circuaiation - homepage | circulationcirc.ahajournals.org/content/13/2/161.full.pdfcause of cardiac...
TRANSCRIPT
CircuaIationFEBRUARY, 1956VOL. XIII NO. 2
OFFICIAL JOURNAL ofthe AMERICAN HEART ASSOCIATION
Electric Instability of the Hearta/
The Concept of the Current of Oxygen Differential inCoronary Artery Disease
Bi11 13EnNAR1) L. BROEMAIAN, D\1.I).,IhvID S. LEIGHNINGER, M.D., AN!) CLAUDE S. BECK, \..
Normally oxygenate(l dog hearts and hearts rendered unifornmly anoxi(c exhibit electric sta-bilitv: there is no lifference in resting electric potentials, and spontaneous ventricular fibrillationdoes not occur. When .In area of mnvocarlium is rendlered isehemic, the resulting "trigger" may
destroy the coordinated mechanism of the heart. A current of oxygenldifferential is produced
across the zone of contact between red and blue myocarditini resulting in 'electric instability.."In the electrically stable, unifornmly anoxic heart, perfusion of aln area with red blood produces a
"reverse trigger" and electric instability. Application of these concepts and therapeutic implica-tions to human coronary (lisease appears justified.
IN the vast majority of deaths due tocoronary artery disease, the immediatecause of cardiac arrest remains obscure.
In only a relatively small group (ean cardiacdeath be explained on the basis of the degreeof reduction of total coronary inflow and ex-tensive destruction of myocardiumii. These pa-tients have "muscle death;" the heart becomieshypodynamic, and eventually fails.' IPresuma-b)ly, little can be accomplished with respect toprotecting these patients from death. How-ever, in the much larger group who die ofmechanism death," destruction of the coor-
dinated heart beat occurs in a heart, withadequate total coronary inflow anld functionalimiyocardium.1 Such a catastrophe appears tobe, to a large degree, preventable. Clinico-pathologic studies such as those of Yater and(o-workers2 and Blumigart3 confirin this ( on-cept of mechanism death in patients dyingfr oiii coroniary disease.
It has hecome immcreasiiigly evideit that deathin coronsary disease is not so much d(Ie to re-
This work was done in the lal)oratorV of 1)Dr. ClaudeS. Beek and suil)l)oite(l 1bN grants fromn the Ulite(lStates Puhlic Health Serivice tiind the Cleveland AreaIleart Souietv.
161
duction in total coronary inflow as to uneven orunbalanced distribution of the available sup-ply. The development of adequate functioningintercoronary channels4 serves to reduce thisimbalance and gives protection against mech-anism death. Methods which safely and effec-tively produce these channels should be appliedto patients with coronary disease.
Trigger concept: In order to better under-stand the events leading to death in the pres-ence of coronary disease, the concept of thetrigger mechanism has been evolved. The triggerwas originally defined as an ischemic area ofmyocardiumii capable of sending out impulsesthat in turn destroy the normal mechanism.5The addition of small amounts of blood to thisarea can obviate the destructive properties ofthe trigger. Extenisive experimental and clini-cal experieni(e with the surgical treatment forcoronary artery dlisease has substantiated theconcept of the trigger mechanism and hasdemoimstrated the remarkably beneficial effectof a few(cubli (enftilneters of blood delivered toa potentially ischemnic area in preserving thecoordinated mnechanism and viability of heartmuscle.'' 6
The present study is a preliminary attemptCirculation, Volume XIII, February, 195(3
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

12JI,,CTRIC INSTABILITY OF 1J1PAT
to define further the mode of production of thetrigger area and mechanism death, and toevaluate the associated bioelectric phe-nomena. Experimentally, extensive studieshave beeni carried out concerniing the effect ofvarious forms of "injury" on the heart. Coro-nary artery ligation has been considered themethod par excellence for producing "injury."The area of ischemia, or trigger area, whichresults has certaini electrophysiologic features.Ani "injured" region has been defined7 as onewhich undergoes subnormal changes ini theintensity of polarization owing to impairment,of its ability to polarize or depolarize. Duringdiastole, the "injured" area is electrically nega-tive with respect to surrounding myocardium,haviing a more or less sharp boundary at themargin of the "injured" zone.8 9 During systolethe "injured" area may be electrically positivewith respect to the "noninijured" muscle '1The "current of injury" which results from
this electric imbalance is manifested by de-viation of the S-T segment, of the electro-cardiogram. The "injured" area is character-ized by S-T segment elevation in direct leadsderived from its surface and in indirect leadspositively influenced by this area. Theoreti-cally, areas adjacent to the injured area wouldbe expected to exhibit S-T segment depression."
Since "injury" as such rarely occurs clinii-cally, and for reasons to he discussed later,we prefer to use the term "trigger" defined asan area of myocardium which is relativelyischemic with respect to contiguous better-oxygenated muscle; it is characterized bydiastolic electric negativity and demonstratesS-T segment elevation ini direct, electrocardio-graphic leads from its surface.
Studies in this laboratory and others'2 havedemonstrated that suiddeni perftusioni of a pre-viously occluded coroniary artery frequentlyresults ini venitricular fibrillation and death ofthe animal. This observation suggested to oneof us (C. S. B.) the theoretic possibility thatthe deleterious effects of the trigger wereproduced by a marked difference of oxygencontent, oni either side of an area of contact;this zonie may be static and well defined or maybe rapidly undergoing change in position.
Concept of reverse trigger: Total anoxia (or
asphyxia), although the most advanced formof "inijury" of the heart, does not cause ventric-ular fibrillation. We will explore the theoreticproposition that perfusion of one coronaryartery with oxygenated b)loo10 during totalanoxia will cause a previously "electricallystable" heart to develop the (characteristicsof a trigger in the anoxic muscle, and demoin-strate "eleetric inistal)ilitv."
MATERIALS A-ND METHODS
The observations herein plresented wvere madeduring the course of thousands of operations on (logs(allie(l out in the (levelopment of the present opera-tive treatment for coronarvartery disease.' Undelether or intravenous Nembutal anesthesia, thechest was opened viaa. left lateral incision. Respira-tion was miialintatine(l 1w metins of the Rand-Wolferespiirator. The p)elical(lium was openedl andl suturedto the chest waldsa (ladle for the heart.
Mletho(ls for P-rodii.ictg Trigger Area(1) Multiple small aritery*)occlusion. Three or
more small arteries usually supplying ain area t theapex arie ligated.7 Through small cannulae inserteddistal to the occlusion, 1)lood may b)e pelfusedl intothe potential trigger. .area.
(2) Large artery occlusion. The left (lescen(ling or
circumflex artery is (annulatedl neal its origin (fig.1). Perfusion is nimamtamie(l via a cannulated ca.rloti(l
Fi(;. 1. IPerfusion system for left cireuniflex co(o-nary artcrv. With clanip A open anh(l clamp B close(l,distal artery is perfuscd via the caroti(l artery. Withclamp A closed 1i1(1 clalnI) B open, (listal artery isperfused from p)ressullre ot tte at 1). C~l~amping ofttlliilig at C produces coml)lete (cilrcllnflex occlusiol.
16;2
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BROFMAN, LEIGHNINGER AND BE'CK
artery.3 The trigger is produced by clamping theperfusion system to the test artery.
