clinical review clinical review - bmj · pr3-anca positive and mpo-anca positive patients.10 48 49...
TRANSCRIPT

STATE OF THE ART REVIEW
Management of ANCA associated vasculitisZachary S Wallace assistant professor of medicine 1 2 3, Eli M Miloslavsky assistant professor ofmedicine 2 3
1Clinical Epidemiology Program, Division of Rheumatology, Allergy, and Immunology, Mongan Institute, Department of Medicine, MassachusettsGeneral Hospital, Boston, MA, USA; 2Rheumatology Unit, Division of Rheumatology, Allergy, and Immunology, Department of Medicine, MassachusettsGeneral Hospital, Boston, MA, USA; 3Harvard Medical School, Boston, MA, USA
AbstractABSTRACTAnti-neutrophil cytoplasmic antibody (ANCA) associated vasculitis (AAV)is a small to medium vessel vasculitis associated with excess morbidityand mortality. This review explores how management of AAV has evolvedover the past two decades with pivotal randomized controlled trialsshaping the management of induction and maintenance of remission.Contemporary AAV care is characterized by approaches that minimizethe cumulative exposure to cyclophosphamide and glucocorticoids,increasingly use rituximab for remission induction and maintenance, andconsider therapies with less toxicity (for example, methotrexate,mycophenolate mofetil) for manifestations of AAV that do not threatenorgan function or survival. Simultaneously, improvements in outcomes,such as renal and overall survival, have been observed. Additional trialsand observational studies evaluating the comparative effectiveness ofagents for AAV in various patient subgroups are needed. Prospectivestudies are necessary to assess the effect of psychosocial interventionson patient reported outcomes in AAV. Despite the expanding array oftreatments for AAV, little guidance on how to personalize AAV care isavailable to physicians.
IntroductionAnti-neutrophil cytoplasmic antibody (ANCA) associatedvasculitis (AAV) is a necrotizing vasculitis primarily affectingsmall to medium sized vessels.1 AAV is a heterogeneouscondition that includes three clinicopathologic conditions:granulomatosis with polyangiitis (GPA, formerly Wegener’sgranulomatosis), microscopic polyangiitis, and eosinophilicgranulomatosis with polyangiitis (EGPA).1 It affects men andwomen from a wide age spectrum and diverse racialbackgrounds (fig 1). The most commonly affected organsinclude the respiratory tract, eyes, kidneys, skin, and nervoussystem.
Most patients with AAV are ANCA positive at some point intheir clinical course, with antibodies targeting either proteinase3 (PR3-ANCA positive) or myeloperoxidase (MPO-ANCApositive).3-5 Mounting evidence suggests that phenotypingpatients according to ANCA type (PR3-ANCA positive orMPO-ANCA positive), rather than as GPA or microscopicpolyangiitis, may better identify homogeneous groups that sharesimilar genetics, pathogenesis, organ involvement, and responseto treatment (fig 1).6-10
Pivotal trials (table 1 and table 2) over the past several decadeshave shaped contemporary strategies for induction andmaintenance of remission, which have led to improvements inrelapse rates, renal outcomes, quality of life, morbidity, andoverall survival.26-33 However, AAV remains associated with ahigher risk of death than the general population,34 35 and patientscontinue to accrue organ damage from disease activity andtreatment.36
Here, we focus on clinical trials that have shaped thecontemporary management of induction and maintenance ofremission in AAV, specifically GPA and microscopicpolyangiitis; EGPA is considered a distinct disease with differentapproaches to management. We consider how the increasingamount of data from trials and observational studies mightinform a personalized approach to AAV care.
Incidence and prevalence of AAVA population based study conducted in Olmstead County,Minnesota, USA, estimated the annual incidences of GPA andmicroscopic polyangiitis to be 1.3 (95% confidence interval 0.8to 1.8) per 100 000 and 1.6 (1.0 to 2.2) per 100 000, respectively.The prevalence of AAV in that study was 42.1 (29.6 to 54.6)per 100 000.37 Similar estimates of annual incidence of GPAwere reported in a large US health insurance claims database
Correspondence to: [email protected] (or @zach_wallace_md on Twitter)
Series explanation: State of the Art Reviews are commissioned on the basis of their relevance to academics and specialists in the US and internationally. For this reasonthey are written predominantly by US authors
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 1 of 16
Clinical Review
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

(1.3 (1.2 to 13.4) per 100 000),38 as well as the UK GeneralPractice Research Database (0.8 (0.8 to 0.9) per 100 000).39
Natural historySeverity of AAV varies widely, leading many people todifferentiate between severe and non-severe disease (fig 2).Severe disease is characterized by manifestations that threatenthe function of vital organs, such as diffuse alveolar hemorrhage,glomerulonephritis, mononeuritis multiplex, sensorineuraldeafness, scleritis, or gangrene.41-44 Non-severe disease, incontrast, is characterized by disease affecting the sinuses, nares,and/or mucocutaneous surfaces, as well as pulmonary nodules,tracheobronchial disease, and arthritis. Despite thisdichotomization, manifestations considered severe may beindolent and non-severe manifestations may contributesignificantly to disease morbidity.Sinonasal, pulmonary, and musculoskeletal manifestations arethe most common presenting symptoms. A minority of patientspresent with chronic non-severe disease, often limited to thesinuses and the upper airway. More often, patients withnon-severe disease develop severe disease, after months to yearsof non-severe manifestations.45 This highlights the importanceof early recognition and treatment initiation. Severe disease,however, may be fulminant and unheralded. Renal involvementis the most common severe manifestation and can lead to endstage renal disease (ESRD), which is estimated to affect 30%of patients with renal involvement after five years.26
Generally, severe AAV is fatal if left untreated.46 Even withtreatment, excess mortality remains. A recent meta-analysisfound that the standardized mortality ratio of death in AAVcompared with the general population was 2.7 (95% confidenceinterval 2.3 to 3.2).35 47
Pathogenesis of ANCA associatedvasculitisThe cause of AAV is unknown, but approximately 20% ofdisease risk is due to genetic factors, which differ betweenPR3-ANCA positive and MPO-ANCA positive patients.10 48 49
The role of MPO-ANCA in pathogenesis is well establishedgiven observations that the transfer of MPO-ANCA antibodiesinto experimental mouse models induces vasculitis.50 51 Evidencesupporting the pathogenic role of PR3-ANCA is less strong butis inferred from certain observations: PR3-ANCA antibodiesappear years before clinical presentation; genetic variants inproteinase 3 (the antigenic target of PR3-ANCA) are seen inPR3-ANCA positive AAV; PR3-ANCA titers correlate withdisease activity in some patients; and B cell targeted therapy isefficacious in PR3-ANCA positive patients.52 As such, currenttherapies include broad immunosuppression and B cell targetedtreatment.However, as our understanding of the pathogenesis of AAVexpands, so do the therapeutic options. Myeloperoxidase andproteinase 3 are enzymes found in neutrophils, which are thetargets of ANCA antibodies and play a key role inpathogenesis.50 Neutrophil extracellular traps (NETs) have beenrecently recognized as important in the pathogenesis.53
Moreover, although immunoglobulins and complement areinfrequently observed in biopsy specimens, the alternativepathway is now considered pathogenically important, andcomplement inhibitors (such as anti-C5a) may have efficacy inAAV.54 55
Sources and selection criteriaWe identified relevant studies for inclusion by a search ofPubMed, Embase, and Cochrane databases from 2009 to 2019.We searched for the following phrases: “ANCA-associatedvasculitis”, “Wegener’s granulomatosis”, “granulomatosis withpolyangiitis”, and/or “microscopic polyangiitis”. We reviewedapproximately 500 abstracts of systematic reviews,meta-analyses, randomized controlled trials (RCTs), andobservational studies that were published in English. We alsoreviewed published management guidelines after reviewingwebsites and publications from professional rheumatology (forexample, American College of Rheumatology, British Societyof Rheumatology), nephrology, and other specialty societies.In addition to studies identified using these approaches, we alsoincluded landmark studies. With the exception of high profileRCTs recently reported in abstract form, only peer reviewedstudies were eligible for inclusion.25 56 We prioritizedmeta-analyses and RCTs with the exception of the managementof specific manifestations (for example, sinus disease) for whichdata are more limited to case series. We generally excludedstudies that enrolled patients with other forms of vasculitis (forexample, polyarteritis nodosa) unless results from stratifiedanalyses were available.
Evolution of clinical trial design in ANCAassociated vasculitisCase series from the US National Institutes of Health shapedthe initial AAV treatment paradigm. Subsequently, recognitionof the importance of multicenter studies in AAV and relatedconditions led to the formation of the Glomerular DiseaseCollaborative Network (GDCN), the French Vasculitis StudyGroup (FVSG), the European Vasculitis Study Group (EUVAS),and the Vasculitis Clinical Research Consortium (VCRC).57 Thesuccess of clinical trials organized by these groups confirmedthat large, well designed studies in AAV were feasible andtransformed AAV treatment. However, review of this experiencereveals challenges to designing AAV trials that affect our abilityto compare results across studies. Firstly, although recent effortshave been made to standardize trial design, trials historicallyrelied on variable enrollment criteria, primary outcomemeasures, and definitions of remission and relapse.58 Secondly,the doses and durations of glucocorticoid regimens have variedwidely.42 Considering these limitations is important as we reviewAAV clinical trials from the past 20 years.
Induction of remissionGlucocorticoids in AAV remission inductionGlucocorticoids bind to cytosolic glucocorticoid receptors,causing decreased expression of pro-inflammatory proteins andrapid non-genomic effects.59 Their quick onset of action androbust anti-inflammatory effects have made them a cornerstoneof AAV care.60 However, significant toxicity (table 3) andincomplete efficacy as monotherapy necessitate a secondimmunosuppressive agent.61
The optimal dose, route, and duration of glucocorticoids remainsuncertain. Intravenous methylprednisolone, typically in dosesof 1000 mg daily for three days, is often used for severe endorgan involvement, although the evidence base supporting thispractice is weak.62 Ongoing uncertainty about the role ofintravenous glucocorticoids is shown by the design of clinicaltrials for severe AAV, with some studies requiring their use and
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 2 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

others using oral glucocorticoids or leaving the decision to thediscretion of the investigator.13 15-17
Similar variation exists in the dose and duration ofglucocorticoid therapy, with trials using courses ranging from5.5 months to more than 24 months.42 Oral glucocorticoids aretypically started at prednisone equivalent 1 mg/kg/day andtapered to 30-40 mg/day by one month and 10-20 mg/day bythree months.44 63
Only recently have studies assessed the optimal duration of oralglucocorticoids. The PEXIVAS trial, which enrolled 704patients, used a two-by-two factorial design comparing plasmaexchange versus no plasma exchange and standard dose versusreduced dose glucocorticoids in a non-blinded manner. Theprimary outcome was death or ESRD. The reducedglucocorticoid dose arm used 55% of the standard dose regimenover the first six months of therapy,64 achieving the sameefficacy as the standard dose arm with fewer serious infections.56
Additional studies are needed to optimize the use ofglucocorticoids to balance their efficacy and toxicity. This hasbeen facilitated by the development of a novel tool, theglucocorticoid toxicity index, now being used in clinical trials.65
Refining cyclophosphamide to minimizetoxicityProspective case series describing the efficacy of oral dailycyclophosphamide in combination with prednisone for GPAheralded the modern era of AAV treatment.45 46 66
Cyclophosphamide is an alkylating agent that causes broadimmunosuppression, including B cell depletion.67-70 Despitegood response rates, the risk of relapse and toxicity (table 3)became evident with growing experience, leading to multiplestudies comparing oral daily with intravenous pulsecyclophosphamide.11 46 71 72
Of these, the CYCLOPS trial was the first remission inductiontrial to use the contemporary regimen in which azathioprine issubstituted for cyclophosphamide after three to six months oftherapy (see section on remission maintenance).19 CYCLOPSwas an unblinded controlled trial that randomized 149 patientswith renal disease due to ANCA positive (99%) GPA ormicroscopic polyangiitis to daily or pulse cyclophosphamide(table 1).15 The primary outcome, time to remission over 18months, was no different between the daily and pulse groups(hazard ratio 1.1, 95% confidence interval 0.8 to 1.6). Themedian time to remission was three months in both groups. Thedaily group received double the amount of cyclophosphamideas the pulse group (16 g v 8 g; P=0.001). No difference wasseen in the proportion achieving remission at nine months (88%in both groups).In a retrospective follow-up study of CYCLOPS, the daily grouphad a 50% reduction in the risk of relapse (hazard ratio 0.5, 0.3to 0.9) over a median of 4.3 years compared with the pulsegroup, independent of ANCA type.73 Leukopenia was morecommon in the daily group than the pulse group (45% v 26%;P=0.02). In both the 18 month analysis and a long termfollow-up study, no difference was seen in risk of malignancy,severe infection, death, or change in renal function between thetwo treatment arms.
