copd prescribing guidelines - south staffordshire joint ... · south staffordshire area prescribing...
TRANSCRIPT
Cannock Chase Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group East Staffordshire Clinical Commissioning Group
South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Approved August 2017 Written by MMSESSP (2015), updated 2017 Review August 2018
South Staffordshire Area Prescribing Group
COPD Prescribing Guidelines
Inhaler choices in this guideline are different from previous versions produced by the APG.
It is not expected patients controlled on established therapy will be changed without clinical assessment.
All NEW patients should be initiated on inhaler therapy as per these guidelines.

South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 1
COPD Prescribing Guidelines This guideline is intended for use to aid diagnosis in patients with a suspected diagnosis of a COPD, and the management of patients with a confirmed diagnosis of COPD. It
is aimed primarily at cost-effective prescribing, and will be reviewed annually as evidence is rapidly emerging in this field
Diagnosis
COPD is a common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow obstruction that is due to airway and/or alveolar
abnormalities. The disease is predominately caused by smoking but other environmental exposures may contribute.2, 3
3. Interpreting Spirometry
Quality assessment Is it airflow
obstruction? Severity assessment Make sure it isn’t asthma
3 blows with FEV1 values within 100ml of one another
FEV1/ FVC <0.7 FEV1
> 80% Mild = GOLD stage 1 Check reversibility to salbutamol (>200ml consider asthma).
Consider any other clinical signs or
symptoms of asthma.
50 - 80% Moderate= GOLD 2
FVC obtained after blowing out ≥ 6 seconds
30 - 50% Severe -= GOLD 3
< 30% Very Severe= GOLD 4
1. Consider COPD if: Any of the following indicators are present in an individual over 35 years old.
Dyspnoea that is - Progressive - Characteristically worse with exercise - Persistent.
Recurrent wheeze Chronic cough – may be intermittent, and/or unproductive Chronic sputum production
- any pattern of chronic sputum production may indicate COPD History of exposure to risk factors and host factors
- tobacco smoke/smoke from cooking and heating fuels occupational dusts and chemicals - family history of COPD and/or childhood factors
Recurrent lower respiratory tract infections
AND do not have clinical features of Asthma: Chronic unproductive cough Significantly variable breathlessness Night-time wakening with breathlessness and/or wheeze Significant diurnal or day-to-day variability of symptoms
The presence of multiple key indicators increases the probability of diagnosis of COPD.
2. Required tests: FBC Chest X-ray Spirometry (note, hand-held
spirometers MUST NOT be used for diagnosis but can be used for monitoring or screening)1.
Diagnosis of COPD if post bronchodilator
spirometry demonstrates: FEV
1/FVC <70%

South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 2
COPD Prescribing Guidelines
Possible Alternative Diagnosis
Asthma Congestive Heart Failure
Bronchiectasis Tuberculosis
Lung Cancer (Chest X Ray- If ≥ 3 week history of cough and /or increasing breathlessness)
Management of Stable COPD Re-assess historic diagnosis of COPD and make sure it was confirmed by spirometry
A patient’s needs change over time according to the progression of COPD, hence regularly review disease severity and effectiveness of current
regimen and accordingly modify the treatment 2
Monitor disease progression at least annually: FEV1, symptoms (mMRC & CAT), document exacerbations ( frequency, severity, type, likely cause, sputum
volume & purulence) and smoking status1
Check inhaler technique and compliance to treatment regimen regularly.
Encourage all patients to stop smoking - beneficial at all ages.
Offer annual influenza vaccinations and one-off pneumococcal vaccination.
Pulmonary rehabilitation improves symptoms, quality of life, physical and emotional state. Refer to pulmonary rehabilitation when mMRC score is
≥2 (or for GOLD classification B-D).
Promote use of individualised self-management plan and rescue packs. Template of self-management plan can be found on net.Formulary.
Screen for common comorbidities e.g. lung cancer (2-4 times more common), IHD, heart failure, arrhythmias, hypertension, CVA, peripheral
vascular disease, depression, anxiety, diabetes/metabolic syndrome, bronchiectasis, sleep apnoea, anaemia, osteoporosis, malnutrition/obesity,
GORD.2
Consider referral to local services as appropriate e.g. community respiratory team/consultant led respiratory clinic, physiotherapists, dietician
(follow current malnutrition guidelines if BMI/MUST score is low or high respectively), occupational therapy, social services, and palliative care
teams.
