congenital heart defects and maternal fever: systematic review and meta-analysis
TRANSCRIPT

ORIGINAL ARTICLE
Congenital heart defects and maternal fever: systematic reviewand meta-analysisQY Shi1,8, JB Zhang2,8, YQ Mi3, Y Song4, J Ma5,9 and YL Zhang6,7,9
OBJECTIVE: To systematically review and meta-analyze the relation between maternal fever in the first trimester and congenitalheart defect (CHD) in offspring.STUDY DESIGN: We searched PubMed (1977–2012), Embase (1974–2012) and the Cochrane Library (2012) databases to identifyrelevant articles. Random effects model were performed, with the conduction of subgroup analysis.RESULT:Meta-analysis yielded a pooled odds ratio of 1.53 (95% confidence interval = 1.36 to 1.73) for the magnitude of the relationbetween maternal fever in the first trimester and CHD in offspring. As to subgroup analysis, it is associated with ventricular septaldefects (VSDs) and right obstructive defects.CONCLUSION: Our analysis suggests that maternal fever in the first trimester is the risk factor of congenital heart diseases inoffspring. Through the subgroup analysis, we find that exposure to maternal fever is the risk factor of VSD and right obstructivedefects.
Journal of Perinatology (2014) 34, 677–682; doi:10.1038/jp.2014.76; published online 8 May 2014
INTRODUCTIONCongenital heart defects (CHDs) are one of the most prevalent andserious birth defects, and they are the leading causes of death fromcongenital malformations.1–2 Many genetic and environmentalfactors that may relate to CHDs have been studied, but the causesof CHD are still unclear. Some reports have shown that increasedmaternal age at conception was associated with increased risk forCHD.3 About 1% of cardiovascular malformations can be attributedto maternal diseases, such as type 1 diabetes, phenylketonuria,epilepsy.4–6 Another 1% of cardiovascular malformations arecaused by teratogen exposure.7 Among these teratogens, maternalfever has been an important one. Maternal fever has been provedto associate with many birth defects, especially defects of thecentral nervous system.8–10 More recently, a number of studieshave sought to explore the association between maternal feverand CHD. Nonetheless, the results of individual studies weredifferent. For example, Botto et al.11 reported positive associationbetween maternal fever in the first trimester and CHD (odds ratio(OR) = 1.8, 95% confidence interval (CI) = 1.4–2.4), whereas Osteret al.12 showed insignificant association (OR=1.1, 95% CI = 0.9–1.4).In addition, the relation of maternal fever and the subtypes of CHDwere also variable. For instance, Botto et al.11 indicated a significantassociation between maternal fever and ventricular septal defect(VSD; OR=1.8, 95% CI = 1.1–2.9), whereas Oster et al.12 helddifferent opinion (OR= 1.12, 95% CI = 0.77–1.64). The results mightbe unreliable owing to the small sample size of subtypes of eachstudy, thus it is necessary to synthesize them to obtain a summary
point estimate. For above reasons, we systematically reviewed andmeta-analyzed the relation between maternal fever in the firsttrimester and CHD in offspring.
METHODSIdentification of studiesWe searched PubMed (1977–2012), Embase (1974–2012) and the CochraneLibrary (2012) databases to identify relevant articles. We examined thereference lists of all known primary and review articles to identify cited articlesnot captured by the electronic searches. Language restrictions were notapplied. A variable of the following search terms was used: (CHDs OR conge-nital heart disease OR congenital heart malformation OR congenital heartblock) AND (maternal fever OR maternal febrile OR maternal hyperthermiaOR maternal pyrexia OR (fever AND pregnancy) OR (febrile AND pregnancy)OR (hyperthermia AND pregnancy) OR (pyrexia AND pregnancy)). Besides,we also searched terms of (birth defects) AND (risk factors).
