cold reactive lymphocytotoxic antibodies in pulmonary...
TRANSCRIPT

Indian Journal of Experimental Biology Vol. 38, July 2000, pp. 643-650
Cold reactive lymphocytotoxic antibodies in pulmonary tuberculosis: Correlation with disease activity and HLA
R R ajalingam * & N K Mehra
Department of Hi stocompatibility and Immunogenetics, All India Institute of Medical Sciences, New Delhi II 0 029, India
and
R C J ai n
La Ia Ram Sarup Institute of Tuberculosis and Allied Di seases, Mehrauli , New Delhi II 0 016, India
Received 3 1 May 1999; revised 6 April 2000
Cold reactive lymphocytotoxic antibodies (LCA) are more reactive in cold than at 37°C and occur following infection , immuni zation or vacci nation and in va ri ous autoimmune diseases. In the present study, LCA acti vity against T and Blymphocytes has been investigated in patients with pulmonary tuberculosis (PTB ), their various clinical sub-groups and consanguineous relatives. Further, the relevance of HLA factors in LCA activity was analyzed. The sera from 144 PTB patients, 52 famil y contacts and 52 healthy individuals were tested for presence of LCAs by a modified two-stage NIH microlymphocytotoxici ty assay. A significant increase in LCA activity against both T (32.6% vs 5.7%, P<O.OOOI) and B (59.7% vs 13.4%, P < 0.0000001) cell s was observed in PTB patients as compared to healthy cont rols. There was no corre lation between seru m LCA acti vity and sputum acid-fast baci lli status. However, only B cell LCAs revealed significan t increase in parallel to di sease advancement as assessed by X-ray chest examination. Further, LCA activ ity was more pronounced in drug responders than drug fail ure group of patients. No significant difference in the distribution of HLA class I and class II antigens was observed between LC A positi ve and LCA negati ve patients. However, panel cells carrying HLAA I , -A II and -DR3 were often found reactive in LCA positive patient sera. In household family contacts, LCAs were significantl y increased on ly against B cells as compared to healthy control s (38.4% vs 13.4%, P<O.Ol ). This study suggests that Mycobacterium tuberculosis infection/exposure could account for the occurrence of LCAs in pulmonary tuberculosis and the strength of these antibodies is related to disease severit y and the extent of lung involvement.
Cold reactive lymphocytotoxic antibodies (LCAs) are complement binding lgM or IgG c lass of antibodies that are more reactive in the eold temperatures than at 37°C 1
• They are known to occur in autoimmune diseases2
-4
, following immunization or vaccination5
d . f . b . 67 d b . 8· 10 an m ect10ns y vtmses · an myco actena . Their presence in healthy indi viduals is rare, except after multiple pregnancies or transfu sions' ' .
Although the exact stimulus for LCA production is obscure, their increased incidence in nonconsanguineous relatives of patients with systemic lupus erythematosus (SLE) 12
, rheumatoid arthritis4 and in inflammatory bowel di sease 13 suggests an important role of environmental agents. In some studies, the presence of LCAs has been correlated with a particular HLA-DR phenotype of the host4
·14
,
although others failed to observe such an
*Present address : D 150 Fairchild Center, Department of Structural Biology, Stanford University School o f Medici ne, Stanford, CA 94305 Fax: (650)723-8464 Tel: (650)723-5469 E-mail : lingam @cmgm.stanford.edu
association 15• Presence of LCAs . have been
demonstrated in the sera of patients with pulmonary tuberculosi s in earlier studies8
'16
. In the present study LCA activity against T and B cells has been investigated in North Indian PTB patients, thei r various clinical sub-groups and consanguineous relatives. Further, the influence of human leukocyte antigen (HLA)-Iinked factors in the production of LCAs was determined in this study.
