clinical and scientific aspect of inlay fixed partial dentures
TRANSCRIPT

1
UNIVERSITY OF SIENA
SCHOOL OF DENTAL MEDICINE
PHD PROGRAM:
“DENTAL MATERIALS AND CLINICAL APPLICATIONS”
Ph D THESIS OF:
Carlo Monaco
TITLE
“Clinical and scientific aspect of Inlay Fixed Partial Dentures”

2
ACCADEMIC YEAR 2004/2005 December 2005
Siena Italy
Committee:
Promoter Prof. Marco Ferrari
Co-Promoter Prof. R. Scotti
Prof. xxxxxxxxxxxx
Prof. xxxxxxxxxxxx
Prof. xxxxxxxxxxxx
Prof. xxxxxxxxxxxx
TITLE
“Clinical and scientific aspect of Inlay Fixed Partial Dentures” _____________________________________________________________
CANDIDATE
Carlo Monaco
December 2005

3
CONTENTS
Chapter 1: General introduction
1.1 Tooth structure removal associated with various preparation designs
1.2 Metal-free inlay retainer restorations
1.3 Indication and contraindications of inlay-fixed partial denture
Chapter 2: The use of fiber reinforced composites in dentistry
2.1 Fiber-reinforced composite systems
2.2 Properties of the fibers and polymer matrices
2.3 Impregnation of the fibers
2.4 Quantity of fibers
2.5 Direction of the fibers
2.6 Position of fibers
2.7 Water sorption of FRC matrix
Chapter 3: Marginal adaptation of IFPDs
3.1 Marginal adaptation of three partial bridges made with different structure
material.
Chapter 4: Criteria for selecting the materials for IFPDs
4.1 Fracture strength of three partial bridges made with different structure material.
Chapter 5: laboratory process for high volume fiber framework
5.1 Fiber reinforced composite with a high volume framework: a technical
procedure.
Chapter 6: Different structure of the framework
6.1 Clinical Evaluation of Fiber-Reinforced Composite IFPDs.
Chapter 7: adhesive procedures
7.1 Inlay Bridge With a New Microfilled Composite: A Clinical Report

4
Chapter 8: Clinical trial
8.1 Randomized controlled trial of Fiber-Reinforced Composite Inlay Fixed Partial
Dentures: two-year results.
Chapter 9: Alternative materials as regards FRC
9.1 Fatigue test in shear: its effect on bond of a glass-infiltrated alumina ceramic to
human dentin, using different luting procedures.
Chapter 10 Other clinical application of FRC
11.1 Clinical evaluation of teeth restored with quartz fiber-reinforced epoxy resin
posts.
Chapter 11 Conclusions
Summary
5
Chapter 1 General Introduction
When missing tooth structure or teeth are replaced, minimal biologic risk should be
involved to reestablish function and esthetics. To proven reliability and durability of
complete-crown metal ceramics made them the method of choice for posterior single-
tooth restorations and fixed partial denture (FPD). However, this restoration required
considerable reduction of tooth structure. The increased use of the adhesive
technique and preservation of dental tissues have greatly impacted conservative tooth
preparation design. The development of fibre-reinforced composite (FRC)
technology and all-ceramic systems has opened the potential for fabrication of metal-
free restorations with durability and good aesthetics.
This thesis contains a study on several different basic and clinical aspects related to
the use of inlay-fixed partial dentures made with fiber-reinforced composites and all
ceramic systems.
Starting from the assessment of the differences between the amount of tooth structure
removed for conventional preparation and various innovative designs for fixed
prosthodontics, the next step was to analyse the different materials that can be used
when missing tooth must be replaced. Inlay-fixed partial dentures and dental
implants are the true alternatives to the conventional metal-ceramic three-unit
bridges; for these reason an overview regarding the properties advantages and
disadvantages of fiber-reinforced materials is presented. As actually different fiber-
reinforced composites are available on the market, it is important for the clinician to
know the properties of each system to select the more appropriate for the specific
clinical application.
The first objective of this thesis was to evaluate before and after fatigue the marginal
adaptation of inlay fixed partial dentures made with different materials and establish
a connection between the quality of continuous/non-continuous margins and the
mechanical properties of different materials. The second was indeed to conduct a
study to assess the fracture strength and the dye penetration after fatigue of one fiber-
reinforced composite and two all-ceramic systems, and to verify the existence of a
correlation between the mechanical resistance and the microleakage. Another goal of
this thesis was in fact to evaluate if and how different methods of positioning of the

6
fibers for the framework can increase the fracture strength and reduced the flexibility
of the bridges.
The design of the fiber framework is an important prerequisite to obtain a durable
clinical success when using fiber-reinforced composite. Another step of this thesis
was to describe the technical procedure to obtain a framework with a high volume of
fiber; for these reason a clinical study comparing the survival rate of inlay fixed
partial dentures made with different framework design is presented.
Bonding procedures represent the goal for the term of partial restorations. The next
step of this thesis was to describe the luting procedures and the surface treatment for
the inlay bridges and to compare the clinical performances and the post-operative
sensibility of three- and two-step adhesive systems after two-year observation period.
Alternative materials to the metal-ceramic restorations went through rapid
developments in the last few years, in particular alumina- and zirconia based
ceramics. Both these materials represent the future alternatives of the fiber-reinforced
composite but their clinical applications in partial restorations are still limited. The
next steps of this thesis were the analysis of the bond of a glass-infiltrated alumina
ceramic to human dentin, using different luting procedures.
Finally the use of fiber-reinforced composite in the reconstruction of the
endodontically treated teeth is examined with according to the aim of the minimal
intervention philosophy.
1.1 Tooth structure removal associated with various preparation designs
The introduction of more invasive complete crown preparation for metal- and all-
ceramic crowns has been correlated with an increase in pulpal complications since
these restorations require considerable reduction of tooth structure (Creugers et al
1994). For a metal-ceramic shoulder preparation, a facial tooth reduction of about 1.3
to 1.5 mm and an occlusal reduction of 2.0 mm are recommended (McLean JW 1980,
Rosenstiel et al 1995). In 1966, only 0.4% to 2% radiographic periapical pathologies
were found (Ericsson et al 1966), whereas in 1970, 2.9% was reported (Schwartz et
al 1970), and about 10 years later up to 4.0% periapical pathologies were detected
(Kerschbaum et at 1981). These results are explained by the use of air turbines () and
more invasive shoulder or chamfer preparations compared to the feather-edge design

7
used in the 1960s and 1970s (Klötzer 1984). A lower number of endodontic
complications are associated with less invasive preparations. In a literature review,
inlay restorations at 10 years showed a lower rate of loss of pulpal vitality (5.5%)
compared to complete crowns (14.5%) (Kerschbaum et al 1981). The mechanical
reliability and broad range of indications have made complete crowns the preferred
denture retainer. However, wing—shaped retainers with retentive elements such as
grooves made of metal have demonstrated a remarkable long-term success rate if the
clinical protocol is followed carefully (Creugers et al 1992). The gravimetric analysis
(Edelhoff et al 2002) showed that for a metal-ceramic crown retainer preparation,
almost eight times more tooth structure must be removed compared to an adhesive
wing-and groove attachment for a resin-bonded cast-metal fixed partial denture. The
“new” half-crown preparation assigned for all ceramic fixed partial dentures (FPDs)
required a similar amount of tooth structure removal as the onlay and cost
approximately half of the tooth structure of a complete crown design. The percentage
of tooth structure removal associated with the different preparation designs for a
mandibular premolar was 19.3% for mesial/distal occlusal inlay without transverse
ridge or central groove, 30.4% for mesial/distal occlusal inlay with transverse ridge
or central groove and 75.9% for mete-ceramic complete crown. Similar percentages
of tooth structure removal were found for the same kind of preparation in mandibular
molar (19.3%, 25.5%, 73.1%).
The inclusion of enamel promotes a superior bond over dentin, lower post-
cementation sensitivity, improved support of the materials used for the restorations,
and reduced endodontic intervention.
The positive influence of tooth structure preservation on the life expectancy of the
pulp was reported in the literature. For cast-metal resin- bonded FPDs, a 0.13% rate
of loss of pulpal vitality up to 5 years was reported, compared to 9.1% for complete
crown abutments in the same period (Paszyna et al 1990).
1.2 Metal-free inlay retainer restorations
For the past 30 yr, some dentists have avoided the use of full coverage retainers for
fixed partial dentures in order to conserve sound tooth substance. Generally, metal-
reinforced systems are the materials of choice for fabricating posterior fixed partial
dentures because of their reliability and durability. Inlay-retained FPDs made of

8
metal alloys are been usually seated using the conventional cementation technique
and cements (Kopp 1970). Before adhesive techniques were introduced to restorative
dentistry, conventionally cemented partial crowns or inlays, made of cast gold, were
used instead of full coverage crowns to retain a pontic (Boitel 1969). A common
problem was the loss of retention of a retainer, with subsequent secondary caries
development (Roberts 1970). As a result, more effective intracoronal retention with
the help of boxes, grooves, and pins was demanded (Weinberg 1970). These
solutions, however, mitigated the advantage of minimal invasiveness compared with
complete-crown retainers. In the 1980s, adhesive techniques allowed the luting of
metallic frameworks to dental enamel by using metal retainer wings made of cast
gold or non-precious metal (Rochette 1973, Livaditis 1983). Inadequately retentive
preparation shapes and insufficient stability of the metal framework were perceived
to have been contributing factors. After initially frequent losses of retention, more
defined and retentive preparations, along with improved adhesives, led to acceptable
retention rates, especially in anterior teeth (Rammelsberg et al 1993). The aesthetic
limitations caused by the metallic framework remained a problematic issue. The dark
framework on the oral surfaces of abutment teeth eliminated translucency and gave
the teeth a greyish appearance (Livaditis 1983) Restorations made of metal alloys are
characterized by certain basic disadvantages. These base metal components that form
on the surface of the alloy during the metal-ceramic fusing process may have a
negative effect on the adjacent soft tissue. In addition, the opaque, darkish
appearance created by certain metal denture retainers in the abutment teeth is
considered to be unattractive. Partial preparations like inlays, onlays or partial
crowns are recommended as retainers for short-span FPDs in caries-resistant
dentitions. In addition to facilitating superior periodontal health, partial retainers
enable preservation of healthy tooth structure. The combination of highly translucent
prosthodontic materials and resin composite cements has enhanced the use of the
adhesive technique and launched a new era of restorative treatment options with
promising initial clinical results (Sorensen et al 1999). New in vitro findings and a
better understanding of stress formation in fiber-reinforced composite (FRC)
(Vallittu 1996, Freilich et al 2004) and in all-ceramic restorations led to less invasive
preparations extended to existing systems. There has been limited use and no
published clinical data of all-ceramic posterior FPDs retained either by wings or

9
inlays, mostly because of the low strength, the strength scatter, and the time-
dependent strength decrease of ceramics owing to slow crack growth (Fischer et al
2003). The reduced invasiveness of these resin-bonded inlay-retained FPDs makes
them an appealing alternative to conventional preparations in cases where the
residual dentition exhibits low caries activity. Metal-free materials such as fiber-
reinforced composites or high strength pressed ceramics exhibit outstanding
corrosion resistance. The esthetics properties of these systems must be attributed to
the high translucency of the materials and the fact than the restorations are entirely
fabricated of tooth-coloured materials thereby achieving a high degree of light
transmission. However, restorations made of these materials are not as strong as
those that are metal-supported because of their particular mechanical properties. To
achieve adequately strong dental restorations, therefore, certain modifications are
necessary in the preparations fabrications, and cementation methods. The preparation
geometry on an inlay retainer offers favourable prerequisites for the adhesive
cementations technique. The preparation is usually surrounded by dental enamel, and
the location of the preparation margin allows a rubber dam to be placed to ensure
complete isolation. Adhesive cementation could offer one of the most effective ways
of countering the loss of retention, which is one of the most frequent causes of failure
of conventional inlay-retained fixed partial dentures.
1.3 Indication and contraindications of inlay-fixed partial denture
The indications have to be strictly observed because of the special properties of the
metal-free materials. As a result, careful assessment and planning prior to beginning
the prosthodontic treatment measures are requisite. Furthermore, the following
prerequisites must be met if the successful results are to be achieved with metal free-
inlay-retained FPDs.
1. Good oral hygiene
2. Low susceptibility to caries
3. Parallel alignment of abutment teeth
4. Immobility of the abutment teeth
5. Minimum height of abutment teeth ≥ 5mm (connector thickness)

10
6. Maximum mesiodistal extension of the interdental gap of 9 mm (width of
premolar) if pressed ceramic is used and 12 mm (width of molar) if fiber-
reinforced composite materials are used.
Severe parafunctions, short clinical crowns (<5mm) and extensive defects of the
clinical crown, as well as the loosening of teeth because of factors related to the
periodontium, have been established as contraindications. The cusps of
endodontically pre-treated teeth are included in the preparation to protect them.
Metal-free inlay-retained fixed partial dentures must be adhesively cemented because
of the primary friction compared with metal-supported systems (Edelhoff et al 2001).
Existing therapy-resistant periodontopathologic complains as well as allergies to the
components of dentin adhesives or luting composites, therefore, must be classified as
absolute contraindications. Gingival bleeding could compromise the adhesive bond
between the resin and the prepared tooth. In preparation for adhesive cementation,
therefore, all signs of periodontal inflammation should be eliminated.
In addition to a thorough intraoral examination, radiographs (proximal caries,
periodontum) of the designed abutment teeth and irreversible hydrocolloid
impressions recommended for evaluating these factors. Special attention must be
paid to generalized wear facets, the position of the antagonist contacts, existing
hyperbalances, the length of the clinical crown, the pontic span, and the alignment of
the abutment teeth. In addition, canine guidance must be ensured to protect the inlay-
retained fixed partial denture from torsional stress. If it is not established, its
reconstruction during the restorative procedures should be considered.

11
References
Boitel RH. Pin abutment for crown and bridge work. Dtsch Zahnarztl Z 1969;
24:705–707.
Creugers NH, Kayser AF, van 't Hof MA. A meta-analysis of durability data
on conventional fixed bridges. Community Dent Oral Epidemiol. 1994 Dec;22:448-
52.
Creugers NH, Kayser AF, Van't Hof MA. A seven-and-a-half-year survival
study of resin-bonded bridges. J Dent Res. 1992 Nov;71:1822-5.
Edelhoff D, Sorensen JA. Tooth structure removal associated with various
preparation designs for posterior teeth Int J Periodontics Restorative Dent.
2002;22:241-9.
Edelhoff D, Spiekermann H, Yildirim M. Metal-free inlay-retained fixed
partial dentures. Quintessence Int. 2001 Apr;32(4):269-81.
Ericsson S, Hedegard B, Wennstrom A. Roentgenographic study of vital
abutment teeth. J Prosthet Dent 1966;16:981-987.
Fischer H, Weber M, Marx R. Lifetime prediction of allceramic bridges by
computational methods. J Dent Res 2003;82: 238–242.
Freilich MA, Meiers JC. Fiber-reinforced composite prostheses. Dent Clin
North Am. 2004, 448:545-62.
Kerschbaum T, Voss R. Practical efficacy of crowns and inlays Dtsch
Zahnarztl Z. 1981 Apr;36:243-9.
Klötzer WT. Die traumatische Schadigung der pulpa bei der Uberkronung.
Dtsch Zahnarztl 1984;39:791-794
Kopp EN. Partial veneer retainers. J Prosthet Dent. 1970;23:412-9.
Livaditis GJ. Etched metal resin-bonded restorations: principles in retainer
design. Int J Periodontics Restorative Dent 1983; 3: 34–47.
McLean JW. The cast metal-ceramic crown. In: The science and art of dental
ceramics. Chicago: Quintessence, 1980:202.
Paszyna C, Kerschbaum T, Marinello CP, Pfeiffer P. Clinical long-term
results with bonded bridges Dtsch Zahnarztl Z. 1990 Jul;45:406-9.
Rammelsberg P, Pospiech P, Gernet W. Clinical factors affecting adhesive

12
fixed partial dentures: a 6-year study. J Prosthet Dent 1993; 70: 300–307.
Roberts DH. The failure of retainers in bridge prostheses. An analysis of
2,000 retainers. Br Dent J 1970; 128: 117–124
Rochette AL. Attachment of a splint to enamel of lower anterior teeth. J
Prosthet Dent 1973; 30: 418–423.
Rosenstiel SF, Land MF, Fujimoto J. The contemporary Fixed
Prosthodontics. The metal-ceramic crown preparation, ed 2. St.Louis :Mosby Year
Book, 1995:180-193.
Schwartz NL, Whitsett LD, Berry TG, Stewart JL. Unserviceable crowns and
fixed partial dentures: lifespan and causes for loss of serviceability. Am J Dent
1970;81:1395-1401.
Sorensen JA, Cruz M, Mito WT, Raffeiner O, Meredith HR, Foser HP. A
clinical investigation on three-unit fixed partial dentures fabricated with a lithium
disilicate glass-ceramic. Pract Periodontics Aesthet Dent. 1999 Jan-Feb;11:95-106.
Vallittu PK. A review of fiber-reinforced denture base resins. J Prosthodont
1996;5(4):270—6.
Weinberg LA. Vertical nonparallel pin-inlay fixed partial prosthesis.J
Prosthet Dent. 1970;23:420-33.

13
Chapter 2: The use of fiber reinforced composites in dentistry
Fibre-reinforced materials combine the basically different mechanical properties of
fibres and a matrix, in which the fibres are embedded. The fibres demonstrate high
tensile strength, a high tensile modulus, and low shear strength, while the matrix is
characterized by high toughness. In an optimum fibre-reinforced material, the tensile
strength of the fibre is combined with the high toughness of the matrix. Fibre-
reinforced technology is used wherever high stress occurs and low weight is required,
such as in the aeronautical and shipbuilding industries.
Low weight combined with high strength is also required in removable denture
prosthetics, for which PMMA resins have proved to be particularly suitable due to
their resistance to the oral environment. Since complete dentures may fracture, glass-
fibre reinforcements had been discussed by dental interest groups for decades.
(Grotsch, 1965a; Grotsch, 1965b; Mc Creight, 1967). Research mainly focused on
the reinforcement of PMMA denture base materials by means of fibres (Vallittu,
1996). Most scientists found that increased mechanical strength values can be
achieved by means of fibre reinforcement (Vallittu, 1996), with the fracture
resistance enhancing with an increasing fibre content (Vallittu et al. 1994).
2.1 Fiber-reinforced composite systems
Glass fibre-reinforced composites (FRC) were introduced to dentistry in the late
1990s and were advertised as a universal aesthetic material for nearly every dental
indication. Several in vitro studies confirmed good material properties and good
marginal adaptation (Behret et al., 1999; Körber et al., 1996; Göhring et al., 2001,
Goldberg et al., 1992; Behr et al., 1999; Karmaker et al., 1997).
Composite materials are a combination of two or more distinct components forming
a new material with enhanced properties. While many combinations exist, the most
common composites in engineering are composed of strong fibers held by a binder or
matrix. Unlike traditional materials, the properties of composites can be designed
simultaneously with structural aspects. This allows composite designers to
manipulate material properties by changing fiber orientation, fiber content, and
geometry. Additionally, the most common types of matrix materials are polymers

14
(Barbero, 1998). Attempts have been made to reinforce dental polymers with several
types of fibers for various treatment modalities during the past 30 years. Studies have
tested polyethylene fibers (Ladizesky et al., 1992), carbon/ graphite fibers (Kilfoil et
al., 1983; Malquarti et al., 1990; Ruyter et al., 1986), or glass fibers (Goldberg et al.,
1992, Imai et al., 1999; Meiers et al., 2000; Vallittu et al., 1996). There exist
potential applications for fiber-reinforced composites (FRC) in prosthodontics,
periodontics, and orthodontics. Several in vitro studies have been conducted to find
out and understand the factors influencing dental FRC properties (Vallittu et al.,
1994; Viguie et al., 1994; Behr et al., 2000; Vallittu et al., 1998; Vallittu et al., 2000;
Nohrstrom et al., 2000). Important factors influencing the mechanical properties of
FRCs include:
(1) inherent material properties of fibers and polymer matrices,
(2) fiber surface treatment (sizing) and impregnation of fibers with resin,
(3) quantity of fibers (Lassila et al., 2002),
(4) direction of fibers
(5) position of fibers (Vallittu, 2002; Chung et al 1998; Ellakwa et al., 2001)
(6) water sorption of FRC matrix (Lassila et al., 2002).
The main FRCs are represented by systems with different characteristics. Glass
fiber–reinforced systems (Vectris; Ivoclar-Vivadent, Schaan, FL and FibreKor;
Jeneric/Pentron, Wallingford, CT) use continuously oriented fibers preimpregnated
with monomers ready for heat or light curing (“prepregs”). FibreKor prepregs are
unidirectional and adapted manually. Vectris uses a vacuum/pressure device to shape
the framework. The Vectris framework consists of 3 different prepregs that can be
distinguished by the fiber orientation; prepregs with parallel fibers are called
“pontic,” those with a 45-degree alignment are called “single,” and those with a 90-
degree alignment are the “frame” prepregs. A third prepreg system (EverStick,
Turku, Finland) comprises glass fibers preimpregnated with thermoplastic polymers.
Another system (Connect-Band; SDS Belle, Orange, CA) consists of woven
“plasma-etched” polyethylene fibers that must be impregnated by the user before
manual adaptation. Fixation of the fibers in the matrix occurs only by mechanical
means, and perfect impregnation depends on the skill of the user.
15
2.2 Properties of the fibers and polymer matrices
The composition of glass fibers used for dental applications varies. Continuous fibers
for polymer-glass fiber composite are usually made of alkali-free glass (up to 1%
Na2O + K2O) know as E-glass (electrical glass). E-glass is based on the SiO2-Al2-O3-
CaO-MgO system, which has good glass-forming ability. Because of the high
calcium oxide (CaO) content, glass similar to this composition shows poor resistance
to acidic solutions. For this reason, the composition of E-glass is modified by
introducing boron oxide (B2O3) and by decreasing the CaO content (Hlavác, 1983).
The composition for E-glass is presented in table 1. Four other types of glass used in
polymer-fiber composites, S-glass and R-glass (both high-tensile-strength glass),
acid-resistant, and alkaline-resistant glass, are also included. Glass composition
influences the hydrolytic stability or corrosion resistance of the fibers (Ehrenstein et
al., 1990). The amount of B2O3 in glass fibers influences the hydrolytic stability of
the glass fiber surface. B2O3, which lowers surface energy of the molten glass, may
concentrate in the surface layers of the glass fiber during the production process
(Loewenstein, 1966). Because B2O3 is exceedingly reactive with water (Loewenstein,
1966), susceptibility of the glass fiber-polymer interface to hydrolytic degradation in
the presence of B2O3 may be increased if the composites are used in an aqueous
environment.
Unidirectional glass fibers are fiber rovings or yarns consisting of 1.000 to 200.000
single glass fibers. Unidirectional fibers give anisotropic mechanical properties to the
composite, and are suitable for applications in which the direction of highest stress is
known. For example, the fibers can be used to efficiently reinforce polymers in one
direction if there is adequate adhesion between the polymer and the fibers. Possible
uses of this type of material in prostheses would include the pontics of the fixed
partial denture and some removable partial denture designs (Vallittu, 1997).
Bidirectional weaves reinforce structures in two directions and are therefore useful
when the direction of highest stress in the prosthesis is difficult to predict. The
rovings or yarns can be woven in different weaves in which the fibers are oriented in
two directions. The weaves may have various textile structures, such as linen, twill,
or satin weave (Airasmaa et al., 1994). The efficiency of bidirectional fiber

16
reinforcement (fibers at a 45° angle to the force) is ½, in the contrast to unidirectional
fiber reinforcement, which has a reinforcing efficiency of 1. Examples of indications
for bidirectional weaves may be resin crowns and some types of removable partial
dentures, such as overdentures.
Table 1. Composition of different glass fibers (wt%)
Components E-glass Acid-
resistant
glass
Alkaline-
resistant
glass
R-glass S-glass
SiO2 53-55 56-58 62 60 62-65
Al2O3 14-16 12 0.8 25 20-25
CaO 20-24 17-22 5.6 6-9 -
MgO * 2-5 - 6-9 -
B2O3 6-9 - - - 0-1
K2O ≤1 0.4 - 0.1 -
Na2O § 0.1-2 14.8 0.4 0-1
Fe2O3 § 0.2-2 - 0.3 0.2
ZrO2 - 2 - - -
ZnO 0-0.7 2 0 - -
* Total amount of CaO and MgO is 20-24wt%-
§ Total amount of K2O, Na2O, and Fe2O3 < 1wt%.
2.3 Impregnation of the fibers
Many authors have investigated the impregnation of the fibers with the matrix
because poor impregnation creates problems using FRC in dentistry. (Miettinen et
al., 1999; Vallittu et al 1998). Fiber reinforcement is only successful if the loading
force can be transferred from the matrix to the fiber. In the case of voids between the
matrix and the fiber, the load-bearing capacity of the FRC decreases.
Poorly impregnated fibers cause another problem: the increase in water absorption in
FRC Issac, 1999; Miettinen et al., 1999; Jancar et al., 1993) which reduces the
mechanical properties (Söderholm et al., 1990; Söderholm et al., 1984). Voids and
cracks in the laminate allows water to enter. A reliable adhesion between the fibers
and the matrix reduces voids and cracks, which can limit the water absorption. In the
case of glass fiber-reinforced reconstructions, the fibers are covered with a silane-

17
coupling agent. Plueddemann postulates a condensation reaction between the silanol
groups and the glass surface (Plueddemann, 1982). The more siloxane bridges that
exist, the less water will be absorbed resulting in more adhesion between matrix and
fibers. Furthermore, the composition of the glass fibers is particularly important. The
content of alkali and earth-alkali ions and boron oxide has to be considered due to the
increased reactivity of these ions and oxides to water. The mechanism of hydrolytic
degradation is based on the leaching effect of boron oxide from the glass surface
(Vallittu, 1999).
It should be noted that by correct treatment of the glass fibers in the sizing procedure,
the corrosion of the glass fiber surface could be diminished. Thus, glass fibers from
different manufactures and with different surface chemistry might behave differently
in this respect. Furthermore, voids of poorly impregnated fibers are oxygen reserves
(Vallittu, 1999). The oxygen inhibits radical polymerization of the polymer matrix.
This decreases the strength of the FRC and increases the residual monomer content,
which can lead to irritant reactions in the oral mucosa (Hensten-Pettersen, 1998)
To solve all these problems, pre-impregnated (pre-pregs) FRC are used. Pre-
impregnated means that the glass fibers are covered with a silane coupling agent and
then pulled through convoluted paths around supports with a bath of light- and/or
heat-curable monomer systems of polymers (Goldberg, 1999).
Pre-pregs of various sizes can be produced to facilitate clinical application. In
dentistry, generally three systems are used to form fiber-reinforced frameworks for
fixed partial dentures with pre-impregnated glass fibers. One system, like Vectris
(Ivoclar, Schaan, FL) is based on a vacuum/pressure adaptation of the fibers in a
mold (Unterbrink, 1999). The purpose of this procedure is to maximize the fiber
content, decrease the number of voids in the framework, and reduce the technique
sensitivity in order to improve the mechanical properties. Other systems, like
FibreKor (Jeneric/Pentron, Wallingford,CT), prefer a manual adaptation of the pre-
impregnated fibers. (Freilich et al., 1998). The advantage of this procedure is said to
reduce the equipment needed in its manufacturing. The third system (Stick, Stick
Tech Ltd, Turku, Finland) is based on pre-impregnated glass fibers with
thermoplastic polymers, which form a multiphase polymer matrix for FRC with
light-curing monomers.