(3) Reduced perfusion. Instead of complete oc-clusion of the test artery, it is perfused from a reser-voir with one of the following: A. Venous bloodpreviously collected under oil from the animal. B.Anemic blood in which the hemoglobin concentra-tion is reduced by dilution with plasma or saline.C. Oxygenated blood under reduced perfusion pres-sure, at a reduced rate of flow.14
Production of reverse trigger: Generalized myo-cardial anoxia may be induced by simply clampingthe tracheal tube and progressively asphyxiating theanimal. The test artery is then perfused with oxy-genated blood from a pressure bottle at a meanpressure of 100 mm. Hg. MIyocardial anoxia may alsobe produced by allowing the animal to rebreathe toany desired oxygen concentration (5 to 10 per centoxygen) in the inspired air, the carbon dioxide beingabsorbed by soda lime. An alternate method forregulating the inspired air is to control the oxygenconcentration via the anesthesia machine. The useof regulated anoxia rather than asphyxia obviates themany other secondary factors produced by asphyxia,including the effects on the cardiac and respiratorycenters.
Electrocardiographic studies. These were carriedout by employing condenser-coupled, amplifier-typedirect writers. Usually a Sanborn Viso-Cardiette or4-channel electrocardiograph was used, the latterpermitting simultaneous tracings from indirect aswell as direct epicardial leads at normal paper speedsand at speeds of 50 mm. per second (twice normal).The direct epicardial or sweep electrode consistedof a saline-soaked cotton-tipped "V" lead. Thiselectrode was applied to the epicardium and sweptacross designated areas during continuous recording.The sensitivity of the epicardial lead was reduced to1/10 to 1/20 of standard because of the much highervoltages existing at the epicardial surface. Thissweep electrode was found to produce no pressureeffect upon the epicardium and when it was sweptacross the epicardial surface the isoelectric line re-mained remarkably stable.
Usually one of the limb leads was recorded atstandard sensitivity before or after the epicardiallead when the single channel recorder was used.The 4-channel apparatus permitted simultaneousrecording of the following: (1) an esophageal leadat the level of the apex; (2) an intracavitary leadusing an electrode-tipped cardiac catheter insertedvia the left atrial appendage; since introduction intothe left ventricular cavity usually provoked inter-mittent premature ventricular beats, this electrodewas usually withdrawn to the mitral orifice; (3) aunipolar limb lead, usually aVF; (4) a direct epi-cardial sweep lead,
Control tracings were made before and after eachprocedure. In most cases, the various procedureswere performed repeatedly to demonstrate the re-
producibility and the reversibility of certain find-ings.
RESULTS
Figures 2 to (6 demonstrate typical electro-cardiographic observations during the variousstudies.
Control Studies
Sweep epicardial leads, whether from baseto apex (fig. 2) or from descending coronaryarea to circumflex (fig. 5), exhibited the samegeneral characteristics over the surface of theleft ventricle. The height of the R wave variedsomewhat over the precordium; in some in-stances it appeared constant over the area ofexploration (fig. 6). The R wave was alwaysfollowed by a well-defined S wave. The S-Tsegment was usually isoelectric or slightlyelevated and was followed by a rather deeplyinverted T wave. In general, the ST-T segmentwas definitely depressed.
Generally, there was little significant changein the unipolar limb leads after the chest andpericardium were opened. In aVF, the QRSwas almost invariably upright. The S-T wasisoelectric, followed by an inverted T wave(fig. 5).The esophageal lead + with the electrode
placed at the level of the apex, showed a Qwave with a fairly tall R, isoelectric S-T andinverted T wave (fig. 5). The intracavitary leadrevealed a pure QS wave with a slightlyelevated or isoelectric S-T segment and small,upright T wave (fig. 5). This is similar to intra-cavitary leads from the left ventricle reportedby others."-"Repeat control studies after ligatures were
placed in position around test arteries showedno significant change. Following cannulationand perfusion of the test artery via the carotid,there was also no significant change, nor didconstant perfusion of the test artery from thepressure bottle at a mean pressure of 100 mm.Hg alter the electrocardiogram (fig. 5).
Effects of M1ultiple Artery Occlusion
Sudden occlusion of multiple small arteriessupplying a given area of myocardium wasfollowed by the appearance, within 60 seconds,
1693
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

E16LECTRIC INSTABILITY OF HEART
BASEAr APEX
FIG. 2. Multiple ligation at apex. In this and subsequent figures, the insert represents the triggerarea (stippled); the arrow shows the direction of the epicardial sweep lead. Sensitivity: 1 cm. = 15 mv.
A. Control. B. Trigger produced by multiple ligation at apex. S-T segment depression at basewith abrupt transition to S-T segment elevation over cyanotic apex. C. Reverse trigger. Stippledarea perfused via multiple cannulae with red blood at 100 mm. Hg from pressure bottle during as-phyxia, so that surrounding muscle is deeply cyanotic after 5 minutes. Over base, ST-T segmentnot as depressed as in control; over pink area transition to marked ST-T depression. Note apparentshift in "isoelectric" line.
FIG. 3. Multiple ligation producing trigger area near apex, but leaving apex pink. Control omitted.Sensitivity: 1 cm. = 5 mv.
A. Stippled area cyanotic (trigger). Over pink base, no S-T segment depression. Marked S-T ele-vation over trigger with abrupt transition to S-T depression at pink apex. Lead aVR shows S-T seg-ment depression, aVL shows S-T elevation. B. Asphyxia superimposed upon trigger. Entire heart nowcyanotic to some degree. Although S-T segment deviations persist, they are not so marked.
164
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BROFMIAN, LEIGHNINGER AND BECK16
DESC. CIRCUM.
ti~~~~A '. ~~~~~~~~A4
ljJ~
%..1-
. T
y,7F7777T...F -F-I&IJI V
FIG. 4. Left descending artery perfusion. Epicardial sweep lead from descending (D) to circumflex(C) area. Sensitivity: 1 cm. = 15 my.
A. Control. B. Occlusion of descending. Stippled area cyanotic (trigger.). S-T segment elevationover trigger area with minimal S-T depression over pink area. C. Control, 30 seconds after B. D.Reverse trigger. Asphyxia for 2 minutes, perfusion of descending area with oxygenated blood for2 minutes. Stippled area pink. Slight S-T segment depression near transition zone, with S-T ele-vation over cyanotic area. E, F, G. Reverse trigger at 3, 5 and 7 minutes. ST-T segment depressionover pink area progressively pronounced.
165
A
r-.
.j.
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

166lECTRIC INSTABILITY OF HEIART
4 5 (;., f:
.,: _, *: . 0:: ..
t^r a.7 r;t >7i3 5: s And:. i 7^ t: :, :- s7 or:4 . . 77 5 . ..:r,;.R 4 7
i, ,.
... F, at%
.'.\ . . .' .*.* -. .' VV. .N .VV.'
FIG. 5. Circumflex perfusion. Simultaneous 4-channel recording. Esophageal lead (esoph.) atapex. Intracavitary (I-C) lead at mitral orifice. Limb lead aVF. Epicardial sweep lead (sensitivity:1 cm. 20 mv.) across positions 1 to 6 as designated on insert. Double speed (50 mm. per second)recording in A, B, C, D, H. In C and H extra inserts to show continuous sweep across transitionzone.
