communication and team building: practical strategies for clinical practice€¦ · practical...
TRANSCRIPT

ANCC.EliteCME.com Page 1
Chapter 1: Communication and Team Building: Practical Strategies for Clinical Practice
2 Contact Hours
Release Date: 8/2/2016 Expiration Date: 8/2/2019
AudienceThe target audience for this education program is nurses who want to: 1) Enhance their ability to communicate effectively in order to
advocate for patients, families, and themselves; and 2) Improve their teambuilding skills.
Purpose statementErrors in health care cost millions of dollars each year as well as countless loss of life. Good and clear communication is a key to the prevention of medical errors and helping to ensure a healthy work
environment. This course focuses on practical strategies for the improvement of both verbal and non-verbal communication.
Learning objectives � Explain how appearance can influence professional
communication. � Describe effective non-verbal communication strategies. � Demonstrate effective verbal communication strategies. � Describe de-escalation techniques for defusing anger and agitation. � Explain strategies for effective written, telephone, and social
media communication.
� Examine communication techniques associated with medical errors.
� Describe how communication failures contribute to medical errors. � Discuss the incidence and prevalence of various types of
workplace bullying. � Identify effective strategies to defuse workplace bullying. � Discuss effective team building strategies in healthcare.
How to receive credit ● Read the entire course online or in print which requires a 2-hour
commitment of time. ● Depending on your state requirements you will asked to complete
either: ○ An affirmation that you have completed the educational
activity.
○ A mandatory test (a passing score of 70 percent is required). Test questions link content to learning objectives as a method to enhance individualized learning and material retention.
● Provide required personal information and payment information. ● Complete the MANDATORY Self-Assessment and Course
Evaluation. ● Print your Certificate of Completion.
Accreditations and approvalsElite is accredited as a provider of continuing education by the American Nurses Credentialing Center’s Commission on Accreditation.
Individual state nursing approvalsIn addition to states that accept ANCC, Elite is an approved provider of continuing education in nursing by: Alabama, Provider #ABNP1418 (valid through April 30, 2017); California Board of Registered Nursing, Provider #CEP15022; District of Columbia Board of
Nursing, Provider # 50-4007; Florida Board of Nursing, Provider #50-4007; Georgia Board of Nursing, Provider #50-4007; and Kentucky Board of Nursing, Provider #7-0076 (valid through December 31, 2017).
FacultyAdrianne Avillion, D.Ed., RN
Adrianne E. Avillion, D.Ed., RN, is an accomplished nursing professional development specialist and healthcare author. She earned a doctoral degree in adult education and a M.S. in nursing from Penn State University and a BSN from Bloomsburg University. Dr. Avillion has held a variety of nursing positions as a staff nurse in critical care and physical medicine and rehabilitation settings as well as leadership roles in professional development. She has published extensively and is a frequent presenter at conferences and conventions devoted to the specialty of continuing education and nursing professional development. Dr. Avillion owns and is the CEO of Strategic Nursing Professional Development, a business that specializes in continuing
education for healthcare professionals and provides consulting services in nursing professional development. Her most recent publications include The Path to Stress-Free Nursing Professional Development: 50 No-Nonsense Solutions to Everyday Challenges and Nursing Professional Development: A Practical Guide for Evidence-Based Education.Content ReviewerSusan Reese, MSN, RNActivity DirectorJune D. Thompson, DrPH, MSN, RN, FAEN, Lead Nurse Planner

Page 2 ANCC.EliteCME.com
DisclosureResolution of Conflict of InterestIn accordance with the ANCC Standards for Commercial Support for continuing education, Elite implemented mechanisms prior to the planning and implementation of the continuing education activity, to identify and resolve conflicts of interest for all individuals in a position to control content of the course activity.
Sponsorship/Commercial Support and Non-EndorsementIt is the policy of Elite not to accept commercial support. Furthermore, commercial interests are prohibited from distributing or providing access to this activity to learners.
DisclaimerThe information provided in this activity is for continuing education purposes only and is not meant to substitute for the independent
medical judgment of a healthcare provider relative to diagnostic and treatment options of a specific patient’s medical condition.
©2016: All Rights Reserved. Materials may not be reproduced without the expressed written permission or consent of Elite Professional Education, LLC. The materials presented in this course are meant to provide the consumer with general information on the topics covered. The information provided was prepared by professionals with practical knowledge of the areas covered. It is not meant to provide medical, legal, or professional advice. Elite Professional Education, LLC recommends that you consult a medical, legal, or professional services expert licensed in your state. Elite Professional Education, LLC has made all reasonable efforts to ensure that all content provided in this course is accurate and up to date at the time of printing, but does not represent or warrant that it will apply to your situation nor circumstances and assumes no liability from reliance on these materials. Quotes are collected from customer feedback surveys. The models are intended to be representative and not actual customers.
IntroductionMembers of the interdisciplinary stroke rehabilitation team are meeting to discuss Mrs. Peterson, a 75-year-old female who suffered an ischemic stroke ten days ago. Maryanne, a registered nurse with five years of experience working with stroke patients, represents nursing at the meeting. It is a lively meeting and most members are in agreement that Mrs. Peterson is ready for discharge to her home, where she lives with her husband. Therapy representatives speak confidently about Mrs. Peterson’s progress, and Dr. Thomas, the team’s physiatrist (i.e. a physician who specializes in physical medicine and rehabilitation) agrees with them. One-by-one, team members give their input in an assertive manner. Maryanne, known as a “good” nurse who is quiet and unassuming, patiently waits for her “turn” to speak. She and other nurses on the stroke rehabilitation unit have some concerns that Mrs. Peterson becomes confused at night and has difficulty ambulating and concentrating after 9PM. As the meeting concludes, Maryanne still has not presented her concerns. She attempts to do so as the therapists prepare to leave the meeting room. They assure Maryanne that Mrs. Peterson is “probably just tired that late in the evening.” The physiatrist agrees, and discharge is planned for tomorrow. Maryanne is furious and returns to the nurses’ station. She and her nursing colleagues vent their anger and complain that they are not respected and that “without nursing” no one would ever be rehabilitated. The nurse manager overhears this conversation and asks to speak to Maryanne privately. Maryanne insists that the nurse manager talk to the physiatrist about the lack of respect shown to nurses. The manager asks Maryanne, “What did you do to earn their respect today? More importantly, what did you do to serve as the patient’s advocate?”
During a quarterly education meeting of the local chapter of Sigma Theta Tau International (STT, The Honor Society of Nursing), a nurse presented the research findings from her doctoral dissertation. She recently earned a doctor of nursing science (DNS degree), and her colleagues are justifiably proud of her. The nurse presented her findings clearly and concisely, appearing slightly nervous, understandable given that this is the first time she is presenting in front of a group. At the conclusion of her presentation, she faced the group and encouraged them to participate in nursing research saying, “So you see, even a little tiny person like me can make a difference.”
Mark is being oriented to his new position as an intensive care nurse. His preceptor, Elaine, has over ten years’ experience as a critical care nurse in various settings. She is impatient with Mark and continually
makes negative comments about having to orient new nurses in front of other nurses and patients. Elaine is supervising Mark as he prepares to administer Lasix intravenously over a period of one to two minutes via hospital policy. Elaine rolls her eyes and tells Mark to just, “Shove it in. No one takes that long to give Lasix in the real world.” Mark hesitates, and Elaine grabs the syringe and swiftly administers the drug. The patient does not suffer any adverse effects. Mark is angry and, after his shift is over, approaches the nurse manager about Elaine’s behavior. The nurse manager tells Mark, “Elaine is one of the best nurses I have. She must have given the drug correctly. And as for the way she talks to you and about you…Did you do anything to stop her from treating you like this? She is a bit of a bully, but you either have to stand up to her or just put up with her. If you want to work on this unit it is best to just figure out a way to get along with her.”
● Why should Maryanne, or any nurse for that matter, wait for her “turn” to present critical information essential to the patient’s wellbeing?
● Why would any nurse, let alone a nurse who has earned a doctorate and conducted research to improve patient care, describe herself as a “little tiny person,” thereby diminishing her achievements and disrespecting herself?
● Why would a nurse allow him/herself to be bullied and observe unsafe patient care regardless of what an inappropriate nurse manager says or how an ineffective preceptor behaves?
The preceding three scenarios, all based on actual events, are all too common occurrences. All three violate principles of good communication and, in the last scenario, appropriate patient care. It is likely that most, if not all nurses, would be able to describe the principles of good communication if asked. Multiple education programs describe how to communicate effectively and are offered in the hope that education will improve communication, which is essential to the provision of safe and effective patient care. However, education regarding “good” communication is ineffective unless such education addresses the communication process as it exists in the actual work setting.
This education program provides information about practical strategies to enhance professional communication and improve team functioning in the actual work setting.

ANCC.EliteCME.com Page 3
APPEARANCE AND ITS IMPACT ON PROFESSIONAL COMMUNICATIONRoberta is the nurse manager of an adult surgical unit in a large metropolitan medical center. After a ten-hour day, she is longs to go home and forget about the problems at work. A knock at her office door makes her pause. The daughter of a patient asks to speak to her. The daughter tells Jennifer that, “I am not pleased at all with some of the ways the nurses are taking care of my mother. I do not even know who the nurses are; you cannot tell nurses from the people who deliver the meal trays. The one who was taking care of my mother today had on some kind of baggy top and pants with cartoon characters all over them and dirty sneakers. Her fingernails were about an inch long and when she went to change my mother’s dressing, her nails actually scratched my mother! What is going on? What kind of hospital is it where you cannot tell who is who and the nurses look like they just got out of bed without even combing their hair?!
Members of several hospitals and colleges of nursing organized a nursing conference to showcase staff nurses who have successfully conducted nursing research projects. Most of the presenters were female nurses, but two presenters were male nurses. The male nurses were dressed in coats and ties and present with confidence. Many of the female presenters were dressed in business attire, but at least half were very casually dressed: one in jeans and a hoodie sweater and others in sneakers and slacks and sweatshirts. The female nurses, with two exceptions, apologized for coming “unprepared,” and all giggled intermittently throughout their presentations. At the end of the day, several awards were presented for best presentation and best research projects. The two male nurses won all of the awards. Afterwards some of the female presenters complained about the favoritism shown to male nurses.
Members of the Nursing Practice Committee at a large community hospital are working to help revise the department’s dress code. The
issue of piercings comes up and many of the committee members believe that nose rings, lip rings, tongue rings, etc. should be prohibited. One of the committee members protested, saying that wearing a nose ring was important to her cultural background and that prohibiting them was disrespectful and prejudiced. After considerable debate, small nose rings were approved to be worn. Later that week, the nurse manager of the traumatic brain injury rehabilitation unit asked one of the nurses on the unit to remove her nose ring because of the danger of injury. “Many of our patients are very agitated and confused, and I am afraid that you will be hurt if one of them pulls out your nose ring.” The nurse objected and filed a complaint with the director of nursing, who reprimanded the nurse manager for violating the dress code. The next day an agitated patient pulled out the nose ring, and the nurse suffered lacerations, which ultimately became infected.
Some people may argue that professionals should not be judged on appearance. However, the three preceding scenarios, again adapted from real-life situations, show that appearance plays a role not only in communication, but also in professionalism and safety.
● Why would nurses choose to compromise their professionalism and/or safety by dressing inappropriately?
● How is communication affected by appearance?
Communication is integral to all aspects of nursing care including interacting with patients, team members, or leadership members. Appearance plays a significant role in communication. The appearance nurses and other healthcare professionals present is very important. Appearance is a sensitive subject for many people. But with the current trend of “casual” dress, appearance can enhance or undermine career possibilities as well as potentially compromise patient care.
Advice from the business worldBusiness experts offer the following advice regarding appearance [1]:
● First impressions count. A patient, family member, colleague, or prospective employer forms impressions of the nurse the instant they meet him or her (him/her). Some business experts refer to proper dress and appearance as one of the major ways to earn instant respect. An impeccably dressed professional may ultimately perform his/her job poorly, and an inappropriately dressed professional may turn out to be the best nurse on the unit; however, a negative first impression may mean someone does not get a “second chance” to show he or she (s/he) is a competent professional.
