critical care fellow university of new mexico hospital · critical care fellow university of new...
TRANSCRIPT

Osmotic Demyelination Syndrome
Emily Horn, MD Critical Care Fellow
University of New Mexico Hospital

Case Presentation
50F presents to ER w/ weakness and frequent falls;
hematemesis x2
EtOHism since age 15 w/ significant increase in intake of
exclusively hard liquor (1 pint vodka daily) x8 months
PMH/PSH: Chr HCV, EtOHism
No home meds; NKDA
SHx: 1 pint vodka daily, 1 ppd, no IVDU
FHx: EtOHism
Physical Exam
VS: 36.4 109 102/61 95/60 18 96% 2L
Gen: NAD, A&O x2 after receiving Librium
CV: tachycardic, reg rhythm
Chest: CTAB
Abd: mild diffuse tenderness, ascites

Labs
11.1
31
8.6 169 Coags normal
Lactate 4.8
118
3.1
79
22
8
1.06
146
Tot bili 2.6
AP 111
AST 164
ALT 73

Serum Sodium Course
Time
8/30 @ 1301 2L NS, 2L LR
8/30 @ 2040
8/31 @ 0335
8/31 @ 1532
9/1 @ 1718 (2L NS that AM)
Serum Sodium
118
126 (+8 in <8 hrs)
131
134 (+16 in 24 hrs)
144 (+26 in 48 hrs)

Hospital Course
8/30: admitted from ER to MICU
9/1: transferred to Medicine
MRI for reported dysarthria PTA – unable to complete 2/2 motion artifact
CT 9/2 neg acute; nonspecific mod diffuse brain volume loss, greater than expected for age
9/6: transferred to MICU for resp failure 2/2 suspected aspiration event; intubated
9/7: extubated
9/8: re-intubated for tachypnea/hypoxia
9/9: agitated – Precedex started w/ Fentanyl prn
9/10: unresponsive – Precedex D/Ced
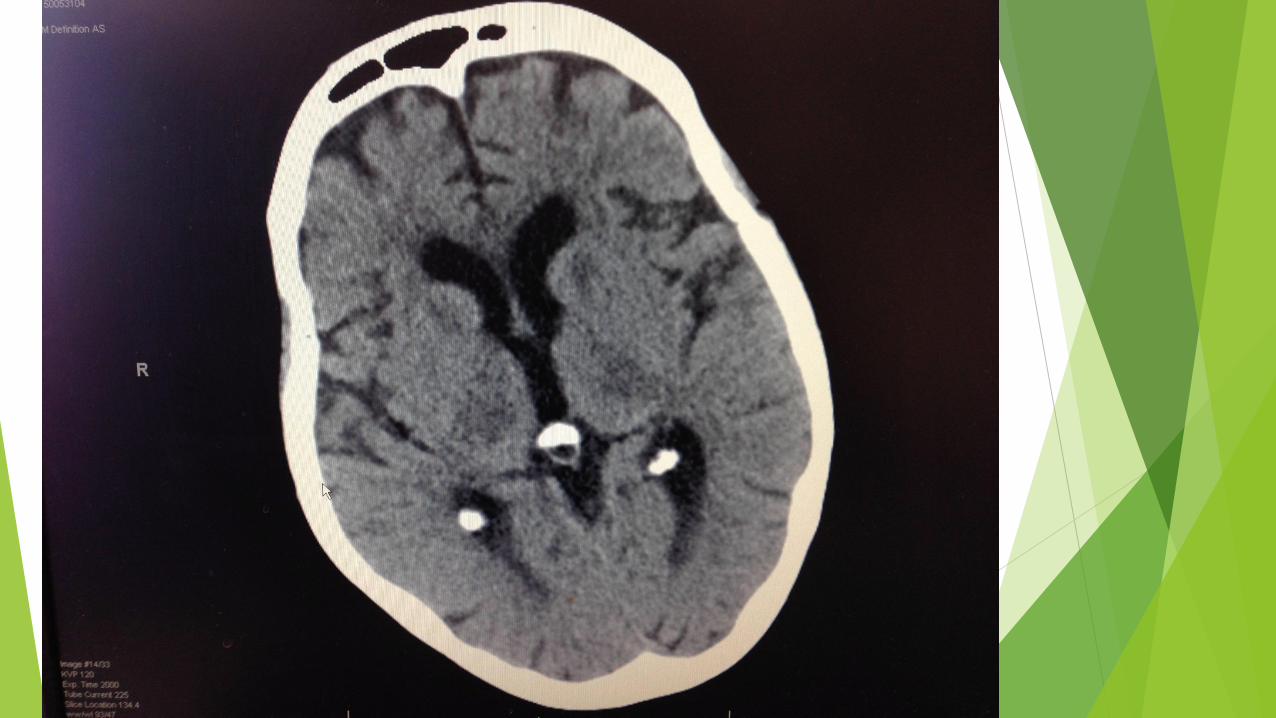
9/13: CT w/ symmetric decreased attenuation involving pons, lateral aspects of caudate heads, and thalami
Hospital Course
9/14: MRI w/ symmetric increased T2 prolongation involving the
central pons and bilateral thalami, lentiform nuclei, and external
capsules