Rituximab versus cyclophosphamideFor patients with complications or for whom cyclophosphamidetreatment was not successful, an alternative was needed. Caseseries reported the efficacy of peripheral CD20+ B celldepletion,74-76 motivating the design of the Rituximab in
ANCA-Associated Vasculitis (RAVE) trial,16 which transformedthe management of AAV (table 1).RAVE randomized 197 patients with newly diagnosed orrelapsing severe ANCA positive GPA or microscopicpolyangiitis to a 5.5 month glucocorticoid taper plus eitherrituximab (four weekly 375 mg/m2 doses) or oral dailycyclophosphamide for three to six months followed byazathioprine. Patients in the rituximab arm received noprescribed treatment beyond glucocorticoids and the first fourdoses of rituximab. In contrast to other AAV trials, this was adouble blind, double dummy, non-inferiority trial which had aprimary outcome that required patients to be off glucocorticoidsby six months. Most patients were PR3-ANCA positive (68%)and classified as GPA (77%); 48% had no major renalinvolvement. RAVE excluded patients with diffuse alveolarhemorrhage requiring ventilatory support and/or renal failurewith a creatinine concentration greater than 4.0 mg/dL (354μmol/L).The primary outcome, complete remission off glucocorticoidsat six months, was reached by 64% of patients randomized torituximab compared with 53% of those randomized tocyclophosphamide (P<0.001 for non-inferiority). Rituximabwas not statistically superior to cyclophosphamide (P=0.09)overall but was found to be superior among patients withrelapsing disease at baseline (odds ratio 1.40, 95% confidenceinterval 1.03 to 1.91) and, in a post hoc analysis, among thosewho were PR3-ANCA positive (odds ratio 2.11, 1.04 to 4.30).7
Rituximab without additional remission maintenance therapyremained non-inferior to cyclophosphamide-azathioprine at 18months when rates of sustained completion remission werecompared (39% v 33%).77 Over 18 months, 74% of patientsachieved complete remission off glucocorticoids at any time.No difference was seen between rituximab andcyclophosphamide with respect to the frequency, severity, ortime to relapse over 18 months. Outcomes were similar amongpatients with major renal involvement at baseline regardless ofwhether they were randomized to cyclophosphamide orrituximab.16 78 No significant difference was seen in the rates ofadverse events between the two treatment arms, althoughcyclophosphamide was associated with more pneumonias(P=0.03).16 This equivalency was surprising but likely reflectsthe countering effects of glucocorticoid exposure and reducedcyclophosphamide exposure on risk of infection.A companion EUVAS trial, RITUXVAS, randomized 44patients (3:1) with severe AAV associated renal vasculitis torituximab plus two intravenous cyclophosphamide infusions orintravenous cyclophosphamide for three to six months followedby azathioprine.17 Both groups achieved sustained remission atsimilar rates (76% v 82%; P=0.7) and had similar rates of severeadverse events (42% v 36%; P=0.8).Given the efficacy and comparable safety profile of rituximab,rituximab is often chosen for induction of remission.79 Theoptimal dosing regimen has not been studied, but the mostcommon regimens include 375 mg/m2 weekly for four weeksor 1000 mg twice over two weeks. Cyclophosphamide remainsa cornerstone of therapy for many providers,80 especially whererituximab is prohibitively expensive.81 The relatively shortfollow-up in RAVE limited an assessment of differences in longterm outcomes, such as malignancy and survival, between thetwo treatment arms, but recent observational data suggest thatrituximab, in contrast to cyclophosphamide, is not associatedwith an increased risk of malignancy.32
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 3 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

Other approaches to remission induction:methotrexate and mycophenolate mofetilMethotrexate and mycophenolate mofetil have also been studiedfor induction of remission. Methotrexate has its effects byincreasing extracellular adenosine, whereas mycophenolatemofetil inhibits DNA synthesis.82 The NORAM trial wasdesigned following studies suggesting that methotrexate mayhave efficacy in non-severe AAV.83-86 NORAM was an openlabel, non-inferiority EUVAS trial that randomized 100 patientswith non-severe GPA or microscopic polyangiitis to eithermethotrexate or daily cyclophosphamide for 12 months (table1).12 Patients with organ threatening or life threatening diseasewere excluded.Most patients in NORAM were PR3-ANCA positive (74%) andhad GPA (94%). The primary outcome, the proportion inremission at six months, was achieved by a similar proportionof patients in the methotrexate and cyclophosphamide arms(90% v 94%), and the median time to remission was also similar(3 v 2 months; P=0.3). However, methotrexate was associatedwith a longer time to remission among patients with moreextensive disease and a shorter time to relapse among all patientsthan was cyclophosphamide (hazard ratio 1.9, 95% confidenceinterval 1.1 to 3.3). Over 18 months, methotrexate wasassociated with more flares than cyclophosphamide (70% v47%). Compared with cyclophosphamide, methotrexate wasassociated with fewer episodes of leukopenia (3 v 14; P=0.01)but more episodes of liver dysfunction (7 v 1: P=0.04).NORAM has two significant limitations. Firstly, it used 12months of oral cyclophosphamide, so how methotrexate wouldcompare with contemporary three to six monthcyclophosphamide regimens is unclear. Secondly, all therapywas tapered and discontinued by 12 months, after which manyof the flares occurred. Prolonged methotrexate treatment mayhave prevented flares and been well tolerated. Methotrexate iscommonly used in rheumatology because of its favorable safetyprofile, as confirmed in a recent large trial evaluating its efficacyfor secondary prevention of cardiovascular disease,87 but shouldbe avoided in patients with a glomerular filtration rate below30 mL/min/1.73 m2.MYCYC was an open label, non-inferiority, randomizedcontrolled EUVAS trial that compared mycophenolate mofetilwith cyclophosphamide for induction of remission (table 1).18
It followed several small prospective studies that foundmycophenolate mofetil to be efficacious in MPO-ANCA positiveAAV.88-90 In MYCYC, 140 patients newly diagnosed as havingGPA or microscopic polyangiitis (59% PR3-ANCA positive,38% MPO-ANCA positive) were randomized to eithermycophenolate mofetil (76% on 2 g/day of mycophenolate) orpulse cyclophosphamide; both arms received azathioprinefollowing remission. Patients with life threatening disease andthose with rapidly declining renal function were excluded, butmost (81%) had renal disease and the severity of renal diseasewas generally worse than in those enrolled in NORAM.A similar proportion of patients in the mycophenolate mofetiland cyclophosphamide groups achieved remission at six months(67% v 61%), showing non-inferiority (risk difference 5.7%,90% confidence interval −7.5% to 19%). However, morepatients in the mycophenolate mofetil group relapsed afterremission (33% v 19%; incidence rate ratio 1.97, 95%confidence interval 0.96 to 4.23). This difference was stronglydriven by differences in response according to ANCA type;48% of PR3-ANCA positive patients in the mycophenolatemofetil group compared with 24% of PR3-ANCA positivepatients in the cyclophosphamide group relapsed. Notably, the
rates of serious infection were similar between themycophenolate mofetil and cyclophosphamide arms (26% v17%; odds ratio 1.7, 0.68 to 4.19), as were the rates of otheradverse events (for example, ESRD and death).NORAM and MYCYC show that methotrexate andmycophenolate mofetil can induce remission in selected patientsbut may be associated with a higher risk of relapse. They maybe particularly useful for patients in whom conventionaltherapies have failed or are contraindicated and/or in those atlower risk of flare (such as MPO-ANCA). They may not beideal for patients in whom a relapse could portend organ failure,significant effect on quality of life, serious toxicity from excessglucocorticoids, or life threatening disease. Of note,mycophenolate mofetil received the lowest grade of endorsementby members of EUVAS in their recommendations for themanagement of AAV, although these were published before thepublication of MYCYC.44
RAVE, NORAM, and MYCYC highlight the relative safetyfrom an infection perspective of contemporarycyclophosphamide regimens. However, these observations arederived from clinical trials in which patient selection and closemonitoring may influence infection rates. Observational datamay better assess these risks and be used to compare the relativeefficacy of different regimens (for example, methotrexate,mycophenolate mofetil) versus rituximab in patients with lesssevere disease.
Plasma exchange in ANCA associatedvasculitisIn cases of diffuse alveolar hemorrhage, rapidly progressiveglomerulonephritis, or both, plasma exchange is sometimesused in conjunction with other therapies. Until recently, MEPEXwas the only large trial evaluating the efficacy of plasmaexchange in AAV patients with biopsy provenglomerulonephritis associated with a creatinine concentrationabove 5.8 mg/dL (table 1).14 MEPEX was a EUVAS trial thatrandomized 137 patients (43% PR3-ANCA positive, 52%MPO-ANCA positive) to oral cyclophosphamide and aglucocorticoid taper with either seven plasma exchanges or threedays of pulse methylprednisolone. Patients randomized toplasma exchange were more likely to be alive and free ofdialysis and to have a creatinine concentration below 5.8 mg/dLat three months than were those randomized to pulsemethylprednisolone (69% v 49%; P=0.02). However, four yearsafter randomization, a post hoc analysis found that differencesin ESRD and death were not sustained.91 A subsequentmeta-analysis concluded that insufficient evidence was availableto assess the efficacy of plasma exchange for preventing ESRDand/or death in AAV.92
To assess the ongoing uncertainty about the efficacy of plasmaexchange, PEXIVAS randomized AAV patients withglomerulonephritis (with a glomerular filtration rate <50mL/min/1.73 m2), diffuse alveolar hemorrhage, or both tostandard therapy (rituximab or cyclophosphamide andglucocorticoids) plus plasma exchange or standard therapyonly.56 64 PEXIVAS enrolled 704 patients (41% PR3-ANCApositive, 59% MPO-ANCA positive), 98% of whom had renaldisease. In contrast to MEPEX, both arms received pulsemethylprednisolone. No difference was seen in the rate of ESRDor death from any cause (co-primary endpoints) between patientsrandomized to plasma exchange and those randomized tostandard therapy (28% v 31%; hazard ratio 0.86, 0.65 to 1.13)at seven years. No difference was seen when the outcomes ofESRD and death were analyzed separately.
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 4 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

Despite differences in inclusion criteria and treatment, bothPEXIVAS and MEPEX suggest that plasma exchange does notprovide a long term benefit over standard of care in AAV. Posthoc analyses of PEXIVAS and other trials are needed to clarifythe potential utility of plasma exchange in subgroups of patients.Patients who are positive for both ANCA and anti-glomerularbasement membrane should continue to receive plasmaexchange.93-95
Summary of remission inductionInduction of remission has evolved considerably over the pastfew decades (table 1). Today, high dose glucocorticoids pluseither rituximab or cyclophosphamide are used more often. Caseseries using combination rituximab and cyclophosphamide tospare glucocorticoid exposure have been published, but theevidence base supporting this practice remains weak.96 97 Themain limitation to use of rituximab is its cost,98 althoughbiosimilar rituximab may cost less.99 Toxicity fromcyclophosphamide may be minimized by reducing the dose inpatients with renal impairment and with advancing age, as wellas by limiting duration of treatment. Plasma exchange does notseem to add efficacy for severe disease. In cases of non-severedisease, methotrexate or mycophenolate mofetil may be options,but neither has been compared with rituximab.Additional studies comparing long term outcomes betweentreatments, stratified by ANCA type and other disease features,are warranted in addition to cost effectiveness analyses. Thecost effectiveness of regimens for induction of remission needsto be evaluated from multiple societal perspectives, consideringthe impact of biosimilar rituximab costs and incorporating longterm observational outcome data as they become available.100
Maintenance of remissionThe vast majority of patients with AAV will achieve remissionwith contemporary regimens, but approximately a third ofpatients will relapse by 18 months and less than a third willremain in relapse-free remission for more than a decade.77 101 Apersonalized approach to maintenance of remission based onpatient specific and disease specific factors would balance thebenefits of disease quiescence with the cost and morbidity ofprolonged immunosuppression. This is particularly importantgiven that most deaths occurring more than a year after thediagnosis of AAV are due to infection, malignancy, andcardiovascular disease rather than active vasculitis.34 The past20 years have greatly advanced the approach to maintenance ofremission, with several effective agents and treatment strategiesnow in use.
Oral agentsCyclophosphamide, azathioprine, methotrexate, andmycophenolate mofetil have been investigated in randomizedtrials of maintenance therapy (table 2). All studies inducedremission with prednisone and cyclophosphamide, butcyclophosphamide dosing strategies (daily v pulse, duration)varied between trials.CYCAZAREM was an unblinded, controlled EUVAS trial thatrandomized 144 patients with newly diagnosed severe AAV(57% PR3-ANCA positive, 39% MPO-ANCA positive) toazathioprine or continued cyclophosphamide for maintenanceof remission (table 2). Azathioprine is thought to have efficacybecause of its effect on DNA synthesis. Over 18 months, therelapse rate (severe and non-severe) was similar betweenazathioprine and cyclophosphamide (15.5% v 13.7%; P=0.65).19
CYCAZAREM changed the treatment paradigm in AAV,limiting cyclophosphamide treatment to three to six months toavoid serious morbidity associated with prolongedcyclophosphamide exposure (table 3).102-104
Azathioprine was compared with methotrexate in WEGENT(table 2), a randomized, controlled, unblinded FVSG trial of126 patients with newly diagnosed systemic AAV (60%PR3-ANCA positive, 31% MPO-ANCA positive).20
Methotrexate was hypothesized to have fewer adverse eventsthan azathioprine, but both were found to have similar rates ofadverse events (19% v 11%; P=0.21). The surprisingly highadverse event rate in the methotrexate arm may have resultedfrom a lack of dose adjustment for renal impairment. At 24months, methotrexate and azathioprine had similar rates ofsevere and non-severe relapse-free survival (hazard ratio 0.92,0.52 to 1.65), but the trial was not powered to assess thisoutcome.20
Azathioprine was found to be superior to mycophenolate mofetilfor maintenance of remission in the IMPROVE trial conductedby EUVAS (table 2).21 This was an open label RCT that enrolled156 patients with newly diagnosed AAV (58% PR3-ANCApositive, 33% MPO-ANCA positive). Over a median of 39months, participants randomized to mycophenolate mofetilrelapsed (severe and non-severe) more often than did thoserandomized to azathioprine (hazard ratio 1.80, 1.10 to 2.93).21
Given these observations, both azathioprine and methotrexateare considered effective oral agents for maintenance of remissionin AAV.44 Mycophenolate mofetil remains a potential alternativeagent, particularly given its efficacy in MYCYC, but may beinferior to azathioprine.18 Notable aspects of this evidence baseare that most patients had GPA, were PR3-ANCA positive, andhad severe disease.
