colorado state innovation model (sim) cohort 3 request for...
TRANSCRIPT

1 | P a g e
Colorado State Innovation Model (SIM) Cohort 3
Request for Application (RFA) Packet

2 | P a g e
REQUEST FOR APPLICATION (RFA) TIMELINE OVERVIEW
For questions related to the Cohort 3 SIM Practice Request for Application (RFA), please email [email protected] or call 303-724-8968.
SCHEDULE OF ACTIVITIES TIMELINE (All times are listed as local Colorado time)
SIM Cohort 3 Application Posted at: http://bit.ly/sim3application
November 15, 2017
SIM Cohort 3 FAQs Posted at: http://bit.ly/sim3rfafaq
November 15, 2017
SIM Cohort 3 RFA Submission Deadline Applications Must Be Submitted Online By Date and Time Listed
January 19, 2018 11:59 pm MST
SIM Cohort 3 RFA Informational Webinar(s)
To register click on the hyperlinks listed below or visit the Colorado SIM office webpage at: http://bit.ly/2zVdaVl
Or by clicking the individual hyperlinks below: ● November 30 - Register Now● December 6 - Register Now● January 4 - Register Now
November 30, 2017 7:30 am – 8:30 am MST
December 6, 2017 12:15 pm – 1:15 pm MST
January 4, 2018 7:30 am – 8:30 am MST
SIM Cohort 3 Anticipated Notification April/May 2018
SIM Cohort 3 Practice Participation Agreements Signed May/June 2018
SIM Cohort 3 Anticipated Start/Kick-Off June 2018

3 | P a g e
TABLE OF CONTENTS:
EXECUTIVE SUMMARY 4
SECTION I. Program Overview & Eligibility 7 SIM Background 7 Key Definitions 8 Practice Site Eligibility 8 Advantages of SIM Participation 9 Expectations of SIM Participation for SIM-Only Practice Sites 10 Expectations of SIM Participation for SIM/CPC+ Practice Sites 10 Overview of Practice Transformation Program Support 11 HIT Support 12 Available Funding 13 Support from Payers 14
SECTION II. SIM Framework & Milestones 16 Overview of Milestones 16
SECTION III. Practice Application 17 Practice Application Instructions and Questions 17 Practice Site Roster, Key Contacts, and NPIs 17
SECTION IV. Practice Application Review & Selection Process 18Overview of Practice Application Review 18 Practice Application Review Committee 18 Practice Application Review and Selection Process 18
REFERENCES 20
ADDITIONAL DOCUMENTS SIM Framework and Milestones SIM Clinical Quality Measure (CQM) Reporting Summary SIM Cohort 3 Assessments and Reporting Schedule SIM Cohort 3 Practice Participation Agreement- Draft SIM Cohort 3 Application Instructions and Questions

4 | P a g e
EXECUTIVE SUMMARY
The Colorado State Innovation Model (SIM) is a governor’s office initiative that is funded by the Center for Medicare & Medicaid Services (CMS). The goal is to improve the health of Coloradans by increasing access to integrated physical and behavioral healthcare services in coordinated systems and encouraging SIM practices to test value-based payment structures. The SIM initiative will reach 400 primary care providers and four community mental health centers during its four-year timeline and strives to influence the healthcare of 80% of Colorado residents through its efforts, which include regional health connectors and local public health agencies, by 2019.
To achieve this goal, SIM will select primary care practice sites from across the state to receive practice transformation support to help them integrate behavioral and physical health in primary care and facilitate a transition to value-based payments.
The University of Colorado is issuing this request for application (RFA) on behalf of the SIM office. Approximately 150 practice sites will be selected to participate in the third cohort of SIM and engage in practice transformation activities. These practices will join 246 practice sites that currently participate in the first and second SIM cohorts. Participating practice sites will receive support from and work with practice transformation organizations (PTOs) to develop competencies associated with the SIM Practice Transformation Building Blocks as outlined within the SIM Framework and Milestones. The building blocks are based on Thomas Bodenheimer’s “The 10 Building Blocks of High Performing Primary Care, revised to reflect SIM priorities.”1 The building blocks, and their component milestones, are designed to strengthen delivery of comprehensive primary care by moving toward greater integration of behavioral health services and help providers succeed with alternative payment models. Practice sites in Cohort 3 will qualify for achievement-based payments of up to $6,500 per practice site and may apply for up to $40,000 in competitive grants. These practice transformation supports, among others, are designed to advance the delivery of person-centered, team-based care with an emphasis on integrated care.
Participation in SIM helps providers prepare for a changing healthcare landscape that has been shaped by the Medicare Access and CHIP Reauthorization Act (MACRA), bipartisan legislation that was signed in 2015 and designed to pay providers for the quality and effectiveness of the care they provide Medicare beneficiaries. Other payers have implemented value-based payment models. This shift from fee-for-service payments to reimbursement that will increasingly be based on the value of care provided puts the onus on practices to demonstrate higher-quality care that improves health outcomes while reducing costs. Success in this value-based reimbursement world requires different skills and processes, including the integration of behavioral and physical health in primary care settings. The SIM initiative helps guide practice sites along this path with intensive coaching to implement integrated care and turn data into actionable information that helps build sustainable models. Seven public and private payers signed a Memorandum of Understanding (MOU) with the SIM office, in which they committed to work collaboratively with SIM to transform the way primary care and behavioral healthcare is delivered and financially supported in the practice sites selected for SIM within their networks. Get more details on how SIM helped providers integrate care: www.colorado.gov/healthinnovation.
Eligibility: Primary care practice sites in Colorado that use electronic health records (EHRs) are eligible to apply for this opportunity.

5 | P a g e
Benefits: Practice sites participating in SIM will receive multiple benefits, including: Area Benefit
Practice Transformation Support Services
● Practice facilitation: o Access to support from a certified Practice Transformation Organization o Preparation for Medicare Quality Payment Program (QPP) and other initiatives that
require a transition from fee-for-service to value-based payments o Development of high-functioning care teams within your practice using efficient
workflows o Implementation of your practice vision for integrating behavioral health into your
primary care practice ● Technical support from a Clinical Health Information Technology Advisor (CHITA) ● Opportunities to earn Continuing Medical Education (CME) and Maintenance of Certification
(MOC) credits ● Opportunity to learn from peers during Collaborative Learning Sessions with other SIM
practice sites during the Cohort 3 time frame Financial Support
● Opportunity to earn achievement-based payments of up to $6,500 per practice site for achieving milestones within key building blocks
● Opportunity to apply for competitive grants up to $40,000 to support behavioral health integration
● Practice sites receive value-based payments from one or more SIM participating private and public payers
Recognition ● Certificate of recognition signed by the governor’s office Health Information Technology
● In-person technical support provided by a CHITA ● Support connecting to a health information exchange to share data and coordinate care ● Subsidies for nonprofit practice sites to install or upgrade broadband, a key step toward
developing the infrastructure necessary to provide telehealth services
Data ● Access to aggregated claims data that allows cost and utilization data to be tracked across providers and payers to improve population health management
● Access to aggregated clinical quality data to compare practice site level data with the SIM cohort and inform quality improvement efforts
Connections to Community Resources
● Access to a Regional Health Connector (RHC), a local person dedicated to connecting practice sites to resources that can improve patient outcomes
● Connection to local public health resources and data related to population health
Business Support ● Access to data benchmarking to help practice sites assess business processes ● Educational sessions that help practice representatives develop skills in budgeting and
administrative processes to support value-based payments Patient Outcomes ● Integrated behavioral healthcare produces significant positive results, including decreased
patient depression levels, improved quality of life, decreased stress, and lower rates of hospitalization
● Having access to behavioral health services for patients is expected to reduce the total cost of care. Some studies indicate that integrated care leads to a reduction of inappropriate use of medical services and cost-savings in big-ticket items, such as emergency department visits and hospitalizations (see References at end of the document for citations)
Provider Satisfaction • Integrated behavioral health services may improve patient and provider satisfaction by reducing
access barriers, improving communication and enabling providers to influence comorbidities between physical and behavioral health issues

6 | P a g e
Each practice will receive guidance and supported from these professionals along with other resources:
Expectations: During the Cohort 3 timeline, SIM practice sites will work to achieve a set of milestones within the SIM Practice Transformation Building Blocks as outlined in the SIM Framework and Milestones. These building blocks focus on strengthening the delivery of comprehensive primary care and moving toward greater integration of behavioral health services.
All participating practice sites will receive SIM Practice Transformation Program support and will be expected to meet requirements as outlined in the table on the following page. Additional detail can be found in the Expectation of SIM Participation for SIM-Only and SIM/CPC+ Practice Sites sections.
Alignment with Comprehensive Primary Care Plus (CPC+): The SIM team worked with CMS to align the initiative with CPC+, another initiative funded by CMS through the Centers for Medicare and Medicaid Innovation (CMMI) to strengthen primary care and help practice sites shift from volume-based to value-based payment systems. Practice sites participating in CPC+ are eligible for and encouraged to apply for SIM. These complementary initiatives offer unique benefits to practice sites that are interested in integrating behavioral and physical health in primary care settings. Practice sites that participate in both initiatives will receive support from SIM that will build on the support provided by CPC+. SIM support will focus on behavioral health integration, business support, and health information technology assistance.
In addition to meeting all requirements of CPC+, practice sites that participate in both SIM and CPC+ must meet the expectations outlined in the table below. These expectations are slightly modified from those required of practices that participate in the SIM initiative alone. Expectations for CPC+ practices have been designed to reduce the burden of participating in two initiatives while enhancing outcomes beyond what would be expected as a result of participating in CPC+ alone.
Shared Expectations of All SIM Practice Sites
1) Identify a cross-functional Quality Improvement Team to implement improvements based on theSIM Practice Transformation Building Blocks.
2) Complete a set of practice assessments to identify key areas of focus for improvement.
3) Participate in SIM evaluation activities.
7 | P a g e
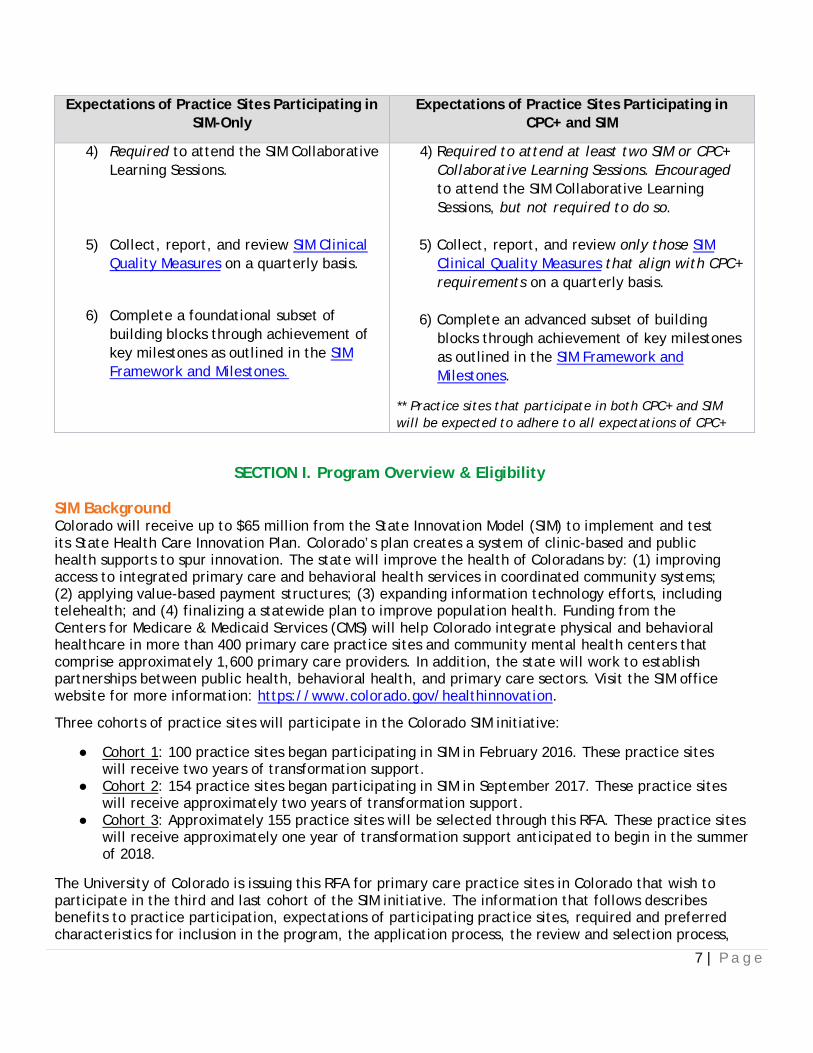
Expectations of Practice Sites Participating in SIM-Only
Expectations of Practice Sites Participating in CPC+ and SIM
4) Required to attend the SIM Collaborative Learning Sessions.
5) Collect, report, and review SIM Clinical Quality Measures on a quarterly basis.
6) Complete a foundational subset of building blocks through achievement of key milestones as outlined in the SIM Framework and Milestones.
4) Required to attend at least two SIM or CPC+ Collaborative Learning Sessions. Encouraged to attend the SIM Collaborative Learning Sessions, but not required to do so.
5) Collect, report, and review only those SIM Clinical Quality Measures that align with CPC+ requirements on a quarterly basis.
6) Complete an advanced subset of building blocks through achievement of key milestones as outlined in the SIM Framework and Milestones.
** Practice sites that participate in both CPC+ and SIM will be expected to adhere to all expectations of CPC+
SECTION I. Program Overview & Eligibility SIM Background Colorado will receive up to $65 million from the State Innovation Model (SIM) to implement and test its State Health Care Innovation Plan. Colorado’s plan creates a system of clinic-based and public health supports to spur innovation. The state will improve the health of Coloradans by: (1) improving access to integrated primary care and behavioral health services in coordinated community systems; (2) applying value-based payment structures; (3) expanding information technology efforts, including telehealth; and (4) finalizing a statewide plan to improve population health. Funding from the Centers for Medicare & Medicaid Services (CMS) will help Colorado integrate physical and behavioral healthcare in more than 400 primary care practice sites and community mental health centers that comprise approximately 1,600 primary care providers. In addition, the state will work to establish partnerships between public health, behavioral health, and primary care sectors. Visit the SIM office website for more information: https://www.colorado.gov/healthinnovation.
Three cohorts of practice sites will participate in the Colorado SIM initiative:
● Cohort 1: 100 practice sites began participating in SIM in February 2016. These practice sites will receive two years of transformation support.
● Cohort 2: 154 practice sites began participating in SIM in September 2017. These practice sites will receive approximately two years of transformation support.
● Cohort 3: Approximately 155 practice sites will be selected through this RFA. These practice sites will receive approximately one year of transformation support anticipated to begin in the summer of 2018.
The University of Colorado is issuing this RFA for primary care practice sites in Colorado that wish to participate in the third and last cohort of the SIM initiative. The information that follows describes benefits to practice participation, expectations of participating practice sites, required and preferred characteristics for inclusion in the program, the application process, the review and selection process,

