convolution and model- based dosecalculation methods in
TRANSCRIPT
Radiotherapy is an established treatment modality of cancer where radiation is delivered to the patients from internal or external sources. This thesis explores and introduces improvements to computational methods that are used in the application of internal and external radiotherapy. The summary discusses radiotherapy planning and reviews model-based dose calculation methods in internal and external radiotherapy. Treatment planning methods of internal radionuclide therapy are devloped and applied to analyze radionuclide therapy cases. The thesis also reports on the development of a pencil-beam dose kernel -based calculation method for external photon therapy that also accounts for local variations in tissue material densities in 3D space.
Aalto-D
D 57
/2016
9HSTFMG*aghchi+
ISBN 978-952-60-6727-8 (printed) ISBN 978-952-60-6728-5 (pdf) ISSN-L 1799-4934 ISSN 1799-4934 (printed) ISSN 1799-4942 (pdf) Aalto University School of Science Department of Neuroscience and Biomedical Engineering www.aalto.fi
BUSINESS + ECONOMY ART + DESIGN + ARCHITECTURE SCIENCE + TECHNOLOGY CROSSOVER DOCTORAL DISSERTATIONS
Joakim P
yyry C
onvolution and model-based dose calculation m
ethods in radionuclide and external-beam photon therapy
Aalto
Unive
rsity
2016
Department of Neuroscience and Biomedical Engineering
Convolution and model-based dose calculation methods in radionuclide and external-beam photon therapy
Joakim Pyyry
DOCTORAL DISSERTATIONS







Preface
This project started twenty years ago in the spring of 1996, when my
Thesis advisors Kalevi Kairemo and Mikko Tenhunen recognized a need
to improve treatment planning for radionuclide therapy. At the time, I
was developing a treatment planning system for brachytherapy, and we
started to extend the system to include radionuclide dose calculations. I
am greatly indebted to my advisors for their support, creativity, and drive
that pushed me to move this project forward. I also want express my
gratitude to the patients presented in the case studies and the clinical
staff involved in the patient care and data acquisition.
During my doctoral studies, I have been employed by Varian Medical
Systems Finland Oy (formerly Varian-Dosetek Oy) working in radiother-
apy research and development projects. I want to thank all my colleagues
at Varian for the motivating and inspiring work environment where fight-
ing against cancer is our common goal. Pekka Aalto created a world-class
treatment planning research and development center at Dosetek in Fin-
land, and supported me in many ways during the years. I am grateful to
Ramin Baghaie for the support and encouragement that he gave me to
finalize my doctoral studies, and for his perceptive review and comments
on the manuscript.
I want to thank all the co-authors of the publications and my other
collaborators. Jyrki Alakuijala has been an outstanding mentor induct-
ing me to the process of scientific publication, as well as to the world
of professional software development. The AAA method would not ex-
ist without Waldemar Ulmer’s and Wolfgang Kaissl’s early investigations
and Hannu Helminen’s key contributions during the first implementa-
tion. Since then, numerous people have contributed to the success of the
AAA and its improvements: particularly the members of the VMS Fin-
land Applied Research Department and the large user base of medical
1

Preface
physicists around the world.
At Aalto University, my sincere thanks go to Professor Toivo Katila,
who guided me during the start of my doctoral studies, and to Professor
Lauri Parkkonen who took over the supervision during the final stretch of
my studies. I am grateful to the official pre-examiners, Professor Dietmar
Georg and Dr. Mark Lubberink, for their insightful comments and appro-
priate suggestions. I want to express my gratitude to Raine Vasquez for
his critical language review.
The encouragement and care from my parents Helena and Jorma has
enabled my education and other endeavors in life. Thank you. Olavi and
Ansa, you fill me with joy and keep me energized with your speed of move-
ment and creativity. Finally Noora: without your love, companionship, ex-
emplary passion for scientific writing and encouragement to finalize this
undertaking, it would have taken me yet another twenty years.
Helsinki, March 22, 2016,
Joakim Pyyry
2
Contents
Preface 1
Contents 3
List of Publications 5
Author’s Contribution 7
1. Introduction 11
1.1 Principles of radiotherapy . . . . . . . . . . . . . . . . . . . . 12
1.2 Brachytherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
1.3 Radionuclide therapy . . . . . . . . . . . . . . . . . . . . . . . 12
1.4 External-beam radiotherapy . . . . . . . . . . . . . . . . . . . 13
1.5 Radiation physics of photons and electrons . . . . . . . . . . 14
1.6 Radiation transport and absorbed dose calculations . . . . . 15
1.7 Aims of the Thesis . . . . . . . . . . . . . . . . . . . . . . . . . 17
2. Radiotherapy treatment planning and sources of radiation 19
2.1 Dose calculation in radionuclide therapy . . . . . . . . . . . . 19
2.2 Distribution of activity in radionuclide therapy . . . . . . . . 21
2.3 Treatment machine modeling . . . . . . . . . . . . . . . . . . 23
3. Model-based convolution and superposition methods in ab-
sorbed dose calculation 25
3.1 Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
3.2 Point-spread and kernel methods . . . . . . . . . . . . . . . . 26
3.2.1 Brachytherapy . . . . . . . . . . . . . . . . . . . . . . . 26
3.2.2 Radionuclide therapy . . . . . . . . . . . . . . . . . . . 27
3.2.3 3D kernel methods in external-beam therapy . . . . . 27
3.3 Pencil-beam methods . . . . . . . . . . . . . . . . . . . . . . . 28
3

Contents
3.3.1 Exponential modeling of pencil beams . . . . . . . . . 29
3.3.2 Superposition of pencil beams . . . . . . . . . . . . . . 29
3.3.3 Build-up and build-down correction . . . . . . . . . . 30
3.4 Computational considerations . . . . . . . . . . . . . . . . . . 31
3.4.1 Performance characteristics . . . . . . . . . . . . . . . 31
3.4.2 Parallel computing . . . . . . . . . . . . . . . . . . . . 32
4. Summary of results 35
4.1 Patient-specific distributions in radionuclide therapy . . . . 35
4.2 A pencil beam superposition algorithm in external radio-
therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
5. Discussion and conclusions 41
5.1 Overall results . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
5.2 Contribution to the field . . . . . . . . . . . . . . . . . . . . . 42
5.3 Future directions . . . . . . . . . . . . . . . . . . . . . . . . . 43
5.4 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Errata 57
Publications 59
4

List of Publications
This thesis consists of an overview and of the following publications which
are referred to in the text by their Roman numerals.
I J. Laitinen, J. Alakuijala, H. Helminen, S. Sallinen, M. Tenhunen, and
K. Kairemo. Spect-based radioimmunotherapy planning system. In
IEEE Engineering in Medicine and Biology 19th Annual Conference,
Chicago, 781–784, 1997.
II J.O. Laitinen, K.J. Kairemo, A.P. Jekunen, T. Korppi-Tommola, and M.
Tenhunen. The effect of three dimensional activity distribution on the
dose planning of radioimmunotherapy for patients with advanced in-
traperitoneal pseudomyxoma. Cancer 80, 2545–2552, 1997.
III J.O. Laitinen, M. Tenhunen, and K.J. Kairemo. Absorbed dose esti-
mates for I-131 labelled monoclonal antibody therapy in patients with
intraperitoneal pseudomyxoma. Nucl Med Commun 21, 355–360, 2000.
IV J.O. Pyyry, J. Merenmies, M. Tenhunen, M. Heikinheimo, K. Parto,
M. Arola,K. Rönnholm, H. Isoniemi, R. Karikoski, E.L. Kamarainen,
M. Seppänen,J. Heikkonen, F. Augensen, W.H. Wegener, D.M. Golden-
berg, and K.J. Kairemo . Radioimmunotherapy for recurrent childhood
hepatoblastoma after liver transplantation. World Journal of Nuclear
Medicine 7, 146–157, 2008.
V W. Ulmer, J. Pyyry, and W. Kaissl. A 3D photon superposition/convolution
algorithm and its foundation on results of Monte Carlo calculations.
5

List of Publications
Physics in Medicine and Biology 50, 1767–1790, 2005.
VI L. Tillikainen, H. Helminen, T. Torsti, S. Siljamäki, J. Alakuijala, J.
Pyyry, and W. Ulmer. A 3D pencil-beam-based superposition algorithm
for photon dose calculation in heterogeneous media. Physics in Medicine
and Biology 53, 3821–3839, 2008.
6

Author’s Contribution
Publication I: “Spect-based radioimmunotherapy planning system”
The author (J. Laitinen) implemented the dose-kernel-based dose calcula-
tion algorithm and dose visualization system and integrated the methods
into an existing brachytherapy treatment planning system. The author
was solely responsible of the production of the manuscript.
Publication II: “The effect of three dimensional activity distributionon the dose planning of radioimmunotherapy for patients withadvanced intraperitoneal pseudomyxoma”
The author (J. Laitinen) developed and utilized a radiotherapy planning
system to register images and calculate doses. The author analyzed the
results and was primarily responsible of the writing and revision of manuscript.
Publication III: “Absorbed dose estimates for I-131 labelledmonoclonal antibody therapy in patients with intraperitonealpseudomyxoma”
The author (J. Laitinen) utilized the developed radiotherapy planning sys-
tem and MIRD methodology to analyze radiation doses in patients receiv-
ing radioimmunotherapy. The author was primarily responsible of the
production of the manuscript.
7

Author’s Contribution
Publication IV: “Radioimmunotherapy for recurrent childhoodhepatoblastoma after liver transplantation”
The author constructed the dose kernels for In-111 and Y-90 and analyzed
the radiation doses utilizing the developed software employing automatic
image registration and point-dose-kernel dose calculation. The author
was jointly responsible for the production of the manuscript contributing
to the absorbed dose calculation section and to the methods related to dose
calculations and image registration.
Publication V: “A 3D photon superposition/convolution algorithmand its foundation on results of Monte Carlo calculations”
The author participated in developing the methods and verification of the
implementation of the methods. The author analyzed the radiation doses
utilizing the developed software and co-ordinated experimental verifica-
tion of the methods. The author assisted in the production and review of
the manuscript.
Publication VI: “A 3D pencil-beam-based superposition algorithmfor photon dose calculation in heterogeneous media”
The author participated in developing the methods related to the expo-
nential basis functions and scaling for tissue heterogeneities. The au-
thor had a minor role in assisting in the production and review of the
manuscript. This article was also part of the PhD thesis of Tillikainen
(2009).
8

Abbreviations and Symbols
A Activity distribution
e Electron radiation
E Energy
Φ Angular fluence
γ Photon radiation
h Pencil-beam dose kernel
k Point-dose kernel
λ Distance from the central axis
~p Spatial position co-ordinate (px, py, pz)
µ Attenuation co-efficient
N Number of elements
Ω Direction
~r Spatial position
ρ Density
σ Total cross section
SR Radiative stopping power
T TERMA — Total energy released in the material
3D Three dimensional
AAA Analytical anisotropic algorithm
CAX Central axis
9

Abbreviations and Symbols
CCC Collapsed cone convolution
CPU Central processing unit (of a computer)
CT Computed tomography
FFT (Discrete) fast Fourier transform
GPU Graphics processing unit
IMRT Intensity modulated radiotherapy
ICRU International commission on radiation units and measurements
MIRD Committee on medical internal radiation dose
MC Monte Carlo
MoAb Monoclonal antibody
MR Magnetic resonance
MSM Multiple source models
OLINDA Organ level internal dose assessment
PB Pencil beam
PET Positron emission tomography
QA Quality assurance
SBRT Stereotactic body radiation therapy
SC Superposition/convolution
S-factor Specific absorbed dose factor in MIRD methodology
SPECT Single-photon emission computed tomography
TERMA Total energy released in the material
TPS Treatment planning system
VMAT Volumetric modulated arc therapy
VOI Volume of interest
10

1. Introduction
Cancer is a malignant disease which is among the leading causes of mor-
tality in the world, with approximately 14 million new cases annually in
2012 leading to 8.2 million deaths, according to World Health Organiza-
tion. Cancer incidences rise with aging of the population, and it is esti-
mated that there will be 70% more cancer cases within next two decades.
(WHO 2015)
Cancer is a generic term for a group of diseases. The defining feature
of cancer is the rapid growth of abnormal cells that spread to other organs
by invading adjoining parts of the body or through circulation referred to
as metastasizing. Metastases cause the majority of deaths from cancer.
Every cancer type requires a tailored approach to treatment. Treat-
ment regimens include multiple modalities: surgery, radiotherapy, and
chemotherapy. The different modalities are often used in combination.
The goal of the treatment is to cure cancer or to prolong life, in addition to
improving the patient’s quality of life. Radiotherapy is a key component
of comprehensive cancer care, but worldwide access to it is low. As Atun
et al. (2015) point out there are considerable benefits to further develop
radiotherapy and scale it up worldwide.
This Thesis explores and introduces improvements to computational
methods that are used in the application of radiotherapy. These meth-
ods are routinely used in clinical radiotherapy practice and fall under the
domain of computational physics. The methods are very relevant as they
provide an optimal balance of accuracy and speed in the everyday practice
of radiotherapy.
11

