critical care of the transplant patient · critical care of the transplant patient dr. liesel...
TRANSCRIPT

Critical Care of the Transplant
Patient
Dr. Liesel Bösenberg
Specialist Physician
Fellow in Critical Care
Kalafong Hospital & SBAH

Organ, organ on the wall, what to we do if
you fail us all?
• Aim of talk is to give broad overview on this topic
• Solid organ transplants:
• Liver transplant patients
• What‟s up with the kidney
• Heart , lung and heart-lung transplant
• The bone marrow

Liver transplant patients:

Managing complications related to ESLD:
Cerebral function and encephalopathy
• Seen in acute and acute-on-chronic liver failure
• Ranges from delirium to coma
• Development in patients with cirrhosis poor
prognostic sign with 1-year survival <42%
• HE is a clinical diagnosis

Pathogenesis of HE:
• Increased Ammonia due to hepatic dysfunction and
porto-systemic shunting
• Ammonia metabolized to glutamine which leads to
astrocyte swelling and glutamine-induced
mitochondrial dysfunction
• Cerebral oedema and intracranial hypertension
• Underlying sepsis or GIT haemorrhage are
important precipitants for acute decompensation
• After OLT calcineurin inhibitors may lower threshold
for convulsions and alter LOC

Management of HE:
• Treat precipitant and support organ systems
appropriately
• Intracranial pressure monitoring not recommended
in these patients
• Manage GIT haemorrhage , SBP etc.
• Lactulose 45ml per NG until evacuation occurs then
enough to achieve 2-3 soft movements per day
• It is a non-absorbable dissaccharide that acidifies
the colonic lumen and has an osmotic cathartic
effect
• Lactulose enemas for severe HE

Treatment of HE

Screening and treatment of infections:
• Pneumonia and SBP in 20-40% o cirrhotic patients
admitted to ICU with sepsis
• „immunocompromise‟ in cirrhosis result of
decreased macrophage clearance, deficiency in
complement reactions and down regulation of the
monocyte human leucocyte antigen- DR expression
• Monocytes also have decreased expression of Il-10
• Sepsis in cirrhosis overwhelming pro-inflammatory
component
• Organisms to watch out for MRSA, VRE,
Acinetobacter

Cardiovascular:
• Hyperdynamic circulation with a low SVR,
increased Q, low normal or decreased systlic
arterial BP
• Splanchnic and systemic vasodilatation and renal
vasoconstriction
• Up regulation of RAAS system, increased
sympathetic drive
• CAD in 20-30% of these patients
• HD management in sepsis- unknown if targets need
to be modified in ESLD
• Norepinephrine, vasopressin , extracorporeal
albumin dialysis , hydrocortisone

Hepatopulmonary syndrome and
portopulmonary hypertension
• HPS = liver cirrhosis, abnormal pulmonary gas exchange, intrapulmonary vascular dilation, resolution in up to 80% post-transplant
• Severe hypoxia due to vascular shunt
• Mortality is 16% at 19 days and 38% at one year
• Orthodeoxia and platypnoea
• PPHT = portal hypertension with pulmonary hypertension, in 20% of pretransplant patients
• Response to epoprostenol ( PGI2 analogue)
• Mechanical ventilation according to ARDS protocols, PEEP 5-12 cmH2O

Associated renal dysfunction: HR syndrome
• Pathophysiology relates to intense renal
vasoconstriction secondary to SNS activation as a
response to splanchnic vasodilatation due to
increased nitric oxide production in portal
hypertension
• Hallmark is a low u-Na
• Type 1 and Type 2
• Best studied therapy is albumin 1mg/kg plasma
volume expansion then 20-40g/day for 14 days
• Also octreotide 100-200 g SC tds
• Also use alpha agonists to increase BP

Delisting happens…

Post liver transplant: Post reperfusion
syndrome:
• Poorly understood- happens when there is
reperfusion of the portal vein through the donor
graft
• Hypotension, bradicardia, vasodilatation, pulmonary
hypertension, hyperkalaemia and sometimes
cardiac arrest
• Resolves with fluid loading and electrolyte
management

Post-op care: early complications:
• Technical
• Complications related to existing liver disease
• Complications of the immunosuppressive agents
• Graft function
• Monitoring graft function in ICU:
• General parameters:
• Liver perfusion, bile production, haemodynamics
• Coagulation : INR and the prothrombin time
• Biochemistry: glucose, gases and lactate
• AST, bilirubin, ALP/ GGT

