combined internal and external osteosynthesis a biological approach to the treatment of complex...
TRANSCRIPT
ELSEVIER
Injury Vol. 29, Suppl. No. 3, pp. S-C22-S-C28,1998 © 1998 Elsevier Science Ltd. All rights reserved
Printed in Great Britain 0020-1383/98 $19.00+0.00
Combined internal and external osteosynthesis A biological approach to the treatment of complex fractures of the proximal tibia
A. Gerber, R. Ganz
Department of Orthopaedic Surgery, University of Berne, Inselspital, CH-3010 Bern
Summary 1
Lateral plating was combined with external fixation to treat 18 complex, proximal, tibial fractures with severe soft tissue injury. All patients were followed up until functional restoration of the limb had been achieved. In 15 cases, bone healing was uneventful. One deep infec- tion without knee joint arthritis, one delayed union and one malunion necessitated revision. Pin track compli- cations were negligible and soft tissue breakdown was not observed. The short-term results regarding the func- tional outcome showed a painless condition and good function in all patients. The method of fixation described is more invasive than the currently proposed minimally invasive combined fixation techniques, but can be regarded as an optimization of the mechanical and bio- logical advantages of the implants..
Keywords: complex proximal tibial fracture, biologi- cal osteosynthesis, combined fixation technique
Injury 1998, Vol. 29, Suppl. 3
Introduction
Treatment of complex meta-epiphyseal fractures is characterized by the difficulty of achieving accurate joint reconstruction and sufficient stabilization without jeopardizing the usually severely traumatized soft tis- sue envelope. On the proximal tibia, non-operative treatment using casts, braces or traction is complicated
1 Abstracts in German, French, Italian, Spanish, Japanese and Russian are printed at the end of this supplement.
by prolonged hospital stays and poor functional results (1,2) and the incidence of infection and soft tissue prob- lems associated with double plate fixation (3) has been reported to be high (4,5).
Mast applied the technique of combined internal and external osteosynthesis for the first time when treating a difficult distal intra-articular humeral fracture where, instead of posterior and medial plating, a posterior plate was used in combination with a lateral external fixator to neutralize the bending moments on the plate (6). He applied these techniques successfully in the treatment of complex ankle joint fractures (7). The field of appli- cation extended to other locations, including the proxi- mal tibia (8). Only one series of six patients has ever been reported (9) using a similar configuration to the one described here. Good results for proximal tibial frac- tures treated with minimally invasive techniques, such as the'Ilizarov system (10,11) or the hybrid fixation sys- tems, have been presented (12-14). In the current study, we describe the mechanical testing of combined inter- nal plate and external fixator techniques, emphasize some technical aspects of this method, and present our own clinical results for this technique.
Theoretical and technical considerations
According to Mast (8) the term substitution describes the function of the external fixator when used to com- pensate for the broken cortex until it is healed. Near the proximal end of the tibia, one can theoretically use two fixator systems, one medial and one lateral for neutral- ization of the adverse forces which become manifest

Gerber: Treating the proximal tibia
during the fun4tional rehabilitation of complex frac- tures. Circular, ring type systems such as the Ilizarov or hybrid fixation systems represent a mechanical opti- mization. However, the lateral pins penetrate through a rather mobile soft tissue layer compared with the medial side with an increased risk of pin track infections and increased difficulty in preserving alignment in frac- tures extending into the diaphysis.
The combination of a lateral plate with a medial fix- ator is more invasive but allows a more individual fix- ation of the given fracture type (Fig. 1). The long level arm of the external fixator ensures good stability although assembled in a simple manner (one Schanz screw in each fragment). The external fixator may be used as a distractor and maintained in combination with internal fixation.
When combined with an external fixator the dimen- sion of the plate can be smaller and a limited number of screws is necessary to fix the fracture. In this way a more elastic system is created allowing a modification of the mechanical properties (tension, compression) and /or the correction of an axial deviation (varus/valgus) in the postoperative phase. The implants needed are avail- able in most of the hospitals and are not terribly expen- sive.
