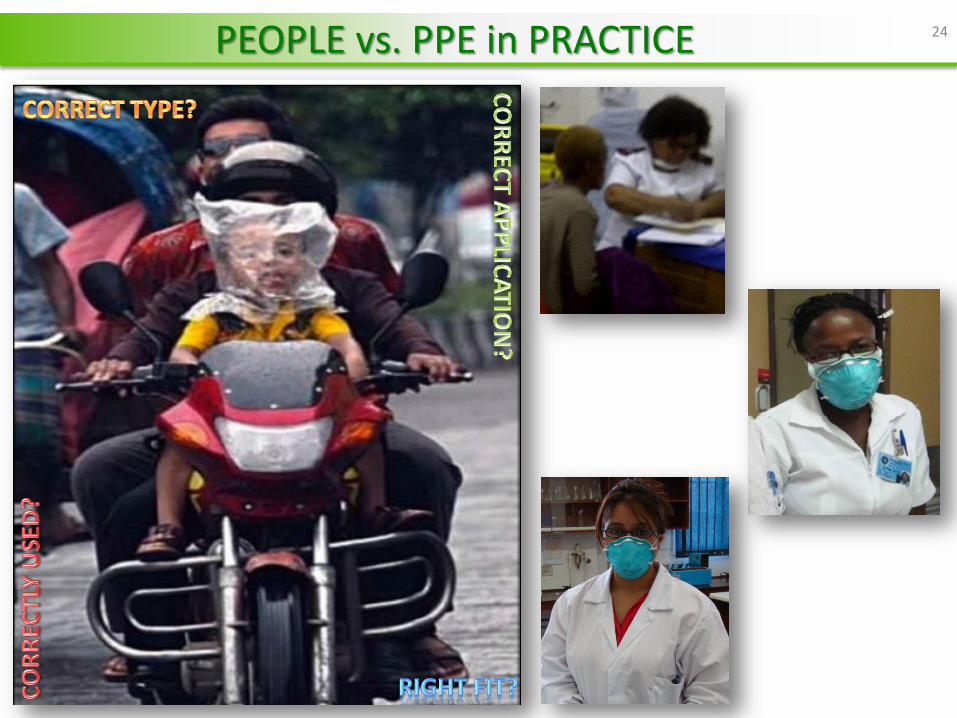
PEOPLE vs. PPE in PRACTICE 24
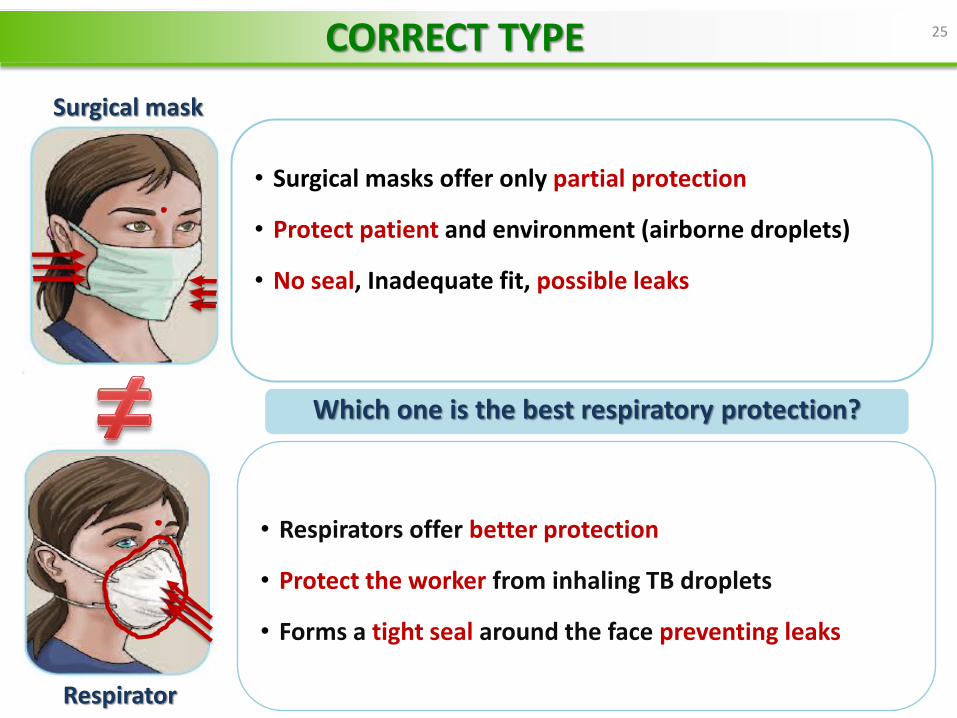
Which one is the best respiratory protection?
