cigna healthcare of arizona medicare advantage … · cigna healthcare of arizona medicare...
TRANSCRIPT
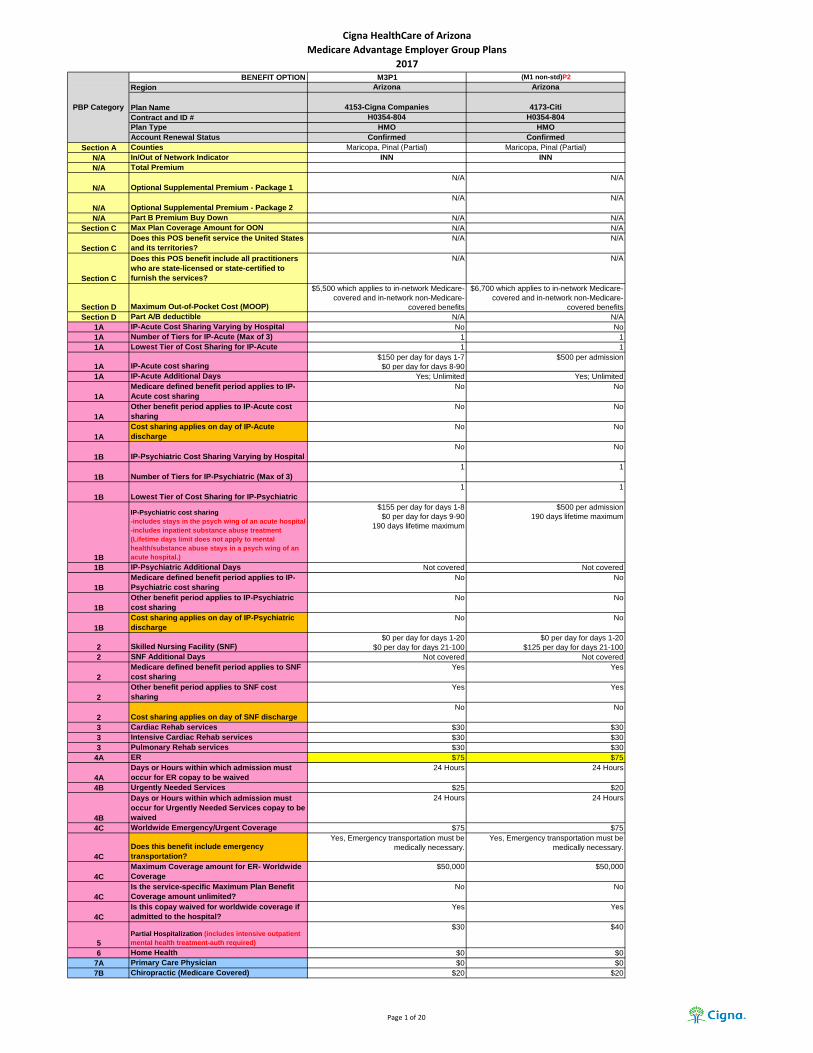
Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION M3P1 (M1 non-std)P2
Region Arizona Arizona
Plan Name 4153-Cigna Companies 4173-Citi
Contract and ID # H0354-804 H0354-804
Plan Type HMO HMO
Account Renewal Status Confirmed Confirmed
Section A Counties Maricopa, Pinal (Partial) Maricopa, Pinal (Partial)
N/A In/Out of Network Indicator INN INN
N/A Total Premium
N/A Optional Supplemental Premium - Package 1
N/A N/A
N/A Optional Supplemental Premium - Package 2
N/A N/A
N/A Part B Premium Buy Down N/A N/A
Section C Max Plan Coverage Amount for OON N/A N/A
Section C
Does this POS benefit service the United States
and its territories?
N/A N/A
Section C
Does this POS benefit include all practitioners
who are state-licensed or state-certified to
furnish the services?
N/A N/A
Section D Maximum Out-of-Pocket Cost (MOOP)
$5,500 which applies to in-network Medicare-
covered and in-network non-Medicare-
covered benefits
$6,700 which applies to in-network Medicare-
covered and in-network non-Medicare-
covered benefits
Section D Part A/B deductible N/A N/A
1A IP-Acute Cost Sharing Varying by Hospital No No
1A Number of Tiers for IP-Acute (Max of 3) 1 1
1A Lowest Tier of Cost Sharing for IP-Acute 1 1
1A IP-Acute cost sharing $150 per day for days 1-7
$0 per day for days 8-90
$500 per admission
1A IP-Acute Additional Days Yes; Unlimited Yes; Unlimited
1A
Medicare defined benefit period applies to IP-
Acute cost sharing
No No
1A
Other benefit period applies to IP-Acute cost
sharing
No No
1A
Cost sharing applies on day of IP-Acute
discharge
No No
1B IP-Psychiatric Cost Sharing Varying by Hospital
No No
1B Number of Tiers for IP-Psychiatric (Max of 3)
1 1
1B Lowest Tier of Cost Sharing for IP-Psychiatric
1 1
1B
IP-Psychiatric cost sharing
-includes stays in the psych wing of an acute hospital
-includes inpatient substance abuse treatment
(Lifetime days limit does not apply to mental
health/substance abuse stays in a psych wing of an
acute hospital.)
$155 per day for days 1-8
$0 per day for days 9-90
190 days lifetime maximum
$500 per admission
190 days lifetime maximum
1B IP-Psychiatric Additional Days Not covered Not covered
1B
Medicare defined benefit period applies to IP-
Psychiatric cost sharing
No No
1B
Other benefit period applies to IP-Psychiatric
cost sharing
No No
1B
Cost sharing applies on day of IP-Psychiatric
discharge
No No
2 Skilled Nursing Facility (SNF) $0 per day for days 1-20
$0 per day for days 21-100
$0 per day for days 1-20
$125 per day for days 21-100
2 SNF Additional Days Not covered Not covered
2
Medicare defined benefit period applies to SNF
cost sharing
Yes Yes
2
Other benefit period applies to SNF cost
sharing
Yes Yes
2 Cost sharing applies on day of SNF discharge
No No
3 Cardiac Rehab services $30 $30
3 Intensive Cardiac Rehab services $30 $30
3 Pulmonary Rehab services $30 $30
4A ER $75 $75
4A
Days or Hours within which admission must
occur for ER copay to be waived
24 Hours 24 Hours
4B Urgently Needed Services $25 $20
4B
Days or Hours within which admission must
occur for Urgently Needed Services copay to be
waived
24 Hours 24 Hours
4C Worldwide Emergency/Urgent Coverage $75 $75
4C
Does this benefit include emergency
transportation?
Yes, Emergency transportation must be
medically necessary.
Yes, Emergency transportation must be
medically necessary.
4C
Maximum Coverage amount for ER- Worldwide
Coverage
$50,000 $50,000
4C
Is the service-specific Maximum Plan Benefit
Coverage amount unlimited?
No No
4C
Is this copay waived for worldwide coverage if
admitted to the hospital?