Mechanical testing
Testing conditions
The mechanical properties of several fixation configu- rations of the proximal tibia were tested using an artifi- cial bone model (Synthes educational kit). A medial,
S-C23
wedge-shaped defect with lateral bone contact was cre- ated in the proximal tibial metaphysis. The material used for fixation consisted of 9-hole steel T-plates for the tibia, the corresponding cortical screws, and a half- frame AO external fixator.
The mechanical tests were performed on an Instron 4302 machine, applying an axial 0.1 kN force in a stan- dardized way on the model (Fig. 2) and measuring the corresponding deformation (Fig. 3). The values were recorded as a graph on an x / y plotter. The test was repeated several times for each sample. The stiffness (N/mm) was defined as the mean slope of three com- parable curves.
Sample 1 Having adjusted the T-plate to the lateral cortex, it
was fixed with three cortical screws in the proximal frag- ment and three cortical screws in the distal fragment such that bone contact of the fragments was achieved beneath the plate. The external fixator was applied per- pendicularly to the facies medialis of the tibia and to the plate using one Schanz screw in each fragment respec- tively. In sample 1 neither distraction nor compression forces were applied to the external fixator.
Sample 2 The medial fixator was removed and placed laterally
through the free holes of the plate without distraction or compression between the pins.
Sample 3 The external fixator was removed and a second 9-hole
T-plate was fixed medially using the same screw con- figuration as laterally.
Fig. 1: This example shows the versatility of the external fixator. In the proximal comminuted segment the fixator is placed in buttress mode with distraction between the first two pins. In the distal part of the fracture where stability through interfrag- mentary compression was possible, the fixator was placed in tension against the plate, changing its mechanical property to a tension band.
Injury 1998, Vol. 29, Suppl. 3
Sample 4 The medial plate was removed leaving the lateral
plate as the only fixation.
Testing results
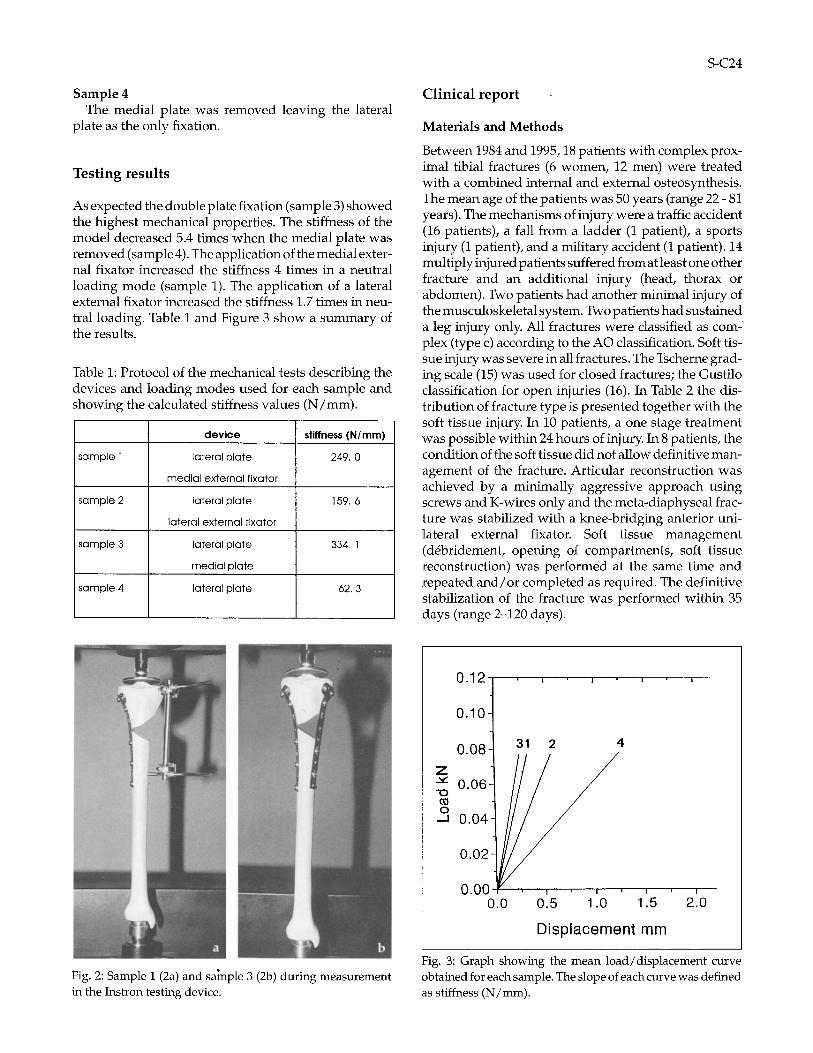
As expected the double plate fixation (sample 3) showed the highest mechanical properties. The stiffness of the model decreased 5.4 times when the medial plate was removed (sample 4). The application of the medial exter- nal fixator increased the stiffness 4 times in a neutral loading mode (sample 1). The application of a lateral external fixator increased the stiffness 1.7 times in neu- tral loading. Table 1 and Figure 3 show a summary of the results.
