combining telehealth capabilities to strengthen delivery
TRANSCRIPT

Vickie de Jong
Project Officer
Acute Care@Home
Metro South Health
Vickie IrvingClinical Health SpecialistTelstra Health
Combining telehealth capabilities to strengthen delivery of home-
based acute care models

What is Remote Patient
Monitoring (RPM)?
• The monitoring of patients remotely – using an app on the patients mobile phone/tablet and Bluetooth equipment for the monitoring of vital signs
• Used in conjunction with normal HITH care and home visits

Photo credit Getty Images/iStockphoto
The Metro South RPM Trial
• A partnership with Telstra Health and the Telehealth Support Unit
• Dual Site 6 month trial – QEII and Redland Hospitals
• Commenced 27th August 2018
• First trial of this kind for HITH patients in Australia

1. Faster response to clinical
deterioration
2. Earlier identification of patient
stabilisation (to support
discharge)
3. Improved patient safety
through real time access to
observation data
4. Improved patient flow,
decreased transfers in &
reduced ED presentations
5. Increased referral rates to HITH
programs in line with improved
clinical decision-making and
provider confidence
6. Increased Diagnostic Related
Group’s and patient acuity
7. Decreased Length Of Stay and
improved service efficiency
8. Decrease in unnecessary travel
for patients and clinicians
9. Increased use of
videoconferencingGoals/Aims

Technology Drivers for HITH
Photo credit Getty Images/iStockphoto
Service Model Intent “Patients who are admitted to hospital substitution services receive care and treatment which is comparable to the services offered in a traditional hospital setting” Qld Department of Health Hospital in the Home Guideline
Safety & Quality Standards “Measurement of physiological observations plays a significant role in detecting clinical deterioration. Abnormal observations may occur at any time during a patient’s admission. Multiple studies and adverse events have shown that patients in acute care settings often go for prolonged periods without having appropriate physiological observations measured. When this occurs it can mean that clinical deterioration may not be recognised, and treatment may be delayed” Safety and Quality Improvement Guide Standard 9: Recognising and Responding to Clinical Deterioration in Acute Healthcare
“The delivery of comprehensive care is based on partnering with patients, carers and families to identify, assess and manage patients’ clinical risks, and determine their preferences for care; and on communication and teamwork between members of the healthcare team” NSQHS 5: Comprehensive Care

Combined capabilities to improve clinical outcomes
✓Care Planning (Engage)
✓Remote Patient Monitoring –
Quantitative & Qualitative data (Identify)
✓Secure Videoconferencing (Respond)
✓Affordable and accessible (Sustain)
Combined capabilities to improve clinical outcomes
üCare Planning (Engage)
üRemote Patient Monitoring –
Quantitative & Qualitative data (Identify)
üSecure Videoconferencing (Respond)
üAffordable and accessible (Sustain)

Client Application
• Cross platform (Android and iOS) on phone or tablet
• Consumer Bluetooth device integration (iHealth TGA
devices)
• Unmetered data usage when connected to the Telstra
network
• Care plan view including ability to track progress and
compliance
• Care plan task reminders (To do list)
• Offline capability

Provider Portal • Secure Web hosted Portal
• Immediate data synchronisation (online)
• Triage dashboard to improve caseload management ‘by exception’
• Coloured “bubbles” show the patient’s risk level -severity
• Automatically sorts patient results according to their risk level
• Configurable and templated health checks
• Simple secure video call initiation

How it works
Patient downloads MyCareManager
application
Patients provided Bluetooth devices
and/or manual data entry
Tasks & reminders pushed through to
patients
MyCareManager triages data
Alerts generated when data is outside parameters or tasks are missed

Trial Participants Key stats from MSHHS pilot patient dataTotal of 68 patients registered as active users of the MCM App (1st November 2018 to 28 February 2019)
64% of patient
participants are male
Average distance from
hospital ~ 7 km
59% of patient
participants are
diagnosed with cellulitis
Average age of patient
participants
~ 46 years old
Average number of
clinic visits ~ 1.7
Average number of
home visits ~ 3.5

