cme current concepts in aesthetic upper...
TRANSCRIPT

CME
Current Concepts in Aesthetic UpperBlepharoplastyRod J. Rohrich, M.D., Dana M. Coberly, M.D., Steven Fagien, M.D., and James M. Stuzin, M.D.Dallas, Texas; and Boca Raton and Coconut Grove, Fla.
Learning Objectives: After studying this article, the participant should be able to: 1. Discuss nomenclature and anatomyassociated with upper blepharoplasty. 2. Perform preoperative assessment, decision-making, and counseling of patients.3. Describe current surgical planning, eyelid marking, and various techniques used in upper blepharoplasty, includinglasers. 4. Recognize and treat postoperative complications from blepharoplasty.
Traditional blepharoplasty has often involved the exci-sion of both lax skin and muscle and excessive removal of fat,leaving patients long term with a hollow orbit and a harsh,operated appearance that accelerates the aging process. Cur-rent methods of periorbital rejuvenation are more conser-vative, are based on concise preoperative evaluation, andinvolve the limited resection of the coveted soft tissue fromthe eye to restore a youthful appearance. The authors de-scribe anatomy, preoperative assessment, decision-makingand counseling of patients, surgical planning, eyelid mark-ing, and various techniques, including lasers, along withpostoperative complications associated with current con-cepts in aesthetic upper blepharoplasty. (Plast. Reconstr.Surg. 113: 32e, 2004.)
The eyes, or more precisely, periorbital tis-sues, are paramount in facial beauty, exhibit-ing youth and a plethora of expressions. Un-fortunately, this area is also one of the first toshow aging from the effects of gravity, ultravi-olet radiation, and animation. Traditionalblepharoplasty has involved the excision of laxskin and muscle and the removal of fat, some-times leaving patients long term with a holloworbit and harsh, operated appearance and of-ten accelerating the aging process. Currentmethods of periorbital rejuvenation are moreconservative in the resection of coveted softtissue from the eye. This is consistent withother areas of the face where precious softtissue is shaped, not necessarily removed. Theideal youthful appearance can be seen in mod-els and movie stars by studying the appearanceof their eyes. Beautiful young eyelids are full,
not hollow, with a crisp tarsal upper lid creaseand elastic support of the underlying soft tis-sue, creating a smooth, taut pretarsal and pre-septal upper eyelid (Fig. 1). The pretarsal eye-lid show is often only 2 to 3 mm in theaesthetically attractive eye. Periorbital skin issmooth with no rhytids or redundant folds.The eyebrows must always be addressed in theevaluation of the eyelid for proper restorationof a youthful and functional eye.
HISTORICAL PERSPECTIVE
Eyelid surgery was described in an Indiandocument, the Susruta, more than 2000 yearsago. Arabian surgeons cauterized excess eyelidskin to relieve drooping in the tenth and elev-enth centuries.1 Avicenna (980 to 1037) per-formed the first recorded blepharoplasty, ex-cising excess upper eyelid skin. Paré2 describedthe functional correction of excess eyelid skinin the sixteenth century. In the 1830s severalauthors discussed the resection of redundanteyelid skin.3–5 Sichel,6 in 1844, described her-niated intraorbital fat. Bourguet7 reported sep-arate fat compartments in the eyelids and histechnique for excising excess fat through atransconjunctival approach to prevent scar-ring. The modern blepharoplasty and detailedanatomy of the orbital fat compartments weredescribed by Costañares in 1951.8 Loeb9 andFurnas10 described removing redundant mus-cle in the late 1970s. These techniques focused
From the University of Texas Southwestern Medical Center. Received for publication May 24, 2002; revised November 13, 2002.
DOI: 10.1097/01.PRS.0000105684.06281.32
32e

on resection of redundant tissue, and only re-cently have authors gained an appreciation forthe conservative resection of periorbital fat.11–13
Deep or “hollow” upper eyelid sulci are com-mon results of the modern blepharoplasty, pre-sumably from overresection of soft tissue.14
This is especially true in patients with a prom-inent globe or negative upper periorbital vec-tor. Siegel15 believes that the height of the foldshould be determined by the balance of mo-tors—the levator versus the orbicularis. If thelevator is weak, a slightly lower fold should bechosen.