RituximabRituximab’s efficacy in inducing remission,16 combined withthe experience of long term B cell depletion in rheumatoidarthritis,105 led to several reports of its use for AAV remissionmaintenance.106-108 Subsequently, two RCTs compared rituximabwith azathioprine for maintenance of remission.MAINRITSAN 1 (table 2), an unblinded, randomized, controlledFVSG trial of 115 newly diagnosed or relapsing patients withAAV (70% PR3-ANCA positive, 23% MPO-ANCA positive),compared rituximab (500 mg twice over 14 days followed byinfusions every six months until month 18) with azathioprine(for 22 months). All patients were treated with pulsecyclophosphamide for induction of remission. Azathioprine wasassociated with more severe relapses than rituximab (29% v5%; hazard ratio 6.61, 1.56 to 27.96).22
At five years, 42 months after the last rituximab infusion,rituximab remained superior to azathioprine but relapse-freesurvival was reduced in both groups (58% v 37%; P=0.01).109
Although few deaths occurred, rituximab was associated withbetter survival at five years (100% v 93%; P=0.045).109
Moreover, a cost effectiveness analysis from the French societalperspective found rituximab to be cost effective compared withazathioprine.110 A notable criticism of MAINRITSAN 1 is thatthe dose of azathioprine was decreased from 2 mg/kg to 1.5mg/kg at 12 months and to 1 mg/kg at 18 months, whereas therituximab exposure remained unchanged.The RITAZAREM study randomized 170 patients (72%PR3-ANCA positive, 28% MPO-ANCA positive) with relapsingdisease to rituximab 1 g every four months or azathioprine formaintenance of remission after induction with rituximab (table2). Preliminary data presented in abstract form showed that
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 5 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from
rituximab was superior to azathioprine for preventing diseaserelapse (13% v 38%; hazard ratio 0.30, 0.15 to 0.60; P<0.001),further supporting the efficacy of rituximab for maintainingremission.25
Timing of rituximabMAINRITSAN 1 and RITAZAREM used a fixed interval ofrituximab retreatment. However, observations that relapses areless frequent in patients with undetectable peripheral B cellsand that rising ANCA titers may predict a flare led toMAINRITSAN 2 (table 2).77 111 112 This open label RCTconducted by the FVSG compared fixed interval rituximab (asused in MAINRITSAN 1) with retreatment only when peripheralB cells became detectable or a significant rise in the ANCA titeroccurred (that is, tailored therapy).113 MAINRITSAN 2 enrolled162 patients with newly diagnosed or relapsing AAV (47%PR3-ANCA positive, 31% MPO-ANCA positive). Fixed intervaland tailored approaches were equivalent with regard to the riskof severe and non-severe relapse over 28 months (10% v 17%;P=0.22). Patients in the tailored arm received significantly fewerrituximab infusions than those in the fixed interval arm (median3 (interquartile range 2-4) versus 5 (5-5)). Safety was similarin the fixed interval and tailored arms (85% v 91% severe events;P=0.5), but numerically fewer patients had infections in thetailored arm (9 v 16). Although the optimal timing and dose ofrituximab retreatment remain uncertain, personalization ofretreatment regimens holds promise.
Duration of treatmentThe optimal duration of AAV maintenance therapy remainsunknown.114 Although some patients can remain in drug-freeremission, the prevalence of relapse increases steadily overtime.101 109 REMAIN, an open label RCT that enrolled 117patients with severe AAV (52% PR3-ANCA positive, 44%MPO-ANCA positive), found that discontinuing azathioprineand prednisone after 24 months of treatment was associatedwith a higher risk of non-severe and severe relapse (63% v 22%;odds ratio 6.0, 2.6 to 13.8) and ESRD (7.8% v 0%; P=0.01)compared with continued treatment for 48 months (table 2).23
Similarly, a meta-analysis of 13 studies which included 983patients with diverse AAV manifestations found that prolongedtreatment with glucocorticoids was associated with fewerrelapses than shorter durations (hazard ratio 0.4, 0.3 to 0.5).115
Being able to stratify patients according to risk of relapse isnecessary to eventually personalize care in a way that optimallybalances the risk of relapse and potential toxicity of variousregimens. Several risk factors for relapse have been identified(table 4). Multiple studies have shown that PR3-ANCA positivepatients have an approximately twofold higher risk of relapsethan MPO-ANCA positive patients.16 101 More severe renaldamage has been associated with a reduced risk ofrelapse.122 129 130 Potential serum and urine biomarkers of diseaseactivity have been identified but need further study beforeclinical use.123 127 Risk stratification and development ofbiomarkers able to predict relapse are critical to personalizingthe approach to maintenance therapy.
Treatment challenges associated withspecific manifestationsSinus involvement, tracheobronchial disease, orbitalpseudotumor, and interstitial lung disease are particularlychallenging manifestations of AAV because they can be thesole manifestation, can be hard to diagnose and treat, and can
cause significant, irreversible damage. Studies of thesemanifestations are limited to case series, providing a limitedevidence base for recommendations.
Sinonasal diseaseSinusitis is common in GPA.36 45 Evaluation by an experiencedotolaryngologist is useful in patients with sinusitis and suspectedGPA, because up to 40% of patients with disease limited to thesinuses and respiratory tract may be ANCA negative and anotolaryngologist can help to differentiate active sinus diseasefrom damage.45 Nasal septal perforation and saddle nosedeformity are well described manifestations of AAV damage,but bony erosion, persistent nasal congestion, crusting, andepistaxis may persist after appropriate treatment. Distinguishingbetween damage and active disease is important, as treatingdamage with immunosuppression may unnecessarily increasethe risks of infection and other complications.No studies have investigated the optimal treatment regimen forsinonasal manifestations, but all agents that have beeninvestigated for induction of remission are thought to beefficacious. In addition, topical treatment with saline andcorticosteroids, as recommended for general chronic sinusitis,131
can be helpful.
Tracheobronchial manifestationsSubglottic stenosis, tracheobronchitis, and bronchial masses areuncommon manifestations of GPA but cause substantialmorbidity.132-134 Tracheobronchial manifestations are oftendecoupled from disease activity elsewhere and can occur duringimmunosuppressive therapy, suggesting that these manifestationsmay not respond to immunomodulation.132-134 In general,bronchial masses are treated with immunosuppression, but themanagement of subglottic stenosis is controversial. One caseseries of 21 patients observed that a series of intralesionalglucocorticoid and dilations over a mean follow-up of 41 monthsdid not result in any tracheostomies, a marked improvementfrom previous reports.135 Other case series of up to 43 patients,in contrast, have reported variable success ofimmunosuppressives (methotrexate, cyclophosphamide,rituximab) in combination with prednisone.132 133 136
Orbital inflammatory diseaseOrbital inflammatory disease is challenging to treat because itoften does not fully respond to immunosuppression and relapsesare common.137 138 One of the largest case series of 59 patientswith orbital masses suggested improved outcomes withrituximab compared with cyclophosphamide (91% v 52%response).138 However, the study’s small sample size andretrospective nature limit the generalizability of these findings.
Interstitial lung diseaseInterstitial lung disease (ILD) is increasingly observed inassociation with MPO-ANCA antibodies with or without othermanifestations of AAV.139-141 Whereas treatment of ILD inpatients with other AAV manifestations follows the typicalapproaches described earlier, the management of ILD and apositive ANCA test without other AAV manifestations isuncertain. In a small case series that included 36 patients,approximately 20-30% of patients with ANCA positivity andILD went on to develop AAV, especially those who wereMPO-ANCA positive.142 A case series of 12 patients with usualinterstitial pneumonia associated with ANCA positivity reportedimprovement in ILD with immunosuppression,143 but other series(n<20) did not report a benefit.144 145 Additional studies of this
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 6 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

unique AAV subgroup are needed. The role of nintedanib infibrotic lung disease associated with ANCA is of interest, givenits efficacy in idiopathic pulmonary fibrosis and sclerodermalung disease.146
Supplementary therapies in AAVTrimethoprim-sulfamethoxazole is an important treatmentadjunct for preventing Pneumocystis jirovecii pneumonia (PCP)in patients with AAV (table 3). Although no randomized studiesexist to guide PCP prophylaxis in patients with rheumatologicdisease, the American Thoracic Society suggests treatment inpatients receiving 20 mg or more of prednisone for four weeksor longer, especially if combined with anotherimmunosuppressive agent.147 Uncertainty exists as to whethertrimethoprim-sulfamethoxazole has a role in preventing relapseof GPA, based on a randomized study in 81 patients that showedbenefit in those with upper airway involvement.148 However, itsefficacy is not thought to be sufficient for it to be used asmonotherapy.44
In addition to calcium and vitamin D, postmenopausal womenand men aged over 50 who are receiving prednisone equivalentof at least 7.5 mg for three months or more or are at high riskfor major osteoporotic fracture (based on FRAX tool) shouldreceive treatment with a bisphosphonate or another agent.149
Finally, reviewing and completing appropriate vaccinations isof particular importance in patients with AAV.
Organ transplantation in AAVRapidly progressive glomerulonephritis and interstitial lungdisease are two manifestations of AAV that can causeirreversible organ failure. Renal transplantation is safe andeffective in appropriately selected patients with ESRD due toAAV.150-152 Among AAV patients with ESRD who are waitlistedfor a transplant, renal transplantation is associated with a 70%reduction in the risk of all cause death (relative risk 0.30, 95%confidence interval 0.25 to 0.37), largely driven by a reductionin the risk of death due to cardiovascular disease (0.10, 0.06 to0.16).153 Although recommendations vary, patients with a lowglomerular filtration rate (<20 mL/min/1.73 m2) withoutexpected recovery should be evaluated for transplantationcandidacy, ideally before dialysis.154 AAV should be in remissionfor at least 12 months and the ANCA titer should be negativebefore transplantation.155 156 In contrast to renal disease, outcomesin lung transplantation for AAV are poorly described.157
Quality of life in AAVAAV is associated with depression and anxiety, as well as aworse quality of life compared with the general population.158-161
These differences often persist in disease remission and highlightthe challenges of managing both the physical and psychosocialaspects of living with AAV. When reported, quality of lifeoutcomes in AAV trials have not differed between treatmentarms. Differences in quality of life observed in MAINRITSAN1 are difficult to interpret because completion of the survey wasoptional and a significant amount of data is missing.162 Therecent development of an AAV specific patient reported outcomemeasure will enable the assessment of AAV specific quality oflife (for example, AAV symptoms, side effects, emotionalimpact, uncertainty) in future studies.163 No studies haveevaluated psychosocial interventions in AAV.
Emerging treatmentsThe development of novel agents and optimization of the useof existing therapeutics are rapidly evolving research areas inAAV. Given the recognition of the importance of thecomplement pathway in the pathogenesis of AAV, several agentstargeting the complement activation product C5a are beingstudied, including a phase III trial of avacopan, an oral C5areceptor inhibitor, for induction of remission. Two phase IIstudies, CLEAR and CLASSIC, showed the potential efficacyof avacopan in inducing remission in combination withrituximab or cyclophosphamide.55 164 The CLEAR studysuggested that avacopan may have a dramatic steroid sparingeffect, which would be a tremendous advance.55 IFX-1, amonoclonal antibody targeting C5a, is being studied in phaseII trials.165 In addition to complement pathway targets, a phaseIII trial is studying abatacept, a cytotoxic T lymphocyteassociated protein 4 antagonist, for non-severe GPA.166 167
The optimal dose and duration of glucocorticoid treatmentremains an area of active investigation in both induction andmaintenance of remission.125 167-170 For example, a single centerstudy of 49 patients found that the combination of rituximaband cyclophosphamide with two weeks or less of glucocorticoidsled to 96% of patients achieving remission at six months.125
A growing evidence base suggests that personalized approachesto treatment of AAV may be possible. Identifying optimalstrategies that balance the adverse events and cost ofmaintenance therapy against morbidity associated with activedisease and treatment is a critical area of future investigation.In particular, remission induction and maintenance studiesstratified by ANCA type can further elucidate whetherPR3-ANCA positive and MPO-ANCA positive patients responddifferently to treatment. Additional studies of non-severe AAVare essential to assess the efficacy of less toxic treatment options.
GuidelinesThe European League Against Rheumatism (EULAR) and theBritish Society for Rheumatology (BSR) have publishedguidelines on the management of AAV.44 81 Notably, both werewritten before the publication of several recent pivotal trials, sotheir recommendations should be interpreted cautiously. Generalagreement exists between the EULAR and BSR guidelines.Both reflect the growing therapeutic options that clinicians havefor induction and maintenance of remission in AAV. Bothguidelines advocate for prolonged glucocorticoid exposure,which remains controversial. The EULAR and BSR guidelinesemphasize the need to routinely assess patients for diseaserelated and treatment related toxicities, including cardiovasculardisease, diabetes, and hypogammaglobulinemia, which couldnot be covered in this review.
ConclusionManagement of AAV has evolved considerably in recentdecades, a period characterized by substantial improvements inoutcomes, including renal outcomes and overall survival. Asour understanding of the pathogenesis of AAV expands, so toodoes the pipeline of therapeutic options for AAV, especiallythose with the potential to substantially reduce glucocorticoidexposure. Additional studies are needed to define personalizedapproaches to the management of AAV.
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 7 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

Research questions1.Should induction and maintenance of remission be managed differently
for patients with ANCA associated vasculitis (AAV) who are PR3-ANCApositive and those who are MPO-ANCA positive?
2.What are the risks and benefits of reducing the cumulative exposure toand/or duration of glucocorticoid therapy used during induction andmaintenance of remission?
3.What is the comparative effectiveness of methotrexate, mycophenolatemofetil, and rituximab for non-severe AAV?
4.What interventions can effectively improve the quality of life of patientswith AAV and meet their psychosocial needs?
Glossary of abbreviationsAAV—ANCA associated vasculitisANCA—anti-neutrophil cytoplasmic antibodyBSR—British Society for RheumatologyEGPA—eosinophilic granulomatosis with polyangiitisESRD—end stage renal diseaseEULAR—European League Against RheumatismEUVAS—European Vasculitis Study GroupFVSG—French Vasculitis Study GroupGDCN—Glomerular Disease Collaborative NetworkGPA—granulomatosis with polyangiitisILD—interstitial lung diseaseMPO—myeloperoxidaseNET—neutrophil extracellular trapPCP—Pneumocystis jirovecii pneumoniaPR3—proteinase 3RCT—randomized controlled trialVCRC—Vasculitis Clinical Research Consortium
Patient involvementThree patients from our practice kindly volunteered to review this manuscript.In response to their feedback, minor edits were made to the manuscript. Onewas a 40 year old man with ANCA associated vasculitis (AAV) who hascutaneous vasculitis, arthritis, and pulmonary masses. He suggestedhighlighting the importance of early diagnosis and treatment recommendationand appreciated our proposal to study psychosocial interventions for AAV.The second patient was a 60 year old man with AAV who has sinusitis,pulmonary nodules, and neuropathy. He suggested highlighting the balanceof costs and benefits of fixed rituximab maintenance therapy. The third patientwas a 67 year old man with AAV causing scleritis, sialadenitis, hearing loss,pancreatitis, sinusitis, and lung nodules. He appreciated the value of thismanuscript but did not recommend any specific changes.
