cms quality payment plan: opportunities towards health
TRANSCRIPT

CMS Quality Payment Program: Opportunities Towards Health Equity August 2017
This material was prepared by Health Services Advisory Group, the Medicare Quality Improvement Organization for Arizona, California, Florida, Ohio, and the U.S. Virgin Islands, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services, based on material from Telligen, the Quality Innovation Network National Coordinating Center. The contents presented do not necessarily reflect CMS policy. Publication No. QN-11SOW-XC-10272017-01
Table of Contents
Quick Glance ...................................................................................................................................1
Introduction ......................................................................................................................................2
The Role of QIN-QIOs in Addressing Disparities by Improving Health Equity ............................3
Broad Opportunities to Advance Health Equity under the CMS Quality Payment Program (QPP)4
QPP Overview ................................................................................................................................5
QIN-QIO Role in QPP .....................................................................................................................6
Opportunities to Advance Health Equity for Specific Populations under the QPP .........................7
A. American Indians and Alaska Natives (AI/AN) ...................................................................... 7
B. Persons with Communication Challenges ............................................................................... 9
C. Persons with Disabilities ........................................................................................................ 15
D. Rural Populations .................................................................................................................... 16
E. Other Priority Populations ...................................................................................................... 17
Opportunities to Improve Disparities Data Collection under the QPP ..........................................17
Appendix A. Health Equity............................................................................................................19
Appendix B: QPP Improvement Activities: Aligned with QIN-QIO Tasks, Health Equity Plan Priorities, and Target Groups .........................................................................................................20
Appendix C. QPP Quality Measures: Aligned with QIN-QIO Tasks and Health Equity Plan Priorities .........................................................................................................................................38
Appendix D. QPP Advancing Care Information: Aligned with QIN-QIO Tasks and Health Equity Plan Priorities .....................................................................................................................43
Appendix E. ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities, and Target Groups .........................................................................................................50
Appendix F. Merit-Based Incentive Payment System (MIPS) ......................................................71
Appendix G. Alternative Payment Models (APM) and Advanced APMs ....................................73
Appendix H. Comparisons Between MIPS, APMs, and Advanced APMs ...................................75
Appendix I. List of Acronyms .......................................................................................................76

CMS QPP Opportunities Towards Health Equity
Quick Glance
Health Services Advisory Group │1

CMS QPP Opportunities Towards Health Equity
Introduction
This document is a resource for Quality Innovation Network-Quality Improvement Organizations (QIN-QIOs) and the clinicians in their networks. It describes how the CMS Quality Payment Program (QPP)1 can potentially:
• Reward clinicians for furthering health equity;• Incentivize clinicians to work with QIN-QIOs on health equity initiatives; and• Advance the goals set out under the CMS Health Equity Plan.
Under the QPP, clinicians have the opportunity, through data reporting, to systematically track the impacts they are making on their patients’ health status while being rewarded financially for their efforts. Clinicians can choose, from among many options, how to participate in the QPP and which measures to report. These choices will determine the focus of their quality improvement efforts.
Equipped with the information contained in this document, QIN-QIOs can help clinicians identify QPP quality measures that are supported by QIN-QIO programs and that optimize benefits for the patient, community, and the clinician.
In this document, you will find a brief description of: 1) the QIN-QIOs’ work to advance health equity; 2) the CMS Quality Payment Program; 3) QPP provisions that support the collection of standardized demographic data (a prerequisite for assessing and addressing disparities); and 4) QPP measures that can advance the health of priority populations. In addition, Appendices B, C, D, and E provide cross-walks of QPP measures against QIN-QIO tasks and CMS Office of Minority Health (OMH) Health Equity Goals.
Disclaimer: This document is a resource for QIN-QIOs, produced by the Disparities Learning and Action Network (LAN) under the auspices of the Quality Innovation Network National Coordinating Center (QIN NCC). It is not intended to grant rights or impose obligations. The official Medicare program provisions are contained in the relevant laws, regulations, and rulings. Every reasonable effort has been made to ensure the document’s accuracy.
1 Also referred to as the Medicare Access and Children's Health Insurance Program (CHIP) Reauthorization Act (MACRA) Quality Payment Program (QPP).
Health Services Advisory Group │2

CMS QPP Opportunities Towards Health Equity
The Role of QIN-QIOs in Addressing Disparities by Improving Health Equity
Exhibit 1. Tasks of the QIN-QIO 11th Statement of Work
B.1: IMPROVING CARDIAC HEALTH AND REDUCING CARDIAC HEALTHCARE DISPARITIES
B.2: REDUCING DISPARITIES IN DIABETES CARE: EVERYONE WITH DIABETES COUNTS (EDC)
C.2: REDUCING HEALTHCARE-ACQUIRED CONDITIONS (HACs) IN NURSING HOMES
C.3: PROMOTE EFFECTIVE COMMUNICATION &COORDINATION OF CARE
C.3.6: MEDICATION SAFETY AND ADVERSE DRUG EVENT PREVENTION
C.3.10: ANTIBIOTIC STEWARDSHIP INCOMMUNITIES
D.1: QUALITY IMPROVEMENT THROUGH VALUE-BASED PAYMENT, QUALITY REPORTING AND THEPHYSICIAN FEEDBACK REPORTING PROGRAM
E.1: QUALITY IMPROVEMENT INITIATIVES
F.1: IMMUNIZATIONS: IMPROVING MEDICAREBENEFICIARY IMMUNIZATION RATES THROUGHIMPROVED TRACKING, DOCUMENTATION, ANDREPORTING WITH A SPECIAL FOCUS ON REDUCING IMMUNIZATION HEALTH CARE DISPARITIES
G.1: BEHAVIORAL HEALTH: IMPROVING IDENTIFICATION OF DEPRESSION AND ALCOHOLUSE DISORDER IN PRIMARY CARE AND CARETRANSITIONS FOR BEHAVIORAL HEALTHCONDITIONS
H.1 TRANSFORMING CLINICAL PRACTICE INITIATIVE
QIN-QIOs have long been integral to healthcare improvement initiatives by working with trusted local entities to improve health at the community level since 1972.2
The QIN-QIOs’ 11th Statement of Work (2014-2019) includes three tasks that explicitly focus on addressing disparities in cardiac health, diabetes, and immunizations (Exhibit 1). In addition, the QIN NCC, which supports the QIN-QIOs, was tasked with establishing a Disparities Learning and Action Network (LAN) for the QIN-QIOs.
The Disparities LAN, launched in December 2015, helps QIN-QIOs and the clinicians and patients within their networks to meet the goals for addressing disparities under the 11th Statement of Work. To the extent possible, the Disparities LAN seeks to add even more value for its participants and partners by aligning its efforts with those of the CMS Office of Minority Health (OMH) and by planning events that support healthcare organizations’ efforts to meet accreditation, certification, QPP, and other requirements.
2 Read more about the work QIN-QIOs are doing here.
Health Services Advisory Group │3

CMS QPP Opportunities Towards Health Equity
Health Disparities and Health Equity
“Health disparities are differences in health outcomes closely linked with social, economic, and environmental disadvantage. [Disparities] are often driven by the social conditions in which individuals live, learn, work, and play. Characteristics including race, ethnicity, disability, sexual orientation or gender identity, socio-economic status, geographic location, and other factors historically linked to exclusion or discrimination are known to influence the health of individuals, families, and communities.”3 Disparities are the metrics we use to measure the progress made towards reaching health equity.4
Health equity is a shared goal for QIN-QIOs, OMH, and many of the clinicians and partners working with QIN-QIOs to improve the quality of healthcare. Health equity is the state in which every person has the ability to be their “healthiest self.” Disparities are present when persons who do not have clean drinking water, fresh quality food, safe and secure housing, reliable and accessible transportation, adequate educational and healthcare services, and/or who have communication, accessibility, or other societal challenges (e.g., bias or discrimination) have more difficulty reaching optimal health status due to interacting factors present in their communities. For additional information on health equity, please see Appendix A.
QIN-QIOs play an important part in connecting the dots for clinicians and showing how various initiatives, such as the QPP, can reduce disparities and improve health equity for their patients.
Broad Opportunities to Advance Health Equity under the CMS Quality Payment Program (QPP)
The recently enacted QPP5 gives clinicians new tools, models, and incentives to help give their patients the best possible care. It also presents an opportunity to leverage complementary goals of the QPP, QIN-QIO tasks, and OMH Health Equity goals by selecting measures that address shared goals. QIN-QIOs can refer to Appendices B, C, D, and E for crosswalks of QPP measures against QIN-QIO tasks and CMS OMH Health Equity goals. There are four sets of QPP measures used in the crosswalks:
• Merit-Based Incentive Payment System (MIPS)o Appendix B - Improvement Activitieso Appendix C - Quality
3 CMS. Building an Organizational Response to Health Disparities. 4 Braveman, P. 2014.What Are Health Disparities and Health Equity? We Need to Be Clear. 5 QPP was first passed with bipartisan support in March 2015 and finalized on October 14, 2016.
Health Services Advisory Group │4
CMS QPP Opportunities Towards Health Equity
o Appendix D - Advancing Care Information (ACI)o Appendix E - Alternative Payment Models (APMs)
We envision that these crosswalks can help QIN-QIOs engage clinicians in activities that meet shared goals.
QPP Overview
Clinicians can choose how to take part in the QPP based on their practice size, specialty, location, and patient population. Clinicians may participate in the QPP under one of two tracks: the Merit-Based Incentive Program (MIPS) or through an Advanced Alternative Payment Model (APM). Clinicians have the opportunity to earn a positive payment adjustment and avoid a negative payment adjustment by submitting data on the quality of care provided, quality improvement activities conducted, and technology used. QPP-eligible clinicians include more than 700,000 clinicians including physicians, physician assistants, nurse practitioners, clinical nurse specialists, and registered nurse anesthetists who bill Medicare at least $30,000/year and who care for at least 100 Medicare patients.
A. Merit-Based Incentive Program (MIPS)
MIPS replaces the Physician Quality Reporting System (PQRS), the Medicare EHR Incentive Program (also known as Meaningful Use), and the Value-Based Modifier and adds the Improvement Activities Performance Category. Under the MIPS option, clinicians can choose what measures they will report in three categories: quality, improvement activities, and advancing care information. In addition, beginning in 2018, a portion of each clinician’s MIPS score will be determined based on the cost category.
Clinicians may participate in the MIPS by choosing one of three participation levels: test, partial, or full. To participate in the test level, clinicians must submit the minimum amount of 2017 data to Medicare to avoid a negative payment adjustment. For partial level participation, clinicians have until October 2, 2017 to start collecting data and must report at least 90 days of data. For full participation, clinicians must submit a full year of data to Medicare. Data should be submitted by March 2018 to avoid a penalty and potentially earn a positive payment adjustment. Performance-based payment adjustments will begin on January 1, 2019. Each clinician’s or clinician group’s score is calculated based on the data submitted. Additional information on MIPS is shown in Appendix F.
B. Advanced Alternative Payment Models (APMs)
Under the Advanced APM option, clinicians are rewarded for improving the quality of care. An APM is a payment approach that gives added incentive payments to provide high-quality and cost-efficient care. APMs can apply to a specific clinical condition, a care episode, or a population. Advanced APMs are a subset of APMs designated by CMS. Practices participating
Health Services Advisory Group │5

in advanced APMs must use certified Electronic Health Record (EHR) technology and can earn more for taking on some risk related to their patients' outcomes. For the 2017 Performance Year, there are seven Advanced APM options:
• Comprehensive ESRD Care (CEC) - Two-Sided Risk• Comprehensive Primary Care Plus (CPC+)• Next Generation ACO Model• Shared Savings Program - Track 2• Shared Savings Program - Track 3• Oncology Care Model (OCM) - Two-Sided Risk• Comprehensive Care for Joint Replacement (CJR) Payment Model (Track 1- CEHRT)
Additional information on Advanced APMs can be found in Appendix G.
QIN-QIO Role in QPP
Exhibit 2, below, in addition to Appendices B, C, D, and E, shows that many QIN-QIO tasks are aligned with MIPS Performance Category measures. The QPP gives clinicians the opportunity, through data reporting, to systematically demonstrate the specific impacts they are making on their patients’ health status while being rewarded financially for their efforts. It also creates new opportunities for QIN-QIOs to engage clinicians. As part of their scope of work, QIN-QIOs are tasked with raising awareness of the QPP and supporting clinicians’ successful participation in the program:
• For eligible clinicians in groups more than 15 clinicians (through the QIN-QIOs’ QPPtask);
• For eligible clinicians in groups of 15 or fewer clinicians, if the QIN-QIO holds a QPP-SURS contract (SURS= Small, Underserved, Rural, or Health professional Shortagearea)
The QIN-QIOs also help practices to attain QPP readiness by supporting the Transforming Clinical Practice Initiative (TCPI). To improve both QIN-QIOs’ and clinician’s chances of success, QIN-QIOs can:
• Help MIPS-track clinicians select reporting metrics that best fit their practice andpopulation; and
• Help all clinicians improve their performance on reporting metrics that align withQIN-QIO tasks (cardiac care, diabetes care, etc.).
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │6

