critical care and emergency neuroscience: the essentials · pdf filecritical care and...
TRANSCRIPT

Critical Care and Emergency Neuroscience: The Essentials
May 19, 2016
Links to video presentations available on next page
Yale School of MedicineDepartments of Neurology and Neurosurgery
YaleCMECONTINUING MEDICAL EDUCATION

VIDEO PRESENTATIONS
Pre-hospital Neuroscience Diagnosis and Management Evie G. Marcolini MD, FACEP, FAAEM https://vimeo.com/179369053
Remote Neurological Consultations Joseph L. Schindler MD https://vimeo.com/180081525
Y-Access Neuroscience Triage and Transfer: Collaborating with Regional Hospitals Victor A. Morris MD and Andrew Ulrich MD https://vimeo.com/179369536
Interventions for Neurovascular Emergencies Charles C. Matouk MD https://vimeo.com/179369055
ICU Management for Ischemic and Hemorrhagic Stroke Nils H. Petersen MD, PhD, MSc https://vimeo.com/179369054
Surgical Management of Neuroscience Emergencies Patrick R. Tomak MD https://vimeo.com/179369545
Management of Status Epilepticus Emily J. Gilmore MD https://vimeo.com/179369797
Hypoxic Ischemic Injury Carolina B. Maciel MD https://vimeo.com/179369812
Brain Death and Organ Donation David M. Greer MD, MA, FCCM, FAHA https://vimeo.com/180051694
Partnering with New England Organ Bank Alexandra K. Glazier Esq. https://vimeo.com/180051690
Navigating Prognosis in the Neuro ICU David Y. Hwang MD https://vimeo.com/180051692
Giving Patients a Chance: Case Presentation with Former Neuro ICU Patient Emily J. Gilmore MD and Andy Morrison https://vimeo.com/180051693

Critical Care & Emergency Neuroscience: The Essentials
May 19, 2016
LEARNING OBJECTIVES This course will enable participants to:
• Review the pre-hospital management of acute neurologic disease• Describe patterns of communication and transfer between facilities for the acutely ill neuroscience
patient• Outline the diagnostic workup and management of cerebrovascular disease• Demonstrate approach to management of seizures and status epilepticus in the critically ill patient• Describe nuances and definitions of brain death determination• Discuss dynamics of communication and patient experience in the setting of acute neurologic
illness
ACCREDITATION STATEMENT The Yale School of Medicine is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
DESIGNATION STATEMENTThe Yale School of Medicine designates this live activity for a maximum of 6.5 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
EMS-I Six (6.0) Continuing Education Credits have been approved by the Connecticut Department of Public Health, Office of EMS, for EMS-I's who complete this program.

Critical Care & Emergency Neuroscience: The Essentials
May 19, 2016
Schedule
AM 7:00am Registration and Continental
Breakfast
8:00am Welcome and Introductions
8:15am Pre-hospital Neuroscience Diagnosis and Management Evie G. Marcolini MD, FACEP, FAAEM
8:45am Remote Neurological Consultations Joseph L. Schindler MD
9:15am Y-Access Neuroscience Triage and Transfer: Collaborating with Regional Hospitals Victor A. Morris MD and Andrew Ulrich MD
9:45am Panel Discussion
10:00am Interventions for Neurovascular Emergencies Charles C. Matouk MD
10:30am ICU Management for Ischemic and Hemorrhagic Stroke Nils H. Petersen MD, PhD, MSc
11:00am Refreshment Break
11:15am Surgical Management of Neuroscience Emergencies Patrick R. Tomak MD
11:45am Management of Status Epilepticus Emily J. Gilmore MD
PM 12:15pm Lunch
1:10pm Hypoxic Ischemic Injury Carolina Maciel MD
1:40pm Brain Death and Organ Donation David M. Greer MD, MA, FCCM, FAHA
2:10pm Partnering with New England Organ Bank Alexandra K. Glazier Esq.
2:40pm Navigating Prognosis in the Neuro ICU David Y. Hwang MD
3:00pm Giving Patients a Chance: Case Presentation with Former Neuro ICU Patient Emily J. Gilmore MD and Andy Morrison
3:25pm Closing Remarks Kevin N. Sheth MD
3:30pm Adjourn
Faculty
COURSE DIRECTORS: Kevin N. Sheth MD Associate Professor, Departments of Neurology and Neurosurgery Division Chief, Neurocritical Care and Emergency Neurology Yale School of Medicine
Charles C. Matouk MD Assistant Professor Departments of Neurosurgery and Radiology and Biomedical Imaging Yale School of Medicine
Jessica White PA-C Lead Physician Assistant, Neuroscience Intensive Care Unit Yale School of Medicine
GUEST SPEAKERS: Alexandra K. Glazier Esq. President and CEO of the New England Organ Bank U.S. Department of Health and Human Services Advisory Committee on Organ Transplantation
Andy Morrison Former Neuro ICU Patient
YALE SCHOOL OF MEDICINE FACULTY: Emily J. Gilmore MD Assistant Professor of Neurology Staff Neurointensivist, Neuroscience Intensive Care Unit
David M. Greer MD, MA, FCCM, FAHA Harry M. Zimmerman & Nicholas and Viola Spinelli Professor of Neurology Professor of Neurosurgery Vice Chairman, Department of Neurology
David Y. Hwang MD Assistant Professor of Neurology Staff Neurointensivist, Neuroscience Intensive Care Unit
Carolina B. Maciel MD Clinical Fellow in Neurology Neurocritical Care and Emergency Neurology
Evie G. Marcolini MD, FACEP, FAAEM Assistant Professor of Emergency Medicine Staff Neurointensivist, Neuroscience Intensive Care Unit
Victor A. Morris MD Assistant Professor of Medicine (General Medicine) Director, Hospitalist Service Associate Chief Medical Officer Vice President, Physician and Patient Access Services Yale-New Haven Hospital
Nils H. Petersen MD, PhD, MSc Assistant Professor of Neurology Staff Neurointensivist, Neuroscience Intensive Care Unit
Joseph L. Schindler MD Associate Professor, Departments of Neurology and Neurosurgery Clinical Director, Yale-New Haven Stroke Center
Patrick R. Tomak MD Assistant Professor of Neurosurgery
Andrew Ulrich MD Vice Chair, Clinical Operations Department of Emergency Medicine Clinical Director of Electrophysiology

Faculty and Planning Committee Disclosures
Critical Care and Emergency Neuroscience: The Essentials May 19, 2016
DISCLOSURE SUMMARY It is the policy of Yale University School of Medicine, through its Center for Continuing Medical Education, to ensure balance, independence, objectivity, and scientific rigor in all its educational programs. All faculty participating in this symposium are required to disclose to the program audience (orally or with slide): any relevant financial relationship(s) they (or spouse/partner) have with a commercial interest that benefits the individual in any financial amount that has occurred within the past 12 months; and the opportunity to affect the content of CME about the products or services of the commercial interest. The Center for Continuing Medical Education will ensure that any conflicts of interest are resolved before the educational activity occurs.