Incident data overview –MSHHS pilot patient data and MCM App data
Top Responses – High risk Health Check incidents*Excl Process & Technical Errors
No. of interventions Percentage
Home Visit Scheduled 37 17%
Home Visit Scheduled (Transfer In Avoided) 1 <1%
Clinic Visit Scheduled 17 8%
Additional Observations 15 7%
Phone call to patient 11 5%
Top Responses – High risk Observation incidents*Excl Process & Techniclal Errors
No. of interventions Percentage
Home Visit Scheduled 16 17%
Home Visit Scheduled (Clinic Visit Avoided) 1 1%
Phone call to patient 9 9%
Phone call to patient (Home Visit avoided) 1 1%
Additional Observations 8 8%
Clinic Visit Scheduled 6 6%
Referred to medical officer 1 1%
Patient diagnosis Average no. of incidents per dayCellulitis 4.7Heart failure 5.5Hyperemesis 1.5Hypertension 4.0Infection 5.3Mastitis 9.0UTI 2.0Warfarinization 5.2
All patients 4.7
3 avoided events for high risk incidents (4 in total) – home visit, transfer in, clinic visit
Clinicians are more likely to seek ‘in-person’ review when qualitative data (symptoms) is combined with quantitative data
Incident categories (312 incidents analysed)
54%41%
5%
High Low Medium
Incidents per day by diagnosis (based on data from 32 patients and 466 incidents)
Responses to high risk observation incidents
Responses to high risk health check incidents

Incident data overview –MSHHS pilot patient data and MCM App data
Clinic visit
scheduled
Data entry
error
Home Visit
Scheduled
Incorrect both
are Pulse
Observations
scheduled
Observations
taken
*Patient
dischargedPhone Call
Referred to
medical officer
Technology
IssueTOTAL
Cellulitis29
(10.2%)
9
(3.2%)
62
(21.9%)-
10
(3.5%)
26
(9.2%)
113
(39.9%)
32
(11.3%)-
2
(0.7%)
283
(100%)
Heart Failure -2
(9.1%)
3
(13.6%)
1
(4.5%)
4
(18.2%)
1
(4.5%)
8
(36.4%)-
3
(13.6%)-
22
(100%)
Hyperemesis2
(66.7%)
1
(33.3%)- - - - - - - -
3
(100%)
Hypertension - - - - - -2
(50.0%)
1
(25%)
1
(25%)-
4
(100%)
Infection2
(10.5%)-
5
(26.3%)- -
3
(15.8%)
4
(21.1%)
4
(21.1%)-
1
(5.3%)
19
(100%)
Mastitis - -2
(22.2%)- - -
3
(33.3%)
4
(44.4%)- -
9
(100%)
UTI - - - - - - -4
(100%)- -
4
(100%)
Warfarinization -3
(3.9%)
30
(39.0%)- -
3
(3.9%)
20
(26.0%)
20
(26.0%)-
1
(1.3%)
77
(100%)
TOTAL (including ‘other’)37
(8.5%)
15
(3.4%)
110
(25.3%)
1
(0.2%)
14
(3.2%)
35
(8.0%)
150
(34.5%)
65
(14.9%)
4
(0.9%)
4
(0.9%)
435
(100%)
Further breakdown of actions taken for all incidents (by diagnosis)
Cellulitis, Heart Failure, Infection (all types) and patients undergoing Warfarinization generated the most clinical incidents requiring proactive intervention by the MSHHS Clinical Team.
1 clinic visit and 1 transfer in avoided(high risk incidents)
1 visit avoided(high risk incident)
1 visit avoided (low risk incident)

Patient survey results34/38 participants completed the survey
Happiness:
97% very or mostly satisfied
Ease of use (App):
73% very easy or easy to use
Ease of use (medical equipment):
97% very easy or easy to use
Comfort having observations remotely monitored:
97% very comfortable or comfortable
Preference to be monitored at home in future:
87% definitely or probably would
46% of patients had issues connecting to the internet
Behaviour Change:
93% Care Plan Adherence
“Fantastic Idea, gives reassurance being able to monitor your obs in your own home. Comforting for family members.”
“Great service saves so much time and money”
“Seems like a great system which should save beds in hospital. Best hospital I've been in!”
Outcomes so far – Patient Experience & Behaviour change

Right care, right place, right time
• 44 year old male with upper limb cellulitis
• No co-morbidities
• Admitted to HITH for IVAB’s, enrolled onto trial for RPM
• Observations and Health Checks were scheduled for 8am the next day……
CASE STUDY ONE

CASE STUDY ONE
The next day …
Photo credit: Cristan Lozan on Unsplash

Despite a deteriorating clinical presentation,
this 44 year old patient still didn’t call for
help…
We called him.
Photo credit: Cristan Lozan on Unsplash
CASE STUDY ONE

Outcome• Ambulance transport arranged from hospital
• Accurate clinical assessment made remotely
• Patient deterioration identified early
• Intervention and treatment occurred several hours faster than the standard HITH model
• Clinician did not need travel to the patient’s residence
• Sepsis avoided
• Patient made full recovery
• Paradigm shift from reactive response proactive response
CASE STUDY ONE

