clinical sequence assessments and semg feedback€¦ · · 2016-10-06clinical sequence...
TRANSCRIPT
A Beginner’s Guide by
Todd Shewman Peter Konrad Version 1.0 January 2011
CLINICAL SEQUENCE ASSESSMENTS And SEMG FEEDBACK
Surface Electromyography (SEMG)
ISBN 0-9771622-4-9
I
Clinical Sequence Assessments and SEMG Feedback
Printed by Noraxon U.S.A, Inc.
ISBN 0-9771622-4-9 Copyright © 2011 by Noraxon U.S.A., Inc. Reproduction without written permission is granted to educational institutions for educational purposes only. Noraxon is a registered trademark of Noraxon U.S.A., Inc. All rights reserved. All other company and product names contained herein may be trademarks or registered trademarks of their respective companies and are sole property of their respected owners. The authors have made every effort to ensure the accuracy of the information contained within the book. However, appropriate information sources should be consulted, especially for new or unfamiliar procedures. It is the responsibility of each individual to evaluate the appropriateness of a particular finding in the context of actual clinical situations and with due considerations to new developments. The authors, editors and publisher cannot be held responsible for any typographical or other errors found in this book. Further, the authors and publisher are not responsible (as a matter of product liability, negligence, or otherwise) for any injury resulting from any material contained herein. Noraxon U.S.A. Inc. 13430 N. Scottsdale Road, Suite 104 Scottsdale, Arizona 85254 Tel: (480) 443-3413 Fax: (480) 443-4327 E-mail: [email protected] Support E-mail: [email protected] Web Site: www.noraxon.com
New address effective on February 14, 2011 Noraxon U.S.A. Inc. 15770 North Greenway-Hayden Loop, Suite 100 Scottsdale, AZ 85260 Tel: (480) 443-3413 Fax: (480) 443-4327 E-mail: [email protected] Support E-mail: [email protected] Web Site: www.noraxon.com
II
Clinical Sequence Assessments and SEMG Feedback
Table of Contents: Preface ……………………………………………………………… III Rationale - SEMG Advantages and Limitations ……………................. 1 Clinical Integration of SEMG …………………………………………... 2 Assessment Parameters of Patients Using SEMG ……………………… 4 Kinesiologic SEMG Sequence Assessments ……………………………. 5 Interpretation of Clinical SEMG Data - General Principles ………….. 6 Phases of Proposed Sequences Assessments and Observations………... 9 Clinical Procedures ……………………………………….…………..... 11 Baseline/Postural Evaluation – Sitting or Standing…………… 11 Phase 2 Active Range of Motion/Dynamic Phase……………. 11 Qualitative Analysis ......………………………………………………….. 13 Clinical Procedure – Dynamic Phases – Step by Step Instructions……. 14 Advanced Considerations for Active Range of Motion Phases………… 15 Regional Applications of Sequence Assessments Using Surface Electromyography ………………………………………………… ………………………….. 19 Temporomandibular Region…………………………………. 21 Cervical Region………………………………………………. 33
Shoulder Girdle Region………………………………………. 44 Low Back and Trunk Region………………………………… 56 Hip Region………………………………… ………………… 70 Knee Region………………………………………………….. 80
Basic SEMG Feedback Applications……………………………………. 92 SEMG Feedback Technique 1 : Isolation of Muscle Activity . 93 SEMG Feedback Technique 2 Threshold-based
Down-training ……………………………………………….. 94 SEMG Feedback Technique 3: Activation Recognition Training ……………………………………………………... 95 SEMG Feedback Technique 4: Activation Discrimination Training ……………………………………………………. 96 SEMG Feedback Technique 5: Threshold based Uptraining 97 SEMG Feedback Technique 6: Coordination Training ….,.. 98
III
Clinical Sequence Assessments and SEMG Feedback
Preface Privileged to work with a number of distinguished clinicians and educators worldwide, the authors acknowledge the healthcare challenges from many perspectives. The challenges faced by many facets of rehabilitation are often daunting. The authors are convinced that surface electromyography (SEMG) can add valuable information to the evaluation and treatment process when treating patients with musculoskeletal dysfunction. Analysis with SEMG can help clinicians in identifying relationships between muscle impairments and other physical and psychologic impairments. SEMG techniques offer distinct conveniences compared with other means of muscle monitoring. The SEMG clinical techniques outlined in this booklet are designed at a rudimentary level to educate the novice clinician on how to record neuromuscular activity from the skin surface, quantify and document the results, and to present ideas on the use of SEMG as a feedback tool. When used as a tool for patient treatment, SEMG imparts real-time, refined, valuable information regarding the physiologic status of the neuromuscular system and, outcome of treatment or therapeutic intervention. When SEMG is combined with clinical data and a variety of therapies, impairment may be reduced and function enhanced. Clinicians and patients benefit from the information SEMG offers. The authors have attempted to provide a breakdown of easy to use clinical techniques for the various anatomical regions. Previous to this booklet, important clinical publications titled “Introduction to Surface Electromyography” and “Clinical Applications in Surface Electromyography” were written for broader audiences and are highly recommended by the authors. This booklet was written to bring a concentrated focus of fundamental Kinesiologic SEMG for the novice user. Covered are the very basic components of SEMG pertaining to the temporomandibular, cervical, shoulder, low back, hip and knee regions. The reader will notice that the majority of the text is written from a kinesiologic perspective and psychologic portions are modest. This is not to promote one discipline, or approach over another, but rather the clinical SEMG procedures included are designed as novice educational material for movement based assessments. The booklet provides a brief overview of rationale as well as advantages and limitation of SEMG. We then provide the reader an overview of basic principles of assessment and analysis/documentation criteria. Finally, the booklet continues by presenting step by step instructions on how to perform a basic SEMG assessment for each anatomical region. Basic analysis items for each, a “checklist” of SEMG signal interpretation possibilities, and a chart outlining common muscle imbalance impairments with possible SEMG signal expectations. The final portion is a brief summary dedicated toward SEMG feedback techniques that may be used in conjunction with therapeutic exercise or as ergonomic and/or proprioceptive techniques. It is important for the reader to understand that the assessment procedures provide specific, yet flexible protocols that may generate clinically pertinent information showing various dysfunctions, however, they are not “rigid” and should be thought of only as a potential starting point. It is the authors’ bias that clinicians must choose from among the techniques and options to
IV
Clinical Sequence Assessments and SEMG Feedback
determine which protocol, or portion of the protocols will work best with the case at hand and encourage the reader to think well outside of contents presented. It is the authors’ hope and goal that readers will expand well beyond the techniques presented in the booklet. We would also like to take the opportunity to thank the countless people who provided input and support throughout the project. This includes clinicians and individuals worldwide that have implemented the techniques and for sponsors to allow us to test the techniques in educational settings. Without them, this booklet would simply not be possible. We hope that in some way the information provided will be of assistance to those who embrace the technology. D. Todd Shewman Dr. Peter Konrad
1
Clinical Sequence Assessments and SEMG Feedback
Surface Electromyography Clinical Sequence Assessments and SEMG Feedback
A Beginner’s Guide Rationale Clinicians are often required to assess muscle function associated with impairments and disabilities in patients. Muscles function both passively and actively to help guide and limit motion of the skeletal system so that functional, goal directed activities can be accomplished with daily tasks, athletic events, etc. Agonist, antagonist and, synergist muscles function together to control arthrokinematics and produce a desired osteokinematic effect. Governed by the central nervous system, muscles must produce a biomechanically efficient pattern of motion along the involved kinematic chain or dysfunction and pain will likely result. Muscle control may be influenced by a number of factors including nociception, segmental and suprasegmental motor reflexes, perception, metabolic and nutritional issues and a host of factors related to articular function and periarticular connective tissues. Repeated dysfunctional cycles may exacerbate aberrant movement proximal and distal to the origin of the problem resulting in a dysfunctional spiral, until intervention becomes mandatory. Analysis with Surface Electromyography (SEMG) can help clinicians to identify relationships between muscle impairments and other physical impairments. Classification of impairments with observed functional limitations and disabilities may then be used to guide treatment planning in a thoughtful way1. The effects of interventions designed to impact muscle function can also be objectively verified, quantified, and documented with SEMG. In addition, patients can use SEMG feedback to learn more efficient patterns of movement control and transfer those skills to functional contexts. SEMG Advantages and Limitations During an initial clinical evaluation, on the most basic level, movements are observed and relevant muscles palpated. These evaluation techniques however, are and will always be subjective and qualitative. Manual muscle testing is an alternative with some degree of quantification, however, these techniques are insensitive to small changes in levels of muscle activity, activity near resting levels, and to muscle activity patterns performed during dynamic, functional activities. Mechanical dynamometers can be used to measure resultant forces from muscle contraction with greater accuracy. However, in addition to being void of muscle activity levels at rest and precision, techniques involving dynamometers have a propensity to be limited to static or simple situations. Isokinetic devices present a means of quantifying torque, timing, and joint motion relationships during static or dynamic conditions. The disadvantages with these systems are that the equipment is often bulky, expensive and generally restricts movements to isolated joint segments in fixed planes. Other computer-assisted dynamometers measure force output during functional or simulated functional tasks. Again, many of these restrict the subject to certain movements, and do not provide the ability to isolate activity of particular muscles. This is not to suggest these techniques and technologies are without some advantages, however, SEMG supplies a window into the movement system unattainable by any other means.
2
Clinical Sequence Assessments and SEMG Feedback
SEMG is the recording of the algebraic sum of muscle action potentials from the skin surface. It is used to monitor muscle activity, which is a direct representation of the outflow of motor neurons in the spinal cord to the muscle as a result of voluntary or reflex action2. For a more detailed, fundamental overview of EMG, the reader is referred to “The ABC of EMG” Konrad P (Noraxon USA http://www.noraxon.com/emg/emg.php3 ). As an indicator of muscle activity, SEMG offers certain advantages.
1. The subject need not be positioned in fixed postures, but is free to assume any fixed position or perform any functional movement that is desired.
2. Recordings can be made from most skin surfaces. 3. Muscle activity can be easily assessed where dynamometers would be impractical. (e.g.
facial muscles). 4. Surface EMG recordings are non-invasive and painless. No needles or noxious stimuli are
ever involved. 5. Surface EMG recordings are highly sensitive to small changes in muscle activity, low
levels of activity as well as forceful contractions. 6. Within certain limits, the activity of particular muscles or muscle groups can be
distinguished. 7. Set up is relatively quick and uncomplicated.
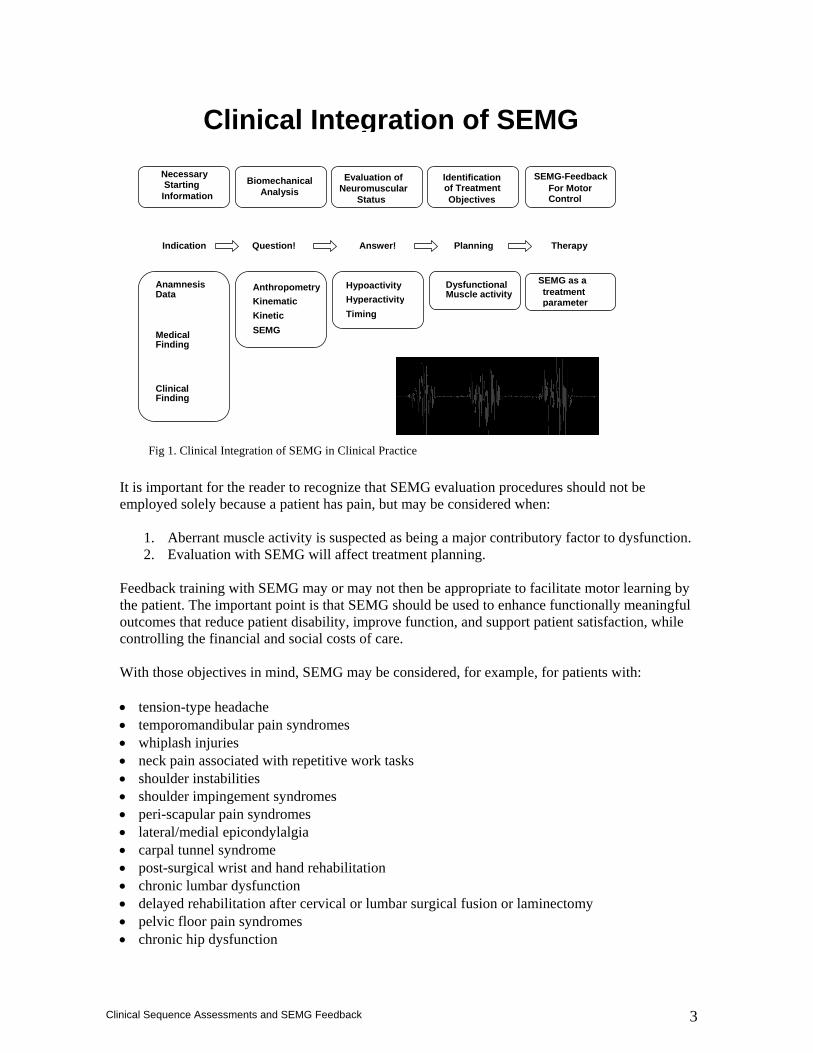
SEMG like any evaluation technique is not without its limitations. SEMG may be conceptualized in contrast to percutaneous needle EMG. With percutaneous needle EMG studies, the electrical activity of individual motor units may be visualized, and the effects of muscle and neurological disease may be evaluated. Individual motor units cannot be reliably discriminated with SEMG. Rather, SEMG is used to assess the magnitude and timing of overall muscle contractions. SEMG examines the assembly of motor events that subserve useful activity. SEMG may be used as an evaluation tool and as a form of feedback treatment (to be presented in future booklets) during the rehabilitation process and has been shown to provide reliable and descriptive information that is valuable for researchers and practitioners under static and dynamic conditions.3-11 Therefore, SEMG offers insight into the active component of muscle imbalance and a relatively simple means of monitoring patterns of muscle activity that result in disability due to soft tissue and articular impairments and can be linked by clinicians to the results of physical examination. Clinical Integration of SEMG The value of SEMG relies heavily on the appropriate integration of SEMG data in the clinical setting and its link to pending therapy decisions. (Figure 1). Therefore, to make use of such technologies clinically, two main elements must be addressed:
1. It must be relatively easy to use. 2. It must be clinically relevant.
3
Clinical Sequence Assessments and SEMG Feedback
It is important for the reader to recognize that SEMG evaluation procedures should not be employed solely because a patient has pain, but may be considered when:
1. Aberrant muscle activity is suspected as being a major contributory factor to dysfunction. 2. Evaluation with SEMG will affect treatment planning.
Feedback training with SEMG may or may not then be appropriate to facilitate motor learning by the patient. The important point is that SEMG should be used to enhance functionally meaningful outcomes that reduce patient disability, improve function, and support patient satisfaction, while controlling the financial and social costs of care. With those objectives in mind, SEMG may be considered, for example, for patients with: • tension-type headache • temporomandibular pain syndromes • whiplash injuries • neck pain associated with repetitive work tasks • shoulder instabilities • shoulder impingement syndromes • peri-scapular pain syndromes • lateral/medial epicondylalgia • carpal tunnel syndrome • post-surgical wrist and hand rehabilitation • chronic lumbar dysfunction • delayed rehabilitation after cervical or lumbar surgical fusion or laminectomy • pelvic floor pain syndromes • chronic hip dysfunction
Clinical Integration of SEMG
Medical Finding
Clinical Finding
Anamnesis Data
Necessary Starting Information
Anthropometry KinematicKineticSEMG
Biomechanical Analysis
Question!
HypoactivityHyperactivityTiming
Evaluation of Neuromuscular
Status
Answer!
Identificationof Treatment Objectives
Dysfunctional Muscle activity
Planning
SEMG-Feedback For Motor Control
SEMG as a
treatment parameter
Therapy Indication
Fig 1. Clinical Integration of SEMG in Clinical Practice
4
Clinical Sequence Assessments and SEMG Feedback
• delayed rehabilitation after anterior cruciate ligament repair • delayed rehabilitation after total knee replacement • selected patellofemoral pain syndromes Assessment Parameters of Patients Using SEMG The amplitude of the SEMG signal is generally expressed as some number of microvolts (uV), noted as series of relatively instantaneous measurements, or averaged or integrated over a clinically meaningful period of time. Amplitude analyses are conducted to evaluate the magnitude (“how much activity”) and timing patterns (“when does the activity occur”) of muscle activity. Inferences are drawn regarding a muscle’s role in effecting a particular posture or movement, and how pathologic processes alter that role. The SEMG activity of a homologous muscle pair or that of an agonist, compared with its antagonists or synergists, is examined to assess muscle balance. Use of SEMG amplitudes has been described for examination and feedback training with a wide variety of musculoskeletal disorders12. Clinically less common than amplitude analyses is investigation in the frequency domain to study muscular fatigue. SEMG amplitude tracings may be processed to reveal a range of component frequencies, the spectrum of which shifts in a reliable way with fatigue. For the purpose of this booklet, assessment will be limited to rudimentary evaluations using amplitude analyses. Future booklets will introduce basic SEMG-Feedback techniques. For more extensive approaches, the reader is referred elsewhere12. It is imperative for the reader to understand that all patients should undergo a thorough clinical examination prior to a SEMG evaluation. If not by the SEMG practitioner, then by a close associate/assistant, with whom the SEMG data can be shared. Sorting and interpreting the SEMG evaluation results exclusive of the examination assessment and examination results yields little information and may actually impede treatment planning. The objectives of the clinical SEMG evaluation are fourfold:
1. To expose and identify abnormal levels and patterns of muscle activity. 2. To expose related neuromuscular impairments and identify potential psychologic
contributions. 3. To establish how, or if objectives 1 and 2 are linked together. 4. To integrate qualitative and quantitative SEMG data with the clinical exam in preparation
for treatment.
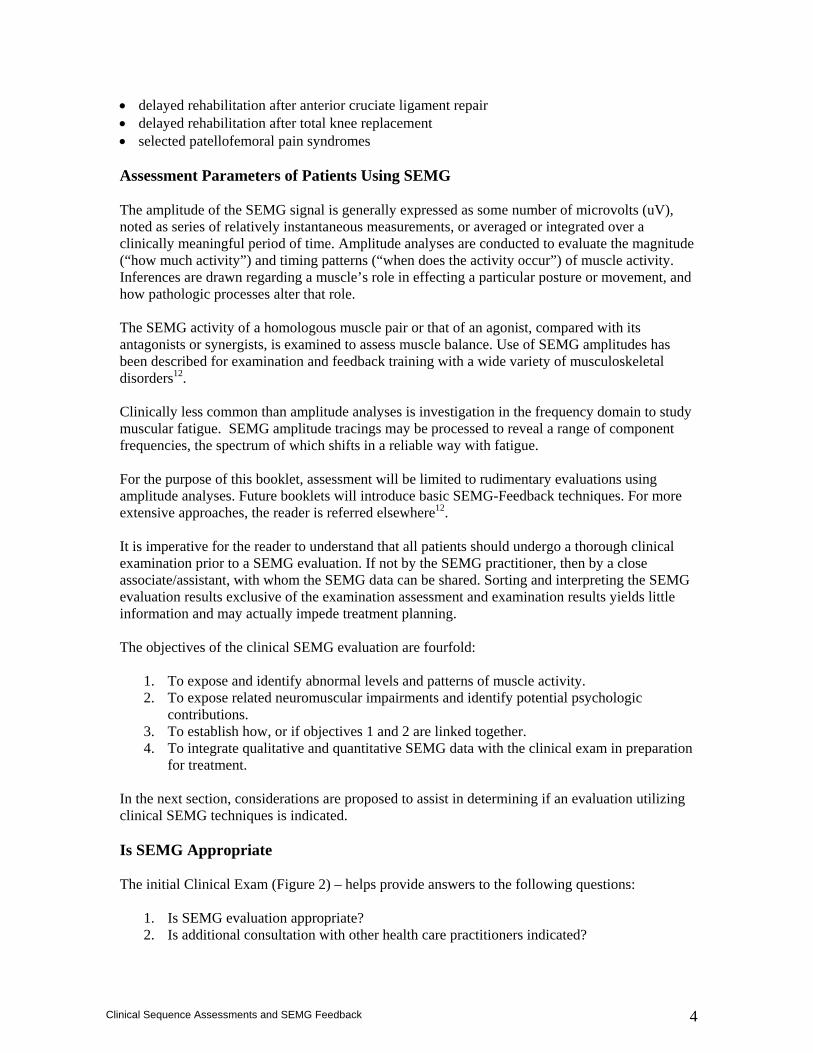
In the next section, considerations are proposed to assist in determining if an evaluation utilizing clinical SEMG techniques is indicated. Is SEMG Appropriate The initial Clinical Exam (Figure 2) – helps provide answers to the following questions:
1. Is SEMG evaluation appropriate? 2. Is additional consultation with other health care practitioners indicated?
5
Clinical Sequence Assessments and SEMG Feedback
3. If evaluation with SEMG is indicated, should the SEMG evaluation include kinesiologic techniques, psychophysiologic techniques, or both?
4. What treatment options are there? The first level is the clinical exam, which is made on the basis of referral criteria, history and intake, physical examination, and screening questionnaires. As outlined by Kasman,12 SEMG evaluation is indicated if all of the following conditions exist:
1. Functional limitations and disability are clearly identified. 2. Neuromuscular impairments are a suspected component. 3. Serious medical or psychologic pathology is unlikely, or, is concurrently being addressed
by a care provider. 4. Information regarding muscle activity is likely to assist with insight into the case and have
an impact on treatment planning.
Kinesiologic SEMG Sequence Assessments The kinesiologic clinical SEMG sequence assessments presented in this booklet are a series of procedures designed to systematically evaluate and analyze muscle activity specific to various body regions. They are presented in an effort to allow the novice user to characterize muscle function under clinically relevant circumstances. The assessments are not exhaustive, to the contrary, they are uncomplicated protocols designed to be relatively brief, yet clinically meaningful; that is, to identify the associated conditions under which muscle activity is dysfunctional and when it is not. Additional considerations are also presented; however, more complex SEMG assessment possibilities are beyond the scope of this booklet. It is the hope of the authors that novice readers will explore more advanced techniques found elsewhere.12 The SEMG findings may be inferred and should be balanced with clinical findings discovered during the initial clinical exam. Recording sites included in the protocols are generally selected based on common neuromuscular impairments from available literature that includes SEMG. Popular recording sites for each region are included. Additional recording channels outside of those presented may be of interest and may be found in the literature and in more advanced assessments. Activity of the target muscles are monitored during habitual and if possible, corrected postures, and basic functional movements. The Clinical Kinesiologic SEMG Sequence Assessments should be thought of as a menu of beginning options for the novice due to the ease of setup, simplicity of techniques and
Fig 2. During the clinical exam, if SEMG is deemed appropriate, the “type” of SEMG evaluation needs to be determined.
6
Clinical Sequence Assessments and SEMG Feedback
information that can be extracted. However, once experienced, the reader is encouraged to explore more advanced techniques. For any particular patient, the clinician should consult the history and intake, and select techniques that are relevant for the individual patient. Psychophysiologic and Proprioceptive Techniques Psychophysiogic evaluations are commonly conducted with patients exhibiting remarkable psychologic components with concurrent neuromuscular complaints. Proprioceptive techniques are largely subjective procedures which may be used with patients where pain management is the focus. They are generally used with subjects demonstrating unilaterally involved, subjectively reported hyperactive muscles. The focus of the procedure is to evaluate if patients do exhibit these proprioceptive deficits, when they may occur and to reveal the muscle activity associated with these deficits. Proprioceptive SEMG feedback techniques may also be used to assist the patient in gaining control of involuntary muscle hyperactivity. This is not to suggest that all patients will have psychophysiologic and/or proprioceptive dysfunction. However, it is important for clinicians across professions to become familiar with other evaluation options that are available and not covered in this booklet. Psychophysiologic and proprioceptive techniques have been deliberately excluded in this booklet in an effort to focus on simple Kinesiologic evaluation techniques. This is not to diminish the effectiveness or applicability of these options, but rather to bring focus on rudimentary kinesiologic techniques. Kinesiologic SEMG techniques The kinesiologic assessment techniques/protocols are presented in a manner that would reasonably be integrated within an SEMG evaluation sequence. It is imperative to understand the 2 basic techniques are designed primarily for the novice and more advance techniques and prioritizing of techniques and/or sequences should be considered. For the purpose of this booklet the two procedures are the Postural Baseline and Active Range of Motion procedures.
Interpretation of Clinical SEMG Data - General Principles
SEMG amplitude interpretation of Kinesiologic SEMG data is perhaps the most challenging and made on the basis of several variables. The following categories of analytical questions relating to muscular activity can be addressed using the clinical SEMG sequence assessments: 1. Is the muscle active? 2. Is the muscle hyperactive or hypoactive? 3. When is the muscle active? These questions and recording results are dissected further and a variety of sub-categories arise:
1. How active is the muscle? (e.g. Hyperactive/Hypoactive) 2. What is the dynamic relationship to antagonists/synergists? 3. Temporal Components “Do the muscles fire when they should”? 4. Do the muscle(s) deactivate when appropriate? 5. What are the corresponding clinical signs?
7
Clinical Sequence Assessments and SEMG Feedback
When planning clinical SEMG investigations it is very important to pursue reasonable comparison conditions. Often, with the exception of many TMD pain-patients, data cannot be MVC normalized; therefore, the strategy is to create ratios and quantity differences between two findings. The following comparison classes can be considered:
• Pre-test : Post-test to demonstrate “tendencies”. • Left to right side differences between involved/uninvolved sides. • Activity A vs. B ; Evaluates muscle activity during different movements/positions. • Signal portion A vs. B.; Demonstrates time domain changes in amplitude. • Muscle A vs. B.; Allows the qualitative comparison of synergists and antagonists. • Patient vs. Norm-curve dysfunctional EMG patterns.
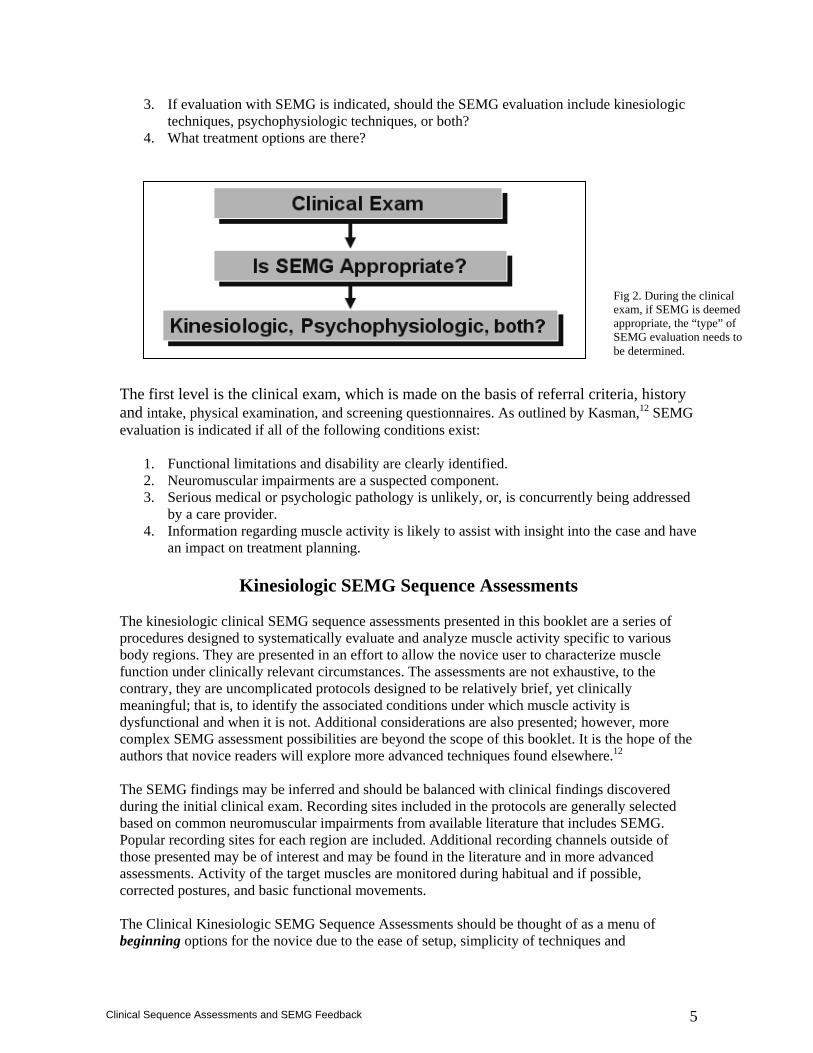
The following section outlines more specific criteria using a structured approach that may be included when interpreting SEMG data from the clinical sequence assessments. Observational Criteria To interpret a clinical SEMG finding, the authors propose a system of 3 systematic observational categories (Groups). Based on the previous question type (nominal, ordinal, metric) this is done using qualitative terms, calculated values or data tendencies. Due to its relative nature (microvolts vary from subject to subject), it is helpful to describe clinical SEMG with a mixture of qualitative terms and signal ratios to additional clinical findings such as kinematic and/or postural characteristics that correlate with SEMG findings. Group A Focuses on the single selected recording sites and describes the SEMG signal in terms of amplitude, and timing characteristics:
Parameter Observe and Document Magnitude of amplitude (Figure 3)
Increased, decreased, absent
Timing of activation (Figure 4)
Early, late or asynchronous
Time domain changes (Figure 4)
Amplitude increase/decrease
Fig 3. Possible corresponding qualitative views of SEMG curves if comparing to the homologous partner. The three qualitative analysis possibilities include; Hyperactivity (Too much), Hypoactivity (Too little) and Inhibited (remarkably absent) when compared to the homologous partner. All aberrant activity is represented by red curves.
8
Clinical Sequence Assessments and SEMG Feedback
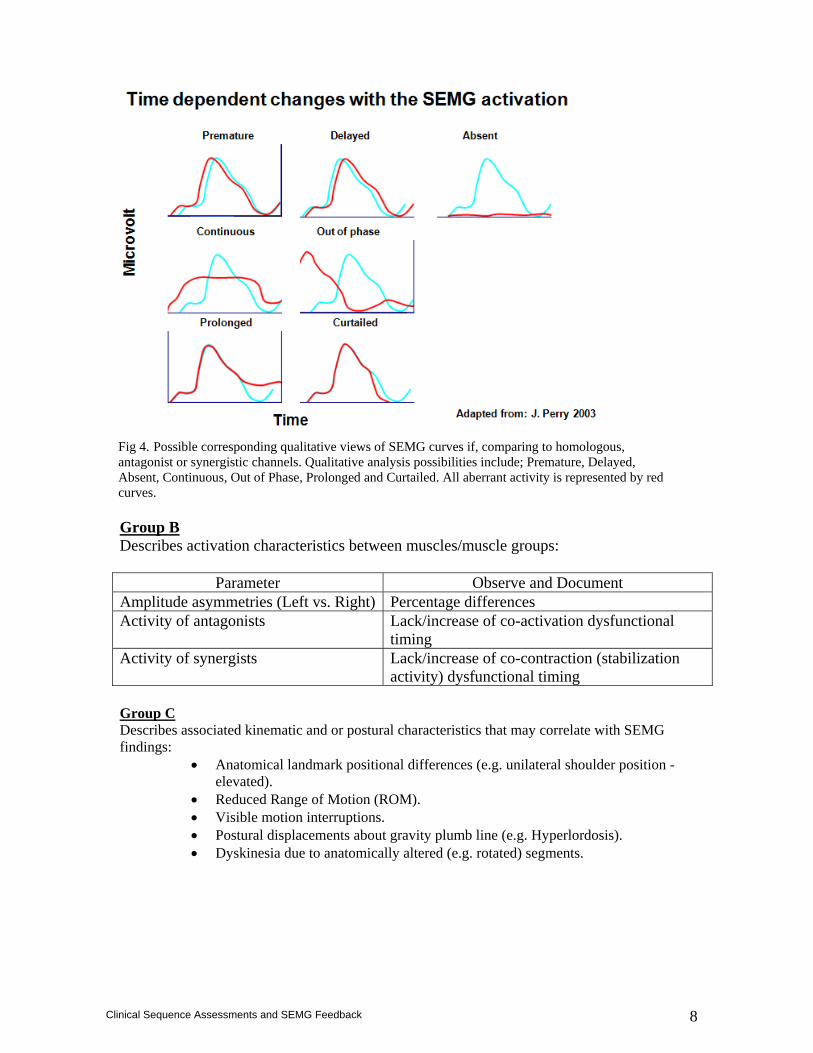
Group B Describes activation characteristics between muscles/muscle groups:
Parameter Observe and Document Amplitude asymmetries (Left vs. Right) Percentage differences Activity of antagonists Lack/increase of co-activation dysfunctional
timing Activity of synergists Lack/increase of co-contraction (stabilization
activity) dysfunctional timing Group C Describes associated kinematic and or postural characteristics that may correlate with SEMG findings:
• Anatomical landmark positional differences (e.g. unilateral shoulder position - elevated).
• Reduced Range of Motion (ROM). • Visible motion interruptions. • Postural displacements about gravity plumb line (e.g. Hyperlordosis). • Dyskinesia due to anatomically altered (e.g. rotated) segments.
Fig 4. Possible corresponding qualitative views of SEMG curves if, comparing to homologous, antagonist or synergistic channels. Qualitative analysis possibilities include; Premature, Delayed, Absent, Continuous, Out of Phase, Prolonged and Curtailed. All aberrant activity is represented by red curves.
9
Clinical Sequence Assessments and SEMG Feedback
Phases of Proposed Sequences Assessments and Observations Phase 1 - Baseline/Static Phase The Baseline/Postural SEMG phase assists in providing answers to the questions: 1. Is the muscle active? 2. Is the muscle(s) hyperactive or hypoactive? SEMG Baseline/postural assessments have been popular for clinical and experimental studies for all regions. Evaluations are relatively quick, simple and may yield a great deal of information if conducted with precision and combined with clinical exam findings. The baseline/postural phase is used for the analysis of muscle activity of the relative resting activity during the patient’s habitual seated or standing posture. In essence, it is a window into how much muscular energy the patient is expending to maintain postural rest. This phase allows for the documentation and observance of muscle activity during the patient’s habitual posture, symmetrical activity between homologous pairs, and relative activity among muscle groups during habitual rest position in either the seated or standing positions. If performed post intervention (e.g. exercise or therapeutic modalities), it also may also demonstrate the effects of the chosen intervention. During the baseline portion of the SEMG evaluation, the patient is commonly assessed in a habitual postural (standing and/or seated) position. In these positions, muscles oppose gravity, and disturbances in muscle activation patterns are believed to be associated with a disturbance in postural homeostasis.13
Posture may be defined as the relative position of the various parts of the body with respect to the egocentric coordinate system (one another), the exocentric coordinate system (environment), and the geocentric coordinate system (gravitational field). The orientation of any body part may be described in terms of these frameworks. Thus, posture in this context reflects a dynamic process. When and how one moves, one is unaware of the complex neuromuscular processes that control the postural components. Postural control involves the meaningful integration of many different neural systems, including those associated with cognition. The mechanical problem of maintaining the posture of any single region of the body is that there are profound effects on proximal and distal regions. Therefore, the postural system as a whole and regionally must meet four main challenges:
1. It must maintain a steady state in the presence of gravity (e.g. postural rest). 2. It must generate responses that anticipate movement (e.g. muscle activity prior to
repetitive movement). 3. It must be adaptive. 4. Postural control must be integrated with voluntary goal-directed movement.
Due to their varying functions, morphology, and amounts of adipose tissue, different muscles or muscle groups have dissimilar SEMG postural or resting values, and resting values vary as a function of posture. Adaptive changes in muscle length are likely both the cause and effect of faulty postures. Adaptive muscle length/tension relationships effect static/baseline amplitudes and predispose
10
Clinical Sequence Assessments and SEMG Feedback
dynamic evaluations to altered muscle recruitment patterns. For example, minor postural adjustments of the upper extremity or torso are known to affect the baseline activity of the erector spinae musculature.14 Disturbances to the postural system may be due to one or more factors: pain, postural habits (forward head posture), anatomical features, neurologic impairment, or emotional arousal. Therefore, it is imperative for the clinician to note any associated impairments that may influence aberrant postural responses. Position and posture are also important issues for dynamic SEMG recordings. An example of influences of posture and position on dynamic SEMG evaluation and treatment are described by Middaugh et al.15 The authors demonstrate how forward head posture and arm position are noted for augmentation of the resting activity of the Upper Trapezius. Recruitment patterns of the Upper Trapezius were noted to be inefficient during movement when the posture was poor and more efficient closer to the ideal postural position. Regardless, it is necessary that postural information obtained from the initial clinical exam (e.g. patient postural alignment) be incorporated in order to properly interpret the SEMG data. Simple clinical methods include the use of a flexible ruler for spinal curves, digital photographs relative to gravitation plum-lines to more complex computer programs. An elevated baseline level implies that a muscle has insufficient opportunity for rest. SEMG amplitude and frequency spectral changes and other physiologic indexes of fatigue have been reported with 5% to 10% maximal volitional isometric contraction (MVIC) sustained for one hour,16,17 and, associated prospectively and retrospectively with upper quadrant musculoskeletal complaints.18-20 When represented as a percentage of maximal volitional isometric contraction (%MVIC), higher static muscle loads have been associated with muscle pain and resting jaw muscle activity21-24
where pain free subjects demonstrate resting levels of 1-2% MVIC for the temporalis anterior and masseter in men and women.25 This data is broadly consistent with ergonomic recommendations for trapezius sites of about 1% MVC and is considered acceptable for the major part of the work day if adequate breaks in the load pattern are allowed.26 Musculoskeletal illness has also been linked to prolonged contraction levels above 2%MVIC for the low back.27 In summary, low amplitude levels (e.g. approximately 2% MVIC or less) appear to be representative of physiologic amplitude values. Clinically, this provides an efficient method to determine acceptable static/baseline amplitudes, which may be operationally defined as less than about 2%MVIC amplitude for tasks that are functionally performed for about one hour or longer (e.g. habitual postural position). However, as mentioned earlier, the limitation is that in orthopedic pain patients, it is not uncommon that a maximal effort is sometimes not possible, thereby requiring an alternative/additional analyses such as the use of qualitative reporting as listed in this booklet. More easily stated, baseline levels from non-postural muscles should be close to internal noise levels of the SEMG recording instrumentation. The following section outlines basic clinical instructions for obtaining baseline and dynamic/movement recordings. It is presumed that the clinician is familiar with basic skin preparation procedures and has prioritized recording sites.
11
Clinical Sequence Assessments and SEMG Feedback
Clinical Procedures
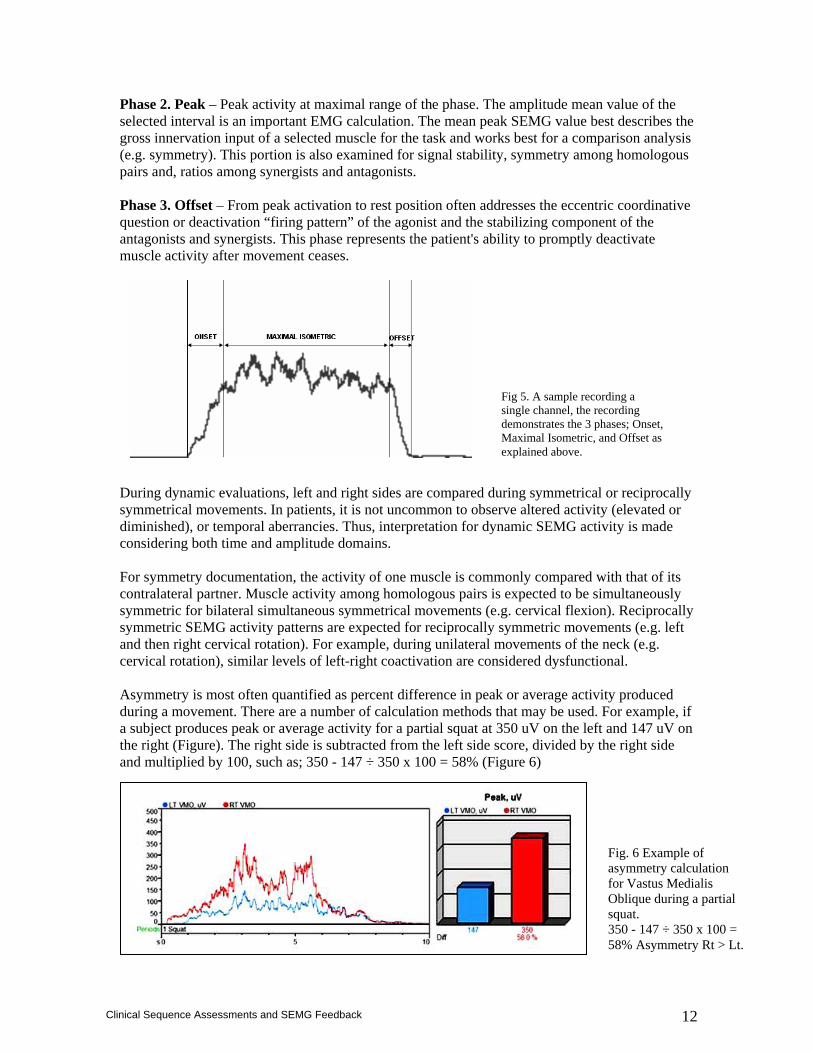
Clinical Procedure– Baseline/Postural Evaluation – Sitting or Standing 1. Ask the patient to assume their spontaneous or natural sitting or standing position. It is recommended that clinicians use neutral language, such as "sit or stand comfortably". 2. Observe the SEMG amplitude during a 15 to 60-second baseline period for consistency. Document the average SEMG amplitude during a 5 to 15-second baseline period assuming it is similar to that of the previously observed period. 3. Compare activity levels, variability within a single muscle site and for symmetry between the left and right of homologous pairs. This initial “habitual posture” recording should be recorded and saved. 4. Advanced considerations - For remarkable concurrent SEMG and postural asymmetries recorded during the habitual sitting posture, consider repositioning a forward head alignment and equalizing ischial weight bearing or place a folded towel under one buttock. This influences hip/sacral stability and may affect activation levels. Examine recording with these changes and save if changes are significant as this may provide evidence of distal involvement. For remarkable concurrent SEMG and postural asymmetries recorded during the habitual standing posture, consider repositioning the subject in a more “ideal” biomechanical alignment, then examine the recording with changes and save if changes are significant as this may provide evidence of distal involvement. 5. Document positions that relieve asymmetric or excessive muscle activity and ensure these positions also support biomechanically efficient joint alignment. Phase 2 - Active Range of Motion/Dynamic Phase The dynamic SEMG phases assist in answering the questions below and links them directly to a functional activity: 1. When is the muscle active? 2. How active is the muscle? Hyperactive/Hypoactive 3. What is the dynamic relationship to antagonists/synergists? 4. What do the temporal components demonstrate? 5. Do the muscles deactivate? Intuitively, clinically common, functional movements specific to each region are performed to investigate the relationship between agonists, antagonists and synergists of the chosen region. Typically, there is a functional dynamic and a brief isometric component. Thus, each dynamic phase is broken down into three basic sub-phases for interpretation (Figure 5): Phase 1. Onset – Represents the muscle activity from the rest position to maximal or desired maximal range of motion. This addresses the coordinative question or “firing pattern” of the muscle activity and represents the patient's ability to promptly and symmetrically (during bilateral movements) activate/recruit the monitored muscles.
12
Clinical Sequence Assessments and SEMG Feedback
Phase 2. Peak – Peak activity at maximal range of the phase. The amplitude mean value of the selected interval is an important EMG calculation. The mean peak SEMG value best describes the gross innervation input of a selected muscle for the task and works best for a comparison analysis (e.g. symmetry). This portion is also examined for signal stability, symmetry among homologous pairs and, ratios among synergists and antagonists. Phase 3. Offset – From peak activation to rest position often addresses the eccentric coordinative question or deactivation “firing pattern” of the agonist and the stabilizing component of the antagonists and synergists. This phase represents the patient's ability to promptly deactivate muscle activity after movement ceases. During dynamic evaluations, left and right sides are compared during symmetrical or reciprocally symmetrical movements. In patients, it is not uncommon to observe altered activity (elevated or diminished), or temporal aberrancies. Thus, interpretation for dynamic SEMG activity is made considering both time and amplitude domains. For symmetry documentation, the activity of one muscle is commonly compared with that of its contralateral partner. Muscle activity among homologous pairs is expected to be simultaneously symmetric for bilateral simultaneous symmetrical movements (e.g. cervical flexion). Reciprocally symmetric SEMG activity patterns are expected for reciprocally symmetric movements (e.g. left and then right cervical rotation). For example, during unilateral movements of the neck (e.g. cervical rotation), similar levels of left-right coactivation are considered dysfunctional. Asymmetry is most often quantified as percent difference in peak or average activity produced during a movement. There are a number of calculation methods that may be used. For example, if a subject produces peak or average activity for a partial squat at 350 uV on the left and 147 uV on the right (Figure). The right side is subtracted from the left side score, divided by the right side and multiplied by 100, such as; 350 - 147 ÷ 350 x 100 = 58% (Figure 6)
Fig. 6 Example of asymmetry calculation for Vastus Medialis Oblique during a partial squat. 350 - 147 ÷ 350 x 100 = 58% Asymmetry Rt > Lt.