Where medication is initiated for persistent breathlessness, monitor and discontinue if no improvement.
Refer for oxygen assessment, following local pathways, when stable O2 saturations (not on exertion) are less than or equal to 92% breathing air.
A palliative care approach should be taken for end-of-life COPD patients. Main treatment goals should be symptom reduction and management of future risk of exacerbations. Referral to palliative care teams should be considered.
South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 3
COPD Prescribing Guidelines
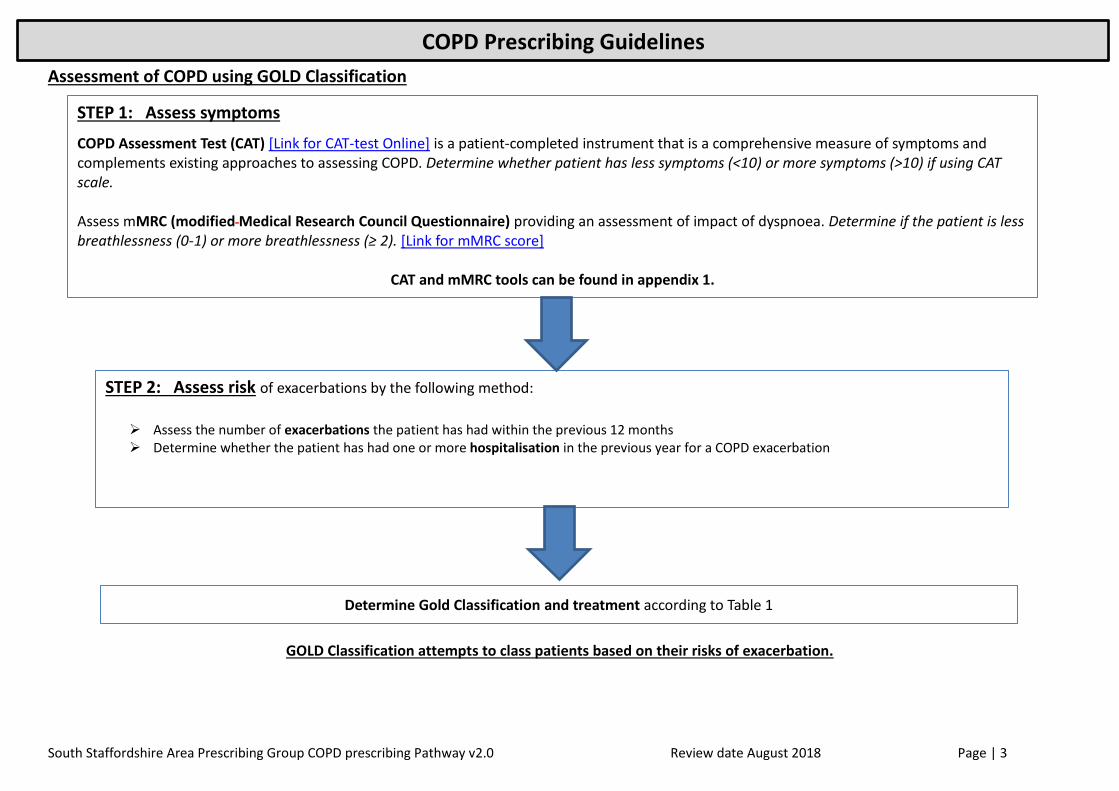
Assessment of COPD using GOLD Classification
GOLD Classification attempts to class patients based on their risks of exacerbation.
STEP 1: Assess symptoms
COPD Assessment Test (CAT) [Link for CAT-test Online] is a patient-completed instrument that is a comprehensive measure of symptoms and complements existing approaches to assessing COPD. Determine whether patient has less symptoms (<10) or more symptoms (>10) if using CAT scale. Assess mMRC (modified Medical Research Council Questionnaire) providing an assessment of impact of dyspnoea. Determine if the patient is less breathlessness (0-1) or more breathlessness (≥ 2). [Link for mMRC score]
CAT and mMRC tools can be found in appendix 1.