● Appropriate dress empowers a person. Confidence, self-esteem, and self-empowerment can begin with looking best. Research shows that people who dress appropriately and professionally are more likely to garner respect from colleagues, subordinates, and supervisors.
Nursing consideration: Confidence, self-esteem, and self-empowerment make it easier to communicate and to serve as patient and nursing advocates.
● Hygiene is more important than the cost of clothing. Research also shows that good hygiene is associated with generating a positive impression. Clean, wrinkle-free clothes, polished shoes, fingernails that are short and clean, and adherence to personal hygiene are essential to making a good impression, dressing appropriately, and working with confidence.
● Dress for the role. Nurses dress in the uniform/scrubs designated by the facility in which s/he works. But if that nurse is a presenter at a conference or is representing the organization at a business meeting, business attire (e.g. not jeans and sweatshirts as in the second scenario example) such as a dress, or coat and tie is the expected norm.
Nurses and other clinicians may argue that they are not working for a business. That is a mistaken notion. Healthcare facilities are businesses; they are in the business of healthcare, and first impressions affect how well patients and families interact with those entrusted with their care.
Advice from the nursing worldDress codes in nursing must be practical. Nurses should be able to wear clothing that is comfortable and allows freedom of movement. Scrubs are often the uniform of choice and meet the criteria for most nurses. But nurses must be sure to present a professional appearance at all times. They must also be sure that their manner of dress adheres to infection control standards.
A review of the literature shows that appearance and communication effectiveness are linked. The professional part of nursing includes behavior and image as they relate to establishing and maintaining
trusting relationships and creating a healing environment [2]. Image contributes to the legitimization of status and is reflected in personal hygiene, clothing, jewelry, and make-up [3].
The literature also shows that nurses want to be recognized and respected for their knowledge, not their appearance. However, patients want healthcare professionals to appear professional and recognizable. They want to be able to distinguish between registered nurses, nursing assistants, lab technicians, and housekeeping personnel [2].
Page 4 ANCC.EliteCME.com
Many healthcare organizations use an evidence-based approach in creating dress codes by reviewing the literature and conducting in-house studies. Some nurses feel strongly about being able to wear various types of jewelry or long, artificial fingernails. However, while respecting the right to self-expression, it is important to recognize how such self-expression affects patients and impacts professional image [4].
EBP alert! Some experts recommend that organizations take the time to investigate patient preferences as they develop and implement dress codes. Results of a study published in a 2013 issue of The Journal of Nursing Administration indicated that patients’ preferences were [2]:
○ Not in favor of all white uniforms. ○ Not in favor of nurses wearing perfume, body piercings,
excessive jewelry, and/or long nails. ○ For hair to be worn off the shoulders. ○ For any color uniform. ○ For all nurses to have short, clean fingernails. ○ For nurses to wear clean clothes and shoes. ○ For healthcare workers to wear identification indicating their
role (e.g. RN, LPN, etc.).
EBP alert! Nail enhancements such as artificial nails, wraps, tips, acrylics, gels, etc. are often points of contention when developing a dress code. Some organizations now prohibit nurses from wearing any type of nail enhancement. Research shows that outbreaks of infections have been traced to healthcare workers’ artificial fingernails. Research also shows that hospital workers with nail enhancements can have more bacteria both before and after hand washing than workers with natural nails. It is recommended that natural nails be kept short, clean, and not extend past the fingertips [5].
In summary, appearance is linked to professionalism and effective communication. Recommendations for professional appearance based on findings from research studies include [1,2,3,4,5]:
● Wear only uniforms or scrubs that are clean, without wrinkles, and in good repair.
● Wear shoes that are clean and in good repair. ● Keep jewelry to a minimum and on a small scale. Jewelry that is
large or has sharp edges, for example, can scratch patients and compromise skin integrity. Large earrings or long necklaces can be grabbed by agitated patients and can injure the nurse.
● Conforming to the healthcare facility’s dress code. ● That a professional appearance is linked to effective
communication.
EFFECTIVE NON-VERBAL COMMUNICATIONCharlotte is acting as preceptor to a newly licensed RN. Ellen, the “new” RN is eager to learn and is progressing well through orientation. Today Charlotte is observing as Ellen teaches a patient and his family about medications he will be taking upon discharge. Ellen sits down with the patient and provides a thorough explanation of the prescribed medications. She evaluates how well the patient and family have learned about the medication by asking them to verbally tell her important factors, such as when and how to take the medication, what side effects are possible, and what to do if side effects occur. However, throughout the teaching session Ellen swings her foot back and forth, which seems to distract the patient. She also taps her finger on the bedside table as she conducts the teaching session. Later, Charlotte tells Ellen that she provided complete and accurate information and did a good job evaluating how well the patient and family acquired the necessary knowledge. However,
Charlotte also tells Ellen that her non-verbal communication may have been distracting to the patient and family and offers her some suggestions to improve these non-verbal skills. Ellen tells Charlotte, “I am glad you told me. You know I was a little nervous and did not even realize that I was swinging my foot or tapping on the table!”
The preceding scenario shows how easy it is to display nervousness without being aware. Non-verbal communication can have a significant impact on patient care. It can also have a significant impact when communicating with colleagues.
There can be a significant difference between the words people speak and what their non-verbal behaviors indicate. This is sometimes referred to as sending mixed messages, i.e. saying one thing while non-verbal behaviors or body language indicates something different. It is imperative that nurses reconcile their verbal and non-verbal communication.
First impressionsThe importance of first impressions has already been mentioned in regards to professional appearance. And, linked to professional appearance, is the ability to communicate confidence with non-verbal (as well as verbal) appearance [6]. For nurses who want to project confidence, whether working with patients, meeting with colleagues, or speaking in public, some basic body language initiatives include [6]:
● Posture: Stand or sit “tall” with shoulders back. Do not slouch. ● Eye contact: Maintain eye contact unless it is culturally
inappropriate. ● Facial expression: Have a calm, pleasant expression and do not
frown. Smile as appropriate. Keep facial muscles relaxed. ● Gestures: Hand and arm movements should be purposeful and
deliberate. Avoid fidgeting or meaningless, distracting gestures such as swinging feet or tapping an object with a pen or finger.
● Look interested: An attentive expression indicates active listening and interest in communicating with others.
Nursing consideration: When nurses are about to enter into a situation where they are not as confident as they would like to be (such as facing an angry family member or presenting information at an important clinical patient conference), they should pause for a moment, take a deep breath and “check” their body language to incorporate the preceding suggestions for confident body language.
ANCC.EliteCME.com Page 5
Detecting non-verbal signs of defensivenessIt is important for nurses to be able to recognize how their body language may project feelings of defensiveness; a behavior that is the result of preparing to defend oneself against criticism or attack. It is equally important to be able to detect feelings of defensiveness in others. Facing challenging situations can trigger defensiveness. Dealing with a performance appraisal, anticipating presenting clinical findings to a group of colleagues during grand rounds, or correcting the behavior of a subordinate can spark defensiveness. Here are some non-verbal behaviors that indicate defensiveness [6]:
● Hand and/or arm gestures that are small and close to the body. ● Minimal facial expressions.
● Body physically turned away from the person who is attempting to communicate with him/her.
● Arms crossed in front of the body. ● Eyes downcast. ● Minimal eye contact.
Nursing consideration: By picking up on signs of defensiveness, nurses may be able to help others (such as patients or colleagues) to become calmer as well as help themselves regroup and reduce their own defensiveness.
Detecting signs that people are not listeningNurses are often called upon to speak to individuals as well as large and small groups in healthcare settings. Examples include providing patient education to patients and families, presenting clinical information during change of shift, team or committee meetings, and presenting a paper or poster at a nursing conference. It is important to be able to “pick up” on signals that the “audience” is not interested or is unable to comprehend what is being said.
Behaviors that indicate lack of engagement include when “audience” members [6]:
● Keep their heads down. ● Look around the room but not at the presenter. ● Continually check smart phones. ● Fiddle with clothing or papers. ● Are sitting in a slumped position. ● Fidget. ● Doodle or write on paper.
Nursing consideration: When a nurse detects that someone is not aying attention, s/he needs to re-engage the audience by [6,7]:
● Making sure his/her own body language is engaging, and not defensive or agitated, or showing obvious signs of nervousness such as giggling or wringing hands.
● Making sure s/he is displaying confident body language. ● Showing enthusiasm for whatever is being discussed. If the
nurse is bored, the audience will likely also be bored. ● Refocusing the audience by asking a direct question. ● Clarifying if the audience understands, and if the speaker can be
heard and is speaking clearly and distinctly. ● Allowing time for a brief “stretch” break. ● Asking the “audience” if they have any questions.
These suggestions can be especially important when conveying patient education. In this case, an audience of one requires that the nurse continually observe him/her for attentiveness. Failure to absorb the information the nurse is relaying can have serious consequences post-discharge. At the conclusion of the teaching session, knowledge acquisition must be assessed. Never assess knowledge by asking yes and no questions. Instead have patients/families demonstrate how to change a dressing, list side effects of medication, etc. [7].
Signs that someone is lyingDetecting signs of lying can be important when assessing patients, families, and colleagues for behaviors that are less than truthful. Are patients/families lying about being ready for discharge? Are colleagues lying about completing necessary competency work? The following signs are not proof of lying, but can provide clues that someone is not being honest in communication [6]:
● Little or no eye contact. ● Rapid eye movements with constricted pupils. ● Hands or fingers placed in front of the mouth when speaking.
● Body turned away from other persons. ● Unusual or unnatural body gestures. ● Reddened face or neck. ● Increased perspiration. ● Voice changes such as throat clearing, stammering, and/or changes
in pitch.
If these signs are noted the nurse needs to ask more questions or ask for more detailed information to help determine if someone is being truthful or not.
Some words about personal space Personal space is “the area surrounding an individual that is perceived as private by the individual who may regard a movement into the space by another person as intrusive” [8]. Personal space varies among cultures and, to a certain extent, from person to person. Here are some generalities about Americans’ perceptions of personal space [9]:
● Personal space begins to develop around the age of three or four. ● Personal space can be classified according to four categories:
intimate space, personal space, social space, and public space. ● Intimate space extends about 18 inches in every direction. Family,
pets, and one’s closest friends are those who can comfortably enter this space.
● Personal space extends from 1.5 to four feet away from the body. Friends and acquaintances can enter this space, but strangers are definitely forbidden from entering this space.
● Social space extends from four to 12 feet away from the body. This is the space within which people feel comfortable interacting with new acquaintances or strangers.
● Public space is beyond 12 feet and is open to everyone.
Nursing consideration: Nurses must continually enter patients’ intimate space as part of routine nursing care. It is essential that nurses and all other healthcare professionals show utmost respect for patients in these situations. Keep patients covered as much as possible, close doors, and draw bed curtains. Space considerations are also important when interacting with colleagues. Types of personal space must be respected at all times.

Page 6 ANCC.EliteCME.com
Conclusion: Summary of effective non-verbal communication strategiesNurses must be alert to non-verbal communication behaviors. Even in the midst of the busiest of days, proper non-verbal communication can go a long way to enhancing over-all communication as well as earning the respect of colleagues and defusing potentially argumentative situations. Important non-verbal communication behaviors include [1,5,6,7]:
● Dress appropriately. Clothes and shoes should be clean and neat and fingernails short and clean. Jewelry should be kept to a minimum.
● Display interest and empathy. Pay attention to those involved in the interaction. Show interest and, as warranted, compassion. Do not rush or show impatience.
● Display confidence. Stand or sit “tall.” Do not slump. ● Keep gestures purposeful and to a minimum. Avoid nervous,
repetitive gestures. Keep arms at sides. Avoid crossing arms across the body.
● Practice appropriate body language. Observe body posture and gestures in a mirror.
