contentscopharm.uobaghdad.edu.iq/wp-content/uploads/sites/6...their combination in the management of...
TRANSCRIPT

CONTENTS
ARTICLES Page
Comparative Evaluation of Using Intranasal Desmopressin, Parenteral Diclofenac or 1
their Combination in the Management of Acute Renal Colic Pain in Iraqi Patients
Ibrahim A. Majeed
Synthesis of Schiff bases of Benzaldehyde and Salicylaldehyde as anti-inflammatory Agents 5 Tagreed N-A Omar
Anti-fungal Activity of Punica Granatum I.peels Powder and Extracts from Pathogenic 12
Samples
Siham S. Shaokat , Hamoudi A. Hameed , Hassan J. Mohammad
The Release Of Diazepam From Different ConventionalAnd Hollow Type Suppository 21
Bases
Balkis A. Kamal
Effect of Ergotamine and its Combination with Vitamin E or Melatonin on Total 27
Antioxidant Status in Migraine Patients
Shahlaa H. Ali , Salim A. Hamadi , Ashwaq N. Al- Jaff .
Effect of Silibinin in Lowering the Intraocular Pressure in Normotensive Rabbits: 34
Interaction with Pilocarpine and Cyclopentolate
Saad A. Hussain , Haider M. Mohammed , Munaf H. Abdulrazzaq , Ahmed T. Numan
Effect of Silibinin in Lowering the Intraocular Pressure in Normotensive Rabbits: 39
Interaction with Betaxolol
Saad A. Hussain , Haider M. Mohammed , Ahmed H. Jwaied , Munaf H. Abdulrazzaq

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Desmopressin in renal colic
1
Evaluation of Using Intranasal Desmopressin, Parenteral Diclofenac or their Combination in the Management of Acute Renal Colic Pain in
Iraqi Patients Ibrahim A. Majeed*1
*Department of Clinical Pharmacy, College of Pharmacy, University of Baghdad, Baghdad, Iraq.
Abstract There is a suggestion that an antidiuretic hormone-induced decrease in diuresis might contribute to the rapid relief of the acute pain in renal colic. This study was designed to evaluate the efficacy of desmopressin nasal spray compared with diclofenac given intramuscularly in patients with acute renal colic. The study included 75 patients randomized into three different groups; group A received desmopressin (40 μg, nasal spray), group B diclofenac (75 mg) intramuscularly and group C, both desmopressin and diclofenac. Pain was assessed using a visual analogue scale (a 10-cm horizontal scale ranging from `no pain' to `unbearable pain') at baseline, 10, 20 and 30 min after administering the treatments. On admission, the pain level was the same in all three groups. At 10 min the pain decreased in all groups to a level that was not significantly different. At 20 min groups B and C had similar mean pain levels (5.8), whereas in group A it was 5.7. At 30 min, groups B and C scored 3.0 and 2.5 respectively, and group A 6.1. All three treatments were equally effective at 10 and 20 min but at 30 min there was a stabilization/slight increase in pain level in group A. In conclusion, these results indicate that desmopressin may be used to treat renal colic either alone or combined, increasing the analgesic effect of other drugs like diclofenac Key words: renal colic, intranasal desmopressin, diclofenac
: الخالصة وعز إلـ د ـي ذي ـق ة ىيوجد مقترح على أن هورمون المضاد للتدرر المحث لنقصن اإلدرار واـل ة إزاـل ي حصـوة الكلـي م الحـاد ـف هـذه الدراسـة . األـل
ة ى . صممت لتقييم كفاءة مادة ديسموبريسين عن طريق العضـلة للمرضـى المصـابين بحصـوة الكلـي وت عـل ريض بصـورة 75الدراسـة احـت ـمة مجـاميع المجموعـة رام 40اسـتلمت ديسموبريسـين ) أ(عشوائية تم تقسيمهم الى ثالـث ف , ميكروـك اك ) ب(المجموعـة .زذذ االـن دايكلوفيـن
اك ) ج(والمجموعة . ملغم عن طريق العضلة 75 دوائين ديسموبريسـين و دايكلوفيـن ي , استلمت كال اـل اس العيـن يم بواسـطة القـي م ـق 10( االـلالج دقيقة بعد تناول ا 30, 20, 10عند خط الشروع , ) لمدرج من ال الى غير محتمل االلم سم للقياس االفقي دخول مسـتوى . لـع د اـل عـن
وي 10عند , االلم كان متساوي في جميع المجاميع رق معـن اك ـف ن هـن م يـك ذي ـل ة , دقائق قل في كل المجاميع الى المستوى اـل د الدقيـق 20عـنة مجموعـة 30عند , 5.7كان ) أ(بينما مجموعة 8.5لها متوسط مستوى االلم ) ج , ب ( مجموعة ة ) ج , ب ( دقيـق ت القيـم , 3.5كاـن
ي , 6.1) أ(على التوالى ولمجموعة 2.5 أثير ـف ت متسـاوية الـت ة كاـن ي 20, 10كل العالجـات الثالـث ن ـف ة ولـك اك 30دقيـق ان هـن ة ـك دقيـقائج اوضـحت ان ديسموبريسـين ) . أ(استقرارًا على نقصان ضئيل في مستوى االلم عند لمجموعـة ك النـت ي االسـتنتاج تـل الج ـف د يسـتعمل لـع ـق
. المغص الكلوي منفردًا أو مركبًا لزيادة التأثير المسكن لالدوية االخرى مثل دايكلوفيناك دايكلوفيناك , ديسموبريسين , داخل تجويف االنف , مغص كلوي : مفتاح الكلمات
Introduction Renal colic is caused by an increase in pelvi-ureteric pressure secondary to an obstruction of the urinary tract. This increase in pressure causes a prostaglandins-mediated increase in renal blood flow and a subsequent increase in diuresis which, in turn, further increases intrapelvic pressure. Modulation of ADH is probably one of the most important mechanisms leading to an increased diuresis (1, 2) and one of the roles of prostaglandins (PGs) seems to be blocking the action of antidiuretic hormone (ADH) by interfering with cAMP-
mediated signal transmission (3). NSAIDs (inhibitors of PG synthesis) have long been used as effective agents in the treatment of renal colic. They block other PG-induced effects, such as afferent arteriolar vasodilatation, which causes an increase in diuresis and consequently raises pelvic pressure. They also reduce local oedema and inflammation, and inhibit the stimulation of ureteric smooth muscle, which is responsible for increased peristalsis and subsequently increased ureteric pressure. There is a suggestion that an ADH-induced decrease in diuresis might
1 Corresponding author : E-mail : [email protected]@yahoo.com Received : 23/9/2006 Accepted : 8/7/2007

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Desmopressin in renal colic
2
contribute to the rapid relief of the pain of renal colic(4). Desmopressin (1-desamino-8-D-argininevasopressin) is a synthetic structural analogue of ADH. Compared with ADH, it has a greater antidiuretic effect, a longer duration of action and reduced vasopressor activity. These properties make it a first-line drug for replacement therapy in central diabetes insipidus(5) and a very effective agent in the treatment of nocturnal enuresis (6).The marked antidiuretic effect of desmopressin is probably responsible for its efficacy in the treatment of renal colic (1). Peripherally, it has been shown that desmopressin suppresses the spontaneous contractions of circular smooth muscle fibers in the renal pelvis of rabbits (7). The same effect could be possible in humans. Some authors reported the role of desmopressin in stimulating the secretion of b-endorphins by the hypothalamus (8-11), which could explain a possible additional central analgesic effect of the drug. To assess the efficacy of intranasal desmopressin in relieving the acute pain of renal colic caused by urolithiasis, we compared the analgesic efficacy of this drug with of one of the most widely used NSAIDs in renal colic, diclofenac. We also compared desmopressin alone with desmopressin plus diclofenac. The study was enhanced by using the recently marketed intranasal spray form of desmopressin Patients and Methods This prospective, randomized trial was conducted between May and June 2005 in the emergency department, Al-Nasirya General Hospital, and included 75 patients (45 men and 30 women, mean age 40.3 ± 3.4 years) admitted to the emergency service with renal colic caused by lithiasis and who had previously received no treatment. The patients were randomly assigned to three groups; group A received desmopressin 40 µg intranasally, group B diclofenac 75 mg intramuscularly and group C, both desmopressin and diclofenac. A detailed history was taken and the patients examined. The time of onset and duration of the pain and associated symptoms were recorded, with the number and dates of former episodes, the elimination of calculus and eventual previous documentation of stones by imaging. Vital signs and positive findings of the routine physical examination were evaluated and recorded. Patients with evidence of high blood pressure, coronary disease, rhinitis, influenza, anticoagulant therapy, and peptic ulcer, renal or liver failure were excluded from the study, as
were any pregnant women. A visual analogue scale was used to assess the intensity of pain; this consisted of a 10-cm horizontal scale ranging from `no pain' to `unbearable pain', with values recorded to the nearest millimeter. The pain was assessed on admission and at 10, 20 and 30 min after therapy was administered. In all patients a plain X-ray of the urinary system was taken and any adverse reactions were recorded. The results, presented as mean + SD, were assessed statistically by comparative statistics (one-way ANOVA). Results After the random assignment, each group includes 25 patients. The mean duration of pain was 15.07 h, with slight differences among the three groups (14.5, 19.8 and 12.7 in groups A, B and C, respectively). The mean number of previous episodes was 1.3 (1.5, 1.32 and 1.09, in A, B and C, respectively). There were no significant differences in age, blood pressure, radial pulse, or axillary temperature, or in the laboratory values, i.e. for factors related to urinary osmolarity. The intensity of pain at presentation was similar in all groups (.table 1). After 10 min the pain scores were also similar, but at 20 min groups B and C had the same score, whereas group A had a higher score (5.3), and at 30 min, the scores were lower in groups B and C than in group A. In table (2) there were significant differences in pain score with time from baseline in all groups (P<0.01). Scores at 0, 10 and 20 min between groups were similar, but after 20 min the pain scores were lower in groups B and C. After 30 min, the differences between A and B, and between A and C, were significant (P<0.01). Although the differences between B and C were not significantly different, the score was lowest in group C. In Group A, there were significant differences between the first pain assessment and those at 10 and 20 min, but not after 30 min (i.e. pain increased after having diminished at 10 and 20 min).

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Desmopressin in renal colic
3
Table 1. The changes in mean pain score in the three groups with time after
administration of therapy.
Values were expressed asmean + SD, number of patients= 25 in all groups, values with non-identical superscripts (a, b, c, d) were considered significantly different P < 0.05. Table 2. Number of responders to treatment and their percentage after administration of
drugs. Number of responders to treatment
Response time (min)
Desmopres-sin 40µg
Diclofenac 75 mg
Combination
10 9 (36%) 21 (84%) 22 (88%)
20 8 (32%) 2 (8%) 3 (12%)
30 1 (4%) 2 (8%) 0 (0%)
Total 18 (72%) 25 (100%) 25 (100%)
Number of patients in each group = 25. Discussion Treating renal colic with intranasal desmopressin 40 μg induced prompt pain relief, with significant decreases in pain scores after only 10 min. This effect was maintained at 20 min and then decreased slightly, in contrast to a former study (1) in which the effect lasted longer (thus reflecting the progressive intranasal absorption of desmopressin, with a plasma peak that can occur up to 4 h after administration, indicating a relatively slow absorption through the nasal mucosa) (10). Within group A (as in group C), there were apparently two subgroups of patients with marked differences in their response to therapy (table 2). Thus, although the mean response to therapy after 10 and 20 min
was similar in the three groups, the response of individual patients showed that groups A and C had a greater proportion of patients with a marked decrease in their pain scores. Thus there seem to be two populations of individuals who will or will not respond to desmopressin. This was reported previously in two different studies (1, 2), in which 44% and 54% of patients, respectively, had complete pain relief. However, the underlying mechanism(s) are unknown; some authors suggest that it could be caused by individual variation in the intranasal absorption of desmopressin (10). Explaining these findings may detect factors that could be used to identify those patients in whom intranasal desmopressin may be more effective. As in a previous study (1), the administration of an NSAID with desmopressin was very effective in relieving pain, although the desmopressin was given before the NSAID and not simultaneously. NSAID action is more effective in the presence of higher plasma levels of ADH (4). In group C, none of the patients remain not responding to treatment after 20 min, which suggests that an NSAID with desmopressin may potentate each drug's analgesic effect, with no significant increase in adverse reactions. The mechanisms of action of NSAIDs and desmopressin were mentioned previousely (8-12). The antidiuretic effect of desmopressin is more intense than that induced by PG inhibition, but it is not caused by a decrease in renal blood flow. The antidiuretic action of NSAIDs may in effect be nephrotoxic, by decreasing renal blood flow and the GFR (through an increase in preglomerular resistance) in an already obstructed, dysfunctional kidney. This functional compromise is not clinically detectable, as PG inhibitors act selectively on the obstructed kidney, leaving the contralateral organ unscathed and allowing serum creatinine levels to remain within normal limits (13).The ease of administration of desmopressin, its low cost, good tolerability and lack of clinically relevant side effects make it safe. Studies using desmopressin therapy for up to 3 years have shown no toxic reactions or significant changes in laboratory values. Thus the results of the present study suggest that desmopressin intranasal spray may be a useful addition to the therapy for renal colic, either alone or combined with NSAIDs. It is a safe drug which is easy to administer and apparently effective in treating renal colic. Other issues which need to be explored include the optimum dosage, method of use (i.e. in an ambulatory setting), whether there is a reduction in the need for diagnostic or
Pain score
Response time (min)
Desmopress-in 40µg
Diclofenac 75 mg
Combination
0 7.5±1.2a 7.7±2.0a 7.65±1.5a
10 5.7±0.9b 5.8±1.1b 5.8±1.0b
20 5.3±0.8b 3.8±0.6c 3.7±0.7c
30 6.1±0.9b 3.0±0.6c 2.5±0.3d

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Desmopressin in renal colic
4
therapeutic interventions and whether it reduces the rate of hospital admissions. That there seem to be some patients who do not respond or respond only minimally to desmopressin needs further clarification; characteristics should be identified in this group which might explain their lack of response. In conclusion, these results indicate that desmopressin may be used to treat renal colic either alone or combined, increasing the analgesic effect of other drugs like diclofenac References
1. El-Sherif AE, Salem M, Yahia H, al-Sharkawy WA, al-Sayrafi M. Treatment of renal colic by desmopressin intranasal spray and diclofenac sodium. J Urol 1995; 153: 1395-1398.
2. Constantinides C, Kapralos V, Manousakas T, Mitropoulos D, Alamanis C, Dimopoulos C. Management of renal colic with intranasal desmopressin spray. Acta Urol Belg 1998; 66: 1-3.
3. Marumo F, Edelman IS. Effect of Ca++ and prostaglandin E1 on vasopressin activation of renal adenyl cyclase. J Clin Invest 1971; 50: 1613-1620.
4. Grenabo L, Aurell M, Delin K, Holmlund D, Sjodin JG. Antidiuretic hormone levels and the effect of indomethacin on ureteral colic. J Urol 1983; 129: 941-943.
5. Robinson AG. DDAVP in the treatment of central diabetes insipidus. New Engl J Med 1976; 294: 507-511.
6. Miller K, Goldberg S, Atkin B. Nocturnal enuresis: experience with long-term use of intranasally administered desmopressin. J Pediat 1989; 114: 723-726.
7. Kimoto Y, Constantinou CE. Effects of
(1-desamino-8-arginine) vasopressin and papaverine on rabbit renal pelvis. Eur J Pharmacol 1990; 175: 359-362.
8. Patchev VK, Racke K, Almedida OF. Adrenalectomy and experimental hypercorticalism modulate the basal, corticotropin- releasing-hormone and arginine-vasopressinstimulated release of hypothalamic beta-endorphin. Neuroendocrinology 1991; 54: 111-117.
9. Kjaer A. Vasopressin as a neuroendocrine regulator of anterior pituitary hormone secretion. Acta Endocr 1993; 129: 489-496.
10. Seif SM, Zenser TV, Clarochi FF, Davis BB, Robinson AG. DDAVP (1-desamino-8-D-arginine-vasopressine) treatment of central diabetes insipidus ± mechanism of prolonged antidiuresis. J Clin Endocr Metab 1978; 46: 381-388.
11. Kapcala LP, Weng CF, Juang HH. Protein kinase C activators stimulate b-endorphin secretion from hypothalamic cells. Brain Res Bull 1992; 29: 553-557.
12. Kjaer A, Knigge U, Bach FW, Warberg J. Permissive, mediating and potentiating effects of vasopressin in the ACTH and beta-endorphin response to histamine and restraint stress. Neuroendocrinology 1993; 58: 588-596.
13. Perlmutter A, Miller L, Trimble LA, Marion DN, Vaughan ED , Felsen D. Toradol, an NSAID used for renal colic, decreases renal perfusion and ureteral pressure in a canine model of unilateral ureteral obstruction. J Urol 1993; 149;926-930.

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Synthesis of anti-inflammatory aromatic Schiff bases
5
Synthesis of Schiff Bases of Benzaldehyde and Salicylaldehyde as Anti-inflammatory Agents
Tagreed N. Omar*,1 * Department of Pharmaceutical Chemistry , College of Pharmacy , University of Baghdad ,Baghdad , Iraq
Abstract
Three Schiff bases from Benzaldehyde and Salicylaldehyde have been synthesized (A, 1and 2) and two of them (1and 2) have been tested for anti-inflammatory activity. The p-aminobenzene sulfonamide has been synthesized from acetanilide through the addition of excess chlorosulfonic acid then concentrated ammonia solution; Schiff base of this derivative (2) exhibited good level of activity against egg-white induced edema in rat hind paw, while the other tested derivative exhibited no activity. Key words: Schiff bases, sulfonamide derivatives, salicylaldehyde
:الخالصة وقــد اختبــرت فعاليــة اثنتــين منهــا ) A,1,2(تــم فــي هــذه الدراســة تخليــق ثــالث قواعــد شــف مــن البنزالديهايــد والسالســيل الديهايــد
ن حـامض . كمضادات لاللتهابات رة ـم ة كبـي ان البارا امينوبنزين سلفون امايد هو احد االمينات قد تم تخليقه من االستاناليد من خالل اضافة كمـيي الجـرذان . روسلفونيك ومن ثم سائل االمونيا المركزالكلو ات المسـتحدثة ـف دة كمضـاد لاللتهاـب ة جـي ان قاعدة شف لهذا المشتق قد اظهرت فعالـي
.بواسطة زالل البيض٬ اما القاعدة الثانية المخلقة فلم تظهر أي فعالية مضادة لاللتهاباتIntroduction
Non-steroidal anti-inflammatory drugs (NSAIDs) are widely used for the treatment of pain, inflammatory conditions and fever (1,2). Their efficacy has been documented in a number of clinical disorders including osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, gout and dental pain (3). In the past decades; it has become apparent that there are two separate cyclooxygenase (COX) gene products, COX-1 and COX-2, which can initiate the metabolism of arachidonic acid to prostaglandins (PGs) and related lipid mediators (3). COX-1 expressed in most tissues of the body and largely governs the hemostatic production of arachidonic acid metabolism; whereas COX-2 is induced in response to inflammatory stimuli or physiologic stress and is responsible for the enhanced production of eicosanoid mediators characteristics of these situations. All classical NSAIDs inhibit COX-2 as well as COX-1 to varying degrees, thus they can be considered non-specific (4, 5). For a long time Sparatore and co-workers have been described sets of Schiff bases (diaryl- and arylheteroaryl azomethines) endowed with strong and long lasting anti-inflammatory activity against the rat hind paw edema induced by carrageenan (6). The same compounds reduced, dose dependently, the nitric oxide and PGEs production (7). All these properties were mainly correlate with the presence of phenolic functions, which can
display a generic anti-oxidant and radical scavenging activity, more than with the presence of the azomethine function (7). On the other hand, the azomethine function is endowed with multiform reactivity and particularly is able to react with thiol groups (8). Thus it could establish easily some kind of link with enzymatic or receptorial proteins. The diarylazomethines are isosteric with stilbenes and like these can exist in interconvertible cis and trans forms. Suitable substituted cis-stilbene derivatives are characterized by potent inhibitory activity on COX-2, quite similarly with that observed for a variety of vicinal diarylheterocycles, among which important anti-inflammatory drugs, like celecoxib and valdecoxib, are found(9). In the last class of drugs, the central five member ring may be of very different nature, either heterocyclic or carbocyclic (10,11); while the nature of substitutents on the two benzene rings is believed to be responsible for COX-2 selectivity by insertion into the secondary pocket of the enzyme, with the p-sulfonamido and p-methylsulfonyl groups playing a key role (12). Accordingly, we have now designed and synthesized Schiff bases of salicylaldehyde (compounds 1 and 2). Some of them bearing these peculiar substituents, in addition to azomethine function, which could play some peculiar role in the interaction with COX enzymes.
1 Corresponding author : E-mail: [email protected]@yahoo.com Received : 11/11/2006 Accepted : 8/7/2007