Yes Yes
5
Partial Hospitalization (includes intensive outpatient
mental health treatment-auth required)
$30 $40
6 Home Health $0 $0
7A Primary Care Physician $0 $0
7B Chiropractic (Medicare Covered) $20 $20
PBP Category
Page 1 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION M3P1 (M1 non-std)P2
Region Arizona Arizona
Plan Name 4153-Cigna Companies 4173-Citi
Contract and ID # H0354-804 H0354-804
Plan Type HMO HMO
Account Renewal Status Confirmed Confirmed
PBP Category
7B Routine Chiropractic$20 per visit for up to 12 routine visits per
year
$20 per visit for up to 12 routine visits per
year
7C Occupational Therapy $30 $25
7D Physician Specialist $30 $25
7E
Mental Health-Individual sessions (includes intensive
outpatient mental health treatment-auth required)
$30 $25
7E
Mental Health-Group sessions (includes intensive
outpatient mental health treatment-auth required)
$30 $25
7F Podiatry (Medicare Covered) $30 $25
7F Routine Podiatry $30 $25
7G
Other Health Care (Physician Assistants, Nurse
Practitioners, etc..)In PCP office - $0
In Specialist office - $30
In PCP office - $0
In Specialist office - $25
7H Psychiatric-Individual $30 $25
7H Psychiatric-Group $30 $25
7I PT and SP $30 $25
8A Diagnostic Procedures/Tests $0 $0
8A Lab Services $0 $0
8B Diagnostic Radiological Services (MRI, CT, PET)
mammography and ultrasound-$0
CMG/ASC/HospOP - $125
non-cardiac nuclear studies - $0
cardiac nuclear studies - $30
mammography and ultrasound-$0
CMG/ASC/HospOP - $175
non-cardiac nuclear studies - $0
cardiac nuclear studies - $25
routine stress test - $25
8B Therapeutic Radiological Services (radiation therapy)$0 $25
8B X-Ray Services $0 $0
9A Hospital Outpatient Services
$0 for colorectal screenings
$30 for HospOP nonSurgical
$100 for HospOP Surgical
$0 for colorectal screenings
$40 for HospOP nonSurgical
$200 for HospOP Surgical
9B Ambulatory Surgical Center (ASC)
$0 for colorectal screenings.
$75 for all other CMG & contracted ASC
facility services.
$0 for colorectal screenings
All else-$175
9C
OP Substance Abuse-Individual (includes intensive
outpatient treatment-auth required)$30 $25
9C
OP Substance Abuse-Group (includes intensive
outpatient treatment-auth required)$30 $25
9D Outpatient Blood Services$0 with deductible waived for first three pints $0
10A Ambulance - Ground $200 $150
10A Ambulance - Air $200 $150
10B Transportation Not covered Not covered
11A DME
POV, scooters, power wheelchairs, air
fluidized beds - $100
all other DME-$0
POV, scooters, power wheelchairs, air
fluidized beds - 20%
all other DME-$0
11B Prosthetics $0 $0
11B Medical Supplies $0 $0
11C
Diabetic Supplies
Coverage of meters and supplies is limited to
preferred manufacturers. Non-preferred brand
diabetic test strips & monitors are not covered.
Members are eligible for one glucose monitor
every two years and 200 glucose test strips per
30-day period. (Not applicable for Lacera)
$0 $0
11C Diabetic Therapeutic Shoes or Inserts $0 $0
12 Renal Dialysis $30 $25
13A Acupuncture and Other Therapies Not covered Not covered
13B OTC Items (Max Monthly Coverage) Not covered Not covered
13B
Does unused max coverage amount carry
forward to next period?
Not covered Not covered
13C Meal Benefit Not covered Not covered
13C How many weeks does your Meal Benefit last?
Not covered Not covered
13C
What is the maximum number of meals the
benefit provides?
Not covered Not covered
13D/E/F Home Safety Devices benefit (max coverage)
Not covered Not covered
13D/E/F Healthy Rewards/Choices Not covered Not covered
13D/E/F Additional Medical Nutritional Therapy Not covered Not covered
14A Medicare Covered Preventive services $0 $0
14B Annual Physical Exam Not covered Not covered
14C Health Education Not covered Not covered
14C Nutritional/Dietary Benefit* Not covered Not covered
14C Additional Smoking & Tobacco Use Cessation
Not covered Not covered
14C Fitness Benefit* (Silver & Fit) $0 $0
14C Enhanced Disease Management Not covered Not covered
14C Tele-Monitoring Services* Not covered Not covered
14C
Remote Access Technologies (including Web/
Phone Based Technologies & Nursing Hotline)*
$0 $0
14C Bathroom Safety Devices* Not covered Not covered
14C Counseling Services Not covered Not covered
14C In-Home Safety Assessment Not covered Not covered
Page 2 of 20
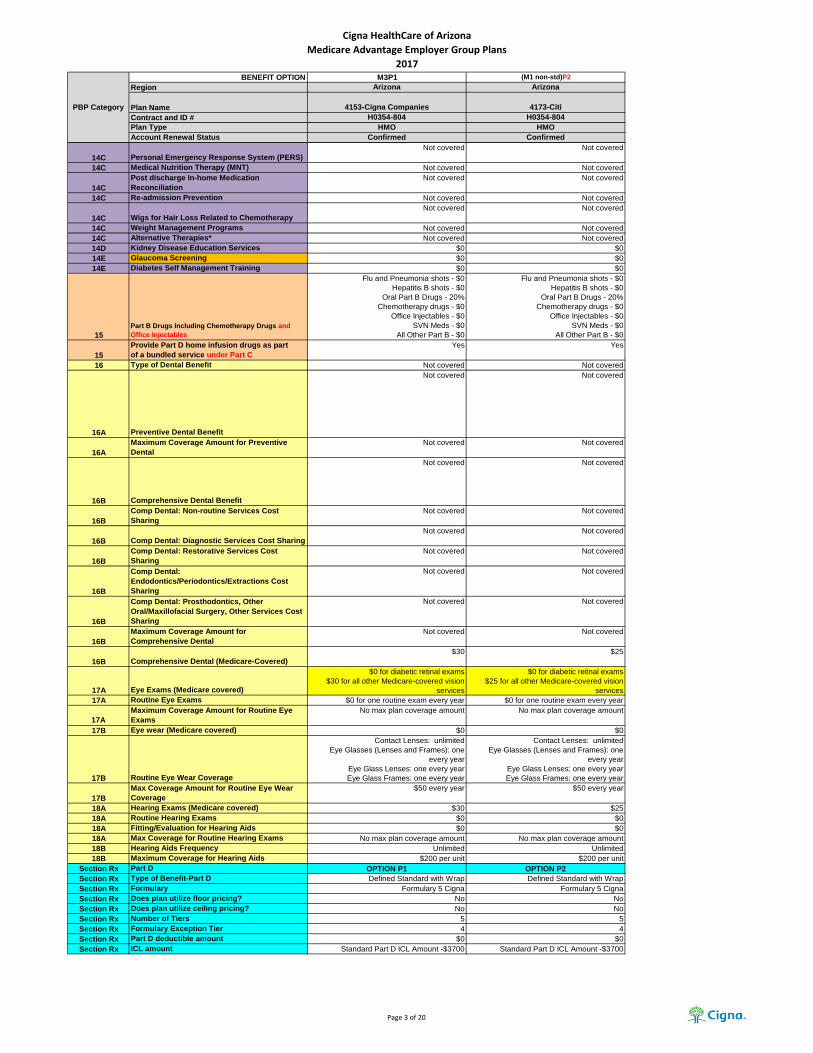
Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION M3P1 (M1 non-std)P2
Region Arizona Arizona
Plan Name 4153-Cigna Companies 4173-Citi
Contract and ID # H0354-804 H0354-804
Plan Type HMO HMO
Account Renewal Status Confirmed Confirmed
PBP Category
14C Personal Emergency Response System (PERS)
Not covered Not covered
14C Medical Nutrition Therapy (MNT) Not covered Not covered
14C
Post discharge In-home Medication
Reconciliation
Not covered Not covered
14C Re-admission Prevention Not covered Not covered
14C Wigs for Hair Loss Related to Chemotherapy
Not covered Not covered
14C Weight Management Programs Not covered Not covered
14C Alternative Therapies* Not covered Not covered
14D Kidney Disease Education Services $0 $0
14E Glaucoma Screening $0 $0
14E Diabetes Self Management Training $0 $0
15
Part B Drugs Including Chemotherapy Drugs and
Office Injectables
Flu and Pneumonia shots - $0
Hepatitis B shots - $0
Oral Part B Drugs - 20%
Chemotherapy drugs - $0
Office Injectables - $0
SVN Meds - $0
All Other Part B - $0
Flu and Pneumonia shots - $0
Hepatitis B shots - $0
Oral Part B Drugs - 20%
Chemotherapy drugs - $0
Office Injectables - $0
SVN Meds - $0
All Other Part B - $0
15
Provide Part D home infusion drugs as part
of a bundled service under Part C
Yes Yes
16 Type of Dental Benefit Not covered Not covered
16A Preventive Dental Benefit
Not covered Not covered
16A
Maximum Coverage Amount for Preventive
Dental
Not covered Not covered
16B Comprehensive Dental Benefit
Not covered Not covered
16B
Comp Dental: Non-routine Services Cost
Sharing
Not covered Not covered
16B Comp Dental: Diagnostic Services Cost Sharing
Not covered Not covered
16B
Comp Dental: Restorative Services Cost
Sharing
Not covered Not covered
16B
Comp Dental:
Endodontics/Periodontics/Extractions Cost
Sharing
Not covered Not covered
16B
Comp Dental: Prosthodontics, Other
Oral/Maxillofacial Surgery, Other Services Cost
Sharing
Not covered Not covered
16B
Maximum Coverage Amount for
Comprehensive Dental
Not covered Not covered
16B Comprehensive Dental (Medicare-Covered)
$30 $25
