complications of colles' fracture and...
TRANSCRIPT

627
SOME COMPLICATIONS OF COLLES' FRACTUREAND THEIR TREATMENT
By W. H. STEPHENSON, F.R.C.S.From the Department of Surgery, Postgraduate Medical School of London, Hammersmith Hospital
Though Colles' fracture is a common injury itscomplications and their treatment are seldomdealt with in surgical papers. In this paper it isproposed to discuss the following complications:
I. Redisplacement.2. Mal-union.3. Laxity of the inferior radio-ulnar joint.4. Joint stiffness and adhesions.5. Traumatic arthritis of the wrist joint.6. Pain over the ulnar aspect of the wrist.7. Late rupture of the extensor pollicis longus
tendon.8. Sudeck's atrophy (post-traumatic osteo-
dystrophy).9. Injuries of the median nerve.
io. Prolonged absence from work.
I. RedisplacementThis is the commonest complication of im-
portance. Between I 5 and 20 per cent. of allColles' fractures for which reduction has beenrequired show some degree of redisplacement.The three main causes for this are (a) faulty im-mobilization, (b) gross comminution and (c) com-pression of bone on the dorsal aspect of thefracture.
Immobilization of the joints immediately aboveand below the site of a fracture is a cardinalprinciple in treatment, but the standard fixation ofa colles' fracture, whether by plaster cast or otherforms of splintage, makes no attempt to fix theelbow joint and so control rotation of the forearm.It is imperative, therefore, that whatever splintageis used it should be applied with considerable careand should be observed at frequent intervals,especially during the first two weeks. It has beenstated by Lambrinudi, and repeated by Charnley(I950), that fixation with the forearm in pronationand wrist in ulnar deviation is the most reliableposition for holding reduction. Immobilization in
other positions has been tried, such as the CottonLoder (full palmar-flexion of the wrist and ulnardeviation with extreme pronation of the forearm),but no position is completely successful in pre-venting redisplacement.
Gross comminution may be seen in all agegroups but is more commonly observed in theelderly. Comminution means instability, and evenwith the best support redisplacement is thereforealways a possibility.
Compression of bone on the dorsal aspect of thefracture is the direct result of the causative force.In some instances it is so well marked that aftergood reduction has been obtained a distinct gapmay be seen dorsally between the fracture surfacesin the lateral radiograph.
TreatmentMinor degrees of malalignment may be accepted
as they are compatible with good function. Inelderly subjects even gross redisplacement may beaccepted and it may be justifiable to allow theprimary displacement to remain unreduced.Success from simple manipulation can be expectedup to 14 days from the initial injury, after whichtime the use of the Thomas' wrench offers morechance of success. Beyond the third week it isbetter to accept the position and treat the case asone of mal-union, because forcible attempts at re-duction are usually unsuccessful and may do harm.
2. Mal-UnionMal-union is also a common complication. The
severity and type of deformity vary considerably.The normal forward inclination of the plane of thearticular surface of the radius is 20°, but this islost in nearly 20 per cent. of patients. Thearticular surface may be at right angles to the shaftor even grossly tilted backwards. This is thecommonest form of mal-union occurring alone.
Protected by copyright.
on 16 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.314.627 on 1 D
ecember 1951. D
ownloaded from

628 POSTGRADUATE MEDICAL JOURNAL Decemtiber 1951
...Q
......
FIG. i .-Mal-united Colles' fracture with inferior radio-ulnar dislocation and traumatic arthritis.The patient, a man aged 68, had sustained the fracture many years previously. Thewrist was painless, the grip good and the range of mnovement almost full.
It may be accompanied by shortening of theradius, or by radial and dorsal displacement of thelower fragment giving prominence to the head ofthe ulna and broadening of the wrist. In thesecircumstances some distortion of the anatomy ofthe inferior radio-ulnar joint is inevitable andsubluxation or even dislocation of this joint maybe found.
