cronicon · corneal pseudo guttae can be noticed after trauma, intraocular inflammation, infection,...
TRANSCRIPT

CroniconO P E N A C C E S S EC OPHTHALMOLOGY
Case Report
A Review of Fuchs Endothelial Dystrophy
Rubina Shah*, Kamran Wali and Afzal Hussian
National Eye center, Lahore, Pakistan
Citation: Rubina Shah., et al. “A Review of Fuchs Endothelial Dystrophy”. EC Ophthalmology 9.3 (2018): 148-153.
*Corresponding Author: Rubina Shah, National Eye center, Lahore, Pakistan.
Received: January 11, 2018; Published: February 28, 2018
Abstract
Fuchs endothelial dystrophy is known for bilateral, asymmetrical, gradual progression with major loss of vision due to corneal odema. It can be inherited as autosomal dominant transmission. The endothelial cells synthesize a thickened Descemet’s membrane with focal excrescences of altered basement membrane material (guttae).
Keywords: Corneal Edema; Corneal Endothelium; Corneal Transplantation; Descemet’s Membrane; Fuchs’ Dystrophy Growth Factors; Guttae
In this article a brief review about the disease early presentation, histopathology, epidemiology and possible influencing factors are discussed. The current management protocol is summarized.
Introduction
Fuchs initially described bilateral corneal stromal and epithelial edema in elderly patients, without the benefit of slit lamp microscopy [1]. Fuchs’ endothelial corneal dystrophy (FECD) is progressive diseases which can initial begin in the fifth through seventh decades in life. An autosomal dominant inheritance pattern shows fifty percent of family clustering [2-6]. Where Females are susceptible to Fuchs’ dystrophy that develops corneal guttae 2.5 times more than males, corneal edema progressing 5.7 times more often than males [6]. Ma-govern., et al. explained a family association with early-onset FECD that recently has been recently diagnosed to have a distinct genetic loci and mutations from adult onset of disease [4,7].
A 50 year male patient presented with chief compliant of tearing, photophobia, Halos around light and irritation with mild to moderate pain, foreign body sensation, and gradual loss vision for distance and near in right eye more than left. Visual acuity noted was 20/120 OD and 20/80 OS. Best corrected visual acuity was not improving in right eye whereas +2.00/-1.00*80 vision improved by 20/30 with N12 OD and N5 OS respectively.
His ocular history was presbyopia and spectacle wear for 10 years. Patient medical history was positive for diabetes and hypertension. He was using medication for both but couldn’t recall his prescription. Family ocular history was positive as his sister has the same malady of decline vision with sign and symptoms.
Case Study
Social history was not showing any drugs like alcohol, tobacco and recreational drug use. He was oriented to time place and person. The intraocular pressure checked was 20 mmHg OD and 16 mmHg OS at 10.00 am. Confrontation wasn’t applicable while extra ocular movements was orthophoric for near and distance. Patient was examined thoroughly with and without fluorescein instillation.
As shown in picture slit lamp biomicroscopy revealed central corneal guttae right eye. On direct illumination technique the guttae appear as dark spot on the posterior surface of corneal (Figure 1) and a dew drop resemblance on retroillumination (Figure 2). To an inexperienced person it would be cumbersome to correctly differentiate from guttae as pigment dusting often present on the endothelium layer. Patients at initial stage of disease are asymptomatic. The guttae spread peripherally to coalesce centrally changing to a beaten metal appearance associated with hyperpigmentation. Descemet’s membrane becomes prominently thickened, grayish, and irregular. Clinical appearance may show ‘buried guttae’ centrally with fibrous thickening of Descemet’s membrane covered the presence of guttae [6,8].
149
A Review of Fuchs Endothelial Dystrophy
Citation: Rubina Shah., et al. “A Review of Fuchs Endothelial Dystrophy”. EC Ophthalmology 9.3 (2018): 148-153.
Figure 1: Courtesy of Jay H. Krachmer, MD, University of Minnesota.
Figure 2: Photo courtesy of Brice Critser, CRA.