ANATOMICAL CONSIDERATIONS
The upper eyelid can be divided into tarsaland orbital portions at the level of the supra-tarsal fold. In Caucasians, it is located approx-imately 8 to 10 mm from the palpebral marginand results from a fusion of the levator apo-neurosis, orbital septum, and fascia of the or-bicularis oculi into the dermis. In the tarsalportion, these layers insert onto the anteriorsurface of tarsus. This area degenerates withage, which may lead to a high fold, with orwithout upper lid ptosis, and/or skin laxity ofthe lid. Loss of crease attachments may causethe skin to rest toward or beyond the uppereyelid/lash margin, with a tendency to inter-fere with upper outer visual fields.14
In the Asian eyelid, the orbital septum in-serts more inferiorly onto the distal expansionon the levator aponeurosis, which allows morepreaponeurotic fat to reside lower on the up-per eyelid. This results in a lower or absenteyelid crease.16 Siegel reported that the levatoraponeurosis in Caucasians joins a network offascia in the upper lid rather than the dermis.17
He believes the major difference between Cau-casian and Asian eyelids is the level at whichthe fascia fuses to create the fold. The layers offascia are infiltrated with fat in Asians.18 Thetwo main compartments of orbital fat arefound posterior to the orbital septum. They arethe nasal or medial (orbital) and temporal orlateral (preaponeurotic) compartments, whichare separated by the superior oblique muscle.The medial fat is usually pale yellow or white,and the lateral fat is yellow.
Histologically, the differences are in agreater amount of connective tissue and bloodvessels in the medial fat; the lateral fat has agreater amount of carotenoids.19 Preseptalretroorbicularis fat is located between the or-bital septum and the orbicularis. It is often asignificant factor in lateral lid hooding andpuffiness. Subcutaneous fat may be present be-tween the orbicularis and the skin immediatelybeneath the eyebrow and also contributes tofull upper eyelids.20,21
The motor nerve supply to the upper eyelidsis from the buccal, zygomatic, and frontalbranches of the facial nerve. Multiple inter-communications among facial nerve branchesresult in an extensive nerve supply to all pe-ripheral areas of the orbicularis.22 Studies inmonkeys showed that resection of preseptaland supraorbital orbicularis oculi muscle orpretarsal muscle only did not result in lagoph-thalmos, but resection of all three componentsdid.23 During sleep there is a persistent tone ofthe orbicularis to keep the eyes closed. If themotor nerves are blocked, the upper lid willopen.
CLINICAL EVALUATION
The surgical approach must take into con-sideration the repositioning of underlying softtissue and the redraping of skin. These tissueslose elasticity and support with aging, a condi-tion termed dermatochalasis in the skin.Blepharochalasis is a recurrent, intermittent,inflammatory condition of the eyelids resultingin edema, erythema, and thin excess eyelidskin secondary to histamine response and re-
FIG. 1. Periorbital volume depletion with aging. Adaptedfrom Fagien, S. Advanced rejuvenative upper blepharoplas-ty: Enhancing aesthetics of the upper periorbita. Plast. Re-constr. Surg. 110: 278, 2002.
Vol. 113, No. 3 / AESTHETIC UPPER BLEPHAROPLASTY 33e

lated to increased immunoglobulin E. In con-trast to dermatochalasis, blepharochalasis isdifficult to correct and likely to recur. In theolder population, a fold of excess upper eyelidskin can impair the function of the eye, specif-ically by obstruction of visual fields. A preoper-ative workup may include a consultation withan ophthalmologist for documentation of vi-sual field impairment to determine whetherthe obstruction is of visual significance (so thatits correction is medically necessary) to qualifypatients for potential insurance benefits.
Evaluation of the upper eyelid must includean evaluation of the eyebrow.24 Brow ptosisshould be corrected to achieve repositioning ofheavy eyebrow skin, which may be compen-sated by frontalis contraction to keep the eye-brows above the orbital rim. Aging causes theeyebrow fat to descend over the upper lid,giving it a full appearance. Once the visualobstruction has been removed by eyelid skinresection, the brows may look even heaviersince elevation is no longer needed for thevisual field. This results in a more aged appear-ance.25–27 If this tissue is resected rather thanresuspended, an overexposure of under-lying tissues may result, giving a hollowappearance.14,28
Medical and ophthalmologic histories mustbe obtained from the patient, including anyhistory of chronic illness, hypertension, diabe-tes, cardiac disease, bleeding disorders, thyroiddisturbances, or surgery. Medications, includ-ing aspirin and other anticoagulants, are listedand withheld for at least 2 weeks preopera-tively. Patients must be specifically questionedconcerning dietary supplements that may alsoaffect clotting29 as well as concerning their vi-sion, corrective lenses, previous surgery ortrauma, glaucoma, allergic reactions, excesstearing, and dry eyes.30 A Schirmer test shouldbe conducted if the patient has dry eyes oroccasional symptoms, and referral to an oph-thalmologist is recommended.31–33
PREOPERATIVE MARKINGS
Preoperative markings are critical to assessand are made with the patient sitting uprightand in neutral gaze. The brow needs to beelevated to the proper position before anymarks are made. The supratarsal fold is locatedat approximately 8 to 9 mm above the ciliarymargin in women and at 7 to 8 mm in men. Amark should be made just inferior to this fold(Fig. 2). The upper marking must be at least 10
mm from the lower edge of the brow and notinclude any thick brow skin. The use of a pinchtest for redraping the skin is helpful.14 Theshape of the skin resection is lenticular inyounger patients and more trapezoid-shapedlaterally in older patients (Fig. 3). The index ofsafety is much higher laterally (one can removemore skin) and becomes more critical as theincision proceeds medially (Figs. 4 and 5). Theincision may need to be extended laterally witha larger excision, but extension lateral to theorbital rim should be avoided if possible toprevent a prominent scar, especially in malepatients and patients with thick skin. Similarly,the medial markings should not be extendedmedial to the medial canthus for larger resec-tions because extensions onto the nasal side-wall result in webbing. If excessive skin ispresent medially, a W-plasty may need to beperformed. The amount of fat to be resectedshould be determined preoperatively, with thepatient in up-gaze, down-gaze, and medial andlateral ranges of motion, with photographicdocumentation.