Contributors: ZSW had the idea for the article. Both authors did the literature searchand planned and wrote the article. ZSW accepts full responsibility for the finishedarticle, had access to any data, and controlled the decision to publish; he is theguarantor.
Funding: ZSW receives funding from NIH/NIAMS (K23AR073334 and L30AR070520).
Competing interests: We have read and understood the BMJ Group policy ondeclaration of interests and declare the follow interests: none.
Provenance and peer review: Commissioned; externally peer reviewed.
1 Jennette JC, Falk RJ, Bacon PA, etal . 2012 revised International Chapel Hill ConsensusConference Nomenclature of Vasculitides. Arthritis Rheum 2013;65:1-11.10.1002/art.37715 23045170
2 Cornec D, Cornec-Le Gall E, Fervenza FC, Specks U. ANCA-associated vasculitis -clinical utility of using ANCA specificity to classify patients. Nat Rev Rheumatol2016;12:570-9. 10.1038/nrrheum.2016.123 27464484
3 Bosch X, Guilabert A, Font J. Antineutrophil cytoplasmic antibodies. Lancet2006;368:404-18. 10.1016/S0140-6736(06)69114-9 16876669
4 Guillevin L, Durand-Gasselin B, Cevallos R, etal . Microscopic polyangiitis: clinical andlaboratory findings in eighty-five patients. Arthritis Rheum 1999;42:421-30.10.1002/1529-0131(199904)42:3<421::AID-ANR5>3.0.CO;2-6 10088763
5 Finkielman JD, Lee AS, Hummel AM, etal. WGET Research Group. ANCA are detectablein nearly all patients with active severe Wegener’s granulomatosis. Am J Med2007;120:643. 10.1016/j.amjmed.2006.08.016 17602941
6 Pagnoux C, Springer J. Editorial: Classifying antineutrophil cytoplasmic antibody(ANCA)-associated vasculitides according to ANCA type or phenotypic diagnosis: salt orpepper?Arthritis Rheumatol 2016;68:2837-40. 10.1002/art.39860 27588958
7 Unizony S, Villarreal M, Miloslavsky EM, etal. RAVE-ITN Research Group. Clinicaloutcomes of treatment of anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitisbased on ANCA type. Ann Rheum Dis 2016;75:1166-9.10.1136/annrheumdis-2015-208073 26621483
8 Rahmattulla C, Mooyaart AL, van Hooven D, etal. European Vasculitis GeneticsConsortium. Genetic variants in ANCA-associated vasculitis: a meta-analysis. Ann RheumDis 2016;75:1687-92. 10.1136/annrheumdis-2015-207601 26443607
9 Hilhorst M, van Paassen P, Tervaert JWLimburg Renal Registry. Proteinase 3-ANCAVvasculitis versus Mmyeloperoxidase-ANCA Vasculitis. J Am Soc Nephrol2015;26:2314-27. 10.1681/ASN.2014090903 25956510
10 Lyons PA, Rayner TF, Trivedi S, etal . Genetically distinct subsets within ANCA-associatedvasculitis. N Engl J Med 2012;367:214-23. 10.1056/NEJMoa1108735 22808956
11 Guillevin L, Cordier JF, Lhote F, etal . A prospective, multicenter, randomized trialcomparing steroids and pulse cyclophosphamide versus steroids and oralcyclophosphamide in the treatment of generalized Wegener’s granulomatosis. ArthritisRheum 1997;40:2187-98. 10.1002/art.1780401213 9416856
12 De Groot K, Rasmussen N, Bacon PA, etal . Randomized trial of cyclophosphamideversus methotrexate for induction of remission in early systemic antineutrophil cytoplasmicantibody-associated vasculitis. Arthritis Rheum 2005;52:2461-9.10.1002/art.21142 16052573
13 Wegener’s Granulomatosis Etanercept Trial (WGET) Research Group. Etanercept plusstandard therapy for Wegener’s granulomatosis. N Engl J Med 2005;352:351-61.10.1056/NEJMoa041884 15673801
14 Jayne DR, Gaskin G, Rasmussen N, etal. European Vasculitis Study Group. Randomizedtrial of plasma exchange or high-dosage methylprednisolone as adjunctive therapy forsevere renal vasculitis. J Am Soc Nephrol 2007;18:2180-8.10.1681/ASN.2007010090 17582159
15 de Groot K, Harper L, Jayne DR, etal. EUVAS (European Vasculitis Study Group). Pulseversus daily oral cyclophosphamide for induction of remission in antineutrophil cytoplasmicantibody-associated vasculitis: a randomized trial. Ann Intern Med 2009;150:670-80.10.7326/0003-4819-150-10-200905190-00004 19451574
16 Stone JH, Merkel PA, Spiera R, etal. RAVE-ITN Research Group. Rituximab versuscyclophosphamide for ANCA-associated vasculitis. N Engl J Med 2010;363:221-32.10.1056/NEJMoa0909905 20647199
17 Jones RB, Tervaert JW, Hauser T, etal. European Vasculitis Study Group. Rituximabversus cyclophosphamide in ANCA-associated renal vasculitis. N Engl J Med2010;363:211-20. 10.1056/NEJMoa0909169 20647198
18 Jones RB, Hiemstra TF, Ballarin J, etal. European Vasculitis Study Group (EUVAS).Mycophenolate mofetil versus cyclophosphamide for remission induction inANCA-associated vasculitis: a randomised, non-inferiority trial. Ann Rheum Dis2019;78:399-405. 10.1136/annrheumdis-2018-214245 30612116
19 Jayne D, Rasmussen N, Andrassy K, etal. European Vasculitis Study Group. A randomizedtrial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmicautoantibodies. N Engl J Med 2003;349:36-44. 10.1056/NEJMoa020286 12840090
20 Pagnoux C, Mahr A, Hamidou MA, etal. French Vasculitis Study Group. Azathioprine ormethotrexate maintenance for ANCA-associated vasculitis. N Engl J Med2008;359:2790-803. 10.1056/NEJMoa0802311 19109574
21 Hiemstra TF, Walsh M, Mahr A, etal. European Vasculitis Study Group (EUVAS).Mycophenolate mofetil vs azathioprine for remission maintenance in antineutrophilcytoplasmic antibody-associated vasculitis: a randomized controlled trial. JAMA2010;304:2381-8. 10.1001/jama.2010.1658 21060104
22 Guillevin L, Pagnoux C, Karras A, etal. French Vasculitis Study Group. Rituximab versusazathioprine for maintenance in ANCA-associated vasculitis. N Engl J Med2014;371:1771-80. 10.1056/NEJMoa1404231 25372085
23 Karras A, Pagnoux C, Haubitz M, etal. European Vasculitis Society. Randomised controlledtrial of prolonged treatment in the remission phase of ANCA-associated vasculitis. AnnRheum Dis 2017;76:1662-8. 10.1136/annrheumdis-2017-211123 28546260
24 Charles P, Terrier B, Perrodeau É, etal. French Vasculitis Study Group. Comparison ofindividually tailored versus fixed-schedule rituximab regimen to maintain ANCA-associatedvasculitis remission: results of a multicentre, randomised controlled, phase III trial(MAINRITSAN2). Ann Rheum Dis 2018;77:1143-9.29695500
25 Smith R, Jayne D, Merkel PA. A randomized, controlled trial of rituximab versusazathioprine after induction of remission with rituximab for patients with ANCA-associatedvasculitis and relapsing disease [abstract 806]. Arthritis Rheumatol 2019;71(suppl 10).
26 Rhee RL, Hogan SL, Poulton CJ, etal . Trends in long-term outcomes among patientswith antineutrophil cytoplasmic antibody-associated vasculitis with renal disease. ArthritisRheumatol 2016;68:1711-20. 10.1002/art.39614 26814428
27 Wallace ZS, Zhang Y, Lu N, Stone JH, Choi HK. . Improving Mortality in End-Stage RenalDisease Due to Granulomatosis With Polyangiitis (Wegener’s) From 1995 to 2014: DataFrom the United States Renal Data System. Arthritis Care Res (Hoboken)2018;70:1495-500. 10.1002/acr.23521 29361200
28 Wallace ZS, Lu N, Miloslavsky E, Unizony S, Stone JH, Choi HK. Nationwide Trends inHospitalizations and In-Hospital Mortality in Granulomatosis With Polyangiitis (Wegener’s).Arthritis Care Res (Hoboken) 2017;69:915-21. 10.1002/acr.22976 27389595
29 Wallace ZS, Lu N, Unizony S, Stone JH, Choi HK. Improved survival in granulomatosiswith polyangiitis: A general population-based study. Semin Arthritis Rheum 2016;45:483-9.10.1016/j.semarthrit.2015.07.009 26323883
30 Holle JU, Gross WL, Latza U, etal . Improved outcome in 445 patients with Wegener’sgranulomatosis in a German vasculitis center over four decades. Arthritis Rheum2011;63:257-66. 10.1002/art.27763 20862686
31 Rahmattulla C, Berden AE, Wakker SC, etal . Incidence of malignancies in patients withantineutrophil cytoplasmic antibody-associated vasculitis diagnosed between 1991 and2013. Arthritis Rheumatol 2015;67:3270-8. 10.1002/art.39317 26246307
32 van Daalen EE, Rizzo R, Kronbichler A, etal . Effect of rituximab on malignancy risk inpatients with ANCA-associated vasculitis. Ann Rheum Dis 2017;76:1064-9.10.1136/annrheumdis-2016-209925 27899372
33 Heijl C, Harper L, Flossmann O, etal. European Vasculitis Study Group (EUVAS). Incidenceof malignancy in patients treated for antineutrophil cytoplasm antibody-associated
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 8 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from
vasculitis: follow-up data from European Vasculitis Study Group clinical trials. Ann RheumDis 2011;70:1415-21. 10.1136/ard.2010.145250 21616914
34 Flossmann O, Berden A, de Groot K, etal. European Vasculitis Study Group. Long-termpatient survival in ANCA-associated vasculitis. Ann Rheum Dis 2011;70:488-94.10.1136/ard.2010.137778 21109517
35 Tan JA, Dehghan N, Chen W, Xie H, Esdaile JM, Avina-Zubieta JA. Mortality inANCA-associated vasculitis: ameta-analysis of observational studies. Ann Rheum Dis2017;76:1566-74. 10.1136/annrheumdis-2016-210942 28468793
36 Robson J, Doll H, Suppiah R, etal . Damage in the anca-associated vasculitides: long-termdata from the European vasculitis study group (EUVAS) therapeutic trials. Ann RheumDis 2015;74:177-84. 10.1136/annrheumdis-2013-203927 24243925
37 Berti A, Cornec D, Crowson CS, Specks U, Matteson EL. The Epidemiology ofAntineutrophil Cytoplasmic Autoantibody-Associated Vasculitis in Olmsted County,Minnesota: A Twenty-Year US Population-Based Study. Arthritis Rheumatol2017;69:2338-50. 10.1002/art.40313 28881446
38 Panupattanapong S, Stwalley DL, White AJ, Olsen MA, French AR, Hartman ME.Epidemiology and Outcomes of Granulomatosis With Polyangiitis in Pediatric andWorking-Age Adult Populations In the United States: Analysis of a Large National ClaimsDatabase. Arthritis Rheumatol 2018;70:2067-76. 10.1002/art.40577 29806148
39 Watts RA, Al-Taiar A, Scott DG, Macgregor AJ. Prevalence and incidence of Wegener’sgranulomatosis in the UK general practice research database. Arthritis Rheum2009;61:1412-6. 10.1002/art.24544 19790134
40 Stone JH, Hoffman GS, Merkel PA, etal. International Network for the Study of the SystemicVasculitides (INSSYS). A disease-specific activity index for Wegener’s granulomatosis:modification of the Birmingham Vasculitis Activity Score. Arthritis Rheum 2001;44:912-20.10.1002/1529-0131(200104)44:4<912::AID-ANR148>3.0.CO;2-5 11318006
41 van der Woude FJ, Rasmussen N, Lobatto S, etal . Autoantibodies against neutrophilsand monocytes: tool for diagnosis and marker of disease activity in Wegener’sgranulomatosis. Lancet 1985;1:425-9. 10.1016/S0140-6736(85)91147-X 2857806
42 Keller SF, Miloslavsky EM. Corticosteroids in antineutrophil cytoplasmicantibody-associated vasculitis. Rheum Dis Clin North Am 2016;42:91-101, viii.10.1016/j.rdc.2015.08.010 26611553
43 Bosch X, Guilabert A, Espinosa G, Mirapeix E. Treatment of antineutrophil cytoplasmicantibody associated vasculitis: a systematic review. JAMA 2007;298:655-69.10.1001/jama.298.6.655 17684188
44 Yates M, Watts RA, Bajema IM, etal . EULAR/ERA-EDTA recommendations for themanagement of ANCA-associated vasculitis. Ann Rheum Dis 2016;75:1583-94.10.1136/annrheumdis-2016-209133 27338776
45 Hoffman GS, Kerr GS, Leavitt RY, etal . Wegener granulomatosis: an analysis of 158patients. Ann Intern Med 1992;116:488-98. 10.7326/0003-4819-116-6-488 1739240
46 Fauci AS, Haynes BF, Katz P, Wolff SM. Wegener’s granulomatosis: prospective clinicaland therapeutic experience with 85 patients for 21 years. Ann Intern Med 1983;98:76-85.10.7326/0003-4819-98-1-76 6336643
47 Tan JA, Choi HK, Xie H, Sayre EC, Esdaile JM, Aviña-Zubieta JA. All-Cause andCause-Specific Mortality in Patients With Granulomatosis With Polyangiitis: APopulation-Based Study. Arthritis Care Res (Hoboken) 2019;71:155-63.10.1002/acr.23587 29692001
48 Merkel PA, Xie G, Monach PA, etal. Vasculitis Clinical Research Consortium. Identificationof functional and expression polymorphisms associated with risk for antineutrophilcytoplasmic autoantibody-associated vasculitis. Arthritis Rheumatol 2017;69:1054-66.10.1002/art.40034 28029757
49 Xie G, Roshandel D, Sherva R, etal . Association of granulomatosis with polyangiitis(Wegener’s) with HLA-DPB1*04 and SEMA6A gene variants: evidence from genome-wideanalysis. Arthritis Rheum 2013;65:2457-68. 10.1002/art.38036 23740775
50 Jennette JC, Falk RJ. Pathogenesis of antineutrophil cytoplasmic autoantibody-mediateddisease. Nat Rev Rheumatol 2014;10:463-73. 10.1038/nrrheum.2014.103 25003769
51 Xiao H, Heeringa P, Hu P, etal . Antineutrophil cytoplasmic autoantibodies specific formyeloperoxidase cause glomerulonephritis and vasculitis in mice. J Clin Invest2002;110:955-63. 10.1172/JCI0215918 12370273
52 Wallace ZS, Stone JH. Personalized Medicine in ANCA-Associated Vasculitis ANCASpecificity as the Guide?Front Immunol 2019;10:2855.10.3389/fimmu.2019.02855 31867013
53 Kessenbrock K, Krumbholz M, Schönermarck U, etal . Netting neutrophils in autoimmunesmall-vessel vasculitis. Nat Med 2009;15:623-5. 10.1038/nm.1959 19448636
54 Wu EY, McInnis EA, Boyer-Suavet S, etal . Measuring Circulating Complement ActivationProducts in Myeloperoxidase- and Proteinase 3-Antineutrophil CytoplasmicAntibody-Associated Vasculitis. Arthritis Rheumatol 2019;71:1894-903.10.1002/art.41011 31215772
55 Jayne DRW, Bruchfeld AN, Harper L, etal. CLEAR Study Group. Randomized trial of c5areceptor inhibitor avacopan in ANCA-associated vasculitis. J Am Soc Nephrol2017;28:2756-67. 10.1681/ASN.2016111179 28400446
56 Walsh M, Merkel PA, Peh CA, etal. PEXIVAS Investigators. Plasma Exchange andGlucocorticoids in Severe ANCA-Associated Vasculitis. N Engl J Med 2020;382:622-31.10.1056/NEJMoa1803537 32053298
57 Jayne D. 22. Lessons from the European Vasculitis Study Group trials. Rheumatology(Oxford) 2014;53(suppl 2):i1210.1093/rheumatology/keu209 .