Hospital Course
9/16: comfort care
9/17: pt death
Hyponatremia
Occurs in 15-20% of hospital admissions; independent risk factor for mortality
Present in the setting of a wide variety of conditions
Managed by clinicians with a wide variety of backgrounds
Diverse institution- and specialty-based approaches to treatment
Few well-designed, prospective studies
Limited evidence-based approaches, especially when duration unknown
Unpredictable treatment response, especially in profound hyponatremia
Spasovski et al. Clinical practice guideline on diagnosis and treatment of hyponatremia. Nephrol Dial Transplant 2014 Apr;29 Suppl 2:i1-i39.
Geoghegan et al. Sodium correction practice and clinical outcomes in profound hyponatremia. Mayo Clin Proc 2015;90(10):1348-55.

Central Pontine Myelinolysis

Osmotic Demyelination Syndrome

Definitions
CPM (central pontine myelinolysis) – solitary, symmetric,
demyelinating focus in the central pons
EPM (extrapontine myelinolyses) – symmetrically arranged
lesions of similar histology in other areas: thalamus,
globus pallidus, putamen, lateral geniculate body,
cerebellar white matter
UptoDate. Osmotic demyelination syndrome and overly rapid correction of hyponatremia.

Pathogenesis: hyponatremia
Difference in osmolality between brain and plasma extracellular to intracellular movement of water brain edema
Adaptive mechanism
Reduction in intracellular osmotically active particles (mostly potassium and organic solutes) in an attempt to restore brain volume
Process takes 24-48 hrs
Spasovski et al. Clinical practice guideline on diagnosis and treatment of hyponatremia. Nephrol Dial Transplant 2014 Apr;29 Suppl 2:i1-i39.
Pathogenesis: demyelination
Correction of hypoNa movement of water out of brain
Rapid fall in brain volume demyelination
Osmotic shrinkage of endothelial cells opening of BBB entry
of complement and other cytotoxic plasma components
Loss of cell water + movement of Na and K back into cells initial
increase in cell cation concentration before repletion of organic
osmolytes (myoinositol, glutamate, glutamine) direct astrocyte
injury apoptosis disruption in function of myelin-producing
oligodendrocytes, release of cytokines, and activation of microglia
Sterns et al. Brain volume regulation in response to hypo-osmolality and its correction. Am J Med
2006;119(7Suppl1):S12.
Gankam-Kengne et al. Astrocytes are an early target in osmotic demyelination syndrome. J Am Soc
Nephrol 2011 Oct;22(10):1834-45.