The following indicates participants’ responses to disclosure policy: Name Role Nothing to Disclose Speaker (and/or spouse/partner) has
significant corporate relationship(s) with:
Role of service/financial relationship
Emily J. Gilmore MD F X Alexandra K. Glazier Esq.
F X
David M. Greer MD, MA, FCCM, FAHA
F X
David Y. Hwang, MD F X
Carolina Maciel MD F X
Evie G. Marcolini MD, FACEP, FAAEM
F X
Charles C. Matouk MD PC/F Not available at time of printing
Victor A. Morris MD F X
Andy Morrison F X
Nils H. Petersen MD, PhD, MSc
F X
Allison Rentfro PhD PC X
Kevin N. Sheth MD PC X
Joseph L. Schindler MD
F X
Patrick Tomak MD F X
Andrew Ulrich MD F X
Jessica White PA-C PC X
After review by the Course Director, it has been determined there are no conflicts of interest. Legend: F=Faculty PC=Planning Committee

Critical Care and Emergency Neuroscience: The Essentials May 19, 2016
This conference is supported by educational grants from
Chiesi USA, Inc.
Elekta, Inc.
Penumbra, Inc.
HOW TO OBTAIN YOUR CME CERTIFICATE
In order to obtain your certificate you must complete an online post-test and evaluation.
You will receive an email from Yale CME within 5 business days post-conference, with the instructions below:
1. A link to login to your profile will be provided in the email
2. Login using your email address and password
3. Click on “My live conferences”
4. A list of your registered conferences will appear. Enter the eligible credits for the conference you wish to print
your certificate
5. Click “Save”
6. Click “Start” to complete the post-test; click “Submit”
7. Upon completion of the post test, click “Start” to complete the evaluation; click “Submit evaluation”
8. Click “Print” to print your certificate
Questions – please contact Yale CME at 203.785.4578 or [email protected]
The views of the speakers do not necessarily reflect the views of the Yale School of Medicine
~~~~~~~~~~~~~~~~~~~~~
Recording of this session by attendees is strictly prohibited

Remote Neurological Consultations
Joseph Schindler, MD
Director, Acute Stroke and TeleStroke Services
Yale‐New Haven Hospital
No Disclosures
Agenda
• Defining telemedicine
• The origins of telemedicine
• Models for teleneurology
• TeleStroke
• Tele‐ICU
• Obstacles
• The Future

Definitions
American Telemedicine Association defines:
Telemedicine: The exchange of medical information from one site to another via electronic communications to improve the health status of patients. (curative aspect)
Telehealth: A broader term encompassing aspects of remote health care and not restricted to clinical services. (preventive, promotive, curative)
Origins of Telemedicine
• 1905: Cardiology application: Dutch physician Willem Einthoven long distance transfer of electrocardiograms
History of Telemedicine: Evolution, Context, Transformation. Bashshur,R and Shannon,G. 2010.
Illustration from the cover of Radio News, a popular science magazine from the mid‐20s, visualizing the potential future impact of advances in telecommunication technology on the practice of medicine.

Origins of Telemedicine
• 20’s,30’s,40’s: Norway, Italy, France utilizing radioconsultations for patients aboard boats
• 50’s: Transmission of radiographic images
• 1967: Audiovisual circuit between MGH and LoganAirport for medical consultations
• Late 60’s:NASA initiates active telemedicine program during missions monitoring physiological parameters
Telemedicine Applications in Neurology
Application Telemedicine Technology NeurologyAreas
Practitioners Status
Acute Care RTV Carts,Robots Stroke,ICU Physician,RN Many ActiveNetworks
Inpatient RTV/SF Carts,Robots GeneralNeurology
Physician,RN Activeproviders
Outpatient RTV/SF Desktop PC,carts
PD,MS,Epilepsy,dementia
APP,RN Rural Areas
Home Care Remote,text,email
Home devices
Chronic Disease
None Pilot Studies
Conclusions – Computer-based technology can now be used to integrate electronic medical information, clinical assessment tools, neuroradiology, laboratory data, and clinical pathways to bring state-of the-art expert stroke care to underserved areas. (Stroke. 1999;30:464-469.)

The “Perfect Storm” for Acute Stroke
• IV t‐PA has a narrow therapeutic window
• About 30‐50% of stroke codes are mimics
• IV t‐PA administration carries risk
• Most ER physicians are not comfortable administering IV t‐PA without neurological expertise
• Fewer neurologists are interested in providing acutestroke coverage and fewer can get to the bedside
Telestroke Networks
Muller-Barna,P. Schwamm,L. Haberl,R. Telestroke Increases the use of Acute Stroke Therapy. Curr Opinion Neurology 2012, 25: 5-10.

Telestroke vs. Telephone
• STRokE Doc trial: 1st randomized control trial of telemedicine vs. telephone (2008)
• Accuracy (98% telemedicine vs. 82% telephone)
• Specificity (98% telemedicine vs. 92% telephone)
• Sensitivity (100% telemedicine vs. 58% telephone)
Conclusions:
• Telemedicine is superior over telephone
• When an ER physician and neurologist agree that a patient is eligible for lysis, they are generally correct
• When collaboratively determined that a patient is not eligible, they are too frequently wrong
The Telephone and the Neurological Examination
• Encephalopathy vs. Aphasia
• Severity of the deficit
• Brainstem evaluation
• Conversion disorder
A picture is worth a thousand wordsA video is worth…

Stroke mimic patients classified according to initial NIHSS. NIHSS indicates National Institutes of Health Stroke Scale.
