cricoid pressure: are we really doing it right? nichole m. doyle, md university of kansas som...
TRANSCRIPT

Cricoid Pressure: Are We Really Doing it Right?
Nichole M. Doyle, MD
University of Kansas SOM Wichita
4/14/2011

Outline• Introduction• Cricoid Pressure Study• Cricoid Pressure Basics• Cricoid vs BURP procedure
Cricoid Study Design• 143 Anesthesiolgists, Residents,CRNA’s, OR Staff and RT’s•Pre-didactic questionairre•Simulated RSI/Emergent intubation•Short power point presentation•Allowed to practice on simulator• Returned 2 months later for repeat testing

Questionnaire• Yrs of experience• Formal training• How cricoid pressure was learned• Indications and Contraindications for
CP• When is CP released• How many Newtons should be applied• What is a Newton• Did person feel adequately trained
Results From Questionnaire
• 100% found the didactic training beneficial
• 99% of participants found the simulation beneficial
• 55% of participants learned to apply cricoid pressure from observation or OJT
• 72% had not received formal training

Results from Questionnaire Cont.
• 20% incorrectly believed primary function was to improve visualization
• 7% Knew the proper amount of pressure to apply
• 11% Knew what a Newton was• 67% Felt inadequately trained

Results From Simulation• Correct Location Improved from 45%-
88%• Correct amount of pressure before LOC
improved from 68%-74%• Correct amount of pressure after LOC
improved from 3%-56%• Drop in Pressure during DL decreased
from 100% to 29%• Cricoid pressure released appropriately
increased from 94%-98%

Cricoid Pressure• Pressure applied to cricoid cartilage
with goal of occluding hypopharynx and prevent aspiration
• Still controversial but still a medicolegal standard of care
• Cricoid cartilage is used because it’s the only complete ring
• Often confused with BURP procedure
Technique Using the thumb and index finger on either side of
the cricoid cartilage apply 10 Newtons of pressure directly backwards prior to induction of anesthesia
Increase pressure to 30 Newtons upon loss of consciousness
Maintain pressure until position of endotracheal tube is confirmed by breath sounds and permission is given by intubating personnel
10 Newtons is the force of gravity on an object with a mass of approx 1kg
Therefore approx 2-3lbs for awake pts and approx 7lbs-10lbs for unconscious pts
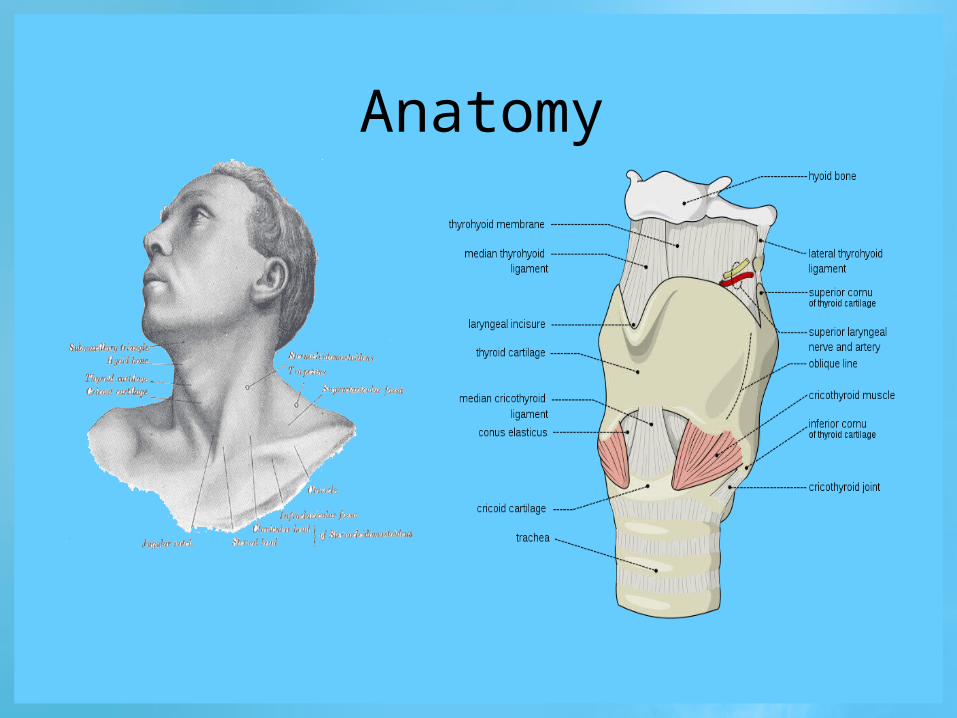
Anatomy