17A Eye Exams (Medicare covered)
$0 for diabetic retinal exams
$30 for all other Medicare-covered vision
services
$0 for diabetic retinal exams
$25 for all other Medicare-covered vision
services
17A Routine Eye Exams $0 for one routine exam every year $0 for one routine exam every year
17A
Maximum Coverage Amount for Routine Eye
Exams
No max plan coverage amount No max plan coverage amount
17B Eye wear (Medicare covered) $0 $0
17B Routine Eye Wear Coverage
Contact Lenses: unlimited
Eye Glasses (Lenses and Frames): one
every year
Eye Glass Lenses: one every year
Eye Glass Frames: one every year
Contact Lenses: unlimited
Eye Glasses (Lenses and Frames): one
every year
Eye Glass Lenses: one every year
Eye Glass Frames: one every year
17B
Max Coverage Amount for Routine Eye Wear
Coverage
$50 every year $50 every year
18A Hearing Exams (Medicare covered) $30 $25
18A Routine Hearing Exams $0 $0
18A Fitting/Evaluation for Hearing Aids $0 $0
18A Max Coverage for Routine Hearing Exams No max plan coverage amount No max plan coverage amount
18B Hearing Aids Frequency Unlimited Unlimited
18B Maximum Coverage for Hearing Aids $200 per unit $200 per unit
Section Rx Part D OPTION P1 OPTION P2
Section Rx Type of Benefit-Part D Defined Standard with Wrap Defined Standard with Wrap
Section Rx Formulary Formulary 5 Cigna Formulary 5 Cigna
Section Rx Does plan utilize floor pricing? No No
Section Rx Does plan utilize ceiling pricing? No No
Section Rx Number of Tiers 5 5
Section Rx Formulary Exception Tier 4 4
Section Rx Part D deductible amount $0 $0
Section Rx ICL amount Standard Part D ICL Amount -$3700 Standard Part D ICL Amount -$3700
Page 3 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION M3P1 (M1 non-std)P2
Region Arizona Arizona
Plan Name 4153-Cigna Companies 4173-Citi
Contract and ID # H0354-804 H0354-804
Plan Type HMO HMO
Account Renewal Status Confirmed Confirmed
PBP Category
Section Rx Tier Label Description
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drug
Tier 5: Specialty
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drug
Tier 5: Specialty
Section Rx Tier Drug Types
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Non-Preferred Generic and Preferred
Brand
Tier 4: Non-Preferred Generic and Non-
Preferred Brand
Tier 5: Generic and Brand
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Non-Preferred Generic and Preferred
Brand
Tier 4: Non-Preferred Generic and Non-
Preferred Brand
Tier 5: Generic and Brand
Section Rx
Standard Retail Pharmacy Cost Share – Daily
Supply
Tier 1: $0.16
Tier 2: $0.50
Tier 3: $1.40
Tier 4: $3.17
Tier 1: $0.00
Tier 2: $0.33
Tier 3: $1.50
Tier 4: $3.17
Section Rx
Standard Retail Pharmacy Cost Share – One
Month Supply
Tier 1: $5
Tier 2: $15
Tier 3: $42
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Section Rx
Standard Retail Pharmacy Cost Share – Two
Month Supply
Tier 1: $10
Tier 2: $30
Tier 3: $84
Tier 4: $190
Tier 5: Not Available
Tier 1: $0
Tier 2: $20
Tier 3: $90
Tier 4: $190
Tier 5: Not Available
Section Rx
Standard Retail Pharmacy Cost Share – Three
Month Supply
Tier 1: $15
Tier 2: $45
Tier 3: $126
Tier 4: $285
Tier 5: Not Available
Tier 1: $0
Tier 2: $30
Tier 3: $135
Tier 4: $285
Tier 5: Not Available
Page 4 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION M3P1 (M1 non-std)P2
Region Arizona Arizona
Plan Name 4153-Cigna Companies 4173-Citi
Contract and ID # H0354-804 H0354-804
Plan Type HMO HMO
Account Renewal Status Confirmed Confirmed
PBP Category
Section Rx
Preferred Retail Pharmacy Cost Share – Daily
supply
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Section Rx
Preferred Retail Pharmacy Cost Share – One
Month Supply
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Section Rx
Preferred Retail Pharmacy Cost Share – Two
Month Supply
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Section Rx
Preferred Retail Pharmacy Cost Share – Three
Month Supply
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Section Rx Retail Pharmacy days supply
30 days for one month supply
60 days for two month supply
90 days for three month supply
(60 and 90 day excludes Tier 5)
30 days for one month supply
60 days for two month supply
90 days for three month supply
(60 and 90 day excludes Tier 5)
Section Rx
Standard Mail Order Pharmacy Cost Share –
Daily Supply
Tier 1: $0.16
Tier 2: $0.50
Tier 3: $1.40
Tier 4: $3.17
Tier 1: $0.00
Tier 2: $0.33
Tier 3: $1.50
Tier 4: $3.17
Section Rx
Standard Mail Order Pharmacy Cost Share -
One Month Supply
Tier 1: $5
Tier 2: $15
Tier 3: $42
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Section Rx
Standard Mail Order Pharmacy Cost Share –
Three Month Supply
Tier 1: $15
Tier 2: $45
Tier 3: $126
Tier 4: $285
Tier 5: Not Available
Tier 1: $0
Tier 2: $30
Tier 3: $135
Tier 4: $285
Tier 5: Not Available
Section Rx Standard Mail Order Pharmacy Days Supply
30 days for a one month supply
90 days for three month supply
(90 day excludes Tier 5)
30 days for a one month supply
90 days for three month supply
(90 day excludes Tier 5)
Section Rx Out of Network Pharmacy Cost Share
Tier 1: $5
Tier 2: $15
Tier 3: $42
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Section Rx Out of Network Pharmacy Days Supply 30 days for one month supply 30 days for one month supply
Section Rx LTC Pharmacy Cost Share – Daily Supply
Tier 1: $0.00
Tier 2: $0.48
Tier 3: $1.35
Tier 4: $3.06
Tier 1: $0.00
Tier 2: $0.32
Tier 3: $1.45
Tier 4: $3.06
Section Rx LTC Pharmacy Cost Share – One Month Supply
Tier 1: $5
Tier 2: $15
Tier 3: $42
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Section Rx LTC Pharmacy days supply 31 days for one month supply 31 days for one month supply
Section Rx Gap coverage Not covered All tiers: Full coverage
Section Rx OOP Threshhold TypeMedicare-defined post threshold cost shares -
$4950
Medicare-defined post threshold cost shares -
$4950
Section Rx OOP Threshhold Tiers All Tiers All Tiers
Page 5 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
Section A Counties
N/A In/Out of Network Indicator
N/A Total Premium
N/A Optional Supplemental Premium - Package 1
N/A Optional Supplemental Premium - Package 2
N/A Part B Premium Buy Down
Section C Max Plan Coverage Amount for OON
Section C
Does this POS benefit service the United States
and its territories?
Section C
Does this POS benefit include all practitioners
who are state-licensed or state-certified to
furnish the services?
