common algorithm of the management of infertility
TRANSCRIPT

• The young, enthusiastic and energetic chief consultant at Rupal Hospital For Women, Surat, India (for last 15 years)
• Medical director and IVF consultant at Blossom IVF Centre, Surat, India (for last 2 years)
• Diploma in Reproductive Medicine from Kiel, Germany
• Intense training in Advanced infertility treatment at numerous workshops and conferences in USA and Europe.
• Specialized in all kind of gynec endoscopic surgeries.
• Promotes health awareness by conducting
Seminars and writing articles and specialty related books
• In addition of being techno-savvy person, she loves making friends, and keenly interested in music and Guajarati literature. She is actively associated with the leading cultural club of Surat-Tarbatar.
Dr Rupal N Shah
M.D.(OBGYN)Diploma in Reproductive Medicine(Germany)

Common algorithm of the management of Infertility
Dr Rupal N Shah M.D;D.G.O
Diploma In Reproductive Medicine (Germany)
Blossom IVF Centre
&
Rupal Hospital For Women
Surat,India

Objectives:
1. To present the practical concepts in the management of
infertility
2. To discuss the best possible clinical management options
with local perspective.

When to start investigations and treatment?
• Whenever couple feels like having to be investigated and treated..
• Minimum tests to be offered are
-Semen test
-TVS
20-30 Years 1 Year
30-35 Years 6 Months
35-40 Years Immediately
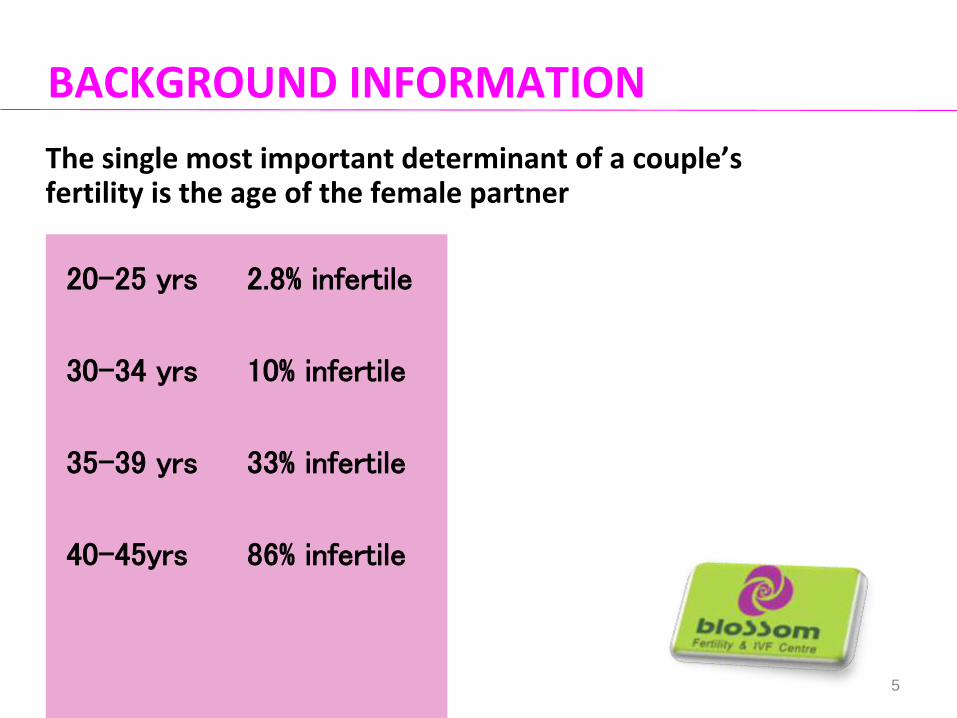
BACKGROUND INFORMATION
The single most important determinant of a couple’s fertility is the age of the female partner
20-25 yrs 2.8% infertile
30-34 yrs 10% infertile
35-39 yrs 33% infertile
40-45yrs 86% infertile
5

CURRENT GUIDELINES
The current clinical approach to the investigations and the management of infertility is backed by the evidence-based guidelines issued by:
Royal College of Obstetricians and Gynecologists (RCOG)
American Society of Reproductive Medicine (ASRM)
European Society of Human Reproduction and Embryology (ESHRE)

INVESTIGATIONS
1st Visit
Trans vaginal USG
TSH and prolactin (apart from CBC, RBS, HIV, HbsAg, Hbelectrophoresis)
Semen analysis
AMH(ML>5 years,patient’s age >35 years)

Trans vaginal USG
• D2 USG : AFC
• 1st visit:
• >10 to 12 follicles per ovary (PCOS),
• Persistent hemorrhagic cysts with low-level echoes (endometriosis)
• Anatomical conditions: fibroids, polyps, and Mülleriananomalies (uterine septum)

• Age related decline in female fertility well recognised...
– Starts at 30,
– rapid decline after 37,
– virtually zero at 43.
• Ovarian reserve tests1. Total D2 antral follicle count.(<5 ,Poor outcome)2. AMH of 2 to 6 (<2 Poor ovarian reserve,>6 PCO)3. D2 FSH > 10 IU/l poor response to ART
No evidence for ovarian volume,- ovarian blood flow- inhibin B, -estradiol (E2)
Investigations for Ovarian Reserve

Investigations to be required subsequently
Screening test for Tubal patency
• HSG
• Diagnostic laparoscopy + Hysteroscopy