Materials and Methods Patients (Table 1)- Patients ( 144) with active
pulmonary tuberculosis attending the out patient TB clinic of the Lata Ram Samp Institute of Tuberculosis and Allied Diseases, Mehrauli, New Delhi during 1991-95 were included in the study . The criteri a for 'active' pulmonary tuberculosis includes the presence of respiratory symptoms (fever, cough , expectoration and malaise) with chest radiol ogical changes suggestive of infection by tubercle bacilli. Only those patients who had no history of past treatment were included in the study. Sputum smears were examined atleast twice in each patient at the beginning of anti-

644 IND IAN J EXP BIOL, JULY 2000
Table I -Cl inical fea tures of pulmonary tuberculosi s patients studied
Clinical groups Patients st udied Number Per cen t
Total number 144 100
Sex
Male 89 62 Female 55 38
Sputum smear/culture
Positive 104 72 Negative 40 28
X-ray chest lesions
Unilateral limited 43 30 Bilateral li mited 28 19.5 Unilateral extensive 21 14.5 Bilateral extensive 52 36
Response to chemotherapy
Responders 54 38 Failures 50 35
tuberculosis treatment, as well as subsequently at monthly intervals for acid-fas t baci lli (AFB) by auramine stain fluorescent microscopy17
. All smear negati ve or doubtful cases were re-examined by the standard sputum culture method. The extent of the disease was assessed on chest roentgenograms before the initiation of specific chemotherapy and based on the lung lesions, the disease was classified as unilateral limited (UL) , bilateral limited (BL), unilateral extensive (UE) and bilateral extensive (BE) . The disease was considered ' limited' if it invol ved less than one-third of the lung fields in a hemithorax and 'extensive' if the lesions were more profuse.
The sputum positive patients were further classified according to thei r response to chemotherapy. Those who responded to the first-line anti-tuberculosis chemotherapeutic agents i.e., a combination of isoniazid, rifampicin, pyrazinamide and streptomycin/ethambutol were classified as 'drug responders'. The response to treatment was defined as clinical and radiological improvement with disappearance of AFB in the sputum on smear examination within 3 months from the start of chemotherapy. On the other hand, patients who did not respond to treatment with first line drug regimes and were found to be consistently sputum smear AFB positive for atleast three months were included in the 'drug fai lure' group. Most of the patients were hospitalized to ensure drug compliance. The outpatients were asked to report to the doctor every Monday to confirm their drug compliance. The drug failure patients were further treated with second line drugs.
A detailed record was mai ntained on the type and extent of tuberculosis, results of sputum smear/ culture and history of treatment. Strict follow up was done for each patient for atleast one year. The detailed clinical features of the patients are presented in Table I. The average age of the pat ients was 36.2 ± I years with a male to female ratio of 1.6: I .
Household family contacts- One of the parents/ brothers/sisters/children of the sputum smear positive group of patients with acti ve tuberculosis li ving under the same roof and similar nutritional conditions, having no symptoms of PTB (respiratory complaints and symptoms including fever, cough and ex pectoration and malai se), were included in the ' household family contacts' group (n =52). The average age of thi s group was 34.7 ± I years with a male to female ratio of 1.5: I. X-ray chest and sputum examination were carried out in these individuals and only those showing negative results were included in the study. These were followed for more than a year by health visitors/ community social workers of the hospital. Anyone with a recent history of fever or viral illness was excluded.
Controls- A total of 52 age (average ages = 36.7 ±I years) and sex (male to female ratio= 1.6: I ) matched unrelated healthy individuals belonging to the same soc io-economic sta t:us and ethnic background were included as controls in the study . None of them gave a family history of tuberculosis or any other related disease. Individuals with a recent hi story of fever or vira l illness were exc luded. None of the controls had a hi story of previous blood transfusions and fema les with more than one pregnancy were exc luded in order to avoid possible influence of alia-stimulation.
Serum samples - Serum samples from each patient were collected before the start of an ti-tuberculosis chemotherapy and stored at -35°C unti l assayed for LCA activity . In order to study the effect of antituberculosis chemotherapy on T and B cell LCAs, serial samples from 30 active sputum smear/ culture positive hospitali zed patients ( 16 drug responders, 14 drug failures) were included randomly for analysis. The samples were obtained before the start of chemotherapy and after 3, 5 and 12 months of chemotherapy.
. Lymphocytotoxicity assay for LCAs- Presence of LCAs in the test sera was determined by the standard two-stage NIH microlymphocytotox icity assa/ 8
,
mod ifi ed for the cold conditions r. Essentiall y, it consisted of reaction of each serum in I 111 quantities

RAJALINGAM et. al.: LYMPHOCYTOTOXINS IN PULMONARY TUBERCULOSIS 645
with -I 000 lymphocytes for 30 min, addition of 5 J..LI of rabbit complement and incubation for a further three hours period at I 5°C. Cytotoxicity was assessed by the eosin-dye exclusion method using phasecontrast microscopy. Further, all sera were also tested simultaneously under room temperature ( -25°C) conditions. Lymphocytes from a panel of 86 healthy volunteers with known HLA phenotypes was used to screen for cytolysis. This panel of cells covered all of the known HLA antigens found in Asian Indians. The HLA profile of the panel was similar to the individual allele frequencies observed in the random population. Twenty ml heparinized blood (10-15 I.U. of preservative free heparin/ml) was freshly drawn from each individual and lymphocytes were separated on ficoll-hypaque density gradient centrifugation. T and B cells were separated using nylon wool columns and used to test T and B lymphocytes specific LCA.