Section D Maximum Out-of-Pocket Cost (MOOP)
Section D Part A/B deductible
1A IP-Acute Cost Sharing Varying by Hospital
1A Number of Tiers for IP-Acute (Max of 3)
1A Lowest Tier of Cost Sharing for IP-Acute
1A IP-Acute cost sharing
1A IP-Acute Additional Days
1A
Medicare defined benefit period applies to IP-
Acute cost sharing
1A
Other benefit period applies to IP-Acute cost
sharing
1A
Cost sharing applies on day of IP-Acute
discharge
1B IP-Psychiatric Cost Sharing Varying by Hospital
1B Number of Tiers for IP-Psychiatric (Max of 3)
1B Lowest Tier of Cost Sharing for IP-Psychiatric
1B
IP-Psychiatric cost sharing
-includes stays in the psych wing of an acute hospital
-includes inpatient substance abuse treatment
(Lifetime days limit does not apply to mental
health/substance abuse stays in a psych wing of an
acute hospital.)
1B IP-Psychiatric Additional Days
1B
Medicare defined benefit period applies to IP-
Psychiatric cost sharing
1B
Other benefit period applies to IP-Psychiatric
cost sharing
1B
Cost sharing applies on day of IP-Psychiatric
discharge
2 Skilled Nursing Facility (SNF)
2 SNF Additional Days
2
Medicare defined benefit period applies to SNF
cost sharing
2
Other benefit period applies to SNF cost
sharing
2 Cost sharing applies on day of SNF discharge
3 Cardiac Rehab services
3 Intensive Cardiac Rehab services
3 Pulmonary Rehab services
4A ER
4A
Days or Hours within which admission must
occur for ER copay to be waived
4B Urgently Needed Services
4B
Days or Hours within which admission must
occur for Urgently Needed Services copay to be
waived
4C Worldwide Emergency/Urgent Coverage
4C
Does this benefit include emergency
transportation?
4C
Maximum Coverage amount for ER- Worldwide
Coverage
4C
Is the service-specific Maximum Plan Benefit
Coverage amount unlimited?
4C
Is this copay waived for worldwide coverage if
admitted to the hospital?
5
Partial Hospitalization (includes intensive outpatient
mental health treatment-auth required)
6 Home Health
7A Primary Care Physician
7B Chiropractic (Medicare Covered)
PBP Category
M3P3 M4P3
Arizona Arizona
4178-City of New York 4100-Honeywell
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
Maricopa, Pinal (Partial) Maricopa, Pinal (Partial)
INN INN
N/A N/A
N/A N/A
N/A N/A
N/A N/A
N/A N/A
N/A N/A
$5,500 which applies to in-network Medicare-
covered and in-network non-Medicare-
covered benefits
$5,500 which applies to in-network Medicare-
covered and in-network non-Medicare-
covered benefits
N/A N/A
No No
1 1
1 1
$150 per day for days 1-7
$0 per day for days 8-90
$0 per admission
Yes; Unlimited Yes; Unlimited
No No
No No
No No
No No
1 1
1 1
$155 per day for days 1-8
$0 per day for days 9-90
190 days lifetime maximum
$0 per admission
190 days lifetime maximum
Not covered Not covered
No No
No No
No No
$0 per day for days 1-20
$0 per day for days 21-100
$0 per day for days 1-20
$0 per day for days 21-100
Not covered Not covered
Yes Yes
Yes Yes
No No
$30 $12
$30 $12
$30 $12
$75 $75
24 Hours 24 Hours
$25 $25
24 Hours 24 Hours
$75 $75
Yes, Emergency transportation must be
medically necessary.
Yes, Emergency transportation must be
medically necessary.
$50,000 $50,000
No No
Yes Yes
$30 $12
$0 $0
$0 $0
$20 $12
Page 6 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
7B Routine Chiropractic
7C Occupational Therapy
7D Physician Specialist
7E
Mental Health-Individual sessions (includes intensive
outpatient mental health treatment-auth required)
7E
Mental Health-Group sessions (includes intensive
outpatient mental health treatment-auth required)
7F Podiatry (Medicare Covered)
7F Routine Podiatry
7G
Other Health Care (Physician Assistants, Nurse
Practitioners, etc..)
7H Psychiatric-Individual
7H Psychiatric-Group
7I PT and SP
8A Diagnostic Procedures/Tests
8A Lab Services
8B Diagnostic Radiological Services (MRI, CT, PET)
8B Therapeutic Radiological Services (radiation therapy)
8B X-Ray Services
9A Hospital Outpatient Services
9B Ambulatory Surgical Center (ASC)
9C
OP Substance Abuse-Individual (includes intensive
outpatient treatment-auth required)
9C
OP Substance Abuse-Group (includes intensive
outpatient treatment-auth required)
9D Outpatient Blood Services
10A Ambulance - Ground
10A Ambulance - Air
10B Transportation
11A DME
11B Prosthetics
11B Medical Supplies
11C
Diabetic Supplies
Coverage of meters and supplies is limited to
preferred manufacturers. Non-preferred brand
diabetic test strips & monitors are not covered.
Members are eligible for one glucose monitor
every two years and 200 glucose test strips per
30-day period. (Not applicable for Lacera)
11C Diabetic Therapeutic Shoes or Inserts
12 Renal Dialysis
13A Acupuncture and Other Therapies
13B OTC Items (Max Monthly Coverage)
13B
Does unused max coverage amount carry
forward to next period?
13C Meal Benefit
13C How many weeks does your Meal Benefit last?
13C
What is the maximum number of meals the
benefit provides?
13D/E/F Home Safety Devices benefit (max coverage)
13D/E/F Healthy Rewards/Choices
13D/E/F Additional Medical Nutritional Therapy
14A Medicare Covered Preventive services
14B Annual Physical Exam
14C Health Education
14C Nutritional/Dietary Benefit*
14C Additional Smoking & Tobacco Use Cessation
14C Fitness Benefit* (Silver & Fit)
14C Enhanced Disease Management
14C Tele-Monitoring Services*
14C
Remote Access Technologies (including Web/
Phone Based Technologies & Nursing Hotline)*
14C Bathroom Safety Devices*
14C Counseling Services
14C In-Home Safety Assessment
M3P3 M4P3
Arizona Arizona
4178-City of New York 4100-Honeywell
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
$20 per visit for up to 12 routine visits per
year
$12 per visit for up to 12 routine visits per
year
$30 $12
$30 $12
$30 $12
$30 $12
$30 $12
$30 $12
In PCP office - $0
In Specialist office - $30
In PCP office - $0
In Specialist office - $12
$30 $12
$30 $12
$30 $12
$0 $0
$0 $0
mammography and ultrasound-$0
GMG/ASC/HospOP - $125
non-cardiac nuclear studies - $0
cardiac nuclear studies - $30
mammography and ultrasound-$0
CMG/ASC/HospOP - $125
non-cardiac nuclear studies - $0
cardiac nuclear studies - $12
routine stress test - $12
$0 $12
$0 $0
$0 for colorectal screenings
$30 for HospOP nonSurgical
$100 for HospOP Surgical
$0 for colorectal screenings
All else-$12
$0 for colorectal screenings
All else-$75
$0 for colorectal screenings
All else-$12
$30 $12
$30 $12
$0 with deductible waived for first three pints $0 with deductible waived for first three pints
$200 $0
$200 $0
Not covered Not covered
POV, scooters, power wheelchairs, air
fluidized beds - $100
all other DME-$0
$0
$0 $0
$0 $0
$0 $0
$0 $0
$30 $12
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$0 $0
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$0 $0
Not covered Not covered
Not covered Not covered
$0 $0
Not covered Not covered
Not covered Not covered
Not covered Not covered
Page 7 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
14C Personal Emergency Response System (PERS)
14C Medical Nutrition Therapy (MNT)
14C
Post discharge In-home Medication
Reconciliation
14C Re-admission Prevention
14C Wigs for Hair Loss Related to Chemotherapy
14C Weight Management Programs
14C Alternative Therapies*
14D Kidney Disease Education Services
14E Glaucoma Screening
14E Diabetes Self Management Training
15
Part B Drugs Including Chemotherapy Drugs and
Office Injectables
15
Provide Part D home infusion drugs as part
of a bundled service under Part C
16 Type of Dental Benefit
16A Preventive Dental Benefit
16A
Maximum Coverage Amount for Preventive
Dental
16B Comprehensive Dental Benefit
16B
Comp Dental: Non-routine Services Cost
Sharing
16B Comp Dental: Diagnostic Services Cost Sharing
16B
Comp Dental: Restorative Services Cost
Sharing
16B
Comp Dental:
Endodontics/Periodontics/Extractions Cost
Sharing
16B
Comp Dental: Prosthodontics, Other
Oral/Maxillofacial Surgery, Other Services Cost
Sharing
16B
Maximum Coverage Amount for
Comprehensive Dental
16B Comprehensive Dental (Medicare-Covered)
17A Eye Exams (Medicare covered)
17A Routine Eye Exams
17A
Maximum Coverage Amount for Routine Eye
Exams
17B Eye wear (Medicare covered)
17B Routine Eye Wear Coverage
17B
Max Coverage Amount for Routine Eye Wear
Coverage
18A Hearing Exams (Medicare covered)
18A Routine Hearing Exams
18A Fitting/Evaluation for Hearing Aids
18A Max Coverage for Routine Hearing Exams
18B Hearing Aids Frequency
18B Maximum Coverage for Hearing Aids
Section Rx Part D
Section Rx Type of Benefit-Part D
Section Rx Formulary
Section Rx Does plan utilize floor pricing?