18
2.4 Quantity of fibers
The strength of a fibre-reinforced material depends on the volume content of the
fibres. The better the densification of the glass-fibre, the higher the mechanical
strength will be (Agarwal et al.,1990; Zanghellini, 1997). Highly densified fibre
elements, however, are too rigid to be formed at will. Therefore, Vectris is pressed
into the desired form and simultaneously densified during the forming procedure in
the VS 1. Subsequently, the matrix is polymerized with light, which secures the
shape of the framework (Fig. 1).
Fig.1. Scanning electron microscopic image of the cross-section of Vectris Pontic fibres before (left) and after (right) densification in the Vectris VS1 device. (Courtesy of Dr. Urs Lendenmann)
2.5 Direction of the fibers
In dental reconstructions, unidirectional and bi- or multidirectional fiber orientation
is used. Unidirectional fibers produce anisotropic mechanical properties in the
composite (Goldberg et al., 1994; Issac, 1998; Jauss, 1997; Vallittu, 1998) and are
preferred when the direction of the highest stress is known. In other cases the rovings
can be woven in such a way that the fibers are oriented in two or three directions,
giving the FRC so-called orthotropic mechanical properties (Vallittu, 1998).
However, the efficiency of woven multidirectional fiber reinforcement is reduced as
described in the Krenchel-formula (Elias, 1992). Numerous articles demonstrate the
relationship between the quantity of fibers in the polymer matrix and the
enhancement of the flexural, transverse and impact strength of fiber-reinforced
reconstructions (Zanghellini, 1992) has been described that with increasing fiber
content, the flexural strength increases linearly. The fiber quantity in the polymer
matrix should be defined in volume not weight percentage.
In the case of carbon-, aramid- or ultra-high-modulus polyethylene fibers (UHMPE),
which have a lower density than glass fibers, the fiber content can lead to misleading
results with regard to the strength of FRC (Vallittu, 1998). Vallittu describes a
formula to transform fiber weight percentage into volume percentage (Vallittu,
1997).

19
2.6 Position of fibers
Previous dental FRC research on position and orientation has focused upon the
effects of the question of fiber reinforcement directionality (i.e. random or
longitudinal orientations) (De Boer, 1984; Galan et al., 1989). It is widely accepted
that directional orientation of the fiber long axis perpendicular to an applied force
will result in strength reinforcement. Forces that are parallel to the long axis of the
fibers, however, produce matrix-dominated failures and consequently yield little
actual reinforcement. Design strategies are on occasion employed to provide multi-
directional reinforcement, to minimize the highly anisotropic behavior of
unidirectional fiber reinforcement. Multidirectional reinforcement, however, is
accompanied by a decrease in strength in any one direction when compared with
unidirectional fiber, as described by Krenchel (Vishu, 1998). In most instances in the
dental literature, fiber reinforcement has been positioned in the center of a composite
specimen (De Boer, 1984). Yet from engineering applications, it is known that the
position and orientation of the reinforcement within a construction influences
mechanical properties (Hull, 1990). For a small sized construction, such as a dental
prosthesis, the quality and characteristics of the FRC are important and demand
careful attention. Fiber reinforcement should be optimal when designing prostheses
and their components. As an example, the components (e.g. connector, pontic,
retainer) of a FRC fixed partial denture (FPD) need to be designed to withstand
masticatory loading (Dyer, 2002). While it is known that tension side fiber
reinforcement strengthens a loaded construction, the effect of varying the cross-
sectional design in a FRC structure is not fully known. Respectively, all factors
relating to design and failure of FRC structures should be investigated and better
understood. In conclusion, position and fiber orientation influenced the load to initial
and final failure, and specimen deflection. Tension side reinforcement was most
effective in increasing the load to initial and final fracture (Dyer et al., 2004).
2.7 Water sorption of FRC matrix
Glass fibers are those most often used for reinforcing polymers in prosthetic dentistry
because of the good aesthetic qualities of glass fiber (Vallittu, 1997) and goog
bonding of glass fibers to polymers via silane coupling agents (Rosen, 1978; Mittal,

20
1992; Vallittu, 1997). The most common type of glass used in fiber production is the
so-called E-glass (electrical glass), and this type of glass is also most often used in
dental fiber composites (Vallittu, 1998).
An aqueous environment, such as in the oral cavity, can induce “corrosion” effects in
the surface of glass fibers resulting from water that diffuses through the polymer
matrix (Ehrenstein GW, 1990). This can lead to a reduction of the mechanical
properties and changes in the composite structure, because the surface of the glass
fibers is affected by the hydrolysis of alkali and earth alkali oxides in the glass and
leaching of ions. The composition of the glass is therefore decisive for the hydrolytic
stability of the glass fibers. The silanization used to bond the fibers to the polymer
matrix also influences the hydrolytic stability of the composite (Pantano et al., 1992).
The polymers used in prosthetic dentistry are often multiphase acrylic resin systems
made from prepolymerized powder beads (predominantly poly[methyl methacrylate]
or PMMA) and a liquid of monomers such as methyl methacrylate (MMA) with
ethyleneglycol dimethacrylate (EGDMA) or 1,4-butanediol dimethacrylate (1,4-
BDMA) as cross-linking agents. (Ruyter et al., 1982 ; Öysaed et al., 1982; Öysaed et
al., 1989; Hill, 1981). Water sorption of such multiphase acrylic resins is
approximatively 2wt% (Al-Mulla et al., 1989; Kalanchandra et al., 1987a;
Kalanchandra et al., 1987b; Miettinen et al., 1997). The cross-linking agent EGDMA
has little effect on the water sorption of denture base polymers (Jagger et al., 1990;
Arima et al., 1996). In a fiber-polymer composite, the water sorption is also affected
by the impregnation of fibers with a resin. If there are regions in which the fibers are
not completely embedded with resin, there will be voids in the structure of cured
composite that increase water sorption (Peltonen, 1992; Vallittu, 1995a; Vallittu,
1995b). In conclusion, water has a plasticizing effect resulting from interaction with
the polymer structure (Ruyter et al., 1986). Many studies on the water sorption of
denture base polymers have been carried out, and it has been concluded that water
sorption decreases the mechanical properties of denture base polymers (Hargreaves,
1979).

21
Fig.1
The picture shows the structure of the fiber-
reinforced composite. On the left side there
is the veneering composite (Targis; Ivoclar-
Vivadent) and on the right side the fiber of
pontic (Vectris; Ivoclar-Vivadent) embedded
of Bis-GMA 24.5% and triethylene glycol
dimethacrylates 6.2% with 65% of glass
fibers.
Fig.2
The weave glass fibers of frame (Vectris;
Ivoclar-Vivadent) are moistly constituted of
Bis-GMA 35.2% and triethylene glycol
dimethacrylates 8.8% with 50% of glass
fibers.
Fig.3
The glass fiber is 10 mm of diameter.
References
Agarwal BD, Broutman LJ (1990). Analysis and performance of fiber
composites. 2 ed. New York: John Wiley & Sons.
Airasmaa I, Johansson CJ, Kokko J. Lujitemuovitekniikka (ed 1). Hameenlinna,
Arvi A Karisto Oy 1984 pp 246-271. [in Finnish].
Barbero EJ. Introduction to composite material design. Ann Arbor, MI: Taylor
and Francis; 1998. pp. 2 and 9.
Behr M, Rosentritt M, Lang R, Handel G. Flexural properties of fiber
reinforced composite using a vacuum/pressure or a manual adaptation
manufacturing process. J Dent 2000; 28(7):509—14.

22
Behr M, Rosentritt M, Leibrock A, Schneider-Feyrer S, Handel G. In-vitro
study of fracture strength and marginal adaptation of fibre-reinforced adhesive fixed
partial inlay dentures. J Dent 1999; 27: 163–168.
Chung KH, Ling T, Wang F. Flexural strength of a provisional resin material
with fibre addition. J Oral Rehabil 1998;25: 214—7.
DeBoer J, Vermilyea SG, Brady RE. The effect of carbon fiber orientation on
the fatigue resistance and bending properties of two denture resins. J Prosthet Dent
1984; 51:119—21.
Dyer SR, Lassila LVJ, Jokinen M, Vallittu PK. Effect of fiber position and
orientation load of fiber-reinforced composite. Dent Mater 2004;20:947–955.
Dyer SR. Current design factors in fiber reinforced composite fixed partial
dentures. In: Vallittu PK, editor. The Second International Symposium on Fibre-
Reinforced Plastics in Dentistry. Symposium Book on the Scientific Workshop on
Dental Fibre-Reinforced Composite on 13 October 2001 in Nijmegen, The
Netherlands; 2002.
Ehrenstein GW, Schmiemann A, Bledzki A, Spaude R. Corrosion phenomena
in glass-fiber reinforced thermosetting resins. In:Cheremisinoff NP (ed). Handbook
of ceramics and composites, vol 1. New York: Marcel Dekker, 1990:231-268.
Ehrenstein GW, Schmiemann A, Bledzki A. Corrosion phenomena in glass-
fiber-reinforced thermosetting resins, in Cheremisinoff NP (ed): Handbook of
ceramic and composites (ed 1). New York, Dekker, 1990 pp 231-268.
Ellakwa AE, Shortall AC, Shehata MK, Marquis PM. The influence of fibre
placement and position on the efficiency of reinforcement of fibre reinforced
composite bridgework. J Oral Rehabil 2001;28(8):785—91.
Galan D, Lynch E. The effect of reinforcing fibres in denture acrylics. J Irish
Dent Assoc 1989;35:109—13.
Göhring TN, Peters OA, Lutz F. Marginal adaptation of bonded slot-inlays
anchoring four-unit fixed partial dentures. J Prosthet Dent 2001; 86: 81–92.
Goldberg AJ, Burstone CJ. The use of continuous fiber reinforcement in
dentistry. Dent Mater 1992;8(3):197—202.
Grotsch G Glasfaserverstärkte Kunststoffe - Allgemeines und zahnärztliche
Probleme um glasfaservertärkte Kunststoffe (GFK). Quintessenz 1965b;16:47-9.

23
Grotsch G. Glasfaserverstärkte Kunststoffe (GFK). Quintessenz 1965a;16:109-
10.
Hargreaves AS. Equilibrium water uptake and denture base resin behaviour. J
Dent 1979; 6:342-349).
Hlavác J. Glass technology, Hlavác J (ed): The technology of glass and
ceramic. An Introduction (ed 1). Amsterdam, Elsevier, 1983 pp 55-220.
Hull D. An introduction to composite materials. Cambridge: University Press;
1990. pp. VII, 24—5, 36—7.
Imai T, Yamagata S, Watari, F, Kobayashi, M, Nagayama K, Toyoizumi H,
Uga M, Nakamura S. Temperature-dependence of the mechanical properties of FRP
orthodontic wire. Dent Mater J 1999;18(2):167—75.
Kilfoil BM, Hesby RA, Pelleu Jr GB. The tensile strength of a composite resin
reinforced with carbon fibers. J Prosthet Dent 1983;50(1):40—3.
Körber KH, Körber S. Mechanische Festigkeit von Faserverbundbrücken
Targis/Vectris. ZWR 1996; 105: 693–702.
Ladizesky NH, Ho CF, Chow TW. Reinforcement of complete denture bases
with continuous high performance polyethylene fibers. J Prosthet Dent
1992;68(6):934—9.
Lassila LV, Nohrstrom T, Vallittu PK. The influence of short-term water
storage on the flexural properties of unidirectional glass fiber-reinforced
composites. Biomaterials 2002;23(10):2221—9.
Loewenstein KL. Glass systems in Holliday L (ed). Composite materials (ed 1).
Amsterdam, Elsevier, 1966 pp 129-287.
Malquarti G, Berruet RG, Bois D. Prosthetic use of carbon fiber-reinforced
epoxy resin for esthetic crowns and fixed partial dentures. J Prosthet Dent
1990;63(3):251—7.
Mc Creight LR. Overview of fiber composites. J Dent Res 1967;46:1192.
Meiers JC, Freilich MA. Conservative anterior tooth replacement using fiber-
reinforced composite. Oper Dent 2000; 25(3):239—43.
Mittal KL. Reminiscing of silane coupling agents. In: Mittal (ed). Silanes and
other coupling agents. Utrecht VSP, 1992:3-12.
Nohrstrom TJ, Vallittu PK, Yli-Urpo A. The effect of placement and quantity

24
of glass fibers on the fracture resistance of interim fixed partial dentures. Int J
Prosthodont 2000;13(1):72—8.
Oysaed H, Ruyter IE.Water sorption and filler characteristics of composites for use in posterior teeth. J Dent Res. 1986;65:1315-8.
Pantano CG, Carman LA, Warner S. Glass fiber surface effects in silane
coupling. In: Mittal KL (Ed). Silanes and Other Coupling Agents. Utrecht VSP,
1992:229-240.
Peltonen P Järvelä P. Methodology for determining the degree of impregnation
from continuous glass fibre prepreg. Polymer Testing 1992;11:215-244).
PK, Lassila VP, Lappalainen R. Transverse strength and fatigue of denture
acrylic—glass fiber composite. Dent Mater 1994;10(2):116—21.
Rosen MR. From treating solution to filler surface and beyond. The life history
of a silane-coupling agent. J Coat Tech 1978;50:70-82.
Ruyter IE, Ekstrand K, Bjork N. Development of carbon/graphite fiber
reinforced poly (methyl methacrylate) suitable for implant-fixed dental bridges.
Dent Mater 1986;2(1):6—9.
Ruyter IE, Oysaed H. Conversion in different depths of ultraviolet and visible
light activated composite materials. Acta Odontol Scand. 1982;40:179-92.
Vallittu PK, Lassila VP, Lappalainen R. Acrylic resin-fiber composite--Part I:
The effect of fiber concentration on fracture resistance. J Prosthet Dent
1994;71:607-612.
Vallittu PK. A review of fiber-reinforced denture base resins. J Prosthodontics
1996;5:270-276.
Vallittu PK. Compositional and weave pattern analyses of glass fibers in dental
polymer fiber composites. J Prosthodont 1998;7(3):170—6.
Vallittu PK. Curing of a silane coupling agent and its effect on the transverse
strength of autopolymerizing polymethylmethacrylate-glass fibre composite. J Oral
Rehabil. 1997 Feb;24(2):124-30.
Vallittu PK. Effect of 180-week water storage on the flexural properties of E-
glass and silica fiber acrylic resin composite. Int J Prosthodont 2000;13(4):334—9.
Vallittu PK. Glass fiber reinforcement in repaired acrylic resin removable
dentures: preliminary results of a clinical study. Quintessence Int. 1997
Jan;28(1):39-44.

25
Vallittu PK. Some aspects of the tensile strength of undirectional glass fibre-
polymethyl methacrylate composite used in dentures. J Oral Rehabil. 1998
Feb;25(2):100-5.
Vallittu PK. Strength and interfacial adhesion of FRC-tooth system. In: Vallittu
PK, editor. The Second International Symposium on Fibre-Reinforced Plastics in
Dentistry. Symposium Book on the Scientific Workshop on Dental Fibre-
Reinforced Composite on 13 October 2001 in Nijmegen, The Netherlands; 2002.
Viguie G, Malquarti G, Vincent B, Bourgeois D. Epoxy/carbon composite
resins in dentistry: mechanical properties related to fiber reinforcements. J Prosthet
Dent 1994; 72(3):245—9.
Vishu S. Handbook of plastic testing technology, 2nd ed. New York: John
Wiley; 1998. pp. 546.
Zanghellini G (1997). Faserverstärkung – die Festigkeit ist eine Funktion des
Volumenanteils der Fasern im FRCWerkstoff. Phillip J 14:390-393.

26
Chapter 3: Marginal adaptation of inlay-fixed partial dentures
Missing single-tooth situations offer several reconstructive treatments modalities.
The traditional way is the reconstruction with a conventional metal-ceramic fixed
partial denture (FPD) (Valderhaug 1991). This technique requires a full-coverage
preparation of the abutment teeth. Consequently, a large quantity of sound tooth
structure is destroyed during the preparation (Edelhoff et al 2002). This is
particularly problematic in healthy and young teeth with large pulpal chambers. In
order to limit this destruction and thanks to the evolution of adhesive dentistry,
(Perdigão et al 1999) and implantology, adhesive fixed partial dentures (AFPD)
(Freilich et al 1998) and dental implants ( Leal et al 2001) represent the current
alternatives. These treatments have several advantages over conventional bridges,
especially in relation to conservation of tooth structure and their reversibility (Lutz et
al 2000). Nevertheless when an implant is contraindicated or refused by the patient,
metal-free restorative options may become attractive. Better bonding properties to
composite cements, more appropriate biomechanical behaviour, and enhanced
aesthetics are expected with the use of composite or ceramic compared to metal
alloys. Inlay-, onlay- and partial crown-anchored FPDs can be bonded to the adjacent
teeth and show acceptable short-term results (Göhring et al 2002, Monaco et al
2003). Fiber reinforced composites (FRC) (Krejci et al 1998), high-strength
reinforced ceramics (Edelhoff et al 2001) and a combination of these two materials
(Rosentritt et al 2003) have been proposed for the fabrication of metal-free inlay
fixed partial dentures (IFPDs). Physical data on reinforced composites suggest that
these materials are best suited for conservative inlay FPDs (Göhring et al 1999).
With a carefully executed bonding technique, good results in marginal adaptation
have been achieved with composite inlays (Lutz et al 1991). The stress-resistant
marginal integrity of composite inlays has been attributed to their dentin-like
elasticity modulus (Krejci et al 1994, Braem et al 1995)
The following study regards the different marginal adaptation measured as
continuous/noncontinuous margin of three materials with different Young modulus.

27
FRC are a new material group with a significantly shorter history of use than more
traditional materials. Glass fibers have been reported to considerably improve the
strength of dental polymers when the fibers were silanated and preimpregnated with
the polymer (Karmaker et al 1997). The combination between resin composite and
fiber seems to better comply with stress and provides a straightforward approach in
the laboratory procedure because casting is not necessary (Vallittu 1999). After
simulation of oral stresses, the fracture resistance and marginal adaptation of IFPDs
made with FRC were better than the ones of all-ceramic restorations (Loose et at
1998).
The interest of clinicians in all ceramic systems is rapidly increasing as stronger and
tougher materials are developed and commercialized along with novel processing
technologies. This development has recently led to the application of zirconia-based
ceramics in dentistry. Moreover, the computer aided design-computer aided
manufacturing (CAD-CAM) is among the most recent advances in dental technology
for direct fabrication of all-ceramic restorations (Wiedhahn et al 2000). The
framework must then be veneered with conventional feldspathic porcelain in order to
achieve the appearance of the natural dentition. Adjustments by grinding may then be
required to improve the fitting of the restoration, and sandblasting of the inner
surface of the restoration is commonly used to enhance the adhesion of the luting
agent to the framework (Kern et al 1998). Yttrium oxide is a stabilizing oxide added
to pure zirconia (Y-TZP) to stabilize it at room temperature and to generate a
multiphase material known as partially stabilized zirconia. The high initial strength
and fracture toughness of Y-TZP results from the physical property of partially
stabilized zirconia. The ability of Y-TZP, so-called ‘‘transformation toughening’’, to
transform from tetragonal crystalline structure to a more voluminous monoclinic
structure that helps to prevent crack propagation, contributes to the strength and
toughness of the ceramic (Ardlin 2002, Williams 1997). In vitro studies of Y-TZP
specimens demonstrated a flexural strength of 900 to 1200 MPa. Y-TZP-based
materials have demonstrated a fracture toughness of 9-10 MPa/ m½, which is almost
double the value demonstrated by alumina-based materials, and almost 3 times the
value demonstrated by lithium disilicate–based materials (Christel et al 1989). An in
vitro study evaluating Y-TZP FPDs under static load demonstrated fracture
resistance of more than 2000 N (Tinschert et al 2001).

28
Points in question are the loading forces that can be withstood as well as the quality
of marginal adaptation that might be reached with FRC and high strength ceramic
systems when used for IFPD restorations. The most relevant mechanical properties to
reduce the clinical failures during loading are flexural strength and fracture toughness
but little information is available on IFPDs. Since mechanical failure is mainly
caused by excessive stresses or deformation that can have a destructive effect on
tooth-restoration interface, a full understanding of stress fields developed in the
dental bridge becomes particularly important. On one hand, some studies with finite
element analysis (Magne et al 2002, Tanimoto et al 2004) suggest that inlay FPDs
made with FRC may be a viable alternative to traditional more invasive FPDs.
Resiliency of the composite may prevent the development of harmful stresses at the
adhesive interface, and reinforcement of the fibers may protect the pontic from
excessive strains, resulting in the restoration’s ability to withstand high functional
loads.
On the other hand, zirconia-ceramic IFPDs exhibited the highest resistance to
fracture when compared to metal-ceramic and glass-ceramic and the failures of the
all-ceramic bridges were always cohesive; located at the connector area that represent
the weakest parts of the bridge (Kılıçarslan et al 2004).
These studies provided insight into a number of biomechanical issues, yet they did
not reveal the marginal adaptation at the tooth/restoration interface during occlusion
and clenching. Although there was positive mechanical behaviour of the new tested
materials, further investigations should be performed on the marginal quality of these
materials.
The aim of this in vitro study was to evaluate the marginal adaptation using
quantitative scanning electron microscope analysis of inlay FPDs made with fiber-
reinforced composite and different ceramic high strength materials after simultaneous
thermal cycling and mechanical loading under the simulation of dentinal fluid that
simulated approximately five years of oral service. The null hypothesis was that there
is no difference in marginal adaptation of the IFPDs before and after fatigue using
materials with different flexural strength and Young’s modulus.

29
MATERIALS AND METHODS
Thirty-six human caries-free molars and premolars of nearly identical size with
completed root growth and stored in a 0.1% thymol solution were selected for this
study. The teeth were randomly and equally divided into 3 groups. The apex of each
root was sealed with an adhesive bonding system and resin composite (Optibond FL,
Kerr; Miris, Coltene, Switzerland) without removal of pulpal tissue and fixed with
the composite on aluminum bases.
Afterwards, the teeth and aluminium bases were immersed in an autopolymerizing
resin (Technovit 4071, Heraeus-Kulzer, Friedrichsdorf, Germany) to an apical depth
of two thirds of the root length to create a strong load-resistant support. Each couple
of teeth (one molar and one premolar) were blocked together with the same
autopolymerizing resin at a distance of 10 mm to each other to prevent movement
during the preparation, impression and luting procedures. In this way, the device
simulated an edentulous space resulting from the loss of one molar. A plastic holding
device with 2 holes was used as a support for the inlay bridges. Two rubber dampers
that were slightly taller than the holes were inserted in the holding device. Eccentric
holes were drilled into the rubber dampers to create a larger distance between the
abutments and to increase the tilting of the abutments toward the space when placed
under load. One holding device with the same distance between the rubber dumpers
was created (Fig.1). To simulate the intrapulpal pressure during the cavity
preparations and the luting procedures, a cylindrical cavity was prepared in each
pulpal chamber 1,5 mm below the amelo-cementum junction. A metal tube with a
diameter of 1.4mm was luted into the cavity with the same adhesive and composite
used to fix them on the bases. Through a connecting silicone tube, the pulpar
chamber was evacuated with a vacuum pump (Vacubrand GmbH, & Co, Wertheim,
Germany), filled with a bubble-free mixture of horse serum (PAA Laboratories
GmbH, Linz, Austria) and phosphate-buffered saline solution (PBS;Oxoid Ltd,
Basingstoke, Hampshire, England) with the aid of a 3-way valve, and finally
connected to a serum infusion bottle. This bottle was placed vertically 34cm above
the specimen to simulate the normal hydrostatic pressure of 25mm Hg within the
tooth until the test was terminated.

30
Tooth preparation Different cavity preparations were made on the teeth to simulate a frequent clinical
situation and to create the space accommodation for the different structure
frameworks. The cavities were prepared with the use of rotating diamond bur (80-
25�m grain size, FG 8113NR, 3113NR; Intensiv SA, Viganello Switzerland; Sirius
180 XL red contra-angle handpiece, Micro-Mega, Bresançon, France) with water-
cooling.
Fig.1. The teeth were blocked together
at a distance of 10 mm to prevent any
movement. The device simulated an
edentulous space resulting from the
loss of one molar. The metal tube luted
into the cavity was filled with a bubble-
free mixture of horse serum and
phosphate-buffered saline solution to
simulate the intra pulpal pressure.
Fig.2-a.
Fig.2-b. Fig.2. The onlay preparation in the molar (a) and inlay cavity in the premolar (b) had mesial
margin in enamel (left) and distal margin in dentin (right). The margins were divided in
different portions to analyze the marginal adaptation in a selective way. A-B: occlusal
enamel, B-C, D-E: approximal enamel, C-D: cervical enamel, F-G, H-I: approximal dentin,
G-H: cervical dentin.
The inlay preparation made in the premolar was a MOD cavity with mesial margin in
dentin, 1 mm below the cementum-enamel junction (CEJ), and distal margin in
enamel, 1 mm above the CEJ. The vestibular-palatal width was 3 mm at the cervical
margin that increased to 4 mm at the upper part of the cavity; the cervical preparation
breadth was 2 mm, similar to the occlusal depth. The onlay preparation made in the
molar was a two cusps partial covering with mesial margin in dentin, 1 mm below
the CEJ and distal margin in enamel, 1 mm above the CEJ. The vestibulo-palatal
31
width was like the premolar preparation and the reduction of the cusps was 2.5 mm,
with 2 mm of occlusal depth in the central fossa (Fig.2a-b).
All dentin surfaces were sealed immediately after the tooth preparation with a 3-step
adhesive system (Optibond FL, Kerr; batch n°25881). Phosphoric acid (Ultraetch,
Ultradent) was applied on dentin for 15 seconds and then rinsed for 30”. The primer
was spread on the dentin for 30” with a microbrush without scrubbing and after, the
bonding was applied to the dentin. After a minimal penetration time of 20 seconds,
the resin was air-thinned and polymerized (Optilux 500, Demetron Inc, Danbury,
Conn.) for 60 seconds. Butt joint cavity finishing lines were finished with a diamond
bur (25mm grain size, N° 3113 NR Intensiv SA) by the use of water-cooling under a
stereomicroscope (Leica MZ6). The polymerised bonding was removed with the
same diamond bur only from the cavity enamel finish lines without touching the
sealed dentin. Impressions were made with Imprint II polyvinyl siloxane (3M ESPE)
with a simultaneous mixing technique according the manufacturer’s instructions.
Provisional restorations were made with Fermit N (Ivoclar-Vivadent) and inserted
without interim cement in analogy to the clinical procedure.
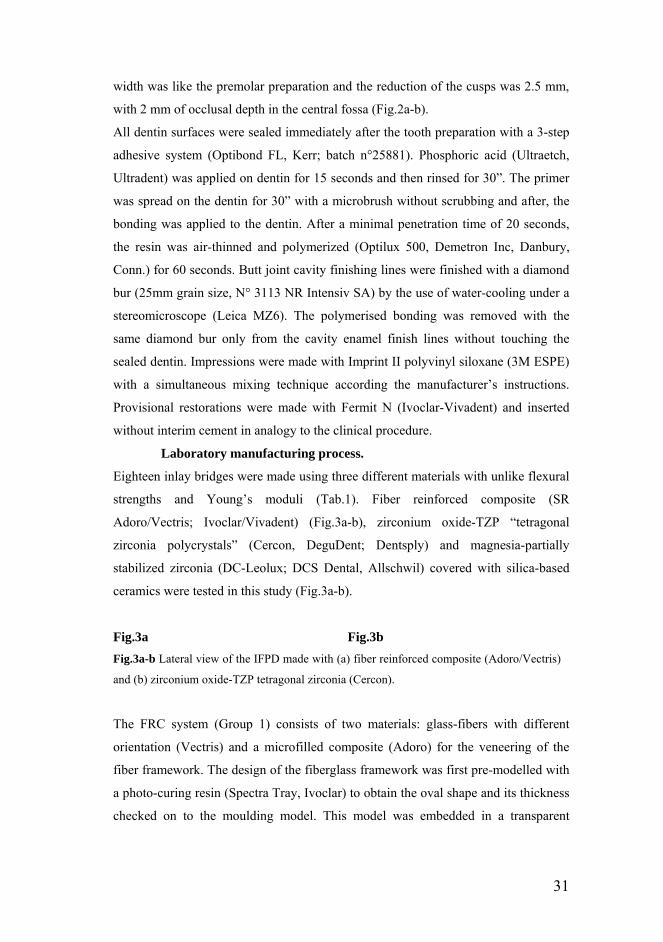
Laboratory manufacturing process.
Eighteen inlay bridges were made using three different materials with unlike flexural
strengths and Young’s moduli (Tab.1). Fiber reinforced composite (SR
Adoro/Vectris; Ivoclar/Vivadent) (Fig.3a-b), zirconium oxide-TZP “tetragonal
zirconia polycrystals” (Cercon, DeguDent; Dentsply) and magnesia-partially
stabilized zirconia (DC-Leolux; DCS Dental, Allschwil) covered with silica-based
ceramics were tested in this study (Fig.3a-b).
Fig.3a
Fig.3b Fig.3a-b Lateral view of the IFPD made with (a) fiber reinforced composite (Adoro/Vectris)
and (b) zirconium oxide-TZP tetragonal zirconia (Cercon).
The FRC system (Group 1) consists of two materials: glass-fibers with different
orientation (Vectris) and a microfilled composite (Adoro) for the veneering of the
fiber framework. The design of the fiberglass framework was first pre-modelled with
a photo-curing resin (Spectra Tray, Ivoclar) to obtain the oval shape and its thickness
checked on to the moulding model. This model was embedded in a transparent