Cytotoxicity was scored according to the method described by Serjeantson and Dr/ i.e., 0 = < 20% cell death, I =20-50% cell death, 2=51-75% cell death, 3 = 76-90% cell death, and 4 = > 90% cell death. The individual scores of a serum against each of the 86 panel cells were added, and the mean was designated as the 'cytotoxic score' of that particular serum. The sera giving cytotoxic score of > 0.6 were considered positive to LCA activity .
HI.A testing-All patients, controls and house hold family contacts as well as donors included in the screening panel were serologically tested for the
expression of HLA class I and class II antigens using the standard two stage NIH microlymphocytotoxicity assay 18
• Heparinized blood (20 ml; 10-15 I.U. of preservative free heparin/mL) was freshly drawn from each individual and lymphocytes were separated on ficoll-hypaque density gradient centrifugation. T and B cells were separated using nylon wool columns. A minimum of two to three antisera were used for testing each of the serological specificity in HLA-A, B, C and DR loci. The serological trays identified 18 locus A alleles, 47 locus B alleles, 7 locus C and 19 locus DR/DQ alleles.
The serological test results of HLA class II alleles were further confirmed by the molecular techniques of polymerase chain reaction and sequence specific oligonucleotide probe (PCR-SSOP) hybridization . Generic testing for alleles in HLA-DRB 1, DQA I and DQB I was performed using a set of specific primers and 80 probes, biotinylated at their 5' end. Details of the procedure have been described elsewhere 19
.
Statistical analysis- The statistical analysis was carried out using the standard X2 test. P < 0.05 considered statistically significant.
Results LCA activity in PTB patients and controls- Out of
the 144 PTB patient sera, 47 (32.6%) showed LCA activity against T lymphocytes and 86 (59.7%) against B lymphocytes whereas the controls had marginal or no LCA activity (3 of 52 against T cells
Table 2- Distribution of cytotoxic scores among controls, patients with pulmonary tuberculosi s and their healthy family contacts
Cytotoxic Health~ controls (n=52) PTB Eatients (n=l44) Famil~ contacts (n=52) score T-cell B-cell T-cell B-cell T-cell B-cell
No.% No. % No.% No. % No. % No.%
LCA negative
0 II (21.1) 2 (3.8) 4 (2.7) 0 8 (15.4) 0 0-0.2 35 (67.3) 25 (48.1) 44 (30.5) 14 (9 .7) 22 (42.3) 8 (15.4) 0.2-0.6 3 (5.8) 18 (34.6) 49 (34) 44 (30.5) 19 (36.5) 24 (46.1) Total 49 (94.2) 45 (86.5) 97 (67.3) 58 (40.2) 49 (94.2) 32 (61.5)
LCA positive
0.6-1.0 0 2 (3.8) 22(15.3) 37 (25.7) 2 (3 .8) 15 (28.8) 1.0-1.4 I ( 1.9) 2 (3.8) 7 (4.8) 21 (14.6) I ( I. 9) 4 (7.7) 1.4-1.8 0 3 (5 .8) 8 (5.5) 8 (5 .5) 0 I ( I. 9) 1.8-2.0 2 (3.7) 0 5 (3.5) 3 (2. 1) 0 0 >2 0 0 5 (3.5) 17(11.8) 0 0 Total 3 (5.7) 7 ( 13.4) 47 (32.6)" 86 (59.7)[ 3 (5.7) 20 (38.4)"
P values: . c < 0.000 I Control T-cell s vs PTB T-cell s) f< 0.000000 I (Control B-cells vs PTB 8-cell s) a< 0.0 I (Control 8-cells vs control 13-cclls)

646
70
60
-* 50 '-"
.0 .... .... 40 .... .....