Table 1: Protocol of the mechanical tests describing the devices and loading modes used for each sample and showing the calculated stiffness values (N/mm).
dev ice stiffness (N /mm)
sample 1 lateral plate 249. 0
medial external fixator
sample 2 lateral plate 159, 6
lateral external fixator
sample 3 lateral plate 334, 1
medial plate
sample 4 lateral plate 62, 3
S-C24
Clinical report
Materials and Methods
Between 1984 and 1995, 18 patients with complex prox- imal tibial fractures (6 women, 12 men) were treated with a combined internal and external osteosynthesis. The mean age of the patients was 50 years (range 22 - 81 years). The mechanisms of injury were a traffic accident (16 patients), a fall from a ladder (1 patient), a sports injury (1 patient), and a military accident (1 patient). 14 multiply injured patients suffered from at least one other fracture and an additional injury (head, thorax or abdomen). Two patients had another minimal injury of the musculoskeletal system. Two patients had sustained a leg injury only. All fractures were classified as com ~ plex (type c) according to the AO classification. Soft tis- sue injury was severe in all fractures. The Tscherne grad- ing scale (15) was used for closed fractures; the Gustilo classification for open injuries (16). In Table 2 the dis- tribution of fracture type is presented together with the soft tissue injurY. In 10 patients, a one stage treatment was possible within 24 hours of injury. In 8 patients, the condition of the soft tissue did not allow definitive man- agement of the fracture. Articular reconstruction was achieved by a minimally aggressive approach using screws and K-wires only and the meta-diaphyseal frac- ture was stabilized with a knee-bridging anterior uni- lateral external fixator. Soft tissue management (d6bridement, opening of compartments, soft tissue reconstruction) was performed at the same time and repeated and/or completed as required. The definitive stabilization of the fracture was performed within 35 days (range 2-120 days).
Fig. 2: Sample 1 (2a) and sainple 3 (2b) during measurement in the Instron testing device.
0.12 , ,
0 . 1 0
0 . 0 8 31 2 4
Z 0 . 0 6 -
o 0 . 0 4
0 . 0 2
0 . 0 0 ', ' , " , '0 '.5 ).0 0 . 5 1 . 1 2'.0
D i s p l a c e m e n t m m
Fig. 3: Graph showing the mean load/displacement curve obtained for each sample. The slope of each curve was defined as stiffness (N/mm).
Gerber: Treating the proximal tibia S-C25
Plate osteosynthesis was performed through a lateral approach in all patients. In 17 patients the external fix- ation was applied medially, in one patient laterally to preserve the reconstructed medial soft tissues, whereby the Schanz screws placed in each main fragment passed through a plate hole. For intraarticular fractures treated in one stage, additional screws and even K-wires were used for articular reconstruction. In two patients, an autogenous bone graft was inserted in the same proce- dure. After definitive surgery the following supple- mentary surgical procedures were required: autoge- nous bone graft, a gastrocnemius flap, four split thick- ness skin grafts.
After surgery all operated legs were elevated until swelling of the soft tissues had resolved. Motion of the knee was achieved with a CPM apparatus. Range of motion was limited to varying extents in the early weeks and all patients were allowed to bear partial weight, i.e. 5 and 15 Kp, depending on the fracture type.
Instructions were given regarding pin care and wound dressing. All patients were seen weekly in the out-patient clinic as long as the fixator was in place.
After a mean time of 11 weeks (range 6-20 weeks) for radiological evidence of progressive fracture consoli- dation to appear, the external fixation was removed in 16 patients.fin two patients the external fixator had to be removed earlier due to a complication (see below).