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Synthesis of anti-inflammatory aromatic Schiff bases
6
CH
N CH
N C
O
HO
(1)
CH
N
(2)
OH
S NH2
O
O
(A)
Experimentals A. Chemistry Materials: Acetanilide (Riedel-Dehaen, Germany), ammonia solution, benzaldehyde, salicylaldehyde, chlorosulfonic acid, absolute ethanol and ether (BDH, England), all solvents and materials used were of analar type and used without further purification. General procedure:Melting points were determined by capillary method on Thomas Hoover apparatus (England) and IR spectra were recorded on model 500 scientific IR spectrophotometry, Buck Company (USA). Ascending thin layer chromatography (TLC) was run on DC-Kartan SI Alumina 0.2 mm to check the purity and progress of reaction. The identification of compounds was done using iodine vapor and the chromatograms were eluted by methanol: acetic acid:ether: benzene (1:1:6:2) (13) Method for Preparation of p-aminobenzene sulfonamide (a) Preparation of p-acetamidobenzene sulfonyl chloride
Acetanilide (6.67gm, 49.4mmol) was placed in 250ml flask and melted in the flask over a free flamed and caused the compound to solidify over the lower part of the flask by swirling the liquid formed and immersion in an ice bath momentarily. The chlorosulfonic acid (17ml, 262mmol) was added all at once with continuous shaking, then the reaction mixture was heated on a water bath for 90 minutes in order to complete the reaction. The mixture was cooled and the oily substance was poured with stirring. This suspension was filtered off with suction, pumped and washed with a little cold
water and dried to give crude product, which was used immediately in the next step without further purification(13). (b) Preparation of p-acetamidobenzene sulfonamide The crude p-acetamidobenzene sulfonyl chloride was transferred to the rinsed reaction flask, and a mixture of concentrated ammonia solution (24 ml) and water (24 ml) was added to the flask. The contents of the flask were mixed thoroughly and heated with occasional swirling to just below the boiling point for about 20 minutes. The sulfonyl chloride will be converted into a pasty suspension of the corresponding sulfonamide. The suspension was cooled in an ice bath and then dilute sulfuric acid was added until the mixture was just acid to Congo red paper. The product was collected in Buchner funnel, washed with a little cold water and drained as completely as possible to give 53% yield of faint yellow crystals with melting pint of 213-214 oC and Rf values of 0.45. IR (in KBr disk): 3376cm-1 and 3304cm-1 (N-H stretching vibration of primary sulfonamide); 3227cm-1 (N-H stretching vibration of secondary amide); 1660cm-1 (C=O stretching vibration of secondary amide); 1598cm-1 and 1530cm-1 (C=C stretching vibration of aromatic ring); 1327cm-1 and 1157cm-1 (S=O stretching vibration of sulfonamide). (c) Preparation of p-aminobenzene sulfonamid
The crude p-acetamidobenzene sulfonamide was transferred to a flask contain a mixture of concentrated hydrochloric acid (10 ml) and water (30 ml). The mixture was boiled gently under reflex for 90 minutes. Cooled to room temperature and activated charcoal (2 gm) was added. The mixture was boiling gently under reflux for 90 minutes. Cooled to room temperature and activated charcoal 92gm) was added. The mixture was heated to boiling and filtered with suction through a hardened filter paper. The filtrate (a solution of 4-aminobenzene sulfonamide hydrochloride) was placed in a beaker and sodium bicarbonate was added in portions with stirring until the suspension become neutral by testing with litmus paper. The mixture was cooled in ice bath and filtered by suction and dried to give 51% yield of the white crystals with melting point of 160-161
oC (reported 163-165 oC) (14) and Rf value of 0.75. IR (in KBr disk): 3461cm-1 and 3373cm-1 (N-H stretching vibration of primary amine); 3247cm-1 (N-H stretching vibration of sulfonamide); 1639cm-1 (N-H bending of primary amine); 1600cm-1, 1571 cm-1 and

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Synthesis of anti-inflammatory aromatic Schiff bases
7
1504cm-1 (C=C stretching vibration of aromatic); 1309cm-1 and 1145cm-1 (S=O stretching vibration of sulfonamide). General Method for preparation of azomethines (Schiff bases) To a solution of 10 mmol aniline (compound A), salicylamide (compound 1), or p-aminobenzene sulfonamide (compound 2)in 50 ml of absolute ethanol, 12 mmol of benzaldehyde (compound 1) or salicylaldehyde (compound 2) were added and the mixture was refluxed for a reliable time; 6 hr for compound 1, 18 for the remaining compounds 1 and 2. After cooling the precipitate was collected, the solution was concentrated and a second part of the product was obtained. The joined fractions were washed with dry ether to remove some unreacted aldehyde and then crystallized by dissolution in dimethylformamide (DMF) and gradual addition of absolute ethanol. Compound 1: melting point (151-152 oC), yield (55% of the yellow crystals), Rf value (0.64); IR in KBr disk: 3346 cm-1 (O-H stretching vibration of phenol); 1655cm-1 (C=O stretching vibration); 1620cm-1 (C=N stretching vibration of imine). Compound 2: melting point (193-195 oC), yield (49% of the orange crystals), Rf value (0.86); IR in KBr disk: 3342 cm-1 (O-H stretching vibration of phenol); 3246cm-1 (N-H stretching vibration of sulfonamide); 1617cm-1 (C=N stretching vibration of imine); 1313cm-1 and 1163cm-1 (S=O stretching vibration of sulfonamide) B. Pharmacology Albino rats weighing (150 ± 10 gm) were supplied by the National Center for Quality Control and Drug Research. Animals were fed commercial chew and had free access to water add libitum, and were divided into four groups (each group consist of 6 rats) as follow: group A: served as control and treated with the vehicle (propylene glycol 50% v/v); group B: treated with indomethacin (reference agent) in a dose of 2mg/kg suspended in propylene glycol (15); group C and D: treated with tested compounds 1
and 2 respectively in a dose of 200mg/kg and 100mg/kg respectively as finely homogenized suspension in 50% v/v propylene glycol (initial dose of 200mg/kg was trialed and compounds which exhibited a statistically significant activity at this dose were further tested at doses decreasing by a factor of 2). Anti-inflammatory activity The anti-inflammatory activity of the tested compounds was studied using egg-white induced edema model (16). Acute inflammation was induced by a subcutaneous injection of 0.05ml of undiluted egg-white into the planter side of the left hind paw of the rats; 15 minutes after i.p. administration of the drugs or their vehicle. The paw thickness was measured by vernier at eight time intervals (0, 15, 30, 60, 120, 180, 240 and 300 minutes) after vehicle or drug administration. Statistical significance versus control group was evaluated by Student’s t-test and P-values less than 0.05 were considered significant. Results and Discussion Compounds 1 and 2 were screened for anti-inflammatory activity and their results together with indomethacin and control groups are summarized in table(1). Compound 2 exhibited significant inhibition of the egg-white-induced rat paw edema at the i.p. dose of 100mg/kg; which may resulted mainly from the nature of sulfonamide constituents on the aromatic ring. In Conclusion, the previously observed strong anti-inflammatory activity of Schiff bases has been now confirmed in compound 2. This activity may be attributed mainly to the incorporation of sulfonamide group substituent to the aromatic ring with only secondary contribution from the azomethine double bond. However, this issue deserves further investigations and further recommendations are warranted to demonstrate their selectivity towards COX-2 isoenzyme , As shown in fig(1) .

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Synthesis of anti-inflammatory aromatic Schiff bases
8
Table (1): The anti-inflammatory activity of the indomethacin and tested compounds.
Time (min.) Control Indomethacin Compound 1 Compound 2
0 4.46 ± 0.05 4.40 ± 0.17 4.45 ± 0.50 4.43 ± 0.15
15 5.41 ± 0.18 5.41 ± 0.1 5.40 ± 0.26 5.43 ± 0.10
30 6.05 ± 0.16 6.06 ± 0.13 6.07 ± 0.10 5.82 ± 0.07
60 6.35 ± 0.07 6.20 ± 0.14 6.30 ± 0.15 6.05 ± 0.09
120 6.5 ± 0.09 5.75 ± 0.10 6.29 ± 0.05 5.73 ± 0.12
180 5.93 ± 0.11 5.40 ± 0.10 5.75 ± 0.20 5.39 ± 0.07
240 5.38 ± 0.09 5.11 ± 0.04 5.24 ± 0.45 5.13 ± 0.05
300 5.2 ± 0.1 5.01 ± 0.01 5.13 ± 0.13 5.05 ± 0.04
Data are expressed as means ± SEM. n = 6.
Anova Test: The data illustrated in table (2), shows that there are highly significant differences between
the action of prepared drugs and between Indomethacin and control, also the time intervals shows highly significant between each its zones.
Table (2): Anova Test Source of Variation SS df MS F calc. F tab. 0.01 F tab.0.05
Rows 9.98395 7 1.426278571 73.487947(*) 3.6395896 2.4875777 Columns 0.424025 3 0.141341667 7.282524689(**) 4.8740462 3.072467
Error 0.407575 21 0.019408333
Total 10.81555 31 (*) Highly significant differences between time intervals with the probability of ≥ 0.01 type 1 error. (**) Highly significant differences between drugs action with the probability of ≥ 0.01 type 1 error.
Acknowledgment Greater thanks for every bit of help supported by every one help in presenting this work especially those in the department of pharmaceutical chemistry and the department of pharmacology –
College of Pharmacy – University of Baghdad. Iam also grateful Dr. Kawkab Y. Saour (Ph.D.) and Dr. Monther Faisal (Ph.D.) for their valuable helps.

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Synthesis of anti-inflammatory aromatic Schiff bases
9
IR spectrum of compound 1 in Kbr disk.
HC N C
O
HO
IR spectrum of p-aminobenzene sulfonamide in KBr disk.
H2N S NH2
O
O

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Synthesis of anti-inflammatory aromatic Schiff bases
10
Fig. (1): Paw thickness of rats treated with indomethacin, compound 1 and compound 2 with respect
to control. Results are expressed as means ± SEM (n=6).
IR spectrum of compound 2 in KBr disk.
HC N
OH
S NH 2
O
O

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Synthesis of anti-inflammatory aromatic Schiff bases
11
References:1. Harvey, R.A. and Champe, P.C.:
Lippincott's illustrated reviews: Pharm,acology (3rd ed.). Lippincott Williams and Wilkins, Philadelphia, 2006; 495.
2. Katzung, B.G.: Basic and clinical pharmacology (9th Ed.). Mc Graw-Hill, New York, 2004; 298.
3. Dubois, R.N.; Abramson, S.B.; Grofford, L.; et al.: Cyclooxygenase in biology and disease. FASEB J. 1998; 12: 1063-1073.
4. Simon, L.S.: Biologic effects of nonsteroidal anti-inflammatory drugs. Curr. Opin. Pheumatol. 1997; 9: 178-182.
5. Lipsky, P.E.; Abramson, S.B.; Grofford, L.; Dubois, R.N. and Vande Puttle L.B.A.: The classification of cyclooxygenase inhibitors. J. Rheumatol. 1998; 25: 2298-2302.
6. Karia, F. D.;Parsania, P. H. Asian J. Chem. 1999, 11 (3), 991-995.
7. More, P. G.;Bhalvankar, R . B.;Pattar, S. C. J. Indian Chem Soc. 2001, 78 (9), 474-475 .
8. Singh, W. M.; Dash, B. C. Pesticides 1988, 22(11), 33-37.
9. Pathak, P.; Jolly, V. S.; Sharma,K. P. Oriental. J. Chem. 2000, 16(1), 161-162.
10. Samadhiya, S.; Halve, A. Orient. J .Chem. 2001, 17 (1), 119-122.
11. Aydogan, F.; Öcal, N.; Turgut, Z.; and Yolacan, C. Bull. Korean Chem. Soc. 2001, 22, 476-480 .
12. Taggi, A. E.; Hafez, A. M.; Wack, H.; Young, B.; Ferraris, D.; Lectka, T. J.
Am. Chem. Soc. 2002, 124, 6626-6635.
13. Sparatore, F.; Pirisino, G.; Alamanni, M.C.; Monca-Dimich, P. and Satta, M.; Boll. Chim. Farm. 1978; 117: 638; Chem. Abstr. 1979; 91: 13760 b.
14. Cardile, V., Panico, A.M.; Geronikaki, A.; Gentile, B. and Ronsisvalle, G.: Farmaco. 2002; 57: 1009.
15. Harada, K.: In: The chemistry of the carbon-nitrogen double bond, Patai, S. (ED.). Interscience Publishers, London, New York, 1970; 255-298.
16. Talley, J.J.: Progr. Med. Chem. 1999; 36: 201.
17. Dannhardt, G. and Kiefer, W.: Eur. J. Med. Chem. 2001; . 36.
18. Chavatte, P.; Yous, S.; Marot, C.; Baurin, N.; Lesieur, D. J. Med. Chem. 2001; 44: 3223.
19. Reitz, D.B and Isakson, P.C: Curr. Pharm. Design 1995; 1: 211.
20. Mahdi, M.F.: Synthesis and preliminary pharmacological evaluation of new non-steroidal anti-inflammatory agents, Ph.D. Thesis, College of Pharmacy, University of Baghdad, 2006.
21. Furniss, B.S.; Hannaford, A.J.; et al.: Vogel's textbook of practical organic chemistry (4th Ed.). Longman, London, 1978; pp. 651.
22. Turull, A. and Queralt, J.; Medascape Newsletters 2001; 66(1): 27-37.
23. Vogel, H.G. and Goethe, J.H.: Drug discovery and evaluation. Pharmacological assay (2nd Ed.). Springer-Verlag, Berlin Heidelbers, 2002; 751.

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Anti-fungal activity of punica granatum
12
Anti-fungal Activity of Punica Granatum I.peels Powder and Extracts from Pathogenic Samples
Siham S.Shaokat*,1 , Hamoudi A.Hameed** , Hassan J.Mohammad*** * Ministry of Industry and Minerals Ministry of Industry and Minerals , Baghdad , Iraq **Ministry of Industry and Minerals Chief of food and Drugs sector , Baghdad , Iraq *** Prof. of Biopharmacy/Expert/Iben-Cena Center of Research. , Baghdad , Iraq Abstract Thirty five samples were collected from patients (1-30) years old, suffered from, infected skin , rushes, boils , oral thrush, anal & vaginal itches. Candida albicans 57.3% (20 isolates) and Candida tropicalis 22.5% (8 isolates) Aspergillus fumegatus 11.5% (4 isolates) Aspergillus nigar 8.7%(3 isolates) , were isolated & identified from these samples. Alcoholic & water hot extracts of the punica granatum (Pomegranate) peels as well as the dried powder were prepared. The anti-fungal activity of the extracts was evaluated by means of the agar-well diffusion assay. The extract exhibited potent activity against yeast. The Minimum inhibitory concentrations were 128-1024 μg/ml against Candida albicans and Candida tropicalis .Their was little difference between the activities of alcoholic extract & aqueous extract. These results suggest the Pomegranate Peels extract which contains gallotanic acid as a promising anti-fungal agent. Key wards : Antifungal agents, Plant extracts, Candida isolation
الخالصة: ريات التاليةعزلت وشخصت الفط, سنة 130من مرضى مصابين بإمراض جلدية مختلفة ألعمار من , نموذج 35تم جمع
Candida albicans (57.3%) ,Candida tropicalis(22.5%) , Aspergillus fumegatus (11.5%) ,Aspergillus nigar(8.7%) ة باســتخدا ى الفطريــات المعزوـل ة والماثيــة عـل ة المستخلصــات الكحولـي م إيجــاد فعالـي ي الوســط ألزرعـي الصــلب وطري مـت ة االنتشــار ـف قــة طريـق
ى عـزالت ة عـل ت قياسـات Candida tropicalis , Candida albicans التخفيف في أنابيب االختبار ووجدت أعلى فعالـي وكاـنة \مايكروكرام 1024 128الجرع المثبطة الصغرى ن المستخلصـات المائـي ل ـم ى بقلـي ة اعـل ة المستخلصـات الكحولـي ت فعالـي ل وكاـن أن . ـم
ة المس ى حـام فعالـي وي عـل ي تحـت ة ضتخلصـات الـت ات الجلدـي ي عـالج االلتهاـب دة ـف ا مفـي ات تجعلـه ك ضـد الفطرـي ات األغشــية , الكالوتانـي والتهاـب .المخاطية وإصابات الفم
Introduction The common name of Punica granatum is Pomegranate, belong to Family Punicaceae , of the Order Myrtales, Subclass Rosidae,Class Magndiopsida Pomegranate has a long history as food Medicine and herbal use dating back more than 3,000 years[1]. Both the stem and the root barks contain unusual alkaloids, known as 'pelletierines', which paralyze tapeworms so that they are easily expelled from the body by using a laxative[2]. The plant is also rich in tannin, the dried peels of the fruit contains about 26% which makes it an effective astringent. It is used externally in the treatment of vaginal discharges, mouth sores and throat infections[ 3]. Pomegranate(Punica granatum) peel extracts have been shown to possess significant antioxidant activity in various in vitro models, it has already been established that antioxidant activity in pomegranate juices is higher when extracted from whole pomegranate [ 4 ,5, 6,7,8]. Australian researchers found that their scientific investigation of pomegranate flower
extract improved hyperglycaemia in type II diabetes and obesity in which gallic acid is mostly responsible for its glycaemic activity[ 9,10,
11]. Concentrated pomegranate juice( CPJ) improves lipid profiles in diabetic patients with hyperlipidemia ,they concluded that (CPJ) consumption may modify heart disease risk factors in hyperlipidemic patients ,and its inclusion therefore in their diets may be beneficial[ 12,13 ]. Additionally,research findings on excess triglyceride accumulation and increased fatty acid oxidation in the diabetic heart, which contribute to cardiac dysfunction, suggested that pomegranate flower extract improves abnormal cardiac lipid metabolism[ 14]. In recent study, pomegranate juice was found to slow down cholesterol oxidation by almost half and reduce the retention of disproportionate LDL cholesterol [15]. Flavonoid –rich polyphenol fractions from pomegranate fruit have been shown to exert anti proliferative,anti-invasive
1 Corresponding author : E-mail : [email protected]@yahoo.com Received : 13/9/2005 Accepted : 4 /11/2007