Pathogenesis: demyelination
Demyelination primarily occurs in areas of the brain that
are slowest in re-accumulating osmotically active
substances after rapid correction of hypoNa
Yeates et al. Salt and water: a simple approach to hyponatremia. CMAJ 2004;170(3):365.

Risk Factors
Serum Na at presentation
Majority < 105 mEq/L
Vast majority < 120 mEq/L
Duration of hypoNa
Present for at least 2-3 days (time required for cerebral adaptation)
Assume significant duration unless history c/w acute water intoxication
Sterns et al. Neurologic sequelae after treatment of severe hyponatremia: a multicenter
perspective. J Am Soc Nephrol 1994;4(8):1522.

Risk Factors
Rapid rate of correction
Rate of correction over 24-hr period a more important determinant than maximum rate in any given hour
Greatest risk for irreversible and disabling brain injury
Raised by > 20 mEq/L in 24 hrs OR
Corrected to > 140 mEq/L
Occasional pts develop ODS even when corrected by 9-12 mEq/L/day
Target a rate of correction < 9 mEq/L in any 24-hr period
Verbalis et al. Hyponatremia treatment guidelines 2007: expert panel recommendations. Am J Med 2007;120(11 Suppl 1):S1.

Risk Factors
Underlying malnutrition
EtOHism
Liver transplantation
Simultaneous hypoxia or sepsis
Geoghegan et al. Sodium correction practice and clinical outcomes in profound
hyponatremia. Mayo Clin Proc 2015 Oct;90(10):1348-55.

Risk Factors
Rare in ESRD treated w/ HD
Rise in serum osmolality w/ increase in Na counterbalanced by fall in serum osmolality w/ removal of urea
Azotemia enhances brain reuptake of organic osmolytes, minimizing cellular shrinking
Oo et al. Does uremia protect against the demyelination associated with correction of hyponatremia during hemodialysis? A case report and literature review. Semin Dial 2003;16(1):68.
Mechanisms of Overly Rapid Correction
Following therapy specifically directed at raising the sodium concentration
Auto-correction
Following cessation of a reversible stimulus to ADH release rapid excretion of excess free water
Requires normal kidney function
UptoDate. Osmotic demyelination syndrome and overly rapid correction of hyponatremia.

Mechanisms of Overly Rapid Correction:
Auto-correction
Administration of NS in true volume depletion: restoration of euvolemia rapidly suppresses ADH release, allowing excretion of excess water
Administration of glucocorticoids in adrenal insufficiency
Discontinuation of thiazides (interfere w/ urinary dilution)
Discontinuation of drugs causing SIADH
Spontaneous resolution of a transient cause of SIADH
Treatment with a vasopressin receptor antagonist
UptoDate. Osmotic demyelination syndrome and overly rapid correction of hyponatremia.

Epidemiology
Non-optimal correction of profound hyponatremia is common
Infrequently associated with serious morbidity
Retrospective review (5 yrs, 1 ICU): 412 pts w/ Na <120
211 (51.2%) w/ optimal correction at 24 hrs
87 (21.1%) under-corrected
114 (27.9%) over-corrected
One case of ODS
Geoghegan et al. Sodium correction practice and clinical outcomes in profound hyponatremia. Mayo Clin Proc 2015 Oct;90(10):1348-55.

Clinical Manifestations
Typically delayed for 2-6 days after overly rapid correction
Symptoms often irreversible or partially reversible
Dysarthria, dysphagia, parapesis/quadriparesis, behavioral
disturbances, lethargy, confusion, disorientation, obtundation, coma
Seizures less common
“Locked in” syndrome
Sterns et al. Neurologic sequelae after treatment of severe hyponatremia: a multicenter
perspective. J Am Soc Nephrol 1994;4(8):1522.
Detection
MRI >>> CT
Even MRI may not become positive for 4 wks after onset,
especially if diffusion-weighed imaging not used
Karp et al. Pontine and extrapontine myelinolysis: a neurologic disorder following rapid
correction of hyponatremia. Medicine (Baltimore). 1993;72(6):359.