Fx-Typ Fx-Numbel
41-C11 1
41-C12 1
41=C22 5
41-C23 6
41-C31 3
41-C32 1
41 -C33 1
Soft t issue in ju ry Closed f ractures Open fractures
G2 G3 TI Til TIIIA TIIIB TIIIC
1 2 1
3 1 1 1
2 1
1
1
Table 2: Distribution of soft tissue injury in relation to fracture type. The Tscherne and Gustilo classifications were used for closed and open fractures respectively.
Results
15 of 18 fractures healed without complications. In an alcohol dependent patient, a deep infection necessitated the removal of all fixation devices and thorough d6bridement 8 weeks after the operation. However, the fracture healed with plaster fixation within a year of the accident without additional surgery. In another patient, there were no signs of fracture healing four months post- operatively. Limited decortication, cancellous bone grafting and lateral repeat plating were performed after
removal of the external fixator. 14 months after the accident, the fracture had healed. In one patient with a varus deformity after removal of the fixator, a high tibial valgus osteotomy had to be performed two years later. In one patient, an arthroscopy with medial partial meniscectomy was performed after fracture healing due to persistent knee pain.
At the most recent physical examination, the mean range of motion of all knees was flexion/extension 129 ° (range 110-145 °) -2 ° (range (-10)-(+5°)) -0 ° (4 patients with flexion contracture)
Discussion
The mechanical testing presented here shows a com- parison of the bending properties of several types of fix- ation on the proximal tibia. The test is a considerable simplification of the reality since bone quality and frac- ture type have not been considered and torsion tests have not been performed. However, it was of interest to measure the mechanical effect of the external fixator on the system and to note the nearly comparable bending stiffness of double plate fixation and combined lateral plate and medial external fixation.
Anatomical joint reconstruction, axial alignment, and relative stability of the meta-diaphysis allowing imme- diate passive motion while keeping complications to a minimum are major goals in the treatment of complex proximal tibial fractures. Long hospital stays and com- plications due to bed rest made other treatment modal- ities superior to traction (1).
Cast immobilization or cast bracing as proposed by some authors do not provide enough stability and lead to a loss of reduction and malunion respectively (2). Open reduction and internal fixation would seem to allow accurate joint reconstruction and provide stable fracture fixation. The extensive bone exposure required for double plate fixation however increases the risk of soft tissue complications and infection. Moore et al. (17) reported wound dehiscence and/or infection in 8 of 11 bicondylar fractures treated with double plate fixation. Young and Barrack report that 7 of 8 knees became infected after open reduction and internal fixation (5). Jakob and Wagner showed a rate of 38% wound heal- ing problems and 15% deep infections in bicondylar tib- ial plateau fractures treated by double plating with the soft tissue problems being mainly on the antero-medial side (4).
In this context, the use of an external fixator as a sub- stitute is an attractive concept. Several variations of this principle have been proposed. Marsh (13) presented 21 complex fractures of the tibial plateau treated with closed reduction, interfragmentary screw fixation and application of a medial unilateral half pin external fix- ator. Although all fractures healed a high incidence of pin track problems (7 cases) and 2 cases of septic arthri-
Injury 1998, Vol. 29, Suppl. 3
tis were observed. These complications were attributed clearly to the external fixator which was left until the fractures consolidated, 13.5 weeks on average. Soft tis- sue breakdown did not occur.
The use of ring type systems, such as the Ilizarov or hybrid fixator systems, combined with minimal inter- nal osteosynthesis for joint reconstruction offers high mechanical properties but pin track problems are not to be underestimated since the device has to be left in situ more or less until the fracture has healed. Ilizarov him- self described the technique on the proximal tibia show- ing amazing results without mentioning any complica- tions (10). Watson et al. (11) reported on 50 complex frac- tures treated with the Ilizarov external fixator. All frac- tures healed on average within 15 weeks and the aver- age time of external fixation was 17 weeks. Complica- tions were not mentioned. In Murphy's series of 5 severe fractures of the proximal tibia treated with limited open reduction and a small circular external fixation device, union was achieved within 4-5 months and the exter- nal fixator was removed after 3 months. One pin track infection with septic arthritis was reported. Weiner et al. (18) treated 25 proximal tibial fractures with com- bined minimal internal and external fixation. The fixa- tor consisted of tensioned wires and half pins attached to a semicircular frame. Pin track problems were reported to be common and septic arthritis occurred twice. One malunion and one delayed union were observed.