CMS QPP Opportunities Towards Health Equity
Exhibit 2. Crosswalk of QIN-QIO Tasks and 2017 MIPS Performance Categories
QIN-QIO Tasks
# of Applicable Improvement
Activities Measures
# of Applicable Quality Measures
# of Applicable Advancing Care
Information Measures
(Set 1/Set 2)
B.1 – Cardiac Health 47 6 10/5 B.2 – Diabetes Care/Everyone withDiabetes Counts 49 6 9/5
C.2 – Nursing Home Care 16 1 1/2
C.3 – Care Coordination 39 18 7/4
C.3.6 – Medication Safety 37 11 9/7 D.1 – Quality Reporting/QualityPayment Program 16 0 3/2
E.1 – Quality ImprovementInitiatives 27 9 9/5
F.1 – Immunizations 7 0 5/4
G.1 – Behavioral Health 52 5 6/5 H.1 – Transforming Clinical Practice Initiative (TCPI) 22 5 1/2
Opportunities to Advance Health Equity for Specific Populations under the QPP
Under the QPP, clinicians can choose from a host of metrics that are most relevant to their patient populations and communities. Only two special populations – American-Indians and persons living in rural areas – are explicitly named under the QPP, but many QPP measures have far-reaching implications for other populations, including persons with chronic diseases, people with disabilities, persons of color, and people with limited English proficiency. We describe below the challenges and existing support for several vulnerable populations, and how QPP measures and other provisions might be leveraged to improve their health.
C. American Indians and Alaska Natives (AI/AN)
The QPP will impact clinicians at Indian Health Service, Tribally-operated, and Urban Indian health clinics or centers (I/T/Us). The Indian Health Service (IHS) is a federal agency that is part of the Department of Health and Human Services (HHS). IHS provides
Health Services Advisory Group │7

quality healthcare to American Indians and Alaska Natives (AI/AN) with the mission to raise the physical, mental, social, and spiritual health of AI/AN to the highest level.6
As a federal agency, IHS provides services to approximately 2.2 million AI/AN.7 This includes AI/AN Medicare eligible persons over the age of 65, younger disabled persons, and those using dialysis services. A Tribal Epidemiology Center 2013 report, Best Practices in American Indian and Native American Health,8 states the “Indian Health Care Delivery System (IHCDS) consists of approximately 594 healthcare facilities located in 35 states, including 49 hospitals and 545 ambulatory facilities (231 health centers, five school-based health centers, 133 health stations, and 180 Alaska Native village clinics), where direct healthcare services are provided by some 3,000 priority primary care providers,” many of who will be participating in QPP. According to the IHS Office of Information Technology, QPP affects clinicians who participate in Medicare Part B and therefore impacts most AI/AN Medicare beneficiaries who receive clinical professional services at I/T/U outpatient facilities.
Nationwide, I/T/Us are well equipped to address QPP strategic objectives as seen with their improved Patient Centered Medical Home (PCMH) model,9 certification of the electronic health records system Resource Patient Management System (RPMS),10 and goals of their quality framework.11
Smaller tribally-operated or Urban Indian clinics have the option to enroll as a Federally Qualified Health Center (FQHC), Rural Health Center (RHC), Critical Access Hospital (CAH), or larger group, or to be covered under an IHS unique tax identification number (TIN) or National Provider Identification (NPI). Many tribal and urban health centers are located in health professional shortage areas (HPSA)12 and serve the medically underserved. This alone may be a challenge if they cannot meet patient volume thresholds for QPP participation (i.e., see less than 100 Medicare eligible patients or receive less than $30,000 in Medicare reimbursements per year).
CMS QPP Opportunities Towards Health Equity
6 Overview. https://www.ihs.gov/aboutihs/overview/. Accessed May 5, 2017. 7 Indian Health Service. https://www.ihs.gov. Accessed May 5, 2017. 8 Tribal Epidemiology Centers, 2013. Best Practices in American Indian and Alaska Native Public Health.
http://www.glitc.org/forms/epi/tec-best-practices-book-2013.pdf. Accessed May 5, 2017. 9 Improving Patient Care (IPC). url: https://www.ihs.gov/ipc/. Accessed May 5, 2017. 10 Resource and Patient Management System. url: https://www.ihs.gov/RPMS/. Accessed May 5, 2017. 11 Indian Health Service (2017). New Quality Framework to Guide Delivery of Care at Indian Health Service. url:
https://www.ihs.gov/newsroom/pressreleases/2016pressreleases/new-quality-framework-to-guide-delivery-of-care-at-indian-health-service/. Accessed May 5, 2017.
12 HRSA, 2016. Health Professional Shortage Areas. url: https://bhw.hrsa.gov/shortage-designation/hpsas. Accessed May 5, 2017.
Health Services Advisory Group │8

I/T/Us that do meet the threshold and have fewer than 15 MIPS-eligible clinicians can benefit from technical assistance tailored to their needs: the QPP final rule set aside $100 million in technical assistance to support QPP participation for MIPS-eligible clinicians in small practices, rural areas, and health professional shortage areas (HPSAs), including I/T/Us. Several QIN-QIOs hold contracts to provide that support.
CMS QPP Opportunities Towards Health Equity
QPP MIPS performance measures provide specific opportunities to improve health equity for AI/AN through the options indicated in Appendix B.
QIN-QIOs can make a difference in Indian Health by supporting I/T/U participation in the QPP and by helping clinicians to work and conduct quality improvement activities in Indian Health Service, RHC and FQHC care settings. In combination with regular and meaningful CMS consultation with tribal officials,13 these actions can help address disparities on many levels.
Improvement Activity IA_PM_3 rewards clinicians for participating
in IHS, RHC, or FQHC care, using data and conducting continuous quality improvement activities to improve that care. This activity is highly weighted, meaning that it
counts for 20 or 40 possible points for clinicians’ Improvement
Activity score.
D. Persons with Communication Challenges
Most patients experience barriers to communicating with their clinicians. These barriers may relate to limited English proficiency; low health literacy; or disabilities including visual, hearing, and cognitive challenges. Communication challenges limit our opportunities to access care, receive an accurate diagnosis, follow an appropriate course of treatment, and be as healthy as we can be.
Priority 5 of the CMS Health Equity Plan14 for Improving Quality in Medicare is to improve communication and language access for individuals with limited English proficiency and persons with disabilities. Additionally, a recent brief from the CMS Office of Minority Health titled “Understanding Communication and Language Needs of Medicare Beneficiaries” provides additional details about Medicare beneficiaries with communication challenges
13 Centers for Medicare and Medicaid Services. Tribal Consultation. url: https://www.cms.gov/Outreach-and-Education/American-Indian-Alaska-Native/AIAN/Consultation.html, accessed May 5, 2017
14 Centers for Medicare and Medicaid Services (2015). The CMS Equity Plan for Improving Quality in Medicare. url: https://www.cms.gov/About-CMS/Agency-Information/OMH/OMH_Dwnld-CMS_EquityPlanforMedicare_090615.pdf
Health Services Advisory Group │9

nationwide and state-by-state. The brief also summarizes existing protections for these beneficiaries.15
Deploying effective communication strategies can help healthcare organizations to improve access, make care more patient-centered, and improve outcomes for all patients. Described below are common communication challenges in healthcare, solutions to overcome communication challenges, and new opportunities to improve communication under the QPP rule.
i. Common Communication Challenges in Healthcare
Research suggests that patients who receive adequate communication supports such as professional interpreter services and enhanced communication protocols can better manage chronic health conditions like diabetes16 and asthma17; better understand their medication regimens18,; have shorter hospital stays19; and experience fewer hospital readmissions20, 21 and patient safety events.22, 23, 24, 25 Barriers to communication include:
• Limited English Proficiency (LEP)
o Persons with LEP, defined as people who report speaking English less than“very well,” comprise approximately 8% of the Medicare population15, 26 or
CMS QPP Opportunities Towards Health Equity
15 Centers for Medicare and Medicaid Services (2017). Understanding Communication and Language Needs of Medicare Beneficiaries. https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/Issue-Briefs-Understanding-Communication-and-Language-Needs-of-Medicare-Beneficiaries.pdf, accessed 6/13/2017
16 Schillinger, D. et al. "Closing the loop: physician communication with diabetic patients who have low health literacy." Archives of internal medicine163.1 (2003): 83-90.
17 Paasche-Orlow MK et al. "Tailored education may reduce health literacy disparities in asthma self-management." American journal of respiratory and critical care medicine 172.8 (2005): 980-986.
18 Schillinger, Dean, et al. "Language, literacy, and communication regarding medication in an anticoagulation clinic: a comparison of verbal vs. visual assessment." Journal of health communication 11.7 (2006): 651-664.
19 Lindholm, Mary, et al. "Professional language interpretation and inpatient length of stay and readmission rates." Journal of general internal medicine27.10 (2012): 1294-1299.
20 Jack, Brian W., et al. "A reengineered hospital discharge program to decrease rehospitalization: a randomized trial." Annals of internal medicine150.3 (2009): 178-187.
21 Coleman EA., et al. "The care transitions intervention: results of a randomized controlled trial." Archives of internal medicine 166.17 (2006): 1822-1828.
22 Stewart MA. "Effective physician-patient communication and health outcomes: a review." CMAJ: Canadian Medical Association Journal 152.9 (1995): 1423.
23 Betancourt JR et al. "Improving patient safety systems for patients with limited English proficiency: a guide for hospitals." Rockville, MD: Agency for Healthcare Research and Quality (2012): 12-0041.
24 Karliner, Leah S., et al. "Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature." Health services research 42.2 (2007): 727-754.
25 Edwards M. et al. "The development of health literacy in patients with a long-term health condition: the health literacy pathway model." BMC Public Health 12.1 (2012): 1.
26 Robert Wood Johnson Foundation/State Health Access Data Assistance Center, 2014. State Estimates of Limited English Proficiency by Health Insurance Status. url: http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2014/rwjf414189
Health Services Advisory Group │10

3.7 million people. And while the largest concentration of Medicare beneficiaries with limited English proficiency can be found in California, Hawaii, and New York,15 all states have some Medicare beneficiaries with LEP. QIN-QIOs and providers may find it useful to peruse the National Council on Aging’s interactive map27 showing the proportion of Medicare beneficiaries who have limited English proficiency, by county.
• Low Health Literacy
o This condition affects most Americans. As noted in Ten Attributes of HealthLiterate Health Care Organizations,28 a recent report from the IOM RoundTable on Health Literacy, a majority of Americans (88%, according to theNational Assessment of Adult Literacy) have difficulty processinginformation they receive from their healthcare providers. This challengeresults not only from individuals’ capacities, but also from the complexity ofinformation communicated by healthcare providers, and the demands placedon patients and caregivers by the healthcare system.
• Disabilities
o A recent CMS data analysis shows that close to 8% of all Medicarebeneficiaries are blind or have low vision, and that racial and ethnicminorities are disproportionately affected, especially American Indian andAlaska Native beneficiaries (15%).15
o The CMS analysis also shows that nearly 15% of Medicare beneficiaries areconsidered deaf or hard of hearing. Further, prevalence of hearingimpairments is highest among beneficiaries who are American Indian orAlaska Native (20%), white (16%), or Native Hawaiian or other PacificIslander (15%), and lowest among those who are Asian (11%) or black (9%).Further information about groups most affected by hearing impairment isprovided in the CMS issue brief.15
ii. Solutions to Overcome Communication Challenges
There are many things providers can do to help patients overcome communication challenges. Some of the strategies are listed below.
CMS QPP Opportunities Towards Health Equity
27 National Council on Aging. Limited English Proficiency Visualization. url: https://www.ncoa.org/economic-security/benefits/visualizations/lepmap/, accessed May 5, 2017.
28 Brach C, Keller D, Hernandez LM, Baur C, Parker R, Dreyer B, Schyve P, Lemerise AJ, Schillinger D, 2012. The Ten Attributes of Health Literate Organizations. url: http://www.ahealthyunderstanding.org/Portals/0/Documents1/IOM_Ten_Attributes_HL_Paper.pdf
Health Services Advisory Group │11