A. Control, before perfusion. B. Circumflex artery perfused via carotid. Also no change whencircumflex perfused from pressure bottle at 100 mm. Hg. C. Circumflex occlusion, 2 minutes. Stip-pled area cyanotic (trigger). S-T segment elevation in esophageal, intracavitary, and foot lead.Epicardial sweep shows S-T segment depression over the pink area with transition to S-T elevationover the trigger area. D. Total asphyxia-4 minutes. Except for the slower rate, there is no signifi-cant change from the control. E. Control (at normal paper speed). F. Circumflex perfused by de-saturated venous blood from pressure bottle. Stippled area cyanotic. S-T deviations similar to thoseproduced by trigger in C. G. Reverse trigger. Asphyxia for 6 minutes. Circumflex perfusion withoxygenated blood. S-T segment depression in indirect leads. ST-T elevation over cyanotic area withtransition to ST-T depression over oxygenated (stippled) area. H. Circumflex occlusion (trigger)again. Indirect leads again show S-T segment elevation. S-T depression over pink area with transitionto S-T elevation over trigger. (Note electric alternans, most obvious in epicardial leads over trigger.)
166
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
BR{OFMAN, LEIGHNINGER' AND BECK16
.r.4A . JIrfA!AALL.4A.LI.
V.w
rW\Ar\t\A.vvr.rv4
RELEASE
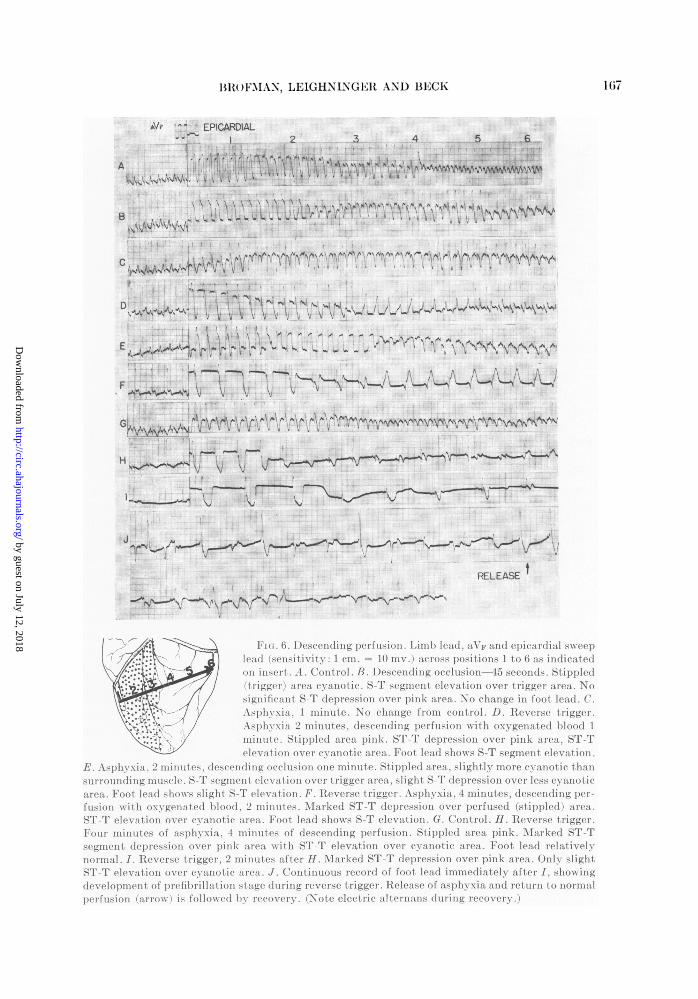
Fim. 6. Descending jperfusionl. Limb lead, aVF and epicardial sweeplea(1 (sensitivity 1 cm. = 10 my.) across positions 1 to 6 as indicatedon iiisert. A. Control. B. lDescending occlusion-45 seconds. Stippled(trigger) area cyanotic. S-T segment elevation over trigger area. Nosignificant S-T depression over pink area. No change in foot lead. C.Asphyxia, 1 minute. No change from control. D. Reverse trigger.Asphyxia 2 minutes, descending perfusion with oxygenated blood 1minute. Stippled area pink. ST-T depression over pink area, ST-Televation over cyanotic area. Foot lead shows S-T segment elevation.
E. Asphyxi, 2 iuts desceliding occlusioii one minute. Stippled area, slightly more cyanotic thansurrounding muscle. S-T segmient elevation over trigger area, slight S-T depression over less cyanoticarea. Foot leadshow slight S-T elevation. F. Reverse trigger. Asphyxia, 4 minutes, descending per-fusion wirth oxygenated blood, 2 minutes. Marked ST-T depression over perfused (stippled) area.ST-T elevation ovet. cyanotic area. Foot lead shows S-T elevation. G. Control. H. Reverse trigger.Four minutes of asphyxia, 4 minutes of descending perfusion. Stippled area pink. i\arked ST-Tsegment (depression over pink area with ST-T elevation over cyanotic area. Foot lead relativelynormal. I. Reverse trigger, 2 minutes after H. Marked ST-T depression over pink area. Only slightST-T elevation over cy'ianotic ar~ea. J. Continuous record of foot lead immediately after I, showingdevelopment of lprefilbrillat ion stage (luring reverse trigger. Release of asphyxia and return to normalperfusion (arrow~) is followed by reuover.)-. (Note electric alternans (luring recovery.)
167
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELECTRIC INSTABILITY OF HEART
of a rather sharply defined, increasingly cya-notic area which appeared to lose its contrac-tility. In some instances, ligation of everyavailable branch immediately resulted inventricular fibrillation.5 Within 30 to 60 secondsthe S-T changes associated with the triggerarea appeared (figs. 2 and 3). Figure 2Bdemonstrates the change in the epicardial leadas the sweep is made from the pink base to theblue apex. At the base there is rather markedS-T segment depression, of uniform degree,until the edge of the cyanotic trigger area isreached. At the margin of the trigger areathere is a sudden shift in the direction of theS-T segment from depression to isoelectric andthen to elevation. The diastolic baseline (T-Psegment) appears to have dropped 6 mm. in thetransition (or equivalent to minus 9 mv.). Thedegree of S-T segment depression over thepink area and the elevation over the blue areaare approximately the same, suggesting thatthe predominant factor in producing theseST-T changes is the diastolic negativity of thetrigger area8 and the relative positivity of thepink area. The maximal surface resting poten-tial difference is approximately 9 mv. At deeperlevels within the myocardium it is presumablyprogressively decreased but still elevated atthe endocardium.15' 17
Production of a reverse trigger (fig. 2C)results in a gradual loss of contractility as theheart became more cyanotic except for theperfused apical area. The epicardial lead showsa rather isoelectric ST-T segment over thecyanotic base. At the margin there is a suddenrise of the diastolic baseline without a corre-sponding rise of the ST-T segment so that adepressed S-T segment appears to be almostentirely a measure of the difference (14 mv.)in resting diastolic potential across the marginalarea.
In the case demonstrated in figure 3, multipleligation produced a cyanotic area near theapex, surrounded by pink, normally contractingmuscle at the base and at the apex (fig. 3A).The epicardial lead at the pink base shows noS-T depression. At the boundary zone the S-Tsegment becomes elevated and then falls asthe boundary at the apex is reached, at whichpoint marked S-T segment depression appears.
Again there is an apparent shift in the diastolicbaseline, particularly in the transition near theapex. Here the difference in the diastolic base-line is approximately 6 mv. which is also theaverage S-T elevation over the trigger and thedepression over the pink apex.When asphyxia is superimposed upon the
multiple ligation trigger (fig. 3B) the pink areaalso becomes cyanotic so that there is not sogreat a degree of difference in oxygenationacross the marginal area. By the same token,the degree of S-T segment elevation over thetrigger is somewhat decreased.