Ali S F et al. J Am Heart Assoc 2014;3:e000838
© 2014 Ali S F et al.
Johnson Memorial Hospital
St. Francis Hospital
Hartford Hospital
Sharon Hospital
Day Kimball Hospital
Westerly Hospital
William Backus Hospital
Middlesex Hospital
New Britain General Hospital
Yale-New Haven Hospital
Waterbury Hospital
St. Mary’s Hospital
Danbury Hospital
Griffin Hospital
Milford Hospital
Bridgeport Hospital
Norwalk Hospital
Stamford Hospital
Greenwich Hospital
Lawrence & Memorial Hospital
Windham Hospital
MidState Medical Center
Hospital of St. Raphael
Bradley Memorial Hospital
New Milford Hospital
St. Vincent Hospital
Bristol Hospital
Dempsey HospitalCCMC
Rockville Hospital
Manchester Hospital
Comprehensive Stroke Centers
Charlotte Hungerford
Telestroke Model
Switzer J, et al. A Web‐based Telestroke System Facilitates Rapid Treatment of Acute Ischemic Stroke in Rural Emergency Departments. The Journal of Emergency Medicine Volume 36, Issue 1 2009 12 ‐ 18

Disruptive Innovation
Low Cost Video Technology
“Off the shelf” video technology: Polycom Platform

Lawrence and Memorial HospitalPre/Post Telestroke
2007 2009
# ischemic strokes 114 159 39% # stroke codes 136 68 50% # IV t-PA cases 10 (8.7%)1 (7%)2 26 (16.3%)1 (38%)2 90%# cases contraindications 18 5 78%# cases documented as being “too mild’ 13 1 92%
1 Total lysis/Total Ischemic Strokes2 Total lysis/Stroke Codes
Thrombolysis Amongst TelestrokeNetworks
TeleStroke Units Serving as a Model of Care in Rural Areas
by Peter Müller-Barna, Gordian J. Hubert, Sandra Boy, Ulrich Bogdahn, Silke Wiedmann, Peter U. Heuschmann, and Heinrich J. Audebert
StrokeVolume 45(9):2739-2744
August 25, 2014
Copyright © American Heart Association, Inc. All rights reserved.

Map of Southeast Bavaria with TeleMedical Project for integrative Stroke Care (TEMPiS) TeleStroke Units.
Müller-Barna P et al. Stroke. 2014;45:2739-2744
Copyright © American Heart Association, Inc. All rights reserved.
Patients with stroke and transient ischemic attack (TIA) admitted to TeleMedical Project for integrative Stroke Care (TEMPiS) hospitals and number of teleconsultations.
Müller-Barna P et al. Stroke. 2014;45:2739-2744
Copyright © American Heart Association, Inc. All rights reserved.
Numbers, rates, and door-to-needle times (including interquartile range [IQR]) of intravenous thrombolysis (IVT) performed in all patients with ischemic stroke.
Müller-Barna P et al. Stroke. 2014;45:2739-2744
Copyright © American Heart Association, Inc. All rights reserved.

Tele‐ICU
Tele-ICU
• 1977: Trial of “television” consultation with university based intensivists compared to telephone consultation
• 1997: Trial of 24 hour remote monitoring, computer based data transmission to communicate with bedside staff
Lilly Clinics Chest Medicine 2015; Grundy et al Crit Care Med 1982; Grundy et al JACEP 1977; Rosenfeld et al Crit Care Med 2000; Breslow Crit Care Med v32 2004
The Need for ICU Expertise
• Recommendation for 24 hour staffing of ICUs by Leapfrog group and others in early 2000’s
• Staffing ICU 24/7 with intensivists is expensive• National shortage of intensivists persists (in 2012, under 600
board certified neurointensivists nationally)• Telemedicine is one method of addressing these issues
Use of audiovisual technology combined with electronic media and data systems to evaluate and treat patients
Young et al JAMA 2000; American Telemedicine Association 2014

Telemedicine in the ICU (Tele-ICU)
InSIGHT Control CenterNew Haven, Connecticut
Intensive Care Unit
Other ICUs ReceivingInSIGHT Coverage
American Telemedicine Association Guidelines, May 2014
Yale-New Haven Tele-ICU
Courtesy of Dr. Peter Marshall
The daily practice of neurointensivists focuses on the recognition of subtle changes in the neurological examination, interactions between the brain and systemic derangements, and brain physiology.
Wijman CA, et al. Research and technology in neurocritical care. Neurocrit Care. 2012;16(1):42-54

Select Robotic Telepresence
Vespa,, et al. "Intensive care unit robotic telepresence facilitates rapid physician response to unstable patients and decreased cost in neurointensive care." Surgical neurology 67.4 (2007): 331-337.
Robotic Tele‐presence (RTP) Reduces Response Times
Vespa,, et al. "Intensive care unit robotic telepresence facilitates rapid physician response to unstable patients and decreased cost in neurointensive care." Surgical neurology 67.4 (2007): 331-337.
Remote NICU Monitoring
Vespa, Paul M. "Multimodality monitoring and telemonitoring in neurocritical care: from microdialysis to robotic telepresence." Current opinion in critical care 11.2 (2005): 133-138.

Jefferson NICU Protocol for RTP
Rincon et al. "Implementation of a model of robotic tele-presence (RTP) in the neuro-ICU: effect on critical care nursing team satisfaction."Neurocritical care 17.1 (2012): 97-101.
The daily practice of neurointensivists focuses on the recognition of subtle changes in the neurological examination, interactions between the brain and systemic derangements, and brain physiology.