• For language barriers:
o Ask patients about their language needs.o Offer qualified professional medical interpreters (in person, by telephone, or
video service) or certified bilingual clinicians, and partner with communityhealth workers.
o Offer sign language interpreters, knowing that: American Sign Language (ASL) is its own language and not simply a
signed version of English. Not all Deaf patients understand writtenEnglish.
Some patients may speak sign languages other than ASL.o Have on-hand health education materials and forms translated into the top
languages spoken by your patient population.o If you have interpreters on staff, include them in your quality improvement
and patient safety efforts. See for example the toolkit “Improving Safety forPatients with Limited English Proficiency” developed by the Agency forHealthcare Research and Quality.29
o Look for additional strategies and guidance in a forthcoming resource fromthe CMS Office of Minority Health.
• For low health literacy:
o Remember that most people have difficulty understanding healthcareinformation.
o Use the Health Literacy Universal Precautions Toolkit to better communicatewith all your patients.30
o Use teach-back to check patient understanding. Know that it takes practice todo teach-back effectively, and online training is available.31
• For persons with vision and hearing impairments:
o For Deaf persons: Offer sign language interpreting services (in-person or video). Use non-verbal cues, e.g. tap patient on shoulder when calling them
from the waiting room.
CMS QPP Opportunities Towards Health Equity
29 TeamSTEPPS Enhancing Safety for Patients with Limited English Proficiency Module. url: https://www.ahrq.gov/teamstepps/lep/index.html, accessed 8.9.2017
30 AHRQ Health Literacy Universal Precautions Toolkit. url: https://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/literacy-toolkit/index.html, accessed 8.9.2017
31 Teach-Back Toolkit. url: www.teachbacktraining.org/, accessed 8.9.2017
Health Services Advisory Group │12

o For persons who are hard of hearing: Offer audio amplifiers. Use non-verbal cues, e.g. tap patient on shoulder when calling them
from the waiting room. Review tip sheets such as the UCSF page on communicating with
people with hearing loss.32
o For persons who have visual impairments: Offer magnifying readers. Make sure lighting is strong enough for patients to read. Offer to read forms aloud. Learn more on how to communicate with persons who have visual
impairments (e.g., read the tip sheet from the American Foundationfor the Blind).33
o For persons with cognitive impairments: Know that many patients with cognitive impairments can make their
own healthcare decisions, though the decision-making process may beharder or take longer.
Share information with the patient in small, manageable pieces, overseveral sessions if need be.
Know your patient’s legal guardians (if any) and rights. ReviewAHRQ’s guides on the topic “Making Informed Consent an InformedChoice” for more details.34
For everyone:
Clear communication starts with respect for the patient. Here are several tips from the Agency for Healthcare Research and Quality to show respect and put patients at ease34:
• Be courteous.• Sit down so you are at the same level as your patients.• Make eye contact with your patients.• Listen to your patients, and try not to interrupt them.
CMS QPP Opportunities Towards Health Equity
32 Communicating with People with Hearing Loss. url: https://www.ucsfhealth.org/education/communicating_with_people_with_hearing_loss/, accessed 8.9.2017
33 Communicating Comfortably. url: afb.org/info/friends-and-family/etiquette/communicating-comfortably/235, accessed 8.9.2017
34 Agency for Healthcare Research and Quality. Making Informed Consent an Informed Choice. url: https://www.ahrq.gov/professionals/systems/hospital/informedchoice/index.html, accessed 8.9.2017
Health Services Advisory Group │13

• Use a caring tone of voice.• Display comfortable body language.• Be attentive to your patient's personal comfort during the discussion.• Don't rush the discussion.• Encourage the patient to ask questions.
Healthcare organizations are testing new ways to better communicate with their patients and improve outcomes every day.35, 36 We encourage QIN-QIOs and healthcare organizations to continue sharing insights, ideas and successes in this area.
iii. Opportunities to Improve Communication under the QPP
For MIPS-Eligible Clinicians:
Clinicians eligible for MIPS can be rewarded for supporting effective communication with patients by selecting one or more MIPS Quality Measures or Improvement Activities that support or are influenced by clear communications. These measures are shown in Appendices B, C, D, and E. While the descriptions of MIPS Performance Measures and Improvement Activities may not explicitly include terminology related to clear communication, there is an opportunity for QIN-QIOs to offer such content as part of their technical assistance package. For example, providers can select Performance Measure “Diabetes: Hemoglobin A1c (HbA1c) Poor Control (>9%)” (quality ID 001) and Improvement Activity IA_BE_3, “Engagement with QIN-QIO to implement self-management training programs.” Then, as part of their technical assistance package, QIN-QIOs can offer content on clear communications to improve providers’ performance on HbA1c control.
For Clinicians Enrolled in Advanced APMs:
Clinicians in Advanced APMs must report on quality metrics and meet requirements specific to each model. Within each model, program payment systems, requirements and metrics support and incentivize clinicians to assess and address communication needs for all patients – including patients with LEP, low health literacy, or communication difficulties resulting from disabilities. For example:
The Comprehensive Primary Care Plus (CPC+) model offers practices a care management fee per patient per month, which can be used to defray costs related to communication supports and services.
CMS QPP Opportunities Towards Health Equity
35 Berkman ND et al. Health Literacy Interventions and Outcomes: An Update of the Literacy and Health Outcomes Systematic Review of the Literature. Evidence Report/ Technology Assessment no. 199. (Prepared by RTI International–University of North Carolina Evidence-based Practice Center under contract 290-2007- 10056-I.) Rockville, MD: Agency for Healthcare Research and Quality; 2011.
36 Paasche-Orlow, Michael K., and Michael S. Wolf. "Promoting health literacy research to reduce health disparities." Journal of health communication15.S2 (2010): 34-41.
Health Services Advisory Group │14

The Oncology Care Model requires the provision of navigation and language services.
Several APM quality metrics focus on process and outcome measures that are likely to be strongly influenced by the quality of communication between clinicians and patients. These include readmission rates and metrics related to counseling and chronic disease self-management services.
E. Persons with Disabilities
One in five adults in the U.S. – more than 53 million people – report having a disability in vision, cognition, mobility, self-care, and/or independent living.37 Among Medicare beneficiaries, 41 % of those who are dually eligible have a disability.38 State-by-state prevalence of disability is available on the CDC Disability and Health website.
People with disabilities face added difficulties related to health. Co-morbid conditions occur at a higher prevalence among those with a disability – for example, the World Health Organization (WHO) reports that diabetes in people with schizophrenia is over twice as high than the general population,39 and cardiovascular morbidity was found to be increased 2-3 fold in people with severe mental illness.40 Further, for individuals of an underserved racial/ethnic group, having a disability amplifies health disparities.41 African Americans with disabilities report that their health is fair or poor almost five times more often than African Americans without disabilities.42
The CMS Office of Minority Health’s Equity Plan addresses some of the many challenges that people with disabilities face through three of its priorities: Increase the Ability of the Health Care Workforce to Meet the Needs of Vulnerable Populations (Priority 4); Improve Communication and Language Access for Individuals with Limited English Proficiency and Persons with Disabilities (Priority 5); and Increase Physical Accessibility of Health Care Facilities (Priority 6). In addition, a recent CMS Office of Minority Health brief provides
CMS QPP Opportunities Towards Health Equity
37 Courtney-Long, EA; Carroll, DD; Zhang, QC; Stevens, AC; Griffin-Blake, S; Armour, BS; and VA Campbell. (2015). Prevalence of Disability and Disability Type Among Adults — United States, 2013. MMWR. July 31, 2015 / 64(29); 777-783.
38 CMS Office of Minority Health. The CMS Equity Plan for Improving Quality in Medicare. 39 World Health Organization. (2016). Disability and Health. 40 Brown S, Mitchell C, Kim M; Inskip H.(2010). Twenty-five year mortality of a community cohort with
schizophrenia. Br J Psychiatry. 2010 Feb;196(2):116-21. 41 Blick R.N., Franklin M.D., Ellsworth D.W., Havercamp S.M., Kornblau, B.L. (2015). The Double Burden: Health
Disparities Among People of Color Living with Disabilities. Ohio Disability and Health Program. url: http://nisonger.osu.edu/sites/default/files/u4/the_double_burden_health_disparities_among_people_of_color_living_with_disabilities.pdf, accessed 6/6/2017
42 Centers for Disease Control and Prevention. Disability status data: fair or poor self-rated health by demographic groups. http://dhds.cdc.gov/dataviews/tabular?viewId=1074&geoId=1&subsetId=-1. Published November 24, 2014. Accessed November 2, 2015
Health Services Advisory Group │15

details on current protections for persons with disabilities under Federal law and CMS rules.43
Appendices B, C, D, and E identify areas where MIPS performance measures and ACO metrics directly or indirectly relate to improved care for persons with disabilities. These include many of the improvement activities related to beneficiary engagement and activities that relate to conditions that more often afflict persons with disabilities. QIN-QIOs can help clinicians “connect the dots” by showing clinicians how they can improve their performance on these metrics by improving access to care for persons with disabilities.
F. Rural Populations
There are 62 million Americans living in various rural and frontier U.S. regions. The QPP offers incentives and supports for small and rural practices44:
$100 million was set aside for QPP technical assistance over the next five years to MIPS-eligible clinicians in small practices, rural areas, and practices in HPSAs. In addition, the TCPI assists practices to prepare for APMs.
Solo and small practices may join virtual groups to combine MIPS reporting, anticipated to start in year two of the program.
In the Advancing Care category, small practices, rural practices, and practices located in HPSAs, and non-patient-facing MIPS eligible clinicians can get full points in the Improvement Activities category by completing one high-weighted or two medium-weighted Improvement Activities. By contrast, other practices will be required to complete four medium-weighted or two high-weighted MIPS Improvement Activities to get a perfect Improvement Activities score.45
The National Rural Health Association (NRHA) has also outlined what rural physicians and providers should know.46 Under the QPP rule, QIN-QIOs can encourage rural healthcare clinicians to select one or more MIPS Performance Measures that support rural health, as indicated in Appendix B.
CMS QPP Opportunities Towards Health Equity
43 Centers for Medicare and Medicaid Services (2017). Increasing the Physical Accessibility of Health Care Facilities. https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/Issue-Brief-Physical-AccessibilityBrief.pdf, accessed 6/13/2017
44 About Rural Health in America. https://nosorh.org/about-rural-health-in-america/ 45 CMS (2016). Quality Payment Program: Executive Summary (final rule). url:
https://qpp.cms.gov/docs/QPP_Executive_Summary_of_Final_Rule.pdf , accessed 5.8.2017 46 National Rural Health Association. MACRA and You: What is MACRA, and what does it mean for rural
providers and patients? url: https://www.ruralhealthweb.org/getattachment/Advocate/MACRA-and-Rural/NRHA_MACRA_analysis.pdf.aspx?lang=en-US, accessed May 8, 2017
Health Services Advisory Group │16

G. Other Priority Populations
Everyone deserves the opportunity to reach their highest health potential. Health equity involves eliminating barriers so that everyone can reach optimal health status. Health disparities prevent everyone from reaching their health goals and occur when certain people disproportionately experience a higher burden of morbidity and mortality and have lower quality, access, and use of healthcare and related services (e.g., health insurance). All six goals of the OMH Health Equity Plan are focused on the elimination of health disparities.
Populations experiencing health disparities include people of color, women, children, and older patients, those with special healthcare needs (e.g., cognitive, sensory, mental health, or physical disabilities), those with lower-incomes and those living in rural, and urban underserved areas. Other communities experiencing disparities include those experiencing disparities due to religious beliefs, sexual orientation, and gender identity, or LEP. These groups have been designated as priority populations by some Federal agencies.47
Priority populations interact with the nine factors of the Culture of Health Action Framework (education, employment, health systems and services, housing, income/wealth, physical environment, public safety, social environment, and transportation) resulting in various dimensions in which disparities present themselves. Disparities can also occur within subsets of populations. For example, health status among Hispanics has been shown to vary based on length of time in the US, immigration status, and primary language spoken.48
The types of disparities and the populations they affect vary greatly by locality. Multiple entities have developed health needs assessments (e.g., Montana health needs assessment example) to identify groups whose health would benefit from targeted efforts. Addressing health disparities positively affects the overall quality and cost of care for our communities and our nation as a whole. Appendices B - E demonstrate ways in which QIN-QIOs can assist clinicians in selecting QPP measures focused on reducing disparities specific to their communities.
Opportunities to Improve Disparities Data Collection under the QPP
Assessing and monitoring disparities requires that clinicians routinely collect standardized data on patients’ race, ethnicity, sexual orientation, gender identity, and other social, psychological, and behavioral aspects of health disparities.
CMS QPP Opportunities Towards Health Equity
47 Healthcare Research and Quality Act of 1999 (Public Law 106-129). 48 Kaiser Family Foundation. 2016. Disparities in Health and Health Care: Five Key Questions and Answers
Health Services Advisory Group │17