Large Artery OcclusionWithin 30 to 60 seconds after ligation of the
left descending or the left circumflex coronaryartery the area supplied by the occluded arterybecomes hypodynamic and increasingly cya-notic with a distinct boundary at the wsell-oxy-genated myocardium. Figure 4 demonstrateschanges in the epicardial lead when the leftdescending coronary was the test artery. Cor-responding sweeps with the epicardial lead weremade from the descending area to the circum-flex area. Two minutes after the control tracing(fig. 4.4), the typical electrocardiographicmanifestations of the trigger area are present(fig. 4B). There is marked ST-T elevation overthe cyanotic area with a sudden transition atthe margin to S-T isoelectricity and then de-pression. After a control period, asphyxia, plusperfusion of the left descending with oxygen-ated blood produces a reverse trigger. At twominutes of this reverse trigger (fig. 4D) thereis a tendency toward ST-T depression on theoxygenated side of the margin with ST-Televation on the cyanotic side. The diastolicbaseline appears to have dropped approxi-mately 10 mv. With further maintenance ofthe reverse trigger, progressive changes occurlso that at five minutes (fig. 4F), marked ST-Televation is present over the trigger area, withan evident shift in the baseline of 15 my. Atseven minutes (fig. 4G), marked ST-T depres-sion is present over the well-oxygenated areawith only slight ST-T elevation over thetrigger.
Figure 5 demonstrates typical electrocar-diographic findings in a dog with the left
168
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
B1RO1FAN, LEIGHNINGER AND BECK1
circumflex as the test artery. Simultaneousesophageal, intracavitary, limb, and sweep leadsare shown. Perfusion of the circumflex arteryvia the carotid produced no significant changefrom the control record (fig. 5A, B). Twominutes after circumflex occlusion (fig. 5C),S-T elevation is present in the esophageal,intracavitary and foot leads. The sweep leadshows S-T segment depression over the well-oxygenated area, with transition to S-T eleva-tion across the margin of the trigger. After areturn to control conditions, total asphyxiafor four minutes produces little alteration fromthe control record (fig. 5D). Perfusion of thecircumflex area at 100 mm. Hg pressure withvenous blood produces similar electrocardio-graphic changes to those produced with com-plete occlusion (fig. 5F). When the circumflexis then perfused with well-oxygenated bloodduring complete asphyxia, reverse triggerchanges occur (fig. 5G): there is S-T segmentdepression in the esophageal, intracavitary,and foot leads; S-T segment elevation overthe cyanotic area with a transition to S-Tsegment depression across the margin of thewell-oxygenated area. A complete reversal ofthese S-T segment changes follows a return tonormal oxygenation with occlusion of thecircumflex (fig. 5H). Electric alternans is seento develop and is most obvious in leads overthe trigger area.
Figure 6 demonstrates left descending per-fusion. Lead aVF is shown with the sweep leads.Within 45 seconds of descending occlusion,uniformly marked S-T segment elevation ispresent over the trigger area with a transitionto slight S-T depression across the margin(fig. 5B). With generalized asphyxia (fig. SC),there is again little change from the controluntil the descending is perfused with oxygen-ated blood (fig. 6D), at which time S-T segmentelevation appears on the cyanotic side of themargin (and in the foot lead). Occlusion of theleft descending during asphyxia (fig. 6E) pro-duces S-T segment-elevation over the occludedarea and S-T depression over the cyanotic butrelatively better-oxygenated area. Productionof a reverse trigger (fig. GF) then demonstratesmarked ST-T depression over the well-oxygen-ated descending area with a transition to ST-T
elevation over the cyanotic area. The apparentfall in the diastolic baseline is approximately12 mv. Following a control period (fig. 6G),a prolonged reverse trigger (fig. 6H) ultimatelyproduces marked ST-T depression over theoxygenated area with little or no elevation overthe cyanotic area (fig. 6I). Again marked shiftsin the baseline occur. A continuous record(aVF) then shows (fig. 6J) the onset of rapidlyprogressive ventricular ectopic activity, whichis uniformly followed by ventricular fibrilla-tion. In this instance ventricular fibrillationwas prevented by a return to normal oxygena-tion and perfusion.
General ObservationsLigation of the left descending or circumflex
results in ventricular fibrillation and suddendeath in 50 to 70 per cent of the dogs subjectedto this procedure. In dogs which do not fibrillateafter 10 to 20 minutes of occlusion, sudden re-lease of the ligature results in the onset of ven-tricular fibrillation in approximately 30 percent of the animals in which this is done. Directepicardial leads over the suddenly perfusedarea usually shows an immediate reversal ofthe S-T segment from elevation to depression.
In more than 50 dogs subjected to generalizedanoxia (asphyxia), spontaneous ventricularfibrillation did not occur. Epicardial leadsshowed no significant S-T deviations. Deathis accompanied by pacemaker failure or A-Vconduction failure. Resuscitation can be ac-complished readily with return to normaloxygenation.
In dogs rendered generally anoxic, perfusionof a coronary artery with oxygenated bloodmay induce ventricular fibrillation. As pre-viously shown, S-T segment deviations appearonly with the perfusion.
DISCUSSION
Current of Oxygen Differential:
It has long since been demonstrated that"injury currents" may develop at the marginof infarcts with the result that the balance ofelectric potential difference in the heart as awhole is affected.18 These "currents of injury"have been produced in many ways in the ex-
16;9
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

10ELEiCTRIC INSTABILITY OF HEART
perimental animal. The simplest and com-monest method is the production of an areaof ischemia by complete large artery ligation.Partial ligation has also been used."' Directinjury to areas of heart muscle has beenachieved by extremes of heat and cold, chemi-cals, pressure, the application of suction, anddirect trauma to the myocardium. The directapplication of these methods to human coro-nary disease has provided valuable physiologicand electrocardiographic information, but ismisleading in some respects. "Injury" as such,does not occur in human coronary disease.Asphyxia, with generalized myocardial anoxia,is "injury" of the highest order, and yet no"current of injury" is produced. It is only whenthere is a relative reduction in the total injury,i.e., perfusion of part of the myocardium withoxygenated blood, that the so-called "currentof injury" appears. Thus, it can be demon-strated that the electric manifestations of"injury" depend upon a difference in the degreeof oxygenation of contiguous areas of myo-cardium.Our studies have shown that this current is
produced following large artery ligation andalso multiple small artery ligation. The methodof reduced perfusion, as shown in figure 5F, alsoproduces currents when the degree of oxygena-tion of the perfused area is reduced to approxi-mately 50 per cent of the normal perfusion.'4(These studies will be described in a later pub-lication.)
Suffice it to say, insofar as the human myo-cardium is concerned, it would appear that the"current of injury" is really a current of oxygendifferential and depends upon the relativeoxygenation in contiguous areas.