(,1 !!': ~
'"' 30 < u ...:l e 20
= '"' ~ r:J) 10
0
INDIAN 1 EXP BIOL, JULY 2000
D AFB -ves {n==40)
• AFB +ves {n==104)
c 37 .5%
T cells
b 55%
B cells
f 61.5%
Fig. 1 -Comparison of lymphocytotoxicity in the sera of patients with pulmonary tuberculosis based on sputum acid fast bacillary (AFB) status. P values: b<O.OOl, c<O.OOOl, f<O.OOOOOO l (controls vs diseased). Shaded area denotes the levels ofT and B cell LCAs in healthy controls.
g
80
Fig. 2- Occurrence of lymphocytotoxic antibodies in pulmonary tuberculosis patients with different stages of radiographic lung lesions. P values: a<O.Ol , b<O.OOl, d<O.OOOOl , g<O.OOOOOOOOO I (as compared to controls). UL=unilaterallimited (n= 43); UE=unilateral
RAJALINGAM et. al.: LYMPHOCYTOTOXINS IN PULMONARY TUBERCULOSIS 647
i.e., 5.7% and 7 of 52 against B cells, 13.4%). The difference in LCA activity of controls and patients was statistically significant i.e. T cells: X2 = 14.5, P<O.OOOl; B cells: X2 =32.8, P<O.OOOOOOI (Table 2) . On the other hand, the LCA activity against T cells in the healthy household fami ly contacts was found to be similar to that of controls (3 of 52, 5.7%) while B cell LCA increased significantly .as compared to controls (20 of 52, 38.4%, X2 = 8.5, P < 0.0 I). All sera tested at room temperature (-25°C) conditions were found to be negative for cytotoxicity.
LCAs and sputum positivity- The LCA activity against both T and B lymphocytes increased in both AFB positive and negative patients as compared to controls (Fig. 1) i.e. , controls vs AFB negative group, T cell s: X2 = 14.5, P<O.OOOI ; B cells: X2 = 18.0, P < 0.00 I; control s vs AFB posi tive, T cells: X2 = 12.45, P < 0.00 I , B cells: X2 = 32.3, P < 0.000000 I. No statistically significant differences were observed when the two patient groups were compared with each other.
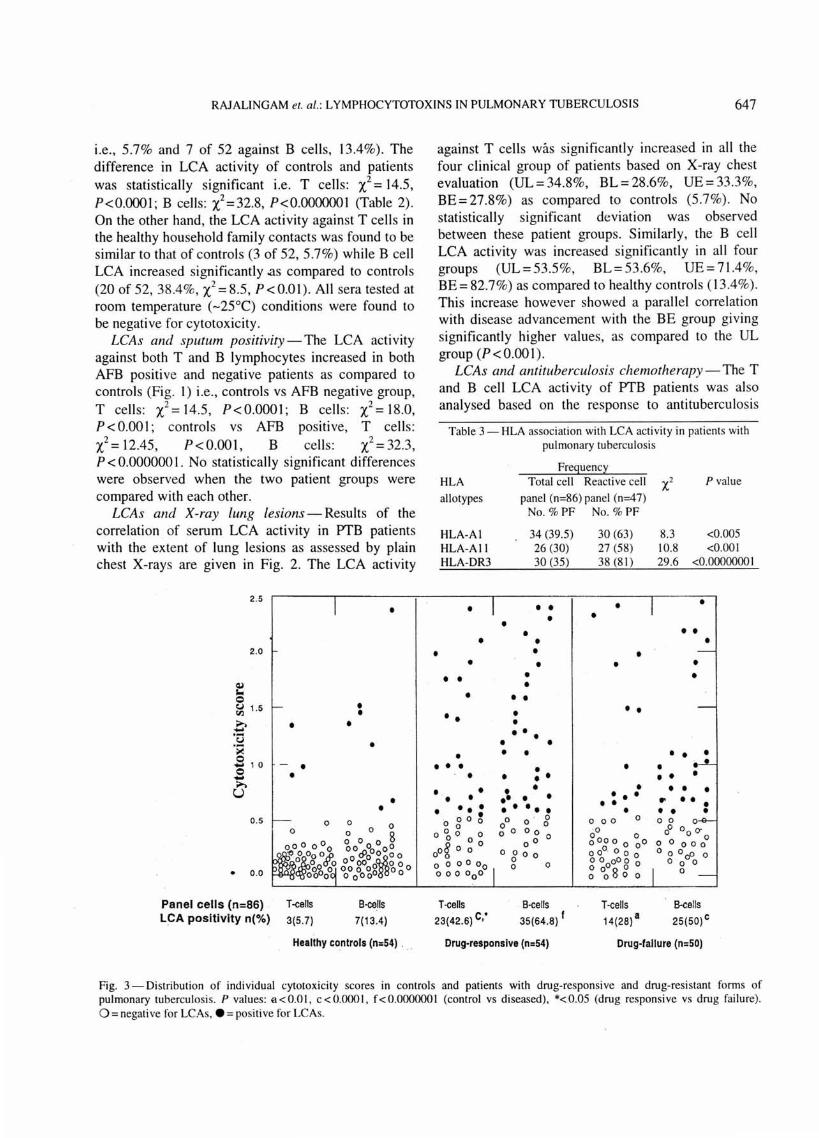
LCAs and X-ray lung lesions-Results of the correlation of serum LCA activity in J.YTB patients with the extent of lung lesions as assessed by plain chest X-rays are given in Fig. 2. The LCA activity
~ -0
2 .5
2.0
~ 1.5
0 ·o -~
s 10 0 -..... u
0.5
• 0 .0
•
- . •
Panel cells (n=86) . T-eens LCA positivity n(%) 3(5 .7)
• • •
•
•
B-cells
7(13.4)
•
•
Healthy controls (n=54) .