● Pay attention to the body language of others. If body language indicates disinterest or annoyance, stop and calmly ask for clarification. Do not allow personal body language to reflect the anger or fears of others. Stay calm. Anger, fear, frustration, and other emotions can be contagious.
● Maintain appropriate distance from others. Respect personal space.
Nursing consideration: Nurses may feel that they do not have time to focus on some issues of non-verbal communication. However, everyone looks in a mirror at least once a day. Double check appearance. Observe posture. Look at facial expressions. A nurse may not realize that although s/he is telling patients or colleagues that s/he has time to talk or to help, his/her facial expression is indicating something quite different. Taking a second to take a deep breath and compose oneself makes it easier to present body language that is appropriate to the situation.
EFFECTIVE VERBAL COMMUNICATIONStacey is an RN who is preparing to present a paper about her work on a pediatric oncology unit. She has worked on the unit for three years, and is both excited and nervous about speaking to a large group of colleagues at a national pediatric nursing conference. Stacey presented the paper to a local chapter of the Society of Pediatric Nurses, but was dissatisfied with the outcome. A number of nurses seemed to lose interest in what she was saying. Stacey asks her mentor Josie, an RN with 15 years of experience in pediatrics who has presented at several nursing conferences, for help. Josie looks and listens as Stacey “presents” the paper to her. Josie compliments Stacey on her knowledge and the work she has put into the presentation. But, she says, “You do not sound confident. You frequently giggle, speak in a very soft voice, and keep saying, ‘you know, you know’. We will record your presentation so you can hear how you sound and make some improvements.”
James is an RN preparing to teach Sandy, a 32-year-old woman with Stage-III breast cancer, and her husband Phil how to take care of her surgical wound. Sandy has had a mastectomy and will be going home with two drains in place as well as a wound dressing. James is a bit apprehensive. He knows that Sandy is fearful and angry about “having to get cancer.” Her husband is fearful and has privately told James that, “I do not know if I can deal with this.” James takes a deep breath to calm himself and enters Sandy’s room. James starts by greeting both Sandy and Phil, and starts by telling them, “I know this is a difficult time. What I want to do today is help you to learn how to change the dressing and deal with the drains until they are removed next week when you see your surgeon at her office. I also want to answer questions you may have and do my best to help you get ready to go home.”
Roberta is the nursing representative at interdisciplinary rounds. In the past, she has had difficulty engaging other members of the team and has been hesitant in presenting patient information from the nursing perspective. Today, however, she speaks confidently. She stands tall and speaks in a clear, concise manner in a tone of voice that is easily
heard by everyone. After rounds are over, a physician stops her and asks, “What happened to you? Frankly, I usually do not pay much attention when you speak, but today you brought up some really important patient information.” Roberta smiles and tells him, “I have learned to communicate as a patient and nursing advocate!”
What do the preceding three scenarios have to say about verbal communication? In the first scenario, Stacey is an ineffective communicator because her verbal behaviors are distracting and indicate a lack of confidence. In the second scenario, James is an example of good verbal communication. He tells his patient and her husband what he is going to do, acknowledges they are facing a difficult situation, and is empathetic as he offers them his help. The final scenario is an example of a nurse who has learned to enhance her verbal communication skills and is now an effective patient and nursing advocate.
Nursing consideration: Various factors impact nurses’ communication with patients, families, and colleagues. Nurses have the same emotional responses to life as everyone else and experience anxiety, stress, fears, and personal biases. It is imperative that nurses learn to understand their personal responses and to control their emotions as they communicate with others [10].
Effective verbal communication requires that the nurse express her/his ideas and viewpoints clearly, concisely, and confidently. Language should be adapted in content and style to suit the audience [11].
EBP alert! Research shows that effective communication requires the use of empathy. Empathetic communication requires that nurses attempt to understand the perspective and viewpoint of the person or persons with whom they are communicating. It also requires that the nurse focus on the message the patient, family member, or colleague is trying to convey [10].
General principles of effective verbal communicationNurses are busy professionals and must work efficiently to accomplish all that is necessary in a work shift. Because of such time constraints, it is essential that communication with patients and families be completed effectively. This means nurses must take the time to incorporate principles of good verbal communication into everyday speech. This is also important when communicating with peers and
supervisors. A major point to remember is that good communication skills apply to every communication situation. Here are some basic general recommendations to implement when communicating verbally [10,11,12]:
● Remember to reconcile verbal and non-verbal communication techniques. Words must match body language.

ANCC.EliteCME.com Page 7
● Listen attentively. Express interest in what others are saying and how they are behaving. Do not interrupt or try to finish someone’s sentences or anticipate their thoughts and feelings.
● Be aware of any personal prejudices or misconceptions that may exist as well as those of with whomever s/he is communicating.
● Be objective. Do not show disgust, amusement, or annoyance. ● Speak clearly and concisely. Do not mumble. Do not rush or speak
rapidly. ● Be aware of the pitch and loudness of the voice. High-
pitched tones are difficult for older adults to hear. Some people, particularly younger women, speak in high-pitched tones. Research shows that lower pitched tones are easier to hear and covey confidence compared to high pitched tones. Speak loudly enough to be heard. Do not shout, but do not whisper.
● Do not turn every statement into a question. It seems to be a habit for some people to raise the pitch of their voices at the end
of statements, making the statements sound like questions. Avoid this habit.
● Use terminology appropriate to the situation. For example, when talking to patients avoid sophisticated healthcare terminology. When speaking to colleagues, be sure to use professional terminology. Avoid slang and profanity when talking to patients and when addressing professional colleagues.
Nursing consideration: It is easy to tell nurses to “take your time when you communicate” but this is not always easy to accomplish in practice. There are always so many tasks to complete and responsibilities to fulfill. However, it is actually quicker to take the time to communicate carefully and deliberately as it helps to provide information accurately the first. Speaking rapidly and in a hurry usually means that information will need clarification or that mistakes will be made because of misunderstandings or miscommunication.
Therapeutic communication techniquesBefore discussing therapeutic communication techniques, it is helpful to take the time to think about questions. Nurses always ask questions. They need to ask questions in order to assess patients’ state of health and well-being. They need to ask questions of colleagues in order to
acquire information needed to provide the best possible patient care. It is important for nurses to know how to ask questions appropriately (i.e. therapeutic communication) as well as how not to ask questions.
How NOT to ask questionsHere are some question types of avoid [11,12]:
● “Yes and no” questions: Questions that require only a simple response do not provide opportunities for discussion. For example, do not ask a patient, “Do you understand how to change your dressing after you go home?” Patients may say “yes” just to end the conversation or to avoid admitting they do not understand how to do something. Instead the nurse may say, “I am going to watch you change your dressing today. I want to be sure you are able to do this at home and I want to give you a chance to ask me any questions you may have.” When presenting information to colleagues do not say, “Do you understand how to use the new infusion pump?” Instead say “I am going to watch you demonstrate how to use the new infusion pump so that we both can be sure you are comfortable with the procedure and I can answer any questions you may have.”
● Leading questions: These kinds of questions suggest the answer that the questioner wants to hear. For example, “You want to apply to the preceptor program, do you not?” or “You want your father to sign up for meals on wheels, right?” In other words, the person asking the questions is providing the answer to the question. This does not give the other person (e.g. patient, family, colleague, etc.) a chance to answer truthfully without fear of ramification.
● Negative questions or disapproval: Negative questions cast blame or seek to cast blame. For example, “Why did you not double check that insulin dose?” or “Whose fault is it that the infusion pump was set incorrectly?” or “Why were you late for the Nursing Research Council meeting?” Such questions trigger guilt, anger, and/or resentment and definitely do not enhance communication.
Good ways to ask questionsHere are some examples of “good” ways to ask questions [11]:
● Open-ended questions: These kinds of questions start with words such as how, what, where, when, etc. They encourage longer, more detailed responses. They also help people to clarify their thoughts and express themselves more clearly. For example, the nurse might say to a colleague, “What do you think about the proposed new policy concerning emergency response teams?”
● Clarifying questions: These questions summarize the speaker’s words and show that the nurse was listening attentively to the speaker. The nurse reflects back what the speaker by rephrasing her/his statements. For example, the nurse might say, “If I understand you correctly, you are saying that you believe
chemotherapy will make you feel worse than the cancer is making you feel.”
● Probing questions: Probing questions are actually statements that explore the speaker’s statements, behaviors, and beliefs more deeply. For example, “Explain what kinds of responsibilities you had when you worked as a nurse manager on a respiratory care unit.”
● Hypothetical questions: Hypothetical questions are especially useful during job interviews, competency assessments, or performance evaluations. An example would be: “How would you deal with a colleague who ridicules you in front of a patient?”
Therapeutic communication strategies Therapeutic communication is defined as the process of interacting that focuses on enhancing the physical and emotional well-being of a patient [13]. This definition can be expanded to include communication between colleagues. The purpose of therapeutic communication among professional colleagues is to enhance professional development and organizational effectiveness [7].
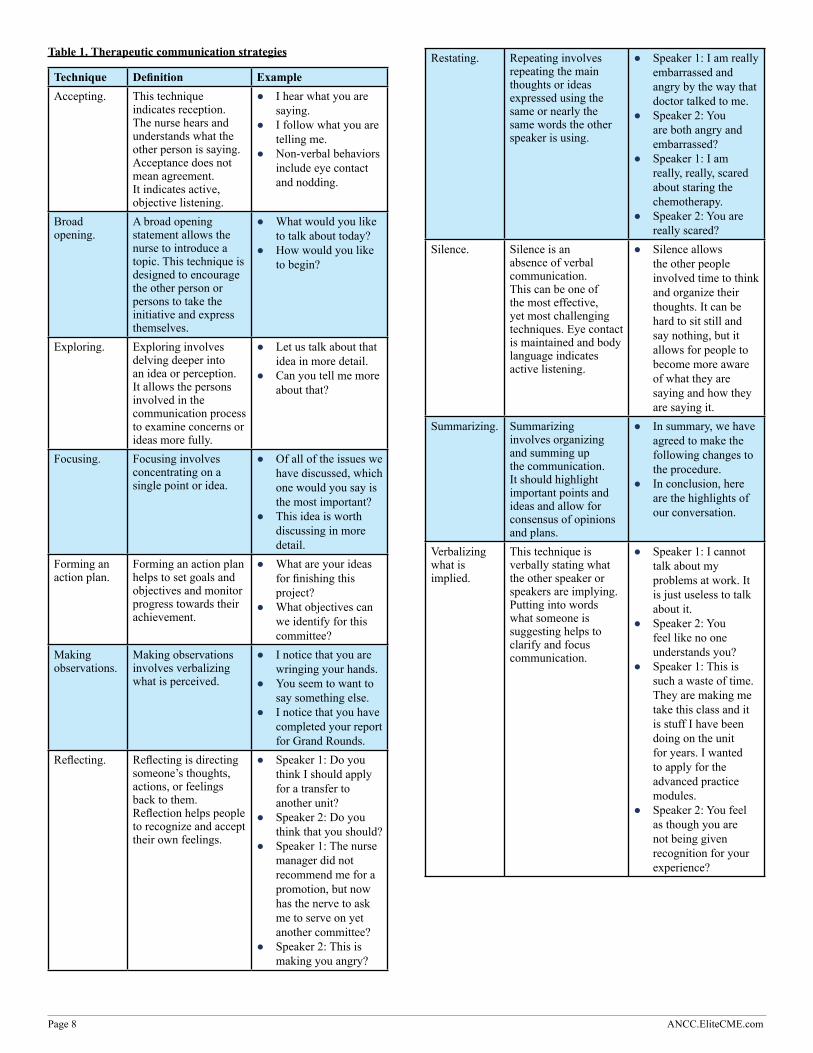
Table 1 contains some therapeutic communication strategies that should help to improve communication between healthcare professionals and patients or families as well as among healthcare professionals [11,12].