Fig 5. A sample recording a single channel, the recording demonstrates the 3 phases; Onset, Maximal Isometric, and Offset as explained above.

13
Clinical Sequence Assessments and SEMG Feedback
Calculated in this manner, asymmetry exceeding a range of 10-15% has been reported to be of significance in masticatory muscles.28 For cervical thoracic, and lumbar paraspinal recording sites, 20% has been reported as being significant,29,30 and Middaugh demonstrated a 35% difference in the upper trapezius was significant.31 The observation of symmetry was also documented within fair degrees for 6 muscles of surrounding the knee.32 Generally speaking, symmetrical movement should produce relatively symmetrical muscle activity from homologous muscle pairs and reciprocal movement should produce reciprocally symmetrical muscle activity from homologous muscle pairs. Qualitative Analysis Due to potential differences in recording setup, adipose tissue, impedance, muscle cross-sectional area, and numerous other factors, useful comparisons between different subjects and different studies for SEMG values recorded between days, subjects, muscles or studies, the normalization process is required.33-36 and thus comparison and/or interpretation of qualitative analysis should be done with extreme caution. This is not to suggest qualitative analysis has no value. As mentioned previously, timing features may be qualitatively assessed. (e.g. smooth and well-timed). In addressing the analytical questions proposed previously, muscle activity may be documented using qualitative analysis in the following manner: Is the muscle active? This question is quickly answered by observing the SEMG signal during any recording technique. It is answered at the most elementary level with “yes” or “no”. Caution should be exercised to ensure the quality of the SEMG baseline allows a clear identification of active SEMG. For this, fundamental knowledge of the instrumentation (e.g. filtering and amplification) must be known to the user. Without this knowledge, noise may be interpreted as “increased activity” when it fact it may be noise. Post movement, a healthy subject tends to exhibit prompt return to baseline levels. For example, if SEMG activity remains elevated, this may be qualitatively described as a “delay in returning to original baseline levels.” Overall, baseline values from non-postural muscles should be relatively close to the internal noise levels of the instrumentation. This does however, limit microvolt values to within the same session assuming electrodes are not removed and replaced between techniques. Further, relative microvolt (uV) values may be expressed as long as they are not compared across sessions and subjects. Other than timing parameters, this is the only quantitative measure that can freely be performed with uV based data. Comparisons of uV based SEMG activity of the same muscle and electrode application can be one of the most important analysis strategies in clinical settings because it does not require normalization. Within the same session, the percentage differences of muscle activation are studied between test positions and movements which may reveal a difference in performance and efficiency. Is the muscle hyperactive or hypoactive? This question requires at least one comparison item. The most common of which is the same muscle on the contralateral side. It is commonly expressed as minimally, moderately or severely
14
Clinical Sequence Assessments and SEMG Feedback
elevated relative to the contralateral side. The underlying assumption is that the detection conditions on the one side are equal to the contralateral. A very strict electrode application technique is needed to create suitable conditions for such comparisons. When is the muscle active? The timing characteristics of a muscle may be qualitatively described within a certain movement event or in comparison to other muscles. For example, when a subject moves their limb(s) from rest position to perform a movement, muscle activity may be described qualitatively as “prompt and smooth” or aberrant. Timing may also be described relative to the contralateral side, a synergist or antagonist (e.g. Lower Trapezius activity significantly delayed relative to the Upper Trapezius during arm elevation). It is important to note that timing characteristics are quantitative in nature and descriptive dimensions are usually expressed in milliseconds and not microvolts. Therefore, clinicians are expected to be able to calculate percentages of asymmetry, MVIC or, a standardized submaximal reference contraction. If this is not feasible, most clinicians are obliged to refrain from cross-day, cross-site and cross-subjects recording comparisons or, reconcile the use of non-normalized data. Clinicians may decide that non-normalized data are valid and reliable for some particular evaluation process; however, the limitation is that non-normalized comparisons are much less reliable and clinicians may interpret data incorrectly, and ultimately may be subjected to faulty clinical judgments. Due to the current large variation in healthy populations, it quickly becomes difficult to distinguish correctly between healthy subjects and those with abnormalities. Further, by avoiding normalization techniques, cross-day, cross-site and cross-subject comparisons simply can not be validated. Simple computations, such as asymmetry, allow for full interpretation with the other clinical SEMG techniques.
Clinical Procedure – Dynamic Phases – Step by Step Instructions 1. Have the subject sit or stand in a relaxed and upright position without additional support. 2. Begin recording while the patient is in their habitual standing or seated position. 3. Instruct the patient on how to perform the desired movement (e.g. bilateral shoulder flexion) and have the patient perform the movement 2-3 times. 4. Subjectively compare activity levels (timing, variability, symmetry and synergy) for consistency while performing these practice movements. 5. Repeat the movement once from #3 and save this recording if it appears consistent to previous trial efforts. The purpose behind this method is due to reliability of amplitude over five repetitions. Correlations between the first movement amplitude (peak) and the other four movement peaks has been reported to be relatively low (<0.40). However, the correlation between the second to fifth movement peaks was reported as very high (>0.90).37 This suggests that the third and above repetitions represent a reliable estimate of the recruitment pattern for the patient. In some cases consistency may be difficult to obtain. In these cases, a number of trials may be saved or applying a mathematical average (ensemble average) to time normalize the trials is recommended. 6. Compare activity levels (timing, variability, symmetry and synergy) of the final saved recording.
15
Clinical Sequence Assessments and SEMG Feedback
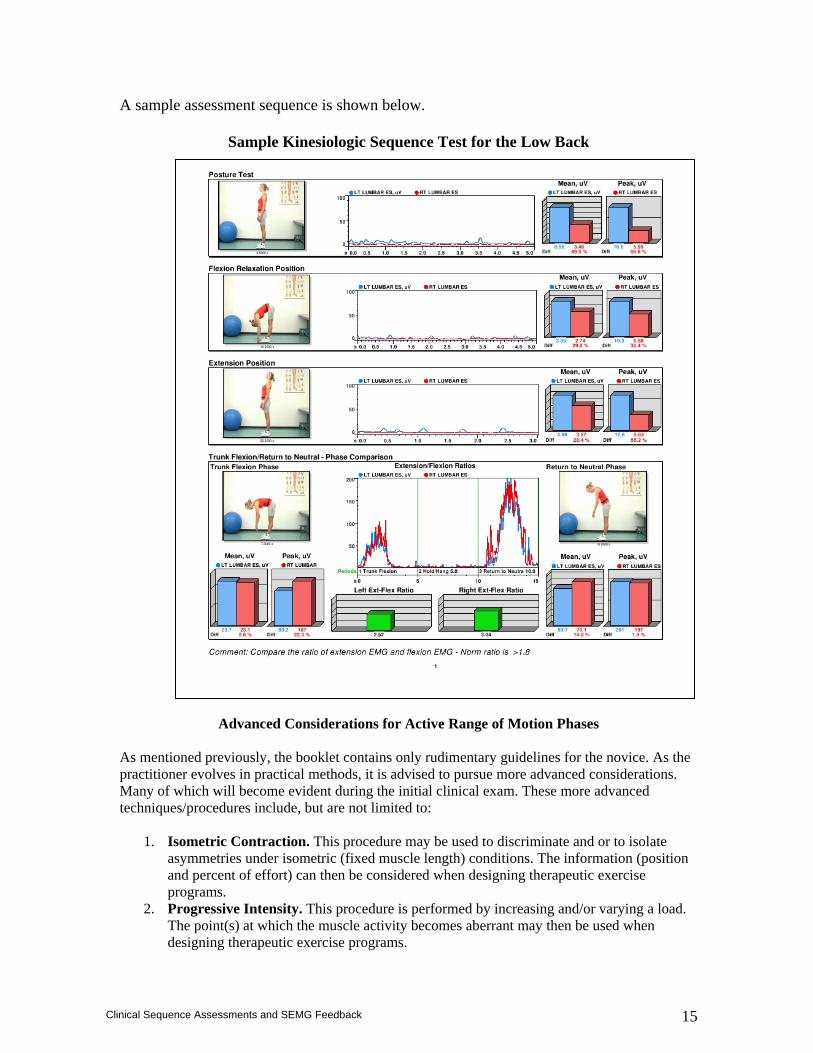
A sample assessment sequence is shown below.
Sample Kinesiologic Sequence Test for the Low Back
Advanced Considerations for Active Range of Motion Phases
As mentioned previously, the booklet contains only rudimentary guidelines for the novice. As the practitioner evolves in practical methods, it is advised to pursue more advanced considerations. Many of which will become evident during the initial clinical exam. These more advanced techniques/procedures include, but are not limited to:
1. Isometric Contraction. This procedure may be used to discriminate and or to isolate asymmetries under isometric (fixed muscle length) conditions. The information (position and percent of effort) can then be considered when designing therapeutic exercise programs.
2. Progressive Intensity. This procedure is performed by increasing and/or varying a load. The point(s) at which the muscle activity becomes aberrant may then be used when designing therapeutic exercise programs.

16
Clinical Sequence Assessments and SEMG Feedback
3. Progressive Velocities. This procedure is performed using a relevant constant load and the velocity of movement is varied. The velocity and point in ROM where the muscle activity becomes aberrant may then be used when designing therapeutic exercise programs.
4. Open and Closed Kinetic Chains. Generally used for the lower extremities (e.g. hip, knee etc). Aberrant patterns under both open and closed kinetic chain movements are noted. Combining with Progressive Intensities and Velocities is also not uncommon. The parameters under which the muscle activity becomes aberrant may then be used when designing therapeutic exercise programs.
17
Clinical Sequence Assessments and SEMG Feedback
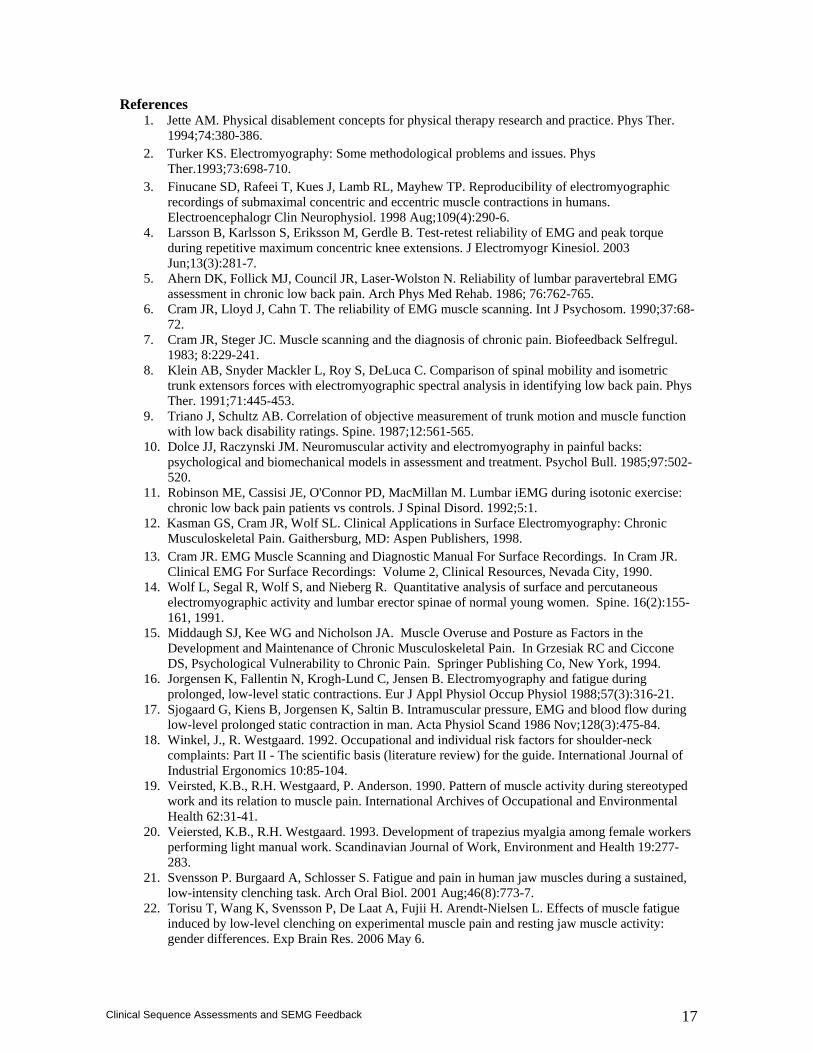
References 1. Jette AM. Physical disablement concepts for physical therapy research and practice. Phys Ther.
1994;74:380-386. 2. Turker KS. Electromyography: Some methodological problems and issues. Phys
Ther.1993;73:698-710. 3. Finucane SD, Rafeei T, Kues J, Lamb RL, Mayhew TP. Reproducibility of electromyographic
recordings of submaximal concentric and eccentric muscle contractions in humans. Electroencephalogr Clin Neurophysiol. 1998 Aug;109(4):290-6.
4. Larsson B, Karlsson S, Eriksson M, Gerdle B. Test-retest reliability of EMG and peak torque during repetitive maximum concentric knee extensions. J Electromyogr Kinesiol. 2003 Jun;13(3):281-7.
5. Ahern DK, Follick MJ, Council JR, Laser-Wolston N. Reliability of lumbar paravertebral EMG assessment in chronic low back pain. Arch Phys Med Rehab. 1986; 76:762-765.
6. Cram JR, Lloyd J, Cahn T. The reliability of EMG muscle scanning. Int J Psychosom. 1990;37:68-72.
7. Cram JR, Steger JC. Muscle scanning and the diagnosis of chronic pain. Biofeedback Selfregul. 1983; 8:229-241.
8. Klein AB, Snyder Mackler L, Roy S, DeLuca C. Comparison of spinal mobility and isometric trunk extensors forces with electromyographic spectral analysis in identifying low back pain. Phys Ther. 1991;71:445-453.
9. Triano J, Schultz AB. Correlation of objective measurement of trunk motion and muscle function with low back disability ratings. Spine. 1987;12:561-565.
10. Dolce JJ, Raczynski JM. Neuromuscular activity and electromyography in painful backs: psychological and biomechanical models in assessment and treatment. Psychol Bull. 1985;97:502-520.
11. Robinson ME, Cassisi JE, O'Connor PD, MacMillan M. Lumbar iEMG during isotonic exercise: chronic low back pain patients vs controls. J Spinal Disord. 1992;5:1.
12. Kasman GS, Cram JR, Wolf SL. Clinical Applications in Surface Electromyography: Chronic Musculoskeletal Pain. Gaithersburg, MD: Aspen Publishers, 1998.
13. Cram JR. EMG Muscle Scanning and Diagnostic Manual For Surface Recordings. In Cram JR. Clinical EMG For Surface Recordings: Volume 2, Clinical Resources, Nevada City, 1990.
14. Wolf L, Segal R, Wolf S, and Nieberg R. Quantitative analysis of surface and percutaneous electromyographic activity and lumbar erector spinae of normal young women. Spine. 16(2):155-161, 1991.
15. Middaugh SJ, Kee WG and Nicholson JA. Muscle Overuse and Posture as Factors in the Development and Maintenance of Chronic Musculoskeletal Pain. In Grzesiak RC and Ciccone DS, Psychological Vulnerability to Chronic Pain. Springer Publishing Co, New York, 1994.
16. Jorgensen K, Fallentin N, Krogh-Lund C, Jensen B. Electromyography and fatigue during prolonged, low-level static contractions. Eur J Appl Physiol Occup Physiol 1988;57(3):316-21.
17. Sjogaard G, Kiens B, Jorgensen K, Saltin B. Intramuscular pressure, EMG and blood flow during low-level prolonged static contraction in man. Acta Physiol Scand 1986 Nov;128(3):475-84.
18. Winkel, J., R. Westgaard. 1992. Occupational and individual risk factors for shoulder-neck complaints: Part II - The scientific basis (literature review) for the guide. International Journal of Industrial Ergonomics 10:85-104.
19. Veirsted, K.B., R.H. Westgaard, P. Anderson. 1990. Pattern of muscle activity during stereotyped work and its relation to muscle pain. International Archives of Occupational and Environmental Health 62:31-41.
20. Veiersted, K.B., R.H. Westgaard. 1993. Development of trapezius myalgia among female workers performing light manual work. Scandinavian Journal of Work, Environment and Health 19:277-283.
21. Svensson P. Burgaard A, Schlosser S. Fatigue and pain in human jaw muscles during a sustained, low-intensity clenching task. Arch Oral Biol. 2001 Aug;46(8):773-7.
22. Torisu T, Wang K, Svensson P, De Laat A, Fujii H. Arendt-Nielsen L. Effects of muscle fatigue induced by low-level clenching on experimental muscle pain and resting jaw muscle activity: gender differences. Exp Brain Res. 2006 May 6.

18
Clinical Sequence Assessments and SEMG Feedback
23. Torisu T, Wang K, Svensson P, De Laat A, Fujii H. Arendt-Nielsen L. Effects of muscle fatigue induced by low-level clenching on experimental muscle pain and resting jaw muscle activity: gender differences. Exp Brain Res. 2006 May 6.
24. Svensson P. Burgaard A, Schlosser S. Fatigue and pain in human jaw muscles during a sustained, low-intensity clenching task. Arch Oral Biol. 2001 Aug;46(8):773-7.
19
Clinical Sequence Assessments and SEMG Feedback
Regional Applications of Sequence Assessments Using Surface Electromyography
This section of the booklet will provide an introduction to rudimentary assessment guidelines for clinical applications using surface electromyography (SEMG) for selected anatomical regions. Each chapter will proceed as follows:
1. Begin with a brief overview of the literature and description of considerations for the beginning practitioner.
2. An outline of a basic sequence assessment for the region. 3. The Clinical Procedure includes:
A. A list of the most common recording sites with corresponding electrode placement figure. The complete set of three figures may be found in the appendix at the end of the booklet. Proper skin preparation is important and it is assumed the reader is accomplished. For more information in this regard, the reader is referred to the companion publication “ABC of EMG by Dr. Peter Konrad.
B. Additional recording sites for consideration, but not as popular. C. A list of the proposed Kinesiologic Sequence phases for the region. D. Step by step instructions on how to conduct each phase. The reader is reminded to
have the subject practice the movement in between each phase prior to recording. 4. General interpretation considerations. In this section, the reader is given a brief outline
with references for what they may expect to see. It is important to know that although referenced, these are general guidelines and invariably patients can and some will likely vary from the expected recruitment patterns.
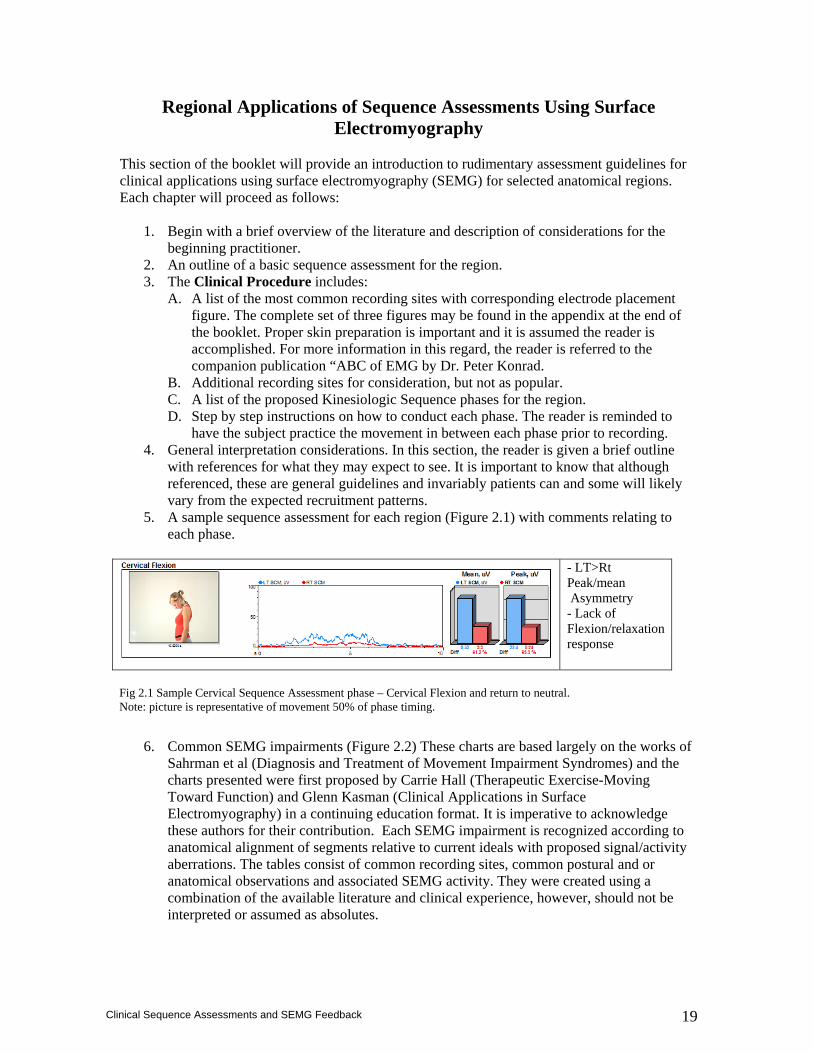
5. A sample sequence assessment for each region (Figure 2.1) with comments relating to each phase.
- LT>Rt Peak/mean Asymmetry - Lack of Flexion/relaxation response
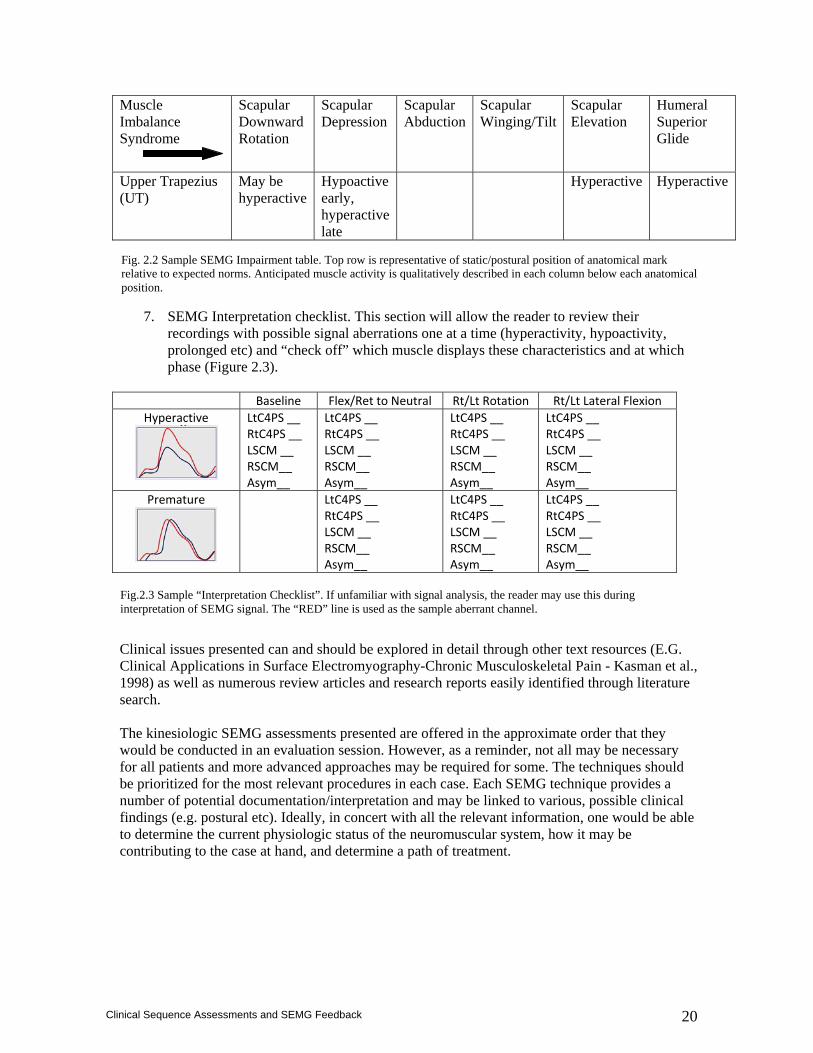
6. Common SEMG impairments (Figure 2.2) These charts are based largely on the works of
Sahrman et al (Diagnosis and Treatment of Movement Impairment Syndromes) and the charts presented were first proposed by Carrie Hall (Therapeutic Exercise-Moving Toward Function) and Glenn Kasman (Clinical Applications in Surface Electromyography) in a continuing education format. It is imperative to acknowledge these authors for their contribution. Each SEMG impairment is recognized according to anatomical alignment of segments relative to current ideals with proposed signal/activity aberrations. The tables consist of common recording sites, common postural and or anatomical observations and associated SEMG activity. They were created using a combination of the available literature and clinical experience, however, should not be interpreted or assumed as absolutes.
Fig 2.1 Sample Cervical Sequence Assessment phase – Cervical Flexion and return to neutral. Note: picture is representative of movement 50% of phase timing.
20
Clinical Sequence Assessments and SEMG Feedback
Muscle Imbalance Syndrome
Scapular Downward Rotation
Scapular Depression
Scapular Abduction
Scapular Winging/Tilt
Scapular Elevation
Humeral Superior Glide
Upper Trapezius (UT)
May be hyperactive
Hypoactive early, hyperactive late
Hyperactive Hyperactive
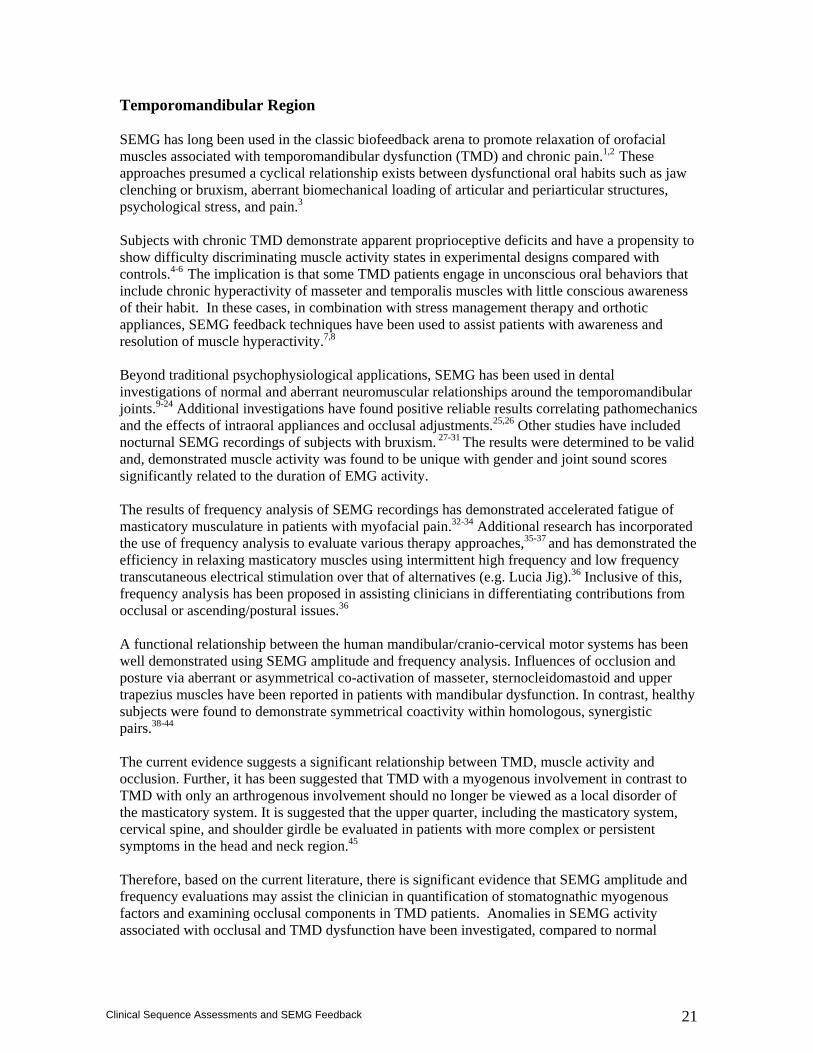
7. SEMG Interpretation checklist. This section will allow the reader to review their
recordings with possible signal aberrations one at a time (hyperactivity, hypoactivity, prolonged etc) and “check off” which muscle displays these characteristics and at which phase (Figure 2.3).
Baseline Flex/Ret to Neutral Rt/Lt Rotation Rt/Lt Lateral Flexion
Hyperactive
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Premature
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Clinical issues presented can and should be explored in detail through other text resources (E.G. Clinical Applications in Surface Electromyography-Chronic Musculoskeletal Pain - Kasman et al., 1998) as well as numerous review articles and research reports easily identified through literature search. The kinesiologic SEMG assessments presented are offered in the approximate order that they would be conducted in an evaluation session. However, as a reminder, not all may be necessary for all patients and more advanced approaches may be required for some. The techniques should be prioritized for the most relevant procedures in each case. Each SEMG technique provides a number of potential documentation/interpretation and may be linked to various, possible clinical findings (e.g. postural etc). Ideally, in concert with all the relevant information, one would be able to determine the current physiologic status of the neuromuscular system, how it may be contributing to the case at hand, and determine a path of treatment.
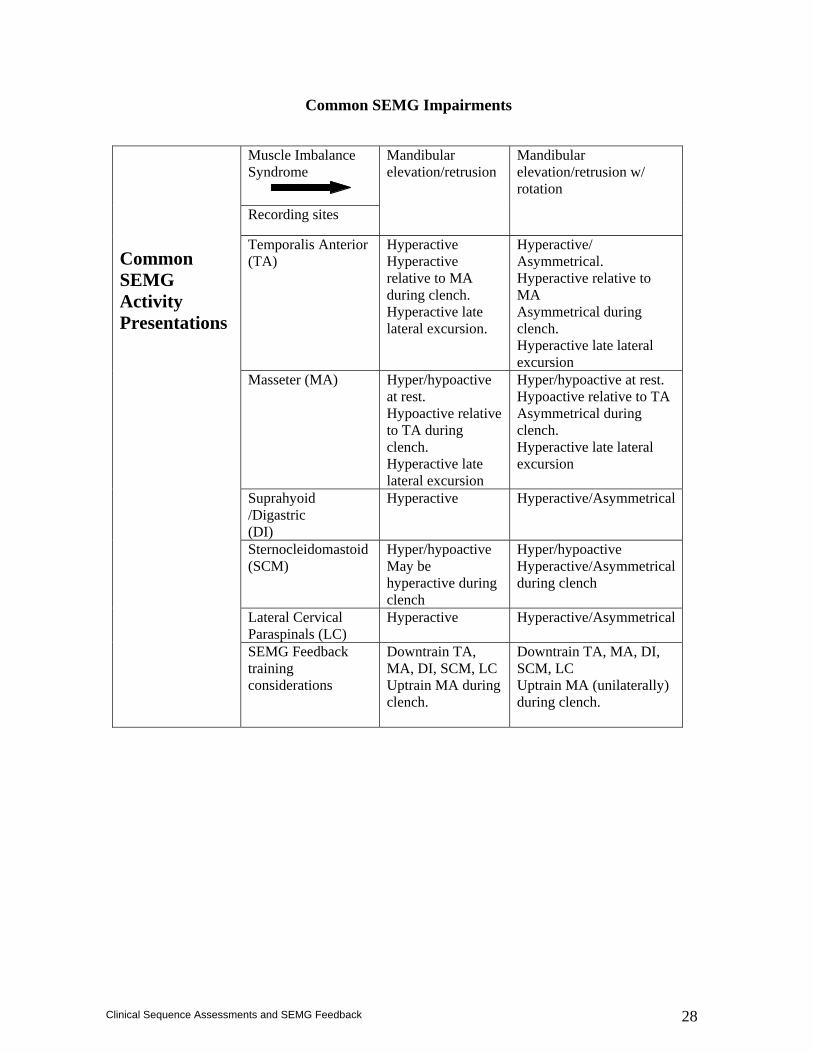
Fig. 2.2 Sample SEMG Impairment table. Top row is representative of static/postural position of anatomical mark relative to expected norms. Anticipated muscle activity is qualitatively described in each column below each anatomical position.
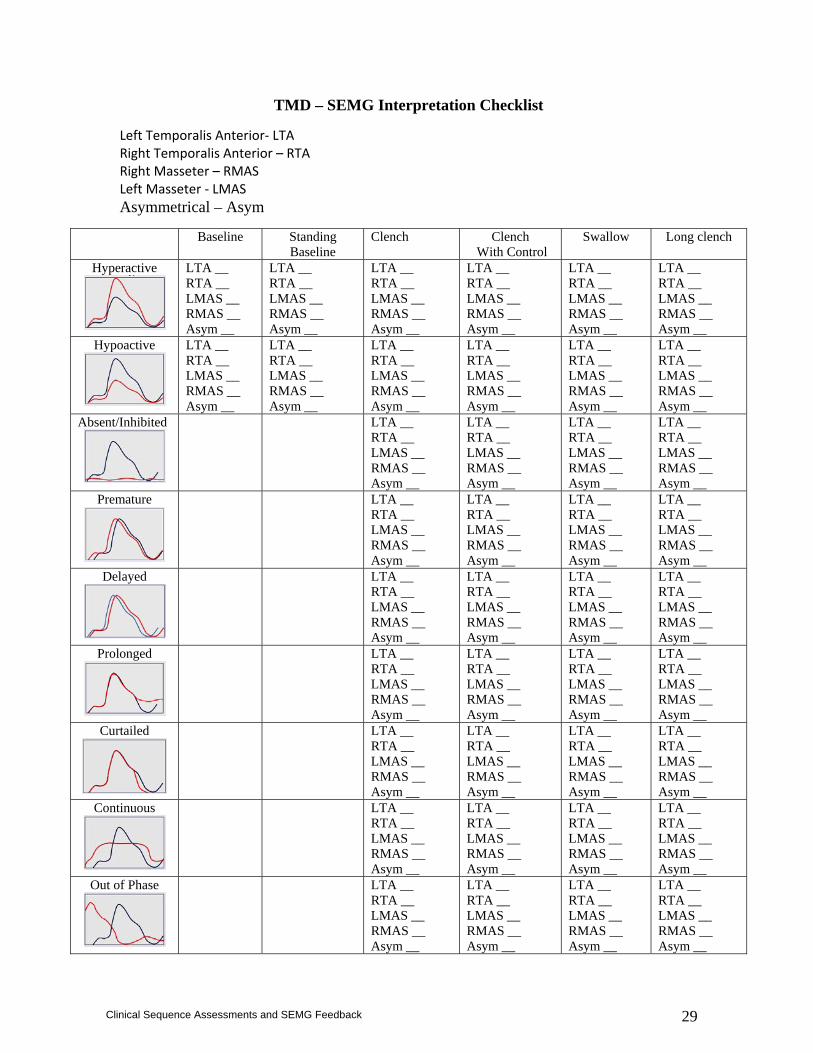
Fig.2.3 Sample “Interpretation Checklist”. If unfamiliar with signal analysis, the reader may use this during interpretation of SEMG signal. The “RED” line is used as the sample aberrant channel.
21
Clinical Sequence Assessments and SEMG Feedback
Temporomandibular Region SEMG has long been used in the classic biofeedback arena to promote relaxation of orofacial muscles associated with temporomandibular dysfunction (TMD) and chronic pain.1,2 These approaches presumed a cyclical relationship exists between dysfunctional oral habits such as jaw clenching or bruxism, aberrant biomechanical loading of articular and periarticular structures, psychological stress, and pain.3 Subjects with chronic TMD demonstrate apparent proprioceptive deficits and have a propensity to show difficulty discriminating muscle activity states in experimental designs compared with controls.4-6 The implication is that some TMD patients engage in unconscious oral behaviors that include chronic hyperactivity of masseter and temporalis muscles with little conscious awareness of their habit. In these cases, in combination with stress management therapy and orthotic appliances, SEMG feedback techniques have been used to assist patients with awareness and resolution of muscle hyperactivity.7,8 Beyond traditional psychophysiological applications, SEMG has been used in dental investigations of normal and aberrant neuromuscular relationships around the temporomandibular joints.9-24 Additional investigations have found positive reliable results correlating pathomechanics and the effects of intraoral appliances and occlusal adjustments.25,26 Other studies have included nocturnal SEMG recordings of subjects with bruxism. 27-31 The results were determined to be valid and, demonstrated muscle activity was found to be unique with gender and joint sound scores significantly related to the duration of EMG activity. The results of frequency analysis of SEMG recordings has demonstrated accelerated fatigue of masticatory musculature in patients with myofacial pain.32-34 Additional research has incorporated the use of frequency analysis to evaluate various therapy approaches,35-37 and has demonstrated the efficiency in relaxing masticatory muscles using intermittent high frequency and low frequency transcutaneous electrical stimulation over that of alternatives (e.g. Lucia Jig).36 Inclusive of this, frequency analysis has been proposed in assisting clinicians in differentiating contributions from occlusal or ascending/postural issues.36 A functional relationship between the human mandibular/cranio-cervical motor systems has been well demonstrated using SEMG amplitude and frequency analysis. Influences of occlusion and posture via aberrant or asymmetrical co-activation of masseter, sternocleidomastoid and upper trapezius muscles have been reported in patients with mandibular dysfunction. In contrast, healthy subjects were found to demonstrate symmetrical coactivity within homologous, synergistic pairs.38-44 The current evidence suggests a significant relationship between TMD, muscle activity and occlusion. Further, it has been suggested that TMD with a myogenous involvement in contrast to TMD with only an arthrogenous involvement should no longer be viewed as a local disorder of the masticatory system. It is suggested that the upper quarter, including the masticatory system, cervical spine, and shoulder girdle be evaluated in patients with more complex or persistent symptoms in the head and neck region.45 Therefore, based on the current literature, there is significant evidence that SEMG amplitude and frequency evaluations may assist the clinician in quantification of stomatognathic myogenous factors and examining occlusal components in TMD patients. Anomalies in SEMG activity associated with occlusal and TMD dysfunction have been investigated, compared to normal
22
Clinical Sequence Assessments and SEMG Feedback
subjects and expressed in terms of baseline amplitude, relative asymmetry, and timing including mandibular and cervical recording sites.10, 20-24
Further, due to the extensive contributing systems and potential limiting treatment factors due to a variety of circumstances, behavioral interventions cannot be ignored. From a psychophysiologic SEMG feedback perspective, the facilitation of relaxation and kinesthetic awareness in patients with TMD and tension type headaches continues to appear helpful and is straightforward. 46-47
For a more comprehensive approach using SEMG in TMD inclusive of dental interpretations, the reader is referred to “Introduction to Surface Electromyography in Temporomandibular Dysfunction” D.T. Shewman – Noraxon USA.
Clinical Procedure
Recording Sites
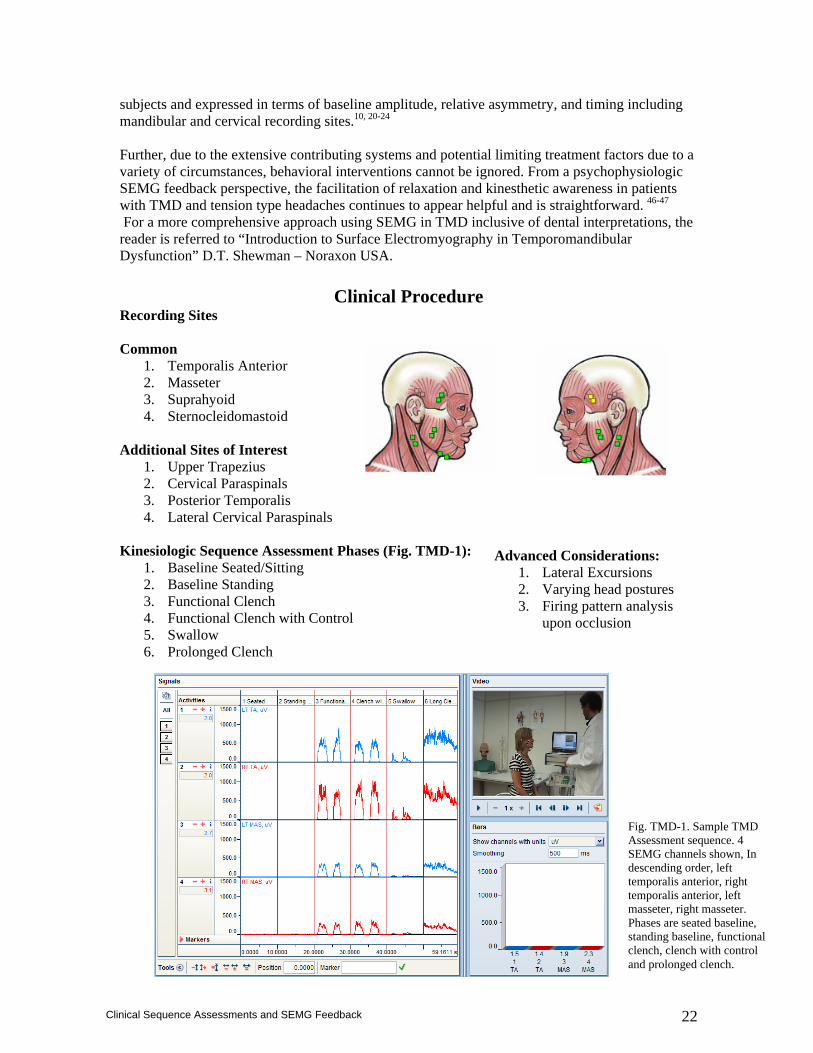
Common 1. Temporalis Anterior 2. Masseter 3. Suprahyoid 4. Sternocleidomastoid
Additional Sites of Interest
1. Upper Trapezius 2. Cervical Paraspinals 3. Posterior Temporalis 4. Lateral Cervical Paraspinals
Kinesiologic Sequence Assessment Phases (Fig. TMD-1):
1. Baseline Seated/Sitting 2. Baseline Standing 3. Functional Clench 4. Functional Clench with Control 5. Swallow 6. Prolonged Clench
Advanced Considerations: 1. Lateral Excursions 2. Varying head postures 3. Firing pattern analysis
upon occlusion
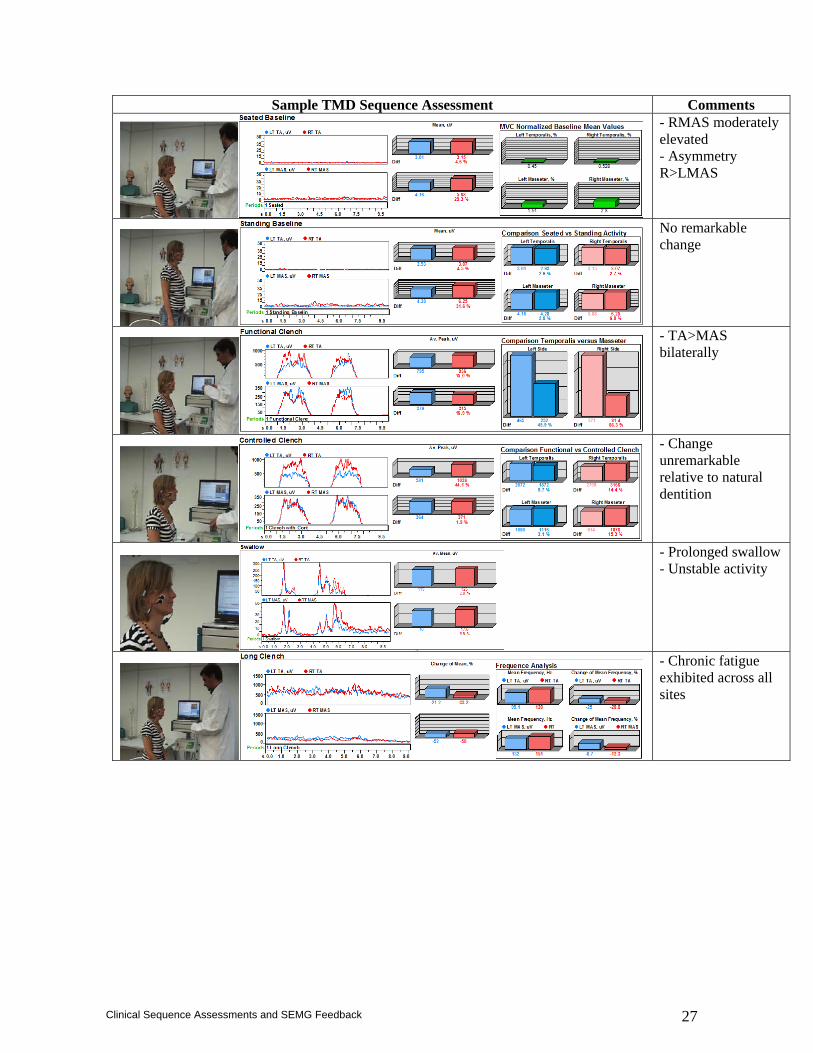
Fig. TMD-1. Sample TMD Assessment sequence. 4 SEMG channels shown, In descending order, left temporalis anterior, right temporalis anterior, left masseter, right masseter. Phases are seated baseline, standing baseline, functional clench, clench with control and prolonged clench.