Introduction
1.1 Principles of radiotherapy
Radiotherapy refers to the utilization of ionizing radiation for a therapeu-
tic effect, typically for cancer treatment; for a comprehensive overview of
the subject see e.g. Halperin et al. (2008). Radiation is delivered either ex-
ternally, from outside the body, or internally. Internal therapy is further
divided to brachytherapy and radionuclide therapy. In brachytherapy, a
radioactive source is placed in or near the tumor; in radionuclide therapy,
the radioactive isotopes are delivered systemically inside the body.
Ionizing radiation causes damage in cells, with increased damage by
the amount of energy deposited by the ionizing radiation in the tissue.
Both normal tissue and cancer cells are affected but exhibit different cell-
survival probability for the same radiation dose level. Many cancer cells
are more sensitive to radiation than healthy tissue due to the reduced
efficacy of the biochemical repair processes of the damaged cell nuclei un-
dergoing reproduction (due to the growth of the cancer). In addition, the
ability to focus the radiation for a higher dose in the tumor compared to
normal tissue allows for improved therapeutic ratio.
1.2 Brachytherapy
Brachytherapy is a form of radiotherapy where sealed radioactive sources
are placed in the vicinity of the treated tumor. Typically it is applied
internally via cavities or interstitially with needles. It is oldest form of
radiotherapy as it was first applied in 1901 shortly after the discovery of
radioactivity. Low dose rate delivery typically can involve permanent im-
plants of sealed sources or temporary application of radioactive sources
for several hours. Shorter high dose rate treatments are typically per-
formed with afterloading devices where the radioactive source is moved
in and out off the treatment region using remote control.
1.3 Radionuclide therapy
Radionuclide therapy is an internal radiotherapy technique which relies
on certain biological mechanisms to provide a higher concentration of ra-
dionuclides in the vicinity of cancerous cells in order to produce a higher
radiation dose. Often radionuclide therapy relies on radiolabeled car-
riers like liposomes, antibodies, or nano-particles to localize in tumors
12

Introduction
(Williams et al. 2008). The radionuclides are administered systemically
via circulation, or into cavities.
The radionuclides that are useful for therapy undergo three modes of
decay: beta, alpha, and electron capture or isomeric transition by emis-
sion of Auger and Coster-Kronig electrons. Selection criteria, in addition
to the mode of decay, include energy of released particles, chemical prop-
erties, production methods, as well as biological behavior (Zweit 1996).
Similarly to other modes of radiotherapy — knowledge of the absorbed
radiation dose is needed to assess the toxicity and efficacy of radionuclide
therapy. The absorbed dose is a macroscopic concept, but for radionuclide
therapy microdosimetry — study of radiation energy deposition in micro-
scopic volumes — may be indicated for low-energy auger-emitters (Humm
et al. 1993). The notion of biological effective dose has been introduced to
take into account the biological effects various dose rates and different
types of radiation. The aspects of radiobiology can be utilized in radionu-
clide therapy in order to estimate the best dose for tumor control, while
protecting the healthy tissues (Pouget et al. 2015).
1.4 External-beam radiotherapy
External-beam radiotherapy is a mode of radiation treatment where the
radiation originates from sources externalto the body. The radiation types
used are photons, electrons, or heavier charged particles. The most com-
mon is photon therapy using megavoltage brehmsstrahlung x-rays gener-
ated by linear electron accelerators. Photon beams can also be generated
with a radioactive source such as cobalt-60. Charged-particle therapy has
its own role in cancer management but is not discussed in the Thesis.
The external beam is directed from outside the body to the site of the
treatment target (tumor). In order to ensure a conformal and high radi-
ation dose inside the target, the radiation needs to be focused from mul-
tiple directions to the common target. The beam intensity and shape are
typically produced by a computer-controlled multi-leaf collimation device
integral to the treatment delivery system.
13

Introduction
1.5 Radiation physics of photons and electrons
Photon radiation interacts with matter and deposits energy via complex
interaction cascades. When photons interact with material, the primary
photon is absorbed in the interaction. A secondary photon is re-emitted in
a scattering (coherent or incoherent) interaction. The scattering process is
similar to a change in the direction and energy of the photon; this change
occurs through absorption and emission of photons. In the process, elec-
trons are also ejected from the interacting atoms or they are created as
electron — positron pairs. The main interactions of photons with atoms
are called photoelectric absorption, Rayleigh (coherent) scattering, Comp-
ton (incoherent) scattering, and electron — positron pair production. The
relative importance of various interactions varies with photon energy and
the medium. The total mass attenuation coeffiecients have been tabu-
lated extensively by Hubbell and Seltzer (1996) and Figure 1.1 shows an
example of photon attenuation factors as function energy.
Figure 1.1. Photon attenuation is plotted separately for each interaction type with the to-tal mass attenuation factor as a function of energy in iron medium (Tuszynski2010).
In photon radiotherapy, electrons are generated in the interactions of
the photons with matter. These electrons interact intensively with mat-
ter. Electrons interacting with the orbital electrons of the atoms create
secondary electrons and lose part of their initial energy. Photons are cre-
ated when the electrons interact with the Coloumb field of the nucleus
of the atom in a process called brehmsstrahlung. The electromagnetic
interactions couple the electrons and photons into a combined shower of
particles which makes the modeling of the phenomenon complicated.
14

Introduction
1.6 Radiation transport and absorbed dose calculations
The radiation transport problem can be described as a linear differential
equation that takes the form of the Boltzmann transport equation origi-
nally formulated by Ludwig Boltzmann to describe the statistical behav-
ior of a thermodynamic system not in a thermodynamic equilibrium. The
transport equation can be solved by numerical grid-based methods, as has
been demonstrated in the radiotherapy domain by several groups (Kotilu-
oto et al. 2007; Vassiliev et al. 2010). However, the historically more im-
portant method in the field of radiotherapy has been the stochastic Monte
Carlo (MC) solution to the Boltzmann transport equation (Andreo 1991;
Rogers 2006). There have been several practical implementations where
speed and accuracy have been optimized for routine clinical use (Neuen-
schwander et al. 1995; Fippel et al. 1997; Fippel et al. 1999; Kawrakow
and Fippel 2000; Fix et al. 2010).
The Boltzmann equation for transport of photons (γ) can be written as
Ω · ~∇Φγ + σγt Φγ = qγ + qγγ (1.1)
and for electrons (e) the Boltzmann-Fokker-Planck transport equation as
Ω · ~∇Φe + σetΦe − ∂
∂E(SRΦe) = qe + qee + qγe (1.2)
where Φ(~r,E, Ω) describes the angular fluence for photons and electrons
and is a function of spatial position (~r), energy (E) and direction (Ω).
The macroscopic total cross sections for photons is σγt and for electrons
σet . SR(~r,E) is the combined restricted collisional and radiative stopping
power. The scattering source terms can be written in the integral form as
qγγ(~r,E, Ω) =
∫ ∞
0dE′
∫
4π
σγγt (~r,E′ → E, Ω · Ω′)Φ(~r,E, Ω)dΩ′ (1.3)
qγe(~r,E, Ω) =
∫ ∞
0dE′
∫
4π
σγet (~r,E′ → E, Ω · Ω′)Φ(~r,E, Ω)dΩ′ (1.4)
qee(~r,E, Ω) =
∫ ∞
0dE′
∫
4π
σeet (~r,E′ → E, Ω · Ω′)e(~r,E, Ω)dΩ′, (1.5)
where qγγ is the photon source resulting from photon interactions, qγe
is the electron source resulting from photon interactions and qee is the
electron source resulting from electron interactions. The corresponding
macroscopic differential cross sections are σγγt , σγet , σeet for photon–photon,
photon–electron, and electron–electron interactions respectively. The
15

Introduction
above equations are somewhat simplified in the interactions such that
photons can produce electrons but electrons do not produce photons. Addi-
tionally, the pair-production particles are assumed to be electrons (instead
of an electron–positron pair). Additionally, the electrons are transported
with a continuous slowing down approximation. In the radiotherapy do-
main, these simplifications are not affecting the accuracy of the solution
(Vassiliev et al. 2010).
The solution of the transport equation allows for an accurate deter-
mination of the absorbed energy in the material including the relevant
physics. As reviewed earlier, photons are indirectly ionizing particles and
do not deposit significant energy, but through interaction with medium
they transfer their energy to electrons and positrons that ionize and trans-
fer their energy until it is exhausted. The energy absorbed can be further
converted into absorbed dose which is strictly defined as mean energy im-
parted (by ionizing radiation) per mass (ICRU 1988).
In this Thesis methods that directly solve the transport equation are
not utilized but rather other methods to calculate the absorbed dose are
employed. These methods are typically phenomenological models or math-
ematical constructs that separate the effects of scattered radiation from
the primary radiation such as the Superposition/convolution (SC) algo-
rithm and are reviewed further in Chapter 3.
16
Introduction
1.7 Aims of the Thesis
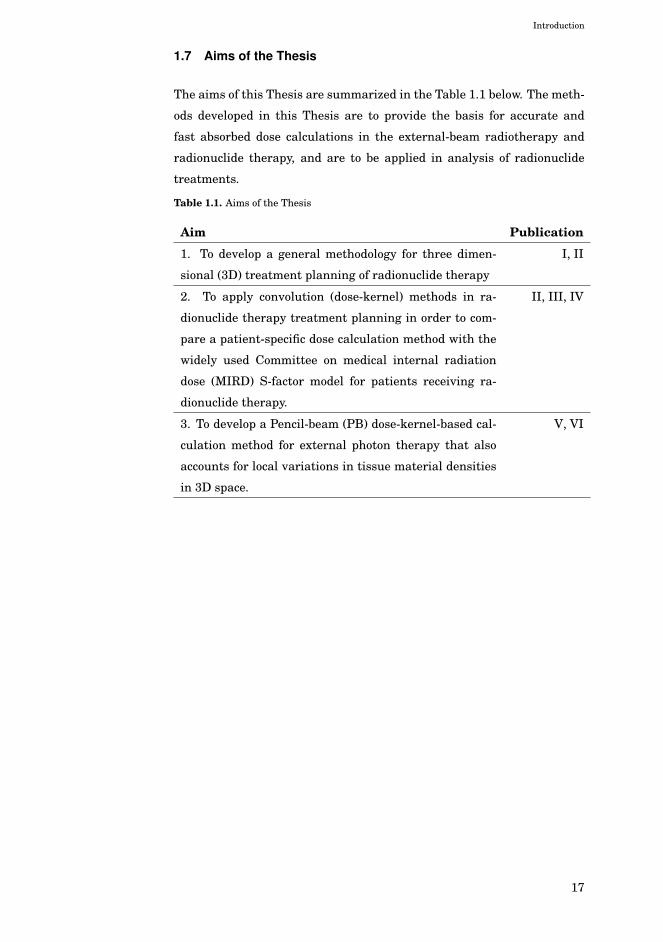
The aims of this Thesis are summarized in the Table 1.1 below. The meth-
ods developed in this Thesis are to provide the basis for accurate and
fast absorbed dose calculations in the external-beam radiotherapy and
radionuclide therapy, and are to be applied in analysis of radionuclide
treatments.
Table 1.1. Aims of the Thesis
Aim Publication
1. To develop a general methodology for three dimen-
sional (3D) treatment planning of radionuclide therapy
I, II
2. To apply convolution (dose-kernel) methods in ra-
dionuclide therapy treatment planning in order to com-
pare a patient-specific dose calculation method with the
widely used Committee on medical internal radiation
dose (MIRD) S-factor model for patients receiving ra-
dionuclide therapy.
II, III, IV
3. To develop a Pencil-beam (PB) dose-kernel-based cal-
culation method for external photon therapy that also
accounts for local variations in tissue material densities
in 3D space.
V, VI
17

Introduction
18

2. Radiotherapy treatment planning andsources of radiation
The overall radiotherapy treatment planning process aims to model the
treatment outcome. Current practice is to calculate and analyze radia-
tion dose as a surrogate for biological effectiveness of the treatment. The
overall process is depicted in Figure 2.1. The process is similar for ra-
dionuclide and external-beam therapy. The main difference is the patient-
specific radionuclide imaging that is used to construct the radiation source
model in radionuclide therapy, whereas in external-beam therapy the
source modeling is independent of the patient.
The treatment planning process starts with acquisition of anatomical
images used for anatomy modeling and dose calculation. X-ray Computed
tomography (CT) is suitable for dose calculation purposes due to its ge-
ometrical accuracy and ability to provide density and material composi-
tion data. Magnetic resonance (MR) imaging provides great soft tissue
contrast and is very useful for determining the boundaries of critical or-
gans and extent of macroscopic tumor growth. Anatomy modeling is done
by manually or semi-automatically segmenting the image data, providing
geometrical models of the patient’s anatomy. Dose calculation uses the
source model and an algorithm to solve the radiation transport problem
in the patient-specific geometry. The resulting dose distribution is visu-
alized and analyzed utilizing e.g. dose volume histograms (Drzymala et
al. 1991). A computer implementation of the radiotherapy process and
methods is called a Treatment planning system (TPS).
2.1 Dose calculation in radionuclide therapy
The absorbed dose in radionuclide therapy has commonly been calculated
using biokinetic data from a diagnostic tracer study, using a method de-
veloped by the MIRD (Watson et al. 1993). The traditional MIRD method
19