Page 8 ANCC.EliteCME.com
Table 1. Therapeutic communication strategies
Technique Definition ExampleAccepting. This technique
indicates reception. The nurse hears and understands what the other person is saying. Acceptance does not mean agreement. It indicates active, objective listening.
● I hear what you are saying.
● I follow what you are telling me.
● Non-verbal behaviors include eye contact and nodding.
Broad opening.
A broad opening statement allows the nurse to introduce a topic. This technique is designed to encourage the other person or persons to take the initiative and express themselves.
● What would you like to talk about today?
● How would you like to begin?
Exploring. Exploring involves delving deeper into an idea or perception. It allows the persons involved in the communication process to examine concerns or ideas more fully.
● Let us talk about that idea in more detail.
● Can you tell me more about that?
Focusing. Focusing involves concentrating on a single point or idea.
● Of all of the issues we have discussed, which one would you say is the most important?
● This idea is worth discussing in more detail.
Forming an action plan.
Forming an action plan helps to set goals and objectives and monitor progress towards their achievement.
● What are your ideas for finishing this project?
● What objectives can we identify for this committee?
Making observations.
Making observations involves verbalizing what is perceived.
● I notice that you are wringing your hands.
● You seem to want to say something else.
● I notice that you have completed your report for Grand Rounds.
Reflecting. Reflecting is directing someone’s thoughts, actions, or feelings back to them. Reflection helps people to recognize and accept their own feelings.
● Speaker 1: Do you think I should apply for a transfer to another unit?
● Speaker 2: Do you think that you should?
● Speaker 1: The nurse manager did not recommend me for a promotion, but now has the nerve to ask me to serve on yet another committee?
● Speaker 2: This is making you angry?
Restating. Repeating involves repeating the main thoughts or ideas expressed using the same or nearly the same words the other speaker is using.
● Speaker 1: I am really embarrassed and angry by the way that doctor talked to me.
● Speaker 2: You are both angry and embarrassed?
● Speaker 1: I am really, really, scared about staring the chemotherapy.
● Speaker 2: You are really scared?
Silence. Silence is an absence of verbal communication. This can be one of the most effective, yet most challenging techniques. Eye contact is maintained and body language indicates active listening.
● Silence allows the other people involved time to think and organize their thoughts. It can be hard to sit still and say nothing, but it allows for people to become more aware of what they are saying and how they are saying it.
Summarizing. Summarizing involves organizing and summing up the communication. It should highlight important points and ideas and allow for consensus of opinions and plans.
● In summary, we have agreed to make the following changes to the procedure.
● In conclusion, here are the highlights of our conversation.
Verbalizing what is implied.
This technique is verbally stating what the other speaker or speakers are implying. Putting into words what someone is suggesting helps to clarify and focus communication.
● Speaker 1: I cannot talk about my problems at work. It is just useless to talk about it.
● Speaker 2: You feel like no one understands you?
● Speaker 1: This is such a waste of time. They are making me take this class and it is stuff I have been doing on the unit for years. I wanted to apply for the advanced practice modules.
● Speaker 2: You feel as though you are not being given recognition for your experience?

ANCC.EliteCME.com Page 9
Offering constructive criticism Constructive criticism, also referred to as feedback, is a challenge. It means that someone is going to be told about areas for improvement. Here are some suggestions for making constructive criticism as effective as possible [11].
● Use constructive criticism for important issues. ● Offer positive feedback as well as identifying areas for
improvement. Start by saying something positive whenever possible.
● Explain the purpose of the constructive criticism. The nurse might say, “I would like to give you some feedback about the way you performed that sterile dressing change.”
● Give constructive criticism immediately. The more quickly it is given, the more relevant the information provided. Waiting too long makes the issues surrounding the need for improvement vague and unclear.
● Be direct. Be honest. Do not drag the situation on and on. This can lead to feelings of anxiety and resentment.
For example, suppose a nurse who is on orientation is being observed as she presents bedside change of shift report. Her preceptor might say to her, “You gave an accurate report and relayed the most pertinent information. But your voice was very quiet and you spoke very, very quickly. It was hard to understand what you were saying, and people had to ask you to repeat yourself several times. Slow down when you are speaking and speak in a tone of voice that can be easily heard and understood.”
Nursing consideration: Constructive feedback should be given in a private setting. It should never be done in front of patients or colleagues.
Examples of non-therapeutic communicationSome of the following examples seem to be obviously wrong. However, in the midst of a busy day or during an intense conversation, it can be easy to make a comment that is highly non-therapeutic. Here are some examples of communication that will inhibit good communication and probably escalate argumentative situations [11,12]:
● Advising: Telling someone what to do. ● Belittling someone: Minimizing someone’s concerns or fears.
● Challenging: Demanding proof. ● Denial: Refusing to admit that problems or concerns exist. ● Disagreeing: Opposing someone’s ideas or beliefs. ● Disapproving: Denouncing someone’s behavior or ideas. ● Making stereotyped comments: Offering meaningless platitudes
such as, “Everything will be OK.”
DEFUSING ANGER AND AGITATIONWarning signs that someone may becoming violent:During an RN’s annual performance review, the nurse manager is concerned that the RN is becoming increasingly angry and the nurse manager fears that the RN may be losing control.
A family member becomes angry over what he perceives as inadequate nursing care being provided to his wife. A nursing assistant attempts to calm him down, but with little success.
An RN is relaying information about a patient with a C-5 spinal cord injury to members of the rehabilitation team. She notices that the physical therapist seems uncomfortable with what she is saying. Is the therapist becoming angry?Nurses often face situations that have the potential to escalate to verbal and/or physical violence. It is important that nurses be able to recognize potential violence in patients, visitors, and colleagues. Some physical signs that someone may become violent include:
● Avoiding eye contact or frowning or glaring. ● Clenched fists. ● Clenched jaws. ● Pale or flushed face. ● Rapid, shallow breathing. ● Restless, repetitive movements such as pacing. ● Signs of extreme fatigue such as dark circles under the eyes. ● Shaking. ● Sweating. ● Tone of voice becomes loud. ● Language becomes abusive. ● Trembling. ● Violations of personal space. ● Violent gestures.
The preceding signs are warnings of the potential for imminent verbal or physical violence. But are there sings that can be recognized before the problem is about to occur?
In the workplace, violence can begin as small incidents that may progress to physical or emotional violence. It is hoped that by recognizing behaviors that suggest the potential for violence, such violence can be prevented.
The following warning signs do not mean that violence is inevitable. It does mean, however, that the person exhibiting such signs is under high levels of stress. Nurses must be prepared to recognize the behaviors that indicate the potential for serious trouble such as [14]:
● Blaming others for their mistakes. ● Changes in normal behavior patterns that are disruptive to the
workplace. ● Complaining of being treated unfairly. ● Crying, sulking, and/or temper tantrums. ● Disregarding the safety and health of others. ● Disrespecting authority. ● Forgetfulness. ● Insisting that s/he is always right. ● Making inappropriate statements. ● Making mistakes or errors at work. ● Poor decision making. ● Problems focusing and concentrating. ● Pushing the limits of acceptable behavior. ● Quality of work deteriorates. ● Refusal to acknowledge mistakes and job performance problems. ● Swearing or emotional language. ● Talking repeatedly about the same problems without taking steps
to resolve them. ● Unable to take criticism.
Behaviors may progress to verbal threats, intimidation, and marked suspicion of others [11]. What can nurses do if they notice these behaviors in their colleagues?
First, recognize when someone is going through tough times such as loss of a loved one, financial stress, a divorce, or other traumatic events. Nurses should be supportive and help these people to seek help from available resources. In the workplace, nurses who are concerned about a colleague should report their concerns to their supervisors, human resources department, or employee assistance program, as well as the violence prevention program in the workplace if one exists. If the organization does not have a violence prevention program, nurses should promote the development of one [11].

Page 10 ANCC.EliteCME.com
Nursing consideration: Nurses may be reluctant to seek help regarding a colleague’s behavior for many reasons, such as fear of retaliation, the belief that nothing will be done, concern that they will be labeled as troublemakers, or from a desire not to get involved. However, failure to report may end up in tragedy. It is essential to report any suspicions that violence may be imminent.
Defusing anger and agitation: De-escalation techniquesAndrea is a professional development specialist who is responsible for the continuing education of the critical care areas in her hospital. She is in the process of overseeing the Advanced Cardiovascular Life Support (ACLS) certification/recertification program. All nurses who work in designated critical care areas must be ACLS certified as a condition of their employment. Jason, a critical care nurse who works in the emergency department, has failed the written component of the test associated with recertification. He knocks on Andrea’s office door and bursts into the room. Jason is obviously angry and wants to know what Andrea is going to do to “keep me from losing my job.”
Rob is on his way to the cardiac care unit where he is an assistant nurse manager. As he passes the main entrance to the hospital, he sees an irate visitor shouting at the information desk’s receptionist, “What do you mean you cannot tell me what room my girlfriend is in? Did she say she does not want to see me? Is she spreading lies that I have been hitting her? You better tell me where she is or you will be sorry!”
Stephanie is a member of the Nursing Clinical Care Excellence Committee. During one of the meetings, the group is working on new requirements for the clinical advancement program. The majority of the committee members agree that to progress to the highest level of clinical practitioner, a master’s degree should be required. One of the nurses becomes angry and complains that, “We do not need some stupid degree to be promoted. Just because some of you have nothing better to do than go to school does not mean the rest of us do not have better things to do with our time!” The angry nurse throws her pen across the room and glares at her colleagues.
The preceding scenarios are just a few examples of situations that have the potential to become violent. What should be done when facing these kinds of situations? Here are some initial actions to take [12,15,16]:
● Trust instinct. If something does not seem “right” about an interaction, the nurse should be prepared and take steps to protect themselves and others.
● Know the organization’s policy and procedures for dealing with verbal and/or physical violence. Know how to call for help and do not hesitate to do so. Know how to implement organizational procedures for dealing with violence and help colleagues to acquire such knowledge as well.
● Participate in practice drills for dealing with violence. If your organization does not conduct such drills, encourage that they begin to do so.
● Avoid being alone with a potentially violent person. If interactions must be conducted in private, such as performance evaluations or providing constructive criticism, make sure that the environment offers ways to call for help if needed. Do not allow office doors to be locked so that you are in a locked space with a potentially violent person. Never allow the potentially violent person to be seated or remaining standing between you and an exit. Position yourself so that you have easy access to an exit.
Joseph Shrand, MD, an instructor at Harvard Medical School, has identified three major reasons why people become angry. Adapted for nurses, these are [15]:
● Resources: Resources include items such as money, or in the work setting, promotions and job availability.
● Residence: This does not refer just to a person’s home, but the workplace and the setting in which nurses practice.
● Relationships: Relations are not just members of a family. Relationships include co-workers, supervisors, and patients/families.
Anger occurs when someone believes that something (e.g. resources, residence, and/or relationships) is about to be taken away from her/him. Envy is also a trigger for anger. Envy occurs when somebody has something someone else wants (e.g. a promotion) [15].
EBP alert! Shrand developed a ten level anger scale, which ranges from irritation to rage [15]:
○ Irritation. ○ Aggravation. ○ Annoyance. ○ Frustration. ○ Impatience. ○ Displeasure. ○ Anger. ○ Wrath. ○ Fury. ○ Rage.
Shrand suggests that in addition to paying attention to the anger of others, people (in this case nurses) should be aware of their own levels of anger and what triggers each level.
How can anger be defused before it escalates to dangerous levels? First, it is important to implement the appropriate non-verbal and verbal communication techniques. In addition to doing this, there are additional techniques that may help to defuse anger.
Scott Taylor, in an article for Security Solutions Magazine, noted that processing the factors contributing to conflict may need to be accomplished in a very short period of time [16]. He describes an overview of the “OODA” Loop, developed during the Korean War by United States (U.S.) Colonel John Boyd [16]:
● Observe: Observe all factors contributing to the conflict situation. Look at the situation in its entirety. This is also referred to as situational awareness.
● Orientation: Orientation involves gathering information by observation and comparing it to the training, experience, and knowledge possessed by the person attempting to defuse the conflict.