Inclusion and exclusion criteriaStudies were included in the meta-analysis when they met the followinginclusion criteria. Subject: Studies were included if they reported theassociations between maternal fever in the first trimester and CHDs inoffspring. Study design: Studies were included if they were case–controlstudies or cohort studies. Exposure: Studies were included if exposurerelated to fever or febrile illness with fever were clear and similar. Exposurewindow: Studies were included if exposure window was approximately inthe first trimester during pregnancy. Outcome: Studies were included if thediagnosis of CHDs in offspring were clearly presented and the diagnostic
1Tianjin Second People’s Hospital, School of Graduate, Tianjin Medical University, Tianjin, China; 2Tianjin Teda International Cardiovascular Disease Hospital, Clinical College ofCardiovascular, Tianjin Medical University, Tianjin, China; 3Depanment of Chinese Integrative Medicine, Tianjin Second People’s Hospital, Tianjin Medical University, Tianjin, China;4Coronary Care Unit, Tianjin Teda International Cardiovascular Disease Hospital, Clinical College of Cardiovascular, Tianjin Medical University, Tianjin, China; 5Department ofHealth Statistics, College of Public Health, Tianjin Medical University, Tianjin, China; 6Institute of Reproductive and Child Health/Ministry of Health Key Laboratory of ReproductiveHealth, School of Public Health, Peking University Health Science Center, Beijing, China and 7Department of Epidemiology and Biostatistics, School of Public Health, PekingUniversity, Beijing, China. Correspondence: Dr Jun Ma, Department of Health Statistics, College of Public Health, Tianjin Medical University, 22 Qi-Xiang-Tai Road, Tianjin 300070,China or Dr YL Zhang, Institute of Reproductive and Child Health/Ministry of Health Key Laboratory of Reproductive Health, School of Public Health, Peking University HealthScience Center, Beijing 100191, China.E-mail: [email protected] or [email protected] authors contributed equally to this work.9These authors contributed equally to this work.Received 5 November 2013; revised 27 February 2014; accepted 13 March 2014; published online 8 May 2014
Journal of Perinatology (2014) 34, 677–682© 2014 Nature America, Inc. All rights reserved 0743-8346/14
www.nature.com/jp

approach of cases and control groups were identical. Data: Studies wereincluded if we could get the information of OR and 95% CI.The electronic searches were scrutinized and two independent
reviewers (YL Zhang and QY Shi) examined titles and abstracts to decideif the full-text articles should be obtained (n= 75). We decided to get full 35reports of the 75 studies after looking through titles, abstracts andreferences. The decision to exclude any of these studies was made by theconsensus of two authors.Finally, four studies were excluded for the duplicate data from the same
study programs. Sixteen studies reporting influenza, infection, medication,sauna bathing and working temperature without the clear information offever were excluded. Eight studies were excluded as they reportedexposure window as the entire pregnancy period (Figure 1).
Quality assessmentStudy quality was assessed by two researchers (QY Shi and JB Zhang) usingNewcastle-Ottawa Scale on case–control studies.13 Three major compo-nents, that is, selection of case and controls (Selection), comparability ofcase and controls (Comparability) and ascertainment of exposure(Exposure), comprized the scale, including eight small items (four onSelection, one on Comparability and three for Exposure). A study can beawarded a maximum of one * for each numbered item within the Selectionand Exposure categories. A maximum of two * can be given forComparability. Where reviewers disagreed, specific criteria were discussedwith a third reviewer until consensus was reached.
Data extraction proceduresTwo reviewers (QY Shi and JB Zhang) independently extracted basicinformation in a standardized manner: first author, year, data acquisition
(period), CHD infants/fever mothers, CHD infants/non-fever mothers andinterview time. Data on information of exposure, diagnosis of outcomesand detailed information of subtypes of CHD were collected.
Statistical analysisThe main outcome in this analysis was the OR and its 95% CI. We pooledthe ORs depending on the heterogeneity. Heterogeneity was evaluatedgraphically with forest plots and statistically with χ2 and I2 tests. I2 is anestimate of the proportion of total variation in study estimates that is dueto heterogeneity. I2>25% indicate significant heterogeneity. The fixedeffects model was used to estimate the variance of the summary OR whenstudy heterogeneity was low and the random effects model when studyheterogeneity was moderate to high. We also count the weight of eachstudy according to the formula: wi = (1/ai+1/bi+1/ci+1/di)
-1. All analyseswere conducted with Stata statistical software (version 11; Stata Corp LD,College Station, TX, USA).
RESULTSStudies included in meta-analysisIn this analysis, seven studies involving 12 030 cases and 51 729controls were included.11–12,14–18 All the seven studies wereretrospective studies, and they were published from 1989 to 2011.Four of seven studies were conducted in America.11–12,14,18 Therest of the three were, respectively, conducted in Hungary,17
Finland15 and China.16 Four of seven had reported different kindsof CHDs in detail.11,12,15,18 All had reported diagnostic methodsof CHD and five had declared diagnostic time around 1yearold.11–12,14–15,17 The information of exposure, diagnostic informa-tion and subtypes of CHD are shown in Tables 1,2 andSupplementary Table 1, respectively. The assessment of the studyquality was available in Table 3.