32
silicone impression paste (Transil) to form a mould. Then this resin was removed and
the fibers were applied into the silicone-mould. The pre-impregnated ‘pontic’ fibers
were condensed in a deep-drawing, polymerization process. After a cycle of vacuum-
forming process and then cured by light in VS1 unit (Ivoclar-Vivadent) for 10 min.
according to the manufacturer’s recommendations, the FRC was sandblasted with
Rocatec system (3M ESPE) with small grain size of 80µm at 2,5 bar of pressure for
10 seconds and treated with silane (Wetting agent, Ivoclar-Vivadent). A sheet of
wave fibers ‘frame’ was placed upon the ‘pontic’ structure and the cycle in VS1 was
repeated. The Adoro material was built incrementally using the Quick pre-curing
light unit. The final polymerization / tempering was performed in the Lumamat 100
unit by means of light and heat. The additional tempering step at 104°C was done to
maximize the strength and the surface quality of the restorations.
Cercon (Group 2) is a CAM system that can produce a framework of zirconium
oxide-TZP. The Cercon brain machine automatically mills the framework from an
unsintered zirconium oxide blank (Cercon Base). After that the chalky-soft state is
sintered in the Cercon heat furnace at 1350°C. Finally, the framework is veneered
with low-fusing dental ceramic (Cercon ceram S), which is specially tailored to the
coefficient of thermal expansion of zirconium oxide.
The principle of the Precident system DCS (Group 3) is based on touchless contact-
free measurement and milling in a CAD/CAM process. These two operations are
separated for organizational reasons. The data of the abutments are taken with the
help of a non-contact laser (Preciscan) that at maximum resolution can take 300.000
points/minute. The acquired data are transferred by modem to the milling machine
(Precimill) that can prepare the sub-structure from a sintered magnesia-partially
stabilized zirconia DC-Leolux. Finally the framework is covered with low-fusing
ceramic (Cercon ceram S). The framework of the ceramic bridges (group 2 and 3)
was extended until 1 mm of the margins of the cavity preparation in order to have
etchable silica-based ceramic on the closing margins and optimize the adhesion with
tooth tissue. All the connections of the inlay/onlay with the pontic elements were
3.5X3.5 mm.
Adhesive Procedure

33
The provisional restorations were removed and the inner surfaces of the teeth
previously sealed with bonding were sandblasted with CoJet system (3M ESPE) with
small grain size of 30 µm at 2 bar of pressure for 2 seconds. The inner surfaces of
the FRC and only the zirconium area of the ceramic bridges were treated with CoJet
system (30µm at 2 bar x 10s). The closing ceramic margins were etched with 10%
hydrofluoric acid for 60 seconds and 2 layers of silane-coupling agent (Monobond S,
Ivoclar Vivadent) were applied and heated for 1 minute (ID 500; Coltene
Switzerland) on all the inner surfaces. All enamel and dentin surfaces were luted with
Optibond FL and Tetric Transparent (Ivoclar-Vivadent) by applying the ultrasonic
technique according to the manufacturer’s instructions. The luting cement was light
activated for 60 sec. each from cervical, buccal, lingual and occlusal surfaces. The
margins of the restorations were then finished with 15µm diamond burs
(Composhape, Intensiv) and polished with a composite finishing and polishing kit
(Hawe Neos Dental) in a slow-speed handpiece (Fig.4).
Fig.4 Adhesive inlay
bridge made in fiber
reinforced composite
after the luting
procedures.
Evaluation
The samples were cleaned with rotating nylon brushes (Hawe Neos) and toothpaste
(Signal Anti Caries) before making the impressions for the replicas. Seven partial
impressions for each bridge before and after the thermal and mechanical test were
taken to compare the quality of the marginal adaptation. Six different categories
(approximal enamel, approximal dentin, cervical enamel, cervical dentin, occlusal
and buccal enamel) were recorded to identify the areas with greater stress (Fig. 5).
Gold sputtered (SCD 030, Provac, FL-9496 Balzers, Liechtenstein) epoxy resin
replicas (Epofix, Struers, D-2610 Rodovre, Denmark) of all samples were fabricated
by using polyvinylsiloxane impressions (President Plus Light-body, Colténe AG,
Altstätten, Switzerland). They were subjected to a quantitative evaluation of marginal

34
adaptation at a standard 200x magnification in the SEM (XL20, Philips, NL-5600
Eindhoven, Netherlands) by using a custom made module programmed within an
image processing software (Scion Image, Scion Corp, Frederik, MA 21703, USA).
All specimens were subjected to the quantitative evaluation and examined for
continuous margins (no gap, no interruption of continuity), non-continuous margins
(gap due to adhesive or cohesive failure; fracture of restorative material or fracture of
enamel related to restoration margins), overhangs and underfilled margins. The
percentages of continuous/non-continuous margin were evaluated separately for
tooth-luting composite and luting composite-restoration interfaces. The specimens
were mechanically loaded at the vestibular cusp of the pontic element in a computer-
controlled masticator with 1.200.000 cycles of 49 N each, at a frequency of 1.7 Hz. A
total of 3,000 thermocycles of type 5°C to 55°C to 5°C were performed
simultaneously (Fig.6). The chamber was automatically emptied after 2 minutes for
10 s with air pressure to avoid mixing the cold and warm water (Krejci et al 1990a,
Krejci et al 1993). By having the specimen holders mounted on a rubber rest, a
sliding movement of the bridges was produced during the loading. These conditions
are believed to simulate approximately five years of clinical service (Krejci et al
1990b, Krejci et al 2003). Differences in means were compared with the use of
matched pairs t tests and one-way analysis of variance (ANOVA). The level of
significance was set at P=0.05.

35

36
legend
Kind of replica
P: premolar, M: molar
1. DM
Distal molar
Approximal enamel: a-b; c-d
Cervical enamel: b-c
2. MP
Mesial premolar
Approximal dentin: a-b; c-d Cervical dentin: b-c
3.
VP VM BM
Vestibolar premolar Vestibolar molar Buccal molar
P; Approximal enamel: a-b M; Cervical dentin: c-d Approximal dentin: d-e Buccal enamel: e-f
4. PP
PM
Palatal premolar Palatal molar
P; Approximal enamel: a-b M; Approximal dentin: c-d Cervical dentin: d-e
5. OP OM
Occlusal premolar Occlusal molar
P; occlusal enamel: a-b; c-d M; occlusal enamel: e-f
6. GP
7. GM
Gingival premolar Gingival molar
P; cervical enamel: a-b M; cervical dentin: c-d
Fig. 5. Outline of the non-destructive replica technique.
a
d
cba
b c
d
b
a
e c
d
f
b
a c
e d
a b
c d
e f
a b c d

37
Fig.6. (Left) Loading machine with six watertight cells (A) and the thermocycle device (B).
(Right) The arrow down indicates the rubber dampers that increase the tilting of the
abutments when placed under load. The finger point to the silicone tube filled with a mixture
of horse serum and phosphate-buffered saline solution to simulate the intra pulpal pressure
during all stress cycles. The dot arrow shows the level of the water during the thermocycles.
RESULTS
All restorations were in place after completing the stress test, meaning that the
retention amounted to 100% for all groups. Neither restoration nor abutment
fractures was found after fatigue loading. Only two hairline fractures of the veneering
material that spread in the buccal and vestibular area were found in the gingival part
of the connection between the pontic and the abutment tooth in the FRC group (Fig.
10a-b).
Marginal adaptation was analyzed at the interface of the luting composite and the
abutment inlay/onlay (CI) and at the interface of the tooth and luting composite (TC).
The results of the marginal adaptation expressed in percentage are represented in
table 1. Significant statistical differences (P<0.05) were found for all groups before
and after loading concerning the percentage of continuous margins (CM) as the total
marginal length at the luting cement-restoration and luting cement-tooth interfaces.
No differences were observed after the cycle test between the three groups at the
luting cement-restoration interface (Fig.7). However, significant statistical
differences were found after loading between the FRC and the other two ceramic
systems at the luting cement-tooth interfaces (Fig.8).
The prevailing marginal defect in all groups was pure marginal opening (Fig.11a-b).
Some fractures pointed out after the final observation were traced back as enamel-
dentinal fractures (EF) and filling fracture (FF). No significant difference was
detected in the sub-fracture of the dental tissue (EF) near the margin between the
three groups. However, significant changes (P<0.05) were found in hairline cracks in
the restoration (FF) along the margins between DC-Leolux (4.1%), FRC (0.4) and
Cercon (1.7) after loading. In some cases non continuous “pure” margin identified as
only “open margin” changed in EF or FF. No more than 0.5% of the “overhangs” and

38
“underfilled margins” were found before and after loading, with no significant
differences among the groups. No difference in “continuous margin” was detected
between approximal enamel and approximal dentin. The inner comparison of the
same groups between the onlay preparation (molar) and the inlay cavity (premolar)
didn’t show significant difference (P>0.05). Severe changes in continuous margin
were detected at the tooth-luting composite interface in the dentinal margin after the
test. The values were 20.8% for group 1, 53.8% for group 2 and 32.2% for the last
group Statistical difference was found between Cercon and the other two groups
(P<0.05).
Luting composite-inlay
interface (CI)
Adoro/Vectris Cercon DC Leolux
Before loading 94.6 ± 3.1 92.9 ± 5 96.2 ± 2.1
After loading 88 ± 6.7 85.7 ± 6.1 82.2 ± 9.8
Luting composite-tooth interface (TC)
Before loading 86.7 ± 6.7 93.3 ± 3.4 96.1 ± 2.4
After loading 62.5 ± 16.4 83.2 5.9 75.3 ± 7
Table 1. Percentage of “continuous margin” for the total marginal length before and
after loading (means±SD) at the luting composite-inlay and composite-tooth
interfaces.

39
65
70
75
80
85
90
95
100
Adoro/Vectris before
DC-Leoluxbefore
DC-Leoluxafter
Adoro/Vectris after
Cerconbefore
Cerconafter
Mar
gina
lada
ptat
ion
lutin
g co
mpo
site
-rest
orat
ion
inte
rface
65
70
75
80
85
90
95
100
Adoro/Vectris before
DC-Leoluxbefore
DC-Leoluxafter
Adoro/Vectris after
Cerconbefore
Cerconafter
Mar
gina
lada
ptat
ion
lutin
g co
mpo
site
-rest
orat
ion
inte
rface
Fig. 7. Continuous margin at luting composite-restoration interface (CI) with
quantilies (red line), means/Anova (green lines), means and standard deviation
(blue line).
30
40
50
60
70
80
90
100
1 A BEFORE 1 B AFTER 2 A BEFORE 2 B AFTER 3 A BEFORE 3 B AFTER
Mar
gina
lada
ptat
ion
lutin
g co
mpo
site
-toot
hin
terfa
ce
Adoro/Vectris before
DC-Leoluxbefore
DC-Leoluxafter
Adoro/Vectris after
Cerconbefore
Cerconafter
30
40
50
60
70
80
90
100
1 A BEFORE 1 B AFTER 2 A BEFORE 2 B AFTER 3 A BEFORE 3 B AFTER
Mar
gina
lada
ptat
ion
lutin
g co
mpo
site
-toot
hin
terfa
ce
Adoro/Vectris before
DC-Leoluxbefore
DC-Leoluxafter
Adoro/Vectris after
Cerconbefore
Cerconafter

40
Fig. 8. Continuous margin at tooth-luting composite (TC).
Fig. 9. Continuous margin
of FRC restoration. The left
area (A) represent the
enamel, the middle part the
luting cement and the right
share shows the restoration
(C). The finger points to the
luting cement-tooth
interface whereas the arrow
indicates the luting cement-
restoration interface.
Fig. 10a.
Fig. 10b. Fig. 10a. Hairline fracture of the veneering material in the gingival part of the connection
between the pontic and the abutment in FRC group. The finger indicates the micro crack that
spread in the vestibular area. The black frame in the upper part clearly shows at 200
magnifications (fig.10b) the fissure in the resin composite.
Fig. 11a.
Fig. 11b. Fig. 11. These images show the same portion before (a) and after (b) the stress cycles. The
inner area (A) represent the ceramic restoration (Cercon), the luting cement constitute the
middle part (B), whereas the upper portion (C) show the dental tissue. The arrows and the
fingers indicate the “continuous” (10a) and “non continuous” margins (10b) as result of the 5-
year simulation period.
DISCUSSION

41
Although this study might have some limitations in respect to its clinical relevance,
the absence of detachments or fractures of the inlay bridges suggest that both ceramic
and fiber reinforced composite systems could be utilized in clinical practice.
Nevertheless, some remarks must be made in regard to the quality of the margins and
the hairline fractures found in the FRC group. The most critical areas in dental
bridges and particularly in IFPDs are represented by the connection at the gingival
portion of the pontic between the abutments because this surface constitutes the
tensile side of the beam (Magne et al 1999). When occlusal forces are applied
directly to the long axis of the bridge at the midspan (pontic), compressive stresses
will develop at the occlusal aspect of the connector at the marginal ridge, and tensile
stresses will develop at the gingival surface of the connector (Kelly et al 1995).
These tensile stresses could contribute to the propagation of micro cracks located at
the gingival surface of the connector through the veneering material in an occlusal
direction, and may eventually result in fracture of the composite. The presence of
hairline fractures in the gingival area of the pontic in two bridges of FRC group could
be related to the greater flexibility of the fiber framework compared to the ceramic
materials supported by zirconia framework. These micro cracks can compensate the
smaller stiffness of the fiber but at any rate could determine the beginning of the
delamination or fracture of the layering material.
The clinical fracture resistance of IFPDs is related to the size, shape, and position of
the connectors and to the span of the pontic. The basis for the proper design of the
connectors and the pontic is the law of beams: deflection of a beam increases as the
cube of its length, it is inversely proportional to its width, and it is inversely
proportional to the cube of its height (Raigrodski 2004). Moreover, the flexibility of
the beam is in direct relation to the amount and the type of the fibers that go to make
up the framework. The position of the FRC layer had an effect on the flexural
strength of the test specimen. The highest flexural strength was achieved when the
FRC layer was located at the tension side of the test specimens. The particulate filler
composite is the weakest phase of the test specimen. When it is located on the
tension side, the fracture can easily initiate. The FRC structure benefits most when
the tensile stresses can be transferred to the reinforcing fibers. The veneering

42
particulate filler composite is strong in compression stress and, therefore, the FRC
structure requires less reinforcement fibers on the compression side (Murphy 1998).
Usually, it is preferable to place the FRC laminates symmetrically relating to the
FRC framework, to prevent polymerization shrinkage effect, thermal stresses, and
possible deformation during polymerization (Lassila et a2004).
Nevertheless, it is often very difficult to design the FRC framework to form an
optimal design because of the abutment location and occlusal parameters.
One theoretical assertion is that lower-elastic modulus frameworks would determine
a better stress transfer to the tooth and reduce tensile stresses at the adhesive interface
(Vallittu et al 2000), even though no scientific evidence has shown this to be true.
Vallittu (Vallittu et al 2004) supposed that a lower modulus of elasticity might allow
the FPD to deflect to some extent during function without the formation of stresses
that may cause debonding. Brunton (Brunton et al 1999) preferred restorative
materials such as fiber-reinforced composites rather than ceramic materials because
of the material’s flexibility, repairable properties, and equivalent fracture resistance.
They reported that fiber-reinforced composite material showed similar fracture
resistance when compared to ceramic material under compressive loads for posterior
restorations.
Contrary to these results, in our study the direct comparison between fiber-reinforced
composite and ceramic reinforced systems suggests that different materials could
have an influence on the quality of the margin primarily at the luting composite-tooth
interface. In any case the null hypothesis was rejected. The statistical difference
expressed in percentage between the FRC and the other all-ceramic restorations
could be related to the different flexibility of the frameworks. Our results could
suggest that the smaller stiffness of the fiber-composite complex can negatively
influence the marginal adaptation under load. The fibre framework may absorb the
stress generated during loading but the increased flexibility might have led to the
opening of the margins.
Any significant difference between “approximal enamel” and “approximal dentin”
was found within each group for both interfaces after the fatigue test. All these
margins are in enamel but deferred from the base of the cavity box. The first margin
continues in the “cervical enamel”, the second keeps up in the “cervical dentin”. The
opening of the margin in the cervical dentin doesn’t have an influence on the

43
overhanging enamel. The bonding between the luting composite and the enamel is so
strong that the gap created at the dentin interface stopped at the cementum-enamel
junction. Marginal adaptation at the dentinal margins decreased in a dramatic way
after mechanical loading. The percentage of continuous margin changed from 21 to
54% after the test. A statistical difference was found between the stiffer system
(Cercon) and the other two groups. In any case, the disintegration of the margins in
dentin is so high in all groups that the IFPDs could be contraindicated when one or
both abutments have margins in dentin until the adhesion between the luting
composite and the dentin is improved.
The marginal adaptation at the interface between the luting composite and restoration
decreased after mechanical and thermal loading but no significant difference was
found between all groups. The values ranged between 82,2 and 88%.
Successful ceramic-resin bonding is achieved by the formation of chemical bonds
and micromechanical interlocking at the resin-ceramic interface. With conventional
silica-based ceramics, acid etching and application of a silane coupling agent create a
rough surface of increased wettability for successful ceramic resin bonds. Zirconium-
oxide ceramics are not silica based and the application of acidic agents, such as
hydrofluoric acid, does not create a sufficiently roughened surface for enhanced
micromechanical retention. Advances in adhesive dentistry have resulted in the
recent introduction of modern surface conditioning methods such as silica coating
that require airborne particle abrasion of the surface before bonding in order to
achieve high bond strength. In this technique, the surfaces are air abraded with
aluminum oxide particles modified with silica (Kern et al 1998, Özcan 2002). The
blasting pressure results in the embedding of silica into the ceramic surface,
rendering the silica-modified surface more chemically reactive for the resin through
silane coupling agents. The tribochemical silica coating followed by silanization,
which increased the silica content on the ceramic surface, evidently enhanced the
bond between the ceramic surfaces and the luting cement. Since the silica layer is
well attached to the ceramic surface, this provides a basis for silanes to enhance the
resin bond. Airborn particle abrasion with Al2O3 abrasive particles has proven to be
effective both for composite, aluminum- and zirconium-oxide ceramics (Derand et al
2000). In our study the adhesion between dental tissue and all ceramic bridges was
increased leaving one millimetre or more of silica based ceramic along the margins

44
without zirconia at the interface. This treatment can explain the good results of the
marginal adaptation at both adhesive interfaces of the all-ceramic systems.
Within the limitations of the experimental study, several conclusions can be drawn.
The flexibility of the framework may play an important role in the marginal
adaptation of adhesive inlay/onlay bridges. More rigid materials may transfer the
stress to the margin to smaller degree than flexible materials, which may result in a
more stable bond to the dental tissues under load. When FRC are used for IFPDs
high fiber volume fraction and well-designed framework shape must is mandatory to
increase at maximum the stiffness of the inlay bridges. All ceramic systems
reinforced with zirconia could be used for inlay FPDs in the clinical practice but
simplified CAD/CAM technique is required to allow faster construction of the
zirconia framework. As the marginal adaptation in dentin after load was low in all
groups tested, the IFPDs might be contraindicated when abutments’ margins reach
dentin independent of the bridge material used, until the adhesion between the luting
cement and the dentin will be improved.

45
References
Ardlin B.I. Transformation-toughned zirconia for dental inlays, crowns and
bridges: chemical stability and effect of low-temperature aging on flexural strength
and surface structure. Dental Materials 2002; 18:590-95.
Braem MJ, Lambrechts P, Gladys S, Vanherle G. In vitro fatigue behavior of
restorative composites and glass ionomers. Dent Mater 1995;11:137- 41.
Brunton PA, Cattell P, Burke FJ, Wilson NH. Fracture resistance of teeth
restored with onlays of three contemporary tooth-colored resin-bonded restorative
materials. The Journal of Prosthetic Dentistry 1999; 82:167-71.
Christel P, Meunier A, Heller M, Torre JP, Peille CN. Mechanical properties
and short-term in-vivo evaluation of yttrium-oxide-partially-stabilized zirconia.
Journal of Biomedical Materials Research 1989; 23:45-61.
Derand P, Derand T. Bond strength of luting cements to zirconium oxide
ceramics. The International Journal of Prosthodontics 2000; 13:131-35.
Edelhoff D, Sorensen JA. Tooth structure removal associated with various
preparation designs for posterior teeth. The International Journal of Periodontics &
Restorative Dentistry 2002; 22:241-49.
Edelhoff D, Spiekermann H, Yildirim M. Metal-free inlay-retained fixed partial
dentures. Quintessence International 2001; 32:269-81.
Freilich MA, Duncan JP, Meiers JC. Preimpregnated, fiber-reinforced
prostheses. Part I. Basic rationale and complete-coverage and intracoronal fixed
partial denture designs. Quintessence International 1998; 29:689-96.
Göhring TN, Mörmann WH, Lutz F. Clinical and scanning electron
microscopic evaluation of fiber-reinforced inlay fixed partial dentures: preliminary
results after one year. J Prosthet Dent 1999;82:662-8.
Göhring TN, Schmidlin PR, Lutz F. Two-year clinical and SEM evaluation of
glass-fiber-reinforced inlay fixed partial dentures. American Journal of Dentistry
2002; 15:35-40.
Karmaker AC, Di Benedetto AT, Goldberg AJ. Continuous fiber reinforced
composite materials as alternatives for metal alloys used for dental applicances.
Journal of Biomaterials Applications 1997; 11:318-28.
Kelly JR, Tesk JA, Sorensen JA. Failure of all-ceramic fixed partial dentures in

46
vitro and in vivo: analysis and modeling. Journal of Dental Research 1995; 74:1253-
8.
Kern M, Wegner SM. Bonding to zirconia ceramic: adhesion methods and their
durability. Dental Materials 1998; 14:64-71
Kern M, Wegner SM. Bonding to zirconia ceramic: adhesion methods and their
durability. Dental Materials 1998; 14: 64–71.
Kılıçarslan MA, Kedici PS, Küçükeşmen HC, DDS, Uludag BC. In vitro
fracture resistance of posterior metal-ceramic and all-ceramic inlay-retained resin-
bonded fixed partial dentures. The Journal of Prosthetic Dentistry 2004; 92:365-70.
Krejci I, Boretti R, Giezendanner P, Lutz F. Adhesive crowns and fixed partial
dentures fabricated of ceromer/FRC: clinical and laboratory procedures. Practical
Periodontics and Aesthetic Dentistry 1998; 10:487-98.
Krejci I, Duc O, Dietschi D, de Campos E. Marginal adaptation, retention and
fracture resistance of adhesive composite restorations on devital teeth with and
without posts. Operative Dentistry 2003; 28:127-35.
Krejci I, Kuster M, Lutz F. Influence of dentinal fluid and stress on marginal
adaptation of resin composites. Journal of Dental Research 1993; 72:490-94.
Krejci I, Lutz F, Gautschi L. Wear and marginal adaptation of composite resin
inlays. J Prosthet Dent 1994;72:233-44.
Krejci I, Lutz F. In-vitro test results of the evaluation of dental restoration
systems. Correlation with in-vivo results (in German) Schweizer Monatsschrift fur
Zahnmedizin 1990; 100:1445-49.
Krejci I, Reich T, Lutz F, Albertoni M. An in vitro test procedure for evaluating
dental restoration systems. 1. A computer-controlled mastication simulator (in
German) Schweizer Monatsschrift fur Zahnmedizin 1990; 100:953-60.
Lassila LVJ, Vallittu PK. The effect of fiber position and polymerization
condition on the flexural properties of fiber-reinforced composite. The Journal of
Contemporary Dental Practice 2004; 2:014-026.
Lassila LVJ, Vallittu PK. The effect of fiber position and polymerization
condition on the flexural properties of fiber-reinforced composite. The Journal of
Contemporary Dental Practice 2004; 2:014-026.
Leal FR, Cobb DS, Denehy GE, Margeas RC. A conservative aesthetic solution

47
for a single anterior edentulous space: case report and one-year follow-up. Practical
Procedures & Aesthetic Dentistry 2001; 13:635-41.
Loose M, Rosentritt M, Leibrock A, Behr M, Handel G. In vitro study of
fracture strength and marginal adaptation of fiber-reinforced-composite versus all
ceramic fixed partial dentures. The European Journal of Prosthodontics and
Restorative Dentistry 1998; 6:55-62.
Lutz F, Göhring TN. Fiber-reinforced inlay fixed partial dentures: maximum
preservation of dental hard tissue. Journal of Esthetic Dentistry 2000; 3:164-71.
Lutz F, Krejci I, Barbakow f. Quality and durability of marginal adaptation in
bonded composite restorations. Dent Mater 1991;7:107-13.
Magne P, Perakis N, Belser U, Krejci I. Stress distribution of inlay-anchored
adhesive fixed partial dentures: a finite element analysis of the influence of
restorative materials and abutment preparation design. The Journal of Prosthetic
Dentistry 2002; 87:516-27.
Magne P, Versluis A, Douglas WH. Rationalization of incisor shape:
experimental-numerical analysis. The Journal of Prosthetic Dentistry 1999; 81:345-
55.
Monaco C, Ferrari M, Miceli GP, Scotti R. Clinical evaluation of fiber-
reinforced composite inlay FPDs. The International Journal of Prosthodontics 2003;
16:319-25.
Murphy J. Reinforced plastics handbook. 2nd ed. Oxford: Elsevier Science;
1998.p. 237-67.
Özcan M. The use of chairside silica coating for different dental applications: a
clinical report. The Journal of Prosthetic Dentistry 2002; 87:469–72.
Perdigão J, Lopes M. Dentin bonding-state of art 1999. The Compendium of
Continuing Education in Dentistry 1999; 20:1151-62.
Raigrodski A. Contemporary materials and technologies for all-ceramic fixed
partial dentures: A review of the literature. The Journal of Prosthetic Dentistry 2004;
92:557-562.
Rosentritt M, Behr M, Handel G. Fixed partial dentures: all-ceramics, fibre-
reinforced composites and experimental systems. Journal of Oral Rehabilitation
2003; 30:873-77.

48
Tanimoto Y, Nishiwaki T, Nemoto K. Numerical failure of glass-fiber-
reinforced composites. Journal of Biomedical Materials Research. 2004; 68A:107-
13.
Tinschert J, Natt G, Mautsch W, Augthun M, Spiekermann H. Fracture
resistance of lithium disilicate-, alumina-, and zirconia-based three-unit fixed partial
dentures: a laboratory study. The International Journal of Prosthodontics 2001;
14:231-38.
Valderhaug J. A 15-year clinical evaluation of fixed prosthodontics. Acta
Odontologica Scandinavica 1991;49:35-40.
Vallittu PK, Sevelius C. Resin-bonded, glass fiber-reinforced composite fixed
partial dentures: a clinical study. The Journal of Prosthetic Dentistry 2000; 84:413-
418.
Vallittu PK. Prosthodontic treatment with a glass fiber-reinforced resin-bonded
fixed partial denture: a clinical report. The Journal of Prosthetic Dentistry 1999;
82:132-35
Vallittu PK. Survival rates of resin-bonded, glass fiber–reinforced composite
fixed partial dentures with a mean follow-up of 42 months: A pilot study. The
Journal of Prosthetic Dentistry 2004; 91:241-246.
Wiedhahn K. Cerec 3 as the first step in digitizing the dental office.
International Journal of Computerized Dentistry 2000; 3:67-71.
Williams D. Ceramics transformed: manipulating crystal structures to toughen
bioceramics. Medical Device Technology 1997; 8:6-8.