58 Monti S, Quinn K, Christensen R, etal. Treatment Response Criteria for Anti-neutrophilCytoplasmic Antibodies (ANCA)-vasculitis: Results of a Scoping Review [abstract 2791].Arthritis Rheumatol 2019;71(suppl 10).
59 Stahn C, Buttgereit F. Genomic and nongenomic effects of glucocorticoids. Nat Clin PractRheumatol 2008;4:525-33. 10.1038/ncprheum0898 18762788
60 Moore PM, Beard EE, Thoburn TW, Williams HL. Idiopathic (lethal) granuloma of themidline facial tissues treated with cortisone: report of a case. Laryngoscope1951;61:320-31. 10.1288/00005537-195104000-00004 14825921
61 Walton EW. Giant-cell granuloma of the respiratory tract (Wegener’s granulomatosis). BrMed J 1958;2:265-70. 10.1136/bmj.2.5091.265 13560836
62 Bolton WK, Sturgill BC. Methylprednisolone therapy for acute crescentic rapidly progressiveglomerulonephritis. Am J Nephrol 1989;9:368-75. 10.1159/000167998 2801784
63 Hoang LT, Lim LL, Vaillant B, Choi D, Rosenbaum JT. Antineutrophil cytoplasmicantibody-associated active scleritis. Arch Ophthalmol 2008;126:651-5.10.1001/archopht.126.5.651 18474775
64 Walsh M, Merkel PA, Peh CA, etal. PEXIVAS Investigators. Plasma exchange andglucocorticoid dosing in the treatment of anti-neutrophil cytoplasm antibody associatedvasculitis (PEXIVAS): protocol for a randomized controlled trial. Trials 2013;14:73.10.1186/1745-6215-14-73 23497590
65 Miloslavsky EM, Naden RP, Bijlsma JWJ, etal . Development of a Glucocorticoid ToxicityIndex (GTI) using multicriteria decision analysis. Ann Rheum Dis 2017;76:543-6.10.1136/annrheumdis-2016-210002 27474764
66 Fauci AS, Wolff SM. Wegener’s granulomatosis: studies in eighteen patients and a reviewof the literature. Medicine (Baltimore) 1973;52:535-61.10.1097/00005792-197311000-00002 4748591
67 Cupps TR, Edgar LC, Fauci AS. Suppression of human B lymphocyte function bycyclophosphamide. J Immunol 1982;128:2453-7.6978904
68 Zhu LP, Cupps TR, Whalen G, Fauci AS. Selective effects of cyclophosphamide therapyon activation, proliferation, and differentiation of human B cells. J Clin Invest1987;79:1082-90. 10.1172/JCI112922 3494044
69 Stevenson HC, Fauci AS. Activation of human B lymphocytes. XII. Differential effects ofin vitro cyclophosphamide on human lymphocyte subpopulations involved in B-cellactivation. Immunology 1980;39:391-7.7002766
70 Popa ER, Stegeman CA, Bos NA, Kallenberg CG, Tervaert JW. Differential B- and T-cellactivation in Wegener’s granulomatosis. J Allergy Clin Immunol 1999;103:885-94.10.1016/S0091-6749(99)70434-3 10329824
71 Haubitz M, Schellong S, Göbel U, etal . Intravenous pulse administration ofcyclophosphamide versus daily oral treatment in patients with antineutrophil cytoplasmicantibody-associated vasculitis and renal involvement: a prospective, randomized study.Arthritis Rheum 1998;41:1835-44.10.1002/1529-0131(199810)41:10<1835::AID-ART16>3.0.CO;2-Q 9778225
72 Adu D, Pall A, Luqmani RA, etal . Controlled trial of pulse versus continuous prednisoloneand cyclophosphamide in the treatment of systemic vasculitis. QJM 1997;90:401-9.10.1093/qjmed/90.6.401 9205678
73 Harper L, Morgan MD, Walsh M, etal. EUVAS investigators. Pulse versus daily oralcyclophosphamide for induction of remission in ANCA-associated vasculitis: long-termfollow-up. Ann Rheum Dis 2012;71:955-60. 10.1136/annrheumdis-2011-200477 22128076
74 Specks U, Fervenza FC, McDonald TJ, Hogan MC. Response of Wegener’sgranulomatosis to anti-CD20 chimeric monoclonal antibody therapy. Arthritis Rheum2001;44:2836-40.10.1002/1529-0131(200112)44:12<2836::AID-ART471>3.0.CO;2-W 11762944
75 Keogh KA, Ytterberg SR, Fervenza FC, Carlson KA, Schroeder DR, Specks U. Rituximabfor refractory Wegener’s granulomatosis: report of a prospective, open-label pilot trial.Am J Respir Crit Care Med 2006;173:180-7. 10.1164/rccm.200507-1144OC 16224107
76 Keogh KA, Wylam ME, Stone JH, Specks U. Induction of remission by B lymphocytedepletion in eleven patients with refractory antineutrophil cytoplasmic antibody-associatedvasculitis. Arthritis Rheum 2005;52:262-8. 10.1002/art.20718 15641078
77 Specks U, Merkel PA, Seo P, etal. RAVE-ITN Research Group. Efficacy ofremission-induction regimens for ANCA-associated vasculitis. N Engl J Med2013;369:417-27. 10.1056/NEJMoa1213277 23902481
78 Geetha D, Specks U, Stone JH, etal. Rituximab for ANCA-Associated Vasculitis ImmuneTolerance Network Research Group. Rituximab versus cyclophosphamide forANCA-associated vasculitis with renal involvement. J Am Soc Nephrol 2015;26:976-85.10.1681/ASN.2014010046 25381429
79 Specks U. Pro: Should all patients with anti-neutrophil cytoplasmic antibody-associatedvasculitis be primarily treated with rituximab?Nephrol Dial Transplant 2015;30:1083-7.10.1093/ndt/gfv217 25999375
80 Kronbichler A, Jayne DR. Con: Should all patients with anti-neutrophil cytoplasmicantibody-associated vasculitis be primarily treated with rituximab?Nephrol Dial Transplant2015;30:1075-81. 10.1093/ndt/gfv216 25999374
81 Ntatsaki E, Carruthers D, Chakravarty K, etal. BSR and BHPR Standards, Guidelinesand Audit Working Group. BSR and BHPR guideline for the management of adults withANCA-associated vasculitis. Rheumatology (Oxford) 2014;53:2306-9.10.1093/rheumatology/ket445 24729399
82 Brown PM, Pratt AG, Isaacs JD. Mechanism of action of methotrexate in rheumatoidarthritis, and the search for biomarkers. Nat Rev Rheumatol 2016;12:731-42.10.1038/nrrheum.2016.175 27784891
83 Hoffman GS, Leavitt RY, Kerr GS, Fauci AS. The treatment of Wegener’s granulomatosiswith glucocorticoids and methotrexate. Arthritis Rheum 1992;35:1322-9.10.1002/art.1780351113 1445449
84 Sneller MC, Hoffman GS, Talar-Williams C, Kerr GS, Hallahan CW, Fauci AS. An analysisof forty-two Wegener’s granulomatosis patients treated with methotrexate and prednisone.Arthritis Rheum 1995;38:608-13. 10.1002/art.1780380505 7748215
85 Stone JH, Tun W, Hellman DB. Treatment of non-life threatening Wegener’sgranulomatosis with methotrexate and daily prednisone as the initial therapy of choice. JRheumatol 1999;26:1134-9.10332980
86 de Groot K, Mühler M, Reinhold-Keller E, Paulsen J, Gross WL. Induction of remissionin Wegener’s granulomatosis with low dose methotrexate. J Rheumatol1998;25:492-5.9517769
87 Ridker PM, Everett BM, Pradhan A, etal. CIRT Investigators. Low-dose methotrexate forthe prevention of atherosclerotic events. N Engl J Med 2019;380:752-62.10.1056/NEJMoa1809798 30415610
88 Han F, Liu G, Zhang X, etal . Effects of mycophenolate mofetil combined withcorticosteroids for induction therapy of microscopic polyangiitis. Am J Nephrol2011;33:185-92. 10.1159/000324364 21311184
89 Hu W, Liu C, Xie H, Chen H, Liu Z, Li L. Mycophenolate mofetil versus cyclophosphamidefor inducing remission of ANCA vasculitis with moderate renal involvement. Nephrol DialTransplant 2008;23:1307-12. 10.1093/ndt/gfm780 18065810
90 Stassen PM, Tervaert JW, Stegeman CA. Induction of remission in active anti-neutrophilcytoplasmic antibody-associated vasculitis with mycophenolate mofetil in patients whocannot be treated with cyclophosphamide. Ann Rheum Dis 2007;66:798-802.10.1136/ard.2006.060301 17179175
91 Walsh M, Casian A, Flossmann O, etal. European Vasculitis Study Group (EUVAS).Long-term follow-up of patients with severe ANCA-associated vasculitis comparing plasmaexchange to intravenous methylprednisolone treatment is unclear. Kidney Int2013;84:397-402. 10.1038/ki.2013.131 23615499
92 Walsh M, Catapano F, Szpirt W, etal . Plasma exchange for renal vasculitis and idiopathicrapidly progressive glomerulonephritis: a meta-analysis. Am J Kidney Dis 2011;57:566-74.10.1053/j.ajkd.2010.10.049 21194817
93 Levy JB, Turner AN, Rees AJ, Pusey CD. Long-term outcome of anti-glomerular basementmembrane antibody disease treated with plasma exchange and immunosuppression.Ann Intern Med 2001;134:1033-42.10.7326/0003-4819-134-11-200106050-00009 11388816
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 9 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from
94 Jindal KK. Management of idiopathic crescentic and diffuse proliferative glomerulonephritis:evidence-based recommendations. Kidney Int Suppl 1999;70:S33-40.10.1046/j.1523-1755.1999.07005.x 10369193
95 Cui Z, Zhao J, Jia XY, etal . Anti-glomerular basement membrane disease: outcomes ofdifferent therapeutic regimens in a large single-center Chinese cohort study. Medicine(Baltimore) 2011;90:303-11. 10.1097/MD.0b013e31822f6f68 21862934
96 Pepper RJ, McAdoo SP, Moran SM, etal . A novel glucocorticoid-free maintenance regimenfor anti-neutrophil cytoplasm antibody-associated vasculitis. Rheumatology (Oxford)2019;58:260-8.30239910
97 Cortazar FB, Muhsin SA, Pendergraft WF3rd, etal . Combination Therapy With Rituximaband Cyclophosphamide for Remission Induction in ANCA Vasculitis. Kidney Int Rep2017;3:394-402. 10.1016/j.ekir.2017.11.004 29725643
98 NHS England Specialised Services Clinical Reference Group for SpecialisedRheumatology. Clinical Commissioning Policy: Rituximab for the treatment ofANCA-associated vasculitis in adults. 2015. https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2015/01/a13-ritux-anca-vascul.pdf.