● Decide: Decide on the best course of action. Determine what communication techniques are best used in the given situation.
● Action: Take appropriate steps to resolve the conflict.
Dealing with conflictWhen dealing with conflict, nurses should remember that they are in charge of how they react in any given situation. Keeping this in mind, experts suggest the following steps (adapted for this program for nurses) when dealing with conflict [16]:
Call the person by name. People usually respond positively to hearing their own name. This makes conversation more personal and indicates interest in what they are concerned about. If someone’s name is unknown, as in the case of an angry visitor, ask for their

ANCC.EliteCME.com Page 11
name as soon as possible. Use people’s names often throughout the conversation. For example, “Jason I know you are concerned about passing the ACLS exam and keeping your job in the ED. I want you to know, Jason, that I will work with you to help you prepare for and retake the exam.”
Use active listening. Clarifying, reflecting, and using open-ended questions helps people to know that the nurse is trying to understand their questions and concerns, as well as their frustrations. This helps the angry person to feel they are being given opportunity to vent their irritations. On a subconscious level, hearing their words reflected back to them can help angry people to know that nurses are showing understanding and empathy of the situation that is causing anger. For example, “Stephanie, you are saying that taking the time to return to school is not something you have time to do currently?”
Suspend judgment; slow down. Avoid being judgmental in either words or body language. Time should be taken to show that the angry person’s concerns are being taken seriously. Do not rush. Show respect for the other person’s feelings and beliefs. For instance, “I understand
that you are concerned about your mother’s care, Mr. Foster. I want to hear what you think and work with you to resolve your concerns.”
Get the other person to say “yes.” It is difficult for someone to stay angry if the nurse is agreeing with them. Use clarifying statements and questions to show that the angry person’s point of view has been understood. For example, “So you are saying that you are frustrated because other nurses have been promoted and you have not?”
Avoid clichés. Clichés such as “calm down,” or “everything is going to work out” will most likely exacerbate, not defuse, the situation.
Show empathy. Demonstrating empathy goes a long way towards defusing anger. Showing objective compassion is helpful. For instance, “I know it is very difficult seeing your mother suffer. I am truly sorry you and your family are going through this.”
Be consistently courteous. The person who is upset at the end of a nurse’s shift or in the midst of a busy evening deserves the same level of concern, compassion, and time spent as the person who needs defusing during a “not so busy” time period.
APPROPRIATE COMMUNICATION ON THE TELEPHONE, IN WRITING, AND ON SOCIAL MEDIA
Telephone etiquetteDespite the prevalence of texting, emailing, and other technological written communication, the telephone is still in use. Nurses on many nursing units carry telephones provided by the organization so that they are easily reached no matter where they are on the unit. Here are some basic tips for communicating on the telephone [17,18].
Always identify yourself. When answering the telephone, start by saying “good morning” or “good afternoon,” etc. followed by the name of the department or unit, and the name and title of the person speaking, e.g., “Good morning, 4 West, Ellen Burns, RN speaking.” If answering with a cell phone, “Ellen Burns, RN speaking” is appropriate.
When placing a call, the nurse should always identify her/himself, e.g., “Good morning. This is Ellen Burns, RN calling from 4 West. May I speak with Dr. Wells?”
Nursing consideration: Never answer a phone by saying “yeah” or “yes.” The principles of good verbal communication must be followed on the telephone as well as in person.
Be mindful of the tone of voice being used. Speak slowly, clearly, and distinctly. Do not speak in high-pitched tones that can be difficult to hear. Avoid slang and profanity. The tone of voice should be confident and respectful.
Nursing consideration: Avoid sitting slumped in a chair or slouching if standing. Sit or stand up straight. If the call is becoming tense, take a deep breath and smile. This will make the tone of voice calmer and more positive. Practice by listening to personal recordings. There will be a surprising difference when speaking in an upright position and smiling versus slumping and frowning!
Listen attentively. Do not interrupt or finish someone’s sentences. Convey interest in what the other person has to say.
Avoid drinking or eating during telephone conversations. Eating or drinking can garble speech and is simply rude. Do not chew gum during telephone conversations.
Explain interruptions or needing to end the conversation unexpectedly. Emergencies occur at any time on nursing units. If the conversation needs to be quickly terminated, apologize briefly, explain that there is an emergency to be attended to, and that someone will call back as soon as possible.
Prepare prior to making the call. It helps to think through what needs to be said and what information needs to be obtained prior to making a call. Jot down what is to be said and what information must be acquired.
End the call on a positive note. Summarize what has been said as appropriate. Ask the other person if s/he has anything else that needs to be said and if there are any remaining questions.
Email etiquetteUsing proper, professional email etiquette is absolutely essential in the healthcare setting. These guidelines will help nurses and other healthcare professionals to compose professional emails that are also the Health Insurance Portability and Accountability Act (HIPAA) compliant [19,20,21].
Be aware of limiting professional email addresses for business only. Do not use a professional email address for personal emails or to send jokes, chain letters, invitations to personal events, etc. In other words, use the professional email address for issues relating to business only.
Use exclamation points sparingly. Too many exclamation points can indicate that the writer is overly emotional or immature. Avoid
caricatures such as smiley faces or pictures of flowers, etc. These are business communications, not chats on social media.
Use the subject line to clearly explain the purpose of the email. The way the subject line is completed can determine if the email will even be opened. Avoid typographical errors and/or using all small case or all upper case letters. For example, when sharing information about a committee or council meeting the subject might be: “Decision regarding preceptor requirements.”
Nursing consideration: Avoid using all caps in the body of the email. This gives the impression of shouting.
Page 12 ANCC.EliteCME.com
Treat emails as formal business correspondence. Only time and contact should determine the tone of email. If writing to someone for the first time without prior contact, address him/her as Ms., Dr., Mr., etc. Never assume that email allows for informality. Most people will say “call me Susan” after establishing a professional relationship, but some will not.
Avoid acronyms. Use complete sentences and type full words. For example, “Did u get the minutes from the meeting? Some of it just made me LOL.” This is completely inappropriate.
Never address emails as though they are listings on social media. For example, a group email that begins “Yo’ dudes” will more than likely be deleted without being read.
Proofread before sending. Check spelling and grammar. Make sure all information is correct.
Be careful trying to be funny. Humor is a tricky thing in emails. Something that seems funny to the writer may come across very differently or even offensively in writing. When in doubt, leave it out!
Be very careful about hitting “reply all.” Reply only to those who absolutely need a response. There may be someone on the list that should not read what is going to be sent.
Sending to “all” results in very full mail boxes, and many people do not necessarily need to read all of this “stuff.” Avoid sending emails that are not necessary. Business emails are sent to relay critical information or inquire about critical information that is needed.
Never send an email when angry. It is tempting to immediately respond to an email that is upsetting. Such quick responses usually exacerbate a tense situation. If an email is written in this kind of situation, do not send it. Wait a few hours or even overnight. Read it again. Then respond using appropriate communication strategies.
Respond in a timely manner. Even if the email asks for information that may not be available for hours or even days, it is courteous to reply by explaining when the information will be available and when the writer may expect to receive it. This avoids frustration and, incidentally, receiving numerous follow-up emails asking for the same information over and over.
Keep it brief. Emails should be brief. Content should relate to information identified in the subject heading.
Emails are never private. Never assume that emails are confidential. Despite all available technological safeguards, emails are never private. People often leave computers unattended, or someone may hit “reply all” by mistake, etc. Assume that emails can (and will) be read by others in addition to the designated recipients.
Health Insurance Portability and Accountability Act (HIPAA) and emailsNurses and other healthcare professionals must be concerned with adhering to HIPAA guidelines when communicating via email. Email communication is allowed, but with precautions. Most HIPAA regulations call for reasonable safeguards, and reasonable approaches. But determining what is reasonable requires thought and caution. Here are some guidelines that should help with email HIPAA adherence [22]:
● Healthcare providers may communicate electronically (e.g. email), but must incorporate reasonable safeguards when doing so. Precautions should be taken to avoid unintentional disclosures. For example, email addresses should be confirmed prior to sending patients emails.
● Healthcare providers must take precautions to protect the integrity of information and protect information shared over open networks.
● Patients should be warned about the risks of using email that includes patient health information.
● “Patients may initiate communications with a provider using email. If this situation occurs, the healthcare provider can assume (unless the patient has explicitly stated otherwise) that email communications are acceptable to the individual.”
● Patients have the right to ask healthcare providers to communicate with them by alternative means or at alternative locations, if reasonable. For example, if email communication is unacceptable to a patient, other means of communicating must be used.
● Healthcare providers must implement policies and procedures to restrict access as well as protect the integrity of and guard against unauthorized access to email communication.
● Healthcare providers may communicate electronically (e.g. email), but must incorporate reasonable safeguards when doing so. Precautions should be taken to avoid unintentional disclosures. For example, email addresses should be confirmed prior to sending patients emails.
● Healthcare providers must take precautions to protect the integrity of information and protect information shared over open networks.
● Patients should be warned about the risks of using email that includes patient health information.
● “Patients may initiate communications with a provider using email. If this situation occurs, the healthcare provider can assume (unless the patient has explicitly stated otherwise) that email communications are acceptable to the individual.”
● Patients have the right to ask healthcare providers to communicate with them by alternative means or at alternative locations, if reasonable. For example, if email communication is unacceptable to a patient, other means of communicating must be used.
● Healthcare providers must implement policies and procedures to restrict access as well as protect the integrity of and guard against unauthorized access to email communication.
Appropriate communication on social and professional mediaMaxine is a home health nurse in a small town. She is having an especially challenging time taking care of an elderly patient with an advanced malignancy of the ovaries. Mrs. Ames, the patient, is quite wealthy and prominent in the community and quite demanding as well. The patient and her family are rather contemptuous of the nursing profession. Maxine overhears them talking about her, telling another member of the family, “After all she is just a nurse. All she really does is clean up after people.” Maxine tries to retain her professionalism and remain objective, but after one particularly hard day she vents her frustrations on her social media page and comments that, “Just because this old lady is rich and owns half the town, she thinks she can treat me like dirt.” Readers can easily guess the identity of the patient. A casual acquaintance, one of Maxine’s social media “friends”, reads the post and realizes that Maxine is complaining about Mrs. Ames. This acquaintance happens to be a close friend of
Mrs. Ames’ daughter. The daughter is informed and gains access to the post. A complaint is lodged with the State Board of Nursing and an investigation begins. Maxine is in danger of receiving a formal reprimand and possible suspension of her nursing license.
Beth is a nursing student doing a clinical rotation on a pediatric oncology unit. She loves her work and becomes especially attached to a little girl who is battling a rare form of brain cancer. Beth posts a short video on YouTube that shows Beth and the little girl laughing and playing with a large stuffed animal, a present from Beth. Beth does not name the patient in the video, which is only about 30 seconds in length. The patient’s room number is clearly visible in the background. At the conclusion of the video Beth is seen alone in her dorm room as she talks about how brave her patients are and how proud she is to be a nurse. The video was seen by one of the RNs on
ANCC.EliteCME.com Page 13
the pediatric oncology unit who reports it to the nurse manager of the unit, who in turn reports it to the Vice-President for Nursing. The student had violated the organization’s confidentiality policy and the Health Insurance Portability and Accountability Act (HIPAA) and was expelled from the nursing program. Additionally, the nursing program was not allowed to come back to that hospital for clinical experiences, and the hospital faced violations of HIPAA.
Mike is an RN who is awaiting news on whether or not he has received a much-desired promotion. He is confident that the promotion is his. In addition to being highly qualified for the position, he has made it a point to become friendly with the nurse manager, offering to work overtime as needed and being supportive in times of stress. Mike posts on his social media page, “I really have this promotion locked up! It is just a stepping stone to bigger and better things. That stupid nurse manager fell for my ‘goody-goody’ act of working overtime and listening to her whining when she had a bad day. If she only knew what I really think of her.” The next day Mike is informed that he is not getting the promotion. As time passes Mike is passed over for other promotions and requests for transfer to other units are not granted. Mike ultimately resigns, wondering what happened to all of his plans. Little did he know that his nurse manager saw his post as did several other members of the management team.