All except two fractures healed in our series. A deep infection without knee joint contamination occurred in an older alcohol dependent patient and was treated by removal of the fracture fixation material and subsequent d6bridement. In the patient with delayed union, poor
S-C26
circulatory conditions related to extreme nicotine abuse were observed preoperatively. Delayed union necessi- tated reoperation; soft tissue problems were not observed when they might have been expected for a more aggressive primary surgical procedure.
Pin track infection and pin loosening are known to be quite frequent problems in fracture treatment with external fixation and represent a limiting factor in com- bined internal and external fixation. The incidence of such complications is known to be low at the beginning of the treatment and to increase with time (19). In our cases, the high mechanical properties of the plate in com- parison to simple screw fixation allowed an earlier removal of the external device compared with the times mentioned in the literature. Because the external fixator was used to stabilize the meta-diaphyseal fracture, the proximal pin could be placed at least 2 cm away from the joint surface which explains the absence of septic arthritis in our series. Another factor explaining the absence of pin track problems may be the meticulous pin care instructions given to each patient.
All in all, including our report, cases of soft tissue breakdown were not observed for combined osteosyn- thesis which represents a significant advantage of this technique when compared with the high rate of com- plications in patients treated with double plating. Con- solidation in correct alignment does not seem to be a problem in combined osteosynthesis. Considering the severity of trauma, the rates of delayed union and mal- union are low.
The short-term results regarding the functional out- come of the various series are difficult to compare because a standardized comparable evaluation is lack- ing. In our patients, a painless condition and a good
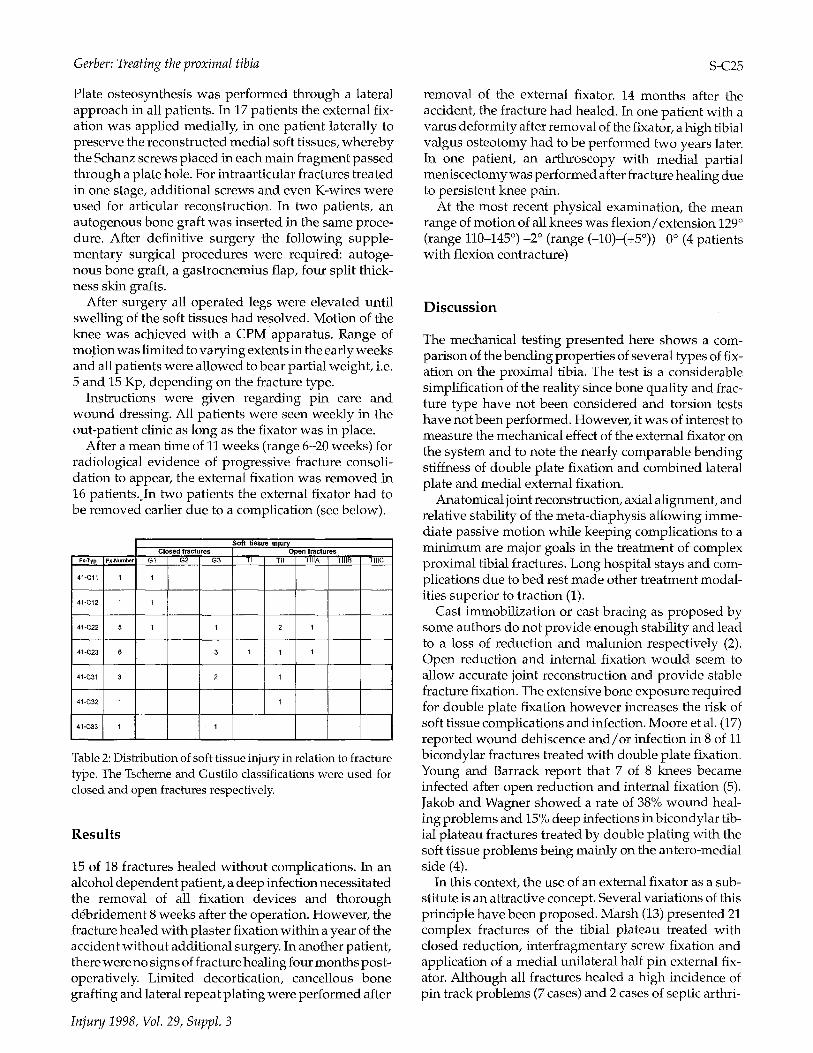
Fig. 4: High-energy injUry with fracture of the distal humeral meta-epiphysis, avulsion of the volar-radial musculature, including a laceration of the radial nerve and a gaping volar skin defect of the elbow region. The case demonstrates the use of a combined internal-external fixation. The external fixator is applied as a substitute for a second plate on the distal humerus.

