comprehensive analysis of variables affecting delayed gastric emptying following...
TRANSCRIPT
ORIGINAL ARTICLE
Comprehensive Analysis of Variables Affecting DelayedGastric Emptying Following Pancreaticoduodenectomy
John W. Kunstman & Annabelle L. Fonseca &
Maria M. Ciarleglio & Xiangyu Cong & Abby Hochberg &
Ronald R. Salem
Received: 20 January 2012 /Accepted: 7 March 2012 /Published online: 27 March 2012# 2012 The Society for Surgery of the Alimentary Tract
AbstractIntroduction Delayed gastric emptying (DGE) occurs commonly following pancreaticoduodenectomy (PD), and criteria for itsclinical diagnosis have recently been standardized by an international consensus group. We evaluated 24 operative and peri-operative variables to assess which were independent risk factors for DGE development. Secondarily, we also examined DGEincidence over time and evaluated the consensus guidelines’ ability to diagnose DGE in patients with complicated post-operativecourses.Methods A prospective, single-surgeon database of 235 patients undergoing PD at an academic tertiary center wasretrospectively reviewed and DGE was assessed per published guidelines.Results DGE occurred in 42 patients overall (17.9 %), with incidence falling from 30.0 to 9.1 % during the study period. Post-operative abscess, pancreatic fistula formation, pulmonary comorbidity, and increased intraoperative blood loss were found to beindependent risk factors (p<0.05) for DGE on multivariate analysis. Changes in operative technique, such as pylorus preserva-tion, did not associate with DGE. In a separate analysis, when patients with confounding post-operative events such as re-intubation or re-laparotomy were excluded, DGE incidence was 11.9 %.Conclusions Perturbation of the operative bed by a secondary complication seems to be the dominant risk for DGE development.The consensus guidelines for DGE diagnosis, while indispensable, may overestimate DGE incidence.
Keywords Pancreaticoduodenectomy . Delayed gastricemptying . ISGPS
Introduction
Pancreaticoduodenectomy (PD) remains the standard of carefor resectable neoplasia of the pancreatic head and surround-ing tissues. A tremendous reduction in operative mortalityhas been observed in patients undergoing PD with currentoperative mortality rates of less than 3 % the norm, com-pared to 30 % in the 1970s.1 Operative volume stronglycorrelates with reduced PD mortality at both the institutionaland surgeon level.2,3 However, even high-volume surgeonsand centers continue to report significant rates of operativemorbidity following PD of 25–45 %.1,4 PD-specific causesof operative morbidity such as post-operative pancreaticfistula formation and delayed gastric emptying (DGE) areof particular interest to pancreatic surgeons. DGE, the etiol-ogy of which remains uncertain but is likely multifactorial,is usually self-limiting, but is associated with increasedlength of stay, hospital costs, and development of additionalpost-operative morbidity.4,5
Meeting Information: Given as a podium presentation at the 92ndAnnual Meeting of the New England Surgical Society on September23, 2011 by Dr. Kunstman.
J. W. Kunstman :A. L. Fonseca :R. R. Salem (*)Section of Surgical Oncology, Department of Surgery,Yale University School of Medicine,P.O. Box 208062, New Haven, CT 06520-8062, USAe-mail: [email protected]
M. M. Ciarleglio :X. CongYale Center for Analytical Sciences,Yale University School of Public Health,60 College Street, P.O. Box 208034, New Haven,CT 06520-8034, USA
A. HochbergDrexel University College of Medicine,2900 W. Queen Lane,Philadelphia, PA 19129, USA
J Gastrointest Surg (2012) 16:1354–1361DOI 10.1007/s11605-012-1873-y

Previously, a limitation of DGE research has been the lack ofa universal definition for clinical diagnosis of DGE. A varietyof schemes have been described,6–8 with resultant confusionover the true incidence of DGE and whether its effects can bemitigated by changes in clinical practice.9 The InternationalStudy Group of Pancreatic Surgeons (ISGPS) advocated a newconsensus definition for DGE in 2007 (Table 1).10 Aside fromthe obvious benefits of standardization, the ISGPS definitionsalso recognized the clinical heterogeneity of DGE by subdivid-ing the criteria by severity. These new criteria have beenvalidated11,12 and employed in a small number of studies re-evaluating DGE within the consensus guidelines.13,14 The pri-mary aim of our study was to broaden this effort via a robustreappraisal of operative and peri-operative risk factors poten-tially correlated with development of DGE as defined by theISGPS guidelines. As some of our practice patterns havechanged over the study period, we found it feasible to evaluateseveral variables not previously assessed for DGE correlation.Furthermore, a secondary aim of this study was to assess DGEincidence and severity over time in our cohort.
An additional secondary aim of this study was to assess theutility of the ISGPS definitions in cases of questionable DGE.Several authors have expressed concern that the consensusguidelinesmay overestimate actual DGE incidence due to theirreliance on timing of dietary resumption and nasogastric tube(NGT) presence for DGE diagnosis.12,15–17 Post-operativeevents unrelated to DGE but still affecting these aspects ofpatient care could result in the inappropriate diagnosis of DGEin certain patients. To analyze this possibility, we developed aninstitutional modification of the ISGPS criteria for DGE diag-nosis that excluded patients with such potentially confoundingpost-operative events. We then re-assessed the incidence andseverity of DGE as well as risk factors correlating with DGEdevelopment in patients when defined by this modification.