8 | P a g e
and timelines for practice selection.
Key Definitions Practice: For purposes of this RFA, a practice is defined as a “practice site or physical location.” A practice may have one tax identification number (TIN) that includes multiple providers in several locations, but for purposes of SIM, a “practice site” is defined as one physical location. For example, a practice with one TIN might have five locations; for this RFA, those sites are considered five “practice sites,” and each practice site must submit its own application. For the initial cohort, a desire to have a wide diversity of practice types resulted in a limitation on the number of accepted practice sites within a given healthcare group or system. For SIM Cohorts 2 and 3, an effort will be made to accept as many qualified practice sites as possible in a group or system to help expedite transformation within the overall organization.
Primary Care: As defined by the Institute of Medicine (IOM), primary care is the provision of integrated, accessible health care services by clinicians who are accountable for addressing the large majority of personal health care needs (such as preventative counseling, screening, early intervention, management of acute problems as well as coordination of care). In addition to this the primary care provider is tasked with not only developing a sustained partnership with patients but practicing in the context of family and community as well.
An eligible primary care practice site must be capable of providing a majority of its patients’ comprehensive primary, preventive, chronic, and acute care.
“Non-traditional” practice sites that provide a full range of primary care services and otherwise meet the requirements can be considered for participation. Non-traditional practice sites could include school-based clinics, local public health clinics, practice sites providing primary care services to specified groups of patients (such as women’s health clinics), and others.
Applicants that are not clearly traditional primary care practice sites but representatives believe the sites provide primary care services will be considered on a case-by-case basis. On the application, “non-traditional” practice sites will be asked to address how the practice meets the IOM definition of primary care. Prior to review or acceptance, these practice sites might be required to provide additional information (such as billing information), to substantiate that they provide comprehensive primary care services.
If practice eligibility remains unclear after review of a practice site’s completed application, participation recommendations will be made by the Practice Application Review Committee that is convened by the University of Colorado. Final decisions will be made by the SIM office.
Behavioral Health Care: For SIM, the term “behavioral health care” includes the spectrum of services used to diagnose, prevent and manage substance use disorders, health behavior aspects of disease, and mental health.
Practice Site Eligibility To be eligible for participation in SIM Cohort 3:
1. Practice sites must be physically located in Colorado.2. Individual practice sites must complete and submit the application in its entirety online
before 11:59 pm MST on January 19, 2018.3. Practice sites must meet the IOM definition of primary care (outlined above).4. Practice sites must currently use an EHR.
9 | P a g e
Healthcare systems or multi-site organizations as well as other sponsoring organizations interested in participating in SIM Cohort 3 should encourage their practice sites to apply and can assist practice sites in preparing their applications. Some sections within the application MUST be completed by the practice site; in particular, questions in narrative sections should be completed by a lead clinician or another key leader from the practice site. An individualized narrative that gives the reviewers a sense of the practice site culture and commitment to integrated care greatly increases the likelihood of a practice site being offered the opportunity to participate in Cohort 3. It is critical to submit an application that addresses all questions as applicable and has been thoroughly reviewed in order to ensure consideration for participation in Cohort 3.
Advantages of SIM Participation In addition to practice transformation support and monetary compensation, there are many other benefits to practice sites participating in SIM, which include but are not limited to:
1. Benefits to patients that are reflected in clinical quality measures (CQMs) and other indicators of practice performance, which can have an effect on practice success in alternative payment models, including: a. Integrated or collaborative behavioral healthcare produces significant positive results,
including decreases in patient depression levels, improvement in quality of life, decreased stress and lower rates of hospitalization. 2-5
b. Improved access to behavioral health services is expected to reduce the total cost of care. Some studies indicate that integrated care leads to a reduction of inappropriate use of medical services and cost-savings in big-ticket items like emergency department visits and hospitalizations. 6-9
c. Integrated behavioral health services may improve patient satisfaction by reducing access barriers, improving communication and enabling providers to influence comorbidities between physical and behavioral health issues. 10
2. Benefits to providers from implementing an integrated model of care, as reported by primary care physicians, include: 5
a. Better communication b. More comprehensive services c. Better management of depression, anxiety, and alcohol abuse d. More convenient services for patients e. Reduced mental health stigma f. Better coordination of mental and physical health g. Quicker appointments for mental health services h. Better health education i. Enhanced provider satisfaction
3. Behavioral health screening, treatment and care coordination are essential components of advanced models of primary care and various advanced payment models.
4. Business consulting expertise provided through SIM will help practice sites prepare for value-based budgeting as they move from fee-for-service to value-based payments, bundled payments, and shared savings.
5. Clinical health information technology (HIT) support will help practice sites optimize their EHRs, create access to registry functionality, and generate better data to manage patient care including gaps in care, risk stratification, management of cost of care, care management, and

10 | P a g e
care coordination. 6. Practice sites will gain access to peer-to-peer learning and sharing so they are not
struggling on their own and reinventing what others have already figured out.7. Practice sites will have access to SIM achievement-based payments to offset some of the costs
associated with the requirements to participate in SIM.8. Continuing Medical Education (CME) credits and eligibility for Part IV Maintenance of
Certification (MOC) credit toward board recertification requirements will be offered.
Expectations of SIM Participation for SIM-Only Practice Sites Expectations of SIM participation for SIM-Only practice sites, those not participating in CPC+ are listed below:
1. Identifying a cross-functional Quality Improvement (QI) Team to implement improvementsbased on the SIM Practice Transformation Building Blocks. This QI Team should be maintainedthroughout the duration of SIM and include representation from various roles within thepractice. For most practice sites, this team will include a provider, office administrator,clinical support, and front desk staff. Depending on the practice, it might also include abehavioral health professional and/or a care manager.
a. Dedicating time for the QI Team to meet with the practice facilitator up to twice amonth for approximately one hour each time.
b. Dedicating time as needed to work with a CHITA who will assist with practice datareporting and data-driven quality improvement.
2. Completing a set of practice assessments to identify key areas of focus for improvement.These baseline and periodic project assessments include the Medical Home Practice Monitor,the Integrated Practice Assessment Tool (IPAT), the SIM Milestone Attestation Checklist (MAC),HIT Assessment, and the Clinician and Staff Experience Survey that will help practices trackprogress over time. An overview of assessments, including a timeline can be found in SIMCohort 3 Assessments and Reporting Schedule.
3. Collecting, reporting and reviewing SIM clinical quality measures (CQMs) on a quarterly basis.CQMs that will be collected, reported and reviewed are outlined in SIM Clinical QualityMeasure (CQM) Reporting Requirements.
a. Based on their patient demographics, practice sites will be asked to select either thepediatric measure set or the adult measure set. Family and/or mixed practice sitescan choose either one of the measure sets to report throughout their participation inSIM.
b. SIM-Only adult practice sites will report a total of six required CQMs. SIM-Only pediatricpractice sites will report a total of four required CQMs. Practice sites are encouragedbut not required to report additional CQMs from a secondary measure set based onpractice reporting ability and arrangements with payers.
4. Attending two regional SIM Collaborative Learning Sessions. In a spirit of fostering a truepeer-to-peer learning community, practice representatives may be asked to share insightsthrough presentations and panel discussions at these sessions.
5. Participating in SIM evaluation activities. This includes completing baseline as well asperiodic and end-of-project assessments. This process might also include key informantinterviews with TriWest, an organization contracted to conduct an evaluation of the SIMInitiative, and other evaluation-related requirements specified by TriWest or CMS.
6. Completing SIM-Only identified building blocks through achievement of key milestones. Thekey milestones required for SIM-Only practices to receive SIM achievement-based payments topractices are outlined in Section II and in the SIM Practice Transformation Building Blocks(see SIM Frameworks and Milestones; also outlined in Section II).

11 | P a g e
Expectations of SIM Participation for SIM/CPC+ Practice Sites Practice sites that participate in both CPC+ and SIM will be expected to adhere to all expectations of CPC+, including: Undertaking care delivery transformation activities outlined in the Care Delivery Requirements established by CMS that are focused around five Comprehensive Primary Care Functions: (1) Access and Continuity; (2) Care Management; (3) Comprehensiveness and Coordination; (4) Patient and Caregiver Engagement; and (5) Planned Care and Population Health.
Practice sites participating in both SIM and CPC+ will meet similar requirements as the SIM-Only practices, but the requirements have been tailored to closely align with existing CPC+ expectations. The requirements are as follows:
1. Identifying a cross-functional Quality Improvement (QI) Team to implement improvements
based on the SIM Practice Transformation Building Blocks. This QI Team should be maintained throughout the duration of SIM and include representation from various roles within the practice. For most practice sites, this team will include a provider, office administrator, clinical support, and front desk staff. Depending on the practice, it might also include a behavioral health professional and/or a care manager.
a. Dedicating time for the QI Team to meet with the practice facilitator up to twice a month for approximately one hour each time.
b. Dedicating time as needed to work with a CHITA who will assist with practice data reporting and data-driven quality improvement.
2. Completing a set of practice assessments to identify key areas of focus for improvement. These baseline and periodic project assessments include the Integrated Practice Assessment Tool (IPAT), Medical Home Practice Monitor, and the Clinician and Staff Experience Survey that will help practices track progress over time. An overview of assessments, including a timeline can be found in SIM Cohort 3 Assessments and Reporting Schedule.
3. Collecting, reporting and reviewing SIM Clinical Quality Measures (CQMs) that align with CPC+ requirements on a quarterly basis. Reporting on the practice-level measures established annually by CMS. Note that the CQMs reported for CPC+ will count for SIM, and no additional measures for SIM are required. CQMs that will be collected, reported, and reviewed are outlined in SIM Clinical Quality Measure (CQM) Reporting Requirements.
4. Participating in at least two CPC+ or SIM Collaborative Learning Sessions. SIM/CPC+ practice sites are encouraged to attend the SIM Collaborative Learning Sessions, but may attend the CPC+ session instead.
5. Participating in SIM evaluation activities. This includes completing baseline as well as periodic and end-of-project assessments. This process might also include key informant interviews with TriWest, an organization contracted to conduct an evaluation of the SIM initiative, and other evaluation-related requirements specified by TriWest or CMS.
6. Completing SIM/CPC+ identified building blocks through achievement of key milestones. The key milestones required for SIM/CPC+ practices to receive SIM payments to practice are outlined in Section II and in SIM Framework and Milestones.
Overview of Practice Transformation Program Support Practice sites will be provided with a practice facilitator and a CHITA and linked with a Regional Health Connector (RHC) to deliver a comprehensive, personalized package of in-office support that will allow practices to successfully realize SIM initiative goals and connect them with community and state resources. The practice facilitator and CHITA will be provided by one or more practice transformation organizations (PTOs) selected by a rigorous procurement process to ensure that practice sites benefit from highly-skilled personnel. The RHC will be deployed through local organizations selected for their
12 | P a g e
existing, trusted relationships in the communities they serve. An overview of each role is provided below:
1. Practice Facilitator Role:a. Support implementation of an ongoing change and quality improvement process
through Quality Improvement Teamsb. Facilitate Quality Improvement Team activities to focus on achieving SIM Milestonesc. Identify and help resolve challenges in achieving milestonesd. Facilitate the development of sustainable quality improvement techniques and
processese. Coordinate and facilitate practice site access to additional practice transformation
resources, including coordination with the local RHC2. CHITA Role:
a. Assist in completion of HIT Assessment as well as the identification and assessment ofcurrent HIT resources
b. Support the enhancement of practice capacity to implement data-driven qualityimprovement
c. Assist with the development and implementation of practice workflow for datacollection, reporting, validation and analysis
d. Facilitate data-driven quality improvement prioritiese. Link practice sites with technical assistance available through various SIM and non-SIM HIT
resources3. RHC Role:
a. Provide information regarding state and regional transformation and community healthresources
b. Facilitate the connection of practice site to local public health and other communityresources
c. Establish ongoing supportive relationships with practice sites that can be sustainedbeyond the year of active practice transformation support
4. Other activities included in SIM include:a. A baseline assessment to help practices identify strengths and opportunities for
improvement using the SIM Practice Transformation Building Blocks as outlined within theSIM Framework and Milestones and based on Thomas Bodenheimer’s “The 10 BuildingBlocks of High Performing Primary Care.”
b. Offering two peer-to-peer Collaborative Learning Sessionsc. Opportunities that help you develop business processes that are beneficial in value-based
payment modelsd. Support moving toward greater integration of behavioral health care. Practice
Transformation support will be tailored to each practice site’s unique needs and prioritiesvia a model that is aligned with the CPC+ Behavioral Health Integration Menu of Options
HIT Support Practice sites will be provided with the following resources related to HIT:
1. Data Aggregation: SIM practice sites will receive a license to a data aggregation tool that allowscost and utilization data to be tracked across providers and payers that support practices in theinitiative. This tool is intended to help practice sites access data across the medicalneighborhood, manage population health and integrate it with their clinical data, and view totalcost of care.
2. Broadband Subsidies: Eligible practice sites will be connected to the Colorado Telehealth
13 | P a g e
Network, which can help practices access federal telecom subsidies. Participants that access this support, on average, save 49 percent on their telecom spending. Eligible sites include nonprofit organizations that oversee the following:
a. Hospitalsb. Rural health clinicsc. Local health departmentsd. Community safety net clinics and federally qualified health centerse. Health centers providing healthcare to migrant workersf. Post-secondary educational institutions offering healthcare instructiong. Teaching hospitalsh. Medical schoolsi. Other nonprofit health care providers in a consortium
3. Connection to Health Information Exchanges: The SIM office is currently pursuing avenues to helppractice sites connect to health information exchanges and maximize data exchange with otherclinicians and hospital systems.
Available Funding SIM practice sites can access the following funds to help advance practice transformation activities.
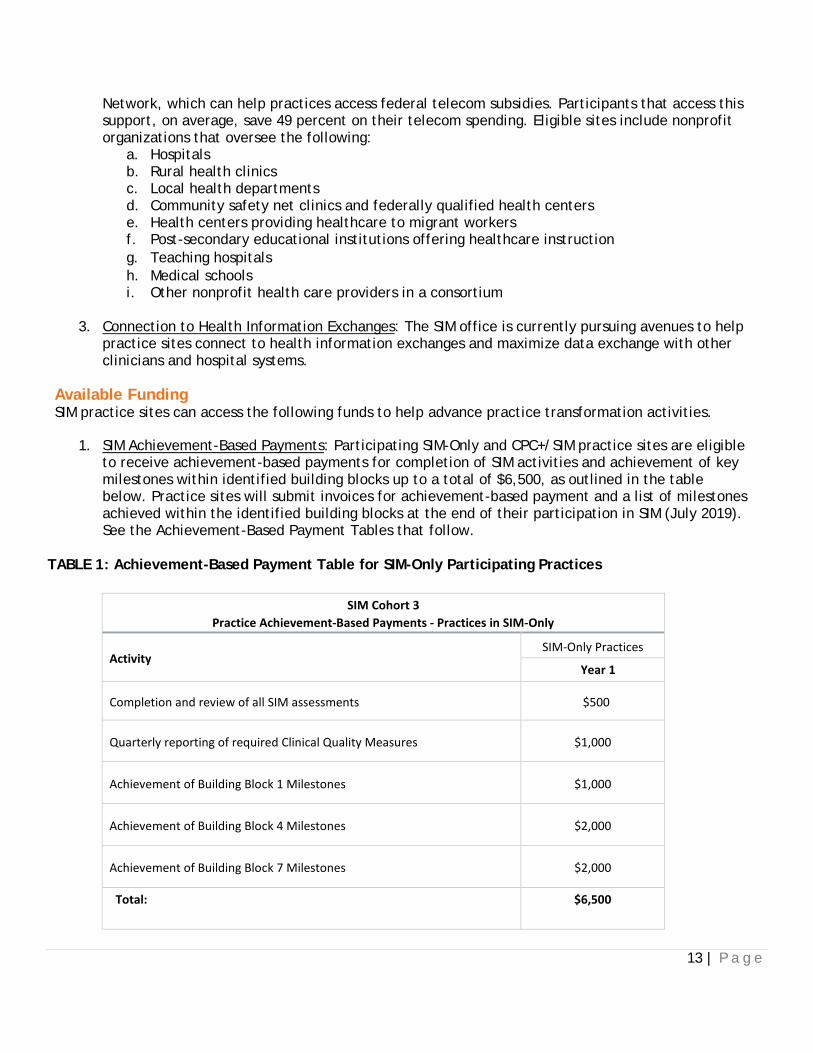
1. SIM Achievement-Based Payments: Participating SIM-Only and CPC+/SIM practice sites are eligibleto receive achievement-based payments for completion of SIM activities and achievement of keymilestones within identified building blocks up to a total of $6,500, as outlined in the tablebelow. Practice sites will submit invoices for achievement-based payment and a list of milestonesachieved within the identified building blocks at the end of their participation in SIM (July 2019).See the Achievement-Based Payment Tables that follow.
TABLE 1: Achievement-Based Payment Table for SIM-Only Participating Practices
SIM Cohort 3 Practice Achievement-Based Payments - Practices in SIM-Only
Activity SIM-Only Practices
Year 1
Completion and review of all SIM assessments $500
Quarterly reporting of required Clinical Quality Measures $1,000
Achievement of Building Block 1 Milestones $1,000
Achievement of Building Block 4 Milestones $2,000
Achievement of Building Block 7 Milestones $2,000
Total: $6,500