One of the strategic goals of the QPP rule is to “improve data and information sharing to provide accurate, timely, and actionable feedback to clinicians and other stakeholders.” Additionally, the CMS OMH Health Equity Plan includes a priority area to “Expand the collection, reporting, and analysis of standardized data.”14 Consistent with both goals, the QPP requires clinicians to report on their use of electronic health data under the Advancing Care Information Performance Category. This reporting requirement replaces the Medicare Electronic Health Record (EHR) Incentive Program, otherwise known as Meaningful Use. Clinicians are required to report information on selected measures that demonstrate the effective use of certified electronic health record technology (CEHRT) to support patient engagement and improved health care quality. Specifically, clinicians will be required to report on five - six measures (depending on the CEHRT edition (2014 or 2015)) that relate to the following areas:
• e-Prescribing
• providing patient access to health information
• conducting security risk analyses
• sending summary of care records
• request/accept summary of care measure
There are additional, optional Advancing Care Information measures for which clinicians will receive a bonus score during the initial years of the QPP.
For the transition year, these pertain to reporting to public health or clinical data registries. For example, the “Immunization Registry Reporting” measure states that “the MIPS eligible clinician is in active engagement with a public health agency to submit immunization data.” Reporting such data will allow public health agencies to then analyze progress toward statewide or regional healthcare goals, which often include goals toward eliminating or reducing health disparities. Additionally, clinicians can then utilize race/ethnicity and other health disparities data collected in their EHRs to stratify results of their analyses to identify whether health disparities exist in their populations. Clinicians can opt to report on a number of population health-related metrics within the categories of quality measures and improvement activities.
CMS QPP Opportunities Towards Health Equity
Activity ID “IA_PM_9” within improvement activities is for
“Participation in research that identifies interventions, tools, or
processes that can improve a targeted patient population.”
Electing to engage in such improvement activities will align a clinician with the goal of reducing
health disparities among the populations that they serve.
Health Services Advisory Group │18

CMS QPP Opportunities Towards Health Equity
Appendix A. Health Equity
The Robert Wood Johnson Foundation (RWJF) Culture of Health Action Framework49 describes nine factors that drive community improvement efforts focused on improving health equity by addressing health disparities in the following areas:
• Education
• Employment
• Health Systems and Services
• Housing
• Income/Wealth
• Physical Environment
• Public Safety
• Social Environment
• Transportation
The RWJF report describes the cost of health inequity as much higher than the cost of prevention and offers a variety of resources and toolkits to identify potential partners for community initiatives. Communities can benefit from the framework by understanding how health systems and services are connected to other community-based goals. The quality of healthcare is often associated with and affected by other community services (such as the presence of sidewalks and parks for outdoor exercise or public transportation to access health services).
49 Read the full RWJF report here: Communities in Action: Pathways to Health Equity
Health Services Advisory Group │19

CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │20
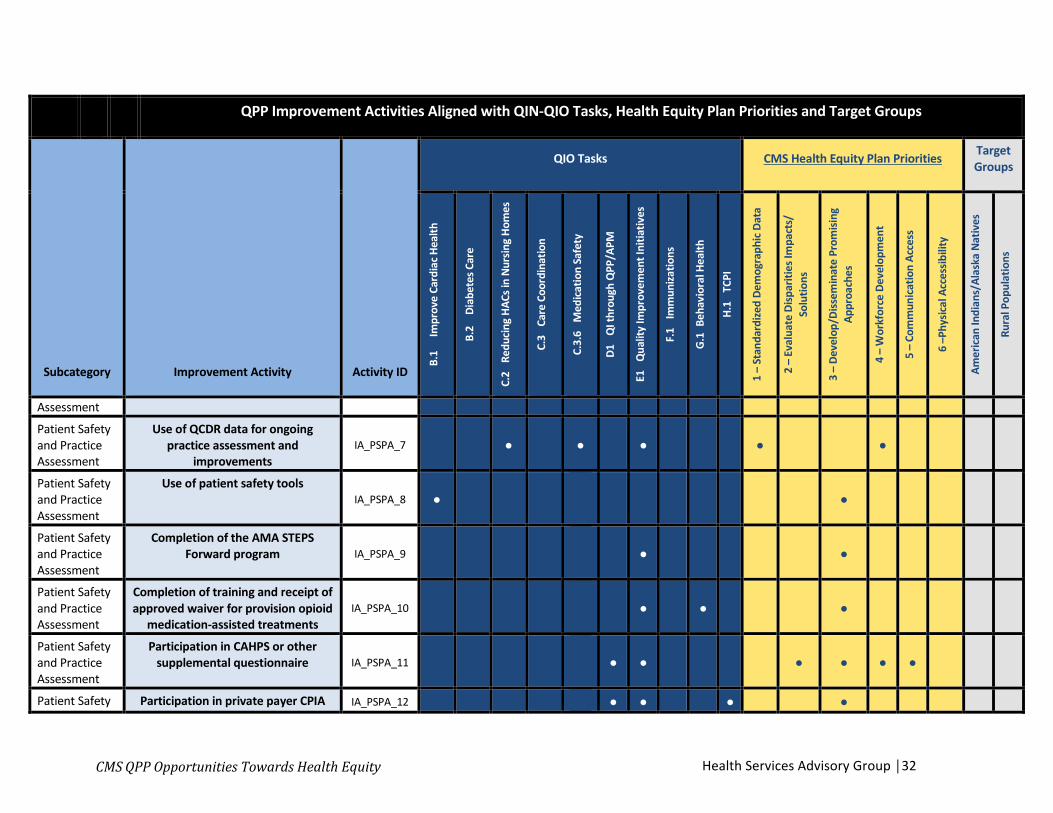
Appendix B: QPP Improvement Activities: Aligned with QIN-QIO Tasks, Health Equity Plan Priorities, and Target Groups
There are two ways in which clinicians may participate in the Quality Payment Program: 1) the Merit-based Incentive Payment System (MIPS) or Advanced Alternative Payment Models (Advanced APMs). Under MIPS, completing and reporting Improvement Activities are one of three ways physicians may get rewarded for care. There are eight Improvement Activity focus areas: Achieving Health Equity, Behavioral/Mental Health, Beneficiary Engagement, Care Coordination, Emergency Response and Preparedness, Expanded Practice Access, Patient Safety and Practice Assessment, and Population Management.
This document highlights Improvement Activities with mutual areas of focus between QIO Tasks and CMS Health Equity Plan Priorities. In some instances, Improvement Activities may target groups. Additional information on Improvement Activities may be found on the CMS website here.
For a downloadable version of these tables in Excel, visit https://www.hsag.com/contentassets/2e27a7ed0dd84a52a8dda33c727feefd/opportunities-towards-health-equity_app_b_mips_ia_crosswalk_508.xlsx. Please note that the Excel spreadsheets are currently 508-compliant but may not be 508-compliant after edits are made.
Disclaimer: This summary was prepared by the QIN NCC as a tool to assist QIN-QIOs. It is not intended to grant rights or impose obligations. The official Medicare Program provisions are contained in the relevant laws, regulations, and rulings. Every reasonable effort has been made to ensure accuracy.

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Achieving Health Equity
Engagement of new Medicaid patients and follow-up IA_AHE_1 ● ● ● ● ● ● ● ● ●
Achieving Health Equity
Leveraging a QCDR to standardize processes for screening IA_AHE_2 ● ● ● ● ● ● ● ● ● ● ●
Achieving Health Equity
Leveraging a QCDR to promote use of patient-reported outcome tools IA_AHE_3 ● ● ● ● ● ● ● ● ● ●
Achieving Health Equity
Leveraging a (Qualified Clinical Data Registry) QCDR for use of standard
questionnaires IA_AHE_4 ● ● ● ● ● ● ● ● ● ● ●
Health Services Advisory Group │21CMS QPP Opportunities Towards Health Equity

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Behavioral and Mental Health Diabetes screening IA_BMH_1 ● ● ● ● ● ●
Behavioral and Mental Health Tobacco use IA_BMH_2 ● ● ● ● ● ●
Behavioral and Mental Health Unhealthy alcohol use IA_BMH_3 ● ● ● ● ●
Behavioral and Mental Health Depression screening IA_BMH_4 ● ● ● ● ● ● ●
Behavioral and Mental Health
MDD prevention and treatment interventions IA_BMH_5 ● ● ● ● ● ●
Behavioral and Mental Health
Implementation of co-location PCP and MH services IA_BMH_6 ● ● ● ●
Behavioral and Mental Health
Implementation of integrated Primary Care Behavioral Health
(PCBH) model IA_BMH_7 ● ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │22

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Behavioral and Mental Health
Electronic Health Record Enhancements for BH data capture IA_BMH_8 ● ● ● ● ●
Beneficiary Engagement
Use of certified EHR to capture patient reported outcomes IA_BE_1 ● ● ● ● ● ● ● ●
Beneficiary Engagement
Use of QCDR to support clinical decision making IA_BE_2 ● ● ● ● ● ● ●
Beneficiary Engagement
Engagement with QIN-QIO to implement self-management training
programs IA_BE_3 ● ● ● ● ● ● ● ● ●
Beneficiary Engagement
Engagement of patients through implementation of improvements in
patient portal IA_BE_4 ● ● ● ● ● ● ● ● ●
Beneficiary Engagement
Enhancements/regular updates to practice websites/tools that also
include considerations for patients IA_BE_5 ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │23

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
with cognitive disabilities
Beneficiary Engagement
Collection and follow-up on patient experience and satisfaction data on
beneficiary engagement IA_BE_6 ● ● ● ● ● ● ● ● ● ● ●
Beneficiary Engagement
Participation in a QCDR, that promotes use of patient engagement
tools IA_BE_7 ● ● ● ● ● ● ●
Beneficiary Engagement
Participation in a QCDR, that promotes collaborative learning network opportunities that are
interactive
IA_BE_8 ● ● ● ● ● ● ●
Beneficiary Engagement
Use of QCDR patient experience data to inform and advance
improvements in beneficiary engagement
IA_BE_9 ● ● ● ● ● ● ● ● ● ● ● ● ●
Beneficiary Engagement
Participation in a QCDR, that promotes implementation of patient IA_BE_10 ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │24

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
self-action plans
Beneficiary Engagement
Participation in a QCDR, that promotes use of processes and tools that engage patients for adherence
to treatment plan
IA_BE_11 ● ● ● ● ●
Beneficiary Engagement
Use evidence-based decision aids to support shared decision-making IA_BE_12 ● ● ● ● ● ● ● ●
Beneficiary Engagement
Regularly assess the patient experience of care through surveys,
advisory councils and/or other mechanisms
IA_BE_13 ● ● ● ● ● ● ● ● ● ● ● ● ● ●
Beneficiary Engagement
Engage patients and families to guide improvement in the system of care IA_BE_14 ● ● ● ● ● ● ● ●
Beneficiary Engagement
Engage patients, family and caregivers in developing a plan of
care IA_BE_15 ● ● ● ● ● ● ● ● ●
Beneficiary Incorporate evidence-based IA_BE_16 ● ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │25

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Engagement techniques to promote self-management into usual care
Beneficiary Engagement
Use of tools to assist patient self-management IA_BE_17 ● ● ● ● ● ● ● ● ● ● ●
Beneficiary Engagement
Provide peer-led support for self-management IA_BE_18 ● ● ● ● ●
Beneficiary Engagement
Use group visits for common chronic conditions (e.g., diabetes) IA_BE_19 ● ● ● ● ● ● ● ● ●
Beneficiary Engagement
Implementation of condition-specific chronic disease self-management
support programs IA_BE_20 ● ● ● ● ● ●
Beneficiary Engagement
Improved practices that disseminate appropriate self-management
materials IA_BE_21 ● ● ● ● ● ● ● ● ●
Beneficiary Engagement
Improved practices that engage patients pre-visit IA_BE_22 ● ● ● ● ● ● ● ●
Beneficiary Integration of patient coaching IA_BE_23 ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │26

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Engagement practices between visits
Care Coordination
Implementation of use of specialist reports back to referring clinician or
group to close referral loop. IA_CC_1 ● ● ● ● ●
Care Coordination
Implementation of improvements that contribute to more timely communication of test results
IA_CC_2 ● ● ● ●
Care Coordination
Implementation of additional activity as a result of TA for improving care
coordination IA_CC_3 ● ● ● ● ● ● ● ● ● ● ●
Care Coordination
TCPI participation IA_CC_4 ● ● ● ● ● ●
Care Coordination
CMS partner in Patients Hospital Engagement Network IA_CC_5 ● ● ● ● ● ● ●
Care Use of QCDR to promote standard IA_CC_6 ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │27

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Coordination practices, tools and processes in practice for improvement in care
coordination
Care Coordination
Regular training in care coordination IA_CC_7 ● ● ● ●
Care Coordination
Implementation of documentation improvements for practice/process
improvements IA_CC_8 ● ● ● ● ● ●
Care Coordination
Implementation of practices/processes for developing
regular individual care plans IA_CC_9 ● ● ● ● ● ● ●
Care Coordination
Care transition documentation practice improvements IA_CC_10 ● ● ● ● ● ●
Care Coordination
Care transition standard operational improvements IA_CC_11 ● ● ● ● ●
Care Coordination
Care coordination agreements that promote improvements in patient IA_CC_12 ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │28

