control of renal function. learning objectives know the effects of aldosterone, angiotensin ii and...
TRANSCRIPT

Control of Renal Function

Learning Objectives
• Know the effects of aldosterone, angiotensin II and antidiuretic hormone on kidney function.
• Understand what happens when extracellular K+ becomes elevated and how this is regulated.
• Know how the kidneys help regulate Ca2+ levels.• Understand the molecular of the diuretics
presented in lecture.

Review of Aldosterone
Acts primarily on the principle cells of thecortical collecting tubules.Stimulates Na+/K+-ATPase.This increases Na+ reabsorption and K+ secretion.

Review of Angiotensin II
• Powerful Na+-retaining hormone.- Stimulates aldosterone- Constricts efferent arterioles.
- Reduces peritubular capillary hydrostatic pressure.
- Increase the filter fraction.
- Stimulates Na+/K+-ATPase in the proximal tubules, loops of Henle, distal tubules, and the collecting tubules.
• As discussed last time, angiotensin II is important in pressure diuresis and natriuresis.

Review of ADH
• Conrols H2O reabsorption or excretion.
- Acts by increasing the H2O permeability of the distal tubule and collecting tubules.- Increase urea permeability in the medullary collecting tubule.
Helps conserve H2O during dehydration.

Potassium

Changing K+
It is very important to keep extracellular K+ regulated

Regulating K+
• The intracellular fluid can act as a buffer, by taking up or releasing K+.
• Some factors that increase the uptake of K+ into cells are:
insulin, aldosterone and alpha-adrenergic stimulation
• Some factors that increase the release of K+ from cells are:Strenuous exercise (release for muscle), cell lysis and blocking the actions of insulin, aldosterone, alpha-adrenergic stimulation.

Renal Control of K+
• Proximal tubule and ascending loop of Henle reabsorb large amounts of K+. This level of reabsorption does not normally change much.
• Most regulation of K+ is done in the late distal tubule and cortical collecting tubule. There, K+ can be reabsorbed or secreted at varying degrees.

K+ Secretion in the Principal Cells• Principal cells make up ~ 90% of
the epithelial cells in the late distal tubule and cortical collecting tubule.
• These cells can secrete a large amount of K+.
• When K+ is high, the rate of K+ secretion in the principal cells is high.
• When K+ is low, the rate of secretion is low. Then, the rate of K+ reabsorption by the intercalated cells can exceed the secretion rate by the proximal cells.
• What hormone controls the rate of K+ secretion in the principal cells?
Regulation of K+ Secretion
• Increased extracellular K+ causes:- An increase in Na+/K+-ATPase activity in the
principal cells.- An increase in aldosterone.
- This further increases Na+/K+-ATPase activity and increases permeability of the luminal membrane of epithelial cells.
- Aldosterone increases reabsorption of Na+ and H2O, but increases the excretion of K+.

Acidosis and K+ Levels
• Acute increases in H+ inhibits the Na+/K+-ATPase in the principal cells.
• What does this do to K+ secretion?- Decreases secretion
• What does decreased secretion do to extracellular K+ levels?- Increases extracellular K+

Renal Regulation of Ca2+
In the kidneys, parathyroid hormone:*Stimulates the reabsorption of Ca2+ in the thick ascending loop of Henle and distal tubules.*Stimulates the conversion of vitamin D to a more active form (vitamin D increases Ca2+
absorption from the small intestines.).

Practice Question
• If a person does not secrete enough aldosterone (Addison’s Disease), what do you expect to happen to the body’s level of Na+, H2O, and K+?
Diuretics
• Diuretics increase the rate of urine output.
• Most act by decreasing the rate of Na+ reabsorption.
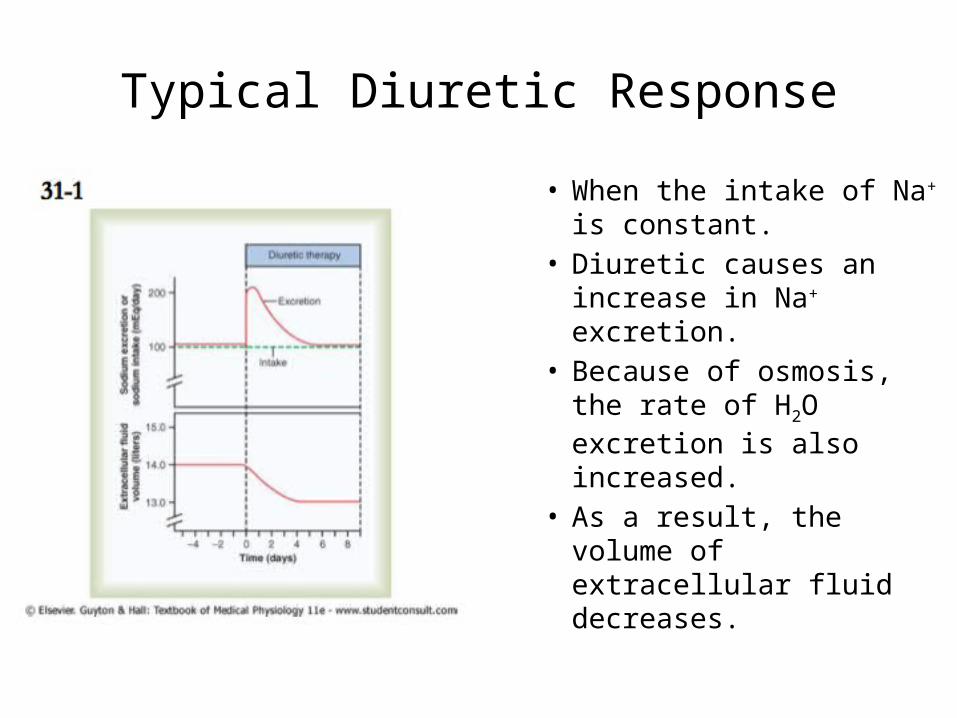
Typical Diuretic Response
• When the intake of Na+ is constant.
• Diuretic causes an increase in Na+ excretion.
• Because of osmosis, the rate of H2O excretion is also increased.
• As a result, the volume of extracellular fluid decreases.