Radiotherapy treatment planning and sources of radiation
Acquire Images
Model Anatomy Calculate Dose
Model Source
Analyze & Visualize
SPECT
Acquire Images
Model Anatomy Calculate Dose
Model Source
Analyze & Visualize
CT, MR
a) b)
CT, MR
Figure 2.1. The treatment planning process for a) radionuclide therapy and b) external-beam radiotherapy are very similar.
includes a model patient phantom where various organ-to-organ contri-
butions of dose have been pre-calculated with the MC method to solve the
above transport equations. When applied in a clinical setting, the MIRD
method fails to include patient-specific anatomy and non-homogenous dis-
tribution of the radionuclide inside a given organ. A computer implemen-
tation of the methodology that is currently widely used is called Organ
level internal dose assessment (OLINDA) (Stabin et al. 2005).
Various authors have studied methods that overcome these limitations.
Although Traino et al. (2013) report on a simplified patient-specific method
based on the MIRD S-factors, the most common solution is to calculate the
absorbed dose distributions using a point-source-kernel approach with
patient-specific activity maps (Sgouros et al. 1990; Sgouros et al. 1993;
Erdi et al. 1994; Kolbert et al. 1997; Giap et al. 1995b; Giap et al. 1995a;
Erdi et al. 1998; Gardin et al. 2003; Guy et al. 2003; Loudos et al. 2009).
This method is also utilized in papers I, II, III and IV. Another approach
is to utilize the so called voxel S-factors to calculate patient-specific dose
estimates in combination with point kernels as described by Jackson et
al. (2013). As in external-beam radiotherapy, MC calculations have also
been proposed and applied in radionuclide therapy for patient-specific
dose calculations by Tagesson et al. (1996) and Furhang et al. (1996a)
and Furhang et al. (1997) and more recently applied e.g. by Ljungberg
et al. (2002), Chiavassa et al. (2005), Prideaux et al. (2007), Marcatili et
al. (2013), and Grimes and Celler (2014). Dieudonné et al. (2013) has
compared accuracy between the dose kernel methods and MC methods.
20

Radiotherapy treatment planning and sources of radiation
2.2 Distribution of activity in radionuclide therapy
Overall treatment planning and dosimetry of radionuclide therapy re-
quires an estimation of the radionuclide activity distribution in the pa-
tient over time (Strand et al. 1993b; Sgouros et al. 1990). This cumulative
activity distribution can be derived form nuclear medical imaging tech-
niques (planar gamma camera, Positron emission tomography (PET), and
Single-photon emission computed tomography (SPECT)) and pharmacoki-
netic data. The image data has to be quantified so that absolute activity
counts needed for cumulative activity distribution can be obtained. Ad-
ditionally, pharmacokinetic modeling complements the estimation of cu-
mulated activity in the image. The basic pharmacokinetic modeling of
radiolabeled Monoclonal antibody (MoAb) has been reviewed by Strand et
al. (1993a) and a software package to calculate cumulated activities has
recently been developed by Kletting et al. (2013).
The general goal for emission-computed tomography is to be able to
quantitatively determine localization volumes and measurement of activ-
ities in small and large tumors. There are various factors that affect the
accuracy of the quantification of emission-computed images. In SPECT,
the most important physical factors are scatter and attenuation correc-
tions, limited spatial and energy resolutions of gamma cameras, septal
penetration of high energy photons, and statistical noise of low count
densities. The system resolution is about 9 mm and full-width-at-half-
maximum of SPECT devices range from 7 - 18 mm, which leads to partial
volume effects i.e. loss of apparent activity within small objects (Erlands-
son et al. 2012). The use of PET would provide improved spatial resolution
and quantification. For PET systems, the spatial resolution is about 6 -
13 mm. The limitations of PET has been the availability of the technology
and problems associated with short lived radionuclides. Lubberink et al.
(1999) and Lundqvist et al. (1999) discuss the use of PET for radionuclide
quantification and dosimetry.
For treatment planning purposes, the imaging can be done prior to
therapy or during therapy to verify estimate actual dose delivered, and
both methods where used in II, III and IV. The pre-therapy imaging can
be carried out using an appropriate radionuclide label for the targeting
agent with a gamma camera or positron camera. The pre-therapy forms
the basis of targeted radionuclide therapy planning. Therapy imaging is
more demanding but is essential for confirming the information provided
21

Radiotherapy treatment planning and sources of radiation
by pre-therapy planning study.
The information that is crucial to dosimetry is tracer concentration at
several time points throughout the residence time of the tracer. The im-
ages need to be corrected for detector uniformity of response and dead-
time, photon attenuation and scattering effects (Ott 1996). The conver-
sion of image data in counts per voxel to concentration requires calibra-
tion data of phantoms imaged with known radioactive concentration of
tracer. The accuracy of the kinetics of the radionuclide concentration is
furthermore restricted by the temporal sparseness imaging data.
The kinetics of the therapeutic dose may vary from the tracer dose.
Although the pre-therapy dosimetry is important in the guidance of the
treatment, the actual dose delivered in treatment needs to be determined
using on-therapy imaging. The estimation of doses in III and IV where
done based on on-therapy SPECT images and quantification using planar
gamma camera images with a standard source as a reference.
Obtaining qualitative data of activity distributions from SPECT re-
quires careful methods in acquiring and processing the data (Ott 1996;
Leichner et al. 1993; Dewaraja et al. 2012). Quantitative planar and
SPECT images can be obtained by using attenuation and scatter correc-
tion methods. Hutton et al. (2011) have produced a recent review of the
current scatter correction methods and notes that the most widely used
ones are the scatter subtraction by multiple energy window approaches,
as described by Macey et al. (1995). Ljungberg et al. (1994) have com-
pared a few different methods and concluded that there is no significant
difference in quantification accuracy between them.
Improved reconstruction accuracy using iterative methods is an active
research area (see e.g. (Beekman et al. 2002; Ouyang et al. 2007)). An
application of such methods in radionuclide therapy with absorbed dose
estimation has been reported by Cheng et al. (2014). The emerging hy-
brid SPECT/CT and PET/CT devices are also aiding in better reconstruc-
tion and image processing methods for quantitative imaging by providing
complementary information about the attenuation properties of the pa-
tient (Cade et al. 2013). It is essential to validate the methodology used
to extract quantitative information from reconstructed images because
different devices and reconstruction algorithms have a big effect on the
quality of the images.
22

Radiotherapy treatment planning and sources of radiation
2.3 Treatment machine modeling
In order to characterize the energy fluence output of a linear accelera-
tor suitable for transport equation solvers or model-based SC and Pencil
beam (PB) algorithms, one needs a physical source model of the treatment
machine. The output of a treatment machine is well understood thanks
to the extensive study of radiation output based on the geometrical con-
struction (of the machine) by utilizing the MC method — see e.g. Mohan
et al. (1985), Ma et al. (1999), Sheikh-Bagheri and Rogers (2002b) and
Sheikh-Bagheri and Rogers (2002a) using MC based tools like BEAM as
described by Rogers et al. (1995).
For practical application, simplified models have been developed that
divide the main sources of radiation into several components that can be
described by a small set of model parameters. These are called Multiple
source models (MSM) and have been developed by various independent
researchers like Liu et al. (1997), Fix et al. (2001b), Deng et al. (2004),
Fippel et al. (2003), Fix et al. (2004), and Tillikainen et al. (2007) for the
purposes of dose calculations. Another use for simplified source models
is in Quality assurance (QA), where independent monitor unit calcula-
tions can be performed with simplified energy fluence models (Georg et
al. 2007).
Typical MSM models include a point source for primary radiation from
the bremsstrahlung target and finite size sources to account for extra-
focal radiation from flattening filter, primary collimators, and secondary
jaws. The models also include treatment of the electrons escaping the
linear accelerator in addition to the photon sources. Figure 2.2 shows
schematically a two source photon model with the target and flattening
filter showing in red as the effective photon sources; in addition, electrons
are generated in air by the photon radiation. Some of the models are de-
rived from MC simulation data tuned to match a given linear accelerator,
which is a very time consuming process (Ojala 2014). A more practical
approach is to fit model parameters to a set of measurements for a given
treatment unit in an automated fashion as described by Tillikainen et al.
(2007).
Various photon beam dose models are reported to reproduce dose calcu-
lation results in water within 1-2% accuracy (Jiang et al. 2001; Fix et al.
2001a). Ahnesjö et al. (2005) report the performance of their MSM for a
large number of clinical linear accelerators in which 87% machines can
23

Radiotherapy treatment planning and sources of radiation
Figure 2.2. A schematic drawing of a medical linear accelerator as the radiation sourcein external-beam radiotherapy.
be modeled within 2.5% maximum error. The final element of the model-
ing of the output of a linear accelerator is the back-scatter to the monitor
chamber (Verhaegen et al. 2000; Jiang et al. 2001). The back scatter effect
can be included as a correction factor or as a more comprehensive model
like that described by Liu et al. (2000). The overall accuracy of dose calcu-
lation approach determined both by the accuracy of the source model and
the radiation transport in the patient geometry is discussed in the next
section.
24

3. Model-based convolution andsuperposition methods in absorbeddose calculation
3.1 Background
Widely used model-based dose calculation methods are SC and PB algo-
rithms. The models in these algorithms separate the handling of the pri-
mary photons from the scattered photons, and later combine the effects of
scattered radiation by distributing this in a large volume. The underlying
physics can be utilized to calculate the model parameters, or the parame-
ters can be obtained by fitting the model to measurements. Although both
algorithms separate the primary radiation from the scattered radiation,
they differ in how the separation is done.
In the SC method, the scatter is modeled as a point-spread kernel —
as a Three dimensional (3D) kernel for a given point in the interacting
matter — whereas, in the PB method, the scatter is modeled as a planar
(2D) depth-dependent kernel that is distributed perpendicularly to the
ray lines of the primary radiation from a external point source. Figure
3.1 illustrates the different view points of the a) PB and b) SC algorithms.
The PB method views dose deposited from a small narrow beam with a
varying shape at each depth that includes all effects from upstream scat-
tering events and utilizes this to compose broad beam distributions. The
SC method looks at an unidirectionally moving single photon always in-
teracting at the same point and producing a point-dose-spread kernel that
is used in an macroscopic situation.
The case c) shows kernel of radiation dose of a single point source which
is utilized for internal radiotherapy (brachytherapy or radionuclide ther-
apy), where radiation can be modeled as point sources inside the Volume
of interest (VOI). This method is different from the two others as no sep-
aration of scattered dose is attempted, rather the dose kernel includes all
25

Model-based convolution and superposition methods in absorbed dose calculation
effects of a single point source depositing dose by interactions with the
matter.
a) b) c)
Figure 3.1. Different kernel-based methods have different geometrical separation of thesource term (primary) and the scattered radiation dose. The kernels from leftto right a) PB kernel b) a point-spread kernel and c) point source dose kernel.
3.2 Point-spread and kernel methods
3.2.1 Brachytherapy
The most widely used method to calculate absorbed dose around brachy-
therapy sources are based on the formalism and data from the AAPM
Task Group 43 recommendations (Rivard et al. 2004; Nath et al. 1995).
The method allows inclusion of the effects of the anisotropic distribution
around linear sealed radioactive sources. The method provides absorbed
dose distribution in water medium. The effect of medium heterogene-
ity can be included using transport equation solvers (Poon et al. 2008;
Zourari et al. 2010; Lemaréchal et al. 2015) or by applying the SC method
for brachytherapy as investigated by Carlsson and Ahnesjö (2000b) and
Carlsson and Ahnesjö (2000a). The more accurate methods are especially
useful in the context of improving dose calculation results in the pres-
ence of radiation shields (Tedgren and Ahnesjö 2003; Petrokokkinos et al.
2011).
26