23
Clinical Sequence Assessments and SEMG Feedback
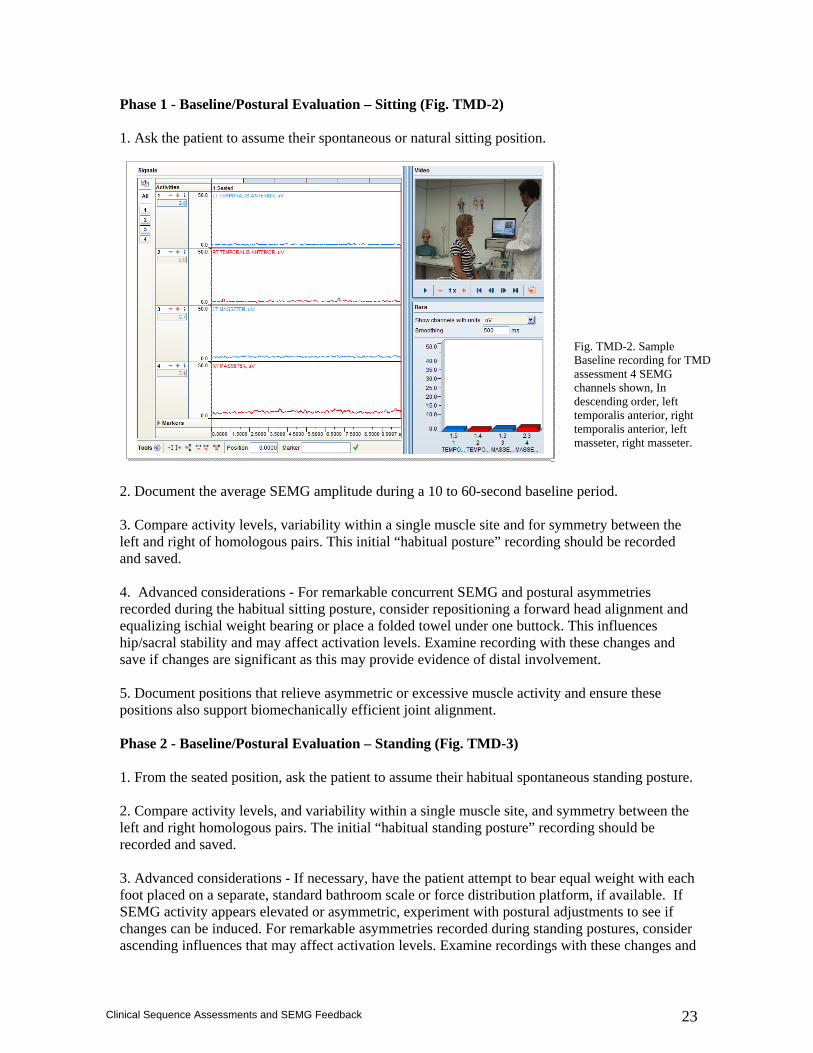
Phase 1 - Baseline/Postural Evaluation – Sitting (Fig. TMD-2) 1. Ask the patient to assume their spontaneous or natural sitting position. 2. Document the average SEMG amplitude during a 10 to 60-second baseline period. 3. Compare activity levels, variability within a single muscle site and for symmetry between the left and right of homologous pairs. This initial “habitual posture” recording should be recorded and saved. 4. Advanced considerations - For remarkable concurrent SEMG and postural asymmetries recorded during the habitual sitting posture, consider repositioning a forward head alignment and equalizing ischial weight bearing or place a folded towel under one buttock. This influences hip/sacral stability and may affect activation levels. Examine recording with these changes and save if changes are significant as this may provide evidence of distal involvement. 5. Document positions that relieve asymmetric or excessive muscle activity and ensure these positions also support biomechanically efficient joint alignment. Phase 2 - Baseline/Postural Evaluation – Standing (Fig. TMD-3) 1. From the seated position, ask the patient to assume their habitual spontaneous standing posture. 2. Compare activity levels, and variability within a single muscle site, and symmetry between the left and right homologous pairs. The initial “habitual standing posture” recording should be recorded and saved. 3. Advanced considerations - If necessary, have the patient attempt to bear equal weight with each foot placed on a separate, standard bathroom scale or force distribution platform, if available. If SEMG activity appears elevated or asymmetric, experiment with postural adjustments to see if changes can be induced. For remarkable asymmetries recorded during standing postures, consider ascending influences that may affect activation levels. Examine recordings with these changes and
Fig. TMD-2. Sample Baseline recording for TMD assessment 4 SEMG channels shown, In descending order, left temporalis anterior, right temporalis anterior, left masseter, right masseter.
24
Clinical Sequence Assessments and SEMG Feedback
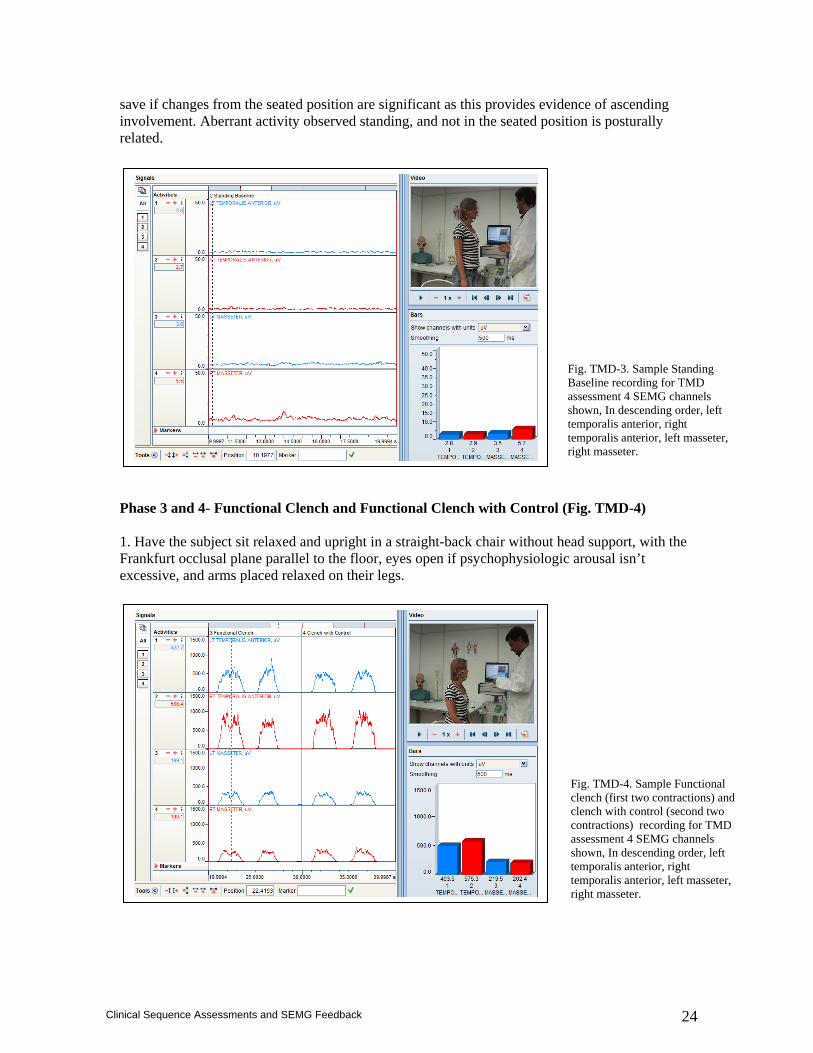
save if changes from the seated position are significant as this provides evidence of ascending involvement. Aberrant activity observed standing, and not in the seated position is posturally related. Phase 3 and 4- Functional Clench and Functional Clench with Control (Fig. TMD-4) 1. Have the subject sit relaxed and upright in a straight-back chair without head support, with the Frankfurt occlusal plane parallel to the floor, eyes open if psychophysiologic arousal isn’t excessive, and arms placed relaxed on their legs.
Fig. TMD-3. Sample Standing Baseline recording for TMD assessment 4 SEMG channels shown, In descending order, left temporalis anterior, right temporalis anterior, left masseter, right masseter.
Fig. TMD-4. Sample Functional clench (first two contractions) and clench with control (second two contractions) recording for TMD assessment 4 SEMG channels shown, In descending order, left temporalis anterior, right temporalis anterior, left masseter, right masseter.
25
Clinical Sequence Assessments and SEMG Feedback
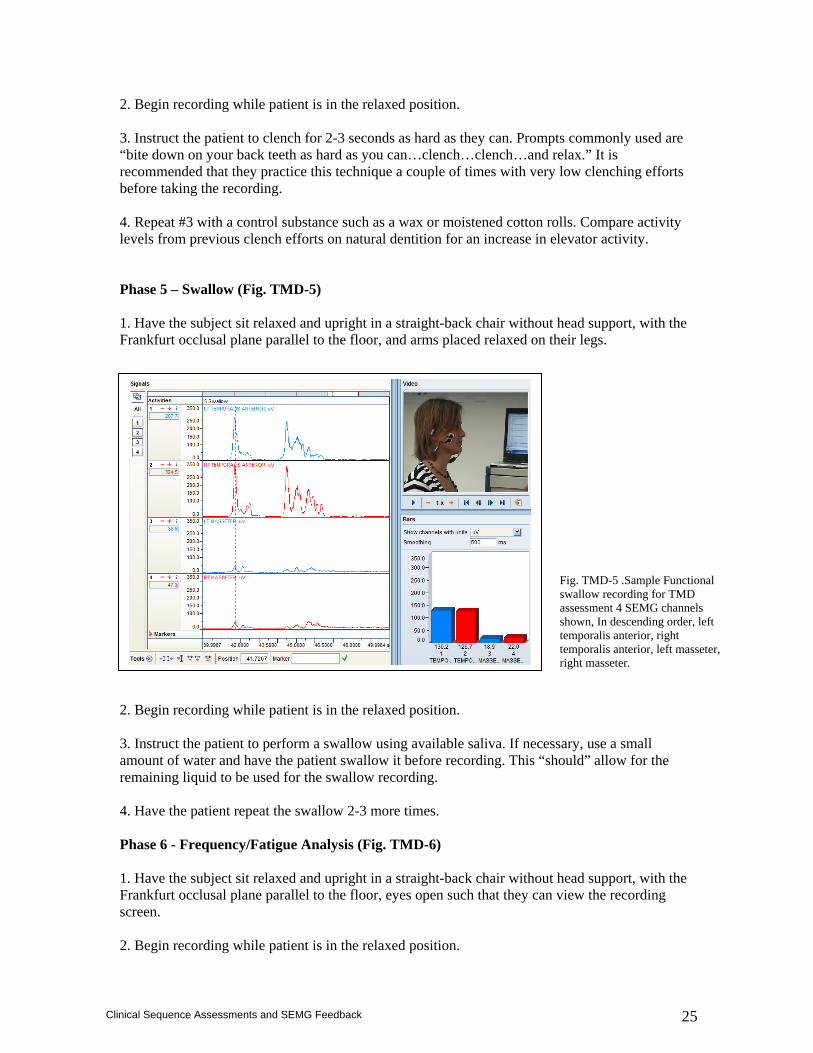
2. Begin recording while patient is in the relaxed position. 3. Instruct the patient to clench for 2-3 seconds as hard as they can. Prompts commonly used are “bite down on your back teeth as hard as you can…clench…clench…and relax.” It is recommended that they practice this technique a couple of times with very low clenching efforts before taking the recording. 4. Repeat #3 with a control substance such as a wax or moistened cotton rolls. Compare activity levels from previous clench efforts on natural dentition for an increase in elevator activity. Phase 5 – Swallow (Fig. TMD-5) 1. Have the subject sit relaxed and upright in a straight-back chair without head support, with the Frankfurt occlusal plane parallel to the floor, and arms placed relaxed on their legs. 2. Begin recording while patient is in the relaxed position. 3. Instruct the patient to perform a swallow using available saliva. If necessary, use a small amount of water and have the patient swallow it before recording. This “should” allow for the remaining liquid to be used for the swallow recording. 4. Have the patient repeat the swallow 2-3 more times. Phase 6 - Frequency/Fatigue Analysis (Fig. TMD-6) 1. Have the subject sit relaxed and upright in a straight-back chair without head support, with the Frankfurt occlusal plane parallel to the floor, eyes open such that they can view the recording screen. 2. Begin recording while patient is in the relaxed position.
Fig. TMD-5 .Sample Functional swallow recording for TMD assessment 4 SEMG channels shown, In descending order, left temporalis anterior, right temporalis anterior, left masseter, right masseter.
26
Clinical Sequence Assessments and SEMG Feedback
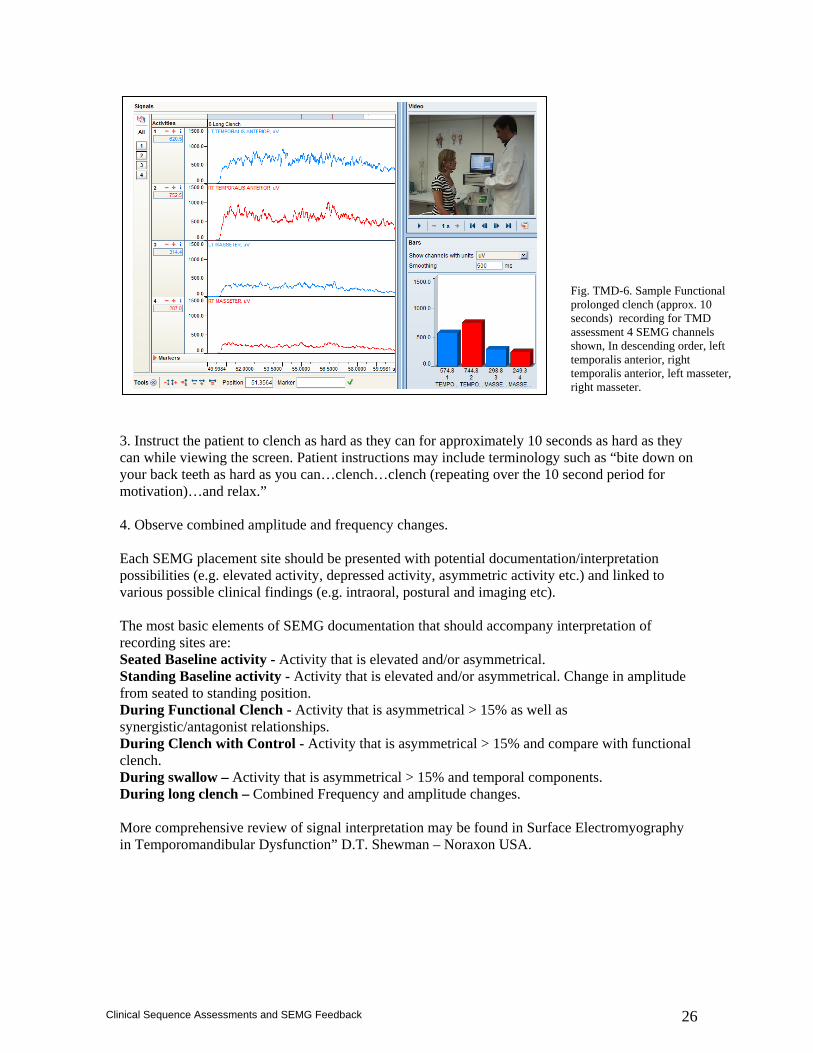
3. Instruct the patient to clench as hard as they can for approximately 10 seconds as hard as they can while viewing the screen. Patient instructions may include terminology such as “bite down on your back teeth as hard as you can…clench…clench (repeating over the 10 second period for motivation)…and relax.” 4. Observe combined amplitude and frequency changes.
Each SEMG placement site should be presented with potential documentation/interpretation possibilities (e.g. elevated activity, depressed activity, asymmetric activity etc.) and linked to various possible clinical findings (e.g. intraoral, postural and imaging etc). The most basic elements of SEMG documentation that should accompany interpretation of recording sites are: Seated Baseline activity - Activity that is elevated and/or asymmetrical. Standing Baseline activity - Activity that is elevated and/or asymmetrical. Change in amplitude from seated to standing position. During Functional Clench - Activity that is asymmetrical > 15% as well as synergistic/antagonist relationships. During Clench with Control - Activity that is asymmetrical > 15% and compare with functional clench. During swallow – Activity that is asymmetrical > 15% and temporal components. During long clench – Combined Frequency and amplitude changes. More comprehensive review of signal interpretation may be found in Surface Electromyography in Temporomandibular Dysfunction” D.T. Shewman – Noraxon USA.
Fig. TMD-6. Sample Functional prolonged clench (approx. 10 seconds) recording for TMD assessment 4 SEMG channels shown, In descending order, left temporalis anterior, right temporalis anterior, left masseter, right masseter.
27
Clinical Sequence Assessments and SEMG Feedback
Sample TMD Sequence Assessment Comments
- RMAS moderately elevated - Asymmetry R>LMAS
No remarkable change
- TA>MAS bilaterally
- Change unremarkable relative to natural dentition
- Prolonged swallow - Unstable activity
- Chronic fatigue exhibited across all sites
28
Clinical Sequence Assessments and SEMG Feedback
Common SEMG Impairments
Muscle Imbalance Syndrome
Recording sites
Mandibular elevation/retrusion
Mandibular elevation/retrusion w/ rotation
Temporalis Anterior (TA)
Hyperactive Hyperactive relative to MA during clench. Hyperactive late lateral excursion.
Hyperactive/ Asymmetrical. Hyperactive relative to MA Asymmetrical during clench. Hyperactive late lateral excursion
Masseter (MA) Hyper/hypoactive at rest. Hypoactive relative to TA during clench. Hyperactive late lateral excursion
Hyper/hypoactive at rest. Hypoactive relative to TA Asymmetrical during clench. Hyperactive late lateral excursion
Suprahyoid /Digastric (DI)
Hyperactive Hyperactive/Asymmetrical
Sternocleidomastoid (SCM)
Hyper/hypoactive May be hyperactive during clench
Hyper/hypoactive Hyperactive/Asymmetrical during clench
Lateral Cervical Paraspinals (LC)
Hyperactive Hyperactive/Asymmetrical
Common SEMG Activity Presentations
SEMG Feedback training considerations
Downtrain TA, MA, DI, SCM, LC Uptrain MA during clench.
Downtrain TA, MA, DI, SCM, LC Uptrain MA (unilaterally) during clench.
29
Clinical Sequence Assessments and SEMG Feedback
TMD – SEMG Interpretation Checklist
Left Temporalis Anterior‐ LTA Right Temporalis Anterior – RTA Right Masseter – RMAS Left Masseter ‐ LMAS Asymmetrical – Asym
Baseline Standing Baseline
Clench Clench With Control
Swallow Long clench
Hyperactive
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
Hypoactive
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
Absent/Inhibited
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
Premature
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
Delayed
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
Prolonged
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
Curtailed
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
Continuous
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
Out of Phase
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
LTA __ RTA __ LMAS __ RMAS __ Asym __
30
Clinical Sequence Assessments and SEMG Feedback
References
1. Cannistraci AJ, Frtiz G. Dental applications of biofeedback. In Basmajian JV, ed. Biofeedback: Principles and Practice for Clinicians, 3rd ed. Baltimore, MD: Williams and Wilkins, 1989; 289-305.
2. Gervitz RN, Glaros AG, Hopper D, Schwartz MS. Temporomandibular disorders. In: Schwartz MS, ed. Biofeedback: A Practitioner’s Guide, 2nd ed. New York: Guilford Press; 1995;411-428.
3. Nicholson RA, Townsend DR, Gramling SE. Influence of a scheduled-waiting task on EMG reactivity and oral habits among facial pain patients and no-pain controls. Appl Psychophysiolo Biofeedback 24:235-247;1999.
4. Flor H, Schugens M, Birbaumer N. Discrimination of muscle tension in chronic pain patients and healthy controls. Biofeedback Self Regul. 17:165-177;1992.
5. Glaros AG. Awareness of physiological responding under stress and nonstress conditions in temporomandibular disorders. Biofeedback Self Regul. 21:261-272;1996.
6. Flor H, Furst M, Birbaumer N. Deficient discrimination of EMG levels and overestimation of perceived tension in chronic pain patients. Appl Psychophysiol Biofeedback. 1999 Mar;24(1):55-66.
7. Hijzen TH, Slanger JL, Van Houweligan HC. Subjective, clinical and EMG effects of biofeedback and splint treatment. J Oral rehabil. 13:529-539;1986.
8. Turk D, Hussein Z, Rudy T. Effects of intraoral appliance and biofeedback/stress management alone and in combination in treating temporomandibular disorders. J Prosthet Dent. 70:158-164;1993.
9. Angeles-Medina F, Nuno-Licona A, Alfaro-Moctezuma P, Osorno-Escareno C. Development and application of reflexodent in the quantitative functional ewvaluation of chewing control in patients with temporomandibular joint dysfunction and a control group. Arch Med Res. 31:197-201;2000.
10. Ferrario VF, Sforza C, Miani A Jr, D’Addona A, Barbini E. Electromyographic activity of human masticatory muscles in normal young people: statistical evaluation of reference values for clinical applications. J Oral Rehabil. 20:271-280;1993.
11. Harper RP, de Bruin H, Burcea I. Muscle activity during mandibular movements in normal and retrognathic subjects. J Oral Maxillofac Surg. 55:225-233;1997.
12. Hellestrand E, Hellsing G. Temporomandibular disorders: a pilot study of activation patterns and motor unit analysis of jaw muscles. Aust Prosthodont. 9:39-43;1995.
13. Jankelson RR. Neuromuscular Dental Diagnosis and Treatment. St. Louis: Ishiyaku EuroAmerica Publishers; 1990.
14. Lafreniere CM, Lamontague M, el-Saly R. The role of the lateral pterygoid muscles in TMJ disorders during static conditions. Cranio. 15:38-52;1997.
15. Lund JP, Windmer CG. An evaluation of the use of surface electromyography in the diagnosis, documentation, and treatment of dental patients. J Craniomandibular Disord Facial Oral Pain. 3:125-137; 1989.
16. Pinho JC, Caldas FM, Mora MJ, Santana-Penin U. Electromyographic activity in patients with temporomandibular disorders. J Oral Rehabil. 27:985-990;2000.
17. Yoshida K. The elctromyographic activity of the masticatory muscles during temporomandibular joint clicking. Schweiz Monatsschr Zahnmed. 105:24-29;1995.
18. Christensen LV, Kundinger KK . Activity index and isometric contraction velocity of human jaw muscles. J Oral Rehabil 1991 Nov;18(6):555-61
19. Yamaguchi, K. Satoh, K. Komatsu, K. Kojima, N. Inoue, K. Minowa & Y. Totsuka Electromyographic activity of the jaw-closing muscles during jaw opening - comparison of cases
of masseter muscle contracture and TMJ closed lock. J Oral Rehabil. 2002 Nov;29(11):1063-8. 20. Visser A, McCarroll RS, Oosting J, Naeije M Masticatory electromyographic activity in healthy
young adults and myogenous craniomandibular disorder patients. J Oral Rehabil 1994 Jan;21(1):67-76
21. Ferrario VF, Sforza C, Colombo A, Ciusa V. An electromyographic investigation of masticatory muscles symmetry in normo-occlusion subjects. J Oral Rehabil. 2000 Jan;27(1):33-40.
22. Abekura H, Kotani H, Tokuyama H, Hamada T. Asymmetry of masticatory muscle activity during intercuspal maximal clenching in healthy subjects and subjects with stomatognathic.dysfunction syndrome. J Oral Rehabil 1995 Sep;22(9):699-704
31
Clinical Sequence Assessments and SEMG Feedback
23. Naeije M, McCarroll RS, Weijs WA Electromyographic activity of the human masticatory muscles during submaximal clenching in the inter-cuspal position. J Oral Rehabil 1989 Jan;16(1):63-70
24. Céline Bodéré, Say Hack Téa, Marie Agnes Giroux-Metges and Alain Woda. Activity of masticatory muscles in subjects with different orofacial pain conditions. Pain Volume 116, Issues 1-2, July 2005, Pages 33-41.
25. Toslka P, Morris RW, Preiskel HW. Occulsal adjustment therapy for craniomandibular disorders: a clinical assessment by double-blind method. J Prosthet Dent. 68:957-964;1992.
26. Christiansen LV, Rassouli NM. Experimental occulsal interferences. J Oral Rehabil. 22:515-520; 1995.
27. Minagi S, Akamatsu Y, Matsunaga T, Sato T. Relationship between mandibular position and the coordination of masseter muscle activity during sleep in humans. J Oral Rehabil. 1998 Dec;25(12):902-7.
28. Haketa T, Baba K, Akishige S, Fueki K, Kino K, Ohyama T. Utility and validity of a new EMG-based bruxism detection system. Int J Prosthodont. 2003 Jul-Aug;16(4):422-8.
29. Piquero K, Sakurai K. A clinical diagnosis of diurnal (non-sleep) bruxism in denture wearers. J Oral Rehabil. 2000 Jun;27(6):473-82.
30. Kazuyoshi Baba, DDS, PhD/Tadasu Haketa, DDS, PhD/Yoshiyuki Sasaki, DDS, PhD/Takashi Ohyama, DDS, PhD/Glenn T. Clark, DDS, MS. Association Between Masseter Muscle Activity Levels Recorded During Sleep and Signs and Symptoms of Temporomandibular Disorders in Healthy Young Adults. J Orofac Pain 2005;19:226–231.
31. Minagi S, Akamatsu Y, Matsunaga T, Sato T. Relationship between mandibular position and the coordination of master muscle activity during sleep in humans. J Oral Rehabil. 25:902-907;1998.
32. Gay T, Maton B, Rendell J, Majourau A. Characteristics of muscle fatigue in patients with myofascial pain-dysfunction syndrome. Arch Oral Biol. 39:847-852;1994.
33. Palla S, Ash MM: Effect of the bite force on the power spectrum of the surface electromyogram of human jaw muscles. Arch Oral Biol 1981; 26:287-295.
34. Lindstrom I, Hellsing G: Masseter muscle fatigue in man objectively quantified by analysis of myo-electric signals. Arch Oral Biol 1983;28:297-301.
35. Eble OS, Jonas IE, Kappert HF. Transcutaneous electrical nerve stimulation (TENS): its short-term and long-term effects on the masticatory muscles. J Orofac Orthop 2000;61(2):100-11.
36. Thomas NR: Utilization of Electromyopgraphic Spectral Analysis in the Diagnosis and Treatment of Craniomandibular-Dysfunction. In Hickman D (ed), Neuromuscular Dentistry: The Next Millenium Anthology V, Seattle: International College of Cranio-Mandibular Orthopedics, 1999.
37. Frucht S, Jonas I, Kappert HF. Muscle relaxation by transcutaneous electric nerve stimulation (TENS) in bruxism. An electromyographic study. Fortschr Kieferorthop. 1995 Sep;56(5):245-53.
38. Palazzi C, Miralles R, Soto MA, et al. Body position effects on EMG activity of sternocleidomastoid and master muscles in patients with myogenic cranio-cervical-mandibular dysfunction. Cranio. 14:200-209;1996.
39. Zuniga C, Miralles R, Mena B, et al. Influence of variation in jaw posture on sternocleidomastoid and trapezius Electromyographic activity. Cranio 199513:157-162;1995.
40. J Oral Rehabil 1999 Nov;26(11):865-76 Electrognathographic and electromyographic observations on jaw depression during neck extension. McKay DC, Christensen LV.
41. Santander H, Miralles R, Jimenez A, Zuniga C, Rocabado M, Moya H. Influence of stabilization occlusal splint on craniocervical relationships. Part II: Electromyographic analysis. Cranio 1994 Oct;12(4):227-33.
42. Eriksson PO, Zafar H, Nordh E. Concomitant mandibular and head-neck movements during jaw opening-closing in man. Oral Rehabil 1998 Nov;25(11):859-70.
43. Ferrario VF, Sforza C, Dellavia C, Tartaglia GM. Evidence of an influence of asymmetrical occlusal interferences on the activity of the sternocleidomastoid muscle. J Oral Rehabil. 2003 Jan;30(1):34-40.
44. Yamasawa H. Electromyographic power spectral analysis of sternocleidomastoid muscle during sustained voluntary clenching. Kokubyo Gakkai Zasshi. 1998 Mar;65(1):84-92.
45. de Wijer A, Steenks MH, de Leew JR Bosman F, Helders PJ. Symptoms of the cervical spine in temporomandibular and cervical spine disorders. J Oral Rehabil 1996 Nov;23(11):742-50.
46. Crider AB, Glaros AG. A meta-analysis of EMG biofeedback treatment of temporomandibular disorders. J Orofac Pain. 1999 Winter;13(1):29-37.

32
Clinical Sequence Assessments and SEMG Feedback
47. Erlandson PM Jr, Poppen R. Electromyographic biofeedback and rest position training of masticatory muscles in myofascial pain-dysfunction patients. J Prosthet Dent. 1989 Sep;62(3):335-8.
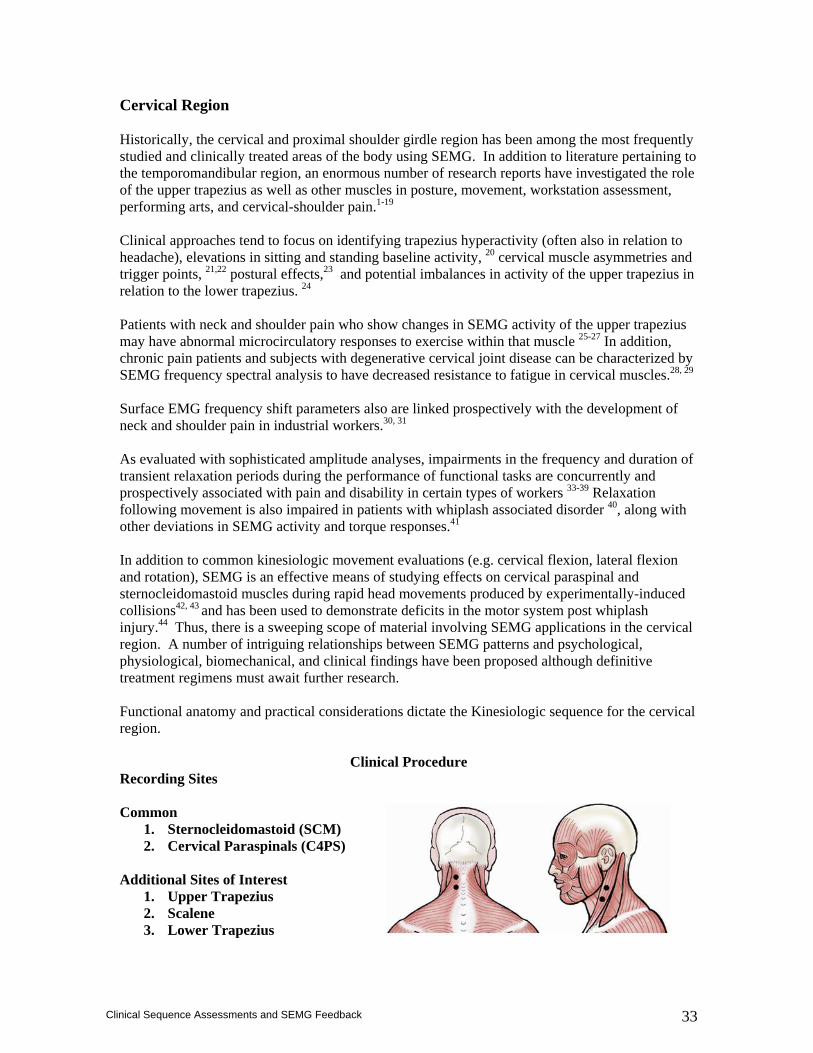
33
Clinical Sequence Assessments and SEMG Feedback
Cervical Region Historically, the cervical and proximal shoulder girdle region has been among the most frequently studied and clinically treated areas of the body using SEMG. In addition to literature pertaining to the temporomandibular region, an enormous number of research reports have investigated the role of the upper trapezius as well as other muscles in posture, movement, workstation assessment, performing arts, and cervical-shoulder pain.1-19 Clinical approaches tend to focus on identifying trapezius hyperactivity (often also in relation to headache), elevations in sitting and standing baseline activity, 20 cervical muscle asymmetries and trigger points, 21,22 postural effects,23 and potential imbalances in activity of the upper trapezius in relation to the lower trapezius. 24 Patients with neck and shoulder pain who show changes in SEMG activity of the upper trapezius may have abnormal microcirculatory responses to exercise within that muscle 25-27 In addition, chronic pain patients and subjects with degenerative cervical joint disease can be characterized by SEMG frequency spectral analysis to have decreased resistance to fatigue in cervical muscles.28, 29 Surface EMG frequency shift parameters also are linked prospectively with the development of neck and shoulder pain in industrial workers.30, 31
As evaluated with sophisticated amplitude analyses, impairments in the frequency and duration of transient relaxation periods during the performance of functional tasks are concurrently and prospectively associated with pain and disability in certain types of workers 33-39 Relaxation following movement is also impaired in patients with whiplash associated disorder 40, along with other deviations in SEMG activity and torque responses.41 In addition to common kinesiologic movement evaluations (e.g. cervical flexion, lateral flexion and rotation), SEMG is an effective means of studying effects on cervical paraspinal and sternocleidomastoid muscles during rapid head movements produced by experimentally-induced collisions42, 43 and has been used to demonstrate deficits in the motor system post whiplash injury.44 Thus, there is a sweeping scope of material involving SEMG applications in the cervical region. A number of intriguing relationships between SEMG patterns and psychological, physiological, biomechanical, and clinical findings have been proposed although definitive treatment regimens must await further research. Functional anatomy and practical considerations dictate the Kinesiologic sequence for the cervical region.
Clinical Procedure Recording Sites Common
1. Sternocleidomastoid (SCM) 2. Cervical Paraspinals (C4PS)
Additional Sites of Interest
1. Upper Trapezius 2. Scalene 3. Lower Trapezius
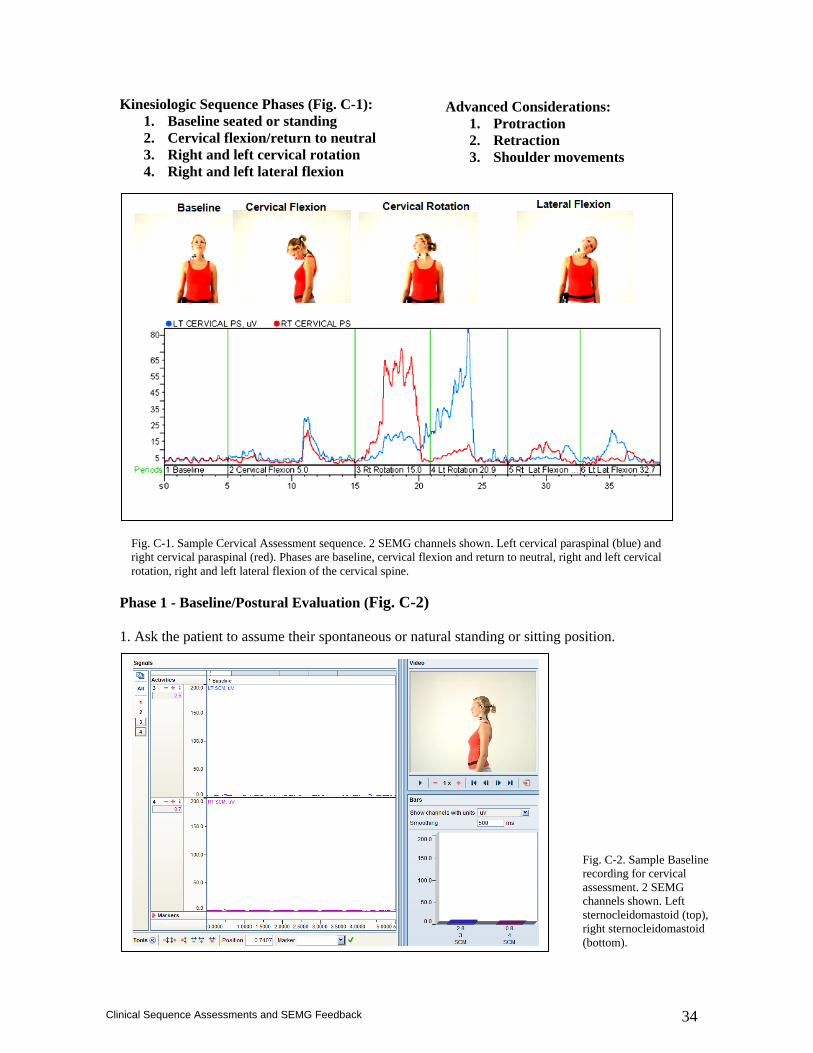
34
Clinical Sequence Assessments and SEMG Feedback
Kinesiologic Sequence Phases (Fig. C-1): 1. Baseline seated or standing 2. Cervical flexion/return to neutral 3. Right and left cervical rotation 4. Right and left lateral flexion
Phase 1 - Baseline/Postural Evaluation (Fig. C-2) 1. Ask the patient to assume their spontaneous or natural standing or sitting position.
Advanced Considerations: 1. Protraction 2. Retraction 3. Shoulder movements
Fig. C-1. Sample Cervical Assessment sequence. 2 SEMG channels shown. Left cervical paraspinal (blue) and right cervical paraspinal (red). Phases are baseline, cervical flexion and return to neutral, right and left cervical rotation, right and left lateral flexion of the cervical spine.
Fig. C-2. Sample Baseline recording for cervical assessment. 2 SEMG channels shown. Left sternocleidomastoid (top), right sternocleidomastoid (bottom).
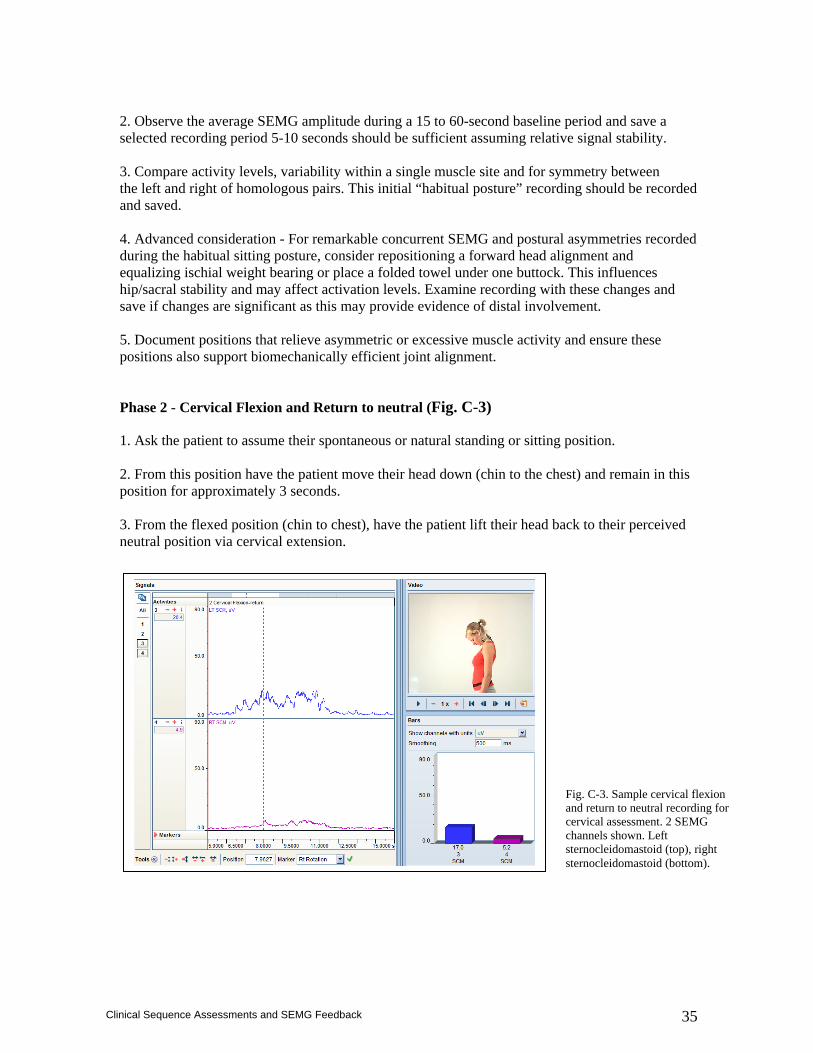
35
Clinical Sequence Assessments and SEMG Feedback
2. Observe the average SEMG amplitude during a 15 to 60-second baseline period and save a selected recording period 5-10 seconds should be sufficient assuming relative signal stability. 3. Compare activity levels, variability within a single muscle site and for symmetry between the left and right of homologous pairs. This initial “habitual posture” recording should be recorded and saved. 4. Advanced consideration - For remarkable concurrent SEMG and postural asymmetries recorded during the habitual sitting posture, consider repositioning a forward head alignment and equalizing ischial weight bearing or place a folded towel under one buttock. This influences hip/sacral stability and may affect activation levels. Examine recording with these changes and save if changes are significant as this may provide evidence of distal involvement. 5. Document positions that relieve asymmetric or excessive muscle activity and ensure these positions also support biomechanically efficient joint alignment.
Phase 2 - Cervical Flexion and Return to neutral (Fig. C-3)
1. Ask the patient to assume their spontaneous or natural standing or sitting position. 2. From this position have the patient move their head down (chin to the chest) and remain in this position for approximately 3 seconds. 3. From the flexed position (chin to chest), have the patient lift their head back to their perceived neutral position via cervical extension.
Fig. C-3. Sample cervical flexion and return to neutral recording for cervical assessment. 2 SEMG channels shown. Left sternocleidomastoid (top), right sternocleidomastoid (bottom).
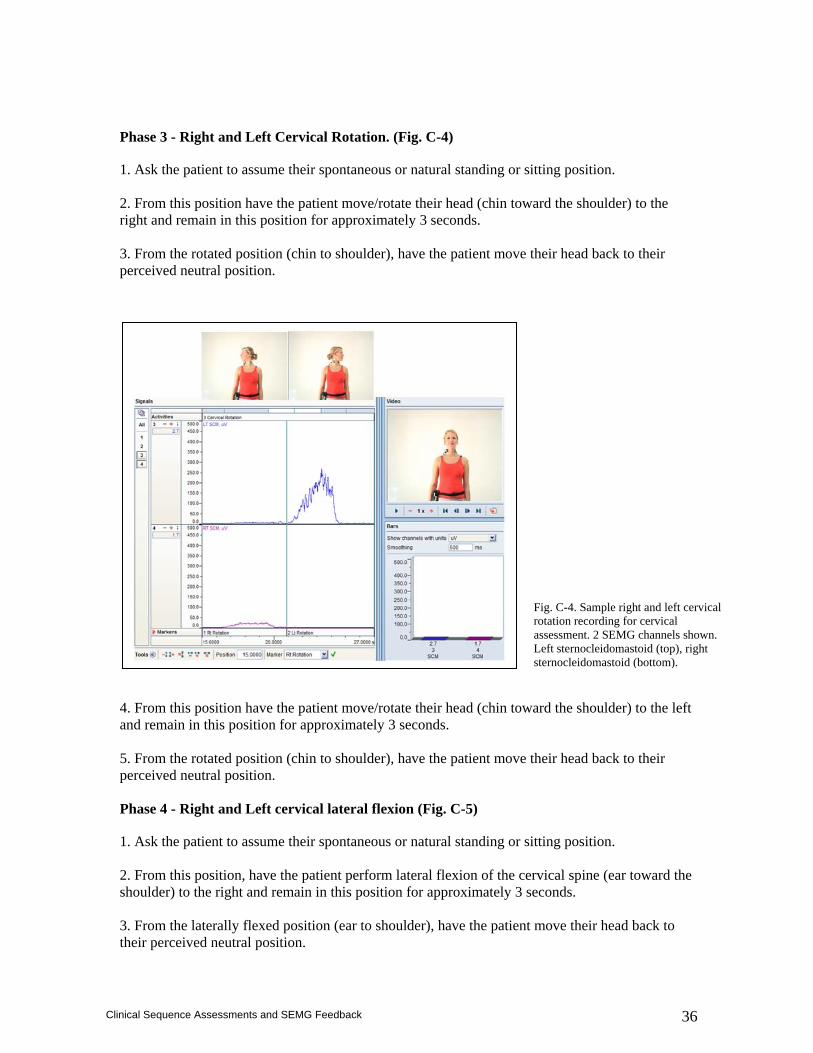
36
Clinical Sequence Assessments and SEMG Feedback
Phase 3 - Right and Left Cervical Rotation. (Fig. C-4)
1. Ask the patient to assume their spontaneous or natural standing or sitting position. 2. From this position have the patient move/rotate their head (chin toward the shoulder) to the right and remain in this position for approximately 3 seconds. 3. From the rotated position (chin to shoulder), have the patient move their head back to their perceived neutral position. 4. From this position have the patient move/rotate their head (chin toward the shoulder) to the left and remain in this position for approximately 3 seconds. 5. From the rotated position (chin to shoulder), have the patient move their head back to their perceived neutral position. Phase 4 - Right and Left cervical lateral flexion (Fig. C-5)
1. Ask the patient to assume their spontaneous or natural standing or sitting position. 2. From this position, have the patient perform lateral flexion of the cervical spine (ear toward the shoulder) to the right and remain in this position for approximately 3 seconds. 3. From the laterally flexed position (ear to shoulder), have the patient move their head back to their perceived neutral position.