Materials and Methods
Patient Selection
We conducted a retrospective review of 235 consecutivepatients who underwent PD for any indication by a single
surgeon at Yale-NewHaven Hospital from 2003 to 2011. Datacollection and analysis were performed under a protocol ap-proved by the Yale University School of Medicine HumanInvestigations Committee (HIC#0912006089). After reviewof our cohort, 23 unique variables were identified and evalu-ated for each patient. These are listed in Table 2 and includedemographic characteristics, comorbidities, operative/peri-op-erative variables, and concurrent complications. An aggregatecomorbid score was evaluated; consisting of the sum ofcomorbid conditions affected each individual patient. Opera-tive period was also analyzed as an independent variable,resulting in 24 total assessed variables.
Operative Technique
Pylorus-preserving pancreaticoduodenectomy (PPPD) was car-ried out when not precluded by oncologic or disease-specificconsiderations; in all other cases, a classic (Kausch–Whipple)PD was performed. Pancreaticojejunostomy was performed ina two-layer end-to-side fashion utilizing duct-to-mucosa recon-struction, while hepaticojejunostomy was performed in asingle-layer end-to-side fashion. Gastro-/duodenojejunostomywas performed in an end-to-side (Billroth II) fashion. Early inthe case series, these were performed in a retrocolic fashion, butour approach changed to antecolic positioning in 2008. Simi-larly, closed suction drainage of the peritoneum was routinelyemployed early in the series with placement of two drainsadjacent to the hepatico- and pancreaticojejunostomies, respec-tively. However, intraperitoneal drains were rarely employedafter 2005, as evidence concerning their necessity was integrat-ed into our practice.18
Post-operative Care
Patients were admitted to the surgical intensive care unit post-operatively and were transferred to a surgical ward on post-operative day (POD) 1 in routine cases. NGTs were routinelyemployed until 2008. After which, they were selectivelyemployed in rare instances (i.e., patient required prolongedmechanical ventilation). When routinely utilized (prior to2008), the NGT was removed on POD #1–2 unless outputwas persistently large in volume; subsequently, an oral dietwas slowly reinstituted. When NGTwere not routinely utilized(after 2008), a liquid diet was initiated on POD#2–3 andadvanced as tolerated. In these patients, NGT reinsertion wasdictated by individual circumstance and usually occurred inthose patients requiring re-intubation, re-laparotomy, or persis-tent emesis/inability to tolerate oral intake.
Defining DGE
Incidence and severity analysis was undertaken utilizing theconsensus ISGPS definitions for clinical diagnosis of DGE as
Table 1 ISGPS consensus definition for clinical diagnosis of DGE
DGE Grade NGT Required Unable to toleratesolid oral intakeby POD
A 4–7 days or reinsertion >POD 3 7
B 8–14 days or reinsertion >POD 7 14
C >14 days or reinsertion >POD 14 21
Adapted from10
J Gastrointest Surg (2012) 16:1354–1361 1355

Table 2 Patient, operative, and peri-operative variables assessed for association with DGE
Patient characteristic No DGE (N0193) DGE (N042) p value
Age 62.9 (±1.7) years 62.7 (±4.2) years 0.9412
Gender 0.3855
Female 97 (50.3 %) 18 (42.9 %)
Male 96 (49.7 %) 24 (57.1 %)
Tumor Type 0.7134
Benign 56 (29.0 %) 11 (26.2 %)
Malignant 137 (71.0 %) 31 (73.8 %)
Type of Resection 0.3185
Pylorus-preserving PD (PPPD) 127(65.8 %) 31(73.8 %)
Classic (Kausch–Whipple) PD 66 (34.2 %) 11 (26.2 %)
Gastro-/Duodenojejunostomy 0.7180
Antecolic 127 (66.2 %) 29 (69.1 %)
Retrocolic 65 (33.9 %) 13 (31.0 %)
Intra-peritoneal drain placement 0.0287
Yes 21 (10.9 %) 10 (23.8 %)
No 172 (89.1 %) 32 (76.2 %)
Intra-operative estimated blood loss 523.0 (±57.5) ml 768.9 (±270.8) ml 0.0168
Intra-operative crystalloid infused 4662.4 (±220.4) ml 5351.2 (±647.3) ml 0.0177