49
Chapter 4: Criteria for selecting the materials for IFPDs

50
In case of single missing posterior teeth, the adjacent teeth often contain small
occlusal or proximal restorations or initial carious lesions. Conventional porcelain
fused to metal fixed partial dentures (FPDs) provide high fracture strength and have a
long clinical history (Freilich et al 1998, Pauli 1996). But in most cases full or partial
coverage preparations are needed to stabilize the remaining tooth structure and
provide sufficient retention. A significant amount of sound tooth structure must be
removed when fabricating conventional FPDs (Rammelsberg et al 1995).
Fiber-reinforced composites are a new material group with a significantly shorter
history of clinical use than more traditional prosthodontic materials. These materials
differ in the preparation of their laminates (Behr et al 2000, Behr et al 2001).
In posterior areas, however, high mastication forces (approximately 500 to 600 N10)
may restrict the use of metal-free IFPDs. The aim of this in vitro study was to
examine the fracture strength of metal-free 3-unit posterior IFPDs after aging in an
artificial oral environment. One glass fiber–reinforced composites and 2 all-ceramic
systems were tested.
Materials and Methods
The previously eighteen inlay bridges made using three different materials with
unlike flexural strengths and Young’s moduli were loaded until the fracture after the
fatigue machine. FRC (SR Adoro/Vectris; Ivoclar/Vivadent), zirconium oxide-TZP
“tetragonal zirconia polycrystals” (Cercon, DeguDent; Dentsply) and magnesia-
partially stabilized zirconia (DC-Leolux; DCS Dental, Allschwil) covered with silica-
based ceramics were tested in this study. The fracture strength of each IFPD was
determined by mechanically loading them to failure with a universal testing machine
(Instron) after the aforementioned artificial aging. The force was applied on the
center of the pontics using a steel ball (6 mm diameter, 1 mm/minute crosshead
speed). To ensure regular force distribution and minimize the transmission of local
force peaks from the steel ball to the cusps of the pontics, a layer of tin foil (0.5 mm)
was inserted. The failure determination was set at a 10% loss of the maximum
loading force. Radiologic examinations (X-ray, Castellini, Italy) were made to
document the different fracture patterns. Median standard deviation values were
calculated for all groups. The statistical analysis was performed using the Mann-

51
Whitney U test and the Kruskal- Wallis test for nonnormal distributed values (JMP
5.1). The level of significance was set to p =0.05.
Results
All fracture strength results are shown in Figures 1-2. The results for all samples are
given in Table 1. The values for FRC Adoro/Vectris system was 1382N (1172N 25%
percentile, 1549N 75% percentile), for DSC DC-Leolux 1433N (1239N 25%
percentile, 1570N 75% percentile), and for Cercon system was 1695N (1538N 25%
percentile, 1814N 75% percentile). There was no statistical difference between FRC
and DC-Leolux, and DC-Leolux and the Cercon system. In contrast, there was a
statistical difference between the FRC group and the Cercon system. Fig. 3 shows a
representative pattern of fracture for a fiber-reinforced composite IFPD. The failure
of the IFPDs can be attributed to either fractures of the facing material or shearing of
the facing material from the framework fibers. No discernible damage to the
framework fibers was observed. Fig 4 shows the characteristic failure pattern of an
allceramic IFPD. The fractures occurred mainly at the connectors between the pontic
and the abutment in combination with a complete fracture of the restoration.
Table. Results for all samples FRC DC-Leolux Cercon 1 1613 1789 1846 2 1528 1497 1804 3 1467 1440 1744 4 1297 1426 1646 5 1177 1278 1580 6 1160 1123 1413 Total 1373,7 1425,5 1672,2 Standard deviation 189,7 223,9 160,7
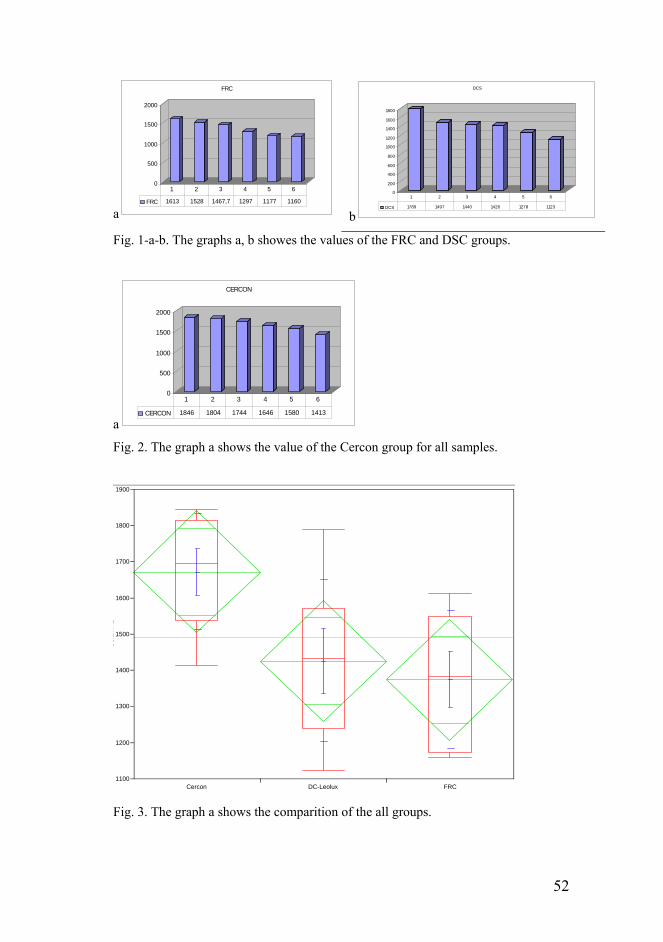
52
a
0
500
1000
1500
2000
FRC
FRC 1613 1528 1467,7 1297 1177 1160
1 2 3 4 5 6
b
0
200
400
600
800
1000
1200
1400
1600
1800
DCS
DCS 1789 1497 1440 1426 1278 1123
1 2 3 4 5 6
Fig. 1-a-b. The graphs a, b showes the values of the FRC and DSC groups.
a
0
500
1000
1500
2000
CERCON
CERCON 1846 1804 1744 1646 1580 1413
1 2 3 4 5 6
Fig. 2. The graph a shows the value of the Cercon group for all samples.
Fig. 3. The graph a shows the comparition of the all groups.
Col
umn
1
1100
1200
1300
1400
1500
1600
1700
1800
1900
Cercon DC-Leolux FRC

53
Discussion
The examination methods used for testing fracture strength follow established
procedures previously described in the literature ( Pauli 1996, Behr et al 2000, Behr
et al 2001). The artificial oral environment allowed for the simulation of parameters
such as temperature changes, mastication force, frequency of occlusal loads, and
resiliency of the human periodontium (Krejci et al 1990). The advantage of this
system is the application of similar conditions on each specimen. This system can be
used for aging dental restorations in vitro to estimate mechanical properties of new
dental materials before any timeconsuming and large-scale clinical investigations are
undertaken (Rosentritt et al 1997, Delong et al 1983). Assuming maximum
mastication forces of about 500 N (Hidaka et al 1999) in posterior chewing areas, the
results found in this study were within the range for the fiber-reinforced systems
(Adoro/Vectris) and for the all-ceramic system (DC-Leolux, Cercon).
The results for the Adoro/Vectris IFPD are increased to those found in a vitro study
conducted by Behr (Behr et al 1999) comparing tub-shaped and box-shaped
preparation techniques with Targis/Vectris. In this study the framework were
composed only of the pontic prepreg fibers and showed fracture strength values of
696 N (531 N/958 N) in the box-shaped preparation and 722 N (665 N/818 N) in the
tub-shaped preparation. The Vectris framework consists of 3 different prepregs that
can be distinguished by the fiber orientation; prepregs with parallel fibers are called
“pontic,” those with a 45-degree alignment are called “single,” and those with a 90-
degree alignment are the “frame” prepregs. Kolbeck (Kolbeck et al 2002)
investigated with the Targis/vectris system a combination of pontic prepreg and
single prepreg fibers and showed nearly exactly the same fracture strength than those
without the single prepreg [723 N (692N/806 N)]. Thus, one might interpret that for
Vectris/Targis IFPDs, it is more important to prepare a tub-shaped cavity without
sharp inner edges rather than to use a large quantity of different prepreg fibers. A
disadvantage of the tub-shaped cavity might be the greater potential for pulp
irritation or exposure. In any cases, the value for the FRC group was lower than
1000N and rather near to the threshold of the 500N. The laboratory technique used in
our study allows the extension in the vestibular and buccal side to support the
layering material like in metal framework and hold it in all loading directions. The
framework in the FRC was made in an anatomical shape in the pontic element with

54
parallel and weave fiberglasses. Vestibular and buccal FRC extensions in the pontic
element can increase the bonding area between the framework and resin composite as
well as hold the veneer material better during occlusal loading. This observation
suggested that modified design of frameworks could increase the bond strength of
resin composite to the fiber framework when chewing (Monaco et al 2003). The
fiber-reinforced materials have higher bending tendencies because of their lower
modulus compared to the more brittle ceramic material, but when the ceramic
material is supported by the zirconia framework the values can widely increase above
the threshold of the 500N. The ceramic fractures occur at the connectors between
pontic and abutment, where embrasure contours are critical. It should be kept in mind
that all of the results reported herein are from an in vitro study. Clinical conditions
may be more critical than those simulated in vitro and potentially may result in lower
forces creating failure. Despite of these potential limitations, however, the results of
this study support further investigation, and the clinical application of these materials
seems possible and promising.
References
Freilich MA, Karmaker AC, Burstone CJ, et al: Development and clinical applications of a light-polymerized fiber reinforcedcomposite. J Prosthet Dent 1998;80:311-318
Pauli C: Fracture strength of ceramometal and all-ceramic posterior fixed partial dentures. ZWR 1996;11:626-632
Rammelsberg P, Behr M, Pospiech P, et al: Adhesively fixed partial dentures: Esthetic and substance preserving alternatives for conventional fixed partial dentures. DZZ 1995;50: 224-227
Behr M, Rosentritt M, Lang R, et al: Flexural properties of fiber reinforced composite using a vacuum/pressure or a manual adaptation manufacturing process. J Dent 2000;28: 509-514.
Behr M, Rosentritt M, Latzel D, et al: Comparison of three types of fiber-reinforced composite molar crowns on their fracture resistance and marginal adaptation. J Dent 2001;29:187-196
Krejci I, Reich T, Lutz F, et al: In vitro test results of the evaluation of dental restoration systems. Correlation with in vivo results. Schweiz Monatsschr Zahnmed 1990;100:1445-1449.
Rosentritt M, Leibrock A, Lang R, et al: Regensburger masticator. Mater Test 1997;39:77-80
Delong R, Douglas WH: Development of an artificial oral environment for the testing of dental restoratives: Bi-axial force and movement control. J Dent Res 1983;62:32-36

55
Hidaka O, Iwasaki M, Saito M, et al: Influence of clenching intensity on bite force balance, occlusal contact area and average bite pressure. J Dent Res 1999;78:1336-1344.
Behr M, Rosentritt M, Leibrock A, et al: In vitro study of fracture strength and marginal adaptation of fiber-reinforced adhesive fixed partial inlay dentures. J Dent 1999;27:163-168.
Monaco C, Ferrari F, DDS, Miceli GP, Scotti R. Clinical Evaluation of Fiber-
Reinforced Composite Inlay Fixed Partial Dentures. Int J Prosthodont 2003;16:319-
325.

56
Chapter 5: laboratory process for high volume fiber framework
Missing single-tooth situations offer several reconstructive treatments modalities.
Adhesive bonded restorations made with fiber-reinforced composite (FRC) have
been proposed for the fabrication of metal-free inlay fixed partial dentures (IFPDs).
Nevertheless, for a small sized construction, such as a dental prosthesis, the design
and characteristics of the fiber framework are important and demand careful
attention. Fiber reinforcement should be optimal when the designing of the
prostheses and their components need to be realized to withstand masticatory
loading. This technical procedure describes the way to realize the cusp-supporting
framework with high volume of fibers and completely support the layering material.

57
The IFPD is indicated in all clinical cases were the replacement of a single tooth is
required but treatment with a dental implant cannot be realized. In this situation, an
inlay bridge offers a more conservative method of tooth replacement compared to a
crown retained conventional bridge because tooth preparations are limited to the
occluso and mesio/distal surfaces of abutment (Fig.1). However these preparations
are more clinical sensitive technique and required a careful laboratory procedure
(Monaco et al 2003). The cavity preparation must give the space to the fiber
framework that must completely support the pontic element. Freilich (Freilich at al
2002) hypothesized the increased rigidity and a broader base of support provided by
the FRC substructure was needed to support the composite veneer. Thus, they added
a substantial amount of FRC bulk to the pontic component of the substructure (low-
volume design), resulting in the creation of the “high-volume” substructure design
and examined their relationship with the clinical performance.
This technical procedure describes the realization of the fiber framework with an
anatomical shape and high volume of fibers that allows the extension of the pontic
element to support the layering material. The final design of the bridge’s framework
is similar to metal framework with extensions in the vestibular and buccal side to
completely hold up the veneer composite and avoid the cohesive fracture of the
composite.
Laboratory Technique
The glass fiber framework (Vectris; Ivoclar Vivadent) is made with pre-impregnated
‘pontic’ and ‘frame’ fibers with a monomer consisting of dimethacrylates and the
final sub-structure has an anatomical shape of the framework and a high volume of
the glass fibers.
The design of the fiberglass framework is first pre-modeled by a photo-curing resin
(Spectra Tray, Ivoclar Vivadent) to obtain the oval shape and its thickness is checked
in the molding model. The dental technician must empty the space for the veneering
material and check with carefulness the space of the connector surface. This area
must be minimum 9mm2 (3x3m), otherwise the flexibility of the framework could
increase and determine the worsening of the marginal adaptation. The photo-curing
resin framework is embedded in a transparent silicone impression paste to form a
mould. Then the resin model is removed and the glass fibers are inserted into the

58
silicone-mould. The pre-impregnated pontic fibers are condensed into the desired
shape by a vacuum- forming process and then cured by light in a VS1 unit (Ivoclar
Vivadent) for 10 min. According to the manufacturer’s recommendations, the pontic
fibers are treated with silane to increase the bonding to the following fiber layer. A
sheet of weave fibers (frame) is placed upon the pontic structure and the cycle in VS1
is repeated. After the moulding of the sheet fibers all excesses are removed with a
carbide bur and the framework is tried on the master model (Fig. 2). The veneering
material is built incrementally using a Quick light-curing unit. Finally, the IFPD is
placed into a Lumamat 100 unit (Ivoclar Vivadent) for the final application of light
and heat (104°C) to complete polymerization and maximize strength and other
physical characteristics (Fig. 3). After the polishing the IDPD is ready for the luting
procedures (Fig. 4).
Discussion
Many FRC researches on position and orientation have focused upon the effects of
the question of fiber reinforcement directionality like random, longitudinal
orientations or weaved. It is widely accepted that directional orientation of the fiber
long axis perpendicular to an applied force will result in strength reinforcement.
Forces that are parallel to the long axis of the fibers, however, produce matrix-
dominated failures and consequently yield little actual reinforcement. Design
strategies are on occasion employed to provide multi-directional reinforcement, to
minimize the highly anisotropic behavior of unidirectional fiber reinforcement ( Dyer
et al 2004). A higher volume fraction of fibers in the resin matrix improves the
mechanical properties. Moreover, the flexibility of the beam is in direct relation to
the amount, position and the type of the fibers that go to make up the framework. The
position of the FRC layer had an effect on the flexural strength of the framework.
The highest flexural strength was achieved when the FRC layer was located at the
tension side of the test specimens. The FRC structure benefits most when the tensile
stresses can be transferred to the reinforcing fibers (Vallittu 1998).
This laboratory technique allows the extension in the vestibular and buccal side to
support the veneering material like in metal or zirconia frameworks and hold it in all
loading directions. Vestibular and buccal FRC extensions in the pontic element can

59
increase the bonding area between the framework and resin composite as well as hold
the veneer material better during occlusal loading.
Conclusion
The design of the FRC framework can play an important role in supporting the
layering material in order to optimize the position and orientation of fibers that
should maximize the stress transferred from matrix to fibers and increase mechanical
properties of IFPDs.
Fig. 1 The presence of old restorations
on the abutments near the edentulous
space is the typical situation for the
IFPDs
Fig. 2 The anatomical fiber framework is
designed to completely support the
veneering composite and increase the
mechanical properties of the IFPD.
Fig. 3 . IFPD made with fiber reinforced
composite.
Fig.4 Follow-up after 2 years.
References
Dyer SR, Lassila LVJ, Jokinen M, Vallittu PK. Effect of fiber position and
orientation on fracture load of fiber-reinforced composite. Dent Mater 2004;20:
947–955.
Freilich MA, Meiers JC, Duncan JP, Eckrote KA, Goldberg AJ. Clinical
evaluation of fiber-reinforced fixed bridges. J Am Dent Assoc 2002;133:1524-
1534.
Monaco C, Ferrari F, DDS, Miceli GP, Scotti R. Clinical Evaluation of Fiber-

60
Reinforced Composite Inlay Fixed Partial Dentures. Int J Prosthodont 2003;16:319-
325.
Vallittu PK. Some aspects of the tensile strength of undirectional glass fibre-
polymethyl methacrylate composite used in dentures. J Oral Rehabil. 1998
Feb;25(2):100-5.

61
Chapter 6: Different structure of the framework
The traditional treatment for a single tooth replacement is a conventional fixed partial
denture (FPD). This technique requires a full-coverage preparation of the abutments.
Consequently, a large quantity of sound tooth is destroyed during the preparation
(Creugers et al 2000). This is particularly problematic in healthy and young teeth
with extensive pulp. In addition, the mean of a FPD is estimated at 8.3-10.3 years
(Creugers et al 2000, Näpänkangas et al 2002). Furthermore, a young patient would
require numerous replacements of this restoration over a lifetime. In order to limit
this destruction and thanks to evolution of adhesive dentistry, (Perdigão et al 1999)
resin bonded fixed partial dentures (RBFPDs) (Freilich et al 1998) and dental
implants (Leal et al 2001) constitute the current alternatives. These treatments have
several advantages over conventional bridges, especially in relation to conservation
of tooth structure and their reversibility (Hussey et al 1996).
Nevertheless, published data on the survival of RBFPDs with metal framework are
still controversial. Some study reports that resin-bonded bridges placed in the
posterior region were less retentive that FPDs placed in the anterior region (Creugers
et al 1997, Creugers et al 1992). De Kanter (De Kanter et al 1998) reported only 46%
and 62% of primary survival rates at 5 years of RBFPDs respectively for
conventional and modified preparation forms. A multi-centers study (Kerschbaum et
al 1996) reported a success rate of 66% that increased to 82% with additional
rebonding.
However, tooth-colored framework and a metal-free prosthetic reconstruction cannot
be built with this technique. Consequently, alternative materials such as high-strength
pressed ceramic (Sorensen et al 1999) and fiber-reinforced composites (FRC) have
achieved (Freilich et al 1998) a certain degree of popularity in restorative dentistry
today. Various types of fibers such as carbon fiber, aramid fiber and ultra-high
modulus polyethylene fiber have been tested (Ekstrand et al 1987, Gutterridge 1992,
Uzun et al 1999, Larson et al 1991, Hess et al 1987) as reinforcing materials, and it
has been shown that the fibers also increase the elastic modulus and flexural strength
of dental polymer. Recently, glass fibers have been used to reinforce denture base
polymers (Krause et al 1989). Glass fibers are favorable for denture base polymer

62
when used in light curing type resin because they have excellent transparency
compared to the other fibers (Vallittu 1999a). The advantages of FRC restorations are
that the laboratory procedure is simple because casting is not necessary, and the
bonding ability between resin and reinforced fiber is superior to that between resin
and casting metal, although surface treatment of fiber is necessary to obtain a strong
bonding (Vallittu 1999b). Reinforcement of dental resins with short or long fibers has
shown positive results and, generally, better mechanical properties when compared to
metal wires in polymers reinforcement (Vallittu 1996c). A glass FRC system made of
prefabricated glass fiber elements along with processing and curing equipment
(Targis-Vectris, Ivoclar-Vivadent) was introduced in 1996 (Krejci et al 1998). A
recent in vitro study reported high fracture strength of 700 N of fiber-reinforced
adhesive IFPDs. With one exception, the break always ran along the interface
between fiber-composite or in the Targis material itself (Behr et al 1999).
The framework in the FRC is supposed to be made in an oval shape in the pontic
element with parallel and weave fiberglasses. This laboratory technique allows the
extension in the vestibular and buccal side to support the layering material like in
metal framework and hold it in a continuous manner. In the present study, the
frameworks was made with different uses and shapes of the fiberglasses to
investigate the clinical behavior of IFPDs.
The purpose of this study was to collect survival data on posterior IFPDs, which were
placed under controlled clinical conditions and to identify the correlation between the
design of fiber frameworks and survival of IFPDs.
Materials and methods
Thirty patients were selected and received an indirect restoration. The selection of the
patients followed two criteria: their refusal to treatment with dental implants and
informed written consent. Selection of male and female subjects was restricted to
those aged 18-60 years and in good general and periodontal health. Patients with the
following factors were excluded from the clinical trial: patients receiving drugs that
modify pain perception, pregnancy or breast feeding, eating disorders, periodontal
surgery, well-known allergy to chemical compounds used in this study and active
periodontal disease.

63
From January 1998 to January 2002 forty-one IFPDs were inserted. Average service
time of Targis-Vectris was 27.2 months. Twenty-four restorations were placed in
mandibular teeth and 17 in maxillary teeth and evaluated using the USPHS criteria.
According to the manufacturer’s instructions the Vectris frameworks in the IFPDs
are made with pre-impregnated ‘pontic’ and ‘frame’ fibers (Ivoclar: Scientific
Document 1996). The FRC framework was made with only pontic fiber in nineteen
restorations (Group 1) and with pontic and frame pre-impregnated fiberglass in
twenty-two restorations (Group 2) according to the manufacturer’s instructions. In
the Group 1 the design of pontic element was made in a cylindrical shape whereas in
the Group 2 was modified in oval shape to hold the layering material in a continuous
manner (Fig 1). The final shape of Group 2 was similar to metal framework with
extensions in the vestibular and buccal side to support completely the veneer
composite.
Clinical Preparation Technique
At baseline all patients were tested for dentin sensitivity. In the rank order data, a
score of 0 was defined as no pain, 1-4 as mild sensitivity, which was provoked by the
dentists’ air blast, and 5-10 as strong sensitivity, which was spontaneously reported
by the patient during drinking or eating. The same measurement was performed again
at each recall. The status of the gingival tissues adjacent to the test sites was observed
at baseline and each recall.
Before cavity preparation a rubber dam was placed and all cavities were prepared
according to modified principles for adhesive inlays retainers to obtain adequately
strong dental restorations. No additional bonding FRC wings were made to obtain
more adhesional surface. The cavities were prepared with 80µm (No. 8113R, No.
8113NR, Intensiv SA) and finished with 25µm (No. 3113R, No. 3117, Intensiv SA)
diamond burs in a medium-speed handpiece with a water spray. All the dentin
surfaces of the cavity preparations were sealed with a three-component enamel-
dentin adhesive system (Syntac, Ivoclar-Vivadent). Undercuts and deep parts of the
cavities were covered with a resin composite (Tetric ceram, Ivoclar-Vivadent)
polymerized for 40 sec. All cavity margins were in enamel and extrasulcus. The
distance to marginal gingival was at least 1 mm. Complete mandibular and maxillary

64
arch impressions were taken with a polyvinyl siloxane (Imprint II, 3M ESPE). A
light-cured resin (Fermit-N, Ivoclar-Vivadent) was used as temporary restoration.
Laboratory Technique
The design of the fiberglass framework was first pre-modeled by a photo-curing resin
(Spectra Tray, Ivoclar) to obtain the oval shape and its thickness checked onto the
molding model. This model was embedded in a transparent silicone impression paste
to form a mould. Then this resin was removed and the fibers were applied into the
silicone-mould (Fig 2). The pre-impregnated ‘pontic’ fibers were condensed in a
deep-drawing, polymerization process. After a cycle of vacuum packing and heat in
VS1 unit (Ivoclar-Vivadent) for 9.30 min. according to the manufacturer’s
recommendations, the FRC was sandblasted with CoJet system (3M ESPE) with
small grain size of 30�m at 2,5 bar of pressure for 10 seconds or roughened with
8o�m diamond bur and treated with silane (Wetting agent, Ivoclar-Vivadent). A
sheet of wave fibers ‘frame’ was placed upon the ‘pontic’ structure and the cycle in
VS1 was repeated. The Targis material was built incrementally using Targis Quick.
Finally, the IFPD was placed into the Targis Power unit (Ivoclar-Vivadent) for the
final application of light and heat to complete polymerization and maximize strength
and other physical characteristics.
Adhesive Procedure
The IFPDs restorations were definitively inserted within 2 weeks after the impression
was made. The operating field was isolated with a rubber dam, provisional
restorations were removed and prepared teeth were cleaned with rubber cup and
pumice slurry (Fig 3). Restoration surfaces were treated with a 25�m diamond bur
(n.3274, Intensiv) in a medium-speed handpiece and a silane-coupling agent
(Monobond S, Ivoclar-Vivadent) was applied on the treated surfaces. All enamel and
dentin surfaces were treated with Syntac (Ivoclar-Vivadent) according to the
manufacturer’s instructions. The dual-cured composite resin cement Variolink II
(Vivadent), was applied to the inlays and the inside of the cavities with a disposable
brush. The luting cement was light activated for 60 sec. each from cervical, buccal,
lingual and occlusal surfaces. Occlusion and articulation were carefully checked after

65
the cementing step. The restorations were then finished with 15 µm diamond burs
(Composhape, Intensiv) and polished with a composite finishing and polishing kit
(Hawe Neos Dental) and Occlubrush (Hawe Neos Dental) in a slow-speed handpiece.
Evaluation
One investigator evaluated all the restorations directly after the final polishing (Fig 4)
and after 6, 12, 24 and 48 months. During the recalls, the patients came back to the
office to answer questions about post-operative sensitivity. Partial or total debonding
of IFPDs and framework or resin composite fractures were considered failures.
Patients with failure were examinated immediately to verify the assumption and the
precise time of the failure. The restorations were evaluated, using the USPHS
modified parameters, to check their stability and longevity in regard to the following
characteristics: color match, marginal discoloration, secondary caries, surface
texture, marginal adaptation, fracture and postoperative sensitivity. The scores were
Alfa (ideal), Bravo (clinically acceptable), Charlie (clinically unacceptable) scores.
Statistical Analysis
Statistical analysis was applied to compare the restorations at baseline and after last
recall, and to check for differences between Group 1 and 2. The Wilcoxon’s
matched-pairs signed ranks test and McNemar test measured the restorations’ success
at the appropriate time intervals and were used to rate all parameters. The Chi-square
test was used to examine for a significant difference in fracture rate between IFPDs
with conventional fiber framework structure and those with modified. The null
hypothesis was rejected at the 5% level. The survival estimation method of Kaplan-
Maier was used with statistical software (Primer 4.02, Stanton A. Glantz, McGraw-
Hill).
Results
No partial/total debonding of the IFPDs or breakage of fiber frameworks were shown
during the observation period. Three partial adhesional/cohesional veneering
composite fractures (Fig 5) occurred in the occlusal-buccal side of the pontic element
in Group 1 after 3, 4 and 8 months. Intraoral repairs were made in all cases of

66
breakage and two IFPDs were completely replaced after a few weeks because the
composite repairs had debonded. After each failure, the fiber framework was visible
at low magnification (Zeiss 3.6x35mm). One cohesive fracture of Targis (Fig 6)
occurred in the abutment in Group 2 after 46 months. The FPD was repaired after
two weeks of intraoral exposion and it is still in place. No statistical differences
regarding fractures were showed between baseline and last recall and between Group
1 and 2 (P>0.05). The percentage of Bravo color match for the IFPDs increased from
7% at baseline to 29% at last recall with statistically significant difference (P<0.048).
The small changes noted during the follow-up period in clinical results for the
abutments were not statistically significant (Table 1). Four patients reported
postoperative hypersensitivity. These patients reported temperature sensitivity and
chewing pain for periods lasting from 1 week to 2 months. These complaints
disappeared completely within 6 months. The Kaplan-Maier survival estimation was
86% for Group 1 and Group 2 (Fig 7).
Table 1 Clinical Results Based on USPHS Criteria
Abutments (n=82)
Baseline
Alfa
Last Recall
Alfa
Baseline
Bravo
Last Recall
Bravo
% Alfa at
Last
Recall
Marginal discoloration 82 79 0 3 96
Secondary caries 82 81 0 1 99
Marginal adaptation 82 80 0 2 98
Postoperative sensibility 78 82 4 0 100
IFPDs (n=41)
Fracture 41 37 0 4 90
Surface texture 41 36 0 5 88
Color match 38 29 3 12 71
Discussion
Inlay fixed partial dentures with fiber framework offer a new option to restore a
missing tooth with a less invasive method and with better esthetic treatment than with