Fig. C-4. Sample right and left cervical rotation recording for cervical assessment. 2 SEMG channels shown. Left sternocleidomastoid (top), right sternocleidomastoid (bottom).
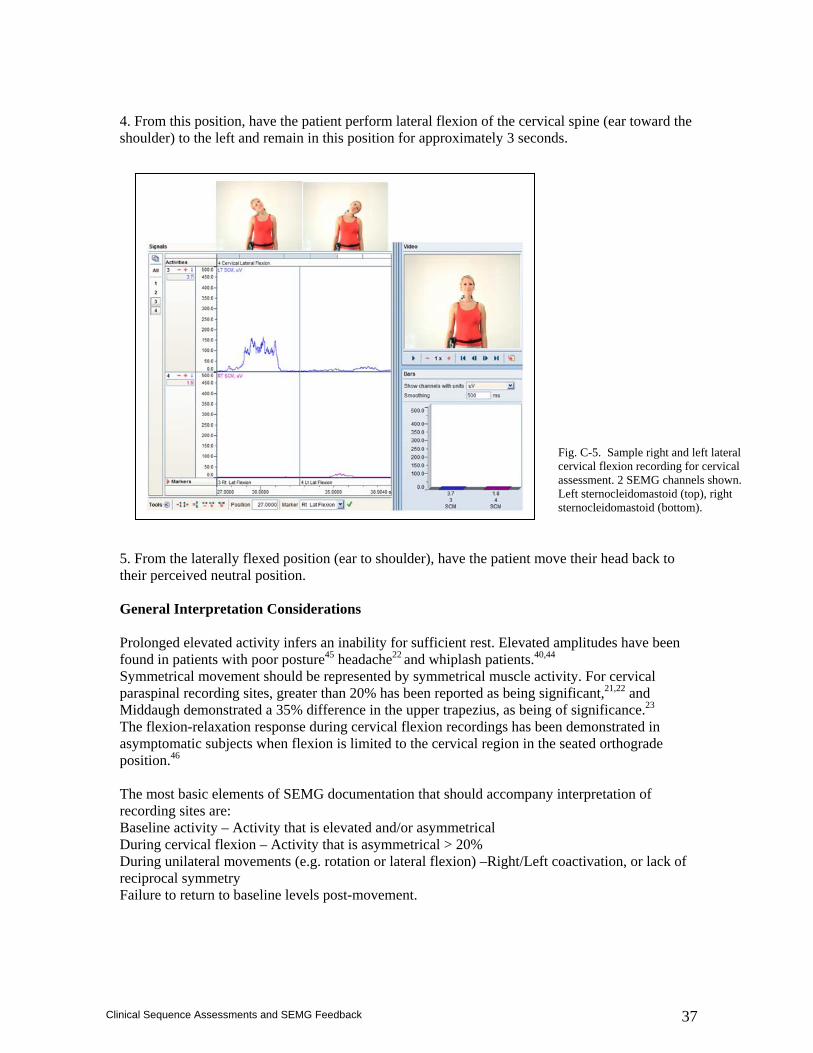
37
Clinical Sequence Assessments and SEMG Feedback
4. From this position, have the patient perform lateral flexion of the cervical spine (ear toward the shoulder) to the left and remain in this position for approximately 3 seconds. 5. From the laterally flexed position (ear to shoulder), have the patient move their head back to their perceived neutral position. General Interpretation Considerations Prolonged elevated activity infers an inability for sufficient rest. Elevated amplitudes have been found in patients with poor posture45 headache22 and whiplash patients.40,44 Symmetrical movement should be represented by symmetrical muscle activity. For cervical paraspinal recording sites, greater than 20% has been reported as being significant,21,22 and Middaugh demonstrated a 35% difference in the upper trapezius, as being of significance.23 The flexion-relaxation response during cervical flexion recordings has been demonstrated in asymptomatic subjects when flexion is limited to the cervical region in the seated orthograde position.46 The most basic elements of SEMG documentation that should accompany interpretation of recording sites are: Baseline activity – Activity that is elevated and/or asymmetrical During cervical flexion – Activity that is asymmetrical > 20% During unilateral movements (e.g. rotation or lateral flexion) –Right/Left coactivation, or lack of reciprocal symmetry Failure to return to baseline levels post-movement.
Fig. C-5. Sample right and left lateral cervical flexion recording for cervical assessment. 2 SEMG channels shown. Left sternocleidomastoid (top), right sternocleidomastoid (bottom).
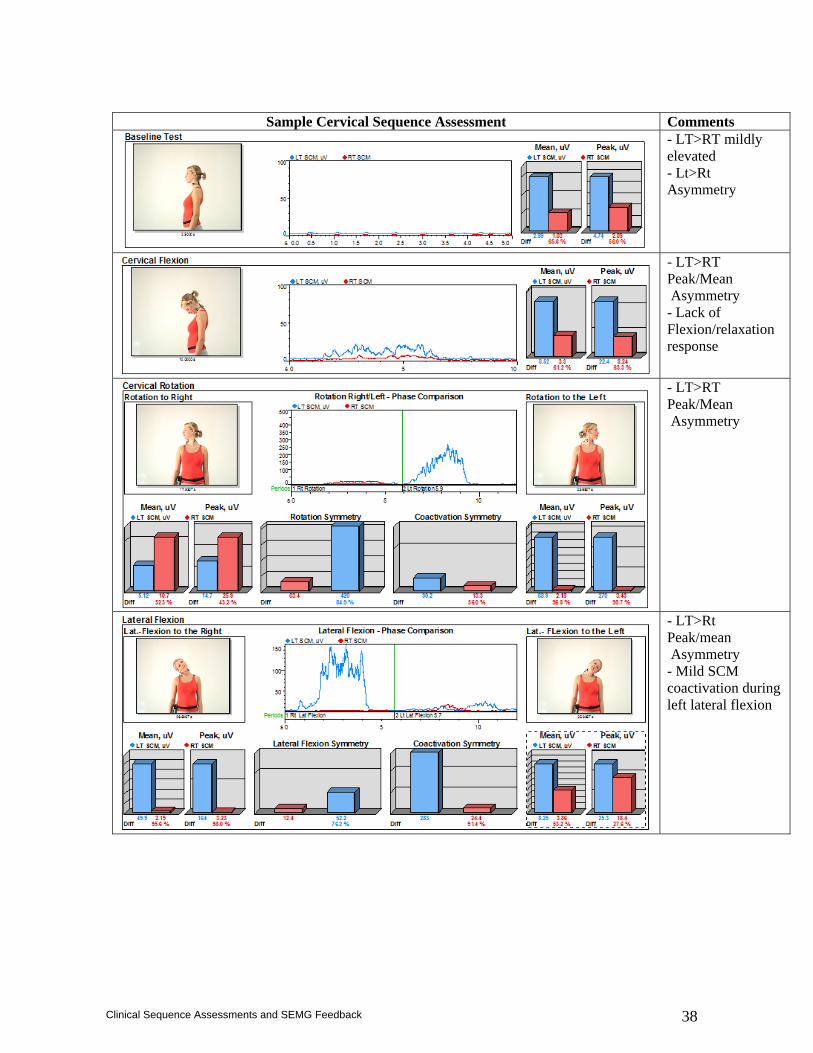
38
Clinical Sequence Assessments and SEMG Feedback
Sample Cervical Sequence Assessment Comments
- LT>RT mildly elevated - Lt>Rt Asymmetry
- LT>RT Peak/Mean Asymmetry - Lack of Flexion/relaxation response
- LT>RT Peak/Mean Asymmetry
- LT>Rt Peak/mean Asymmetry - Mild SCM coactivation during left lateral flexion
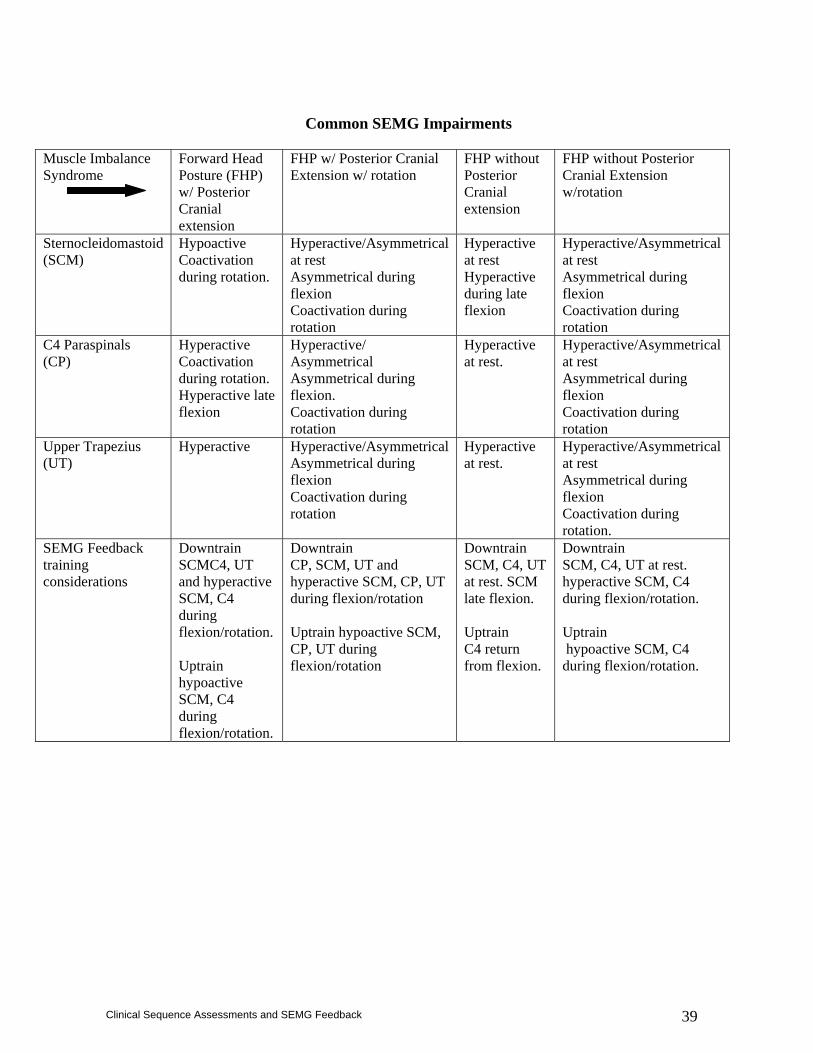
39
Clinical Sequence Assessments and SEMG Feedback
Common SEMG Impairments
Muscle Imbalance Syndrome
Forward Head Posture (FHP) w/ Posterior Cranial extension
FHP w/ Posterior Cranial Extension w/ rotation
FHP without Posterior Cranial extension
FHP without Posterior Cranial Extension w/rotation
Sternocleidomastoid (SCM)
Hypoactive Coactivation during rotation.
Hyperactive/Asymmetrical at rest Asymmetrical during flexion Coactivation during rotation
Hyperactive at rest Hyperactive during late flexion
Hyperactive/Asymmetrical at rest Asymmetrical during flexion Coactivation during rotation
C4 Paraspinals (CP)
Hyperactive Coactivation during rotation. Hyperactive late flexion
Hyperactive/ Asymmetrical Asymmetrical during flexion. Coactivation during rotation
Hyperactive at rest.
Hyperactive/Asymmetrical at rest Asymmetrical during flexion Coactivation during rotation
Upper Trapezius (UT)
Hyperactive
Hyperactive/Asymmetrical Asymmetrical during flexion Coactivation during rotation
Hyperactive at rest.
Hyperactive/Asymmetrical at rest Asymmetrical during flexion Coactivation during rotation.
SEMG Feedback training considerations
Downtrain SCMC4, UT and hyperactive SCM, C4 during flexion/rotation. Uptrain hypoactive SCM, C4 during flexion/rotation.
Downtrain CP, SCM, UT and hyperactive SCM, CP, UT during flexion/rotation Uptrain hypoactive SCM, CP, UT during flexion/rotation
Downtrain SCM, C4, UT at rest. SCM late flexion. Uptrain C4 return from flexion.
Downtrain SCM, C4, UT at rest. hyperactive SCM, C4 during flexion/rotation. Uptrain hypoactive SCM, C4 during flexion/rotation.
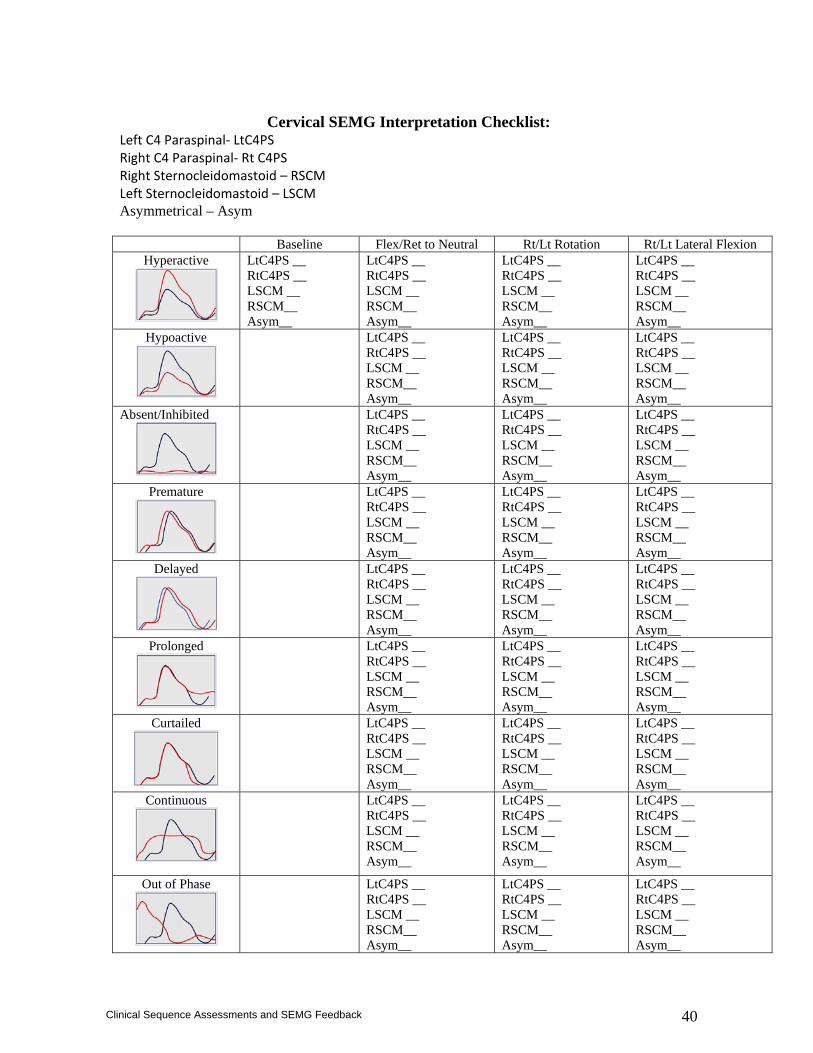
40
Clinical Sequence Assessments and SEMG Feedback
Cervical SEMG Interpretation Checklist:
Left C4 Paraspinal‐ LtC4PS Right C4 Paraspinal‐ Rt C4PS Right Sternocleidomastoid – RSCM Left Sternocleidomastoid – LSCM Asymmetrical – Asym Baseline Flex/Ret to Neutral Rt/Lt Rotation Rt/Lt Lateral Flexion
Hyperactive
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Hypoactive
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Absent/Inhibited
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Premature
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Delayed
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Prolonged
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Curtailed
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Continuous
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
Out of Phase
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
LtC4PS __ RtC4PS __ LSCM __ RSCM__ Asym__
41
Clinical Sequence Assessments and SEMG Feedback
References
1. Basmajian JV, De Luca CJ. Muscles Alive: Their Functions Revealed by Electromyography, 5th ed. Baltimore, MD: Williams & Wilkins; 1985.
2. Chan RF, Chow C, Lee GP, To L, Tsang XY, Yeung SS, Yeung EW. Self-perceived exertion level and objective evaluation of neuromuscular fatigue in a training session of orchestral violin players. Appl Ergon. 31:335-41;2000.
3. Elert J, Karlsson S, Gerdle B. One-year reproducibility and stability of the signal amplitude ratio and other variables of the electromyogram: test-retest of a shoulder forward flexion test in female workers with neck and shoulder problems. Clin Physiol.18:529-538;1998.
4. Enwemeka C, Bonet I, Jayanti A, et al. Postural correction in persons with neck pain, II: integrated electromyography of the upper trapezius in three simulated neck positions. J Orthop Sports Phys Ther. 8:240-242;1986.
5. Hagberg M. Occupational musculoskeletal stress disorders of the neck and shoulder: a review of possible pathophysiology. Int Arch Occup Environ Health. 53:269-278;1984.
6. Johnsson B. Measurement and evaluation of local muscular strain in the shoulder during constrained work. J Hum Ergol (Tokyo). 11:73-88;1982.
7. Kleine BU, Schumann NP, Bradl I, Grieshaber R, Scholle HC. Surface EMG of shoulder and back muscles and postural analysis in secretaries typing at visual display units. Int Arch Pccup Environ Health. 72:387-394;1999.
8. Lannersten L, Harms-Ringdahl K. Neck and shoulder muscle activity during work with different cash register systems. Ergonomics. 33:49-65;1990.
9. Lowe BD, Wurzelbacher SJ, Shulman SA, Hudock SD. Electromyographic and discomfort analysis of confined-space shipyard welding processes. Appl Ergon. 32:255-269;2001.
10. Madeleine P, Lundager B, Voight M, Arendt-Nielsen L. Shoulder muscle co-ordination during chronic and acute experimental neck-shoulder pain. An occupational study. Eur J Appl Physiol Occup Physiol. 79:127-140;1999.
11. Milerad E, Ericson MO, Nisell R, Kilbom A. An Electromyographic study of dental work. Ergonomics. 34:953-962;1991.
12. Rissen D, Melin B, Sandsjo L, Dohns I, Lundberg U. Surface EMG and psychophysiogical stress reactions in women during repetitive work. Eur J Appl Physiol. 83:215-220;2000.
13. Roe C, Bjorklund RA, Knardahl S, Waersted M, Vollstad NK. Cognitive performance and muscle activation in workers with chronic shoulder myalgia. Ergonomics. 44:1-16;2001.
14. Roman-Liu D, Tokarski T, Kaminska J. Assessment of the musculoskeletal load of the trapezius and deltoid muscles during hand activity. Int J Occup Saf Ergon. 7:179-193;2001.
15. Schuldt K. On neck muscle activity and load reduction in sitting postures: an Electromyographic and biomechanical study with applications in ergonomics and rehabilitation. Scand J Rehabil Med Suppl. 19:1-49;1988.
16. Schuldt K, Ekholm J, Marms-Ringdahl K, et al. Effects of arm support or suspension on neck and shoulder muscle activity during sedentary work. Scand J Rehabil Med. 19:77-84;1987.
17. Vasseljen O, Johansen B, Westgaard R. The effect of pain reduction on perceived tension and EMG recorded trapezius muscle activity in workers with shoulder and neck pain. Scand J Rehabil Med. 27:243-252;1995.
18. Vasseljen O Jr, Westgaard RH. Arm and trunk posture during work in relation to shoulder and neck pain and trapezius activity. Clin Biomech (Bristol, Avon)12:22-31;1997.
19. Villanueva MB, Jonai H, Sotoyama M, Hisanaga N, Takeuchi Y, Saito S. Sitting posture and neck and shoulder muscle activities at different screen height settings of the visual display terminal. Ind Health. 35:330-336;1997.
20. Cram JR, Kasman GS. An Introduction to Surface Electromyography. Gaithersburg, MD: Aspen Publishers, 1998.
21. Donaldson S, Donaldson M. Multi-channel EMG assessment and treatment techniques. In: Cram JR, ed. Clinical EMG for Surface Recordings. Vol 2. Nevada City, CA: Clinical Resources. 1990;143-173.
22. Donaldson CCS, Skubick DL, Clasby RG, Cram J. The evaluation of trigger point activity using dynamic EMG techniques. Am J Pain Mange. 4:118-122;1994.
42
Clinical Sequence Assessments and SEMG Feedback
23. Middaugh SJ, Kee WG, Nicholson JA. Muscle overuse and posture as factors in the development and maintenance of chronic musculoskeletal pain. In: Greziak RC, Ciccone DS, eds. Psychological Vulnerability to Chronic Pain. New York: Springer Publishing Co; 1994;55-89.
24. Taylor W. Dynamic EMG biofeedback in assessment and treatment using a neuromuscular re-education model. In: Cram JR, ed. Clinical EMG for Surface Recordings. Vol 2. Nevada City, CA: Clinical Resources. 1990;175-196.
25. Larsson R, Oberg PA, Larsson SE. Changes of trapezius muscle blood flow and electromyography in chronic neck pain due to trapezius myalgia. Pain. 79:45-50;1999.
26. Larsson SE, Alund M, Cai H, Oberg PA. Chronic pain after soft-tissue injury of the cervical spine: trapezius muscle blood flow and electromyography at static loads and fatigue. Pain. 1994 May;57(2):173-80.
27. Lofgren H, Larsson R, Larsson SE. Outcome of surgery for cervical radiculopathy evaluated by determination of trapezius muscle microcirculation and electromyography. Eur J Pain. 2001;5(1):39-48.
28. Gogia P, Sabbahi M. Median frequency of the myoelectric signal in cervical paraspinal muscles. Arch Phys Med Rehabil. 71:408-414;1990.
29. Electromyographic analysis of neck muscle fatigue in patients with osteoarthritis of the cervical spine. Spine. 1994 Mar 1;19(5):502-6. Gogia PP, Sabbahi MA.
30. Falla D, Rainoldi A, Merletti R, Jull G. Myoelectric manifestations of sternocleidomastoid and anterior scalene muscle fatigue in chronic neck pain patients. Clin Neurophysiol. 2003 Mar;114(3):488-95.
31. Lundblad I, Elert J, Gerdle B. Worsening of neck and shoulder complaints in humans are correlated with frequency parameters of the electromyogram recorded 1-year earlier. Eur J Appl Physiol Occup Physiol. 79:7-16;1998.
32. Falla D, Rainoldi A, Merletti R, Jull G. Myoelectric manifestations of sternocleidomastoid and anterior scalene muscle fatigue in chronic neck pain patients. Clin Neurophysiol. 2003 Mar;114(3):488-95.
33. Hansson GA, Nordander C, Asterland P, et al. Sensitivity of trapezius electromyography to differences between work tasks – influence of gap definition and normalization methods. J Electromyogr Kinesiol. 10:103-115;2000.
34. Larsson B, Bjork J, Elert J, Gerdle B. Mechanical performance and electromyography during repeated maximal isokinetic shoulder forward flexions in female cleaners with and without myalgia of the trapezius muscle and in healthy controls. Eur J Appl Physiol. 83:257-267;2000.
35. Sundelin G, Hagberg M. The effects of different pause types on neck and shoulder EMG activity during VDU work. Ergonomics. 39:527-537;1989.
36. Veirested KB. Sustained muscle tension as a risk factor in trapezius myalgia. In: Nielsen R, Jorgensen K, eds. Advances in Industrial Ergonomics and Safety. London: Taylor & Francis; 1993;15-19.
37. Veiersted KB, Westgaard RH, Andersen P. Electromyographic evaluation of muscular work pattern as a predictor of trapezius myalgia. Scand J Work Environ Health. 19:284-290;1993.
38. Veiersted KB, Westgaard RH, Andersen P. Pattern of muscle activity during stereotyped work and its relation to muscle pain. Int Arch Ocup Environ Health. 62:31-41;1990.
39. Winkel J, Westgaard RH. Occupational and individual risk factors for shoulder-neck complaints, part II: the scientific basis (literature review) for the guide. Int J Indust Ergon. 10:85-104;1992.
40. Nederhand MJ, Ijzerman MJ, Hermans HJ, Baten CP, Zilvold G. Cervical muscle dysfunction in the chronic whiplash associated disorder grade II (WAD-II). Spine. 25:1938-1943;2000.
41. Kendell Elert J, Larsson B, Mansson B, Gerdle B. Chronic pain and difficulty relaxing postural muscles in patients with fibromyalgia and chronic whiplash associated disorders. J Rheumatol. 28:1361-1368;2001.
42. Brault JR, Siegmund GP, Wheeler JB. Cervical muscle response during whiplash: evidence of a lengthening muscle contraction. Clin Biomech. 15:426-435;2000.
43. Siegmund GP, Sanderson DJ, Myers BS, Inglis JT. Awareness affects the response of human subjects exposed to a single whiplash-like perturbation. Spine. 2003 Apr 1;28(7):671-9.
44. Sterling M, Jull G, Vicenzino B, Kenardy J, Darnell R. Development of motor system dysfunction following whiplash injury. Pain. 2003 May;103(1-2):65-73.
43
Clinical Sequence Assessments and SEMG Feedback
45. McLean L. The effect of postural correction on muscle activation amplitudes recorded from the cervicobrachial region. J Electromyogr Kinesiol. 2005 Dec;15(6):527-35.
46. Meyer JJ, Berk RJ, Anderson AV. Recruitment patterns in the cervical paraspinal muscles during cervical forward flexion: evidence of cervical flexion-relaxation. Electromyogr Clin Neurophysiol. 1993 Jun;33(4):217-23.

44
Clinical Sequence Assessments and SEMG Feedback
Shoulder Girdle Region The principles described for the temporomandibular and cervical regions in previous sections are also largely applicable to the shoulder girdle. These include issues related to postural alignment, conscious recognition of aberrant muscle activity states, and the production of interspersed rest during functional tasks range through the upper quadrant. Using surface as well as intramuscular fine wire recordings, EMG amplitude and frequency spectral methods have been reported extensively in the study of healthy experimental subjects, workers and athletes.1-15
Methodological considerations have also been addressed.16-18 Normalized dynamic activity patterns from healthy subjects19abnormal patterns from athletes with and without shoulder pain 20,21 have been investigated. SEMG has also been used to evaluate various therapeutic exercises for the shoulder in healthy subjects 22-28 to assist in determining training goals for specific sports29
and patients with shoulder pain.30 There have also been reports on the use of SEMG feedback training to treat posterior and anterior shoulder instability and subluxation. 33-35 More recently, SEMG has been used to evaluate alterations in recruitment patterns following fatiguing contractions and have been combined with sophisticated kinematic assessment systems to investigate the effects of scapular muscle fatigue 36,37 and scapular muscle imbalances associated with impingement syndrome.38 It seems apparent from the literature that changes in the relative recruitment levels of scapular muscles occur with fatigue and injury. An assumption that is often anecdotally stated 39 and gathering scientific validation is in relation to imbalance among the upper trapezius and lower trapezius. 40 Clinically, practitioners see cases of neck and shoulder pain of mixed etiology where the lower trapezius or serratus anterior appears hypoactive and the upper trapezius is hyperactive during shoulder and arm elevation maneuvers, but the precise functional role of the lower trapezius requires additional scientific clarification. Alterations in scapular kinematics clearly exist in some patients with painful shoulders that involve excessive vertical displacement of the scapula, and this pattern may be resolved easily with corrective movement feedback cues.41 Decreased activity from the serratus anterior during swimming and scaption movements has been associated with painful shoulders in experimental designs.42 Additional study combining surface and intramuscular electromyographic recordings with kinematic measurements are required to resolve lower trapezius issues which are technically daunting. Nevertheless, it may be recognized that use of SEMG for lower trapezius training is clinically popular, has intuitive appeal, and clinical experience has demonstrated positive outcomes. Given the current evidence and increasing understanding of muscle imbalance, clinicians should also direct attention to the lower fibers of the serratus anterior as a primary site for clinical evaluation.
Clinical Procedure Recording Sites Common:
1. Upper Trapezius (UTP) 2. Middle Trapezius/Interscapular (MTP) 3. Lower Trapezius/Interscapular (LTP) 4. Serratus Anterior (SER) 5. Infraspinatus (INF)
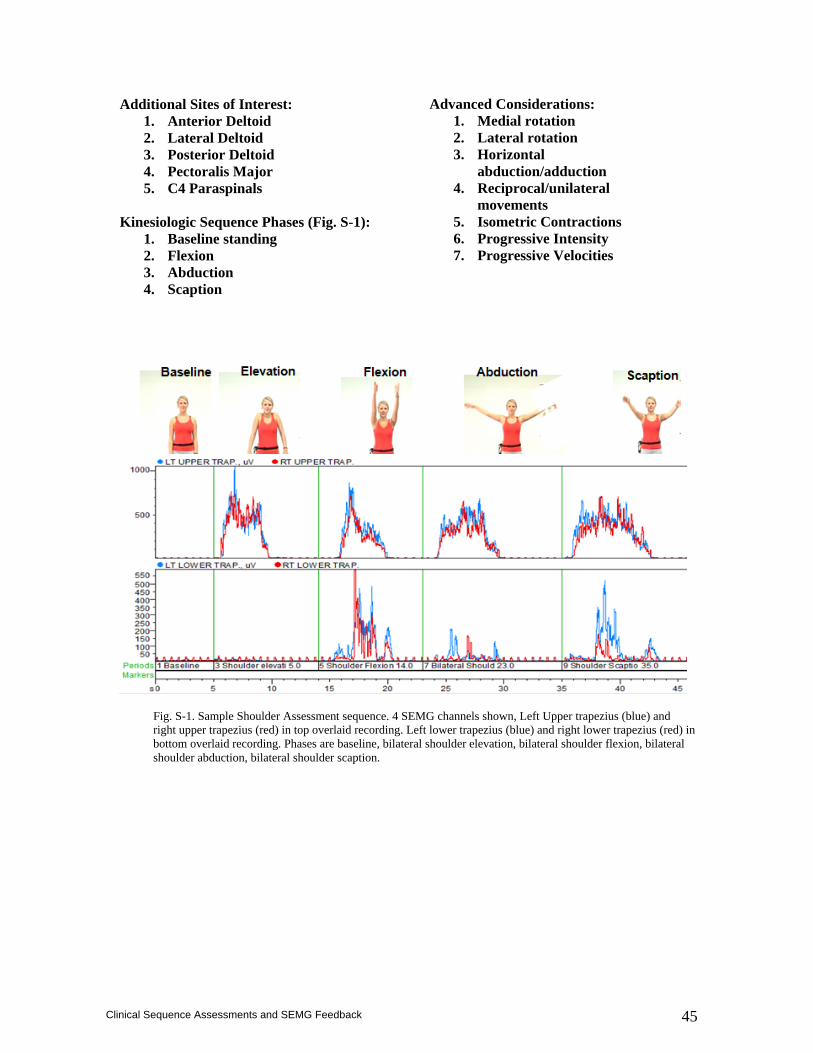
45
Clinical Sequence Assessments and SEMG Feedback
Additional Sites of Interest: 1. Anterior Deltoid 2. Lateral Deltoid 3. Posterior Deltoid 4. Pectoralis Major 5. C4 Paraspinals
Kinesiologic Sequence Phases (Fig. S-1):
1. Baseline standing 2. Flexion 3. Abduction 4. Scaption
Advanced Considerations: 1. Medial rotation 2. Lateral rotation 3. Horizontal
abduction/adduction 4. Reciprocal/unilateral
movements 5. Isometric Contractions 6. Progressive Intensity 7. Progressive Velocities
Fig. S-1. Sample Shoulder Assessment sequence. 4 SEMG channels shown, Left Upper trapezius (blue) and right upper trapezius (red) in top overlaid recording. Left lower trapezius (blue) and right lower trapezius (red) in bottom overlaid recording. Phases are baseline, bilateral shoulder elevation, bilateral shoulder flexion, bilateral shoulder abduction, bilateral shoulder scaption.
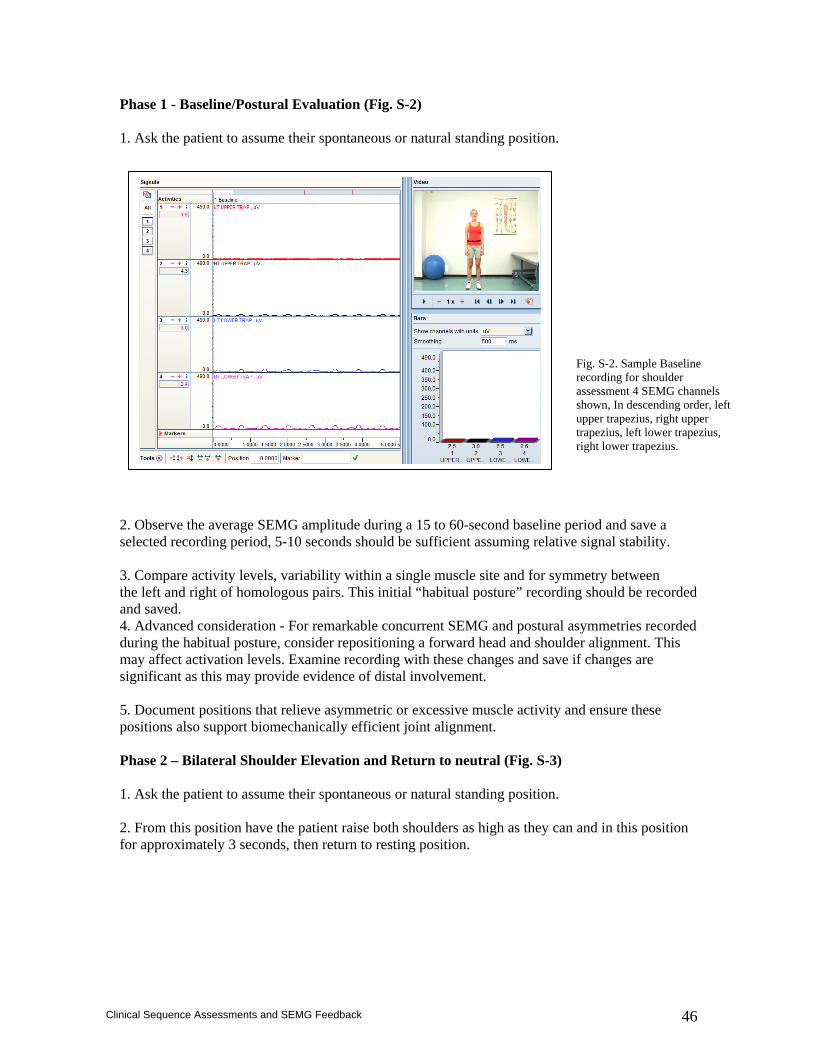
46
Clinical Sequence Assessments and SEMG Feedback
Phase 1 - Baseline/Postural Evaluation (Fig. S-2) 1. Ask the patient to assume their spontaneous or natural standing position. 2. Observe the average SEMG amplitude during a 15 to 60-second baseline period and save a selected recording period, 5-10 seconds should be sufficient assuming relative signal stability. 3. Compare activity levels, variability within a single muscle site and for symmetry between the left and right of homologous pairs. This initial “habitual posture” recording should be recorded and saved. 4. Advanced consideration - For remarkable concurrent SEMG and postural asymmetries recorded during the habitual posture, consider repositioning a forward head and shoulder alignment. This may affect activation levels. Examine recording with these changes and save if changes are significant as this may provide evidence of distal involvement. 5. Document positions that relieve asymmetric or excessive muscle activity and ensure these positions also support biomechanically efficient joint alignment. Phase 2 – Bilateral Shoulder Elevation and Return to neutral (Fig. S-3) 1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position have the patient raise both shoulders as high as they can and in this position for approximately 3 seconds, then return to resting position.
Fig. S-2. Sample Baseline recording for shoulder assessment 4 SEMG channels shown, In descending order, left upper trapezius, right upper trapezius, left lower trapezius, right lower trapezius.
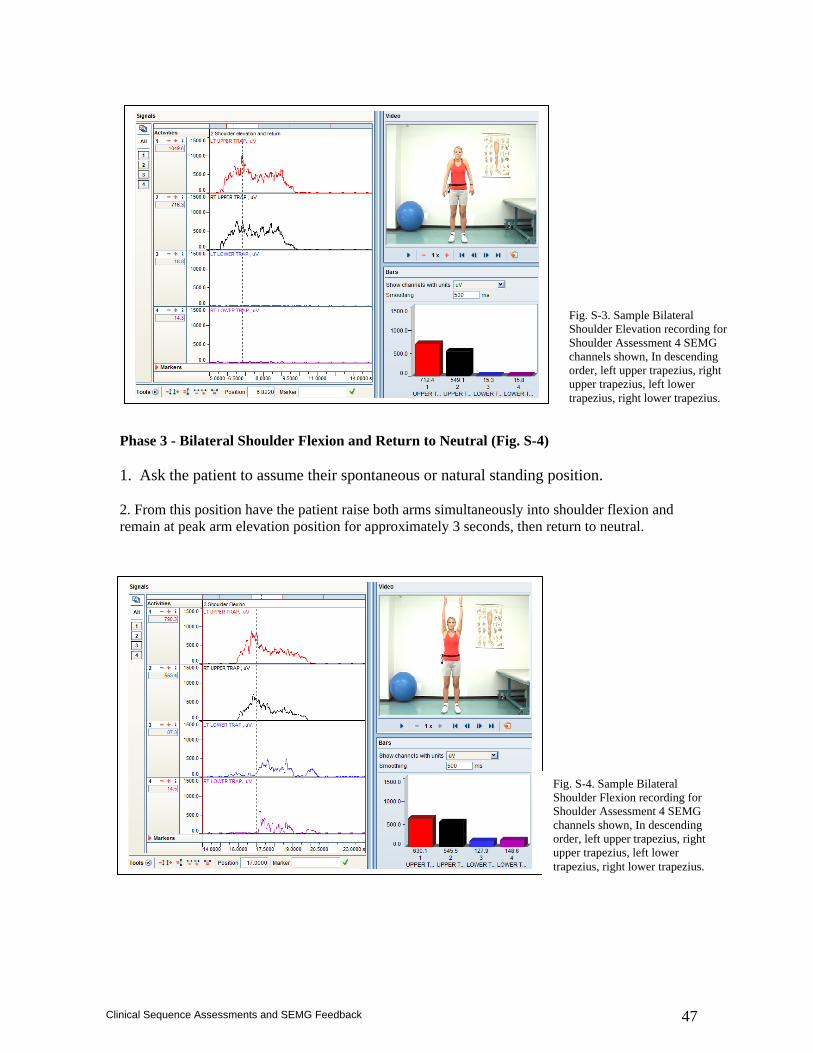
47
Clinical Sequence Assessments and SEMG Feedback
Phase 3 - Bilateral Shoulder Flexion and Return to Neutral (Fig. S-4) 1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position have the patient raise both arms simultaneously into shoulder flexion and remain at peak arm elevation position for approximately 3 seconds, then return to neutral.
Fig. S-3. Sample Bilateral Shoulder Elevation recording for Shoulder Assessment 4 SEMG channels shown, In descending order, left upper trapezius, right upper trapezius, left lower trapezius, right lower trapezius.
Fig. S-4. Sample Bilateral Shoulder Flexion recording for Shoulder Assessment 4 SEMG channels shown, In descending order, left upper trapezius, right upper trapezius, left lower trapezius, right lower trapezius.
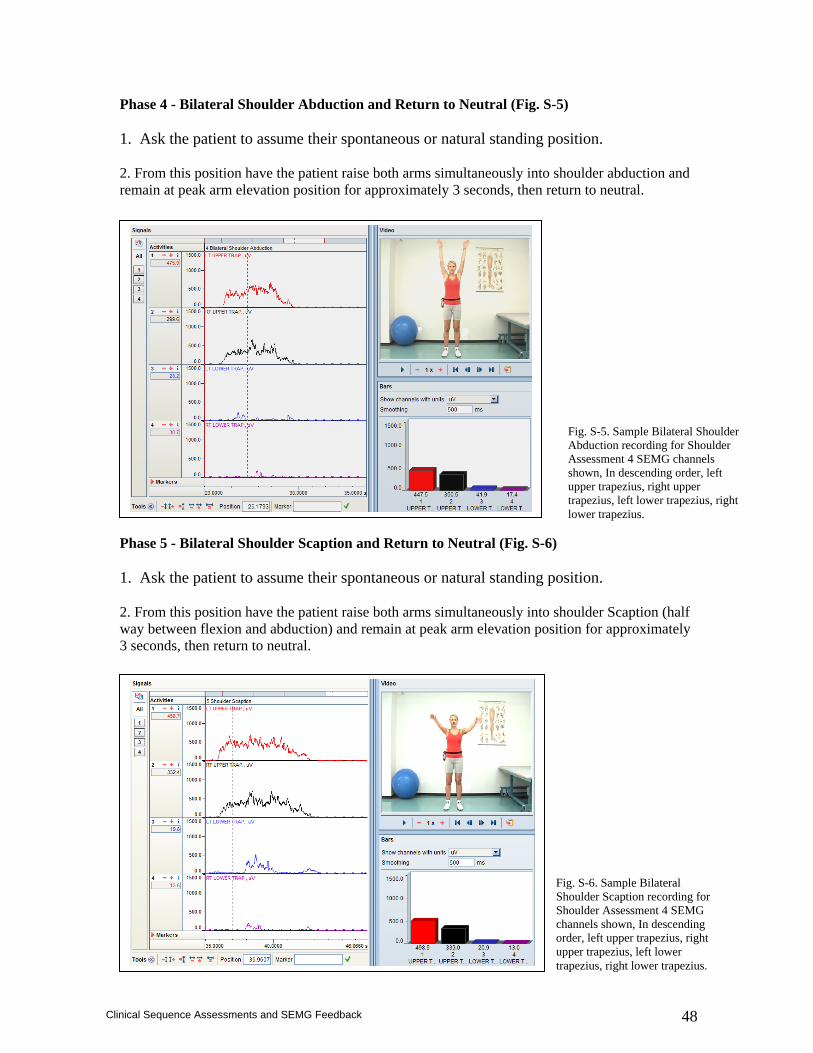
48
Clinical Sequence Assessments and SEMG Feedback
Phase 4 - Bilateral Shoulder Abduction and Return to Neutral (Fig. S-5) 1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position have the patient raise both arms simultaneously into shoulder abduction and remain at peak arm elevation position for approximately 3 seconds, then return to neutral. Phase 5 - Bilateral Shoulder Scaption and Return to Neutral (Fig. S-6) 1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position have the patient raise both arms simultaneously into shoulder Scaption (half way between flexion and abduction) and remain at peak arm elevation position for approximately 3 seconds, then return to neutral. General Documentation/Interpretation Considerations:
Fig. S-5. Sample Bilateral Shoulder Abduction recording for Shoulder Assessment 4 SEMG channels shown, In descending order, left upper trapezius, right upper trapezius, left lower trapezius, right lower trapezius.
Fig. S-6. Sample Bilateral Shoulder Scaption recording for Shoulder Assessment 4 SEMG channels shown, In descending order, left upper trapezius, right upper trapezius, left lower trapezius, right lower trapezius.

49
Clinical Sequence Assessments and SEMG Feedback
Symptomatic subjects tend to exhibit elevated baseline activity in the upper trapezius.43 Patients with chronic myalgia of the trapezius tend to exhibit a decrease in the ability to relax the trapezius.44 Qualitatively normalized recordings demonstrate the upper, middle and lower fibers of the trapezius gradually increase during arm elevation19,45-48 (flexion, scaption and abduction), decrease predictably and the upper trapezius is dominant during scapular elevation (shrug).45 Patients with impingement, adhesive capsulitis or instability tend to demonstrate altered upper:lower trapezius ratios, decreased lower and middle trapezius activity and relatively lower serratus anterior activity.20, 38, 49- 52 Most basic elements of SEMG documentation that should accompany interpretation of recording sites are: Baseline activity - Activity that is elevated and/or asymmetrical During bilateral Shoulder elevation - Activity that is asymmetrical > 35% and delayed return to baseline levels. During bilateral movements - Activity that is asymmetrical > 35% and/or altered temporal components.