Model-based convolution and superposition methods in absorbed dose calculation
3.2.2 Radionuclide therapy
As discussed earlier, the point-source-kernel approach can provide patient-
specific dose calculations in radionuclide therapy by using an activity map
of the distribution of the radionuclide as input. Absorbed dose distribu-
tion D(~r) at point ~r of known cumulative activity distribution A(~r) in a
homogenous medium can be calculated with a convolution integral (Giap
et al. 1995b):
D(~r) =
∫
V ′A(~r ′)k(|~r − ~r ′|)dV ′, (3.1)
where k(r) is a point source dose kernel (i.e. a spherically symmetric dose
distribution of point source of unit cumulative activity, see 3.1 c)). The
kernels can be obtained from MC simulations, analytical calculations, or
physical measurements. Dose kernels have been constructed using the
MC method, for instance by Furhang et al. (1996b) and Reiner et al.
(2009), or from cross sectional material data by Leichner (1994).
The convolution integral is effectively computed discretely using the
(Discrete) fast Fourier transform (FFT) as investigated by various au-
thors, both in the realm of brachytherapy and radionuclide therapy dose
calculations (Boyer and Mok 1986a; Giap et al. 1995b). The 3D kernel
and the 3D activity map are transformed into the Fourier space, where
the convolution is calculated by multiplication and transformed back to
the spatial domain using an inverse FFT providing the solution to the
convolution integral.
3.2.3 3D kernel methods in external-beam therapy
As discussed earlier, in external-beam therapy the 3D dose kernel has a
different meaning compared to internal therapy. Here, the 3D kernel is
a cumulative dose-spread array of photons interacting in a single point
in the medium. It includes all the effects of photon and electron scatter
interactions leading to adsorbed energy (radiation dose) in the medium.
These dose-spread arrays can be calculated and tabulated by using the
MC method, see Mackie et al. (1988).
The kernel methods rely on the fact that the broad beam dose can be
composed of multiple point irradiations that cause a response that can be
summed up over the whole problem (superposition). The attenuation of
incident photons interacting in the medium is calculated and the Total
energy released in the material (TERMA) is determined. The transport of
energy by scattered photons and electrons is described by the point-spread
27

Model-based convolution and superposition methods in absorbed dose calculation
kernel. The dose distribution is the superposition of the kernels, weighted
by the magnitude of the TERMA impulse for all interaction sites. These
methods were actively developed for the radiotherapy treatment planning
calculations in mid 1980s by several independent groups, as reported by
Mackie et al. (1985), Boyer and Mok (1986b), Boyer and Mok (1985), and
Boyer et al. (1989), Mohan and Chui (1987) and Ahnesjö et al. (1987).
In the most simplest geometries (homogenous materials and simplified
source models), the kernels are spatially invariant, making the superpo-
sition a convolution integral similar to Equation 3.1 where the activity
term A(~r ′) is replaced by TERMA T (~r ′). In this case, this can be very
effieciently computed with the FFT method and was studied by various
authors like Boyer and Mok (1985), Boyer et al. (1989), and Mohan and
Chui (1987). Boyer (1984) and Boyer and Mok (1986b) have extended the
methods for heterogeneous materials by separating kernels into single
and multiple scattering events and applying first order approximations.
The basis of the approximations were developed further by Wong et al.
(1996). The more elaborate treatment of heterogeneity is to scale kernels
by ray-tracing methods, which has become the more prevalent method. A
computationally effective method for the density-scaling is to utilize spa-
tial discretization of the scattering angle and parametrization of scatter
kernels with exponential basis functions, as employed by Ahnesjö (1989)
in his Collapsed cone convolution (CCC) algorithm.
3.3 Pencil-beam methods
The specifics of PB methods as described in VI and V are summarized in
this section. The overview here is compressed and more details can be
found in the original papers. The algorithm has also been commercially
released as the Analytical anisotropic algorithm (AAA) in EclipseTM TPS.
The heterogeneity correction applied in this method is also analogous to
ray-tracing methods used in the 3D SC algorithms.
A PB kernel is a function produced by a narrow beam of monoenergetic
photons of energy E, impinging on a semi-infinite perpendicular water
phantom as depicted in Figure 3.1 a). The polyenergetic PB kernel func-
tion is hβ(z, r), where z and r represent the distance from the surface and
the orthogonal distance from the central axis, respectively. The kernels
hβ(z, r) can been obtained from MC simulations (Ahnesjö et al. 1992) or
deconvolutions from measurements, as described by Storchi and Woud-
28

Model-based convolution and superposition methods in absorbed dose calculation
stra (1996) and Storchi et al. (1999).
3.3.1 Exponential modeling of pencil beams
The methods described in V and VI assume that the pencil beam can be
separated into depth-directed and lateral components. The depth-directed
component accounts for the total energy deposited by the pencil beam for
each layer pz in the calculation grid:
Iβ(pz) = Φβ
∫ ∫hβ(t, υ, pz) dt dυ, (3.2)
where Φβ is the primary energy fluence for the beamlet β.
Lateral dose deposition is modeled as a sum of N radial exponential
functions both in VI and Ahnesjö et al. (1992), whereas in V the lateral
shape is modeled as Gaussian functions. The kernel is separated into sec-
tors at angle θ as the fraction of energy deposited onto an infinitesimally
small angular sector at distance λ from the beamlet central axis. The an-
gular sectors allow for the heterogeneity correction in the lateral direction
by ray-tracing along the discrete rays that represent the collapsed sec-
tors. Given a number N of exponential function components (defined by
coefficients µi), the exponential representation of the lateral pencil-beam
component for a given depth plane pz is of the form
kβ(θ, λ, pz) =N∑
i=1
ci(θ, pz)1
µie−µiλ, (3.3)
where the attenuation coefficients µi are the same for all planes to allow
an efficient computer implementation. The weight parameters ci(θ, pz)
are fitted to the underlying PB kernel data obtained from MC simulations.
The parameter N is chosen to balance between speed and accuracy, and
in the implementation in VI we use the value N = 6.
3.3.2 Superposition of pencil beams
In a homogeneous water, the energy Eβ(~p) deposited from a pencil-beam
beamlet β into a point ~p is the product of the energy deposited on the
calculation plane (Iβ) and the corresponding lateral scatter kernel (kβ). A
factor of 1/λ is also included for normalization:
Eβ(~p) = Iβ(pz)1
λkβ(θ, λ, pz), (3.4)
To account for heterogenous material, the density-scaling approxima-
tion where each spatial dimension of the scatter process is scaled locally
29

Model-based convolution and superposition methods in absorbed dose calculation
by the inverse relative electron density 1/ρw can be used:
ρw(~p) := ρelec(~p)/ρelecwater, (3.5)
where ρelec is the local electron density at point ~p and ρelecwater the electron
density of water. It is necessary to account for the effective (radiological)
distance deff(X) =∫X ρw(~p)d~p for an arbitrary path X.
The scaling of the lateral scatter kernel is done by calculating the ra-
diological path length in a radial manner from the center of the pencil
beam. Then the heterogeneity-corrected lateral kernel k′β(θ, λ, pz) is given
by
k′β(θ, λ, pz) = kβ(θ,p′zpzλ′, p′z)ρw(~p), (3.6)
where λ′ is the effective radius computed as λ′ = deff(Cβ(θ, pz)). This radi-
ological pathlength scaling method based on electron density is a common
approach to account for tissue heterogeneities in kernel based models,
as reported in the review by Ahnesjö and Aspradakis (1999), and has
been found to be more appropriate than the scaling based on mass den-
sity by Seco and Evans (2006).
The I function also needs to be scaled for heterogeneities by expressing
it in terms of effective depth p′z. Thus, the heterogeneity corrected depth-
directed component I ′β is calculated as
I ′β(pz) = Iβ(p′z)ρw( ~pβ), (3.7)
where ~pβ is the point on the pencil-beam central axis at depth pz, p′z is the
effective depth given by deff(Pβ), where Pβ is the path from pencil-beam
entry point to ~pβ.
The heterogeneity-corrected energy distribution from a single beamlet
β is then calculated as:
Eβ(~p) = I ′β(pz)1
λk′β(θ, λ, pz). (3.8)
The total deposited energy into a grid point ~p is then simply an integral
of contribution of all the individual beamlets over the broad beam area:
Etot(~p) =
∫ ∫
β′Eβ′(~p) dβ′. (3.9)
3.3.3 Build-up and build-down correction
The separation of the heterogeneity correction into two components, the
depth-directed component in (3.7) and the lateral scatter component in
30
Model-based convolution and superposition methods in absorbed dose calculation
(3.6) is clearly an approximation, but it produces good results after suf-
ficient distance from the material interface in slab-like phantoms. How-
ever, near the interfaces it fails to reproduce the gradual build-up and
build-down effects — instead, the dose would jump abruptly to a new
equilibrium level. This is caused by the fact that the scattered particles
originating before the interface are not correctly taken into account by
this method.
The size of the build-up or build-down transition is determined by the
mean range of the scattered particles. Also, the dominant scatter com-
ponent in a therapeutic radiation beam is forward-directed. Thus to re-
produce these effects using a pencil-beam based model, it is not sufficient
to scale the pencil beam in its entirety by the effective distance, but a
method to account for the forward-directed energy shift is needed.
The technique chosen in this work is to employ a forward build-up con-
volution kernel to the energy deposition introduced in V and refined in
VI using a build-up kernel kb. The convolution is done with the energy
density distribution in terms of effective distance in the following way:
Eb(~p) =
∫ pz
t=0Etot(px, py, t)kb(deff)ρw(px, py, t)dt, (3.10)
where deff is the (signed) effective distance from (px, py, pz) to (px, py, t),
and the multiplication with ρw is due to the change of variables from effec-
tive depth to true depth. This correction effectively shifts energy deeper,
so the original pencil beams would no longer be accurately reproduced.
For example, the original build-up at the surface of the pencil beam would
be further stretched. Hence, it is necessary to pre-compensate in the I
function in (3.2) using a deconvolution approach.
3.4 Computational considerations
3.4.1 Performance characteristics
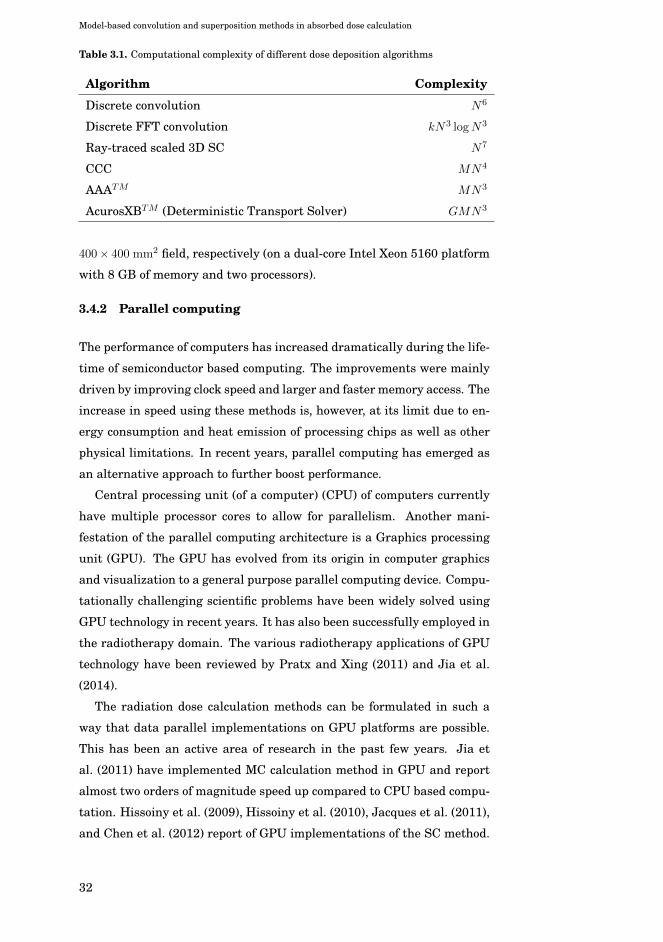
In this section, computational complexity of various SC algorithms is re-
viewed. For the purpose of the analysis, a 3D calculation grid N ×N ×Nwill be considered with M number of rays for ray-tracing for scatter scal-
ing and G is the number of energy groups. The Table 3.1 contains the
computational complexities of the various dose calculation algorithms.
An example of running time of a computer implementation of the PB
method in VI is about 10 s for a 40 × 40 mm2 field and about 60 s for a
31
Model-based convolution and superposition methods in absorbed dose calculation
Table 3.1. Computational complexity of different dose deposition algorithms
Algorithm Complexity
Discrete convolution N6
Discrete FFT convolution kN3 logN3
Ray-traced scaled 3D SC N7
CCC MN4
AAATM MN3
AcurosXBTM (Deterministic Transport Solver) GMN3
400× 400 mm2 field, respectively (on a dual-core Intel Xeon 5160 platform
with 8 GB of memory and two processors).
3.4.2 Parallel computing
The performance of computers has increased dramatically during the life-
time of semiconductor based computing. The improvements were mainly
driven by improving clock speed and larger and faster memory access. The
increase in speed using these methods is, however, at its limit due to en-
ergy consumption and heat emission of processing chips as well as other
physical limitations. In recent years, parallel computing has emerged as
an alternative approach to further boost performance.
Central processing unit (of a computer) (CPU) of computers currently
have multiple processor cores to allow for parallelism. Another mani-
festation of the parallel computing architecture is a Graphics processing
unit (GPU). The GPU has evolved from its origin in computer graphics
and visualization to a general purpose parallel computing device. Compu-
tationally challenging scientific problems have been widely solved using
GPU technology in recent years. It has also been successfully employed in
the radiotherapy domain. The various radiotherapy applications of GPU
technology have been reviewed by Pratx and Xing (2011) and Jia et al.
(2014).
The radiation dose calculation methods can be formulated in such a
way that data parallel implementations on GPU platforms are possible.
This has been an active area of research in the past few years. Jia et
al. (2011) have implemented MC calculation method in GPU and report
almost two orders of magnitude speed up compared to CPU based compu-
tation. Hissoiny et al. (2009), Hissoiny et al. (2010), Jacques et al. (2011),
and Chen et al. (2012) report of GPU implementations of the SC method.
32