Intra-operative colloid infused 0.1751
Yes 121 (62.7 %) 31 (73.8 %)
No 72 (37.3 %) 11 (26.2 %)
Intra-operative blood product use 0.2710
Yes 36 (18.7 %) 11 (26.2 %)
No 157 (81.4 %) 31 (73.8 %)
Intra-operative urine output 557.0 (±49.4) ml 636.8 (±136.4) ml 0.2036
Nasogastric tube placement 0.0207
Yes 109 (56.5 %) 32 (76.2 %)
No 84 (43.5 %) 10 (23.8 %)
Comorbidities
Diabetes 41 (21.2 %) 12 (28.6 %) 0.3049
Hypertension 94 (48.7 %) 22 (52.4 %) 0.6660
Pancreatitis 35 (18.1 %) 9 (21.4 %) 0.6204
Pulmonary 12 (6.2 %) 9 (21.4 %) 0.0032
Coronary Artery Disease 25 (13.0 %) 8 (19.1 %) 0.3060
Creatinine - mean (95 % C.I) 0.9 (0.9–1.0) mg/dL 1.1 (0.9–1.2) mg/dL 0.0560
Aggregate Comorbidity Score 0.0288
0 66 (34.2 %) 7 (16.7 %)
1 64 (33.2 %) 18 (42.9 %)
2 49 (25.4 %) 9 (21.4 %)
3 11 (5.7 %) 8 (19.1 %)
4 3 (1.6 %) 0 (0.0 %)
Post-operative complications
Intra-abdominal abscess 11 (5.7) 7 (16.7) 0.0208
Pancreatic fistula 8 (4.1) 9 (21.4) 0.0003
Anastomotic Leak 1 (0.5) 2 (4.8) 0.0675
Wound Infection 20 (10.4) 5 (11.9) 0.7691
Aggregate comorbid score defined as sum of total assess comorbid conditions present in each individual patient
1356 J Gastrointest Surg (2012) 16:1354–1361
seen in Table 1. An institutional “Yale modification” wasemployed for a separate analysis of DGE diagnosis in thepresence of confounding post-operative events that wouldaffect length of NGT placement or diet tolerance. The Yalemodification excluded those patients who (1) required re-laparotomy during the same hospital stay resulting in NGTreplacement, (2) required mechanical ventilation at any timebeyond post-operative day 2, or (3) required prolonged NPOstatus for an objectively diagnosed non-DGE cause (i.e., high-output pancreatic fistula).
Analysis
Univariate analysis was performed using logistic or ordinalregression models as appropriate to evaluate variables associ-ated with DGE incidence and severity. Variables with p values<0.10 on the univariate analysis were considered for entry intothe multivariate model. When independent variables werefound to be highly correlated with one another, multiple mod-els were constructed to include individual highly correlatedvariables with all other non-correlated variables to avoid esti-mation problems and model instability. Stepwise model selec-tion was utilized for multivariate model refinement, with onlythose variables with p values <0.15 included in the final model.When multiple models were constructed, the least significant(i.e., greatest in value) p value was considered definitive.
To evaluate whether the incidence of DGE changed overtime, we subdivided our cohort of patients with DGE into fourconsecutive quartiles based on date of surgery and examinedthe incidence and severity of DGE in each quartile. Operativeperiod was also included as an independent variable in theabove-described statistical models; however, due to the smallnumber of high-grade (class B/C) DGE in the fourth quartile,the third and fourth quartiles were combined into a singleperiod for the purposes of analysis. All statistical analyses wereperformed using SAS v. 9.2 (SAS Institute, Inc., Cary, NC).
Results
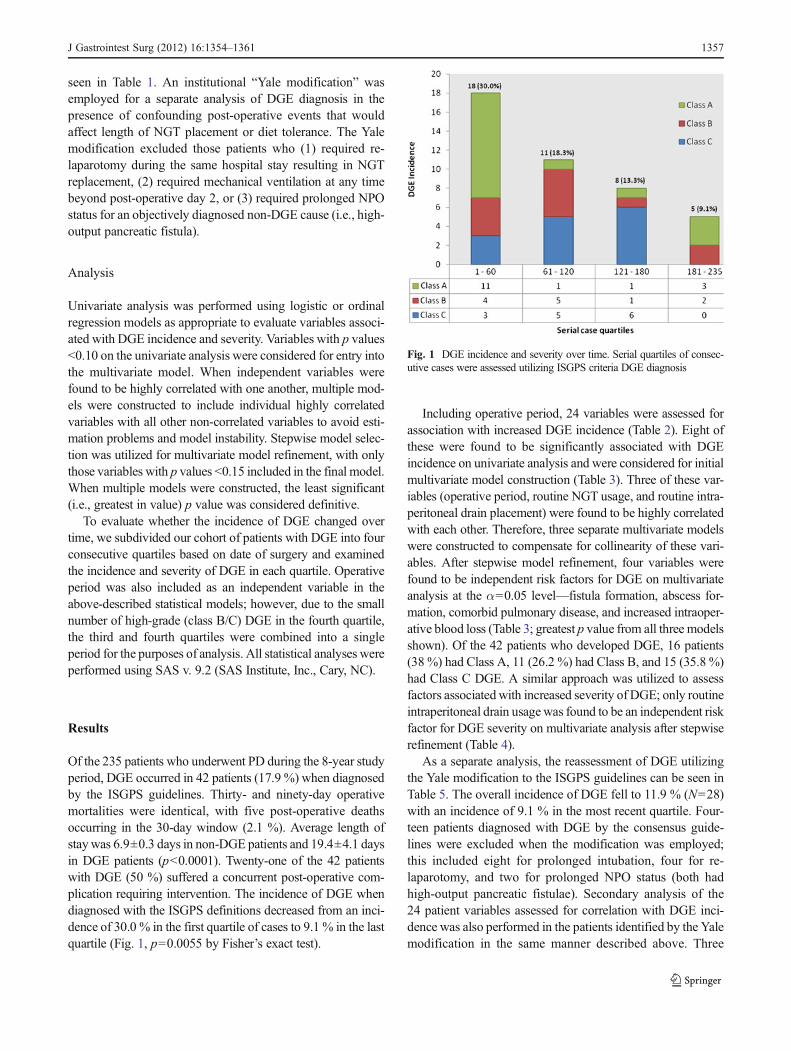
Of the 235 patients who underwent PD during the 8-year studyperiod, DGE occurred in 42 patients (17.9 %) when diagnosedby the ISGPS guidelines. Thirty- and ninety-day operativemortalities were identical, with five post-operative deathsoccurring in the 30-day window (2.1 %). Average length ofstaywas 6.9±0.3 days in non-DGE patients and 19.4±4.1 daysin DGE patients (p<0.0001). Twenty-one of the 42 patientswith DGE (50 %) suffered a concurrent post-operative com-plication requiring intervention. The incidence of DGE whendiagnosed with the ISGPS definitions decreased from an inci-dence of 30.0 % in the first quartile of cases to 9.1 % in the lastquartile (Fig. 1, p00.0055 by Fisher’s exact test).