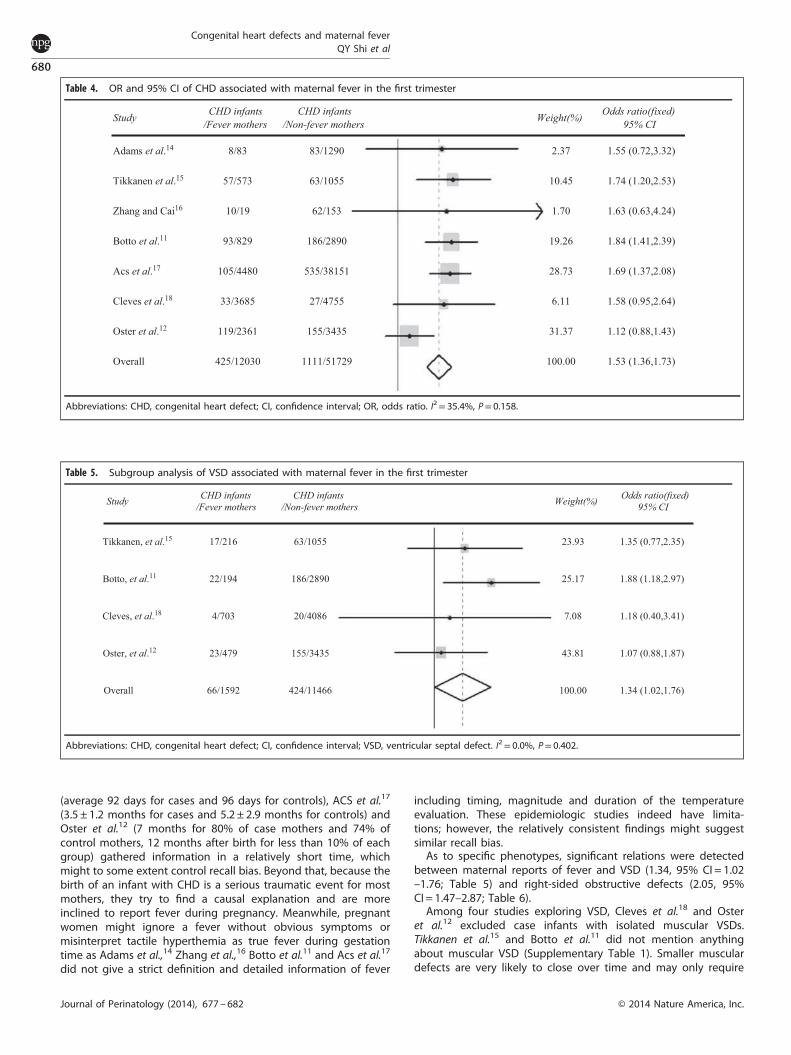
The association between CHD and maternal feverTable 4 shows the pooled estimate of the association betweennon-classified CHD and maternal fever in the first trimestergenerated by meta-analysis for all the seven studies combined.The pooled estimate for all seven studies combined was 1.53(95% CI = 1.36–1.73). There was unobvious heterogeneity inwomen with maternal fever (I2 = 35.4%). There was no significantheterogeneity among the studies (P= 0.158).
Influence of individual studiesWe observed the shift of point estimate and 95% CI from themiddle line through removing individual studies to analyze theinfluence of each study (Supplementary Figure 1). The pooled ORchanged more or less when excluding any study from our meta-analysis. The results indicated that study by Oster et al. moved thefarthest from the middle line, thus proving to be the mostinfluential study of pooled size effect.Figure 1. Flow chart of meta-analysis
Table 1. Exposure and exposure window of seven studies
Study Exposure Exposure window
Adams et al.14 Fever From the month before conception to the third month of gestationTikkanen et al.15 Fever exceeding 38°C During the first trimester of pregnancyZhang and Cai16 Cold with fever During the first trimester of pregnancyBotto et al.11 Any source of fever and specific source of fever From 1 month before conception to the third month of pregnancyAcs et al.17 Flu with fever during epidemic months (between
December and April) in epidemic and nonepidemicyears
During the second and third month of pregnancy
Cleves et al.18 Urinary tract infection with fever (above 101°F) During the first trimester of pregnancyOster et al.12 Fever of 101°F or higher (⩾38.3°C) From 3 months before pregnancy to the end of the first trimester of
pregnancy
Congenital heart defects and maternal feverQY Shi et al
678
Journal of Perinatology (2014), 677 – 682 © 2014 Nature America, Inc.

Subgroup analysisAlthough the heterogeneity of the seven studies was low, wecould not rule out the possibility that they canceled out with eachother. And considering etiological difference of various CHD, weconducted subgroup analysis of CHD. The common classificationof CHD include VSD, atrial septal defect (ASD), atrioventricularseptal defect, conotruncal defects, Ebstein anomaly, anomalouspulmonary venous return, right obstructive defects, left obstruc-tive defects and so on. Supplementary Table 1 shows thephenotypes of CHD in each study. We confirmed any sort ofCHD above as a subgroup if at least three studies reported theassociation between it and maternal fever and in each study atleast three cases were reported for this disease. Finally, we definedfive subgroups: VSD, ASD, conotruncal defects, right obstructivedefects and left obstructive. The associations of fever with cardiacphenotypes are outlined in Tables 5, 6, Supplementary Tables 2, 3and 4. The aggregated OR associated with maternal fever in thefirst trimester for VSD in offspring was 1.34 (95% CI = 1.02–1.76),1.46 (95% CI = 0.95–2.23) for ASD, 1.22 (95% CI = 0.91–1.63) forconotruncal defects, 2.05 (95%CI = 1.47–2.87) for right obstructivedefects and 1.32 (95% CI = 0.88–1.96) for left obstructive defects.There was significant unexplained heterogeneity for studies forchildren with ASD (I2 = 61.7%, P= 0.050) and left obstructivedefects (I2 = 82.4%, P= 0.003). There was no evidence of hetero-geneity for studies in children with VSD, conotruncal defects andright obstructive defects (I2 = 0%).