Citation: Rubina Shah., et al. “A Review of Fuchs Endothelial Dystrophy”. EC Ophthalmology 9.3 (2018): 148-153.
A Review of Fuchs Endothelial Dystrophy
150
Figure 3: Photo courtesy Rubi Shah National Eye Center.
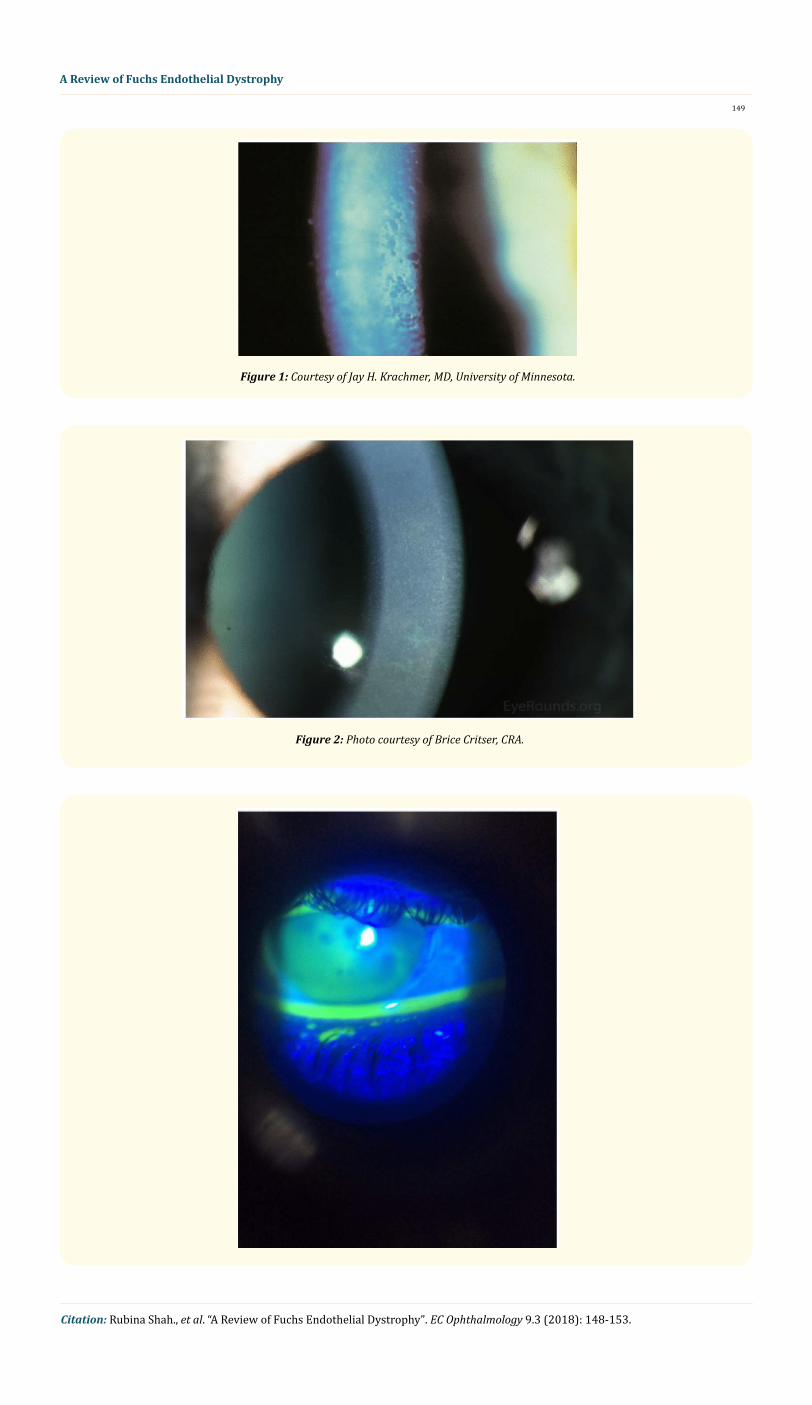
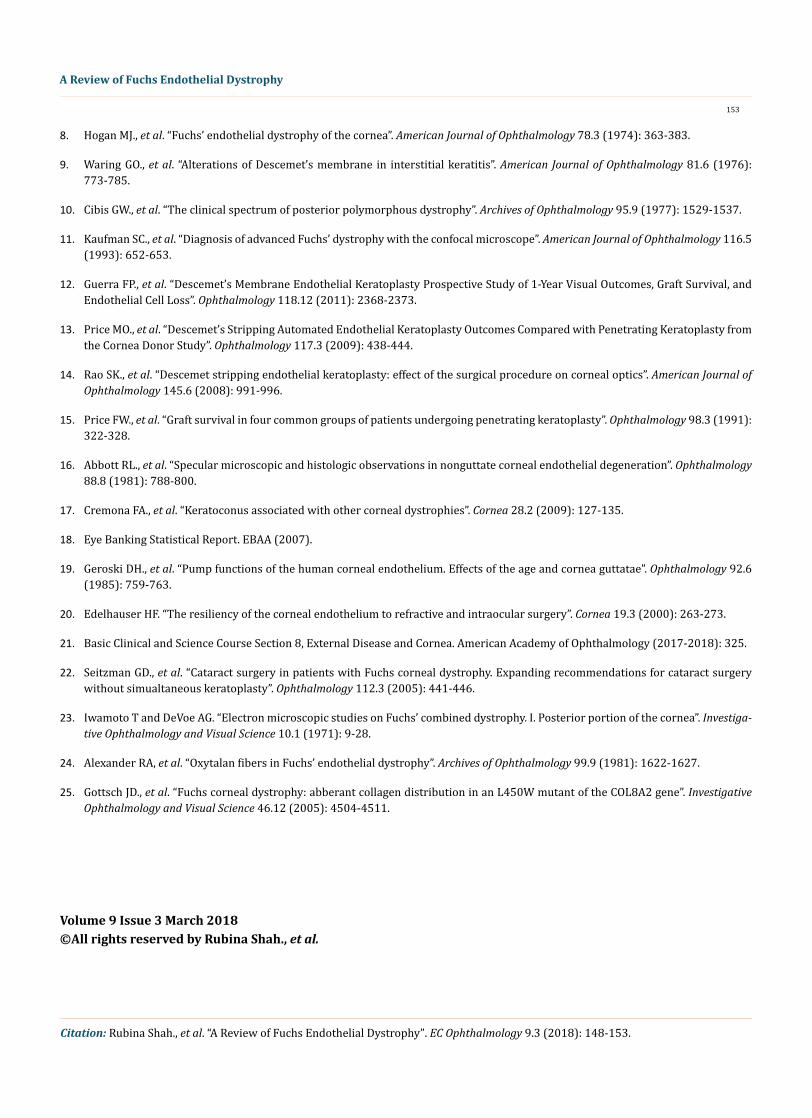
As shown in figure swelling of the corneal stroma right eye produced prominent vertical wrinkles or striae in Descemet’s membrane slightly noticed due to poor resolution of camera. A stippled pattern is noticeably followed by microcystic epithelial edema. The disrup-tion of tear film was highlighted by using fluorescein staining.
Vision deteriorated most prominently in the morning. Stromal edema progressively caused in a ground-glass opacification and central cornea showed markedly thickening. The epithelial microcystic changes unite to form bullae leads to epithelial erosions and fingerprint lines pattern. Vision can reduce further due to stromal haze and irregularities of corneal surface.