SURGICAL TECHNIQUE
Subcutaneous injection with 3 cc of 1% lido-caine with 1:100,000 epinephrine using a 27-gauge, 11⁄2-inch needle 7 minutes before oper-ative scrub preparation will allow time formaximum vasoconstriction. Hyaluronidase hasbeen added to the local anesthetic for morerapid and even spreading of local anesthesia,but diplopia and pupillary dilatation can occursecondary to posterior spread of lidocaine.28
The local anesthetic should be injected super-ficially to avoid any subcutaneous or intraor-bicularis hematoma formation. Incisions aremade superficially with a fresh no. 15 bladethrough the epidermis only, and the pre-
FIG. 2. The planned surgical incision is located 2 to 3 mmbelow the apparent supratarsal fold. Adapted from Fagien,S. Advanced rejuvenative upper blepharoplasty: Enhancingaesthetics of the upper periorbita. Plast. Reconstr. Surg. 110:278, 2002.
34e PLASTIC AND RECONSTRUCTIVE SURGERY, March 2004

marked strip of skin is resected with finecurved scissors (Fig. 6). If redundant orbicu-laris muscle is present, this resection can in-clude the predetermined amount of orbicu-laris muscle to be resected. This can also beused to define the supratarsal fold. Hemostasisis obtained using pinpoint insulated cautery(Colorado microdissection needle, Stryker-Leibinger, Inc., Kalamazoo, Mich.). A smallincision is made into each fat compartment ofthe eyelid in which resection of redundant fathas been planned. The fat is teased out andresected using pinpoint cautery (Fig. 7). Thisfat usually includes the medial or nasal com-partment, which contains white fat (Fig. 8).Yellow fat can also be found in this area but itis usually more superficial and lateral to the
white fat; this fat is usually preserved to avoidvolume depletion of the upper periorbita thatcan manifest as notches or depressions in thisregion (Fig. 9).
Once fat resection is completed, a lower lidlateral canthopexy may be performed throughthe upper blepharoplasty incision (Figs. 10 and11). An incision is made laterally to expose thelateral orbital rim. A 5-0 Vicryl suture is placedthrough the anterior lamella of the lateral can-thus and secured to periosteum on the insideof the lateral orbital rim at the level of theupper limbus. It is important to place this su-ture inside the rim and posteriorly to avoidtenting the lower lid over the eye. This lift willbe subtle and will resolve over time while pre-venting ectropion in the postoperative course.Once hemostasis is obtained, any final adjust-ments concerning shape are made, especiallylaterally, to maximize the appearance of bilat-eral eyelid symmetry. The incision is closed
FIG. 4. Surgical markings in a lenticular shape. Adaptedfrom Fagien, S. Advanced rejuvenative upper blepharoplas-ty: Enhancing aesthetics of the upper periorbita. Plast. Re-constr. Surg. 110: 278, 2002.
FIG. 5. Preoperative markings.
FIG. 3. Upper eyelid skin resection increases in size bothvertically and laterally as the periorbital area ages: young(above), middle age (center), and old (below). Adapted fromFagien, S. Advanced rejuvenative upper blepharoplasty: En-hancing aesthetics of the upper periorbita. Plast. Reconstr.Surg. 110: 278, 2002.