STEP 2: Assess risk of exacerbations by the following method:
Assess the number of exacerbations the patient has had within the previous 12 months Determine whether the patient has had one or more hospitalisation in the previous year for a COPD exacerbation
Determine Gold Classification and treatment according to Table 1
South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 4
COPD Prescribing Guidelines
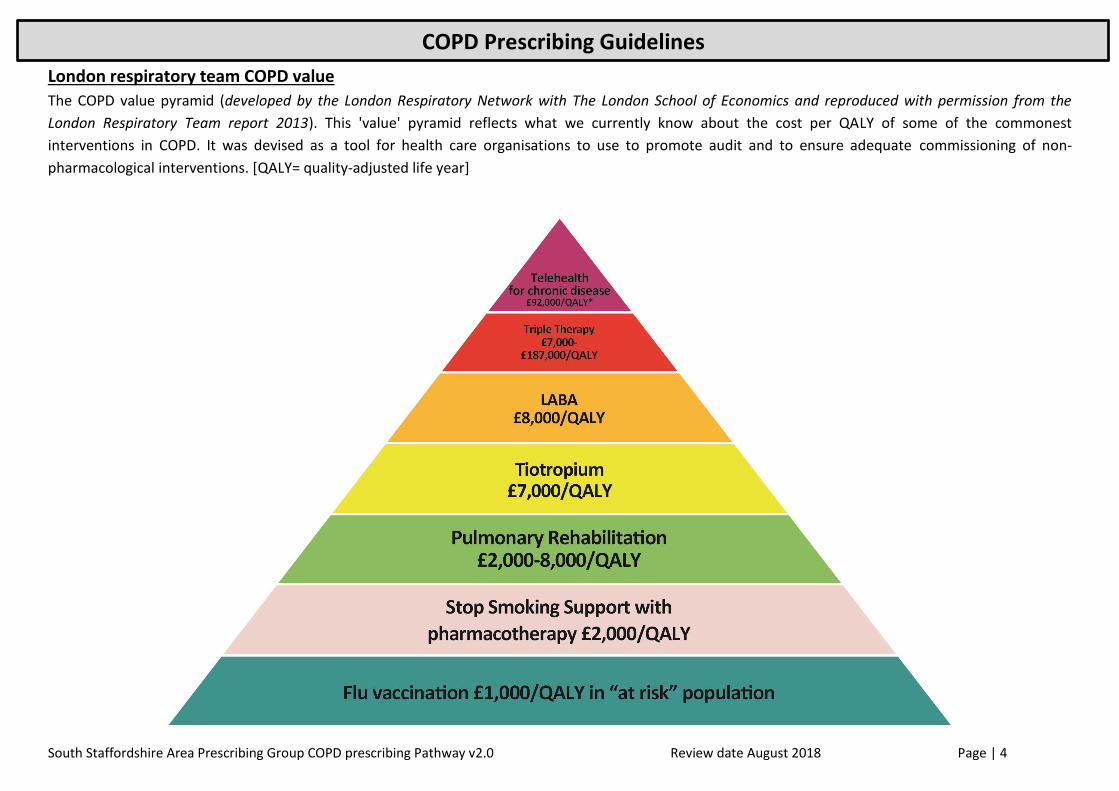
London respiratory team COPD value
The COPD value pyramid (developed by the London Respiratory Network with The London School of Economics and reproduced with permission from the
London Respiratory Team report 2013). This 'value' pyramid reflects what we currently know about the cost per QALY of some of the commonest
interventions in COPD. It was devised as a tool for health care organisations to use to promote audit and to ensure adequate commissioning of non-
pharmacological interventions. [QALY= quality-adjusted life year]

South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 5
COPD Prescribing Guidelines
Table 1: Gold Classification & Respective Drug Treatment –
Patients can start in any classification and can migrate between groups, therefore regular assessment is essential
Short-acting beta-agonist bronchodilators should continue as required for all patients.
(See Appendix 2 – for in list of inhaler brands, dosing, costs & images)
Symptom Assessment (Use highest result to guide classification)
Ris
k A
sse
ssm
en
t
Exacerbation history CAT <10 CAT ≥10
mMRC 0-1 mMRC ≥2
≥ 2 OR
≥1 leading to a hospital admission
Group C
LAMA
If further exacerbations: LAMA + LABA
(alternative option: LAMA + ICS)
Group D
LAMA + LABA
If further exacerbations: LAMA + LABA + ICS
(alternative 2nd line option: LABA + ICS)
If further exacerbations with LAMA/LABA/ICS seek specialist opinion.