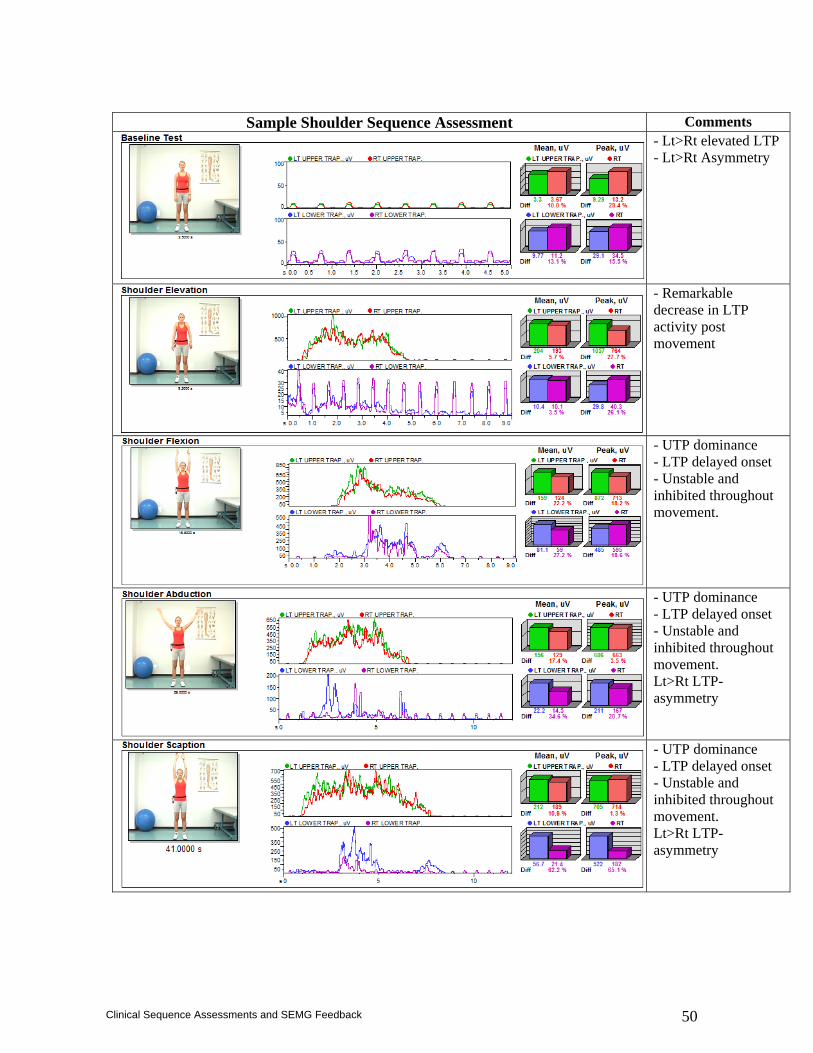
50
Clinical Sequence Assessments and SEMG Feedback
Sample Shoulder Sequence Assessment Comments
- Lt>Rt elevated LTP - Lt>Rt Asymmetry
- Remarkable decrease in LTP activity post movement
- UTP dominance - LTP delayed onset - Unstable and inhibited throughout movement.
- UTP dominance - LTP delayed onset - Unstable and inhibited throughout movement. Lt>Rt LTP-asymmetry
- UTP dominance - LTP delayed onset - Unstable and inhibited throughout movement. Lt>Rt LTP-asymmetry
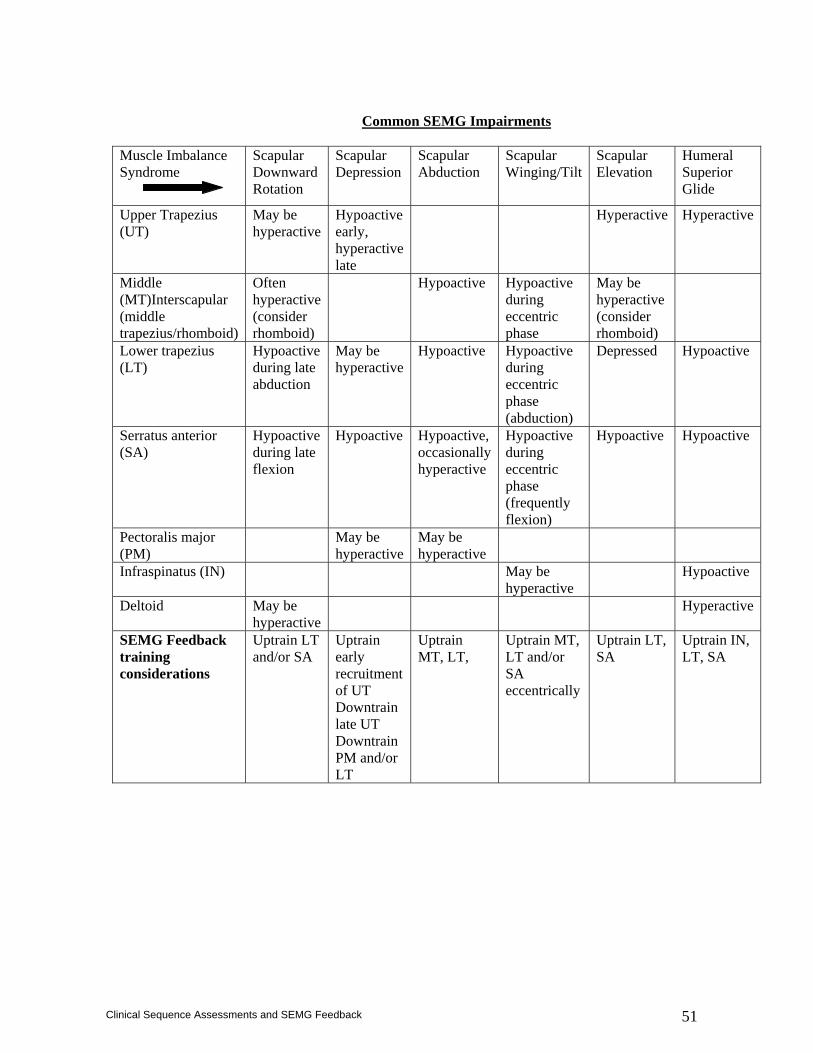
51
Clinical Sequence Assessments and SEMG Feedback
Common SEMG Impairments
Muscle Imbalance Syndrome
Scapular Downward Rotation
Scapular Depression
Scapular Abduction
Scapular Winging/Tilt
Scapular Elevation
Humeral Superior Glide
Upper Trapezius (UT)
May be hyperactive
Hypoactive early, hyperactive late
Hyperactive Hyperactive
Middle (MT)Interscapular (middle trapezius/rhomboid)
Often hyperactive (consider rhomboid)
Hypoactive Hypoactive during eccentric phase
May be hyperactive (consider rhomboid)
Lower trapezius (LT)
Hypoactive during late abduction
May be hyperactive
Hypoactive Hypoactive during eccentric phase (abduction)
Depressed Hypoactive
Serratus anterior (SA)
Hypoactive during late flexion
Hypoactive Hypoactive, occasionally hyperactive
Hypoactive during eccentric phase (frequently flexion)
Hypoactive Hypoactive
Pectoralis major (PM)
May be hyperactive
May be hyperactive
Infraspinatus (IN) May be hyperactive
Hypoactive
Deltoid May be hyperactive
Hyperactive
SEMG Feedback training considerations
Uptrain LT and/or SA
Uptrain early recruitment of UT Downtrain late UT Downtrain PM and/or LT
Uptrain MT, LT,
Uptrain MT, LT and/or SA eccentrically
Uptrain LT, SA
Uptrain IN, LT, SA
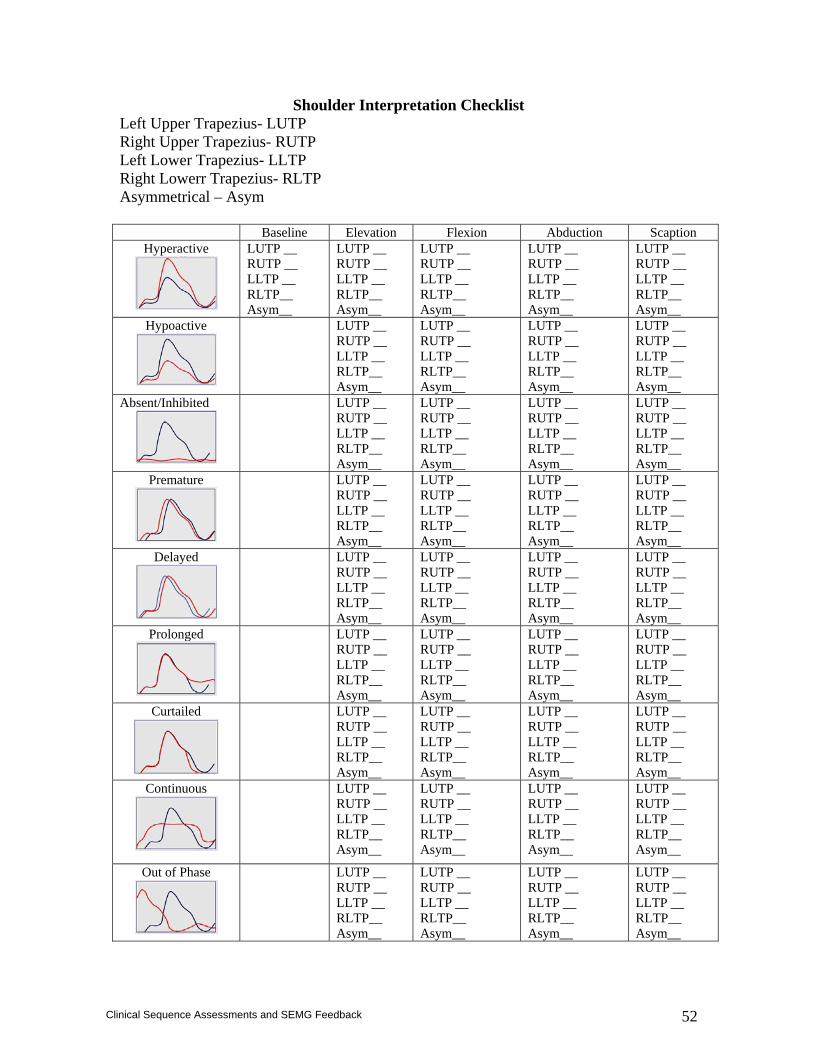
52
Clinical Sequence Assessments and SEMG Feedback
Shoulder Interpretation Checklist Left Upper Trapezius- LUTP Right Upper Trapezius- RUTP Left Lower Trapezius- LLTP Right Lowerr Trapezius- RLTP Asymmetrical – Asym Baseline Elevation Flexion Abduction Scaption
Hyperactive
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
Hypoactive
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
Absent/Inhibited
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
Premature
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
Delayed
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
Prolonged
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
Curtailed
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
Continuous
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
Out of Phase
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
LUTP __ RUTP __ LLTP __ RLTP__ Asym__
53
Clinical Sequence Assessments and SEMG Feedback
References
1. Chow JW, Carlton LG, Lim YT, Shim JH, Chae WS, Kuenster AF. Muscle activation during the tennis volley. Med Sci Sports Exerc.31:846-854;1999.
2. Cook CJ, Kothiyal K. Influence of mouse position on muscular activity in the neck, shoulder and arm in computer users. Appl Ergon 29:439-443;1998.
3. Grant KA, Habes DJ. An Electromyographic study of strength and upper extremity muscle activity in simulated meat cutting tasks. Appl Ergon. 28:129-137;1997.
4. Jensen B, Schibye B, Sogaard K, Simonsen E, Sjogaard G. Shoulder muscle load and muscle fatigue among industrial sewing-machine operators. Eur J Appl Physiolo. 57:467-475;1993.
5. Jobe F, Moynes D, Tibone J, Perry J. An EMG analysis of the shoulder in throwing and pitching: a second report. Am J Sports Med. 12:218-220;1984.
6. Larsson B, Kalberg C, Elert J, Gerdle B. Reproducibility of surface EMG during dynamic shoulder forward flexions: a study of clinically healthy subjects. Clin Physiol. 19:433-439;1999.
7. Pink M, Jobe F, Perry J, Browne A. Scovazzo ML, Kerrigan J. The painful shoulder during the butterfly stroke: an Electromyographic and cinematographic analysis of twelve muscles. Clin Orthp. 288:60-72;1992.
8. Pink M, Jobe F, Perry J. Electromyographic analysis of the shoulder during the golf swing. Am J Sports Med. 18:137-140;1990.
9. Maffet MW, Jobe FW, Pink MM, Brault J, Mathiyakom W. Shoulder muscle firing patterns during the windmill softball pitch. Am J Sports Med. 1997 May-Jun;25(3):369-74.
10. Rodriguuez R, Cook S, Sandborn P. Electromyographic analysis of rowing stroke biomechanics. J Sports Med Phys Fitness. 30:103-108;1990.
11. Sundelin G. Patterns of Electromyographic shoulder muscle fatigue during MTM-paced repetitive arm work with and without pauses. Int Arch Occup Envirvon Health. 64:485-493;1993.
12. Winkel J, Westgaard RH. Occupational and individual risk factors for shoulder-neck complaints, part II: the scientific basis (literature review) for the guide. Int J Indust Ergon. 10:85-104;1992.
13. Elert J, Gerdle B. The relationship between contraction and relaxation during fatiguing isokinetic shoulder flexions. An electromyographic study. Eur J Appl Physiol Occup Physiol 1989;59(4):303-9.
14. Aaras A. Postural load and the development of musculo-skeletal illness. Scand J Rehabil Med Suppl 1987;18:5-35.
15. Hagberg M. Electromyographic signs of shoulder muscular fatigue in two elevated arm positions. Am J Phys Med 1981 Jun;60(3):111-21.
16. Elert J, Sterner Y, Nyberg V, Gerdle B. Lack of gender differences in the ability to relax between repetitive maximum isokinetic shoulder forward flexions: a population-based study among northern Swedes. Eur J Appl Physiol. 83:246-256;2000.
17. Kelly BT, Kadrmas WR, Kirkendall DT, Speer KP. Optimal normalization tests for shoulder muscle activation: an Electromyographic study. J Orthop Res. 14:647-653;1996.
18. Farina D, Madeleine P, Graven-Nielsen T, Merletti R, Arendt-Neilsen L. Standardising surface electromyogram recordings for assessment of activity and fatigue in the human upper trapezius muscle. Eur J Appl Physiol 2002 Apr:86(6):469-78
19. Bagg SD, Forrest WJ. Electromyographic study of the scapular rotators during arm abduction in the scapular plane. Am J Phys Med 1986 Jun;65(3):111-24.
20. Wadsworth DJ, Bullock-Saxton JE. Recruitment patterns of the scapular rotator muscles in freestyle swimmers with subacromial impingement. Int J Sports Med. 1997 Nov;18(8):618-24.
21. Cools AM, Witvrouw EE, Declercq GA, Danneels LA, Cambier DC. Scapular muscle recruitment patterns: trapezius muscle latency with and without impingement symptoms. Am J Sports Med. 2003 Jul-Aug;31(4):542-9.
22. Ballantyne BT, O’Hare SJ, Paschall JL et al. Electromyographic activity of selected shoulder muscles in commonly used therapeutic exercises. Phys Ther. 73:668-682;1993.
23. Decker MJ, Hintermeister RA, Faber KJ, Hawkins RJ. Serratus anterior muscle activity during selected rehabilitation exercises. Am J Sports Med. 27:784-791;1999.
24. Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ. Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med.26:210-220;1998.
54
Clinical Sequence Assessments and SEMG Feedback
25. Malanga GA, Jenp YN, Growney ES, An KN. EMG analysis of shoulder positioning in testing and strengthening the supraspinatus. Med Sci Sports Exerc. 28:661-664;1996.
26. McCann PD, Wootten ME, Kadaba MP, Bigliani LU. A kinematic and electromyographic study of shoulder rehabilitation exercises. Clin Orthop. 288:179-188;1993.
27. Uhl TL, Carver TJ, Mattacola CG, Mair SD, Nitz AJ. Shoulder musculature activation during upper extremity weight-bearing exercise. J Orthop Sports Phys Ther. 2003 Mar;33(3):109-17.
28. Ekstrom RA, Donatelli RA, Soderberg GL. Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther. 2003 May;33(5):247-58.
29. Sakurai S, Ohtsuki T. Muscle activity and accuracy of performance of the smash stroke in badminton with reference to skill and practice. J Sports Sci. 2000 Nov;18(11):901-14.
30. Moseley A, Jobe FW, Pink M, Perry J, Tibone JE. EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med. 20:128-1134;1992.
31. Sulliuvan P, Portney L. Electromyographic activity of shoulder muscles during unilateral upper extremity proprioceptive neuromuscular facilitation patterns. Phys Ther. 60:668-682;1993.
32. Roe C, Brox JI, Bohmer AS, Vollestad NK. Muscle activation after supervised exercises in patients with rotator tendinosis. Arch Phys Med Rehabil.81:67-72;2000.
33. Beall S, Diefenbach G, Allen A. Electromyographic biofeedback in the treatment of voluntary posterior instability of the shoulder. Am J Sports Med. 15:175-178;1987.
34. Reid et al. Anterior shoulder instability in athletes: Comparison of isokinetic resistance exercises and an Electromyographic biofeedback reeducation program – a pilot program. Physiother Canada. Fall:251-259;1996.
35. Young MS. Electromyographic biofeedback use in the treatment of voluntary posterior dislocation of the shoulder: a case study. J Orthop Sports Phys Ther. 20:171-175;1994.
36. Cools AM, Witvrouw EE, De Clercq GA, Danneels LA, Willems TM, Cambier DC, Voight ML. Scapular muscle recruitment pattern: electromyographic response of the trapezius muscle to sudden shoulder movement before and after a fatiguing exercise. J Orthop Sports Phys Ther. 2002 May;32(5):221-9.
37. McQuade KJ, Dawson J, Smidt GL. Scapulothoracic muscle fatigue associated with alterations in scapulohumeral rhythm kinematics during maximum resistive shoulder elevation. J Orthop Sports Phys Ther. 28:74-80:1998.
38. Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. 80:276-291;2000.
39. Taylor W. Dynamic EMG biofeedback in assessment and treatment using a neuromuscular re-education model. In: Cram JR, ed. Clinical EMG for Surface Recordings. Vol 2. Nevada City, CA: Clinical Resources. 1990;175-196.
40. Cools AM, Witvrouw EE, Declercq GA, Danneels LA, Cambier DC. Scapular muscle recruitment patterns: trapezius muscle latency with and without impingement symptoms. Am J Sports Med. 2003 Jul-Aug;31(4):542-9.
41. Babyar S. Excessive scapular motion in individuals recovering from painful and stiff shoulders: causes and treatment strategies. Phys Ther. 76:226-238;1996.
42. Scovazzo ML, Browne A, Pink M, Jobe FW, Kerrigan J. The painful shoulder during freestyle swimming: an Electromyographic cinematographic analysis of twelve muscles. Asm J Sports Med. 19:577-582;1991.
43. Szeto GP, Straker LM, A comparison of symptomatic and asymptomatic office workers performing monotonous keyboard work-- neck and shoulder muscle recruitment patterns. Man Ther. 2005 Nov;10(4):270-80.
44. Larsson B, Bjork J, Elert J, Gerdle B. Shoulder forward flexions in female cleaners with and without myalgia of the trapezius muscle and in healthy controls. J Appl Physiol 2000 Nov;83(4 -5):257-67.
45. Büll ML, de Freitas V, Vitti M. Electromyographic study of the trapezius (pars superior) and serratus anterior (pars inferior) in free movements of the arm. Anat Anz. 1990;171(2):125-33.
46. Guazzelli Filho J, de Freitas V, Furlani J. Electromyographic study of the trapezius muscle in free movements of the shoulder. Electromyogr Clin Neurophysiol. 1994 Jul-Aug;34(5):279-83.
47. Campos GE, De Freitas V, Vitti M. Electromyographic study of the trapezius and deltoideus in elevation, lowering, retraction and protraction of the shoulders. Electromyogr Clin Neurophysiol. 1994 Jun;34(4):243-7.

55
Clinical Sequence Assessments and SEMG Feedback
48. Büll ML, Vitti M, De Freitas V. Electromyographic study of the trapezius (pars superior) and serratus anterior (pars inferior) muscles in free movements of the shoulder. Electromyogr Clin Neurophysiol. 1989 Mar;29(2):119-25.
49. Cools AM, Declercq GA, Cambier DC, Mahieu NN, Witvrouw EE. Trapezius activity and intramuscular balance during isokinetic exercise in overhead athletes with impingement symptoms. Scand J Med Sci Sports. 2007 Feb;17(1):25-33.
50. Matias R, Pascoal AG. The unstable shoulder in arm elevation: a three-dimensional and electromyographic study in subjects with glenohumeral instability. Clin Biomech (Bristol, Avon). 2006;21 Suppl 1:S52-8.
51. Pande, P, Peat M. Electromyography in voluntary posterior instability of the shoulder. The American Journal of Sports Medicine. 1989; 17:644-648.
52. McMahon PJ, Jobe FW, Pink MM, Brault JR, Perry J. Comparative electromyographic analysis of shoulder muscles during planar motions: anterior glenohumeral instability versus normal. J Shoulder Elbow Surg. 1996 Mar-Apr;5(2 Pt 1):118-23.
53. Lin JJ, Wu YT, Wang SF, Chen SY. Trapezius muscle imbalance in individuals suffering from frozen shoulder syndrome. Clin Rheumatol. 2005 Nov;24(6):569-75.
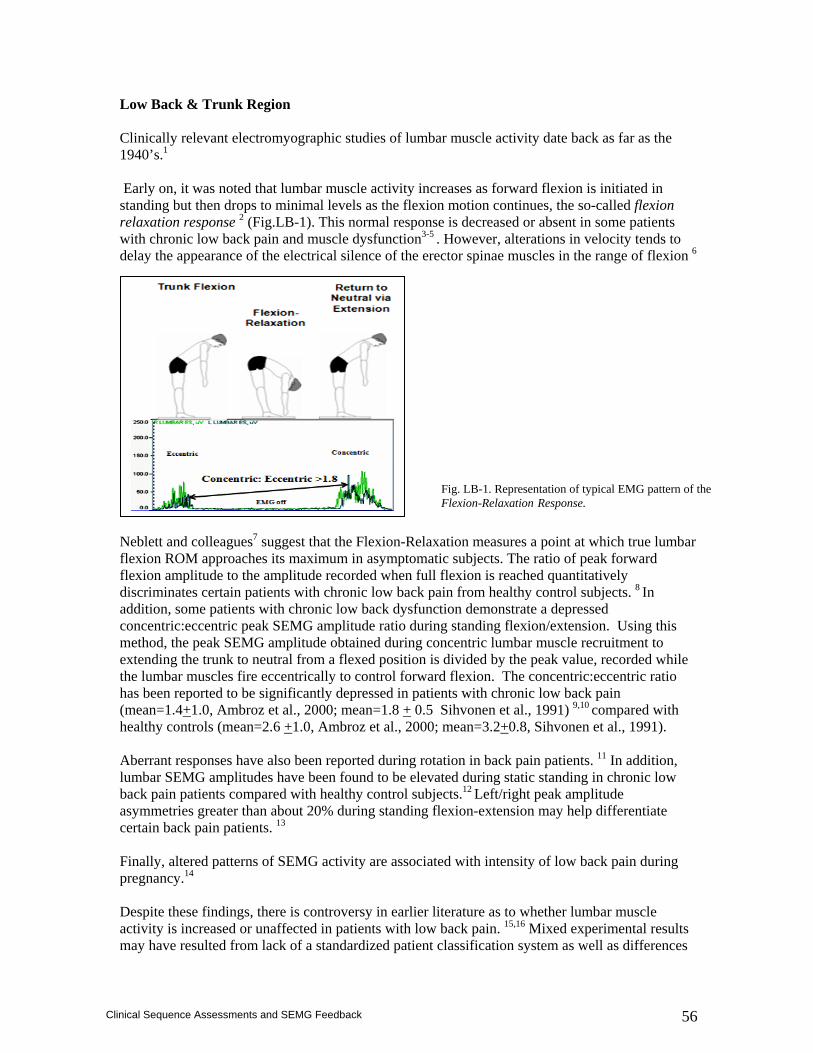
56
Clinical Sequence Assessments and SEMG Feedback
Low Back & Trunk Region Clinically relevant electromyographic studies of lumbar muscle activity date back as far as the 1940’s.1 Early on, it was noted that lumbar muscle activity increases as forward flexion is initiated in standing but then drops to minimal levels as the flexion motion continues, the so-called flexion relaxation response 2 (Fig.LB-1). This normal response is decreased or absent in some patients with chronic low back pain and muscle dysfunction3-5 . However, alterations in velocity tends to delay the appearance of the electrical silence of the erector spinae muscles in the range of flexion 6 Neblett and colleagues7 suggest that the Flexion-Relaxation measures a point at which true lumbar flexion ROM approaches its maximum in asymptomatic subjects. The ratio of peak forward flexion amplitude to the amplitude recorded when full flexion is reached quantitatively discriminates certain patients with chronic low back pain from healthy control subjects. 8 In addition, some patients with chronic low back dysfunction demonstrate a depressed concentric:eccentric peak SEMG amplitude ratio during standing flexion/extension. Using this method, the peak SEMG amplitude obtained during concentric lumbar muscle recruitment to extending the trunk to neutral from a flexed position is divided by the peak value, recorded while the lumbar muscles fire eccentrically to control forward flexion. The concentric:eccentric ratio has been reported to be significantly depressed in patients with chronic low back pain (mean=1.4+1.0, Ambroz et al., 2000; mean=1.8 + 0.5 Sihvonen et al., 1991) 9,10 compared with healthy controls (mean=2.6 +1.0, Ambroz et al., 2000; mean=3.2+0.8, Sihvonen et al., 1991). Aberrant responses have also been reported during rotation in back pain patients. 11 In addition, lumbar SEMG amplitudes have been found to be elevated during static standing in chronic low back pain patients compared with healthy control subjects.12 Left/right peak amplitude asymmetries greater than about 20% during standing flexion-extension may help differentiate certain back pain patients. 13 Finally, altered patterns of SEMG activity are associated with intensity of low back pain during pregnancy.14 Despite these findings, there is controversy in earlier literature as to whether lumbar muscle activity is increased or unaffected in patients with low back pain. 15,16 Mixed experimental results may have resulted from lack of a standardized patient classification system as well as differences
Fig. LB-1. Representation of typical EMG pattern of the Flexion-Relaxation Response.
57
Clinical Sequence Assessments and SEMG Feedback
in experimental design that underestimated the complexity of movement control of the trunk.17 The preponderance of evidence, though, suggests that whereas many patients with chronic low back pain show typical patterns of lumbar muscle activity in static postures and during standing movements, aberrant SEMG patterns (e.g., absence of a flexion/relaxation response, depressed concentric:eccentric ratio, and large left/right asymmetries during standing flexion-extension; markedly elevated postural baseline activity ) are rarely seen in healthy subjects. Patients with chronic low back pain and segmental hypermobility as well as radicular symptoms may be most likely to demonstrate abnormal SEMG findings.18 Lifting tasks are often a problem for patients with chronic lumbar dysfunction, which have been studied extensively with SEMG. Investigators have carefully controlled movement variables as well as combined SEMG monitoring with kinematic assessment to study the dynamics of lifting and then formulate recommendations for functional lifting techniques.19-24 Lumbar as well as abdominal and gluteal SEMG recordings have also been used to assist with biomechanical modeling of other tasks, to analyze stabilization and other therapeutic exercises, and to gradate the intensity of low back exercise prescription.25-36 These lines of investigation hold promise toward the development of a sophisticated understanding of neuromuscular control of the trunk, with important implications for the prescription of exercise in injured populations as well as injury prevention in industry. Exciting work in this domain pertains to differentiation of patients with chronic low back pain and spinal instability from healthy control subjects on the basis of motor control responses from rectus abdominis and oblique abdominal muscles.37 Exercises using an abdominal drawing in maneuver, purported to promote trunk stability and selectively facilitate activity of the internal oblique, in fact result in increased SEMG amplitude ratios of internal oblique:rectus abdominis as well as decreased pain and improved function in controlled designs.37,38 Another area of SEMG investigation of lumbar dysfunction with impressive results involves frequency spectral analysis. Compression and shift of SEMG frequency components accompany muscle fatigue and a variety of related techniques have been used to study the effects of resisted isometric trunk extension as well as repeated lifting. 39-45 SEMG frequency parameters used to quantify fatigue and recovery have discriminated chronic low back pain patients from controls with remarkable accuracy, 46-49 although very simple methods for clinicians may be less forthcoming.50 SEMG feedback training can be combined productively with back muscle strengthening.51 Feedback training with SEMG can also be used to teach patients to lower static levels of lumbar muscle activity52 as well as resolve left/right paraspinal muscle asymmetries.53 In addition, SEMG techniques have been used to evaluate the effects of manual spinal manipulation on muscle activity.54,55 Behavioral correlates help to predict outcomes with SEMG feedback training.56 Maladaptive responses to emotional stressors are linked with lumbar muscle hyperactivity and associated with inability to consciously discriminate muscle activity levels at the low back.57,58 Treatment regimens that incorporate SEMG feedback training (for reduction of lumbar paraspinal muscle hyperactivity) result in lowered levels of lumbar muscle activity as well as reduced pain, less affective distress, and lowered consumption of health care services that persist to at least a 24 month follow-up.59
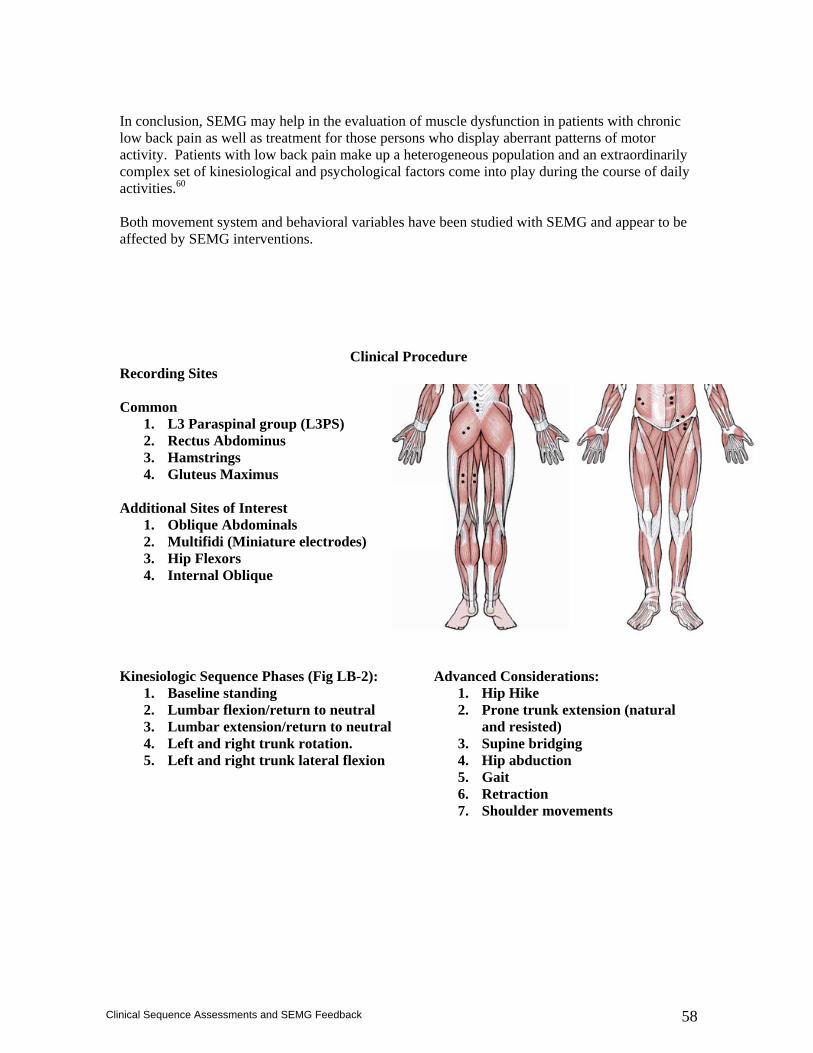
58
Clinical Sequence Assessments and SEMG Feedback
In conclusion, SEMG may help in the evaluation of muscle dysfunction in patients with chronic low back pain as well as treatment for those persons who display aberrant patterns of motor activity. Patients with low back pain make up a heterogeneous population and an extraordinarily complex set of kinesiological and psychological factors come into play during the course of daily activities.60 Both movement system and behavioral variables have been studied with SEMG and appear to be affected by SEMG interventions.
Clinical Procedure Recording Sites Common
1. L3 Paraspinal group (L3PS) 2. Rectus Abdominus 3. Hamstrings 4. Gluteus Maximus
Additional Sites of Interest
1. Oblique Abdominals 2. Multifidi (Miniature electrodes) 3. Hip Flexors 4. Internal Oblique
Kinesiologic Sequence Phases (Fig LB-2):
1. Baseline standing 2. Lumbar flexion/return to neutral 3. Lumbar extension/return to neutral 4. Left and right trunk rotation. 5. Left and right trunk lateral flexion
Advanced Considerations: 1. Hip Hike 2. Prone trunk extension (natural
and resisted) 3. Supine bridging 4. Hip abduction 5. Gait 6. Retraction 7. Shoulder movements
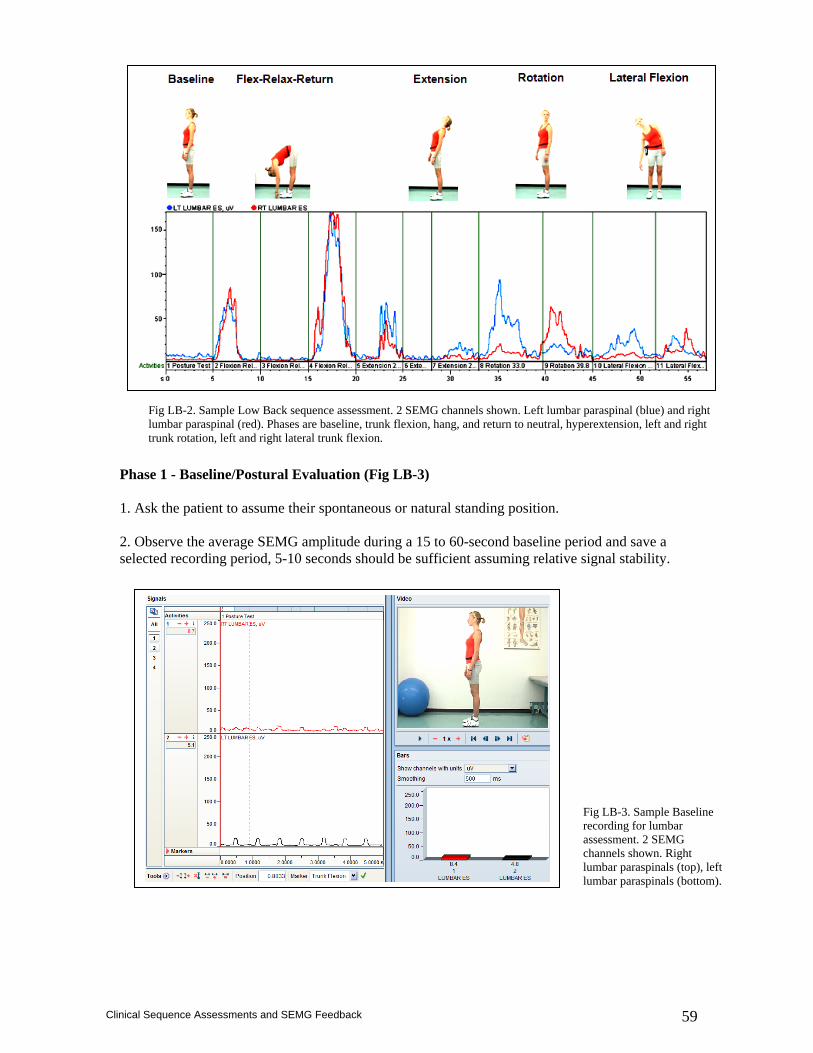
59
Clinical Sequence Assessments and SEMG Feedback
Phase 1 - Baseline/Postural Evaluation (Fig LB-3) 1. Ask the patient to assume their spontaneous or natural standing position. 2. Observe the average SEMG amplitude during a 15 to 60-second baseline period and save a selected recording period, 5-10 seconds should be sufficient assuming relative signal stability.
Fig LB-2. Sample Low Back sequence assessment. 2 SEMG channels shown. Left lumbar paraspinal (blue) and right lumbar paraspinal (red). Phases are baseline, trunk flexion, hang, and return to neutral, hyperextension, left and right trunk rotation, left and right lateral trunk flexion.
Fig LB-3. Sample Baseline recording for lumbar assessment. 2 SEMG channels shown. Right lumbar paraspinals (top), left lumbar paraspinals (bottom).
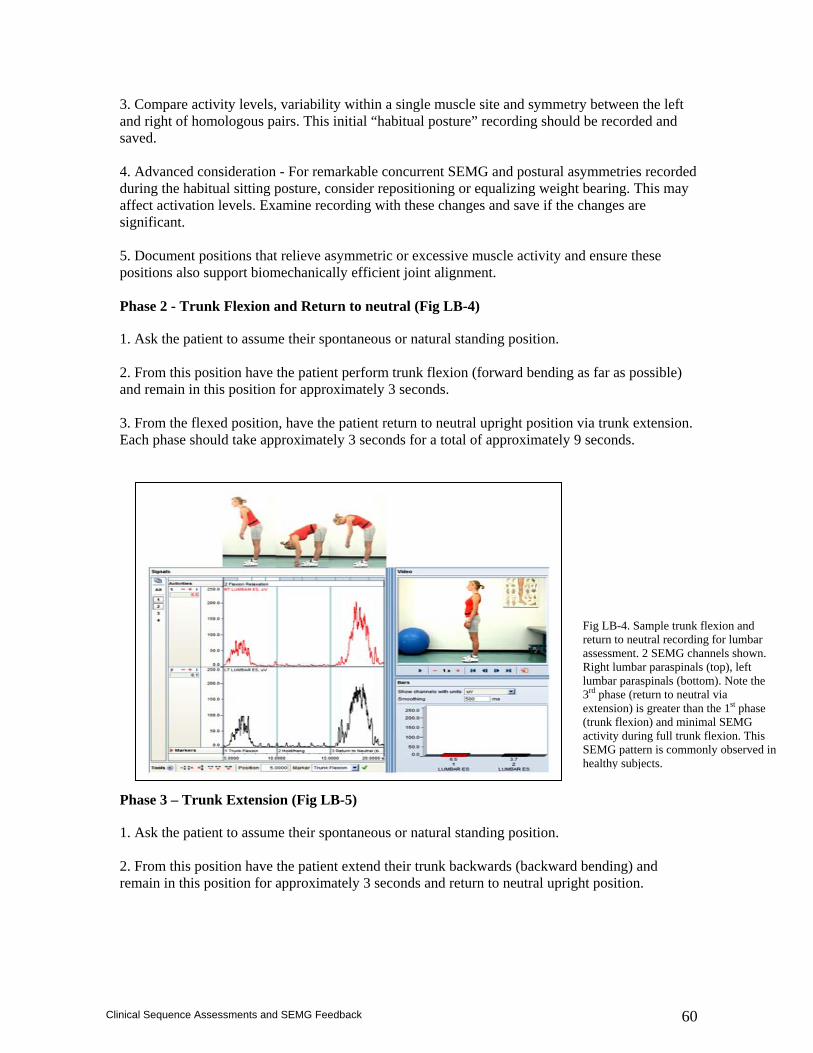
60
Clinical Sequence Assessments and SEMG Feedback
3. Compare activity levels, variability within a single muscle site and symmetry between the left and right of homologous pairs. This initial “habitual posture” recording should be recorded and saved. 4. Advanced consideration - For remarkable concurrent SEMG and postural asymmetries recorded during the habitual sitting posture, consider repositioning or equalizing weight bearing. This may affect activation levels. Examine recording with these changes and save if the changes are significant. 5. Document positions that relieve asymmetric or excessive muscle activity and ensure these positions also support biomechanically efficient joint alignment. Phase 2 - Trunk Flexion and Return to neutral (Fig LB-4)
1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position have the patient perform trunk flexion (forward bending as far as possible) and remain in this position for approximately 3 seconds. 3. From the flexed position, have the patient return to neutral upright position via trunk extension. Each phase should take approximately 3 seconds for a total of approximately 9 seconds.
Phase 3 – Trunk Extension (Fig LB-5)
1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position have the patient extend their trunk backwards (backward bending) and remain in this position for approximately 3 seconds and return to neutral upright position.
Fig LB-4. Sample trunk flexion and return to neutral recording for lumbar assessment. 2 SEMG channels shown. Right lumbar paraspinals (top), left lumbar paraspinals (bottom). Note the 3rd phase (return to neutral via extension) is greater than the 1st phase (trunk flexion) and minimal SEMG activity during full trunk flexion. This SEMG pattern is commonly observed in healthy subjects.
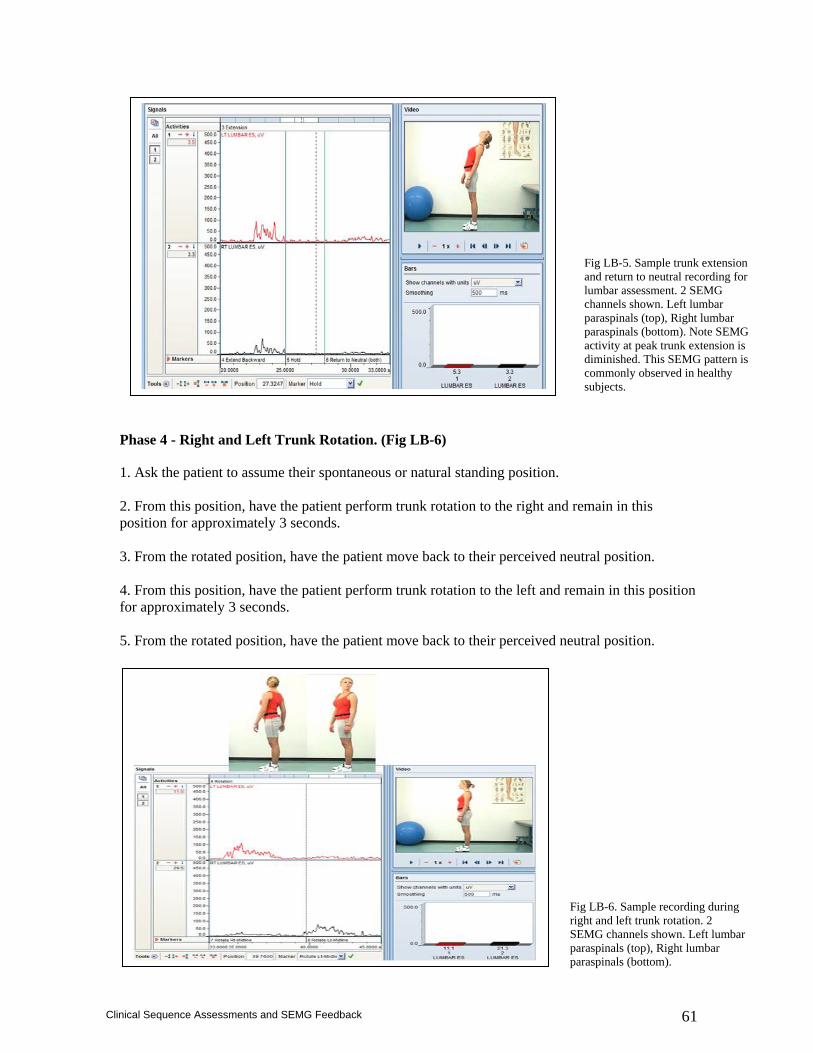
61
Clinical Sequence Assessments and SEMG Feedback
Phase 4 - Right and Left Trunk Rotation. (Fig LB-6)
1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position, have the patient perform trunk rotation to the right and remain in this position for approximately 3 seconds. 3. From the rotated position, have the patient move back to their perceived neutral position. 4. From this position, have the patient perform trunk rotation to the left and remain in this position for approximately 3 seconds. 5. From the rotated position, have the patient move back to their perceived neutral position.