99 Kay J, Schoels MM, Dörner T, etal. Task Force on the Use of Biosimilars to TreatRheumatological Diseases. Consensus-based recommendations for the use of biosimilarsto treat rheumatological diseases. Ann Rheum Dis 2018;77:165-74.10.1136/annrheumdis-2017-211937 28866648
100 Latimer NR, Carroll C, Wong R, Tappenden P, Venning MC, Luqmani R. Rituximab incombination with corticosteroids for the treatment of anti-neutrophil cytoplasmicantibody-associated vasculitis: a NICE single technology appraisal. Pharmacoeconomics2014;32:1171-83. 10.1007/s40273-014-0189-z 25059204
101 Puéchal X, Pagnoux C, Perrodeau É, etal. French Vasculitis Study Group. Long-termoutcomes among participants in the WEGENT trial of remission-maintenance therapy forgranulomatosis with polyangiitis (Wegener’s) or microscopic polyangiitis. ArthritisRheumatol 2016;68:690-701. 10.1002/art.39450 26473755
102 Pryor BD, Bologna SG, Kahl LE. Risk factors for serious infection during treatment withcyclophosphamide and high-dose corticosteroids for systemic lupus erythematosus.Arthritis Rheum 1996;39:1475-82. 10.1002/art.1780390906 8814058
103 Qiu TT, Zhang C, Zhao HW, Zhou JW. Calcineurin inhibitors versus cyclophosphamidefor idiopathic membranous nephropathy: A systematic review and meta-analysis of 21clinical trials. Autoimmun Rev 2017;16:136-45. 10.1016/j.autrev.2016.12.005 27988429
104 Clowse MEB, Copland SC, Hsieh TC, etal. WGET Research Group. Ovarian reservediminished by oral cyclophosphamide therapy for granulomatosis with polyangiitis(Wegener’s). Arthritis Care Res (Hoboken) 2011;63:1777-81. 10.1002/acr.20605 22127969
105 Keystone E, Fleischmann R, Emery P, etal . Safety and efficacy of additional courses ofrituximab in patients with active rheumatoid arthritis: an open-label extension analysis.Arthritis Rheum 2007;56:3896-908. 10.1002/art.23059 18050221
106 Pendergraft WF3rd, Cortazar FB, Wenger J, etal . Long-term maintenance therapy usingrituximab-induced continuous B-cell depletion in patients with ANCA vasculitis. Clin J AmSoc Nephrol 2014;9:736-44. 10.2215/CJN.07340713 24626432
107 Smith RM, Jones RB, Guerry MJ, etal . Rituximab for remission maintenance in relapsingantineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum 2012;64:3760-9.10.1002/art.34583 22729997
108 Cartin-Ceba R, Golbin JM, Keogh KA, etal . Rituximab for remission induction andmaintenance in refractory granulomatosis with polyangiitis (Wegener’s): ten-yearexperience at a single center. Arthritis Rheum 2012;64:3770-8.10.1002/art.34584 22730028
109 Terrier B, Pagnoux C, Perrodeau É, etal. French Vasculitis Study Group. Long-termefficacy of remission-maintenance regimens for ANCA-associated vasculitides. AnnRheum Dis 2018;77:1150-6. 10.1136/annrheumdis-2017-212768 29724729
110 Montante A, Le Bras A, Pagnoux C, etal. French Vasculitis Study Group. Cost-effectivenessof rituximab versus azathioprine for maintenance treatment in antineutrophil cytoplasmicantibody-associated vasculitis. Clin Exp Rheumatol 2019;37(Suppl 117):137-43.31162031
111 Jones RB, Furuta S, Tervaert JWC, etal. European Vasculitis Society (EUVAS). Rituximabversus cyclophosphamide in ANCA-associated renal vasculitis: 2-year results of arandomised trial. Ann Rheum Dis 2015;74:1178-82.10.1136/annrheumdis-2014-206404 25739829
112 Tomasson G, Grayson PC, Mahr AD, Lavalley M, Merkel PA. Value of ANCAmeasurements during remission to predict a relapse of ANCA-associated vasculitis--ameta-analysis. Rheumatology (Oxford) 2012;51:100-9.10.1093/rheumatology/ker280 22039267
113 ClinicalTrials.gov. Comparison Study of Two Rituximab Regimens in the Remission ofANCA Associated Vasculitis. 2018. https://clinicaltrials.gov/ct2/show/NCT01731561.
114 Specks U. Accurate relapse prediction in ANCA-associated vasculitis-the search for theHoly Grail. J Am Soc Nephrol 2015;26:505-7. 10.1681/ASN.2014080817 25324503
115 Walsh M, Merkel PA, Mahr A, Jayne D. Effects of duration of glucocorticoid therapy onrelapse rate in antineutrophil cytoplasmic antibody-associated vasculitis: A meta-analysis.Arthritis Care Res (Hoboken) 2010;62:1166-73. 10.1002/acr.20176 20235186
116 Fussner LA, Hummel AM, Schroeder DR, etal. Rituximab in ANCA-AssociatedVasculitis-Immune Tolerance Network Research Group. Factors Determining the ClinicalUtility of Serial Measurements of Antineutrophil Cytoplasmic Antibodies TargetingProteinase 3. Arthritis Rheumatol 2016;68:1700-10. 10.1002/art.39637 26882078
117 Watanabe H, Sada KE, Matsumoto Y, etal. Japan Research Committee of the Ministryof Health, Labour, and Welfare for Intractable Vasculitis, and the Research Committeeof Intractable Renal Disease of the Ministry of Health, Labour, and Welfare of Japan.Association between reappearance of myeloperoxidase-antineutrophil cytoplasmic antibodyand relapse in antineutrophil cytoplasmic antibody-associated vasculitis: subgroup analysisof nationwide prospective cohort studies. Arthritis Rheumatol 2018;70:1626-33.10.1002/art.40538 29790303
118 Lionaki S, Blyth ER, Hogan SL, etal . Classification of antineutrophil cytoplasmicautoantibody vasculitides: the role of antineutrophil cytoplasmic autoantibody specificityfor myeloperoxidase or proteinase 3 in disease recognition and prognosis. Arthritis Rheum2012;64:3452-62. 10.1002/art.34562 23023777
119 Hogan SL, Falk RJ, Chin H, etal . Predictors of relapse and treatment resistance inantineutrophil cytoplasmic antibody-associated small-vessel vasculitis. Ann Intern Med2005;143:621-31. 10.7326/0003-4819-143-9-200511010-00005 16263884
120 Walsh M, Flossmann O, Berden A, etal. European Vasculitis Study Group. Risk factorsfor relapse of antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum2012;64:542-8. 10.1002/art.33361 21953279
121 Solans-Laqué R, Fraile G, Rodriguez-Carballeira M, etal. Spanish Registry of systemicvasculitis (REVAS) from the Autoimmune Diseases Study Group (GEAS) of the SpanishSociety of Internal Medicine (SEMI). Clinical characteristics and outcome of Spanish
patients with ANCA-associated vasculitides: Impact of the vasculitis type, ANCA specificity,and treatment on mortality and morbidity. Medicine (Baltimore) 2017;96:e6083.10.1097/MD.0000000000006083 28225490
122 Lionaki S, Hogan SL, Jennette CE, etal . The clinical course of ANCA small-vesselvasculitis on chronic dialysis. Kidney Int 2009;76:644-51. 10.1038/ki.2009.218 19536079
123 Monach PA, Warner RL, Tomasson G, etal . Serum proteins reflecting inflammation, injuryand repair as biomarkers of disease activity in ANCA-associated vasculitis. Ann RheumDis 2013;72:1342-50. 10.1136/annrheumdis-2012-201981 22975753
124 Ishizaki J, Takemori A, Suemori K, etal. Research Committee of Intractable VasculitisSyndrome and the Research Committee of Intractable Renal Disease of the Ministry ofHealth, Labour and Welfare of Japan. Targeted proteomics reveals promising biomarkersof disease activity and organ involvement in antineutrophil cytoplasmic antibody-associatedvasculitis. Arthritis Res Ther 2017;19:218. 10.1186/s13075-017-1429-3 28962592
125 Pepper RJ, McAdoo SP, Moran SM, etal . A novel glucocorticoid-free maintenance regimenfor anti-neutrophil cytoplasm antibody-associated vasculitis. Rheumatology (Oxford)2019;58:260-8.30239910
126 Berti A, Warner R, Johnson K, etal. RAVE-ITN Research Group. The association of seruminterleukin-6 levels with clinical outcomes in antineutrophil cytoplasmic antibody-associatedvasculitis. J Autoimmun 2019;105:102302. 10.1016/j.jaut.2019.07.001 31320177
127 O’Reilly VP, Wong L, Kennedy C, etal . Urinary soluble CD163 in active renal vasculitis.J Am Soc Nephrol 2016;27:2906-16. 10.1681/ASN.2015050511 26940094
128 Lieberthal JG, Cuthbertson D, Carette S, etal. Vasculitis Clinical Research Consortium.urinary biomarkers in relapsing antineutrophil cytoplasmic antibody-associated vasculitis.J Rheumatol 2013;40:674-83. 10.3899/jrheum.120879 23547217
129 Mahr A, Katsahian S, Varet H, etal. French Vasculitis Study Group (FVSG) and theEuropean Vasculitis Society (EUVAS). Revisiting the classification of clinical phenotypesof anti-neutrophil cytoplasmic antibody-associated vasculitis: a cluster analysis. AnnRheum Dis 2013;72:1003-10. 10.1136/annrheumdis-2012-201750 22962314
130 Pierrot-Deseilligny Despujol C, Pouchot J, Pagnoux C, Coste J, Guillevin L. Predictors atdiagnosis of a first Wegener’s granulomatosis relapse after obtaining complete remission.Rheumatology (Oxford) 2010;49:2181-90. 10.1093/rheumatology/keq244 20675708
131 Rudmik L, Soler ZM. Medical Therapies for Adult Chronic Sinusitis: A Systematic Review.JAMA 2015;314:926-39. 10.1001/jama.2015.7544 26325561
132 Langford CA, Sneller MC, Hallahan CW, etal . Clinical features and therapeuticmanagement of subglottic stenosis in patients with Wegener’s granulomatosis. ArthritisRheum 1996;39:1754-60. 10.1002/art.1780391020 8843868
133 Girard C, Charles P, Terrier B, etal . Tracheobronchial stenoses in granulomatosis withpolyangiitis (Wegener’s): a report on 26 cases. Medicine (Baltimore) 2015;94:e1088.10.1097/MD.0000000000001088 26266344
134 Quinn KA, Gelbard A, Sibley C, etal . Subglottic stenosis and endobronchial disease ingranulomatosis with polyangiitis. Rheumatology (Oxford) 2019;58:2203-11.10.1093/rheumatology/kez217 31199488
135 Hoffman GS, Thomas-Golbanov CK, Chan J, Akst LM, Eliachar I. Treatment of subglotticstenosis, due to Wegener’s granulomatosis, with intralesional corticosteroids and dilation.J Rheumatol 2003;30:1017-21.12734898
136 Seo P, Specks U, Keogh KA. Efficacy of rituximab in limited Wegener’s granulomatosiswith refractory granulomatous manifestations. J Rheumatol 2008;35:2017-23.18688911
137 Holle JU, Voigt C, Both M, etal . Orbital masses in granulomatosis with polyangiitis areassociated with a refractory course and a high burden of local damage. Rheumatology(Oxford) 2013;52:875-82. 10.1093/rheumatology/kes382 23293138
138 Durel CA, Hot A, Trefond L, etal . Orbital mass in ANCA-associated vasculitides: data onclinical, biological, radiological and histological presentation, therapeutic management,and outcome from 59 patients. Rheumatology (Oxford) 2019;58:1565-73.10.1093/rheumatology/kez071 30887055
139 Hozumi H, Oyama Y, Yasui H, etal . Clinical significance of myeloperoxidase-anti-neutrophilcytoplasmic antibody in idiopathic interstitial pneumonias. PLoS One 2018;13:e0199659.10.1371/journal.pone.0199659 29928060
140 Alba MA, Flores-Suárez LF, Henderson AG, etal . Interstital lung disease in ANCAvasculitis. Autoimmun Rev 2017;16:722-9. 10.1016/j.autrev.2017.05.008 28479484
141 Kagiyama N, Takayanagi N, Kanauchi T, Ishiguro T, Yanagisawa T, Sugita Y.Antineutrophil cytoplasmic antibody-positive conversion and microscopic polyangiitisdevelopment in patients with idiopathic pulmonary fibrosis. BMJ Open Respir Res2015;2:e000058. 10.1136/bmjresp-2014-000058 25593704
142 Liu GY, Ventura IB, Achtar-Zadeh N, etal . Prevalence and clinical significance ofantineutrophil cytoplasmic antibodies in north american patients with idiopathic pulmonaryfibrosis. Chest 2019;156:715-23. 10.1016/j.chest.2019.05.014 31181198
143 Hosoda C, Baba T, Hagiwara E, etal . Clinical features of usual interstitial pneumoniawith anti-neutrophil cytoplasmic antibody in comparison with idiopathic pulmonary fibrosis.Respirology 2016;21:920-6. 10.1111/resp.12763 26994375
144 Homma S, Matsushita H, Nakata K. Pulmonary fibrosis in myeloperoxidase antineutrophilcytoplasmic antibody-associated vasculitides. Respirology 2004;9:190-6.10.1111/j.1440-1843.2004.00581.x 15182268
145 Hervier B, Pagnoux C, Agard C, etal. French Vasculitis Study Group. Pulmonary fibrosisassociated with ANCA-positive vasculitides. Retrospective study of 12 cases and reviewof the literature. Ann Rheum Dis 2009;68:404-7. 10.1136/ard.2008.096131 18957485
146 Distler O, Highland KB, Gahlemann M, etal. SENSCIS Trial Investigators. Nintedanib forsystemic sclerosis-associated interstitial lung disease. N Engl J Med 2019;380:2518-28.10.1056/NEJMoa1903076 31112379
147 Limper AH, Knox KS, Sarosi GA, etal. American Thoracic Society Fungal Working Group.An official American Thoracic Society statement: Treatment of fungal infections in adultpulmonary and critical care patients. Am J Respir Crit Care Med 2011;183:96-128.10.1164/rccm.2008-740ST 21193785
148 Stegeman CA, Tervaert JW, de Jong PE, Kallenberg CGDutch Co-Trimoxazole WegenerStudy Group. Trimethoprim-sulfamethoxazole (co-trimoxazole) for the prevention ofrelapses of Wegener’s granulomatosis. N Engl J Med 1996;335:16-20.10.1056/NEJM199607043350103 8637536
149 Buckley L, Guyatt G, Fink HA, etal . 2017 American College of Rheumatology Guidelinefor the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. ArthritisRheumatol 2017;69:1521-37. 10.1002/art.40137 28585373
150 Hruskova Z, Geetha D, Tesar V. Renal transplantation in anti-neutrophil cytoplasmicantibody-associated vasculitis. Nephrol Dial Transplant 2015;30(Suppl 1):i159-63.25324359
151 Shen J, Gill J, Shangguan M, Sampaio MS, Bunnapradist S. Outcomes of renaltransplantation in recipients with Wegener’s granulomatosis. Clin Transplant 2011;25:380-7.10.1111/j.1399-0012.2010.01248.x 20394635
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 10 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

152 Geetha D, Eirin A, True K, etal . Renal transplantation in antineutrophil cytoplasmicantibody-associated vasculitis: a multicenter experience. Transplantation 2011;91:1370-5.10.1097/TP.0b013e31821ab9aa 21508899
153 Wallace ZS, Wallwork R, Zhang Y, etal . Improved survival with renal transplantation forend-stage renal disease due to granulomatosis with polyangiitis: data from the UnitedStates Renal Data System. Ann Rheum Dis 2018;77:1333-8.10.1136/annrheumdis-2018-213452 29760156
154 Meier-Kriesche HU, Kaplan B. Waiting time on dialysis as the strongest modifiable riskfactor for renal transplant outcomes: a paired donor kidney analysis. Transplantation2002;74:1377-81. 10.1097/00007890-200211270-00005 12451234
155 Moran S, Little MA. Renal transplantation in antineutrophil cytoplasmic antibody-associatedvasculitis. Curr Opin Rheumatol 2014;26:37-41.10.1097/BOR.0000000000000006 24257368
156 Little MA, Hassan B, Jacques S, etal . Renal transplantation in systemic vasculitis: whenis it safe?Nephrol Dial Transplant 2009;24:3219-25. 10.1093/ndt/gfp347 19602476
157 Weinkauf J, Puttagunta L, Stewart K, etal . Lung transplantation for severe antineutrophiliccytoplasmic antibody-associated vasculitis. Transplant Proc 2010;42:2707-10.10.1016/j.transproceed.2010.04.053 20832574
158 Koutantji M, Harrold E, Lane SE, Pearce S, Watts RA, Scott DG. Investigation of qualityof life, mood, pain, disability, and disease status in primary systemic vasculitis. ArthritisRheum 2003;49:826-37. 10.1002/art.11471 14673970
159 Basu N, McClean A, Harper L, etal . The characterisation and determinants of quality oflife in ANCA associated vasculitis. Ann Rheum Dis 2014;73:207-11.10.1136/annrheumdis-2012-202750 23355077
160 Carpenter DM, Thorpe CT, Lewis M, Devellis RF, Hogan SL. Health-related quality of lifefor patients with vasculitis and their spouses. Arthritis Rheum 2009;61:259-65.10.1002/art.24235 19177525
161 Tomasson G, Boers M, Walsh M, etal . Assessment of health-related quality of life as anoutcome measure in granulomatosis with polyangiitis (Wegener’s). Arthritis Care Res(Hoboken) 2012;64:273-9. 10.1002/acr.20649 21954229
162 Pugnet G, Pagnoux C, Terrier B, etal. French Vasculitis Study Group. Rituximab versusazathioprine for ANCA-associated vasculitis maintenance therapy: impact on globaldisability and health-related quality of life. Clin Exp Rheumatol 2016;34(Suppl97):S54-9.27049404
163 Robson JC, Dawson J, Doll H, etal . Validation of the ANCA-associated vasculitispatient-reported outcomes (AAV-PRO) questionnaire. Ann Rheum Dis 2018;77:1157-64.10.1136/annrheumdis-2017-212713 29695498
164 Merkel PA, Niles JL, Jimenez R, etal. A randomized clinical trial of CCX168, an orallyadministered c5ar inhibitor for treatment of patients with ANCA-associated vasculitis[abstract 978]. Arthritis Rheumatol 2016;68(suppl 10).