0 OR 1 (not leading to
hospital admission)
Group A
Bronchodilator (SAMA or LAMA)
Evaluate effect: continue, stop or try alternative class of bronchodilator
Group B
A long-acting bronchodilator
(LABA or LAMA)
If persistent symptoms: LAMA + LABA
Inhaler choices for management of stable patients – try to maintain device consistency if possible
Inhaler type LABA LAMA LABA/LAMA LABA/ICS
MDI Formoterol Easyhaler 12mcg Fostair MDI 6/100mcg
Breezhaler Onbrez Breezhaler 150mcg Seebri Breezhaler 44mcg Ultibro Breezhaler 85/43mcg
Respimat Sprivia Respimat 2.5mcg Spiolto Respimat 2.5/2.5mcg
Ellipta Incruse Ellipta 55mcg Anoro Ellipta 22/55mcg Relvar Ellipta 22/92mcg
Genuair Eklira Genuair 322mcg Duaklir Genuair 12/340mcg
Other DPI Fostair NEXThaler 6/100mcg
DuoResp Spiromax 9/320mcg

South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 6
COPD Prescribing Guidelines
Treatment algorithms according to GOLD ABCD grade 2
Notes:
1. Trial of Roflumilast & Macrolide should only be initiated by respiratory specialist. Roflumilast is now recommended by NICE however locally
prescribing should remain within secondary care.
2. Theophylline may be considered to be used as an additional bronchodilator and it needs to monitored as per the BNF.

South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 7
COPD Prescribing Guidelines
Managing COPD Exacerbations
Considerations: (circle as appropriate) Favours specialist treatment Favours treatment at home
Able to cope at home: No Yes
Breathlessness: Severe Mild
General condition: Poor / deteriorating Good
Level of activity: Poor / confined to bed Good
Cyanosis: Yes No
Worsening Peripheral Oedema: Yes No
Level of consciousness: Impaired Normal
LTOT currently received: Yes No
Social circumstances: Living alone / not coping Good
Acute confusion: Yes No
Rapid rate of onset: Yes No
Significant morbidity: Yes No
SaO2 <90%: Yes No
Decide where to treat: Hospital Home
Referral to community respiratory clinic/secondary care should be considered for:
Diagnostic uncertainty
Uncontrolled COPD
Patient wants a second opinion
Bullous lung disease
Assessment for pulmonary rehabilitation or lung transplantation
Dysfunctional breathing
Onset of symptoms under 40 years or a family history of alpha 1-
antitrypsin deficiency
Assessment for oxygen therapy, long-term nebuliser therapy or oral
corticosteroid therapy
Onset of cor pulmonale
Symptoms disproportionate to lung function deficit
Frequent infections
Haemoptysis (2 week wait)
Rapid decline in FEV1
South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 8
COPD Prescribing Guidelines
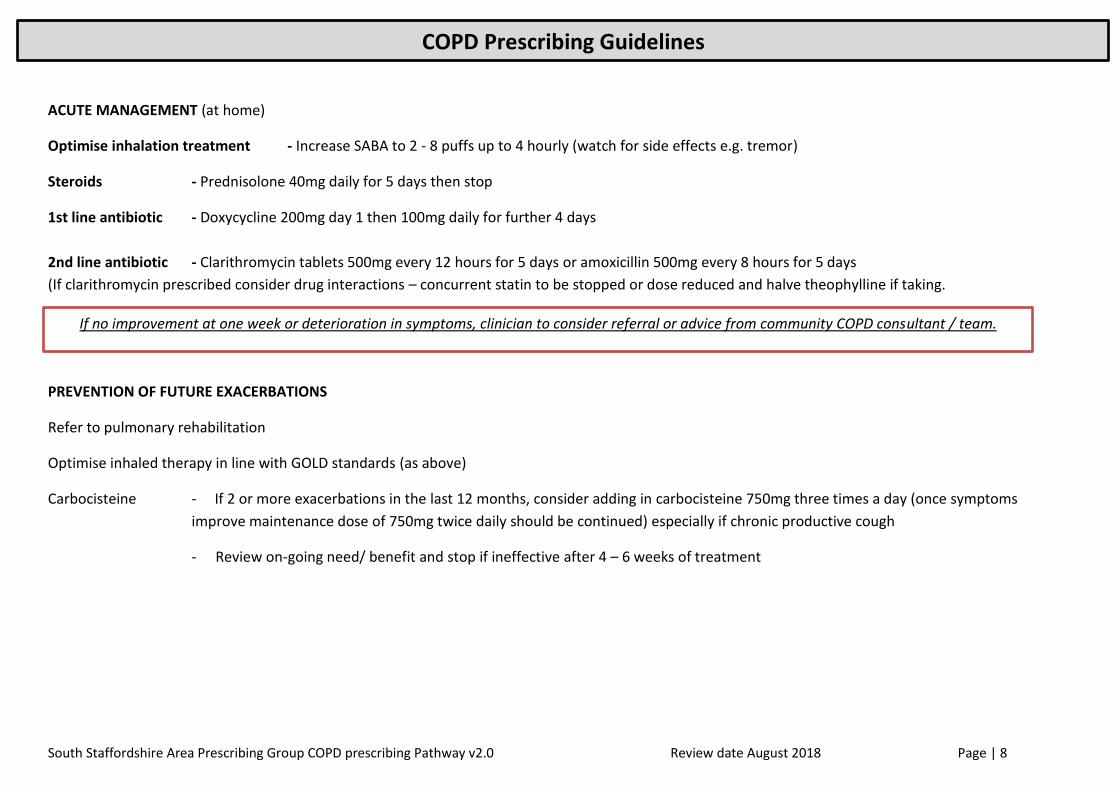
ACUTE MANAGEMENT (at home)
Optimise inhalation treatment - Increase SABA to 2 - 8 puffs up to 4 hourly (watch for side effects e.g. tremor)
Steroids - Prednisolone 40mg daily for 5 days then stop
1st line antibiotic - Doxycycline 200mg day 1 then 100mg daily for further 4 days
2nd line antibiotic - Clarithromycin tablets 500mg every 12 hours for 5 days or amoxicillin 500mg every 8 hours for 5 days
(If clarithromycin prescribed consider drug interactions – concurrent statin to be stopped or dose reduced and halve theophylline if taking.
PREVENTION OF FUTURE EXACERBATIONS
Refer to pulmonary rehabilitation
Optimise inhaled therapy in line with GOLD standards (as above)
Carbocisteine - If 2 or more exacerbations in the last 12 months, consider adding in carbocisteine 750mg three times a day (once symptoms
improve maintenance dose of 750mg twice daily should be continued) especially if chronic productive cough
- Review on-going need/ benefit and stop if ineffective after 4 – 6 weeks of treatment
If no improvement at one week or deterioration in symptoms, clinician to consider referral or advice from community COPD consultant / team.

South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 9
COPD Prescribing Guidelines
References:
1. Rytila P, Helin T, Kinnula V. The use of microspirometry in detecting lowered FEV1 values in current or former cigarette smokers. Primary Care Respiratory Journal