Typical Diuretic Response
• Why does the rate of Na+ excretion decrease after a few days?
• Other mechanisms are activated, e.g., a decreased arterial pressure (from less blood volume) would cause an increase in angiotensin II. This would increase the GFR and reabsorption of Na+.

“Loop” Diuretics
• “Loop” diuretics (e.g., furosemide (Lasix)) inhibit the Na+/2Cl-/K+ cotransporter in the thick ascending loop of Henle.
• This decreases the reabsorption of Na+, Cl-, and K+. The extra ions in the tubular lumen osmotically increase the amount of H2O in the tubular lumen.
• What would Lasix do to the countercurrent mechanism?– - Decrease the reabsorption of
ions into the medullary interstitial fluid and thus decrease the effectiveness of the countercurrent mechanism. Know how this would affect renal function.
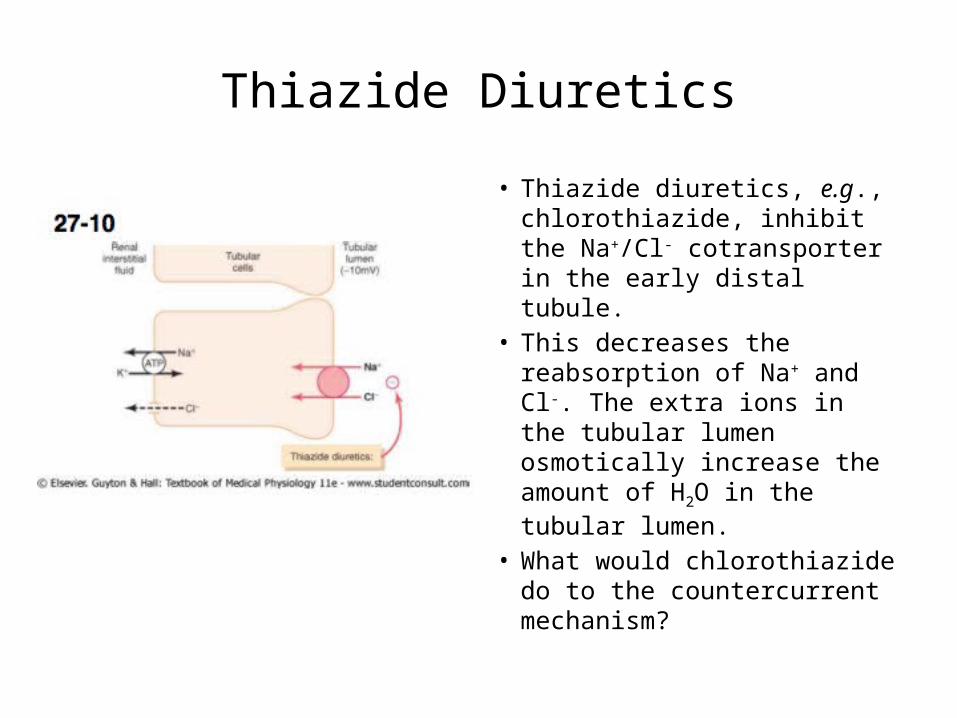
Thiazide Diuretics
• Thiazide diuretics, e.g., chlorothiazide, inhibit the Na+/Cl- cotransporter in the early distal tubule.
• This decreases the reabsorption of Na+ and Cl-. The extra ions in the tubular lumen osmotically increase the amount of H2O in the tubular lumen.
• What would chlorothiazide do to the countercurrent mechanism?

Competitive Inhibitors of Aldosterone
• Competitive inhibitors of aldosterone, e.g., spironolactone, inhibit aldosterone’s Na+/K+-ATPase in the cortical collecting tubule.
• This decreases the reabsorption of Na+ and the secretion of K+.
• Hence, these are called “K+-sparing” diuretics.

Na+ Channel Blockers
• Inhibition of Na+ channels in cortical collecting tubule, e.g., amiloride, decrease the reabsorption of Na+.