14 | P a g e
TABLE 2: Achievement-Based Payment Table for SIM/CPC+ Participating Practices
SIM Cohort 3
Practice Achievement-Based Payments Practices in SIM and CPC+
Activity
SIM/CPC+ Practices
Year 1
Completion and review of all SIM assessments $500
Quarterly reporting of required Clinical Quality Measures $1,000
Achievement of Building Block 4 Milestones $1,000
Achievement of Building Block 7 Milestones $1,000
Achievement of Building Blocks 8, 9, or 10 Milestones (choose two of these Building Blocks) $3,000
Total: $6,500
2. Small Grants via the Practice Transformation Fund: Participating SIM-Only and CPC+/SIM practice
sites can apply for competitive grants of up to $40,000 to assist in meeting SIM milestones and achieving goals outlined in their Practice Improvement Plans. The Small Grants Program will be administered by the SIM office. Funds for this opportunity are provided via a generous grant from The Colorado Health Foundation. Applicants will be selected through a competitive process based on the overall quality of the application, the likelihood that the project will help the practice achieve the practice transformation milestones, and practice need, including the needs of the practice’s target population and the demonstrated need for the project. Examples of how some Cohort 1 practice sites have utilized their small grants and this funding has helped further promote Practice Transformation can be found on the SIM Media Page.
Support from Payers In Colorado, public and private payers have voluntarily developed a multi-payer approach to support and expand broad-based accountable, whole person, patient-centered care transformation through a variety of initiatives. Within this landscape, seven payers signed a Memorandum of Understanding (MOU) with the SIM office, in which they committed to work collaboratively with SIM to transform the way primary care and behavioral healthcare are delivered and financially supported in the practice sites selected for SIM within these networks. These payers are collaborating to:
1. Focus on primary care practice sites and behavioral health settings seeking to ingrate care 2. Support providers in delivering and coordinating integrated care that improves population
health, and increases quality while reducing costs 3. Increase providers’ abilities to manage whole-person care 4. Develop necessary infrastructure to support integration and delivery of whole-person care

15 | P a g e
5. Encourage practice sites to continually evolve towards higher-levels of integration throughtransformation of care delivery supported by alternative payment models (APMs)
6. Support a data aggregation tool (referenced above) to help providers analyze data from payersthat support them in the SIM initiative in one tool
7. Participate in SIM-sponsored Multi-Stakeholder Symposiums that facilitate active dialoguebetween providers and health plan representatives to ensure mutually-beneficial partnerships
Payers participating in SIM have agreed to apply organization-specific payment model(s) and establish their own agreements with practice sites selected for SIM Cohort 3. Payers already have APMs in place with many practice sites in their networks to support primary care transformation. For SIM, value-based payments received through a payer-specific APM will support practice site work around behavioral health integration.
While each payer is using its own payment model to support SIM’s transformation goals, which is negotiated directly between the payer and the practice, the payment model(s) that payers will apply to SIM practice sites include the following basic elements:
1. Fee-for-service payments2. Payments that include behavioral health integration through one of the following
mechanisms:a. Upfront paymentsb. Population-based payments (e.g., PMPM)c. Care coordination paymentsd. Payment for additional codes
3. Shared savings opportunities OR incentive payments based on performance and/or outcomeslinked to quality
Payers’ existing APMs are already tied to outcomes measures for each plan, and payers are working collaboratively to align their measures in support of behavioral health integration. Participating payers have aligned practice expectations to the SIM Practice Transformation Building Blocks as outlined in the SIM Framework & Milestones. Payers’ payment methodologies are designed to support practice capacity and infrastructure to achieve the milestones within these building blocks during the course of the initiative. Additionally, payers have aligned around the SIM set of CQMs and claims-based measures that will help practice sites identify things that influence healthcare quality, utilization, and costs.
Selection for SIM support DOES NOT guarantee that practice sites already receiving payment support from payers will receive any additional value-based payments for participation in SIM. As noted, payers have established their own agreements with practice sites and use different approaches that include:
1. Continuation of existing models/commitments: Some payers are continuing existing paymentarrangements with practice sites that are already participating in APMs; this includes practice sitesparticipating in other payer-specific or federal initiatives.
2. Extension of existing models/commitments to new practice sites: Some payers are extending themodels used in current initiatives (e.g., CPC+, payer-specific programs/projects) to additionalnew practice sites participating in SIM.
3. Modification of existing models/commitments to include new funding: Some payers havemodified the models used in current, ongoing initiatives to include new funding forprogression through the practice transformation milestones outlined in the SIM Frameworkand Milestones.

16 | P a g e
The payment models that payers are applying to SIM practice sites are aligned with a continuum of APMs established by the Health Care Payment and Learning Action Network (HCPLAN), a national collaborative of public and private stakeholders working to accelerate the healthcare system’s adoption of effective APMs. Payers are using models within Categories 2 and 3. A copy of the HCPLAN framework, and a brief description of each SIM payer’s payment model, can be found in the Addendum to the MOU.
Colorado’s selection as a Round 1 CPC+ region provides additional opportunities and resources to support care delivery and payment reform efforts in the state, which are heightened by Medicare’s participation as a payer. Primary care practice sites are eligible and encouraged to participate in CPC+ and SIM. However, initiatives that are designed to test or identify the most appropriate methods for using value-based payments, particularly those sponsored by CMS, are not intended to be additive to existing payment models. All eligible practice sites selected for CPC+ will receive payment support from payers participating in CPC+, per the requirements of the model. However, practice sites selected for CPC+ that are also selected for SIM Cohort 3 will likely not receive additional value-based payments for their participation in SIM, depending on the payer. Participation in SIM does qualify practice sites for the Health First Colorado (Colorado’s Medicaid Program) Alternative Payment Model (APM), which will begin in 2018. The APM program is offered to Primary Care Medical Providers (PCMPs) who are contracted with and participating in the Health First Colorado Accountable Care Collaborative (ACC), the platform for Medicaid care delivery in Colorado. The ACC will transition from the Regional Care Collaborative Organization structure to the Regional Accountable Entity (RAE) structure in the summer of 2018. Get more information about the Health First Colorado APM: http://bit.ly/2ref3YC. Please note due to the timing of the Health First Colorado (Medicaid) RAE selection and contracting process, final determination of the SIM Cohort 3 practices that Medicaid will support might not occur until after the SIM Cohort 3 practice selection process is complete. The SIM office team is working on a timeline and communication strategy for this process.
SECTION II. SIM Framework & Milestones Overview of Milestones The SIM Framework and Milestones are intended to be benchmarks that guide and measure where participating practice sites are in their transformation journeys. They are derived from the Bodenheimer Building Blocks and the Comprehensive Primary Care (CPC) initiative milestones and activities and reflect the priorities of payers that support SIM practices. The milestones have been developed by the SIM office, Multi-Payer Collaborative, and the University to emphasize and support SIM’s focus on advancing behavioral health integration within primary care settings.
The Colorado SIM Practice Transformation Building Blocks and their associated milestones are not application criteria, but rather a roadmap for where practice sites will be headed based on their participation in SIM. Practice sites should consider their commitment to achieving these benchmarks when determining whether to apply for the SIM initiative.
Practice sites are expected to maintain “good standing” with the behavioral health focus of the initiative through successful completion of identified building blocks and achievement of key milestones as outlined below. If practice sites are not in good standing with SIM, payers will individually determine the effect to their programs, which might affect the payment a practice receives from its payers. The SIM office will work with practice transformation organizations and the University to support transformation and to

17 | P a g e
determine a practice site’s standing. Practice standing information will be shared with payers to inform practice eligibility for payment from individual payers.
Practices must achieve identified building blocks through completion of key milestones to maintain “good standing.” Requirements to maintain “good standing” for each year are outlined below:
Practice Sites Participating in SIM-Only: ▪ Project Year 1:
Practice sites must achieve Year 1 milestones within building blocks: 1, 2, 3, 4, and 7.
Practice Sites Participating in SIM and CPC+: ▪ Project Year 1:
Practice sites must achieve Year 1 milestones within building blocks: 1, 2, 3, 4, 7, 8, 9, and 10.
Since Cohort 3 practices are only participating in SIM for one year and will be focused on Year 1 milestones to achieve good standing, many practices will enter into SIM with previous work in both quality improvement and behavioral health integration. Practices are encouraged to work on Year 2 milestones if they have already achieved milestones in Year 1, as they reflect sustainable change and continued advancement, but Cohort 3 practices will not be measured on these milestones.
SECTION III. Practice Application
Practice Application Instructions and Questions The SIM Cohort 3 Practice Request for Application (RFA) can be accessed electronically here: http://bit.ly/sim3application. Specific questions related to the Cohort 3 Applications are outlined in SIM Cohort 3 Application Instructions and Questions.
Please note that to be considered for participation in Cohort 3, practice sites must complete the online application by the deadline of January 19, 2018, at 11:59 pm MST. Hard copy or emailed applications will NOT be accepted.
For additional information, questions or concerns email [email protected]; call 303-724-8968.
Practice Site Roster, Key Contacts, and NPIs Applications with incomplete information in the Practice Site Key Contacts and Practice Site Provider Roster sections, including omitted National Provider Identifiers (NPIs), may be considered ineligible.
Each participating practice site is required to have five key contacts on file with SIM: Primary Practice Contact, Practice/Office Manager, Provider Champion, Contact for Payers/Insurance Companies, Health Information Technology (HIT)/Electronic Health Record (EHR) Contact and Primary Healthcare System or Multi-Site Organization Contact. Additionally, including a practice contact for payers or insurance companies will result in more direct communication between your practice and its payers, if applicable. The same person within a practice may fill multiple roles and can be listed as a key contact more than once. It is important that these practice contacts are accurate and up-to-date as specific SIM communications will be directed to the appropriate contact based on the information included in this section of the application.
18 | P a g e
Please note the critical importance of including accurate NPIs and Taxonomy Codes because cost and utilization data from the All-Payer Claims Database (APCD) is driven by accurate attribution of the right patients to the right providers, which begins with having the correct NPIs.
SECTION IV. Practice Application Review & Selection Process
Overview of Practice Application Review The University of Colorado will coordinate a comprehensive, thorough, complete and impartial review of each application received. An incomplete practice application might be disqualified and not considered for review if the required information is not provided.
All applications submitted in response to this RFA will be reviewed and evaluated by a Practice Application Review Committee. Practice sites will be required to meet the basic eligibility criteria outlined in Section I. Practice sites will be evaluated and ranked based on responsiveness of the application. A list of all applications and ranking will be provided to the SIM office. The SIM office will consider payer support and other factors that affect the overall diversity of the cohort and will select practice sites for Cohort 3 based on the recommendations from the Practice Application Review Committee and the payers that participate in the Multi-Payer Collaborative.
Practice Application Review Committee The Practice Application Review Committee will be a multi-stakeholder review panel convened by the University of Colorado for the purpose of making a recommendation to the SIM office regarding practice sites for SIM Cohort 3. The Practice Application Review Committee will comprise subject matter experts. The University of Colorado will adhere to the following guiding principles in convening the review committee: Ensuring there are no conflicts of interest among the reviewers regarding which practice sites are selected (including asking that reviewers who have conflicts to recuse themselves from discussions of specific practice sites), facilitating the independent review of applications, and ensuring the fair and impartial treatment of all applicants. The size of this committee will be dictated by the number of practice applications received.
Practice Application Review and Selection Process The first level of review will be conducted by University staff to determine whether a practice site meets the initial eligibility criteria, including being a primary care practice in Colorado as defined by the IOM. "Non-traditional" primary care practice sites that otherwise meet the requirements will be reviewed by an internal committee convened by the University of Colorado and the SIM office to determine if they meet the definition of primary care.
Recommendations regarding the ranking and mix of practice sites for the third SIM cohort will be determined at an in-person meeting of the reviewers and will be informed by the following process:
1. Each application will be assigned to a primary and secondary reviewer. 2. Each reviewer will be assigned to a set of applications and will have access to a set of
accompanying scoring sheets online. Reviewers will use these scoring sheets to identify the required elements that have been met by the applicant and to assign the application points based on the degree to which the reviewer believes that the applicant meets the required and preferred elements. The point total is the “reviewer score,” which will be used to inform whether the practice site is recommended for participation in SIM.
3. The primary reviewer will present the case at the in-person meeting, and then the secondary

19 | P a g e
reviewer will present any discrepancies in his/her assessment of the practice. 4. The group will then vote on assigning a practice to one of four categories:
i. Strongly recommend ii. Recommend iii. Consider with some concerns iv. Do not recommend at this time
5. The reviewer score will be used to break ties when there are decisions about which practice sites should be included on the recommended list.
The SIM office will make the final determination of which practice sites are included in Cohort 3 based on recommendations from the review committee after considering payer support for each practice and elements needed to ensure a diverse cohort of practice sites.

20 | P a g e
REFERENCES
1. Bodenheimer, T., et al., The 10 building blocks of high-performing primary care. Ann Fam Med,2014. 12(2): p. 166-71.
2. Archer, J., Bower, P., Gilbody, S., Lovell, K., Richards, D., Gask, L., Coventry, P. (2012).Collaborative care for depression and anxiety problems. Cochrane Database of SystematicReviews, (10). doi:10.1002/14651858.cd006525.pub2
3. Butler, M., Kane, R. L., McAlpine, D., Kathol, R. G., Fu, S. S., Hagedorn, H., & Wilt, T. J. (2008).Integration of Mental Health/Substance Abuse and Primary Care. Evidence Reports/TechnologyAssessments, (173).
4. Kwan, B. M., & Nease, D. E. (2013). The State of the Evidence for Integrated Behavioral Health in PrimaryCare. Integrated Behavioral Health in Primary Care, 65-98. doi:10.1007/978-1-4614-6889- 9_5
5. Gallo, J. J. (2004). Primary Care Clinicians Evaluate Integrated and Referral Models of BehavioralHealth Care For Older Adults: Results From a Multisite Effectiveness Trial (PRISM-E). The Annals ofFamily Medicine, 2(4), 305-309. doi:10.1370/afm.116
6. Melek, S. P., Norris, D. T., & Paulus, J. (2014). Economic Impact of Integrated Medical-BehavioralHealthcare. Milliman American Psychiatric Association Report.
7. Franko. (2015, November 21). Measuring Integrated Care: “or trying to weigh a moving wave.”Retrieved from https://cherokeeacademy.wordpress.com/2015/11/21/measuring-integrated- care-or-trying-to-weigh-a-moving-wave/
8. Miller, B. F., Gilchrist, E. C., Brown Levey, S., Gordon, P., Kurtz, P., & Melek, S. (2016). Leveragingalternative payment methodologies in support of comprehensive primary care: Results from the SHAPEevaluation on integrated behavioral health. [Manuscript submitted for publication].
9. Blount, A., Schoenbaum, M., Kathol, R., Rollman, B. L., Thomas, M., O'donohue, W., & Peek, C.J. (2007). The economics of behavioral health services in medical settings: A summary of theevidence. Professional Psychology: Research and Practice, 38(3), 290-297. doi:10.1037/0735-7028.38.3.290
10. Katon, W. J., Lin, E. H., Korff, M. V., Ciechanowski, P., Ludman, E. J., Young, B., . . . Mcculloch,D. (2010). Collaborative Care for Patients with Depression and Chronic Illnesses. New EnglandJournal of Medicine, 363(27), 2611-2620. doi:10.1056/nejmoa1003955