TreatmentIn many patients with mal-union the functional
result is satisfactory even when the deformity isgross (Fig. i). Conservative treatment is in-dicated when the deformity is slight, the disabilityonly moderate and the patient elderly. At theoutset a course of active exercises and hot waxbaths may regain adequate movement and power.
Operation is seldom indicated. As a generalrule its aim should be directed solely to the im-provement of function, and it is therefore rarely
advised for mal-union when function is adequate.However, in the younger age groups and especiallyin women with gross dorsal tilting of the lowerradial fragment, an osteotomy through the fractuiesite may be performed to restore normal alignmenteven though wrist movements have not beenseriously restricted.
In these patients the object of the operation is todelay late traumatic arthritis and to improve theappearance of the wrist. The osteotomy is per-formed through a dorsal approach at the level ofthe old fracture. It is important to fill with a bonegraft the dorsal defect created when alignment hasbeen restored lest displacement should recur. Thewrist is then immobilized in plaster until unionhas taken place.When in addition to dorsal tilting there is con-
siderable shortening of the radius and some radialdisplacement, surgical interference may be re-quired on account of pain, stiffness and an un-
Protected by copyright.
on 16 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.314.627 on 1 D
ecember 1951. D
ownloaded from
December 1951 S'1'EPHENSON: Some Comlplications of Col/es' Fractture 629
sightly deformity. Here much of the disability isdue to the derangement of the inferior radio-ulnar joint, and excision of the lower IA in. of theulna gives a satisfactory result. Following thisoperation (vide infra), the prominence of theulnar head is abolished, pronation and supinationare considerably improved or fully restored anddiscomfort is relieved. The results following morecomplicated operations are uncertain and oftendisappointing.Very occasionally in cominuted fractures a
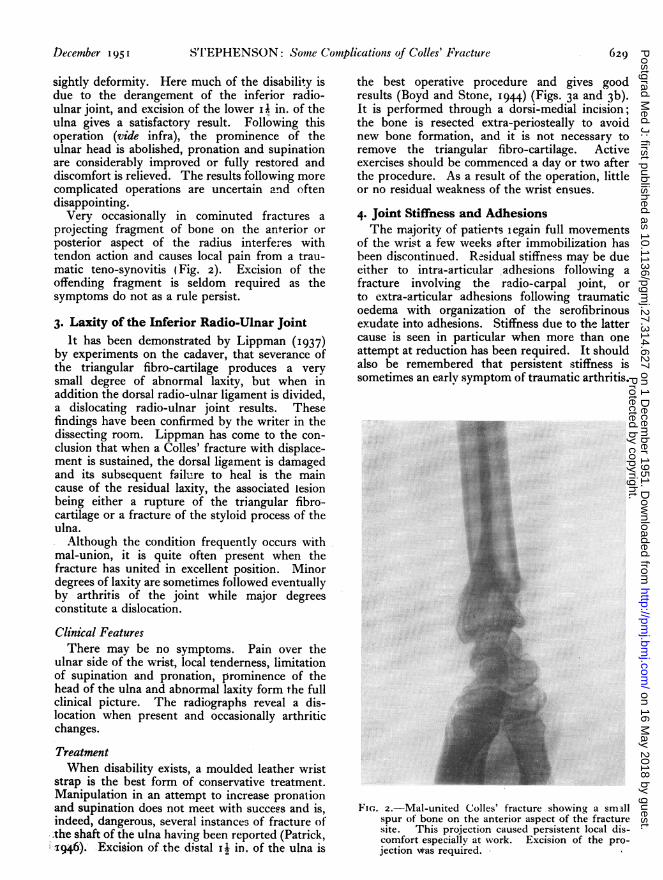
projecting fragment of bone on the anterior orposterior aspect of the radius interferes withtendon action and causes local pain from a trau-matic teno-synovitis (Fig. 2). Excision of theoffending fragment is seldom required as thesymptoms do not as a rule persist.