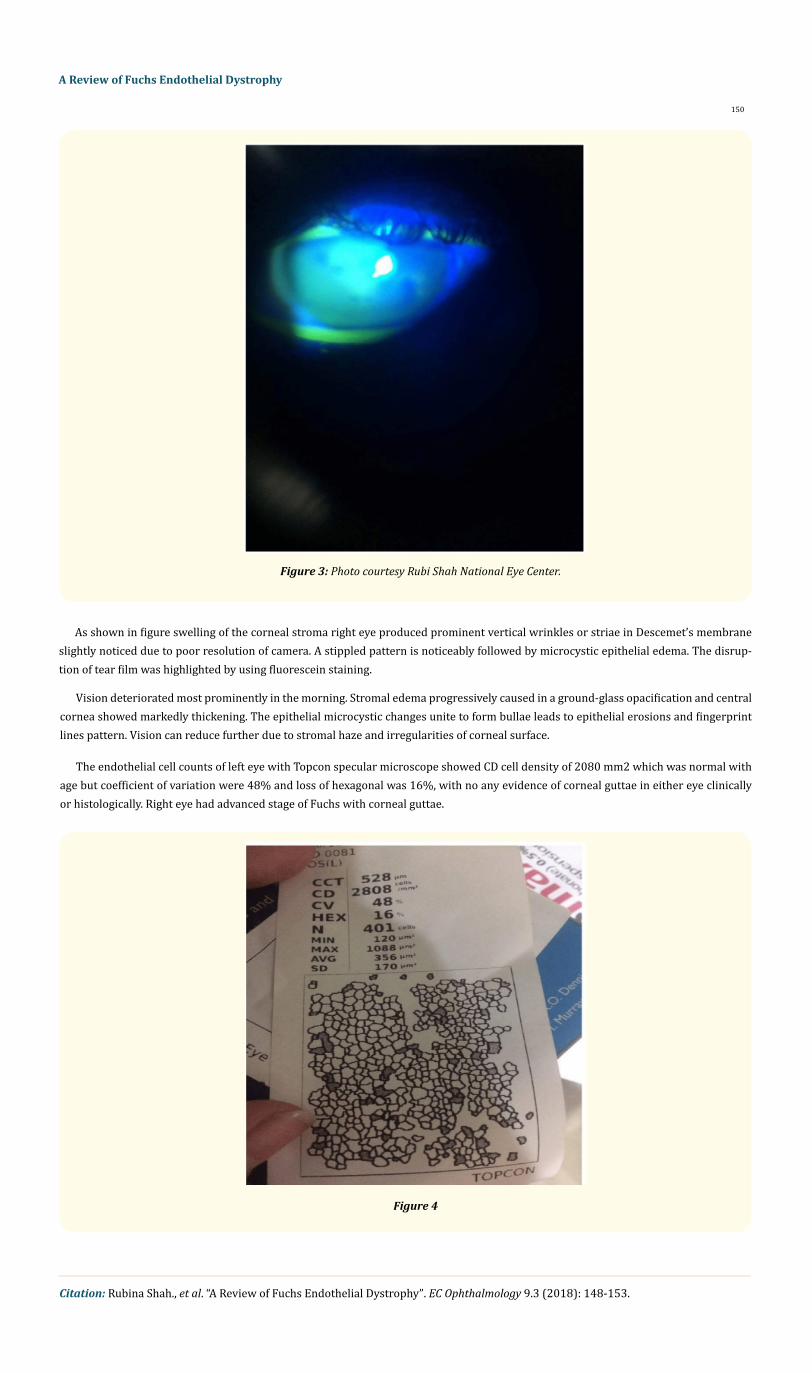
The endothelial cell counts of left eye with Topcon specular microscope showed CD cell density of 2080 mm2 which was normal with age but coefficient of variation were 48% and loss of hexagonal was 16%, with no any evidence of corneal guttae in either eye clinically or histologically. Right eye had advanced stage of Fuchs with corneal guttae.
Figure 4

Citation: Rubina Shah., et al. “A Review of Fuchs Endothelial Dystrophy”. EC Ophthalmology 9.3 (2018): 148-153.
A Review of Fuchs Endothelial Dystrophy
151
Focal gutta is known for formation without corneal edema which has been observed in interstitial keratitis shows a linear arrangement under the deep vessels [9]. Macular dystrophy and posterior polymorphous dystrophy also have guttae formation [10]. The association of corneal and anterior segment findings make differential diagnosis straightforward.