August 2017
Colorado State Innovation Model (SIM) Framework and Milestones “Good standing” is defined as the following for each project year:
Practice Sites participating in SIM-Only:
• Project Year 1: Practice sites must achieve Year 1 milestones within building blocks: 1, 2, 3, 4, and 7.
• Project Year 2: Practice sites must achieve Year 2 milestones within building blocks: 1, 2, 3, 4, 7, and any two additional building blocks.
Practice Sites participating in SIM and CPC+:
• Project Year 1: Practice sites must achieve Year 1 milestones within building blocks: 1, 2, 3, 4, 7, 8, 9, and 10.
• Project Year 2: Practice sites must achieve Year 2 milestones within building blocks: 1, 2, 3, 4, 7, 8, 9, and 10.
BUILDING BLOCK YEAR-1 MILESTONES YEAR-2 MILESTONES GOAL
1 Engaged leadership that
supports integration and
change
• Practice establishes agreement(s) with payer(s) covering at least 150
patients.
• Practice has completed an annual budget that includes SIM revenue and
planned expenses.
• Practice develops quality improvement (QI) team and meets monthly.
• Practice leadership is present at meetings and clinical champion
attends collaborative learning sessions.
• Practice has vision for behavioral health integration, and has identified a
pathway for behavioral health transformation signed by leadership.
• Leadership allocates appropriate resources to complete QI work.
• Practice designs plan to evaluate impact of value-based payment
agreements.
Practice establishes agreement(s)
with payer organization(s) that cover
at least 150 patients across payers,
for value-based payment program(s)
to support practice transformation
under SIM.
2 Practice uses data to
drive change
• Practice successfully submits CQMs quarterly.
• Practice reviews data with practice facilitator (PF)/clinical health information
technology advisor (CHITA) quarterly.
• Practice begins using model for improvement and has identified opportunities
for improvement using CQM data.
• Practice begins using a data aggregation tool provided by SIM to review cost
and utilization data.
• Practice reviews CQM data to inform rapid cycle improvement
processes.
• Practice develops processes for providing performance feedback to
providers, including CQM, cost, and utilization data.
• Practice conducts regular PDSA/QI activities on identified CQMs.
Practice uses EHR clinical quality
measures to provide quarterly
panel reports on all SIM measures
not extracted through claims data;
uses claims data provided through
a data aggregation tool to inform
QI processes.
3 Practice population is
empaneled
• Practice has assessed patient panel and assigned primary care providers/care
teams to 75% of patient population.
• Practice reviews payer attribution lists monthly.
• Practice designs and implements process for validating primary care provider/
care team assignment with patients.
• Practice maintains 75% empanelment of patients with provider/care
teams.
• Practice develops policies to support empanelment, including definitions,
changing PCPs, assigning new patients, and ensuring continuous coverage.
Practice has, and maintains, at
least 75% of its patient population
empaneled.
August 2017
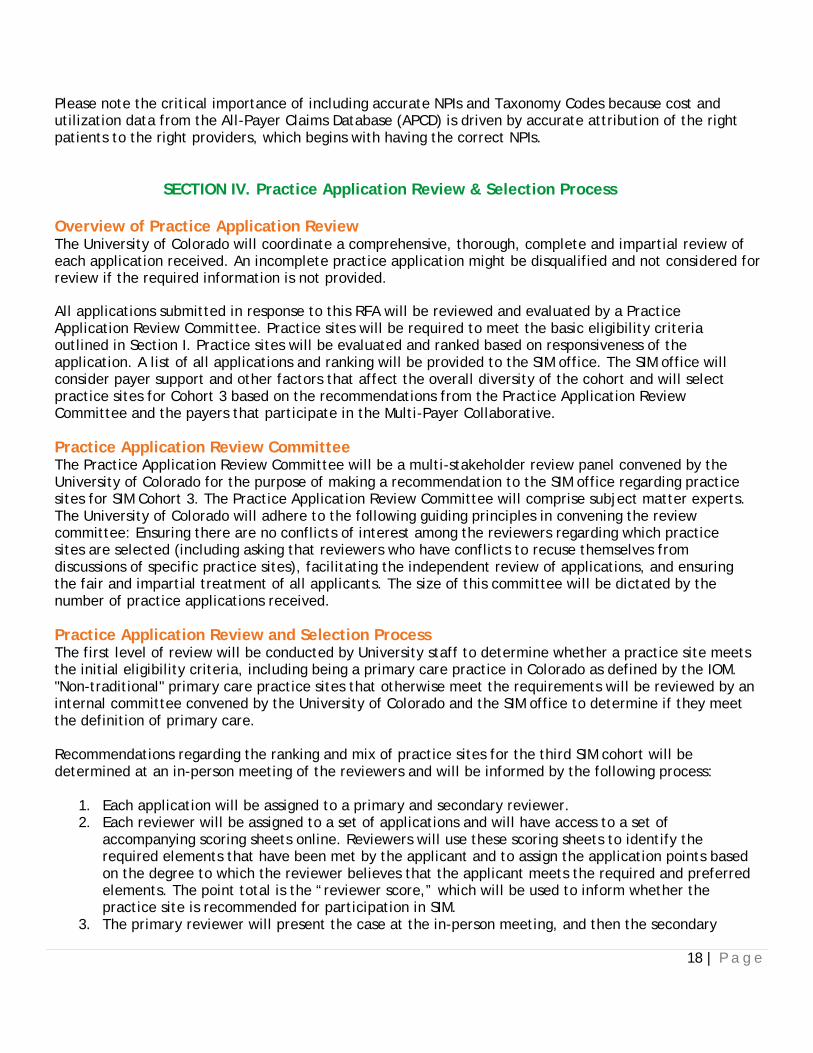
BUILDING BLOCK YEAR-1 MILESTONES YEAR-2 MILESTONES GOAL
4 Practice provides
team-based care
• Practice uses established tool to assess baseline team relationships.
• Practice has written job descriptions, including clear roles andresponsibilities.
• Practice identifies and implements a team-based care strategy (team
huddle, collaborative care planning).
• Practice reevaluates team relationship using tool from Year 1.
• Practice develops protocols for shared workflows for three quality
measures (with at least one behavioral health measure).
• Practice reviews roles/responsibilities for team-based care activities
to ensure accountability for various tasks assigned.
The care team uses shared operations,
workflows, and protocols to facilitate
collaboration and consistently
implements specific shared workflows
rather than informal processes for
at least three measures, including at
least one behavioral health measure.
5 Practice has built
partnership with patients
• Practice evaluates patient population to identify one preference-sensitive
condition that is appropriate for decision aids or self-management support
tools.
• Practice identifies and selects evidence-based decision aids or self-
management support tools for identified conditions.
• Practice has established a Patient and Family Advisory Council (PFAC) and
meets at least quarterly.
• Practice identifies patients and families eligible for selected decision aids
or self-management support tools.
• Practice implements decision aids or self-management support tools and
establishes protocol and workflow for use.
• Practice develops process for tracking and evaluating use of decision aids
or self-management support tools.
• Practice uses PFAC to evaluate care experience.
Practice has established use of
evidence-based shared decision-
making aids or self-management
support tools for at least one,
preference-sensitive condition, and
tracks the use of these tools.
Practice has established a PFAC to
provide input and feedback on
practice transformation activities and
progress.
6 Practice risk stratifies
and actively manages patient population using data
• Practice identifies, documents a risk stratification methodology.(Recommended, but not required for pediatric practices)
• Practice identifies strategy to identify care gaps (e.g. patient registry, data
aggregation tool) and prioritize high-risk patients/families.
• 75% of empaneled patients are risk-stratified. (Recommended, but notrequired for pediatric practices)
• 75% of high-risk patients/families have a documented care plan.
• Practice implements proactive care gap management and tracks
outcomes.
• Practice embeds care plan template in EHR.
Practice uses population-level data
to manage care gaps, develop care
management care plans and
implement those plans for high-risk
patients/ families.
7 Practice screens for
behavioral health and substance use disorders and links primary care to behavioral health and social services
• Practice identifies behavioral health resources for patients/families,
including support from SIM participating health plans and Regional
Health Connectors (RHCs).
• Practice identifies a screening tool for reporting on at least two
behavioral health screening measures for SIM (depression, maternal
depression, developmental disorders, obesity, and substance use disorders
[i.e., unhealthy alcohol use, other drug dependence, and tobacco use]);
screens 25% of patients.
• Practice has documented process for connecting patients/families with
behavioral health resources (from screening), including standing orders and
or/protocols and follow-up.
• 50% of patients are screened for behavioral health conditions.
• Practice performs an assessment of community resources, with
Regional Health Connector support when possible, to assist
patients/families with social needs (such as food, housing,
transportation).
• 50% of patients identified with behavioral health need are connected to
resource.
Practice screens at least 90% of
appropriate patients/families for
substance use disorder and/or other
behavioral health needs, and includes
behavioral health and community
services as part of care management
strategies.

August 2017
BUILDING BLOCK YEAR-1 MILESTONES YEAR-2 MILESTONES GOAL
8 Practice provides
prompt access to care,
including behavioral
healthcare
• Practice has representative with EHR access available 24 hours, 7 days per
week.
• Practice performs an assessment of referral pathways and available after-
hours support for behavioral health, working with RHCs when possible.
• Practice identifies data sources and technology necessary for bi-directional
data sharing.
• Practice has established a collaborative agreement with at least one
behavioral health provider.
• Practice develops plan for bi-directional data sharing with behavioral
health provider.
Practice, at a minimum, has
established collaborative care
management agreements with
behavioral health providers in the
community and members of the care
team can articulate how to use those
agreements.
Practice has ability to share clinical
data based on collaborative care
management agreements with
behavioral health providers bi-
directionally within 7 days.
9 Practice provides
comprehensive care coordination
for primary/behavioral
healthcare
• Practice can identify total cost of care for patient panel, and subset of
patients with behavioral health conditions.
• Practice identifies and implements policy and procedures that include
timely follow-up for emergency department (ED) and hospital admissions.
• Practice contacts 50% of patients within 7 days of hospitalization or ED
visit, including medication reconciliation.
• Practice identifies cost drivers for patients with behavioral health
condition(s) and incorporates in QI processes.
• Practice creates and reports a measurement to assess impact and guide
improvement on at least one of the following:
1. Notification of ED visit in a timely fashion
2. Medication reconciliation process completed within 72 hours
3. Notification of admission and clinical information exchange at the time
of admission
4. Information exchange between primary care and specialty care related
to referrals
Practice has reduced total cost of
care while maintaining or improving
quality of care for patients, including
those with depression and substance
use disorders, compared with non-SIM
practices.
10 Practice has fully
integrated behavioral
healthcare to provide
whole-person care
• Practice uses referral pathway identified for behavioral health
needs (including available after-hours support and a representative
with EHR access available 24 hours, 7 days per week).
• Practice develops a plan to systematically measure and track patient
behavioral health outcomes.
• Practice develops care plans that include patient actions to manage
behavioral health conditions.
• Practice systematically measures and tracks patient behavioral health
outcomes.
• Practice documents and implements protocols to identify and manage care
for high-risk behavioral health populations.
• Practice identifies and implements at least two opportunities to adjust its
protocols to improve behavioral health status of patients.
• Practice demonstrates advanced access to behavioral health services.
Patient behavioral health outcomes
are systematically measured over
time and treatment is adjusted as
needed, as measured by outreach,
registry and other information readily
available for purpose of monitoring
and adjustment.

1
Colorado State Innovation Model (SIM) Clinical Quality Measures (CQMs)
Reporting Summary

2
SIM Clinical Quality Measure (CQM) Reporting Schedules: Cohort 3
Table of Contents
Reporting Schedules ..................................................................................................................................................................................... 3
SIM Cohort 3 Practice Sites Participating in SIM Only ............................................................................................................................................. 3
Adult Practice Sites .............................................................................................................................................................................................. 3
Pediatric Practice Sites ......................................................................................................................................................................................... 3
SIM Cohort 3 Practice Sites Participating in CPC+ .................................................................................................................................................... 3
Adult Practice Sites .............................................................................................................................................................................................. 4
SIM CQM Measure Sets ................................................................................................................................................................................ 5
Adult Measure Set ................................................................................................................................................................................................... 5
Pediatric Measure Set .............................................................................................................................................................................................. 6
SIM/CPC+ Measure Set ............................................................................................................................................................................................ 7
Summary of Reporting Requirements ........................................................................................................................................................... 8
CPC+ CQM Reporting Requirements........................................................................................................................................................................ 9
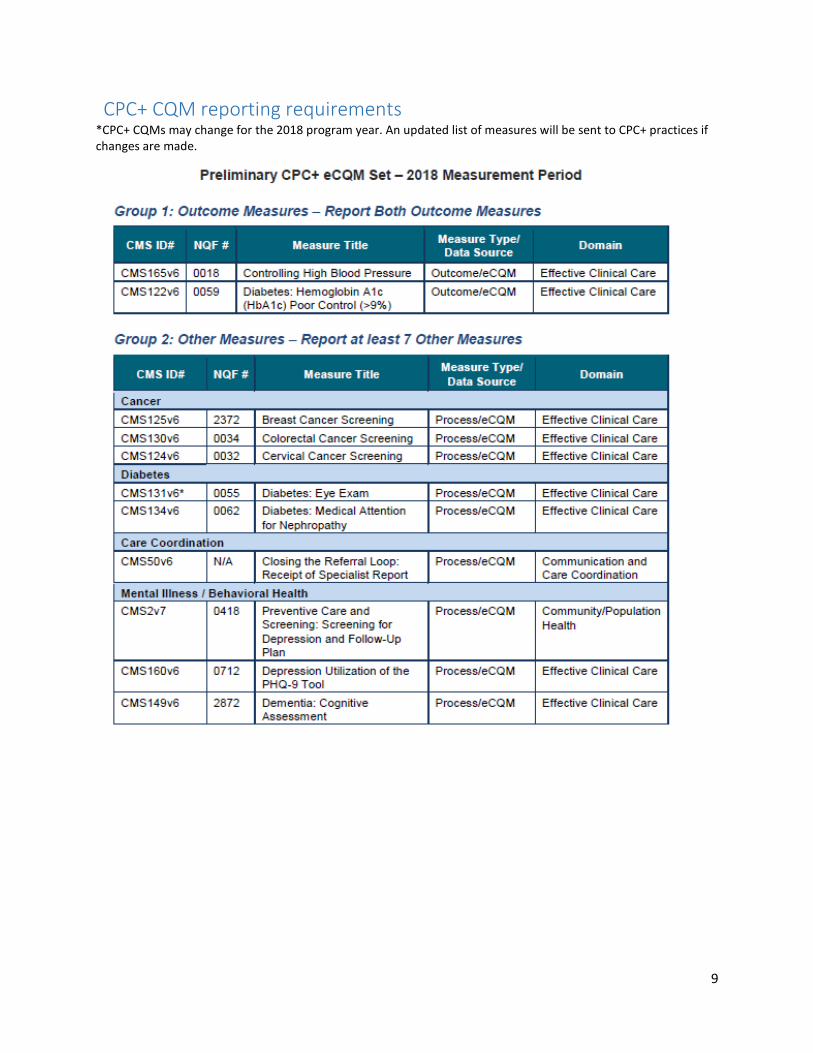
SIM CQM Measurement Periods .......................................................................................................................................................................... 11
SIM NPI and Taxonomy Code Update and Attribution Fact Sheet................................................................................................................. 14
SIM Attribution Model Summary ................................................................................................................................................................ 16