Publication bias analysisWe conducted Begg’s funnel plot and Egger’s correspondingasymmetry test for the eight studies. Egger’s test provided littleevidence of publication bias (P= 0.914).
DISCUSSIONThis is the first meta-analysis review of association betweenmaternal fever in the first trimester and CHD in offspring. Thestudies of the association between maternal fever and birthdefects in offspring date back to the beginning of last century. Anobstetrician found that the number of neonates with birth defectsincreased significantly after global pandemic influenza in 1918,and almost all women delivering those babies had had the flu.19 Inthose studies of the association between maternal fever and birthdefects in offspring, neural tube defects are the most studiedabout birth defects.8–10 A systematic review and meta-analysisabout published literature from 1980 to 2003 regarding maternalfever and neural tube defects suggested that the odds of childrenwith neural tube defects when their mother had maternalinfluenza or fever during pregnancy was 1.92 (95% CI = 1.61–-2.29).8 However, the studies on association between maternalfever in the first trimester and CHD in offspring are far less thanthe neural tube defects. Our systematic review and meta-analysisof the published literature showed that in women who hadexperienced fever in the first trimester of their pregnancy, therewas a significant association between maternal fever and CHD inaggregate (OR= 1.53, 95% CI = 1.36–1.73; Table 4). In addition, forspecific heart defects, significant relations were detected betweenmaternal reports of fever and VSD (OR= 1.34, 95% CI = 1.02–-1.76; Table 5) and right-sided obstructive defects (OR= 2.05, 95%CI = 1.47–2.87; Table 6).Because all of the seven studies were retrospective, it is
necessary to evaluate their potential recall bias. Generally, therewere several means to control recall bias, such as elaboratedprotocols or objective indicators. In seven studies, Adams et al.14
conducted interviews for more than 3 years after conception, sorespondents might have failed to recall whether they hadexperienced fever or which medications they had used, the sameas Botto et al.11 (2–12 years ) and Cleves et al.18 (6 weeksto 24 months). Zhang et al.16 (soon after delivery), Tikkanen et al.15
Table 2. Diagnostic characteristics of seven studies
Study Congenital heart defects Diagnostic time Diagnostic methods
Adams et al.14 Conotruncal defects During their first year of life By the Metropolitan Atlanta CongenitalDefects Program
Tikkanen et al.15 VSD, ASD, CAS, LHHS, ECD, other defects Before 1 year of age Cardiac catheterization, ultrasound,sugery or autopsy
Zhang and Cai16 All defects and VSD Before 8 days after birth By pediatricians or pathologist who hadno knowledge of maternal cold history
Botto et al.11 Outflow tract defects, VSD, ASD, AVSD,Ebstein anomaly, anomalous pulmonaryvenous return, all right obstructive defectgs,all left obstructive defects
During the first year of life An anatomic diagnosis and an overallclinical diagnosis
Acs et al.17 All defects From the second trimesterof pregnancy to the end ofthe first postnatal year
Be identified in the Hungarian CongentialAbnormality Registry (HCAR)
Cleves et al.18 Conotruncal defects, VSD, ASD, AVSD,right-sided obstructive defects, left-sidedobstructive defects, anomalous pulmonaryvenous return
Not mention Echocardiogram, heart catheterization, orsurgical or autopsy report
Oster et al.12 VSD, ASD, AVSD, Ebstein anomaly, right-sidedobstructive defects, left-sided obstructive defects,total anomalous pulmonary venous return
By 1 year of age Echocardiography, catheterization, surgery,or autopsy
Abbreviations: ASD, atrial septal defect; AVSD, atrioventricular septal defect; CAS, conus arterious; ECD, endocardial cushion defect; LHHS, left hearthypoplastic syndrome; VSD, ventricular septal defect.