Model-based convolution and superposition methods in absorbed dose calculation
Additionally, Chen et al. (2011) report an extremely efficient implementa-
tion of the CCC algorithm, where calculation times can be pushed below 1
s per beam for a grid of 2563 calculation points on modern GPU platforms
(NVIDIA GTX295). Gu et al. (2009) has applied GPU technology to suc-
cessfully implement an ultra-fast dose calculation engine using the PB
method. These developments open up new opportunities for interactive
dose shaping tools and more accurate solutions to the inverse problems in
radiotherapy treatment planning.
33

Model-based convolution and superposition methods in absorbed dose calculation
34

4. Summary of results
4.1 Patient-specific distributions in radionuclide therapy
The first aim for this research was to produce a dose planning system for
radioimmunotherapy by leveraging an existing radiotherapy treatment
planning system and implementing a faster dose kernel convolution algo-
rithm. The aim was also to develop novel 3D absorbed dose visualization
methods. The results reported in I were a successful implementation of
a radionuclide therapy planning system utilizing a fast point dose ker-
nel calculation method and expanding visualization and user interface of
the existing radiotherapy TPS. The developed system was used to ana-
lyze variability of biological uptake and clearance of the therapy agent
in various patients and to estimate absorbed doses based on a point dose
kernel dose calculation method in II. The main results were that both the
inter-patient variability of biological clearance and localized differences
for individual patients warrant the use of serial SPECT imaging to be
able to determine patient-specific absorbed doses.
The clearance times for two different patients are plotted in Figure 1
of II. The clearance is assumed to contain two exponential components,
thus the biological half-lives was calculated for both components. The ex-
ponential trend for the clearance determined from the SPECT images is
also shown in the same figure. Spatial variation of the activity clearance
was analyzed in the intra-therapeutic SPECT images by dividing the im-
ages into sub-volumes 64 cm3 (4 x 4 x 4 cm). The biological half-lives
and clearance times of for each of these sub-volumes were calculated and
the results are summarized in Table 1 (II). Additionally, patient absorbed
doses were calculated based on cumulated activity and the activity map
from the first SPECT study.
35
Summary of results
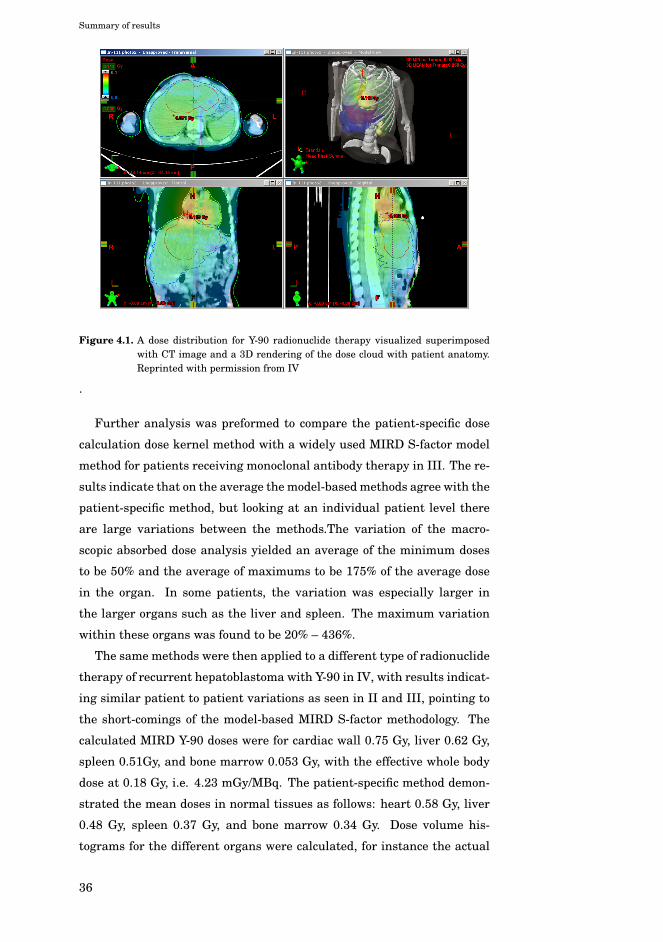
Figure 4.1. A dose distribution for Y-90 radionuclide therapy visualized superimposedwith CT image and a 3D rendering of the dose cloud with patient anatomy.Reprinted with permission from IV
.
Further analysis was preformed to compare the patient-specific dose
calculation dose kernel method with a widely used MIRD S-factor model
method for patients receiving monoclonal antibody therapy in III. The re-
sults indicate that on the average the model-based methods agree with the
patient-specific method, but looking at an individual patient level there
are large variations between the methods.The variation of the macro-
scopic absorbed dose analysis yielded an average of the minimum doses
to be 50% and the average of maximums to be 175% of the average dose
in the organ. In some patients, the variation was especially larger in
the larger organs such as the liver and spleen. The maximum variation
within these organs was found to be 20% – 436%.
The same methods were then applied to a different type of radionuclide
therapy of recurrent hepatoblastoma with Y-90 in IV, with results indicat-
ing similar patient to patient variations as seen in II and III, pointing to
the short-comings of the model-based MIRD S-factor methodology. The
calculated MIRD Y-90 doses were for cardiac wall 0.75 Gy, liver 0.62 Gy,
spleen 0.51Gy, and bone marrow 0.053 Gy, with the effective whole body
dose at 0.18 Gy, i.e. 4.23 mGy/MBq. The patient-specific method demon-
strated the mean doses in normal tissues as follows: heart 0.58 Gy, liver
0.48 Gy, spleen 0.37 Gy, and bone marrow 0.34 Gy. Dose volume his-
tograms for the different organs were calculated, for instance the actual
36

Summary of results
liver tumor dose was in average 0.51 Gy, with a range 0.22-0.96 Gy. A
visualization of the calculated doses is shown in Figure 4.1.
4.2 A pencil beam superposition algorithm in external radiotherapy
The development of a PB dose calculation method for external photon
therapy was undertaken in V and further refined in VI. The earlier paper
outlines the methods and foundations of the density-scaling methodology
of the pencil beams and depth-dependent component.
As presented in VI, there is generally a good agreement between the
calculations utilizing the presented method and MC simulations in differ-
ent kind of heterogeneous phantoms. Most of the observed discrepancies
were within (2%, 2 mm), where the dose difference is specified with re-
spect to the field Central axis (CAX) dmax. Considerably larger deviations
were found only in the central axis depth dose of the smallest field size
(30×30 mm2) in the lung slab phantom for the 18 MV beam, where discrep-
ancies in the order of 8% were observed inside the lung insert (ρw = 0.3).
These discrepancies are of comparable magnitude (∼5%), as observed by
Arnfield et al. (2000), for the CCC superposition model in similar situa-
tions. The explanation for the discrepancies lies in the fact that in high
energy beams of small field size there is a loss of electronic equilibrium
on the central axis, which is not modeled with rectilinear kernel scaling
approaches. The electronic disequilibrium on the field central axis in the
low-density material becomes larger as the field size decreases and the
beam energy increases and there are more electrons traveling away from
the corresponding volume element on the central axis than towards it.
The re-buildup effect is overestimated in our method on the lung-water
interface, as seen in Figure 4.2, which is contrary to other SC models that
tend to underestimate the effect. This difference in the algorithm behav-
ior is due to the build-up kernel correction method used in the presented
method, which is not used in other SC algorithms. The build-up kernel
has been designed such that the build-up between vacuum and water is
correctly reproduced, whereas the build-up effect between lung and water
is probably smaller, which could explain the observed overestimation in
the re-buildup region. Fotina et al. (2009) provided comparisons between
AAA and SC methods to MC calculations, that show good agreement for
both of the methods with slightly better agreement for the SC method.
In higher density material (bone, ρw = 1.85) the discrepancies between
37

Summary of results
20
40
60
80
100
0 50 100 150 200 250 300-8
-6
-4
-2
0
2
4
6
8
Per
cent
dep
th d
ose
(%)
Diff
eren
ce (%
)
Depth (mm)
(a)
AAA Fs30VMC Fs30
Diff Fs30
20
40
60
80
100
0 50 100 150 200 250 300-8
-6
-4
-2
0
2
4
6
8
Per
cent
dep
th d
ose
(%)
Diff
eren
ce (%
)
Depth (mm)
(b)
AAA Fs50VMC Fs50
Diff Fs50
20
40
60
80
100
0 50 100 150 200 250 300-8
-6
-4
-2
0
2
4
6
8
Per
cent
dep
th d
ose
(%)
Diff
eren
ce (%
)
Depth (mm)
(c)
AAA Fs100VMC Fs100
Diff Fs100
20
40
60
80
100
0 50 100 150 200 250 300-8
-6
-4
-2
0
2
4
6
8
Per
cent
dep
th d
ose
(%)
Diff
eren
ce (%
)
Depth (mm)
(d)
AAA Fs200VMC Fs200
Diff Fs200
Figure 4.2. Calculated ’AAA’ and MC-simulated ’VMC’ depth dose curves in the lung slabphantom for the 6 MV beam. (a) Field size 30× 30 mm2, (b) 50× 50 mm2, (c)100× 100 mm2, and (d) 200× 200 mm2. Reprinted with permission from VI.
our PB algorithm and MC simulations are in the order of (2%, 2 mm).
For lower energies (6 MV beam), our method overestimates the dose sys-
tematically about 1% inside the high-density material. For higher energy
(18 MV), the discrepancies near the heterogeneity border of the bone slab
phantom are smaller.
When compared to previously published experimental verification of
the presented method, some agreements and some disagreements were
found. In the work of Van Esch et al. (2006), the current method was
compared to ionization chamber and film measurements in several homo-
geneous and heterogeneous phantoms. The lateral profile comparisons
in the phantom with cork insert are in good agreement with the results
in the lung block phantom shown in Figure 4.3. The corresponding depth
dose comparisons for 6 MV show a significantly better agreement with the
MC simulations in the work than the comparisons to ionization chamber
measurements presented by Van Esch et al. (2006). This apparent contra-
diction can be explained by the fact that the ionization chamber itself can
cause significant dose perturbations (6 . . . 12%) at the point of measure-
ment in case of electronic disequilibrium. These kinds of perturbations
occur especially for a small field size, in low-density media.
The main results for the methods in V and VI are that excellent agree-
38

Summary of results
0
10
20
30
40
50
60
70
80
90
-200 -150 -100 -50 0 50 100 150 200-8
-6
-4
-2
0
2
4
6
8
Rel
ativ
e do
se (%
)
Diff
eren
ce (%
)
Depth (mm)
(a)
AAA D100VMC D100
Diff D100
0
10
20
30
40
50
60
70
80
-200 -150 -100 -50 0 50 100 150 200-8
-6
-4
-2
0
2
4
6
8
Rel
ativ
e do
se (%
)
Diff
eren
ce (%
)
Depth (mm)
(b)
AAA D160VMC D160
Diff D160
0
20
40
60
80
100
-200 -150 -100 -50 0 50 100 150 200-8
-6
-4
-2
0
2
4
6
8
Rel
ativ
e do
se (%
)
Diff
eren
ce (%
)
Depth (mm)
(c)
AAA D75VMC D75
Diff D75
0
10
20
30
40
50
60
70
80
90
-200 -150 -100 -50 0 50 100 150 200-8
-6
-4
-2
0
2
4
6
8
Rel
ativ
e do
se (%
)
Diff
eren
ce (%
)
Depth (mm)
(d)
AAA D110VMC D110
Diff D110
Figure 4.3. Calculated ’AAA’ and MC-simulated ’VMC’ dose profiles in the lung blockphantom for 6 and 18 MV beams. (a) 6 MV, depth 100 mm (b) 6 MV, depth160 mm, (c) 18 MV, depth 100 mm, and (d) 18 MV, depth 160 mm. Reprintedwith permission from VI
ment with MC method and experiments are obtained in homogenous ma-
terial as well as good results for the lateral heterogeneities (both water-
lung and water-bone interfaces) are obtained with lateral scaling of scat-
ter kernels. The method is computationally very efficient for use in a
routine clinical setting.
39