Section Rx Does plan utilize ceiling pricing?
Section Rx Number of Tiers
Section Rx Formulary Exception Tier
Section Rx Part D deductible amount
Section Rx ICL amount
M3P3 M4P3
Arizona Arizona
4178-City of New York 4100-Honeywell
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$0 $0
$0 $0
$0 $0
Flu and Pneumonia shots - $0
Hepatitis B shots - $0
Oral Part B Drugs - 20%
Chemotherapy drugs - $0
Office Injectables - $0
SVN Meds - $0
All Other Part B - $0
Flu and Pneumonia shots - $0
Hepatitis B shots - $0
Oral Part B Drugs - 20%
Chemotherapy drugs - $0
Office Injectables - $0
SVN Meds - $0
All Other Part B - $0
Yes Yes
Not covered Preventive and Comprehensive Dental
Not covered Oral exam: four every year
Cleaning: two every year
Bitewing x-ray: one every year
Full mouth & panoramic x-ray: one every
three years
$5 per office visit - see notes for other cost
sharing
Not covered
No max plan coverage amount
Not covered Diagnostic Services: unlimited;
Restorative Services: unlimited;
Endodontics/Periodontics/Extractions:
unlimited;
Prosthodontics/Oral Surgery: unlimited;
Not covered
Not covered
Not covered
$0-$240
Not covered
$0-$115
Not covered
$12-$430
Not covered
$0-$2,376
Not covered
No max plan coverage amount
$30 $12
$0 for diabetic retinal exams
$30 for all other Medicare-covered vision
services
$0 for diabetic retinal exams
$12 for all other Medicare-covered vision
services
$0 for one routine exam every year $0 for one routine exam every year
No max plan coverage amount No max plan coverage amount
$0 $0
Contact Lenses: unlimited
Eye Glasses (Lenses and Frames): one
every year
Eye Glass Lenses: one every year
Eye Glass Frames: one every year
Contact Lenses: unlimited
Eye Glasses (Lenses and Frames): one
every year
Eye Glass Lenses: one every year
Eye Glass Frames: one every year
$50 every year $50 every year
$30 $12
$0 $0
$0 $0
No max plan coverage amount No max plan coverage amount
Unlimited Unlimited
$200 per unit $200 per unit
OPTION P3 OPTION P3
Defined Standard with Wrap Defined Standard with Wrap
Formulary 5 Cigna Formulary 5 Cigna
No No
No No
5 5
4 4
$0 $0
Standard Part D ICL Amount -$3700 Standard Part D ICL Amount -$3700
Page 8 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
Section Rx Tier Label Description
Section Rx Tier Drug Types
Section Rx
Standard Retail Pharmacy Cost Share – Daily
Supply
Section Rx
Standard Retail Pharmacy Cost Share – One
Month Supply
Section Rx
Standard Retail Pharmacy Cost Share – Two
Month Supply
Section Rx
Standard Retail Pharmacy Cost Share – Three
Month Supply
M3P3 M4P3
Arizona Arizona
4178-City of New York 4100-Honeywell
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drug
Tier 5: Specialty
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drug
Tier 5: Specialty
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Non-Preferred Generic and Preferred
Brand
Tier 4: Non-Preferred Generic and Non-
Preferred Brand
Tier 5: Generic and Brand
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Non-Preferred Generic and Preferred
Brand
Tier 4: Non-Preferred Generic and Non-
Preferred Brand
Tier 5: Generic and Brand
Tier 1: $0.00
Tier 2: $0.16
Tier 3: $1.00
Tier 4: $1.00
Tier 5: $1.00
Tier 1: $0.00
Tier 2: $0.16
Tier 3: $1.00
Tier 4: $1.00
Tier 5: $1.00
Tier 1: $0
Tier 2: $5
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $5
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $10
Tier 3: $60
Tier 4: $60
Tier 5: Not Available
Tier 1: $0
Tier 2: $10
Tier 3: $60
Tier 4: $60
Tier 5: Not Available
Tier 1: $0
Tier 2: $15
Tier 3: $90
Tier 4: $90
Tier 5: Not Available
Tier 1: $0
Tier 2: $15
Tier 3: $90
Tier 4: $90
Tier 5: Not Available
Page 9 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
Section Rx
Preferred Retail Pharmacy Cost Share – Daily
supply
Section Rx
Preferred Retail Pharmacy Cost Share – One
Month Supply
Section Rx
Preferred Retail Pharmacy Cost Share – Two
Month Supply
Section Rx
Preferred Retail Pharmacy Cost Share – Three
Month Supply
Section Rx Retail Pharmacy days supply
Section Rx
Standard Mail Order Pharmacy Cost Share –
Daily Supply
Section Rx
Standard Mail Order Pharmacy Cost Share -
One Month Supply
Section Rx
Standard Mail Order Pharmacy Cost Share –
Three Month Supply
Section Rx Standard Mail Order Pharmacy Days Supply
Section Rx Out of Network Pharmacy Cost Share
Section Rx Out of Network Pharmacy Days Supply
Section Rx LTC Pharmacy Cost Share – Daily Supply
Section Rx LTC Pharmacy Cost Share – One Month Supply
Section Rx LTC Pharmacy days supply
Section Rx Gap coverage
Section Rx OOP Threshhold Type
Section Rx OOP Threshhold Tiers
M3P3 M4P3
Arizona Arizona
4178-City of New York 4100-Honeywell
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
30 days for one month supply
60 days for two month supply
90 days for three month supply
(60 and 90 day excludes Tier 5)
30 days for one month supply
60 days for two month supply
90 days for three month supply
(60 and 90 day excludes Tier 5)
Tier 1: $0.00
Tier 2: $0.16
Tier 3: $1.00
Tier 4: $1.00
Tier 5: $1.00
Tier 1: $0.00
Tier 2: $0.16
Tier 3: $1.00
Tier 4: $1.00
Tier 5: $1.00
Tier 1: $0
Tier 2: $5
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $5
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $15
Tier 3: $90
Tier 4: $90
Tier 5: Not Available
Tier 1: $0
Tier 2: $15
Tier 3: $90
Tier 4: $90
Tier 5: Not Available
30 days for a one month supply
90 days for three month supply
(90 day excludes Tier 5)
30 days for a one month supply
90 days for three month supply
(90 day excludes Tier 5)
Tier 1: $0
Tier 2: $5
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $5
Tier 3: $30
Tier 4: $30
Tier 5: $30
30 days for one month supply 30 days for one month supply
Tier 1: $0.00
Tier 2: $0.16
Tier 3: $0.97
Tier 4: $0.97
Tier 5: $0.97
Tier 1: $0.00
Tier 2: $0.16
Tier 3: $0.97
Tier 4: $0.97
Tier 5: $0.97
Tier 1: $0
Tier 2: $5
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $5
Tier 3: $30
Tier 4: $30
Tier 5: $30
31 days for one month supply 31 days for one month supply
All tiers: Full coverage All tiers: Full coverage
Medicare-defined post threshold cost shares -
$4950
Medicare-defined post threshold cost shares -
$4950
All Tiers All Tiers
Page 10 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
Section A Counties
N/A In/Out of Network Indicator
N/A Total Premium
N/A Optional Supplemental Premium - Package 1
N/A Optional Supplemental Premium - Package 2
N/A Part B Premium Buy Down
Section C Max Plan Coverage Amount for OON
Section C
Does this POS benefit service the United States
and its territories?