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
tracking across settings
Care Coordination
Practice improvements for bilateral exchange of patient information IA_CC_13 ● ● ● ● ● ● ●
Care Coordination
Practice improvements that engage community resources to support
patient health goals IA_CC_14 ● ● ● ● ● ● ● ● ●
Emergency Response & Preparedness
Participation on Disaster Medical Assistance Team (DMAT), registered
for 6 months. IA_ERP_1 ● ● ● ● ● ●
Emergency Response & Preparedness
Participation in a 60-day or greater effort to support domestic or
international humanitarian needs. IA_ERP_2 ● ● ● ● ● ●
Expanded Practice Access
Provide 24/7 access to eligible clinicians or groups who have real-
time access to patient's medical IA_EPA_1 ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │29

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
record
Expanded Practice Access
Use of telehealth services that expand practice access IA_EPA_2 ● ● ● ● ● ● ●
Expanded Practice Access
Collection and use of patient experience and satisfaction data on
access IA_EPA_3 ● ● ● ● ● ● ● ● ● ● ● ● ●
Expanded Practice Access
Additional improvements in access as a result of QIN-QIO TA IA_EPA_4 ● ● ● ● ● ● ●
Patient Safety and Practice Assessment
Participation in an AHRQ-listed patient safety organization. IA_PSPA_1 ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │30

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Patient Safety and Practice Assessment
Participation in MOC Part IV IA_PSPA_2 ● ● ● ●
Patient Safety and Practice Assessment
Participate in IHI Training/Forum Event; National Academy of
Medicine, AHRQ Team STEPPS(R) or other similar activity
IA_PSPA_3 ● ● ●
Patient Safety and Practice Assessment
Administration of the AHRQ Survey of Patient Safety Culture:
Administration of the AHRQ Survey of Patient Safety Culture and submission of data to the comparative database.
IA_PSPA_4 ● ● ● ● ● ● ●
Patient Safety and Practice Assessment
Annual registration in the Prescription Drug Monitoring
Program IA_PSPA_5 ● ● ●
Patient Safety and Practice
Consultation of the Prescription Drug Monitoring
IA_PSPA_6 ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │31
-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Assessment
Patient Safety and Practice Assessment
Use of QCDR data for ongoing practice assessment and
improvements IA_PSPA_7 ● ● ● ● ●
Patient Safety and Practice Assessment
Use of patient safety tools IA_PSPA_8 ● ●
Patient Safety and Practice Assessment
Completion of the AMA STEPS Forward program IA_PSPA_9 ● ●
Patient Safety and Practice Assessment
Completion of training and receipt of approved waiver for provision opioid
medication-assisted treatments IA_PSPA_10 ● ● ●
Patient Safety and Practice Assessment
Participation in CAHPS or other supplemental questionnaire IA_PSPA_11 ● ● ● ● ● ●
Patient Safety Participation in private payer CPIA IA_PSPA_12 ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │32

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
and Practice Assessment
Patient Safety and Practice Assessment
Participation in Joint Commission Evaluation Initiative IA_PSPA_13 ● ● ●
Patient Safety and Practice Assessment
Participation in Bridges to Excellence or other similar program IA_PSPA_14 ● ● ●
Patient Safety and Practice Assessment
Implementation of antibiotic stewardship program IA_PSPA_15 ● ● ● ●
Patient Safety and Practice Assessment
Use of decision support and standardized treatment protocols IA_PSPA_16 ● ● ● ● ● ● ●
Patient Safety and Practice Assessment
Implementation of analytic capabilities to manage total cost of
care for practice population IA_PSPA_17 ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │33

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Patient Safety and Practice Assessment
Measurement and improvement at the practice and panel level IA_PSPA_18 ● ● ● ●
Patient Safety and Practice Assessment
Implementation of formal quality improvement methods, practice
changes or other practice improvement processes
IA_PSPA_19 ● ● ●
Patient Safety and Practice Assessment
Leadership engagement in regular guidance and demonstrated
commitment for implementing practice improvement changes
IA_PSPA_20 ● ● ●
Patient Safety and Practice Assessment
Implementation of fall screening and assessment programs IA_PSPA_21 ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │34

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Population Management
Participation in systematic anticoagulation program IA_PM_1 ● ● ●
Population Management
Anticoagulant management improvements IA_PM_2 ● ● ●
Population Management
RHC, IHS or FQHC quality improvement activities IA_PM_3 ● ● ● ● ● ● ●
Population Management
Glycemic management services IA_PM_4 ● ● ●
Population Management
Engagement of community for health status improvement IA_PM_5 ● ● ● ● ● ● ● ●
Population Management
Use of toolsets or other resources to close healthcare disparities across
communities IA_PM_6 ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
Population Management
Use of QCDR for feedback reports that incorporate population health IA_PM_7 ● ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │35

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
Population Management
Participation in CMMI models such as Million Hearts Campaign IA_PM_8 ● ● ● ● ●
Population Management
Participation in population health research IA_PM_9 ● ● ● ● ● ● ● ●
Population Management
Use of QCDR data for quality improvement such as comparative
analysis reports across patient populations
IA_PM_10 ● ● ● ● ● ●
Population Management
Regular review practices in place on targeted patient population needs IA_PM_11 ● ● ● ● ● ● ● ● ● ● ● ●
Population Management
Population empanelment IA_PM_12 ● ● ● ●
Population Management
Chronic care and preventative care management for empanelled
patients IA_PM_13 ● ● ● ● ● ● ● ●
Population Management
Implementation of methodologies for improvements in longitudinal IA_PM_14 ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │36

-
–
-
- -
-
-
- -
-
QPP Improvement Activities Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Subcategory Improvement Activity Activity ID
QIO Tasks CMS Health Equity Plan Priorities Target Groups
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Amer
ican
Indi
ans/
Alas
ka N
ativ
es
Rura
l Pop
ulat
ions
care management for high risk patients
Population Management
Implementation of episodic care management practice improvements IA_PM_15 ● ● ● ● ● ●
Population Management
Implementation of medication management practice improvements IA_PM_16 ● ● ● ● ● ● ●
*Please note, MIPS measures marked as applicable to the TCPI are based on alignment with TCPI Common Measures for PracticeTransformation Networks (PTNs). Many of the other MIPS measures not indicated are generally related to the overarching goals of TCPI. Additional information about TCPI measures can be found here.
**For the “Weight” column, “H” indicates a weighting of high, while “M” indicates a weighting of medium.
***Target Groups are only indicated when explicitly named in the measure. Many of the other MIPS measures not indicated are generally related to the overarching goals of target groups.
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │37
Appendix C. QPP Quality Measures: Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
This document highlights MIPS Quality Measures with QIN-QIO Tasks and CMS Health Equity Plan Priorities. Additional information on MIPS Quality Measures may be found on the CMS website here.
For a downloadable version of these tables in Excel, visit https://www.hsag.com/contentassets/2e27a7ed0dd84a52a8dda33c727feefd/opportunities-towards-health-equity_app_c_mips_quality_crosswalk_508.xlsx. Please note that the Excel spreadsheets are currently 508-compliant but may not be 508-compliant after edits are made.
Disclaimer: This summary was prepared by the QIN NCC as a tool to assist QIN-QIOs. It is not intended to grant rights or impose obligations. The official Medicare Program provisions are contained in the relevant laws, regulations, and rulings. Every reasonable effort has been made to ensure accuracy.
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │38

-
–
-
- -
- -
- -
–
QPP MIPS Quality Measures Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
Subcategory Quality Measure Quality
ID High
Priority
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
E.1
Qua
lity
Impr
ovem
ent
Initi
ativ
es
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Data
2 –
Eval
uate
Disp
ariti
esIm
pact
s/ S
olut
ions
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
App
roac
hes
4 –
Vuln
erab
le P
opul
atio
ns
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Communication and Care Coordination
Dementia: Caregiver Education and Support 288 ● ● ● ● ● ● ●
Communication and Care Coordination
Dementia: Counseling Regarding Safety Concerns 286 ● ● ● ● ● ● ●
Communication and Care Coordination
Diabetic Retinopathy: Communication with the Physician Managing Ongoing Diabetes Care
19 ● ● ● ● ● ●
Communication and Care Coordination
Falls: Plan of Care 155 ● ● ● ● ● ●
Communication and Care Coordination
Adult Major Depressive Disorder (MDD): Coordination of Care of Patients with Specific Comorbid
Conditions
325 ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │39

-
–
-
- -
- -
- -
–
QPP MIPS Quality Measures Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
Subcategory Quality Measure Quality
ID High
Priority
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
E.1
Qua
lity
Impr
ovem
ent
Initi
ativ
es
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Data
2 –
Eval
uate
Disp
ariti
esIm
pact
s/ S
olut
ions
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
App
roac
hes
4 –
Vuln
erab
le P
opul
atio
ns
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Community/ Population Health
Preventive Care and Screening: Screening for Clinical Depression and
Follow-Up Plan 134 ● ● ● ● ● ● ●
Community/ Population Health
Preventive Care and Screening: Screening for High Blood Pressure
and Follow-Up Documented 317 ● ● ● ● ● ●
Community/ Population Health
Preventive Care and Screening: Tobacco Use: Screening and
Cessation Intervention 226 ● ● ● ●
Community/ Population Health
Preventive Care and Screening: Unhealthy Alcohol Use: Screening &
Brief Counseling 431 ● ● ● ● ●
Effective Clinical Care
Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy
(appropriate use of) 326 ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │40

-
–
-
- -
- -
- -
–
QPP MIPS Quality Measures Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
Subcategory Quality Measure Quality
ID High
Priority
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
E.1
Qua
lity
Impr
ovem
ent
Initi
ativ
es
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Data
2 –
Eval
uate
Disp
ariti
esIm
pact
s/ S
olut
ions
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
App
roac
hes
4 –
Vuln
erab
le P
opul
atio
ns
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Effective Clinical Care Controlling High Blood Pressure 236 ● ● ● ● ● ● ● ● ●
Effective Clinical Care Diabetes: Eye Exam 117 ● ● ● ● ●
Effective Clinical Care Diabetes: Foot Exam 163 ● ● ● ● ●
Effective Clinical Care
Diabetes: Hemoglobin A1c (HbA1c) Poor Control (>9%) 1 ● ● ● ● ● ● ● ●
Effective Clinical Care
Hypertension: Improvement in Blood Pressure 373 ● ● ● ● ● ● ●
Effective Clinical Care
Statin Therapy for the Prevention and Treatment of Cardiovascular
Disease 438 ● ● ● ● ● ● ●
Effective Clinical Care
Stroke and Stroke Rehabilitation: Discharged on Antithrombotic
Therapy 32 ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │41

-
–
-
- -
- -
- -
–
QPP MIPS Quality Measures Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
Subcategory Quality Measure Quality
ID High
Priority
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
E.1
Qua
lity
Impr
ovem
ent
Initi
ativ
es
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Data
2 –
Eval
uate
Disp
ariti
esIm
pact
s/ S
olut
ions
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
App
roac
hes
4 –
Vuln
erab
le P
opul
atio
ns
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Patient Safety Documentation of Current Medications in the Medical Record 130 ● ● ● ● ● ● ● ● ● ●
*Please note, MIPS Quality measures marked as applicable to the TCPI are based on alignment with TCPI Common Measures for Practice Transformation Networks (PTNs). Many of the other MIPS measures not indicated are generally related to the overarching goals of TCPI. Additional information about TCPI measures can be found here.
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │42

Appendix D. QPP Advancing Care Information: Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
This document highlights Advancing Care Information measures with QIO Tasks and CMS Health Equity Plan Priorities. The 2017 Advancing Care Information category has 2 sets of measures to choose from based on EHR edition: 1) Advancing Care Information Objectives and Measures (composed of 25 measures) and 2) 2017 Advancing Care Information Transition Objectives and Measures (composed of 11 measures).
Additional information on Advancing Care Information may be found on the CMS website here.
For a downloadable version of these tables in Excel, visit https://www.hsag.com/contentassets/2e27a7ed0dd84a52a8dda33c727feefd/opportunities-towards-health-equity_app_d_mips_aci_crosswalk-508.xlsx. Please note that the Excel spreadsheets are currently 508-compliant but may not be 508-compliant after edits are made.
Disclaimer: This summary was prepared by the QIN NCC as a tool to assist QIN-QIOs. It is not intended to grant rights or impose obligations. The official Medicare Program provisions are contained in the relevant laws, regulations, and rulings. Every reasonable effort has been made to ensure accuracy.
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │43

-
–
-
- -
-
-
- -
-
MIPS Advancing Care Information Measures Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
Objective Objective Name
Measure ID/ 2017 Measure
ID
Performance Score Weight/Required for
Base Score
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Advancing Care Information Objectives and Measures
Public Health and Clinical Data Registry Reporting
Clinical Data Registry Reporting
ACI_PHC DRR_5 0/NO ● ● ● ● ●
Health Information Exchange
Clinical Information Reconciliation
ACI_HIE_ 3 Up to 10%/NO ● ● ● ● ● ● ● ●
Electronic Prescribing e-Prescribing ACI_EP_1 0/YES ● ● ● ● ●
Public Health and Clinical Data Registry Reporting
Electronic Case Reporting
ACI_PHC DRR_3 0/NO ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │44