2008. 17(4): 232–7
2. From the Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017. Available
from: http://www.goldcopd.org/ <Accessed on 19.03.2017>
3. NICE 2010 COPD guidelines
4. IMPRESS Guide to the relative value of COPD interventions July 2012
5. www.medicines.org.uk – all drug files accessed
6. British National Formulary, BMA March 2014 https://www.medicinescomplete.com/mc/bnf/current/ <Accessed 20.03.2017>
7. Chemist and Druggist March 2017 http://www.medicines.org.uk/emc/ <Accessed 20.03.2017>
ACKNOWLEDGEMENTS TO ALICE TURNER AND PAN BIRMINGHAM APC
South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 10
COPD Prescribing Guidelines
Appendices
Appendix 1 –
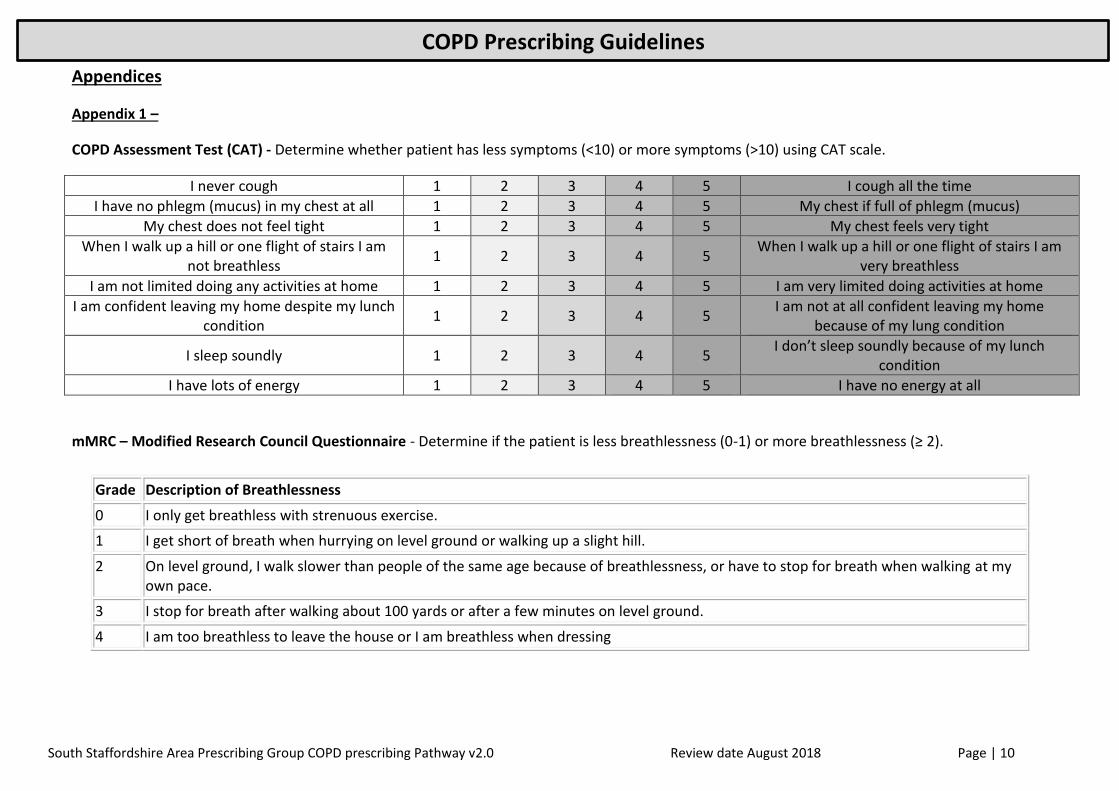
COPD Assessment Test (CAT) - Determine whether patient has less symptoms (<10) or more symptoms (>10) using CAT scale.
I never cough 1 2 3 4 5 I cough all the time
I have no phlegm (mucus) in my chest at all 1 2 3 4 5 My chest if full of phlegm (mucus)
My chest does not feel tight 1 2 3 4 5 My chest feels very tight
When I walk up a hill or one flight of stairs I am not breathless
1 2 3 4 5 When I walk up a hill or one flight of stairs I am
very breathless
I am not limited doing any activities at home 1 2 3 4 5 I am very limited doing activities at home
I am confident leaving my home despite my lunch condition
1 2 3 4 5 I am not at all confident leaving my home
because of my lung condition
I sleep soundly 1 2 3 4 5 I don’t sleep soundly because of my lunch
condition
I have lots of energy 1 2 3 4 5 I have no energy at all
mMRC – Modified Research Council Questionnaire - Determine if the patient is less breathlessness (0-1) or more breathlessness (≥ 2).
Grade Description of Breathlessness
0 I only get breathless with strenuous exercise.
1 I get short of breath when hurrying on level ground or walking up a slight hill.
2 On level ground, I walk slower than people of the same age because of breathlessness, or have to stop for breath when walking at my own pace.