Section C
Does this POS benefit include all practitioners
who are state-licensed or state-certified to
furnish the services?
Section D Maximum Out-of-Pocket Cost (MOOP)
Section D Part A/B deductible
1A IP-Acute Cost Sharing Varying by Hospital
1A Number of Tiers for IP-Acute (Max of 3)
1A Lowest Tier of Cost Sharing for IP-Acute
1A IP-Acute cost sharing
1A IP-Acute Additional Days
1A
Medicare defined benefit period applies to IP-
Acute cost sharing
1A
Other benefit period applies to IP-Acute cost
sharing
1A
Cost sharing applies on day of IP-Acute
discharge
1B IP-Psychiatric Cost Sharing Varying by Hospital
1B Number of Tiers for IP-Psychiatric (Max of 3)
1B Lowest Tier of Cost Sharing for IP-Psychiatric
1B
IP-Psychiatric cost sharing
-includes stays in the psych wing of an acute hospital
-includes inpatient substance abuse treatment
(Lifetime days limit does not apply to mental
health/substance abuse stays in a psych wing of an
acute hospital.)
1B IP-Psychiatric Additional Days
1B
Medicare defined benefit period applies to IP-
Psychiatric cost sharing
1B
Other benefit period applies to IP-Psychiatric
cost sharing
1B
Cost sharing applies on day of IP-Psychiatric
discharge
2 Skilled Nursing Facility (SNF)
2 SNF Additional Days
2
Medicare defined benefit period applies to SNF
cost sharing
2
Other benefit period applies to SNF cost
sharing
2 Cost sharing applies on day of SNF discharge
3 Cardiac Rehab services
3 Intensive Cardiac Rehab services
3 Pulmonary Rehab services
4A ER
4A
Days or Hours within which admission must
occur for ER copay to be waived
4B Urgently Needed Services
4B
Days or Hours within which admission must
occur for Urgently Needed Services copay to be
waived
4C Worldwide Emergency/Urgent Coverage
4C
Does this benefit include emergency
transportation?
4C
Maximum Coverage amount for ER- Worldwide
Coverage
4C
Is the service-specific Maximum Plan Benefit
Coverage amount unlimited?
4C
Is this copay waived for worldwide coverage if
admitted to the hospital?
5
Partial Hospitalization (includes intensive outpatient
mental health treatment-auth required)
6 Home Health
7A Primary Care Physician
7B Chiropractic (Medicare Covered)
PBP Category
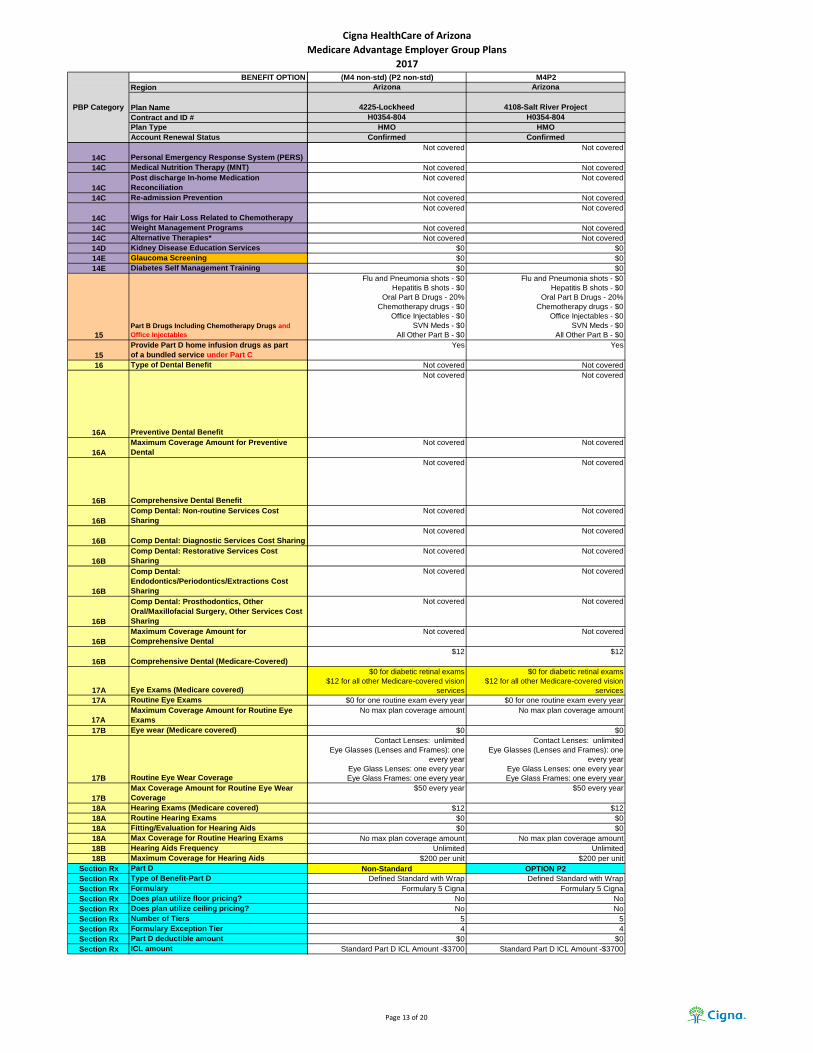
(M4 non-std) (P2 non-std) M4P2
Arizona Arizona
4225-Lockheed 4108-Salt River Project
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
Maricopa, Pinal (Partial) Maricopa, Pinal (Partial)
INN INN
N/A N/A
N/A N/A
N/A N/A
N/A N/A
N/A N/A
N/A N/A
$5,500 which applies to in-network Medicare-
covered and in-network non-Medicare-
covered benefits
$5,500 which applies to in-network Medicare-
covered and in-network non-Medicare-
covered benefits
N/A N/A
No No
1 1
1 1
$250 Per day up to $1,000 Max per
Confinement
$0 per admission
Yes; Unlimited Yes; Unlimited
No No
No No
No No
No No
1 1
1 1
$250 per day up to $1,000 max per
confinement
190 days lifetime maximum
$0 per admission
190 days lifetime maximum
Not covered Not covered
No No
No No
No No
$0 per day for days 1-20
$0 per day for days 21-100
$0 per day for days 1-20
$0 per day for days 21-100
Not covered Not covered
Yes Yes
Yes Yes
No No
$12 $12
$12 $12
$12 $12
$75 $75
24 Hours 24 Hours
$25 $25
24 Hours 24 Hours
$75 $75
Yes, Emergency transportation must be
medically necessary.
Yes, Emergency transportation must be
medically necessary.
$50,000 $50,000
No No
Yes Yes
$12 $12
$0 $0
$0 $0
$12 $12
Page 11 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
7B Routine Chiropractic
7C Occupational Therapy
7D Physician Specialist
7E
Mental Health-Individual sessions (includes intensive
outpatient mental health treatment-auth required)
7E
Mental Health-Group sessions (includes intensive
outpatient mental health treatment-auth required)
7F Podiatry (Medicare Covered)
7F Routine Podiatry
7G
Other Health Care (Physician Assistants, Nurse
Practitioners, etc..)