Fig LB-5. Sample trunk extension and return to neutral recording for lumbar assessment. 2 SEMG channels shown. Left lumbar paraspinals (top), Right lumbar paraspinals (bottom). Note SEMG activity at peak trunk extension is diminished. This SEMG pattern is commonly observed in healthy subjects.
Fig LB-6. Sample recording during right and left trunk rotation. 2 SEMG channels shown. Left lumbar paraspinals (top), Right lumbar paraspinals (bottom).
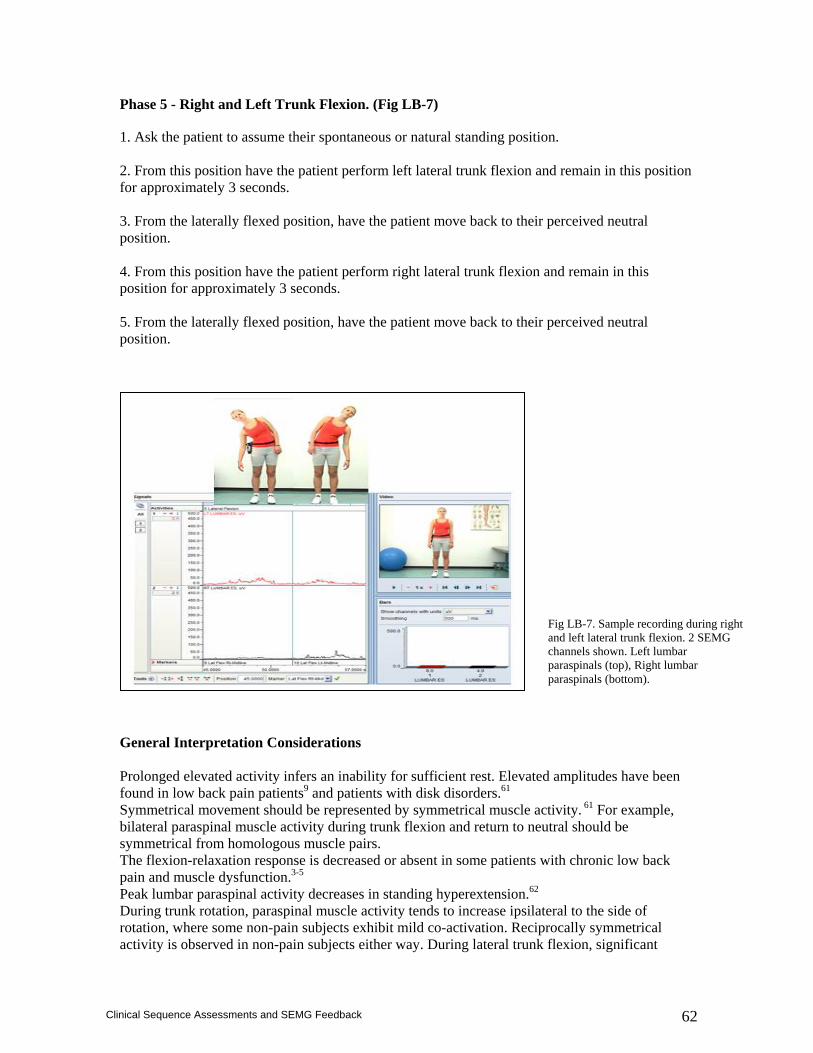
62
Clinical Sequence Assessments and SEMG Feedback
Phase 5 - Right and Left Trunk Flexion. (Fig LB-7)
1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position have the patient perform left lateral trunk flexion and remain in this position for approximately 3 seconds. 3. From the laterally flexed position, have the patient move back to their perceived neutral position. 4. From this position have the patient perform right lateral trunk flexion and remain in this position for approximately 3 seconds. 5. From the laterally flexed position, have the patient move back to their perceived neutral position. General Interpretation Considerations Prolonged elevated activity infers an inability for sufficient rest. Elevated amplitudes have been found in low back pain patients9 and patients with disk disorders.61 Symmetrical movement should be represented by symmetrical muscle activity. 61 For example, bilateral paraspinal muscle activity during trunk flexion and return to neutral should be symmetrical from homologous muscle pairs. The flexion-relaxation response is decreased or absent in some patients with chronic low back pain and muscle dysfunction.3-5 Peak lumbar paraspinal activity decreases in standing hyperextension.62 During trunk rotation, paraspinal muscle activity tends to increase ipsilateral to the side of rotation, where some non-pain subjects exhibit mild co-activation. Reciprocally symmetrical activity is observed in non-pain subjects either way. During lateral trunk flexion, significant
Fig LB-7. Sample recording during right and left lateral trunk flexion. 2 SEMG channels shown. Left lumbar paraspinals (top), Right lumbar paraspinals (bottom).
63
Clinical Sequence Assessments and SEMG Feedback
increases in activity from the side opposite to bending side during concentric portion (return to neutral) is common in healthy subjects63 and reciprocal symmetry is commonly observed.64 The most basic elements of SEMG documentation that should accompany interpretation of recording sites are: Baseline activity - Activity that is elevated and/or asymmetrical During trunk flexion - Activity that is asymmetrical > 20% Lack of Flexion/relaxation response during trunk flexion:return to neutral phase. During unilateral movements – Activity that is not reciprocally symmetrical.
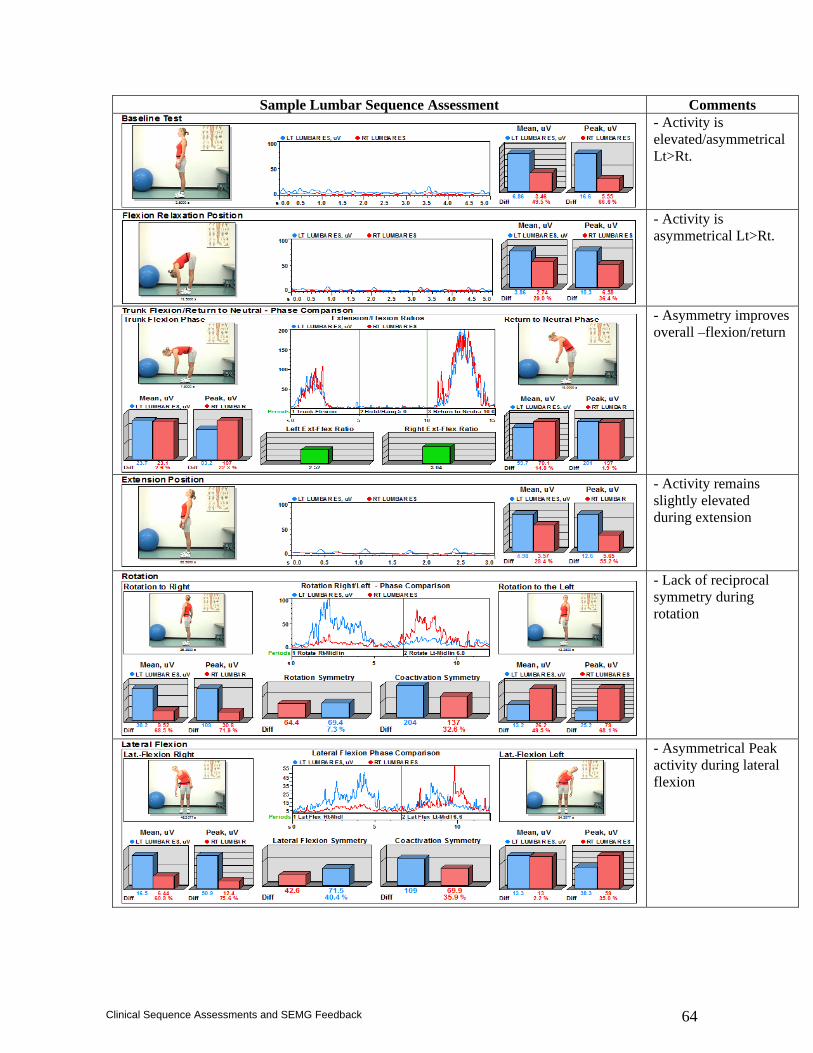
64
Clinical Sequence Assessments and SEMG Feedback
Sample Lumbar Sequence Assessment Comments
- Activity is elevated/asymmetrical Lt>Rt.
- Activity is asymmetrical Lt>Rt.
- Asymmetry improves overall –flexion/return
- Activity remains slightly elevated during extension
- Lack of reciprocal symmetry during rotation
- Asymmetrical Peak activity during lateral flexion
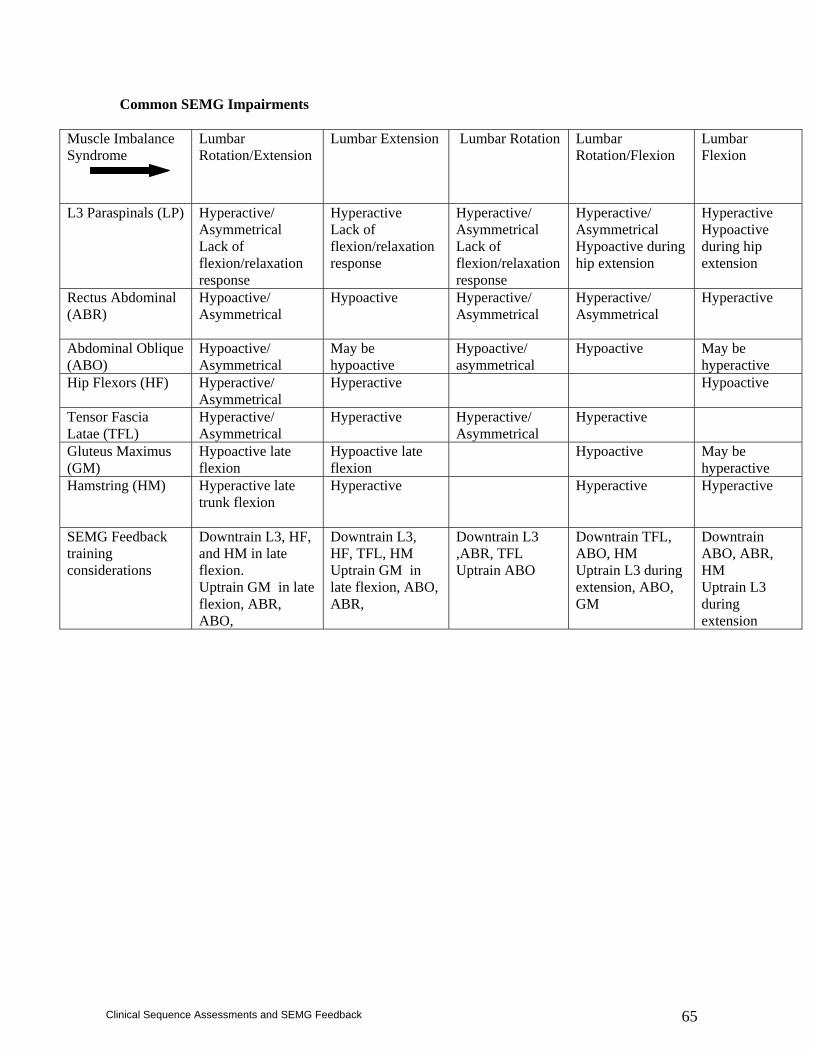
65
Clinical Sequence Assessments and SEMG Feedback
Common SEMG Impairments
Muscle Imbalance Syndrome
Lumbar Rotation/Extension
Lumbar Extension Lumbar Rotation Lumbar Rotation/Flexion
Lumbar Flexion
L3 Paraspinals (LP) Hyperactive/ Asymmetrical Lack of flexion/relaxation response
Hyperactive Lack of flexion/relaxation response
Hyperactive/ Asymmetrical Lack of flexion/relaxation response
Hyperactive/ Asymmetrical Hypoactive during hip extension
Hyperactive Hypoactive during hip extension
Rectus Abdominal (ABR)
Hypoactive/ Asymmetrical
Hypoactive Hyperactive/ Asymmetrical
Hyperactive/ Asymmetrical
Hyperactive
Abdominal Oblique (ABO)
Hypoactive/ Asymmetrical
May be hypoactive
Hypoactive/ asymmetrical
Hypoactive May be hyperactive
Hip Flexors (HF) Hyperactive/ Asymmetrical
Hyperactive Hypoactive
Tensor Fascia Latae (TFL)
Hyperactive/ Asymmetrical
Hyperactive Hyperactive/ Asymmetrical
Hyperactive
Gluteus Maximus (GM)
Hypoactive late flexion
Hypoactive late flexion
Hypoactive May be hyperactive
Hamstring (HM) Hyperactive late trunk flexion
Hyperactive Hyperactive Hyperactive
SEMG Feedback training considerations
Downtrain L3, HF, and HM in late flexion. Uptrain GM in late flexion, ABR, ABO,
Downtrain L3, HF, TFL, HM Uptrain GM in late flexion, ABO, ABR,
Downtrain L3 ,ABR, TFL Uptrain ABO
Downtrain TFL, ABO, HM Uptrain L3 during extension, ABO, GM
Downtrain ABO, ABR, HM Uptrain L3 during extension

66
Clinical Sequence Assessments and SEMG Feedback
Lumbar SEMG Interpretation Checklist: Left L3 Paraspinal‐ LL3PS Right L3 Paraspinal‐ RL3PS Right Gluteus Maximus– RGMX Left Gluteus Maximus– LGMX Asymmetrical - Asym Baseline Flex/Ret to Neutral Rt/Lt Rotation Rt/Lt Lateral Flexion
Hyperactive
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
Prolonged-Lack of Flex/relax response
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
Hypoactive
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
Absent/Inhibited
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
Premature
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
Delayed
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
Curtailed
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
Continuous
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
Out of Phase
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
LL3PS __ RL3PS __ RGMX __ LGMX __ Asym__
67
Clinical Sequence Assessments and SEMG Feedback
References
1. Price JP, Claire MH, Ewehardt RH. Studies in low back-ache with persistent spasm. Achiev Phys Med. 29:703-709;1948.
2. Shirado O, Ito T, Kaneda K, Strax TE. Flexion-relaxation phenomenon in back muscles. Am J Phys Med. 74:139-143, 1995.
3. Ahern DK, Follick MJ, Council JR, Laser-Wolston N, Litchman H. Comparison of lumbar paravertebral EMG patterns on chronic low back pain patients and non-patient controls. Pain. 34:153-160, 1988.
4. Triano J, Schulz AB. Loads transmitted during lumbosacral spinal manipulative therapy. Spine. 22:1955-1964;1997.
5. Solomonow M, Baratta RV, Banks A, Freudenberger C, Zhou BH. Flexion-relaxation response to static lumbar flexion in males and females. Clin Biomech (Bristol, Avon). 2003 May;18(4):273-9.
6. Sarti MA, Lison JF, Monfort M, Fuster MA. Response of the flexion-relaxation phenomenon relative to the lumbar motion to load and speed. Spine. 2001 Sep 15;26(18):E421-6.
7. Neblett R, Mayer TG, Gatchel RJ, Keeley J, Proctor T, Anagnostis C. Quantifying the Lumbar Flexion-Relaxation Phenomenon: Theory, Normative Data, and Clinical Applications. Spine. 2003 Jul 1;28(13):1435-1446.
8. Watson PJ, Booker CK, Main CJ, Chen AC. Surface electromyography in the identification of chronic low back pain patients: the development of the flexion relaxation ratio. Clin Biomech (Bristol, Avon). 3:165-171;1997.
9. Amroz C, Scott A, Ambroz A, Evelyn EO. Chronic low back pain assessment using surface electromyography. JOEM. 42:660-669, 2000.
10. Sihvonen T, Partanen J, Hanninen O, Soimakallio S. Electric behavior of low back muscles during lumbar pelvic rhythm in low back pain patients and healthy controls. Arch Phys Med Rehabil. 72:1080-1087, 1991.
11. Wolf SL, Nacht M, Kelly JL. EMG feedback training during dynamic movement for low back pain patients. Behav Ther. 13:395-406, 1982.
12. Cram JR, Kasman, GS. Introduction to Surface Electromyography. Gaithersburg, MD: Aspen Publishers, 1998.
13. Donaldson CCS. The effects of correcting muscle asymmetry upon chronic low back pain. Calgary, Alberta: University of Calgary:1989. Dissertation.
14. Sihvonen T, Httunen M, Makkonen M, Airaksinen O. Functional changes in back muscle activity correlate with pain intensity and prediction of low back pain during pregnancy. Arch Phys Med Rehabil. 79:1210-1212;1998.
15. Sherman RA, Arena JG. Biofeedback for assessment and treatment of low back pain. In: Basmaijian JV, Nyberg R, eds. Rational Manual Therapies. Baltimore: Williams & Wilkins; 1993; 177-198.
16. Nouwen A, Bush C. The relationship between paraspinal EMG and chronic low back pain. Pain. 20:109-123;1984.
17. Wolf SL, Wolf LB, Segal RL. The relationship of extraneous movements to lumbar paraspinal muscle activity: implications for EMG biofeedback training applications to low back pain patients. Biofeedback Self Regul. 14:63-74, 1989.
18. Sihvonen T, Lindgren KA, Airaksinen O, Manninen H. Movement disturbances of the lumbar spine and abnormal back muscle Electromyographic findings in recurrent low back pain. Spine. 22:289-295;1997.
19. Brown JM, Mills JH, Baker A. Neuromuscular control of lifting in the elderly. Gerontology. 40:298-306, 1994.
20. Mientjes MI, Norman RW, Wells RP, McGill SM. Assessment of an EMG-based method for continuous estimates of low back pain compression during asymmetrical occupational tasks. Ergonomics. 42:868-879;1999.
21. Nielsen PK, Andersen L, Jorgensen K. The muscular load on the lower back and shoulders due to lifting at different lifting heights and frequencies. Appl Ergon. 29:445-450;1998.
22. Scholz JP, Milford JP, McMillan AG. Neuromuscular coordination of squat lifting, I: effect of load magnitude. Phys Ther. 75:119-132, 1995.
68
Clinical Sequence Assessments and SEMG Feedback
23. Toussaint HM, de Winter AF, de Haas T, de Looze MP, Van Dieen JH, Kingma I. Flexion relxation during lifting: implications for torque production by muscle activity and tissue strain at the lumbo-sacral joint. J Biomech. 28:199-219, 1995.
24. Vakos JP, Nitz AJ, Threkeld AJ, Shapiro R, Horn T. Electromyographic activity of selected trunk and hip muscles during a squat lift: effect of varying the lumbar posture. Spine. 19:687-695, 1994.
25. Arokoski JP, Kankaanpaa M, Valta T, et al. Back and hip extensor muscle function during therapeutic exercises. Arch Phys Med Rehabil. 80:842-850,1999.
26. Arokoski JP, Valta T, Airaksinen O, Kankaanpaa M. Back and abdominal muscle function during stabilization exercises. Arch Phys Med Rehabil. 82:1089-1098;2001.
27. Callaghan JP, GunningJL, McGill SM. The relationship between lumbar spine load and muscle activity during extensor exercises. Phys Ther. 78:8-18,1998.
28. Fiebert I, Keller CD. Are “passive” extension exercises really passive? J Orthop Sports Phys Ther. 19:111-116, 1994.
29. Lavender SA, Marras WS, Miller RA. The development of response strategies in preparation for sudden loading to the torso. Spine. 18:2097-2105, 1993.
30. McGill S. Low back exercises: evidence for improving exercise regimens. Phys Ther. 78:754-765, 1998.
31. Robinson ME, Cassisi JE, O’Conner PD, MacMillan M. Lumbar iEMG during isotonic exercise, chronic back pain patients versus controls. J Spinal Disord. 5:8-15, 1992.
32. Shields RK, Heiss DG. An Electromyographic comparison of abdominal muscle synergism during curl and double straight leg lowering exercises with control of the pelvic position. Spine. 22:1873-1879, 1997.
33. Souza GM, Baker LL, Powers CM. Electromyographic activity of selected trunk muscles during dynamic spine stabilization exercises. Arch Phys Med Rehabil. 82:1551-1557;2001.
34. Udermann BE, Graves JE, Donelson RG, Ploutz-Snyder L, Boucher JP, Iriso JH. Pelvic restraint effect on lumbar gluteal and hamstring muscle Electromyographic activation. Arch Phys Med Rehabil. 80:428-431, 1999.
35. Vera-Garcia FJ, Grebier SG, McGill SM. Abdominal muscle response during curl-ups on both stable and labile surfaces. Phys Ther. 80:564-569, 2000.
36. Vezina J, Hubley-Kozey CL. Arch Phys Med Rehabil. 81:1370-1379, 2000. 37. O’Sullivan PB, Twomey L, Allison GT. Altered abdominal muscle recruitment in patients with
chronic back pain following a specific exercise intervention. J Ortho Sports Phys Ther. 114-124, 1998.
38. O’Sullivan PB, Phyty GD, Twomey LT, Allison GT. Evaluation of specific stabilizing exercises in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine. 22:2959-2967;1997.
39. Biederman HJ, Shanks GL, Forrest WJ, Inglis J. Power spectrum analysis of Electromyographic activity: discriminators in the differential assessment of patients with chronic low back pain. Spine. 16:1179-1184, 1991.
40. Dolan P, Mannion AF, Adams MA. Fatigue of the erector spinae muscles: a quantitative assessment using “frequency banding” of the surface electromyographic signal. Spine. 20:149-159, 1995.
41. Potvin JR, Norman RW. Quantification of erector spinae muscle fatigue during prolonged, dynamic lifting tasks. Eur J Appl Physiol. 67:554-562, 1993.
42. Roy SH, Oddsson LI. Classification of paraspinal muscle impairments by surface electromyography. Phys Ther. 78:838-851;1998.
43. Thompson DA, Biedermann HJ. Electromyographic power spectrum analysis of the paraspinal muscles. Long-term reliability. Spine. 18:2310-2313;1993.
44. Tsuboi T, Satou T, Egawsa K, Izuni Y, Miyazaki M. Spectral analysis of electromyogram in lumbar muscles: fatigue induced endurance contraction. Eur J App Physiol. 69:361-366, 1994.
45. Umezu Y, Kawazu T, Tajima F, Ogata H. Spectral Electromyographic fatigue analysis of back muscles in healthy adult women compared with men. Arch Phys Med Rehabil. 79:536-538;1998
46. Klein AB, Snyder-Mackler L, Roy SH, De Luca CJ. Comparison of spinal mobility and isometric trunk extensor forces with Electromyographic spectral analysis in identifying low back pain. Phys Ther. 71:445-454, 1991.
69
Clinical Sequence Assessments and SEMG Feedback
47. Peach JP, McGill SM. Classification of low back pain with the use of spectral electromyogram parameters. Spine. 23:1117-1123;1998.
48. Roy SH, De Luca CJ, Emley M, Buijs RJC. Spectral electromyographic assessment of back muscles in patients with low back pain undergoing rehabilitation. Spine. 20:38-48, 1995.
49. Roy SH, De Luca CJ, Snyder-Mackler L, Emley MS, Crenshaw RL, Lyons LP. Fatigue, recovery, and low back pain in varsity rowers. Med Sci Sports Exerc. 22:463-469, 1990.
50. Mofroid M, Reid S, Henry SM, Haugh LD, Ricamato A. Some endurance measures in persons with chronic low back pain. J Ortho Sports Phys Ther. 20:81-87;1994.
51. Asfour SS, Kahlil TM, Waly SM, Goldberg ML, Rosomoff HL. Biofeedback in back muscle strengthening. Spine. 15:510-513, 1990.
52. Large RG, Lamb AM. Electromyographic (EMG) feedback in chronic musculoskeletal pain: a controlled trial. Pain 17:167-177, 1983.
53. Donaldson S, Romney D, Donaldson M, Skubick D. Randomized study of the application of single motor unit biofeedback training to chronic low back pain. J Occup rehabil. 4:23-37, 1994.
54. Lehman GL, McGill SM. Spinal manipulation causes variable spine kinematic and trunk muscle Electromyographic responses. Clin Biomech (Bristol, Avon). 16:293-299;2001.
55. Lehman GL, Vernon H. McGill SM. Effects of a mechanical pain stimulus on erector spinae activity before and after a spinal manipulation in patients with back pain: a preliminary investigation. J Manipulative Physio Ther. 24:402-406;2001.
56. Large RG. Prediction of treatment response in pain patients: the illness self-concept repertory grid and EMG feedback. Pain. 21:279-287, 1985.
57. Flor H, Schugens MM, Birbaumer N. Discrimination of muscle tension in chronic pain patients and healthy controls. Biofeedback Self regul. 17:165-177, 1992.
58. Flor H, Birbaumer N, Schugens MM, Lutzengerger W. Symptom-specific psychophysiological responses in chronic pain patients. Psychophysiology. 29:452-460, 1992.
59. Flor H, Birbaumer N. Comparison of the efficacy of Electromyographic biofeedback, cognitive-behavior therapy, and conservative medical interventions in the treatment of chronic musculoskeletal pain. J Consult Clin Psychol. 61:653-658, 1993.
60. Geisser ME, Robinson ME, Richardson C. A time series analysis of the relationship between ambulatory EMG, pain, and stress in chronic low back pain. Biofeedback Self Regul. 20:339-355, 1995.
61. Arena JG, Sherman RA, Bruno GM, Young TR. Electromyographic recordings of 5 types of low back pain subjects and non-pain controls in different positions. Pain. 1989 Apr;37(1):57-65.
62. Wolf S.L. Bobinac-Georgievski A. Vlado Braus V. Montani M. Electrokinesiologic measurement of trunk sagittal mobility and lumbar erector spinae muscle activity. Journal of Rehabilitation Research and Development Vol. 34 No. 4, Oct. 1997 Pages 470-478.
63. Kuriyama N. Hiromoto I. Electromyographic Analysis of the Lumbar Spinal Muscles with Low Back Pain. J Nippon med Sch 2005;72(3)
64. Kasman GS, Cram JR, Wolf SL. Clinical Applications in Surface Electromyography: Chronic Musculoskeletal Pain. Gaithersburg, MD: Aspen Publishers, 1998.
70
Clinical Sequence Assessments and SEMG Feedback
Hip Region Investigations of hip musculature with EMG date back more than 50 years.1 Needle EMG has been used to document compartmentalization and/or functional differentiation within hip musculature.2,3 This and additional research using both surface and indwelling electrodes has been conducted examining hip musculature during various exercises which, could serve as a basis for improving the design and specificity of therapeutic exercises.4,5 Relationships of timing between extremity, trunk and hip musculature related to stability has been investigated with Surface and percutaneous EMG.6-8 There is also research that examines the hip musculature during gait 9 and recent kinesiological studies published related to hip prosthetics.10,11 In one interesting case series, decreased intramuscular EMG activity from gluteus maximus and gluteus medius muscles as well as aberrant tonic activity from tensor fascia lata, rectus femoris, and adductor longus was identified during gait analysis in patients with osteoarthritis who were to undergo total hip arthoplasty.12 SEMG has also been used to monitor return of hip abductor function post neurologic insult.13
These findings would seem to be consistent with the clinical theory of Sahrmann14 who provides a classification and intervention framework for muscle imbalance syndromes around the hip and body regions.15 As with other muscle imbalance impairment syndromes, scientific evidence is being gathered that appear to adhere to Sahrmann’s classifications,16,17 and are available in others texts,18 but would benefit from additional research. Compared to that of the other regions covered in this booklet, there is a dearth of reports pertaining to the hip in the clinical realm. Imbalances among the gluteus maximus and hamstring muscles, or gluteus medius and tensor fascia lata, for example, may be amenable to SEMG assessment and feedback training. Recordings from the deep lateral rotators of the hip, such as the piriformis, are not feasible with SEMG.
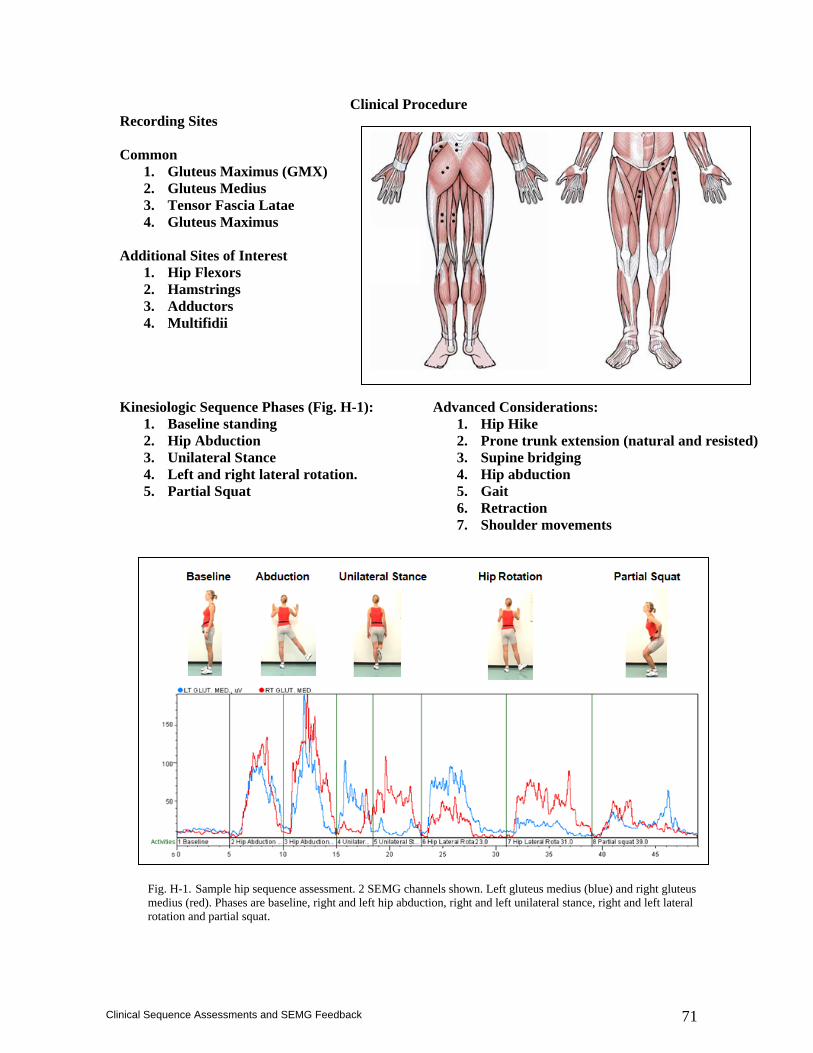
71
Clinical Sequence Assessments and SEMG Feedback
Clinical Procedure Recording Sites Common
1. Gluteus Maximus (GMX) 2. Gluteus Medius 3. Tensor Fascia Latae 4. Gluteus Maximus
Additional Sites of Interest
1. Hip Flexors 2. Hamstrings 3. Adductors 4. Multifidii
Kinesiologic Sequence Phases (Fig. H-1):
1. Baseline standing 2. Hip Abduction 3. Unilateral Stance 4. Left and right lateral rotation. 5. Partial Squat
Advanced Considerations: 1. Hip Hike 2. Prone trunk extension (natural and resisted) 3. Supine bridging 4. Hip abduction 5. Gait 6. Retraction 7. Shoulder movements
Fig. H-1. Sample hip sequence assessment. 2 SEMG channels shown. Left gluteus medius (blue) and right gluteus medius (red). Phases are baseline, right and left hip abduction, right and left unilateral stance, right and left lateral rotation and partial squat.
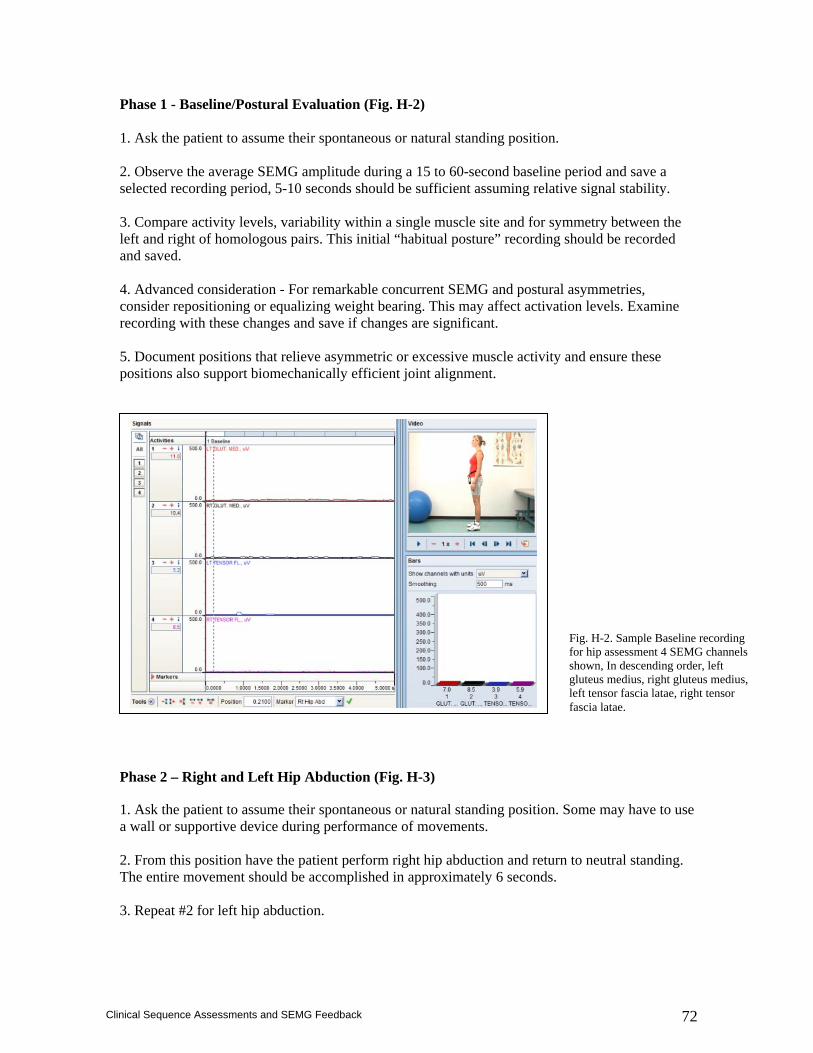
72
Clinical Sequence Assessments and SEMG Feedback
Phase 1 - Baseline/Postural Evaluation (Fig. H-2) 1. Ask the patient to assume their spontaneous or natural standing position. 2. Observe the average SEMG amplitude during a 15 to 60-second baseline period and save a selected recording period, 5-10 seconds should be sufficient assuming relative signal stability. 3. Compare activity levels, variability within a single muscle site and for symmetry between the left and right of homologous pairs. This initial “habitual posture” recording should be recorded and saved. 4. Advanced consideration - For remarkable concurrent SEMG and postural asymmetries, consider repositioning or equalizing weight bearing. This may affect activation levels. Examine recording with these changes and save if changes are significant. 5. Document positions that relieve asymmetric or excessive muscle activity and ensure these positions also support biomechanically efficient joint alignment.
Phase 2 – Right and Left Hip Abduction (Fig. H-3)
1. Ask the patient to assume their spontaneous or natural standing position. Some may have to use a wall or supportive device during performance of movements. 2. From this position have the patient perform right hip abduction and return to neutral standing. The entire movement should be accomplished in approximately 6 seconds. 3. Repeat #2 for left hip abduction.
Fig. H-2. Sample Baseline recording for hip assessment 4 SEMG channels shown, In descending order, left gluteus medius, right gluteus medius, left tensor fascia latae, right tensor fascia latae.
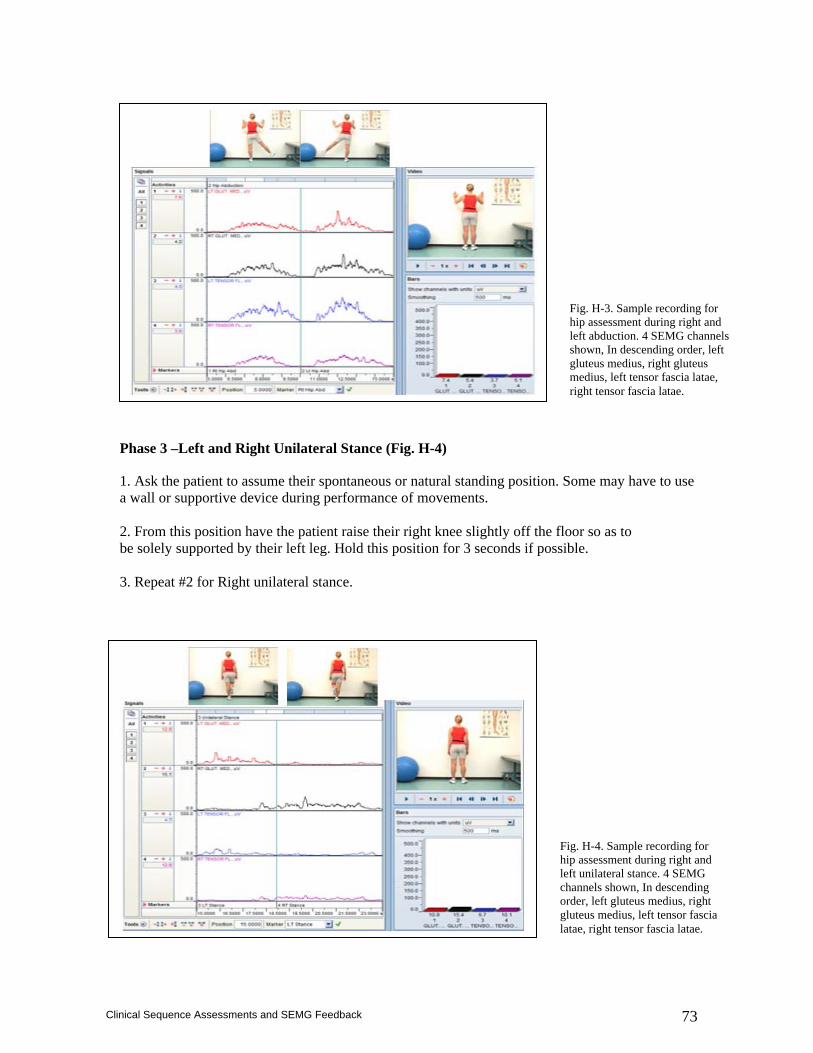
73
Clinical Sequence Assessments and SEMG Feedback
Phase 3 –Left and Right Unilateral Stance (Fig. H-4)
1. Ask the patient to assume their spontaneous or natural standing position. Some may have to use a wall or supportive device during performance of movements. 2. From this position have the patient raise their right knee slightly off the floor so as to be solely supported by their left leg. Hold this position for 3 seconds if possible. 3. Repeat #2 for Right unilateral stance.
Fig. H-3. Sample recording for hip assessment during right and left abduction. 4 SEMG channels shown, In descending order, left gluteus medius, right gluteus medius, left tensor fascia latae, right tensor fascia latae.
Fig. H-4. Sample recording for hip assessment during right and left unilateral stance. 4 SEMG channels shown, In descending order, left gluteus medius, right gluteus medius, left tensor fascia latae, right tensor fascia latae.
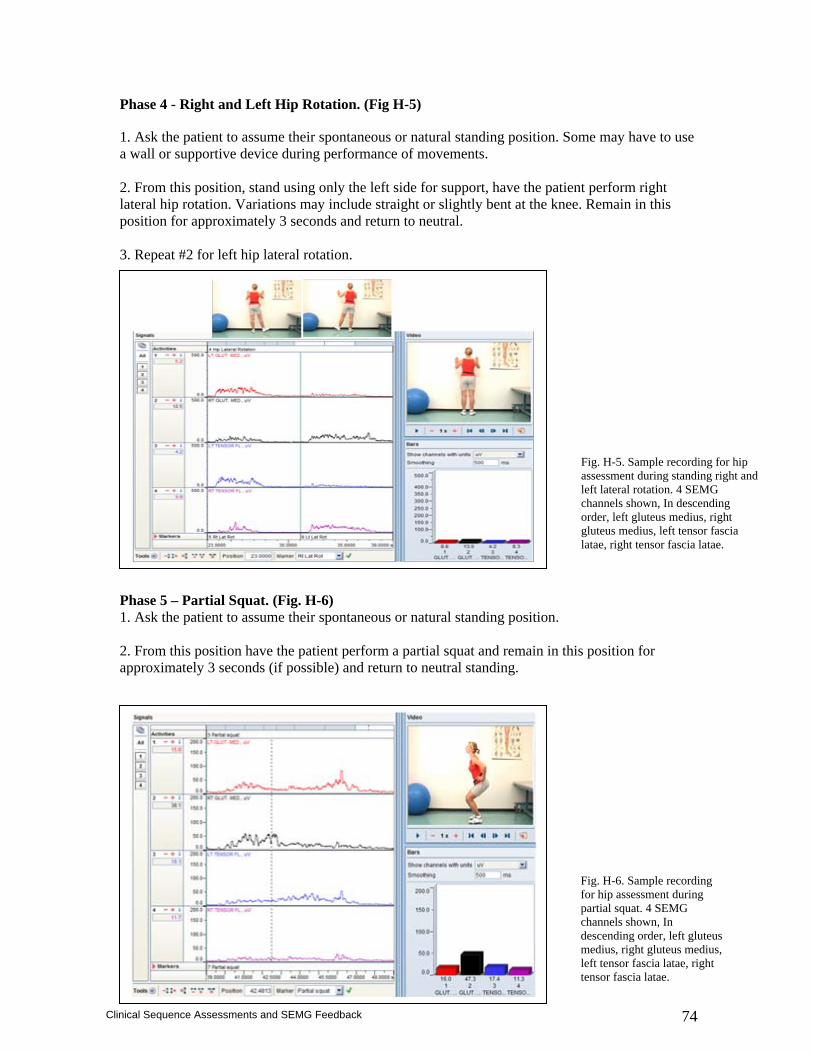
74
Clinical Sequence Assessments and SEMG Feedback
Phase 4 - Right and Left Hip Rotation. (Fig H-5)
1. Ask the patient to assume their spontaneous or natural standing position. Some may have to use a wall or supportive device during performance of movements. 2. From this position, stand using only the left side for support, have the patient perform right lateral hip rotation. Variations may include straight or slightly bent at the knee. Remain in this position for approximately 3 seconds and return to neutral. 3. Repeat #2 for left hip lateral rotation. Phase 5 – Partial Squat. (Fig. H-6) 1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position have the patient perform a partial squat and remain in this position for approximately 3 seconds (if possible) and return to neutral standing.
Fig. H-5. Sample recording for hip assessment during standing right and left lateral rotation. 4 SEMG channels shown, In descending order, left gluteus medius, right gluteus medius, left tensor fascia latae, right tensor fascia latae.
Fig. H-6. Sample recording for hip assessment during partial squat. 4 SEMG channels shown, In descending order, left gluteus medius, right gluteus medius, left tensor fascia latae, right tensor fascia latae.

75
Clinical Sequence Assessments and SEMG Feedback
General Interpretation Considerations Prolonged elevated activity infers an inability for sufficient rest. Elevated amplitudes have been found in hip pain patients9. Symmetrical movement should be represented by symmetrical muscle activity. For example, bilateral muscle activity during a partial squat and return to neutral should be symmetrical from homologous muscle pairs. The most basic elements of SEMG documentation that should accompany interpretation of recording sites are: Baseline activity - Activity that is elevated and/or asymmetrical During left/right Abduction - Activity that is reciprocally asymmetrical > 20% During left/right single leg raise - Activity that is reciprocally asymmetrical > 20% During left/right external rotation - Activity that is reciprocally asymmetrical > 20% During partial squat - Activity that is reciprocally asymmetrical > 20%
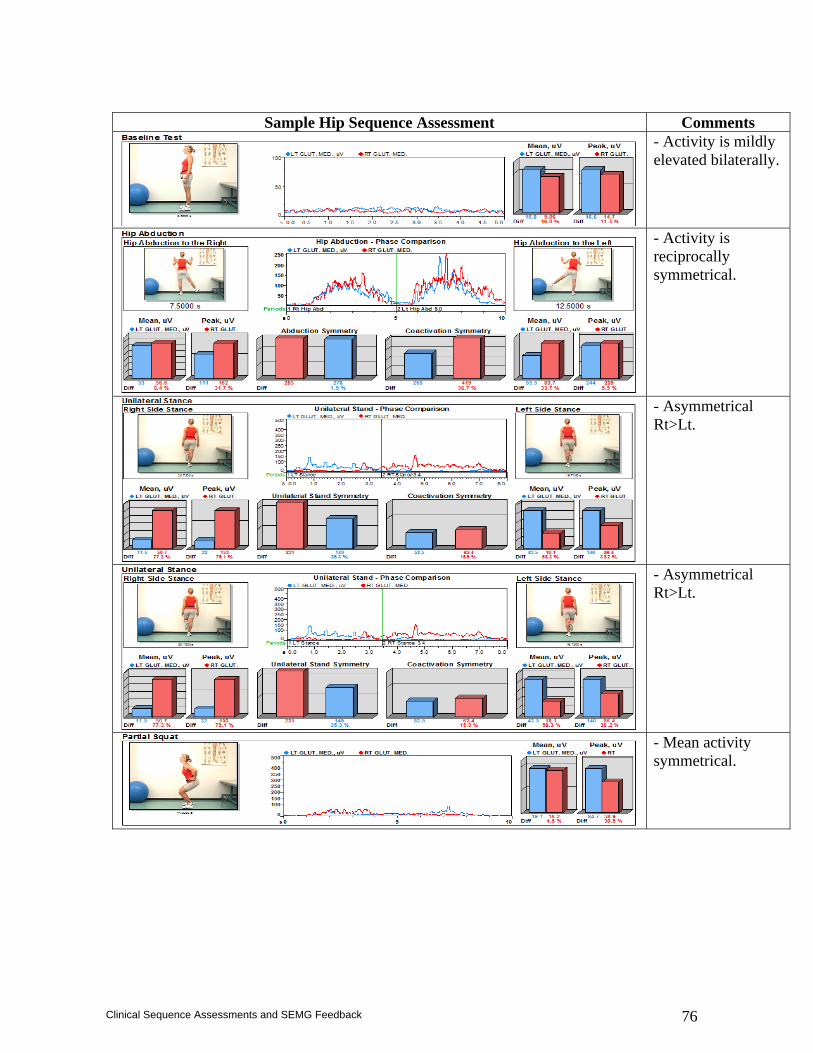
76
Clinical Sequence Assessments and SEMG Feedback
Sample Hip Sequence Assessment Comments
- Activity is mildly elevated bilaterally.