Table 3. Quality ratings of seven studies
Study Selection Comparability Exposure
Adams et al.14 ★★★★ ★★ ★★★Tikkanen et al.15 ★★★ ★ ★★Zhang and Cai16 ★★★ ★ ★★Botto et al.11 ★★★★ ★★ ★★★Acs et al.17 ★★★★ ★★ ★★★Cleves et al.18 ★★★★ ★★ ★★★Oster et al.12 ★★★★ ★★ ★★★
Congenital heart defects and maternal feverQY Shi et al
679
© 2014 Nature America, Inc. Journal of Perinatology (2014), 677 – 682
(average 92 days for cases and 96 days for controls), ACS et al.17
(3.5 ± 1.2 months for cases and 5.2 ± 2.9 months for controls) andOster et al.12 (7 months for 80% of case mothers and 74% ofcontrol mothers, 12 months after birth for less than 10% of eachgroup) gathered information in a relatively short time, whichmight to some extent control recall bias. Beyond that, because thebirth of an infant with CHD is a serious traumatic event for mostmothers, they try to find a causal explanation and are moreinclined to report fever during pregnancy. Meanwhile, pregnantwomen might ignore a fever without obvious symptoms ormisinterpret tactile hyperthemia as true fever during gestationtime as Adams et al.,14 Zhang et al.,16 Botto et al.11 and Acs et al.17
did not give a strict definition and detailed information of fever
including timing, magnitude and duration of the temperatureevaluation. These epidemiologic studies indeed have limita-tions; however, the relatively consistent findings might suggestsimilar recall bias.As to specific phenotypes, significant relations were detected
between maternal reports of fever and VSD (1.34, 95% CI = 1.02–1.76; Table 5) and right-sided obstructive defects (2.05, 95%CI = 1.47–2.87; Table 6).Among four studies exploring VSD, Cleves et al.18 and Oster
et al.12 excluded case infants with isolated muscular VSDs.Tikkanen et al.15 and Botto et al.11 did not mention anythingabout muscular VSD (Supplementary Table 1). Smaller musculardefects are very likely to close over time and may only require
Table 4. OR and 95% CI of CHD associated with maternal fever in the first trimester
Study CHD infants/Fever mothers
CHD infants/Non-fever mothers Weight(%) Odds ratio(fixed)
95% CI
Adams et al.14 8/83 83/1290 2.37 1.55 (0.72,3.32)
Tikkanen et al.15 57/573 63/1055 10.45 1.74 (1.20,2.53)
Zhang and Cai16 10/19 62/153 1.70 1.63 (0.63,4.24)
Botto et al.11 93/829 186/2890 19.26 1.84 (1.41,2.39)
Acs et al.17 105/4480 535/38151 28.73 1.69 (1.37,2.08)
Cleves et al.18 33/3685 27/4755 6.11 1.58 (0.95,2.64)
Oster et al.12 119/2361 155/3435 31.37 1.12 (0.88,1.43)
Overall 425/12030 1111/51729 100.00 1.53 (1.36,1.73)
Abbreviations: CHD, congenital heart defect; CI, confidence interval; OR, odds ratio. I2= 35.4%, P= 0.158.
Table 5. Subgroup analysis of VSD associated with maternal fever in the first trimester
Study CHD infants/Fever mothers
CHD infants/Non-fever mothers Weight(%) Odds ratio(fixed)
95% CI
Tikkanen, et al.15 17/216 63/1055 23.93 1.35 (0.77,2.35)
Botto, et al.11 22/194 186/2890 25.17 1.88 (1.18,2.97)
Cleves, et al.18 4/703 20/4086 7.08 1.18 (0.40,3.41)
Oster, et al.12 23/479 155/3435 43.81 1.07 (0.88,1.87)
Overall 66/1592 424/11466 100.00 1.34 (1.02,1.76)
Abbreviations: CHD, congenital heart defect; CI, confidence interval; VSD, ventricular septal defect. I2= 0.0%, P= 0.402.
Congenital heart defects and maternal feverQY Shi et al
680
Journal of Perinatology (2014), 677 – 682 © 2014 Nature America, Inc.
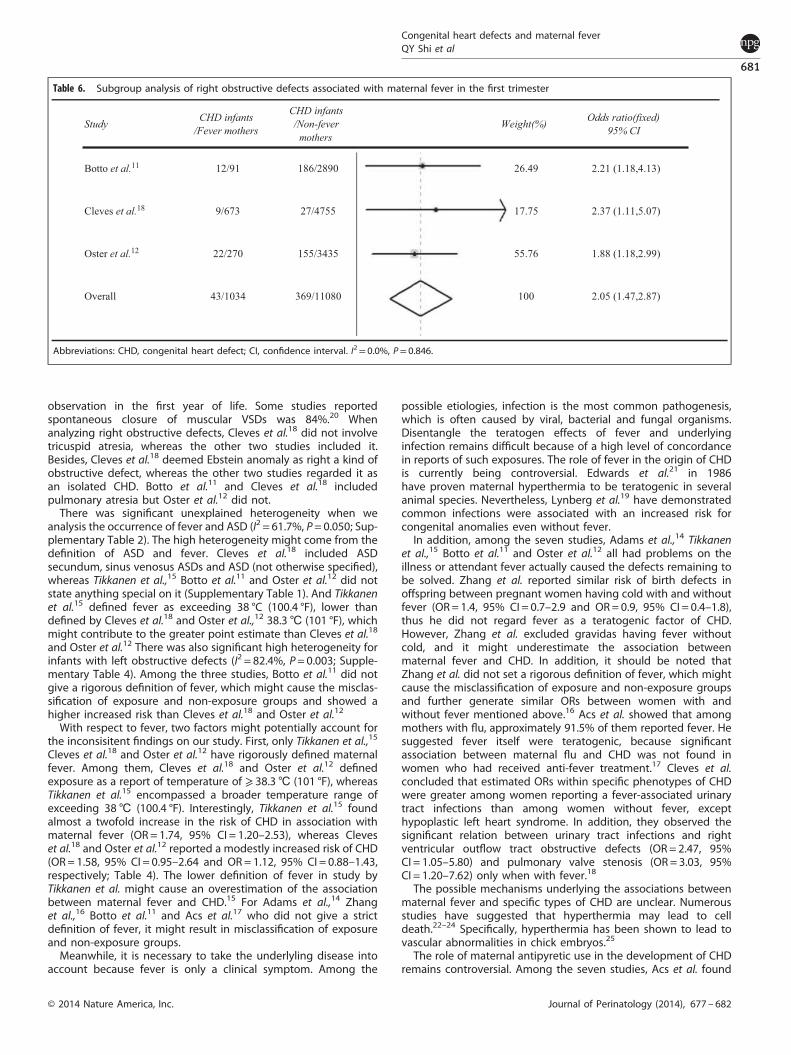
observation in the first year of life. Some studies reportedspontaneous closure of muscular VSDs was 84%.20 Whenanalyzing right obstructive defects, Cleves et al.18 did not involvetricuspid atresia, whereas the other two studies included it.Besides, Cleves et al.18 deemed Ebstein anomaly as right a kind ofobstructive defect, whereas the other two studies regarded it asan isolated CHD. Botto et al.11 and Cleves et al.18 includedpulmonary atresia but Oster et al.12 did not.There was significant unexplained heterogeneity when we