Gerber: Treating the proximal tibia S-C27
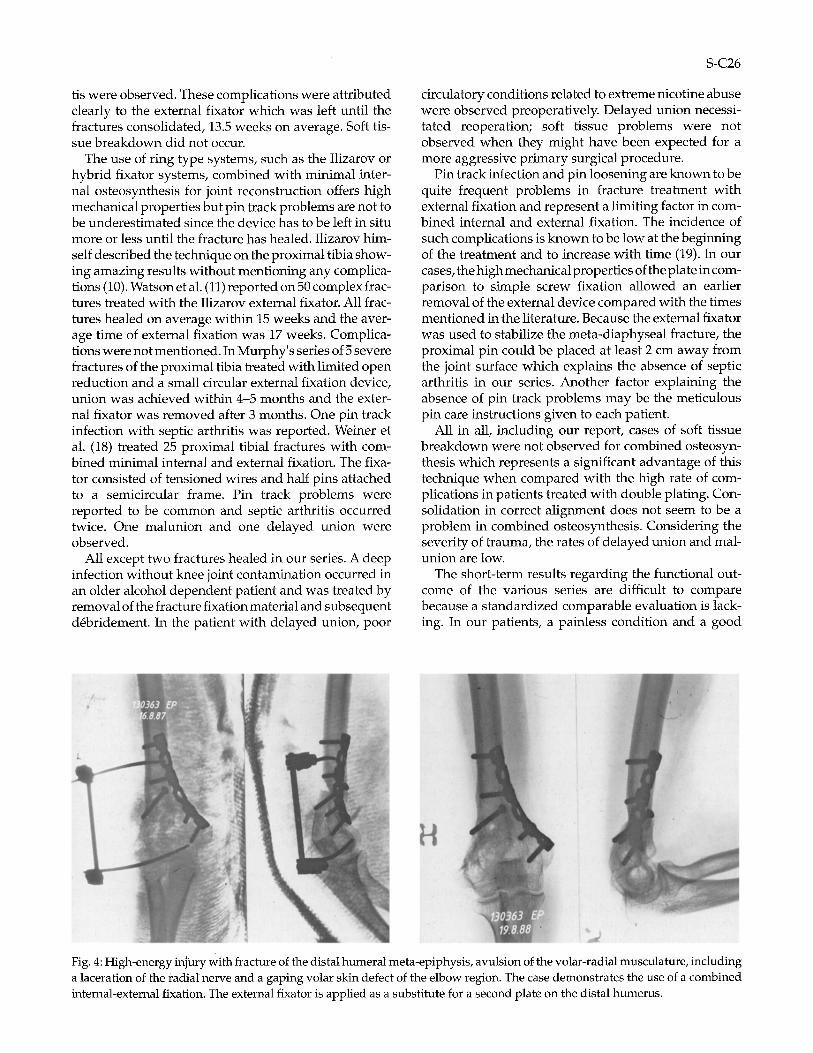
Fig. 5: Example of combined internal and external osteosyn- thesis as one surgical instrument respecting the philosophy of biological fracture treatment. This fracture healed without complications. The cosmetic and functional results are optimal.
functional outcome were observed at the last follow-up in all patients. The principle of substitution described above can be applied in the same way and for the same reason in other locations. The method was successfully applied in the treatment of complex fractures of the dis- tal humerus (Fig. 4) and the distal tibia (7), (20).