against T cells was significantly increased in all the four clinical group of patients based on X-ray chest evaluation (UL = 34.8%, BL = 28.6%, UE = 33.3%, BE=27.8%) as compared to controls (5.7%). No statistically significant deviation was observed between these patient groups. Similarly, the B cell LCA activity was increased significantly in all four groups (UL=53.5%, BL=53.6%, UE=71.4%, BE= 82.7%) as compared to healthy controls (13.4%). This increase however showed a parallel correlation with disease advancement with the BE group givi ng significantly higher values, as compared to the UL group (P<O.OOI).
LCAs and antituberculosis chemotherapy - The T and B cell LCA activity of J.YTB patients was also analysed based on the response to antituberculosis
Table 3- HLA association with LCA acti vi ty in patients with pulmonary tuberculosis
Freguenc~
HLA Total cell Reactive cell x2 P value
allotypes panel (n=86)panel (n=47) No. % PF No. % PF
HLA-Al 34 (39.5) 30 (63) 8.3 <0.005 HLA-All 26 (30) 27 (58) 10.8 <0.001 HLA-DR3 30 (35) 38 (8 1) 29.6 <0.0000000 I
• • • • • • • •
• • • • • • • • • • • • • • • • • • • •• • • •
• • • • • • • • •
• • • • • • • • • • • • • • • • •• • • • • • . . . : • • ••• • • •
. 0 0 0 0 0 0 0 0 0 0
0 0 g 0 0
0 ° 0 0 oo · O
0 0 0 0 0 00 oooo 0 0o
00~ 0 0 ° 0 8 0 0 0 00. 0 0 0
0 o o o o0 0 0 o o
0ooo 0
0 0 8 0 0 0 0 000 0 0 0 0
T-cells B-cells T-cells B-e ells 23(42.6) c,• 35(64.8) I 14(28) a 25(50)c
Drug-responsive (n=54) Drug-failure (n=SO)
Fig. 3-Distribution of individual cytotoxicity scores in controls and patients with drug-responsive and drug-resi stant forms of pulmonary tuberculosis. P values: a< 0.0 I, c < 0.000 l, f< 0.000000 I (control vs diseased), *< 0.05 (drug responsive vs drug fai lure). 0 =negative fo r LCAs, e =positive for LCAs.

648 INDIAN J EXP BIOL, JULY 2000
chemotherapy. As compared to the values in healthy controls (T cell: 5.7%; B cell : 13.4%), the LCA against T and B cells was found to be significantly increased in both drug-responsive (T cell: 42.6%, P<0.0001, B cell: 64.8%, P<0.0000001 ) as well as drug-failure group of patients (T cell: 28 .0%, P < 0.0 I , B cell: 50.0%, P < 0.000 I) . Generally, the cytotoxicity was more pronounced in drug responders than failure patients and the difference between these two groups was found to be statistically significant only with T cells (X2 = 4.1, P < 0.05).
The serial serum sample analysis for LCA activity in 30 patients (16 drug responders, 14 drug failure) revealed no significant impact of anti-tuberculosis treatment on LCA activity. Only 3 drug responders and 2 failure patients showed a fall (equivalent to controls) in the LCA activity (against both T and B cells) after three months of treatment.