analysis the occurrence of fever and ASD (I2 = 61.7%, P= 0.050; Sup-plementary Table 2). The high heterogeneity might come from thedefinition of ASD and fever. Cleves et al.18 included ASDsecundum, sinus venosus ASDs and ASD (not otherwise specified),whereas Tikkanen et al.,15 Botto et al.11 and Oster et al.12 did notstate anything special on it (Supplementary Table 1). And Tikkanenet al.15 defined fever as exceeding 38 °C (100.4 °F), lower thandefined by Cleves et al.18 and Oster et al.,12 38.3℃ (101 °F), whichmight contribute to the greater point estimate than Cleves et al.18
and Oster et al.12 There was also significant high heterogeneity forinfants with left obstructive defects (I2 = 82.4%, P= 0.003; Supple-mentary Table 4). Among the three studies, Botto et al.11 did notgive a rigorous definition of fever, which might cause the misclas-sification of exposure and non-exposure groups and showed ahigher increased risk than Cleves et al.18 and Oster et al.12
With respect to fever, two factors might potentially account forthe inconsisitent findings on our study. First, only Tikkanen et al.,15
Cleves et al.18 and Oster et al.12 have rigorously defined maternalfever. Among them, Cleves et al.18 and Oster et al.12 definedexposure as a report of temperature of ⩾ 38.3℃ (101 °F), whereasTikkanen et al.15 encompassed a broader temperature range ofexceeding 38℃ (100.4 °F). Interestingly, Tikkanen et al.15 foundalmost a twofold increase in the risk of CHD in association withmaternal fever (OR = 1.74, 95% CI = 1.20–2.53), whereas Cleveset al.18 and Oster et al.12 reported a modestly increased risk of CHD(OR= 1.58, 95% CI = 0.95–2.64 and OR= 1.12, 95% CI = 0.88–1.43,respectively; Table 4). The lower definition of fever in study byTikkanen et al. might cause an overestimation of the associationbetween maternal fever and CHD.15 For Adams et al.,14 Zhanget al.,16 Botto et al.11 and Acs et al.17 who did not give a strictdefinition of fever, it might result in misclassification of exposureand non-exposure groups.Meanwhile, it is necessary to take the underlyling disease into
account because fever is only a clinical symptom. Among the
possible etiologies, infection is the most common pathogenesis,which is often caused by viral, bacterial and fungal organisms.Disentangle the teratogen effects of fever and underlyinginfection remains difficult because of a high level of concordancein reports of such exposures. The role of fever in the origin of CHDis currently being controversial. Edwards et al.21 in 1986have proven maternal hyperthermia to be teratogenic in severalanimal species. Nevertheless, Lynberg et al.19 have demonstratedcommon infections were associated with an increased risk forcongenital anomalies even without fever.In addition, among the seven studies, Adams et al.,14 Tikkanen
et al.,15 Botto et al.11 and Oster et al.12 all had problems on theillness or attendant fever actually caused the defects remaining tobe solved. Zhang et al. reported similar risk of birth defects inoffspring between pregnant women having cold with and withoutfever (OR= 1.4, 95% CI = 0.7–2.9 and OR= 0.9, 95% CI = 0.4–1.8),thus he did not regard fever as a teratogenic factor of CHD.However, Zhang et al. excluded gravidas having fever withoutcold, and it might underestimate the association betweenmaternal fever and CHD. In addition, it should be noted thatZhang et al. did not set a rigorous definition of fever, which mightcause the misclassification of exposure and non-exposure groupsand further generate similar ORs between women with andwithout fever mentioned above.16 Acs et al. showed that amongmothers with flu, approximately 91.5% of them reported fever. Hesuggested fever itself were teratogenic, because significantassociation between maternal flu and CHD was not found inwomen who had received anti-fever treatment.17 Cleves et al.concluded that estimated ORs within specific phenotypes of CHDwere greater among women reporting a fever-associated urinarytract infections than among women without fever, excepthypoplastic left heart syndrome. In addition, they observed thesignificant relation between urinary tract infections and rightventricular outflow tract obstructive defects (OR= 2.47, 95%CI = 1.05–5.80) and pulmonary valve stenosis (OR = 3.03, 95%CI = 1.20–7.62) only when with fever.18