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Anti-fungal activity of punica granatum
13
and proapoptotic actions in breast and prostate cancer cells and other solid malignancies[16,17,18,19,20,21]. Topical application of pomegranate fruit and seed oil extract tested on mouse skin appears to posses chemopreventive activity in skin tumours[22]. It has been found that the methanolic extract of pomegranate peels posses wound healing activity against an excision wound on the skin of Wistar rats[23]. The whole plant, but in particular the bark, is antibacterial, antiviral Furthermore pomegranate juice provides an HIV-1 entry inhibitor by preventing the virus binding to the cellular receptor CD4[24]. The dried rind of the fruit is used in the treatment of amoebic dysentery and diarrhoea . It is a specific remedy for tapeworm infestation[ 25,26]. Pomegranate rind extract has been shown to have gastro-protective activity through its antioxidant mechanism , it posses strong antibacterial activity against different species of entropathogenes which cause diarrhoea and dysentery, E.coli, Salmonella Shigella sonnei and Shigella flexner
[27,28,29,30,].Pomegranate (outer rind) extract is also screened for their antimicrobial activity against Gram-positive bacteria and yeasts, results founded that pomegranate showed good activity against Staphylococcus aureus and Candida [31].Plants used in Argentin folk medicine screened for antimicrobial activity against Staph. aureus commonly present on skin and mucous membranes which causes boils and abscesses, showed that pomegranate rind extract produced one of the more active results. Pomegranate peels showed also bactericidal effect on Vibrio cholerae[32].
Aim of the Study Candida and related yeasts are endogenous opportunists.Other opportunistic mycoses are caused by exogenous fungi that are globally present in soil, water and air. Several species of the yeast genus Candida are capable of causing candidiasis.They are members of the normal flora of the skin, mucous membranes and gastrointestinal tract. Candida species colonize the mucosal surfaces of all humans during or soon after birth and the risk of endogenous infection is ever present .Candidiasis is the most common systemic mycosis. Filamentous fungi such as Aspergillus are infected eye, ears, nose, and 5% of Natamycin drops used as treatment. Difficulties arising during chemotherapy of Candida albicans necessitate novel chemotherapeutic strategies. The aims of this
study are to investigate anti-fungal properties of water and ethanol, extracts & powder of Punica granatum L.Peels for treatment of several skin infections and inflammatory disorders. Materials and Methods Materials : Sabouraud agar, Potatos agar, Powder of Nystatin were obtained from (Russell, Beecham, and Special) Pomegranate peels powder, Candida albicans standard strain, Tannic acid. Instruments : Zone reader, Oven Memmert.Germany. Pasture pipett, Vortex mixer. Balances ( Sartorius), Homogenizer, Mixer, Incubator, Ultrasonic (soniprep 150HSE) at 20KHZ. Centrifuge, Autoclave, Water bath, Rotary evaporator, Souxhlet apparatus, Magnetic stirrer, Shaker, Incubator. 3-Clinical isolates from different clinical samples collected from three hospitals
Methods : Preparation of medium (33)
All media were prepared according to the manufacturers recommendations and were sterilized by autoclaving at 120C and 15 psi pressure for 15 minutes.
a-Sabouraud agar medium contain the following: Peptone 10gm, glucose 20gm, agar 15gm , distilled water(1000ml) ,pH 6-6.3 This medium recommended for the isolation of fungi from pathological samples.
b- Sabouraud conservation medium: Peptone 30gm, agar 20gm, distilled water (1000ml) pH= 6.5-6.7 this medium recommended for conservation of fungus.
c- Sabouraud agar medium with cycloheximide 0.5gm and Chloramphenicol pH 6-6.3 , &the same as( a ).This medium was recommended for isolation of Dermatophytes and other pathological fungi. Cycloheximide inhibited the growth of saprophytic fungus and Chloramphenicol inhibits the growth of microbial contamination.
d- Sabouraud broth medium: meat pepton 5gm, tryptic casein 5gm, glucose, 20gm, distilled water(1000ml) ,pH 5.7
e- Sabouraud ( Tetrazolium + Chloramphenicol) agar medium , contain the following: Pepton 10gm, glucose 20gm, agar 20gm 2,3,5, triphenyltetrazolium (H.C.L) 0.10gm, Chloramphenicol 0.5gm. For culture rapid

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Anti-fungal activity of punica granatum
14
differential media. The reduction of triphenyltetrazolium by the colonies of fungi appeared as different degree of red colour according to the type of fungusTable (1).
Preparation of MacFrland Standard Solution (33) :
Solution A- 1.175gm of barium chloride BaCl2.2H2O in 100ml of distilled water. Solution B-prepared by the addition of 1ml of concentrated H2SO4 to99ml distilled water.0.5ml of solution A was added to 99.5ml of solution B and the tube was compared with the bacterial suspension to give number of cell approximatively 108x1.5 fungi/ml.
Isolation and Identification of Candida (33) : In culture or tissue, Candida species grow as oval, budding yeast cells( 3-6 µm in size) .They also form pseudo hyphae when the buds continue to grow but fail to detach producing
chains of elongated cells that are pinched or constricted at the septations between cells. Candida albicans is dimorphic, in addition to yeasts and pseudohyphae, it can also produce true hyphae . On agar media within 24 hours at 37Cْ or room temperature. Candida species produce soft cream colored colonies with a yeasty odor. Pseudo hyphae are apparent as submerged growth below the agar surface. Two simple morphology tests distinguish Candida albicans , the most common pathogen from the other species of Candida. After incubation in serum for about 90 minutes at 37Cْ yeast cells of Candida albicans will begin to form true hyphae or germ tubes on nutritionally deficient media. Candida albicans produce large spherical chlamydospores.. Sugar fermentation and assimilation test can be used to confirm the identification and speciate the more common Candida isolates Table (1).
Table(1) – Rapid Identification of Candida albicans (33)
Species
Respones in 4 hours Respones in 24 Hours
Serum + Yeast Media
37C Filamentation=+
P.C.B Chlamydospores = +
Sabouraud+Actidion Growth = +
Inhibition =0
Sabouraud+Tetrazolium
Candida albicans + + + White
Candida stellatoidea + 0 + Rose
Candida tropicalis 0 0 0 Red-Violet
Candida pseudotropicalis 0 0 + Rose
Candida guilliermondii
0 0 + Red
Candida krusei 0 0 0 White
Candida .para krusei 0 0 0 Rose-Red
Candida zeylanoides
0 0 + White
Candida pulcherrima 0 0 0 Rose
Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Anti-fungal activity of punica granatum
15
Isolation and Identification of Aspergillus Aspergillus species grow rapidly, producing aerial hyphae that bear characteristic conidial structures: long conidiophores with terminal vesicles on which chains of conidia present , the species are identified according to morphologic differences in these structures, including the size, shape, texture and color of the conidia. (33)
Collection of Samples Form Patients : Candida albicans : 4 strains from skin infections, 2 strains from middle ear infections, four strains from rushes, 3 from infected boils , 2 from oral thrush, and 2 from anal and 3 from vaginal itches. Microscopic Examination : On direct examination of above samples 10% 0f NaOH or 10% of KOH, the hyphae of Aspergillus species are hyaline, septate,uniform in width. Culture:Aspergillus species grow within a few days on most media at room temperature. Species are identified according to the morphology of their conidial structures.
Collection of Pomegrante Fruit Rinds : The Punica granatum. Peals were obtained from the local market. Washed, cleaned and dried at room temperature or under the sun.
Spesifictions of Pomegranate Fruit Rinds :
The rind of the fruit is usually is irregular concave fragments, 1/20-1/10in.thick, brownish red externally and dull yellow on the inner surface, with depressions left by the seeds. The toothed calyx is present on some pieces. Taste astringent.
Preparation of Punica granatum Peels. Water Extract . A known quantity of Punica granatum peel was weighed and dissolved in 100ml distilled water boiled for 10-15minutes, soaked three hours, filtered twice, the filtrate was collected and evaporated by vacuum rotary evaporator at 55C until crud extract powder was obtained. The crud extract was weighed and dissolved in distilled water to calculate the concentrations needed for different experiments.
Reparation of Punica Granatum Peels. Alcholic Extract . Alcoholic (Ethanol extract was prepared by soaking the peels in 75% ethyl alcohol using (Souxhlet apparatus) at 50C then
filtered, evaporated by vacuum rotary evaporator at 45C and collected (34). Measuring PH : Ten grams of peels extract were dissolved in 50ml of D.W, shacked well by magnetic stirrer for 12 minutes, filtered and measure the pH. Detection of Punica granatum Peels Constituants(35)
Detection of Tannins 10gm of extract was dissolved in 50ml of distilled water, filtered and cooled 1% of lead acetate was added .The appearance of precipitation indicated positive reaction. Detection of Glycosides Equal amounts of Fehling reagent and extract were mixed and boiled 10 minutes in water bath, red precipitation indicated positive reaction (35)
Detection of Phenoles 10gm of Punica powder was dissolved in 50ml of d.w and boiled for 10minutes, filtered, cooled. 1% of iron chloride was added; greenish blue color appeared which indicated the presence of phenol. Detection of Saponines : Five ml of extract was added to1-3ml of Hgcl2; white precipitate was indicated positive reaction. Detection of Resin Fifty ml of ethyl alcohol 96% was added to five gm of pomegranate powder and boiled in water bath for two minutes, filtered (Ederal N02) 10ml of acidified with HCl, was added to filtrate precipitation will occur in the case of positive reaction.
Detection of Alkaloides(36) Ten gm of extract was boiled with 50ml of
d.w acidified with 40% Hcl. The solution was filtered and cooled .0.5ml from filtrate was tested with the following solution: Wagner solution- Grey precipitate positive reaction Mayer solution- white precipitate positive reaction Detection of Comuurins (36) A small quantity of extract was dissolved in alcohol in atest tube covered with filtered paper moisture with NaOH in water bath boiled 2-5minutes. The filter paper was exposed to U.V light (336 nm) the presence of yellow-green colour indicated the presence of comuurins. Detection of Flavones(36) Solution A –10gm of extract/ 5ml of ethyl alcohol 96%( Filtered) Solution B- 10ml of

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Anti-fungal activity of punica granatum
16
Ethyl alcohol 50%. Equal quantity was mixed,yellow precipitate indicated positive reaction, by exposing the spot of flavones to uv light, gave fluorescent spot, or by spraying with sulfomolybdic acid solution gave purple to rose color.
Susceptibility Test(37) Quantitative method, that require measurement of zone diameters give the most precise estimates of antibiotic susceptibility. 40-100 µl extracts from each concentrations (80%,70%, 60%, 50%, 25%) were poured in small holes applied at equal distances in Sabouraud agar seeded with 105-104/ fungi/ml , dried at room temperature , the inhibition zones were read ,after incubation at 28C for 18 hours. Inoculums of 105-104/ fungi /ml were prepared by dilutions with the same medium and spotted on Sabouraud agar. Minimum Inhibitory Concentrations(MICs)(37) he Minimum inhibitory concentrations (MICs) were determined by agar dilution method. Different concentrations of extracts( 2mcg/ml-8392mcg/ml) were diluted with Sabouraud agar in different Petri dishes. Inoculums of 108- 109 fungi /ml were diluted with the same medium to obtain 105-104/ fungi /ml spotted on agar, and incubated at 28C0 . These results were compared with different concentrations of Nystatin and tannic acid diluted with dimethyl formamide and spotted in one cm distance in the same Petri dish .The lowest concentration preventing growth (MIC) was estimated after 18 - 24 hours of incubation by the disappearance of spots. As control, Candida albicans, strain was tested under the same conditions. The activity of different concentrations of Punica granatum. L .. extracts were determined against Candida albicans, , Candida tropicalis , Aspergillus fumegatus& Aspergillus nigar .
(16,17,18,23, 29 30.32.33)
Results and Discussion
Pomegranate has a long history as food Medicine and still continues in the evolution. It is act as antioxidant ,antibacterial anticancer, and anti fungal activities, a gel made from
pomegranate peel has a high polyphenolic content demonstrated wound-healing capacity .Candida albicans 57.3% (20 isolates) and Candida tropicalis 22.5% (8 isolates) Aspergillus fumegatus 11.5% (4 isolates) Aspergillus nigar 8.7%(3 isolates) , were isolated & identified from the following samples. Candida albicans : 4 strains from skin infections, 2 strains from middle ear infections, 4 strains from rushes, 3 from infected boils , 2 from oral thrush, & 2 from anal &3 from vaginal itches. Antibiotic Susceptibility test and Minimum inhibitory concentrations (MICs) Table (2) and Table (3) - Shows the results of activity of alcoholic & water extract by disk diffusion technique of thirty-five strains comparing with control organisms(Candida albicans).The results were the following: 57.3% (20 isolates) Candida albicans 19.5-22 mm zone of inhibition with different concentrations of extracts and Candida tropicalis 22.5% (8 isolates) 21-23.5 , also good activity was noted with water extract with the same microorganism, these results indicated ,excellent activity of alcoholic and water extrat on Candida tropicalis and Candida albicans at different concentration comparing with standards. On the other hand no activity was observed against Aspergillus fumegatus 11.5% (4 isolates) and Aspergillus nigar 8.7 %(3 isolates) These results were in agreement with the studies of Holetz FB. Et al.,Fundacao-O-C.. pomegranate activity on candida albicans (31,
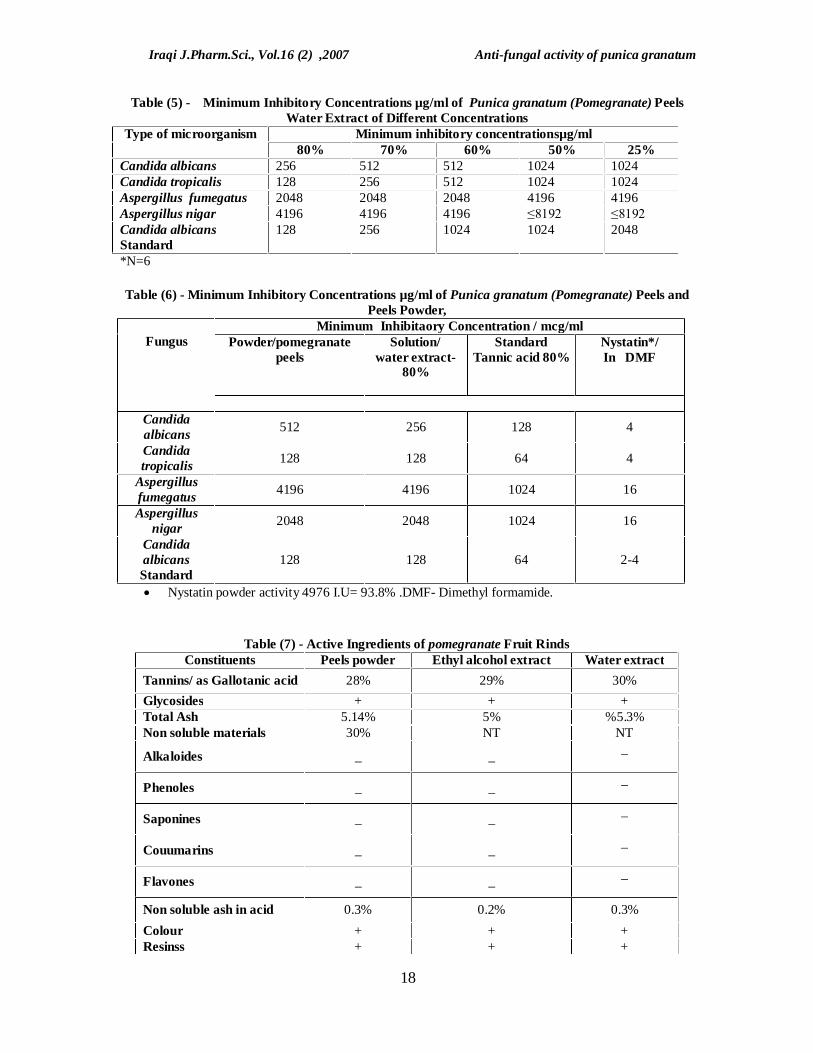
32).The comparative study of minimum inhibitory concentrations of extracts under test against all strains were studied.The results were as follow: MICs for alcoholic extract and water extract against Candida albicans and Candida tropicalis were 128-1024μg/ml, and for The MICs of for alcoholic extract and water extract against strains of Aspergillus fumegatus and Aspergillus nigar were very high as demonstrated in Table (4) and (5). Fig (1) demonstrated the diameters zone of inhibition of different dilutions of alcoholic extract against Candida albicans . The results were compared with the activity of Nystatin and Tannic acid. Table (6),Table (7) demonstrated the active ingredients of Pomegranate peels.

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Anti-fungal activity of punica granatum
17
Table(2) –Diameters Zone of Inhibition /mm of Fungi Under test (Ethanol Extracts )
Average diameters zone of inhibition/mm for different concentrations of Punica granatum
Type of microorganisms 80% 70% 60% 50% 25% 1- Candida albicans 10 22 21.5 21 20 19.5 2- Candida albicans 10 22 22 21 21 20 3- Candida tropicalis 5 23.5 23 22.5 22 21 4- Candida tropicalis 3 23 22.5 22 21 20 5- Aspergillus
fumegatus 4 5 0 0 8 0
6- Aspergillus nigar 3 0 4 2 4 0 7- Candida albicans
Standard 21 21 21 20 19.5
Table (3) - Diameters Zone of Inhibition /mm of Fungi Under test (Water Extracts )
Average diameters zone of inhibition/mm for different concentrations of Punica granatum water extracts
Type of microorganisms 80% 70% 60% 50% 25% 1- Candida albicans 13 21 20 19.5 19 18 2- Candida albicans 7 21.5 21 20 19.5 19 3- Candida 4 tropicalis 22 21 20.5 19 18.5 4- Candida 4 tropicalis 23 22 21.5 21 20 5- Aspergillus
fumegatus 4 4 4 0 0 0
6- Aspergillus nigar 3 0 0 0 0 0 7- Candida albicans
Standard 22 21.5 21 20 19.5
Table (4)- Minimum Inhibitory Concentrations µg/ml of Punica granatum Peels Alcoholic Extract of Different Concentrations
Type of microorganism Minimum inhibitory concentrations/ml
80% 70% 60% 50% 25% Candida albicans 128* 256 1024 1024 1024
Candida tropicalis 64 128 512 1024 1024
Aspergillus fumegatus ≤4196 4196 4196 ≤8192 ≤8192
Aspergillus nigar 2048 2048 2048 4196 4196
Candida albicans Standard
128 256 1024 1024 2048
*N=6
Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Anti-fungal activity of punica granatum
18
Table (5) - Minimum Inhibitory Concentrations µg/ml of Punica granatum (Pomegranate) Peels Water Extract of Different Concentrations
Type of microorganism Minimum inhibitory concentrationsµg/ml 80% 70% 60% 50% 25%
Candida albicans 256 512 512 1024 1024 Candida tropicalis 128 256 512 1024 1024 Aspergillus fumegatus 2048 2048 2048 4196 4196 Aspergillus nigar 4196 4196 4196 ≤8192 ≤8192 Candida albicans Standard
128 256 1024 1024 2048
*N=6
Table (6) - Minimum Inhibitory Concentrations µg/ml of Punica granatum (Pomegranate) Peels and Peels Powder,
Fungus
Minimum Inhibitaory Concentration / mcg/ml Powder/pomegranate
peels Solution/
water extract-80%
Standard Tannic acid 80%
Nystatin*/ In DMF
Candida albicans 512 256 128 4
Candida tropicalis 128 128 64 4
Aspergillus fumegatus 4196 4196 1024 16
Aspergillus nigar 2048 2048 1024 16
Candida albicans Standard
128 128 64 2-4
Nystatin powder activity 4976 I.U= 93.8% .DMF- Dimethyl formamide.
Table (7) - Active Ingredients of pomegranate Fruit Rinds
Constituents Peels powder Ethyl alcohol extract Water extract
Tannins/ as Gallotanic acid 28% 29% 30%
Glycosides + + + Total Ash 5.14% 5% %5.3% Non soluble materials 30% NT NT
Alkaloides _ _ _
Phenoles _ _ _
Saponines _ _ _
Couumarins _ _ _
Flavones _ _ _
Non soluble ash in acid 0.3% 0.2% 0.3%
Colour + + + Resinss + + +