Differential diagnosis
Corneal pseudo guttae can be noticed after trauma, intraocular inflammation, infection, toxins, and thermokeratoplasty. These guttae are transient, representing edema of the endothelial cells, and disappear with resolution of the underlying condition.
Central herpetic disciform keratitis can mimic Fuchs endothelial dystrophies however the presence of underlying keratic precipitates (KP) helps to differentiate the conditions. With acute corneal inflammation, the KP may be difficult to see, but with resolution of the edema they become more prominent.
Chandler’s syndrome can be confused with corneal guttae since its endothelial pattern has a prominent beaten-bronze appearance with overlying corneal edema. However, it is typically unilateral, which helps to differentiate the two conditions.
Prognosis and management
Patient of Fuchs endothelial dystrophy with clear cornea needs no treatment. The medical management protocol of patients with visually significant edema includes topical hypertonic saline solutions, sodium chloride 5% for 4 - 5 times during the day and ointment. Glycerin is also used but cause uncomfortable in patient. A warm blow dryer for 10 - 15 minutes in the morning or throughout the day can reduce corneal dehydration may improve vision. Intraocular pressure must be controlled. Topical carbonic anhydrase inhibitors must be used carefully as it can hinder endothelial pump function. Superficial symptoms like Itching, burning, gritty sensation can be alleviated by Diclofenac 0.1% and ketorolac 0.5% drops but have complication of enhance the risk of poor epithelial healing and corneal melting. Ban-dage contact lens can be used to treat recurrent corneal erosion caused by bullae. The latest techniques shows anterior stromal punctures and multiple ablation pits with Fugo blade can be helpful to treat guttae. Soft contact lenses can be alternatively in cases of bullae forma-tion. Secondly, Cycloplegics, pad, bandage and treat the effected eye. Other techniques like Excimer laser phototherapeutic keratectomy, conjunctival flap and amniotic membrane graft can also be considered.
A surgical care need to consider from two treatment options 1) Keratoplasty without cataract formation and 2) cataract formation with visual disability. The major treatment corneal graft, combined corneal transplant, cataract extraction and lens implant procedure depends on specular microscope results.
The standard criteria for the disease are Penetrating keratoplasty (PK) with or without cataract surgery which involves replacement of whole cornea in spite of only defective endothelial layer. The advancement in this field has made replacement where endothelial kera-toplasty of endothelial layer possible sparing the whole layer of cornea [11].
Descemet membrane stripping automated endothelial keratoplasty (DSEK) involves the procedure of transplant of healthy endothelial layer along with posterior corneal stroma where Descemet membrane endothelial keratoplasty (DMEK) is the transplant of endothelial cells along with Descemet’s membrane [12]. Studies shows DMEK attain visual acuity more than PK [13,14].
It is vital to have a patent signs of decision-making process clinically, as symptomatic blurring in the morning shows evidence of epithelial edema on slit lamp examination. The prognosis for corneal transplant surgery in FECD is better. In one study from Price., et al. described good visual function required postoperatively was found to be slightly slower than Keratoconus, follow up 3 to 84 month follow up showed 98% of patients maintaining clear grafts [15]. Recently, the treatment of option for patients with FECD is endothelial trans-plantation. Significantly, we are no longer dependent on complicated procedure as endothelial transplantation reduced graft survival.
Patient was reluctant to do keratoplasty in right eye so he was managed for corneal edema with 5% ophthalmic saline solution with systane E/D a follow up three weeks.

Citation: Rubina Shah., et al. “A Review of Fuchs Endothelial Dystrophy”. EC Ophthalmology 9.3 (2018): 148-153.
A Review of Fuchs Endothelial Dystrophy
152
Conclusion
Follow up 1: (3 week) rechecked routinely to assess vision and reduced corneal edema.
Discussion
Fuchs endothelial dystrophy can cause bilateral slowly progressive disease of the cornea that can be autosomal dominant type. The considerable pattern is guttae formation which is endothelial cells changes to produce mushroom shaped excrescences. However, their strong lesion present in the center of the cornea procrastinate problems in the coming years. The increasing cornea guttate damages the endothelial cells by reducing it cell thickness. Corneal edema is produces due filling function of endothelial cells makes it arduous for professionals to diagnose.