Wijman CA, et al. Research and technology in neurocritical care. Neurocrit Care. 2012;16(1):42-54
Teleneuro‐ICU Examination
Cranial Nerve Robotics/AV examination Limitation/Adaptation
II Light reflex,VF, papilledema Fundic Exam impaired without technology
II,IV,VI CN palsy, calorics Nurse instruction, field of view
V Corneal Corneal reflex via nurses
VII Facial strength Patient may be intubated
IX,X Elevate palate Visualization difficult
XI Shoulder shrug Nurse training
XII Tongue Intubation, view
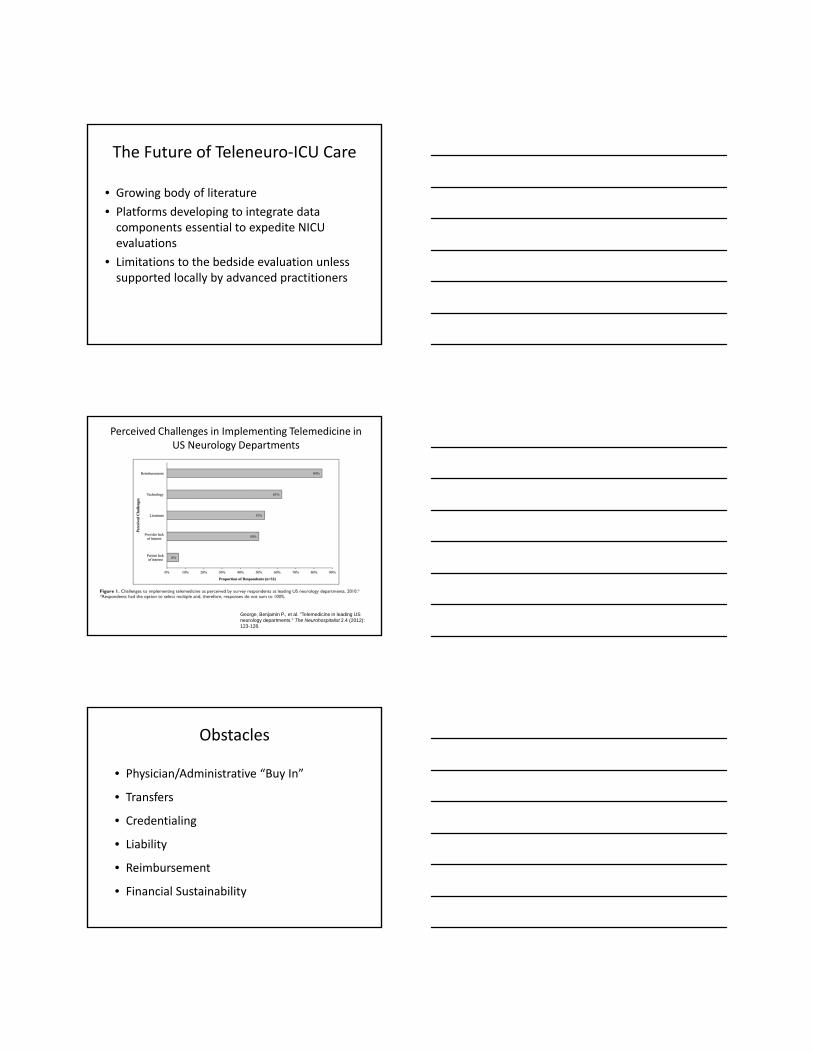
The Future of Teleneuro‐ICU Care
• Growing body of literature
• Platforms developing to integrate data components essential to expedite NICU evaluations
• Limitations to the bedside evaluation unless supported locally by advanced practitioners
Perceived Challenges in Implementing Telemedicine in US Neurology Departments
George, Benjamin P., et al. "Telemedicine in leading US neurology departments." The Neurohospitalist 2.4 (2012): 123-128.
Obstacles
• Physician/Administrative “Buy In”
• Transfers
• Credentialing
• Liability
• Reimbursement
• Financial Sustainability

Liability
• Little precedent
• Assume the same responsibilities as an in‐person “patient‐doctor” relationship 1
• Most litigation involves a perceived loss of opportunity related to a patient not receiving tissue plasminogen activator 2
1 Rousch v. Southern Arizona, Nose & Throat (Ariz. App. Div. 2)2 Zivin, J. Empirical Characteristics of Litigation involving Tissue Plasminogen Activator and Ischemic Stroke. Ann Emerg. Med. 2008;52:160‐164.
http://www.lpklaw.com/medical‐malpractice‐lawyer.php
Reimbursement
• CMS: Originating site (beneficiary) must be in a rural health professional shortage area or a non‐metropolitan statistical area
a. two‐way, real‐time communication
b. Medicare reimbursements at the same level of service as if in person (modifier)
• Bill appropriate CPT code
a. In 2008, AMA approved two new category III codes (remote critical care billing)
b. Payers may not recognize these codes

YaleMedicalGroup/Yale‐NewHavenTeleHealthWorkingGroup
ConnecticutandTelemedicineAnalysisofSubstituteforSenateBillNo.467
PROVIDER INSURANCEPLANS
Definitions/Applicability
• Telehealth provider– licensed physician,psychiatrist,APRN,PA,psychologist,socialworker,certifieddietitian‐nutritionist
• Application– diagnosis,consultation,treatment,education,caremanagement,andself‐managementofpatient’sphysicalandmentalhealth
• Technology– realtime,storeandforward,remotepatientmonitoring
Individualandgroup healthinsurancepoliciesdelivered,issued,renewed,amended,orcontinuedinConnecticutthatcover• Basichospitalexpenses• Basicmedical‐surgicalexpenses• Majormedicalexpenses;or• Hospitalofmedicalservices,includingcoverageprovidedtosubscribersofahealthcarecenter
Requirements • Accessto,orknowledgeofpatient’smedicalhistory• Compliance withstandardofcareforhisorherprofessionexpectedforin‐personcare,butallowstoperformtestingthroughappropriateperipheraldevices
• Patient’sconsentdocumentedinthepatient’smedicalrecordsandHIPAAcompliance
• Coverageofmedicaladvice,diagnosis,care,ortreatmentprovidedthroughtelehealth totheextentthatthoseservicesarecoveredthroughin‐personvisits
• Thesametermsandconditionsthatapplytootherbenefitsunderthepolicy
Prohibitions • PrescribingscheduleI,II,orIIIcontrolledsubstances
• Chargingfacilityortechnicalfees
• Excludingcoverage, providedtelehealth isappropriateforetheservice
• Requiringpreauthorizationfor“emergingtelehealth services”
Demaerschalk B. Smartphone Teleradiology Application is Successfully Incorporated into a Telestroke Network Environment. Stroke. 2012;43:3271‐3277.