Measurement of CurrentsAlthough it is not our purpose at this time to
attempt to explore the various theoreticelectrophysiologic considerations concerningthe genesis of electrocardiographic changesassociated with myocardial ischemia or "in-jury," a few observations are pertinent. Soonafter obstruction of a coronary artery, theischemic area of heart muscle becomes elec-trically negative with respect to the normally
oxygenated imiuscle.'9' 20 According to Katz2'the "injury currents" set up by damaged livingtissue establish their own electric field inde-pendently of the fluctuating electric fieldproduced by activation and restitution of theremaining heart tissue. The S-T segment isthe measure of this electric field.A potential difference exists at the boundary
between well-oxygenated and poorly oxy-genated muscle giving rise to a flow of currentacross the boundary and an associated elec-tric field.7," Obviously, with our presentmethod of recording, absolute measurementsof change in electric potential cannot bemade. (More extensive studies using a direct-coupled amplifier22 are being carried out in anattempt actually to measure diastolic andsystolic differences in potential produced bytrigger areas.) Displacement of the S-T seg-ment in these studies is then an approximateexpression of the sum of the difference inelectric potential existing during systole anddiastole.
Production of CurrentsWhether by larger artery ligation or by
multiple ligations of small branches, a well-defined trigger could always be produced.Although S-T elevation occasionally appearedmost marked in the center of the trigger area,usually there was no gradual or proportionalfall as the margin was approached. As a mat-ter of fact, approximately the same degreeof elevation was maintained until the suddenchange to isoelectric at the margin. In gen-eral, the most marked and abrupt S-T seg-ment changes occurred with the multipleligation technic of trigger production(figs. 2 and 3). In each such experimentthere was an abrupt change from S-T segmentelevation to S-T segment depression at thetransition from trigger to normally perfusedmuscle. However, even in single artery liga-tion most frequently (although not always)there was also found some degree of S-T de-pression over the nonischemic area. This differsfrom the experience of Rakita and co-workers'5who on no occasion found S-T segment depres-sion on the anterior surface of the heart adja-
170
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BROe)IMi\N, LELGHNINGEIR AND BICI1
cent to the area of isehemia. Others17 havefound it, necessary to occlude small terminalbranches in addition to the large artery toproduce marked S-T segment elevatfion in theischemic area. Leads over "uniinijured" regionsshow depressed or isoelectric S-T segm-ients1l' 16
It would appear that three factors are in-volved in determining the current produc-tion and the associated electrocardiographicchanges: (1) The degree of difference in myo-cardial oxygenation in the trigger area and inthe surrounding muscle; (2) The abruptnessof the transition between the two areas and(.3) The relative size of the trigger area.Adequate multiple small artery ligation
produces more complete anoxia of a triggerarea than does large artery occlusion, since itstops all arterial inflow into the area. Withlarge artery ligation, collaterals may bring inenough blood to the marginal areas so thatthere is no abrupt transition, and hence nosudden difference in potential at, the margin.Even in normal dogs1 backflow studies havedemonstrated physiologically functioning col-laterals. It would appear that, the absence ofmarked S-T segment deviation in some studiesis due to a poorly-defined mnargin betweentrigger and nonischemic myocardiumi. Furtherstudies using backflow measurements are nowbeing carried out in an attempt to correlatefurther electrocardiographic chanoges followingartery occlusion with collateral circulation.Even with multiple ligation, there may be
no S-T depression over the normially perfusedarea. In figure 3A, the epicardial lead over thepink base showed no significant depressiondespite the marked S-T segment elevationover the trigger and the marked S-T depressionbeyond the trigger at the apex. This may bedue to a more poorly defined basal marginof the trigger area, due, in this case, to li-gation of only two of the three vessels sup-plying this area.
In all probability humian miyocardial infarc-tion is more like the (hanges produced by themultiple ligation method in that the size anddefinition of the infarcted area is (leterminedby poorly perfused small vessels and collaterals,with the final insult being cc(,(ltusioni or a reduc-
tion ill perfusioni of a large artery. Ill patientswith adequate collaterals,4 complete largeartery occlusion may occur without myocardialinfarction or trigger production.
There would appear to be many similaritiesbetween the current here produced and ordi-nary galvaniic (battery) current. Electromiotixveforce is a function of the nature of the twodissimilar materials in electrolytic contact.When the heart muscle is of uniform oxygen-ation, there is no difference in potential. How-ever, as the difference in oxygenation across thezone of contact increases, voltage is produced.(Whether the difference in potential is directlyrelated to the degree of difference in oxygena-tion is yet to be determined.) Furthermore,the greater the area of the trigger (withincertain limits), the larger the circumference,and hence the larger the area of contact withsurrounding myocardium. Since current (am-peres) is a function of the area of contact be-tween two dissimilar materials, it can be seenthat the larger the area of the trigger, the morecurrent flow. Also, since the trigger acts as avolume source, the current density at a givenarea of the margin would be greater with alarger source.
It would appear, however, from the stand-point of production of currents that there arecertain limits of predisposition as regards sizeof the trigger area. The larger the trigger, thesmaller the nonischemic area, so that wheneach is approximately the same in size, maxi-mum contact exists. However, if the triggerextends to the base, a boundary may be lost.17It would appear, then, that a relatively largertrigger area would be associated with a greatercurrent production than a smaller area, assuin-ing an equally abrupt margin and differencein oxygenation. However, even a very largetrigger might have little electric effect ifcollateral circulation precluded an abrupttransition at the margin. On the other hand, asmall area rendered completely anoxic, with anabrupt margin might have a marked electriceffect.
If the degree of ischemia in the trigger areais uniform throughout, the degree of S-Tsegment elevation in epicardial leads should be
171
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELECTRIC INSTABILITY OF HEART
more or less uniform across the epicardium.Our studies do show relative uniformity exceptnear the margin. This also differs from theobservation of Rakita and co-workers.15The degree of S-T segment elevation over a
trigger area appears to be inversely related tothe size of this area. The larger the triggerbeyond a certain optimum size, the lesser theS-T segment elevation, and the more poorlydefined the margin with the better oxygenatedarea. In clinical electrocardiography, this mayaccount for the lack of S-T segment elevationin massive infarction.These observations appear to be confirmed
by the "reverse trigger" studies. Progressivegeneralized anoxia produces little or no S-Tsegment displacement. Perfusion of a largeartery with normally oxygenated blood resultsin S-T segment elevation over the anoxic areawith S-T depression over the oxygenated area.The degree of these changes also appears highlyvariable. The small oxygenated area in figure 2Cexhibits marked S-T segment depression, whilethe comparatively massive anoxic area showsonly a slight tendency to S-T elevation. In fig-ures 4, 5 and 6, the oxygenated areas are largerbut still small as compared with the anoxicareas, so that eventually the S-T segmentdepression in the perfused area is much moreprominent than the S-T elevation across themargin. However, it should be emphasized thatin the reverse trigger, as in the trigger, withthe production of a difference in tissue oxy-genation in contiguous areas, a difference inpotential is present.
It has been demonstrated experimentallyand in terminal electrocardiograms in man23' 24that conditions which produce gradual overalldiminution in the functional capacity of thecardiac tissue without predisposition to ectopicventricular systoles result in failure of thepacemaker or of A-V conduction, but veryrarely induce ventricular fibrillation. In thestudies herein presented, progressive gener-alized asphyxia or anoxia produced little orno significant change in the various electro-cardiographic leads. No current of oxygen dif-ferential could be demonstrated and ventricu-lar fibrillation did not occur.25 26 Total anoxia,although eventuating in cardiac arrest (as well
as arrest of all other biologic processes), is,per se, not associated with ventricular fibril-lation or sudden cardiac arrest. Furthermore,with return to normal oxygenation, the heartbeat is readily restored.