-
–
-
- -
-
-
- -
-
MIPS Advancing Care Information Measures Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
Objective Objective Name
Measure ID/ 2017 Measure
ID
Performance Score Weight/Required for
Base Score
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Public Health and Clinical Data Registry Reporting
Immunization Registry Reporting
ACI_PHC DRR_1 0 or 10%/NO ● ● ●
Patient Electronic Access
Patient-Specific Education
ACI_PEA_ 2 Up to 10%/NO ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
Patient Electronic Access Provide Patient Access ACI_PEA_
1 Up to 10%/YES ● ● ● ● ● ● ● ● ●
Public Health and Clinical Data Registry Reporting
Public Health Registry Reporting
ACI_PHC DRR_4 0/NO ● ● ● ●
Health Information Exchange
Request/Accept Summary of Care
ACI_HIE_ 2 Up to 10%/YES ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │45

-
–
-
- -
-
-
- -
-
MIPS Advancing Care Information Measures Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
Objective Objective Name
Measure ID/ 2017 Measure
ID
Performance Score Weight/Required for
Base Score
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Coordination of Care Through Patient Engagement
Secure Messaging ACI_CCTP E_2 Up to 10%/NO ● ● ● ● ● ●
Health Information Exchange
Send a Summary of Care
ACI_HIE_ 1 Up to 10%/YES ● ● ● ● ● ●
Public Health and Clinical Data Registry Reporting
Syndromic Surveillance Reporting
ACI_PHC DRR_2 0/NO ● ●
Coordination of Care Through Patient Engagement
View, Download and Transmit (VDT)
ACI_CCTP E_1 Up to 10%/NO ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │46

-
–
-
- -
-
-
- -
-
MIPS Advancing Care Information Measures Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
Objective Objective Name
Measure ID/ 2017 Measure
ID
Performance Score Weight/Required for
Base Score
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Public Health and Clinical Data Registry Reporting
Clinical Data Registry Reporting
ACI_PHC DRR_5 0/NO ● ● ● ● ● ● ●
2017 Advancing Care Information Transition Objectives and Measures
Electronic Prescribing e-Prescribing ACI_TRA
NS_EP_1 0/YES ● ● ● ● ●
Health Information Exchange
Health Information Exchange
ACI_TRA NS_HIE_
1 Up to 20%/YES ● ● ● ● ● ● ● ● ● ● ● ● ●
Public Health Reporting Immunization Registry
Reporting
ACI_TRA NS_PHCD
RR_1 0 or 10%/NO ● ● ●
Medication Reconciliation Medication
Reconciliation
ACI_TRA NS_MR_
1 Up to 10%/NO ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │47

-
–
-
- -
-
-
- -
-
MIPS Advancing Care Information Measures Aligned with QIN-QIO Tasks and Health Equity Plan Priorities
Objective Objective Name
Measure ID/ 2017 Measure
ID
Performance Score Weight/Required for
Base Score
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
E1
Qua
lity
Impr
ovem
ent I
nitia
tives
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Patient Specific Education Patient-Specific
Education
ACI_TRA NS_PSE_
1 Up to 10%/NO ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
Patient Electronic Access Provide Patient Access
ACI_TRA NS_PEA_
1 Up to 20%/YES ● ● ● ● ● ● ● ● ●
Secure Messaging Secure Messaging ACI_TRA
NS_SM_1 Up to 10%/NO ● ● ● ● ● ●
Public Health Reporting Specialized Registry
Reporting
ACI_TRA NS_PHCD
RR_3 0/NO ● ● ● ●
Public Health Reporting Syndromic Surveillance
Reporting
ACI_TRA NS_PHCD
RR_2 0/NO ● ●
Patient Electronic Access View, Download, or
Transmit (VDT)
ACI_TRA NS_PEA_
2 Up to 10% ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │48

*Please note, Advancing Care Information measures marked as applicable to the TCPI are based on alignment with TCPI CommonMeasures for Practice Transformation Networks (PTNs). Many of the other MIPS measures not indicated are generally related to the overarching goals of TCPI. Additional information about TCPI measures can be found here.
Many of the other MIPS measures not indicated are generally related to the overarching goals of target groups.
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │49
Appendix E. ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities, and Target Groups
Accountable Care Organizations (ACO) are required to completely and accurately report quality data to calculate and assess their quality performance. Metrics vary by ACO type and performance year. This document shows quality measures used to assess ACO performance for 2016 and 2017 for the Shared Savings Program and the Next Generation ACO Model. Additional information on ACOs may be found on the CMS website here.
For additional information regarding CAHPS measures and their use in the ACO program, please refer to the CAHPS® Survey for Accountable Care Organizations Participating in Medicare Initiatives website: http://acocahps.cms.gov/en/survey-instruments/. Further documentation on ACO performance measures is provided in the GPRO Web Interface Narrative Specification: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2016_GPRO_WI_Msr_List_Narr_Specs_and_RN.zip
For a downloadable version of these tables in Excel, visit https://www.hsag.com/contentassets/2e27a7ed0dd84a52a8dda33c727feefd/opportunities-towards-health-equity_app-e_aco_crosswalk_508.xlsx. Please note that the Excel spreadsheets are currently 508-compliant but may not be 508-compliant after edits are made.
Disclaimer: This summary was prepared by the QIN NCC as a tool to assist QIN-QIOs. It is not intended to grant rights or impose obligations. The official Medicare Program provisions are contained in the relevant laws, regulations, and rulings. Every reasonable effort has been made to ensure accuracy.
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │50

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Patient/ Caregiver Experience
CAHPS: Getting Timely care, Appointments, and Information
(2016, 2017)
ACO-1
NQF: 0005 ● ● ● ● ● ●
Patient/ Caregiver Experience
CAHPS: How Well Your Providers Communicate (2016, 2017)
ACO-2
NQF: 0005 ● ● ● ● ● ● ● ● ● ● ●
Patient/ Caregiver Experience
CAHPS: Patients’ Rating of Provider (2016, 2017)
ACO-3
NQF: 0005 ● ● ● ● ● ●
Patient/ Caregiver Experience
CAHPS: Access to Specialists (2016, 2017)
ACO-4 N/A ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │51

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Patient/ Caregiver Experience
CAHPS: Health Promotion and Education (2016, 2017)
ACO-5 N/A ● ● ● ● ● ● ● ● ● ●
Patient/ Caregiver Experience
CAHPS: Shared Decision Making (2016, 2017)
ACO-6 N/A ● ● ● ● ● ● ● ● ● ● ●
Patient/ Caregiver Experience
CAHPS: Health Status/Functional Status (2016, 2017)
ACO-7 N/A ● ●
Patient/ Caregiver Experience
CAHPS: Stewardship of Patient Resources (2016, 2017)
ACO-34 N/A ● ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │52
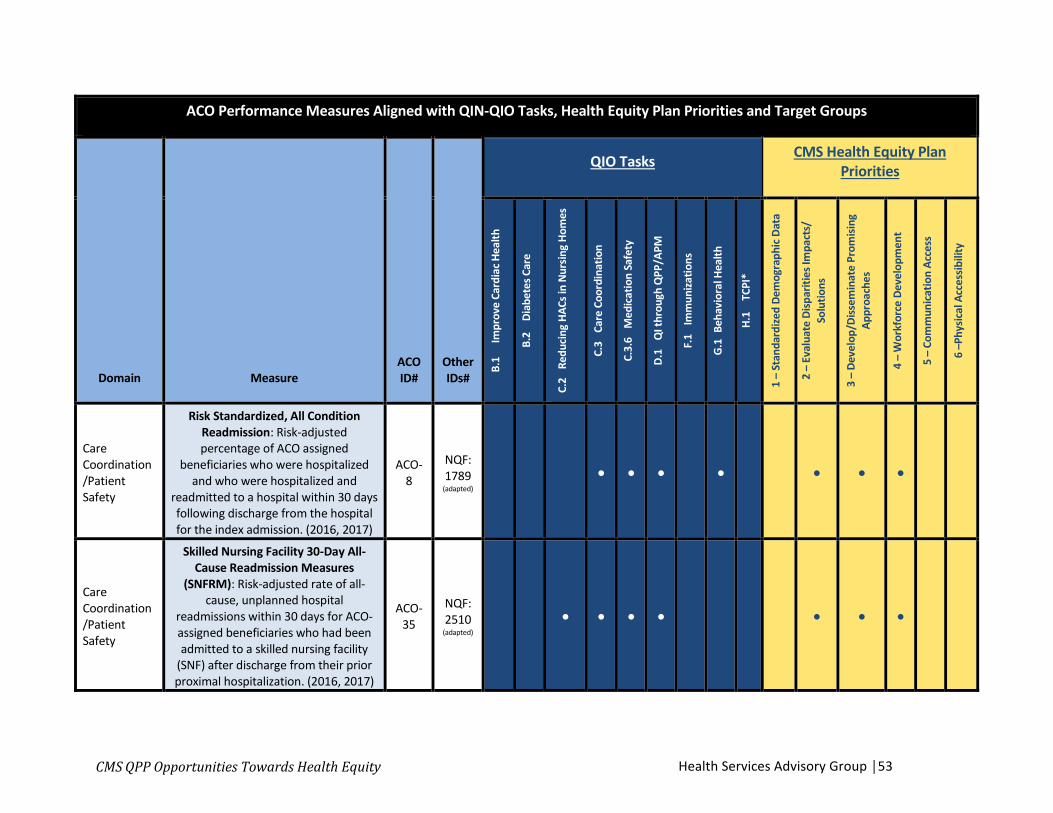
-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Care Coordination /Patient Safety
Risk Standardized, All Condition Readmission: Risk-adjusted percentage of ACO assigned
beneficiaries who were hospitalized and who were hospitalized and
readmitted to a hospital within 30 days following discharge from the hospital for the index admission. (2016, 2017)
ACO-8
NQF: 1789
(adapted)
● ● ● ● ● ● ●
Care Coordination /Patient Safety
Skilled Nursing Facility 30-Day All-Cause Readmission Measures
(SNFRM): Risk-adjusted rate of all-cause, unplanned hospital
readmissions within 30 days for ACO-assigned beneficiaries who had been admitted to a skilled nursing facility
(SNF) after discharge from their prior proximal hospitalization. (2016, 2017)
ACO-35
NQF: 2510
(adapted)
● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │53

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Care Coordination /Patient Safety
All-Cause Unplanned Admissions for Patients with Diabetes: Rate of risk-
standardized, acute, unplanned hospital admissions among
beneficiaries 65 years and older with diabetes who are assigned or aligned
to the ACO. (2016, 2017)
ACO-36 N/A ● ● ● ● ● ● ● ● ●
Care Coordination /Patient Safety
All-Cause Unplanned Admissions for Patients with Heart Failure: Rate of risk-standardized, acute, unplanned
hospital admissions among beneficiaries 65 years and older with
heart failure who are assigned or aligned to the ACO. (2016, 2017)
ACO-37 N/A ● ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │54

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Care Coordination /Patient Safety
All-Cause Unplanned Admissions for Patients with Multiple Chronic
Conditions: Rate of risk-standardized acute, unplanned hospital admissions
among beneficiaries 65 years and older with MCCs who are assigned or
aligned to the ACO. (2016, 2017)
ACO-38 N/A ● ● ● ● ● ● ● ● ● ● ●
Care Coordination /Patient Safety
Acute Composite (AHRQ Prevention Quality Indicator [PQI] #91): Risk-
adjusted rate of admissions for acute Prevention Quality Indicator (PQI) conditions: dehydration, bacterial
pneumonia, or urinary tract infection. (2017)
ACO-43 N/A ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │55

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Care Coordination /Patient Safety
Ambulatory Sensitive Conditions Admissions: COPD or Asthma in Older Adults: All discharges with an ICD-10-CM principal diagnosis code for COPD or asthma in adults ages 40 years and
older, for ACO assigned or aligned beneficiaries with COPD or asthma,
with risk-adjusted comparison of observed discharges to expected
discharges for each ACO.4 This is a ratio of observed to expected
discharges. (2016)
ACO-9
NQF: 0275 ● ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │56