3. Laxity of the Inferior Radio-Ulnar JointIt has been demonstrated by Lippman (I937)
by experiments on the cadaver, that severance ofthe triangular fibro-cartilage produces a verysmall degree of abnormal laxity, but when inaddition the dorsal radio-ulnar ligament is divided,a dislocating radio-ulnar joint results. Thesefindings have been confirmed by the writer in thedissecting room. Lippman has come to the con-clusion that when a Colles' fracture with displace-ment is sustained, the dorsal ligament is damagedand its subsequent failure to heal is the maincause of the residual laxity, the associated lesionbeing either a rupture of the triangular fibro-cartilage or a fracture of the styloid process of theulna.
Although the condition frequently occurs withmal-union, it is quite often present when thefracture has united in excellent position. Minordegrees of laxity are sometimes followed eventuallyby arthritis of the joint while major degreesconstitute a dislocation.
Clinical FeaturesThere may be no symptoms. Pain over the
ulnar side of the wrist, local tenderness, limitationof supination and pronation, prominence of thehead of the ulna and abnormal laxity form the fullclinical picture. The radiographs reveal a dis-location when present and occasionally arthriticchanges.
TreatmentWhen disability exists, a moulded leather wrist
strap is the best form of conservative treatment.Manipulation in an attempt to increase pronationand supination does not meet with success and is,indeed, dangerous, several instances of fracture ofthe shaft of the ulna having been reported (Patrick,x6). Excision of-the distal Ii in. of the ulna is
the best operative procedure and gives goodresults (Boyd and Stone, I944) (Figs. 3a and 3b).It is performed through a dorsi-medial incision;the bone is resected extra-periosteally to avoidnew bone formation, and it is not necessary toremove the triangular fibro-cartilage. Activeexercises should be commenced a day or two afterthe procedure. As a result of the operation, littleor no residual weakness of the wrist ensues.
4. Joint Stiffness and AdhesionsThe majority of patiepts legain full movements
of the wrist a few weeks after immobilization hasbeen disconitinued. Residual stiffness may be dueeither to intra-articular adhesions following afracture involving the radio-carpal joint, orto extra-articular adhesions following traumaticoedema with organization of the serofibrinousexudate into adhesions. Stiffness due to the lattercause is seen in particular when more than oneattempt at reduction has been required. It shouldalso be remembered that persistent stiffness issometimes an early symptom of traumatic arthritis.
.::: ..:: .;..:. .::..:...:...... ..:..:.. ...: :.
~~~~~~~~~~~...
.....
::..... .:..,:.e ........... ... ...
.i
*~~ ~ ~.....-r.!:
*.:.t .:S.r<::!.:.
... ::. ::..... .?, 'S'.:8}:
~~~~~~~~~~~.....:::;
Fie.. 2.-Mal-united Colles' fracture showingY a smIllspur of bone on the anterior aspect of the fracturesite. This projection caused persistent local dis-comfort especially at work. Excision of the pro-jection wras required.
Protected by copyright.
on 16 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.314.627 on 1 D
ecember 1951. D
ownloaded from

630 POSTGRADUATE MEDICAL JOURNAL December i95
.1
COa
FIG. 3 (a).-Colles fracture with inferior radio-ulnarsubluxation.The patient, a man aged 32, complained of pain
over the ulnar aspect of the wrist, weakness of gripand inability to rotate the forearm.
TreatmentActive use of the shoulder, elbow and hand from
the outset is an essential feature of the routinetreatment of a Colles' fracture and plays a largepart in the dispersal of oedema, thus materiallyhelping to prevent subsequent stiffness of thewrist joint.
Active use, hot wax baths and exercises super-vised by the physiotherapist should be instituted,and if after a lapse of several weeks a satisfactoryreturn of movement has not been regained, re-course may be had to manipulation under ageneral anaesthetic and followed by further activeexercises. Manipulation may be repeated ifnecessary.