Generalized asphyxia or anoxia producesmyocardial injury of the highest order, yet"injury currents" do not exist. Despite thehyperexcitability which moderate anoxia pro-duces,27 it is only when a trigger or reversetrigger is produced that ventricular fibrillationand sudden death occur. In the presence ofgeneralized anoxia, perfusion of one coronarybed with oxygenated blood, instead of beingbeneficial, may be catastrophic. The currentof oxygen differential manifested by S-T seg-ment elevation over the more ischemic areais shown to exist only when there is an abrupttransition between two areas having a differ-ence in oxygen perfusion.The S-T segment depression over the better
oxygenated area and the S-T elevation overthe trigger area are expressions of the differ-ence in electrical potential existing across thiszone. The trigger area is considered electricallynegative to the better oxygenated part "andelectric currents will flow until they equalizethe potential difference. Hence an electricfield will be established."' A condition of"electric instability" exists as a result of thiscurrent of oxygen differential.
In these experiments an electromotive forcehas been shown to exist across the marginof the trigger, manifested by S-T segment eleva-tion on one side and/or S-T segment depressionon the other side. This difference in potential isof the order of 5 to 20 mv. as measured at theepicardial surface. Deeper layers of the myo-cardium would be expected to record a lesserdifference in potential.'5 The zone of differenceappears to involve the endocardium, sinceendocardial leads also show S-T segmentelevation immediately under the triggerarea.15, 17
Ventricular FibrillationVentricular fibrillation is associated with
the onset of cardiac arrest in most deaths dueto coronary disease. Other forms of cardiacarrest may occur. (A subsequent publication
172
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
BJROFMIAN, LEJGHNINGER AND BEXCK
will demonstrate their similarity to ventricularfibrillation.) There is no evidence for the roleof "intercoronary reflexes" in coronary deaths.28The production of a trigger area, whether
by inultiple small vessel ligation or by largeartery ligation, has been demonstrated to resultin ventricular fibrillation and death. Triggerareas produced by the method of reducedperfusion within the limits of this study rarelycaused ventricular fibrillation. The reversetrigger, when prolonged for an adequate period,frequently resulted in ventricular fibrillation.With all of these methods S-T segment devia-tiolls typical of currents of oxygen differentialwere produced. However, it is shown that ven-tricular fibrillation is most readily producedwhere the greatest degree of oxygen differentialexists, namely, with complete ligation of ar-teries.
In 1943, Harris'2 demonstrated that ventric-ular fibrillation following coronary arteryligation was introduced by an acceleratingseries of premature beats. These ectopic dis-charges originate in the transitional zone andusually are followed by Ventricular fibrillationws-ithin 10 minutes after artery occlusion. Itwas then suggested that the fundamentalmechanisms that produce local discharges andfibrillation are identical in regional ischemiaand galvanic stimulation. A strong, briefdirect current shock has been shown to pro-duce re-entry of impulses due to progressivedecrease in the refractory period with a pro-gressive increase in conduction time.2' Repeti-tive accelerating discharges starting near thesite of stimulation then initiate ventricularfibrillation. It has been demonstrated thatthe end of systole may be a particularlyvuliierable period.30An ischemic area of iiyocardituiii has a
marked decrease in fibrillation threshold."According to HarriS32 within a very thin sheetof boundary cells between ischemic and non-isehemic mnuscle there is a transition fromadequately circulated cells to cells that areisehemic to a degree sufficient to producecomplete inactivation. Exciting factors actingupon these hyperexcitable cells in the tran-sition zone evoke discharges. Acceleratingectopic stimuli act to decrease the refractory
period and slow conduction throughout theresponding myocardium, predisposing to re-entry of impulses with subsequent venitricularfibrillation.28*
It would appear that there are two pre-requisites for the initiation of ventricular fibril-lation: (1) an area of myocardium which isparticularly vulnerable, i.e., with a loweredfibrillation threshold and (2) an adequatestimulus acting upon this vulnerable area, suchas a galvanic current.Our studies appear to demonstrate that, when
adequate currents of oxygen differential act on anlischemic area of sufficient vulnerability, ven-etric-ular fibrillation is initiated. Harrisi2 has sug-gested that "procedures which raise the gal-vanic fibrillation threshold should effect aprotective influence against fibrillation fol-lowing coronary occlusion, experimental orclinical." However, since these electric currentsare shown to be produced by an abrupt dif-ference in tissue oxygenation, it would appearthat the most effective therapy would be tominimize these currents by the establishmentof enough collateral circulation to prevent orreduce electric instability in any area. Itis emphasized that any procedure which pre-vents "dry" areas following coronary occlusionwill be effective far beyond the expectationsbased upon the small quantity of blood whichwill accomplish this.
COMMENTS AND CONCLUSIONS(1) Mechanism death, which occurs in the
great majority of coronary deaths appears to
* According to Katz21: "It has been consideredthat sporadic activity of an ectopic focus may be theresult of the operation of injury currents acting aselectric stimuli to initiate premature beats. Wher-ever heart muscle is injured the possibility exists ofa greater than normal bioelectric current flue-tuation developing during the heart cycle and thiscurrent may be sufficient in magnitude to stimulateadjacent muscle, especially if it is more excital)le )e-cause of disease. It would have to be the fluctuationat the end of systole rather than the one at its be-ginning which acts as the stimulus since the heartwould be refractory to the latter. The possibility ofthis mechanism giving rise to premature systoles issupported by the demonstration that prematulre1)eats arising during ischemia of the heart have theirorigin within or close to the ischemic area.''
173
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

1ELECTRIC INSTABILITY OF HEART
be due to the interaction of two factors: (1) avulnerable area of ischemic myocardium (trig-ger) and (2) an adequate stimulus the currentof oxygen differential produced by contiguousareas of myocardium of different degrees ofoxygenation. This current in turn dependsupon three factors: (1) the absolute differencein oxygenation of the two areas; (2) the abrupt-ness of the transition from one area to theother and (3) the relative area of the trigger.These factors act to produce an electricallyunstable heart. It is not to be assumed thatventricular fibrillation must occur when thesecurrents are at their maximum. The amountof current necessary is determined by thethreshold of the trigger area, so that fibrillationmay occur when differences of potential aredecreasing. Such factors as the accumulationof abnormal or excessive metabolites, changesin potassium concentration across the contactzone, and products of tissue necrosis un-doubtedly play an intermediary role.The relationship of these two factors, the
current of oxygen differential and the fibrilla-tion threshold, to the production of ventricularfibrillation may be expressed as the Fibrilla-tion Index, that is:
Fibrillation IndexCurrent of Oxygen Differential
Fibrillation ThresholdThus, with a high fibrillation threshold, a largecurrent is necessary to achieve the fibrillationindex. By the same token the fibrillation thresh-old may be reduced to such a low level that anegligible stimulus may be sufficient to reachthe fibrillation index. Agents such as hypo-thermia probably predispose to ventricularfibrillation by such a mechanism.33
In a potentially electrically unstable heart,even very small amounts of oxygenated blooddelivered to the trigger area would be lifesaving.Functioning intercoronary channels reduceelectric instability by modifying the above-named factors.