3 I stop for breath after walking about 100 yards or after a few minutes on level ground.
4 I am too breathless to leave the house or I am breathless when dressing
South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 11
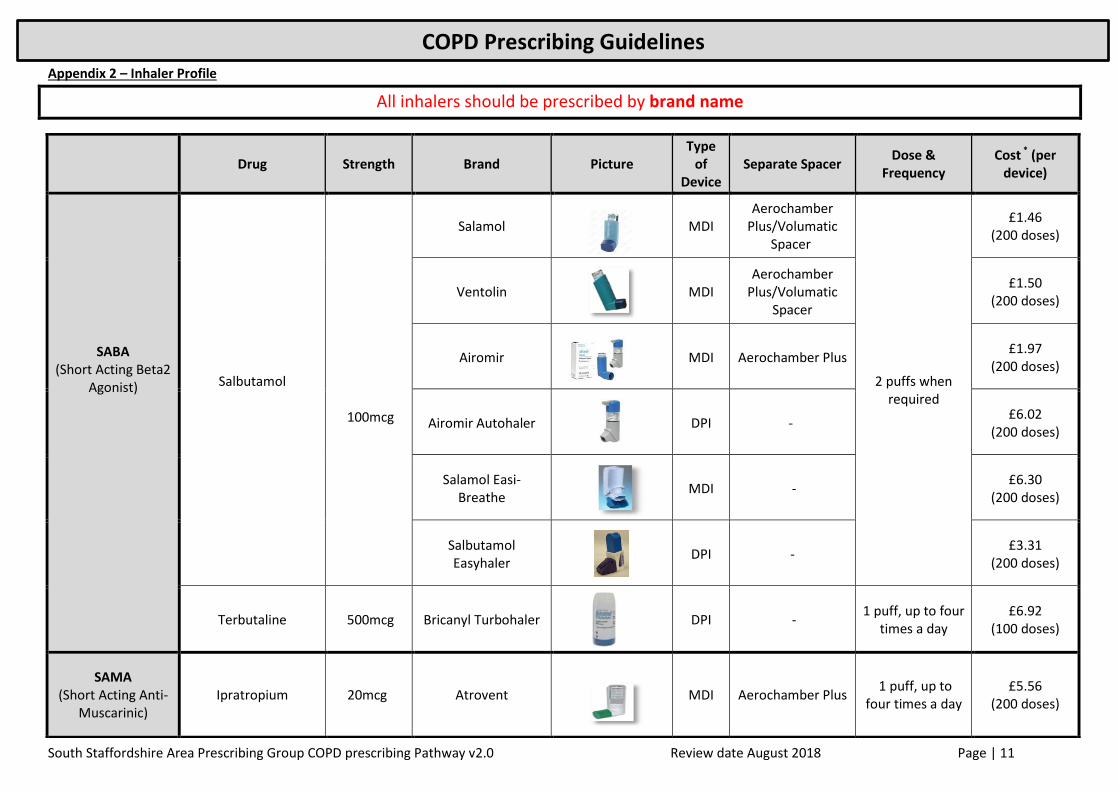
COPD Prescribing Guidelines Appendix 2 – Inhaler Profile
All inhalers should be prescribed by brand name
Drug Strength Brand Picture Type
of Device
Separate Spacer Dose &
Frequency Cost * (per
device)
SABA (Short Acting Beta2
Agonist)
Salbutamol
100mcg
Salamol
MDI Aerochamber
Plus/Volumatic Spacer
2 puffs when required
£1.46 (200 doses)
Ventolin
MDI Aerochamber
Plus/Volumatic Spacer
£1.50 (200 doses)
Airomir
MDI Aerochamber Plus £1.97
(200 doses)
Airomir Autohaler
DPI - £6.02
(200 doses)
Salamol Easi-Breathe
MDI - £6.30
(200 doses)
Salbutamol Easyhaler
DPI - £3.31
(200 doses)
Terbutaline 500mcg Bricanyl Turbohaler
DPI - 1 puff, up to four
times a day £6.92
(100 doses)
SAMA (Short Acting Anti-
Muscarinic) Ipratropium 20mcg Atrovent
MDI Aerochamber Plus 1 puff, up to
four times a day £5.56
(200 doses)

South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 12
COPD Prescribing Guidelines
LABA (Long Acting Beta2
Agonist)
Formoterol 12mcg Easyhaler
Formoterol
DPI - 1 puff Twice
daily
£23.75 (120 doses)
Note: device will last two
months
Indacaterol 150mcg Onbrez Breezhaler &
Caps
DPI - 1 puff Once daily £32.19
(30 doses)
LAMA (Long Acting Anti-
Muscarinic)
Note: inhaler strengths given.
Base drug strengths may be slightly different.
Glycopyrronium 44mcg Seebri Breezhaler &
Caps
DPI - 1 puff Once daily £27.50
(30 doses)
Tiotropium 2.5mcg Sprivia Respimat
DPI - 2 puffs Once
daily £23.00
(60 doses)
Umeclidinium 55mcg Incruse Ellipta
DPI - 1 puff Once daily £27.50
(30 doses)
Aclidinium 322mcg Eklira Genuair
DPI - 1 puff Twice
daily £28.60
(60 doses)
LABA/LAMA combination (Long Acting
Antimuscarinic & Long Acting Beta2
Agonist)
Note: inhaler strengths given.
Base drug strengths may be slightly different.