5. Traumatic Arthritis of the Wrist JointThis condition is an infrequent sequel and by
comparison arises much more commonly afterfracture of the carpal scaphoid. There is no clear
C
CCl
I
FIG. 3 (b).-The same wrist after operation. Fullpainless function was regained.
explanation for this. Interruption of the con-tinuity of the articular cartilage by the fracture linealone is sufficient to initiate arthritic changes, andwhen, as in comminuted fractures, it is often im-possible to restore completely the anatomicalalignment of the articular surface, arthritis occursmore rapidly.
Major degrees of mal-union without recogniz-able interference with the articular cartilage bythe fracture are occasionally followed by arthritis.This is seen chiefly in those patients who makeconstant demands on their wrists at work (e.g.manual labourerr). The condition is then a sequel
Protected by copyright.
on 16 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.314.627 on 1 D
ecember 1951. D
ownloaded from

STEPHENSON: Some Complications of Colles' Fracture
to raised pressure on the articular surfaces andcontinued stresses on the ligaments.
It should be borne in mind that the so-calledtraumatic arthritis may be, in fact, an aggravationor reactivation, caused by the trauma, of a pre-existing chronic arthritis.
Clinical FeaturesThe symptoms may arise very soon after the
fracture or be delayed for years. The signs arethose of an osteoarthritis in any joint, and in theearly stages the diagnosis is based mainly on theclinical features, as the radiographic changes areminimal. Even when the arthritis is advanced,osteophytic lipping is not a well-marked feature inthe radiographs and is best looked for at the tipof the radial styloid process.
TreatmentMild cases benefit by suitable physiotherapy.
When the arthritis is well established the treatmentdepends upon the severity of the symptoms, theoccupation and age of the patient. A mouldedleather wrist support is adequate for the majorityof patients and arthrodesis of the wrist joint isonly rarely indicated.
6. Pain over the Ulnar Aspect of the WristThis is a fairly common complaint after fixation
has been discarded. Although the symptoms maybe present when there is non-union of a fracture ofthe ulnar styloid process, in the writer's experienceit is more frequently found when no such fracturehas been sustained. The pairi is then attributableto an unhealed sprain or partial rupture of theinternal lateral ligament of the wrist, and it maywell be that even in the presence of non-union ofthe ulnar styloid process, the discomfort isligamentous in origin. A point of local tendernessis consistently found close to the proximal attach-ment of this ligament.
TreatmentThe discomfort is almost always of temporary
duration and responds to diathermy.
7. Late Rupture of the Extensor PollicisLongus Tendon
This is an uncommon but well-recognizedcomplication. Formerly it was thought that therupture was due to a process of attrition caused byroughness of the tendon groove on the dorsum ofthe lower end of the radius. However, in a sub-stantial proportion of the reported cases, no re-duction of* the fracture was required and noroughening of the groove found subsequently atoperation. At the present time it is held that anavascular necrosis of the tendon occurs following
injury to the meso-tendon with haematoma forma-tion and subsequent fibrosis. Operative findingstend to support this view (Trevor, 195o). Thelesion is found near the lower border of the dorsalcarpal ligament. At operation in recent ruptures,bruising, yellowish discoloration and fraying ofthe tendon ends may be seen. Only occasionally isroughening of the tendon groove found.
Clinical FeaturesFemales preponderate and the patient is usually
over 50 years of age. The youngest patient re-corded is a girl aged I4 years (McMaster, 1932).Local pain and swelling may precede the rupture,which is sometimes heralded by a sudden snap.In other patients, inability to extend the inter-phalangeal joint of the thumb is the first com-plaint.
Physical examination reveals inability to extendthe interphalangeal joint, slight limitation ofabduction of the thumb and absence of the sub-cutaneous bow-string which is formed by the intacttendon.
TreatmentSatisfactory results have been obtained from a
variety of operations, but the result followingdirect end-to-end suture is always unpredictable.Among the many operations performed are:
(a) Transference of the extensor indicis propriusto the distal end of the tendon. This operationgives gratifying results "and causes minimal inter-ference with the function of the index finger, theonly disability being a suggestion of weakness ofextension and a tendency to radial deviation of thedigit at the metacarpo-phalangeal joint. As theextensor indicis tendon lies on the ulnar side ofthe tendon of the extensor communis digitorum,the unopposed action of the latter tendon leads tothe slight radial deviation.