CVS:
• Watch out for underlying cardiomiopathy
• After transplant hypertension with increased SVR
due to restoration of normal liver function and portal
pressures
• Calcineurin immunosuppressants also have
hypertensive effect, increased afterload may
unmask cardiac dysfunction
• Decreased miocardial contractility due to operation
related issues: prolonged caval clamping, acidosis,
haemorrhage and hypocalcaemia
Respiratory:
• Pleural effusions, ongoing shunting secondary to
HPS with resulting hypoxaemia
• Atelectasis
• Infections
• TRALI


AKI post transplant can happen:

Technical complications:

Graft failure: does anyone have another
donor? Primary non- function

Renal transplants:

Complications related to treatment

Complications in the grafted kidney
• ARF/ CRF
• Nephrotic syndrome
• Drug-induced
• Infection related
• Obstructive uropathy
• Acute obstruction of the transplant artery/vein
• Peri-transplant haematoma
• Urine leak
• Lymphocoele

Lung transplants:BLT/SLT

•Heart-lung transplants reserved for Eisenmenger
secondary to complex congenital heart lesions

The deenervated lung
• Lungs remain permanently deenervated
• Bronchial artery and lymphatic system regenerate
after a few weeks
• Regulation of breathing through chest wall afferents
and wean off ventilation within 48 hrs
• Bronchomotor tone is retained
• The cough response is lost under the anastomosis

Post-op:
• Implantation response within few hours
• Infiltrates on x-ray with peribronchial cuffing due to
lung oedema
• Management supportive with fluid restriction
• Hyperacute rejection: poor prognosis for recovery
• Early rejection: infiltrates and decreased PaO2 after
48-72 hrs: pulse steroids and antibiotics
• BAL and transbronchial biopsies
• Anastomotic problems- broncial/ tracheal stenosis
• Sputum retention

Ischaemia-reperfusion injury:
• Sign of early graft dysfunction
• Also called reperfusion oedema/ reimplantation response
• Incidence of 15-35%
• Native lung has elevated vascular resistance, high blood flow
to dysfunctional allograft and significant V/Q mismatch
• Can occur within 24 hours post-op, manifests with reduced
lung complience, altered gas exchange and hypoxemia
• 97% of radiographs show changes on day one compared to
100% on day 3.
• BAL and transbronchial biopsy might be necessary to
distinguish between infection and hyperacute rejection


Management of IR injury
• ARDS protocol
• PGE1 IVI
• Inhaled NO
• Pentoxifylline
• Inhaled prostacycline
• ECMO

Mx of SLT dysfunction:
• Small tidal volumes
• Tolerate moderate respiratory acidosis
• Lateral decubitis
• “New lung up”
• Bronchoscope
• ILV


Anastomotic problems:
Bronchus dehiscence:
• Suspected if large air leaks from IC drains
• Pneumomediastinum/ -pericardium
• Empyema


• Other mechanical compications include strictures,
stenosis and bronhcomalacia

Infections : Bacterial / viral/fungal




Hyperammonemia syndrome
• High mortality rate
• Severe onset of neurological dysfunction and
deterioration in the first 4 weeks following the
transplant
• High ammonia levels with discordantly low liver
function tests
• Metabolic stressors which lead to increased protein
turnover and a negative nitrogen balance include
allograft rejection , IR , acute GIT bleeding etc.

Long-term complications:
• Obliterative bronchiolitis sign of chronic rejection
• After 6 weeks: Infx with CMV , alsp repeated
pseudomonas and MRSA
• Complications related to immunosuppresive drugs

Heart transplants:

The deenervated heart
• Remember two P waves , resident SA node and
grafted SAnode
• No autonomic innervation - only drugs that act
directly on myocardium can be used
• Atypical response to exercise, hypovolemia and
hypotension
• Increase in Q if preload increases will be delayed
• Verapamil and nifedipine have enhanced effects in
the transplanted heart
• Adenosine can cause profound hypotension and
even asystole
• Amiodarone can cause hypotension

Management of immediate post-op
haemodynamic instability:
• Inotropic support ( milrinone/ epinephrine) for poor LV/RV contractility
• Pressor support ( norepinephrine) : low systemic arterial pressures despite good filling pressures and contractility
• Heart rate support with chronotropic drugs/pacing : intrinsic low gratfted heart rate ( milrinone/ isoprenaline)
• IABP : poor LV function not responding to other measures
• RVAD/LVAD/BiVAD
• Inhaled NO
• Resternotomy for bleeding/tamponade