Vilanterol/ Umeclidinium
22mcg / 55mcg
Anoro Ellipta
DPI - 1 puff Once daily £32.50
(30 doses)
Indacaterol/ Glycopyrronium
85mcg/ 43mcg
Ultibro Breezhaler & Caps
DPI - 1 puff Once daily £32.50
(30 doses)
Olodaterol/ tiotropium
2.5mcg/ 2.5mcg
Spiolto Respimat
DPI - 2 puffs Once
daily £32.50
(60 doses)
Formoterol/ Aclidinium
12mcg/ 340mcg
Duaklir Genuair
DPI - 1 puff Twice
daily £32.50
(60 doses)
South Staffordshire Area Prescribing Group COPD prescribing Pathway v2.0 Review date August 2018 Page | 13
COPD Prescribing Guidelines
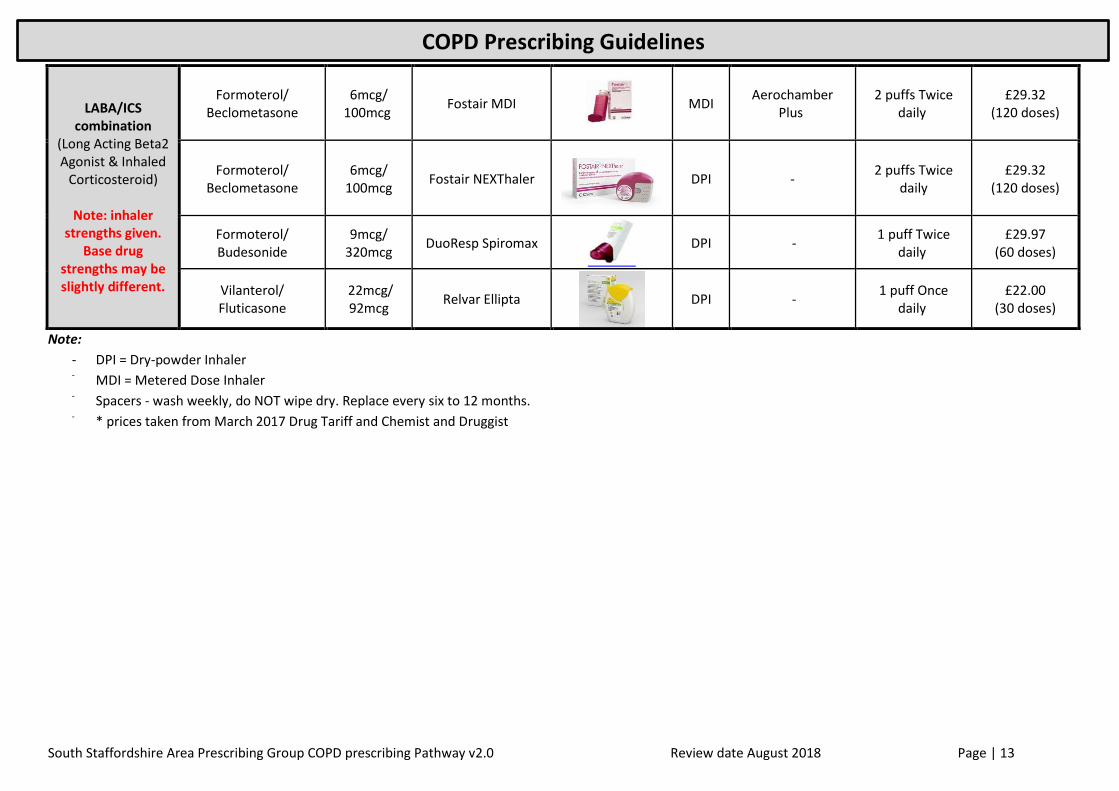
Note:
- DPI = Dry-powder Inhaler - MDI = Metered Dose Inhaler
- Spacers - wash weekly, do NOT wipe dry. Replace every six to 12 months.
- * prices taken from March 2017 Drug Tariff and Chemist and Druggist
LABA/ICS combination
(Long Acting Beta2 Agonist & Inhaled
Corticosteroid)
Note: inhaler strengths given.
Base drug strengths may be slightly different.
Formoterol/ Beclometasone
6mcg/ 100mcg
Fostair MDI
MDI Aerochamber
Plus 2 puffs Twice
daily £29.32
(120 doses)
Formoterol/ Beclometasone
6mcg/ 100mcg
Fostair NEXThaler
DPI - 2 puffs Twice
daily £29.32
(120 doses)
Formoterol/ Budesonide
9mcg/ 320mcg
DuoResp Spiromax
DPI - 1 puff Twice
daily £29.97
(60 doses)
Vilanterol/ Fluticasone
22mcg/ 92mcg
Relvar Ellipta
DPI - 1 puff Once
daily £22.00
(30 doses)