Yater's observations2 are of particular sig-nificance in demonstrating the role of collateralcirculation in preventing sudden death: Inyounger men the onset of the coronary attack
occurs most frequently during strenuous ac-tivity. In the older patients, it occurs at rest.Unexpected death is more frequent in theyoung; longer survival following the acutecoronary attack occurs in the older patients.We have shown that complete deprivation ofblood supply to a given area is not necessaryto produce electric instability. Only anadequate difference in oxygenation is a pre-requisite. Ventricular fibrillation and suddendeath may occur because one area of myocar-dium is well perfused during exercise whereas,because of perhaps a minor degree of arterialdisease, the arterial supply to a contiguousarea is not augmented, thus producing a differ-ence in oxygenation. Ability to receive an aug-mented flow does not necessarily depend uponthe larger coronary -vessels. Disease mayaffect the smaller vessels as w-ell. Coronaryarterial resistance during exercise is prob-ably reduced as a result of relative an-oxia.14 However, if the smaller vessels to agiven area are unable to respond with vasodila-tation while others are well perfused, a differ-ence in oxygenation may again result inelectric imbalance.
(2) The Beck I operation (abrasion of epi-cardium and lining of parietal pericardium,application of an inflammatory agent to thesesurfaces, and partial coronary sinus ligation)effectively produces intercoronary and extra-coronary channels. Relatively small quantitiesof blood are involved in providing a morebalanced distribution of available coronaryartery inflow. The effectiveness of such a surgi-cal procedure appears to lie in the preventionof the electrically unstable heart.
(3) It may be said that, within certain limits,the greater the difference in oxygenation thegreater the electrical instability. Thus, illpatients with generally lowered oxygenationof the myocardium (congestive failure, anemia,cor pulmonale) an area completely deprivedof blood supply would not have as great adifference in oxygenation with respect tosurrounding muscle and hence a lesser degreeof electric instability. By the same token,if a patientawith previously normal myocardialoxygenation develops an area of ischemia, the
174
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BROFMNIAN, LEIGHNINGER AND BECK1
administration of oxygen to this patient, ratherthan proving beneficial, may raise the oxygena-tion of the surrounding myocardium withoutpenetrating to the trigger area, thus increasingthe difference across the margin and predis-posing to greater electric instability.
(4) Angina pectoris and pain associated withmyocardial ischemia and infarction appear tobe related to various degrees of electricalinstability. Sudden death in a patient withangina pectoris may be due to production ofan augmented current, without complete ves-sel occlusion. Coronary pain is not prominentin patients with generally poor myocardialoxygenation, such as in cyanotic congenitalheart disease, cor pulmonale, and congestiveheart failure. By the same token, angina ofeffort is not frequent. Presumably, even withthe production of areas of anoxia, since thesurrounding tissue is also poorly oxygenated,a marked difference of oxygenation does notoccur.
(5) Any difference in oxygenation, whetherit be over a well-circumscribed area or perhapsof a momentarily produced margin, may becatastrophic. It has been repeatedly demon-strated that when coronary ligation does notresult in ventricular fibrillation, sudden releaseof the ligature may then produce fibrillation.Wolferth1' also demonstrated that partial occlu-sion of a large artery is followed by S-T devia-tion in that area and then removal of the liga-ture produces sudden S-T depression. Itappears that the sudden inflow of oxygenatedblood into an ischemic area produces a currentof oxygen differential, which, acting upon therelatively ischemic boundary cells results infibrillation.
It is suggested that cardiac arrest in theoperating room (or under other circumstances)might have a similar explanation. The myo-cardium of the anesthetized patient may besensitized either by the anesthetic agent orother factors. Particularly during induction,sudden fluctuations in aeration of the lungs,blood pressure and coronary oxygen flow,acting on a sensitized heart, might producethese momentary boundary zones, with elec-tric instability, and cardiac arrest.
SUMMARY
The immediate cause of cardiac arrest inmost deaths due to coronary artery disease isobscure. Experiments have been carried out todemonstrate that ventricular fibrillation andsudden death occur in a heart which is elec-trically unstable.
In the normal dog heart, electrocardiographicleads recorded across the surface of the leftventricle directly from the epicardium showuniform electric resting potential. It has beenshown that ligation of a major coronary arteryor multiple ligation of all smaller coronariesto a given area produces a "trigger" area whichfrequently leads to ventricular fibrillation, abreak in the coordinated mechanism of theheart, and death. During diastole, these "trig-ger" areas are electrically negative to thenormally oxygenated myocardium. Duringsystole, this area may be electrically positive.This is best demonstrated by the epicardialtracings showing S-T segment elevation overthe entire trigger area with a sudden change atthe transition zone to isoelectric and depressedS-T segments over the normally perfused area.Measurements of electromotive force at theepicardium show differences in potential acrossthe transition zone of the trigger area ofapproximately 5 to 20 mv. Thus, there isactually a flow of current (current of oxygendifferential) producing electric imbalance.
This electric imbalance can be demon-strated in a reverse manner. Uniform anoxiais produced by asphyxia or other means. De-spite the intense oxygen lack, ventricularfibrillation does not occur and the animalseventually die with an adynamic heart. Epi-cardial tracings in these animals show noelectric imbalance. However, if during thecourse of generalized anoxia, normally oxy-genated blood is perfused through one area ofthe myocardium, a "reverse trigger" is pro-duced. That is, epicardial leads show theanoxic area to become suddenly negative tothe oxygenated region, again with a differencein electric potential across the margin of thetrigger. Only in such cases does ventricularfibrillation and sudden death occur. Thus it
175
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELECTRIC INSTABILITY OF HEART
has been demonstrated that this "trigger"which destroys the coordinated mechanism ofthe heart beat depends upon a difference inoxygenation of two adjacent areas of myo-cardium, and it is characterized by an asso-ciated difference in electric potential acrossthe transitional zone.
Presumably, this marginal area is the truedanger zone. Anoxia (and possibly other fac-tors) render it vulnerable. The ectopic rhythmswhich lead to ventricular fibrillation have beenshown to originate here. The marginal area issharply defined electrically by the differenceof potential across it. Thus, electric instabilityexists. It is this instability, due to an unequaldistribution of coronary blood flow, whichappears to be responsible for the majority ofdeaths in patients with coronary disease. Amore nearly even distribution of coronary flowwould prevent the formation of these triggerzones between anoxic and well oxygenatedmyocardium and thus maintain electric sta-bility of the heart. Any procedure, such as theBeck I operation, which safely and effectivelyproduces intercoronary channels, would tendto prevent or reduce this electric instability.
Further studies are now being conducted onvarious methods for producing and preventingelectric instability. Accurate measurementsof the currents of oxygen differential are beingcarried out.
ACKNOWLEDGMENTThe authors wish to thank the following for their
comments and criticisms: Franklin D. Johnston,M.D., Ann Arbor, Mich., A. Sidney Harris, Ph.D.,New Orleans, La. and Mortimer L. Siegel, MI.D.,Cleveland, 0.
SUMMARIO IN INTERLINGUA
In cordes de can le quales es oxygenate demaniera normal e etiam in cordes de can lequales ha essite rendite uniformemente anoxic,il existe stabilitate electric: il non ha differentiasdel potentiales electric in reposo e nulle fibri-llation ventricular occurre spontaneemente.Quando un portion del myocardio es renditeischemic, le resultante "actionamento" potedestruer le mechanismo coordinate del corde.Un currente de differential oxygenic es pro-ducite a transverso le zona de contacto inter
le myocardio rubie e le myocardio blau, e istoresulta in "instabilitate electric." In cordes quees electricamente stabile proque illos es uni-formemente anoxic, le perfusion de un areapartial con sanguine rubie produce un "retro-actionamento" que etiam resulta in "instabili-tate electric."Omne differentia in oxygenation non im-
porta si illo involve un ben circumscripte areao forsan un margine de production momentari-pote devenir catastrophic. I1 ha essite de-monstrate repetitemente que si un ligationcoronari non produce fibrillation ventricular, ilpote occurrer que tal fibrillation resulta aloraquando le ligatura es subitemente removite. I1pare que le subitanee influxo de sanguineoxygenate a in un area ischemic produce uncurrente de differential oxygenic que resulta infibrillation per ager super le relativementeischemic cellulas marginal.