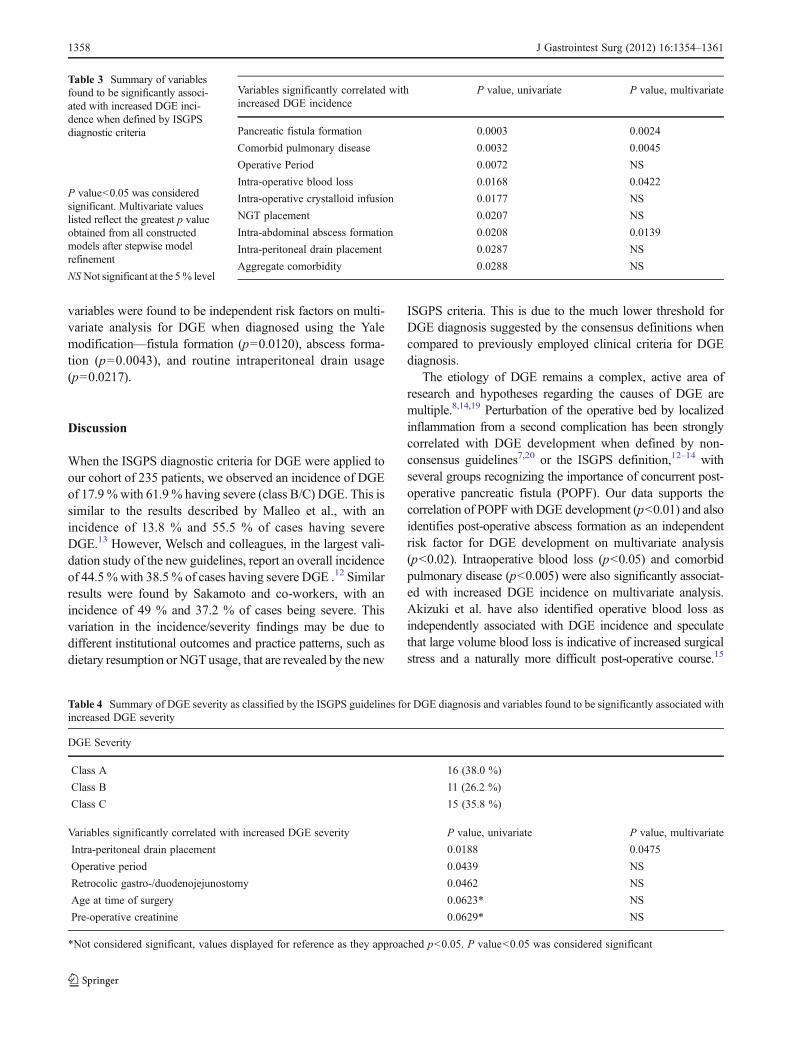
Including operative period, 24 variables were assessed forassociation with increased DGE incidence (Table 2). Eight ofthese were found to be significantly associated with DGEincidence on univariate analysis and were considered for initialmultivariate model construction (Table 3). Three of these var-iables (operative period, routine NGT usage, and routine intra-peritoneal drain placement) were found to be highly correlatedwith each other. Therefore, three separate multivariate modelswere constructed to compensate for collinearity of these vari-ables. After stepwise model refinement, four variables werefound to be independent risk factors for DGE on multivariateanalysis at the α00.05 level—fistula formation, abscess for-mation, comorbid pulmonary disease, and increased intraoper-ative blood loss (Table 3; greatest p value from all three modelsshown). Of the 42 patients who developed DGE, 16 patients(38 %) had Class A, 11 (26.2 %) had Class B, and 15 (35.8 %)had Class C DGE. A similar approach was utilized to assessfactors associatedwith increased severity of DGE; only routineintraperitoneal drain usagewas found to be an independent riskfactor for DGE severity on multivariate analysis after stepwiserefinement (Table 4).