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Anti-fungal activity of punica granatum
19
Conclusions From above study one can concluded that the extract of Pomegranate peels which contains Gallotanic acid is useful for the treatment of several infections and inflammatory disorders due to Candida albicans & Candida tropicalis , these results suggested the possibility of using this raw material in pharmaceutical as cream, ointment, skin solution, lotion ,powder, mouth wash, gargles and even ear drops. Further studies and investigations were needed . References 1- Bown. D. Encyclopaedia of Herbs and their
Uses. Dorling Kindersley, London. 1995 ISBN 0-7513-020-31.
2- Chie J R . Encyclopaedia of Medicinal Plants MacDonald 1984 ISBN 0-356-1054-5.
3- Facciola S. Cornucopia A Source Book of Edible Plants. Kampong Publications 1990 ISBN 0-9628087- 0-9.
4- Schubert-SY; Lansky-EP; Neeman. Antioxidant and eicosanoid enzyme inhibition properties of pomegranate seed fermented juice flavonoids; J-Ethnopharmacol;1999. 66(1): 11-7
5- Negi,P.S. Jayaprakasha G.K. Antioxidant and antibacterial activities of Punica granatum peel extracts. J.Food sci. 2003, 68 (4):1473-1477
6- Lansky, E,p. Physiologically synergistic mixtures of fruit componenas, methods of presentation thereof and method of use thereof. United state patent application Code 50118312 A1. june 2, 2005.
7- Gil MI , et al . Antioxidant activity of pomegranate juice and its relationship with phenolic composition and processing. J .Agric Food Chem. 2000;48(10): 4581-9.
8- Noda Y, et al. Antioxidant activity of pomegranate fruit extract and its anthocyanidins: dephinidin,cyaniding and pelargonidin. J Agric Food Chem. 2002 ;Jan 2; 50(1) : 166-171.
9- Li Y, et al. Punica granatum flower extract, a potent alpha-glucosidase inhibitor, improves postprandial hyperglycaemia in Zucker diabetic fatty rats. Ethopharmacol. 2005 Jun 3; 99 (2): 239-244.
10- Huang TH, et al. Anti-diabetic action of Punica granatum flower extract: activation of PPAR- gamma and identification of an active component.Appl. Pharmacol. 2005 Sept. 1; 207 (2) :160-9.
11- Jafri,-MA; Aslam,-M; Javed,-K; Singh,-S . Effect of Punica granatum Linn. (Flowers) on blood glucose level in normal and alloxan-induced diabetic rats. J-Ethnopharmacol 2000 Jun; 70(3): 309-14.
12- Esmaillzadeh A, et al. Concentrated pomegranate juice improves lipid profiles in diabetic patients with hyperlipidemia. J.Med Food. 2004 ;7(3):305-8.
13- Huang TH, et al. Pomegranate flower improves cardiac lipid metabolism in a diabetic rat model: role of lowering circulating lipids. Br. J. Pharmacol. 2005 , jul; 145(6):767-74.
14- Fiona Mac Rae. Pomegranate juice can help your heart. J Agric Food Chem. ; 2002; Jan 2; 50(1) : 81-6.
15- Sumner MD, et al. Effects of Pomegranate juice consumption on myocardial perfusion in patients with coronary heart disease. Am.J. Cardiol. 2005 Sep.15;96 (6): 810-814.
16- Seeram NP, et al. In vitro antiproliferative, apoptotic and antioxidant activities of punicalagin, ellagic acid and a total pomegranate tannin extract are enhanced in combination with other polyphenols as found in pomegranate juice. J . Nutr.Biochem. 2005;16 (6):360-7.
17- Suzuki R,et al. Cytotoxic effect of conjugated trienoic fatty acids on mouse tumour human monocytic leukemia cells,Lipids. 2001 May; 36(5):477-482.
18- Kawaii S, Lansky EP. Differentiation-promoting activity of pomegranate(Punica granatum) fruit extracts in HL-60 human promylocytic leukemia cells .J Med.Food. 2004,7(1): 13-18.
19- Mehta R, Lansky EP.Breast cancer chemopreventive properties of pomegranate (Punica granatum) fruit extracts in mouse mammary organ culture.Eur.J.cancer preventive.2004,Aug; 13(4) 345-348.
20- Malik A,et al. pomegranate fruit juice for chemoprevention and chemotherapy of prostate cancer. Proc Natl Acad Sci. U S A. 2005 Sep 28;245-7
21- AFAQ f, et al. Anthocyanin-and hydrolysable tannin-rich pomegranate
fruit extracts modulates MAPK and NF-kappaB pathways and inhibits skin tumorigenesis in CD-1 mice.Int. J. Cancer.2005 jan 20;113( 3): 423-433
22- Hora JJ,et al. Chemopreventive effects of pomegranate seed oil on skin tumor

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Anti-fungal activity of punica granatum
20
development in CDI mice. J Med.Food. 2003,6(3): 157-61.
23- Murthy KN, et al. Study on wound healing activity of Punica granatum peel .J Med.Food. 2004,7(2): 256-9.
24- Robert A Neurath, Nathan S, Yun-Yao Li,and AsimK Debnath. Punica granatum (pomegranate) juice provides an HIV-1 entry inhibitor and candidate topical microbicide. BMC Infectious diseases 2004,4:41 doi: 10.1186/1471-2334
25- Prashanth, D; Asha,-M-K; Amit,-A ,. Antibacterial activity of Punica granatum. Fitoterapia ;2001, 72 (2): 171-3.
26- Kohno H,et al. Pomegranate seed oil rich in conjugated linolenic acid suppresses chemically induced colon carcinogenesis in rats. Japan Cancer Sci. 2004 jun;95 (6):481-6.
27- Rani P, Khuller N. Antimicrobial evauation of some medicinal plants for their anti enteric potential against multi-drug resistant Salmonella typhi. India. Phytother. Res. 2004 Aug; 18 (8): 670-3.
28- Ajaikumar KB,et al. The inhibition of gastric mucosal injury by Punica granatum methanolic extract. J-Ethnopharmacol 2005 Jan; 4;96(1-2): 171-176.
29- Das AK. Et al. Studies on anti diarrhoeal activity of Punica granatum seed extract in rat. J-Ethnopharmacol 1999 Dec 15; 68(1-3): 205-208
30- Voravuthikunchai S, et al . Effective medicinal plants against enterohaemorrhagic E.coli 0157: H7. J-Ethnopharmacol 2004 sep;94(1): 49-54.
31- Holetz FB. Et al. Sceening of some plants used in the Brazilian folk medicine for the treatment of infectious diseases. Mem Inst Oswaldo Cruz, 2002 Oct.;97 (7):1027-1031.
32- Guevara JM, et al. The in vitro action of plants on Vibrio cholerae . Rev Gastroenterol Peru. 1994 jan, 14 (1): 27-31.
33- Jawetz, M,and Adelbergs. Medical microbiology 22Edition , 2001 p201 Lange Medical Books/ McGraw-Hill. Medical Publishing Division.
34- Prashanth, D;Padmaja,-R; Samiulla,D-S. Ethanolic extracts of punica granatum, Fitoterapia. 2001 , 72(2): 179-81
35- Harborne, J.B. 1979 Phytochemical methods, Science paper blacks.Chapman et al .London 259
36- Smolensk, S.j., Silnis,H.and Farnsworth,N.R. 1972 Alkaloid screening I-liyda 35 (1);314
37- Kirby,W.M.M. Baur ,A,N., ,Sherris ,K.C.&Turk,M., AntibioticSusceptibility testing by a standardized disc method . Amer.j.clin.Microb1966 43-45
38- Fundacao-O.C.F. Screening of some plants used in Brazilian folk Medicine for the treatment of Infectious diseases. Mem Inst Oswaldo Vol. 97(7) October 2002,P.1027-1031

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Diazepam Hollow Type Suppository
21
The Release of Diazepam from Different Conventional and Hollow Type Suppository Bases
Balkis A. Kamal*,1 *Department of Pharmaceutics , College of Pharmacy, University of Baghdad , Baghdad , Iraq
Abstract : The objective of this study was to investigate the release profile of different fat and water soluble bases using diazepam as a model drug , and then to develop a satisfactory formula with a rapid release of diazepam from suppository bases .The study was conducted using theobroma oil ,glycerol-gelatin and glycerol-PEG1540 bases using conventional mold method for preparation .while the later base was utilized to incorporate diazepam ( buffered solution ) in a hollow type suppositories. The results indicated that all types of bases can be utilized to formulate diazepam as rectal suppositories with acceptable disintegration time ( 12, 10, 6, and 6min.), respectively . While 100% of the released drug had been shown different release profiles with different storage time ( 15, 30, and 45 days ) in a refrigerator at 5°C , best results were obtained , when glycerol- PEG1540 used as a base for both conventional and hollow type mold methods .However , a decrease in the release rate of the drug was seen with glycerol-gelatin and glycerol-PEG1540
and to a lesser extent for glycerol-PEG1540 prepared by hollow type method . Key words: Diazepam , Hollow type suppository
:الخالصة
و من ثم تطوير , أن الهدف من هذه الدراسة هو للبحث عن شكل التحرر لعقار الدايازيبام كنموذج من خالل قواعد لبوسات شحمية و مائية زبدة الكاكاو ( الدراسة تواصلت باستعمال قواعد ان. تركيبة مقنعة بتحرر سريع لعقار الدايازيبام من قواعد هذه اللبوسات ولالكليسير,
جيالتين و ذلك باستخدام طريقة الصب التقليدية بينما استعملت القاعدة االخيرة الدخال الدايازيبام ) 1540بولي اثلين كاليكولالكليسيرول,وقات اشارت النتائج الى ان كل القواعد المستعملة من الممكن استخدامها لتركيب الدايا زيبيام كتحاميل شرجية با. كسائل في تحاميل مجوفة
من العقار المتحرر من هذه القواعد باشكال مختلفة قد تأثر بفترات % 100بينما وجد ان نسبة . دقيقة على التوالي) 6,6,10,12(اضمحالل كقاعدة في 1540بولي اثلين كاليكولكما ان افضل النتائج كانت عندما استعمل الكليسيرول, مئوية 5يومًا في درجة تبريد 45,30,15خزن
الطريقتين الصب و المجوفة كال ومع ذلك فان نقصان في معدل سرعة تحرر العقار قد لوحظ في قاعدة . جيالتين و قاعدة الكليسرول, . بطريقة التجويف 1540بولي اثلين كاليكولو الى حد اقل في قاعدة الكليسيرول 1540بولي اثلين كاليكولالكليسيرول
Introduction : Suppositories are solid dosage forms of various weight and shapes ,intended to be use in the rectum, vagina or even in the urethra (1) , they disintegrate in the body cavity either by melting or by dissolution (2). Rectal anxiolytic suppositories are indicated for patients with systemic sedative action (3), or to avoid hepatic first pass mechanism (4) , and also in post operative treatment (5) .Since most of sedative drugs are used widely , mainly diazepam (6), so it is of wise to use it as suppositories in children and elderly patients
as sedative-hypnotic agent in the management of clinical conditions (7, 8 ) , However , rectal solution of diazepam has not been used widely , due to its ability to leak out of the rectum , and then no efficient drug treatment obtained .This study has conducted by incorporated diazepam as a powder in melted bases and as a buffered solution in an engraved cavity within backbone of solid suppository (9) , in addition to develop most effective rapid release of diazepam from drug solution rather than dispersed diazepam in a suppository bases (10, 11 )
1 Corresponding author : E-mail : ybmmaz @yahoo.com Received : 24/3/2007 Accepted : 29/12/2007

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Diazepam Hollow Type Suppository
22
Experimental Materials :
- Diazepam, supplied by Sammara"a Drug Industry "SDI ,256BN6/2004, - Polyethylene glycol1540 ,BDH chemicals ,Ltd. ,Pool ,England. - Disodium hydrogen orthophosphate , potassium dihydrogen orthophosphate , E.merk ,Darmstadt, Germany. - Polyethylene sorbitan monolaurate ( tween 20 ) , Evans , Liverpool , England . - All other reagents were of analytical grade . Instruments : - Balance , sartorious AG , Gottingen ,Germany . - Dissolution apparatus , Copley , type , FH 16 – D , Nottingham , England . - Disintegration apparatus , water bath , Kotterman ,Ollmann , and Co. ,KG , D- 6360 , Friedberg – Germany . - pH- meter , pH 211 , microprocessor , Italy . - Suppository mold 1Gm. ,stainless steel , ERBO Prazision Forminbau , GMPHD- 7470 , Albstadt , England . - UV- Visible spectrophotometer , Cintra 5 , Double- beam spectrophotometer operation , manual GBC – England . Methods : Preparation of Diazepam suppositories :
The fusion method was used to prepare the conventional suppositories ( table 1. ), by mixing 5 mg.equivalent weight of diazepam in each 1g. . suppository base. After calculation the displacement value , the bases were melted using a water bath with continous stirring until homogenous mixture was produced , the melted mixture then poured into the metal suppository mold , and then cooled in a refrigerator maintained at 5 °C This process was conducted for the formulas ( 1,2 and 3, ) , while formula 4 was prepared by hollow- type method described by ,Watanabe , et al (12 ) , which summarized by melting the bases at 45 °C , then mixing water until homogenous dispersion results . The melted bases then poured into 1g. suppository mold equipped with a cylindrical tube in the center and allowed to stand for two hours at room temperature to solidify ,after that a construction of a hollow cavity in the solidified base , 0.5 ml. of buffered diazepam solution (prepared by mixing diazepam powder in 3% w/w tween 20 buffered in pH 7.8) was added to each cavity, the opening at the back part of the suppository was sealed with the same melted base , each suppository in all formulas contain an equivalent amount 5mg. of diazepam .
Table (1): Different prepared formulas suppositories with various methods
Formula
(1)
bees wax 10% ( Displacement value
0.88 ,Conventional) Theobroma oil 90%
Formula (2)
Gelatin 10%
(Displacement value 1.04 , Conventional )
Glycerin 70%
Water 20%
Formula (3)
PEG1540 30%
(Displacement value 0.98 , Conventional )
Glycerin 50%
Water 20%
Formula (4)
PEG1540 30%
(Displacement value ″not involved″ , Hollow type )
Glycerin 50%
Water 20%
Evaluation of Physical Properties of Suppositories : The prepared suppositories were evaluated for disintegration time according to the method described in British Pharmacopoeia BP (13 ), each determination was carried out in triplicate run. In-Vitro Dissolution Study : The dissolution rates of diazepam release from both conventional and hollow-type suppositories were carried out , a rotating basket dissolution apparatus was used at 50 rpm. maintained at constant temperature of 37°C. The medium used was 500ml. of orthophosphate buffer solution with pH 7.8, at time intervals 2,4,8,16,32,and 64 minutes , 5ml. of samples were withdrawn and the amount of diazepam was determined by UV-spectrophotometry at λmax. 232nm , using phosphate buffer as blank solution, the total percentage of drug released from the mean triplicate samples were estimated . Results and Discussions : The disintegration time for the prepared suppositories in the formulas 1 ,2 ,3 ,and 4 was 12±0.28 , 10±0.1 , 6±0.05 , and 6±0.11 minutes respectively , these results were found in consistent of BP and FDA requirement for disintegration time of rectal suppositories . Tables 2,3,4,5 and figure (1) . show the percentage of diazepam released from 4 different formulas of suppository bases and the method of preparation , At the first day of preparation , the results indicated that the release of diazepam from the

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Diazepam Hollow Type Suppository
23
0102030405060708090
100110
0 20 40 60 80
Formula 1
Formula 2
Formula 3
Formula 4
conventional and hollow - type suppositories is variable. Formula 1, 2 and 3 which they are prepared by conventional method revealed that the rate of diazepam release from insoluble theobroma oil is very slow compared with the rate diazepam released from hydrophilic base glycerol-gelatin and glycerol- PEG bases. The time for 50% drug release was more than 60 minutes from formula 1, compaired with 16 and 5 minutes for bases in formula 2, and 3 ,respectively . These results may be referred to the physico-chemical properties of both drug and the base used (14) . Diazepam is highly lipid soluble , so its presence in low concentrations in theobroma oil base will have slow step of escaping out side the base vehicle (10) . The slow release of diazepam from fatty bases may be attributed to its high lipid solubility and their greater retention within the oily base , that can be candidate to be sustained release dosage form ,when larger dose ( 10 -15 mg. ) diazepam was dispersed in the base (15 ) . On the other hand , the release of diazepam from glycerol-PEG bases showed significant difference ( P< 0.05 ) and revealed to be faster than that incorporated in glycerol-gelatin base ,since the time for 100% of drug release were about 32 and more than 64 minutes, respectively . These results were in consistent with the results obtained from piroxicam released when gelatinous base was employed(16), since gelatinous consistency of glycerinated gelatin in a dispersed system may be formed and decrease the drug release from gelatinous barrier . Meanwhile , the modification of suppository shape (hollow-type) by incorporating the diazepam as 1%(w/v) buffered solution ( formula 4), revealed that the drug release is significantly ( P< 0.05 ) faster than other conventional type used with the same base ( formula 3 ), since the time required for 100% drug release was 8 and 32 minutes , respectively . This result may be attributed to the concept that all the diazepam present in a buffered solution (pH7.8 ,formula 4 ) ,was available to be absorbed and this last about 6 minutes of disintegration time for suppository to be dissolved, compared with that diazepam powder dispersed in glycerol-PEG 1540 base (17) . The effect of storage period on the dissolution rate of diazepam was investigated at 5°C for 15 ,30 ,and 45 day ,the results were indicated that there is no significant difference ( P> 0.05 ) in the drug release from theobroma oil base (Formula 1 ) , when stored for 45 days (fig.2) , since the over all drug released remain limited ( 25-35% ) within the lipophyllic base (11). On the other hand ,the effect of storage on the diazepam
released from glycerol-gelatin base (fig.3) showed no significant decreasing in the amount of diazepam released. This behavior may be attributed to the tendency of free (OH) groups of glycerin to form hydrogen bonds with many functional groups located on amino acids moieties in gelatin , and this may form a cross-linking network that hinder the drug release (18) .This result was in agreement with the result obtained by Hanaee J. ,et .al , (18 ) .In addition ,the release of the drug from glycerol- PEG1540 base for conventional suppositories (Formula 3), showed that the time for 50% drug release was 4-8.5 minutes, besides to that, unusual hollow-type suppository filled with buffered liquid diazepam showed no effect on the drug released , after one month of storage (19 )The over all results of this study , revealed that diazepam can be formulated as a rectal suppository dosage form utilizing glycerol- PEG 1540 as a water soluble base, with best percent of drug release using solution of diazepam within hollow-type method of preparation ..
Table (2) : Effect of storage on the release of diazepam (5mg.) from conventional theobroma oil suppository base at 5 °C
(*) Each value represents the mean SD(±) ,with n=3 samples, and P<0.05 (significant), with corresponding percent of drug release . Figure 1. The percentage of diazepam released from different formulas (suppository bases) at first day of
preparation in phosphate buffer pH7.8 at 37 °C .
Percent of drug released after extensive period of storage time(*) .
45 day 30 Day 15 day One day
Time (min)
0 0 0 0 0 3±0.26 6 ±0.17 6 ±0.3 6±0.2 2 6±0.10 6 ±0.34 8 ±0.17 9±0.17 4
12±0.45 12 ±0.5 15 ±0.5 14± 1.0 8 18±0.52 23±0.46 24 ±1.0 26±2.64 16 22±0.6 26±0.5 29±0.6 30±0.9 32
25±0.25 27±0.69 30 ±0.4 35±1.05 64
Time (min.)
% D
rug
Rel
ease
d

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Diazepam Hollow Type Suppository
24
0
10
20
30
40
50
60
70
80
90
100
0 20 40 60 80
One day
15 day
30 day
45 day
Table (3) : Effect of storage on the release of diazepam (5mg.) from conventional
glycerol-gelatin suppository base at 5 °C .
(*) Each value represents the mean SD(±) ,with n=3 samples, and P<0.05 (significant), with corresponding percent of drug release .
Table (4) :Effect of storage on the release of
diazepam (5mg. ) from conventional glycerol–PEG 1540 suppository base at 5 °C .
Percent of drug released after extensive period of storage time(*)
45 day 30 Day 15 day One day
Time (min)
0 0 0 0 0 17±0.34 18±0.34 20±0.46 22±0.28 2 32±0.05 38±0.05 40±0.57 45±0.28 4 56±0.52 60±0.11 66±0.51 68±0.57 8 77±0.46 82±0.42 90±1.1 93±0.55 16 85±0.48 88±0.40 100±0.0 100±0.0 32 100±0.0 100±0.0 100±0.0 100±0.0 64
(*) Each value represents the mean SD(±) ,with n=3 samples, and P<0.05 (significant), with corresponding percent of drug release .
Table (5) :Effect of storage on the release of diazepam (5 mg.) from hollow-type glycerol-
PEG1540 suppository base 5 °C Percent of drug released after extensive
period of storage time(*) . 45 day 30 Day 15 day One
day Time (min)
0 0 0 0 0 20±1.15 22±0.34 26±0.57 36±0.46 2 42±0.51 50±0.55 68±1.12 84±0.23 4 72±0.52 80±0.51 90±0.56 100±0.0 8 96±0.48 100±0.0 100±0.0 100±0.0 16 100±0.0 100±0.0 100±0.0 100±0.0 32 100±0.0 100±0.0 100±0.0 100±0.0 64
(*) Each value represents the mean SD(±) ,with n=3 samples, and P<0.05 (significant), with corresponding percent of drug release .
Figure 2. Effect of storage on the release of diazepam (5mg.) from conventional theobroma
oil suppository base after different times in phosphate buffer pH7.8 at 37 °C .
Figure 3. Effect of storage on the release of diazepam (5mg.) from glycero-gelatin
conventional suppository base at different times in phosphate buffer pH 7.8 at 37 °C.
Percent of drug released after extensive period of storage time(*) .
45 day 30 Day 15 day One day
Time (min)
0 0 0 0 0 7±0.17 8±0.43 10±0.23 10±0.2 2 17±0.17 20±0.11 21±0.2 22±0.45 4 30±0.17 30±0.28 32±0.34 40±0.23 8 41±0.57 46±0.34 48±0.17 50±0.52 16 51±0.52 53±0.57 60±1.15 66±0.57 32 66±0.55 71±0.32 74±0.57 81±0.11 64
0
10
20
30
40
50
60
70
80
90
100
0 20 40 60 80
One day
15 day
30 day
45 day
Time (min.)
Time (min.)
% D
rug
Rel
ease
d
% D
rug
Rel
ease
d