3
Cohort 3 CQM Reporting Schedules
SIM Cohort 3 Practice Sites Participating in SIM Only
Adult Practice Sites
2018 Q3 (Jul-Sep 18) 2018 Q4 (Oct-Dec 18) 2019 Q1 (Jan-Mar 19) 2019 Q2 (Apr-Jun 19) Test period, practice sites report whatever they can
Choose 3 primary CQMs: Depression Screening
Diabetes: Hemoglobin A1c
Hypertension
Obesity: Adult SUD: Alcohol & Other Drug
Dependence
SUD: TobaccoSecondary CQMs (if needed):
Asthma (new)
Fall Safety
Maternal Depression Screening
SUD: Alcohol= 3 total CQMs required
Choose 4 primary CQMs: Depression Screening
Diabetes: Hemoglobin A1c
Hypertension
Obesity: Adult SUD: Alcohol & Other Drug
Dependence
SUD: TobaccoSecondary CQMs (if needed):
Asthma (new)
Fall Safety
Maternal Depression Screening
SUD: Alcohol= 4 total CQMs required
Choose 5 primary CQMs: Depression Screening
Diabetes: Hemoglobin A1c
Hypertension
Obesity: Adult SUD: Alcohol & Other Drug
Dependence
SUD: TobaccoSecondary CQMs (if needed):
Asthma (new)
Fall Safety
Maternal Depression Screening
SUD: Alcohol= 5 total CQMs required
Pediatric Practice Sites
2018 Q3 (Jul-Sep 18) 2018 Q4 (Oct-Dec 18) 2019 Q1 (Jan-Mar 19) 2019 Q2 (Apr-Jun 19) Test period, practice sites report whatever they can
Choose 2 primary CQMs: Depression Screening
Developmental Screening
Maternal Depression Screening
Obesity: AdolescentSecondary CQMs (if needed):
Asthma (new)= 2 total CQMs required
Choose 3 primary CQMs: Depression Screening
Developmental Screening
Maternal Depression Screening
Obesity: AdolescentSecondary CQMs (if needed):
Asthma (new)= 3 total CQMs required
Report all 4 primary CQMs: Depression Screening
Developmental Screening
Maternal Depression Screening
Obesity: AdolescentSecondary CQMs (if needed):
Asthma (new)= 4 total CQMs required

4
SIM Cohort 3 Practice Sites Participating in CPC+ (see Appendix A for full list of CPC+ CQM reporting requirements)
Adult Practices Sites
2018 Q3 (Jul-Sep 18) 2018 Q4 (Oct-Dec 18) 2019 Q1 (Jan-Mar 19) 2019 Q2 (Apr-Jun 19) Test period, practice sites report whatever they can
Choose 3 primary CQMs:
Depression:a) Depression Screening (SIM/QPP) ORb) Depression Remission at 12
months (CPC+ group 1)
Diabetes: Hemoglobin A1c (CPC+group 1 & SIM/QPP)
Hypertension (CPC+ group 1 & SIM/QPP) SUD: Alcohol & Other Drug
Dependence (CPC+ group 2 &SIM/QPP)
SUD: Tobacco (CPC+ group 3 &SIM/QPP) Secondary CQMs (if needed):
Asthma (SIM/QPP)
Fall Safety (CPC+ group 2 & SIM/QPP)
Maternal Depression Screening
(SIM/QPP)
SUD: Alcohol (SIM/QPP)= 3 total CQMs required
Choose 4 primary CQMs:
Depression:a) Depression Screening ORb) Depression Remission at
12 months
Diabetes: Hemoglobin A1c
Hypertension
SUD: Alcohol & OtherDrug Dependence
SUD: TobaccoSecondary CQMs (if needed):
Asthma
Fall Safety
Maternal Depression Screening SUD: Alcohol
= 4 total CQMs required
Report all 5 primary CQMs:
Depression:a) Depression Screening ORb) Depression Remission at 12
months
Diabetes: Hemoglobin A1c
Hypertension
SUD: Alcohol & Other DrugDependence
SUD: Tobacco SecondaryCQMs (if needed):
Asthma
Fall Safety
Maternal Depression Screening SUD: Alcohol
= 5 total CQMs required

5
SIM Clinical Quality Measure Set
Specifications and guidance found in SIM CQM Guidebook
Adult Measure Set
Measure Condition SIM Metric Title Citation CPC+ QPP
Primary CQMs Depression Preventive Care and Screening: Screening for
Clinical Depression and Follow-up Plan NQF 0418 CMS 2v6
Depression Remission at 12 Months
Diabetes: Hemoglobin A1c Diabetes: Hemoglobin A1c Poor Control NQF 0059 CMS 122v5
Hypertension Controlling High Blood Pressure NQF 0018 CMS 165v5
Obesity: Adult Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-up Plan
NQF 0421 CMS 69v5
No obesity measure (not required for SIM if in CPC+)
Substance Use Disorder: Alcohol and Other Drug Dependence
Initiation & Engagement of Alcohol & Other Drug Dependence Treatment
NQF 0004 CMS 137v5
Substance Use Disorder: Tobacco Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
NQF 0028 CMS 138v5
Secondary CQM Asthma Medication Management for People with
Asthma NQF 1799 CMS n/a
No asthma measure
Fall Safety Falls: Screening for Future Fall Risk NQF 0101 CMS 139v5
Maternal Depression Maternal Depression Screening NQF 1401 CMS 82v4
No maternal depression measure
Substance Use Disorder: Alcohol Preventive Care and Screening: Unhealthy Alcohol Use: Screening & Brief Counseling
NQF 2152 CMS n/a
Alcohol & Other Drug Dependence measure (above)
Measures reported via APCD claims data automatically
Breast Cancer Breast Cancer Screening NQF 2372 CMS 125v5
(clinical) (clinical)
Colorectal Cancer Colorectal Cancer Screening NQF 0034 CMS 130v5
(clinical) (clinical)

6
Pediatric Measure Set
Measure Condition Metric Title Citation QPP
Primary CQMs
Depression Preventive Care and Screening: Screening for Clinical Depression and Follow-up Plan
NQF 0418 CMS 2v6
Development Screening Developmental Screening in the First Three Years of Life (developed by Mathematica)
NQF 1448 CMS 664
No developmental screening measure
Maternal Depression Maternal Depression Screening NQF 1401 CMS 82v4
Obesity: Adolescent Weight Assessment and Counseling for Nutrition and Physical Activity for Children and Adolescents
NQF 0024 CMS 155v5
Secondary CQM
Asthma Medication Management for People with Asthma NQF 1799 CMS n/a

7
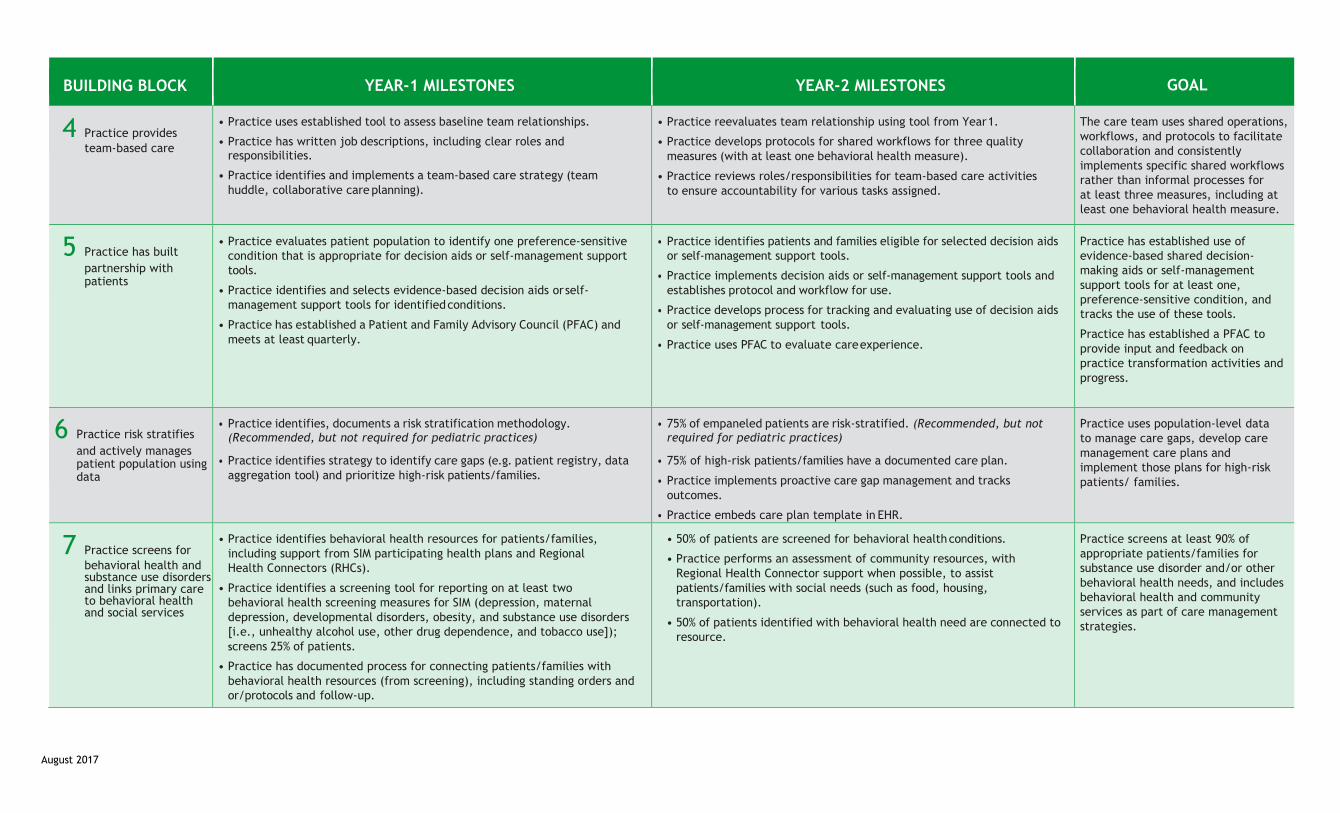
CPC+ CQMs that count for SIM (see Appendix A for full list of PRELIMINARY CPC+ CQM reporting requirements) *CPC+ CQMs may change for the 2018 program year. An updated list of measures will be sent to CPC+ practices if changes are made.
Measure Condition Metric Title Citation
Group 1
Depression Depression Remission at Twelve Months (OR SIM depression measure above)
NQF 0710 CMS 159v5
Diabetes: Hemoglobin A1c Diabetes: Hemoglobin A1c Poor Control NQF 0059 CMS 122v5
Hypertension Controlling High Blood Pressure NQF 0018 CMS 165v5
Group 2
Fall Safety Falls: Screening for Future Fall Risk NQF 0101 CMS 139v5
Substance Use Disorder: Alcohol and Other Drug Dependence
Initiation and Engagement of Alcohol and Other Drug Dependence Treatment
NQF 0004 CMS 137v5
Group 3 Substance Use Disorder: Tobacco Preventive Care and Screening: Tobacco Use: Screening and
Cessation Intervention NQF 0028 CMS 138v5
Breast Cancer Breast Cancer Screening (SIM reported via claims) NQF 2372 CMS 125v5
Colorectal Cancer Colorectal Cancer Screening (SIM reported via claims) NQF 0034 CMS 130v5

8
Summary of Reporting Requirements
Primary vs. Secondary Primary measures are the focus areas where SIM aims to move the needle over the course of
the initiative. Secondary measures are still important, and can be reported, but practice sitesshould focus their practice transformation and data quality efforts on the primary measures.Practice sites will make a good faith effort to report on all primary CQMs for SIM.
If practice sites cannot report a primary CQM in a given quarter, the practice site should select asecondary CQM to report in its place. Practice sites should work with their Clinical HealthInformation Technology Advisor (CHITA) to report all primary CQMs in future quarters. Practicesites are encouraged to work with their CHITA to report on all SIM CQMs, including thesecondary CQMs, over time and should phase them in as appropriate. Additionally, some payersmay ask for secondary CQMs as part of their APM contracts with practices, and practices shouldwork with their CHITAs to understand specific payer reporting requirements and submit thosefor SIM.
Measurement Period Practice sites will report using a trailing year measurement period. If this is not possible, practice
sites will report using a year-to-date (YTD) measurement period. For more information, pleasesee this guidance: http://www.practiceinnovationco.org/wp-content/uploads/2017/01/Changing-SIM-CQM- measurement-period.pdf
For Q4 reporting, practice sites should submit clinical quality measure data from the fullcalendar year January 1 – December 31 (note, trailing year and YTD measurement period areidentical for reporting periods ending December 31 of a given year). This annual CQM report willbe shared with payers who support your practice.
SIM Practice Sites Participating in CPC+ Where applicable, CPC+ measures will count for SIM reporting. SIM will require CPC+ practice
sites to choose the behavioral health measures within each of the 3 CPC+ reporting groups.CPC+ practices are not required to report any additional CQMs for SIM, unless they do notreport the SIM measures within CPC+ reporting groups.
CPC+ practice sites will report metrics in SPLIT for SIM in addition to any required reporting forCPC+ through the CPC+ submission portal or MIPS submission portal. All SIM participatingpractice sites, including CPC+ practice sites, will report CQMs quarterly for SIM, which willfacilitate their preparations for the annual CPC+ report.
9
CPC+ CQM reporting requirements *CPC+ CQMs may change for the 2018 program year. An updated list of measures will be sent to CPC+ practices ifchanges are made.

10
CPC+ CQM reporting requirements *CPC+ CQMs may change for the 2018 program year. An updated list of measures will be sent to CPC+ practices ifchanges are made.
11
SIM CQM measurement period Summary
Practice sites and CHITAs trust annual, full calendar year (Jan - Dec) CQM data; this aligns with
CPC+ and guidance on most NQF/CMS endorsed standards.
The ability to “choose” a measurement period varies widely across EHRs used in SIM practices;
some EHRs only support year-to-date (YTD) reporting, others only support trailing year
reporting, others have more flexible functionality to choose a number of measurement periods.
Practice sites will report CQMs using either a trailing year or YTD measurement period; trailing
year is preferred and YTD is back-up if trailing year is not possible.
Practice sites will report quarterly CQM data for SIM; this allows for real-time data to inform
QI, for practices to gain experience reporting CQMs in preparation for the annual report, and to
identify gaps and issues with CHITAs and remedy prior to “official” full calendar year (Q4)
report.
The Q4 report will serve as the full calendar year (Jan – Dec) report.
Full calendar year (Jan - Dec) CQM report data will be shared with payers that are supporting
the practice site through SIM once annually.
Practice sites/CHITAs will be able to indicate which approach (YTD or trailing year) they are
using when they report CQMs each quarter in SPLIT.
Quarterly measurement of data Currently SIM practices are reporting data quarterly using different measurement periods. In SPLIT, practice sites record the measurement period that CQMs were generated by and whether the standard SIM measure specifications (“standard” – trailing year) were used to generate the CQMs. If a measure is not generated using the “standard” specifications, practices select “alternative” and provide details on how the measure was calculated.
Practice representatives are concerned about how the quarterly data will be used (for payment, benchmarks, etc.). The SIM Office will communicate to payers that practice sites are in “good standing,” signifying that practices are reporting CQMs each quarter (among other milestones). The SIM office will only share practice-site CQM data with payers annually using the data entered in Q4 for the Jan 1 - Dec 31 measurement period.

12
Alternative options
Trailing year Year-to-date (YTD)
**Preferred approach** “Backup” option - if practices are unable to
reporting using trailing year they can report YTD
365-day measurement period immediately prior
to the last day of the current reporting quarter
Measurement period is from the start of the
calendar year to the last day of the current
reporting quarter
For SIM Q4 2018, report 1/1/18– 12/31/18 For SIM Q4 2018, report 1/1/18 – 12/31/18
Pros: This approach is more predictive of end of
year performance and matches the measure
stewards’ intent.
Cons: This approach is slow to respond to process
improvement and most EHRs don’t provide this
function.
Pros: Most EHRs can report utilizing this
approach in a MU dashboard.
Cons: Denominators change during the year
(getting larger as the year goes on), and variable
lookback causes nonsensical results for several of
the CQMs. Most practices don’t trust the data
until at least Q3.
Trailing year measurement periods are more reflective of true performance, stable over time, and
trusted by practice representatives and CHITAs than 90-day and YTD measurement periods. Trailing
year and YTD are both easier to pull reports from EHRs than 90-day reports.
There is mixed feedback about which approach is best from a quality improvement (QI) perspective.
While there is some indication that YTD is easier to report, trailing year may be more meaningful for
practices. However, some EHR vendors only support YTD reporting while other vendors only support
trailing year reporting. Therefore, the SIM Office needs to allow for flexibility in practice CQM
reporting.