7H Psychiatric-Individual
7H Psychiatric-Group
7I PT and SP
8A Diagnostic Procedures/Tests
8A Lab Services
8B Diagnostic Radiological Services (MRI, CT, PET)
8B Therapeutic Radiological Services (radiation therapy)
8B X-Ray Services
9A Hospital Outpatient Services
9B Ambulatory Surgical Center (ASC)
9C
OP Substance Abuse-Individual (includes intensive
outpatient treatment-auth required)
9C
OP Substance Abuse-Group (includes intensive
outpatient treatment-auth required)
9D Outpatient Blood Services
10A Ambulance - Ground
10A Ambulance - Air
10B Transportation
11A DME
11B Prosthetics
11B Medical Supplies
11C
Diabetic Supplies
Coverage of meters and supplies is limited to
preferred manufacturers. Non-preferred brand
diabetic test strips & monitors are not covered.
Members are eligible for one glucose monitor
every two years and 200 glucose test strips per
30-day period. (Not applicable for Lacera)
11C Diabetic Therapeutic Shoes or Inserts
12 Renal Dialysis
13A Acupuncture and Other Therapies
13B OTC Items (Max Monthly Coverage)
13B
Does unused max coverage amount carry
forward to next period?
13C Meal Benefit
13C How many weeks does your Meal Benefit last?
13C
What is the maximum number of meals the
benefit provides?
13D/E/F Home Safety Devices benefit (max coverage)
13D/E/F Healthy Rewards/Choices
13D/E/F Additional Medical Nutritional Therapy
14A Medicare Covered Preventive services
14B Annual Physical Exam
14C Health Education
14C Nutritional/Dietary Benefit*
14C Additional Smoking & Tobacco Use Cessation
14C Fitness Benefit* (Silver & Fit)
14C Enhanced Disease Management
14C Tele-Monitoring Services*
14C
Remote Access Technologies (including Web/
Phone Based Technologies & Nursing Hotline)*
14C Bathroom Safety Devices*
14C Counseling Services
14C In-Home Safety Assessment
(M4 non-std) (P2 non-std) M4P2
Arizona Arizona
4225-Lockheed 4108-Salt River Project
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
$12 per visit for up to 12 routine visits per
year
$12 per visit for up to 12 routine visits per
year
$12 $12
$12 $12
$12 $12
$12 $12
$12 $12
$12 $12
In PCP office - $0
In Specialist office - $12
In PCP office - $0
In Specialist office - $12
$12 $12
$12 $12
$12 $12
$0 $0
$0 $0
mammography and ultrasound-$0
CMG/ASC/HospOP - $75
non-cardiac nuclear studies - $0
cardiac nuclear studies - $12
routine stress test - $12
mammography and ultrasound-$0
CMG/ASC/HospOP - $125
non-cardiac nuclear studies - $0
cardiac nuclear studies - $12
routine stress test - $12
$12 $12
$0 $0
$0 for colorectal screenings
All else-$12
$0 for colorectal screenings
All else-$12
$0 for colorectal screenings
All else-$12
$0 for colorectal screenings
All else-$12
$12 $12
$12 $12
$0 with deductible waived for first three pints $0 with deductible waived for first three pints
$0 $0
$0 $0
Not covered Not covered
$0 $0
$0 $0
$0 $0
$0 $0
$0 $0
$12 $12
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$0 $0
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$0 $0
Not covered Not covered
Not covered Not covered
$0 $0
Not covered Not covered
Not covered Not covered
Not covered Not covered
Page 12 of 20
Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
14C Personal Emergency Response System (PERS)
14C Medical Nutrition Therapy (MNT)
14C
Post discharge In-home Medication
Reconciliation
14C Re-admission Prevention
14C Wigs for Hair Loss Related to Chemotherapy
14C Weight Management Programs
14C Alternative Therapies*
14D Kidney Disease Education Services
14E Glaucoma Screening
14E Diabetes Self Management Training
15
Part B Drugs Including Chemotherapy Drugs and
Office Injectables
15
Provide Part D home infusion drugs as part
of a bundled service under Part C
16 Type of Dental Benefit
16A Preventive Dental Benefit
16A
Maximum Coverage Amount for Preventive
Dental
16B Comprehensive Dental Benefit
16B
Comp Dental: Non-routine Services Cost
Sharing
16B Comp Dental: Diagnostic Services Cost Sharing
16B
Comp Dental: Restorative Services Cost
Sharing
16B
Comp Dental:
Endodontics/Periodontics/Extractions Cost
Sharing
16B
Comp Dental: Prosthodontics, Other
Oral/Maxillofacial Surgery, Other Services Cost
Sharing
16B
Maximum Coverage Amount for
Comprehensive Dental
16B Comprehensive Dental (Medicare-Covered)
17A Eye Exams (Medicare covered)
17A Routine Eye Exams
17A
Maximum Coverage Amount for Routine Eye
Exams
17B Eye wear (Medicare covered)
17B Routine Eye Wear Coverage
17B
Max Coverage Amount for Routine Eye Wear
Coverage
18A Hearing Exams (Medicare covered)
18A Routine Hearing Exams
18A Fitting/Evaluation for Hearing Aids
18A Max Coverage for Routine Hearing Exams
18B Hearing Aids Frequency
18B Maximum Coverage for Hearing Aids
Section Rx Part D
Section Rx Type of Benefit-Part D
Section Rx Formulary
Section Rx Does plan utilize floor pricing?
Section Rx Does plan utilize ceiling pricing?
Section Rx Number of Tiers
Section Rx Formulary Exception Tier
Section Rx Part D deductible amount
Section Rx ICL amount
(M4 non-std) (P2 non-std) M4P2
Arizona Arizona
4225-Lockheed 4108-Salt River Project
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$0 $0
$0 $0
$0 $0
Flu and Pneumonia shots - $0
Hepatitis B shots - $0
Oral Part B Drugs - 20%
Chemotherapy drugs - $0
Office Injectables - $0
SVN Meds - $0
All Other Part B - $0
Flu and Pneumonia shots - $0
Hepatitis B shots - $0
Oral Part B Drugs - 20%
Chemotherapy drugs - $0
Office Injectables - $0
SVN Meds - $0
All Other Part B - $0
Yes Yes
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$12 $12
$0 for diabetic retinal exams
$12 for all other Medicare-covered vision
services
$0 for diabetic retinal exams
$12 for all other Medicare-covered vision
services
$0 for one routine exam every year $0 for one routine exam every year
No max plan coverage amount No max plan coverage amount
$0 $0
Contact Lenses: unlimited
Eye Glasses (Lenses and Frames): one
every year
Eye Glass Lenses: one every year
Eye Glass Frames: one every year
Contact Lenses: unlimited
Eye Glasses (Lenses and Frames): one
every year
Eye Glass Lenses: one every year
Eye Glass Frames: one every year
$50 every year $50 every year
$12 $12
$0 $0
$0 $0
No max plan coverage amount No max plan coverage amount
Unlimited Unlimited
$200 per unit $200 per unit
Non-Standard OPTION P2
Defined Standard with Wrap Defined Standard with Wrap
Formulary 5 Cigna Formulary 5 Cigna
No No
No No
5 5
4 4
$0 $0
Standard Part D ICL Amount -$3700 Standard Part D ICL Amount -$3700
Page 13 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
Section Rx Tier Label Description
Section Rx Tier Drug Types
Section Rx
Standard Retail Pharmacy Cost Share – Daily
Supply
Section Rx
Standard Retail Pharmacy Cost Share – One
Month Supply
Section Rx
Standard Retail Pharmacy Cost Share – Two
Month Supply
Section Rx
Standard Retail Pharmacy Cost Share – Three
Month Supply
(M4 non-std) (P2 non-std) M4P2
Arizona Arizona
4225-Lockheed 4108-Salt River Project
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drug
Tier 5: Specialty