(b) Suture of the distal end of the tendon to theextensor brevis pollicis or to both the extensorbrevis pollicis and abductor pollicis longus.
(c) A free tendon graft.(d) Transference of extensor carpi *radialis
longior or brevior into the distal end of thetendon.
(e) Restoration of the continuity of the tendonby using nylon suture material, fibrous tissueultimately bridging the gap between the tendonends (Trevor, 1950).
8. Sudeck's Atrophy (Post-Traumatic Osteo-Dystrophy)
Sudeck's atrophy may follow a Colles' fracture,but is a relatively more common complication ofminor injuries of the wrist. Its aetiology is notfully understood. It is believed that the injury
F
Dcem7ber x 95 I 631P
rotected by copyright. on 16 M
ay 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.27.314.627 on 1 Decem
ber 1951. Dow
nloaded from

632 POSTGRADUATE MEDICAL JOURNAL December '1I
initiates an abnormal reflex arc, with pain im-pulses forming the afferent side and sympatheticimpulses, both vasoconstrictor and vasodilator,the efferent.
Clinical FeaturesAttention is first drawn to the dystrophy a few
weeks after the injury by pain, with stiffness ofthe w.rist and fingers which is at first due to musclespasm. The pain is materially aggravated bymovement. Vasomotor changes take the form ofa cyanotic, moist, glossy skin.
In radiographs the degree of decalcification isfar greater than that of a simple disuse atrophy.There is at first a patchy decalcification of thebones of the wrist and hand which is seen especiallyclose to the joints; later the decalcification be-comes diffuse, leading to a glassy appearapce. Invery severe and protracted types there may befibrous ankylosis of the carpal joints.
TreatmentTreatment is unsatisfactory, but wax ba.ths,
active use, encouragement and the passage of timemay effect a cure. Immobilization, deep X-raytherapy, injections of local anaesthetic into thecervico-dorsal sympathetic chain and preganglioniccervico-dorsal sympathectomy have been triedwith varying success. Sympathectomy has littleor no effect on the bone changes but relieves thepain temporarily and may abolish the vasomotorphenomena.
PrognosisFull recovery is unlikely. Only when the
dystrophy is mild can a good recovery be an-ticipated, and when severe, a substantial residualdisability is to be expected (Klser Sven, I947-8).
9. Injuries of the Median NerveAn incomplete lesion of the median nerve,
sustained at the time of injury or following re-duction, is by no means uncommon. lt is due to acontusion of the nerve. Clinically it is found thatthe sensory supply of the nerve is partially affected;the motor side almost invariably remains intact.The patient complains of numbness of one ormore digits in the median distribution and onexamination there is impairment but not completeloss of sensation in the affected skin area. As theloss of sensation is only of temporary duration,no treatment is required.More serious injuries of the nerve due to
anterior displacement of bone spicules have beendescribed but are rare. Lesions of the superficialbranch of the radial nerve may also occur.
Io. Prolonged Absence from WorkThis is frequently due to uncomfortable primary
splintage and to failure of the surgeon to insist onactive use of the limb at once. In some modernindustrial centres workers often lose less than aday off work owing to the immediate provision ofsuitable employment.
BIBLIOGRAPHY
BOYD, H. B., and STONE, M. M. (I944),J. Bone Jt. Surg., 26, 313.CHARNLEY, J. (I950), 'Closed Treatment of Common Fractures,'
Edinburgh: Livingstone.KLSER SVEN (1947-48), Acta Orthopaed. Scand., I7, 253.
LIPPMAN, R. K. (I937), Arch. Surg., 35, 772.McMASTER, P. E. (I932), J. Bone Yt. Surg., I4, 93.PATRICK, J. (1946), Ibid., 28, 737.TREVOR, D. (1950), Ibid., 32b, 370.
Protected by copyright.
on 16 May 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.314.627 on 1 D
ecember 1951. D
ownloaded from