Prevention

Re-lowering Na if Overly Rapid
Correction Has Occurred
May reverse BBB breakdown and prevent the infiltration of microglia
More effective than glucocorticoid administration
Recommended if:
Initial Na < 120 mEq/L AND
Present at least 2 days (or unknown duration) AND
Rate of correction has exceeded the maximum recommended goals (< 9 mEq/L in 24 hrs and < 18 mEq/L in 48 hrs)
Gankam et al. Re-induction of hyponatremia after rapid overcorrection of hyponatremia reduces mortality in rats. Kidney Int 2009;76(6):614.
UptoDate. Osmotic demyelination syndrome and overly rapid correction of hyponatremia.

Re-lowering Na if Overly Rapid
Correction Has Occurred
D5W 6 mL/kg IBW over 2 hrs, repeated until at goal
1 mEq/L per hour
Net rate of correction < 9 mEq/L over 24 hrs
E.g. serum Na 115 127 in 16 hrs, target 124 over next 8 hrs
Measure serum Na after each infusion
Desmopressin 2 mcg IV/SQ q6h
Once at goal
D/C D5W
Continue desmopressin to prevent Na from rising again due to excretion of dilute urine
Gankam et al. Re-induction of hyponatremia after rapid overcorrection of hyponatremia reduces mortality in rats. Kidney Int 2009;76(6):614.
UptoDate. Osmotic demyelination syndrome and overly rapid correction of hyponatremia.
Slowing Rate of Correction
Trajectory of correction is too rapid, but has not yet
exceeded the maximum recommended rate of correction
Exceptions
Pts who cannot be relied upon to curtail water intake
Pts w/ hyperacute hyponatremia developing over a few hours 2/2
marked increase in water intake (low risk for ODS)
UptoDate. Osmotic demyelination syndrome and overly rapid correction of hyponatremia.

Slowing Rate of Correction
Desmopressin 2 mcg IV/SQ q6-8h
+/- hypertonic saline @ 10-30 mL/hr to produce rise in serum Na at a
desired rate
Continued until serum Na 125-130
OR
Desmopressin 2 mcg IV/SQ x1, repeated if serum Na rising too quickly
or urine output has increased dramatically
Sterns et al. Overcorrection of hyponatremia is a medical emergency. Kidney Int
2009;76(6):587.

Desmopressin
Administration after a 24-hr limit of 12 mEq/L had been reached or exceeded (n = 6)
Correction prevented from exceeding the 48-hr limit of 18 mEq/L in 5 pts
All 6 received D5W concurrently
Administration in anticipation of over-correction (n = 14)
Correction prevented from exceeding 24- or 48-hr limit in all 14 pts
5 pts received D5W concurrently
Proves feasibility, but not better outcomes, than watchful waiting
Perianayagam et al. DDAVP is effective in preventing and reversing inadvertent overcorrection of hyponatremia. Clin J Am Soc Nephrol 2008;3(2):331.

Management

Re-lowering Serum Na to Treat ODS
Same regimens recommended to re-lower serum Na after overly rapid correction
Initiate ASAP after onset of sx attributed to ODS
No evidence of benefit if begun >24 hrs after onset
Re-lower to a level just below the maximal target value at 48 hrs (< 18 mEq/L above the initial serum Na)
48-hr goal chosen because pts w/ ODS typically present 2-6 days after overly rapid correction
Based on case reports
Soupart et al. Therapeutic relowering of the serum sodium in a patient after excessive correction of hyponatremia. Clin Nephrol 1999;51(6):383.
Oya et al. Reinduction of hyponatremia to treat central pontine myelinolysis. Neurology 2001;57(10):1931.