The possible mechanisms underlying the associations betweenmaternal fever and specific types of CHD are unclear. Numerousstudies have suggested that hyperthermia may lead to celldeath.22–24 Specifically, hyperthermia has been shown to lead tovascular abnormalities in chick embryos.25
The role of maternal antipyretic use in the development of CHDremains controversial. Among the seven studies, Acs et al. found
Table 6. Subgroup analysis of right obstructive defects associated with maternal fever in the first trimester
Study CHD infants/Fever mothers
CHD infants/Non-fever
mothersWeight(%) Odds ratio(fixed)
95% CI
Botto et al.11 12/91 186/2890 26.49 2.21 (1.18,4.13)
Cleves et al.18 9/673 27/4755 17.75 2.37 (1.11,5.07)
Oster et al.12 22/270 155/3435 55.76 1.88 (1.18,2.99)
Overall 43/1034 369/11080 100 2.05 (1.47,2.87)
Abbreviations: CHD, congenital heart defect; CI, confidence interval. I2= 0.0%, P= 0.846.
Congenital heart defects and maternal feverQY Shi et al
681
© 2014 Nature America, Inc. Journal of Perinatology (2014), 677 – 682
the proportion of anti-fever drugs used by the control motherswith flu was greater in the second and/or third month of gestationthan in the case of mothers with flu. The OR of having infants withCHD for mothers taking anti-fever drugs when flu was 1.4 (95%CI = 0.9–2.1), compared with the mothers with fever taking noanti-fever drug (OR= 1.7, 95% CI = 1.3–2.2). Therefore, Acs et al.indicated the protective effect of anti-fever drugs. However, fever-reducing medications was not always used for fever, and theymight provide a protective effect by reducing other symptoms aswell.17 Cleves et al. found no significant difference on the risk ofCHD infants between maternal urinary tract infection with andwithout taking sulfonamide.18
The study also has some limitations. First, because few studieshave examined the relation between maternal fever and CHD,only seven studies could be included. As a result, we need moreprospective studies to corroborate the association betweenmaternal fever and CHD. Second, this meta-analysis onlyaddresses the criterion of consistency of findings across studies.Other criteria for causality remain to be addressed, includingtemporal relationship, dose-response, biologic plausibility andanimal experiments. Last, there might be publication bias owingto the studies with negative results were not publised. As aconsequence, we need more rigorously designed and high-qualified epidemiologic studies.
CONCLUSIONOur analysis suggests that maternal fever in the first trimester isthe risk factor of congenital heart diseases in offspring. Throughthe subgroup analysis, we find that exposure to maternal fever isthe risk factor of VSD and right obstructive defects. Consideringthat maternal fever in the first trimester is common in pregnantwomen, our findings are pervasiveness in individual andpopulation level.
CONFLICT OF INTERESTThe authors declare no conflict of interest.
ACKNOWLEDGEMENTSThis work was supported by the grants from National Natural Science Foundation ofChina (No. 21003077), the Open Project of Key Laboratory of Advanced EnergyMaterials Chemistry (No. KLAEMC-OP201101)
AUTHOR CONTRIBUTIONSYL Zhang, QY Shi and JB Zhang were involved in the conceptualization,research design, execution and write-up of the first draft of the manuscript.YQ Mi, Y Song and J Ma advised on the design of the study, and the analysisand interpretation of the results. All authors were involved in the preparation ofthe manuscript.
REFERENCES1 Rosamond W, Flegal K, Friday G, Furia K, Go A, Greenlund K et al. American Heart
Association Statistics Committee and Stroke Statistics Subcommittee Heart dis-ease and stroke statistics-2007 update: a report from the American Heart Asso-ciation Statistics Committee and Stroke Statistics Subcommittee. Circulation 2007;115(5)):169–171.
2 Zhang YL, Riehle-Colarusso T, Correa A, Li S, Feng X, Gindler J et al. Observedprevalence of congenital heart defects from a surveillance study in china.J Ultrasound Med 2011; 30(7): 989–995.