As a separate analysis, the reassessment of DGE utilizingthe Yale modification to the ISGPS guidelines can be seen inTable 5. The overall incidence of DGE fell to 11.9 % (N028)with an incidence of 9.1 % in the most recent quartile. Four-teen patients diagnosed with DGE by the consensus guide-lines were excluded when the modification was employed;this included eight for prolonged intubation, four for re-laparotomy, and two for prolonged NPO status (both hadhigh-output pancreatic fistulae). Secondary analysis of the24 patient variables assessed for correlation with DGE inci-dence was also performed in the patients identified by the Yalemodification in the same manner described above. Three
Fig. 1 DGE incidence and severity over time. Serial quartiles of consec-utive cases were assessed utilizing ISGPS criteria DGE diagnosis
J Gastrointest Surg (2012) 16:1354–1361 1357
variables were found to be independent risk factors on multi-variate analysis for DGE when diagnosed using the Yalemodification—fistula formation (p00.0120), abscess forma-tion (p00.0043), and routine intraperitoneal drain usage(p00.0217).
Discussion
When the ISGPS diagnostic criteria for DGE were applied toour cohort of 235 patients, we observed an incidence of DGEof 17.9 %with 61.9 % having severe (class B/C) DGE. This issimilar to the results described by Malleo et al., with anincidence of 13.8 % and 55.5 % of cases having severeDGE.13 However, Welsch and colleagues, in the largest vali-dation study of the new guidelines, report an overall incidenceof 44.5 % with 38.5 % of cases having severe DGE .12 Similarresults were found by Sakamoto and co-workers, with anincidence of 49 % and 37.2 % of cases being severe. Thisvariation in the incidence/severity findings may be due todifferent institutional outcomes and practice patterns, such asdietary resumption or NGTusage, that are revealed by the new
ISGPS criteria. This is due to the much lower threshold forDGE diagnosis suggested by the consensus definitions whencompared to previously employed clinical criteria for DGEdiagnosis.
The etiology of DGE remains a complex, active area ofresearch and hypotheses regarding the causes of DGE aremultiple.8,14,19 Perturbation of the operative bed by localizedinflammation from a second complication has been stronglycorrelated with DGE development when defined by non-consensus guidelines7,20 or the ISGPS definition,12–14 withseveral groups recognizing the importance of concurrent post-operative pancreatic fistula (POPF). Our data supports thecorrelation of POPF with DGE development (p<0.01) and alsoidentifies post-operative abscess formation as an independentrisk factor for DGE development on multivariate analysis(p<0.02). Intraoperative blood loss (p<0.05) and comorbidpulmonary disease (p<0.005) were also significantly associat-ed with increased DGE incidence on multivariate analysis.Akizuki et al. have also identified operative blood loss asindependently associated with DGE incidence and speculatethat large volume blood loss is indicative of increased surgicalstress and a naturally more difficult post-operative course.15
Table 3 Summary of variablesfound to be significantly associ-ated with increased DGE inci-dence when defined by ISGPSdiagnostic criteria
P value<0.05 was consideredsignificant. Multivariate valueslisted reflect the greatest p valueobtained from all constructedmodels after stepwise modelrefinement
NS Not significant at the 5% level
Variables significantly correlated withincreased DGE incidence
P value, univariate P value, multivariate
Pancreatic fistula formation 0.0003 0.0024
Comorbid pulmonary disease 0.0032 0.0045
Operative Period 0.0072 NS
Intra-operative blood loss 0.0168 0.0422
Intra-operative crystalloid infusion 0.0177 NS
NGT placement 0.0207 NS
Intra-abdominal abscess formation 0.0208 0.0139
Intra-peritoneal drain placement 0.0287 NS
Aggregate comorbidity 0.0288 NS
Table 4 Summary of DGE severity as classified by the ISGPS guidelines for DGE diagnosis and variables found to be significantly associated withincreased DGE severity
DGE Severity
Class A 16 (38.0 %)
Class B 11 (26.2 %)
Class C 15 (35.8 %)
Variables significantly correlated with increased DGE severity P value, univariate P value, multivariate
Intra-peritoneal drain placement 0.0188 0.0475
Operative period 0.0439 NS
Retrocolic gastro-/duodenojejunostomy 0.0462 NS
Age at time of surgery 0.0623* NS
Pre-operative creatinine 0.0629* NS
*Not considered significant, values displayed for reference as they approached p<0.05. P value<0.05 was considered significant
1358 J Gastrointest Surg (2012) 16:1354–1361

This phenomenon may also apply to those with a pulmonarycomorbidity. These patients may be inherently more likely tomeet the less stringent criteria for DGE diagnosis employed bythe ISGPS guidelines. However, neither increased operativeblood loss nor pulmonary comorbidity correlate significantlywith DGE when defined using the Yale modification, whichexcludes patients requiring re-laparotomy or re-intubation. Thissuggests that increased operative blood loss or a pre-existingpulmonary comorbidity may only be associated with increasedneed for re-laparotomy or re-intubation and not be true inde-pendent risk factors for DGE development.