Demonstration of application

Indications
• Code/Emergent Intubation• Full Stomach/Recent Meal• Delayed gastric emptying
• Trauma, acute abdomen• Incompetent lower esophageal
sphincter• Hiatal hernia, pregnancy, severe
symptomatic GERD

Contraindications
• Suspected cricotracheal injury• Active vomiting• Unstable cervical spine injuries• Foreign body in upper airway• Tracheotomy
Complications• Cricoid Pressure may….
• Interfere with ventilation• Make passage of ETT difficult• Alter laryngeal visualization
• Esp at pressures > 40 N• In awake pts has promoted vomiting• Esophageal rupture• Decreased lower esophageal sphincter
tone• Cricoid Cartilage fracture

BURP Procedure• BURP (Backward, upward, rightward,
procedure)• Is done with the objective of improving
view of intubator during direct laryngoscopy
• Pressure applied to thyroid cartilage• Much less pressure than what is
applied during application of cricoid pressure
Final Points• Pressure amounts given are for adults• Release cricoid pressure if it interferes with
ventilation or visualization• Maintain constant pressure after LOC occurs
until ETT position confirmed• BURP and cricoid pressure are different
maneuvers with different goals• Training improves location and amount of
pressure applied• Participants felt more comfortable applying
CP after teaching
THANK YOU
Questions?
References• Neilipovitz DT, Crosby ET. No evidence for decreased incidence of aspiration after rapid sequence induction. Can J Anaesth
2007;54:748–64 • Brimacombe JR, Berry AM. Cricoid pressure. Can J Anaesth 1997;44:414–25 • Palmer JH, Mac G, Ball DR. The effect of cricoid pressure on the cricoid cartilage and vocal cords: an endoscopic study in anaesthetized
patients. Anaesthesia 2000;55:263–8 • Howells TH, Chamney AR, Wraight WJ, Simons RS. The application of cricoid pressure. An assessment and a survey of its practice.
Anaesthesia 1983;38:457–60 • Ashurst N, Rout CC, Rocke DA, Gouws E. Use of mechanical simulator for training in applying cricoid pressure. Br J Anaesth 1996
Oct;77(4):468-72.• Herman NL, Carter B, Van Decar TK. Cricoid pressure: teaching the recommended level. Anesth Analg 1996;83:859–63 • Schmidt A, Akeson J. Practice and knowledge of cricoid pressure in southern Sweden. Acta Anaesthesiol Scand 2001;45:1210–4• Meek T, Gittins N, Duggan JE. Cricoid pressure: knowledge and performance amongst anaesthetic assistants. Anaesthesia 1999; 54:59–
62 • Rice MJ, Mancuso AA, Gibbs D, Morey TE, Gravenstein N, Deitte LA. Cricoid Pressure Results in Compression of the Postcricoid
Hypopharynx: The Esophageal Position is Irrelevant. International Anesthesia Research Society 2009;109:1546-1552.• Matthews, GA. Survey of cricoid pressure application by anaesthetists, operating department practitioners, intensive care and accident
and emergency nurses. Anaesthesia 2001;56:915-917.• Marcus, Adam. Legal, Clinical Data Paint Conflicting Picture of Cricoid Pressure. Anesthesiology News 2010;36.