Vol. 113, No. 3 / AESTHETIC UPPER BLEPHAROPLASTY 35e

using a running subcutaneous 6-0 Prolene su-ture followed by interrupted simple 6-0 nylonsutures. At the conclusion of the case, the pa-tient should have approximately 2 to 3 mm oflagophthalmos bilaterally (Fig. 12). Suturesshould be placed 1 mm into skin over an intactorbicularis, allowing the muscle to fold on it-self in a pleated fashion with skin closure (Fig.13).14
LASER BLEPHAROPLASTY
Laser blepharoplasty was first described in1984 by Baker et al.34 Incisions may be madewith a scalpel or with a laser. The 1997 Amer-ican Society for Aesthetic Plastic Surgery/American Society of Plastic and Reconstructive
FIG. 8. White fat resection, medial compartment (only ifindicated). Necessity is determined preoperatively by a phys-ical examination.
FIG. 9. Amount of fat to be resected is determinedpreoperatively.
FIG. 10. Intraoperative view of a lower lid canthopexy per-formed through the upper lid incision. Adapted from Fagien,S. Advanced rejuvenative upper blepharoplasty: Enhancingaesthetics of the upper periorbita. Plast. Reconstr. Surg. 110:278, 2002.
FIG. 6. Skin resection. (Above) During resection. (Below)Resection completed.
FIG. 7. Yellow fat resection, medial compartment (only ifindicated). Necessity is determined preoperatively by a phys-ical examination.
36e PLASTIC AND RECONSTRUCTIVE SURGERY, March 2004

Surgeons Laser Task Force Survey found that84 percent of respondents performed laserblepharoplasty. A median time of 3 hours ofhands-on training with the technique was re-ceived before it was incorporated into theirpractice. Disadvantages of the laser techniqueinclude the potential for poor wound healing,loss of tactile (sensation) feedback, time spentlearning, and expense. Possible advantages in-clude decreased bleeding, less time spent ob-taining hemostasis, and less tissue damage
when compared with electrocautery, resultingin better scars and decreased postoperativeedema and ecchymosis.12 Safety issues includeeye protection for the patient with stainlesssteel eye shields and for the operative teamwith protective goggles.35 In our experience,laser use does not have a significant advantageand is used infrequently.
Before the initial incision is made, it must bedecided whether laser resurfacing is to be per-formed. This results in at least 4 to 6 mm ofupper lid shortening, so skin resection must beadjusted accordingly. Cutting of the skinshould be performed in the ultrapulse mode.Dissection is then performed in the continuousmode for more coagulation. Conservative fatresection may also be performed using the la-ser. Once the incision is closed, the carbondioxide laser, alone or in combination with theerbium:yttrium-aluminum-garnet laser, may beused for resurfacing.36 Eye shields are placed toprotect the eyes, and eyelids need to be re-flected with a wet cotton-tipped applicator.The skin is covered postoperatively with a semi-permeable dressing to maintain moisture andminimize pain.37 Seckel et al.38 use the carbondioxide laser directly on the orbicularis muscleto cause visible shrinking of the muscle andseptum.
MALE BLEPHAROPLASTY
In the United States, 16 percent of blepha-roplasties are performed on men, and blepha-roplasty is the second most common cosmeticsurgery performed on male patients.39 Men
FIG. 13. Sutures should be placed 1 mm into skin over anintact orbicularis, allowing the muscle to fold on itself (left)in a pleated fashion with skin closure (right). Adapted fromFagien, S. Advanced rejuvenative upper blepharoplasty: En-hancing aesthetics of the upper periorbita. Plast. Reconstr.Surg. 110: 278, 2002.
FIG. 11. Illustration demonstrating suture placement.Adapted from Fagien, S. Advanced rejuvenative upperblepharoplasty: Enhancing aesthetics of the upper periorbita.Plast. Reconstr. Surg. 110: 278, 2002.
FIG. 12. Closure of incisions: (above) a 6-0 Prolene run-ning subcuticular suture; (below) 6-0 nylon interrupted simplesutures. Approximately 2 mm of lagophthalmos is noted atthe completion of the procedure.
Vol. 113, No. 3 / AESTHETIC UPPER BLEPHAROPLASTY 37e

tend to seek out blepharoplasty more for func-tional reasons than women, but this differencehas become less and less distinct in recentyears. A more natural look is preferred, andthe “operated look” will not be tolerated wellby most male patients. Men will typically not bewearing cosmetics, so all scars must be carefullyconcealed. This also makes male patients sub-optimal candidates for laser resurfacing. Thelateral incision should only infrequently be ex-tended beyond the later orbital rim. In menwith heavy brows, resection of upper eyelidskin only will result in profoundly ptotic brows.Therefore, one should counsel combined browsurgery with upper blepharoplasty. Many menare reluctant to have cosmetic surgery to cor-rect brow ptosis, so careful preoperative coun-seling is needed to prevent a dissatisfied pa-tient with worse brow ptosis postoperatively.40
Often, conservative eyelid resection is all that isrequired.