I1 pare justificate applicar iste conceptos elor implicationes therapeutic a casos de morbocoronari in humanos.
REFERENCES1 BECK C. S. AND LEIGHNINGER, D. S.: Operation
for coronary disease. J. A. M. A. 156: 1226,1954.
2 YATER, W. M., WELSH, P. P., STAPLETON, J. F.AND CLARK, M. L.: Comparison of clinical andpathological aspects of coronary artery diseasein men of various age groups. A study of 950autopsied cases from the Armed Forces In-stitute of Pathology. Ann. Int. Med. 34: 352,1951.
3BLUMGART, H. L.: Relation of effort to attacks ofacute myocardial infarction. J. A. M. A. 128:775, 1945.
4 ZOLL, P. M., WESSLER, S. AND SCHLESSINGER,M. J.: Interarterial coronary anastomosis inthe human heart with particular reference toanemia and relative cardiac anoxia. Circula-tion 4: 797, 1951.
'BECK, C. S.: The development of a new bloodsupply to the heart by operation. Ann. Surg.102: 801, 1935.
6 BROFMAN, B. L.: Results of operation for coronarydisease. Pennsylvania 1I. J. 58: 387, 1955.
7BAYLEY, R. H.: An interpretation of the injuryand the ischemic effects of myocardial infarc-tion in accordance with the laws which deter-mine the flow of electrical currents in homoge-neous volume conductors and in accordance withthe relevant pathological changes. Am. HeartJ. 24: 514, 1942.
176
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

BROFMIAN, LEIGHNINGER AND BECK
8 EYSTER, J. A. E., iIEEK, WM. H., GOLDBERG, H.
AND GILSON, W. E.: Potential changes in an
injured region of cardiac muscle. Am. J.Physiol. 124: 717, 1938.
9SUGARMAN, H., KATZ, L. N., SANDERS, A. AND
JOCHIM, K.: Observations on the genesis ofelectric currents established by injury to theheart. Am. J. Physiol. 130: 130, 1940.
10 WILSON, F. N., ROSENBAUM, F. F. AND JOHNSTON.F. D.: Interpretation of the ventricular com-
plex of the electrocardiogram. Advances IntM,\ed. 2: 1, 1947.
11 WOLFERTH, C. C., BELLET, S., LIVEZEY, M. M_.AND MURPHY, F. D.: Negative displacement ofthe RS-T in the electrocardiogram and its rela-tionship to positive displacement; experimentalstudy. Am. Heart J. 29: 220, 1945.
12 HARRIS, A. S. AND GUEVERA RoJAS, A.: Theinitiation of ventricular fibrillation due tocoronary occlusion. Exper. Med. & Surg. 1:105, 1943.
13 1IAUTZ, F. R. AND GREGG, D. E.: The dynamics ofcollateral circulation following chronic oc-
clusion of the coronary arteries. Proc. Soc.Exper. Biol. & -Med. 36: 797, 1937.
1' WEGRIA, R. W., SEGERS, M., KEATING, R. D.
AND WARD, H. P.: Relationship between thereduction in coronary flow and the appearanceof electrocardiographic changes. Am. HeartJ. 38: 90, 1949.
15 RAKITA, L. BORDNAS, J. Ij., ROTHMAN, S. AND
PRINZMETAL, M.: Studies on the mechanism ofventricular activity. XII Early changes in theRS-T segment and QRS complex followingacute coronary artery occlusion: Experimentalstudy and clinical applications. Am. Heart J.48: 351, 1954.
16 HELLERSTEIN, H. K. AND KATZ, L. N.: Electricaleffects of injury at various myocardial locations.Am. Heart J. 36: 184, 1948.
17 PRUITT, R. D. AND VALENCIA, F.: Immediateelectrocardiographic effects of circumscribedmyocardial injuries: Experimental study. Am.Heart J. 35: 161, 1948.
18 WIGGERS, C. J.: Physiology in Health and Disease.Philadelphia, Lea and Febiger, 1939.
19 BAYLEY, R. H., LA DUE, J. S. AND YORK, D. J.:Electrocardiographic changes produced in the
dog by temporary occlusion of a coronary arteryshowing a new stage in the evolution of myo-cardial infarction. Am. Heart J. 27: 164, 1944.
20 DEWAART, A., STORM, C. J., AND KOUMANS,A. K. .J.: Ligation of the coronary arteries inJavanese monkeys. Am. Heart J. 12: 70, 1936.
21 KATZ, L N.: Electrocardiography. Philadelphia,Lea and Febiger, 1946.
22 HOFF, H. E. AND GEDDES, L. A.: Heart changesand cooling. J. Appl. Physiol. 7: 416, 1955.
23 HARRIS, A. S.: Terminal electrocardiographic pat-terns in experimental anoxia, coronary occlusionand hemorrhagic shock. Am. Heart J. 35: 895,1948.
24 STROUD, M. WY. AND FEIL, H. S.: The terminalelectrocardiogram: Twenty-three case reportsand a review of the literature. Am. Heart J.35: 910, 1948.
25 ,AND MATLOCK, W. P.: The effects of anoxemicanoxia on excitability, conduction, and refracto-riness of mammalian cardiac muscle. Am. J.Physiol. 150: 493, 1947.
26 RANDALL, WM. C.: Electrocardiographic changes inrelation to tolerance of sustained anoxemicanoxia in dogs. Am. Heart J. 27: 234, 1944.
27 HARRIS, At. S. AND RANDALL, W. C.: Mechanismsunderlying electrocardiographie changes ob-served in anoxia. Am J. Physiol. 142: 452,1944.
28 OPDYKE, D. F. AND SELKURT, E. E.: A study ofalleged intercoronary reflexes following coro-nary occlusion. Am. Heart J. 36: 73, 1948.
29 MOE, G. K., HARRIS, A. S. AND WIGGERS, C. J.:Analysis of the initiation of fibrillation by elec-trographic studies. Am. J. Physiol. 134: 473,1941.
30 WIGGERS, C. .J.: Editorial. Defibrillation of theventricles. Circulation Research 1: 191, 1953.
31 , WEGRIA, R. AND PINERA, B.: The effect ofmvocardial ischemia on the fibrillation thresh-old. Am. J. Physiol. 131: 309, 1940.
32 HARRIS, A. S.: Delayed development of ven-tricular ectopic rhythms following experimentalcoronary occlusion. Circulation 1: 1318, 1950.
33 SELMAN, MI. W. AND BROFMAN, B. L.: The ef-fect of hypothermia on survival rates followingcoronary occlusion in dogs. Surgery 37: 707,1955.
177
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
BERNARD L. BROFMAN, DAVID S. LEIGHNINGER and CLAUDE S. BECKDifferential in Coronary Artery Disease
Electric Instability of the Heart: The Concept of the Current of Oxygen
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1956 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.13.2.1611956;13:161-177Circulation.
http://circ.ahajournals.org/content/13/2/161located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from