13
Continued quarterly reporting
Practices need a leading indicator of year-end CQM performance so that they can assess
the results of QI efforts. A good leading indicator should predict performance at the end
of the year when CQMs are submitted to payers (and CMMI).
Quarterly CQM reporting is not very effective as the sole QI tool. Practices are encouraged to use data
to manage their patient populations, guide QI activities, and track performance. SIM, like CPC classic,
supports practices in optimizing patient registries (i.e. diabetes, depression, preventive services) and
coaches practices how to use plan-do-study-act reviews on actionable data.
SIM will maintain quarterly CQM reporting for practices. The goal is to work toward data quality and increase trust in the data. CHITAs and practice representatives should use the quarterly reports to “practice” reporting the CQMs, identify any gaps or issues, and shore up quality of the quarterly data in preparation for the annual report shared with payers.
Quarterly CQM reporting will also help prepare practices for the federal quality payment program (QPP) that has been introduced through the MACRA final rule. While calendar year (Jan – Dec) is the measurement period for QPP, CMS is allowing for a minimum 90-day report. It is unclear how CMS is handling measurement period for partial year reporting. Quarterly CQM reporting for SIM will allow practices to improve data quality for annual QPP and CPC+ reporting for practices participating in both initiatives.
How CQMs will be used/shared
The primary purpose of reporting CQMs is to provide real-time, actionable data for practice QI processes. Additionally, full calendar year CQM data will be provided to payers. Payers are applying organization-specific payment model(s) and establishing their own agreements with participating SIM practices. The use of CQM data in value-based payment arrangements will be determined by each payer individually, and outlined in the agreement with the practice. Lastly, quarterly CQM data will be included in quarterly reports to CMMI and included in the evaluation. Quarterly reporting will allow practices and CHITAs to improve data quality and create trust in the data.
The SIM Office will report to payers that practice sites are in “good standing” for SIM, which includes completing quarterly CQM reporting requirements (among other milestones). CQM data will only be shared with payers for the practices they support once annually.
SIM NPI and Taxonomy Codes Update and Attribution Fact Sheet
How are your individual NPI number and taxonomy code used in SIM?
Your individual National Provider Identifier (NPI) plays a significant role in how SIM identifies your
patients, and their corresponding claims data, in the Colorado All Payer Claims Database (APCD). The
process of connecting you with your patients, which is called attribution, is outlined for SIM purposes in
this document. Providing complete and accurate NPIs allows SIM to calculate cost and utilization data
which is reported back to your practice site.
APCD claims data from each patient’s insurance plan(s) are attributed to SIM providers and used to
calculate cost and utilization reports for each SIM practice site. This is done by matching individual NPIs
submitted by your practice in the SIM practice roster with the individual NPI for the healthcare
provider found in APCD claims.
Another important provider database descriptor is your taxonomy code associated with your individual
NPI in the National Plan and Provider Enumeration System (NPPES). This code associates you with the
specialty most applicable to your professional status. NPPES is an important tool used by many health
plans, credentialing entities and government programs for attribution. The fastest way to update and
confirm NPPES information is to go online.
In the current SIM practice roster individual NPIs and taxonomy codes are incorrect, out of date or
associated with a provider type that might not be included in the SIM attribution model. Your
individual NPI is a unique, one-time and sustained identifier, so it shouldn’t change over time unless
your profession changes (e.g., a practicing physician’s assistant attends medical school and becomes a
doctor).
However, your taxonomy code will change. For example, a medical resident’s taxonomy code reflects
his or her status as a “Student in an Organized Health Care Education/Training Program” (390200000X).
Once residency is completed, the taxonomy code should be changed to reflect specialty, e.g. Family
Medicine (207Q00000X). Taxonomy codes are used in the SIM attribution process to identify SIM-
designated primary care providers, a category that includes the following: physicians, nurse
practitioners, physician assistants, clinical nurse specialists. SIM primary care specialties include: family
medicine, internal medicine, pediatrics, and geriatric medicine.
Patients are attributed to obstetrics/gynecology (OB/GYN) in a secondary attribution run if they were
not first attributed to a primary care provider.
For SIM purposes, if your individual NPI or taxonomy code is incorrect or out-of-date, your patients

might be attributed to another provider by the initiatives attribution process. With a zero or a limited
number of attributed patients, the SIM program cannot generate accurate cost and utilization reports
for your practice site.
What can you do to correct your individual NPIs and taxonomy codes?
Some SIM practice rosters only include individual NPIs for a portion of providers in the practice site. If
your SIM practice roster only includes four NPIs and your practice site has eight providers, there will be
an incomplete number of patients attributed to your practice and incomplete cost and utilization data
reported back to your practice site.
Additionally, updating NPPES information to reflect current provider status improves the accuracy of
SIM’s attribution and thereby the cost and utilization reports delivered to practices. On a broader note,
NPPES is viewed as a primary source for provider status and information. Keeping NPPES regularly
updated helps to ensure accuracy in all sorts of professional databases.
Why update your group or organization NPIs for SIM?
When an individual provider NPI is not available on a claim, the provider's group or organization NPI can
be used to determine attribution. The group or organization NPI also provides insight into the SIM
practice site unit of analysis. Since SIM is working with practice sites versus entire practice organizations,
the group or organization NPI helps determine which providers belong to your practice site.
The group or organization NPI also allows patients to be attributed to SIM participating clinics or centers
that operate under prospective payments such as: federally-qualified health centers (FQHCs), rural
health, community health, public health (federal, state or local), and student health.
If your practice bills Medicare or Medicaid, you have a group or organization NPI and group or
organization taxonomy data in NPPES. Groups should update their information in the same fashion as
individual practitioners on this site: https://nppes.cms.hhs.gov/NPPES/Welcome.do.
Tips for updating your SIM practice roster:
Include individual NPIs for all providers at your practice site to achieve the most accurate
attribution and most complete cost and utilization reports.
Refer to taxonomy code table linked in the SIM practice roster to update your taxonomy codes.
Update your information in the NPPES.
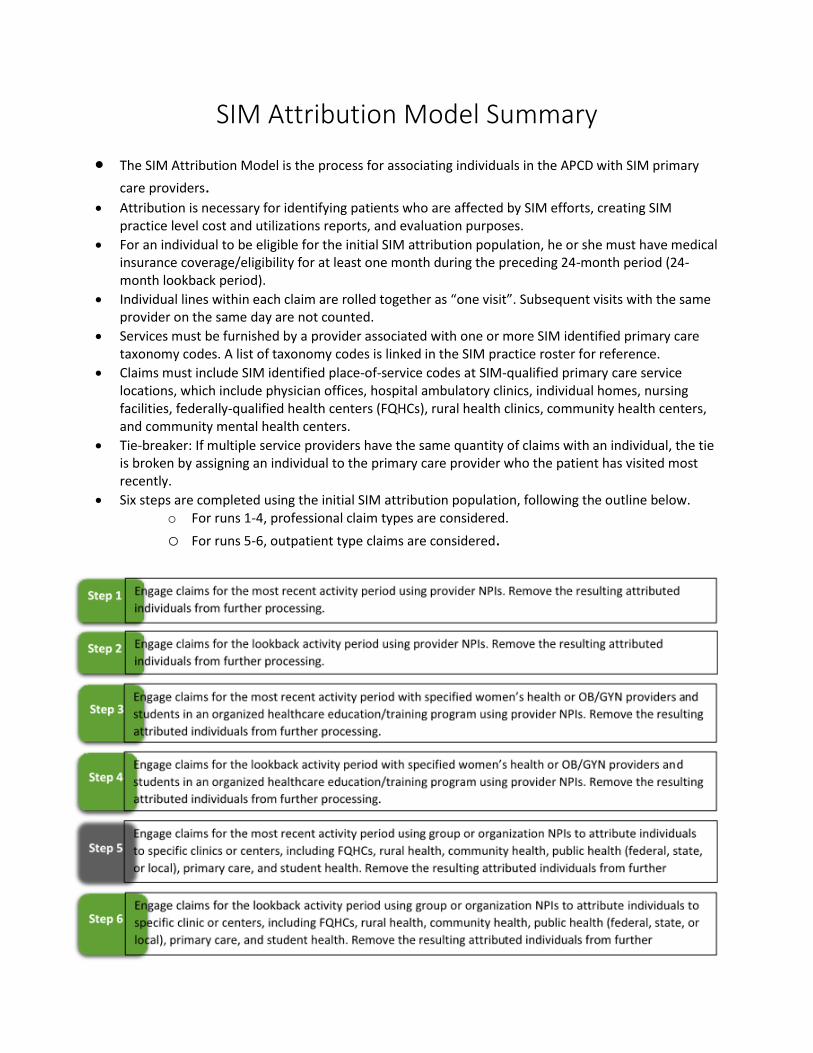
SIM Attribution Model Summary
The SIM Attribution Model is the process for associating individuals in the APCD with SIM primary
care providers. Attribution is necessary for identifying patients who are affected by SIM efforts, creating SIM
practice level cost and utilizations reports, and evaluation purposes.
For an individual to be eligible for the initial SIM attribution population, he or she must have medicalinsurance coverage/eligibility for at least one month during the preceding 24-month period (24-month lookback period).
Individual lines within each claim are rolled together as “one visit”. Subsequent visits with the sameprovider on the same day are not counted.
Services must be furnished by a provider associated with one or more SIM identified primary caretaxonomy codes. A list of taxonomy codes is linked in the SIM practice roster for reference.
Claims must include SIM identified place-of-service codes at SIM-qualified primary care servicelocations, which include physician offices, hospital ambulatory clinics, individual homes, nursingfacilities, federally-qualified health centers (FQHCs), rural health clinics, community health centers,and community mental health centers.
Tie-breaker: If multiple service providers have the same quantity of claims with an individual, the tieis broken by assigning an individual to the primary care provider who the patient has visited mostrecently.
Six steps are completed using the initial SIM attribution population, following the outline below.o For runs 1-4, professional claim types are considered.
o For runs 5-6, outpatient type claims are considered.
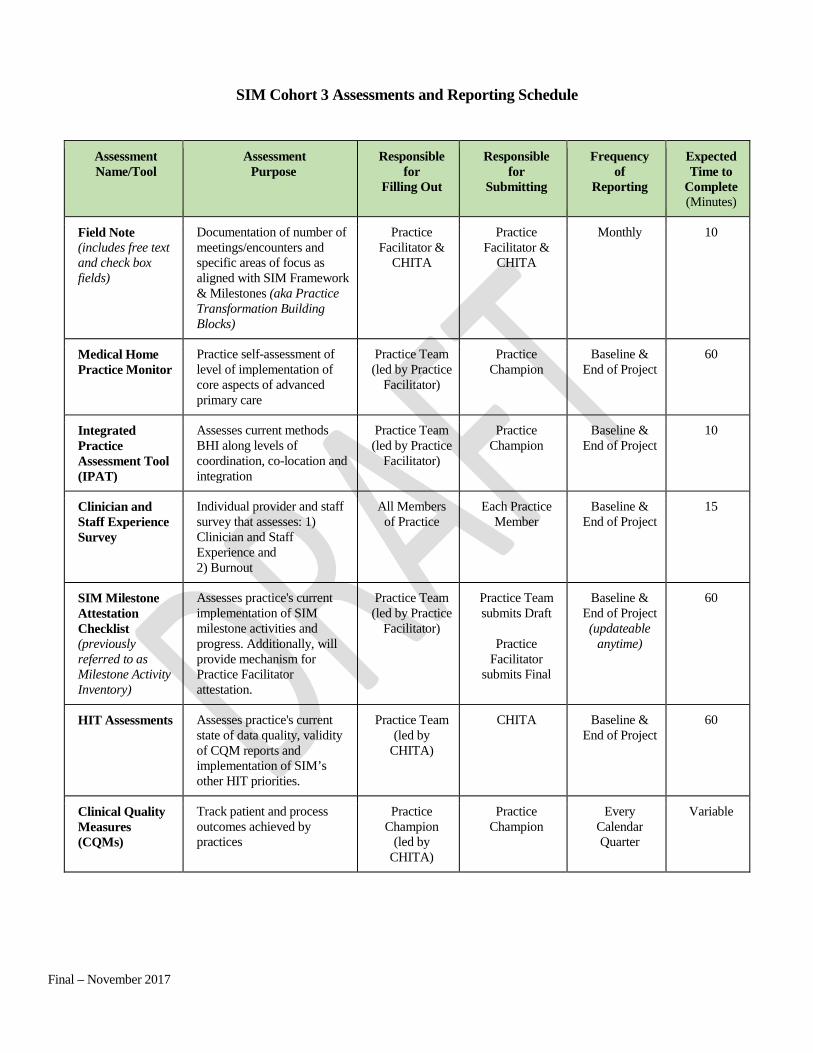
Final – November 2017
SIM Cohort 3 Assessments and Reporting Schedule
Assessment Name/Tool
Assessment Purpose
Responsible for
Filling Out
Responsible for
Submitting
Frequency of
Reporting
Expected Time to
Complete (Minutes)
Field Note (includes free text and check box fields)
Documentation of number of meetings/encounters and specific areas of focus as aligned with SIM Framework & Milestones (aka Practice Transformation Building Blocks)
Practice Facilitator &
CHITA
Practice Facilitator &
CHITA
Monthly 10
Medical Home Practice Monitor
Practice self-assessment of level of implementation of core aspects of advanced primary care
Practice Team (led by Practice
Facilitator)
Practice Champion
Baseline & End of Project
60
Integrated Practice Assessment Tool (IPAT)
Assesses current methods BHI along levels of coordination, co-location and integration
Practice Team (led by Practice
Facilitator)
Practice Champion
Baseline & End of Project
10
Clinician and Staff Experience Survey
Individual provider and staff survey that assesses: 1) Clinician and Staff Experience and 2) Burnout
All Members of Practice
Each Practice Member
Baseline & End of Project
15
SIM Milestone Attestation Checklist (previously referred to as Milestone Activity Inventory)
Assesses practice's current implementation of SIM milestone activities and progress. Additionally, will provide mechanism for Practice Facilitator attestation.
Practice Team (led by Practice
Facilitator)
Practice Team submits Draft
Practice Facilitator
submits Final
Baseline & End of Project (updateable
anytime)
60
HIT Assessments Assesses practice's current state of data quality, validity of CQM reports and implementation of SIM’s other HIT priorities.
Practice Team (led by
CHITA)
CHITA Baseline & End of Project
60
Clinical Quality Measures (CQMs)
Track patient and process outcomes achieved by practices
Practice Champion
(led by CHITA)
Practice Champion
Every Calendar Quarter
Variable
1
State Innovation Model (SIM) Practice Transformation Practice Letter of Agreement to Participate
This agreement (“Agreement” or “Contract”) is made between _________________ (“Practice” or “Contractor”)
and The Regents of the University of Colorado, a body corporate, on behalf of the University of Colorado Denver
(“University”), together hereinafter “the parties”.
RECITALS
Whereas, The State of Colorado will receive up to $65 million from the Center for Medicare and Medicaid Innovation (CMMI) to implement and test its State Health Care Innovation Plan under a Cooperative Agreement commonly referred to as the Colorado State Innovation Model (SIM);
Whereas, The University of Colorado will have funds made available from SIM to provide practice transformation support to approximately 400 primary care practices located in Colorado; and
Whereas, Practice has been selected by the Colorado SIM Office to receive practice transformation support from the University of Colorado.
Now therefore, the parties agree as follows:
1. TERM.This agreement shall be effective on July 1, 2018 or the date of the last signature below whichever is earlier and shall remain in effect until July 31, 2019 unless terminated earlier by one or both of the parties in accordance with the termination clause in Section 5.
2. PRACTICE TRANSFORMATION SUPPORT.Practice will be provided with a Practice Facilitator (PF) and a Clinical Health Information Technology Advisor (CHITA) to deliver a comprehensive, personalized package of support that will allow practices to successfully realize SIM Initiative goals. In addition, a Regional Health Connector (RHC) will be available to connect Practice with community and state resources.
Practice will receive the following practice transformation support provided or coordinated by the University:
1. Support from a Practice Facilitator (PF) over the course of this Agreement to:a. Assist Practice in developing a Quality Improvement (QI) Team.b. Meet with Practice QI Team at least once monthly to implement improvements based
on the practice transformation building blocks as outlined in the SIM Framework andMilestones.
SIM Cohort 3 Practice Participation Agreement - Draft