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Care Coordination /Patient Safety
Ambulatory Sensitive Conditions Admissions: Heart Failure: All
discharges with an ICD-10-CM principal diagnosis code for HF in adults ages 18 years and older, for ACO assigned or
aligned beneficiaries with HF, with risk-adjusted comparison of observed
discharges to expected discharges for each ACO.5 This is a ratio of observed
to expected discharges. (2016)
ACO-10
NQF: 0277 ● ● ● ● ● ● ● ● ●
Care Coordination /Patient Safety
Percent of Primary Care Physicians who Successfully Meet Meaningful
Use Requirements: Percentage of ACO primary care physicians (PCPs) who
successfully attest to either the Medicare or Medicaid EHR Incentive
Program. (2016, 2017)
ACO-11 N/A ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │57
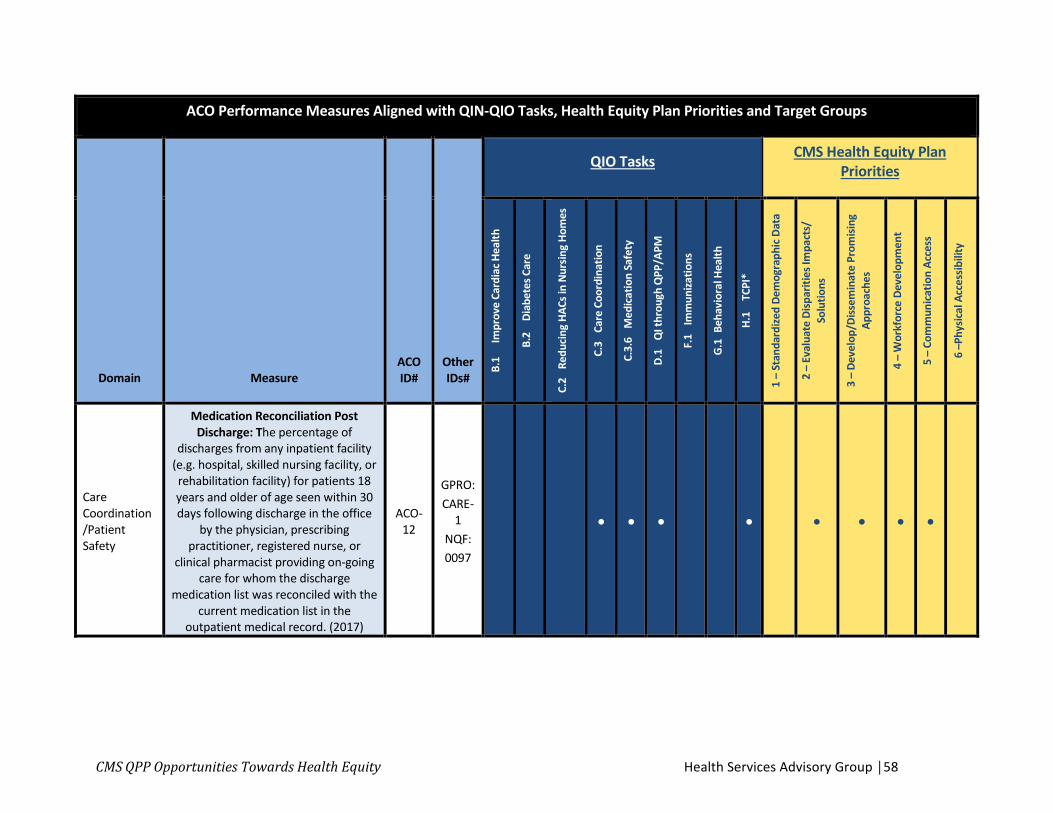
-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Care Coordination /Patient Safety
Medication Reconciliation Post Discharge: The percentage of
discharges from any inpatient facility (e.g. hospital, skilled nursing facility, or rehabilitation facility) for patients 18 years and older of age seen within 30 days following discharge in the office
by the physician, prescribing practitioner, registered nurse, or
clinical pharmacist providing on-going care for whom the discharge
medication list was reconciled with the current medication list in the
outpatient medical record. (2017)
ACO-12
GPRO: CARE-
1 NQF: 0097
● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │58

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Care Coordination /Patient Safety
Documentation of Current Medications in the Medical Record: Percentage of visits for patients aged
18 years and older for which the eligible professional attests to documenting a list of current
medications using all immediate resources available on the date of the
encounter. (2016)
ACO-39
GPRO: CARE-
3 NQF: 0419
● ● ● ● ● ● ● ●
Care Coordination /Patient Safety
Falls: Screening for Future Fall Risk: Percentage of patients 65 years of age
and older who were screened for future fall risk during the
measurement period (2016, 2017)
ACO-13
GPRO: CARE-
2 NQF: 0101
● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │59

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Care Coordination /Patient Safety
Use of Imaging Studies for Low Back Pain: The proportion of ACO assigned beneficiaries with a primary diagnosis of low back pain who did not have an imaging study (plain X-ray, MRI, or CT
scan) within 28 days of diagnosis. (2017)
ACO-44
NQF: 0052
● ● ●
Preventive Health
Preventive Care and Screening: Influenza Immunization: Percentage of patients aged 6 months and older
seen for a visit between October 1 and March 31 who received an influenza
immunization OR who reported previous receipt of an influenza
immunization (2016, 2017)
ACO-14
GPRO: PREV-
7 NQF: 0041
● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │60
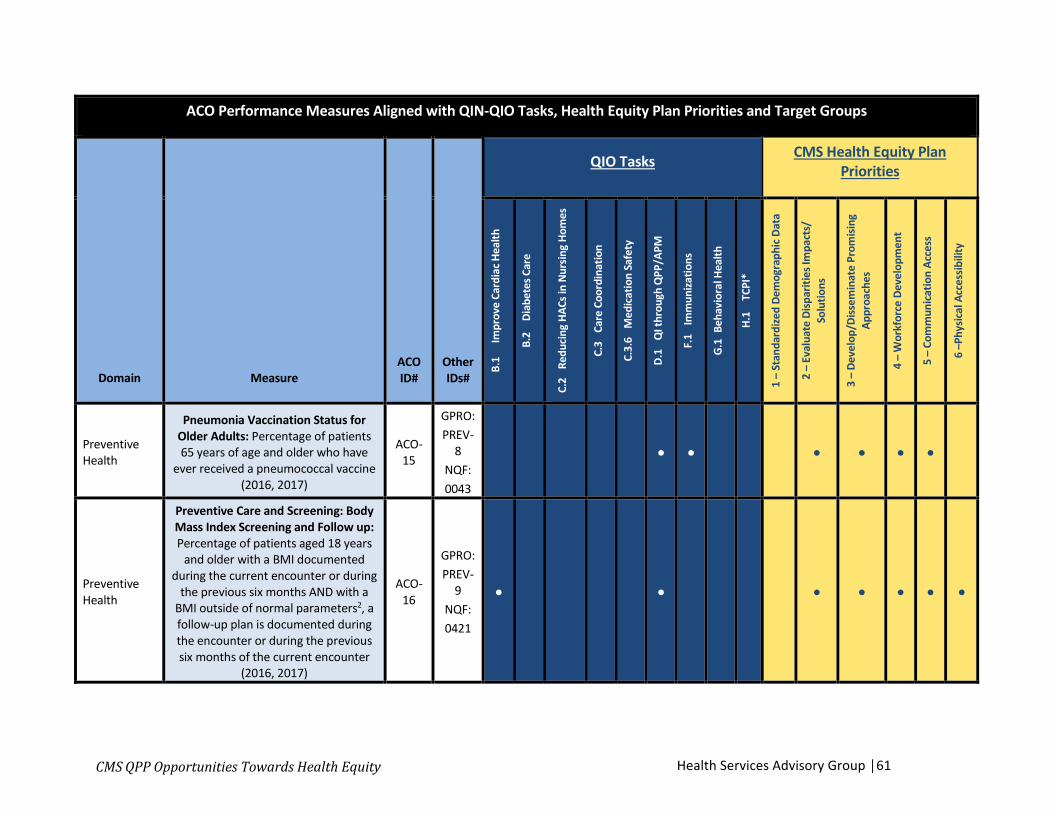
-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Preventive Health
Pneumonia Vaccination Status for Older Adults: Percentage of patients 65 years of age and older who have
ever received a pneumococcal vaccine (2016, 2017)
ACO-15
GPRO: PREV-
8 NQF: 0043
● ● ● ● ● ●
Preventive Health
Preventive Care and Screening: Body Mass Index Screening and Follow up: Percentage of patients aged 18 years
and older with a BMI documented during the current encounter or during
the previous six months AND with a BMI outside of normal parameters2, a follow-up plan is documented during the encounter or during the previous six months of the current encounter
(2016, 2017)
ACO-16
GPRO: PREV-
9 NQF: 0421
● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │61

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Preventive Health
Preventive Care and Screening: Tobacco Use: Screening and Cessation
Intervention: Percentage of patients aged 18 years and older who were
screened for tobacco use one or more times within 24 months AND who
received cessation counseling intervention if identified as a tobacco
user (2016, 2017)
ACO-17
GPRO: PREV-
10 NQF: 0028
● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │62

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Preventive Health
Preventive Care and Screening: Screening for Clinical Depression and
Follow-up Plan: Percentage of patients aged 12 years and older screened for clinical depression on the date of the encounter using an age appropriate
standardized depression screening tool AND if positive, a follow-up plan is
documented on the date of the positive screen (2016, 2017)
ACO-18
GPRO: PREV-
12 NQF: 0418
● ● ● ● ● ● ● ●
Preventive Health
Colorectal Cancer Screening: Percentage of adults 50 - 75 years of
age who had appropriate screening for colorectal cancer (2016, 2017)
ACO-19
GPRO: PREV-
6 NQF: 0034
● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │63

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Preventive Health
Breast Cancer Screening: Percentage of women 50 through 74 years of age who had a mammogram to screen for breast cancer within 27 months (2016,
2017)
ACO-20
GPRO: PREV-
5 ● ● ● ● ● ●
Preventive Health
Preventive Care and Screening: Screening for High Blood Pressure and Follow-up Documented: Percentage of patients aged 18 years and older seen during the reporting period who were screened for high blood pressure AND
a recommended follow-up plan is documented based on the current
blood pressure (BP) reading as indicated (2016)
ACO-21
GPRO: PREV-
11 ● ● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │64

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
Preventive Health
Statin Therapy for the Prevention and Treatment of Cardiovascular Disease: Percentage of the certain patients2—
all considered at high risk of cardiovascular events—who were
prescribed or were on statin therapy during the measurement period.
(2016, 2017)
ACO-42
GPRO: PREV-
13 ● ● ● ● ● ● ●
At Risk Population: Depression
Depression Remission at 12 Months: Adult patients age 18 and older with
major depression or dysthymia and an initial PHQ-9 score > 9 who
demonstrate remission at twelve months defined as PHQ-9 score less
than 5. (2016, 2017)
ACO-40
GPRO: MH-1 NQF: 0710
● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │65

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
At Risk Population: Diabetes
Diabetes: Hemoglobin A1c Poor Control: Percentage of patients 18 - 75
years of age with diabetes who had hemoglobin A1c > 9.0% during the measurement period (2016, 2017)
ACO-27
GPRO: DM-2 NQF: 0059
● ● ● ● ● ●
At Risk Population: Diabetes
Diabetes: Eye Exam: Percentage of patients 18 - 75 years of age with
diabetes who had a retinal or dilated eye exam by an eye care professional during the measurement period or a negative retinal exam (no evidence of retinopathy) in the 12 months prior to the measurement period (2016, 2017)
ACO-41
GPRO: DM-7 NQF: 0055
● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │66

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
At Risk Population: Hypertension
Controlling High Blood Pressure: Percentage of patients 18 - 85 years of
age who had a diagnosis of hypertension and whose blood
pressure was adequately controlled (< 140/90 mmHg) during the
measurement period (2016, 2017)
ACO-28
GPRO: HTN-2 NQF: 0018
● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │67
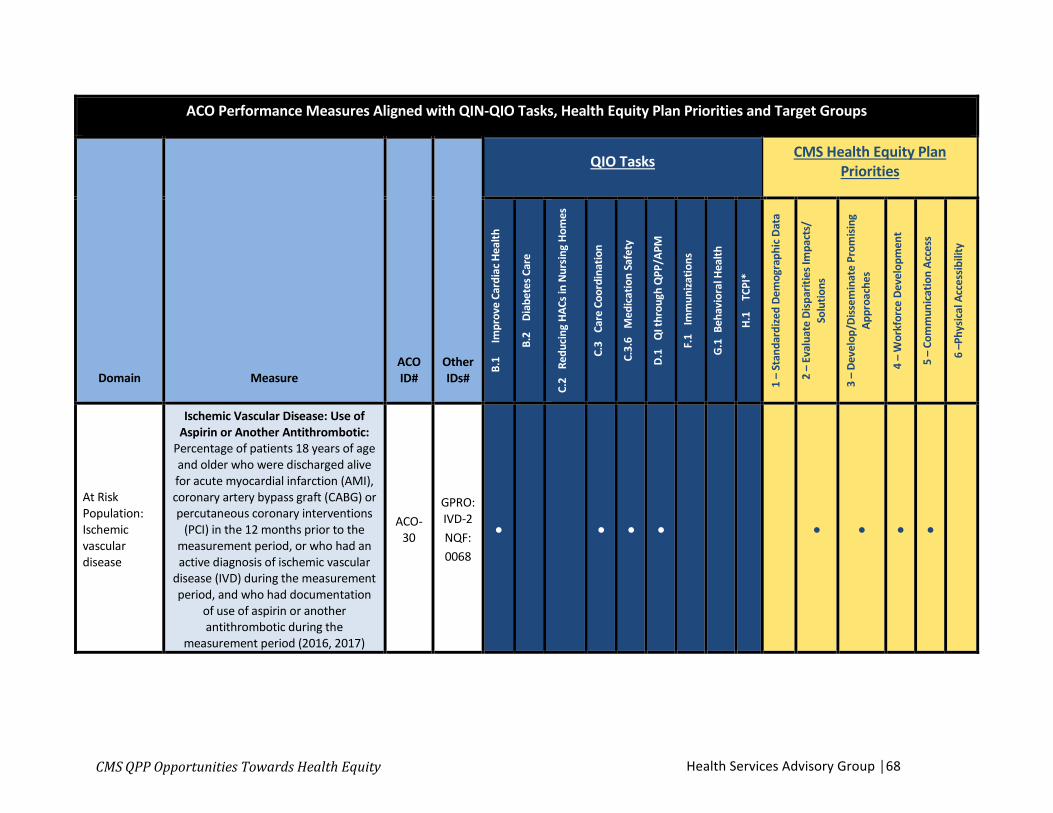
-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
At Risk Population: Ischemic vascular disease
Ischemic Vascular Disease: Use of Aspirin or Another Antithrombotic:
Percentage of patients 18 years of age and older who were discharged alive for acute myocardial infarction (AMI), coronary artery bypass graft (CABG) or percutaneous coronary interventions
(PCI) in the 12 months prior to the measurement period, or who had an active diagnosis of ischemic vascular
disease (IVD) during the measurement period, and who had documentation
of use of aspirin or another antithrombotic during the
measurement period (2016, 2017)
ACO-30
GPRO: IVD-2 NQF: 0068
● ● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │68