POSTOPERATIVE MANAGEMENT
Postoperative care should include a chilledlight gel compress (Swiss Eye Therapy, InvotecInternational, Jacksonville, Fla.) for 48 hours,saline eye drops (Refresh Plus, Allergan Inc.,Irvine, Calif.) while the patient is awake, andlubricating ointment (Refresh P.M., Allergan)for night use. Tobramycin ophthalmic dropsmay be used prophylactically in the early post-operative period, typically three times per dayfor 3 to 5 days. The patient’s head shouldremain elevated to reduce edema and ophthal-mic pressure. The patient is seen in the recov-ery room to evaluate and document vision be-fore discharge and followed up 4 to 5 dayspostoperatively, when all sutures are removed.Lagophthalmos is usually secondary to perior-bital edema and resolves in 1 to 2 weeks. Pre-operative and postoperative patient educationon the use of eye drops and ointment, espe-cially at night, is essential to prevent cornealabrasions and exposure problems.
COMPLICATIONS
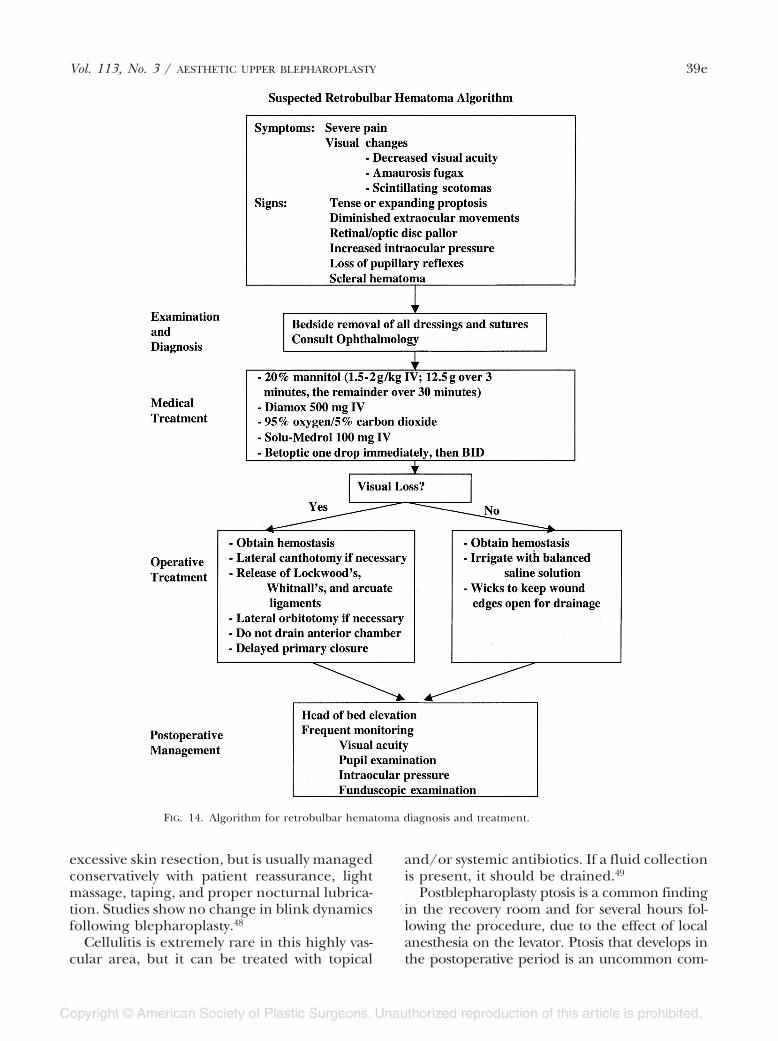
Vision loss due to retrobulbar hematoma isthe most feared complication resulting fromblepharoplasty; fortunately, the occurrence israre. The incidence is reportedly 0.04 percent,or one in 2500 cases.41,42 Acute retrobulbarhematoma may compress neurovascular struc-tures, leading to ischemia of the retina, centralartery, and optic nerve. Symptoms include se-vere pain, visual changes, including hemianop-
sia or amaurosis fugax (like a “window shade”over the lower half of the visual field), andscintillating scotomas (sparkles and flashes)(Fig. 14). Examination will often reveal a tenseand protuberant periorbital area with dimin-ished or absent extraocular movements. Oncethe diagnosis is made, treatment should beimplemented immediately because 90 to 120minutes of ischemia leads to irreversible blind-ness. Wolfort et al.43 reviewed the diagnosis andtreatment of retrobulbar hematoma. All dress-ings should be removed and sutures need to bereleased. An ophthalmologic consultationshould be obtained immediately. The patientshould be given mannitol 20% 1.5 to 2 g/kgintravenously (with the first 12.5 g over a3-minute period and the remainder over a 30-minute period), 500 mg of Diamox (acetazol-amide; Lederle Pharmaceutical Division,American Cyanamid Company, Pearl River,N.Y.) intravenously, 95 percent oxygen/5 per-cent carbon dioxide to dilate intraocular ves-sels, Solu-Medrol (Pharmacia & Upjohn, NewYork, N.Y.) 100 mg intravenously, and Betoptic(Allen USA, Fort Worth, Texas), one drop im-mediately, then twice daily. These actionsshould be taken as the patient is being takenback to the operating room for reexplorationand evacuation of hematoma, as well as possi-ble lateral canthotomy and release of the arcusmarginalis.