Abscess formation (p00.0043) and POPF formation (p00.0120) remain significantly associated with DGE on multi-variate analysis as defined by the more exclusive Yale modifi-cation. This increases the probability that those variables aregenuine independent risk factors for DGE development. Nota-bly, routine intraperitoneal drain placement (p00.0217) wasfound to be an independent risk factor for DGE developmentwhen diagnosed with the Yale modification. When ISGPScriteria are utilized, drain placement approaches but does notreach significance as an independent risk factor for DGE inci-dence (p0 .1056). We find this data particularly noteworthy, asmany surgeons routinely place intraperitoneal drains followingPD. Previously, Conlon et al. did not demonstrate a benefit fromroutine intraperitoneal drainage following pancreatic resection;18
but no explicit disadvantage was noted when they wereemployed. This intriguing finding merits further investigation.
PD is notable for the variety of potential operativeapproaches employed by different surgeons, and operativevariables have been intensely scrutinized for association withDGE. Indeed, DGE as a clinical entity was first described in a1985-study reviewing outcomes of PPPD versus classic PD.21
However, even randomized controlled trials (RCT) conductedprior to the ISGPS guidelines’ publication have often beencontradictory in their conclusions. For instance, Lin et al.notes a significantly greater incidence of DGE in PPPD com-pared to classic PD,22 whereas others trials do not.23,24 Con-versely, there are now four large case series (including thisone) utilizing the ISGPS classification that have all
demonstrated no significant difference in PD/PPPD outcomeswith regard to DGE incidence.12,14,15 Similarly, conflictingpre-ISGPS RCTs regarding impact of antecolic or retrocolicpositioning of the gastro-/duodenojejunostomy on DGEdevelopment also exist;25,26 yet both ours and two otherstudies utilizing the consensus guidelines have noted no sig-nificant difference in DGE incidence with regard to eithertechnique.14,15 The increase in DGE severity we observed inretrocolic anastomoses was not supported as an independentrisk factor on multivariate analysis. While other less commonvariations in surgical technique have yet to be rigorouslyassessed in the ISGPS era, it seems likely that operativevariables play a minor role in DGE development when de-fined by the consensus definitions.
DGE incidence over time has not been rigorously evaluatedusing the ISGPS guidelines for DGE diagnosis, althoughSakamoto and co-workers evaluated DGE in patients whounderwent surgery early versus late in their case series, findingno difference between these two groups.14 Here, after dividingour cohort into quartiles based on operative date, we haveshown a significant decrease in DGE incidence from 30.0 %in the earliest quartile to 9.1 % in the most recent (p00.0055).Due to the retrospective nature of this study, the causality ofthis decrease cannot be conclusively determined, as severalvariables assessed for correlation with DGE changed overtime, while others did not. For instance, over the study course,we noted a decrease in incidence of POPF while abscessdevelopment was unchanged over time. Additionally, variablesnot directly assessed over time, such as improvements in peri-operative care or increased surgeon experience, may have alsoplayed a crucial role in observed decrease. This uncertainty isinherent in retrospective analysis and is the chief limitation ofthis study. The potential causative risk factors for DGE devel-opment identified here would benefit from evaluation in aprospective fashion as there is a paucity of prospective trialsutilizing the new ISGPS consensus guidelines.
Our final aim was to evaluate the utility of the ISGPSguidelines in assessing DGE among patients with potentiallyconfounding post-operative events that could lead to a spuri-ous diagnosis of DGE. The overall reduction of measuredDGE incidence in our cohort from 17.9 % when assessedusing the ISGPS criteria to 11.9 % was expected and may bemore representative of the true rate of DGE in our case series.Standardization is one of the major benefits derived from theISGPS consensus guidelines regarding DGE diagnosis, per-mitting direct comparison of outcomes between institutions asmore studies utilizing the new guidelines accumulate. Thestudies validating the ISGPS definitions note their excellentcorrelation with the actual clinical course of DGE,11,15 butseveral authors have noted the potential for overestimation ofDGE.12,13,16 Aside from the reasons we have attempt to ex-clude here, the inclusive nature of the ISGPS criteria also risksmisdiagnosing post-operative ileus as DGE, which we do not
Table 5 Comparison of DGE incidence utilizing ISGPS consensusdiagnostic criteria versus an institutional (“Yale”) modification excludingpatients with confounding post-operative events that could lead to anaberrant diagnosis of DGE
ISGPS definition;n (%)
Yale modification;n (%)
Class A 16 (38.0) 15 (53.5 %)
Class B 11 (26.2) 8 (28.5 %)
Class C 15 (35.8) 5 (18.0 %)
Total Incidence 42 (17.9) 28 (11.9 %)
This includes patients requiring re-laparotomy, re-intubation, or pro-longed NPO status for non-DGE causes
J Gastrointest Surg (2012) 16:1354–1361 1359

address in the Yale modification of the consensus guidelines.Furthermore, it is possible that some of the patients excludedby our modification did experience DGE but in a clinicallyunapparent fashion due to masking by more severe concurrentcomplications. It has been suggested that a diagnosis of DGEshould not be made without objective evidence (such as CTorradiographs with oral contrast media),17 but this seems overlyburdensome given the self-limited nature of DGE, the currentapproach of clinically diagnosing of DGE that is present inmost surgeon’s practices, and the increased costs and patientrisks that would ensue.