HLA assocwtwn with LCA activity- No significant differences were observed in the distribution of HLA class I and II antigens between LCA positive and LCA negative patients.- In order to identify the HLA specificity of the LCAs in the sera of positive patients, the most common HLA alleles were identified from the panel of reactive cells, and the per cent frequency of these common alleles was calculated for all of the 47 reactive PTB sera (reactive against both T and B cells) (Fig. 3) . The data were compared with HLA profile of the total donor cell panel (n = 86) using X2 stati stics. The reactive cell panel was found to carry HLA-A I , (A II and (DR3 most frequently than the donor cell panel (Table 3).
Discussion This study reveals high incidence of seru m LCAs
in patients with pulmonary tuberculosis and thei r household healthy family contacts suggesting that their occurrence is a sequelae to infecti on/exposure to M. tuberculosis . Such e levated activity of LCAs has already been demonstrated in various infections6
•7
including patients with tuberculosis8'16 suggesting that
a spurt in the activity of this autoantibody may be a consequence of general ized infection. In the present study, cytotoxicity against B cells was observed more often and with greater intensity in PTB patients while the LCAs against T lymphocytes were generally weak and occurred with lesser frequency . Similar trend has been reported in autoimmune disease like rheumatoid
h .. 414 d . I h 1 art ntis · an systemic upus eryt ematosus· . Increased levels of anti-F(ab)2y antibodies in PTB patients,, causi ng an anti-idiotypic antibody response
to anti-M. tuberculosis antibody have been observed20.
It has been shown that the idiotypic antibodies react with surface immunoglobulin receptors on B lymphocytes leading to their activation21
. Thus the elevated activity of heterologous anti-immunoglobulin (i.e. LCAs) denotes a substantial degree of B cell activation in patients and house hold family contacts.
Although the house hold consanguineous family contacts show high B cell cytotoxicity as compared to controls, the in tensity of cytotoxicity does not exceed more than 1.5 score while 18% patien ts (26 out of 144) showed score more than 1.5. These data suggests that the M. tuberculosis infection may be more important for LCA production than the genetic make up of the host. Further, environmental agents have been postulated to be responsible for the increased incidence of LCAs in nonconsangnineous relati ves of patients with SLE12
, rheumatoid arthritis4,
inflammatory bowel di seaseJJ and multi ple sclerosis21.
However, the pathologic s ignificance of the high frequency of LCAs observed among healthy family contacts is uncertain.
Although the exact mechani sm of LCA production in pulmonary tuberculosis is not c lear, some possibilities can be di scussed: i) anti-M. tuberculosis antibodies may be cross reactive with allotypic or idiotypic determinants of B cell receptors or surface proteins on lymphocytes, just as has been shown for anti streptococcal-M antibodies being cross reactivity with several HLA specificities 1
; ii ) M. tuberculosis being an intracellular organism may cause alterations in the cell membrane leading to the production of antibodies against the slightly altered an tigens on the surface of infected cell s. These ant ibodies may in turn cross-react with normal antigens present on lymphocytes; iii ) B cells spontaneously process their own immunoglobulins and present idiotyp ic pept ides on their class II molecules22 leading to the production of antibodies against B cell surface immunoglobulins; iv) immune complexes are known to be efficient stimulators of LCA production in experimental animals23
. The formation of immune complexes leads to unfolding of sites on the autologous Ig molecule that could expose buried antigenic dete rminants not recognized by the host ; v) and further a recent study in South Indian PTB patients suggested that the active di sease (uncontrolled multiplication of M. tuberculosis) and anti -tuberculosis treatment may destroy the mycobacterium loaded h st cells. The membrane/cellular components from these lysed ce ll s may be exposed to produce LCA 16
•

RA1ALINGAM et. a/.: LYMPHOCYTOTOXINS IN PULMONARY TUBERCULOSIS 649
Absence of a significant difference in LCA activity between AFB positive and AFB negative patients indicates that exposure to pathogen rather than the bacterial load is necessary for LCA production. This is true even in healthy family contacts. Indeed the levels of these antibodies do not decrease following successful treatment with anti-tuberculosis chemotherapy. This is in accordance with findings in South Indian PTB patients, in whom the presence of LCA activity have been clocumented in patients treated 10- 15 years before for tuberculosis 16
•
Similarly in SLE patients, the serum LCA was reported to be persistent for many years24
. On the other hand, a progressive decline in LCA activity has been observed in patients with type I diabetes following treatment25
• In the present study, the B cell LCA activity showed a linear increase with disease severity as assessed by X-ray lung lesions of PTB patients. Although the relevance of LCA levels and disease severity in PTB is not clear, it is apparent that the stimulus for LCA production is abundant in patients with bilateral extensive disease. Similar mechanism has been put forward to explain tissue damage in patients with chronic and acute hepatitis26
.