Vision loss can also result from globe perfo-ration44 during infiltration with local anes-thetic. This is extremely rare and, along withcorneal abrasion, can be prevented with cor-neal protectors.
Superficial hematomas usually result fromorbicularis muscle vessel bleeding and do notthreaten vision. When small, they can usuallybe allowed to resolve spontaneously. If larger,they can be evacuated after liquefaction occurs7 to 10 days later.45 Careful control of bloodpressure, use of ice, and elevation of the headhelp to prevent hematoma and ecchymosis.
Diplopia may result from impaired ocularmotility, more commonly in lower blepharo-plasty from involvement of the inferior obliquebut also from upper lid surgery from the verti-cal recti and superior oblique. The etiology ispostulated to be from edema or stretch result-ing in perimuscular hemorrhage. Conservativemanagement is recommended since the diplo-pia will often resolve as the edema and inflam-mation subside.46,47
Lagophthalmos may result from edema or
38e PLASTIC AND RECONSTRUCTIVE SURGERY, March 2004
excessive skin resection, but is usually managedconservatively with patient reassurance, lightmassage, taping, and proper nocturnal lubrica-tion. Studies show no change in blink dynamicsfollowing blepharoplasty.48
Cellulitis is extremely rare in this highly vas-cular area, but it can be treated with topical
and/or systemic antibiotics. If a fluid collectionis present, it should be drained.49
Postblepharoplasty ptosis is a common findingin the recovery room and for several hours fol-lowing the procedure, due to the effect of localanesthesia on the levator. Ptosis that develops inthe postoperative period is an uncommon com-
FIG. 14. Algorithm for retrobulbar hematoma diagnosis and treatment.
Vol. 113, No. 3 / AESTHETIC UPPER BLEPHAROPLASTY 39e

plication of blepharoplasty that should be evalu-ated thoroughly to determine the cause. Lidasymmetry that persists after surgery or developspostoperatively should be evaluated to determinethe degree of ptosis and the amount of levatorfunction. Ptosis can be secondary to edema, op-erative technique, or injury to the levator com-plex. Severe ptosis with poor levator functionrequires reexploration with levator repair. Mildcases may resolve spontaneously and can be man-aged expectantly.50
CONCLUSIONS
Blepharoplasty is a highly successful aes-thetic surgical procedure that requires care-ful preoperative planning and examinationof the patient’s concerns and desires (Figs.15, 16, and 17). Standard resections of fat
and muscle have been replaced with conser-vative and careful resections of only redun-dant soft tissue. Ptotic soft tissues are relo-cated rather than resected. The eyelid mustalways be considered in conjunction with theeyebrow, and correction of periorbital agingmay require brow repositioning as well. Care-ful perioperative technique, meticulous he-mostasis, and attentive postoperative man-agement of blood pressure will prevent mostcomplications.
Rod J. Rohrich, M.D.Department of Plastic SurgeryUniversity of Texas Southwestern Medical Center5323 Harry Hines Boulevard, Suite E7.210Dallas, Texas [email protected]
FIG. 17. Selective skin resection only, with orbicularis preservation and central fat pad removal. Levator advancement andlowering of the supratarsal fold for correction of levator dehiscence. (Left) Preoperative and (right) 13-month postoperative views.
FIG. 15. Upper blepharoplasty using selective skin resection only with orbicularis preservation. No fat removalwas performed. Lower blepharoplasty was also performed. (Left) Preoperative and (right) 2-year postoperative views.
FIG. 16. Upper blepharoplasty using selective skin resection, orbicularis preservation, and central fad pad removal. Endo-scopic brow lift, laser resurfacing, and lower blepharoplasty were also performed, with no lower lid skin resection. (Left)Preoperative and (right) 15-month postoperative views.
40e PLASTIC AND RECONSTRUCTIVE SURGERY, March 2004

ACKNOWLEDGMENT
We sincerely thank Vikram Gavande, M.S., University ofTexas Southwestern Medical School, Dallas, Texas, for hisassistance with the manuscript.
