country team action plan pakistan. where are we now? population growth rate remains high large...
TRANSCRIPT

Country Team Action Plan
PAKISTAN
Where are we now? Population growth rate remains high Large population (25 Percent) has unmet need for
contraception in 2006-07 Contraceptive prevalence rate for modern methods has
stagnated around 22 percent (all methods at 30 percent) Inadequate knowledge and motivation about birth
spacing/ HTSP Health outlets offer limited BS/FP services High abortion rate related to unwanted pregnancies
Selected Best Practice for Pakistan
Integration of quality family planning
services in public health delivery system
Where do we want to be?GOAL
Increase access to quality BS/FP services through health service
delivery system

Areas of Focus
• Policy• Programmatic• Monitoring and Supervision • Commodity/Supplies • Demand Generation• Innovation
Policy Focus
Service Delivery – Ensure FP/BS services at all SDPs – Develop contraceptive uniform pricing policy
for public health system– Sustain commodity support – Improve partnership with private sector and
NGOs for provision of FP/BS information and services particularly for hard to reach areas
Policy Goal
Capacity Development – Revise pre-service curriculum for all
medics and paramedics
– Train and orient all existing medics, paramedics and out reach workers
Programmatic Level• Notify Provincial governments to ensure:
– delivery of BS/FP services through all SDPs and out reach workers – Design and institutionalize system for communication, advocacy &
mobilization – National Communication Strategy
• Involve private sector and NGOs for provision of FP/BS information and services
• Implement LMIS to improve availability rate of contraceptive commodities and sustain supply chain management
• Relevant BS/FP indicators to capture performance/progress to be incorporated in MIS systems
Guiding Principles on Delivery of
BS/ FP Services• No targets or quotas for any contraceptive method• No denial of rights on non-acceptance of birth spacing
options• No incentives for program personnel and FP acceptors• Informed voluntary consent

Monitoring and Supervision
• Notify focal persons at federal, provincial and district level
• Select indicators on BS/FP performance and Progress
• Use of Information for Operational Management and Decision Making
• Strengthen Supervision and Monitoring
What are the possible challenges to the
intervention?• Coordination between Health and Pop Welfare• Absence of warehouse at provincial and district levels• Contraceptives not part of EDL and EDL not uniform
across provinces • Inadequate capacity for management, communication
and M&E• PSDP allocations for implementing BPs• Inadequate information system for supply chain
management • Donor Coordination

Who are the possible partners, allies, and
stakeholders to scale up?– Government of Pakistan
Ministry of Health (MoH), Ministry of Population Welfare (MoPW) and People’s Primary Health Initiative (PPHI)
– Private Sector, Social Marketing & NGOs– Media and communication organizations – Pharmaceutical sector– Community and Religious Leaders– Development Partners
What is the evidence to support this best practice?
• Global and Regional evidence• National data to support scale up
• Gather local evidence on Post Partum IUCD insertion prior to scale up
What are the modifications needed to improve the
intervention’s scalability?• Revise pre-service and in-service curriculum• To implement the BP, revisit Post Partum and
Post-Abortion protocol • Joint review of BS/FP communication
strategy
What are the opportunities of scaling-up?
Opportunities • Political Commitment and Conducive environment • Infrastructure and health facilities (13,000 facilities) to
increase coverage and access • Community-Based Midwives (12,000) and Lady Health
Workers (96,000)• Integration of FP in HIV/AIDS VCT Centres • Introduction of Sino-2 Implant• Donor support
Constraints • Lack of understanding of HTSP as health initiative• Inadequate financing • Barriers to BS/FP practices• Limited Capacity at Management and Program
Implementation • Weak Coordination at all levels
What are the constraints of scaling-up?
What Policy, Regulatory, Budgetary or Other
Institutional Steps are needed• Health Policy to reflect HTSP
• Enable out reach workers to assess and provide the first and subsequent doses of injectables
• PC-I revisions to include HTSP
• PSDP allocations to support implementation
• All training curricula to include module on BP Implementation Strategy
• Add contraceptives in EDL
• Establish technical Committee of Communications, Advocacy, and Mobilization
• Joint Technical Committee on Innovations to review new technologies