- Activity is reciprocally symmetrical.
- Asymmetrical Rt>Lt.
- Asymmetrical Rt>Lt.
- Mean activity symmetrical.
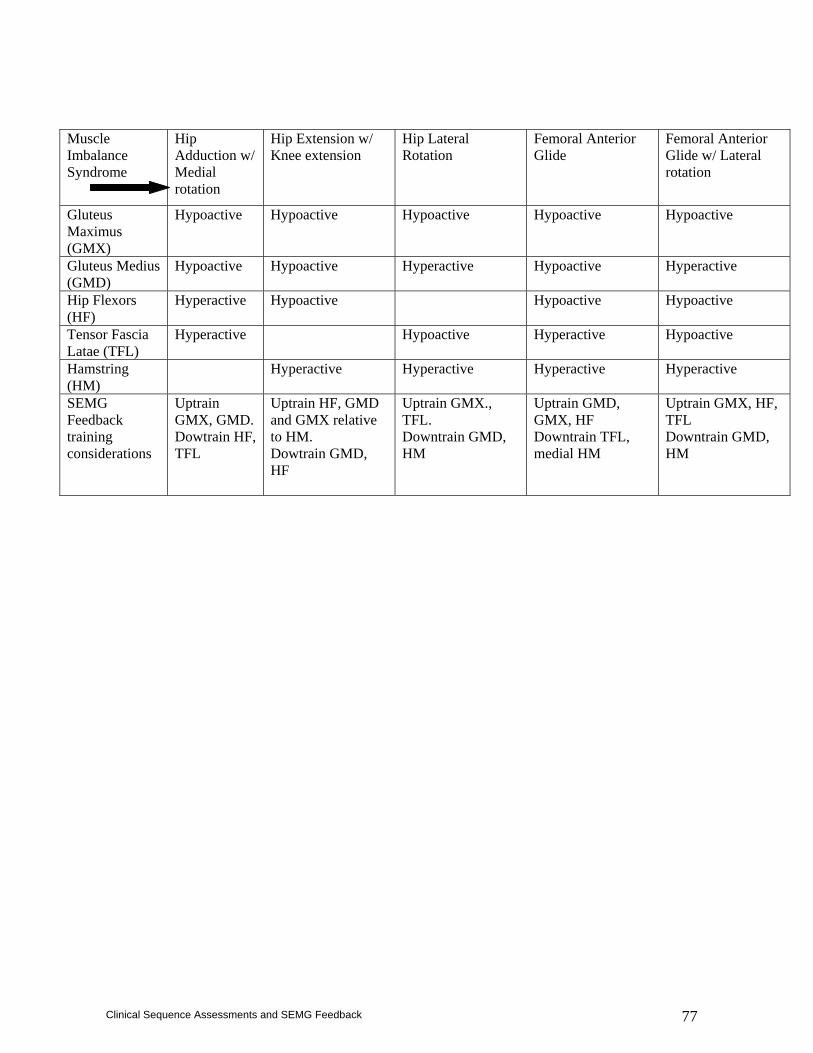
77
Clinical Sequence Assessments and SEMG Feedback
Muscle Imbalance Syndrome
Hip Adduction w/ Medial rotation
Hip Extension w/ Knee extension
Hip Lateral Rotation
Femoral Anterior Glide
Femoral Anterior Glide w/ Lateral rotation
Gluteus Maximus (GMX)
Hypoactive Hypoactive Hypoactive Hypoactive Hypoactive
Gluteus Medius (GMD)
Hypoactive Hypoactive Hyperactive Hypoactive Hyperactive
Hip Flexors (HF)
Hyperactive Hypoactive Hypoactive Hypoactive
Tensor Fascia Latae (TFL)
Hyperactive Hypoactive Hyperactive Hypoactive
Hamstring (HM)
Hyperactive Hyperactive Hyperactive
Hyperactive
SEMG Feedback training considerations
Uptrain GMX, GMD. Dowtrain HF, TFL
Uptrain HF, GMD and GMX relative to HM. Dowtrain GMD, HF
Uptrain GMX., TFL. Downtrain GMD, HM
Uptrain GMD, GMX, HF Downtrain TFL, medial HM
Uptrain GMX, HF, TFL Downtrain GMD, HM
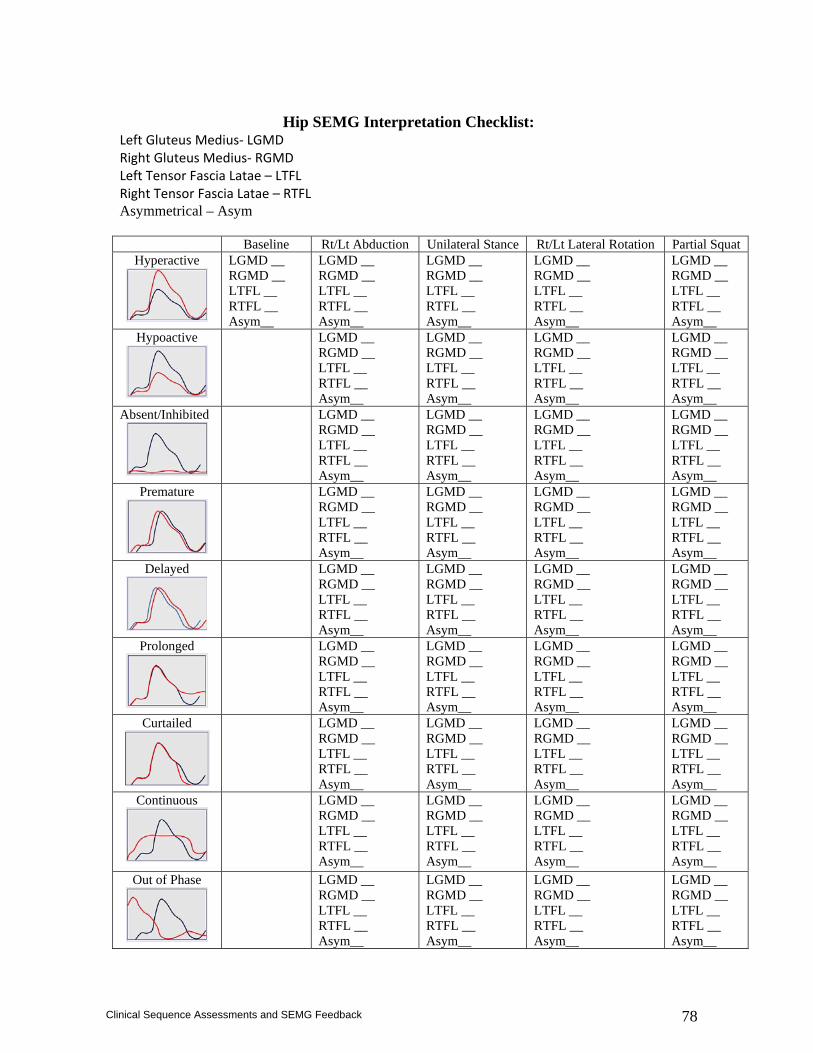
78
Clinical Sequence Assessments and SEMG Feedback
Hip SEMG Interpretation Checklist:
Left Gluteus Medius‐ LGMD Right Gluteus Medius‐ RGMD Left Tensor Fascia Latae – LTFL Right Tensor Fascia Latae – RTFL Asymmetrical – Asym Baseline Rt/Lt Abduction Unilateral Stance Rt/Lt Lateral Rotation Partial Squat
Hyperactive
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
Hypoactive
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
Absent/Inhibited
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
Premature
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
Delayed
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
Prolonged
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
Curtailed
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
Continuous
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
Out of Phase
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__
LGMD __ RGMD __ LTFL __ RTFL __ Asym__

79
Clinical Sequence Assessments and SEMG Feedback
References
1. Basmajian JV, De Luca CJ. Muscles Alive: Their Functions Revealed by Electromyography, 5th ed. Baltimore, MD: Williams & Wilkins; 1985.
2. Functional differentiation within the tensor fasciae latae. A telemetered electromyographic analysis of its locomotor roles. J Bone Joint Surg Am. 1981 Dec;63(9):1457-71.
3. Juker D, McGill S, Kropf P, Steffen T. Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdominal wall during a wide variety of tasks. Med Sci SportsExerc.1998Feb;30(2):301-10.
4. Andersson EA, Nilsson J, Ma Z, Thorstensson A. Abdominal and hip flexor muscle activation during various training exercises. Eur J Appl Physiol Occup Physiol.1997;75(2):115-23.
5. Arokoski JP, Kankaanpaa M, Valta T, Juvonen I, Partanen J, Taimela S, Lindgren KA, Airaksinen O. Back and hip extensor muscle function during therapeutic exercises. Arch Phys Med Rehabil. 1999 Jul;80(7):842-50.
6. Andersson E, Oddsson L, Grundstrom H, Thorstensson A. The role of the psoas and iliacus muscles for stability and movement of the lumbar spine, pelvis and hip. Scand J Med Sci Sports. 1995 Feb;5(1):10-6.
7. Hodges PW, Richardson CA. Contraction of the abdominal muscles associated with movement of the lower limb. Phys Ther. 1997 Feb;77(2):132-42; discussion 142-4.
8. Hodges PW, Richardson CA. Contraction of the abdominal muscles associated with movement of the lower limb. Phys Ther. 1997 Feb;77(2):132-42; discussion 142-4.
9. Winter DA, MacKinnon CD, Ruder GK, Wieman C. An integrated EMG/biomechanical model of upper body balance and posture during human gait. Prog Brain Res. 1993;97:359-67.
10. Neumann, DA. An electromyographic study of the hip abductor muscles as subjects with a hip prosthesis walked with different methods of using a cane and carrying a load. Phys Ther. 79:1163-1173;1999.
11. Neumann DA. Hip abductor muscle activity as subjects with hip prostheses walk with different methods of using a cane. Phys Ther. 78:490-501;1998.
12. Long WT, Dorr LD, Healy B, Perry J. Functional recovery of non-cemented total hip arthoplasty. Clin Orthop. 288:73-77;1993.
13. Kirker SG, Jenner JR, Simpson DS, Wing AM. Changing patterns of postural hip muscle activity during recovery from stroke. Clin Rehabil. 2000 Dec;14(6):618-26.
14. Sahrmann SA. Diagnosis and Treatment of Movement Impairment Syndromes, St Louis: Mosby;2002.
15. Knapik JJ, Bauman CL, Jones BH, Harris JM, Vaughan L. Preseason strength and flexibility imbalances associated with athletic injuries in female collegiate athletes. Am J SportsMed.1991Jan-Feb;19(1):76-81.
16. Nadler SF, Malanga GA, Feinberg JH, Prybicien M, Stitik TP, DePrince M. Relationship between hip muscle imbalance and occurrence of low back pain in collegiate athletes: a prospective study. Am J Phys Med Rehabil. 2001 Aug;80(8):572-7.
17. Nadler SF, Malanga GA, DePrince M, Stitik TP, Feinberg JH. The relationship between lower extremity injury, low back pain, and hip muscle strength in male and female collegiate athletes. Clin J Sport Med. 2000 Apr;10(2):89-97.
18. Hall CM, Brody LT. Therapeutic Exercise Moving Toward Function, Philadelphia: Lippincott Williams and Wilkins; 1999.

80
Clinical Sequence Assessments and SEMG Feedback
Knee Region A large volume of literature relates to clinical SEMG studies of knee musculature. Investigations pertain principally to one of three areas: general knee rehabilitation, muscle function following anterior cruciate ligament injury, and patellofemoral dysfunction. Early studies found SEMG feedback plus exercise superior to exercise alone for normal subjects,1 patients with osteoarthritis, post-meniscectomy, and post-arthroscopy2-5 and post ACL reconstruction. More recent studies found that in patellofemoral pain groups, mean contraction activity in the biofeedback group of the vastus medialis muscles in 3 monthly measurements, and the vastus lateralis muscles at the end of the first month, were significantly higher than those of the control group.6 Although monthly follow-ups did not result in greater clinical improvement when compared with a conventional exercise program, the improvements in SEMG in the treatment group indicate that neural factors accounted for the increase in muscle activity and it may be inferred that novel motor programs may be acquired prior to that of using conventional exercise regimes alone. With these patient populations, SEMG can also be used to document left/right differences during the evaluation process as well as the rehabilitative course of post-operative or non-operative care. Exercise variants can be examined for those that have the optimal effect and then incorporated into home programs. SEMG feedback can be combined with routine exercise protocols to enhance motivation, muscle recruitment, and exercise technique. Injuries to the anterior cruciate ligament result in altered patterns of muscle activity about the knee7-9. SEMG feedback combined with exercise has been used to ameliorate post-surgical inhibition and promote recovery of torque production in a manner superior to exercise alone or exercise plus cutaneous electrical stimulation.10,11. Patients with unrepaired tears of the anterior cruciate ligament spontaneously show increased hamstring and hamstring:quadriceps SEMG activity during stance.12-14 Increased hamstring activation may biomechanically support the intrinsic arthrokinematic role of the anterior cruciate ligament and training for increased hamstring:quadriceps coactivation as has been suggested in a case report.15 This theory supports earlier work where in a small group of subjects mean coactivation of normal limb hamstring activity averaged twice that of the involved ACL limb. This suggests that asymmetry in hamstring coactivation during knee extension may result from ACL dysfunction.16 In an analogous way, the gastrocnemius muscle has also been implicated in contributing to the functional stability in the ACL deficient knee.17 SEMG feedback has been recommended to train the magnitude and timing of the medial gastrocnemius during treadmill walking in patients with anterior cruciate deficiencies and lower functional ability, in a manner that matches spontaneous SEMG patterns displayed by patients with unrepaired tears of the anterior cruciate ligament who report higher life function .18
81
Clinical Sequence Assessments and SEMG Feedback
More recently, SEMG frequency analysis has been used to generate recommendations for strengthening versus endurance training in patients following operative repair of anterior cruciate ligament tears.19 Further, SEMG amplitude and frequency has also been used as a predictor of expected residual quadriceps muscle weakness prior to anterior cruciate ligament reconstruction.20 Imbalanced action of the vastus medialis oblique compared with the vastus lateralis has long been assumed by clinicians to play a role in excessive lateral tracking of the patella and patellofemoral pain. This postulate seems reasonable on the basis of anatomical and kinesiological considerations and numerous investigators have sought to resolve the issue. Some authors have reported a decreased ratio of vastus medialis oblique amplitude relative to that of the vastus lateralis, or other measures of vastus medialis oblique insufficiency, in knees with patellofemoral dysfunction.21 Other experimenters have found a nonselective depression of vastus medialis oblique and vastus lateralis amplitude variables. Yet other investigators have failed to find any difference in recorded muscle activity between healthy control and patellofemoral knees. Consistently, healthy control subjects show normalized vastus medialis oblique:vastus lateralis amplitude ratios of about 1.0 + 0.4, but the functional significance of that point , if any, is not clear. Certainly, there is no systematic evidence that dysfunction of the vastus medialis oblique is linked to patellofemoral dysfunction in the majority of studied subjects.22 The situation is further clouded by lack of a standardized patient classification system, limitations in SEMG amplitude normalization methods, and differences in experimental design. It may be that the activity of the vastus medialis oblique is largely irrelevant to the development and maintenance of patellofemoral dysfunction. Alternatively, dysfunction of the vastus medialis oblique may be an important factor in a subclass of patients or when combined with other etiological factors. SEMG frequency analysis may help elucidate whether the vastus medialis oblique and vastus lateralis muscles display similar or different fatigue characteristics in patients with patellofemoral pain versus healthy controls.23 Further, it has been purported that patients with PFPS may possess a temporal delay in the relationship between the VMO and VL during stair stepping.24 The activity of the vastus medialis longus muscle may prove to be more significant than clinically presumed and greater vastus medialis longus:vastus lateralis. SEMG amplitude ratios have been associated with (not necessarily causal to) increased lateral patellar glide.25 Clinicians should not assume the vastus medialis oblique to be a problem and should avoid feedback training protocols for uptraining the vastus medialis oblique, unless a deficit is demonstrated convincingly during SEMG examination. Numerous exercises have been purported by clinicians to selectively facilitate recruitment of the vastus medialis oblique. These have been evaluated exhaustively and with little controversy.26-28
There is no apparent evidence of selective effects on the vastus medialis oblique with quadriceps set, terminal knee extension, straight leg raise, or various combinations and variants of those exercises, including lateral hip rotation as well as tibial rotation. Activity ratios of the vastus medialis oblique:vastus lateralis have tended to be reported at higher values during closed chain compared with open chain activities. It has been suggested that hip adduction combined with
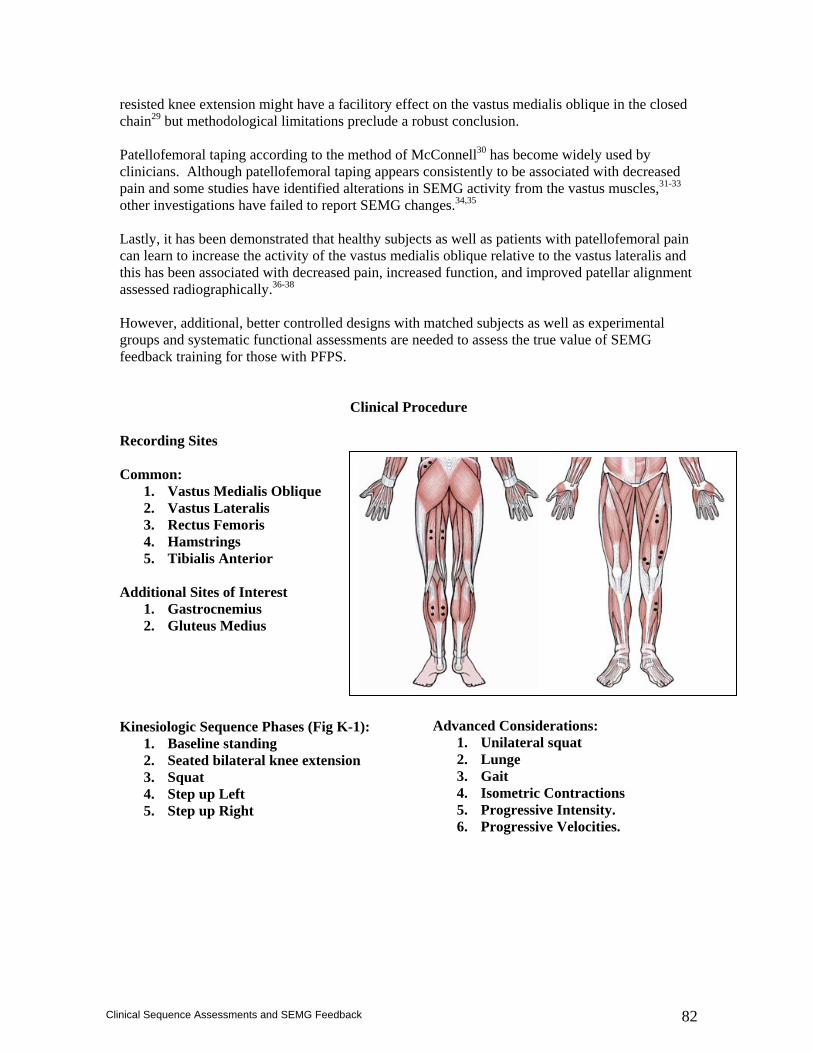
82
Clinical Sequence Assessments and SEMG Feedback
resisted knee extension might have a facilitory effect on the vastus medialis oblique in the closed chain29 but methodological limitations preclude a robust conclusion. Patellofemoral taping according to the method of McConnell30 has become widely used by clinicians. Although patellofemoral taping appears consistently to be associated with decreased pain and some studies have identified alterations in SEMG activity from the vastus muscles,31-33 other investigations have failed to report SEMG changes.34,35 Lastly, it has been demonstrated that healthy subjects as well as patients with patellofemoral pain can learn to increase the activity of the vastus medialis oblique relative to the vastus lateralis and this has been associated with decreased pain, increased function, and improved patellar alignment assessed radiographically.36-38 However, additional, better controlled designs with matched subjects as well as experimental groups and systematic functional assessments are needed to assess the true value of SEMG feedback training for those with PFPS.
Clinical Procedure
Recording Sites Common:
1. Vastus Medialis Oblique 2. Vastus Lateralis 3. Rectus Femoris 4. Hamstrings 5. Tibialis Anterior
Additional Sites of Interest
1. Gastrocnemius 2. Gluteus Medius
Kinesiologic Sequence Phases (Fig K-1):
1. Baseline standing 2. Seated bilateral knee extension 3. Squat 4. Step up Left 5. Step up Right
Advanced Considerations: 1. Unilateral squat 2. Lunge 3. Gait 4. Isometric Contractions 5. Progressive Intensity. 6. Progressive Velocities.
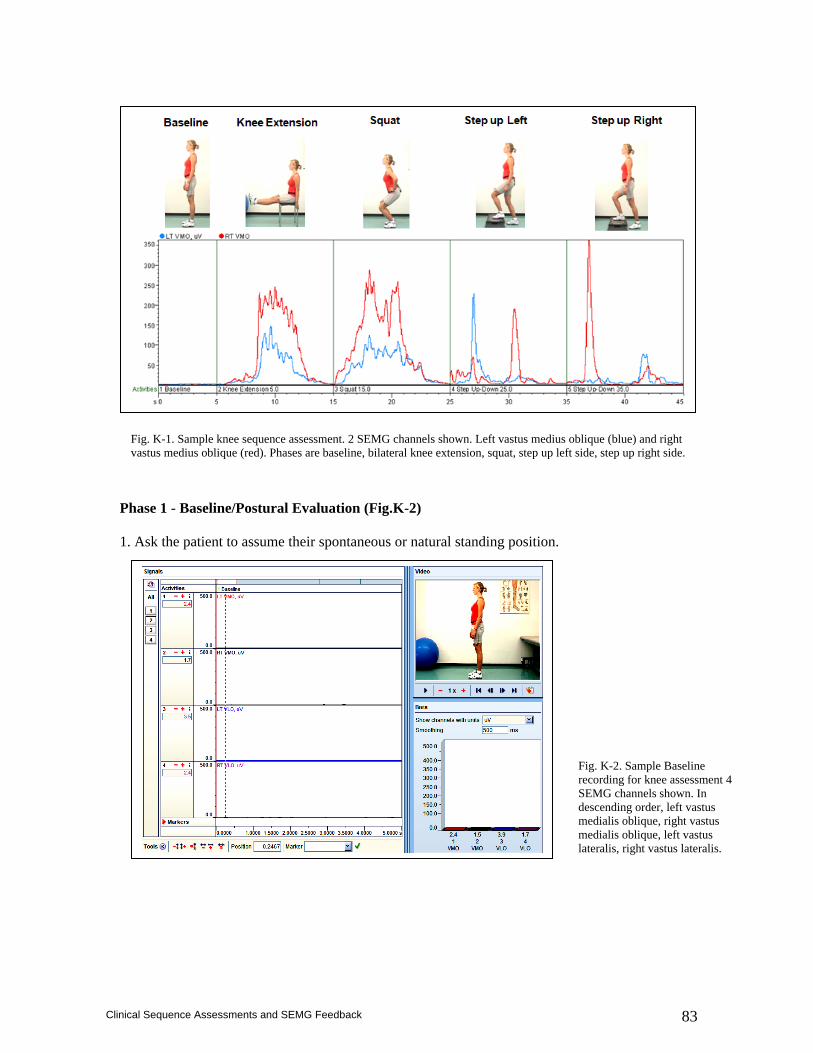
83
Clinical Sequence Assessments and SEMG Feedback
Phase 1 - Baseline/Postural Evaluation (Fig.K-2) 1. Ask the patient to assume their spontaneous or natural standing position.
Fig. K-2. Sample Baseline recording for knee assessment 4 SEMG channels shown. In descending order, left vastus medialis oblique, right vastus medialis oblique, left vastus lateralis, right vastus lateralis.
Fig. K-1. Sample knee sequence assessment. 2 SEMG channels shown. Left vastus medius oblique (blue) and right vastus medius oblique (red). Phases are baseline, bilateral knee extension, squat, step up left side, step up right side.
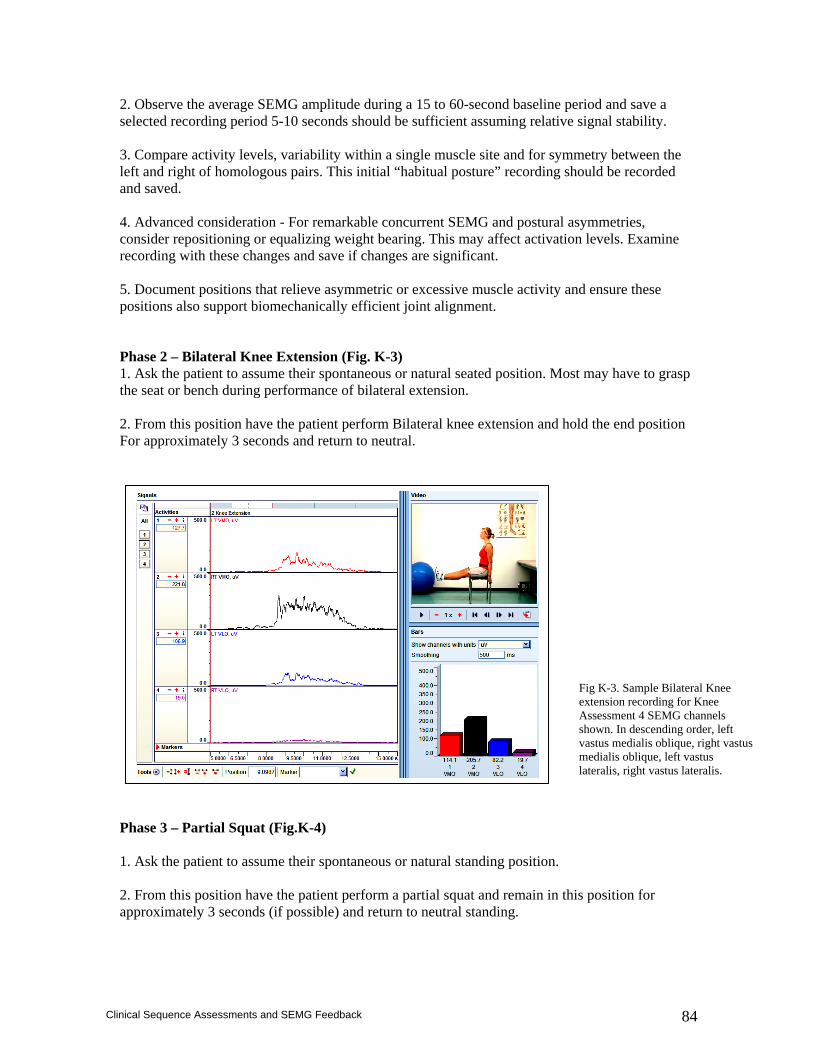
84
Clinical Sequence Assessments and SEMG Feedback
2. Observe the average SEMG amplitude during a 15 to 60-second baseline period and save a selected recording period 5-10 seconds should be sufficient assuming relative signal stability. 3. Compare activity levels, variability within a single muscle site and for symmetry between the left and right of homologous pairs. This initial “habitual posture” recording should be recorded and saved. 4. Advanced consideration - For remarkable concurrent SEMG and postural asymmetries, consider repositioning or equalizing weight bearing. This may affect activation levels. Examine recording with these changes and save if changes are significant. 5. Document positions that relieve asymmetric or excessive muscle activity and ensure these positions also support biomechanically efficient joint alignment. Phase 2 – Bilateral Knee Extension (Fig. K-3) 1. Ask the patient to assume their spontaneous or natural seated position. Most may have to grasp the seat or bench during performance of bilateral extension. 2. From this position have the patient perform Bilateral knee extension and hold the end position For approximately 3 seconds and return to neutral. Phase 3 – Partial Squat (Fig.K-4) 1. Ask the patient to assume their spontaneous or natural standing position. 2. From this position have the patient perform a partial squat and remain in this position for approximately 3 seconds (if possible) and return to neutral standing.
Fig K-3. Sample Bilateral Knee extension recording for Knee Assessment 4 SEMG channels shown. In descending order, left vastus medialis oblique, right vastus medialis oblique, left vastus lateralis, right vastus lateralis.
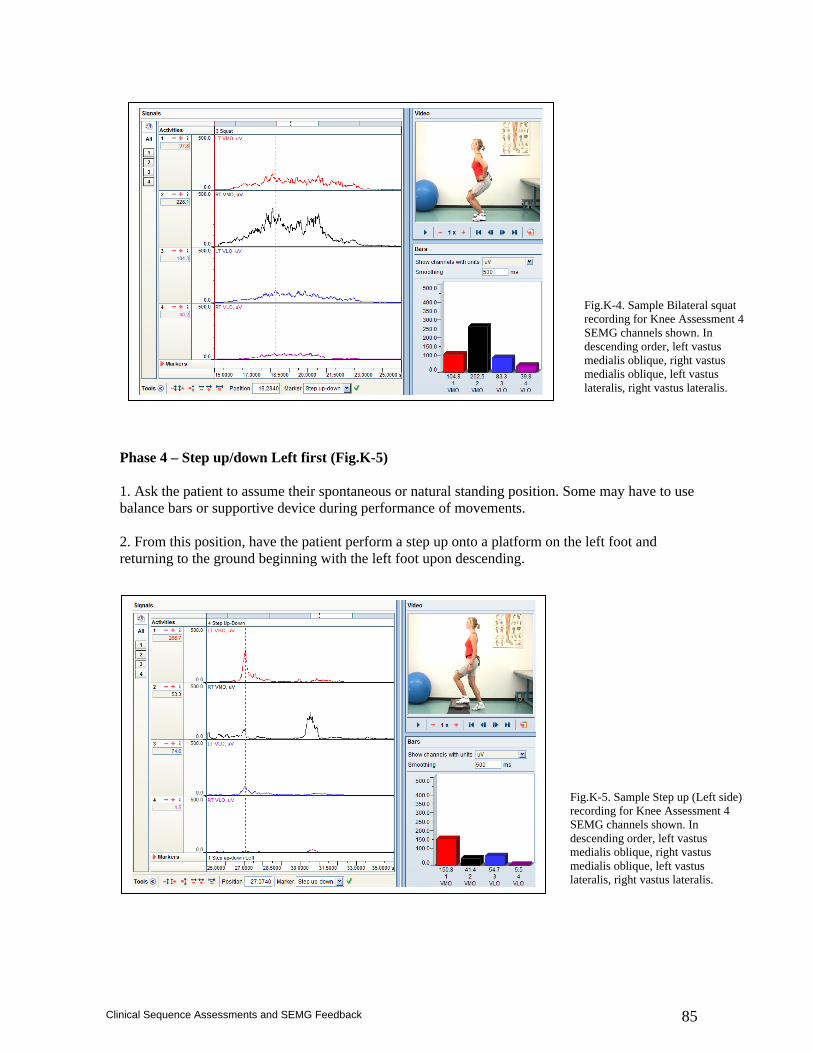
85
Clinical Sequence Assessments and SEMG Feedback
Phase 4 – Step up/down Left first (Fig.K-5) 1. Ask the patient to assume their spontaneous or natural standing position. Some may have to use balance bars or supportive device during performance of movements. 2. From this position, have the patient perform a step up onto a platform on the left foot and returning to the ground beginning with the left foot upon descending.
Fig.K-4. Sample Bilateral squat recording for Knee Assessment 4 SEMG channels shown. In descending order, left vastus medialis oblique, right vastus medialis oblique, left vastus lateralis, right vastus lateralis.
Fig.K-5. Sample Step up (Left side) recording for Knee Assessment 4 SEMG channels shown. In descending order, left vastus medialis oblique, right vastus medialis oblique, left vastus lateralis, right vastus lateralis.
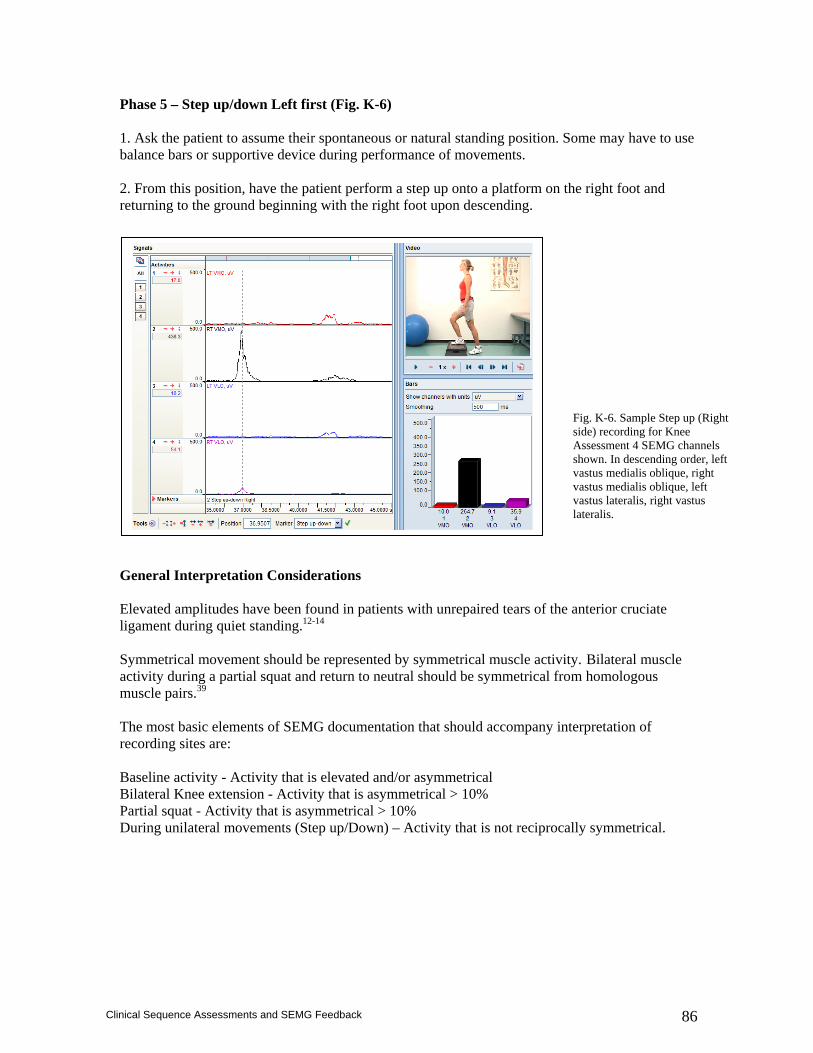
86
Clinical Sequence Assessments and SEMG Feedback
Phase 5 – Step up/down Left first (Fig. K-6) 1. Ask the patient to assume their spontaneous or natural standing position. Some may have to use balance bars or supportive device during performance of movements. 2. From this position, have the patient perform a step up onto a platform on the right foot and returning to the ground beginning with the right foot upon descending. General Interpretation Considerations Elevated amplitudes have been found in patients with unrepaired tears of the anterior cruciate ligament during quiet standing.12-14 Symmetrical movement should be represented by symmetrical muscle activity. Bilateral muscle activity during a partial squat and return to neutral should be symmetrical from homologous muscle pairs.39 The most basic elements of SEMG documentation that should accompany interpretation of recording sites are: Baseline activity - Activity that is elevated and/or asymmetrical Bilateral Knee extension - Activity that is asymmetrical > 10% Partial squat - Activity that is asymmetrical > 10% During unilateral movements (Step up/Down) – Activity that is not reciprocally symmetrical.
Fig. K-6. Sample Step up (Right side) recording for Knee Assessment 4 SEMG channels shown. In descending order, left vastus medialis oblique, right vastus medialis oblique, left vastus lateralis, right vastus lateralis.
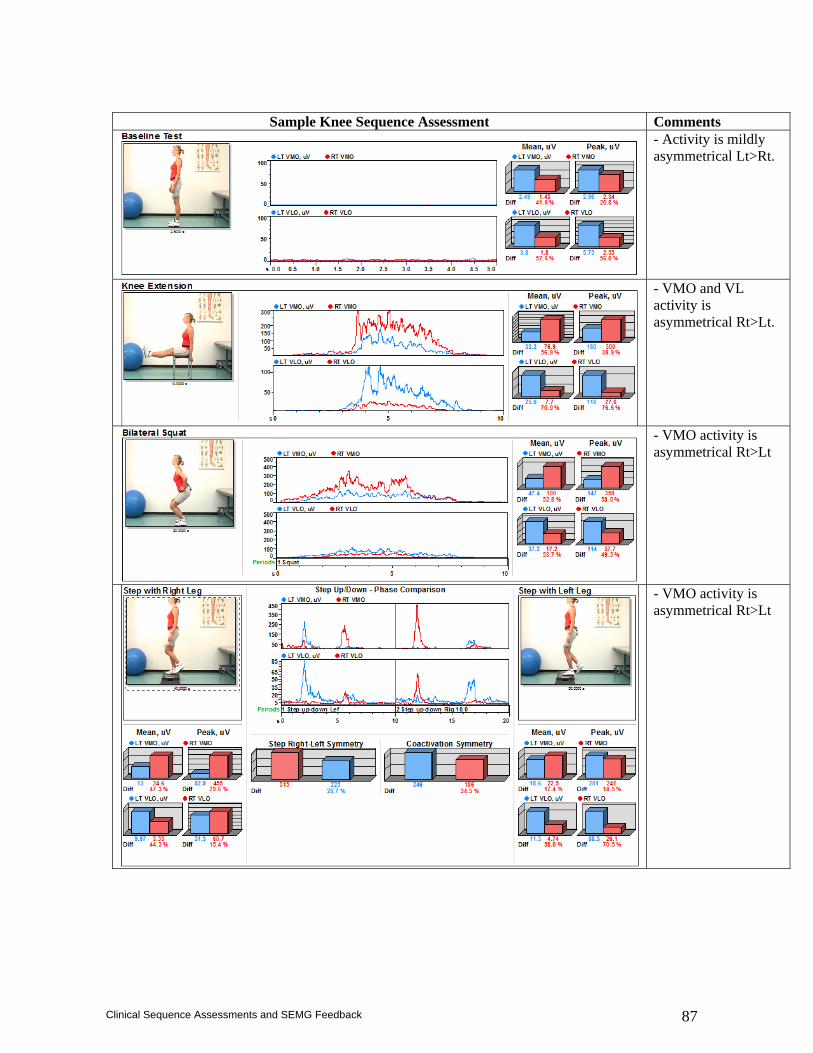
87
Clinical Sequence Assessments and SEMG Feedback
Sample Knee Sequence Assessment Comments
- Activity is mildly asymmetrical Lt>Rt.
- VMO and VL activity is asymmetrical Rt>Lt.
- VMO activity is asymmetrical Rt>Lt
- VMO activity is asymmetrical Rt>Lt
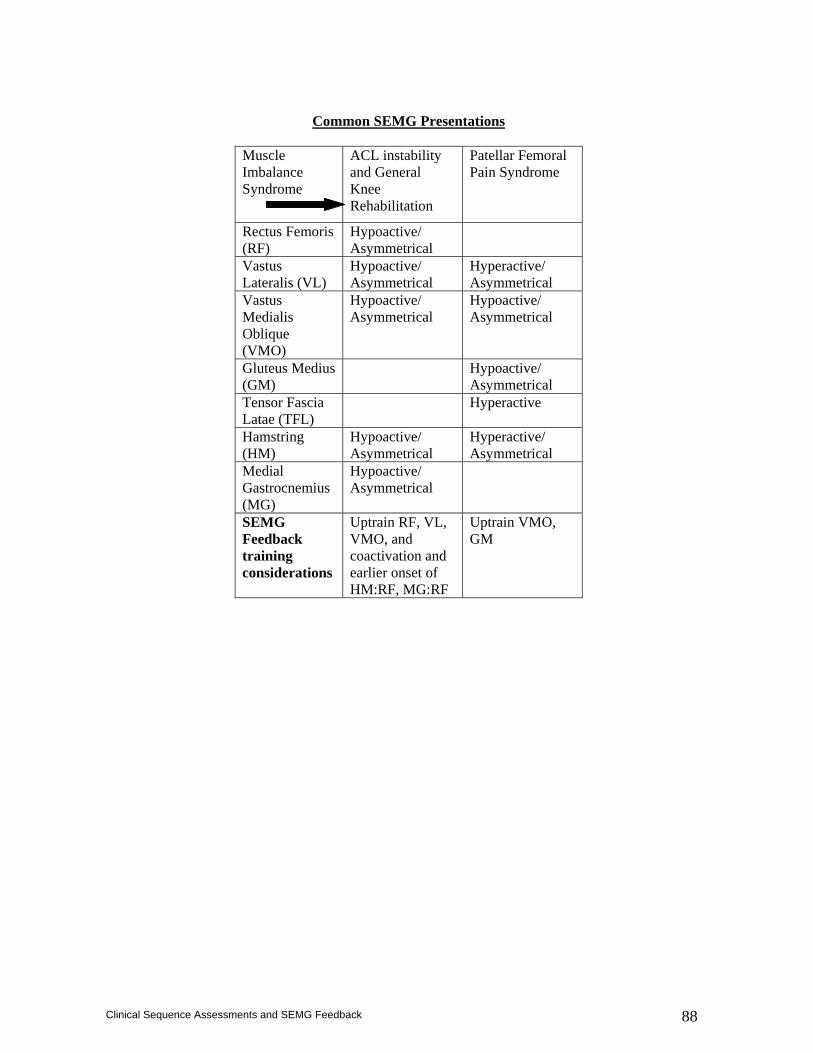
88
Clinical Sequence Assessments and SEMG Feedback
Common SEMG Presentations
Muscle Imbalance Syndrome
ACL instability and General Knee Rehabilitation
Patellar Femoral Pain Syndrome
Rectus Femoris (RF)
Hypoactive/ Asymmetrical
Vastus Lateralis (VL)
Hypoactive/ Asymmetrical
Hyperactive/ Asymmetrical
Vastus Medialis Oblique (VMO)
Hypoactive/ Asymmetrical
Hypoactive/ Asymmetrical
Gluteus Medius (GM)
Hypoactive/ Asymmetrical
Tensor Fascia Latae (TFL)
Hyperactive
Hamstring (HM)
Hypoactive/ Asymmetrical
Hyperactive/ Asymmetrical
Medial Gastrocnemius (MG)
Hypoactive/ Asymmetrical
SEMG Feedback training considerations
Uptrain RF, VL, VMO, and coactivation and earlier onset of HM:RF, MG:RF
Uptrain VMO, GM
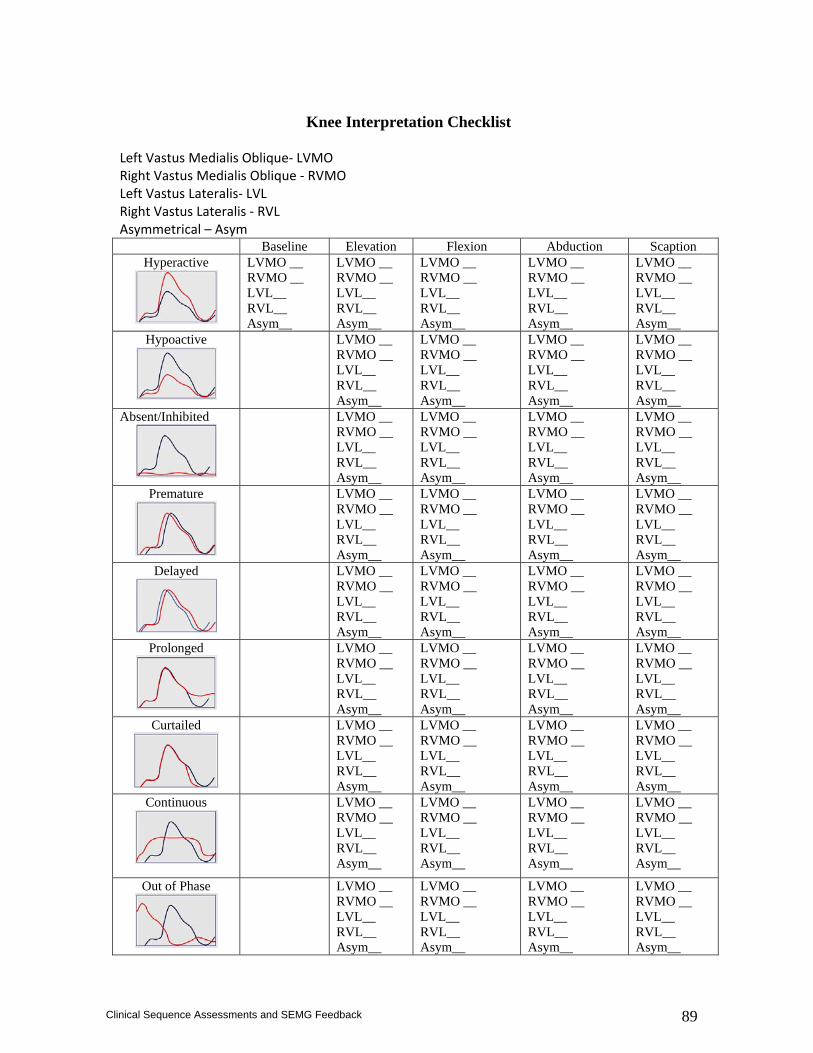
89
Clinical Sequence Assessments and SEMG Feedback
Knee Interpretation Checklist
Left Vastus Medialis Oblique‐ LVMO Right Vastus Medialis Oblique ‐ RVMO Left Vastus Lateralis‐ LVL Right Vastus Lateralis ‐ RVL Asymmetrical – Asym Baseline Elevation Flexion Abduction Scaption
Hyperactive
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
Hypoactive
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
Absent/Inhibited
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
Premature
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
Delayed
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
Prolonged
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
Curtailed
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
Continuous
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
Out of Phase
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
LVMO __ RVMO __ LVL__ RVL__ Asym__
90
Clinical Sequence Assessments and SEMG Feedback
References
1. Croce RV. The effects of EMG biofeedback on strength acquisition. Biofeedback Self Regul. 1986 Dec;11(4):299-310.
2. King AC, Ahles TA, Martin JE, White R. EMG biofeedback-controlled exercise in chronic arthritic knee pain. Arch Phys Med Rehabil. 65:341-343; 1984.