These preceding examples show how social media can jeopardize a career. Unfortunately, healthcare professionals can be very naïve when it comes to the ramifications of using social media.
What exactly is social media? The definition is broad and continually evolving. The term social media generally refers to “internet-based tools that allow individuals to gather and communicate; to share information, ideas, personal messages, images, and other content; and, in some cases, to collaborate with other users in real time”[23]. Examples of the functions and purposes of various types of social media include [23]:
● Social networking (e.g. Facebook, Twitter). ● Professional networking (e.g. LinkedIn). ● Media sharing (e.g. YouTube, Instagram, Flickr). ● Content production (e.g. blogs, podcasts, Tumblr). ● Virtual reality and fan environments (e.g. Second Life).
Use of social media by the general public has increased dramatically over the past decade. In the U.S., the number of adults using social media has increased from eight to 72% since 2005. Social media is used by people of all ages and professions around the world. In 2012, there were more than one billion Facebook users throughout the world. This number represents one-seventh of the population of the world. Every day there are 100 million active Twitter users and more than 65 million tweets and two billion videos are viewed on YouTube [23].
Nursing consideration: The use of social media has been linked to societal trends such as shortening of people’s attention spans and the decline of print news media [23].
Social media use by healthcare professionalsHow do healthcare professionals use social media as part of their professional practices? Here are some reported uses [23]:
● Participation in online communities where they can listen to experts and communicate with colleagues regarding professional issues.
● Crowdsourcing, which is used to access the knowledge and skills of a community to problem solve, gather information, and listen to opinions. For instance, surgical procedures can be streamed live via the Internet and questions can be asked via Twitter in real time.
● Participation in professional continuing education and basic nursing education in colleges and universities. It is estimated that 53% of schools of nursing use online social media platforms as part of the education process.
● Organizational promotion such as communicating with the community, increasing organizational visibility, and marketing products and services.
● Patient care and patient education. Some research suggests that eight in ten Internet users search for healthcare information online, and 74% of these individuals use social media.
Nursing consideration: There is a great deal of healthcare information online. Some of it is reliable and valid, but some is blatantly wrong. Nurses have an obligation to help patients differentiate between reliable and unreliable healthcare education sites.
Appropriate use of social media by nurses and other healthcare professionalsThe major concern regarding the use of social media by nurses and other healthcare professionals focuses on the potential for breaches of patient confidentiality. There are also potentials for legal ramifications. Users may argue that the use of social media is protected by constitutional rights such as freedom of speech, freedom from search and seizures, and the right to privacy. However, breaching governmental, organizational, and institutions of learning confidentiality, honor, and legal mandates makes healthcare professionals vulnerable to discipline for inappropriate professional use of social media. In 2009 for example, the U.S. District Court upheld the expulsion of a nursing student for violating the school’s honor code by making obscene remarks about the race, sex, and religion of patients under her care [23]. Social media is immediate, powerful, and accessible to everyone. A common misconception made by social media users is that posts are private and accessible only to designated persons. This is false. Once content is posted or sent, it can be disseminated to others. Most legal terms of using a social media site may include a very broad waiver of content use rights [24,25].
There are a number of reports of complaints that have been filed against nurses who misuse social media. Here are some common areas of concern [24]:
Breach of privacy or confidentiality against patients. Nurses must remember that any patient information obtained during the provision of patient care must be protected by the nurses. Such information may only be shared with other members of the healthcare team for healthcare delivery purposes. Confidential information must be shared only with the patient’s informed consent, when disclosure is legally required, or when failure to disclose information causes significant harm [24].
Privacy refers to the patient’s expectation and right that s/he be treated with respect and dignity. Posting pictures of patients on social media is an example of a violation of privacy [24].
Nursing consideration: HIPAA regulations are also designed to protect patient privacy by defining how patient information may be used, who may use it, and under what circumstances it can be used. Nurses and other healthcare professionals must be aware of HIPAA mandates and strictly adhere to them.
Failure to report violations of privacy or confidentiality. Nurses and other healthcare professionals who observe or become aware of violations have a moral and legal obligation to report them according to healthcare facility policy. Such failures may result in job loss,
Page 14 ANCC.EliteCME.com
disciplinary action by the State’s Board of Nursing, and, possibly, loss of license to practice nursing [24].
Violence/hostility against peers, supervisors, and employers. Inappropriate use of social media can have significant adverse impact on team-based care and patient outcomes. It may be argued that communication on social media is protected by labor laws and the U.S. Constitutional First Amendment. However, U.S. courts examine, with increasing frequency, what constitutes freedom of speech, and what constitutes violations of organizational policies pertaining to social media comments [24]. What is apparent, however, is that negative comments
adversely affect team functioning and may make it likely that career advancement becomes compromised. For example, if two candidates are equally qualified for promotion and one of them constantly berates colleagues, supervisors, and the employer on social media it is probable that s/he will not be anyone’s first choice for promotion.
It is becoming increasingly likely that employers will use social media when making hiring and career advancement decisions. Faculty members are also using social media to make decisions regarding applicants’ character, professionalism, and the potential for successfully completing a nursing program.
Guidelines for the appropriate use of social media by nurses The National Council of State Boards of Nursing has published a White Paper regarding nurses’ use of social media [25]. Here are some recommendations for avoiding problems when using social media [24,25]:
● Nurses must recognize that they have ethical and legal obligations to maintain patient privacy and confidentiality at all times. This supersedes their desire for self-expression. Their first duty is to their patients.
● Nurses are strictly forbidden from transmitting, via any electronic media, any patient-related image or information that might be reasonably anticipated to violate patient rights to confidentiality or privacy or otherwise degrade or embarrass the patient.
● Nurses must not share, post, or otherwise disseminate any information, including images, about a patient or information gained in the nurse-patient relationship with anyone unless there is a patient care related need to disclose the information or other legal obligation to do so.
● Nurses must not identify patients by name or post or publish information that may lead to identification of patients.
Nursing consideration: Nurses must realize that limiting access to social media postings through privacy settings is NOT sufficient to ensure privacy.
● Nurses must never refer to patients in a disparaging manner, even if the patient is not identified. Nurses must not post or publish information that may lead to identification of a patient.
● Nurses must not take photographs or videos of patients on personal devices, including cell phones. They must follow organizational
policies and procedures for taking photographs or videos of patients for treatment of other legitimate purposes.
● Nurses must maintain professional boundaries in using social media. Nurses should be cautious about having online social relationships with patients or former patients as this interferes with the distinction between a professional and personal relationship. It also puts the nurse in a precarious legal position. During social interaction the patient may take a nurse’s opinion as fact and alter prescribed treatment based on the nurse’s comments, even though the nurse believed that s/he was simply interacting as a friend. Thus, even if patients contact the nurse to initiate a social relationship, the nurse should not do so.
● Nurses should follow organizational policies and procedures regarding the use of social media.
● Nurses must immediately report any identified breaches of confidentiality or privacy.
● Nurses must be aware of and comply with organizational policies regarding the use of employer-owned computers, cameras, and other electronic devices and use of personal devices in the workplace.
● Nurses must not make disparaging remarks about employers or co-workers. They must not make threatening, harassing, profane, obscene, sexually explicit, racially derogatory, homophobic, or other offensive comments.
● Nurses must not post content or otherwise speak on behalf of the employer unless authorized to do so. They must follow all applicable policies of the employer.
COMMUNICATION AND MEDICAL ERROR OCCURRENCEResearch indicates that there are strong positive relationships between a healthcare professional’s communication skills, and a patient’s ability to follow through with medical recommendations, self-manage a chronic medical condition, and implement preventive health behaviors. Research conducted over 30 years shows that the healthcare provider’s ability to explain, listen, and empathize can have a significant impact on biological and functional health outcomes, patient satisfaction, and experience of care [26].
Research also shows that poor communication has a significant negative impact on patient care and teamwork. Medical errors are the third leading cause of death in the U.S. It is estimated that 80% of serious medical errors involve some type of miscommunication, especially during the transfer of care from one provider to the next [27].
EBP alert! A study followed 1,255 patient admissions to two separate inpatient units at Boston Children’s Hospital, half of which took place before a new verbal and written handoff program was introduced. After implementation of this program, providers spent more time communicating face-to-face in quiet areas that facilitated conversation, resulting in fewer omissions or miscommunications regarding patient information during handoffs. Medical errors decreased by 45.8%. Investigators recommended that other healthcare facilities adopt similar protocols to decrease errors and enhance patient safety. The protocol included use of the acronym PASS, which was the foundation of relaying information during handoffs. P represents patient summary. A represents action list for the next team. S represents situation awareness/contingency plans. And S represents synthesis or “read-back” of the information by the person being briefed [27].
The PASS acronym is being adopted by other healthcare organizations in attempts to improve communication at handoffs and improve patient outcomes. Some healthcare providers may believe that using this acronym and identifying quiet places for communication may take “too much time.” However, research shows that these types of protocol did not add time to patient handoffs or decrease time spent at patient bedsides or on other tasks [28].

ANCC.EliteCME.com Page 15
Nursing consideration: Nurses must remember that even as the PASS or similar protocols are implemented, such protocols are only effective if good communication skills (such as communicating confidently and using both verbal and non-verbal appropriate techniques) are part of the process.
BULLyING IN HEALTHCARESandy is being oriented to her new job as an adult oncology nurse. Her preceptor, Margaret, continually makes degrading comments about Sandy and other orientees, complaining that, “These new nurses are so slow. I cannot stand working with them.” She tells Sandy in front of a patient, “You will never be able to give chemo drugs if you do not learn more about them in a hurry.” Sandy has had enough. After they leave the patient’s room, Sandy tells Margaret that she needs to speak to her immediately in the break room. Her tone of voice is polite but firm and she stands tall and maintains eye contact with Margaret. Margaret reluctantly enters the break room muttering, “Now she thinks she needs a break!” Sandy faces Margaret and says firmly, “I realize that I need to learn new skills in order to give good patient care. But it is inappropriate to criticize me in front of patients. If you have something constructive to tell me that will help me to learn, I will appreciate it. I do not appreciate being embarrassed in front of patients.” Margaret is stunned into silence. Just then the nurse manager enters the break room. Margaret tells him, “This new nurse just told me that I embarrass her!” Sandy faces both the nurse manager and Margaret and briefly states what happened in the patient’s room and reiterates that she is eager to learn but will not allow anyone to embarrass her in front of patients. The nurse manager is also surprised and says with a laugh, “Well I guess that is the first time anyone had the guts to stand up to Margaret!” Margaret does stop criticizing Sandy in front of others and Sandy’s orientation is successfully completed. However, she and Margaret always have a rather tense professional relationship.
Dr. Morris is a neurosurgeon known for his abusive treatment of nurses. He has been known to shout at them in front of patients and colleagues and even throw pagers at persons who trigger his anger. If he is telephoned regarding changes in patients’ conditions, he usually shouts at whomever calls, telling them not to bother him, and hangs up. At 7PM one evening Janice, the RN taking care of one of Dr. Morris’s patients, telephones Dr. Morris. She is calling to double check on a medication order that is unclear. She begins to provide information about the medication order, but he interrupts her by saying, “Do not question what I order. Just do as I say.” He then hangs up. Janice informs her nurse manager who tells her not to worry, “The medication is not critical and it can wait until after Dr. Morris makes rounds tomorrow to be clarified.” Janice knows that it is important to clarify the order and begin medication administration. Janice pages the administrative nursing supervisor who calls Dr. Morris. Unfortunately, he also hangs up on the supervisor. Janice tells the supervisor that they need to call the facility’s medical director and administrator on call because the patient needs the medication and waiting until morning is not a good option. The supervisor does so and, ultimately, thanks to the medical director’s intervention, Dr. Morris calls the nursing supervisor and clarifies the order. The next day Janice is summoned to the Vice-President for Nursing’s office and is informed that Dr. Morris has filed a complaint against her and that the nurse manger is also filing a complaint citing insubordination. Janice, in turn, files a grievance against the physician and the nurse manager. The situation takes weeks to resolve, and Janice is ultimately cleared of any wrongdoing. However, Dr. Morris’ abusive behavior continues and the nurse manager is simply transferred to another unit. Janice decides to resign. She believes that since the problem of abusive behavior is not being addressed, patients will eventually suffer serious consequences.