The diagnosis of advanced FECD is simplified by confocal microscope to easily focus the endothelium obscured by vascularization [4]. Magovern first recognized a family association with early-onset FECD [16]. History shows a vast research on Fuchs disease clinically as Abbott., et al. [16] observed six phakic patients with non-guttate corneal endothelial degeneration who had unilateral edema, with only polymorphic corneal endothelial cells in the contralateral eye. With no evidence of corneal guttae in either eye clinically where endothe-lial cell counts were decreased (840 to 1992/mm2) may be a different of FECD as suggested by Abbott., et al. the ultra-structural differ-ences seem significant enough to make it a dissimilar entity.
In one recent report, topographic evidence of Keratoconus showed a typical sign of association FECD. Patients with decreased vision and FECD should be evaluated carefully for corneal steepening or irregularity secondary to Keratoconus as the cause of the reduced acuity [17]. It is unknown if there is a common pathogenesis between the two dystrophies.
FECD is a common indication for corneal transplantation. According to the Eye Bank statistical report, FECD was seen in 9.2% patient undergone corneal transplantation in 2007 [6]. However, there can be additional 15.7% of patients who had corneal edema with post cataract surgeries. There can be chance of patients which may have undiagnosed FECD preoperatively or were diagnosed with FECD but not felt to be at risk for corneal decompensation following surgery.
It is tough to predict the risk of corneal decompensation with cataract surgery in patients with corneal guttae. There is an indirect correlation between corneal hydration and endothelial cell count as by measuring the endothelial cell count with specular microscopy can help to estimate the prognosis. When the cell count is between 2000 and 750 cells/mm2 the compensatory mechanisms of increased metabolic activity and increasing number and density of pump sites may prevent significant corneal swelling [18,19]. However, at 500 cell/mm2 the endothelial cells become so extensive that the normal compensatory mechanisms fail and corneal edema results [20]. The American Academy of Ophthalmology guidelines, as outlined in the External Disease and Corneal textbook (Section 8 in the Basic and Clinical Science Course) suggests that an endothelial cell count of less than 1000 should raise concern about the possibility of corneal decompensation with intraocular surgery [21].
Another option is to perform corneal pachymetry. The American Academy of Ophthalmology guideline found in Section 8 of the Basic and Clinical Science Course [22] and a recent study from Wilmer Eye Institute [15] both suggest that a corneal thickness of over 640 mi-crons (µm) increases the risk of corneal decompensation with cataract surgery. The difficulty with the corneal pachymetry measurements is that there is a significant amount of individual variation in corneal thickness. One helpful technique is to compare the mid-peripheral corneal thickness with the central corneal thickness. If the central corneal thickness exceeds the mid-peripheral thickness, this may be an indication of clinically significant corneal thickening [23-25].
Fuchs endothelial dystrophy is decompensation of corneal endothelial layer. The course is relentless it can gradually reduce vision. The condition may cause blindness if left untreated. In general a good treatment protocol and visual outcome depends on doctor decision pre operatively whether it is associated with cataract or familial associations. The treatment option is Keratoplasty with guttae and corneal opacity but can be unaffordable in developing countries. Surgical procedures have been advanced as an innovation of endothelial trans-plant without touching stroma and descemet membrane which had opened a new hope for an eye practitioners to treat FECD.
Bibliography
1. Fuchs E. “Dystrophia epithelialis corneae”. Graefe’s Archive for Clinical and Experimental Ophthalmology 76.3 (1910): 478-508.
2. Krachmer JH., et al. “A study of sixty-four families with corneal endothelial dystrophy”. Archives of Ophthalmology 96.11 (1978): 2035-2039.