Summary of results
40

5. Discussion and conclusions
5.1 Overall results
The aims of the Thesis were to develop methods to improve dose calcu-
lation in aiding treatment planning of radionuclide and external-beam
therapy. The aims of the Thesis were met and a high level summary of
results in relation to the aims is presented in Figure 5.1.
The Thesis developed methodology for 3D treatment planning of ra-
dionuclide therapy with dose calculation based on quantitative SPECT
images and a point dose kernel calculation method. The dose kernel con-
volution method was applied in several radionuclide therapy cases as a
treatment planning and dosimetric verification tool. Comparisons of the
developed patient-specific dose calculation method with the widely used
MIRD S-factor model was discussed in III and IV. The results show large
variations between the methods at individual patient level and within
target organs. The results indicate that the spatial dose distribution is
needed to further understand therapeutic effect and toxicity of radionu-
clide treatments, and the developed system is useful in the analysis of
radionuclide treatments.
The development of a PB dose kernel based calculation method for ex-
ternal photon therapy that also accounts for local variations in tissue ma-
terial densities in 3D space was reported in V and further refined in VI.
The method performs within clinically acceptable accuracy as compared
to experiments and MC calculations with typical agreement within (2%,
2 mm) for various test problems.
Although the aims of the Thesis were met, there is further room for im-
provement in the source modeling of the radionuclide therapy (i.e. quan-
titative SPECT and automated processing of time-series activity data).
41

Discussion and conclusions
The recent advances in nuclear medicine imaging with hybrid SPECT/CT
devices and PET imaging are enabling this advancement. For instance
Willowson et al. (2008) report on an experimental verification of quantita-
tive methodology based on SPECT/CT that achieves accuracy of activity
quantification in the range of -7%–%4, compared to known activity con-
centrations.
• Implemention of point dose kernel based radionuclide TPS
• Powerful toolset for evaluaton of patient specific 3D dose distiributions
AAim 1. Radionuclide 3D planning methods
• Different therapy cases using point kernel and S-factor methods
• Point kernel methods provide patient specific 3D information for various radionuclides
Aim 2. Radionuclide
therapy case studies
• PB method with 3D heterogeneity correction
• Comparisons to MC calculations show good agreement
• Fast calculation times & wide clinical adoption
Aim 3. External beam dose
computations
Figure 5.1. Main results grouped by the aims of the Thesis.
5.2 Contribution to the field
This Thesis has developed further computational methods that are rele-
vant in the practical application of radionuclide therapy as well external-
beam therapy. Applying the methods in radionuclide therapy has pro-
vided new results on the applicability of the methods as well as a compar-
ison to existing practices of the MIRD formalism.
The application of patient-specific dosimetry in radionuclide therapy
is still in its infancy in the wider clinical practice of 2016. Although the
methods developed as part of this Thesis have been used in clinical prac-
tice since 1997, wider adoption will only be possible when these meth-
ods are introduced in an easy to use commercial package (by Nuclear
Medicine image analysis or general radiotherapy planning software ven-
42

Discussion and conclusions
dors). The work in papers I — IV show that this approach is viable and
is well aligned with toolsets available in radiotherapy planning software
systems.
In papers V and VI a computationally efficient and accurate PB al-
gorithm was developed with 3D treatment of tissue heterogeneity. It is
coupled with an accurate model of the external radiation therapy ma-
chine sources including a robust optimization of the model parameters
described in Tillikainen et al. (2007). It has been commercialized as the
AAA dose calculation algorithm in the widely used EclipseTM Treatment
planning system (Varian Medical Systems, Palo Alto CA). The methods
are used in routine clinical practice — with thousands of treatment plans
calculated daily using these methods and numerous of studies examining
its performance (Ojala et al. 2014; Tsuruta et al. 2014; Liu et al. 2014;
Han et al. 2012; Fotina et al. 2009; Breitman et al. 2007; Van Esch et al.
2006, etc.). Its main contribution is the novel treatment of heterogeneity
with a good balance between speed and accuracy.
5.3 Future directions
Although more rigorous and complete solutions to the radiation transport
exists (see Section 1.6), the model-based superposition and convolution
methods continue have an important role in the radiotherapy modeling.
In the past two decades, they have been the workhorses for dose calcula-
tion as well basis for solutions of the inverse problems. In the future, their
computational efficiency will ensure that they have a role in interactive
use as well as in radiotherapy plan optimization solutions. The methods
also lend themselves for efficient parallel computing implementations, as
discussed in Section 3.4.2.
External-beam radiotherapy has transitioned into image guided ther-
apy and the increased information of the daily patient setup will lend
itself for adaptation of the treatment plan for the current patient state.
This requires advances in rapid and automated dose evaluation, including
quick dose calculation and possible treatment plan optimization. These
computations need to happen in a few seconds in order not to delay the
daily patient treatment. The SC and PB methods are well poised for these
scenarios. These needs are also aligned with the adoption of ultra-high
dose fractions of the Stereotactic body radiation therapy (SBRT) (Lo et al.
2010).
43

Discussion and conclusions
Further improvements in accuracy could potentially be realized by com-
bining transport equation solvers with extremely fast convolution meth-
ods. The approach would perhaps improve the accuracy and modeling of
the relevant physics without compromising the speed of the methods to
provide fine details of the high resolution shape of the primary photon
energy fluence.
Next steps in improving the understanding and radiation dose thera-
peutic efficacy in radionuclide therapy is to adopt more widely the meth-
ods outlined in this Thesis. After that initial step, the next area to im-
prove is the process of acquiring quantitative 3D activity distributions
and their use in the patient-specific dose evaluation. Although the accu-
racy of the dose calculation is currently not the limiting factor, the mod-
eling of the radiation transport could be further enhanced by employing
direct solutions to the transport equation by MC methods or deterministic
solutions.
5.4 Conclusions
The methods developed in this Thesis have proven to be relevant in the
application of radiotherapy. Their relevance for the upcoming improve-
ments in overall radiotherapy applications is also foreseen due to their
computational efficiency. Other methods will complement these as the
computational power available increases over the upcoming years. Accu-
racy and efficacy of radiotherapy can be enhanced when physical modeling
is further improved and applied in clinical practice.
44

References
Ahnesjö, A. (1989). “Collapsed cone convolution of radiant energy for pho-
ton dose calculation in heterogeneous media.” Med Phys 16.4, pp. 577–
592.
Ahnesjö, A. and M. M. Aspradakis (1999). “Dose calculations for external
photon beams in radiotherapy.” Phys Med Biol 44.11, R99–155.
Ahnesjö, A., P. Andreo, and A. Brahme (1987). “Calculation and applica-
tion of point spread functions for treatment planning with high energy
photon beams.” Acta Oncol 26.1, pp. 49–56.
Ahnesjö, A., M. Saxner, and A. Trepp (1992). “A pencil beam model for
photon dose calculation.” Med Phys 19.2, pp. 263–273.
Ahnesjö, A., L. Weber, A. Murman, M. Saxner, I. Thorslund, and E. Tra-
neus (2005). “Beam modeling and verification of a photon beam multi-
source model.” Med Phys 32.6, pp. 1722–1737.
Andreo, P. (1991). “Monte Carlo techniques in medical radiation physics.”
Phys Med Biol 36.7, pp. 861–920.
Arnfield, M. R., C. H. Siantar, J. Siebers, P. Garmon, L. Cox, and R. Mohan
(2000). “The impact of electron transport on the accuracy of computed
dose.” Med Phys 27.6, pp. 1266–1274.
Atun, R., D. A. Jaffray, M. B. Barton, F. Bray, M. Baumann, B. Vikram,
T. P. Hanna, F. M. Knaul, Y. Lievens, T. Y. M. Lui, M. Milosevic, B.
O’Sullivan, D. L. Rodin, E. Rosenblatt, J. Van Dyk, M. L. Yap, E. Zu-
bizarreta, and M. Gospodarowicz (2015). “Expanding global access to
radiotherapy.” Lancet Oncol 16.10, pp. 1153–1186.
Beekman, F. J., H. W. A. M. de Jong, and S. van Geloven (2002). “Effi-
cient fully 3-D iterative SPECT reconstruction with Monte Carlo-based
scatter compensation”. Medical Imaging, IEEE Transactions on 21.8,
pp. 867–877.
45

REFERENCES
Boyer, A. L. (1984). “Shortening the calculation time of photon dose dis-
tributions in an inhomogeneous medium.” Med Phys 11.4, pp. 552–554.
Boyer, A. L. and E. C. Mok (1985). “A photon dose distribution model em-
ploying convolution calculations.” Med Phys 12.2, pp. 169–177.
Boyer, A. L. and E. C. Mok (1986a). “Brachytherapy seed dose distribu-
tion calculation employing the fast Fourier transform”. Med Phys 13,
pp. 525–529.
Boyer, A. L. and E. C. Mok (1986b). “Calculation of photon dose distribu-
tions in an inhomogeneous medium using convolutions.” Med Phys 13.4,
pp. 503–509.
Boyer, A. L., Y. P. Zhu, L. Wang, and P. Francois (1989). “Fast Fourier
transform convolution calculations of x-ray isodose distributions in ho-
mogeneous media.” Med Phys 16.2, pp. 248–253.
Breitman, K., S. Rathee, C. Newcomb, B. Murray, D. Robinson, C. Field,
H. Warkentin, S. Connors, M. Mackenzie, P. Dunscombe, and G. Fallone
(2007). “Experimental validation of the Eclipse AAA algorithm.” J Appl
Clin Med Phys 8.2, pp. 76–92.
Cade, S. C., S. Arridge, M. J. Evans, and B. F. Hutton (2013). “Use of
measured scatter data for the attenuation correction of single photon
emission tomography without transmission scanning.” Med Phys 40.8,
p. 082506.
Carlsson, A. K. and A. Ahnesjö (2000a). “Point kernels and superposition
methods for scatter dose calculations in brachytherapy.” Phys Med Biol
45.2, pp. 357–382.
Carlsson, A. K. and A. Ahnesjö (2000b). “The collapsed cone superposition
algorithm applied to scatter dose calculations in brachytherapy.” Med
Phys 27.10, pp. 2320–2332.
Chen, Q., M. Chen, and W. Lu (2011). “Ultrafast convolution/ superposi-
tion using tabulated and exponential kernels on GPU.” Med Phys 38.3,
pp. 1150–1161.
Chen, Q., W. Lu, Y. Chen, M. Chen, D. Henderson, and E. Sterpin (2012).
“Validation of GPU based TomoTherapy dose calculation engine.” Med
Phys 39.4, pp. 1877–1886.
Cheng, L., R. F. Hobbs, G. Sgouros, and E. C. Frey (2014). “Development
and evaluation of convergent and accelerated penalized SPECT image
reconstruction methods for improved dose-volume histogram estimation
in radiopharmaceutical therapy.” Med Phys 41.11, p. 112507.
46

REFERENCES
Chiavassa, S., M. Bardi, F. Guiraud-Vitaux, D. Bruel, J.-R. Jourdain, D.
Franck, and I. Aubineau-Lani (2005). “OEDIPE: a personalized dosimet-
ric tool associating voxel-based models with MCNPX.” Cancer Biother
Radiopharm 20.3, pp. 325–332.
Deng, J., T. Guerrero, C. M. Ma, and R. Nath (2004). “Modelling 6 MV pho-
ton beams of a stereotactic radiosurgery system for Monte Carlo treat-
ment planning.” Phys Med Biol 49.9, pp. 1689–1704.
Dewaraja, Y. K., E. C. Frey, G. Sgouros, A. B. Brill, P. Roberson, P. B.
Zanzonico, and M. Ljungberg (2012). “MIRD Pamphlet No. 23: Quanti-
tative SPECT for Patient-Specific 3-Dimensional Dosimetry in Internal
Radionuclide Therapy.” J Nucl Med 53.8, pp. 1310–1325.
Dieudonné, A., R. F. Hobbs, R. Lebtahi, F. Maurel, S. Baechler, R. L. Wahl,
A. Boubaker, D. Le Guludec, G. Sgouros, and I. Gardin (2013). “Study of
the impact of tissue density heterogeneities on 3-dimensional abdomi-
nal dosimetry: comparison between dose kernel convolution and direct
Monte Carlo methods.” J Nucl Med 54.2, pp. 236–243.
Drzymala, R. E., R. Mohan, L. Brewster, J. Chu, M. Goitein, W. Harms,
and M. Urie (1991). “Dose-volume histograms.” Int J Radiat Oncol Biol
Phys 21.1, pp. 71–78.
Erdi, A. K., E. D. Yorke, M. H. Loew, Y. E. Erdi, M. Sarfaraz, and B. W.
Wessels (1998). “Use of the fast Hartley transform for three-dimensional
dose calculation in radionuclide therapy”. Med Phys 25.11, pp. 2226–
2233.
Erdi, E. K., M. Loew, E. Yorke, Y. Erdi, and B. Wessels (1994). “Use of
the fast Hartley transform for efficient 3D convolution in calculation
of radiation dose”. Proc. 16th Annual IEEE-EMBS Conference. IEEE.
Piscataway, NJ: IEEE, pp. 639–640.
Erlandsson, K., I. Buvat, P. H. Pretorius, B. A. Thomas, and B. F. Hutton
(2012). “A review of partial volume correction techniques for emission
tomography and their applications in neurology, cardiology and oncol-
ogy.” Phys Med Biol 57.21, R119–R159.
Fippel, M., I. Kawrakow, and K. Friedrich (1997). “Electron beam dose
calculations with the VMC algorithm and the verification data of the
NCI working group.” Phys Med Biol 42.3, pp. 501–520.
Fippel, M., W. Laub, B. Huber, and F. Nüsslin (1999). “Experimental inves-
tigation of a fast Monte Carlo photon beam dose calculation algorithm.”
Phys Med Biol 44.12, pp. 3039–3054.
47