Supportive Therapy
Some pts recover function after prolonged periods of severe
neurologic impairment
Intubation/mech ventilation often required 2/2 aspiration and
resp failure
Recovery from seemingly hopeless neurologic deficits can occur
Supportive tx should be continued 6-8 wks before concluding
irreversibility
Sterns et al. Osmotic demyelination syndrome following correction of hyponatremia. NEJM.
1986;314(24):1535.
Supportive Therapy
Observational study (n = 44; follow-up data in 34) w/ observation period of 3 wks to 44 mos
Complete recovery: 11
Independent w/ some deficits: 11
Dependent on personal help or assistive devices: 10
Death: 2
Outcome independent of severity of neurologic deficits, degree of hypoNa, extent of initial pontine lesion, or persistence of lesion on MRI
Previous mortality nearly 100% w/in 3 months
Menger et al. Outcome of central pontine and extrapontine myelinolysis. J Neurol 1999;246-700-705.

Plasmapheresis
5 case reports w/ improvement (n = 4) or resolution (n = 1) of
neurologic symptoms
Theory: reduction of high molecular myelinotoxic substances, which
were released in response to osmotic stress to cause irreversible
demyelination
Possible benefit difficult to interpret since some pts experience short-
lived, self-limiting episodes of neurologic impairment
Bibl et al. Treatment of central pontine myelinolysis with therapeutic plasmapheresis. Lancet
1999;353(9159):1155.
Grimaldi et al. Plasmapharesis improves the outcome of central pontine myelinolysis. J Neurol
2005;252(6):734.
Saner et al. Treatment of central pontine myelinolysis with plasmapheresis and immunoglobulins in
liver transplant patient. Transpl Int 2008;21(4):390.

IVIG
Case reports
48 year-old man w/ alcoholism: unable to sit unaided, unable to
ambulate mild dysarthria and ataxia
40 year-old man w/ alcoholism: “locked in” syndrome requiring
mechanical ventilation ambulatory with support
IVIG 0.4 g/kg/day x5 days
May represent acceleration of spontaneous recovery
Thirunavukarasu et al. Response to IV immunoglobulin in a case of osmotic demyelination syndrome.
BMJ Case Reports 2015 Nov 25;doi:10.1136/bcr-2015-212985.
Finsterer et al. Immunoglobulins are effective in pontine myelinolysis. Clin Neuropharmacol
2000;23:110-13.

Minocycline (rat studies)
Crosses BBB and inhibits microglial activation and
production of cytokines
Neuroprotective effects in experimental models of other
demyelinating disorders
No human data
Suzuki et al. Minocycline prevents osmotic demyelination syndrome by inhibiting the
activation of microglia. J Am Soc Nephrol 2010 21(12):2090.
Gankam-Kengne et al. Minocycline protects against neurologic complications of rapid
correction of hyponatremia. J Am Soc Nephrol 2010 21(12):2099.

Take-Home Points
Target rate of correction < 9 mEq/L in any 24-hr period
Risk strongly correlates with chronicity of hypoNa
ODS sx typically delayed; MRI findings may be even further delayed
Re-lowering if overly rapid correction
If initial Na < 120 for more than 2 days, and rate has exceeded goal
D5W and Desmopressin
Slowing rate of correction
Desmopressin +/- hypertonic saline
Treatment of ODS
Same as re-lowering if overly rapid correction
No benefit if initiated >24 hrs after symptom onset

Question #1
Which of the following is FALSE regarding correction of hyponatremia?
A. Treatment should continue until serum sodium is in the range of 125-130 mEq/L
B. Treatment does not need to be initiated in cases of hyperacute hyponatremia
C. The goal for the net rate of correction should be <12 mEq/L over 24 hours
D. Will not likely improve outcome if initiated more than 24 hours after the onset of ODS

Question #2
What is the strongest risk factor for the development of ODS?
A. Rate of correction
B. Duration of hyponatremia
C. Presence of renal failure
D. Initial serum sodium level