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Diazepam Hollow Type Suppository
25
0
10
20
30
40
50
60
70
80
90
100
110
0 20 40 60 80
One day
15 day
30 day
45 day
0
10
20
30
40
50
60
70
80
90
100
110
0 20 40 60 80
One day
15 day
30 day
45 day
Figure 4. Effect of storage on the release of diazepam (5mg.) from conventional glycerol-PEG 1540 suppository base at different times in
phosphate buffer pH 7.8 at 37 °C.
Figure 5. Effect of storage on the release of liquid diazepam (5mg.) from hollow-type glycerol-PEG1540 suppository base after
different times in phosphate buffer pH 7.8 at 37 °C .
Conclusion : Based on the results obtained from this study, one can conclude the followings : 1- Diazepam as an anxiolytic drug can be formulated successfully using different suppository bases. 2- Best results obtained , using glycerol- gelatin and glycerol- PEG1540 as a water soluble bases. 3- Hollow-type suppositories can be used, for fast drug release for another drug therapies . References: 1- Ansel HC. ,Allen L.V. ,Popovich N.G.
,"Pharmaceutical Dosage Forms and Drug Delivery Systems " ,8th.. ed. ,Lippincot Williams and Willkins , (2004 ) 318-321 .
2- The Pharmaceutical Codex , 12th. ed. , The Pharmaceutical Press , London (1994) 170-174 , 959-963 , .
3- Bentley"s , "Text Book Of Pharmaceutics " , 8th. ed. ,Bailliere Tindall ,London , (1996) 347-350 .
4- Khan Ru. , El- Refaey H , "Pharmacokinetics and adversed effect profile of rectally administered misoprostol in the third stage of labor " ,
Obstet . ,Gynecol. ,( 2003) 101 ,5 ,968- 974 . 5- Kanamoto I. , Numora K. , " Plasma
morphine concentrations and analgesic effect after rectal adminsteration of suppository " , Japan Journal of Hosp. , Pharmacy , (1998)24 , 150-155 .
6- Pere Munne , M . Ruse , Ed. , (1998) " Diazepam Inchem . Org. .
7- Marija G., Kartina G. , Suzana T. , " Formulation and evaluation of diazepam hydrogel for rectal administration " , Acta Pharma , ( 2005 ), 55, 251-261 .
8- Kofugi K. ,Akamine H. , Togan Y. , " Therapeutic efficacy of sustained drug release from chitosan gel on local inflammation " , International Journal of Pharmaceutics , (2004) ,272 , 65-78 .
9- Deshmukh AA ., Thwaite S. , " Invitro release of diazepam from conventional and double layer PEG suppositories " Drug Development Ind. Pharmacy " , (1989) ,15 ,1289-1307 ..
10- Kazumitsu Y. , Toshikazn Y. , Toshikiro K. , " Design of controlled release morphine
suppositories containing poly glycerol esters of fatty acids " , Biology and Pharmacology Bullten , (2005) ,28 (8) , 1480-1484 .
Time (min.)
% D
rug
Rel
ease
d
Time (min.)
% D
rug
Rel
ease
d

11- Szilvia B. ,Eszter D. ,Istivan E. , " Invitro and Invivo study in rats of rapid release of rectal suppositories containing furosemide ", International Journal of Pharmaceutics , (2002) ,53 , 311-315 .
12- Watanabe Y. , Matsumoto Y. , " Pharmaceutical evaluation of hollow-type suppositories , Improvement of bioavailability of propranolol in rabbits after rectal adminsteration , Journal of
pharmacobiodynamic , (1986) ,9 ,(6) ,526-531.. 13- British Pharmacopoeia (2002),Vol I and
II , London C.D . 14- Realdon N., Raggazi E. , " Effect of drug
solubility ov invitro availability rate from suppositories with PEG excipient " Pharmazie , (2001)56 ,(2) ,163-167 .
15- Toshihito T. , Norihito S , "Evaluation of sustained release suppositories prepared with fatty base including fats with high
melting points ",International Journal of Pharmaceutics , (2004) ,278 , 275- 282 .
16- Eman J., Balkis A. Kamal ," The release of Piroxicam from different suppository bases Iraqi Journal Of Pharmaceutical Sciences , (2002),11 ,15-23 .
17- Kaewnopparat N. ,Roganarat W. ," Enhancement of diazepam release from Witepsol-15 suppositories " Inter., Journal of Pharmaceutical Compounding " (2004),July-Aug. ,1-6 ..
18- Hanaee J. ,Javadzadeh Y.,Taftachi S. ,Farid D. , " The role of various surfactants on the release of Sulbutamol from suppositories , Italian Pharmaco. , (2004) , 59 (11) , 903-906 .
19- Stansilaw J. , Malgozata S., Hallina G. ," Evaluation of paracetamol suppositories by a Pharmacopoeial dissolution test comments on methodology ,European J ., of Pharmam. and Biopharmacy , (2001), 52 ,(June) ,249-254 .

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Ergotamine, vitamin E, melatonin and total antioxidants
27
Effect of Ergotamine and its Combination with Vitamin E or Melatonin on Total Antioxidant Status in Migraine Patients
Shahlaa H. Ali 1 , Salim A. Hamadi ** , Ashwaq N. Al- Jaff**
** Department of Clinical Pharmacy ,College of Pharmacy , University of Baghdad, Baghdad , Iraq
Abstract Free radicals and oxidative damage caused by them have being suggested to be involved in the
pathogenesis of migraine. These may result from distorted equilibrium of pro-oxidant/anti-oxidant system that continuously generates and detoxifies oxidants during normal aerobic metabolism. Escape of such system from equilibrium leads to damage of cellular elements with the depletion of cellular stores of anti-oxidants material such as glutathione and vitamin E. Therefore, free radical scavengers (vitamin E or melatonin) seems to be of potential benefit as prophylactic anti-migraine therapy by neutralizing free radicals overproduction and possibly preventing formation of highly toxic intermediates (such as nitric oxide). In addition of being powerful antioxidant, melatonin was shown to possess promising effects in modulating severity, frequency and duration of migraine attacks. For this reason the present study was conducted to investigate the involvement of changed anti-oxidant defense (measured as total antioxidant status “TAS”) during migraine attack and the possible modulation of such status by classical anti-migraine therapy (ergotamine), antioxidants (vitamin E and melatonin) and their combination. 23 normal subjects and 21 migraine patients with age range of (17-45) years were enrolled in the study. Patients were diagnosed according to neurologist decision to have migraine with and without aura. Migraine patients were divided into three treatment groups; first group treated with ergotamine alone, second group with ergotamine /vitamin E and third group with ergotamine /melatonin. All groups were advised to take their treatments during attacks. Blood samples were drawn from migraine patients and normal subjects before initiation of therapy and after pain has been relived (from migraine patients only) for the investigation of TAS . The results of the study showed that TAS was significantly lower in migraine patients in comparison to control healthy subjects (P<0.05) with a percent reduction ranged from 35.46% to 43.97%. However, there is no significant difference in the level of TAS among migraine patients (P>0.05). Treatment with ergotamine raised significantly the level of TAS by 157%. The addition of vitamin E or melatonin greatly raised TAS by 179% and 176% respectively. The addition of vitamin E to ergotamine showed superior effect to that when melatonin was added. The greater reduction in TAS seen in this study among migraine patients in comparison to control healthy subjects suggests the presence of generalized decrease in antioxidant defense elements. Elevation of TAS by all treatments was very clear. In conclusion the decrease in TAS can be implicated in the pathophysiology of migraine and enhancement of antioxidant system can add a beneficial effect for the management of migraine headache with the use of antioxidants (vitamin E or melatonin) with classical anti-migraine drug.
الخالصـــــــــــةقد سببية داء الشقيقة وهذا اإلجهاد التأكسديتعتبر الجذور الحرة واإلجهاد التأكسدي الناجم عنها من النظريات المفترضة حديثًا في
ينشأ عن عدم التوازن في أنظمة األكسدة واألنظمة المضادة لألكسدة والتي تنتج جذورًا حرة وتعالج سميتها باستمرار خالل عمليات األيض فة إلى نفاذ المحتوى الخلوي من مضادات إن انعدام السيطرة أو الخلل في عمل هذه األنظمة يؤدي إلى تلف المواد الخلوية باإلضا. الخلوي
األكسدة الطبيعية مثل الغلوتاثيون وفيتامين هـ اد القانصة للجذور الحرة مثل فيتامين هـ أو الميالتونين تبدو ذات فائدة وقائية ضد ,لذا فأن الم. أوكسيد النتريك(ور حرة خطيرة مثل داء الشقيقة من خالل معالجة اإلفراط في إنتاج الجذور الحرة وربما بالتقليل من تكون جذ إن ).
. الشقيقة الميالتونين باإلضافة إلى كونه مضادًا فعاًال ضد األكسدة فانه قد اظهر فعالية موعودة في التقليل من حدة وتردد وفترات اإلصابة بألمالحالة الدفاعية الكلية ضد "مقاسًا بشكل (ة وعلى هذا األساس أجريت الدراسة الحالية الستكشاف تدخل تغير العوامل الدفاعية ضد األكسد
األكسدة فيتامين هـ ( ة٬ مضادات األكسد)االرغوتامين(خالل نوبات صداع الشقيقة ومدى إمكانية تغيير هذه الحالة بالعالج التقليدي ") والميالتونين 1745(عمري مريض بداء الشقيقة وبمعل 21شخص سليم و 23ُأجريت الدراسة على .أو باالثنين معًا) سنة) ُشخص .
المرضى كونهم مصابون بداء الشقيقة وفق قرار أخصائي الجملة العصبية قسم المرضى إلى ثالث مجاميع عالجية٬ عولجت المجموعة .الج خالل حدوث ارشد المرضى إلى اخذ الع. األولى باالرغوتامين والثانية باالرغوتامين مع بفيتامين هـ والثالثة باالرغوتامين مع الميالتونين
لقياس ) من مرضى الشقيقة فقط(ُأخذت عينات الدم من مرضى الشقيقة واألصحاء قبل بدء الدراسة وبعد تسكين الم الشقيقة . نوبات الم الشقيقة .الحالة الدفاعية الكلية ضد األكسدة
. mail : -E: ing authorCorrespond [email protected][email protected]
Received : 26/7/2007 Accepted : 29/12/2007

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Ergotamine, vitamin E, melatonin and total antioxidants
28
أظهرت النتائج أن الحالة الدفاعية الكلية ضد األكسدة منخفضة لدى مرضى الشقيقة بالمقارنة مع األصحاء وكانت نسبة االنخفاض بمستوى الحالة الدفاعية الكلية ضد األكسدة بين مرضى وعلى أية حال لم يكن هناك فرق منطقي%. 43.97إلى % 35.46تتراوح بين
كما وان إضافة %. 157إن العالج باالرغوتامين قد أدى إلى ارتفاع منطقي بمستوى الحالة الدفاعية الكلية ضد األكسدة بنسبة . الشقيقة أنفسهموعلى العموم . على التوالي% 176و % 179ضد األكسدة وبنسبة فيتامين هـ أو الميالتونين قد أدى إلى ارتفاع أكبر في الحالة الدفاعية الكلية
يظهر االنخفاض الكبير في الحالة . فقد اظهر فيتامين هـ تفوقًا في رفع الحالة الدفاعية الكلية ضد األكسدة عن تلك التي أظهرها الميالتونيننقص عام في العناصر الدفاعية ضد األكسدة كما وان رفع الدفاعية الكلية ضد األكسدة بين مرضى الشقيقة بالمقارنة مع األصحاء حدوث
تستنتج الدراسة بأن انخفاض الحالة الدفاعية الكلية ضد األكسدة . جميع المجاميع العالجية دالحالة الدفاعية الكلية ضد األكسدة كان واضحًا عني عالج صداع الشقيقة باستخدام مضادات األكسدة مثل فيتامين هـ يمكن أن يكون عامًال في سببية داء الشقيقة وأن تحسينها قد يكون ذا فائدة ف
.أو الميالتونين مضافًة إلى عالجات داء الشقيقة التقليديةIntroduction
The pathophysiological mechanisms of migraine have been discussed for years to be involving the humoral-vascular and neurogenic theories (1). The constriction of cortical vessels may explain the aura, while dilation of extracortical (meningeal) vessels may underlay the throbbing headache (2). Cerebral hypoxia secondary to vasospasm or platelet aggregation may explain impaired vision predisposing migraine headache (3).Causative factors for cerebral vasospasm could be the alteration in ion concentration (low intracellular Mg+2) (4, 5), abnormally released serotonin secondary to platelets aggregation (6), endothelin receptor gene polymorphism (7), impaired mitochondrial oxidative metabolism and altered nitric oxide synthesis and release (8,9,10). The neurogenic theory is strongly postulated without excluding aspects of the humoral theory (2). The familial nature of migraine is greatly linked to the hereditary abnormality of monoaminergic transmission (11). This transmission is vulnerable to sudden changes in internal or external environment to emotional stress, or to overload of afferent systems by excessive glare, smell or other stimuli. Triggering factors, thus could induce a phase of excessive discharge followed by a state of monoamine depletion, hence pain gates would be opened, giving rise to spontaneous pain in the head and neck (12). Many evidences suggest the involvement of serotonin and norepinephrine to be the monoamines of great interest in the pathophysiology of migraine; the effectiveness of anti-migraine drugs like methysergide , pizotifen (serotonin receptors antagonists) and β-blockers (block the action of norepinephrine) solidify such suggestion (13,14). Beside that, the level of serotonin metabolities (5-hydroxyindolacetic acid) is highly elevated in plasma from patients during acute migraine (2). Change in serotonin level can provoke a neurovascular reaction which involve not only constriction or dilation of cerebral and extracerebral blood vessels but also activate nociceptive trigeminovascular system, an effect enforced by releasing vasoactive neuropeptides
(substance P, neurokinin A or calcitonin gen-related polypeptide) ended with sterile or neurogenic inflammation (15). These events were shown to be blocked by sumatriptan or dihydroergotamine (16,17). Calcium channel blockers on the other hand may diminish vasoconstriction whether produced by humoral agents or by intrinsic monoamine pathways; while non-steroidal anti-inflammatory drugs (NSAIDs) presumably suppress the sterile inflammatory response in vessel walls (18, 19). Many authors believe that sterile inflammation within the trigeminovascular system is of great importance in the pathophysiology of migraine headache. This postulate the release of the neurotransmitter substance P, vasodilation, increased vessel permeability, edema of cranial blood vessels and sensitization of sensory nerve endings (20). Biochemical mediators, like nitric oxide and prostaglandins (PGs) may participate in such scenario; where PGE2 and TXA2 levels are shown to be elevated in saliva from patients with migraine headache during acute attacks (21). Furthermore, nitric oxide has the potential to induce oxidative stress by acting as a free radical through the peroxidation pathway (22). The concept of oxidative stress has been accepted in the increasing association of diseases with advanced age. The plausible explanation for such association is based on the implication of free radicals in the pathogenesis of several disorders like cancer and atherosclerosis (23,24,25).Oxidative stress, however, results from distorted equilibrium of pro-oxidant/anti-oxidant system in intact cell. Such system continuously generates and detoxifies oxidants during normal aerobic metabolism (26). Outbalancing such equilibrium leads to damage of lipids, proteins, carbohydrates and nucleic acids; these events might deplete cellular stores of anti-oxidants material such as glutathione and vitamin E (27). Treatment of acute attacks of migraine is achieved with the use of ergotamine. The effectiveness of ergotamine in treatment of migraine attacks was thought to be related to its α-antagonistic activity; in addition the drug is

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Ergotamine, vitamin E, melatonin and total antioxidants
29
known to stimulate 5-HTD1 receptors of the cerebrovascular system. However; several limitations may restrict the use of ergotamine for migraine patients, these include: pregnancy; sepsis; hypertension; cerebral, coronary and peripheral vascular diseases; hepatitis; and renal insufficiency. In addition, the drug has many side effects such as abdominal cramps, parasthesia, nausea and tightness of the chest (2 ). Melatonin, an endogenous neurohormon, shows a promising effect in relieving migraine headache by means of reducing the severity, frequency and duration of migraine attacks (28). The mechanism by which melatonin exert such effect has yet been proven, but this agent possessing many pharmacological properties like scavenging free radicals (29), inhibiting nitric oxide synthase (30), regulating neurovascular system (31) and modulating serotonin actions (32). In the view of the association of various vascular disorders with oxidative stress (33) and because one of the theories of migraine postulate the change in cerebrovascular milieu, the present study was conducted to investigate the involvement of changed anti-oxidant defense (measured as total antioxidant status) during migraine attack and the possible modulation of such status by classical anti-migraine therapy (ergotamine), antioxidants (vitamin E and melatonin) and their combination.
Materials and Methods Materials:
Ergotamine tartrate (as Cafergot® 1mg tablets, Novartis, Switzerland), Vitamin E (as 400 capsules, Cipla, India), Melatonin (as 3mg tablets, American Nutri-ceutical, USA), Total antioxidant status (TAS) Kit, (Randox Laboratories Ltd, UK).
Patients
Twenty-three normal subjects and 21 migraine patients with age range of (17-45) years were enrolled in this study for three months. For inclusion, patients had to have a long-term history of migraine with and without aura diagnosed according to neurologist decision at specialized neurological centers and were managed under neurologist supervision. Patients who are smokers, alcoholics or those with other apparent disease were excluded. No changes in patients’ medications were made during the study and patients were instructed to keep taking their medications. Migraine patients were divided into three treatment groups; first group
treated with ergotamine (1mg) alone, second group with ergotamine (1mg)/vitamin E (400mg) and third group with ergotamine (1mg)/melatonin (3mg). All groups were advised to take their treatments during attacks. Blood samples were drawn from migraine patients and normal subjects before initiation of therapy and after pain has been relived (from migraine patients only) for the investigation of TAS using Randox TAS kit. Method of measurement was followed according to the instructions mentioned in Randox TAS kit. Data were expressed as mean ± standard deviation and differences between means were analyzed by Student’s t-test. P values less than 0.05 were considered significantly different. Results
Table (1) and figure (1) showed that TAS was significantly lower in migraine patients (P<0.05) in comparison to control (normal subjects) with a percent reduction in TAS was ranged from 35.46% to 43.97%. However, there is no significant difference in the level of TAS among migraine patients (P>0.05). Table (1) clearly showed that ergotamine rise significantly the level of TAS by 157%. Interestingly, the addition of vitamin E and melatonin greatly raised TAS by 179% and 176% respectively. This accompanied by shortening the time required for pain to alleviate. Ergotamine treated group required (6.28 ± 3.77 hr) for the pain to alleviate; while ergotamine/vitamin E and ergotamine/melatonin required (4.84 ± 3.6 hr) and (2.77 ± 1.4 hr) respectively. However; only melatonin showed significant difference (P<0.05) in the time required for the pain to alleviate among other therapies. Although the percent improvement in TAS in patients treated with ergotamine/vitamin E and ergotamine/melatonin appears to be similar, there is a significant difference toward the superiority of vitamin E over melatonin when added to ergotamine. In this regard, it seems that the addition of melatonin did not significantly improve TAS over that produced by ergotamine alone (figure 1).