Other complications:
• Infection, malignancy and graft atherosclerosis/ cardiac
allograft vasculopathy
• Infections:
• 45% bacterial and 10% fungal, mortality highest with fungal
• Malignancy:
• 1-2% risk per year
• Skin tumours and lymphomas
• CAV:
• Obliterative atherosclerosis
• Very diffuse, rescue therapy with angiographic interventions/
CABG very difficult
• Statins and Ca channel blockers might delay process

Multi-visceral transplants:

Hemapoetic stem cell transplants

Pulmonary complications:
• Engraftment syndrome:
• 7-35% of patients
• Develops within the first 96 hrs after transplant
• Fever, diarrhoea, erythematous rash, diffuse pulmonary infiltrates, renal impairment
• Mortality of 25%
• Responds fairly well to steroids
• Discontinue GM-CSF
• Diffuse alveolar haemorrhage:
• Progressive dyspnoea, fever and cough & hypoxaemia
• Usually older age, pre-transplant chemotherapy/whole body irradiation
• Bilateral peri-hilar infiltrates
• BAL- hemosiderin-laden macrophages
GVHD:
• Most common symptom is a skin rash
• Manifests in CVS as pericardial effusion
• Also in GIT- NVD and bleeding
• Intestinal perforation
• CT abdomen may show small bowel oedema
• Also neurological complications
• Low grade disease can be treated with steroids

Veno-occlusive disease of liver
• Seen in allogeneic transplants
• Thrombotic occlusion of small hepatic vessels
• Most likely the result of endothelial damage due to
chemotherapy
• Manifests with weight gain, oedema, ascites,tender
hepatomegaly, jaundice and liver failure
• Treatment includes tissue plasminogen activator/
anti- thrombin II concentrates

• Whole lecture on its own, good article

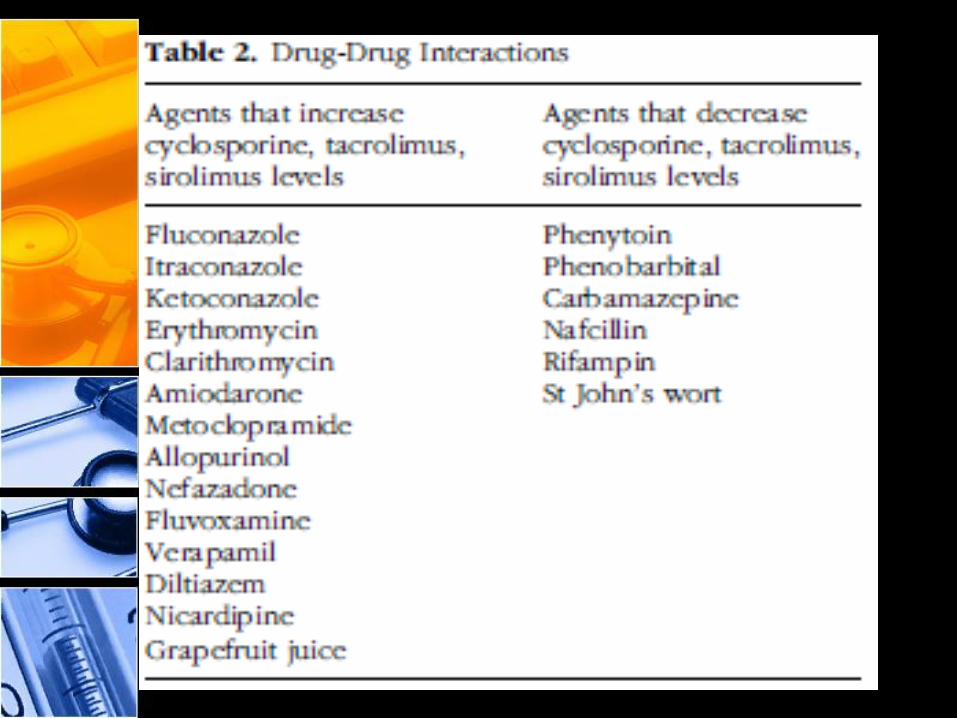
Drug interactions in transplant patients


Further reading