67
metal FPDs. Data on the clinical performance of FRC is needed to estimate the
survival rates as well as to gain knowledge on the appropriate use of fibers in
combination with resin composites. There are few clinical studies on the behavior of
FPDs and most of them are short-term evaluations (Göhring et al 1999, Vallittu et al
2000, Lutz et al 2000). One of the advantages of IFPDs is their intraoral repairing
(Swift et al 1992) but post light curing and heat treatment determine a high degree of
conversion. This treatment improves mechanical properties but it makes the repair of
IFPDs more difficult.
In our study, all adhesional/cohesional veneering composite fractures occurred in the
pontic element in Group 1. Similar failures were reported in an earlier experimental
study with fiber-reinforced composite using a laboratory multistep (Altieri et al
1994). Two of the three intraoral repairs failed after 2 weeks. There are a few
plausible explanations for the failures.
First, the design of the FRC framework can play important role in supporting the
layering material in a continuous manner. Vestibular and buccal FRC extensions in
the pontic element can increase the bonding area between the framework and resin
composite as well as hold the veneer material better during occlusal loading. Failure
was invariably seen in the same position in all bridges with conventional framework
design. This observation suggested that modified design of frameworks could
increase the bond strength of resin composite to the fiber framework when chewing.
Continuous unidirectional fibers gave the highest strength and stiffness only in the
direction of the fiber. Woven fibers are able to reinforce the denture base polymers in
two directions (DeBoer et al 1984). However, definitive recommendations for
prostheses manufacturing currently cannot be made. Further in vitro and clinical
studies must be conducted to confirm this hypothesis.
Second, there might have been inadequate bonding between fiber framework and
composite especially after repair. Rosentritt (Rosentritt et al 1998) demonstrated that
median facing fracture strength of Targis/Vectris bridges was 1450 N after a
simulated clinical service of 5 years but the fracture strengths of the repair IFPDs
were significantly lower compared with the control group after an additional
simulated 2-year interval. However, the median fracture force was still 1000 N
higher than chewing force. Dynamic tests would have different value in comparison
to the static tests. Furthermore, they showed that aluminum oxide pretreatment or

68
abrading with diamond burs and silanization provided in vitro sufficient fracture
strength. Nevertheless, an aqueous environment can induce corrosive effects on the
surface of glass fibers resulting from water absorption through the polymer matrix
(Lassila et al 2002). Other substances, like alcohol, can break the polymer chains
with a softening effect on the composite that can lead to a reduction of the
mechanical strength (Ehrenstein et al 1990). The bonding values between a repair
and an aged framework are about 20% to 70% lower in comparison to the bonding
between a new framework and veneer (Swift et al 1994). Therefore, the design of the
IFPD after repair should help to preserve points of high stress, especially in occlusal
areas.
Third, it is possible that cohesional fractures inside resin composite may be caused
by air entrapment during manufacturing to ensure esthetics. Entrapment of air locally
inhibits polymerization and weakens the structure of materials (Vallittu et al 1997).
Görhing (Görhing et al 1999) described a modified manufacturing technique to
eliminate occlusal multilayering and to reduce the risk of veneering composite
fractures. The matrix chemistry of the repair composite might not influence the
repair strength (Gregory et al 1990), but the composite should provide low viscosity
to achieve a good wetting of the repair point (Rosentritt et al 1997). The moderate
decrease in fracture resistance obtained after veneering repair in vitro of
Targis/Vectris bridges indicates that repeated repair is possible (Rosentritt et al
2001), although it is highly risky to repair an extremely damaged FPD that has lost
more than 50% of the veneer substance.
The percentage of bravo in color match was 29% at last recall and the deterioration
was significant compared to initial status. Some inlay FPDs lost their surface shine
with the color that was slightly too dark/opaque with superficial stains and the
repolishing was only partially successful in reversing the discoloration. Color
changes or resin material can occur through several mechanisms: formation of
degradation products changes in surface structure due to the wear and by extrinsic
staining (Powers et al 1980). Douglas (Douglas 2000) showed that after accelerated
aging the new generation of indirect resins demonstrated color changes at or below a
quantitative level that would be considered acceptable. These changes were in the
magnitude of 0.62 to 3.4�E units. However, Stober (Stober et al 2001) described
changes in color of the same composite after 4 and 8 week storage in various

69
substances generally thought to cause intra-oral discoloration. In particular, red wine
and turmeric solution caused severe discoloration with total differences of ∆E >10 in
all tested composites. It is apparent from our results that it remains essential to
improve the color stability of Targis material used for esthetic facing. In a short-term
observation period, the FRC showed good clinical service but these results need more
observation in order to create a sound basis for the final assessment of this method.
In our study the veneering composite had less fractures with modified FRC
frameworks than with the conventional design. Based on our observations the repair
of FRC fractured veneer is advisable only for small damages.
References
Altieri JV, Burtone CJ, Goldberg AJ, Patel AP. Longitudinal clinical evaluation of fiber-reinforced composite FPDs: a pilot study: J Prosthet Dent 1994;71:16-22.
Behr M, Rosentritt M, Leibrock A, Schneider-Feyrer S, Handel G. In vitro-study
of fracture strength and marginal adaptation of fibre-reinforced adhesive fixed partial inlay dentures. J Dent 1999;27:163-168.
Creugers NH, De Kanter RJ, Van’t Hof MA. Long-term survival data from a
clinical trial on resin bonded bridges. J Dent 1997;25:239-242. Creugers NH, Käyser AF, Van’t Hof MA. A seven-and-half–year survival study
of resin-bonded bridges. J Dent Res 1992;71:1822-1825. Creugers NHJ, De Kanter RJ. Patients’ satisfaction in two long-term clinical
studies on resin-bonded bridges. J Oral Rehabil 2000;27:602-607. Creugers NHJ, Käyser AF, Van’t Hof MA. A meta-analysis of durability data on
conventional fixed bridges: Community Dent and Oral Epidemiol 1994; 22:448-452. De Kanter RJ, Creugers NH,Verzijden CW, Van’t Hof MA. A five-year multi-
practice clinical study on posterior resin-bonded bridges. J Dent Res 1998;77:609-614.
DeBoer J, Vermilyea SG, Brady RE. The effect of carbon fiber orientation on
the fatigue resistance and bending properties of two denture resins. J Prosthet Dent 1984;51:119-121.
70
Douglas DR. Color stability of new-generation indirect resins for prosthodontics application. J Prosthet Dent 2000;83:166-170.
Ehrenstein GW, Schmiemann A, Bledzki A, Spaude R. Corrosion phenomena in
glass-fiber-reinforced thermosetting resins. In: Cheremisinoff NP (ed). Handbook of ceramics and composites, vol 1. New York: Marcel Dekker, 1990:231-268.
Ekstrand K, Ruyter IE. Carbon/graphite fiber reinforced poly(methyl
methacrylate): properties under dry and wet conditions. J Biomed Mater Res 1987;21:1065-1080.
Freilich MA, Duncan JP, Meiers JC, Goldberg AJ. Preimpregnated, fiber-
reinforced prostheses. Part I: basic rationale and complete coverage and intracoronal fixed partial denture designes. Quintessence Int 1998;29:689-696.
Freilich MA, Duncan JP, Meiers JC. Preimpregnated, fiber-reinforced
prostheses. Part I. Basic rationale and complete-coverage and intracoronal fixed partial denture designs. Quintessence Int 1998:29:689-696.
Göhring TN, Krejci I, Lutz F. Adhäsive Inlaybrücken aus glasfaserverstärktem
Komposit. Step by step-Beschreibung der klinischen Anwendung. Schweiz Monatsschr Zahnmed 1999;109:369-379.
Göhring TN, Mörmann WH, Lutz F. Clinical and scanning electron microscopic
evaluation of fiber-reinforced inlay fixed partial dentures: Preliminary results after one year. J Prosthet Dent 1999;82:662-668.
Gregory DC, Pounder B, Bakus E. Bond strengths of chemically dissimilar
repaired composite resins. J Prosthet Dent 1990;64:664-668. Gutterridge DL. Reinforcement of poly(methyl methacrylate) with ultra-high-
modulus polyethylene fiber. J Dent 1992;20:50-54. Hess D, Belser U. Provisional extension bridges reinforced with Kevlar.
Schweiz Monatsschr Zahnmed 1987;97:457-463. Hussey DL, Linden GJ. The clinical performance of cantilevered resin-bonded
bridgework. J Dent 1996;24:251-256. Ivoclar: Scientific Document. Ivoclar-Vivadent, Schaan, FL, 1996. Kerschbaum T, Haastert B, Marinello CP. Risk of debonding in three-unit resin-
bonded fixed partial dentures. J Prosthet Dent 1996;75:248-253. Krause WR, Park SH, Straup RA. Mechanical properties of BIS-GMA resin
short glass fiber composites. J Biomed Mat Res 1989;23:1195-1211. Krejci I,Boretti R, Giezendanner P, Lutz F. Adhesive crowns and fixed partial
dentures fabricated of ceromer/FRC: clinical and laboratory procedures Pract

71
Periodont Aesthet Dent 1998;10:487-498. Larson WR, Dixon DL, Aquilino SA, Clancy JM. The effect of carbon graphite
fiber reinforcement on the strength of provisional crown and fixed partial denture resins. J Prosthet Dent 1991;66:816-20.
Lassila LVJ, Nohrström T, Vallittu K. The influence of short term water storage
on the flexural properties of unidirectional glass fiber-reinforced composite. Biomaterials 2002;23:2221-2229.
Leal FR, Cobb DS, Denehy GE, Margeas RC. A conservative aesthetic solution
for a single anterior edentulous space: case report and one-year follow-up. Pract Proced Aesthet Dent 2001;13:635-641.
Lutz F, Göhring TN. Fiber-reinforced inlay fixed partial dentures: maximum
preservation of dental hard tissue. J Esthet Dent 2000;12:164-171. Näpänkangas R, Salonen-Kemppi MAM, Raustia AM. Longevity of fixed metal
ceramic bridge prostheses: a clinical follow-up study. J Oral Rehabil 2002;29:140-145.
Perdigão J, Lopes M. Dentin bonding-state of art 1999. Compend Contin Educ
Dent 1999;20:1151-1162. Powers JM, Fan PL, Raptis CN. Color stability of a new composite restorative
material under accelerated aging. J Dent Res 1980;59:2071.2074. Rosentritt M, Behr M, Kolbeck C, Handel G. In vitro repair of three-unit fiber-
reinforced composite FPDs. Int J Prosthodont 2001;14:344-349. Rosentritt M, Behr M, Leibrock A, Handel G, Friedl KH. Intraoral repair of
fiber-reinforced composite fixed partial dentures. J Prosthet Dent 1998;79:393-398. Rosentritt M, Leibrock A, Lang R, Behr M, Scharnagl P, Handel G.
Regensburger masticator. Mater Test 1997;3:77-80. Sorensen JA, Cruz M, Mito WT, Raffeiner O, Meredith HR. Foser HP. A
clinical investigation on three-unit fixed partial dentures fabricated with lithium disilicate glass-ceramic. Pract Periodontics Aesthet Dent 1999;11:95-106.
Stober T, Gilde H, Lenz P. Color stability of highly filled composite resin
materials for facings. Dent Mater 2001;17:87-94. Swift EJ, Le Valley BD, Boyer DB. Evaluation of new methods for composite
repair. Dent Mater 1992 ;8:362-5. Swift, EJ, Bryan CC, Boyer DB. Effect of silane coupling agent on composite
repair strengths. Am J Dent 1994;7:200-202. Uzun G, Hersek N, Tincer T. Effect of five woven fiber reinforcements on the

72
impact and transverse strength of a denture base resin. J Prosthet Dent 1999;81:616-620.
Vallittu PK, Sevelius C. Resin-bonded, glass fiber-reinforced composite fixed
partial dentures: a clinical study. J Prosthet Dent 2000; 84:413-418. Vallittu PK. A review of fiber-reinforced denture base resin. J Prosthodont
1996;5:270-276. Vallittu PK. Flexural properties of acrylic resin polymers reinforced with
unidirectional and woven glass fibers. J Prosthet Dent 1999;25:100-105. Vallittu PK. Oxygen inhibition of autopolymerization of
polymethylmethacrylate-glass fiber composite. J Mater Sci Mater Med 1997;8:489.492.
Vallittu PK. Prosthodontic treatment with a glass fiber-reinforced resin-bonded
fixed partial denture: a clinical report. J Prosthet Dent 1999;82:132-135.

73
Chapter 7: adhesive procedures
7.1 Inlay Bridge With a New Microfilled Composite: A Clinical Report
74
The traditional treatment for a single tooth replacement is a conventional fixed
partial denture (FPD). This technique requires a full-coverage preparation of the
abutments. Consequently, a large quantity of sound tooth is destroyed during the
preparation (Creugers et al 2000). This is particularly problematic in healthy and
young teeth with extensive pulp. In addition, the mean of a FPD is estimated at 8.3-
10.3 years (Creugers et al 1994, Näpänkangas et al 2002). Thanks to evolution of
adhesive dentistry (Perdigão 1999) this destruction can be limited. Resin bonded
fixed partial dentures (RBFPDs) (Freilich et al 1998) and dental implants (Leal et al
2001) constitute the current alternatives. These treatments have several advantages
over conventional bridges, especially in relation to conservation of tooth structure
and their reversibility (Hussey et al 1996).
Fiber-reinforced composites (FRC) have achieved (Freilich 1998) a certain degree of
popularity in restorative dentistry today (Vallittu 1999a). Glass fibers are favorable
for denture base polymer when used in light curing type resin because they have
excellent transparency compared to the other fibers. The advantages of FRC
restorations are that the laboratory procedure is simple because casting is not
necessary, and the bonding ability between resin and reinforced fiber is superior to
that between resin and casting metal, although surface treatment of fiber is necessary
to obtain a strong bonding (Vallittu 1999b).
A novel type of composite material (SR Adoro; Ivoclar Vivadent) has been recently
introduced for dental use. One advantage of this new material is the ability to form
good bonding with the polymer matrix of the glass fiber system (Vectris; Ivoclar
Vivadent) and the luting composite.
This clinical report describes the treatment of a patient with a missing lower first
molar with a new microfilled composite supported with a glass fiber framework.
Inlay Bridge indication
The inlay bridge is indicated in all clinical cases were the replacement of a single
tooth is required but treatment with a dental implant cannot be realized. In the
following situations treatment with implants may not be possible: patient rejects
surgical treatment, costs of implant therapy are too high, not enough bone remaining

75
for the placement of an implant, poor prognosis of implant therapy due to patient
related situations, e.g., smoking and insufficient oral hygiene habits. In this situation,
an inlay bridge offers a more conservative method of tooth replacement compared to
a crown retained conventional bridge because tooth preparations are limited to the
occluso and mesio/distal surfaces of abutment. However these preparations are more
technique sensitive and required a careful adhesive luting procedure. Short spans, not
exceeding 10-12 mm (the space of a molar) are recommended and the preparation
must give the space to the fiber framework to support completely the pontic element.
Clinical Report
A 35-year-old woman presented herself in the Department of Prosthetic Dentistry
of University of Bologna for the replacement of the first lower molar. The patient
was previously treated by her dentist with implant technique without success and was
not willing to have another surgical treatment because of the additional expense.
Intraoral examination revealed the presence of OD composite restoration on the
second premolar and an amalgam filling with a medium decay on the second molar.
The patient opted for a treatment with a conservative glass fiber composite RBFPD.
Clinical Preparation Technique
Before cavity preparation a rubber dam was placed and the cavities were prepared
according to modified principles for adhesive inlays retainers to obtain adequately
strong dental restorations.
No additional bonding FRC wings were made to obtain more bonding surface. The
cavities were prepared with 80 µm (No. 8113R, No. 8113NR, Intensiv SA) and
finished with 25 µm (No. 3113R, No. 3117, Intensiv SA) diamond burs in a medium-
speed handpiece with a water spray and ultrasonic points (SonicSys; Kavo). All the
dentin surfaces of the cavity preparations were sealed with an adhesive system
(Excite DSC, Ivoclar Vivadent). Undercuts and deep parts of the cavities were
covered with a resin composite (Tetric Flow, Ivoclar Vivadent) polymerized for 40
sec. All cavity margins were in enamel and extrasulcus. The distance to marginal

76
gingival was at least 1 mm. Complete mandibular and maxillary arch impressions
were taken with a polyvinyl siloxane (Imprint II, 3M ESPE). A light-cured resin
(Fermit-N, Ivoclar Vivadent) supported by glass fibers of Pontic (Ivoclar Vivadent)
was used as temporary restoration.
Adhesive Procedure
The IFPDs restorations were definitively inserted within 2 weeks after the
impression was made. The operating field was isolated with a rubber dam,
provisional restorations were removed, the teeth were cleaned Tubulicid and rubber
cup and pumice slurry and prepared inside restoration surfaces were sandblasted with
CoJet system (3M ESPE) with small grain size of 30 µm at 2 bar of pressure for 10
seconds. The inlay bridge was tried to check the fit of the restoration. The inner
surfaces of the inlay bridge were sandblasted with CoJet system (3M ESPE) with
small grain size of 30 µm at 2 bar of pressure for 10 seconds and a silane-coupling
agent (Monobond S, Ivoclar Vivadent). All enamel and dentin surfaces were treated
with Excite DSC (Ivoclar Vivadent) according to the manufacturer’s instructions.
The dual-cured luting composite Variolink II (Ivoclar Vivadent), was applied to the
inlays and the inside of the cavities with a disposable brush. The restoration was
inserted in the cavities with a stick and all excess of luting composite was removed.
A layer of a glycerin (Liquid Strip; Ivoclar Vivadent) was applied on the margin
before the polymerization (Fig. 119). The luting composite was light activated for 60
sec. each from cervical, buccal, lingual and occlusal surfaces. The restorations were
then finished with 15 µm diamond burs (Composhape, Intensiv) and polished with a
composite finishing and polishing kit (Hawe Neos Dental) and Astrobrush (Ivoclar
Vivadent) in a slow-speed handpiece. Occlusion and articulation were carefully
checked after the luting step.
Discussion
The replacement of missing tooth with a RBFPD is a very conservative
prosthodontic treatment especially when the patients refuse the treatment with
dental implants. This article describes the replacement of a molar with a
conservative inlay bridge resulting in the good success in the short-term follow up.

77
In a previous study on inlay bridge11 the FRC showed good clinical service but
these results need more observation in order to create a sound basis for the final
assessment of this method. In this study the veneering composite had less fractures
with anatomically shaped FRC frameworks which support the occlusal surface of
the pontic teeth than with the conventional design. The two important points to
achieve the success with this conservative technique are the cavity preparation and
the design of the fiber framework. The cavity must give the space to the fiber
framework to support completely the pontic element. With only very small
preparations such as slots debonding has been a problem. For the retention of Inlay
bridges Ivoclar Vivadent recommends at least two surface cavities of the following
extension: Depth of occlusal cavity ≥2.5 mm; approximo-central extension ≥4mm;
axial depth ≥1.2 mm; proximal step tooth and defect oriented, ideally 2 mm;
bucco-oral width ≥3.5 mm. Nevertheless, if the extension of the defect permits, we
try to realize a larger axial depth and adopted the following preparation guidelines.
Occlusal slot must be 2.0-2.5 mm, occlusal step 2.0 mm, proximal step 2.0 mm,
axial depth 2.0 mm and buccal-vestibular width 3.5 or greater.
The potential advantages of this technique are self-evident. First, the procedure can
be completed in two appointments with low-cost and preservation of sound tooth
tissue. Second, the periodontal apparatus of the abutment teeth is not compromised
in any way. Third, because this approach is relatively little invasive. It permits the
patient to opt for other, more traditional tooth replacement methods in the future.
Fourth, repairs can be carried out directly, without the need for any complicated
techniques or materials.
References
Creugers NHJ, De Kanter RJ. Patients’ satisfaction in two long-term clinical
studies on resin-bonded bridges. J Oral Rehabil 2000;27:602-607.
Creugers NHJ, Käyser AF, Van’t Hof MA. A meta-analysis of durability data on
conventional fixed bridges: Community Dent and Oral Epidemiol 1994; 22:448-
452.

78
Näpänkangas R, Salonen-Kemppi MAM, Raustia AM. Longevity
of fixed metal ceramic bridge prostheses: a clinical follow-up study.
J Oral Rehabil 2002;29:140-145. Perdigão J, Lopes M. Dentin bonding-state of art 1999. Compend Contin Educ
Dent 1999;20:1151-1162.
Freilich MA, Duncan JP, Meiers JC. Preimpregnated, fiber-reinforced prostheses.
Part I. Basic rationale and complete-coverage and intracoronal fixed partial
denture designs. Quintessence Int 1998:29:689-696.
Leal FR, Cobb DS, Denehy GE, Margeas RC. A conservative aesthetic solution
for a single anterior edentulous space: case report and one-year follow-up. Pract
Proced Aesthet Dent 2001;13:635-641.
Hussey DL, Linden GJ. The clinical performance of cantilevered resin-bonded
bridgework. J Dent 1996;24:251-256.
Freilich MA, Duncan JP, Meiers JC, Goldberg AJ. Preimpregnated, fiber-
reinforced prostheses. Part I: basic rationale and complete coverage and
intracoronal fixed partial denture designes. Quintessence Int 1998;29:689-696.
Vallittu PK. Flexural properties of acrylic resin polymers reinforced with
unidirectional and woven glass fibers. J Prosthet Dent 1999;25:100-105.
Vallittu PK. Prosthodontic treatment with a glass fiber-reinforced resin-bonded
fixed partial denture: a clinical report. J Prosthet Dent 1999;82:132-135.

79
Chapter 8: Clinical trial
8.2 Randomized controlled trial of Fiber-Reinforced Composite Inlay Fixed Partial
Dentures: two-year results.

80
The metal-ceramic fixed partial denture (FPD) is a standard restoration for a
single tooth replacement in dental practice. This porcelain-fused-to-metal (PFM) has
demonstrated an excellent record of service for many years, but continues to exhibit
several drawbacks (Freilich et al 1998). A significant amount of sound tooth structure
must be removed when fabricating conventional FPDs. Other potential disadvantages
of the conventional FPDs are discoloration of the gingival and visible metal margins
or “shine through” effects of the metal frameworks (Kolbeck et al 2002). Moreover
base metal alloys may exhibit corrosion and/or may elicit an allergic reaction from a
segment of the patient population (Council on Dental Materials, Instruments and
Equipment 1995).
Implant-supported restorations provide high-quality alternatives to conventional
FPDs. However, in some cases the treatment with implants may not be possible: the
patient rejects surgical treatment, the costs of implant therapy are too high, not
enough bone remaining for the placement of an implant (Sewon et al 2000), poor
prognosis of implant therapy due to patient related situations, e.g., smoking (Gruica
et al 2004) and insufficient oral hygiene habits (Quirynen et al 2002).
In these situations, an inlay fixed partial denture (IFPD) offers a more
conservative method of tooth replacement compared to a crown retained
conventional bridge because tooth preparations are limited to the occluso and
mesio/distal surfaces of abutment (Meiers et al 2001). However these preparations
are more technique sensitive and require a careful adhesive luting procedure (Vallittu
2004). Since the bonding procedures strengthen the cusps and provide additional
support for dentition, minimally invasive preparation is feasible (Morin et al 1984).
The alternatives to conventional PFM prostheses include all-ceramic, all-
particulate composite, and fiber-reinforced composite (FRC) systems. The all-
ceramic and all-particulate composite systems have been described for FPDs (Kern et
al 1991) and IFPDs (Beuchat et al 1999) but, in general, exhibit low resilience and
toughness and are subject to fracture (Fischer et al 2003, Zumbuhl et al 2000).
FRC is composed of two types of composite materials: fiber composites to build
the substructure and a hybrid or microfilled composite to veneer the external
surfaces. Initial in vitro investigations of FRC restorations demonstrated promising
results. After simulation of oral stresses, the fracture resistance and marginal
adaptation of adhesively fixed molar crowns, IFPDs and three-unit complete

81
coverage FPDs were better than for all-ceramic restorations (Loose et al 1998). The
fracture resistance of IFPDs showed a mean of about 700N, a value that led to the
expectation that these restorations would be successful under clinical conditions
(Behr et al 1999). Marginal adaptation of adhesively cemented FRC restorations was
shown to remain statistically unchanged after simulation of 5 years of oral stress. It
can be concluded from the in vitro wear investigations that the veneering composite
will have a wear rate comparable to enamel during a period of 5 years, and that it
can bear the load in occlusal contact areas (Kern et al 1999, Knobloch et al 1999).
After 2 years of observation, an investigation on forty IFPDs reported 89.6% of
continuous margin at the tooth-luting composite interface but four inlay bridges
failed for debonding or delamination of veneering material (Göhring et al 2002).
Similar results on the survival rate were obtained in two different studies after a
three-year observation period using two different FRC systems. Behr (Behr et al
2003) achieved 72% of survival rate using the Targis/Vectris (Ivoclar Vivadent Inc.,
Schaan, Liechtenstein) system as Freilich (Freilich et al 2002) that reported 75% of
survival rate for FiberKor/Sculpture (Pentron Laboratory Technologies LLC,
Wallingford, Conn). Fiber-reinforced composite used in IFPDs is a promising
material group but little clinical information is available compared to the traditional
prosthodontic materials.
The purpose of this randomized controlled trial was to collect survival data on
posterior IFPDs, using a new microfilled composite in combination with a fiber
framework system (SR Adoro/Vectris, Ivoclar Vivadent) placed under controlled
clinical conditions and to identify the clinical behaviour of two different bonding
systems used to lute the inlay bridges (Excite DSC versus Syntac, Ivoclar Vivadent).
The null hypothesis tested in this study was: there is no difference in postoperative
sensitivity and clinical behaviour between the two-step dual cured adhesive versus
the three-step adhesive bonding system in IFPDs.
MATERIALS AND METHODS
Thirty-nine patients were screened and received an indirect restoration. The selection
of the patients followed two criteria: their refusal to treatment with dental implants
and informed written consent. The study was approved by the Ethics Committee of

82
the University of Bologna. Selection of male and female subjects was restricted to
those aged 18-60 years and in good general and periodontal health. Patients with the
following factors were excluded from the clinical trial: patients receiving drugs that
modify pain perception, pregnancy or breast feeding, eating disorders, periodontal
surgery, well-known allergy to chemical compounds used in this study. The inclusion
criteria were: patients with a missing tooth, absence of any active perio or pulpal
disease, proximal margin located above the cementum-enamel junction, placement of
the rubber dam possible and the greatest distance between the abutments was smaller
or equal to 12 millimeters. The patients were divided in two groups. In the nineteen
patients of group A the Excite DSC adhesive system was used, in those of group B
the cementation was carried out with Syntac. The randomization of the patients was
performed with the toss of a coin.
From June 2002 to July 2004 thirty-nine IFPDs were inserted. Twenty-two
restorations were placed in mandibular teeth and 17 in maxillary teeth and evaluated
using the USPHS criteria. Three bridges had been luted to replace the first premolar,
fifteen for the second premolar and twenty-one to replace the first molar (Fig. 1-6).
Twenty-four restorations were between 2- and 3-year old, eleven bridges were
included between one and two years and only four restorations were less 1-year old
but had more than six months. Average service time of the IFPDs was 23.4 months.
Clinical Preparation Technique
At baseline all patients were tested for dentin sensitivity. In the rank order data, a
score of zero was defined as no pain (alpha), 1-4 as mild sensitivity (bravo), which
was provoked by the dentists’ air blast, and 5-10 as strong sensitivity (Charlie),
which was spontaneously reported by the patient during drinking or eating. The same
measurement was performed again at each recall. The status of the gingival tissues
adjacent to the test sites was observed at baseline and each recall.
Before cavity preparation a rubber dam was placed and all cavities were prepared
according to modified principles for adhesive inlays retainers to obtain adequately
strong dental restorations. No additional bonding FRC wings were made to obtain
more adhesional surface. The cavities were prepared with 80µm (No. 8113R, No.
8113NR, Intensiv SA) and finished with 25µm (No. 3113R, No. 3117, Intensiv SA)