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Ergotamine, vitamin E, melatonin and total antioxidants
30
Table (1): Effect of treatments of migraine patients with ergotamine and its combination with vitamin E and melatonin on serum TAS.
Serum Total Antioxidant Status (mmol/L)
Control (n=23)
Ergotamine (n=7)
Ergotamine/ Vit E (n=8)
Ergotamine/ Melatonin
(n=6)
Pre-treatment 1.41 ± 0.22 a 0.86 ± 0.15 b 0.91 ± 0.15 b 0.79 ± 0.12 b
Post-treatment
--- 1.35 ± 0.25 * a 1.63 ± 0.09 * b 1.39 ± 0.80 * a
Data are resented as mean ± SD.n= number of patients.*P<0.05 with respect to pre-treatment value. Non-identical superscripts (a,b) among different groups considered significantly different, P<0.05.
Fig. (1): Serum total antioxidant status in control subjects and migraine patients treated with ergotamine (n=7), Ergotamine/Vitamin E (n=8) and Ergotamine/Melatonin (n=6). Data are presented as mean ± SD. *P<0.05 with respect to pre-treatment value (by paired Student’s t-test). Non-identical superscripts (a,b) considered significantly different, P<0.05 (by unpaired Student’s t-test).
Discussion:
Free radicals in the brain and the implication of oxidative damage caused by them have recently being implicated to playing possible role in the pathogenesis of migraine headache. The greater reduction in TAS seen in this study among migraine patients in comparison to control healthy subjects suggests the presence of generalized decrease in antioxidant defense elements. TAS enables assessment of integrated antioxidant system which encompasses all biological components with antioxidant activity. Reduction in TAS has been implicated in several disease stats such as cancer, ischemic heart diseases and poor nutritional stats (34, 35). The most convincing evidence for free radical activity comes from nitric oxide, which is a potent vasodilator and is an important biochemical in the trigeminal-vascular peripheral mechanism of migraine headache (36,37). Infusion of NO donor (glyceryl trinitrate and sodium nitroprusside), immediately induce headache both in healthy subjects and patients suffering from primary headaches with higher intensity in maigiane patients; while slow injection of the nonspecific inhibitor of NO synthase (L-NAM) reduced the spontaneous activity in all neurons (8,38,39). Koulchitsky and coworkers, suggest that NO can induce activation of central trigeminal neurons and that endogenous release of NO may contribute to the ongoing activity of these neurons. The delayed changes in neuronal activity may include gene expression of pro-nociceptive mediators (46). In addition, migraine can be induced via a cGMP-dependent mechanism. Kruuse and coworkers showed that sildenafil significantly induce migraine symptoms and propose that triggering mechanisms may reside within the perivascular sensory nerve terminals or the brainstem (41). NO may interact with other mechanisms for the precipitation of migraine. Strecker and coworkers showed that NO increases meningeal blood flow, an action depends partly on the release and vasodilatory action of calcitonin gene-related peptide (CGRP) from dural afferents; while, prostaglandins show only minimal interaction with NO in this respect (15). Furthermore, platelet levels of nitric oxide, as well as nitric oxide metabolites such as nitrate/nitrite, are increased in migraine patients and rise further during attacks (9,10). Therefore, free radical scavengers may provide a potential
0
0.4
0.8
1.2
1.6
2
2.4
TA
S (m
mol
/L)
Pre-treatment
Post-treatment
Control Ergotamine Ergotamine/Vit E
Ergotamine/Melatonin
**
*
ba
a

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Ergotamine, vitamin E, melatonin and total antioxidants
31
molecular basis for prophylactic antimigraine therapy by neutralizing nitric oxide overproduction and possibly preventing formation of highly toxic peroxynitrite. Interesting results were observed in this study by observing greater elevation of TAS by anti-migraine treatments. In deed, the addition of antioxidants (vitamin E or melatonin) to the traditional treatment (ergotamine) greatly potentiate the effect . Although the present study did not concerned with the mechanism of such an elevation in TAS, it seems that the vasoconstriction effect of ergotamine may involved these events. However, the link between effect of ergotamine and the elevation in TAS is the spotlight for further investigation. Vitamin E is powerful antioxidant that scavenges free radicals within the lipid phase of the cell (42). In addition, it have a structural role in stabilizing membranes (43), thus nowadays, vitamin E is implicated in the therapy of many diseases (44, 45). Melatonin, beside its known antioxidant activity, it was shown to possess the ability to minimize the intensity, frequency and duration of acute migraine attacks (28). In addition, melatonin has many pharmacological effects, of them is the inhibition of nitric oxide synthase (30,46), whether this feature is involved in the relief of migraine headache or in the elevation of TAS this is require further investigation. In our study, melatonin showed no superiority to vitamin E when added to ergotamine with high standard deviation. This may be explained by administration of single rather than maintenance dose of melatonin together with greater fluctuation in plasma melatonin level due to diurnal variation (melatonin plasma level is 10 times higher during night that during the daytime) (47). The age is also an important factor; as we got older the plasma concentration of melatonin decline sharply (48). The present study concluded that the decrease in TAS can be implicated in the pathophysiology of migraine. In addition, enhancement of antioxidant system can add a beneficial effect for the management of migraine headache with the use of antioxidants with classical anti-migraine drug. Acknowledgments The authors grateful Dr. Zuhair Abdul Gafoor (neurologist) and Dr. Ibrahem Adham, Dr. May AL-Sabag, and Dr. Haider Fakhry (Clinical Pharmacist) for their kind help in performing this study. This research is abstracted from High Diploma dissertation submitted to clinical pharmacy department .
References 1. Crowell, G.F. and Carlin, L.I.: Neurologic
complications of migraine. Am. Fam. Physicn. 1982; 26: 139-148.
2. Rang, H.P.; Dale, M.M. and Ritter, J.M.: Clinical conditions in which 5-HT plays a role. In: Pharmacology (4th ed.), Churchill Livingstone, London, 1999, pp. 171-172.
3. Marles, R. J.; Kaminski, J.; Arnason, J. T.; Pazos-Sanou, L.; Heptinstall, S.; Fischer, N. H.; Crompton, C. W.; Kindack, D. G. and Awang, D. V. C.: A bioassay for inhibition of serotonin release from bovine platelets. J. Natural Products. 1992, 55(8): 1044-1056.
4. McCarty, W.: Magnesium taurate and fish oil for prevention of migraine. Medical Hypothesis 1996; 47:461-466.
5. Facchinetti, F.; Sances, G.; Borella, P.; et al.: Magnesium prophylaxis of menstrual migraine: Effects on intracellular magnesium. Headache 1991; 31: 298-301.
6. Weber, J.T.; Oconnor, M.F.; Hayataka, K.; Colson, N.; Medora, R.; Russo, E.B. and Parker, K.K.: Activity of parthenolide at 5-HT (2A) receptors. J. Natural Products 1997; 60(6): 651-653.
7. Tzourio, C.; El Amrani, M.; Poirier, O.; Nicaud, V.; Bousser, M.-G.; and Alperovitch, A.: Association between migraine and endothelin type A receptor (ETA -231 A/G) gene polymorphism. Neurology 2001; 56: 1273-1277.
8. Olesen, J.; Thomsen, L. L.; Lassen, L. H. and Olesen, I. J.: The nitric oxide hypothesis of migraine and other vascular headaches. Cephalalgia 1995; 15: 94-100.
9. Shimomura, T.; Murakami, F.; Kotani, K.; Ikawa, S. and Kono, S.: Platelet nitric oxide metabolites in migraine. Cephalalgia 1999; 19: 218-222.
10. Stepien, A.; Chalimoniuk, M.; Stepien, A. and Chalimoniuk, M.: Level of nitric oxide-dependent cGMP in patients with migraine. Cephalalgia 1998; 18: 631-634.
11. Waeber, C. and Moskowitz, M.A.: Therapeutic implications of central and peripheral neurologic mechanisms in migraine. Neurology. 2003; 61(8 Suppl 4): S9-S20.
12. Van den Bergh,V.; Amery, W.K. and Waelkens, J.: Trigger factors in migraine: a study conducted by the Belgian migraine Society Headache 1987; 27:191-196.
13. Silberstein, S.D.: Evidence-based guidelines for migraine headache. Neurology 2000; 55: 754-762.

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Ergotamine, vitamin E, melatonin and total antioxidants
32
14. Capobianco, D.J.; Cheshire, W.P. and Campbell, J.K.: An overview of the diagnosis and pharmacologic treatment of migraine. Mayo. Clinic. Proceedings. 1996; 71(11): 1055-1066.
15. Strecker, T.; Dux, M. and Messlinger, K.: Increase in meningeal blood flow by nitric oxide - interaction with calcitonin gene-related peptide receptor and prostaglandin synthesis inhibition. Cephalalgia. 2002; 22(3): 233-41.
16. Akpunonu, B.E.; Mutgi, A.B.; Federman, D.J.; et al.: Subcutaneous sumatriptan for treatment of acute migraine in patients admitted to the emergency department: a multicenter study. Ann. Emerg. Med. 1995; 25: 464-469.
17. Becker, W.J.; Riess, C.M. and Hoag, J.: Effectiveness of subcutaneous dihydroergotamine by home injection for migraine. Headache 1996; 36: 144-148.
18. Parantainen, J. and Vapaatalo, H.: Prostaglandins. In: The pathophysiology of migraine. Prostaglandins: Biology and chemistry of prostaglandins and related eicosanoids. Curtis-Prior, B.P. (Ed.), Churchill Livingstone, Edinburgh, 1988; 386-401.
19. Tfelt-Hansen, P. and McEwen, J.: Nonsteroidal anti-inflammatory drugs in the acute treatment of migraine. In: The Headaches (2nd ed.). Olesen, J.; Tfelt- Hansen, P. and Welch, K.M.A. (EDs), Lippincott, Williams and Wilkins, Philadelphia, 2000; 391-397.
20. Moskowitz, M.A.: The neurobiology of vascular head pain. Ann. Neurol. 1984; 16: 157-168.
21. Tuca, J.O.; Planas, J.M. and Parellada, P.P.: Increase in PGE2 and TXA2 in the saliva of common migraine patients. Action of calcium channel blockers. Headache 1989; 29: 498-501.
22. Bagchi, K. and Puri, S.: Free radicals and antioxidants in health and disease. East. Medi. Health J. 1998; 4(2): 350-360.
23. Harman, D.: Role of free radical in aging and disease. Ann. N.Y. Acad. Sci. 1992; 673: 126-141.
24. Lea, A.J.: Dietary factors associated with death rates from certain neoplasms in man. Lancet ; 1966; 2(7458): 332-333.
25. Halliwell, B. and Gutteridge, J.M.C.: Free radicals in biology and medicine (2nd ed.), Oxford, Clarendon press, 1989.
26. Afanas'ev, I.B.: Mechanism of superoxide-mediated damage relevance to mitochondrial aging. Ann. N.Y. Acad. Sci. 2004; 1019: 343-345.
27. Smythies J.: Recent advances in oxidative stress and antioxidants in medicine. J. Orthomolecular Medicine 1998; 13(1): 11-18.
28. Muqdam, M.M.; Salim, A.H. and Ashwaq, N.E.: Clinical evaluation of melatonin alone and in combination with pizotifen in the prophylaxis of migraine. Iraqi J. Pharm. Sci. 2007; 16(1): 1-7.
29. Reiter, R.J.; Calvo, J.R.; Karbownik, M.; Qi, W. and Tan, D.X.: Melatonin and its relation to the immune system and inflammation. Ann. N.Y. Acad. Sci. 2000; 917: 376-386.
30. Bettahi, I.; Pozo, D.; Osuna, C.; Reiter, R.J.; Acuna-Castroviejo, D. and Guerrero, J.M.: Melatonin reduces nitric oxide synthase activity in rat hypothalamus. J. Pineal Res. 1996; 20: 205-210.
31. Savaskan, E.; Olivieri, G.; Brydon, L.; Jockers, R.; Krauchi, K. and Wirz-Justice, A.: Cerebrovascular melatonin MT1-receptor alterations in patients with Alzheimer's disease. Neurosci Lett. 2001; 308: 9-12.
32. Monnet, F.P.: Melatonin modulates [3H] serotonin release in the rat hippocampus: effects of circadian rhythm. J. Neuroendocrinol. 2002; 14: 194-199.
33. Langseth, L.: Antioxidant vitamins and disease prevention. Food Technol. 1994; 7: 80-84.
34. Zachwieja, J.; Bobkowski, W.; Niklas, A.; et al.: Total antioxidant status in children with nephritic syndrome. POI Merkuriusz lek. 2000; 8 (46): 216-7.
35. Car, N.; Vucic, M.; Car, A.; et al.: Superoxide dismutase and total antioxidant status in patient with diabetic ketoacidosis. Diabiologia Croatica. 2000; 29-4:193-196.
36. Silberstein, S.D.; Lipton, R.B. and Goadsby, P.J. (EDs): The pathophysiology of primary headache. In: Headache in Clinical Practice. Oxford, England: Isis Medical Media; 1998; 41-58.
37. Srikiatkhachorn, A.; Suwattanasophon, C.; Ruangpattanatawee, U. and Phansuwan-Pujito, P.: 5-HT2A receptor activation and nitric oxide synthesis: A possible mechanism determining migraine attacks. Headache 2002; 42: 566-574.
38. Iversen, H.K.; Olesen, J.; and Tfelt-Hansen, P.: Intravenous nitroglycerin as an

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Ergotamine, vitamin E, melatonin and total antioxidants
33
experimental model of vascular headache. Basic characteristics. Pain 1989; 38: 17-24.
39. Tassorelli, C.; Joseph, S.A.; Buzzi, M.G. and Nappi, G.: The effects on the central nervous system of nitroglycerin - putative mechanisms and mediators. Prog. Neurobiol. 1999; 57: 607-624.
40. Koulchitsky, S.; Fischer, M.J.M.; De Col, R.; Schlechtweg, P.M. and Messlinger, K.: Biphasic response to nitric oxide of spinal trigeminal neurons with meningeal input in rat – possible implications for the pathophysiology of headaches. Neurophysiol 2004; 92: 1320-1328.
41. Kruuse, C.; Thomsen, L.L.; Birk, S. and Olesen, J.: Migraine can be induced by sildenafil without changes in middle cerebral artery diameter. Brain 2003; 126(1): 241-247.
42. Esterbaner, H.; Dieber-Rotheneder, M.; Striegl, G.; el al.: Role of vitamin E in preventing the oxidation of low-density lipoprotein. Am. J. Clin. Nutr. 1991: 53(suppl 1): 314S-321S.
43. Urano, S.; Inomori, Y.; Sugawara, T.; et al.: Vitamin-E inhibition of retinol-induced hemolysis and membrane-stabilizing behavior. J.Biol. Chem. 1992; 267: 18365-18370.
44. Swann, I.L. and Kendra, J.R.: Anaemia, vitamin E deficiency and failure to thrive in an infant. Clin. Lab. Haematol. 1998; 20(1): 61-63.
45. Sokol, R.I.: Vitamin E deficiency and neurologic disease. Ann. Rev. Nutr. 1988:8:351-73.
46. Leon. J.; Escames, G.; Rodríguez , M.I.; Lopez, L.C.; Tapias, V.; Entrena, A.; Camacho, E.; Carrion, M.D.; Gallo, M.A.; Espinosa, A.; Tan, D.X.; Reiter, R.J. and Acuna-Castroviejo, D.: Inhibition of neuronal nitric oxide synthase activity by N1-acetyl-5-methoxykynuramine, a brain metabolite of melatonin. J. Neurochem. 2006; 98(6): 2023-2033.
47. Takimoto, M.; Hamada, A.; Tomoda, A.; Ohdo, S.; Ohmura, T.; Sakato, H.; Kawatani, J.; Jodoi, T.; Nakagawa, H.; Terazono, H.; Koyanagi, S.; Higuchi, S.; Kimura, M.; Tukikawa, H.; Irie, S.; Saito, H. and Miike, T.: Daily expression of clock genes in whole blood cells in healthy subjects and a patient with circadian rhythm sleep disorder. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005; 289: R1273-R1279.
48. Humbert, W. and Pevet, P.: The decrease of pineal melatonin production with age. Causes and consequences. Ann. N.Y. Acad. Sci. 1994; 719: 43-63.