165 ClinicalTrials.gov. Safety and Efficacy Study of IFX-1 in add-on to Standard of Care inGranulomatosis With Polyangiitis (GPA) and Microscopic Polyangiitis (MPA). 2019. https://clinicaltrials.gov/ct2/show/NCT03712345.
166 ClinicalTrials.gov. Abatacept for the Treatment of Relapsing, Non-Severe, GranulomatosisWith Polyangiitis (Wegener's). 2019. https://clinicaltrials.gov/ct2/show/NCT02108860.
167 Langford CA, Cuthbertson D, Ytterberg SR, etal. Vasculitis Clinical Research Consortium.A Randomized, Double-Blind Trial of Abatacept (CTLA-4Ig) for the Treatment of GiantCell Arteritis. Arthritis Rheumatol 2017;69:837-45. 10.1002/art.40044 28133925
168 ClinicalTrials.gov. Low-dose Glucocorticoid Vasculitis Induction Study. 2020. https://clinicaltrials.gov/ct2/show/NCT02198248.
169 ClinicalTrials.gov. The Assessment of Prednisone In Remission Trial (TAPIR) - PatientCentric Approach. 2018. https://clinicaltrials.gov/ct2/show/NCT01933724.
170 Miloslavsky EM, Niles JL, Wallace ZS, etal . Reducing glucocorticoid duration inANCA-associated vasculitis: A pilot trial. Semin Arthritis Rheum 2018;48:288-92.10.1016/j.semarthrit.2018.01.013 29530330
Published by the BMJ Publishing Group Limited. For permission to use (where not alreadygranted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 11 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from
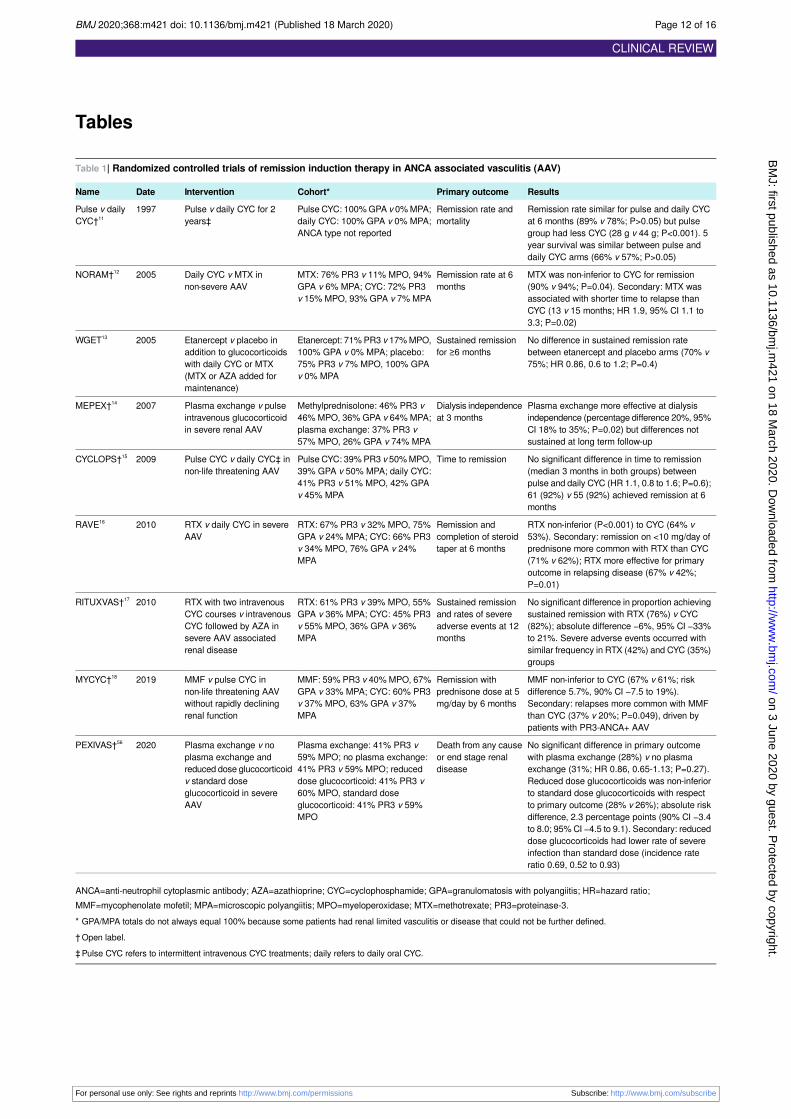
Tables
Table 1| Randomized controlled trials of remission induction therapy in ANCA associated vasculitis (AAV)
ResultsPrimary outcomeCohort*InterventionDateName
Remission rate similar for pulse and daily CYCat 6 months (89% v 78%; P>0.05) but pulsegroup had less CYC (28 g v 44 g; P<0.001). 5year survival was similar between pulse anddaily CYC arms (66% v 57%; P>0.05)
Remission rate andmortality
Pulse CYC: 100% GPA v 0% MPA;daily CYC: 100% GPA v 0% MPA;ANCA type not reported
Pulse v daily CYC for 2years‡
1997Pulse v dailyCYC†11
MTX was non-inferior to CYC for remission(90% v 94%; P=0.04). Secondary: MTX wasassociated with shorter time to relapse thanCYC (13 v 15 months; HR 1.9, 95% CI 1.1 to3.3; P=0.02)
Remission rate at 6months
MTX: 76% PR3 v 11% MPO, 94%GPA v 6% MPA; CYC: 72% PR3v 15% MPO, 93% GPA v 7% MPA
Daily CYC v MTX innon-severe AAV
2005NORAM†12
No difference in sustained remission ratebetween etanercept and placebo arms (70% v75%; HR 0.86, 0.6 to 1.2; P=0.4)
Sustained remissionfor ≥6 months
Etanercept: 71% PR3 v 17% MPO,100% GPA v 0% MPA; placebo:75% PR3 v 7% MPO, 100% GPAv 0% MPA
Etanercept v placebo inaddition to glucocorticoidswith daily CYC or MTX(MTX or AZA added formaintenance)
2005WGET13
Plasma exchange more effective at dialysisindependence (percentage difference 20%, 95%CI 18% to 35%; P=0.02) but differences notsustained at long term follow-up
Dialysis independenceat 3 months
Methylprednisolone: 46% PR3 v46% MPO, 36% GPA v 64% MPA;plasma exchange: 37% PR3 v57% MPO, 26% GPA v 74% MPA
Plasma exchange v pulseintravenous glucocorticoidin severe renal AAV
2007MEPEX†14
No significant difference in time to remission(median 3 months in both groups) betweenpulse and daily CYC (HR 1.1, 0.8 to 1.6; P=0.6);61 (92%) v 55 (92%) achieved remission at 6months
Time to remissionPulse CYC: 39% PR3 v 50% MPO,39% GPA v 50% MPA; daily CYC:41% PR3 v 51% MPO, 42% GPAv 45% MPA
Pulse CYC v daily CYC‡ innon-life threatening AAV
2009CYCLOPS†15
RTX non-inferior (P<0.001) to CYC (64% v53%). Secondary: remission on <10 mg/day ofprednisone more common with RTX than CYC(71% v 62%); RTX more effective for primaryoutcome in relapsing disease (67% v 42%;P=0.01)
Remission andcompletion of steroidtaper at 6 months
RTX: 67% PR3 v 32% MPO, 75%GPA v 24% MPA; CYC: 66% PR3v 34% MPO, 76% GPA v 24%MPA
RTX v daily CYC in severeAAV
2010RAVE16
No significant difference in proportion achievingsustained remission with RTX (76%) v CYC(82%); absolute difference −6%, 95% CI −33%to 21%. Severe adverse events occurred withsimilar frequency in RTX (42%) and CYC (35%)groups
Sustained remissionand rates of severeadverse events at 12months
RTX: 61% PR3 v 39% MPO, 55%GPA v 36% MPA; CYC: 45% PR3v 55% MPO, 36% GPA v 36%MPA
RTX with two intravenousCYC courses v intravenousCYC followed by AZA insevere AAV associatedrenal disease
2010RITUXVAS†17
MMF non-inferior to CYC (67% v 61%; riskdifference 5.7%, 90% CI −7.5 to 19%).Secondary: relapses more common with MMFthan CYC (37% v 20%; P=0.049), driven bypatients with PR3-ANCA+ AAV
Remission withprednisone dose at 5mg/day by 6 months
MMF: 59% PR3 v 40% MPO, 67%GPA v 33% MPA; CYC: 60% PR3v 37% MPO, 63% GPA v 37%MPA
MMF v pulse CYC innon-life threatening AAVwithout rapidly decliningrenal function
2019MYCYC†18
No significant difference in primary outcomewith plasma exchange (28%) v no plasmaexchange (31%; HR 0.86, 0.65-1.13; P=0.27).Reduced dose glucocorticoids was non-inferiorto standard dose glucocorticoids with respectto primary outcome (28% v 26%); absolute risk
Death from any causeor end stage renaldisease
Plasma exchange: 41% PR3 v59% MPO; no plasma exchange:41% PR3 v 59% MPO; reduceddose glucocorticoid: 41% PR3 v60% MPO, standard doseglucocorticoid: 41% PR3 v 59%MPO
Plasma exchange v noplasma exchange andreduced dose glucocorticoidv standard doseglucocorticoid in severeAAV
2020PEXIVAS†56
difference, 2.3 percentage points (90% CI −3.4to 8.0; 95% CI −4.5 to 9.1). Secondary: reduceddose glucocorticoids had lower rate of severeinfection than standard dose (incidence rateratio 0.69, 0.52 to 0.93)
ANCA=anti-neutrophil cytoplasmic antibody; AZA=azathioprine; CYC=cyclophosphamide; GPA=granulomatosis with polyangiitis; HR=hazard ratio;MMF=mycophenolate mofetil; MPA=microscopic polyangiitis; MPO=myeloperoxidase; MTX=methotrexate; PR3=proteinase-3.* GPA/MPA totals do not always equal 100% because some patients had renal limited vasculitis or disease that could not be further defined.† Open label.‡ Pulse CYC refers to intermittent intravenous CYC treatments; daily refers to daily oral CYC.