83
diamond burs in a medium-speed handpiece with a water spray. The design of the
cavity preparations followed the philosophy of maximal preservation of sound tooth
(Göhring et al 1999). Pre-existing restorations were removed and their cavities were
used as abutments after appropriate preparation. In situations of primary carious
lesions, defect-oriented tooth cavities were prepared within the concept of minimal,
but adequately sized, inlay abutments. The cavity had to give the space to the fiber
framework to completely support the pontic element. The form of the cavity was at
least two surfaces with the following extension: depth of occlusal cavity ≥2.5 mm;
occluso-cervical height ≥4mm; axial depth ≥1.2 mm; bucco-oral width ≥3.5 mm. The
measurements of the cavities were verified with a periodontal probe after the
finishing of the cavity margins. Nevertheless, if the extension of the defect permits,
we try to realize a larger axial depth and adopted the following preparation
guidelines. A taper of ≈4° (or larger if given by the pre-existing restoration) was
chosen to simplify insertion. According to the pre-existing restorations, most
proximal boxes were larger. The distribution of the cavity preparations are described
in table 1.
All the dentin surfaces of the cavity
preparations were etched for 15” with
35% phosphoric acid and sealed with two
bonding systems Excite DSC or Syntac
(Ivoclar Vivadent). The same adhesive
system used for the dentin hybridization
was employed for the luting procedure.
Undercuts and deep parts of the cavities
were covered in increments with a highly
viscous composite (Tetric Ceram, Ivoclar
Vivadent) polymerized for 40 sec. The
excesses of the bonding on the enamel surfaces were removed with 25µm (No.
3113R, No. 3117, Intensiv SA) diamond burs in a medium-speed handpiece with a
water spray. All cavity margins were in enamel and extrasulcus. The distance to
marginal gingival was at least 1 mm. Complete mandibular and maxillary arch
Table 1 Different distribution
of the preparations
Slot 9
Mesio-occlusal 21
Disto-occlusal 23
Mesio-disto-occlusal 14
Onlay 5
Overlay 4
Crown 2
Total abutments 78

84
impressions were taken with a polyether material (Permadyne, 3M ESPE). A light-
cured resin (Fermit-N, Ivoclar Vivadent) was used as temporary restoration.
Laboratory Technique
According to the manufacturer’s instructions (Transil technique), the Vectris
frameworks in the IFPDs were made with pre-impregnated ‘pontic’ and ‘frame’
fibers and all restorations had an anatomical shape of the framework like an oval
shape to hold the layering material in a continuous manner and reach a high volume
of the substructure. The final design of the bridge’s framework was similar to metal
framework with extensions in the vestibular and buccal side to completely support
the veneer composite.
The design of the fiberglass framework was first pre-modeled by a photo-curing resin
(Spectra Tray, Ivoclar Vivadent) to obtain the oval shape and its thickness checked in
the molding model. This model was embedded in a transparent silicone impression
paste to form a mould. Then this resin was removed and the fibers were applied into
the silicone-mould (Transil, Ivoclar Vivadent). The pre-impregnated ‘pontic’ fibers
were condensed into the desired shape by a vacuum- forming process and then cured
by light in a VS1 unit (Ivoclar Vivadent) for 10 min. According to the manufacturer’s
recommendations, the FRC was treated with silane (Wetting agent, Ivoclar-
Vivadent). A sheet of wave fibers ‘frame’ was placed upon the ‘pontic’ structure and
the cycle in VS1 was repeated. The SR Adoro material was built incrementally using
a Quick light-curing unit. Finally, the IFPD was placed into a Lumamat 100 unit
(Ivoclar Vivadent) for the final application of light and heat (104°C) to complete
polymerization and maximize strength and other physical characteristics.
Adhesive Procedure
The IFPDs restorations were inserted within 2 weeks after the impression was
made. The operating field was isolated with a rubber dam, provisional restorations
were removed with a sharp probe and the prepared teeth were cleaned with nylon
bristle brushes and water spray. The inner surfaces of the inlay retainers were
sandblasted with CoJet system (3M ESPE) with small grain size of 30 µm at 2 bar of
pressure for 10 seconds. These treated inner surfaces were then silanated by using

85
Monobond-S (Ivoclar Vivadent). Just before the final cementations, the surfaces
were the bonding agent (Heliobond or Excite DSC; Ivoclar Vivadent) was brushed
on the surfaces and air thinned. To prevent early polymerization of this layer
especially for the Heliobond, the bridge was shielded against light until insertion. All
enamel finish lines were conditioned with 35% phosphoric acid gel (Ivoclar
Vivadent) for 30 seconds whereas the dentin surfaces were etched with the same acid
for 15 seconds. The Group A was treated with Excite DSC and Group B with Syntac
according to the manufacturer’s instructions. Both the adhesive bonding systems
weren’t polymerized before the placement of the luting composite. The bonding
agent was blown to a thin layer and the dual-cured composite resin cement Variolink
II (Ivoclar Vivadent) was used to lute the restorations. The luting composite was light
activated for 60 sec. (Optilux 500, Kerr) each from cervical, buccal, lingual, and
occlusal surfaces. Occlusion and articulation were carefully checked after the
cementing step. The restorations were then finished with 15�m diamond burs
(Composhape, Intensiv) and polished with a composite finishing and polishing kit
(Hawe Neos Dental) and silicone-carbide impregnated bristle brushes (Astrobrush,
Ivoclar Vivadent) in a slow-speed handpiece. Approximal finishing was performed
with flexible discs and abrasive strips (Soflex pop-on; 3M ESPE).
Fig. 1. X-ray preoparatory Fig. 2. Initial status
Fig. 3. The cavity preparation Fig. 4. IFPD made with fiber reinforced
composite.

86
Fig.5. The inlay bridges after the
cementation under rubber dam.
Fig. 6. Follow-up after 2 years.
Evaluation
Two independent examiners (C.M., M.C.) evaluated under magnification (Zeiss
3.6x35mm) all the restorations directly after the final polishing and after one week, 6,
12, 24 and 36 months. At baseline, and at 1-yr and 2-yr examinations, X-rays were
performed to check for surplus, marginal gaps, and secondary caries. During the
recalls, the patients came back to the office to answer questions about post-operative
sensitivity. Partial or total debonding of IFPDs, framework or resin composite
fractures and fiber exposures were considered failures. The restorations were
evaluated using the USPHS (Ryge et al 1973) modified parameters, to check their
stability and longevity in regard to the following characteristics: color match,
marginal discoloration, secondary caries, surface texture, marginal adaptation,
fracture and postoperative sensitivity. Alpha (α) means perfect condition, Bravo (β)
show restorations that are clinically acceptable, Charlie (c) indicate a need for
immediate replacement. In cases with only two decision possibilities, eg, debonding
or no debonding, the rating comprised only α or c (c= debonding). Plaque growth
and gingival health at the gingival pontic surfaces, abutment inlays and contralateral
control teeth were also measured using the plaque index (PI) and gingival index (GI).
Statistical analysis was applied to compare the restorations at the baseline and
after the last recall, and to check for differences between Group A and B. The
Wilcoxon’s matched-pairs signed ranks test measured the restorations’ success at the

87
appropriate time intervals and was used to rate all parameters. The Mann-Whitney
test was used to compare the data between the two groups. The null hypothesis was
rejected at the 5% level. The survival estimation method of Kaplan-Maier was used
with statistical software (JMP 5.1).
Table 2. Clinical results based on USPHS criteria after two-year.
Abutments
(n=78)
One week
α
Last
Recall α
One week
β
Last
Recall
β
One week
c
Last
Recall
c
Groups A B A B A B A B A B A B
Marginal
discoloration
38 40 37 40 - - - - - - 1 -
Secondary
caries
38 40 38 40 - - - - - - - -
Marginal
adaptation
38 40 34 40 - - 4 - - - - -
Postoperative
sensibility
23 38 36 40 5 2 - - 10 - 2 -
Debonding 38 40 35 40 - - - - - - 3 -
IFPDs (n=39)
Fracture
(including
chipping)
19 20 17 18 - - - - - - 2* 2
Surface
texture
18 20 18 20 1 - 1 - - - - -
Color match 17 17 17 16 2 3 2 4 - - - -
Fiber
exposure
19 20 19 18 - - - - - - - 2
* The micro fractures were visible only under SEM examination after the detachment of the
bridges.

88
RESULTS
The results are summarized in table2. During the observation time, two debondings
after 2 and 8 months were detected for the IFPDs luted with Excite DSC bonding
system. The detected bridges were immediately replaced with another inlay bridge
luted with Syntac. Some micro cracks in the pontic area of the two detached bridges
were observed under SEM (Fig. 7a-b). Two fiber exposures were noted after 8
months on the occlusal surface of one IFPD. The framework was visible under low
magnification (Zeiss 3.6x35mm) for self-evident color change. This kind of failure
was most probably due to the previous occlusal adjustment done after the
cementation that had left a thin layer of composite upon the fiber framework. The
bridge wasn’t replaced and is under observation now. Some hairline fracture of the
veneering materials near the connection between the pontic and the abutment were
detected in two cases (Fig. 8-9; a-b). No statistical differences regarding
detachment were showed between baseline and last recall between Group A and B
(P>0.05).
There was no fracture of the pontics, inlay retainers or inlay margins. The
IFPDs was always rated “alpha” with respect to secondary caries and surface
texture. The two debonded bridges showed “charlie” rating for the marginal
adaptation on six abutments and marginal discoloration on one abutment at the last
recall. Moderate to severe postoperative sensitivity was rated during the first six
months of the observation period. All hypersensitive teeth belonged to group A
luted with two-step bonding system. The higher values of sensitivity recorded
during the temporary restoration time were reported for group A. These patients
primarily reported strong chewing pain during the mastication and less temperature
sensitivity (10a-b). The dentinal sensitivity diminished after approximately 12
weeks and completely disappeared after six months in all cases except one
abutment that was endodontically treated in the retainer area without removal of
the bridge. The statistical analysis showed significant differences (P<0.05) for the
sensitivity between group A and group B at baseline and inside of group A during
the observation period. Group A showed 42.2% of dentinal sensitivity after 1
month unlike group B that recorded 0%. The percentage of “bravo” for the color
match was stable at 86.8% during the observation period and didn’t change at any

89
time. Plaque growth was moderate but no statistical differences occurred in PI and
GI between the abutments, pontics and contralateral teeth. The Kaplan-Maier
survival estimation was 89.4% for group A and 100% for the group B after 24
months. (Fig 11).
Fig. 7A. Gingival side of the
detached bridge. Some fractured
glass fibers are visible.
Fig. 7B. The pontic fibers are clearly visible
under magnification (x1000) after the
fracture of veneering composite.
Fig. 8A. The presence of old
restorations on the abutments near the
edentulous space is the typical situation
for the IFPDs.
Fig. 8B. The clinical condition doesn’t
permit to make a fiber framework with
ideal dimensions. This characteristic
could cause flexibility of the bridge.
Fig. 9A. The IFPD after 8 months Fig. 9B. The same bridge after 2 years.
The finger indicates the hairline fracture
of the veneering material in the pontic
element near the connection with the
inlay.
Fig. 10A. This image represents
impression of the dentin surface after the
hybridization with Excite DSC. Some
areas show the presence of hallows due
to the intrapulpal pressure that could
cause the hypersensitivity during the
chewing.
Fig. 10B. At 1000 magnification are
clearly visible the ditching created by
the dentinal fluid.
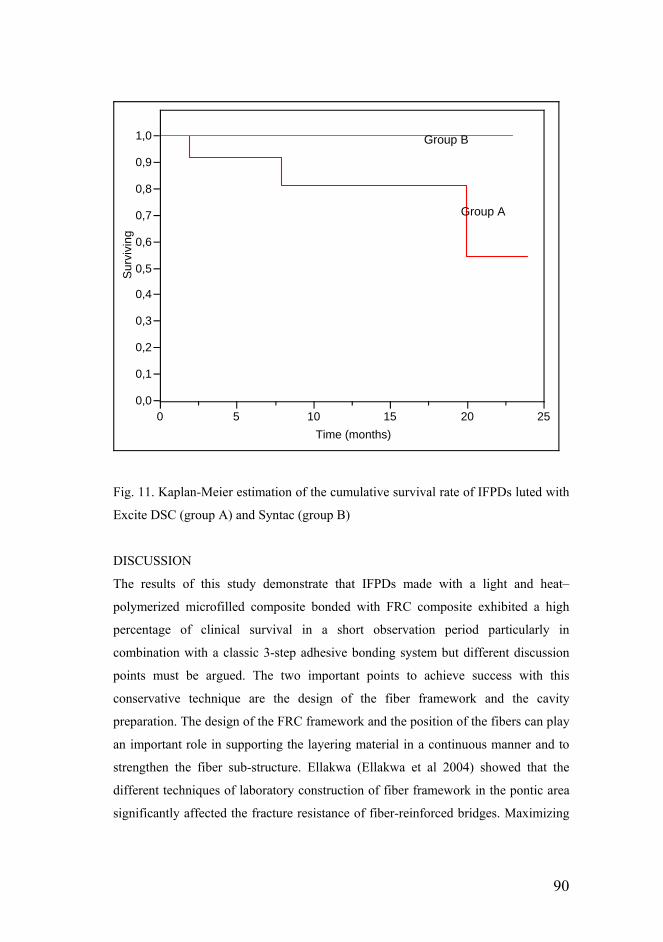
90
0,0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1,0S
urvi
ving
0 5 10 15 20 25Time (months)
Fig. 11. Kaplan-Meier estimation of the cumulative survival rate of IFPDs luted with
Excite DSC (group A) and Syntac (group B)
DISCUSSION
The results of this study demonstrate that IFPDs made with a light and heat–
polymerized microfilled composite bonded with FRC composite exhibited a high
percentage of clinical survival in a short observation period particularly in
combination with a classic 3-step adhesive bonding system but different discussion
points must be argued. The two important points to achieve success with this
conservative technique are the design of the fiber framework and the cavity
preparation. The design of the FRC framework and the position of the fibers can play
an important role in supporting the layering material in a continuous manner and to
strengthen the fiber sub-structure. Ellakwa (Ellakwa et al 2004) showed that the
different techniques of laboratory construction of fiber framework in the pontic area
significantly affected the fracture resistance of fiber-reinforced bridges. Maximizing
Group A
Group B

91
fiber volume fraction by increasing the proportion of fiber to composite should
significantly improve strength (Butterworth et al 2003). The position of the FRC
layer can have an effect on the flexural strength. Continuous unidirectional fibers
gave the highest strength and stiffness only in the direction of the fiber, while woven
fibers were able to reinforce the denture base polymers in two directions (De Boer et
al 1984).
The laboratory technique used in this study allows the extension in the vestibular and
buccal side to support the layering material like in metal framework and hold it in all
loading directions. The framework in the FRC was made in an anatomical shape in
the pontic element with parallel and weave fiberglasses. Vestibular and buccal FRC
extensions in the pontic element can increase the bonding area between the
framework and resin composite as well as hold the veneer material better during
occlusal loading. This observation suggested that modified design of frameworks
could increase the bond strength of resin composite to the fiber framework when
chewing (Monaco et al 2003). A similar approach was used by Freilich (Freilich et al
2002) that hypothesized the increased rigidity and a broader base of support provided
by the FRC substructure was needed to support the composite veneer. Thus, they
added a substantial amount of FRC bulk to the pontic component of the substructure
(low-volume design), resulting in the creation of the “high-volume” substructure
design and examined their relationship with the clinical performance. They observed
a 95 percent survival rate for the high-volume prostheses in contrast to a 62 percent
survival rate for the low-volume prostheses over a 3-year observation period. Similar
clinical results were shown in our previous study (Monaco et al 2003) on the
relationship between composition and substructure design and clinical performance
of Targis/Vectris system after a 4-year follow up period. The authors achieved a
97.5% survival rate for the framework built with parallel and woven fibers modifying
the design of the pontic element in an anatomical shape versus a 84% survival rate
for the restorations with simplified frameworks made only with parallel fibers.
Göhring (Göhring et al 2005) observed 36 posterior FRC IFPDs and after 5 years
they reported 71% of survival rate. Most failures were related to delaminations of the
veneering material and they are in agreement that modified framework design

92
significantly reduced the delamination rate (Göhring et al 2003). However, long-term
clinical studies must be conducted to confirm this hypothesis.
The detachments occurred in two clinical border-line cases. The first happened after
2 months in a patient with parafunctional habits whereas the second occurred after 8
months in a case with long span replacement (11 mm). The examination of the failed
bridges under SEM disclosed micro cracks in the gingival areas between the pontic
element and the inlay probably due to fatigue phenomena of the veneering material.
Lassila (Lassila et al 2004) achieved the highest flexural strength when the FRC layer
was located at the tension side of the test specimens. The particulate filler composite
is the weaker phase of the system. They demonstrated that when it is located on the
tension side, the fracture could easily initiate. The FRC structure benefits most when
the tensile stresses can be transferred to the reinforcing fibers. The veneering
particulate filler composite is strong in compression stress and, therefore, the FRC
structure requires less reinforcement fibers on the compression side. This area
represents a tensile zone and the SEM pictures showed the inner glass fiber of the
substructures.
Key elements for the clinicians include tooth preparation design that must allow an
adequate amount of FRC, an accurate interocclusal registration, and proper insertion
technique. An inadequate interocclusal registration could results in a considerable
occlusal adjustment by the dentist and the potential for inadvertent occlusal exposure
of the FRC substructure of an extremely thin layer of the composite veneer in
functional areas.
Color match of veneering composite (SR Adoro) was extremely stable unlike that of
the predecessor material (Targis) that showed in a previous study (Monaco et al
2003) a percentage of bravo in colour match of 29% at the last recall and the
deterioration was significant compared to the initial status. In this study, the clinical
evaluation of the FRC inlay bridges showed that the microfilled composite veneer
material exhibited good colour stability and resistance to wear. The surface texture
exhibited no change except for one case with a small chipped area most probably due
to a fabrication error.
Group A luted with Excite DSC showed a dentinal sensitivity slightly below 50%
after 1 month unlike group B luted with Syntac that didn’t record post-operative

93
sensitivity. Excite DSC is an ethanol-based, two step, dual-curable, single-bottle
adhesive. Total etch or simplified adhesives are more sensitive to the technique
because optimal hybridization and sealing of dentinal tubules with the wet bonding
technique may differ with each bonding system (Frankenberger et al 2000). Ferrari
(Ferrari et al 2003) confirmed the sensitivity of the technique with this adhesive
system showing in vivo no hybrid layer and extensive nanoleakage after excessive
drying and water tree formation along resin-dentin interfaces during excessive
wetting. Because the volatile adhesive solvent evaporates quickly, the continuous
transudation of dentinal fluid through open dentinal tubules before polymerization of
the adhesive may result in the entrapment of water-filled blisters along the adhesive
interface (Pashley et al 2002, Tay et al 2003). As the patient masticates, these blisters
may create a pumping effect that causes rapid movement of fluid through the tubules,
which in turn may trigger the A-delta nerve fibres in the pulpal-dentin complex
(Brännström et al 1972). Although most bonded restorations are retained because
there is a sufficient well-bonded surface area, a common clinical manifestation of
inconsistent bonding within a restoration is the patient’s complaint concerning post-
operative sensitivity (Unemori et al 2001). Clinically, no postoperative sensibility
was reported by the patients of the group B. This favorable outcome may be related
to the three-step adhesive bonding system associated to the methods used in the study
to seal the dentin before taking the impression. An accurate control times of the
primer and of the bonding agent (>20 s) can ensure against the postoperative
sensibility during the temporary period and after the final luting procedure.
Conclusion
In a short-term observation period, the FRC showed good clinical service but these
results need more observation in order to create a sound basis for the final
assessment of this restoration technique. The clinicians and the dental technicians
need to strictly follow indications, contraindications and instructions to achieve a
satisfactory clinical result. If a conservative inlay FPD is clinically indicated, the
patient must be informed that loss of sound hard tissue is minimal but durability of
a conventional ceramic fused to metal full coverage FPD and implant treatment is
more proven.

94
References
Behr M, Rosentritt M, Handel G. Fiber-reinforced composite crowns and FPDs: a
clinical report. Int J Prosthodont. 2003 May-Jun;16(3):239-43.
Behr M, Rosentritt M, Leibrock A, Schneider-Feyrer S, Handel G. In-vitro study of
fracture strength and marginal adaptation of fibre-reinforced adhesive fixed partial
inlay dentures. J Dent. 1999;27:163-168.
Beuchat M, Krejci I, Lutz F. Minimally invasive unreinforced adhesive
composite bridges: the clinical procedure. Schweiz Monatsschr Zahnmed.
1999;109:507-519.
Brännström M, Aström A. The hydrodynamics of the dentine: its possible
relationship to dental pain. Int Dent J 1972;22:219-227
Butterworth C, Ellakwa AE, Shortall A. Fibre-reinforced composites in
restorative dentistry. Dent Update. 2003;30:300-6.
DeBoer J, Vermilyea SG, Brady RE. The effect of carbon fiber orientation on
the fatigue resistance and bending properties of two denture resins. J Prosthet Dent
1984;51:119-121.
Ellakwa AE, Shortall AC, Marquis PM. Influence of different techniques of
laboratory construction on the fracture resistance of fiber-reinforced composite
(FRC) bridges. J Contemp Dent Pract 2004;4:001-013.
Ferrari M, Tay FR. Technique sensitivity in bonding to vital, acid-etched dentin.
Oper Dent. 2003 Jan-Feb;28:3-8.
Fischer H, Weber M, Marx R. Lifetime prediction of all-ceramic bridges by
computational methods. J Dent Res. 2003;238-242.
Frankenberger R, Kramer N, Petschelt A. Technique sensitivity of dentin
bonding: effect of application mistakes on bond strength and marginal adaptation.
Oper Dent 2000;25:324-330.
Freilich MA, Karmaker AC, Burstone CJ, Goldberg AJ. Development and
clinical applications of a light-polymerized fiber-reinforced composite. J Prosthet
Dent. 1998;80:311-318.
Freilich MA, Meiers JC, Duncan JP, Eckrote KA, Goldberg AJ. Clinical
evaluation of fiber-reinforced fixed bridges. J Am Dent Assoc. 2002

95
Nov;133(11):1524-34; quiz 1540-1.
Freilich MA, Meiers JC, Duncan JP, Eckrote KA, Goldberg AJ. Clinical
evaluation of fiber-reinforced fixed bridges. J Am Dent Assoc. 2002;133:1524-1534
Göhring TN, Mörmann WH, Lutz F. Clinical and scanning electron microscopic
evaluation of fiber-reinforced inlay fixed partial dentures: preliminary results after
one year. J Prosthet Dent 1999; 82: 369-377.
Göhring TN, Roos M. Inlay-fixed partial dentures adhesively retained and reinforced
by glass fibers: clinical and scanning electron microscopy analysis after five years.
Eur J Oral Sci, 2005; 113: 60–69.
Göhring TN, Schmidlin PR, Lutz F. Two-year clinical and SEM evaluation of glass-
fiber-reinforced inlay fixed partial dentures. Am J Dent. 2002;15:35-40.
Göhring TN, Zappini G, Mayer J, Zehnder M. Optimization of glass-fiber
framework for fixed partial dentures: Laser-interferometrical analysis. Quintessenz
Int 2003; 35: 668–675.
Gruica B, Wang HY, Lang NP, Buser D. Impact of IL-1 genotype and smoking
status on the prognosis of osseointegrated implants. Clin Oral Implants Res.
2004;15:393-400.
Kern M, Knode H, Strubb JR. The all-porcelain, resin-bonded bridge.
Quintessence Int. 1991;22:257-262.
Kern M, Strub JR, Lu XY. Wear of composite resin veneering materials in a
dual-axis chewing simulator. J Oral Rehabil. 1999;26:372-378.
Knobloch LA, Kerby RE, Seghi R, van Putten M. Two-body wear resistance and
degree of conversion of laboratory-processed composite materials. Int J Prosthodont.
1999;12:432-438.
Kolbeck C, Rosentritt M, Behr M, Lang R, Handel G. In vitro examination of
the fracture strength of 3 different fiber-reinforced composite and 1 all-ceramic
posterior inlay fixed partial denture systems. J Prosthodont. 2002;11:248-253.
Lassila LVJ, Vallittu PK. The effect of fiber position and polymerization
condition on the flexural properties of fiber-reinforced composite. J Contemp Dent
Pract 2004;2:014-026.
Loose M, Rosentritt M, Leibrock A, Behr M, Handel G. In vitro study of
fracture strength and marginal adaptation of fiber-reinforced-composite versus all

96
ceramic fixed partial dentures. Eur J Prosthodont Restor Dent. 1998;6:55-62.
Meiers JC, Freilich MA. Chairside prefabricated fiber-reinforced resin
composite fixed partial dentures. Quintessence Int. 2001;32:99-104.
Monaco C, Ferrari F, DDS, Miceli GP, Scotti R. Clinical Evaluation of Fiber-
Reinforced Composite Inlay Fixed Partial Dentures. Int J Prosthodont 2003;16:319-
325.
Monaco C, Miceli GP, Scotti R. Die mit dem neuen, mikrogefüllten Komposit-
Material SR Adoro verblendete Inlay-Brücke. Quintessenz Zahntech 2003;3:292-
305.
Morin D, DeLong R, Douglas WH. Cusp reinforcement by the acid-etch
technique. J Dent Res. 1984;63:1075-1078
Pahley DH, Pashley EL, Carvalho RM, Tay FR. The effects of dentin
permeability on restorative dentistry. Dent Clin North Am 2002;46.211-245.
Quirynen M, De Soete M, van Steenberghe D.Infectious risks for oral implants:
a review of the literature. Clin Oral Implants Res. 2002;13:1-19.
Report on base metal alloy for crown and bridge applications: benefits and risks.
Council on Dental Materials, Instruments and Equipment. J Am Dent Assoc
1995;111:479-483.
Ryge G, Snyder M. Evaluating the clinical quality of restorations. J Am Dent
Assoc 1973;87:369-377.
Sewon LA, Ampula L, Vallittu PK. Rehabilitation of a periodontal patient with
rapidly progressing marginal alveolar bone loss: 1-year follow-up. J Clin
Periodontol. 2000;27:615-619.
Tay FR, Pashley DH. Have dentin adhesives become too hydrophilic? J Can
Dent Assoc 2003;69:726-731.
Unemori M, Matsuya Y, Akashi A, Goto Y, Akamine A. Composite resin restoration
and postoperative sensitivity: clinical follow-up in an undergraduate program. J Dent
2001;29:7-13.
Vallittu PK. Survival rates of resin-bonded, glass fiber-reinforced composite
fixed partial dentures with a mean follow-up of 42 months: a pilot study.J Prosthet
Dent. 2004;91:241-246.
Zumbuhl R, Lutz F, Krejci I. In-vitro studies of resin-bonded slot composite bridges

97
compared to conventionally prepared composite bridges. Schweiz Monatsschr
Zahnmed. 2000;110:505-522.

98
Chapter 9: Alternative materials as regards FRC
Fatigue test in shear: its effect on bond of a glass-infiltrated alumina ceramic to
human dentin, using different luting procedures.

99
The concepts of minimally invasive dentistry combined with adhesive technique
have been highly recommended because it’s based on the conservation of dental
structure. (Degrange et al 1997). Hence, the ceramic partial restorations compared
with complete crowns present this conservative approach because they are minimally
invasive. Thus, it is important that the enamel/dentin and the ceramic substrate are
appropriately conditioned to optimize this adhesive process. (Özcan 2002, Özcan &
et al 2002, Özcan 2003, Özok et al 2004,Reis et al 2004).
With the increase of aluminum oxide content (Al2O3) in feldspar ceramics,
there is a significant improvement in the mechanical properties allowing metal-free
restorations to be employed more predictably (Tinschert et al 2000, Guazzato et al
2004). In posterior teeth with high mechanical loading, the ceramics with high
crystalline content (aluminum and/or zirconium oxides) have presented better clinical
results than feldspar-, leucite-, and lithium disilicate-based ceramics (Scotti et al
1995, Oden et al 1998, Hayashi et al 2000, Fradeani et al 2002). However the
increase of the mechanical strength, by increasing the crystalline content and
decreasing the glass content, results in an acid-resistant ceramic whereby any type of
acid conditioning produces insufficient surface changes for adequate bonding to
resin. (Awliya et al., 2000, Derand et al 2000, Madani et al 2000, Ozcan et al 2001,
Della Bona et al 2002, Özcan et al 2003).
Thus, even though the etching with hydrofluoric acid combined with the
silanization is the principal conditioning method of feldspar-, leucite- and lithium
disilicate-based ceramics (silica-based ceramic) (Della Bona et al 2000, Debnath et al
2003, Borges et al 2003, Özcan et al 2003, Della Bona 2004, Melo et al 2005). This
conditioning method does not allow high bond strength to acid-resistant ceramics
(Awliya et al 2000, Derand et al 2000, Madani et al 2000, Ozcan et al 2001, Della
Bona et al 2002). Currently, the tribochemical silica coating method appears to be the
choice conditioning for the acid-resistant ceramic. (Kern et al 1995, Awliya et al
1998, Özcan et al, 2001, Özcan et al 2003, Bottino et al 2005, Valandro et al 2005,
Valandro et al 2005, Amaral et al 2005). Due to the high-speed surface impact of the
alumina particles modified by silica, there is an embedding of these particles on the
ceramic surface (Sun et al 2000). Consequently, there is a chemical bond between the
silica coated ceramic surface and the silane agent (y-
methacryloxypropyltrimethoxysilane), and the latter to the resin material.