The Future: Improved Technology Efficiency
Google Glass

Further Regionalization of Stroke Networks
• Comprehensive Stroke Centers
• “Big Med” 1
• NIH/NINDS
1 Gawande A. Annals of Healthcare: Big Med. The New Yorker. 13 Aug 2013
The Future
• Optimization of technology
• Regionalization of stroke networks
• Development of surrogate outcome measures
• Expansion of platforms conductingteleneurology, tele‐ICU evaluations
• Formalized reimbursement schemes

YAccess Neuroscience Triage and Transfer:Collaborating with Regional Hospitals
Victor Morris, MDAndrew Ulrich, MD
Disclosures•None
Yale New Haven Hospital
• 1541 beds• >80,000 discharges• 142 Adult ICU beds• Advanced Technologies
Yale New Haven Hospital
Yale New Haven Hospital
Yale New Haven Hospital
14 Bed Neuro ICUDedicated RN’sNeuroIntensivists
Yale New Haven Hospital
26 Bed Neurosciences floor/step‐down Dedicated RN’s
Yale New Haven HospitalYAccess
888‐YNHHBED888‐964‐4233
1 minute
Yale New Haven Hospital

Yale-New Haven Hospital est. 1826
Teaching hospital
Medicine / Nursing / EPH
Centers of Excellence
Magnet Designation – 2011
1,541 bed Tertiary referral
3 Adult Emergency Depts.York Street ~100k/yr.
SRC ~35k/yr.
Shoreline ~30k/yr.
Who is Yale New-Haven ED
Our Doors Are Always Open
24/7 365

Who is Yale-New Haven ED
• Level 1 Trauma Center
• > 100,000 ED visits/year(YORK ST.)
• ~40% admission rate
• ~20% ICU admission rate
• 130 STEMI activations/yr.
• 1150+ Stroke codes/yr.
• 3300 Trauma/yr.

Who is Yale New-Haven EDProviders:
• Staffed with 70+ board eligible/certified faculty• Yale University Department of Emergency Medicine• Leading academic and research dept.
• Fellows in ED specialized training programs• US/EMS/Global Health/Admin./RWJ
• 60+ Residents; 4 year program
• APP’s with specialized EM training
Team Leads
Gail D’Onofrio – Chair, Department of Emergency Medicine
Andrew Ulrich - Vice Chair Clinical Operations
Vivek Parwani - York St Medical Director
Evie Marcolini – Director Sky Health; Chair ACEP Critical Care; NICU intensivistCharles Wira – Chair NECC; Chair CT Stroke Task Force; Stroke Call Liaison
Dave Cone – Region 2 Medical director; Former Editor Acad Emerg Med
Who is Yale New-Haven ED
Nursing:
100 RN’s with specialized ED training;
ACLS/TNCC certification
Trained in abbrev NIHSS
Team Leads
Mark Sevilla – Nursing Director Thomas Saxa – Patient Service Manager Clinical Managers Clinical Educators
WHO IS YALE-NEW HAVEN ED
Multiple, simultaneous patient care services
Interpreter Services
Social Work
Chaplain Services
Security-Police
Volunteers
Pharmacists
Care Coordinators
Project Assert

What is Yale-New Haven ED
Facilities 4 resuscitation bays; enable high level critical care
monitoring 68 Beds Critical Care area with 19 major med beds; higher level
hemodynamic monitoring (art lines; CVP monitoring; etCO2) ; tele-critical care monitoring
Equipment Arctic Sun (cooling) Rapid transfuser for trauma 4 State-of-the-Art Ultrasound machines
- CT 64 slice (CTA/CTP)MRI (hyperacute)
What Happens?Pre-Arrival: Communication
YAccess informationResource mobilizationPrepare DI/IR/OR/Pharmacy SupportCare Teams await arrival
Arrival:Rapid Assessment and Treatment:Stabilization/ResuscitationPharmacologic interventionDiagnostic testing
Immediate disposition to Definitive care; IR/OR/NICU
Goal: Rapid identification and initiation of definitive treatment
Key is communication/hand offs
Yale Center for Healthcare Innovation, Redesign and Learning (CHIRAL)
The Yale Center for Healthcare Innovation, Redesign, and Learning(CHIRAL) is a
joint venture of Yale School of Medicine (YSM) and Yale-New Haven Hospital (YNHH) creating a dynamic learning environment to improve patient
safety.

Yale Center for Healthcare Innovation, Redesign and Learning (CHIRAL)
This project aims to develop innovations to improve the safety of inter-facility transfers.
To study and ameliorate failures in shared decision making during ED-ED transfers.
To study and ameliorate systems failures during ED-to-ED transfers.
To evaluate the impact of our system redesign on improving the safety of ED-to-ED transfers.
Project 1:Improve the Safety and Quality of Transitions into Yale-New Haven Hospital for patients with atraumatic intracranial hemorrhage.
Yale Center for Healthcare Innovation, Redesign and Learning (CHIRAL)
Project Aims
1) Define the current process of care transitions for patients with atraumatic intracranial hemorrhage (aICH) and identify latent safety threats that exist within this process
2) Develop and implement a multi-modal, comprehensive set of interventions to reduce these latent safety threats and improve care processes and clinical outcomes for patients with aICH

Brain DeathDetermination
David M. Greer MD, MA, FNCSDepartment of Neurology
Yale University School of Medicine
Disclosures•I serve as editor-in-chieffor Seminars in Neurology

Why did brain death not exist until the1950’s?
Advances in mechanical ventilation haveenabled prolongation of systemic organfunctioning after devastating neurologicalinjury.
Now decisions must be made which arebeyond medical, now involving cultural,ethical and legal issues.