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 12 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

Table 2| Randomized controlled trials* of maintenance therapy in ANCA associated vasculitis
ResultsPrimary outcomeCohortInterventionDateName
No difference in % relapsing: 16% AZA v14% CYC (P=0.65); difference 1.8%, 95%CI −9.9% to 13.0%
Relapse over ~14months
AZA: 54% PR3 v 39% MPO, 61%GPA v 39% MPA; CYC: 59% PR3v 34% MPO, 62% GPA v 38%MPA
Continued daily CYC v AZAafter induction (3-6 months ofdaily CYC)
2003CYCAZAREM19
No difference in adverse event for MTX vAZA: HR 1.65, 95% CI 0.65 to 4.18;P=0.29. Secondary: % of relapse for MTXv AZA: 36% and 33%; P=0.71)
Treatment endingadverse event
AZA: 65% PR3 v 29% MPO, 76%GPA v 24% MPA; MTX: 56% PR3v 33% MPO, 76% GPA v 24%MPA
AZA v MTX after induction (~7months) with pulse CYC
2008WEGENT20
Relapses were more common in MMFgroup than AZA group (55% v 38%; HR1.80, 1.10 to 2.93; P=0.02)
Relapse-free survivalover ~39 months
MMF: 54% PR3 v 37% MPO, 59%GPA v 41% MPA; AZA: 61% PR3v 29% MPO, 69% GPA v 31%MPA
MMF v AZA after ≤6 monthsof induction therapy with pulseor daily CYC
2010IMPROVE21
Major relapse more common with AZAthan RTX (29% v 5%; HR 6.61, 1.56 to27.96; P=0.002). Secondary: RTX wasassociated with better survival than AZA(100% v 93%; P=0.045)
Major relapse atmonth 28
RTX: 77% PR3 v 16% MPO, 82%GPA v 14% MPA†; AZA: 62% PR3v 31% MPO, 69% GPA v 26%MPA†
RTX v AZA for maintenance innewly diagnosed patients after4-6 months of induction withpulse CYC
2014MAINRITSAN 122
Relapse more common in withdrawalgroup than continuation group (63% v22%; HR 2.8, 1.7 to 4.9; P<0.001).Secondary: major relapse more commonwith withdrawal than continuation (35% v14%; P=0.007)
Relapse rate over~925 days
Withdrawal: 59% PR3 v 41%MPO, 47% GPA v 53% MPA;continuation: 46% PR3 v 47%MPO, 47% GPA v 53% MPA
AZA/prednisone for 48 monthsv 24 months after inductionwith CYC
2017REMAIN23
No statistically significant difference inrelapse rates between individually tailoredand fixed schedule RTX (17% v 10%;P=0.2). Secondary: tailored arm receivedfewer RTX infusions (median 3 (IQR 2-4)v 5 (5-5)) and had numerically fewerinfections (9 v 16)
Relapse at month 28Individually tailored: 49% PR3 v34% MPO, 69% GPA v 31% MPA;fixed schedule: 48% PR3 v 30%MPO, 75% GPA v 25% MPA
Individually tailored v fixedschedule RTX for remissionmaintenance after inductionwith CYC, MTX, or RTX
2018MAINRITSAN224
RTX led to fewer relapses than AZA (13%v 38%; HR 0.30, 0.15 to 0.60; P<0.001)
Relapse at 24months
RTX: 72% PR3 v 28% MPO; AZA:71% PR3 v 27% MPO
RTX v AZA for maintenance inrelapsing patients afterinduction with RTX
2019RITAZAREM25
ANCA=anti-neutrophil cytoplasmic antibody; AZA=azathioprine; CYC=cyclophosphamide; GPA=granulomatosis with polyangiitis; HR=hazard ratio; IQR=interquartilerange; MPA=microscopic polyangiitis; MPO=myeloperoxidase; MTX=methotrexate; MMF=mycophenolate mofetil; PR3=proteinase 3; RTX=rituximab.* All were open label studies.† Total of MPA and GPA does not equal 100% because some patients had renal limited vasculitis that could not be further classified.
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 13 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

Table 3| Adverse effects of commonly used medications to treat ANCA associated vasculitis
CommentsAdverse effectsTreatment
Risk of PCP may be reduced by prophylactic use of trimethoprim/sulfamethoxazole,atovaquone, or dapsone. Baseline bone density examination may be considered.Calcium and vitamin D supplementation as well as prophylaxis for glucocorticoidinduced osteoporosis should be considered for bone health. Proton pump inhibitorsor H
2 blockers can be considered in patients with dyspepsia
Infection; osteoporosis; diabetes mellitus;hypertension; psychosis, depression, anxiety,insomnia; skin thinning, bruising, striae
Glucocorticoids
Risk of PCP may be reduced by prophylactic use of trimethoprim/sulfamethoxazole,atovaquone, or dapsone. Toxicity risk may be attenuated by dose adjustment in renalfailure and older age. Treatment with mesna may reduce risk of hemorrhagic cystitiswhen used intravenously. After treatment, patients should be monitored for bladdercancer with periodic urinalysis. In patients who are hoping to conceive in future,consultation with reproductive endocrinology and/or infertility specialists is needed to
Infection including reactivation of latent infection(eg, hepatitis B, human polyomavirus 2 (JC virus));cytopenias; hypogammaglobulinemia; malignancy,especially bladder cancer; hemorrhagic cystitis;infertility, premature menopause in women;teratogenicity
Cyclophosphamide
review options for egg or semen preservation and/or ovarian suppression for womenof childbearing age
Risk of PCP may be reduced by prophylactic use of trimethoprim/sulfamethoxazole,atovaquone, or dapsone. With severe hypogammaglobulinemia orhypogammaglobulinemia in setting of infection, intravenous immunoglobulin may beindicated. Late onset neutropenia can be idiosyncratic and may occur at any timeduring or after period of B cell depletion
Infection including reactivation of latent infection(eg, hepatitis B, human polyomavirus 2 (JC virus));hypogammaglobulinemia; late onset neutropenia
Rituximab
Folic acid supplementation may reduce risk of certain adverse effects (eg,mucocutaneous). Patients should limit alcohol consumption while taking methotrexate.Methotrexate should be avoided when glomerular filtration rate is reduced below 30mL/min/1.73 m2
Infection; gastrointestinal upset; fatigue; oral ulcers;alopecia; transaminitis; pneumonitis; cytopenias;teratogenicity
Methotrexate
Screening for thiopurine methyltransferase enzyme activity can identify patients withlow enzyme activity who are at high risk of azathioprine toxicity. Considered safe foruse in pregnancy
Infection; gastrointestinal upset, pancreatitis;cytopenias; rash; transaminitis
Azathioprine
Mycophenolic acid delayed release formulation may be associated with fewergastrointestinal adverse effects
Infection; gastrointestinal upset; cytopenias;transaminitis; teratogenicity
Mycophenolate mofetil
Test all patients for hepatitis B virus, hepatitis C virus, and tuberculosis infection beforeadministering these drugs and consult with infectious disease specialist beforetreatment if evidence of infection (active or latent) is present. Vaccinations againstinfluenza virus, pneumococcus, and varicella virus should be considered forimmunosuppressed patients according to local recommendations
Pre-treatmentscreening andprevention
ANCA=anti-neutrophil cytoplasmic antibody; PCP=pneumocystis pneumonia.
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 14 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from

Table 4| Potential biomarkers of and/or risk factors for relapse
CommentsDirection of associationPotential risk factor
ANCA testing:
No association between ANCA titer and risk of relapse observed in RAVE.77
Meta-analysis found increase in ANCA is modestly associated with futurerelapse112 (+LR of 2.8, 95% CI 1.7 to 4.9) and highlighted heterogeneity of data,limited number of MPO-ANCA studies. PR3-ANCA titer increase may predictrelapse after RTX for remission induction.114 116 MPO-ANCA seroconversion fromnegative to positive after remission induction may be associated with increasedrisk of flare (OR 26, 95% CI 8.2 to 101.0)117
±Association between increased titer orseroconversion (negative to positive) and risk ofrelapse. Serial monitoring of PR3-ANCA+ andMPO-ANCA+ needs further study
Rising ANCA titer
Compared with MPO-ANCA+, PR3-ANCA+ patients have approximately twofoldhigher risk of relapse16 109 118-121
PR3-ANCA+ increases risk of relapse PR3-ANCA+ v MPO-ANCA+
Risk of relapse 60% lower in patients with renal disease (HR 0.4, 0.2 to 0.8).Cluster of patients with renal involvement had 40-60% reduction in relapse risk(HR 0.4 (0.3 to 0.5) in minimal extrarenal disease and 0.6 (0.4 to 0.9) in extensiveextrarenal disease. Relapse rate is reduced from 0.20 (0.13 to 0.26) per patientyear to 0.08 (0.04 to 0.11) per patient year after ESRD compared with before122
Renal involvement decreases risk of relapse113 114Renal disease
12% of RTX treated patients and 30% of CYC treated patients in RAVE hadrelapse without detectable B cells.77 B cells detectable in most RTX treatedpatients during flare, especially once off fixed schedule RTX109
Major and minor relapses less likely duringperiods of B cell depletion
B cell detection
MMP-3, TIMP-1, and CXCL-13 discriminate between disease activity (AUC>0.8)and remission as well as healthy states (AUC>0.9).123 124 Increases in calprotectin(S100A8/A9) are associated with risk of relapse, especially in PR3-ANCA+patients after RTX treatment.125 After RTX treatment, increasing sIL-6 may predictrelapse (HR 7.2, 1.5 to 34.9)126
Increased levels associated with disease activitycompared with remission. Only sIL-6 has beenstudied as predictor of flare
Serum biomarkers
Soluble CD163 above cut-off had AUC of 0.9 for distinguishing active renalvasculitis.127 Increase in MCP-1 had AUC of 0.9 for distinguishing active renaldisease from remission128
Increased levels associated with active renaldisease. These have not been studied aspredictors of flare
Urine biomarkers
ANCA=anti-neutrophil cytoplasmic antibody; AUC=area under curve; CYC=cyclophosphamide; ESRD=end stage renal disease; HR=hazard ratio; LR=likelihoodratio; MCP-1=monocyte chemoattractant protein 1; MMP-3=matrix metallopeptidase 3; MPO=myeloperoxidase; OR=odds ratio; PR3=proteinase 3; RTX=rituximab;sIL-6=soluble interleukin 6; TIMP-1=tissue inhibitor matrix metalloproteinase 1.
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 15 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from
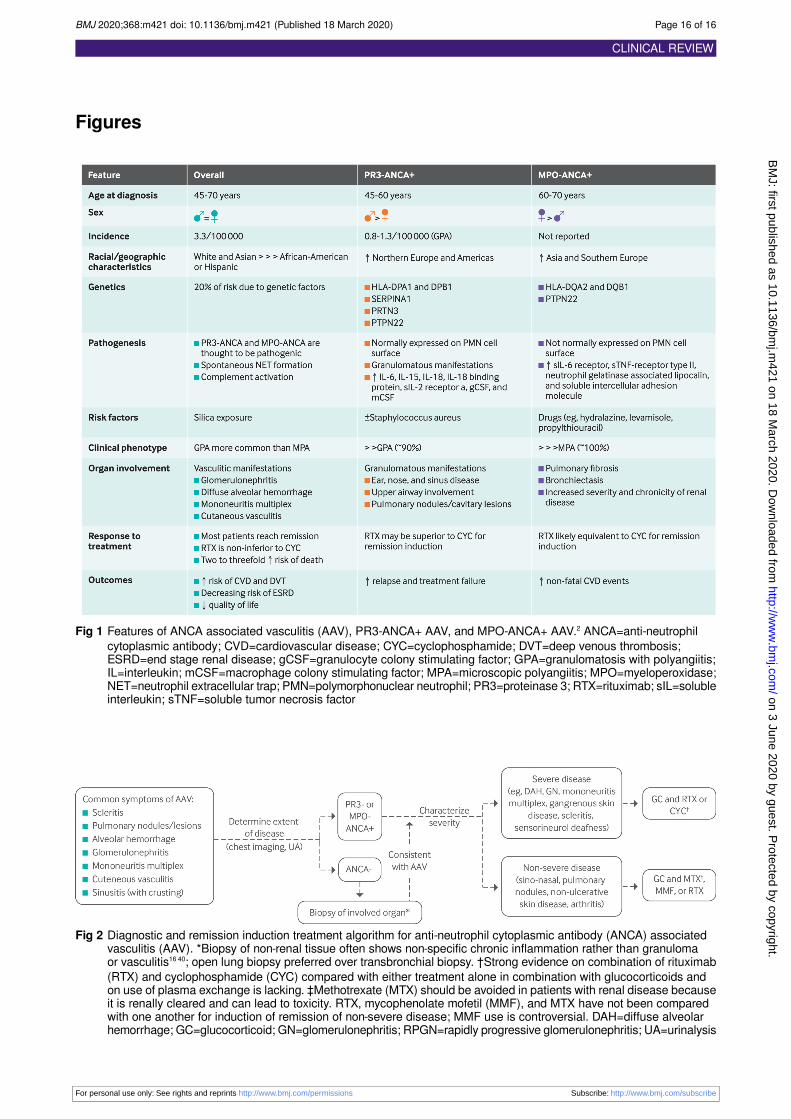
Figures
Fig 1 Features of ANCA associated vasculitis (AAV), PR3-ANCA+ AAV, and MPO-ANCA+ AAV.2 ANCA=anti-neutrophilcytoplasmic antibody; CVD=cardiovascular disease; CYC=cyclophosphamide; DVT=deep venous thrombosis;ESRD=end stage renal disease; gCSF=granulocyte colony stimulating factor; GPA=granulomatosis with polyangiitis;IL=interleukin; mCSF=macrophage colony stimulating factor; MPA=microscopic polyangiitis; MPO=myeloperoxidase;NET=neutrophil extracellular trap; PMN=polymorphonuclear neutrophil; PR3=proteinase 3; RTX=rituximab; sIL=solubleinterleukin; sTNF=soluble tumor necrosis factor
Fig 2 Diagnostic and remission induction treatment algorithm for anti-neutrophil cytoplasmic antibody (ANCA) associatedvasculitis (AAV). *Biopsy of non-renal tissue often shows non-specific chronic inflammation rather than granulomaor vasculitis16 40; open lung biopsy preferred over transbronchial biopsy. †Strong evidence on combination of rituximab(RTX) and cyclophosphamide (CYC) compared with either treatment alone in combination with glucocorticoids andon use of plasma exchange is lacking. ‡Methotrexate (MTX) should be avoided in patients with renal disease becauseit is renally cleared and can lead to toxicity. RTX, mycophenolate mofetil (MMF), and MTX have not been comparedwith one another for induction of remission of non-severe disease; MMF use is controversial. DAH=diffuse alveolarhemorrhage; GC=glucocorticoid; GN=glomerulonephritis; RPGN=rapidly progressive glomerulonephritis; UA=urinalysis
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2020;368:m421 doi: 10.1136/bmj.m421 (Published 18 March 2020) Page 16 of 16
CLINICAL REVIEW
on 3 June 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.m
421 on 18 March 2020. D
ownloaded from