3. Cross HE., et al. “Inheritance of Fuchs’s endothelial dystrophy”. Archives of Ophthalmology 85.3 (1971): 268-272.
4. Magovern M., et al. “Inheritance of Fuchs’ combined dystrophy”. Ophthalmology 86.10 (1979): 1897-1920.
5. Rosenblum P., et al. “Hereditary Fuchs’ dystrophy”. American Journal of Ophthalmology 90.4 (1980): 455-462.
6. Adamis AP., et al. “Fuchs’ endothelial dystrophy of the cornea”. Survey of Ophthalmology 38.2 (1993): 149-168.
7. Gottsch JD., et al. “Inheritance of a Novel COL8A2 mutation defines a distinct early-onset subtype of Fuchs corneal dystrophy”. Inves-tigative Ophthalmology and Visual Science 46.6 (2005): 1934-1939.
153
A Review of Fuchs Endothelial Dystrophy
Citation: Rubina Shah., et al. “A Review of Fuchs Endothelial Dystrophy”. EC Ophthalmology 9.3 (2018): 148-153.
8. Hogan MJ., et al. “Fuchs’ endothelial dystrophy of the cornea”. American Journal of Ophthalmology 78.3 (1974): 363-383.
9. Waring GO., et al. “Alterations of Descemet’s membrane in interstitial keratitis”. American Journal of Ophthalmology 81.6 (1976): 773-785.
10. Cibis GW., et al. “The clinical spectrum of posterior polymorphous dystrophy”. Archives of Ophthalmology 95.9 (1977): 1529-1537.
11. Kaufman SC., et al. “Diagnosis of advanced Fuchs’ dystrophy with the confocal microscope”. American Journal of Ophthalmology 116.5 (1993): 652-653.
12. Guerra FP., et al. “Descemet’s Membrane Endothelial Keratoplasty Prospective Study of 1-Year Visual Outcomes, Graft Survival, and Endothelial Cell Loss”. Ophthalmology 118.12 (2011): 2368-2373.
13. Price MO., et al. “Descemet’s Stripping Automated Endothelial Keratoplasty Outcomes Compared with Penetrating Keratoplasty from the Cornea Donor Study”. Ophthalmology 117.3 (2009): 438-444.
14. Rao SK., et al. “Descemet stripping endothelial keratoplasty: effect of the surgical procedure on corneal optics”. American Journal of Ophthalmology 145.6 (2008): 991-996.
15. Price FW., et al. “Graft survival in four common groups of patients undergoing penetrating keratoplasty”. Ophthalmology 98.3 (1991): 322-328.
16. Abbott RL., et al. “Specular microscopic and histologic observations in nonguttate corneal endothelial degeneration”. Ophthalmology 88.8 (1981): 788-800.
17. Cremona FA., et al. “Keratoconus associated with other corneal dystrophies”. Cornea 28.2 (2009): 127-135.
18. Eye Banking Statistical Report. EBAA (2007).
19. Geroski DH., et al. “Pump functions of the human corneal endothelium. Effects of the age and cornea guttatae”. Ophthalmology 92.6 (1985): 759-763.
20. Edelhauser HF. “The resiliency of the corneal endothelium to refractive and intraocular surgery”. Cornea 19.3 (2000): 263-273.
21. Basic Clinical and Science Course Section 8, External Disease and Cornea. American Academy of Ophthalmology (2017-2018): 325.
22. Seitzman GD., et al. “Cataract surgery in patients with Fuchs corneal dystrophy. Expanding recommendations for cataract surgery without simualtaneous keratoplasty”. Ophthalmology 112.3 (2005): 441-446.
23. Iwamoto T and DeVoe AG. “Electron microscopic studies on Fuchs’ combined dystrophy. I. Posterior portion of the cornea”. Investiga-tive Ophthalmology and Visual Science 10.1 (1971): 9-28.
24. Alexander RA, et al. “Oxytalan fibers in Fuchs’ endothelial dystrophy”. Archives of Ophthalmology 99.9 (1981): 1622-1627.
25. Gottsch JD., et al. “Fuchs corneal dystrophy: abberant collagen distribution in an L450W mutant of the COL8A2 gene”. Investigative Ophthalmology and Visual Science 46.12 (2005): 4504-4511.
Volume 9 Issue 3 March 2018©All rights reserved by Rubina Shah., et al.