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Effect of Silibinin on IOP
34
Effect of Silibinin in Lowering the Intraocular Pressure in Normotensive Rabbits: Interaction with Pilocarpine and Cyclopentolate
Saad A. Hussain *,1 , Haider M. Mohammed* , Munaf H. Abdulrazzaq* , Ahmed T. Numan*
*Department of Pharmacology and Toxicology, College of Pharmacy, University of Baghdad , Baghdad , Iraq. Abstract Previous data indicated the effectiveness of silibinin as intraocular pressure (IOP) - lowering agent. The present study was performed to evaluate the interaction of silibinin with pilocarpine or cyclopentolate in lowering IOP in normotensive rabbits. The effects of topically instilled silibinin hemisuccinate solution (0.75%) alone or adjunctly combined with 2% pilocarpine or 1% cyclopentolate on the IOP of normotensive rabbits were evaluated using indentation tonometry. The results showed that 0.75% solution of silibinin was found more potent than pilocarpine (2% drops) in lowering IOP of normotensive rabbits, while their combination results in longer duration of action. Moreover, the elevated IOP values produced by cyclopentolate (1%drops) were decreased by silibinin, while prior instillation of cyclopentolate did not interfere with the IOP-lowering effect of silibinin. In conclusion Silibinin lowers IOP in normotensive rabbits more than pilocarpine, and their combination elongates the duration of the IOP-lowering effect. This might be due to interference with aqueous humor formation as a possible mechanism. In addition, cyclopentolate did not significantly alter the effect of silibinin on IOP. Key words: silibinin, IOP, pilocarpine, cyclopentolate
الخالصةين لقد ثبت في دراسة سابقة فعالية السيليبينين في خفض الضغط الداخلي لعين االرنب٬ تم تصميم هذه الدراسة لتقييم التداخل بين السيليبين
موضعيا في العينوالبايلوكاربين أو السايكلوبنتوليت عند استخدامهم % 0.75تمت دراسة تأثير االستخدام الموضعي في العين لمحلول .سايكلوبنتوليت على خفض الضغط الداخلي لعين االرانب الطبيعية % 1قطرة بايلوكاربين أو % 2سليبينين لوحده أو بوضعه قبل أو بعد
% 2سيليبينين في خفض ضغط العين الداخلي أكبر من % 0.75أظهرت النتائج بأن تأثير . Indentation tonometryباستخدام تقنية بايلوكاربين وأن استخدامهما معا يؤدي الى اطالة مدى مثل هذا التأثير كما ثبت بأن للسيليبينين القدرة على تقليل االرتفاع الحاصل في .
وعليه يمكن . ين عند استخدام االخير قبل السيليبينين٬ بينما لم يرتفع ضغط الع%1ضغط العين الداخلي الذي أحدثته مادة السايكلوبنتوليت ٬ ان نستنتج بأن السيليبينين افضل من البايلوكاربين في خفض ضغط العين الداخلي لعين االرانب وان استخدامهما معا يطيل مدة هذا التأثير
اضافة الى ان الساكلوبنتوليت لم .ية عمل للسيليبينينويمكن أن يعزى هذا التأثير الى التداخل مع عملية تكوين ماء العين الداخلي كميكانيك .يؤثر على فعالية السيليبينين في خفض الضغط الداخلي للعين
Introduction Two mechanisms underlay the effectiveness of various drugs implicated in the management of elevated intraocular pressure (IOP), the reduction in aqueous humor (AH) inflow and enhancement of AH outflow (1). Reduction of aqueous inflow was observed due to the use of ß -adrenoceptor blockers (2), carbonic anhydrase inhibitors (3) and others including Forskolin (4). However, reduction of AH inflow involves either vascular (5, 6) or ionic mechanisms (7). In a recent study, we reported on a decrease in IOP of normotensive rabbits after ocular instillation of silybinin solution (8). It has been suggested that a direct pharmacological effect on trabecular pathway to be likely involved in pilocarpine-induced fall in IOP (9). The role of cAMP in AH regulation is very well explained (10, 11). It inhibits AH inflow by
blocking ion transport across ciliary epithelium (12). Inhibition of Na+-K+ -2Cl¯ by cAMP decreases the uptake of Cl¯ by ciliary epithelium (13), and the increase in cAMP level, stimulated by ß2 -adrenergic receptor activation in the trabecular meshwork cells, suggested to be responsible for the increased outflow facility after application of ß2 -agonists (14). Silibinin hemisuccinate, a powerful antioxidant flavonoid (15), inhibits cAMP-Phosphodiestrase enzyme, even more potent than theophylline or papaverine (16), an effect that can be utilized for the interference with AH formation and IOP regulation. The present study was designed to examine the interaction between silibinin and pilocarpine or cyclopentolate in lowering IOP of normotensive rabbits, and to provide preliminary evidence for the mechanism of this effect.
1 Corresponding author : E-mail : [email protected][email protected] Received : 15/7/2007 Accepted : 30/12/2007
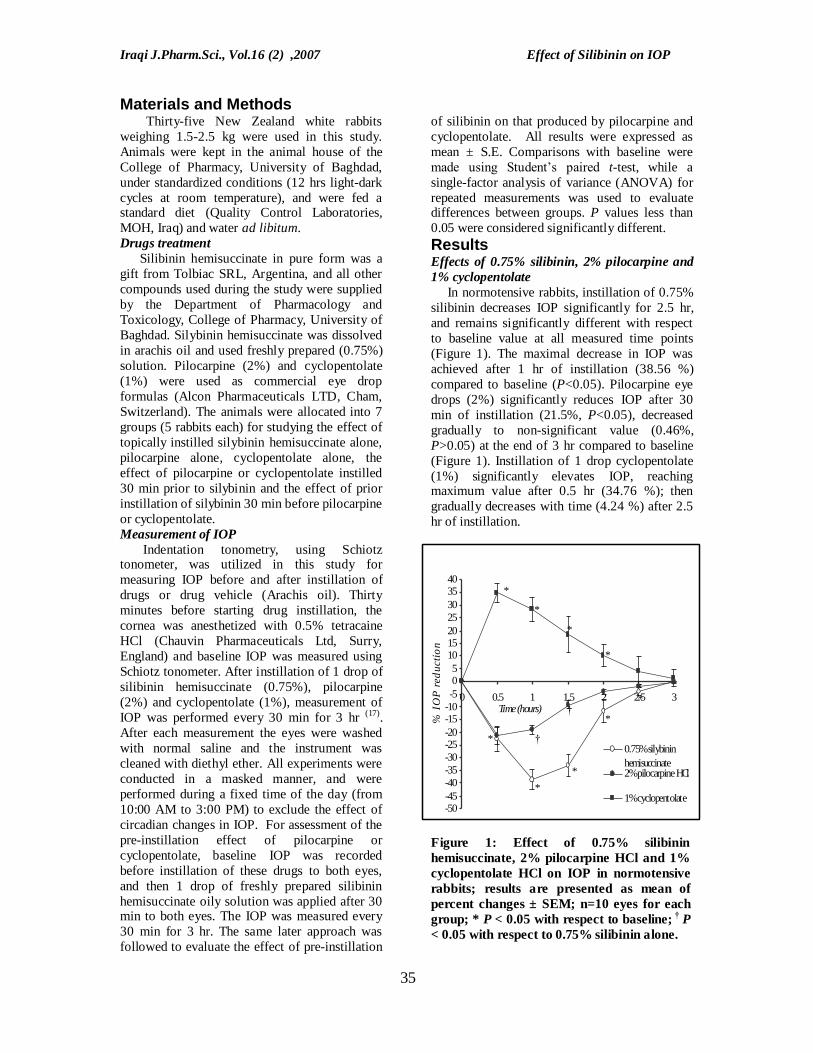
Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Effect of Silibinin on IOP
35
-50-45-40-35-30-25-20-15-10-505
10152025303540
0 0.5 1 1.5 2 2.5 3Time (hours)
% I
OP
red
ucti
on
0.75% silybininhemisuccinate2% pilocarpine HCl
1% cyclopentolate*
*
*
*
*
†
†
*
*
*
*
Materials and Methods Thirty-five New Zealand white rabbits weighing 1.5-2.5 kg were used in this study. Animals were kept in the animal house of the College of Pharmacy, University of Baghdad, under standardized conditions (12 hrs light-dark cycles at room temperature), and were fed a standard diet (Quality Control Laboratories, MOH, Iraq) and water ad libitum. Drugs treatment Silibinin hemisuccinate in pure form was a gift from Tolbiac SRL, Argentina, and all other compounds used during the study were supplied by the Department of Pharmacology and Toxicology, College of Pharmacy, University of Baghdad. Silybinin hemisuccinate was dissolved in arachis oil and used freshly prepared (0.75%) solution. Pilocarpine (2%) and cyclopentolate (1%) were used as commercial eye drop formulas (Alcon Pharmaceuticals LTD, Cham, Switzerland). The animals were allocated into 7 groups (5 rabbits each) for studying the effect of topically instilled silybinin hemisuccinate alone, pilocarpine alone, cyclopentolate alone, the effect of pilocarpine or cyclopentolate instilled 30 min prior to silybinin and the effect of prior instillation of silybinin 30 min before pilocarpine or cyclopentolate. Measurement of IOP Indentation tonometry, using Schiotz tonometer, was utilized in this study for measuring IOP before and after instillation of drugs or drug vehicle (Arachis oil). Thirty minutes before starting drug instillation, the cornea was anesthetized with 0.5% tetracaine HCl (Chauvin Pharmaceuticals Ltd, Surry, England) and baseline IOP was measured using Schiotz tonometer. After instillation of 1 drop of silibinin hemisuccinate (0.75%), pilocarpine (2%) and cyclopentolate (1%), measurement of IOP was performed every 30 min for 3 hr (17). After each measurement the eyes were washed with normal saline and the instrument was cleaned with diethyl ether. All experiments were conducted in a masked manner, and were performed during a fixed time of the day (from 10:00 AM to 3:00 PM) to exclude the effect of circadian changes in IOP. For assessment of the pre-instillation effect of pilocarpine or cyclopentolate, baseline IOP was recorded before instillation of these drugs to both eyes, and then 1 drop of freshly prepared silibinin hemisuccinate oily solution was applied after 30 min to both eyes. The IOP was measured every 30 min for 3 hr. The same later approach was followed to evaluate the effect of pre-instillation
of silibinin on that produced by pilocarpine and cyclopentolate. All results were expressed as mean ± S.E. Comparisons with baseline were made using Student’s paired t-test, while a single-factor analysis of variance (ANOVA) for repeated measurements was used to evaluate differences between groups. P values less than 0.05 were considered significantly different. Results Effects of 0.75% silibinin, 2% pilocarpine and 1% cyclopentolate In normotensive rabbits, instillation of 0.75% silibinin decreases IOP significantly for 2.5 hr, and remains significantly different with respect to baseline value at all measured time points (Figure 1). The maximal decrease in IOP was achieved after 1 hr of instillation (38.56 %) compared to baseline (P<0.05). Pilocarpine eye drops (2%) significantly reduces IOP after 30 min of instillation (21.5%, P<0.05), decreased gradually to non-significant value (0.46%, P>0.05) at the end of 3 hr compared to baseline (Figure 1). Instillation of 1 drop cyclopentolate (1%) significantly elevates IOP, reaching maximum value after 0.5 hr (34.76 %); then gradually decreases with time (4.24 %) after 2.5 hr of instillation. Figure 1: Effect of 0.75% silibinin hemisuccinate, 2% pilocarpine HCl and 1% cyclopentolate HCl on IOP in normotensive rabbits; results are presented as mean of percent changes ± SEM; n=10 eyes for each group; * P < 0.05 with respect to baseline; † P < 0.05 with respect to 0.75% silibinin alone.

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Effect of Silibinin on IOP
36
Effects of pre-treatment with 2% pilocarpine and 1% cyclopentolate The IOP-lowering effect of pilocarpine was enhanced when silibinin instilled 30 min latter, 26.87% compared to 19.0% produced by pilocarpine alone (P<0.05). The reduction in IOP observed in this procedure remains significantly high (40.88%, 49.5%, 43.34%, and 26.87%) compared to that produced by pilocarpine alone (9.23%,4.16%,1.81% and 0.46%) for the time intervals 1.0, 1.5, 2.0, and 2.5 hr respectively (P<0.05) (Figure 2). Moreover, this level reduction in IOP was significantly different compared to that produced by silibinin alone along the entire period beyond the addition of silibinin. When cyclopentolate instilled 30 min prior to silibinin, the latter still have the ability to reverse the elevation of IOP produced by cyclopentolate (from 34.76% to 17.3%) after 30 min of instillation (P<0.05); these changes are not significantly different at the time intervals 1.0, 1.5, and 2.0 hr after instillation of silibinin, P>0.05 (Figure 3). Figure 2: Effect of pre- and post treatment with 0.75% silibinin hemisuccinate on IOP lowering effect of 2% pilocarpine in normotensive rabbits; results are presented as mean of percent changes ± SEM; n=10 eyes for each group; * P < 0.05 with respect to baseline; † P < 0.05 with respect to 2% pilocarpine alone.
Figure 3: Effect of pre- and post treatment with 0.75% silibinin hemisuccinate on IOP rising effect of 1% cyclopentolate in normotensive rabbits; results are presented as mean of percent changes ± SEM. n=10 eyes for each group; * P < 0.05 with respect to baseline; † P < 0.05 with respect to 1% cyclopentolate alone; Pre-treatment with silibinin hemisuccinate did not significantly differ from silibinin hemisuccinate alone P > 0.05. Effects of pre-treatment with silibinin Pre-treatment with silibinin, 30 min before instillation of pilocarpine resulted in additive effect on the IOP lowering activity of pilocarpine (37.5%), which was significantly different, compared to the effect of pilocarpine alone (21.5%). This reduction in IOP remains significantly different with respect to that produced by pilocarpine after 1.0, 1.5 and 2.0 hr. However, the effect of pre-treatment with silibinin did not significantly differ compared to that produced by silybinin alone during all time intervals (P>0.05) (Figure 1). Even when cyclopentolate instilled 30 minutes latter, pre-treatment with silibinin results in highly significant reduction in IOP (31.47% P<0.05), and remains significantly high 1.0, 1.5, and 2.0 hr after instillation of cyclopentolate (-20.08%, -8.92%, -4.12% respectively) compared with the rise in IOP (28.36%, 18.29%, 10.18% and
-50
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
0.5 1 1.5 2 2.5 3Time (hour)
% I
OP
red
uctio
n
2% pilocarpine alonePre-treatment with 0.75% silybinin hemisuccinatepost-treatment with 0.75% silybinin hemisuccinate
**
*
*
*
**
*
*
* *
*
**
†
†
†
†
†
†
†
†
†
-45
-35
-25
-15
-5
5
15
25
35
0.5 1 1.5 2 2.5 3Time (hour)
% C
han
ge i
n IO
P
1% cyclopentolate alone
Post-treatment with 0.75% silybinin hemisuccinate
Pre-treatment with 0.75% silybinin hemisuccinate
0.75% silybinin hemisuccinate alone
**
*
*
*
*
**
*
*
*
*
*
†
†
†
†
†

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Effect of Silibinin on IOP
37
10.18%) produced by cyclopentolate alone (P<0.05). Cyclopentolate appeared to slightly reverse the action of silibinin when instilled 30 min latter; however, such effect did not significantly differ from that produced by silibinin alone (P>0.05). Discussion It has been reported previously in our laboratory that corneal instillation of silibinin lowers IOP in normotensive rabbits in a dose dependent manner. It also delays IOP recovery rate after I.V infusion of 20% sodium chloride solution (8). Although inhibition of cAMP-phosphodiesterase is proposed as a suspected mechanism for the action of silybinin on IOP (18), interference with the cholinergic influence in this respect was evaluated. In the present study, the effect of silibinin on IOP was higher than that produced by pilocarpine, and their combination results in an additive effect. Muscarinic agonists, including pilocarpine, lower IOP through enhancing AH outflow due to contraction of the iris sphincter (19). According to the reported mechanisms of action of silibinin, targeting AH formation and interference with ion transport can be suggested as possible mechanisms (20). Consequently, the mechanisms through which pilocarpine and silibinin produce their effects can be utilized for explaining the additive effect reported when both of them are used at the same time. To confirm the idea that silibinin lowers IOP through a mechanism not related to the cholinergic system, the interaction of silibinin with anticholinergic agent like cyclopentolate was evaluated. Although there is no practical evidence on elevation of IOP in rabbits due to instillation of cyclopentolate, the results reported in this study demonstrated such effect, which can be attributed to the abnormal sensitivity of the locally bred strain of rabbits to the effect of cyclopentolate. In the present work, the rise in IOP produced by instillation of cyclopentolate was effectively reversed by silibinin; meanwhile, the IOP lowering effect of silibinin was not affected by postinstillation of cyclopentolate. Based on these data, one can postulate that silibinin interferes with IOP regulation through reduction of AH inflow. Taken together with the data obtained in previous study (8) about the effect of silibinin on IOP recovery rate and its contralateral effect, one can suggest the interference with AH inflow as a mechanism involved in pilocarpine-silibinin and cyclopentolate-silibinin interactions. The IOP-lowering effect of cholinomimetics is mediated via the activation of the inositol triphosphate
(IP3) pathway that linked to M3-receptors in the ciliary and iris-sphincter muscles (21). Silibinin, on the other hand, strongly inhibits cAMP phosphodiesterase with consequent elevation of cAMP levels (16). The later mediates many biological effects including the inhibition of ion transport by Na+-K+- 2Cl– co-transporter across ciliary epithelium and trabecular meshwork (13,
22), which is similar to that produced by activation of the IP3 pathway initiated by pilocarpine. Regulation of cell volume is very important phenomenon that involved during exposure to hypo- or hypertonic environment, and Na+ - K+- 2Cl – co-transporter is the system responsible for such regulation (23, 7, 24). Infusion of hypertonic sodium chloride solution resulted in shrinkage of ciliary epithelium, and to retain the original volume, ion transporters should be activated to transport Na+ and Cl– across ciliary epithelium (25). Inhibition of this co-transporter by cAMP delayed osmotic recovery rate, an effect reported after silibinin administration. In conclusion, corneal instillation of silibinin lowers IOP in normotensive rabbits, probably through a mechanism not related to the interference with cholinergic influence on IOP. Acknowledgment The authors gratefully thank College of Pharmacy, University of Baghdad for supporting the project and Tolbiac SRL, Argentina for providing pure silibinin powder as a gift. References 1. Moses R A. Intraocular pressure. Moses
RA, Hart W. (eds.), Adler’s Physiology of the Eye. Clinical application, 8th edition, The C.V. Mosby, Santa Louis, 1987; 223.
2. Robinson JC, Kaufman PL. Dose-dependent suppression of aqueous humor formation by timolol in the cynomolgus monkey. J Glaucoma 1993; 2: 251.
3. Shahidullah M, William M, Wilson S, et al. Effects of ion transport and channel-blocking drugs on aqueous humor formation in isolated bovine eye. Invest Ophthalmol Vis Sci 2003; 44: 1185-1191.
4. Caprioli J, Sears M, Bausher L. Forskolin lowers intraocular pressure by reducing aqueous inflow. Invest Ophthalmol Vis Sci 1984; 25: 268.
5. Bill A, Stjernschantz J. Cholinergic vasoconstrictor effects in the rabbit eye: Vasomotor effects of pentobarbital anesthesia. Acta Physiol Scand 1980; 108: 419.

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 Effect of Silibinin on IOP
38
6. Millar JC, Carr RD, Humphries RG, et al. Drug effects on intraocular pressure and vascular flow in the bovine perfused eye using radiolabeled microspheres. J Ocul Pharmacol Ther 1995; 11: 11.
7. Do CW, To CH. Chloride secretion by bovine ciliary epithelium: a model of aqueous humor formation. Invest Ophthalmol Vis Sci 2000; 41: 1853-1860.
8. Mohammed HM, Abdulrazzaq MH, Hussain SA. Effects of silibinin hemisuccinate on the intraocular pressure in normotensive rabbits. Saudi Med J 2007, 28(9): 1397-1401
9. Erickson KE, Schroeder A. Direct effects of muscarinic agents on the outflow pathways in human eyes. Invest Ophthalmol Vis Sci 2000; 41: 1743-1748.
10. Do CW, Kong CW, To CH. cAMP inhibits transepithelial chloride secretion across bovine ciliary body epithelium. Invest Ophthalmol Vis Sci 2004; 45: 3638-3643.
11. Stamer WD, Roberts BC, Epstein DL. Hydraulic pressure stimulates adenosine 3΄, 5΄-cyclic monophosphate accumulation in endothelial cells from Schlemm’s canal. Invest Ophthalmol Vis Sci 1999; 40(9): 1983-1988.
12. Neufeld AH, Sears ML. Cyclic-AMP in ocular tissues of the rabbit, monkey, and human. Invest Ophthalmol Vis Sci 1974; 13: 475.
13. Crook RB, Takahashi K, Mead A, et al. The role of Na-K-2Cl cotransport in blood-to-aqueous chloride fluxes across rabbit ciliary epithelium. Invest Ophthalmol Vis Sci 2000; 41: 2574-2583.
14. Lu Y, Li M, Shen Y. The effects of epinephrine and adrenergic antagonists on adenosine 3΄, 5΄- monophosphate level of bovine trabecular cells in vitro. Zhonghua Yan Ke Za Zhi 1998; 34 (2): 124-126.
15. Altorjay I, Dalmi L, Sari B, et al. The effect of silibinin (Legalon) on the free radical scavenger mechanisms of human erythrocytes in vitro. Acta Physiol Hung 1992; 80: 375-380.
16. Koch HP, Bachner J, Loffler E. Silymarin: potent inhibitor of cyclic AMP
phosphodiesterase. Methods Find Exp Clin Pharmacol 1985; 7(8): 409-413.
17. Vareilles P, Lotti VJ. Effects of timolol on aqueous humor dynamics in the rabbit. Ophthalmol Res 1981; 13: 72-79.
18. Berets A, Anton R, Cazenave JP. The effects of flavonoids on cyclonucleotide phosphodiesterase, Cody V, Middleton E, Harborne JB. (Eds.), Plant Flavonoids in Biology and Medicine: Biochemical, Pharmacological and structure-activity relationships. Alan R. Liss Inc. New York, 1986; 281-296.
19. Wiederholt M, Bielka S, Schweig F, Lütjen-Drecoll E. Regulation of outflow rate and resistance in the perfused anterior segment of the bovine eye. Exp Eye Res 1995; 61: 223.
20. Ruckstuhl M, Landry Y. Inhibition of lung cAMP- and cGMP- phosphodiesterases by flavonoids and other chromone-like compounds. Biochem Pharmacol 1981; 30: 697-702.
21. Berridge M. Inositol triphosphate and calcium signaling. Nature 1993; 361: 315-325.
22. O'Donnell ME, Martinez A, Sun D. Endothelial Na-K-Cl cotransport regulation by tonicity and hormones: Phosphorylation of cotransport protein. Am J Physiol Cell Physiol 1995; 269: 1513-1523.
23. Civan MM, Peterson-Yantorno K, Sanchez-Torres J, Coca-Prados M. Potential contribution of epithelial Na+ channel to net secretion of aqueous humor. J Exp Zool 1997; 279: 498-503.
24. Crook RB, Von Brauchitsch DK, Polansky JR. Potassium transport in non-pigmented epithelial cells of ocular ciliary body: inhibition of a Na+, K+, Cl- cotransporter by protein kinase C. J Cell Physiol 1992; 153: 214-220.
25. Civan M.M, Coca-Prados M, Peterson-Yantorno K. Pathways signaling the regulatory volume decrease of cultured nonpigmented ciliary epithelial cells. Invest Ophthalmol Vis Sci 1994; 35: 2876-2886.