Background
• Mollaret and Goulon initially introducedthe term in 1959, when they described 23patients with irreversible coma, with– Unresponsiveness
– Loss of brainstem reflexes
– Loss of spontaneous respirations
– Flat EEGs
Mollaret P, Goulon M. Le coma depassé. Rev Neurol. 1959;101:3-15.
The correct determination of brain deathis essential in medical care:
To ensure inappropriate measures are notundertakenTo provide finality for families unclear
about prognosisTo preserve vital critical care resourcesFor possible organ donation

Pathology of Brain Death
• The most common causes of braindeath in adults:
– traumatic brain injury
– hypoxic/anoxic brain injury
– subarachnoid hemorrhage
• In children:
– abuse
– motor vehicle accidents
– asphyxia
Brain Death History
President’s Commission Report (1981)
NIH Collaborative Study(1977)
Determination of Death Act
Harvard(1968)
“Irreversible Coma”No brainstem reflexes“Flat” EEGProposed brain death
Defined the futility of brain death
Affirmed the validity of brain death
Proposed guidelines on how to approach brain death diagnosis
Practice Parameters published in 1995, based on the Uniform Determination of Death Act (UDDA): An individual who has sustained either 1) irreversible cessation of circulatory and respiratory functions, or 2) irreversible cessation of all functions of the entire brain, including the brain stem, is dead. A determination of death is made with acceptable medical standards.
Uniform Determination of Death Act, 12 uniform laws annotated 589 (West 1993 and West suppl 1997)

Fundamental Questions
1. Are there patients who fulfill the clinical criteria ofbrain death who recover neurologic function?
2. What is an adequate observation period to ensurethat cessation of neurologic function is permanent?
3. Are complex motor movements that falsely suggestretained brain function sometimes observed in braindeath?
4. What is the comparative safety of techniques fordetermining apnea?
5. Are there new ancillary tests that accurately identifypatients with brain death?

Question #1: recovery of function
• In adults, recovery of neurologicfunction has not been reported after theclinical diagnosis of brain death has beenestablished using the criteria given in the1995 AAN practice parameter. (Level U)
Question #2: Adequate ObservationPeriod
• There is insufficient evidence todetermine the minimally acceptableobservation period to ensure thatneurologic functions have ceasedirreversibly. (Level U)
Question #3: complex motormovements
• For some patients diagnosed as brain dead, complex,non brain mediated spontaneous movements can falselysuggest retained brain function. Additionally, ventilatorautocycling may suggest patient initiated breathing.(Level C)
• Spinally mediated reflexes include DTR s, triple flexion,Babinski’s sign. Also the Lazarus sign with slightspontaneous abduction or adduction of an extremity,raising of the torso to a 40 60 angle, head turning toone side, arm raising, and back arching. In some patientsthis may be seen in synchrony with ventilator deliveredbreaths.

Question #4: safety of apneatechniques
• Apneic oxygenation diffusion todetermine apnea is safe, but there isinsufficient evidence to determine thecomparative safety of techniques forapnea testing. (Level U)
Question #5: New ancillary tests
• Because of a high risk of bias andinadequate statistical precision, there isinsufficient evidence to determine if anynew ancillary tests accurately identifybrain death. (Level U)
Practical (non evidence based)guidance
• Many of the details of the clinicalneurological examination to determine braindeath cannot be established by evidencebased methods. The detailed brain deathevaluation protocol that follows is intended asa useful tool for clinicians. It must beemphasized that this guidance is opinionbased.

Brain Death Determination:4 Steps
1. Clinical evaluation (prerequisites)
2. Clinical evaluation (neurologic assessment)
3. Ancillary tests
4. Documentation
Clinical Evaluation –Prerequisites
• CARDINAL RULES:–Establish cause of coma–Establish irreversibility
Establish Cause + Avoid Pitfalls
– Cause can usually be determined by history,examination, neuroimaging or lab tests
– Exclude the presence of CNS depressant drugeffect by history, drug screen, calculation ofclearance using 5 times the drug’s half life(assuming normal hepatic and renal function),or drug plasma levels in the therapeutic range.
– Prior use of hypothermia may delay drugmetabolism
– BAL of < 0.08% is a practical threshold

Clinical Evaluation –Prerequisites
• No recent administration of continued presence ofneuromuscular blocking agents (assessed withtrain of 4 twitches with maximal ulnar nervestimulation)
• No severe electrolyte, acid base, or endocrinedisturbance (defined by severe acidosis orlaboratory values markedly deviated from thenorm)
• Achieve core temperature: >36 C• Achieve systolic blood pressure: 100 mm Hg
Clinical Evaluation –Prerequisites
• 1 neurologic examination: If a certain period oftime has passed since the onset of the braininsult to exclude the possibility of recovery (inpractice, usually several hours), 1 neurologicexamination should be sufficient to pronouncebrain death. However, some US state statutesrequire 2 examinations.
• All physicians are allowed to determine braindeath in most US states. Some US state orhospital guidelines require the examiner to havecertain expertise.
Clinical Evaluation –Neurologic Assessment
• 3 cardinal features:
1. Coma
2. Absence of brainstem reflexes
3. Apnea

Clinical Evaluation –Neurologic Assessment
• Coma: patients must lack all evidence ofresponsiveness
• No eye opening or eye movement to noxiousstimulation
• Noxious stimulation produces no motorresponse, other than spinally mediated
• Distinguishing between cerebrally or spinallymediated responses requires expertise (andsometimes ancillary testing may be necessary)
Clinical Evaluation –Neurologic Assessment
1. No pupillary response to bright light in eithereye. Pupils usually fixed and 4 9 mm.Constricted pupils should suggest possibledrug intoxication. A magnifying glass shouldbe used for uncertain response.
What are Doll s Eyes ???
What are Doll s Eyes ???
Clinical Evaluation –Neurologic Assessment
2. No eye movements to OCR or OVR testing.Once integrity of C spine ensured, head isbriskly rotated horizontally and vertically.OVRs tested by:
1. Ensure integrity of auditory canal and TM
2. Elevate head to 30 degrees
3. Irrigate one ear at a time with ice water, 50 mL
4. Observe for eye movements for 1 minute
5. Wait 5 minutes before testing opposite ear
Clinical Evaluation –Neurologic Assessment
Confounding factors for the OVR test include
Prior exposure to certain ototoxic drugsaminoglycosides, vancomycin, certain antiepilepticdrugs, tricyclic antidepressants, chemotherapeuticagents, and anticholinergics
Trauma to the globes, orbits, or petrous bone.