• 46 year old female
• Addison's Disease – co-morbidity
• Admitted to HITH - Urosepsis
• Motivated patient – regularly entering observation data into App on ad-hoc basis
Photo credit: Sage Kirk on Unsplash
Patient empowerment
CASE STUDY TWO
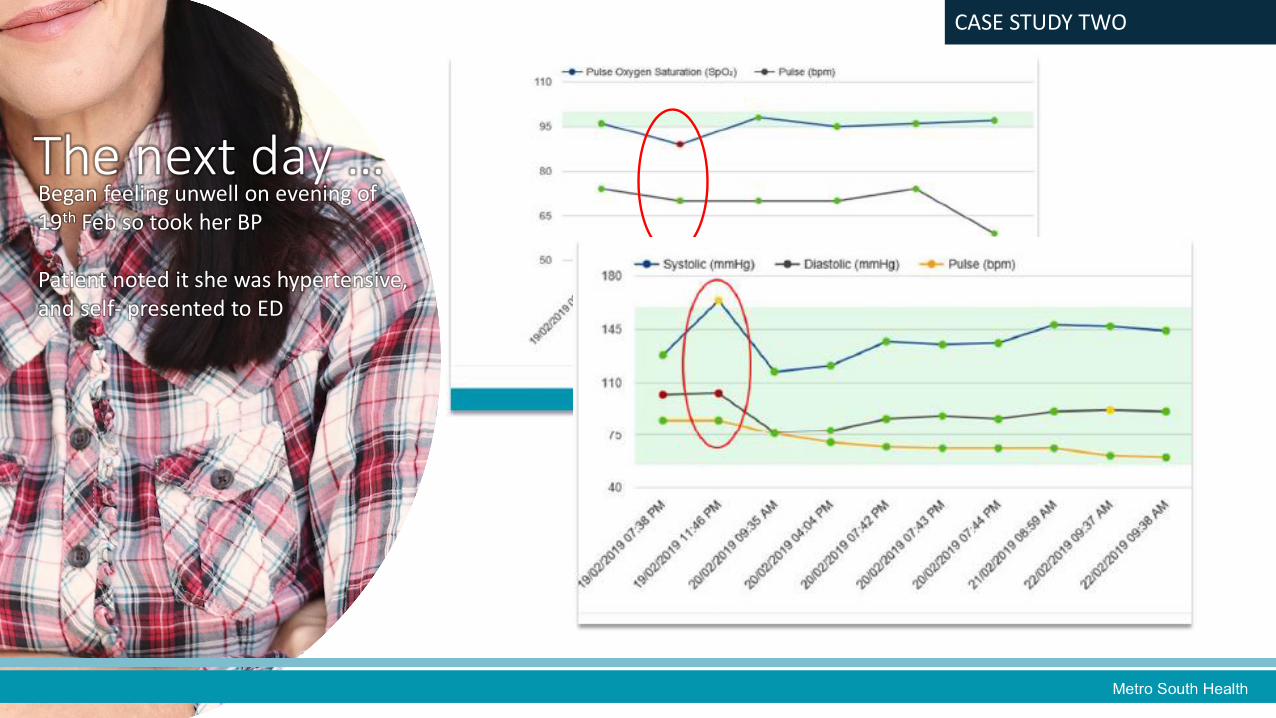
CASE STUDY TWO
The next day …Began feeling unwell on evening of 19th Feb so took her BP
Patient noted it she was hypertensive, and self- presented to ED

Outcome• Triage Category X patient
• Diagnosis: Addisonian Crisis
• Admitted to ED for XXX hours
• Discharged back home on HITH
• Continued RPM trial for X days
• Patient made a full recovery
• RPM data was the catalyst in patient’s decision to present to ED
CASE STUDY TWO
• BYOD technology – increased need for first-line technical support but patient’s like it & feel reassured
• Improve access by offering loan pool of provisioned devices – 49 patients had no suitable device
• PAS Integration to automate admissions/discharges/suspensions to support implementation at scale
• Upfront integration to Qld Health Telehealth Network worthwhile to prevent firewall blockages
• A project officer is essential to embed change & secure buy-in from clinicians
• Stage roll out – implement one site at a time
• New data sources – creates new insights to support change management & captures benefits of investing in technology
• Practice changes – ‘usual care’ home visits optimised –more time spent on responding to patients needs then finding out ‘what’s going on’.
Photo credit: Martin Brosy on Unsplash
The Journey So Far…

QUESTIONS?
Photo credit: Camylla Battani on Unsplash