Laproscopy findings
• Uterus Fibroids, Uterine Anomaly
• Tubes Patency ,Hydrosalpinx
• Ovaries PCOS ,Chocolate Cyst
• POD Endometriosis ,Adhesions

Tubal Block
Hydrosalpinx
• Clipping IVF+ICSI
Mid-tubal or fimbrial block
• IVF-ICSI
Cornual tubal block
• Hysteroscopic cornual catheterisation
• Most rewarding procedure

Endometriosis and Chocolate cyst
Medical Management-Ineffective
Surgical
Recurrence AMH IVF-ICSI
Drainage Drainage and excision of cyst wall

Management depending upon hysteroscopic procedures..P
oly
p/S
ub
mu
cou
sfi
bro
ids • polypectomy
• Hysteroscopicmyomectomy
Intr
aute
rin
e a
dh
esio
ns • Adhesiolysis
• High dose estrogen
• Trial ET
• IVF-ET
Sep
tum • Minor
septum-DO NOT CUT

Abnormal Semen??
• M
• Minimum post-process Semen parameters for successful IUI -5 mill/ml motile sperms
Count Motility(G1+G2)
Morphology Treatment
Mild 15-20 mill/ml 40-50% 30-40% IUI
Moderate 10-15mill/ml 20-40% 10-30% IUI
severe <10mill/ml <10% <10% IVF-ICSI

MALE INFERTILITY
• Medical Management Anti-oestrogens, androgens, bromocriptine and kinin-enhancing drugs , Antioxidants, mast cell blockers and alpha blockers, systemic corticosteroids for treatment of antisperm antibodies have not been shown to be effective in the treatment of Male infertility
• Surgical Management The benefits of the treatment of a varicocele in oligozoospermic men is less certain

ICSI for male infertility
• IVF and ICSI are effective treatments for men with moderate to severe semen abnormalities
• ICSI has made it possible for men with only few sperms to become fathers
• Even in very severe oligospermia and azoospermia ,Sperms for ICSI can be obtained are directly from( testicular biopsy by TESA )as well as aspiration from epididymis (PESA)

Common algorithms…
Based on
• Patient’s age
• Duration of INFERTILITY
• AMH

Age 20-30 years,ML 1-2 years, Semen and TVS NORMAL
1-2 cycles fertile period
2-3 cycles OI+Follicular study
Diagnostic laparoscopy+Hysteroscopy
4 cycles IUI(Tab CC-/+ HMG)
IVF-ICSI

Age 20-30 years,ML 3-5 years, Semen and TVS NORMAL
2-3 cycles OI+Follicular study
Diagnostic laparoscopy+Hysteroscopy
4 cycles IUI(Tab CC-/+ HMG)
IVF-ICSI

Age 20-30 years,ML 5-10 years, Semen and TVS normal
AMH
Normal
>2ng/ml
Diagnostic
Laproscopy+
Hysteroscopy
CC+/- HMG+IUI
(3-4 Cycles)IVF
Abnormal
<2ng/ml
?DHEA
IVF+ICSI

Age 30-35 years,ML 1-2 years,Semen and TVS normal
2 cycles OI+Follicular study
Diagnostic laparoscopy+Hysteroscopy
4 cycles IUI(Tab CC+ HMG)
IVF-ICSI

Age 30-35 years,ML >3 years ,Semen normalAge 35-40 years,ML >1 years ,Semen normal
AMH/AFC
AMH>2
AFC >5
Diagnostic
Laproscopy+
Hysteroscopy
CC+/- HMG+IUI
(3-4 Cycles)IVF
AMH<2
AFC<5
?DHEA
IVF+ICSI

Age 35-40 years,ML >5 years ,Semen normal
AMH > 2
AFC normal
• IVF with own eggs
AMH 1 to 2
AFC less
• IVF-Own eggs/donor eggs
• ?DHEA
AMH < 1
AFC less
• IVF with donor eggs

Age 40-45 years
IVF-ICSI
Own eggs
20% Donor eggs
80%

Direct IVF treatment-Indications
Bilateral Tubal Block
Severe oligoAsthenospermia/Azoospermia
(TESA)
Premature ovarian failure
Age over 40 years
Genetic diseases(Donor gametes)

Surrogacy-Straight away….After hysterectomy
Congenital absence of the uterus
Repeated failure of IVF or Recurrent abortion
Severe intra-uterine adhesions
Severe medical conditions incompatible with pregnancy

PCOS
• Weight reduction
• Ovulation Induction
• Metformin
• Ovarian drilling

PCO drilling
Only 4 punctures with monoplorneedle using 4 watts for 4 seconds
WHO BENEFITS FROM PCO Drilling? CC resistant patients and those who are not responding to routine doses of gonadotrophins,Slim, raised S.LH

PCO drilling
Very damaging procedure
Please,please,please...
Don’t over do it.

Take Home Massages
• Infertility treatment protocols are highly dependent on ovarian age and duration of infertility.
• Hurry UP…Most treatments have higher rates of success in younger women.
• AMH can be a good guide to form a plan.
• ART should be resorted to after 6 months of traditional treatment by infertility expert . ..(After treating the respective cause)
8/29/2014

ONE SATISFIED PATIENT IS WORTH THOUSANDS OF GUIDELINES AND PROTOCOLS…!!!
32www. blossomivfindia.com