Severe globe or facial edema

Clinical Evaluation –Neurologic Assessment
3. Absent corneal reflex by touching cornea withpiece of tissue paper, cotton swab or squirts ofwater. (I press on the cornea)
4. Absent facial movement to noxious stimulation(nasal tickle, pressure on TMJ and supraorbitalridge). Facial myokymias permissible.
5. Absent pharyngeal and tracheal reflexes, testedby stimulation of posterior pharynx with atongue blade or suction device. Assess for coughreflex with tracheal suctioning to level of carina.
Brain Death Examination
APNEA TESTING
• Prerequisites:– Normotension ( 100 mm Hg, with/without pressors)
– Normothermia (>36 C)
– Euvolemia
– Eucapnia (PaCO2 35 45)
– No hypoxia
– No prior CO2 retention (e.g. COPD, OSA, severeobesity)

APNEA TESTING
• Preoxygenate for at least 10 minutes with 100%oxygen to a PaO2 of >200 mm Hg
• Reduce ventilation frequency and/or tidal volumeto establish eucapnia
• Reduce PEEP to 5 cm H20 (O2 desaturation withdecreasing PEEP may suggest difficulty withapnea testing)
• If pulse oximetry O2 sat remains >95%, obtainbaseline ABG
• Disconnect the patient from the ventilator
APNEA TESTING
• Preserve oxygenation by providing oxygen tothe level of the carina with 100% O2 at 4 6liters/min via a catheter in the ET tube
• Observe closely for respiratory movements for8 10 minutes.
• Abort if SBP <90mm Hg
• Abort of O2 sat <85% for >30 seconds.• Retry procedure with T piece, CPAP 10 cm H2O,and 100% O2 12 l/min
APNEA TESTING
• If no respiratory drive is observed, repeat ABG after ~ 8minutes
• If respiratory movements are absent and arterial PCO2 is60 mm Hg (or 20 mm Hg increase in arterial PCO2 overa baseline normal arterial PCO2), the apnea test ispositive.
• If the test is inconclusive, but the patient was stableduring testing, repeat for longer (10 15 minutes), afteragain adequately preoxygenating and reestablishingnormocapnea

Trick of the Trade
• If the patient becomes hypotensive duringapnea testing, reconnect the ventilator ASAPand hyperventilate
Apnea Testing – potentialcomplications
The most common complication ishypotension, which typically occurs whenthere is inadequate pre oxygenation.
Tension pneumothorax has been reported, butit is unclear whether it was related to theapnea testing.
Cardiac arrest during apnea testing is felt to bequite rare, but has been reported.
Goudreau JL, Wijdicks EFM, Emery SF. Neurology. 2000;55:1045-1048.

Ancillary Testing
Brain death is a clinical diagnosis.
Ancillary testing is not required, unless theclinical exam is drawn into question.
Even ancillary testing is potentiallyconfounded in certain circumstances.
Clinical judgment remains paramount.
Preferred tests: SPECT, cerebral angiography,TCD, EEG
Ancillary Tests – cerebralangiography
Cerebral angiography should show an absenceof flow in all intracranial arteries
Contrast will typically fill the external carotidcirculation, also supplying the meningealarterial system.
ICA and vertebral artery flow should arrest atthe point of entry at the dura.
Cantu RC. Lancet. 1973;1:1391-1392.
4 Vessel ConventionalCerebral Angiogram (4VsA)
M. Sawicki, et al. Angiography in the evaluation of brain death. Polish Journal of Radiology. 2009

Ancillary Testing SPECT
• SPECT uses 99mTc HMPAO, injected 15 30 minutesbefore scanning.
• There should be an absence of intracranial perfusion,seen as a lack of uptake of tracer.
• Given the persistent extracranial circulation, there isflow to the meningeal and skull vessels, giving rise tosuch signs as the hollow skull, empty light bulband hot nose signs
Facco E, et al. Intensive Care Med. 1998;24:911-917.
37-year-old woman, S/P cardiac arrest.
EEG Brain DeathNot first line ancillary test for BD; specific methodology must be employed if used
EEG for BD determination:
16- or 18-channel x 30 minMinimum: 8 channel
Impedance:100-10,000 ohms
Inter-electrode distance >10 cm
Sensitivity: at least 2 μV
Filter: High>30 Hz; Low freq < 1 Hz
No response to auditory, visual, or tactile stimuliAmerican Electroencephalographic Society.
J Clin Neurophysiol. 1994;11:10-13.
NORMAL
Electrocerebral Inactivity of BD

Ancillary Tests – TranscranialDoppler
Confirmation of cerebral circulatory arrestwith extra and intracranial Dopplersonography
Bilateral, anterior and posterior, twoexaminations 30 minutes apart.
Systolic spikes or oscillating flow in anycerebral artery (anterior or posterior).
J Neurol Sci. 1998; 159:145-150.
TCD Criteria, continued
Disappearance of intracranial flow signals isdebatably reliable
Studies have excluded patients withventricular drains or large craniotomy.
The sensitivity for confirming circulatoryarrest ranges from 91 99%, but specificity100%.
TCD Brain Death

Other Ancillary Tests
• Multiple reports on MRA, CTA – noprospective studies, NOT VALIDATED.
• Evoked potentials have been studiedextensively in brain death, but have arelatively poor predictive value. This may beimproved with nasopharyngeal electrodeplacement.
Machado C, et al. Electroencephalogr Clin Neurophysiol.1991;80:392-398.
Documentation
• Time of death is:
– The time the arterial PCO2 reached the target value
– The time when the ancillary test has been officiallyreported
Federal and state law requires the physician to contactan organ procurement organization followingdetermination of brain death. (Hopefully, this hasalready been done prior to this point.)