Surgical mask
Respirator
• Surgical masks offer only partial protection
• Protect patient and environment (airborne droplets)
• No seal, Inadequate fit, possible leaks
25
• Respirators offer better protection
• Protect the worker from inhaling TB droplets
• Forms a tight seal around the face preventing leaks
CORRECT TYPE
26
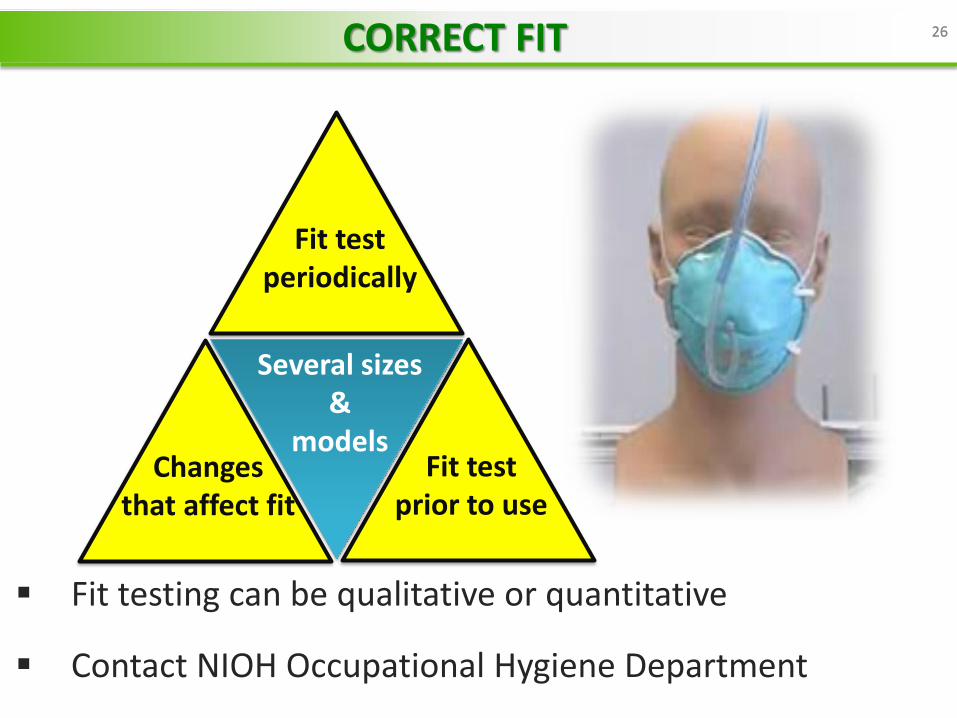
Fit testing can be qualitative or quantitative
Contact NIOH Occupational Hygiene Department
Several sizes &
models Fit test
prior to use Changes
that affect fit
Fit test periodically
26 CORRECT FIT
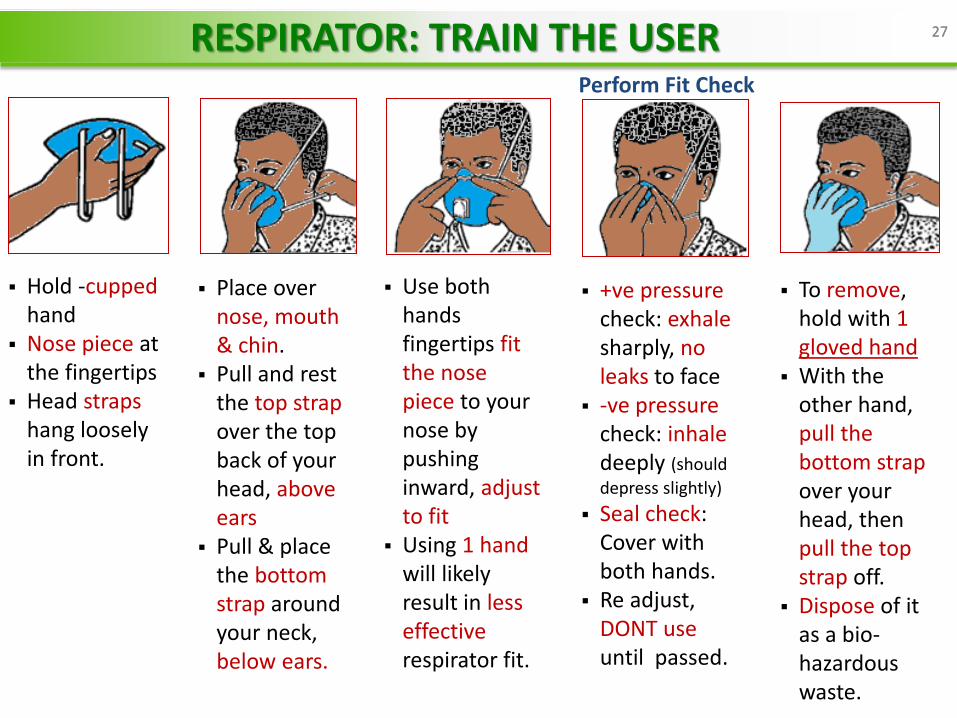
Hold -cupped
hand Nose piece at
the fingertips Head straps
hang loosely in front.
Place over nose, mouth & chin.
Pull and rest the top strap over the top back of your head, above ears
Pull & place the bottom strap around your neck, below ears.