Conclusion
Combined internal and external osteosynthesis for com- plex fractures of the proximal tibia is the treatment of choice in our institution. Compared with those tech- niques using an external fixator and minimally invasive internal fixation, our method is more invasive. Despite the more extensive lateral approach, soft tissue prob- lems were not observed and the relatively short time of external fixation meant that any pin track complications were negligible. More than minimally invasive, the tech- nique carl be considered as optimally invasive combin- ing the mechanical and biological advantages of the implants (Fig. 5). Submuscular lateral tunnelling for plate fixation may represent a further improvement of the technique.
Acknowledgement
The authors express their gratitude to Jacques Cordey and Dieter Wahl at the AO ASIF Research Institute in Davos, for their assistance during mechanical testing.
Injury 1998, Vol. 29, Suppl. 3
References
1. Hohl M, Johnson E, Wyss D. Fractures of the knee. In: Rock- wood C, Green D, eds Fractures in adults. Philadelphia: JP Lippincott, 1991:1725-1752.
2. Apley A. Fractures of the tibial plateau. Orthop. Clin. North Am. 1979;10:61-74.
3. Miiller M, Allg6wer M, Schneider R, Willenegger H, eds Manual of Internal Fixation. 3rd Ed. Berlin, Heidelberg: Springer Verlag, 1991.
4. Jakob R, Wagner H. Zur Problematik der Platten- osteosynthese bei den bicondyl~ren Tibiakopffrakturen. Unfallchirurg 1986;89:304-311.
5. Young M, Barrack R. Complications of internal fixation of tibial plateau fractures. Orthop. Rev. 1994:149-154.
6. Mast J. pers. comm. 1980.
7. Mast J, Spiegel P. Complex ankle fractures. In: Meyers M, ed. The multiply injured patient with complex fractures. Philadelphia: Lea and Febiger, 1984.
8. Mast J, Jakob R, Ganz R, eds Planning and reduction tech- nique in fracture surgery. 1st Ed. Berlin Heidelberg: Springer-Verlag, 1989.
9. Ries M, Meinhard B. Medial external fixation with lateral plate internal fixation in metaphyseal tibia fractures. Clin. Orthop. 1990;256:215-223.
10. Ilizarov G. Treatment of fractures. In: Ilizarov G, ed. Trans- osseous Osteosynthesis. 1st Ed. Berlin, Heidelberg: Springer, 1992:406-444.
11. Watson J, Morandi M, Pearse M. Treatment of complex tib- ial plateau fractures with the Ilizarov external technique. SICOT. Amsterdam, 1996:336.
12. Murphy C, D'Ambrosia R, Dabezies E. The small pin cir- cular fixator for proximal tibial fractures with soft tissue compromise. Orthopedics 1991;14:273-280.
13. Marsh J, Smith S, Do T. External and limited internal fixa- tion for complex fractures of the tibia plateau. J. Bone Joint Surg. 1995;77A(5):661-672.
14. Raschke M, Khodadyan C, Windhagen H, Hoffmann R. Tibial plateau fractures with severe soft tissue damage - Percutaneous screw fixation and supportive composite hybrid fixation - A minimal invasive alternative? SICOT. Amsterdam, 1996:337.
15. Tscherne H, Gotzen L, eds Fractures with soft tissue injuries. Berlin: Springer, 1984.
16. Gustilo R. Current concepts in the managment of open fractures. Instr. Course Lect. 1987;36:359-366.
17. Moore T, Patzakis M, Harvey J. Tibial plateau fractures: definition, demographics, treatment rationale, and long- term results of closed traction managment or operative reduction. J. Orthop. Trauma 1987;1:97-119.
18. Weiner S, Kelly M, Yang E et al. Treatment of severe prox- imal tibia fractures with minimal internal and external fix- ation. J. Orthop. Trauma 1991;5(2):236.
19. Korkala O, Antti-Poika I, Karaharju E. La fixation externe darts les fractures ouvertes de la jambe. Rev. Chir. Orthop. 1987(73):637-642.
20. Tornetta P, Weiner L, Bergman M e t al. Pilon fractures: treatment with combined internal and external fixation. J. Orthop. Trauma 1993;7:489-496.
S-C28