Where, when and how will the best practice be
expanded • National with focus on low performing districts
How
• National Consensus already in place (Karachi Declaration) and MOH-FP road map
• Establishment of BP Secretariat• Dissemination of Country Action Plan through
Provincial and Regional Meetings

What will the cost of expansion and how will
needed resources be mobilized • Detailed costing on the following done at country
level – Training– Contraceptive commodities– Warehouse and storage – Need to cost out management and communication,
advocacy and other areas
• Resources to be provided by GoP and Development Partners
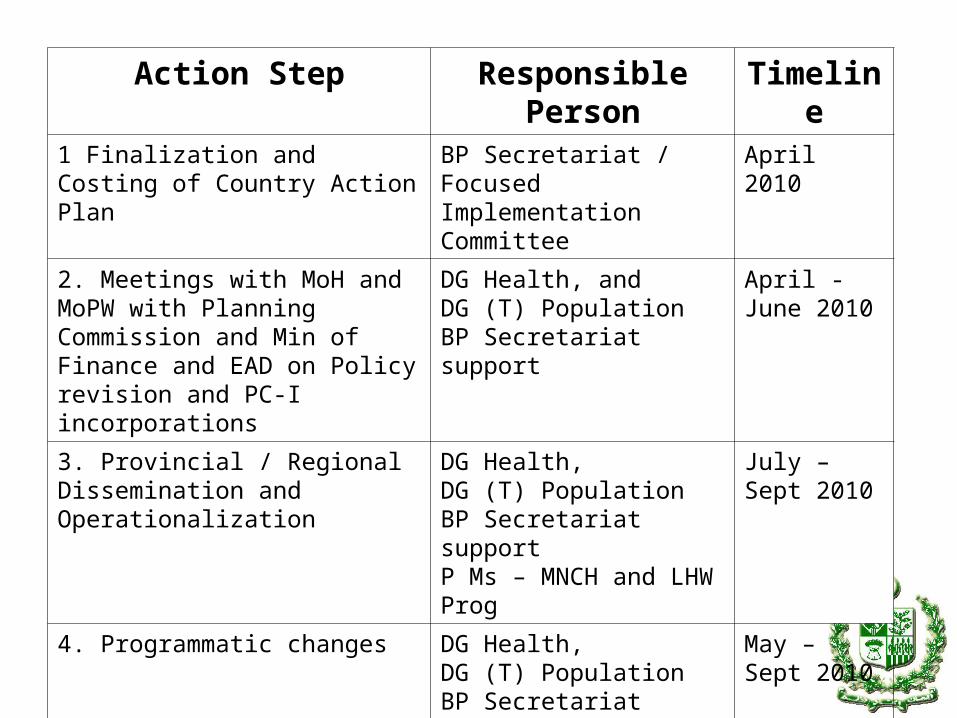
Action Step Responsible Person
Timeline
1 Finalization and Costing of Country Action Plan
BP Secretariat / Focused Implementation Committee
April 2010
2. Meetings with MoH and MoPW with Planning Commission and Min of Finance and EAD on Policy revision and PC-I incorporations
DG Health, and DG (T) Population BP Secretariat support
April - June 2010
3. Provincial / Regional Dissemination and Operationalization
DG Health, DG (T) PopulationBP Secretariat supportP Ms – MNCH and LHW Prog
July – Sept 2010
4. Programmatic changes DG Health, DG (T) PopulationBP Secretariat supportP Ms – MNCH and LHW Prog PNC / PMDC
May – Sept 2010
2121
““I dream of a I dream of a Pakistan, of an Asia, Pakistan, of an Asia, of a world, where of a world, where every pregnancy is every pregnancy is planned, and every planned, and every child conceived is child conceived is nurtured, loved, nurtured, loved, educated and educated and supported”. supported”.
International Conference on Population International Conference on Population & Development held at Cairo in 1994& Development held at Cairo in 1994
22