REFERENCES
Fippel, M., F. Haryanto, O. Dohm, F. Nuesslin, and S. Kriesen (2003). “A
virtual photon energy fluence model for Monte Carlo dose calculation.”
Med Phys 30.3, pp. 301–311.
Fix, M. K., M. Stampanoni, P. Manser, E. J. Born, R. Mini, and P. Rüegseg-
ger (2001a). “A multiple source model for 6 MV photon beam dose calcu-
lations using Monte Carlo.” Phys Med Biol 46.5, pp. 1407–1427.
Fix, M. K., P. Manser, E. J. Born, R. Mini, and P. Rüegsegger (2001b).
“Monte Carlo simulation of a dynamic MLC based on a multiple source
model.” Phys Med Biol 46.12, pp. 3241–3257.
Fix, M. K., P. J. Keall, K. Dawson, and J. V. Siebers (2004). “Monte Carlo
source model for photon beam radiotherapy: photon source characteris-
tics.” Med Phys 31.11, pp. 3106–3121.
Fix, M. K., D. Frei, W. Volken, H. Neuenschwander, E. Born, and P. Manser
(2010). “Monte Carlo dose calculation improvements for low energy elec-
tron beams using eMC.” Phys Med Biol 55.16, pp. 4577–4588.
Fotina, I., P. Winkler, T. Künzler, J. Reiterer, I. Simmat, and D. Georg
(2009). “Advanced kernel methods vs. Monte Carlo-based dose calcula-
tion for high energy photon beams.” Radiother Oncol 93.3, pp. 645–653.
Furhang, E. E., C. S. Chui, and G. Sgouros (1996a). “A Monte Carlo ap-
proach to patient-specific dosimetry”. Med Phys 23, pp. 1523–1529.
Furhang, E. E., G. Sgouros, and C. S. Chui (1996b). “Radionuclide photon
dose kernels for internal emitter dosimetry”. Med Phys 23, pp. 759–764.
Furhang, E. E., C. S. Chui, K. S. Kolbert, S. M. Larson, and G. Sgouros
(1997). “Implementation of a Monte Carlo dosimetry method for patient-
specific internal emitter therapy”. Med Phys 24.7, pp. 1163–1172.
Gardin, I., L. G. Bouchet, K. Assié, J. Caron, A. Lisbona, L. Ferrer, W.
E. Bolch, and P. Vera (2003). “Voxeldoes: a computer program for 3-D
dose calculation in therapeutic nuclear medicine.” Cancer Biother Ra-
diopharm 18.1, pp. 109–115.
Georg, D., T. Nyholm, J. Olofsson, F. Kjaer-Kristoffersen, B. Schneken-
burger, P. Winkler, H. Nyström, A. Ahnesjö, and M. Karlsson (2007).
“Clinical evaluation of monitor unit software and the application of ac-
tion levels.” Radiother Oncol 85.2, pp. 306–315.
Giap, H. B., D. J. Macey, and D. A. Podoloff (1995a). “Development of
a SPECT-based three-dimensional treatment planning system for ra-
dioimmunotherapy”. J Nucl Med 36, pp. 1885–1894.
48

REFERENCES
Giap, H. B., D. J. Macey, J. E. Bayouth, and A. L. Boyer (1995b). “Valida-
tion of a dose-point kernel convolution technique for internal dosimetry”.
Phys Med Biol 40, pp. 365–381.
Grimes, J. and A. Celler (2014). “Comparison of internal dose estimates
obtained using organ-level, voxel S value, and Monte Carlo techniques.”
Med Phys 41.9, p. 092501.
Gu, X., D. Choi, C. Men, H. Pan, A. Majumdar, and S. B. Jiang (2009).
“GPU-based ultra-fast dose calculation using a finite size pencil beam
model.” Phys Med Biol 54.20, pp. 6287–6297.
Guy, M. J., G. D. Flux, P. Papavasileiou, M. A. Flower, and R. J. Ott (2003).
“RMDP: a dedicated package for 131I SPECT quantification, registra-
tion and patient-specific dosimetry.” Cancer Biother Radiopharm 18.1,
pp. 61–69.
Halperin, E. C., C. A. Perez, and L. W. Brady (2008). Perez and Brady’s
Principles and Practice of Radiation Oncology. Philadelphia, PA: Lip-
pincott Williams & Wilkins.
Han, T., F. Mourtada, K. Kisling, J. Mikell, D. Followill, and R. Howell
(2012). “Experimental validation of deterministic Acuros XB algorithm
for IMRT and VMAT dose calculations with the Radiological Physics
Center’s head and neck phantom.” Med Phys 39.4, pp. 2193–2202.
Hissoiny, S., B. Ozell, and P. Després (2009). “Fast convolution-superposition
dose calculation on graphics hardware.” Med Phys 36.6, pp. 1998–2005.
Hissoiny, S., B. Ozell, and P. Després (2010). “A convolution-superposition
dose calculation engine for GPUs.” Med Phys 37.3, pp. 1029–1037.
Hubbell, J. H. and S. M. Seltzer (1996). Tables of X-ray Mass Attenuation
Coefficients and Mass Energy-Absorption Coefficients from 1 keV to 20
MeV for Elements Z = 1 to 92 and 48 Additional Substances of Dosimetric
Interest. URL: http://physics.nist.gov/PhysRefData/XrayMassCoef/
cover.html.
Humm, J. L., J. C. Roeske, D. R. Fisher, and G. T. Chen (1993). “Microdosi-
metric concepts in radioimmunotherapy”. Med Phys 20.2 Pt 2, pp. 535–
541.
Hutton, B. F., I. Buvat, and F. J. Beekman (2011). “Review and current
status of SPECT scatter correction.” Phys Med Biol 56.14, R85–112.
ICRU (1988). Fundamental quantities and units for ionizing radiation
ICRU Publication 60. Bethesda, MD: International Commission on Ra-
diation Units and Measurements.
49
REFERENCES
Jackson, P. A., J.-M. Beauregard, M. S. Hofman, T. Kron, A. Hogg, and R.
J. Hicks (2013). “An automated voxelized dosimetry tool for radionuclide
therapy based on serial quantitative SPECT/CT imaging.” Med Phys
40.11, p. 112503.
Jacques, R., J. Wong, R. Taylor, and T. McNutt (2011). “Real-time dose
computation: GPU-accelerated source modeling and superposition/ con-
volution.” Med Phys 38.1, pp. 294–305.
Jia, X., X. Gu, Y. J. Graves, M. Folkerts, and S. B. Jiang (2011). “GPU-
based fast Monte Carlo simulation for radiotherapy dose calculation.”
Phys Med Biol 56.22, pp. 7017–7031.
Jia, X., P. Ziegenhein, and S. B. Jiang (2014). “GPU-based high-performance
computing for radiation therapy.” Phys Med Biol 59.4, R151–R182.
Jiang, S. B., A. L. Boyer, and C. M. Ma (2001). “Modeling the extrafocal
radiation and monitor chamber backscatter for photon beam dose calcu-
lation.” Med Phys 28.1, pp. 55–66.
Kawrakow, I. and M. Fippel (2000). “VMC++, a fast MC algorithm for Ra-
diation Treatment planning”. The Use of Computers in Radiation Ther-
apy. Ed. by W. Schlegel and T. Bortfeld. Springer Berlin Heidelberg,
pp. 126–128.
Kletting, P., S. Schimmel, H. A. Kestler, H. Hänscheid, M. Luster, M.
Fernez, J. H. Bröer, D. Nosske, M. Lassmann, and G. Glatting (2013).
“Molecular radiotherapy: the NUKFIT software for calculating the time-
integrated activity coefficient.” Med Phys 40.10, p. 102504.
Kolbert, K. S., G Sgouros, A. M. Scott, J. E. Bronstein, R. A. Malane, J
Zhang, H Kalaigian, S McNamara, L Schwartz, and S. M. Larson (1997).
“Implementation and evaluation of patient-specific three-dimensional
internal dosimetry”. J Nucl Med 38.2, pp. 301–308.
Kotiluoto, P., J. Pyyry, and H. Helminen (2007). “MultiTrans SP3 code
in coupled photon-electron transport problems”. Radiation Physics and
Chemistry 76, pp. 9–14.
Leichner, P. K., K. F. Koral, R. J. Jaszczak, A. J. Green, G. T. Chen, and
J. C. Roeske (1993). “An overview of imaging techniques and physical
aspects of treatment planning in radioimmunotherapy”. Med Phys 20.2
Pt 2, pp. 569–577.
Leichner, P. (1994). “A unified approach to photon and beta particle dosime-
try”. J Nucl Med 35, pp. 1721–1729.
Lemaréchal, Y., J. Bert, C. Falconnet, P. Després, A. Valeri, U. Schick, O.
Pradier, M.-P. Garcia, N. Boussion, and D. Visvikis (2015). “GGEMS-
50
REFERENCES
Brachy: GPU GEant4-based Monte Carlo simulation for brachytherapy
applications.” Phys Med Biol 60.13, pp. 4987–5006.
Liu, H. H., T. R. Mackie, and E. C. McCullough (1997). “A dual source
photon beam model used in convolution/superposition dose calculations
for clinical megavoltage x-ray beams.” Med Phys 24.12, pp. 1960–1974.
Liu, H. H., T. R. Mackie, and E. C. McCullough (2000). “Modeling pho-
ton output caused by backscattered radiation into the monitor chamber
from collimator jaws using a Monte Carlo technique.” Med Phys 27.4,
pp. 737–744.
Liu, H.-W., Z. Nugent, R. Clayton, P. Dunscombe, H. Lau, and R. Khan
(2014). “Clinical impact of using the deterministic patient dose calcula-
tion algorithm Acuros XB for lung stereotactic body radiation therapy.”
Acta Oncol 53.3, pp. 324–329.
Ljungberg, M., M. King, G. Hademenos, and S. Strand (1994). “Compari-
son of four scatter correction methods using monte carlo simulated source
distributions”. J Nucl Med 35, pp. 143–151.
Ljungberg, M., K. Sjögreen, X. Liu, E. Frey, Y. Dewaraja, and S.-E. Strand
(2002). “A 3-dimensional absorbed dose calculation method based on
quantitative SPECT for radionuclide therapy: evaluation for (131)I us-
ing monte carlo simulation.” J Nucl Med 43.8, pp. 1101–1109.
Lo, S. S., A. J. Fakiris, E. L. Chang, N. A. Mayr, J. Z. Wang, L. Papiez,
B. S. Teh, R. C. McGarry, H. R. Cardenes, and R. D. Timmerman (2010).
“Stereotactic body radiation therapy: a novel treatment modality.” Nat
Rev Clin Oncol 7.1, pp. 44–54.
Loudos, G., I. Tsougos, S. Boukis, N. Karakatsanis, P. Georgoulias, K.
Theodorou, K. Nikita, and C. Kappas (2009). “A radionuclide dosime-
try toolkit based on material-specific Monte Carlo dose kernels.” Nucl
Med Commun 30.7, pp. 504–512.
Lubberink, M., H. Lundqvist, J. E. Westlin, V. Tolmachev, H. Schneider,
A. Lövqvist, A. Sundin, and J. Carlsson (1999). “Positron emission to-
mography and radio-immunotargeting – aspects of quantification and
dosimetry.” Acta Oncol 38.3, pp. 343–349.
Lundqvist, H., M. Lubberink, V. Tolmachev, A. Lövqvist, A. Sundin, S. Be-
shara, A. Bruskin, J. Carlsson, and J. E. Westlin (1999). “Positron emis-
sion tomography and radioimmunotargeting–general aspects.” Acta On-
col 38.3, pp. 335–341.
51