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 IOP-lowering effect of silibinin
39
Effect of Silibinin in Lowering the Intraocular Pressure in Normotensive Rabbits: Interaction with Betaxolol
Saad A. Hussain *,1 , Haider M. Mohammed* , Ahmed H. Jwaied * , Munaf H. Abdulrazzaq*
*Department of Pharmacology and Toxicology, College of Pharmacy, University of Baghdad , Baghdad , Iraq. Abstract Previous reports demonstrated the effectiveness of silibinin hemisuccinate as a potential intraocular pressure-lowering agent. The exact mechanism by which silibinin exerted this effect has not yet been documented, but might suggested to interfere with aqueous humor formation. The present study was designed to evaluate the comparative efficacy of silibinin as IOP lowering agent to that of betaxolol in normotensive rabbits, and the interaction of silibinin with betaxolol as a way for investigating the possible mechanism of action of silibinin in this respect. The effects of instillation of 0.75% silibinin solution and 0.5% betaxolol eye drops in the eyes of normotensive rabbits were evaluated using indentation tonometry. The results showed that 0.75% solution of silibinin was more potent than betaxolol (0.5%) in lowering IOP in normotensive rabbits. Furthermore, the effect of pre- and post-instillation of silibinin-betaxolol combination showed a characteristic antagonistic feature. In conclusion, silibinin appears to be more potent than betaxolol in lowering IOP in normotensive rabbits; the pre- and post-instillation of silibinin provide experimental evidence for the possible antagonistic effect of betaxolol with the IOP-lowering effect of silibinin. Key words: silibinin, betaxolol, cAMP, PDE-inhibitors
الخالصةمن ثبت من دراسة سابقة فعالية مادة السيليبينين في خفض الضغط الداخلي للعين٬ اال ان ميكانيكية مثل هذا التأثير لم تعرف بعد على الرغم
ل تداخلها مع تكوين السائل الداخلي للعيناحتما تم تصميم هذه الدراسة لمقارنة فعالية السيليبينين في خفض الضغط الداخلي للعين مقارنة .بمادة البيتاكسولول في االرانب٬ وكذلك دراسة التداخل بين البيتاكسولول والسيليبينين عند استخدامهما معا كوسيلة لتكوين فكرة حول
بيتاكسولول قطرات في عيون أرانب % 0.5سيليبينين و % 0.75تمت دراسة تأثير االستخدام الموضعي لمحلول . عمل السيليبينين ميكانيكيةأظهرت النتائج فعالية السيليبينين في خفض الضغط الداخلي . indentation tonometryبيضاء ذات ضغط داخلي طبيعي باستخدام تقنية
. ذي يحدثه البيتاكسولول٬ كما ان استخدام السيليبينين قبل وبعد البيتاكسولول اظهر تضادا واضحا في التأثيرللعين بشكل افضل من ذلك الخل يمكن االستنتاج بأن االستخدام الموضعي للسيليبينين في العين يؤدي الى خفض الضغط الداخلي للعين اكثر من البيتاكسولول٬ كما ان التدا
.ان يعطي فكرة أولية عن ميكانيكية عمل هذا المركب السلبي مع البيتاكسولول يمكن Introduction Although glaucoma is no longer defined as elevated intraocular pressure (IOP) but rather a condition comprises characteristic optic nerve head and visual filed abnormalities (1), lowering IOP is still the major strategy in slowing down glaucomatous damage to the inner structures of the eye and visual filed (2). All current treatment strategies are designed to reduce IOP by reducing the rate of aqueous humor (AH) formation and/or enhance its drainage out of the eye(3). The ciliary epithelium has α2- and 2-adrenergic receptors. Stimulation of α-receptors or inhibition of 2-receptors was thought to reduce AH formation (4). Topical instillation of epinephrine decreases the rate of AH formation, an effect thought to be mediated by -receptor induced increase in cAMP in the ciliary epithelium (5). The participation of cAMP in this effect has been supported by
finding that activators of adenylcyclase (cholera toxin and forskolin) decrease AH formation and hence IOP in experimental animals and human (6). Targeting of this Cl- transport system is thought to be the newer proposed mechanism for the lowering of IOP by the oldest antiglaucomatus drug, Timolol(7). These findings support the major involvement of increased rather than decreased cAMP as a second messenger mechanism in the control of AH formation in normal physiology, as well as in pathological conditions. Interestingly, the action of -blockers in the reduction of AH formation is now suggested to involve cAMP-independent mechanism (7). Furthermore, timolol was shown to reduce epinephrine-induced increase in uveoscleral outflow when the two drugs applied concurrently(8). Inhibition of phosphodiesterase (PDE) by flavonoids has been previously described(9,10);silib
1 Corresponding author : E-mail : [email protected][email protected] Received : 15/7/2007Accepted : 30/12/2007

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 IOP-lowering effect of silibinin
40
powerful antioxidant flavonoid (11) has been shown to reduce IOP in normotensive rabbits when used alone in different concentrations, with greater effect achieved with 0.75% dose(12). The site of action did not exactly pointed but the drug shown to delay IOP recovery rate after i.v. infusion of 20% NaCl solution. This largely suggests an interference with AH inflow mechanism. Interestingly, silybinin was shown to inhibit cAMP-phosphodiesterase enzyme more potent than theophylline or papaverine (13). This study was conducted to evaluate the possible interaction of silibinin with the IOP-lowering effect of the -adrenergic blocker betaxolol in normotensive rabbits. Materials and Methods Twenty New Zealand white rabbits weighing 1.5-2.5 kg were used in this study, and treated according to the ethics of animal experiments approved by the University of Baghdad. Animals were kept in the animal house of the College of Pharmacy, University of Baghdad, under standardized conditions (12 hrs light-dark cycles at room temperature), and were fed standard diet and given water ad libitum. Silibinin hemisuccinate in pure form was a gift from Tolbiac S.R.L. (Argentina) and all other chemicals were supplied by the Department of Pharmacology and Toxicology, College of Pharmacy, University of Baghdad. Silibinin hemisuccinate was dissolved in arachis oil (as a vehicle) and used as freshly prepared (0.75%) solution. Betaxolol 0.5% drops (Alcon, Cham, Switzerland) were used as commercial eye drop formula. Rabbits were allocated into four groups (5 animals each) for studying the effect of topically instilled silibinin hemisuccinate, betaxolol, the effect of topical silibinin instilled 30 min prior to betaxolol, and the effect of topical betaxolol instilled 30 min prior to instillation of silibinin . Measurement of IOP: Indentation tonometry using Schiotz tonometer was utilized in this study for measuring IOP before and after application of drugs or vehicle. Thirty min before starting any application, the cornea was anesthetized with 0.5% tetracaine, and baseline IOP was measured using Schiotz tonometer. After topical instillation of 1 drop of silibinin (0.75%) and betaxolol (0.5%), measurement of IOP was performed every 30 min for 3 hr (14). After each measurement, eyes were washed with normal saline and the instrument was cleaned with diethyl ether. All experiments were conducted by trained subject who is completely unaware about the type of treatment followed, and performed during a fixed time of the day (from 10:00 AM to 3:00
PM) to exclude the effect of circadian changes in IOP.For studying the pre-instillation effect of betaxolol, baseline IOP was recorded after the instillation of betaxolol, and then one drop of silibinin solution was instilled after 30 min into both eyes. IOP was measured every 30 min for 3 hr. The same later approach was followed to evaluate the effect of pre-instillation of silibinin on that produced by betaxolol. Results were presented as a mean value of IOP SD. Comparisons with baseline were made using Student’s paired t-test, while a single-factor analysis of variance (ANOVA) was used to test the statistical differences between groups. P values less than 0.05 were considered significant. Results Effects of 0.75% silibinin and 1% betaxolol: In normotensive rabbits, ocular instillation of 0.75% silibinin decreases IOP for 2.5 hr compared to baseline value and remains significantly different at all measured time points (Table1). The maximum decrease in IOP was achieved after 1 hr of instillation of silibinin (38.56%) compared to baseline value (P<0.05). Application of 1 drop betaxolol (0.5%) eye drop resulted in significant decrease in IOP, with maximum reduction achieved after 1hr (22.08%); then decreased with time and became (2.05%) after 3.0 hr, which found non-significantly different compared to baseline (Table1). Effects of pre-treatment with 0.75% silibinin Corneal instillation of 0.5% betaxolol eye drops produced highly significant reduction in IOP when preceded (30 min) by instillation of 0.75% silibinin (38.35%-3.9%, P<0.05) compared to the effect produced by betaxolol alone (22.08%-6.61%, P<0.05) (Table 1, Figure 1). The higher magnitude of reduction in IOP was achieved during the first 30 min of instillation of 0.5% betaxolol to silibinin-pretreated eyes (38.35%, P<0.05) compared to 10.78% produced by betaxolol alone. The reduction in IOP continued to be significantly high during the next 30 min interval (27.76%, P<0.05) compared to 22.08% produced by 0.5% betaxolol alone. However, the reduction in IOP after this period seems to be non-significant (17.71%, 10.52%, 3.94%, P>0.05) compared to 19.49%, 20.87% and 6.61% produced by 0.5% betaxolol alone at the intervals 1.5, 2.0 and 2.5 hr (P>0.05). The reduction in IOP was significantly different from that produced by 0.75% silibinin alone for the intervals 0.5, 1.0 and 1.5 hr (P<0.05), while found non-significant for the rest of time (P>0.05) (Table, Figure 1).

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 IOP-lowering effect of silibinin
41
Effects post-treatment with silibinin The results presented in table 1 and figure 1 showed that the ocular hypotensive effect of 0.5% betaxolol was slightly changed following the addition of silibinin, and during the first 30 min of application, 0.75% silibinin resulted in
13.61% reduction in IOP compared to 22.08% produced by betaxolol alone (P>0.05). Although the IOP was reduced following the next 30 min (26.52%), it was found comparable to that produced by betaxolol alone (P>0.05).
Table 1. Effects of instillation of silibinin 0.75% and betaxolol 0.5% on the intraocular pressure
(IOP) in normotensive rabbits.
Intraocular Pressure (mmHg) Group Baseline 0.5hr 1.0 hr 1.5 hr 2.0 hr 2.5 hr 3.0 hr
Silibinin 0.75% 28.6 ± 1.9 22.1 ± 0.6* a 17.5 ± 2.8* a 19.1 ± 3.7*
a 25.3 ± 4.0* a 27.5 ± 2.9* a
28.6 ± 1.9 a
Betaxolol 0.5% 31.5 ± 2.3 28.1 ± 3.1* b 24.5 ± 3.9*
b 25.4 ± 3.1* b 24.9 ± 2.3* a 29.4 ± 2.4*
a
30.8 ± 2.0 a
Silibinin pre-treatment
31.7 ± 2.5 24.6 ± 2.2*
c 19.7 ± 2.3* a 22.9 ± 2.7*
a 26.1 ± 2.2* a 28.4 ± 2.5* a 30.5 ± 2.4
a
Silibinin post-treatment
31.7 ± 2.8 28.1 ± 3.4*
b 27.2 ± 3.6* b 23.1 ± 2.6*
b 24.7 ± 3.1* a 29.2 ± 2.6* a 31.5 ± 2.7
a
Values are expressed as mean ± SD; number of eyes in each group = 10; * P< 0.05 with respect to baseline value; values with non-identical superscripts (a,b,c) among different groups are considered significantly different (p<0.05).
Figure 1. Effects of pre- and post- treatment with 0.75% silibinin hemisuccinate on IOP-lowering effect of 0.5% betaxolol in normotensive rabbits; results are presented as mean of % reduction; number of eyes in each group = 10; *P<0.05 with respect to 0.75% silibinin hemisuccinate alone.
-45
-40
-35
-30
-25
-20
-15
-10
-5
00.5 1 1.5 2 2.5 3
Time (hours)
% IO
P re
duct
ion
0.75% Silibinin hemisuccinate 0.5% Betaxolol HCl Pre-treatment with silibinin hemisuccinate Post-treatment with silibinin hemisuccinate
*
*

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 IOP-lowering effect of silibinin
42
Discussion In the present study, topical instillation of
silybinin was shown to strongly lower IOP in normotensive rabbits, an effect that appears significantly greater than that produced by 0.5% betaxolol (Table1). Betaxolol binds to β-adrenergic receptors of the ciliary processes with high affinity (15). Since agonists to all β-adrenergic receptors (β1, β2, and β3) stimulate adenylcyclase via interaction with Gs-protein to increase cAMP production, betaxolol was thought to lower IOP by reducing the intracellular concentrations of cAMP (16). However, it has long been unclear whether the putative reduction in cAMP itself causes the reduction in IOP, an observation reported by Liu et al (1981) who demonstrated that D-timolol, another β-blocker might be as effective as L-timolol in decreasing aqueous flow (17), despite stereospecificity of the β-adrenergic receptors for the L-isomers (18). Meanwhile, if betaxolol reduces aqueous humor formation by blocking β-adrenergic-mediated increase of cAMP production, one would expect cAMP itself to increase inflow. However, cAMP certainly does not markedly increase aqueous inflow. Accordingly, Caprioli et al (1984) reported a decrease in inflow following administration of forskolin, which stimulates endogenous production of cAMP (6). However, the foregoing considerations do not preclude the possibility that betaxolol reduces secretion of aqueous humor exclusively through its action as a nonselective β-adrenergic antagonist, but have raised doubts about that hypothesis. A conflicting result have recently been reported by McLaughlin et al (2001) who demonstrated that application of cAMP did not reverse timolol’s effects; and that timolol and levobunolol produced cAMP-independent inhibition of the regulatory volume increase (RVI) in ciliary cells and increased intracellular Ca2+ and pH; they suggested that inhibition of Cl-/HCO3
- exchange mediates timolol’s inhibition of aqueous humor formation as an alternative mechanism for the reduction of aqueous inflow and then IOP (7). The IOP lowering effect of silibinin is thought to occur via reduction of AH formation, and the site of action has been postulated to be the ciliary epithelium; this is based on previous data reported in our laboratory that revealed delayed recovery time following intravenous infusion of 20% NaCl and a profound contralateral effect on untreated eyes (12). The present study demonstrated that when compared with betaxolol, silibinin was found more effective in
lowering IOP. It appears that neither pre- nor post-instillation of each one of
them improves significantly the IOP-lowering effect produced by any one of them alone. Pre-instillation effect of silibinin appears to completely abolish that of betaxolol; however, the higher magnitude of reduction in IOP already produced by pre-instillation of silibinin (figure 1) might be due to the action of silibinin alone. These effects are very interesting in that the potent action of silibinin might mask that of betaxolol especially when given 30 min before, and this might explain the predominance of silibinin action over that of betaxolol (Figure 1). However, silibinin did not augment the effect of betaxolol when administered latter suggesting interference with its action by previous instillation of betaxolol. This conclusion can be accepted pharmacodynamically since -blockers are known to initiate a decrease in cAMP levels required for the action silibinin (as PDE-inhibitor) and the only effect shown in figure 1 might be attributed to betaxolol alone.The mechanism through which betaxolol reduced IOP is now difficult to correlate with its inhibitory effect on cAMP. Isoproterenol, which stimulate cAMP production, has been reported to increase aqueous humor inflow (19). In contrast, forskolin, which also stimulate cAMP formation, has been found to reduce inflow (20), and isoproterenol itself has reported to reduce IOP in water-loaded rabbits (21). Since silibinin has been proved to inhibit PDE (9) and to produce higher magnitude of reduction in IOP (37.84%) compared to that of betaxolol (22.0%), one could suggest that increasing intracellular cAMP could be the major event through which silibinin reduces IOP. Involvement of cAMP as a target in the events of lowering IOP was clear in many studies that involve application of forskolin (an adenylcyclase activator) via either topical or systemic route (22). Forskolin reduced net aqueous humor inflow in rabbits, and increased ciliary blood flow through activation of adenylcyclase in ciliary epithelium; this action was not blocked by timolol (6). This is quite important to explain why betaxolol blocks the effect of silibinin (a PDE-inhibitor). β-blockers did not block the action of forskolin because the latter was still capable to stimulate synthesis of cAMP, while silibinin requires the presence of already synthesized cAMP to elongate its half-life. For this reason blockade of cAMP synthesis by betaxolol diminish the activity of silibinin. Cyclic AMP was found to

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 IOP-lowering effect of silibinin
43
inhibit transepithelial Cl- secretion across bovine ciliary epithelium by uncoupling the intracellular gap junction (23) and to inhibit other important regulator of aqueous humor dynamics, the Na+-K+-2Cl- cotransporter (24). Inhibition of this cotransporter has found to be associated with higher degree of reduction in IOP. Interestingly, this profile of activity is similar to that produced by 0.75% silybinin (38.5%) in the present study. Although the effect of silibinin on the ocular phosphodiesterase (PDE) has not been studied, a study on beef heart PDE revealed that silibinin was more potent as PDE-inhibitor than theophylline and papaverine in this regard (13). From these findings one can suggest that the strong ocular hypotensive effect produced by silibinin might be attributed to the inhibition of PDE, and the resultant accumulation of cAMP inhibits Na+-K+-2Cl- cotransporter in ciliary epithelium as well as in trabecular meshwork cells. Both effects on inflow and outflow of aqueous humor dynamics could be the possible mechanisms through which silibinin produces this effect, and became a new drug candidate for the reduction of elevated IOP.In conclusion, the results obtained in this study provide experimental evidence that silibinin is more potent in reducing IOP than betaxolol through a mechanism that might be related to increase cAMP levels. Acknowledgment The authors thank the college of Pharmacy, University of Baghdad for supporting the project, and Tolbiac SRL, Argentina for providing pure standardized silibinin hemisuccinate as a gift. References 1. Anderson DR. Glaucoma: The damage
caused by pressure. Am J Ophthalmol 1989; 108: 485.
2. Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Komaroff E. Early Manifest Glaucoma Trial Group: Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol 2003; 121: 48-56.
3. Moses R A. Intraocular pressure. In: Moses RA, Hart W. (Eds.), Adler’s Physiology of the Eye: Clinical application, 8th edition, The C.V. Mosby, Santa Louis, 1987; 22.
4. Andrew S, Titcomb L. Glaucoma In: Walker R, Edwards C.(Eds), Clinical Pharmacy and Therapeutics, (2nd
ed.),Churchill Livingstone, London. 1999; 807-821.
5. Neufeld AH, Sears ML. Cyclic-AMP in ocular tissues of the rabbit, monkey, and human. Invest Ophthalmol Vis Sci 1974; 13: 475.
6. Caprioli J, Sears M, Bausher L. Forskolin lowers intraocular pressure by reducing aqueous inflow. Invest Ophthalmol Vis Sci 1984; 25: 268.
7. McLaughlin WC, Peart D, Purves DR, Carre AD, Peterson-Yantorno K, Mitchell HC, et al. Timolol may inhibit aqueous humor secretion by cAMP-independent action on ciliary epithelial cells. Am J Physiol Cell Physiol 2001; 281: 865-875.
8. Schenker JI, Yablonski ME, Podos SM, Linder L. Fluorophotometric study of epinephrine and timolol in human subjects. Arch Ophthalmol 1981; 99: 1212.
9. Ruckstuhl M, Landry Y. Inhibition of lung cyclic AMP- and cyclic GMP phosphodiesterases by flavonoids and other chromone-like compounds. Biochem Pharmacol 1981; 30: 697-702.
10. Beretz A, Anton R, Cazenave JP. The effects of flavonoids on cyclic nucleotide phosphodiesterases. In: Cody V, Middleton E, Harborne JB. (Eds.), Plant Flavonoids in Biology and Medicine: Biochemical, Pharmacological and Structure-Activity Relationships, Alan R. Liss Inc, New York, 1986; 281-296.
11. Altorjay I, Dalmi L, Sari B, Imre S, Balla G. The effect of silibinin (Legalon) on the free radical scavenger mechanisms of human erythrocytes in vitro. Acta Physiologica Hungarica 1992; 80: 375-380.
12. Mohammed HM, Abdulrazzaq MH, Hussain SA. Effects of silibinin hemisuccinate on the intraocular pressure in normotensive rabbits. Saudi Med J 2007, 28(9): 1397-1401
13. Koch HP, Bachner J, Loffler E. Silymarin: potent inhibitor of cyclic AMP phosphodiesterase. Methods Find Exp Clin Pharmacol 1985; 7(8): 409-413.
14. Vareilles P, Lotti VJ. Effects of timolol on aqueous humor dynamics in the rabbit. Ophthalmol Res 1981; 13: 72-79.
15. 15.Vareilles P, Silverstone D, Plazonnet B, LeDouarec JC, Sears ML, Stone CA. Comparison of the effects of timolol and other adrenergic agents on intraocular

Iraqi J.Pharm.Sci., Vol.16 (2) ,2007 IOP-lowering effect of silibinin
44
pressure in the rabbit. Invest Ophthalmol Vis Sci 1977; 16: 987-996.
16. Hoffman BB, Lefkowitz RL, Taylor P. Neurotransmission: the autonomic and somatic motor nervous system. In: Hardman JG, Limbird LE, Molinoff PB, Ruddon RW, Gilman AG. (Eds.), Goodman and Gilman’s: The Pharmacological Basis of Therapeutics, (9th ed.), McGraw-Hill, New York, 2001; 105-139.
17. Liu HP. Chion CY. Continuous stimulation and instant display of aqueous humor dynamics with a microspectrometer and a sensitive drop counter. Exp Eye Res 1981; 32: 583-592.
18. Lefkowitz R.J, Mukherjee C, Coverstone M, Caron MG. Steriospecific [3H] (-) alprenolol binding site, β-adrenergic receptors and adenylate cyclase. Biochem Biophys Res Commun 1974; 60: 703-709.
19. Brubaker, R.F.: Clinical measurements of aqueous dynamics: implications for addressing glaucoma. In: Civan MM. (Ed.), The Eye’s Aqueous Humor: From
Secretion to Glaucoma, Academic press, San Diego, 1998; 233-284.
20. Tian B, Geiger B, Epstein DL, Kaufman PL. Cytoskeleton involvement in the regulation of aqueous humor outflow. Invest Ophthalmol Vis Sci 2000; 41: 619-623.
21. Gieser SC, Juzych M, Robin AL, Schwartz GF. Clinical pharmacology of adrenergic drugs. In: Ritch R, Shields MB, Krupin T. (Eds.), The Glaucoma, (2nd Ed.), Mosby, St. Louis, 1996; 1425-1448.
22. Lee PY, Podos SM, Mittag T, Severin C. Effect of topically applied forskolin on aqueous humor dynamics in cynomolgus monkey. Invest Ophthalmol Vis Sci 1984; 25: 1206-1209.
23. Gabelt BT, Kaufman PL. Prostaglandin F2 alpha increases uveoscleral outflow in the cynomolgus monkey. Exp Eye Res 1989; 49(3): 389-402.
24. Okada Y, Hazama A. Volume regulatory ion channels in epithelial cells. News Physiol Sci 1989; 4: 238-242.