3. Levitt R, Deisenger JA, Remondet Wall J, Ford L, Cassisi JE. EMG feedback-assisted postoperative rehabilitation of minor arthroscopic knee surgeries. J Sports Med Phys Fitness. 35:218-223;1995.
4. Lucca JA, Recchiuti SJ. Effect of Electromyographic biofeedback on an isometric strengthening program. 63:200-203;p 1983.
5. Sprenger CK, Carlson K, Wessman HC. Application of electromyographic biofeedback following medial menisectomy. Phys Ther. 59:167-169; 1979.
6. Dursun N, Dursun E, Kilic Z. Electromyographic biofeedback-controlled exercise versus conservative care for patellofemoral pain syndrome. Arch Phys Med Rehabil. 2001 Dec;82(12):1692-5.
7. Branch TP, Hunter R, Donath M. Dynamic EMG analysis of anterior cruciate deficient legs with and without bracing during cutting. Am J Sports Med. 17:35-41; 1989.
8. Ciccotti MG, Kerlan RK, Perry J, Pink M. An Electromyographic analysis of the knee during functional activities, II: the anterior cruciate ligament-deficient and –reconstructed profiles. Am J Sports Med. 22:651-658; 1994.
9. Tibone JE, Antich TJ, Fant0on GS, Moynes DR, Perry J. Functional analysis of anterior cruciate ligament instability. Am J Sports Med. 14:276-283; 1986.
10. Draper V. Electromyographic biofeedback and recovery of quadriceps femoris muscles function following anterior cruciate ligament reconstruction. Phys Ther. 9:11-17; 1990.
11. Draper B, Ballard L. Electrical stimulation versus Electromyographic biofeedback in the recovery of quadriceps femoris muscles function following anterior cruciate ligament surgery. Phys Ther. 71:455-463; 1991.
12. Bulgheroni P, Bulgheroni MV, Andrini L, Guffanti P, Giughello A. Gait patterns after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 5:14-21;1997.
13. Devita P, Hortobagyi T, Barrier J, Torry M, Glover KL, Speroni DL, Money J, Mahar MT. Gait adaptations before and after anterior cruciate ligament reconstruction surgery. Med Sci Sports Exerc. 1997 Jul;29(7):853-9.
14. Boerboom AL, Hof AL, Halbertsma JP, van Raaij JJ, Schenk W, Diercks RL, van Horn JR. Atypical hamstrings electromyographic activity as a compensatory mechanism in anterior cruciate ligament deficiency. Knee Surg Sports Traumatol Arthrosc. 2001 Jul;9(4):211-6.
15. Maitland ME, Ajemian SV, Suter E. Quadriceps femoris and hamstring muscle function in a person with an unstable knee. Phys Ther. 79:66-75;1999.
16. Osternig LR, Caster BL, James CR. Contralateral hamstring (biceps femoris) coactivation patterns and anterior cruciate ligament dysfunction. Med Sci Sports Exerc. 1995 Jun;27(6):805-8.
17. Lass P, Kaalund S, leFevre S, Arendt-Nielsen L, Sinkjaer T, Simonsen O. Muscle coordination following rupture of the anterior cruciate ligament. Electromyographic studies of 14 patients. Acta Orthop Scand. 1991 Feb;62(1):9-14.
18. Sinkjaer T. Arendt-Nielsen L. Knee stability and muscle coordination in patients with anterior cruciate ligament injuries: an Electromyographic approach. J Electromyogr Kinesiol.1:209-217; 1991.
19. McHugh MP, Tyler TF, Nicholas SJ, Nrowne MG, Gleim GW. Electromyographic analysis of quadriceps fatigue after ACL reconstruction. J Ortho Sports Phys Ther. 31:25-31; 2001.
20. McHugh MP, Tyler TF, Browne MG, Gleim GW, Nicholas SJ. Electromyographic predictors of residual quadriceps muscle weakness after anterior cruciate ligament reconstruction. Am J Sports Med. 2002 May-Jun;30(3):334-9.
21. Kasman GS. Surface electromyography and patellofemoral dysfunction. In Grelsamer RP, McConnell J, eds. The Patella: A Team Approach. Gaithersburg, MD: Aspen Publishers, 1998; 137-176.
91
Clinical Sequence Assessments and SEMG Feedback
22. Powers, CM. J rehabilitation of patellofemoral joint disorders: a critical review. J Orthop Sports Phys Ther. 28:345-354; 1998.
23. Callaghan MJ, McCarthy CJ, Oldham JA. Electromyographic fatigue characteristics of the quadriceps in patellofemoral pain syndrome. Man Ther. 6:27-33;2001.
24. Cowan SM, Bennell KL, Hodges PW, Crossley KM, McConnell J. Delayed onset of electromyographic activity of vastus medialis obliquus relative to vastus lateralis in subjects with patellofemoral pain syndrome. Arch Phys Med Rehabil. 2001 Feb;82(2):183-9.
25. Powers CM. Patellar kinematics, part I: the influence of vastus muscular activity in subjects with and without patellofemoral pain. Phys Ther. 80:956-964;2000.
26. Callaghan MJ, Oldaham JA. The role of quadriceps exercise in the treatment of patellofemoral pain syndrome. Sports Med. 21:384-391;1996.
27. Laprade J, Culham E, Brouwer B. Comparison of five isometric exercises on the recruitment of the vastus medialis oblique in persons with and without patellofemoral pain syndrome. J Orthop Sports Phys Ther. 3:197-204;p1998.
28. Zakaria D, Harburn KL, Kramer JF. Preferential activation of the vastus medialis oblique, vastus lateralis, and hip adductor muscles during isometric exercises in females. J Orthop Sports Phys Ther. 26:232-28;1997.
29. Hodges P, Richardson C. The influence of isometric hip abduction on quadriceps femoris activity. Scand J Rehabil Med. 25:57-62; 1993.Wise HH, Fiebert IM, Kates J. EMG biofeedback as treatment for patellofemoral pain syndrome. J Orthop Sports Phys Ther. 6:95-103; 1984.
30. McConnell J. The management of chondromalacia patellae: a long term solution. Aust J Physiother. 32:215-223.
31. Gilleard W, McConnell J, Parsons D. The effect of patellar taping on the onset of vastus medialis obliquus and vastus lateralis muscle activity in persons with patellofemoral pain. Phys Ther. 78:25-32;1998.
32. Werner S, Knutsson E, Eriksson E. Effect of taping the patella on concentric and eccentric torque and EMG of knee extensor and flexor muscles in patients with patellofemoral pain syndrome. Knee Surg Sports Traumatol Arthrosc. 1:169-77;1993.
33. Cowan SM, Bennell KL, Hodges PW. Therapeutic patellar taping changes the timing of vasti muscle activation in people with patellofemoral pain syndrome. Clin J Sport Med. 2002 Nov;12(6):339-47.
34. Cerny K. Vastus medialis oblique/vastus lateralis muscle activity ratios for selected exercises in persons with and without patellofemoral pain syndrome. Phys Ther. 75:672-83;1995.
35. Salsich GB, Bretcher JH, aFarwell D, Powers CM. The effects of patellar taping on knee kinetics, kinematics, and vastus lateralis muscle activity during stair ambulation in individuals with patellofemoral pain. J Ortho Sports Phys Ther.. 32:3-10;2002.
36. Ingersoll C, Knight K. Patellar location changes following EMG biofeedback or progressive resistance exercises. Med Sci Sports Med. 23:1122-1127; 1991.
37. LeVeau BF, Rogers c. Selective training of the vastus medialis muscle using EMG biofeedback. Phys Ther. 60:1410-1415; 1980.
38. Wise HH, Fiebert IM, Kates J. EMG biofeedback as treatment for patellofemoral pain syndrome. J Orthop Sports Phys Ther. 6:95-103; 1984.
39. Earl JE, Schmitz RJ, Arnold BL. Activation of the VMO and VL during dynamic mini-squat exercises with and without isometric hip adduction. J Electromyogr Kinesiol. 2001 Dec;11(6):381-6.
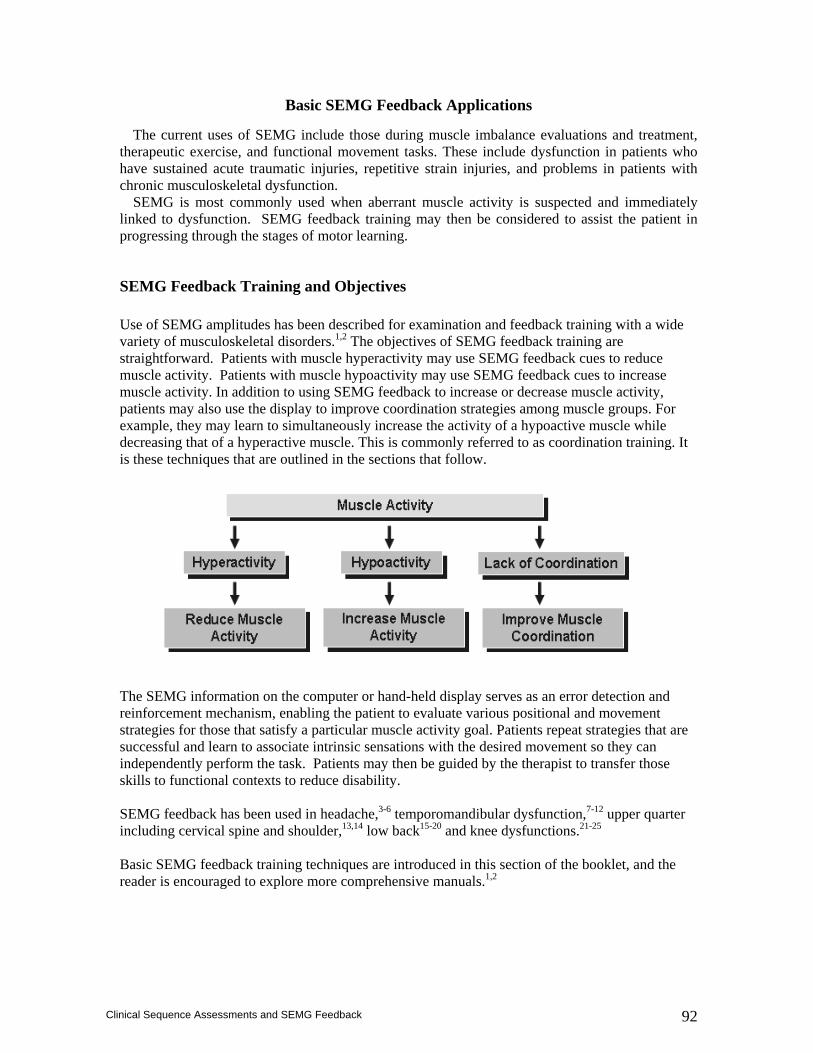
92
Clinical Sequence Assessments and SEMG Feedback
Basic SEMG Feedback Applications The current uses of SEMG include those during muscle imbalance evaluations and treatment,
therapeutic exercise, and functional movement tasks. These include dysfunction in patients who have sustained acute traumatic injuries, repetitive strain injuries, and problems in patients with chronic musculoskeletal dysfunction.
SEMG is most commonly used when aberrant muscle activity is suspected and immediately linked to dysfunction. SEMG feedback training may then be considered to assist the patient in progressing through the stages of motor learning.
SEMG Feedback Training and Objectives Use of SEMG amplitudes has been described for examination and feedback training with a wide variety of musculoskeletal disorders.1,2 The objectives of SEMG feedback training are straightforward. Patients with muscle hyperactivity may use SEMG feedback cues to reduce muscle activity. Patients with muscle hypoactivity may use SEMG feedback cues to increase muscle activity. In addition to using SEMG feedback to increase or decrease muscle activity, patients may also use the display to improve coordination strategies among muscle groups. For example, they may learn to simultaneously increase the activity of a hypoactive muscle while decreasing that of a hyperactive muscle. This is commonly referred to as coordination training. It is these techniques that are outlined in the sections that follow.
The SEMG information on the computer or hand-held display serves as an error detection and reinforcement mechanism, enabling the patient to evaluate various positional and movement strategies for those that satisfy a particular muscle activity goal. Patients repeat strategies that are successful and learn to associate intrinsic sensations with the desired movement so they can independently perform the task. Patients may then be guided by the therapist to transfer those skills to functional contexts to reduce disability. SEMG feedback has been used in headache,3-6 temporomandibular dysfunction,7-12 upper quarter including cervical spine and shoulder,13,14 low back15-20 and knee dysfunctions.21-25 Basic SEMG feedback training techniques are introduced in this section of the booklet, and the reader is encouraged to explore more comprehensive manuals.1,2
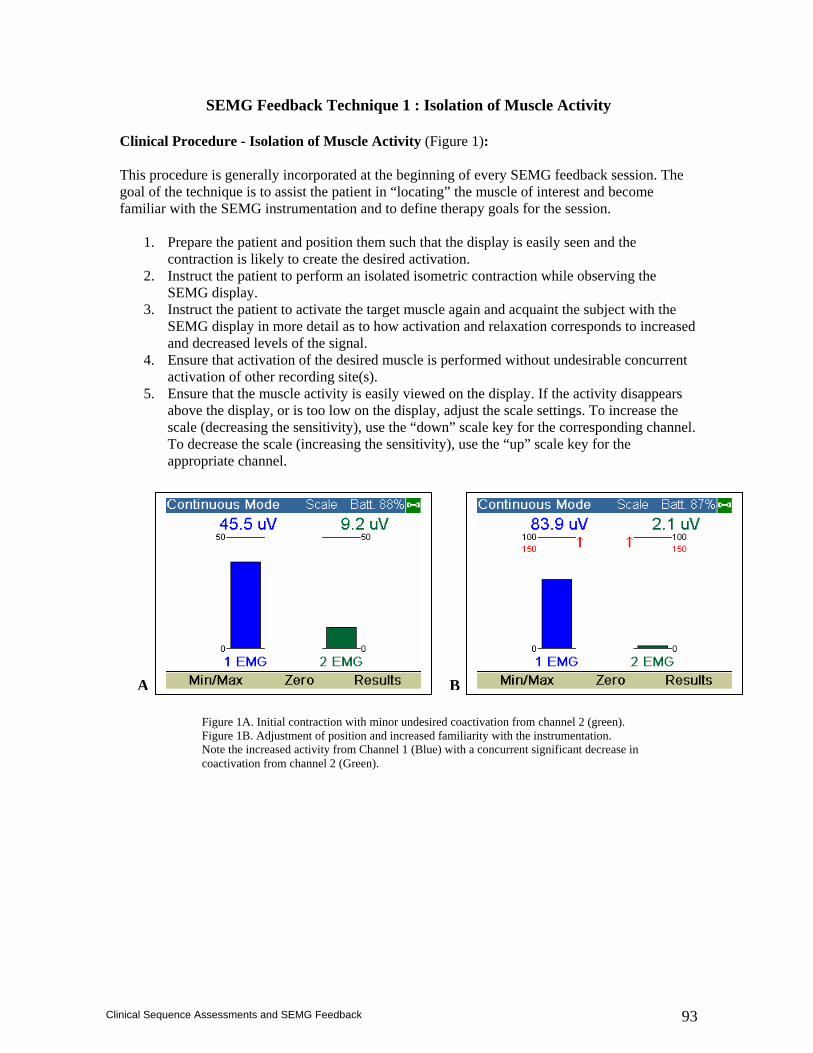
93
Clinical Sequence Assessments and SEMG Feedback
SEMG Feedback Technique 1 : Isolation of Muscle Activity
Clinical Procedure - Isolation of Muscle Activity (Figure 1): This procedure is generally incorporated at the beginning of every SEMG feedback session. The goal of the technique is to assist the patient in “locating” the muscle of interest and become familiar with the SEMG instrumentation and to define therapy goals for the session.
1. Prepare the patient and position them such that the display is easily seen and the contraction is likely to create the desired activation.
2. Instruct the patient to perform an isolated isometric contraction while observing the SEMG display.
3. Instruct the patient to activate the target muscle again and acquaint the subject with the SEMG display in more detail as to how activation and relaxation corresponds to increased and decreased levels of the signal.
4. Ensure that activation of the desired muscle is performed without undesirable concurrent activation of other recording site(s).
5. Ensure that the muscle activity is easily viewed on the display. If the activity disappears above the display, or is too low on the display, adjust the scale settings. To increase the scale (decreasing the sensitivity), use the “down” scale key for the corresponding channel. To decrease the scale (increasing the sensitivity), use the “up” scale key for the appropriate channel.
Figure 1A. Initial contraction with minor undesired coactivation from channel 2 (green). Figure 1B. Adjustment of position and increased familiarity with the instrumentation. Note the increased activity from Channel 1 (Blue) with a concurrent significant decrease in coactivation from channel 2 (Green).
A B
94
Clinical Sequence Assessments and SEMG Feedback
SEMG Feedback Technique 2 (Figure 2): Threshold-based Down-training (relaxation training)
Relaxation Based Strategies Relaxation training is a verbally mediated event in which the practitioner helps the patient change their physiology through the use of actions.14 The therapist instructs the patient how to reduce muscle activity while watching the SEMG display. A number of techniques may be used to assist the patients in reducing hyperactivity. For a more comprehensive outline, the reader is referred to other resources.5,14 In addition to the detailed clinical procedure, some examples include: Progressive Relaxation Training. The therapist instructs the patient how to release muscle tension in isolation with an emphasis upon reducing muscle activity. Autogenic Therapy. Autogenic Therapy uses vocabulary, verbal expressions and images without action. In essence, it is a procedure analogous to self hypnosis. The patient learns to use “self suggestion”, or phrases, to affect their physiology. Guided Imagery. Guided imagery is a more extensive concept than Autogenic Training. It too is a form of "self hypnosis", in which the patient is encouraged to think, utilize kinesthetic, auditory and ocular senses to assist in obtaining a relaxed and comfortable state. Breath Work (Diaphragmatic breathing). When respiration is inefficient, overuse of ancillary muscles during respiration is common. These muscles include the sternocleidomastoid, scalene or upper trapezius. In addition, training of the respiratory system can be one of the avenues for teaching the patient general relaxation. Clinical Procedure – Threshold based Down-training (relaxation training).
1. Instruct the subject to perform a contraction (e.g. shoulder shrug and briefly hold that level of activation steady) as in technique #1.
2. Adjust the scale so that the “baseline” activity level falls within the bottom one-third or so of the display.
3. Set the threshold to a level equivalent to about 80-90% of the subject’s baseline amplitude. Ask the subject to try to relax using a relaxation technique familiar to the reader so that the subject’s activity levels falls below the threshold.
4. If the subject succeeds, move the threshold to a value equivalent to about 80-90% of the new running baseline.
5. Repeat this procedure until the subject seems to be as relaxed as possible. Experiment with different relaxation techniques, and document the average number of microvolts during a 1-3 minute baseline and the lowest 1-3 minute average during the session or the lowest threshold value the patient can consistently maintain.
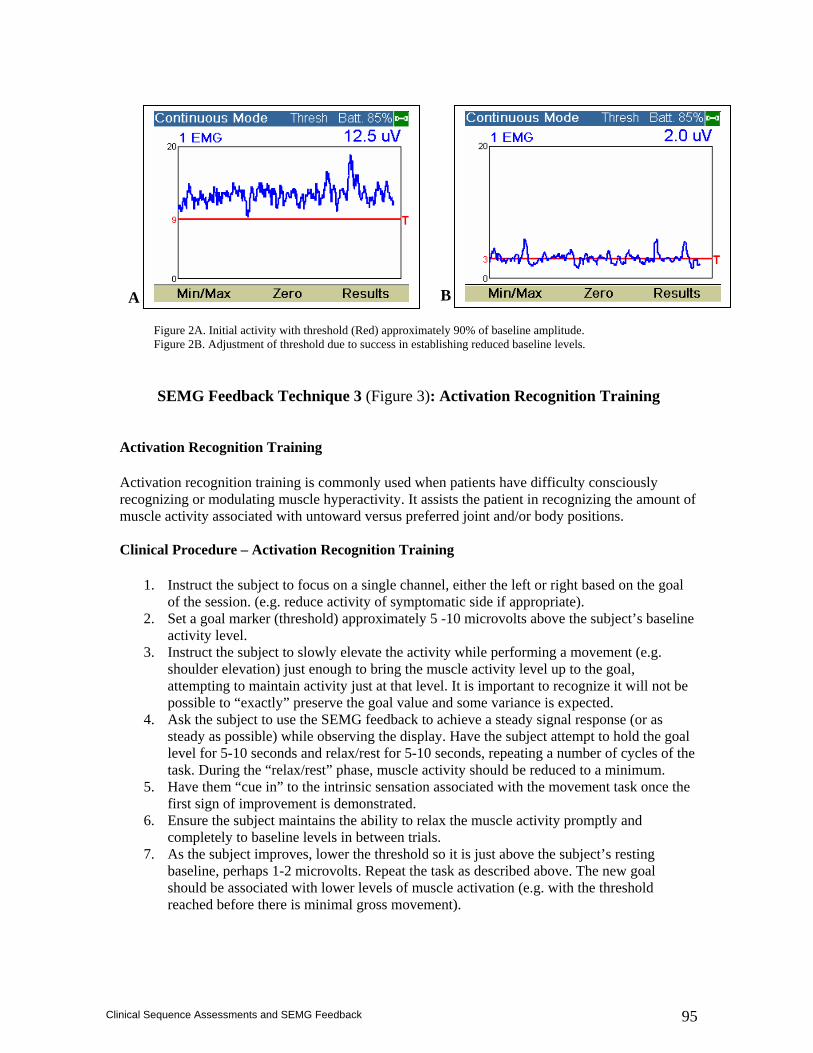
95
Clinical Sequence Assessments and SEMG Feedback
SEMG Feedback Technique 3 (Figure 3): Activation Recognition Training
Activation Recognition Training Activation recognition training is commonly used when patients have difficulty consciously recognizing or modulating muscle hyperactivity. It assists the patient in recognizing the amount of muscle activity associated with untoward versus preferred joint and/or body positions. Clinical Procedure – Activation Recognition Training
1. Instruct the subject to focus on a single channel, either the left or right based on the goal of the session. (e.g. reduce activity of symptomatic side if appropriate).
2. Set a goal marker (threshold) approximately 5 -10 microvolts above the subject’s baseline activity level.
3. Instruct the subject to slowly elevate the activity while performing a movement (e.g. shoulder elevation) just enough to bring the muscle activity level up to the goal, attempting to maintain activity just at that level. It is important to recognize it will not be possible to “exactly” preserve the goal value and some variance is expected.
4. Ask the subject to use the SEMG feedback to achieve a steady signal response (or as steady as possible) while observing the display. Have the subject attempt to hold the goal level for 5-10 seconds and relax/rest for 5-10 seconds, repeating a number of cycles of the task. During the “relax/rest” phase, muscle activity should be reduced to a minimum.
5. Have them “cue in” to the intrinsic sensation associated with the movement task once the first sign of improvement is demonstrated.
6. Ensure the subject maintains the ability to relax the muscle activity promptly and completely to baseline levels in between trials.
7. As the subject improves, lower the threshold so it is just above the subject’s resting baseline, perhaps 1-2 microvolts. Repeat the task as described above. The new goal should be associated with lower levels of muscle activation (e.g. with the threshold reached before there is minimal gross movement).
Figure 2A. Initial activity with threshold (Red) approximately 90% of baseline amplitude. Figure 2B. Adjustment of threshold due to success in establishing reduced baseline levels.
A B
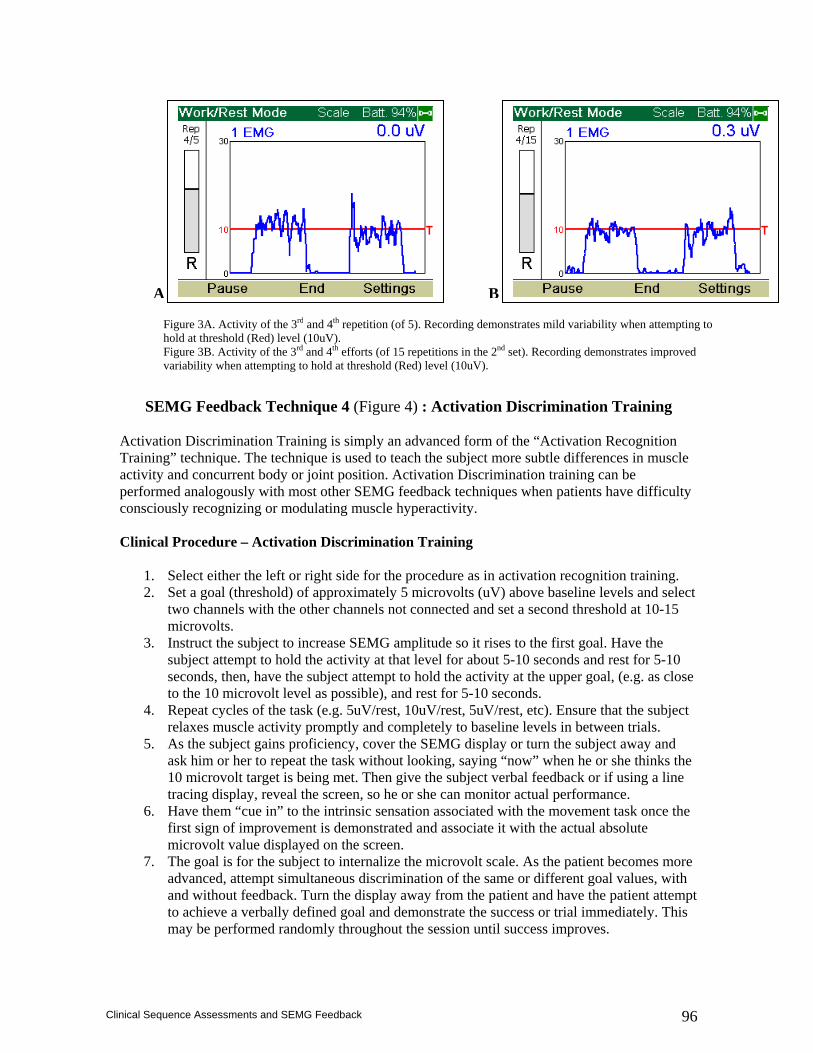
96
Clinical Sequence Assessments and SEMG Feedback
SEMG Feedback Technique 4 (Figure 4) : Activation Discrimination Training
Activation Discrimination Training is simply an advanced form of the “Activation Recognition Training” technique. The technique is used to teach the subject more subtle differences in muscle activity and concurrent body or joint position. Activation Discrimination training can be performed analogously with most other SEMG feedback techniques when patients have difficulty consciously recognizing or modulating muscle hyperactivity. Clinical Procedure – Activation Discrimination Training
1. Select either the left or right side for the procedure as in activation recognition training. 2. Set a goal (threshold) of approximately 5 microvolts (uV) above baseline levels and select
two channels with the other channels not connected and set a second threshold at 10-15 microvolts.
3. Instruct the subject to increase SEMG amplitude so it rises to the first goal. Have the subject attempt to hold the activity at that level for about 5-10 seconds and rest for 5-10 seconds, then, have the subject attempt to hold the activity at the upper goal, (e.g. as close to the 10 microvolt level as possible), and rest for 5-10 seconds.
4. Repeat cycles of the task (e.g. 5uV/rest, 10uV/rest, 5uV/rest, etc). Ensure that the subject relaxes muscle activity promptly and completely to baseline levels in between trials.
5. As the subject gains proficiency, cover the SEMG display or turn the subject away and ask him or her to repeat the task without looking, saying “now” when he or she thinks the 10 microvolt target is being met. Then give the subject verbal feedback or if using a line tracing display, reveal the screen, so he or she can monitor actual performance.
6. Have them “cue in” to the intrinsic sensation associated with the movement task once the first sign of improvement is demonstrated and associate it with the actual absolute microvolt value displayed on the screen.
7. The goal is for the subject to internalize the microvolt scale. As the patient becomes more advanced, attempt simultaneous discrimination of the same or different goal values, with and without feedback. Turn the display away from the patient and have the patient attempt to achieve a verbally defined goal and demonstrate the success or trial immediately. This may be performed randomly throughout the session until success improves.
Figure 3A. Activity of the 3rd and 4th repetition (of 5). Recording demonstrates mild variability when attempting to hold at threshold (Red) level (10uV). Figure 3B. Activity of the 3rd and 4th efforts (of 15 repetitions in the 2nd set). Recording demonstrates improved variability when attempting to hold at threshold (Red) level (10uV).
A B
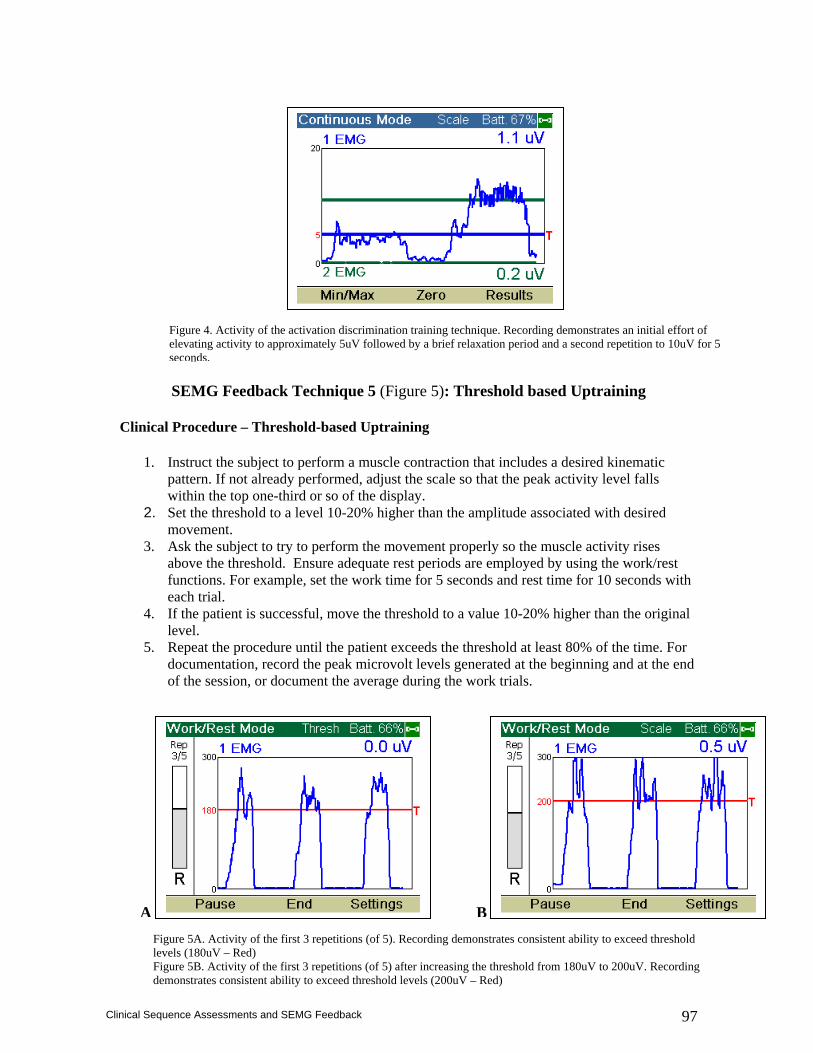
97
Clinical Sequence Assessments and SEMG Feedback
SEMG Feedback Technique 5 (Figure 5): Threshold based Uptraining Clinical Procedure – Threshold-based Uptraining
1. Instruct the subject to perform a muscle contraction that includes a desired kinematic pattern. If not already performed, adjust the scale so that the peak activity level falls within the top one-third or so of the display.
2. Set the threshold to a level 10-20% higher than the amplitude associated with desired movement.
3. Ask the subject to try to perform the movement properly so the muscle activity rises above the threshold. Ensure adequate rest periods are employed by using the work/rest functions. For example, set the work time for 5 seconds and rest time for 10 seconds with each trial.
4. If the patient is successful, move the threshold to a value 10-20% higher than the original level.
5. Repeat the procedure until the patient exceeds the threshold at least 80% of the time. For documentation, record the peak microvolt levels generated at the beginning and at the end of the session, or document the average during the work trials.
Figure 4. Activity of the activation discrimination training technique. Recording demonstrates an initial effort of elevating activity to approximately 5uV followed by a brief relaxation period and a second repetition to 10uV for 5 seconds.
Figure 5A. Activity of the first 3 repetitions (of 5). Recording demonstrates consistent ability to exceed threshold levels (180uV – Red) Figure 5B. Activity of the first 3 repetitions (of 5) after increasing the threshold from 180uV to 200uV. Recording demonstrates consistent ability to exceed threshold levels (200uV – Red)
A B
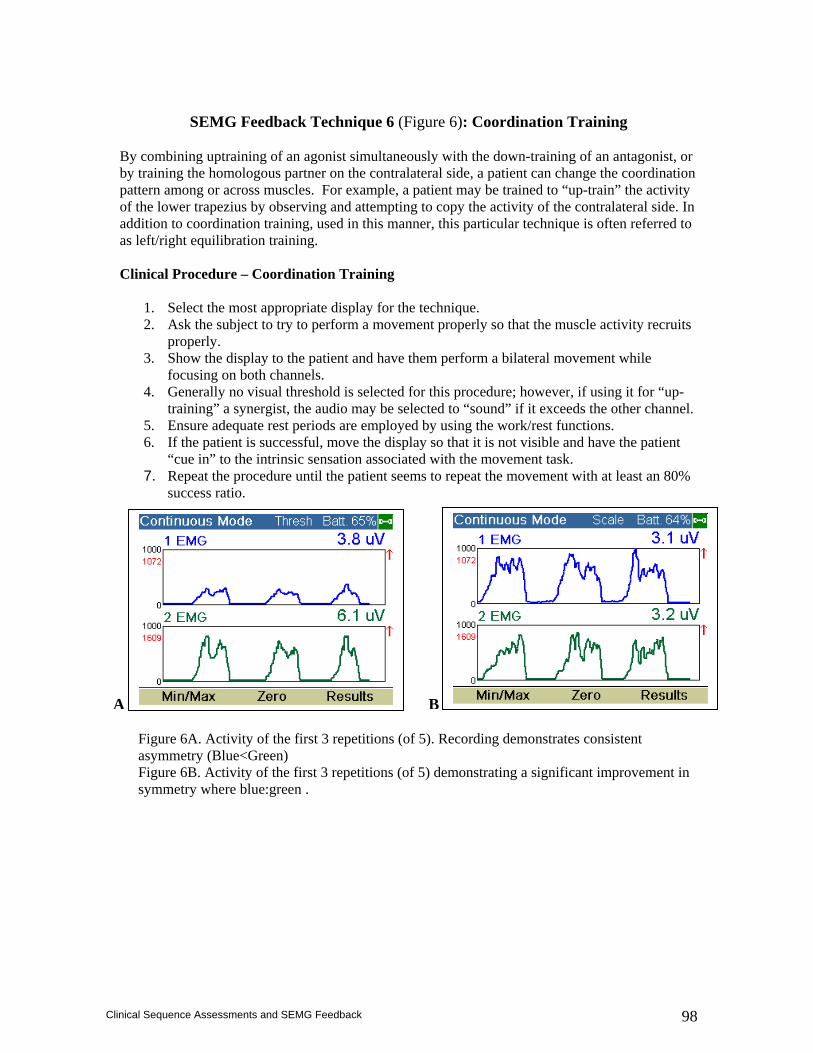
98
Clinical Sequence Assessments and SEMG Feedback
SEMG Feedback Technique 6 (Figure 6): Coordination Training
By combining uptraining of an agonist simultaneously with the down-training of an antagonist, or by training the homologous partner on the contralateral side, a patient can change the coordination pattern among or across muscles. For example, a patient may be trained to “up-train” the activity of the lower trapezius by observing and attempting to copy the activity of the contralateral side. In addition to coordination training, used in this manner, this particular technique is often referred to as left/right equilibration training. Clinical Procedure – Coordination Training
1. Select the most appropriate display for the technique. 2. Ask the subject to try to perform a movement properly so that the muscle activity recruits
properly. 3. Show the display to the patient and have them perform a bilateral movement while
focusing on both channels. 4. Generally no visual threshold is selected for this procedure; however, if using it for “up-
training” a synergist, the audio may be selected to “sound” if it exceeds the other channel. 5. Ensure adequate rest periods are employed by using the work/rest functions. 6. If the patient is successful, move the display so that it is not visible and have the patient
“cue in” to the intrinsic sensation associated with the movement task. 7. Repeat the procedure until the patient seems to repeat the movement with at least an 80%
success ratio.
Figure 6A. Activity of the first 3 repetitions (of 5). Recording demonstrates consistent asymmetry (Blue<Green) Figure 6B. Activity of the first 3 repetitions (of 5) demonstrating a significant improvement in symmetry where blue:green .
A B
99
Clinical Sequence Assessments and SEMG Feedback
References
1. Kasman GS, Cram JR, Wolf SL. Clinical Applications in Surface Electromyography: Chronic Musculoskeletal Pain. Gaithersburg, MD: Aspen Publishers, 1998.
2. Cram JR, Kasman, GS. Introduction to Surface Electromyography. Gaithersburg, MD: Aspen Publishers, 1998.
3. Kroner-Herwig B, Mohn U, Pothmann R. Comparison of biofeedback and relaxation in the treatment of pediatric headache and the influence of parent involvement on outcome. Appl Psychophysiol Biofeedback. 1998 Sep;23(3):143-57.
4. Arena JG, Bruno GM, Hannah SL, Meador KJ A comparison of frontal electromyographic biofeedback training, trapezius electromyographic biofeedback training, and progressive muscle relaxation therapy in the treatment of tension headache. Headache. 1995 Jul-Aug;35(7):411-9.
5. Lacroix JM, Clarke MA, Bock JC, Doxey NC Physiological changes after biofeedback and relaxation training for multiple-pain tension-headache patients. Percept Mot Skills. 1986 Aug;63(1):139-53.
6. Budzynski TH, Stoyva JM, Adler CS, Mullaney DJ. EMG biofeedback and tension headache: a controlled outcome study. Semin Psychiatry. 1973 Nov;5(4):397-410.
7. Erlandson PM Jr, Poppen R. Electromyographic biofeedback and rest position training of masticatory muscles in myofascial pain-dysfunction patients. J Prosthet Dent. 1989 Sep;62(3):335-8.
8. Hijzen TH, Slanger JL, Van Houweligan HC. Subjective, clinical and EMG effects of biofeedback and splint treatment. J Oral rehabil. 13:529-539;1986.
9. Turk D, Hussein Z, Rudy T. Effects of intraoral appliance and biofeedback/stress management alone and in combination in treating temporomandibular disorders. J Prosthet Dent. 70:158-164;1993.
10. Crider AB, Glaros AG. A meta-analysis of EMG biofeedback treatment of temporomandibular disorders. J Orofac Pain. 1999 Winter;13(1):29-37.
11. Erlandson PM Jr, Poppen R. Electromyographic biofeedback and rest position training of masticatory muscles in myofascial pain-dysfunction patients. J Prosthet Dent. 1989 Sep;62(3):335-8.
12. Turk DC, Zaki HS, Rudy TE. Effects of intraoral appliance and biofeedback/stress management alone and in combination in treating pain and depression in patients with temporomandibular disorders. J Prosthet Dent. 1993 Aug;70(2):158-64.
13. Nord S, Ettare D, Drew D, Hodge S. Muscle learning therapy--efficacy of a biofeedback based protocol in treating work-related upper extremity disorders. J Occup Rehabil. 2001 Mar;11(1):23-31.
14. Young MS. Electromyographic biofeedback use in the treatment of voluntary posterior dislocation of the shoulder: a case study. J Orthop Sports Phys Ther. 1994 Sep;20(3):171-5.
15. Wolf SL, Wolf LB, Segal RL. The relationship of extraneous movements to lumbar paraspinal muscle activity: implications for EMG biofeedback training applications to low back pain patients. Biofeedback Self Regul. 1989 Mar;14(1):63-74.
16. Jones AL, Wolf SL. Treating chronic low back pain. EMG biofeedback training during movement. Phys Ther. 1980 Jan;60(1):58-63.
17. Asfour SS, Khalil TM, Waly SM, Goldberg ML, Rosomoff RS, Rosomoff HL. Biofeedback in back muscle strengthening. Spine. 1990 Jun;15(6):510-3.
18. Flor H, Haag G, Turk DC. Long-term efficacy of EMG biofeedback for chronic rheumatic back pain. Pain. 1986 Nov;27(2):195-202.\
19. Donaldson CCS. The effects of correcting muscle asymmetry upon chronic low back pain. Calgary, Alberta: University of Calgary:1989. Dissertation.
20. Sherman RA, Arena JG. Biofeedback for assessment and treatment of low back pain. In: Basmaijian JV, Nyberg R, eds. Rational Manual Therapies. Baltimore: Williams & Wilkins; 1993; 177-198.
21. Beckham JC, Keefe FJ, Caldwell DS, Brown CJ. Biofeedback as a means to alter electromyographic activity in a total knee replacement patient. Biofeedback Self Regul. 1991 Mar;16(1):23-35.
22. Dursun N, Dursun E, Kilic Z. Electromyographic biofeedback-controlled exercise versus conservative care for patellofemoral pain syndrome. Arch Phys Med Rehabil. 2001 Dec;82(12):1692-5.
23. Feller J, Hoser C, Webster K. EMG biofeedback assisted KT-1000 evaluation of anterior tibial displacement. Knee Surg Sports Traumatol Arthrosc. 2000;8(3):132-6.

100
Clinical Sequence Assessments and SEMG Feedback
24. Draper V. Electromyographic biofeedback and recovery of quadriceps femoris muscle function following anterior cruciate ligament reconstruction. Phys Ther. 1990 Jan;70(1):11-7.
25. Levitt R, Deisinger JA, Remondet Wall J, Ford L, Cassisi JE. EMG feedback-assisted postoperative rehabilitation of minor arthroscopic knee surgeries. J Sports Med Phys Fitness. 1995 Sep;35(3):218-23.