Common Pitfalls in Brain DeathTesting
• Severe facial trauma
• Pre existing pupillary abnormalities
• Medications influencing the examination
• Acid base disorders, electrolyte disorders
• Sleep apnea or severe pulmonary diseaseresulting in chronic CO2 retention

What are we doing to improve the field?
• Educational/training endeavors
– Web based training
– Simulation training
– “Champions”
• Creation of a national/international standard
– Reevaluate policies since the 2010 AAN PracticeParameters – under review
– Reevaluate international policies done
– Lobby at a national level for ONE STANDARD
• Brain Death Ethics Subcommittee of NCS
What is the potential???
Potential Live-Years Saved by a Deceased Organ Donor
Schnitzler MA et al. Am J Transplant. 2005;5:2289-96.

Brain Death vs. DCD• Much greater chance for organ retrieval, greater number of
viable organs.
• A 21 yo MVA victim was able to provide to patients on thetransplant waiting list:
– Kidney & pancreas to a 43 yo woman with end stageIDDM – law professor
– Kidney to a 33 yo man in Tennessee
– Liver (split) to 61 yo man with hepatocellular CA
– Liver to a 10 month old with biliary atresia
– Heart to a 54 yo man with Adriamycin inducedcardiomyopathy
– Lung to a 62 yo local man with end stage COPD
– Also donated bone, ligaments, tendon, skin, cornea,saphenous and femoral veins

Navigating Prognosis inNeuroscience Intensive Care Units
David Y. Hwang, MD
Assistant Professor of NeurologyDivision of Neurocritical Careand Emergency Neurology
Yale School of Medicine
Critical Care and Emergency Neuroscience: the EssentialsMay 19, 2016
2
Disclosures
American Brain Foundation – Practice Research Training Fellowship
Apple Pickers Foundation (Westerly, RI)
National Institute on Aging – Loan Repayment Program
Neurocritical Care Society – Research Training Fellowship
3
ICU comfort care practices
Clinical scales
Family discussions
This presentation highlights the importance of prognosis in the Neuro ICU and reviews pitfalls in outcome prediction

4
Six separate Canadian level‐one trauma centers
Adjusted ORs for death following care withdrawal for traumatic brain injury patients
Significant variation exists in comfort care practices among centers caring for neurocritically ill patients
Turgeon et al. CMAJ 2011;182:1581.
5
Moving a stroke patient to a hospital with a higher propensity for feeding tube placement increased odds of placement 1.45‐fold
Variation in feeding tube insertion rates across US hospitals is large for ischemic stroke patients
George et al. Neurology 2014;83:874.
6
Accurate prognosis is critical for situations in which clinicians are discussing comfort care with patients’ families
Reasons for variation in local practices to trach/PEG versus pursue comfort care at various centers is unclear

7
Early impressions of prognosis strongly influence aggressiveness of care for neurocritically ill patients
Zurasky et al. Neurology 2005;64:725
Timing of life support withdrawal decisions for ICH patients
Within first 24 hoursAfter first 24 hours
30%
8
Multiple “scientific” tools for estimating early prognosis for neurocritically ill patients have been developed
Utilize admission clinical and radiologic variables
Relatively easy to learn and apply
Rapidly stratify patients early on
“Objectify” prognosis
Crandall et al. Rev Neurol Dis. 2011;8:23
9
Saposnik et al. Circulation. 2011;123:739

10
Hemphill et al. Neurology. 2009;73:1008
Models for “predicting” outcome are limited by self‐fulfilling prophecies
Morgenstern et al. Neurology 2015;84:1739.
Green = 30‐day mortality predicted by ICH Score
Grey = actual 30‐day mortality when DNR order is avoided for 5 days
11
12
Applying prognosis predictions from population models to individual patients must be done with caution
Hwang et al. Neurology. 2016;86:1.
0.81
0.72
0.55
‐0.46
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Attendings Nurses ICH Score FUNC Score
Spearman’s rankCorrelation (r)
p values < 0.02 for all comparisons betweenproviders and scores
Correlation with 3‐month mRS of subjective predictions and clinical scales for ICH

13
The prognosis that we give a surrogate decision maker is only a small part of his or her own prognostic assessment
Boyd et al. Crit Care Med. 2010;38:1270.
Sources contributing to surrogate’s prognostic impression % Surrogates reporting
Physician’s prognostic estimate ALONE 2%
Physician’s prognostic estimate as PARTIAL role 47%
Patient’s intrinsic qualities and will to live 27%
Patient’s physical appearance 64%
Patient’s survival of prior illnesses 28%
Power of surrogate’s bedside presence 13%
Optimism, intuition, faith 36%
14
Surrogates often interpret physician prognostic estimates with an optimistic bias
Zier et al. Ann Intern Med 2012;156:360.
15
Quantitative estimates of prognosis can even be influenced by how numbers are framed to surrogates
Chapman et al. J Crit Care 2015;30:231.
“Your relative has a _____ chance of dying in the next few days.”
Please rate the risk to your relative with a cross on this scale(0=no risk, 10=highest):
Probability Median number marked on scale (IQR) p
“2%” 2.0 (1‐5) < 0.01
“1 in 50” 5.0 (3‐8)

Recognize that common biases may arise when attempting to predict future “quality of life” (affective forecasting)
Creutzfeldt et al. Stroke 2012;43:3405.
Recall bias (remembering a patient as healthier than he/she really was)
Focusing illusion
Disability paradox
16
People with disabilities often report greater quality of life compared to healthy people asked to imagine disabilities
Carr et al. BMJ 2011;322:1240.Creutzfeldt et al. Stroke 2012;43:3405.
Stroke deficitsresolve completely
Stroke deficits stay and expectations do not change
Response shift
17
When imagining a disability, people tend to focus only on negative impact and overlook positive aspects of life
Attitudes towards decompressive craniectomy in healthy population
Klein at al. Neurocrit Care 2012;16:456.
Actual emotion scores on the Stroke Impact Scale for decompressed patients are no worse than normative data for all stroke patients
Vahedi et al. JNNP 2005;76:1181.
18

Be careful of rushing to judgment with regards to prognosis and future quality of life for patients with brain injury
19
Clinical scales must be applied with caution, and awareness of common biases when meeting with patients’ families is important