REFERENCES
1. Dupuis, C., and Rees, T. D. Historical notes on bleph-aroplasty. Plast. Reconstr. Surg. 47: 246, 1971.
2. Paré, A. (translated by T. Johnson). The Works of ThatFamous Chirurgeon Ambroise Parey [Ambroise Paré]. Lon-don: Mary Clark, 1678.
3. Mackenzie, W. A Practical Treatise on the Diseases of the Eye.London: Longman, 1835.
4. Alibert, J. L. Monographie des Dermatoses ou Precis Theo-rique et Pratique des Maladies de la Peau. Paris: Paynac,1832.
5. Graf, D. Oertliche erbliche Erschlaffung der Lidhaut.Wochenschrift fur die gesammte Heilkunde, 1836. P. 225.
6. Sichel, A. Aphorismes pratiques sur divers pointsd’ophtalmologie. Ann. Ocul. 12: 185, 1844.
7. Bourguet, J. Notre traitement chirurgical de “poches”sous les yeux sans cicatrice. Arch. Fr. Belg. Chir. 31: 133,1928.
8. Costañares, S. Blepharoplasty for herniated intra-or-bital fat: Anatomical basis for a new approach. Plast.Reconstr. Surg. 8: 46, 1951.
9. Loeb, R. Necessity for partial resection of the orbicu-laris oculi muscle in blepharoplasties in some youngpatients. Plast. Reconstr. Surg. 60: 176, 1977.
10. Furnas, D. W. Festoons of orbicularis muscle as a causeof baggy eyelids. Plast. Reconstr. Surg. 61: 540, 1978.
11. Hudson, D. A. A paradigm shift for plastic surgeons: Nolonger focusing on excising skin excess. Plast. Reconstr.Surg. 106: 497, 2000.
12. Fagien, S. Algorithm for canthoplasty: The lateral reti-nacular suspension: A simplified suture canthopexy.Plast. Reconstr. Surg. 103: 2042, 1999.
13. Lessner, A. M., and Fagien, S. Laser blepharoplasty.Semin. Ophthalmol. 13: 90, 1998.
14. Fagien, S. Advanced rejuvenative upper blepharoplas-ty: Enhancing aesthetics of the upper periorbita. Plast.Reconstr. Surg. 110: 278, 2002.
15. Siegel, R. J. Advanced upper lid blepharoplasty. Clin.Plast. Surg. 19: 319, 1992.
16. Doxanas, M. T., and Anderson, R. L. Oriental eyelids:An anatomic study. Arch. Ophthalmol. 102: 1232, 1984.
17. Siegel, R. J. Essential anatomy for contemporary upperlid blepharoplasty. Clin. Plast. Surg. 20: 209, 1993.
18. Siegel, R. J. Oriental blepharoplasty. In L. M. Vistnes(Ed.) Procedures in Plastic and Reconstructive Surgery:How They Do It. Boston: Little, Brown, 1991. Pp. 83–92.
19. Sires, B. S., Saari, J. C., Garwin, G. G., Hurst, J. S., and vanKuijk, F. J. The color difference in orbital fat. Arch.Ophthalmol. 119: 868, 2001.
20. Owsley, J. Q. Resection of the prominent lateral fat padduring upper lid blepharoplasty. Plast. Reconstr. Surg.66: 165, 1980.
21. May, J. W., Jr., Fearon, J., and Zingarelli, P. Retro-or-bicularis oculi fat (ROOF) resection in aestheticblepharoplasty: A 6-year study in 63 patients. Plast.Reconstr. Surg. 86: 682, 1990.
22. Knize, D. M. Muscles that act on glabellar skin: A closerlook. Plast. Reconstr. Surg. 105: 350, 2000.
23. Craig, D. M., and Sullivan, P. K. The resection of or-bicularis oculi muscle from the upper eyelid in ex-
perimental surgery on the monkey. Plast. Reconstr.Surg. 87: 32, 1991.
24. Gunter, J. P., and Antrobus, S. D. Aesthetic analysis ofthe eyebrows. Plast. Reconstr. Surg. 99: 1808, 1997.
25. Flowers, R. S., and Flowers, S. S. Precision planning inblepharoplasty: The importance of preoperative map-ping. Clin. Plast. Surg. 20: 303, 1993.
26. Flowers, R. S., Caputy, G. G., and Flowers, S. S. Thebiomechanics of brow and frontalis function and itseffect on blepharoplasty. Clin. Plast. Surg. 20: 255,1993.
27. Fagien, S. Eyebrow analysis after blepharoplasty in pa-tients with brow ptosis. Ophthal. Plast. Reconstr. Surg. 8:210, 1992.