3 Tikkanen J, Heinonen OP. Risk factors for cardiovascular malformations in Finland.Eur J Epidemiol 1990; 6(4): 348–356.
4 Shaw GM, Malcoe LH, Swan SH, Cummins SK, Schulman J. Congenital cardiacanomalies relative to selected maternal exposures and conditions during earlypregnancy. Eur J Epidemiol 1992; 8(5): 757–760.
5 Frohn-Mulder IM, Meilof JF, Szatmari A, Stewart PA, Swaak TJ, Hess J. Clinicalsignificance of maternal Anti-Ro/SS-A antibodies in children with isolatedheart block. J Am College Cardiol 1994; 23(7): 1677–1681.
6 Jenkins KJ, Correa A, Feinstein JA, Botto L, Britt AE, Daniels SR et al. Non-inheritedrisk factors and congenital cardiovascular defects: current knowledge: a scientificstatement from the American Heart Association Council on Cardiovascular Dis-ease in the Young: endorsed by the American Academy of Pediatrics. Circulation2007; 115(23): 2995–3014.
7 Nora JJ, Nora AH. The evolution of specific genetic and environmental counselingin congenital heart diseases. Circulation 1987; 57(2): 205–213.
8 Moretti ME, Bar-Oz B, Fried S, Koren G. Maternal hyperthermia and the risk forneural tube defects in offspring: systematic review and meta-analysis. Epidemiol2005; 16(2): 216–229.
9 Edwards MJ. Review: hyperthermia and fever during pregnancy. Birth Defects ResA Clin Mol Teratol 2006; 76(7): 507–516.
10 Shahrukh Hashmi S, Gallaway MS, Waller DK, Langlois PH, Hecht JT. Maternal feverduring early pregnancy and the risk of oral clefts. Birth Defects Res A Clin MolTeratol 2010; 88(3): 186–194.
11 Botto LD, Lynberg MC, Erickson JD. Congenital heart defects, maternal febrileillness, and multivitamin use: a population-based study. Epidemiol 2001; 12(5):485–490.
12 Oster ME, Riehle-Colarusso Tiffany, Alverson CJ, Correa A. Associations betweenmaternal fever and influenza and congenital heart defects. J Pediatr 2011; 158(6):990–995.
13 Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses http://www.lri.ca 2000.
14 Adams MM, Mulinare J, Dooley K. Risk factors for conotruncal cardiac defects inAtlanta. J Am Coll Cardiol 1989; 14(2): 432–442.
15 Tikkanen J, Heinonen OP. Maternal hyperthermia during pregnancy and cardio-vascular malformations in the offspring. Eur J Epidemiol 1991; 7(6): 628–635.
16 Zhang J, Cai WW. Association of the common cold in the first trimester ofpregnancy with birth defects. Pediatrics 1993; 92(4): 559–563.
17 Acs N, Banhidy F, Puho E, Czeizel AE. Maternal influenza during pregnancy andrisk of congenital abnormalities in offspring. Birth Defects Res A Clin Mol Teratol2005; 73(12): 989–996.
18 Cleves MA, Malik S, Yang S, Carter TC, Hobbs CA. Maternal urinary tract infectionsand selected cardiovascular malformations. Birth Defects Res A Clin Mol Teratol2008; 82(6): 464–473.
19 Lynberg M C, Khoury MJ, Lu X, Cocian T. Maternal flu, fever, and the risk of neuraltube defects: A population based case-control study. Am J Epidemiol 1994; 140(3):244–255.
20 Miyake T, Shinohara T, Inoue T, Marutani S, Takemura T. Spontaneous closure ofmuscular trabecular ventricular septal defect: comparison of defect position. ActaPaediatr 2011; 100(10): e158–e162.
21 Edwards MJ. Hyperthermia as a teratogen: a review of experimental studies andtheir clinical significance. Teratogenesis Carcinog Mutagen 1986; 6(6): 563–582.
22 Mirkes PE, Cornel LM, Park HW, Cunningham ML. Induction of thermotolerance inearly postimplantation rat embryos is associated with increased resistance tohyperthermia-induced apoptosis. Teratol 1997; 56(3): 210–219.
23 Edwards MJ. Apoptosis, the heat shock response, hyperthermia, birth defects,disease and cancer: where are the common links? Cell Stress Chaperones 1998; 3(4): 213–220.
24 Roulston A, Marcellus RC, Branton PE. Viruses and apoptosis. Annu Rev Microbiol1999; 53: 577–628.
25 Nilsen NO. Vascular abnormalities due to hyperthermia in chick embryos. Teratol1984; 30(2): 237–251.
Supplementary Information accompanies the paper on the Journal of Perinatology website (http://www.nature.com/jp)
Congenital heart defects and maternal feverQY Shi et al
682
Journal of Perinatology (2014), 677 – 682 © 2014 Nature America, Inc.