Conclusion
The etiology of DGE is best considered multifactorial, butincreasing evidence supports the conclusion that localizeddisturbance of the operative bed may be the key contributor.This appears to be closely related to concurrent complicationssuch as post-operative development of an abscess or pancre-atic fistula. Notably, no association between DGE incidenceand post-operative nasogastric decompression or operativevariables such as pylorus preservation and positioning of thegastro-/duodenojejunal anastomosis was noted. The ISGPSguidelines for clinically defining DGE are invaluable in con-ducting DGE research as they allow direct comparison be-tween study groups. However, when applied to a large cohortof patients, the potential for overdiagnosis of DGE by theconsensus definitions is becoming more evident. While werecognize and highly value the standardization the ISGPS hasbrought to clinical diagnosis of DGE, further revision of theguidelines may be advantageous.
Acknowledgments We wish to thank Janis Sandlin, PA-C for hercontributions to data collection. Drs. Ciarleglio, Cong, and Kunstmanhad access to all of the data in the study and carry responsibility for theintegrity of the data and the accuracy of the data analysis.
References
1. Winter, J. M., Cameron, J. L., Campbell, K. A., Arnold, M. A.,Chang, D. C., Coleman, J., Hodgin, M. B., Sauter, P. K., Hruban,R. H., Riall, T. S., Schulick, R. D., Choti, M. A., Lillemoe, K. D.,and Yeo, C. J. 1423 pancreaticoduodenectomies for pancreaticcancer: A single-institution experience. Journal of gastrointestinalsurgery : official journal of the Society for Surgery of the AlimentaryTract 10: 1199–1210; discussion 1210–1191, 2006.
2. Birkmeyer, J. D., Siewers, A. E., Finlayson, E. V., Stukel, T. A.,Lucas, F. L., Batista, I., Welch, H. G., Wennberg, D. E. Hospitalvolume and surgical mortality in the United States. The NewEngland journal of medicine 346: 1128–1137, 2002.
3. Birkmeyer, J. D., Stukel, T. A., Siewers, A. E., Goodney, P. P.,Wennberg, D. E., and Lucas, F. L. Surgeon volume and operativemortality in the United States. The New England journal of medicine349: 2117–2127, 2003.
4. Balcom, J. H. t., Rattner, D. W., Warshaw, A. L., Chang, Y., andFernandez-del Castillo, C. Ten-year experience with 733 pancre-atic resections: changing indications, older patients, and decreasinglength of hospitalization. Archives of surgery (Chicago, Ill. : 1960)136: 391–398, 2001.
5. Balzano, G., Zerbi, A., Braga, M., Rocchetti, S., Beneduce, A. A.,and Di Carlo, V. Fast-track recovery programme after pancreatico-duodenectomy reduces delayed gastric emptying. The British journalof surgery 95: 1387–1393, 2008.
6. Fabre, J. M., Burgel, J. S., Navarro, F., Boccarat, G., Lemoine, C.,and Domergue, J. Delayed gastric emptying after pancreaticoduo-denectomy and pancreaticogastrostomy. The European journal ofsurgery 0 Acta chirurgica 165: 560–565, 1999.
7. van Berge Henegouwen, M. I., van Gulik, T. M., DeWit, L. T.,Allema, J. H., Rauws, E. A., Obertop, H., and Gouma, D. J.Delayed gastric emptying after standard pancreaticoduodenectomyversus pylorus-preserving pancreaticoduodenectomy: an analysisof 200 consecutive patients. Journal of the American College ofSurgeons 185: 373–379, 1997.
8. Yeo, C. J., Barry, M. K., Sauter, P. K., Sostre, S., Lillemoe, K. D.,Pitt, H. A., and Cameron, J. L. Erythromycin accelerates gastricemptying after pancreaticoduodenectomy. A prospective, random-ized, placebo-controlled trial. Annals of surgery 218: 229–237;discussion 237–228, 1993.
9. Traverso, L. W., and Hashimoto, Y. Delayed gastric emptying: thestate of the highest level of evidence. Journal of hepato-biliary-pancreatic surgery 15: 262–269, 2008.
10. Wente, M. N., Bassi, C., Dervenis, C., Fingerhut, A., Gouma, D. J.,Izbicki, J. R., Neoptolemos, J. P., Padbury, R. T., Sarr, M. G.,Traverso, L. W., Yeo, C. J., Buchler, M. W. Delayed gastricemptying (DGE) after pancreatic surgery: a suggested definitionby the International Study Group of Pancreatic Surgery (ISGPS).Surgery 142: 761–768, 2007.
11. Park, J. S., Hwang, H. K., Kim, J. K., Cho, S. I., Yoon, D. S., Lee, W.J., and Chi, H. S. Clinical validation and risk factors for delayed gastricemptying based on the International Study Group of Pancreatic Sur-gery (ISGPS) Classification. Surgery 146: 882–887, 2009.