Following initial studies demonstrating the existence of immune response (lr) and/ or immune suppression (Is) genes in the major histocompatibility complex27
, several HLA alleles have been reported to be positively associated with antibody production in malaria28
, rhesus immunization29, insulin antibody
production30 and influenza H3 hemagglutinin response31
. Similarly, association of HLA-DR2 with the production of M. tuberculosis specific antibodies in patients with pulmonary tuberculosis has been reported32
·33
. In the present study, no deviation was found in the HLA phenotypes of patients as compared to healthy controls suggesting that LCA production in pulmonary tuberculosis is independent of HLA or genetic constitution of the host . Similar results have been reported in leprosy, a re lated mycobacterial infectious disease 10
• Nevertheless, the reactive panel cells in the present study showed significantly higher frequenci es of three HLA alleles, HLA-A I , A I I and DR3 (than the total donor cell panel) suggesting that the M. tuberculosis induced LCAs may have some degree of cross reactivity with these particular HLA phenotypes . We have recently reported that while HLA-DR3 confers protection in PTB, DR2 (ORB I * ISO I and 1502) is strongl y associated with susceptibili ty particularly in the severe, drug resistant form of the disease 19
.
The present study has found evidence of significant immunological disturbance in both PTB patients and healthy family contacts. While the exact role of LCA in the immunopftthogenesis of PTB is uncertain, it is apparent that M. tuberculosis infection/exposure could account for the occurrence of these LCAs in PTB patients and their household contacts while the strength of the LCAs may be correlated with disease severity. Further studies are required to determine the specificity of LCAs and their target lymphocyte subsets.
Acknowledgement The financial assistance to this study by the
Department of Biotechnology, Govt. of India is greatly acknowledged . We thank all volunteers and patients for their willingness to participate in the study .
References I Mottironi V D & Terasaki P I, Infectious mononucleosis,
Rubella and Measles. In: Terasaki P I, Ed , Histocompatibility Testing 1970, (Munksgaard, Copenhagen), 1970; 301.
2 Charlesworth 1 A, Peake P, Campbell LV, Ramma 1, Pussell 8 A, Howard N & Elder G 1, Detection of lymphocytotoxic antibodies in relatives of patients with type I diabetes, Br Med J, 292 ( 1986) 292.
3 Vasan R S, Mehra N K, Malaviya A N & Chaudhri T K, Lymphocytotoxin antibodies in patients with systemic lupus erythematosus and their household contacts, Indian J Med Res, 92 (1990) 147.
4 Taneja V, Mehra N K, Singh R R, Anand C & Malaviya AN, Occurrence of lymphocytotoxins in multi-case rheumatoid arthritis families : relation to HLA, Clin Exp lmmwzol, 86 (1991 ) 87.
5 Kreisler M 1, Hirata A A & Terasaki P I, Antibodies against lymphocytes produced by vaccination, Transplantation, I 0 (1970) 411.
6 Huang S, Lattos D 8, Nelson D 8, Reeb K & Hong R, Antibody associated lymphotoxin in acute infections, J Clin Invest , 52 (1973) 1033.
7 Mayer S, Falkenrodt A & Tongio M M, Cold lymphocytotoxins in infections and parasitic infections , Tissue Antigens , 3 (1973) 431.
8 Kriesler M, Naito S & Terasaki P I, Cytotoxins in di sease, Tran splant Proc, 3 ( 1971 ) 112.
9 Serjeantson S & Dry P, Lymphocytotoxins in leprosy and in asymptomatic hepatiti s B virus infection , Clin Exp lmmwwl, 39 (1980) 289.
10 Naik S, Kumar B, Kaur S & Sehgal S, Cold reactive lymphocytotoxic antibodies in patients with tuberculoid and lepromatous leprosy, lnt .I Lepr, 55 (1987) 273.
II Williams R C, Emmons 1 D & Yunis E 1, Studies of human sera with cytotoxic activit y, J Clin in vest, 50 ( 197 1) 151 4.
12 DeHoratius R 1 & Messer R P, Lymphocytotoxic anti bodies in family members of pati ents wi th systemic lupus erythematosus, J Clinln vest , 55 (1975) 1254.