Use both hands fingertips fit the nose piece to your nose by pushing inward, adjust to fit
Using 1 hand will likely result in less effective respirator fit.
+ve pressure check: exhale sharply, no leaks to face
-ve pressure check: inhale deeply (should
depress slightly)
Seal check: Cover with both hands.
Re adjust, DONT use until passed.
To remove, hold with 1 gloved hand
With the other hand, pull the bottom strap over your head, then pull the top strap off.
Dispose of it as a bio-hazardous waste.
Perform Fit Check
27 27 RESPIRATOR: TRAIN THE USER
Low cost and highly effective
Wash contaminated hands with soap and water
Before leaving work area Before and after patient care and between patients After handling blood and contaminated items Before eating and after using the bathroom Immediately after removing gloves
Hand sanitation (Alcohol rubs or Gemstar etc.)
not effective for some organisms e.g. C.dificille
28 28 HAND HYGIENE
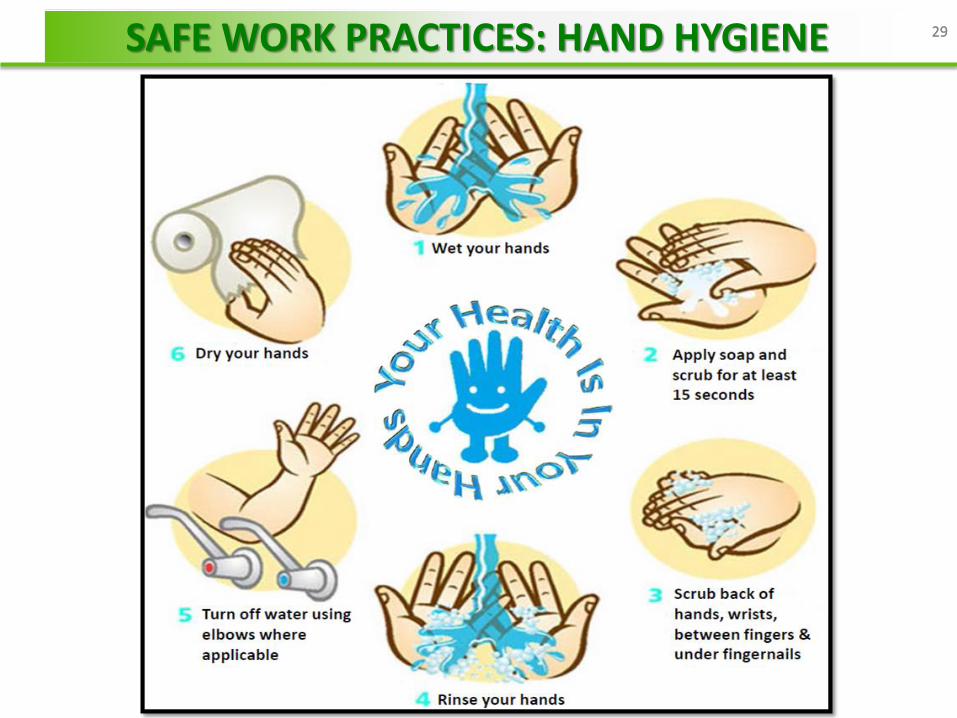
29 29 SAFE WORK PRACTICES: HAND HYGIENE
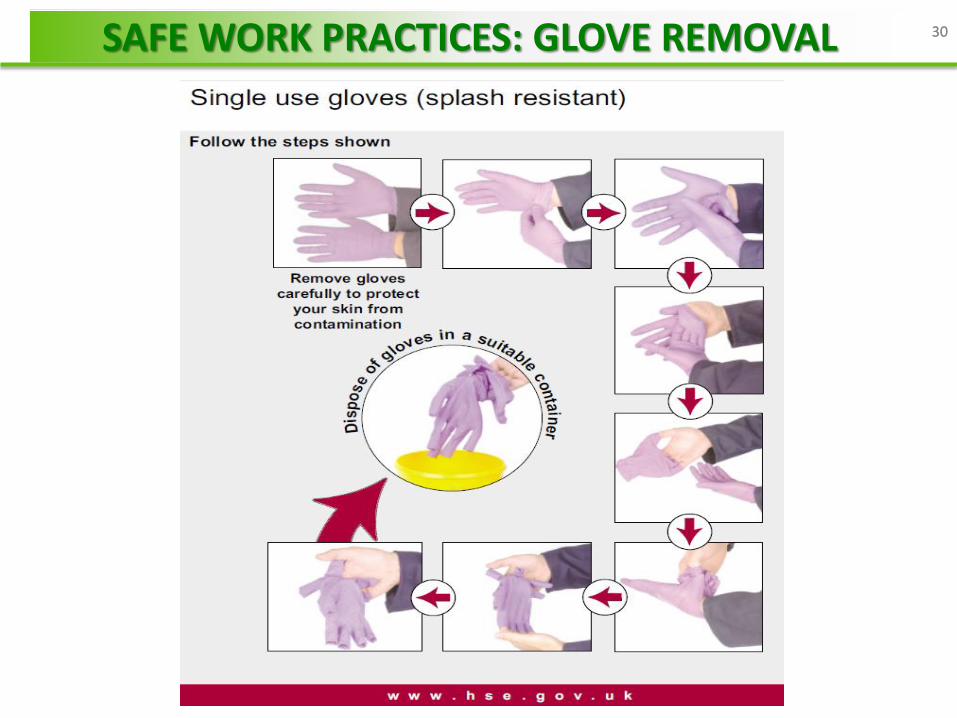
30 30 SAFE WORK PRACTICES: GLOVE REMOVAL
SURVEYS OBSERVATIONS AND INTERVIEWS
Isolation not always possible due to lack of space
Lack of PPE supply or non compliance
Inappropriate masks used in risky areas
Staff don’t adhere to best practices despite being
trained
Engineering controls not functional or not maintained
Costs implications (N95, UVGI service, fit testing)
PERCEPTIONS
Overworked staff-decreased compliance-increase
infections
31 31 CHALLENGES FOR IMPLEMENTATION OF IP

PREVENTION IS BETTER THAN CURE
THANK YOU
Direct line: 011 712 6487
Switchboard: 011 712 6400