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
At Risk Population: Heart Failure
Heart Failure: Beta-Blocker Therapy for Left Ventricular Systolic
Dysfunction: Percentage of patients aged 18 years and older with a
diagnosis of heart failure (HF) with a current or prior left ventricular
ejection fraction (LVEF) < 40% who were prescribed beta-blocker therapy either within a 12 month period when
seen in the outpatient setting OR at each hospital discharge (2016)
ACO-31
GPRO: HF-6 NQF: 0083
● ● ● ● ● ● ●
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │69

-
–
-
- -
-
- -
–
ACO Performance Measures Aligned with QIN-QIO Tasks, Health Equity Plan Priorities and Target Groups
Domain Measure ACO ID#
Other IDs#
QIO Tasks CMS Health Equity Plan Priorities
B.1
Impr
ove
Card
iac H
ealth
B.2
Diab
etes
Car
e
C.2
Redu
cing
HAC
s in
Nur
sing
Hom
es
C.3
Care
Coo
rdin
atio
n
C.3.
6 M
edica
tion
Safe
ty
D.1
QI t
hrou
gh Q
PP/A
PM
F.1
Imm
uniza
tions
G.1
Beha
vior
al H
ealth
H.1
TCPI
*
1 –
Stan
dard
ized
Dem
ogra
phic
Dat
a
2 –
Eval
uate
Disp
ariti
es Im
pact
s/So
lutio
ns
3 –
Deve
lop/
Diss
emin
ate
Prom
ising
Appr
oach
es
4 –
Wor
kfor
ce D
evel
opm
ent
5 –
Com
mun
icat
ion
Acce
ss
6 –P
hysic
al A
cces
sibili
ty
At Risk Population: Coronary Artery Disease
Coronary Artery Disease: Angiotensin-Converting Enzyme Inhibitor or
Angiotensin Receptor Blocker Therapy – Diabetes or Left Ventricular SystolicDysfunction (LVEF<40%): Percentage of patients aged 18 years and olderwith a diagnosis of coronary artery
disease seen within a 12 month period who also have diabetes OR a current
or prior Left Ventricular Ejection Fraction (LVEF) < 40% who were prescribed ACE inhibitor or ARB
therapy (2016)
ACO-33
GPRO: CAD-7 NQF: 0066
● ● ● ● ● ● ● ● ●
*Please note, ACO measures marked as applicable to the TCPI are based on alignment with TCPI Common Measures for PracticeTransformation Networks (PTNs). Many of the other ACO measures not indicated are generally related to the overarching goals of TCPI. Additional information about TCPI measures can be found here.
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │70

CMS QPP Opportunities Towards Health Equity
Appendix F. Merit-Based Incentive Payment System (MIPS)
Clinicians who enroll in MIPS receive payment adjustments based on performance. MIPS rolls together and replaces three CMS reporting programs: the Physician Quality Reporting System (PQRS), Meaningful Use (MU), and the Value-Based Payment Modifier (VBPM) to produce component scores that add up to a single composite score. Payment adjustments are made based on the composite score.
There are four categories of MIPS Performance measures. The Cost category is determined through adjudicated claims information and does not require data submission from clinicians for the 2017 QPP Performance Year. The other three categories (i.e., Quality, Advancing Care Information, and Improvement Activities) include metrics that make up components of the composite score (Exhibit 3).50 Within those three categories, QIN-QIOs can: 1) help clinicians to select metrics that align with QIN-QIO tasks and health equity goals; and 2) support improved performance on those metrics.
1) Improvement Activitiesa. New reporting category, accounts for 15% of the composite scoreb. Focuses on achieving health equity, behavioral and mental health, beneficiary
engagement, care coordination, emergency response and preparedness,expanded practice access, patient safety and practice assessment andpopulation management
c. Most clinicians (with exceptions for small and rural practices) must choose atleast 4.
A crosswalk of MIPS Improvement Activities, QIN-QIO tasks, and OMH Health Equity Goals is shown in Appendix B.
2) Quality
Exhibit 3. 2017 MIPS Performance Categories and Composite Score
Percentages
50 Exhibit 4 citation: CMS QPP Program Performance.
Health Services Advisory Group │71

a. Replaces PQRS, and accounts for 60% of the composite scoreb. Most physicians (with exceptions for small and rural practices) must choose
6 measures.
A crosswalk of MIPS Quality Measures, QIN-QIO tasks, and OMH Health Equity Goals is shown in Appendix C.
3) Advancing Care Informationa. Replaces MU, accounts for 25% of the composite scoreb. Clinicians must report on at least 5 measures and can choose to submit up to
9 measures for extra credit.
A crosswalk of MIPS Advancing Care Information Measures, QIN-QIO tasks, and OMH Health Equity Goals is shown in Appendix D.
CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │72
CMS QPP Opportunities Towards Health Equity
Appendix G. Alternative Payment Models (APM) and Advanced APMs
An APM is a payment approach that gives added incentive payments to provide high-quality and cost-efficient care. APMs can apply to a specific clinical condition, a care episode, or a population. Clinicians who participate in a MIPS APM can report data under the MIPS system to avoid a penalty and earn a bonus. APM participation earns clinicians extra credit on their MIPS scores, counts towards improvement activity scores, reduces reporting requirements, and allows clinicians to be scored under a different, “APM” standard.51
Advanced APMs are a subset of APMs designated by CMS. Practices participating in advanced APMs must use certified Electronic Health Record (EHR) technology, and can earn more for taking on some risk related to their patients' outcomes. If costs go down and quality stays up, practices earn a bigger bonus compared to those reporting under MIPS and regular APMs. If costs go up or quality goes down, practices may lose money. Under Advanced APMs, practices take on more risk related to their patients’ outcomes, have greater flexibility in delivering services to keep patients healthier, and are rewarded financially for delivering high quality care and improving outcomes. Clinicians in Advanced APMs must report on quality metrics and meet requirements specific to each model. Within each model, program payment systems, requirements and metrics support and incentivize clinicians to assess and address needs for all patients.
Clinicians submitting data required by their Advanced APM can earn a 5% incentive payment in 2019 if they receive 25% of Medicare payments or see 20% of Medicare patients through an Advanced APM. Most Advanced APMs also qualify as MIPS APMs, meaning that clinicians who do not meet Advanced APM qualifying participant status can still report under MIPS and earn credit for their APM participation.
Clinicians interested in Advanced APM participation for the 2018 reporting period are encouraged to check regularly for updates at: https://qpp.cms.gov/learn/apms. There are currently 15 Advanced APMs:
Appendix H outlines comparisons between MIPS, APMs, and Advanced APMs.
Accountable Care Organizations (ACOs) are the largest type of alternate payment model in the Medicare program, covering more than 28 million lives across the nation. They are voluntarily formed groups comprised of clinicians and other healthcare entities focused on
51 Alternative Payment Models in the Quality Payment Program. https://qpp.cms.gov/docs/QPP_Advanced_APMs_in_2017.pdf
Health Services Advisory Group │73

CMS QPP Opportunities Towards Health Equity
the coordination of patient care, especially those patients with chronic health conditions. ACOs for the 2017 Performance Year include:
• The Medicare Shared Savings Programs (tracks 1, 2 and 3)• ACO Investment Model (AIM)• Next Generation ACO Model• Comprehensive ESRD Care (CEC) Model• Vermont all-Payer ACO
Most ACOs are one-sided risk models, which qualify as MIPS APMs. This includes all ACOs that are part of the Medicare Shared Savings Program (MSSP), Track 1. Others are two-sided risk models and qualify as Advanced APMs. These include the MSSP (Tracks 2 and 3), CEC, and Next Generation ACO Model.
ACOs are required to completely and accurately report quality data to calculate and assess their quality performance. For example, in 2016 and 2017 for the Shared Savings Program and the Next Generation ACO Model, metrics include National Quality Forum (NQF) Consumer Assessment of Healthcare Clinicians and Systems (CAHPS) measures (CAHPS® Survey for ACOs Participating in Medicare Initiatives) and data gathered from the Group Practice Reporting Option (GPRO) Web Interface reporting.
There is considerable overlap between the quality measures ACOs and other APMs must report on, QIN-QIO tasks, and CMS OMH Health Equity goals. A crosswalk of quality measures for Shared Savings Program and Next Generation ACOs, QIN-QIO tasks, and OMH Health Equity Goals is shown in Appendix E. This crosswalk may help QIN-QIOs to identify potential areas of collaboration and opportunities to further Health Equity goals. Since quality measures vary by model program and by year, the crosswalk table is offered for illustrative purposes, to show how QIN-QIOs can explore opportunities for collaboration with ACOs and other APMs in their area.
Health Services Advisory Group │74

CMS QPP Opportunities Towards Health Equity Health Services Advisory Group │75
Appendix H. Comparisons between MIPS, APMs, and Advanced APMs
Exhibit 4. Comparisons between MIPS, APMs, and Advanced APMs
Requirements not met
Minimum requirements
met Full requirements met Notes Clinician Reporting Status Ineligible for QPP No penalty N/A N/A
MIPS only
Penalty Clinician Medicare
part B rates gradually reduced
by 4 to 9% from 2019 to 2022
No penalty
Bonus Clinician Medicare part B base rates gradually rise by +4 to 9%from 2019 to 2022
Clinicians who fully meet requirements are paid more for the same services starting in 2019. 2019 bonuses and penalties are based on 2017 reporting; 2020 penalties are based on 2018 reporting; etc.
MIPS APM
Clinician is in a MIPS APM, but: The APM does not qualify as an advanced APM OR Clinician is in an advanced APM, but does not meet participation thresholds that would exempt clinician from MIPS reporting
Penalty Same as MIPS only No penalty Bonus
Same as MIPS only
Clinician reports under MIPS, but gets extra credit for APM participation, has fewer reporting requirements, and is scored differently.
APM participation counts towards improvement activity scores.
Advanced APM
Penalty Depends on the
APM's agreement with CMS:
CMS may withhold payments, reduce payment rates, or
APM may owe payments to CMS
N/A
Bonus Annual lump sum payment for 2019-2024 = 5% of the previous year's part B annual payments for covered services
After 2026, annual fees increase +0.75% annually instead of the standard +0.25%
Clinicians who qualify as advanced APM participants are exempt from MIPS reporting.

CMS QPP Opportunities Towards Health Equity
Appendix I. List of Acronyms
APM Alternative Payment Model
AI/AN American Indians and Alaska Natives
APM Alternative Payment Models
CDC Centers for Disease Control and Prevention
CAHPS Consumer Assessment of Healthcare Providers and Systems
CAH Critical Access Hospital
CEHRT Certified Electronic Health Record Technology
CMS Centers for Medicare & Medicaid Services
EHR Electronic Health Record
FQHC Federally Qualified Health Center
HHS Department of Health and Human Services
HPSA Health Professional Shortage Areas
IHS Indian Health Service
IHCDS Indian Health Care Delivery System
I/T/Us Indian Health Service, Tribally Operated and Urban Indian health clinics or centers
LEP Limited English Proficiency
MACRA Medicare Access and CHIP Reauthorization Act
MIPS Merit-Based Incentive Payment
NPI National Provider Identification
OMH Office of Minority Health
PCMH Patient Centered Medical Home model
QPP Quality Payment Program
RPMS Resource Patient Management System
RHC Rural Health Center
WHO World Health Organization
Health Services Advisory Group │76