100
Furthermore these tribological concepts, the resin cements with MDP
monomers (10-methacryloyloxydecyl-dihydrogen-phosphate) have allowed high
bond strength to acid-resistant ceramics, as well as high bonding durability, due to
the bond between the phosphate monomers and the aluminum/zirconium oxides of
the dental ceramic (Kern et al 1998, Wegner et al 2000, Özcan et al 2001, Friederich
et al 2002, Wegner et al 2002, Blatz et al 2003 Özcan et al 2003, Blatz et al 2004,
Hummel et al 2004, Leite et al 2005).
Bond strength- (Ozturk et al 2003) and microleakage-tests (Jacques et al
2003) can be used to evaluate the bonding between the dental substrate and the
ceramic. However, mechanical fatigue tests conducted in a humid environment seem
to be the best in vitro method to predict the clinical performance of dental materials
and restorative techniques. Fatigue is a type of test that may lead to the fracture of a
structure after repeated loading, and may be explained by the spread of microscopic
cracks from areas of force concentration, usually in areas containing macroscopic or
molecular structural defects (Pontius et al 2002, Scotti et al 2002, Wiskott et al
1995). Pontius (Pontius et al 2002) described that 1,200,000 cycles in a mechanical
fatigue test correspond to approximately 5 years of clinical function.
Thus, the purpose of this study was to evaluate the fatigue resistance of the
bonding between human dentin and glass-infiltrated aluminum-based ceramic, using
different luting materials. The hypothesis was that the fatigue resistance can be
modified depending on used luting procedures.
MATERIAL AND METHODS
Selection and preparation of teeth
Forty extracted, caries-free human third molars were used. The teeth were
collected in the Dept. of Oral Science (University of Bologna), after obtaining the
patient’s informed consent. After the extraction, the teeth were immediately
immersed in 0.02%-thimol/24h and stored in distilled water. Part of the crown
was removed, exposing a flat dentin surface of approximately 3mm x 4mm,
which was polished on wet #320, 600, 1000-grit silicon carbide (SiC) paper,
respectively, for 60s to standardize the smear layer.

101
After preparation, each specimen was embedded in a PVC cylinder
(height: 20mm, diameter: 10mm) filled with chemically cured epoxy resin
(Epoxy Resin 285, Schaller, Florence, Italy), remaining exposed only the dentin
surface for luting.
Preparation of alumina ceramic samples
Forty ceramic blocks of a glass-infiltrated alumina ceramic (In-Ceram Alumina
for Cerec 2) (VITA Zahnfabrik, Bad Säckingen, Germany) were fabricated
according to the manufacturer's specifications. These blocks were 3mm x 3mm x
4mm in dimension and the bonding surfaces (3mm x 3mm) of each block were
polished using a 600- to 1200-grit metallographic (3M, St. Paul, USA) in a
polishing machine. The surfaces of all the ceramic blocks were submitted to the
chairside airborne abrasion with 110µm aluminum oxide particles (Al2O3),
following this blasting protocol: a = perpendicular to the surface; b = 10-mm
distance; c = 20-second time; d = 2.8-bar pressure.
Luting procedures
The materials used in this study and the luting technical procedures are described
in Table 1. Four luting protocols were tested following the manufacturer’s
recommendations (luting system [LS] / ceramic surface conditioning [CSC]). The
tooth- and ceramic- sp were randomly divided in four groups (n=10):
GROUP 1: [LS] RelyX Unicem / [CSC] Al2O3;
GROUP 2: [LS] One-Step + Duo-Link / [CSC] Al2O3 + etching with 4%
hydrofluoric acid (Porcelain Etchant) + silane coupling agent (Porcelain Primer).
GROUP 3: [LS] Panavia F / [CSC] Al2O3.
GROUP 4: [LS] Scotchbond 1 + RelyX ARC (3M-Espe) / [CSC] Al2O3 + chairside
airborne abrasion with siliceous acid modified by 30µm Al2O3 particles (Si2Ox)
(blasting procedures: identical to the airborne abrasion with Al2O3) + silane
coupling agent (Tribochemical silica coating) (CoJet System);
102
After the ceramic conditioning and application of the adhesive systems
(excepted in G1), the luting cements were manipulated as recommended by the
manufacturers and applied on the bonding surface of each ceramic block, which
was than cemented to dentin surface. The set-up remained under the constant load
of 750g for 10min and during this period the cement excesses were removed. The
specimens (sp) were stored in distilled water to 37oC for 24 h and then were
submitted to the fatigue test.
Mechanical fatigue test in shear (Figure 2 and 3)
Initially, all sp were grasped in an apparatus, which allows the dentin surface to
be almost perpendicular to the fatigue test. A metallic cylinder were then
positioned on the ceramic surface (perpendicular to dentin surface) and the sp
were subjected to 1 million fatigues cycling shear with sinusoidal load ranging
from 0 to 21N at 8Hz frequency and 37°C water irrigation.
Fatigue resistance scores and statistical analysis
After the fatigue test, it was given a classification (score) for fractured and no-
fractured sp based on the number of the mechanical cycle:
Score 0: samples fractured before cycling.
Score 1: samples fractured between 0 and 199,999 cycles.
Score 2: samples fractured between 200,000 and 399,999 cycles.
Score 3: samples fractured between 400,000 and 599,999 cycles.
Score 4: samples fractured between 600,000 and 799,999 cycles.
Score 5: samples fractured between 800,000 and 999,999 cycles.
Score 6: samples non-fractured up to 1 million cycles.
The collected data were submitted to statistical analysis (Kruskal-
Wallis test and post hoc Tukey test), using a level of significance of 5%.

103
Analysis of the failure modes
The fractured sp during the fatigue test were analyzed in a Scanning Electron
Microscopy (magnification from x200 to x1000) (JEOL–JSM–5400, Jeol Ltd,
Tokyo, Japan) in order to evaluate the sp failure mode, which were classified in
seven types: Type 1) fracture of the luting cement (cohesive); Type 2) fracture of
the dentin (cohesive); Type 3) cohesive fracture of the ceramic (cohesive); Type
4) failure between dentin and adhesive system (adhesive failure); Type 5) failure
between luting cement and ceramic (adhesive failure); Type 6) mixed failure
(type 1 + type 4); Type 7) mixed failure (type 1 + type 5); Type 8) mixed failure
(type 4 + adhesive failure between resin cement and bonding agent). All
micrographics were analyzed by three calibrated observers.
RESULTS
The Kruskal-Wallis nonparametric analysis of the fatigue resistance scores are
shown in Table 2, in which it was possible to note that there were differences
among the studied groups.
The mean score values and standard deviations of the groups are
shown in Table 3, noting that G3 (Score = 5.9 [1 failure]) and G4 (Score = 6
[none failure]) were statistically similar (P=0.33) and had significantly the
highest fatigue resistance, when compared to G1 (Score = 3.9 [5 failures]) and G2
(Score = 3.7 [6 failures]) (P<.03).
In the fractured sp microscopic analyses it was observed that: (1) G1 –
5 fractures type 4 (Figure 4); (2) G2 – 6 fractures type 5 (Figure 5); G3 – 1
fracture type 8 (Figure 6).
DISCUSSION
The hypothesis of this study was confirmed, since the fatigue resistance was
different depending on the protocol used to lute the glass infiltrated alumina

104
ceramic to the dentin. The highest fatigue resistances were obtained whether by
the combination of self-etching primer with MDP-based resin cement (G3) or the
combination of total etching/single bottle with resin cement/tribochemical silica
coating (G4).
The results for G3 may be explained by the combination of the
chemical bonds between the MDP phosphate monomers and the aluminum oxides
(Wegner et al 2000, Özcan et al 2001, Blatz et al., 2003, Hummel et al 2004,
Leite et al 2005), and the dentin treated with self-etching primer. (Uno et al 2000,
Varela et al 2003) For G4, the results may be explicated by the chemical bond
among silica coated ceramic surface, silane agent and the resin material, (Kern et
al 1995), combined with the adequate bonding of the adhesive system to the
dentin (Abu-Hanna et al 2004, Helvatjoglu-Antoniades et al 2004, Reis et al
2004).
The performance of resin cements that contain MDP phosphate
monomers (10-methacryloyloxydecyl-dihydrogen-phosphate) (G3) have been
observed by various studies, which noted a high bonding durability of this cement
to acid-resistant ceramics, such as glass-infiltrated alumina/zirconium ceramic
(Kern et al 1995, Ozcan et al 2001), yttrium-oxide-partially-stabilized zirconia
ceramic (Kern et al 1998, Wegner et al 2000, Wegner et al 2002, Blatz et al
2004), densely-sintered alumina ceramic (Friederich et al 2002, Blatz et al. 2003,
Hummel et al 2004).
Despite the resin cement of G3 was bonded to the acid-resistant
ceramic, one sp showed a failure type 8, since the fracture occurred in two zones:
partial fracture between dentin and adhesive system, and partial fracture between
the adhesive system and resin cement (Panavia). Even though this fracture has not
been statistically significant, since G3 (1 fracture) was statistically similar to G4
(none fracture), it maybe explained due to the features of the dentin adhesive
system and the resin cement employed in G3. The employed self-etching primer
adhesive system exhibited a low pH value, producing a chemical match with the
polymerization chemical process of the dual-cure resin cement. Some studies
have indicated a possible chemical incompatibility between adhesive systems

105
with low pH and resinous materials of chemical- and dual-polymerization.
(Sanares et al 2001, Cheong et al 2003, Suh et al 2003, Tay et al 2003, Tay et al
2003). A correlation was observed between the decline in microtensile bond
strengths of chemical-cured composites coupled to bonded dentin and the acidity
of these adhesives. (Sanares et al 2001) Since single-step self etch adhesives
contain a higher concentration of acidic resin monomers, the coupling of
chemical/dual-cured composites to the hydrated dentin bonded with these
adhesives were also found to be inferior to those achieved by using light-cured
composites. It is known that acidic resin monomers retard the polymerization of
chemical/dual-cured composites that are initiated via peroxide-amine type binary
redox catalysts. Interaction between acidic adhesive resin monomers and the
basic composite tertiary amines results in the consumption of the latter in acid-
base reactions, depriving their capacity of generating free radicals in subsequent
redox reactions. (Suh et al 2003, Tay et al 2003).
In this current study, it was observed that none of the G4 specimens
fractured during the fatigue test, meaning that the two interfaces (resin cement–
ceramic; dentin-adhesive system) supported the fatigue. The high bond-strength
and -durability promoted by tribochemical silica coating combined with resin
cement has also been stated by studies. (Kern et al 1995, Awliya et al 1998,
Özcan et al 2001, Özcan et al 2003, Bottino et al 2005, Valandro et al 2005,
Valandro et al 2005). The fatigue resistance of the interface cement-ceramic can
be explained by the following phenomena: the airborne particle abrasion allows
the ceramic surface to be embedded by silica oxide coated aluminum particle
(Sun et al 2000) forming the silica-modified surface chemically more reactive to
the resin via silane coupling agents. Silane molecules react with water to form
three silanol groups (–Si–OH) from the corresponding methoxy groups (–Si–O–
CH3). (Plueddemann 1970, Ozcan et al 2003, Ozcan et al 2004) The silanol
groups then react further to form a siloxane (–Si–O–Si–O–) network with the
silica surface. Monomeric ends of the silane molecules react with the
methacrylate groups of the adhesive resins in a free radical polymerization
process. (Plueddemann 1970, Jedynakiewicz et al 2001, Ozcan et al 2003, Ozcan
et al 2004). Summarizing, the employed tribochemically assisted system

106
(chairside system) allows a chemical bond among the coated silica, silane
coupling agent and resin cement. Regarding the fatigue resistance of the interface
dentin-adhesive system, some studies stated that the adhesive system used in this
group (G4) present high dentin bond strength (Abu-Hanna et al 2004,
Helvatjoglu-Antoniades et al 2004, Reis et al 2004), due to the hybridization of
dentin (Koshiro et al 2004), as well as the compatibility between the bonding
agent and the resin cement (Sanares et al 2001), which justified the resistance to
the fatigue.
Analyzing the micrographics of the 5 fractured sp of G1 (Figure 4), it
was noted that the failure occurred in the interface dentin – resin cement (type 4).
In this micrographic, the dentin surface coated by the smear layer can also be
observed. This smear layer was not removed because the dentin is not etched and
any bonding agent was applied as recommended by the manufacturer. Thus the
hybrid layer is not formed and the bonding between the cement and the dentin did
not support the mechanical fatigue, explaining the type of fracture.
In G2, 6 fractures type 5 were observed (failures between the resin
cement and ceramic surface). The ceramic surface conditioning (4% hydrofluoric
acid + silane coupling agent) recommended for this luting protocol justified the
noted fracture pattern. Currently, it is stated that the hydrofluoric acid does not
present ability to attack the compact ceramic surface with high alumina content
and low vitreous phase (acid-resistant ceramic), such as the ceramic employed in
the current study (glass-infiltrated alumina ceramic) (Awliya et al 1998, Derand
et al 2000, Madani et al 2000, Ozcan et al 2001, Della Bona et al 2002 Borges et
al 2003, Özcan et al 2003). This glass infiltrated high-alumina core ceramic is
composed of approximately 80w% of crystalline phase (aluminum oxide) and
20w% of glassy phase (aluminum-silicate-lanthanum) (Tinschert et al 2000,
Guazzato et al 2004). Hence, due to the low silica content in this ceramic, the
application of the silane agent also does not contribute to bonding, because the
MPS-based silane agent presents a great chemical bond to silica oxides and a
weak bond to aluminum oxides, which is the basis ingredient of alumina ceramic
(Plueddemann 1970, Kern et al 1994, Ozcan et al 2003, Ozcan et al 2004).
Exactly as stated by Valandro (Valandro et al 2005) the ceramics can be

107
classified into groups depending on how the surface is attacked by the
hydrofluoric acid (HF). Acid-sensitive ceramics are promptly etched by HF
resulting in micro-mechanical retentive ceramic surfaces (e.g.: feldspar-, leucite-
and lithium disilicate-based ceramics) (Della Bona et al 2000, Debnath et al 2003,
Borges et al 2003, Özcan et al 2003, Della Bona et al 2004, Melo et al 2005).
Acid-resistant ceramics do not suffer much surface degradation by HF etching,
preventing a reliable micro-mechanical bond to resin (e.g.: glass-infiltrated
alumina and zirconia ceramic systems, densely-sintered alumina ceramics, and
yttrium-oxide-partially-stabilized zirconia ceramics) (Ozcan et al 2003, Bottino et
al 2005, Valandro et al 2005, Amaral et al 2005).
However, considering the micrographics of the fractured sp of G2, it
can be noted that the interface dentin – adhesive system resisted to the fatigue
test. Thus, the bonding of the G2 adhesive system to the dentin maybe considered
safe, in light of the parameters followed in this study. Some studies have shown
that One Step adhesive system presents high bond strength to the dentin (Cheong
et al 2003, Abdalla et al 2004).
Taking into account the results obtained in G2, in which the bonding to
the dentin was stable and the bonding to the ceramic did not resist to mechanical
fatigue, the clinicians should reflect on the choice of the adhesive system to bond
the dentin and the ceramic surface. For example, if the manufacturer’s
instructions regarding the ceramic surface conditioning were not followed,
namely if the surface ceramic had been conditioned with a tribochemical silica
coating method, in view of the current concepts of adhesion to acid-resistant
ceramic, theoretically the fractured observed fracture in the interface resin cement
– ceramic could not have occurred. The clinicians should attentively observe
some aspects during the luting of all-ceramic restorations. Even though the
manufacturer’s instructions should obviously be considered, a global view
regarding the current concepts to treat the dental hard tissues, as well as the
conditioning of the ceramic surface must be considered in order to optimize the
global performance of the bonded ceramic restorations.

108
Surely, other factors such as the case preview must be planned, the
characteristics of the prosthetic preparations and generally the conditions for the
cementation can affect the global performance, and therefore further clinical
evaluation studies are necessary to state the effect of the change of luting
protocols or the mixing of different protocols. The combination of dentin
adhesive systems with MDP-based resin cement or resin cement/tribochemical
silica coating were the best luting protocols for aluminous ceramic. The
cementation strategies of glass-infiltrated alumina ceramic recommended by the
manufacturers maybe eventually changed in order to optimize the bond to all the
substrate.
Abdalla AI. Microtensile and tensile bond strength of single-bottle adhesives: a
new test method J Oral Rehab 2004;31:379-84.
Abu-Hanna A, Gordan VV. Evaluation of etching time on dentin bond strength
using single bottle bonding systems J Adhes Dent 2004;6:105-10.
Amaral R, Leite FPP, Bottino MA, Valandro LF, Özcan M. Microtensile bond
strength of a resin cement to glass infiltrated zirconia-reinforced ceramic: the effect
of surface conditioning. Dent Mater 2005. (forthcoming)
Awliya W, Odén A, Yaman P, Dennison JB, Razzoog ME. Shear bond strength
of a resin cement to densely sintered high-purity alumina with various surface
conditions. Acta Odontol Scand 1998;56:9-13.
Blatz MB, Sadan A, Arch GH, Lang BR. In vitro evaluation of long-term
bonding of Procera AllCeram alumina restorations with a modified resin luting agent.
J Prosthet Dent 2003;89:381-387.
Blatz MB, Sadan A, Martin J, Lang BR. In vitro evaluation of shear bond
strengths of resin to densely-sintered high purity zirconium-oxide ceramic after long-
term storage and thermal. J Prosthet Dent 2004;91:356-362.
Borges GA, Sophr AM, Goes MF, Correr Sobrinho L, Chan DCN. Effect of
etching and airborne particle abrasion on the microstructure of different dental
ceramics. J Prosthet Dent 2003;89:479-488.
Bottino MA, Valandro LF, Scotti R, Buso L. Effect of surface treatments on the

109
resin bond to zirconium-based ceramic. Int J Prosthodont 2005;18:60-65.
Cheong C, King NM, Pashley DH, Ferrari M, Toledano M, Tay FR.
Incompatibility of self-etch adhesives with chemical/dual-cured composites: two-step
vs one-step systems. Oper Dent 2003;28:747-755.
Consani S, Santos JG, Correr Sobrinho L, Sinhoreti MA, Sousa-Neto MD. Effect
of cement types on the tensile strength of metallic crowns submitted to
thermocycling. Braz Dent J 2003;14(3):193-196.
Degrange M, Roulet JF. Minimally invasive restorations with bonding.
Germany: Quintessence, 1997.
Della Bona A, Anusavice KJ. Microstructure, composition, and etching
topography of dental ceramics. Int J Prosthodont 2002;15:159-167.
Dérand P, Dérand T. Bond strength of luting cements to zirconium oxide
ceramics. Int J Prosthodont 2000;13:131-135.
Dérand P, Dérand T. Bond strength of luting cements to zirconium oxide
ceramics. Int J Prosthodont 2000;13:131-135.
Fradeani M, Redemagni M. An 11-year clinical evaluation of leucite-reinforced
glass-ceramic crowns: a retrospective study. Quintessence Int. 2002;33:503-510.
Friederich R, Kern M. Resin bond strength to densely sintered alumina ceramic.
Int J Prosthodont 2002;15:333-338.
Gemalmaz D. Use of heat-pressed, leucite-reinforced ceramic on anterior and
posterior onlays: a clinical report. J Prosthet Dent 2002;87(2):133-135.
Guazzato M, Albakry M, Ringer SP, Swain MV. Strength, fracture toughness
and microstructure of a selection of all-ceramic materials. Part I. Pressable and
alumina glass-infiltrated ceramics. Dent Mater 2004;20:441-448.
Hayashi M, Tsuchitani Y, Kawamura Y, Miura M, Takeshige F, Ebisu S. Eight-
year clinical evaluation of fired ceramic inlays. Oper Dent. 2000;25:473-481.
Helvatjoglu-Antoniades M, Koliniotou-Kubia E, Dionyssopoulos P. The effect
of thermal cycling on the bovine dentine shear bond strength of current adhesive
systems. J Oral Rehab 2004;31:911-917.
Hummel M, Kern M. Durability of the resin bond strength to the alumina
ceramic Procera. Dent Mater 2004;20:498-508.
Jacques LB, Ferrari M, Cardoso PE. Microleakeage and resin cement film

110
thickness of luted all-ceramic and gold electroformed porcelain-fused-to-metal
crowns. J Adhes Dent 2003;5:145-152.
Jedynakiewicz NM, Martin N. The effect of surface coating on the bond strength
of machinable ceramics. Biomaterials 2001;22:749-52.
Kern M, Thompson VP. Bonding to glass infiltrated alumina ceramic: adhesive
methods and their durability. J Prosthet Dent 1995;73:240-249.
Kern M, Thompson VP. Bonding to glass infiltrated alumina ceramic: adhesive
methods and their durability. J Prosthet Dent 1995;73:240-249.
Kern M, Thompson VP. ESCA surface characterization of the alumina ceramic
In-Ceram after various conditioning methods for resin bonding. J Dent Res
1994;73(sp iss):197. (Abstract #763)
Kern M, Wegner SM. Bonding to zirconia ceramic: adhesion methods and their
durability. Dent Mater 1998;14:64-71.
Koshiro K, Inoue S, Tanaka T, Koase K, Fujita M, Hashimoto M, Sano H. In
vivo degradation of resin–dentin bonds produced by a self-etch vs. a total-etch
adhesive system. Eur J Oral Sci 2004; 112: 368-375.
Kramer N, Lohbauer U, Frankenberger R. Adhesive luting of indirect
restorations. Am J Dent 2000;13:60D-76D.
Leite FPP, Valandro LF, Guidini A, Bottino MA, Kimpara ET. Evaluation of the
tensile bond strength between an aluminous ceramic and two resin cements. Braz
Dent Sci 2005. (forthcoming)
Lopes GC, Baratieri CM, Baratieri LN, Monteiro S Jr, Cardoso Vieira LC.
Bonding to cervical sclerotic dentin: effect of acid etching time. J Adhes Dent
2004;6:19-23.
Madani M, Chu FCS, McDonald AV, Smales RJ. Effects of surface treatments
on shear bond strengths between a resin cement and an alumina core. J Prosthet Dent
2000;83:644-647.
Melo RM, Valandro LF, Leite F, Bottino MA. Bonding to a leucite reinforced
feldspar ceramic. Braz Dent J 2005. (in press)
Nakabayashi N, Pashley DH. Hybridization of dental hard tissues. Tokyo:
Quintessence, 2000.
Odén A, Andersson M, Krystek-Ondracek I, Magnusson D. Five-year clinical

111
evaluation of Procera AllCeram crowns. J Prosthet Dent 1998;80:450-456.
Özcan M, Akkaya A. New approach to bonding all-ceramic adhesive fixed
partial dentures: A clinical report. J Prosthet Dent 2002;88: 252-254.
Özcan M, Alkumru H, Gemalmaz D. The effect of surface treatment on the shear
bond strength of luting cement to a glass-infiltrated alumina ceramic. Int J
Prosthodont 2001;14:335-339
Özcan M, Matinlinna JP, Vallittu PK, Huysmans MC. Effect of drying time of 3-
methacryloxypropyltrimethoxysilane on the shear bond strength of a composite resin
to silica-coated base/noble alloys. Dent Mater 2004;20:586-590.
Özcan M, Vallittu PK. Effect of surface conditioning methods on the bond
strength of luting cement to ceramics. Dent Mater 2003;19:725-731.
Özcan M. Evaluation of alternative intra-oral repair techniques for fractured
ceramic-fused-to-metal restorations. J Oral Rehab 2003; 30:194-203.
Özcan M. The use of chairside silica coating for different dental applications: A
clinical report J Prosthet Dent 2002;87:469-472.
Özok AR, Wu M-K, Gee AJ, Wesselink PR. Effect of dentin perfusion on the
sealing ability and microtensile bond strengths of a total-etch versus an all-in-one
adhesive. Dent Mater 2004; 20, 479-486.
Ozturk N, Aykent F. Dentin bond strengths of two ceramic inlay systems after
cementation with three different techniques and one bonding system. J Prosthet Dent
2003;89:275-281.
Plueddemann EP. Adhesion through silane coupling agents. J Adhesion
1970;2:184-201.
Pontius O, Hutter JW. Survival rate and fracture strength of incisors restored
with different post and core systems and endodontically treated incisors without
coronoradicular reinforcement. J Endod 2002;28:710-715.
Reis A, Loguercio AD, Carvalho RM, Grande RHM. Durability of resin dentin
interfaces: effects of surface moisture and adhesive solvent component. Dent Mater
2004; 20:669-676.
Sanares AME, Itthagarun A, King NM, Tay FR, Pashley DH. Adverse surface
interactions between one-bottle light-cured adhesives and chemical-cured
composites. Dent Mater 2001;17:542-556.
112
Scotti R, Catapano S, D’Elia A. A clinical evaluation of In-Ceram crowns. Int J
Prosthodont 1995;8:320-323.
Scotti R, Ferrari M. Proprietà mechaniche e valutazione in vitro. In: Perni in
fibra: Presupposti teorici ed applicazioni cliniche. Milan: Masson 2002;39-51.
Suh BI, Feng L, Pashley DH, Tay FR. Factors contributing to the incompatibility
between simplified-step adhesives and chemically-cured or dual-cured composites.
Part III. Effect of acidic resin monomers. J Adhes Dent 2003;5:267-282.
Sun R, Suansuwan N, Kilpatrick N, Swain M. Characterization of
tribochemically assisted bonding of composite resin to porcelain and metal. J Dent
2000;28: 441-445.
Tay FR, Pashley DH, Yiu CK, Sanares AM, Wei SH. Factors contributing to the
incompatibility between simplified-step adhesives and chemically-cured or dual-
cured composites. Part I. Single-step self-etching adhesive. J Adhes Dent 2003;5:27-
40.
Tay FR, Pashley DH. Resin bonding to cervical sclerotic dentin: a review. J Dent
2004;32:173-196.
Tay FR, Suh BI, Pashley DH, Prati C, Chuang SF, Li F. Factors contributing to
the incompatibility between simplified-step adhesives and self-cured or dual-cured
composites. Part II. Single-bottle, total-etch adhesive. J Adhes Dent 2003;5:91-105.
Tinschert J, Zwez D, Marx R, Anusavice KJ. Structural reliability of alumina-,
feldspar-, leucite-, mica- and zirconia-based ceramics J Dent 2000;28:529-535.
Uno S, Tanaka T, Kawamoto C, Konishi J, Sano H Microtensile bond strength to
dentin and cavity adaptation of Cerec 2 inlay restoration Am J Dent 2000;13:59.
Valandro LF, Della Bona A, Bottino MA, Neisser MP. Bonding to densely
sintered alumina ceramic: The effect of ceramic surface treatment. J Prosthet Dent
2005;93:…-…..
Valandro LF, Leite FPP, Scotti R, Bottino MA, Neisser MP. Effect of ceramic
surface treatment on the microtensile bond strength between a resin cement and an
alumina-based ceramic. J Adhes Dent 2004; 6(4):327-332.
Varela SG, Rábade LB, Lombardero PR, Sixto JML, Bahillo JDG, Park SA. In
vitro of endodontic post cementation protocols that use resin cements. J Prosthet
Dent 2003;89:146-153.

113
Wegner SM, Gerdes W, Kern M. Effect of different artificial aging conditions
on ceramic-composite bond strength. Int J Prosthodont 2002;15:267-272.
Wegner SM, Kern M. Long-term resin bond strength to zirconia ceramic. J
Adhesive Dent 2000;2:139-147.
Wiskott HWA, Nicholls JL, Belser UC. Stress fatigue: Basic principles and
prosthodontic implications. Int J Prosthodont 1995;8:105-116.
.

114
Chapter 10 Other clinical application of FRC
Clinical evaluation of teeth restored with quartz fiber-reinforced epoxy resin posts.