REFERENCES
Ma, C. M., E. Mok, A. Kapur, T. Pawlicki, D. Findley, S. Brain, K. Forster,
and A. L. Boyer (1999). “Clinical implementation of a Monte Carlo treat-
ment planning system.” Med Phys 26.10, pp. 2133–2143.
Macey, D. J., E. J. Grant, J. E. Bayouth, H. B. Giap, S. J. Danna, R. Siris-
riro, and D. A. Podoloff (1995). “Improved conjugate view quantitation
of I-131 by subtraction of scatter and septal penetration events with a
triple energy window method.” Med Phys 22.10, pp. 1637–1643.
Mackie, T. R., J. W. Scrimger, and J. J. Battista (1985). “A convolution
method of calculating dose for 15-MV x rays.” Med Phys 12.2, pp. 188–
196.
Mackie, T. R., A. F. Bielajew, D. W. Rogers, and J. J. Battista (1988). “Gen-
eration of photon energy deposition kernels using the EGS Monte Carlo
code.” Phys Med Biol 33.1, pp. 1–20.
Marcatili, S., C. Pettinato, S. Daniels, G. Lewis, P. Edwards, S. Fanti, and
E. Spezi (2013). “Development and validation of RAYDOSE: a Geant4-
based application for molecular radiotherapy.” Phys Med Biol 58.8, pp. 2491–
2508.
Mohan, R. and C. S. Chui (1987). “Use of fast Fourier transforms in calcu-
lating dose distributions for irregularly shaped fields for three-dimensional
treatment planning.” Med Phys 14.1, pp. 70–77.
Mohan, R., C. Chui, and L. Lidofsky (1985). “Energy and angular distri-
butions of photons from medical linear accelerators.” Med Phys 12.5,
pp. 592–597.
Nath, R., L. L. Anderson, G. Luxton, K. A. Weaver, J. F. Williamson, and
A. S. Meigooni (1995). “Dosimetry of interstitial brachytherapy sources:
recommendations of the AAPM Radiation Therapy Committee Task Group
No. 43. American Association of Physicists in Medicine.” Med Phys 22.2,
pp. 209–234.
Neuenschwander, H., T. R. Mackie, and P. J. Reckwerdt (1995). “MMC–a
high-performance Monte Carlo code for electron beam treatment plan-
ning.” Phys Med Biol 40.4, pp. 543–574.
Ojala, J. (2014). “Monte Carlo Simulations in Quality Assurance of Dosime-
try and Clinical Dose Calculations in Radiotherapy”. PhD thesis. Tam-
pere University of Technology.
Ojala, J. J., M. K. Kapanen, S. J. Hyödynmaa, T. K. Wigren, and M. A.
Pitkänen (2014). “Performance of dose calculation algorithms from three
generations in lung SBRT: comparison with full Monte Carlo-based dose
distributions.” J Appl Clin Med Phys 15.2, p. 4662.
52

REFERENCES
Ott, R. J. (1996). “Imaging technologies for radionuclide dosimetry”. Phys
Med Biol 41.10, pp. 1885–1894.
Ouyang, J., G. El Fakhri, and S. C. Moore (2007). “Fast Monte Carlo based
joint iterative reconstruction for simultaneous 99mTc/ 123I SPECT imag-
ing.” Med Phys 34.8, pp. 3263–3272.
Petrokokkinos, L., K. Zourari, E. Pantelis, A. Moutsatsos, P. Karaiskos,
L. Sakelliou, I. Seimenis, E. Georgiou, and P. Papagiannis (2011). “Dosi-
metric accuracy of a deterministic radiation transport based 192Ir brachy-
therapy treatment planning system. Part II: Monte Carlo and experi-
mental verification of a multiple source dwell position plan employing a
shielded applicator.” Med Phys 38.4, pp. 1981–1992.
Poon, E., J. F. Williamson, T. Vuong, and F. Verhaegen (2008). “Patient-
specific Monte Carlo dose calculations for high-dose-rate endorectal brachy-
therapy with shielded intracavitary applicator.” Int J Radiat Oncol Biol
Phys 72.4, pp. 1259–1266.
Pouget, J.-P., C. Lozza, E. Deshayes, V. Boudousq, and I. Navarro-Teulon
(2015). “Introduction to radiobiology of targeted radionuclide therapy.”
Front Med (Lausanne) 2, p. 12.
Pratx, G. and L. Xing (2011). “GPU computing in medical physics: a re-
view.” Med Phys 38.5, pp. 2685–2697.
Prideaux, A. R., H. Song, R. F. Hobbs, B. He, E. C. Frey, P. W. Laden-
son, R. L. Wahl, and G. Sgouros (2007). “Three-dimensional radiobiologic
dosimetry: application of radiobiologic modeling to patient-specific 3-
dimensional imaging-based internal dosimetry.” J Nucl Med 48.6, pp. 1008–
1016.
Reiner, D., M. Blaickner, and F. Rattay (2009). “Discrete beta dose ker-
nel matrices for nuclides applied in targeted radionuclide therapy (TRT)
calculated with MCNP5”. Med Phys 36.11, pp. 4890–4896.
Rivard, M. J., B. M. Coursey, L. A. DeWerd, W. F. Hanson, M. S. Huq,
G. S. Ibbott, M. G. Mitch, R. Nath, and J. F. Williamson (2004). “Up-
date of AAPM Task Group No. 43 Report: A revised AAPM protocol for
brachytherapy dose calculations.” Med Phys 31.3, pp. 633–674.
Rogers, D. W., B. A. Faddegon, G. X. Ding, C. M. Ma, J. We, and T. R.
Mackie (1995). “BEAM: a Monte Carlo code to simulate radiotherapy
treatment units.” Med Phys 22.5, pp. 503–524.
Rogers, D. W. O. (2006). “Fifty years of Monte Carlo simulations for medi-
cal physics.” Phys Med Biol 51.13, R287–R301.
53

REFERENCES
Seco, J. and P. M. Evans (2006). “Assessing the effect of electron density
in photon dose calculations.” Med Phys 33.2, pp. 540–552.
Sgouros, G., G. Barest, J. Thekkumthala, C. Chui, R. Mohan, R. E. Bigler,
and P. B. Zanzonico (1990). “Treatment planning for internal radionu-
clide therapy: three-dimensional dosimetry for nonuniformly distributed
radionuclides.” J Nucl Med 31.11, pp. 1884–1891.
Sgouros, G., S. Chiu, K. S. Pentlow, L. J. Brewster, H. Kalaigian, B. Bald-
win, F. Daghighian, M. C. Graham, S. M. Larson, and R. Mohan (1993).
“Three-dimensional dosimetry for radioimmunotherapy treatment plan-
ning”. J Nucl Med 34.9, pp. 1595–1601.
Sheikh-Bagheri, D. and D. W. O. Rogers (2002a). “Monte Carlo calculation
of nine megavoltage photon beam spectra using the BEAM code.” Med
Phys 29.3, pp. 391–402.
Sheikh-Bagheri, D. and D. W. O. Rogers (2002b). “Sensitivity of megavolt-
age photon beam Monte Carlo simulations to electron beam and other
parameters.” Med Phys 29.3, pp. 379–390.
Stabin, M. G., R. B. Sparks, and E. Crowe (2005). “OLINDA/EXM: the
second-generation personal computer software for internal dose assess-
ment in nuclear medicine.” J Nucl Med 46.6, pp. 1023–1027.
Storchi, P. and E. Woudstra (1996). “Calculation of the absorbed dose dis-
tribution due to irregularly shaped photon beams using pencil beam ker-
nels derived form basic beam data.” Phys Med Biol 41.4, pp. 637–656.
Storchi, P. R., L. J. van Battum, and E. Woudstra (1999). “Calculation of
a pencil beam kernel from measured photon beam data.” Phys Med Biol
44.12, pp. 2917–2928.
Strand, S. E., P. Zanzonico, and T. K. Johnson (1993a). “Pharmacokinetic
modeling”. Med Phys 20.2 Pt 2, pp. 515–527.
Strand, S. E., B. A. Jönsson, M. Ljungberg, and J. Tennvall (1993b). “Ra-
dioimmunotherapy dosimetry–a review.” Acta Oncol 32.7-8, pp. 807–
817.
Tagesson, M., M. Ljungberg, and S. E. Strand (1996). “A Monte-Carlo pro-
gram converting activity distributions to absorbed dose distributions in
a radionuclide treatment planning system.” Acta Oncol 35.3, pp. 367–
372.
Tedgren, A. K. C. and A. Ahnesjö (2003). “Accounting for high Z shields in
brachytherapy using collapsed cone superposition for scatter dose calcu-
lation.” Med Phys 30.8, pp. 2206–2217.
54

REFERENCES
Tillikainen, L., S. Siljamäki, H. Helminen, J. Alakuijala, and J. Pyyry
(2007). “Determination of parameters for a multiple-source model of
megavoltage photon beams using optimization methods.” Phys Med Biol
52.5, pp. 1441–1467.
Tillikainen, L. (2009). “Methods for Dose Calculation and Beam Charac-
terization in External Photon Beam Radiotherapy”. PhD thesis. Aalto
University.
Traino, A. C., S. Marcatili, C. Avigo, M. Sollini, P. A. Erba, and G. Mariani
(2013). “Dosimetry for nonuniform activity distributions: a method for
the calculation of 3D absorbed-dose distribution without the use of voxel
S-values, point kernels, or Monte Carlo simulations.” Med Phys 40.4,
p. 042505.
Tsuruta, Y., M. Nakata, M. Nakamura, Y. Matsuo, K. Higashimura, H.
Monzen, T. Mizowaki, and M. Hiraoka (2014). “Dosimetric comparison
of Acuros XB, AAA, and XVMC in stereotactic body radiotherapy for
lung cancer.” Med Phys 41.8, p. 081715.
Tuszynski, J. (2010). Mass Attenuation Coefficient of Iron with contribu-
tions sources of attenuation. Data from XCOM database. URL: http://
commons.wikimedia.org/wiki/File:Ironattenuation.PNG..
Van Esch, A., L. Tillikainen, J. Pyykkonen, M. Tenhunen, H. Helminen,
S. Siljamäki, J. Alakuijala, M. Paiusco, M. Lori, and D. P. Huyskens
(2006). “Testing of the analytical anisotropic algorithm for photon dose
calculation.” Med Phys 33.11, pp. 4130–4148.
Vassiliev, O. N., T. A. Wareing, J. McGhee, G. Failla, M. R. Salehpour, and
F. Mourtada (2010). “Validation of a new grid-based Boltzmann equation
solver for dose calculation in radiotherapy with photon beams.” Phys
Med Biol 55.3, pp. 581–598.
Verhaegen, F., R. Symonds-Tayler, H. H. Liu, and A. E. Nahum (2000).
“Backscatter towards the monitor ion chamber in high-energy photon
and electron beams: charge integration versus Monte Carlo simulation.”
Phys Med Biol 45.11, pp. 3159–3170.
Watson, E. E., M. G. Stabin, and J. A. Siegel (1993). “MIRD formulation”.
Med Phys 20.2 Pt 2, pp. 511–514.
WHO (2015). Cancer, Fact sheet No. 297. World Health Organization. URL:
http://www.who.int/mediacentre/factsheets/fs297/en/.
Williams, L. E., G. L. DeNardo, and R. F. Meredith (2008). “Targeted ra-
dionuclide therapy.” Med Phys 35.7, pp. 3062–3068.
55

REFERENCES
Willowson, K., D. L. Bailey, and C. Baldock (2008). “Quantitative SPECT
reconstruction using CT-derived corrections.” Phys Med Biol 53.12, pp. 3099–
3112.
Wong, E., Y. Zhu, and J. Van Dyk (1996). “Theoretical developments on
fast Fourier transform convolution dose calculations in inhomogeneous
media.” Med Phys 23.9, pp. 1511–1521.
Zourari, K., E. Pantelis, A. Moutsatsos, L. Petrokokkinos, P. Karaiskos, L.
Sakelliou, E. Georgiou, and P. Papagiannis (2010). “Dosimetric accuracy
of a deterministic radiation transport based 192Ir brachytherapy treat-
ment planning system. Part I: single sources and bounded homogeneous
geometries.” Med Phys 37.2, pp. 649–661.
Zweit, J. (1996). “Radionuclides and carrier molecules for therapy”. Phys
Med Biol 41.10, pp. 1905–1914.
56

Errata
Publication IV
The caption in Figure 2. is truncated and the full caption should read as:
Regions of interest used to determine the biological clearance of the In-
111-labelled MoAb are shown. The body contours are taken on purpose
from another imaging to demonstrate that each imaging session may be
individual for body contour drawing.
57

Radiotherapy is an established treatment modality of cancer where radiation is delivered to the patients from internal or external sources. This thesis explores and introduces improvements to computational methods that are used in the application of internal and external radiotherapy. The summary discusses radiotherapy planning and reviews model-based dose calculation methods in internal and external radiotherapy. Treatment planning methods of internal radionuclide therapy are devloped and applied to analyze radionuclide therapy cases. The thesis also reports on the development of a pencil-beam dose kernel -based calculation method for external photon therapy that also accounts for local variations in tissue material densities in 3D space.
Aalto-D
D 57
/2016
9HSTFMG*aghchi+
ISBN 978-952-60-6727-8 (printed) ISBN 978-952-60-6728-5 (pdf) ISSN-L 1799-4934 ISSN 1799-4934 (printed) ISSN 1799-4942 (pdf) Aalto University School of Science Department of Neuroscience and Biomedical Engineering www.aalto.fi
BUSINESS + ECONOMY ART + DESIGN + ARCHITECTURE SCIENCE + TECHNOLOGY CROSSOVER DOCTORAL DISSERTATIONS
Joakim P
yyry C
onvolution and model-based dose calculation m
ethods in radionuclide and external-beam photon therapy
Aalto
Unive
rsity
2016
Department of Neuroscience and Biomedical Engineering
Convolution and model-based dose calculation methods in radionuclide and external-beam photon therapy
Joakim Pyyry
DOCTORAL DISSERTATIONS