Bullying is a serious form of abuse. Bullying can be committed by: persons of authority who bully those over whom they have power; by peers against peers; and even by subordinates against those to whom they report. These two scenarios describe nurses who took appropriate action in the face of serious bullying. Unfortunately, the actual problem of bullying was not addressed and patient care may continue to be in jeopardy. Why is bullying so prevalent in healthcare? What can nurses do to stop it?
Workplace bullying is a serious and escalating problem that affects a significant number of healthcare professionals. Bullying adversely impacts the mental health and well-being of its victims, and, consequently, organizational performance and patient outcomes [29]. The prevalence and negative consequences of bullying have led the American Nurses Association (ANA) to publish a position statement on “Incivility, Bullying, and Workplace Violence.” The statement says, in part [30]: “ANA’s Code of Ethics for Nurses with Interpretive Statements states that nurses are required to create an ethical environment and culture of civility and kindness; treating colleagues, co-workers, employees, students, and others with dignity and respect. Similarly, nurses must be afforded the same level of respect and dignity as others. Thus, the nursing profession will no longer tolerate violence of any kind from any source.”
It is important that the ANA has taken a stand against bullying. However, bullying continues to be tolerated at all levels in many organizations. Excuses for tolerating bullying include:
● “S/he is a really good doctor and we cannot afford to have him/her admit his/her patients elsewhere.”
● “S/he is one of the best nurses on the unit. You just need to figure out how to deal with him/her or just stay out of her way.”
● “I know that this nursing assistant can be really nasty, but s/he has worked here forever and is really good with patients.”
● “This is a high-pressure unit. If you cannot take it, you had better transfer.”
These excuses are unacceptable, but all too prevalent. Nurses must use their communication skills in order to deal effectively (and reduce) the bullying behavior of others. Some experts on nurse-physician communication recommend the following interventions when dealing with bullying behavior committed by physicians [31]:
● Use proven verbal and non-verbal communication skills. As discussed earlier in this program, these skills can have a significant impact on improving communication.
● Think before speaking. Determine the goals of the communication (e.g. to relieve the patient’s pain when previously ordered pain management strategies are failing to work) and determine how to relay information that will help to achieve those goals.
● Provide evidence-based practice (EBP) information whenever possible. When suggesting or discussing patient care options, use evidence to support concerns and ideas.
● Use scripting, which involves using key words to alert healthcare providers to potential patient risks. For example, “I am concerned about…” or “I am not sure that you are aware…” or “I am uncomfortable with...”
● Be aware of body language. Have a confident, but non-threatening posture. Stay at the same level as the person involved in the communication (e.g. if that person is standing, stand. If that person is sitting, sit). Maintain eye contact.
Page 16 ANCC.EliteCME.com
Nursing consideration: The preceding interventions can be used with any person of authority, not just with physicians. The ultimate goal is to communicate with colleagues in an honest, confident manner to facilitate the achievement of desired patient outcomes.
Horizontal violence/bullying: A growing phenomenon Bullying has been defined as a persistent, demeaning, and downgrading of people via vicious words and cruel acts that gradually undermine confidence and self-esteem.
Horizontal violence/bullying has been defined as a consistent pattern of behavior designed to control, diminish, or devalue someone who is on the same level within an organization’s hierarchy [32]. This type of bullying is quite prevalent among nurses. In fact, research shows that the most distressing type of aggression to deal with is nurse-to-nurse aggression [32]. Horizontal bullying has devastating impact on its victims, patients, and the organization as a whole. A 2012 series of surveys conducted by the
Society for Human Resource Management and the Workplace Bullying Institute showed that [32]:
● 80% of harassment cases were legal and were considered to be cruelty.
● 72% of cases involved verbal abuse. ● 62% of cases reported malicious gossiping or spreading rumors or
lies about colleagues. ● 51% of organizations surveyed occurrences of bullying in the
workplace. ● 15% of those surveyed witnessed the emotional or psychological
abuse of coworkers.
Impact of horizontal bullyingImpact on the victim. Research shows that bullying can cause [32]:
● Emotional and physical ill effects that can last a lifetime. ● Hostility and job dissatisfaction. ● Low self-esteem. ● Physical symptoms including: migraines; decreased immune
response; cardiac arrhythmias; hypertension; irritable bowel syndrome; asthma; and nausea, weight gain, and other gastrointestinal problems.
● An increase in sick time. ● Irritability, depression, anxiety, and post-traumatic stress disorder
(PTSD).Impact on the organization. Bullying impacts the organization by leading to [32]:
● A hostile work environment. ● An increase in turnover. ● An increase in medical error occurrence. ● A decrease in the quality and safety of patient care.
Impact on finances. Bullying has an impact on finances as evidenced by [32]:
● An increase in orientation costs because of high turnover. ● An increase in paying sick time for victims as well as the cost of
overtime or agency staffing to cover for the nurses who were sick. ● A potential increase in legal fees and payment for damages as
the result of patient injury (due to medical errors) and legal fees
for nurses filing charges against the organization for allowing bullying/harassment.
Considering the devastating costs related to bullying, why does it continue? Why does bullying occur? According to the literature, some reasons for bullying include [32,33]:
● Misplaced aggression: Persons who are bullied in other areas of their lives (e.g. domestic violence) take out their aggressions at work.
● Desire to feel superior: Some persons who bully do so because it makes them feel superior to others.
● Desire to control: Bullies may be looking for a way to control others or to feel powerful.
● Fear: Wanting to be part of the powerful group. This also includes fear of retaliation. Some people bully, or fail to report bullying or help its victims for fear that they, too, will become victims.
● Denial: People do not like to admit bullying exists, so they call it something else, e.g., “You need to be tough to work on this unit” or “S/he just is not cut out to be a critical care nurse.” These sentences show that bullies tend to blame the victim.
● Management denial: Managers may be bullies. But they may also be willing to ignore bulling by giving excuses, e.g. “S/he is one of the best nurses I have” or “I cannot afford to offend anybody since it is too hard to recruit nurses.”
Reducing bullying in the workplaceEstablish policies that address bullying. Policy development must include [32,33]:
● A clear statement that defines bullying. The policy must define bullying so that all employees can recognize bullying when they observe or commit it.
● A statement stating that the organization has zero tolerance for bullying in any and all forms including verbal, physical, psychological, and social media forms of bullying.
● A statement that says bullying is not tolerated by non-employees who practice within the organization (e.g. physicians, agency nurses).
● Statements that provide examples of bullying behaviors. ● An outline of manager and staff responsibilities as they relate to
bullying. ● Provision of response strategies aimed at early intervention and
informal resolution. ● Provision of clear and confidential grievance, investigation, and
disciplinary procedures.
● Provision of steps that are to be taken in relation to complaints of bullying and how they are to be documented.
● Provision of statements that explain people who report bullying or cooperate in the investigatory processes are protected from retaliation.
● Provision of statements detailing the consequences of failing to report and/or to deal with the phenomenon of bullying.
Nursing consideration: These policies must be adhered to by all employees, including administrative and managerial staff. If organizational leaders and people in positions of authority fail to implement such policies and procedures, they are doomed to be ineffective.
Provide continuing education regarding bullying. All employees (including administrative and management staff and non-clinical personnel) must participate in continuing education that addresses bullying. Information presented should include [32,33]:

ANCC.EliteCME.com Page 17
● Blunt definition and examples of bullying: Bullies and victims must recognize bullying behavior.
● Consequences of bullying including: Impact on victim, patients, the organization, and finances; disciplinary action and reprimands for those who bully; and potential legal ramifications.
● Reasons for bullying: A helpful acronym to help identify reasons for bullying as well as how to differentiate motives for bullying versus helpful behaviors, is MOTIVE:
○ M: Mentor or malice. ○ O: Orient or oppress. ○ T: Team build or torment. ○ I: Inform or intimidate. ○ V: Vindicate or vindictive. ○ E: Empower or embarrass.
● How to respond to bullying: Include appropriate verbal and non-verbal communication techniques, and how to follow policies and procedures to report bullying that cannot or will not be resolved.
● Managers should receive additional training as to how to incorporate behavior (including both positive and negative behaviors) in performance evaluations.
Data regarding patient satisfaction, medical errors, turnover, and sick time, should be compared before and after education regarding bullying was implemented [7,32,33].
TEAM BUILDING STRATEGIESTEAMS cannot function effectively without good communication. No team can be effective or productive unless all members consistently implement the principles of good communication.
Good communication does not mean that everyone agrees with everyone else at all times. Differences of opinions will occur. These differences can strengthen a team, rather than impair it, if communication is open, honest, and therapeutic.Effective team building starts with an administrative team that does the following [34]:
● Develops a clearly communicated overall purpose for the organization and a system for relaying such communication on an
ongoing basis. All employees need to know and understand the organization’s vision, mission, and purpose.
● Recognizes employees who support and advance the organization’s values, vision, and mission.
● Facilitates the integration of new employees into the system. A solid orientation with well-trained preceptors is critical to achieving this goal.
● Leads by example. Administrators need to be seen to be a hands-on part of the team. They need to be visible and model the behaviors they expect to see in their employees.
● Solicits feedback on prospective decisions from those who are affected by them.
Nursing teamsNurses are members of both nursing department teams and interdisciplinary teams. It is important to remember that all team members, regardless of the position in the organizational hierarchy, must have input into how the team functions. Nursing team leaders must have three goals for their teams [35]:
● Provide safe and appropriate clinical care. ● Provide high quality services to both patients and families. ● Use resources (both financial and human resources) wisely.
EBP alert! Research shows that leaders who find ways to use people’s strengths spend less time trying to deal with their weaknesses. All adults have life experiences that can contribute to effective team functioning regardless of position or level of education. Effective leaders find ways to incorporate their team’s strengths into decision making processes and work distribution [7,35].
Research also shows that taking the time to incorporate team building exercises can help to improve team functioning. For examples, leaders should [7,35,36]:
● Encourage team members to share personal histories and experiences. They should ask team members, “What has worked well for you in the past?”
● Clearly state the vision, mission, and purpose of the team and how these issues correlate with organizational goals.
● Clearly explain the responsibilities of each person on the team. ● Determine assignments based on the strengths of each individual
team member. ● Establish norms for decision making. Let team members know
what decisions will be made by the individual, by the team, and by the team leader.
● Establish a process for giving and receiving feedback. Emphasize that feedback should be constructive, not a mechanism for arguing or complaining. This process should encourage feedback swiftly and easily in all directions, from peer to peer, from supervisor to staff member, and from subordinate to supervisor.
● Provide opportunities for team members to share positive experiences. Encourage team members to acknowledge colleagues who have made particularly useful contributions to team functioning and patient care.
EBP alert! esearch confirms that the utilization of active leadership skills designed to inspire and intellectually stimulate are important to establishing programs that lead to patient and staff satisfaction [34,35].
There are many teams in healthcare, not just the team that works on a particular unit or in a specific department. Teams are also formed for the purpose of establishing committees, councils, and task forces. Some of these teams will work together for an indefinite period of time. Some teams will work together for a limited period of time in order to accomplish a specific purpose (e.g. choosing a new piece of patient care equipment or selecting a new system for electronic medical records (EMRs)). Regardless of the amount of time the team members will work together, most, if not all, teams go through four stages [35,36]:
● Forming: The team members get to know one another. They are generally polite, and avoid controversy. Little progress is made at this stage. Team members that agree with everything that is said or fail to contribute, are generally trying to learn about the team’s purpose and what must be accomplished as well as learning about each other.