12. Welsch, T., Borm, M., Degrate, L., Hinz, U., Buchler, M. W., andWente, M. N. Evaluation of the International Study Group ofPancreatic Surgery definition of delayed gastric emptying after pan-creatoduodenectomy in a high-volume centre. The British journal ofsurgery 97: 1043–1050, 2010.
13. Malleo, G., Crippa, S., Butturini, G., Salvia, R., Partelli, S.,Rossini, R., Bacchion, M., Pederzoli, P., and Bassi, C. Delayedgastric emptying after pylorus-preserving pancreaticoduodenec-tomy: validation of International Study Group of PancreaticSurgery classification and analysis of risk factors. HPB: theofficial journal of the International Hepato Pancreato BiliaryAssociation 12: 610–618, 2010.
14. Sakamoto, Y., Yamamoto, Y., Hata, S., Nara, S., Esaki, M., Sano,T., Shimada, K., and Kosuge, T. Analysis of Risk Factors forDelayed Gastric Emptying (DGE) after 387 Pancreaticoduodenec-tomies with Usage of 70 Stapled Reconstructions. Journal of gastro-intestinal surgery : official journal of the Society for Surgery of theAlimentary Tract 15: 1789–1797, 2011.
15. Akizuki, E., Kimura, Y., Nobuoka, T., Imamura, M., Nagayama,M., Sonoda, T., and Hirata, K. Reconsideration of postoperativeoral intake tolerance after pancreaticoduodenectomy: prospectiveconsecutive analysis of delayed gastric emptying according to theISGPS definition and the amount of dietary intake. Annals ofsurgery 249: 986–994, 2009.
16. Fernandez-del Castillo, C. Consensus defining postpancreatec-tomy complications: an opportunity we cannot ignore. Surgery142: 771–772, 2007.
17. Reber, H. A. Delayed gastric emptying—what should be requiredfor diagnosis? Surgery 142: 769–770, 2007.
1360 J Gastrointest Surg (2012) 16:1354–1361

18. Conlon, K. C., Labow, D., Leung, D., Smith, A., Jarnagin, W.,Coit, D. G., Merchant, N., and Brennan, M. F. Prospective ran-domized clinical trial of the value of intraperitoneal drainage afterpancreatic resection. Annals of surgery 234: 487–493; discussion493–484, 2001.
19. Kim, D. K., Hindenburg, A. A., Sharma, S. K., Suk, C. H., Gress,F. G., Staszewski, H., Grendell, J. H., and Reed, W. P. Is pyloro-spasm a cause of delayed gastric emptying after pylorus-preservingpancreaticoduodenectomy? Annals of surgical oncology 12: 222–227, 2005.
20. Riediger, H., Makowiec, F., Schareck, W. D., Hopt, U. T., andAdam, U. Delayed gastric emptying after pylorus-preserving pan-creatoduodenectomy is strongly related to other postoperativecomplications. Journal of gastrointestinal surgery: official journalof the Society for Surgery of the Alimentary Tract 7: 758–765,2003.
21. Warshaw, A. L., and Torchiana, D. L. Delayed gastric emptying afterpylorus-preserving pancreaticoduodenectomy. Surgery, gynecology& obstetrics 160: 1–4, 1985.
22. Lin, P. W., Shan, Y. S., Lin, Y. J., and Hung, C. J. Pancreaticoduo-denectomy for pancreatic head cancer: PPPD versus Whipple proce-dure. Hepato-gastroenterology 52: 1601–1604, 2005.
23. Seiler, C. A., Wagner, M., Bachmann, T., Redaelli, C. A., Schmied,B., Uhl, W., Friess, H., and Buchler, M. W. Randomized clinicaltrial of pylorus-preserving duodenopancreatectomy versus classi-cal Whipple resection-long term results. The British journal ofsurgery 92: 547–556, 2005.
24. Tran, K. T., Smeenk, H. G., van Eijck, C. H., Kazemier, G., Hop, W.C., Greve, J. W., Terpstra, O. T., Zijlstra, J. A., Klinkert, P., Jeekel, H.Pylorus preserving pancreaticoduodenectomy versus standard Whip-ple procedure: a prospective, randomized, multicenter analysis of 170patients with pancreatic and periampullary tumors. Annals of surgery240: 738–745, 2004.
25. Gangavatiker, R., Pal, S., Javed, A., Dash, N. R., Sahni, P., andChattopadhyay, T. K. Effect of antecolic or retrocolic reconstruc-tion of the gastro/duodenojejunostomy on delayed gastric empty-ing after pancreaticoduodenectomy: a randomized controlled trial.Journal of gastrointestinal surgery: official journal of the Societyfor Surgery of the Alimentary Tract 15: 843–852, 2011.
26. Tani, M., Terasawa, H., Kawai, M., Ina, S., Hirono, S., Uchiyama,K., and Yamaue, H. Improvement of delayed gastric emptying inpylorus-preserving pancreaticoduodenectomy: results of a pro-spective, randomized, controlled trial. Annals of surgery 243:316–320, 2006.
J Gastrointest Surg (2012) 16:1354–1361 1361