13 Korsmeyer S 1, Williams R C, Wilson I D & Strickland R G, Lymphocytotox ic antibody in in llammatory bowl disease: a

650 INDIAN J EXP BIOL, JULY 2000
family study, N Eng/ 1 Med, 293 ( 1975) 1117. 14 Wooley PH, Panayi G S & Batchelor J R, Lymphocytotoxins
in rheumatoid arthritis: prevalence, lymphocyte speci ticity and HLA-DR antigens, Ann Rheum Dis, 40 ( 1981) 154.
15 Hazelton R A, A study of lymphocytotoxins in the sera of families of patients with rheumatoid disease, Arthritis Rheum, 27 (1984) 233.
16 Uma H, Selvaraj P, Reetha A M, Xavier T, Prabhakar R & Narayanan P R, Lymphocytotoxic antibodies & immunity in pulmonary tuberculosis, Indian 1 Med Res, I 09 ( 1999) 5.
17 Holst E, Mitchison D A & Radhakri shna S, Examination of smears for tubercle bacilli by fluorescence microscopy, Indian 1 Med Res, 47 (1959) 495.
18 Terasaki P I & McClelland J D, Microdroplet assay of human serum cytotoxin , Nature, 204 (1964) 998.
19 Raj alingam R, Mehra N K, Jain R C, Myneedu V P & Pande 1 N, Polymerase chain reaction based sequence specitic oligonucleotide hybridization analysis of HLA class II antigens in pulmonary twberculosis: Relevance to chemotherapy and di sease severity, 1 Infect Dis, 173 ( 1996) 669.
20 Rajalingam R, Mehra N K, Chopra G S, Puri M M & Jain R C, Anti-lgG autoantibodies and possible immune regulatory mechanisms in patients with pulmonary tuberculosis, Tubercle & Lung Dis, 77 ( 1996) 502.
21 Birdsall H H & Rossen R D, Regulation of antibody release by naturally occurring anti-immunoglobulins in cultures of pokeweed mitogen stimulated human peripheral blood lymphocytes, 1 lmmwwl, 133 ( 1984) 1257.
22 Schocket A L & Weiner H L, Lymphocytotoxic antibodies in family members of patients with multiple sclerosis, Lancet, i (1978) 571.
23 Bogen B, Processing and presentation of immunoglobulin idiotypes toT cells, The Immunologist, I ( 1993) 121.
24 McKearn T J, Stnart F P & Fitch F W, Anti-idiotypic antibody
in rat transplantation immunity. I. Production of anti-idiotypic antibody in animals repeatedly immunized with alloantigens, 1 lmmunol, 113 (1974) 1876.
25 Wintield J B, Winchester R J & Kunkel H G, As ·ociation of cold-reactive antilymphocyte antibodies with lymphopenia in systemic lupus erythmatosus, Arthritis Rheum, 18 ( 1975) 587.
26 Serjeantson S, Theophilus J, Zimmet P, Court J, Grosoley J R & Elliott R B, Lymphocytotoxic antibodies and histocompatibility antigens in juvenile-on et diabetes mellitus, Diabetes, 38 (1981) 26.
27 DeHoratius R J, Henderson C & Strickland R G, Lymphocytotoxins in acute and chronic hepatiti s, Clin Exp lmmunol, 26 ( 1976) 21.
28 McDevitt H 0 & Chinitz A, Genetic control of antibody response: rel ationship between immune response and histocompatibility (H-2) type, Science, 163 ( 1969) 1207.
29 Osoba D, Dick H M, Voller A, Goosen T 1, Goosen T, Draper C C & de The G, Role of the HLA complex in the antibody response to malari a under natural conditions, Immunogenetics, 8 (1979) 323.
30 Raum D D, Awdeh Z L, Page P L, Yunis E J & Alper C A, MHC determinants of response to Rh immunization, 1 lmmunol, 132 (1984) 157.
31 Reeves W G, Gelsthorpe K, van der Minne P, Torensma R & Tattersall R B, HLA phenotype and insulin antibody production, Clin Exp lmmunol, 57 (1984) 443.
32 Bothamley G H, Beck J S, Schreuder G M, D'Amaro J, deYries R R P, Kardjito T & Ivanyi J, Association of tuberculosis and M. tuberculosis-specific antibody levels with HLA, 1 Infect Dis, 159 ( 1989) 549.
33 Selvaraj P, Uma H, Reetha A M, Xavier T, Prabhakar R & Narayanan P R, Influence of HLA-DR2 phenotype on humoral immunity and lymphocyte response to Mycobacterium tuberculosis culture ti lt rate antigens in pulmonary tuberculosis, Indian 1 Med Res, I 07 ( 1998) 208.