2
c. Engage with Practice at least twice monthly (including meeting with Practice QI Team atleast once monthly) to implement improvements based on the practice transformationbuilding blocks as outlined in the SIM Framework and Milestones.
d. Assist Practice with completion of assessments as outlined in the SIM Cohort 3Assessments and Reporting Schedule.
e. Completion of 'Good Standing Attestation' as outlined in the SIM Milestone AttestationChecklist.
f. Support Practices in identifying and resolving challenges in achieving milestones.g. Facilitate the development of sustainable QI processes.
2. Support from a Clinical Health Information Technology Advisor (CHITA) over the course of thisAgreement to:
a. Meet with Practice at least once monthly to implement improvements based on thepractice transformation building blocks as outlined in the SIM Framework andMilestones.
b. Assist Practice with completion of Health Information Technology (HIT) Assessments asoutlined in the SIM Cohort 3 Assessments and Reporting Schedule.
c. Assist Practice by linking to additional HIT resources.d. Assist Practice in identifying model for improvement using CQM data.e. Assist Practice in reviewing CQM data quarterly or at least every three months in
conjunction with Practice Facilitator. Details of CQMs are outlined in the SIM CQMReporting Summary.
f. Assist Practice in identifying CQM data improvement opportunities, such as conductingregular PDSA/QI activities on identified CQMs and reviewing CQM data to inform rapidcycle improvement processes.
g. Assist Practice with submission of CQMs quarterly as outlined in the SIM CQM ReportingSummary.
3. Access to two peer-to-peer Collaborative Learning Sessions over participating grant period toshare lessons learned and best practices.
4. Access to e-Learning modules, webinars, and other learning opportunities, to help Practicemove toward greater integration of behavioral health care, adopt alternative payment models,and implement comprehensive primary care functions.
5. Resources and toolkits to assist with the implementation of behavioral health integration.6. Practice transformation achievement based payments in accordance with the activities outlined
in Exhibit A, SIM Cohort 3 Practice Achievement Based Payments.
3. PRACTICE PARTICIPATION.Practices participating in both SIM and CPC+ will be expected to adhere to all expectations of CPC+ including, but not limited to, undertaking care delivery transformation activities outlined in the CPC+ Care Delivery Requirements established by CMS that are focused around five Comprehensive Primary Care Functions: (1) Access and Continuity; (2) Care Management; (3) Comprehensiveness and Coordination; (4) Patient and Caregiver Engagement; and (5) Planned Care and Population Health. Practice participation requirements for SIM have been tailored to align as closely as possible with corresponding CPC+ expectations and requirements.
Practice will meet the following requirements:

3
1. Develop a Quality Improvement (QI) Team to implement improvements based on the practicetransformation building blocks as outlined in the SIM Framework and Milestones.
2. Dedicate time for the Practice to engage with PF at least twice monthly, including one meetingwith Practice QI Team, and CHITA at least monthly to implement improvements based on thepractice transformation building blocks outlined in the SIM Framework and Milestones.
3. Dedicate time monthly for the Practice to develop and implement improvements based on thepractice transformation building blocks outlined in the SIM Framework and Milestones, includingdata-driven quality improvement activities that will assist with Practice data reporting.
4. Complete a set of Practice assessments to identify key areas of focus for improvement. Anoverview of the required assessments, including a timeline, is described in the SIM Cohort 3Assessments and Reporting Schedule.
5. Collect, report, and review SIM Clinical Quality Measures (CQMs) on a quarterly basis. Reportingon the practice-level CPC+ measures established annually by CMS will satisfy this requirement forSIM, and no additional measures for SIM are required. CQMs that will be collected, reported, andreviewed are outlined in the SIM CQM Reporting Summary.
6. Participate in SIM Collaborative Learning Sessions or, for Practices participating in CPC+,participate in CPC+ Learning System and associated activities. SIM/CPC+ Practices are encouragedto also attend the SIM Collaborative Learning Sessions, but are not required to do so.
7. Participate in SIM evaluation activities. This includes completing baseline as well as periodic andend-of-project assessments. This process might also include key informant interviews withorganization(s) contracted to conduct an evaluation of the SIM Initiative, and otherevaluationrelated requirements specified by the Colorado SIM Office or CMMI.
8. Complete Practice identified practice transformation building blocks outlined in the SIMFramework and Milestones through achievement of key milestones. The key building blocks andmilestones required for Practices to receive practice transformation achievement basedpayments are presented in Exhibit A, SIM Cohort 3 Practice Achievement Based Payments.
9. Meet regularly with the local Regional Health Connector (RHC) over the course of this Agreementto establish an ongoing supportive relationship and facilitate connection to local public healthand other community resources.
4. REPRESENTATIONS.Practice represents that:
1. Practice has the informed support of the clinical and administrative leaders of the Practice and, ifPractice is part of a healthcare system or multi-site organization, the support of appropriatelypositioned clinical and administrative/business leadership in the healthcare system or multi-siteorganization.
2. Practice maintains an accounting system and follows generally accepted accounting principles.3. Practice acknowledges that the Colorado SIM Office has provided the Practice Taxpayer
Identification Number (TIN) and all National Provider Identifier (NPI) numbers provided in theSIM Practice Application to private and public payers and authorized third parties including, butnot be limited to, Center for Improving Value in Health Care, Milliman, and TriWest. Practicefurther acknowledges that updated TINs and NPIs provided to the University or the Colorado SIMOffice throughout Practice’s participation in SIM will be provided to private and public payers andauthorized third parties including, but not be limited to, Center for Improving Value in HealthCare, Milliman, and TriWest.
4
4. Practice acknowledges that the Colorado SIM Office will annually share full calendar-year,practice-level Clinical Quality Measure data and Practice Good Standing as determined by theSIM Milestone Attestation Checklist with private and public payers. The Clinical Quality Measuredata will only be provided to private and public payers that have an existing contract or otheragreement with Practice. The Clinical Quality Measure data provided to private and public payerswill consist of practice-level numerators and denominators for each Clinical Quality Measurereported by the Practice to the University through a quality measurement reporting tool. TheClinical Quality Measure data will not include Personally Identifiable Information (PII) orProtected Health Information (PHI) of any individual. The Clinical Quality Measure data providedby the Colorado SIM Office to private and public payers will be governed by and used solely forthe purposes identified in an existing contract or other agreement between Practice and payer.
5. Practice acknowledges that the University will share Practice information provided by Practice inthe SIM Practice Application, all baseline and ongoing assessments identified in the SIM Cohort 3Assessments and Reporting Schedule, Clinical Quality Measure data and Practice Good Standing,as determined by the SIM Milestone Attestation Checklist, with the Colorado SIM Office andother third parties that are authorized to receive data under an existing contract or otheragreement with the University and/or Colorado SIM Office. Contracts or other agreements withthird parties will include appropriate confidentiality and non-disclosure terms and conditions.Authorized third parties include, but may not be limited to, Regional Health Connector hostorganizations, Practice Transformation Organizations, Center for Improving Value in Health Care,Milliman, and TriWest.
6. Practice acknowledges that private and public payers are providing claims data to authorizedthird party data aggregators for patients attributed to practice and its providers. Practice agreesthat it will enter into agreements with authorized third party data aggregators to access and usethese data throughout Practice’s participation in SIM.
5. TERMINATION.Either party may terminate this Agreement by giving 30 days written notice of an intent to terminate the agreement to the other party. Written notice should be sent to both the Colorado SIM Office (see the address below) and the University whose information is included in Section 6.
Colorado Department of Health Care Policy and Financing Colorado State Innovation Model (SIM) Office Barbara Martin, Colorado SIM Director 1570 Grant Street, Denver, CO 80203 [email protected]
6. NOTICE.All notices, requests, demands, and other communications under this Agreement shall be in writing and shall be
deemed to be given if hand delivered, e-mailed or mailed by certified mail, return receipt requested.
Unless hereinafter changed by written notice to Contractor, any notice to the University shall be delivered, e-mailed or mailed to the University at:
University of Colorado Natalie Buys, Manager of Grants and Contracts University of Colorado School of Medicine Department of Family Medicine

5
12631 East 17th Avenue, Mailstop F-496 Aurora, Colorado 80045 [email protected]
Unless hereinafter changed by written notice to the University, any notice to Contractor shall be delivered, e-mailed or mailed to Contractor at:
Contact Name:
Address:
Email:
Telephone: Fax:
All notices delivered by hand shall be effective upon delivery and all notices mailed by certified mail, return receipt requested, or e-mailed shall be effective when received, as indicated on the return receipt.
7. HEADINGS.Headings herein are for reference only and shall not be considered a substantive part of the Agreement.
8. MODIFICATIONS.No amendment to this Agreement shall be effective unless in writing and signed by the duly authorized representatives of both parties.
9. GOVERNMENTAL IMMUNITY.No term or condition of this contract shall be construed or interpreted as a waiver, express or implied, of any of the immunities, rights, benefits, protections, or other provisions, of the Colorado Governmental Immunity Act, CRS §24-10-101 et seq., or the Federal Tort Claims Act, 28 U.S.C. §§1346(b) and 2671 et seq., as applicable now or hereafter amended.
10. INDEPENDENT CONTRACTOR.Contractor shall perform its duties hereunder as an independent contractor and not as an employee. Neither Contractor nor any agent or employee of Contractor shall be deemed to be an agent or employee of the University. Contractor and its employees and agents are not entitled to unemployment insurance or workers compensation benefits through the University and the University shall not pay for or otherwise provide such coverage for Contractor or any of its agents or employees. Unemployment insurance benefits will be available to Contractor and its employees and agents only if such coverage is made available by Contractor or a third party. Contractor shall pay when due all applicable employment taxes and income taxes and local head taxes incurred pursuant to this contract. Contractor shall not have authorization, express or implied, to bind the University to any agreement, liability or understanding, except as expressly set forth herein. Contractor shall (a) provide and keep in force workers' compensation and unemployment compensation insurance in the amounts required by law, (b)
6
provide proof thereof when requested by the University, and (c) be solely responsible for its acts and those of its employees and agents.
11. COMPLIANCE WITH LAW.Contractor shall strictly comply with all applicable federal and state laws, University policies, rules, and regulations in effect or hereafter established, including, without limitation, laws applicable to discrimination and unfair employment practices.
12. CHOICE OF LAW.Colorado law, and rules and regulations issued pursuant thereto, shall be applied in the interpretation, execution, and enforcement of this contract. Any provision included or incorporated herein by reference which conflicts with said laws, rules, and regulations shall be null and void. Any provision incorporated herein by reference which purports to negate this or any other provision in whole or in part shall not be valid or enforceable or available in any action at law, whether by way of complaint, defense, or otherwise. Any provision rendered null and void by the operation of this provision shall not invalidate the remainder of this Agreement, to the extent capable of execution.

7
THE PARTIES HERETO HAVE EXECUTED THIS AGREEMENT
THE REGENTS OF THE UNIVERSITY OF COLORADO, a body corporate
{PRACTICE}
By_____________________________________ By_____________________________________
_______________________________________ _______________________________________ Printed Name Printed Name
_______________________________________ _______________________________________ Title Title
______________________________________ _______________________________________ Date Date
Exhibit A: SIM Cohort 3 Practice Achievement Based Payments
• Eligibility for SIM Cohort 3 Practice Achievement Based Payments is determined from three sources ofinformation on practice achievements:
1. Submission of all SIM assessments in SPLIT.2. Submission of required SIM CQMs in SPLIT.3. Year 1 Milestone Attestation Checklist as designated for practices participating in SIM-Only and
those practices participating in both SIM and CPC+.
• To receive payment for the submission of assessments, practice must complete all of the requiredassessments including the SIM Milestone Attestation Checklist, Integrated Practice Assessment Tool(IPAT), HIT Assessments, and the Medical Home Practice Monitor (all outlined in the SIM Cohort 3Assessments and Reporting Schedule). In addition, practices will need to achieve a 70% response rate forthe Clinician and Staff Experience Surveys.
• SIM expectations for clinical quality measure (CQM) reporting are outlined in the SIM CQM ReportingSummary can be found in the Resource Hub of the Practice Innovation website herehttp://www.practiceinnovationco.org/sim/.
• SIM Cohort 3 Practice Achievement Based Payment activities that refer to specific practicetransformation building blocks require evidence that a practice has accomplished milestones as outlinedin the SIM Milestone Attestation Checklist.
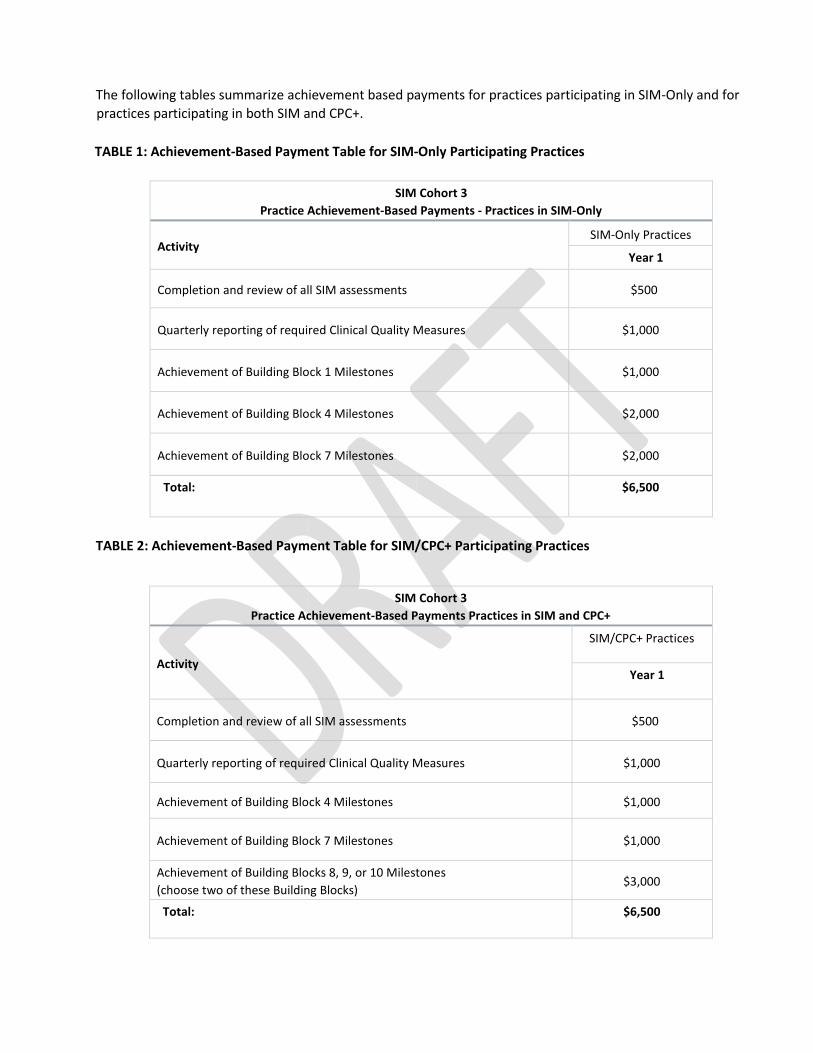
The following tables summarize achievement based payments for practices participating in SIM-Only and for practices participating in both SIM and CPC+.
TABLE 1: Achievement-Based Payment Table for SIM-Only Participating Practices
SIM Cohort 3 Practice Achievement-Based Payments - Practices in SIM-Only
Activity SIM-Only Practices
Year 1
Completion and review of all SIM assessments $500
Quarterly reporting of required Clinical Quality Measures $1,000
Achievement of Building Block 1 Milestones $1,000
Achievement of Building Block 4 Milestones $2,000
Achievement of Building Block 7 Milestones $2,000
Total: $6,500
TABLE 2: Achievement-Based Payment Table for SIM/CPC+ Participating Practices
SIM Cohort 3 Practice Achievement-Based Payments Practices in SIM and CPC+
Activity
SIM/CPC+ Practices
Year 1
Completion and review of all SIM assessments $500
Quarterly reporting of required Clinical Quality Measures $1,000
Achievement of Building Block 4 Milestones $1,000
Achievement of Building Block 7 Milestones $1,000
Achievement of Building Blocks 8, 9, or 10 Milestones (choose two of these Building Blocks) $3,000
Total: $6,500