115
Both researchers and manufacturers have introduced several post-and-core
restorations with the aim of providing reliable systems for reconstruction of
endodontically treated teeth. In spite of these efforts, it is still difficult to predict the
clinical survival times of treated teeth restored with posts and cores (Goodacre et al
1994).
The prognosis is related to several factors, including the type of material used for the
post and core; the shape, dimensions, and length of the post; and the kind of cement
used. The major disadvantage associated with conventional cast-metal posts is
vertical root fracture. Having high rigidity, metal posts appear to vibrate at high
frequencies when loaded with lateral forces. The focusing of these forces in
unpredictable “critical points” may determine longitudinal fractures of the root or
metal corrosion and consequently lead to loss of the tooth (Trabert et al 1984,
Morgano et al 1993, Duret et al 1990).
In 1990, Duret (Duret et al 1990) proposed carbon-fiber posts, among the many
prefabricated fiber post-and-core systems, to reduce the failure rate. These relatively
recent posts are made of equally aligned carbon fibers attached to an epoxy resin
matrix and present an interesting property, anisotropic behaviour. In other words, the
material has different physical responses when loaded in different directions. This
characteristic is of clinical relevance, as it may strongly reduce the possibility of root
fracture and decementation (Morgano et al 1993).
The objective is to create a “cement-post-core” system with homogeneous properties
and physical characteristics similar to tooth tissues. To fulfill esthetic requirements,
quartz- and glass-fiber posts embedded in a filled resin matrix have been developed.
According to the manufacturer, the mechanical properties of these posts are similar to
those of carbon posts and provide an additional esthetic benefit. Fiber posts appear to
be biocompatible, are easy to insert, and are time and cost effective. Moreover, there
is no need for temporary fillings, since the post is placed using a one-stage technique.
The system is conservative with regard to the remaining dental structure and offers
the possibility of orthograde retreatment in cases of endodontic failure (de Rijk
2000). Several in vitro studies have been conducted on carbon- fiber posts, although
only a few investigations have been carried out on the esthetic quartz-fiber post
system. Relatively few reports have evaluated the in vivo effectiveness of carbon-
and quartz-fiber posts.

116
A 6-year clinical study using carbon-fiber posts (Composiposts) (Dallari et al 1996)
reported two failures in 575 restorations. A retrospective study (Fredrikson et al
1998) reported that the Composipost system performs favorably after 2 to 3 years. In
fact, only 2% of treated teeth had to be extracted, and none of these failures were
attributable to the fiber post system. Others (Ferrari et al 2000) evidenced a 3.2%
failure rate among 1,304 treated teeth restored with carbon- and quartzfiber posts in a
6-year study. Neither of these studies reported root fractures. The purpose of the
present prospective clinical follow-up was to evaluate the survival rate of 180
endodontically treated teeth restored using quartz-fiber posts and composite resin
material, and finalized with metal-ceramic or all-ceramic crowns over a 30- month
period.
Materials and Methods
One hundred eighty endodontically treated teeth in 132 patients (aged 18 to 65 years)
were restored by 13 different operators (Table 1). Restored teeth had the following
characteristics: need for prosthetic crown, root canal therapy performed at least 3
months previously with no subjective or objective symptoms, and no lesions visible
upon radiography. Radiographs were taken with the long-cone technique when the
restoration was performed and were examined with approximately 5_ magnification.
Teeth were restored with Æstheti-Plus quartz-fiber posts (RDT) (Figs 1 and 2). This
post system is composed of equally aligned quartz fibers that are longitudinally
embedded in an epoxy resin matrix. Posts are available in three sizes, have a
cylindric, double-section shape, and are 22 mm long. Post 1 has a diameter of 1.4
mm in the wider cylindric section and 1.0 mm at the narrow end, post 2 has a
diameter of 1.8 mm at the large end and 1.2 mm at the narrow portion, and post 3 has
diameters of 2.1 mm and 1.4 mm, respectively. This special shape is apparently
better adapted to the prepared canal. The choice of three different diameters provided
the possibility to find the adequate post dimension following the criteria of maximum
conservation of the residual dental tissue. In accordance with previous studies
(Fredrikson et al 1998 Chalifoux 1998) the following parameters were considered
relevant: number of canals; remaining tooth tissue, defined as complete (C; 66% to
100% of the tooth), partial (P; 33% to 65% of the tooth), or absent (A; 0% to 32% of
117
the tooth), shape of the canal space; and tooth antagonist. Among the 180 treated
teeth, 69% percent presented one root canal, and 31% percent had two or three
canals. In 14 maxillary premolars and 11 molars (four maxillary and seven
mandibular ones), the restorations were done with the anchorage of two posts per
tooth. Thus, among the 180 teeth restored, 205 canals were treated, and the same
number of posts was used. Seventy-nine percent of the canals treated showed a round
shape (R), 19% an oval one (O), and 2% a semicircular shape defined as C. Of the
opposing occluding teeth, 53% were natural teeth, 19% had metal-ceramic crowns,
16% were dentures, 11% occluded with metal-resin crowns, and 1% were not in
occlusion.
Clinical Procedures
Prior to cavity preparation, a rubber dam was placed, and provisional restorations
were removed with 80- µm diamond burs (205, Intensiv) in a medium-speed
handpiece under water cooling. Following direct clinical observation and
radiographic examination, the operator selected the most suitably sized fiber post.
Root preparation was done with a Pre-forma Drill and a Forma Drill in a slow-speed
handpiece with water spray. These calibrated burs provided a uniform preparation
and a thin and equally distributed layer of resin surrounding the post after its
cementation. The post was then reduced to the proper length using an 80-µm
diamond bur (206, Intensiv) in a highspeed handpiece with water spray; the bur was
kept perpendicular to the long axis of the post to avoid damaging the fiber structure
and its mechanical characteristics.
The length of the post was at least equal to the length of the clinical crown, always
respecting the apical gutta percha seal of 4 mm. The root canal was treated with 32%
phosphoric acid (Bisco) for 15 seconds, rinsed with deionized water, and gently dried
with air and a paper cone to verify that no traces of acid remained in the root
preparation.
Equally mixed primers A and B (Bisco) were applied with a Superfine Microbrush
(Microbrush) in the canal and on the post surface and then gently dried to permit the
evaporation of the acetone. Pre-Bond (Bisco) was applied inside the canal with a
paper cone. Next, the two components of the self-curing C&B Resin Cement (Bisco)

118
were mixed and applied at the edge of the root and on the post, which was
immediately placed into the prepared canal. The excess cement was trimmed and
given an adequate setting time (Fig 3). Core buildup was then performed using Core-
Flo (Bisco) or Bis-Core (Bisco) self-curing resin composite. Clinical recalls were
performed at 6, 12, 24, and 30 months. At the last recall, all teeth were crowned.
Three dentists evaluated the clinical performance of the restored teeth. The observers
were not blinded. Outcome was considered successful if the post and core were in
situ with no displacement or detachment of the post, no crown or prosthesis
decementation, and no post, core, or root fracture. Subjective symptoms reported by
the patients were considered potential signs of failure.
Results
After a period of 30 months, three failures were recorded; all took place during the
temporary phases during removal of the resin temporary restoration. The first failure,
recorded after 2 weeks in a maxillary left first premolar, was a cohesive fracture at
the edge of the composite resin of the core and did not involve the post structure. The
remaining dental structure was classified as P (33% to 65%), the canal shape was
oval, the post used had a diameter of 1.4 mm (post 1), the length of the post was 8
mm (slightly longer than the clinical crown), and the antagonist was a natural tooth.
After the fracture, the restoration was immediately replaced and the case was
finalized, and the post was still working successfully after 30 months. The second
and the third failures were adhesive fractures involving the cement-post-core
detaching from the dentinal walls of the root canal. The failures involved two canines
(one maxillary and one mandibular). Both teeth presented a rather low remaining
tooth structure (A; 0% to 32%) and a very large canal diameter, probably because of
excessive preparation during the endodontic therapy. Number 2 posts, which have a
diameter of 1.8 mm in the upper portion, had been used; in spite of this, a thick layer
of cement was around the posts. The lengths of the posts were 11 mm and 9 mm,
respectively. The 9-mm post was somewhat shorter than the clinical crown. Its length
had been imposed by the short root and the necessity to leave an adequate seal of the
apex. The antagonist was a natural tooth in one case and a ceramic crown in the
other. In both cases, the post and core were replaced immediately. The cases were
finalized and were still successful as of this writing. No crown or prosthesis

119
decementations or post, core, or root fractures were recorded. No significant
variations in terms of health of periodontal tissues were observed. No caries were
detected, and no subjective symptoms were reported. The three failures represented
1.7% of all treated teeth, giving a cumulative survival rate of 98.3% in a Kaplan-
Meier survival curve.
Discussion
The implementation of a new, homogeneous post and- core system is a good starting
point for the creation of a reliable substructure for prosthetic rehabilitation. In
combination with resin adhesive systems, resin cements, and composite resins, fiber
posts present biomechanical characteristics similar to those of the dentin. To date, the
favourable clinical outcomes observed encourage more widespread use. In
combination with the resin cement and composite resin restoration, the clinical
performance of the Æstheti-Plus fiber posts was good over a 30-month period. The
causes underlying the three precocious failures of the three restorations were
examined in detail. In the first case, a cohesive fracture, a bubble embedded in the
composite resin was found. The defect may have been due to insufficient
polymerization, possibly because of operator error. In the second and third cases,
adhesive fractures between the cement and the dental tissue were found. These
failures might also have been related to a procedural error by the operators or to the
excess layer of cement around the post, which may have provoked a change in the
mechanical behaviour of the cement-post–composite resin complex. The resin
cements that are supposed to provide the best adhesion (Ross et al 1991, Goldstein et
al 1986) may represent a weak point in the system, mostly when a very thick and non
uniform cement layer surrounds the post. It is reasonable to further detail the
mechanical procedures that the operator may perform during the temporary phases
and relate these to possible failures. It should be underlined that the cases showing
the adhesive failures did not have the 2-mm ferrule of dentin considered to be
important to obtain a high success rate (Assif et al 1991). In accordance with other
clinical studies, the observed success rate of 98.3% was high and no root fractures

120
occurred. Therefore, it was possible to replace the failing restorations (Ferrari et al
2000). Other desirable properties of these posts are their biocompatibility and
resistance to corrosion (Torbjörner et al 1996, Jockisch et al 1992). Fredrikson
(Fredrikson et al 1998) reported no differences in the periodontal conditions between
carbon fiber–treated teeth and controls. Radiographic examination of bone height
measured from the apex to the bone margin mesially and distally showed differences
on the mesial side, but not on the distal surface, between the treated and control teeth.
Other in vitro studies have compared fiber posts with traditional metal posts to
determine which system offers the best mechanical properties. Purton (Purton et al
1996) compared fiber posts and stainless steel root posts by three-point bending tests
to derive the transverse modulus of elasticity of the posts. The carbon-fiber material
was stiffer under transverse loading than stainless steel and thus appears to have
adequate rigidity for its designed purpose. This higher rigidity allows smaller
diameters to be used with equivalent strength, in accordance with the conservative
principles. One weak point of the system is the bond between the post and the
composite core material. The authors therefore suggested that a surface treatment or
modification in configuration should be introduced. Drummod (Drummod 2000)
evaluated the pullout (shear) strength of stainless steel posts and three different fiber
posts and found no significant differences. With respect to flexure strength, all fiber
post systems showed a significant decrease following thermocycling, probably
because of the degradation of the polymer holding the fibers together and/or to the
fibers themselves. The clinical relevance of this data still needs to be investigated.
Relatively few clinical studies examining the success and failure of metallic posts
have been reported. Sorensen (Sorensen et at 1984) reported an 8.6% failure rate
resulting from post dislodgments, root fractures, or post perforations. Others reported
a 6.5% failure rate after 10 years or more (Weine et al 1991) and an 8.3% frequency
of failure after 2 to 3 years (Torbjörner et al 1995). Lewis (Lewis et al 1988) stated
that failures of the post and core are more likely to occur within the first 3 years of
cementation. A retrospective study (Ferrari et al 2000) evaluated the outcome of cast
posts and cores and carbon-fiber posts after 4 years of clinical service. Ninety-five
percent of the teeth restored with fiber posts showed clinical success, 3% were
excluded, and 2% showed endodontic failure. Among the teeth restored with cast
posts, 84% showed clinical success, 9% showed root fracture, 3% showed

121
endodontic failure, 2% had dislodgment of the post or crown, and 2% were excluded.
Statistical evaluation has thus indicated that carbon-fiber posts are superior to
conventional cast posts. In accordance with this study, the failures recorded with
fiber posts were more benign. When a vertical fracture occurs, the entire element
must be extracted. When finalized with all-ceramic crowns, the strong demand for a
post-and-core complex with good esthetic results has guided both researchers and
manufacturers toward the introduction of restoring systems that meet these
requirements. According to a previous study, the clinical behavior of carbon-fiber
posts and quartz-fiber posts is equivalent (Chalifoux 1998). To determine how much
the post aspect will influence light transmission under the thickness of the ceramic,
the following guidelines can be used (Vichi et al 2000). With a 2-mm ceramic
thickness, color differences are clinically irrelevant, while with a ceramic thickness
of 1.5 mm, the color differences are clinically visible in some cases and detectable
only with a spectrophotometer in others. With a ceramic thickness of less than 1.5
mm, the aspect of the post-and-core restoration influences the all-ceramic crown in a
manner that may be clinically unacceptable. The fiber post system offers a time
savings, simple clinical procedures, and reliable results. Moreover, the technique is
less invasive than other post systems because of the shorter length required, and thus
the apical seal can be left around 4 mm (Goerig et al 1983a, Goerig et al 1983b). In
cases of endodontic failures, it is possible to remove the post with the specific bur
(Sakkal 1996). It is obvious that the clinician must follow the manufacturer’s
instructions while treating the remaining dental tissues. The use of a rubber dam is
imperative while performing the restoration. The combination of good mechanical
performance with satisfactory esthetics may be a good starting point toward the
improvement of routine dentistry and toward predicting success. We are awaiting
future evaluations of these encouraging data.
Within a 30-month period, 205 Æstheti-Plus quartz-fiber posts were used to restore
180 teeth with clinical success. The three failures recorded represented 1.7% of
treated teeth. All three failures occurred during the temporary phases. The cohesive
fracture and two adhesive fractures involved only the post-and-core restoration. No
root or post fractures occurred. In the case of failure, it was possible to replace the
restoration without losing the element.
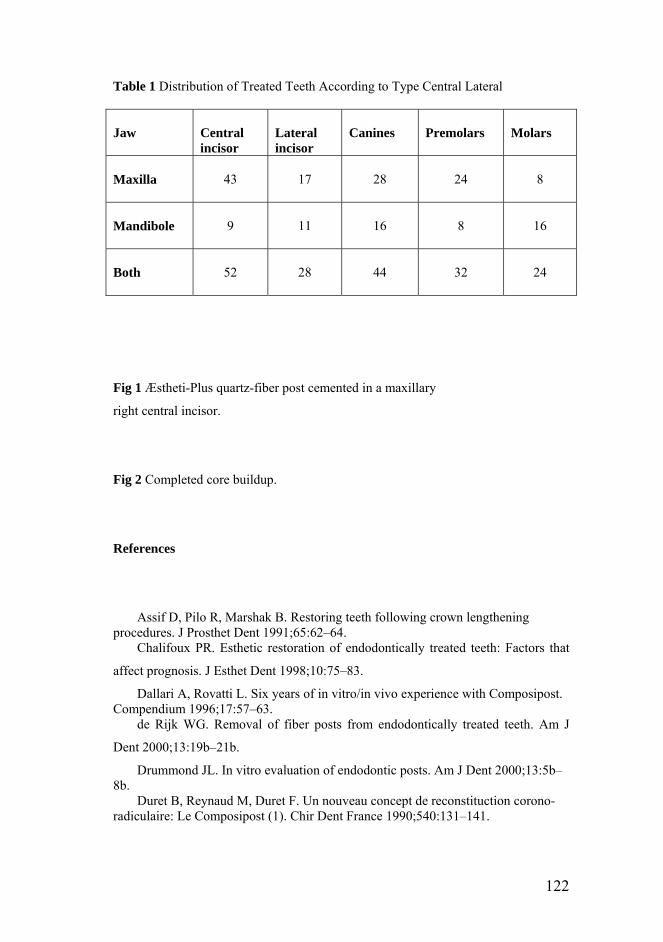
122
Table 1 Distribution of Treated Teeth According to Type Central Lateral Jaw
Central incisor
Lateral incisor
Canines
Premolars
Molars
Maxilla
43
17
28
24
8
Mandibole
9
11
16
8
16
Both
52
28
44
32
24
Fig 1 Æstheti-Plus quartz-fiber post cemented in a maxillary
right central incisor.
Fig 2 Completed core buildup.
References
Assif D, Pilo R, Marshak B. Restoring teeth following crown lengthening procedures. J Prosthet Dent 1991;65:62–64.
Chalifoux PR. Esthetic restoration of endodontically treated teeth: Factors that
affect prognosis. J Esthet Dent 1998;10:75–83.
Dallari A, Rovatti L. Six years of in vitro/in vivo experience with Composipost. Compendium 1996;17:57–63.
de Rijk WG. Removal of fiber posts from endodontically treated teeth. Am J
Dent 2000;13:19b–21b.
Drummond JL. In vitro evaluation of endodontic posts. Am J Dent 2000;13:5b–8b.
Duret B, Reynaud M, Duret F. Un nouveau concept de reconstituction corono-radiculaire: Le Composipost (1). Chir Dent France 1990;540:131–141.

123
Duret B, Reynaud M, Duret F. Un nouveau concept de reconstituction corono-radiculaire: Le Composipost (2). Chir Dent France 1990;542:69–77.
Ferrari M, Vichi A, García-Godoy F. Clinical evaluation of fiberreinforced epoxy resin posts and cast post and cores. Am J Dent 2000;13:15b–18b.
Ferrari M, Vichi A, Mannocci F, Mason PN. Retrospective study of the clinical performance of fiber posts. Am J Dent 2000;13:9b–13b.
Fredrikson M, Astback J, Pameius M, Arvidson K. A retrospective study of 236 patients with teeth restored by carbon fiber reinforced epoxy resin posts. J Prosthet Dent 1998;80:151–157.
Goerig AC, Mueninghoff LA. Management of the endodontically treated tooth.
Part II: Technique. J Prosthet Dent 1983;49:491–497.
Goerig AC, Mueninghoff LA. Management of the endodontically treated tooth.
Part I: Concept for restorative designs. J Prosthet Dent 1983;49:340–345.
Goldstein GR, Hudis SI, Weintraub DE. Comparison of four techniques for the cementation of posts. J Prosthet Dent 1986;55: 209–211.
Goodacre CJ, Spolnik KJ. The prosthodontic management of endodontically
treated teeth: A literature review. Part 1: Success and failure data, treatment concepts.
J Prosthodont 1994;3:243–250.
Jockisch KA, Brown SA, Bauer TW, Merritt K. Biological response to chopped-carbon-fiber-reinforced peek. J Biomed Mater Res 1992;26:133–146.
Lewis R, Smith BG. A clinical survey of failed post retained crowns. Br Dent J 1988;165:95–97.
Morgano SM, Milot P. Clinical success of cast metal posts and cores. J Prosthet Dent 1993;70:11–16.
Purton DG, Payne JA. Comparison of carbon fiber and stainless steel root canal
posts. Quintessence Int 1996;27:93–97.
Ross RS, Nicholls JI, Harrington GW. A comparison of strains generated during placement of five endodontic posts. J Endod 1991; 17:450–456.
Sakkal S. Carbon-fiber post removal technique. Compend Contin Educ Dent Suppl 1996;(20):86S.
Sorensen JA, Martinoff JF. Clinically significant factors in dowel design. J Prosthet Dent 1984;52:28–35.
Torbjörner A, Karlsson S, Ödman PA. Survival rate and failure characteristics for two post designs. J Prosthet Dent 1995;73:439–444.
Torbjörner A, Karlsson S, Syverud M, Hensten-Pettersen A. Carbon fiber reinforced root canal posts. Mechanical and cytotoxic properties. Eur J Oral Sci 1996;104:605–611.
Trabert KC, Cooney JP. The endodontically treated tooth. Restorative concepts and techniques. Dent Clin North Am 1984;28: 293–951.
Vichi A, Ferrari M, Davidson CL. Influence of ceramic and cement thickness on
the masking of various type of opaque posts. J Prosthet Dent 2000;83:412–417.
Weine FS, Wax AH, Wenckus CS. Retrospective study of tapered, smooth post system in place for 10 years or more. J Endod 1991;17: 293–297.

124

125
Chapter 11 summary and conclusions
Until now, clinical application of dental restorations to restore missing posterior teeth
could only be performed using conventional metal systems because of high
mechanical loading in this area. The resin-bonded fixed partial denture (FPD) is a
treatment alternative for replacement of missing teeth when conservation of tooth
structure is needed (Freilich et al 1998). Currently, alternative systems like fibre-
reinforced composite (FRC) dental materials, are recommended for their ability to
withstand these mastication forces. Fibre-reinforced materials combine the basically
different mechanical properties of fibres and a matrix, in which the fibres are
embedded. The fibres demonstrate high tensile strength, a high tensile modulus, and
low shear strength, while the matrix is characterized by high toughness. In an
optimum fibre-reinforced material, the tensile strength of the fibre is combined with
the high toughness of the matrix (Vallittu et al 1999a, Vallittu et al 1999b). Fibre-
reinforced technology is used wherever high stress occurs and low weight is required,
such as in the aeronautical and shipbuilding industries. Numerous attempts have been
made to develop ceramic systems that eliminate metal infrastructures and provide
optimal distribution of reflected light. Currently clinicians have an increasing range
of ceramics capable of delivering high quality aesthetic restorations to choose from
for many clinical indications. New ceramic systems involve reinforced ceramic cores
through dispersion with leucite (Kon et al 1994, Seghi et al 1995, Denry et al 1996,
Mackert et al 1996, Mackert et al 2000), glass infiltration into sintered alumina
(Al2O3) (Probster et al 1994, Sadoun et al 1994), the use of high-purity alumina
(Andersson et al 1993) or zirconium dioxide (zirconia, ZrO2) (Piconi et al 1999).
Conclusions and recommendations
The following conclusions and recommendations may be drawn from our basic and
clinical evaluations on the use of FRC and all ceramic systems applied in partial
restorations:

126
1) Excluding the therapy with dental implants, inlay fixed partial dentures
represent the most conservative treatment for the replacing of the missing
tooth
2) The design of the FRC framework can play important role in supporting the
layering material in a continuous manner. Vestibular and buccal FRC
extensions in the pontic element can increase the bonding area between the
framework and resin composite as well as hold the veneer material better
during occlusal loading.
3) The flexibility of the framework may play an important role in the marginal
adaptation of IFPDs and more rigid materials could transfer the stress to the
margin to a smaller degree than flexible materials
4) The different arrangement of the glass fibers can increase the fracture
strength of FRC three-unit bridges and IFPDs. Increased fracture strength
could be useful in case of long span framework or short clinical abutments
5) fiber reinforced composites exhibit good overall mechanical properties and
the related failure modes are usually more conservative and favorable when
compared to the traditional metal-ceramic three unit bridges.
6) In short observation period the IFPDs in combination with a 3-step adhesive
demonstrated good clinical service but we need more observations in order
to create a sound basis for the final assessment of IFPDs
7) Longer observation periods and comparisons with new reinforced ceramic
materials will help to identify the most suitable choice of material for IFPDs
References
Kon M, Kawano F, Asaoka K, Matsumoto N. Effect of leucite crystals on the strength of glassy porcelain. Dent Mater 1994;13:138–47. Seghi RR, Sorensen JA. Relative flexural strength of six new ceramic materials. Int J Prosthodont 1995;8:239–46. Seghi RR, Denry IL, Rosenstiel SF. Relative fracture toughness and hardness of new dental ceramics. J Prosthet Dent 1995;74:45–50. Denry IL, Mackert Jr. JR, Holloway JA, Rosenstiel SF. Effect of cubic leucite stabilization on the flexural strength of feldspathic dental porcelain. J Dent Res 1996;75:1928–35. Mackert JR, Russell CM. Leucite crystallization during processing of a heat-pressed dental ceramic. Int J Prosthodont 1996;9:261–5.
127
Mackert Jr JR, Williams AL, Ergle JW, Russell CM. Water-enhanced crystallization of leucite in dental porcelain. Dent Mater 2000;16:426–31. Probster L, Diehl J. Slip-casting alumina ceramics for crown and bridge restorations. Quintessence Int 1992;23:25–31. Sadoun M, Asmussen E. Bonding of resin cements to an aluminous ceramic: a new surface treatment. Dent Mater 1994;10:185–9. Andersson M, Oden A. A new all-ceramic crown—a dense-sintered, high purity alumina coping with porcelain. Acta Odontol Scand 1993;51:59–64. Piconi C, Maccauro G. Zirconia as a ceramic biomaterial. Biomaterials 1999;20:1–25. Sadoun M, Asmussen E. Bonding of resin cements to an aluminous ceramic: a new surface treatment. Dent Mater 1994;10:185–9.
Freilich MA, Duncan JP, Meiers JC, Goldberg AJ. Preimpregnated, fiber-reinforced prostheses. Part I: basic rationale and complete coverage and intracoronal fixed partial denture designes. Quintessence Int 1998;29:689-696.
Vallittu PK. Flexural properties of acrylic resin polymers reinforced with
unidirectional and woven glass fibers. J Prosthet Dent 1999a;25:100-105. Vallittu PK. Prosthodontic treatment with a glass fiber-reinforced resin-bonded
fixed partial denture: a clinical report. J Prosthet Dent 1999b;82:132-135.
List of papers part of this thesis Monaco C, Ferrari M, Miceli GP, Scotti R. Clinical Evaluation of Fiber-Reinforced
Composite IFPDs. 2003 Int J Prosthodont 16:319-325.
Monaco C, Miceli GP, Scotti R. Die mit dem neuen, mikrogefüllten Komposit-
Material SR Adoro verblendete Inlay-Brücke. Quintessenz Zahntech 29,3,292-305
(2003).
Malferrari S, Monaco C, Scotti R. Clinical evaluation of teeth restored with quartz
fiber-reinforced epoxy resin posts. 2003 Int J Prosth 16;39-44.
Monaco C, Ferrari M, Caldari M, Baldissara P, Scotti R.
Randomized controlled trial of Fiber-Reinforced Composite Inlay Fixed Partial
Dentures: two-year results. Int J Prosth 2006, n press.
Monaco C, Krejci I, Bortolotto T, Perakis N, Ferrari M, Scotti R.

128
Marginal adaptation of one Fiber Reinforced Composite and two different all-
Ceramic Inlay Fixed Partial Denture Systems. Int J Prosth 2006, in press.
Marginal adaptation of one Fiber Reinforced Composite and two different all-
Ceramic Inlay Fixed Partial Denture Systems. Int J Prosth 2006, in press.
Baldissara P, Valandro LF, di Fiore P, Monaco C, Ferrari M, Bottino MA, Scotti R.
Fatigue test in shear: its effect on bond of a glass-infiltrated alumina ceramic to
human dentin, using different luting procedures. J Adhes Dent 2006, in press.
List of abstract part of this thesis Monaco C, Ferrari M . Randomized clinical trial of inlay fixed partial dentures .
Abstr 585 119CED-NOF of the IADR meeting Amsterdam 14-17 september 2005.
Monaco C. Adhesive inlay bridges with FRC: clinical and laboratory investigations.
Abstr SO460C 119CED-NOF of the IADR meeting Amsterdam 14-17 september
2005.
C. Monaco, P. di Fiore, P. Baldissara, R. Scotti. Fatigue resistance of in-
Ceram/Dentin bonding: a comparative study. 2003 J Dent Res 82. Special issue B
Abstr 1462.
Monaco C, Baldissara P, Caldari M, Scotti R. Six-month evaluation of post
operative sensitivity in IFPDs. J Dent Res Abstr 579. Honolulu 2004
Baldissara P., Melilli D, Monaco C, Ciocca L. Fatigue resistance of fiber posts and
different build-up materials. J Dent Res Abstr 579. Honolulu 2004.
Baldissara P, Quadrelli M, Monaco C, Scotti R. E-Modulus and Flexure Strength of
FRC: Introducing Boron Fibers. Abstr 372 119CED-NOF of the IADR meeting
Amsterdam 14-17 september 2005.

129