Page 18 ANCC.EliteCME.com
● Storming: Most teams go through some type of storming. This can be productive if team members adhere to good communication principles and genuinely want to progress to the development of an effective team that achieves its goals and objectives. There may be periods of blame and frustration, expression of negative emotions, and attempting to challenge leadership. This stage can encourage open expression, but must not be allowed to continue indefinitely or to “take over” the team.
● Norming: During norming, team spirit develops and team performance improves. Ideas are exchanged, members become receptive to change, and identify ways of effective problem solving. Leadership is shared appropriately.
● Performing: Performing is the most productive and effective stage of team development. The team works as a unit and members work to their abilities and strengths. The team reaches a level of openness and trust in other team members.
Nursing consideration: Not all teams reach and maintain the level of the performing stage. Some teams, unfortunately, are ineffective. This requires that leaders and/or staff members work to regroup and assemble a team that “works” for the sake of patients and employees.
SummaryCommunication affects every aspect of healthcare delivery. Research shows that good communication enhances patient outcomes, job satisfaction, and organizational effectiveness. Poor communication leads to an increase in medical errors and compromises patient care and safety. Bullying is arguably the most toxic form of poor communication. Not only does bullying compromise patient safety and negatively impact patient outcomes, but it has a devastating impact on its victims, the organization, and the financial well-being of healthcare facilities.
Principles of good communication involve both verbal and non-verbal communication skills. Using good communication skills can enhance confidence and make healthcare workers more effective employees.
The delivery of safe and appropriate patient care depends on effective team functioning. Building teams that “work” is dependent on good communication and team members who truly want to work together to deliver the best possible patient care.
Therefore, it can safely be said that without effective communication it is not possible to deliver safe and appropriate patient care services that all consumers have a right to expect and receive. It is the obligation of all nurses to work to enhance communication and assist colleagues to do the same.
References1. Williams, D.K. (2013). First impressions count: The business value of dressing for success.
Retrieved May 1, 2016 from http://www.forbes.com/sites/davidkwilliams/2013/08/09/first-impressions-count-the-business-value-of-dressing-for-success/#424df3246a97.
2. Clavelle, J.T., Goodwin, M., and Tivis, L.J. (2013). Nursing professional attire: Probing patient preferences to inform implementation. The Journal of Nursing Administration, 43(3), 172-177.
3. Sullivan, S.E. (2012). Becoming influential: A guide for nurses (2nd ed.). Saddle River, NJ: Prentice Hall.
4. Windel, L. (2008). An evidence-based approach to creating a new nursing dress code. Retrieved May 1, 2016 from https://americannursetoday.com/an-evidence-based-approach-to-creating-a-new-nursing-dress-code/.
5. University of California, San Francisco. (2015). Frequently asked questions. Retrieved May 1, 2016 from https://infectioncontrol.ucsfmedicalcenter.org/faqs.
6. Mindtools.com. (2016). Body language: Understanding non-verbal communication. Retrieved May 2, 2016 from https://www.mindtools.com/pages/article/Body_Language.htm.
7. Avillion, A.E. (2015). Nursing professional development: a practical guide for evidence-based education. Danvers, MASS: HCPro.
8. Medical Dictionary. (2009). Personal space. Retrieved May 4, 2016 from http://medical-dictionary.thefreedictionary.com/personal+space.
9. Livescience.com. (2012). Why do we have personal space? Retrieved May 3, 2016 from http://www.livescience.com/20801-personal-space.html.
10. Garrett, D., Bormann, L., and Link, K. (2016). Therapeutic communication. Retrieved May 4, 2016 from http://nursing.advanceweb.com/Continuing-Education/CE-Articles/Therapeutic-Communication.aspx.
11. University of Kent. Communication skills: Speaking and listening. Retrieved May 3, 2016 from https://www.kent.ac.uk/careers/sk/communicating.htm.
12. Videbeck, S.L. (2011). Psychiatric-mental health nursing (5th ed). Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins.
13. National Commission on Correctional Health Care. (2011). Therapeutic communication and behavioral management. Retrieved May 5, 2016 from http://www.ncchc.org/cnp-therapeutic-communication.
14. Canadian Center for Occupational Health and Safety. (2016). Violence in the workplace: Warning signs. Retrieved May 4, 2016 from https://www.ccohs.ca/oshanswers/psychosocial/violence_warning_signs.html.
15. Tartakovsky, M. (2013). How to defuse anger in ourselves & others. Retrieved May 6, 2016 from http://psychcentral.com/blog/archives/2013/02/25/how-to-defuse-anger-in-ourselves-others/.
16. Taylor, S. (2014). Verbal de-escalation techniques that actually work. Retrieved May 6, 2016 from http://www.securitysolutionsmagazine.biz/2014/08/20/verbal-de-escalation-techniques-that-actually-work/.
17. Advancedetiquette.com. (2012). 8 telephone etiquette tips. Retrieved May 9, 2016 from http://www.advancedetiquette.com/2012/01/8-telephone-etiquette-tips/.
18. OfficeSkills.org. Telephone etiquette. Retrieved May 9, 2016 from http://officeskills.org/telephone_etiquette.html.
19. Businessemailetiquette.com. (2015). Business email etiquette basics. Retrieved May 10, 2016 from http://www.businessemailetiquette.com/business-e-mail-etiquette-basics/.
20. Smith, J., and Sugar, R. (2015). 14 email etiquette rules every professional should know. Retrieved May 9, 2016 from http://www.businessinsider.com/email-etiquette-rules-every-professional-should-know-2015-6.
21. Whitmore, J. (2013). 15 tips to refine your email etiquette. Retrieved May 9, 2016 from http://healthcarecommunication.com/Main/Articles/15_tips_to_refine_your_email_etiquette__10168.aspx.
22. Foxgfrp.com. (2012). HIPAA privacy and security rules are concerned with email, and the web in general. Retrieved May 8, 2016 from http://www.foxgrp.com/blog/hipaa-and-email-rules/.
23. Ventola, C.L. (2014). Social media and health care professionals: Benefits, risks, and best practices. Retrieved May 9, 2016 from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4103576/.
24. Spector, N., and Kappel. (2012). Guidelines for using electronic and social media: The regulatory perspective. Retrieved May 10, 2016 from http://www.nursingworld.org/MainMenuCategories/
ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/Vol-17-2012/No3-Sept-2012/Guidelines-for-Electronic-and-Social-Media.html?css=print.
25. National Council of State Boards of Nursing (NCSBN). (2011). White Paper: A nurse’s guide to the use of social media. Retrieved May 9, 2016 from https://www.ncsbn.org/Social_Media.pdf.
26. Institute of Communication in Healthcare. (2011). Impact of communication in healthcare. Retrieved May 11, 2016 from http://healthcarecomm.org/about-us/impact-of-communication-in-healthcare/.
27. Underwood, T. (2013). Improved “handoff” communication curbs medical errors. Retrieved May 11, 2016 from http://vector.childrenshospital.org/2013/12/improved-handoff-communication-curbs-medical-errors/.
28. The Source. (2014). Medical errors drop with improved communication during hospital shift changes. Retrieved May 11, 2016 from https://source.wustl.edu/2014/11/medical-errors-drop-with-improved-communication-during-hospital-shift-changes/.
29. Ariza-Montes, A., et al. (2013). Workplace bullying among healthcare workers. Retrieved May 9, 2016 from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3774428/.
30. American Nurses Association (ANA). (2015). Incivility, bullying, and workplace violence. Retrieved May 9, 2016 from http://www.nursingworld.org/Bullying-Workplace-Violence.
31. Thompson, R. (2013). Nurse-physician communication: It’s an issue of patient safety. Retrieved May 9, 2016 from http://nursing.advanceweb.com/Continuing-Education/CE-Articles/Nurse-Physician-Communication.aspx.
32. Bartholomew, K. (2014). Ending nurse-to-nurse hostility: Why nurses eat their young and each other (2nd ed.). Danvers, MA: HCPro.
33. The Quarterly. (2013). The impact of bullying in health care. Retrieved May 9, 2016 from http://racma.edu.au/index.php?option=com_content&view=article&id=634&Itemid=362.
34. Barbera, E.F. (2012). 5 team building practices that will make your staff want to stay. Retrieved May 10, 2016 from http://www.ltlmagazine.com/print/article/5-team-building-practices-will-make-your-staff-want-stay.
35. Stanton, K., and Garfield, J. (2011). Learn how to build an effective clinical team. Retrieved May 10, 2016 from http://nursing.advanceweb.com/Continuing-Education/CE-Articles/Team-Building-Essentials.aspx.
36. Craig, M., & McKeown, D. (2015). Teambuilding 1: How to build effective teams in healthcare. Retrieved , 2016 from http://www.nursingtimes.net/roles/nurse-managers/teambuilding-1-how-to-build-effective-teams-in-healthcare/508

ANCC.EliteCME.com Page 19
1. Research shows that which of the following styles of appearance can have a detrimental impact on patient care?a. Wearing uniforms of various colors.b. Wearing nail enhancements. c. Wearing wedding rings.d. Wearing scrubs.
2. All of the following non-verbal behaviors are indicative of good non-verbal communication EXCEPT:a. Stand or sit “tall.”b. Maintain eye contact.c. Hand or arm gestures that are small and close to the body.d. Take a deep breath and pause before entering into an
uncomfortable situation.
3. Which of the following is the most effective way to ask a question?a. Do you know the signs and symptoms of increased intracranial
pressure?b. Why did you give the insulin without having someone double
check it?c. You believe that you are ready to take on a more complex
patient assignment don’t you?d. How would you deal with a visitor who tells you that his
family member is not receiving good care?
4. When attempting to defuse anger and agitation the nurse should:a. Remember that the angry person is in charge of the interaction
and how the nurse reacts.b. Avoid calling the person by name.c. Get the other person to say “yes.”d. Point out why the angry person should not be angry.
5. Which of the following is the most appropriate email strategy?a. When emailing someone for the first time address the person
as Ms., Mr., Dr., etc. b. Routinely hit “reply to all” to ensure that everyone involved
receives enough information.c. Wait to respond to a request for information until all
information is obtained even if this takes several days.d. Assume that emails sent via the organization’s server are
confidential.
6. When using social media nurses should do all of the following EXCEPT:a. Remember that information obtained during provision of care
may be shared only with other members of the healthcare team for healthcare delivery purposes.
b. Realize that they may establish a social networking relationship with a patient only after he/she is discharged.
c. Know that limiting access to social media postings through privacy settings is NOT sufficient to ensure privacy.
d. Report violations of privacy or confidentiality to managers or others according to healthcare facility policy.
7. Research indicates that:a. Half of all medical errors involve some type of
miscommunication.b. Communications skills has not yet been linked to preventive
health behaviors.c. Communication during handoffs should always be conducted
at the patient’s bedside.a. The PASS acronym includes developing contingency plans.
8. Research shows that bullying:a. Is usually committed by a person of authority over a
subordinate.b. The most distressing type of aggression to deal with is nurse-
to-nurse aggression.c. The impact of bullying on the victim usually subsides within a
few weeks.d. Has limited impact on retention of staff.
9. In order to defuse bullying in the workplace:a. Nurses must realistically accept the fact that there is little they
can do to reduce most types of bullying.b. Policies must include a clear definition of bullying.c. Education regarding bullying should be primarily directed
towards clinical staff.d. Avoid using bullying as quality indicators for fear of lawsuits.
10. Building effective healthcare teams includes:a. Avoiding the Storming Stage.b. Focusing on teams that are long-term.c. Utilizing active leadership skills.d. Relying primarily on input from managers.
COMMUNICATION AND TEAM BUILDING: PRACTICAL STRATEGIES FOR CLINICAL PRACTICE
SELF ASSESSMENTSelect the best answer for each question and check your answers at the bottom of the page.
You do not need to submit this self-evaluation exercise with your participant sheet.
Answers:
1.B 2.C 3.D 4.C 5.A 6.B 7.D 8.B 9.B 10.C