SIM Cohort 3 Application Instructions and Questions
Overview, Instructions & Resources: SIM Cohort 3 Application
Overview: Thank you for your interest in the Colorado State Innovation Model (SIM) Initiative and interest in applying for SIM Cohort 3. By completing this online application the Practice Site is demonstrating interest in participating in SIM Cohort 3. Please note all completed applications will be reviewed by a multi-stakeholder review committee that will providerecommendations to the Colorado SIM Office who will make the final selection of practices offered the opportunity toparticipate in the final cohort of SIM, anticipated to begin June 2018.
Instructions: (Abbreviated) The SIM Cohort 3 Application consists of nine sections:
• Practice Site Information• Practice Site Demographics• Practice Site Key Contacts• Practice Site Provider Roster• Health Information Technology (HIT)• Behavioral Health & Practice Transformation• Practice Site Narratives• Participation Attestation• Application Completion Status
The SIM Cohort 3 Application should be completed at the Practice Site level and reflect the demographics, key contacts, and information unique to the Practice Site.
For more information on the SIM Initiative, visit the Colorado SIM Office website: https://www.colorado.gov/healthinnovation
Additional information regarding SIM can also be found at the University Practice Innovation Program Colorado website: http://www.practiceinnovationco.org/sim/
For technical and programmatic questions related to this application please contact: [email protected]
PRACTICE SITE INFORMATION This section collects basic information regarding the Practice Site and Practice Site Healthcare System or Multi-Site Organization (if applicable). Not all questions are required but Practice Sites are encouraged to complete as much information as possible in order to create a more comprehensive practice profile.
1) Has this Practice Site previously applied to participate in SIM?
PRACTICE SITE NAME(S) Please confirm the Practice Site Name(s) below. Some fields have auto-populated based on your previous responses. Please modify where appropriate. The Official Practice Site Name is the formal name, and often the same as the Legal Practice Name. The Preferred Practice Name is the name the Practice Site would like used in SIM communications.
2) Practice Site Name(s):• Preferred Name• Legal Name• Doing Business As (DBA) (Optional)
PRACTICE SITE ADDRESS & PHONE NUMBER(S) Please enter information regarding the Practice Site address and contact information.
3) Practice Site Physical Address: Street Address, City, State, Zip Code4) Practice Site County5) Practice Site Phone Number(s) (Ex. 333-333-3333): Main Phone Number, Other Phone Number (Optional)

PRACTICE SITE BILLING & IDENTIFICATION INFORMATION Please enter information regarding the Practice Site: Taxpayer Identification Number (TIN), Medicaid Billing ID Number(s), and Practice National Provider Identifier (NPI) for [Practice Site].
6) List the TINs this Practice Site uses to bill services (Ex. XX-XXXXXXX):7) Practice Site Group National Provider Identifier (NPI):8) List the Medicaid Billing IDs this Practice Site uses for Medicaid primary care services:9) Is this Practice Site contracted with Medicaid as a Primary Care Medical Provider (PCMP)?9a) Is the Medicaid Billing ID # this Practice Site is contracted under as a PCMP the same as the one provided inquestion eight (8)?9b) Under what Medicaid Billing ID # is this Practice Site contracted as a PCMP?
HEALTHCARE SYSTEM OR MULTI-SITE ORGANIZATION INFORMATION Please indicate if this Practice Site is a part of a Healthcare System or Multi-Site Organization. If applicable complete the additional fields below.
10) Does this Practice Site belong to a larger Healthcare System or Multi-Site Organization?10a) Healthcare System or Multi-Site Organization Name:(Some participating Healthcare Systems and Multi-Site Organizations are listed below. Please select the correct namewithin the list or choose 'Other' and type in the appropriate Healthcare System or Multi-Site Organization name yourPractice Site belongs to.)10ai) Please specify the 'Other' Healthcare System or Multi-Site Organization Name:10b) Healthcare System or Multi-Site Organization Address:10c) Healthcare System or Multi-Site Organization Phone Number(s) (Ex. 333-333-3333):
Practice Site Key Contacts This section aims to collect necessary information regarding [Practice Site] Key Contacts and Healthcare System or Multi-Site Organization Contacts, if applicable. Practices are encouraged to fill out this section as completely and accurately as possible.
PRACTICE SITE & MULTI-SITE ORGANIZATION KEY CONTACTS Please provide information regarding key contacts for this Practice Site. As an individual may fill multiple roles within a Practice Site and they can also be identified in more than one key contact role.
11a) Primary SIM Practice Site Contact 11b) Practice/Office Manager 11c) Provider Champion 11d) Lead Clinician/Provider 11e) Contact for Payers or Insurance Companies (Contact can be based at the Practice Site or at the Healthcare System or Multi-Site Organization level.) 11g) Healthcare System or Multi-Site Organization Contact 1 11h) Healthcare System or Multi-Site Organization Contact 2 (Optional) 11i) Healthcare System or Multi-Site Organization Contact 3 (Optional)
Practice Site Demographics This section collects basic demographics regarding the Practice Site and the Practice Site's Healthcare System or Multi-Site Organization if applicable. Practice Sites are encouraged to complete as much information as possible in order to create a more comprehensive practice profile.
PRACTICE SITE DEMOGRAPHICS Please complete all information regarding this Practice Site's general demographics, including Provider information.
12) Which of the following best describes this Practice Site's Organizational Structure?Federal (Veterans Administration, Department of Defense, etc.) Federally Qualified Health Center Federally Qualified Health Center Look-Alike Freestanding Urgent Care Center Health Maintenance Organization (Ex. Kaiser Permanente, etc.)
Hospital or Health System Owned Mental Health Center Non-Federal Government Clinic (Ex. State, County, City, etc.) Primary Care Residency Practice Private Solo or Group Practice Public Health Service Rural Health Clinic School-Based Clinic Other (Specify)
12a) Please specify 'Other' Practice Site Organizational Structure: 13) Which of the following describes this Practice Site type? (Select all that apply.)
Family Medicine General Internal Medicine Primary Care Pediatrics Nurse-Led Primary Care School-Based Clinic Other (Specify) Non-Traditional (Specify)
13a) If this Practice Site is a 'Non-Traditional' Primary Care Practice, it must still meet the Institute of Medicine (IOM) definition of primary care, "Primary care is the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients, and practicing in the context of family and community."
An applicant primary care Practice Site must be capable of providing a majority of its patients’ comprehensive primary, preventive, chronic, and urgent care. Please describe how this Practice Site meets the Institute of Medicine (IOM) definition of primary care as outlined above:
13b) If this Practice Site is an 'Other' Primary Care Practice, it must still meet the Institute of Medicine (IOM) definition of primary care, "Primary care is the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients, and practicing in the context of family and community."
An applicant primary care Practice Site must be capable of providing a majority of its patients’ comprehensive primary, preventive, chronic, and urgent care. Please describe how this Practice Site meets the Institute of Medicine (IOM) definition of primary care as outlined above:
14) Is this Practice Site engaged in training future primary care practitioners and staff?14a) Describe this Practice Site's training engagement below.
PRACTICE SITE PATIENT POPULATION Please complete all questions regarding this Practice Site's patient population by entering estimates for each. Percentage totals must add up to 100%.
15) Total number of patient visits per year at this Practice Site:16) Percentage of patients in this Practice Site in the following age ranges:
0-17:18-64:65+:Total:
17) Percentage of patients in the following payer categories for this Practice Site:Approximate % of Medicare: Approximate % of Medicaid/CHIP: Approximate % of Commercial or Private Insurance: Approximate % with No Insurance: Approximate % of Other Payer Category: Total:
18) Practice Site Formal Designations for Serving Undeserved Populations:Federally Qualified Health Center Federally Qualified Health Center Look-Alike Rural Health Clinic Indian Health Services Center Colorado Indigent Care Program Community Safety Net Clinic Health Profession Shortage Area Other (Specify) Not Applicable
18a) Please specify 'Other' formal designations for serving underserved populations:
PRACTICE SITE PROVIDER/STAFF CATEGORIES & COUNTS Reference the following table to provide approximate Practice Site totals for each of the provider and staff categories. The values provided in this roster will be used to calculate completion rates for the SIM Clinician & Staff Experience Survey that participating practice sites complete annually.
19) Enter approximate Practice Site totals for the provider/clinician and staff categories listed:Providers/Clinicians Clinical Practice Staff Allied Health Professional Support & Office Staff Other Practice Staff
Practice Site Provider Roster This section aims to collect necessary information regarding the Practice Site's Providers/Clinicians. Practice sites are required to include roster information for their providers. This information can help determine if this Practice Site is eligible for additional financial support from payers participating in SIM. Please include all Providers at this Practice Site who have an NPI.
Common Specialty/Taxonomy Codes for Primary Care Providers: Pediatric Medicine: 208000000X General Practice: 208D0000 Adult Medicine: 207QA0505X Family Medicine: 207Q00000X Internal Medicine: 207R00000X Geriatric Medicine: 207RG0300X
The SIM Taxonomy Code List can be found here: http://resourcehub.practiceinnovationco.org/wp-content/uploads/2017/02/SIM-Taxonomy-Code-List.pdf Please use the link to view a complete list of taxonomy codes for Primary Care Providers.
PRACTICE SITE PROVIDER ROSTER For each Primary Care Provider/Clinician at the Practice Site enter the following: First Name, Last Name, Email, Provider/Clinician Type, NPI, and Taxonomy Code.
Complete the following information for all licensed providers and clinicians at the Practice Site: First Name, Last Name, NPI, Provider/Clinician Type, Taxonomy 1, Taxonomy 2
Health Information Technology (HIT) This section aims to collect details on the Practice Site's Electronic Health Record (EHR) and use of Health Information Technology (HIT).
ELECTRONIC HEALTH RECORD (EHR) SYSTEM Provide the following details regarding this Practice Site’s Electronic Health Record (EHR) System. 20a) Select the Practice Site Electronic Health Record (EHR) System/Product Name: 20ai) Specify 'Other EHR System/Product' name: 20b) Specify EHR version used by the Practice Site:
MEANINGFUL USE ATTESTATION Please answer the following questions regarding attestation of Meaningful Use. 21) Have providers at this Practice Site attested to Meaningful Use?21a) Please indicate the highest stage of Meaningful Use achieved.
CLINICAL QUALITY MEASURES (CQMS) 22) Is this Practice Site currently able to report SIM CQMs per the timeline outlined in the SIM CQM ReportingRequirements, within the RFA document? To review the SIM CQM Reporting Requirements please reference the SIMClinical Quality Measure (CQM) Reporting Requirements document (http://resourcehub.practiceinnovationco.org/wp-content/uploads/2017/02/SIM-CQM-Reporting-Requirements-1.pdf).22a) What resources does this Practice Site need to develop in order to report SIM CQMs?
Behavioral Health & Practice Transformation This section collects details about the Practice Site's participation in Behavioral Health and Practice Transformation activities.
BEHAVIORAL HEALTH 23) Does this Practice Site have access to a Behavioral Health Provider (BHP)?23a) What type of access to a BHP does this Practice Site have?
Full-time Onsite Part-time Onsite Full-time Telehealth Part-time Telehealth Consult Only Other (Specify)
23ai) Specify 'Other' type of access to a BHP that this Practice Site has: 23b) What are the degrees(s) or license(s) of the BHP(s) this Practice Site has access to? 23bi) Specify 'Other' degree or license:
OTHER PRACTICE TRANSFORMATION INITIATIVE PARTICIPATION & WORK 24 Is this Practice Site recognized as a Patient-Centered Medical Home? 24a) Please indicate the organization(s) that recognizes this Practice Site as a 'Medical Home:' 24ai) Specify the standard year for National Committee for Quality Assurance (NCQA-PCMH): 24aii) Specify State-Based Recognition Program name and recognition level received: 24aiii) Specify the recognition level received for Utilization Review Accreditation Commission (URAC): 24aiv) Specify the 'Other Organization' that recognizes this Practice Site as a 'Medical Home': 25) Is this Practice Site participating in CPC+ currently?26) Has this Practice Site participated in any quality improvement (QI) activities or practice transformation initiativeswith Practice Facilitators and/or Quality Improvement Coaches?26a) Identify which of the following quality improvement (QI) activities or practice transformation initiatives thisPractice Site has previously or is currently participating in:26ai) Specify the 'Other' quality improvement (QI) activities or practice transformation initiatives:27) Identify which of the following non-fee-for-service payments from a payer in the last 24 months this Practice Sitehas participated in? (Ex. Shared Savings, PMPM, Global Payments, Episode of Care Payments, etc.)27a) Specify 'Other Medicare ACO Program':27b) Specify non-fee-for-service payment 'Other Program':
Practice Narratives This section provides the opportunity for Practice Sites to share their practice transformation goals and reasons for applying to the SIM Initiative. Please answer each question thoroughly and distinctively for this Practice Site.
28) Explain why this Practice Site is interested in participating in SIM:29) Identify the benefits anticipated from participation in SIM:30) Describe this Practice Site's Leadership, provider and staff commitment to Practice Transformation. Please discusshow leadership will support transformational change and identify resources required for sustainable change.31) Identify the existing or planned processes this Practice Site has for supporting behavioral health integration.32) Please provide any additional information you would like us to consider or any comments you would like to share.
SIM Participation Attestation The section below documents the Practice Site’s attestation to the accuracy of the information provided in the SIM Cohort 3 Application and an understanding of the general expectations of participation in SIM. The attestation below is NOT a commitment to participate in SIM. Practice's selected for SIM Cohort 3 will have the opportunity to accept or decline participation after the offer.
33) By signing this application to be considered for participation in SIM Cohort 3, this Practice Site attests:a. Practice Leadership and/or Healthcare System or Multi-Site Organization Leadership, supports the intentionto move toward increasing integrated primary care and behavioral health.b. The SIM Cohort 3 Application was completed by the staff and/or providers at the PracticeSite with approval of the Healthcare System or Multi-Site Organization, if applicable.c. Commitment to participate in one year of practice transformation and agrees to:
Identify a cross-functional Quality Improvement Team to implement improvements Complete a set of practice assessments to identify key areas of focus for improvement Collect, report, and review SIM Clinical Quality Measures on a quarterly basis Attend two Collaborative Learning Sessions and/or for CPC+ participating practices, participate in CPC+ Learning System and activities Participate in SIM evaluation activities Achieve selected SIM building blocks through achievement of key milestones
d. This Practice Site has the ability and willingness to account for funding received from SIM.e. This Practice Site has the ability and interest to participate in alternative payment modelssuch as Per Member Per Month (PMPM), Bundled Payments, Global Payments, Shared Savings, etc.
34) Please upload your completed University W9 Template here: REQUIRED35) Please upload any additional materials:36) Please provide the name and contact information for the person who should be contacted with questions regardingthis application: First & Last Name, Practice Role, Email Contact, Phone Number36a) In addition to the previously person identified, Practice Sites can enter up to three additional contacts to receivean email confirming the submission of a SIM Cohort 3 Application for [Practice Site Name]: First Name, Last Name,Email