28. Baylis, H. I., Goldberg, R. A., Kerivan, K. M., and Jacobs,J. L. Blepharoplasty and periorbital surgery. Derma-tol. Clin. 15: 635, 1997.
29. Ang-Lee, M. K., Moss, J., and Yuan, C. S. Herbal med-icines and perioperative care. J.A.M.A. 286: 208,2001.
30. Jelks, G. W., and Jelks, E. B. Preoperative evaluation ofthe blepharoplasty patient: Bypassing the pitfalls. Clin.Plast. Surg. 20: 213, 1993.
31. Rees, T. D., and Jelks, G. W. Blepharoplasty and the dryeye syndrome: Guidelines for surgery? Plast. Reconstr.Surg. 68: 249, 1981.
32. McKinney, P., and Byun, M. The value of tear filmbreakup and Schirmer’s tests in preoperative bleph-aroplasty evaluation. Plast. Reconstr. Surg. 104: 566,1999.
33. Fagien, S. The value of tear film breakup and Schirm-er’s test in preoperative blepharoplasty evaluation(Discussion). Plast. Reconstr. Surg. 104: 570, 1999.
34. Baker, S. S., Muenzler, W. S., Small, R. G., and Leonard,J. E. Carbon dioxide laser blepharoplasty. Ophthal-mology 91: 238, 1984.
35. Mele, J. A., III, Kulick, M. I., and Lee, D. Laser bleph-aroplasty: Is it safe? Aesthetic Plast. Surg. 22: 9, 1998.
36. Millman, A. L., and Mannor, G. E. Histologic and clin-ical evaluation of combined eyelid erbium: YAG andCO2 laser resurfacing. Am. J. Ophthalmol. 127: 614,1999.
37. Roberts, T. L., III. Laser blepharoplasty and laser re-surfacing of the periorbital area. Clin. Plast. Surg. 25:95, 1998.
38. Seckel, B. R., Kovanda, C. J., Cetrulo, C. L., Jr., Passmore,A. K., Meneses, P. G., and White, T. Laser blepha-roplasty with transconjunctival orbicularis muscle/septum tightening and periocular skin resurfacing: Asafe and advantageous technique. Plast. Reconstr. Surg.106: 1127, 2000.
39. American Society of Plastic Surgeons. 2000 Gender dis-tribution: Cosmetic surgery. Arlington Heights: Amer-ican Society of Plastic Surgeons, 2000. Availableat http://www.plasticsurgery.org/public–education/loader.cfm?url�/commonspot/security/getfile.cfm&Page ID�1939. Accessed December 29, 2003.
40. Flowers, R. S. Periorbital aesthetic surgery for men: Eye-lids and related structures. Clin. Plast. Surg. 18: 689,1991.
41. Callahan, M. A. Prevention of blindness after blepha-roplasty. Ophthalmology 90: 1047, 1983.
42. DeMere, M., Wood, T., and Austin, W. Eye compli-cations with blepharoplasty or other eyelid surgery:A national survey. Plast. Reconstr. Surg. 53: 634, 1974.
43. Wolfort, F. G., Vaughan, T. E., Wolfort, S. F., and Nevarre,
Vol. 113, No. 3 / AESTHETIC UPPER BLEPHAROPLASTY 41e

D. R. Retrobulbar hematoma and blepharoplasty.Plast. Reconstr. Surg. 104: 2154, 1999.
44. Schechter, R. J. Management of inadvertent intraocularinjections. Ann. Ophthalmol. 17: 771, 1985.
45. Lyon, D. B., and Raphtis, C. S. Management of com-plications of blepharoplasty. Int. Ophthalmol. Clin. 37:205, 1997.
46. Harley, R. D., Nelson, L. B., Flanagan, J. C., and Calhoun,J. H. Ocular motility disturbances following cos-metic blepharoplasty. Arch. Ophthalmol. 104: 542, 1986.
47. Lisman, R. D., Hyde, K., and Smith, B. Complications ofblepharoplasty. Clin. Plast. Surg. 15: 309, 1988.
48. Abell, K. M., Cowen, D. E., Baker, R. S., and Poter, J. D.Eyelid kinematics following blepharoplasty. Ophthal.Plast. Reconstr. Surg. 15: 236, 1999.
49. Rees, T. D., Craig, S. M., and Fisher, Y. Orbital abscessfollowing blepharoplasty. Plast. Reconstr. Surg. 73: 126,1984.
50. Wolfort, F. G., and Poblete, J. V. Ptosis after blepharo-plasty. Ann. Plast. Surg. 34: 264, 1995.
42e PLASTIC AND RECONSTRUCTIVE SURGERY, March 2004