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drug
Tier 5: Specialty
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Non-Preferred Generic and Preferred
Brand
Tier 4: Non-Preferred Generic and Non-
Preferred Brand
Tier 5: Generic and Brand
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Non-Preferred Generic and Preferred
Brand
Tier 4: Non-Preferred Generic and Non-
Preferred Brand
Tier 5: Generic and Brand
Tier 1: $0.10
Tier 2: $0.33
Tier 3: $1.00
Tier 4: $1.00
Tier 5: $1.00
Tier 1: $0.00
Tier 2: $0.33
Tier 3: $1.50
Tier 4: $3.17
Tier 1: $3
Tier 2: $10
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Tier 1: $6
Tier 2: $20
Tier 3: $60
Tier 4: $60
Tier 5: Not Available
Tier 1: $0
Tier 2: $20
Tier 3: $90
Tier 4: $190
Tier 5: Not Available
Tier 1: $9
Tier 2: $30
Tier 3: $90
Tier 4: $90
Tier 5: Not Available
Tier 1: $0
Tier 2: $30
Tier 3: $135
Tier 4: $285
Tier 5: Not Available
Page 14 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
Section Rx
Preferred Retail Pharmacy Cost Share – Daily
supply
Section Rx
Preferred Retail Pharmacy Cost Share – One
Month Supply
Section Rx
Preferred Retail Pharmacy Cost Share – Two
Month Supply
Section Rx
Preferred Retail Pharmacy Cost Share – Three
Month Supply
Section Rx Retail Pharmacy days supply
Section Rx
Standard Mail Order Pharmacy Cost Share –
Daily Supply
Section Rx
Standard Mail Order Pharmacy Cost Share -
One Month Supply
Section Rx
Standard Mail Order Pharmacy Cost Share –
Three Month Supply
Section Rx Standard Mail Order Pharmacy Days Supply
Section Rx Out of Network Pharmacy Cost Share
Section Rx Out of Network Pharmacy Days Supply
Section Rx LTC Pharmacy Cost Share – Daily Supply
Section Rx LTC Pharmacy Cost Share – One Month Supply
Section Rx LTC Pharmacy days supply
Section Rx Gap coverage
Section Rx OOP Threshhold Type
Section Rx OOP Threshhold Tiers
(M4 non-std) (P2 non-std) M4P2
Arizona Arizona
4225-Lockheed 4108-Salt River Project
H0354-804 H0354-804
HMO HMO
Confirmed Confirmed
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
30 days for one month supply
60 days for two month supply
90 days for three month supply
(60 and 90 day excludes Tier 5)
30 days for one month supply
60 days for two month supply
90 days for three month supply
(60 and 90 day excludes Tier 5)
Tier 1: $0.10
Tier 2: $0.33
Tier 3: $1.00
Tier 4: $1.00
Tier 5: $1.00
Tier 1: $0.00
Tier 2: $0.33
Tier 3: $1.50
Tier 4: $3.17
Tier 1: $3
Tier 2: $10
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Tier 1: $9
Tier 2: $30
Tier 3: $90
Tier 4: $90
Tier 5: Not Available
Tier 1: $0
Tier 2: $30
Tier 3: $135
Tier 4: $285
Tier 5: Not Available
30 days for a one month supply
90 days for three month supply
(90 day excludes Tier 5)
30 days for a one month supply
90 days for three month supply
(90 day excludes Tier 5)
Tier 1: $3
Tier 2: $10
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
30 days for one month supply 30 days for one month supply
Tier 1: $0.10
Tier 2: $0.32
Tier 3: $0.97
Tier 4: $0.97
Tier 5: $0.97
Tier 1: $0.00
Tier 2: $0.32
Tier 3: $1.45
Tier 4: $3.06
Tier 1: $3
Tier 2: $10
Tier 3: $30
Tier 4: $30
Tier 5: $30
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
31 days for one month supply 31 days for one month supply
All tiers: Full coverage All tiers: Full coverage
Medicare-defined post threshold cost shares -
$4950
Medicare-defined post threshold cost shares -
$4950
All Tiers All Tiers
Page 15 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
Section A Counties
N/A In/Out of Network Indicator
N/A Total Premium
N/A Optional Supplemental Premium - Package 1
N/A Optional Supplemental Premium - Package 2
N/A Part B Premium Buy Down
Section C Max Plan Coverage Amount for OON
Section C
Does this POS benefit service the United States
and its territories?
Section C
Does this POS benefit include all practitioners
who are state-licensed or state-certified to
furnish the services?
Section D Maximum Out-of-Pocket Cost (MOOP)
Section D Part A/B deductible
1A IP-Acute Cost Sharing Varying by Hospital
1A Number of Tiers for IP-Acute (Max of 3)
1A Lowest Tier of Cost Sharing for IP-Acute
1A IP-Acute cost sharing
1A IP-Acute Additional Days
1A
Medicare defined benefit period applies to IP-
Acute cost sharing
1A
Other benefit period applies to IP-Acute cost
sharing
1A
Cost sharing applies on day of IP-Acute
discharge
1B IP-Psychiatric Cost Sharing Varying by Hospital
1B Number of Tiers for IP-Psychiatric (Max of 3)
1B Lowest Tier of Cost Sharing for IP-Psychiatric
1B
IP-Psychiatric cost sharing
-includes stays in the psych wing of an acute hospital
-includes inpatient substance abuse treatment
(Lifetime days limit does not apply to mental
health/substance abuse stays in a psych wing of an
acute hospital.)
1B IP-Psychiatric Additional Days
1B
Medicare defined benefit period applies to IP-
Psychiatric cost sharing
1B
Other benefit period applies to IP-Psychiatric
cost sharing
1B
Cost sharing applies on day of IP-Psychiatric
discharge
2 Skilled Nursing Facility (SNF)
2 SNF Additional Days
2
Medicare defined benefit period applies to SNF
cost sharing
2
Other benefit period applies to SNF cost
sharing
2 Cost sharing applies on day of SNF discharge
3 Cardiac Rehab services
3 Intensive Cardiac Rehab services
3 Pulmonary Rehab services
4A ER
4A
Days or Hours within which admission must
occur for ER copay to be waived
4B Urgently Needed Services
4B
Days or Hours within which admission must
occur for Urgently Needed Services copay to be
waived
4C Worldwide Emergency/Urgent Coverage
4C
Does this benefit include emergency
transportation?
4C
Maximum Coverage amount for ER- Worldwide
Coverage
4C
Is the service-specific Maximum Plan Benefit
Coverage amount unlimited?
4C
Is this copay waived for worldwide coverage if
admitted to the hospital?
5
Partial Hospitalization (includes intensive outpatient
mental health treatment-auth required)
6 Home Health
7A Primary Care Physician
7B Chiropractic (Medicare Covered)
PBP Category
M4P2 M4P2
Arizona Arizona
4185-Viad
4123-Lacera
Contract Jul 1, 2016 - Jun 30, 2017
H0354-804 H0354-805
HMO HMO
Confirmed Confirmed
Maricopa, Pinal (Partial) Maricopa, Pinal (Partial)
INN INN
N/A N/A
N/A N/A
N/A N/A
N/A N/A
N/A N/A
N/A N/A
$5,500 which applies to in-network Medicare-
covered and in-network non-Medicare-
covered benefits
$5,500 which applies to in-network Medicare-
covered and in-network non-Medicare-
covered benefits
N/A N/A
No No
1 1
1 1
$0 per admission $0 per admission
Yes; Unlimited Yes; Unlimited
No No
No No
No No
No No
1 1
1 1
$0 per admission
190 days lifetime maximum
$0 per admission
190 days lifetime maximum
Not covered Not covered
No No
No No
No No
$0 per day for days 1-20
$0 per day for days 21-100
$0 per day for days 1-20
$0 per day for days 21-100
Not covered Not covered
Yes No
Yes Yes
No No
$12 $12
$12 $12
$12 $12
$75 $75
24 Hours 24 Hours
$25 $25
24 Hours 24 Hours
$75 $75
Yes, Emergency transportation must be
medically necessary.
Yes, Emergency transportation must be
medically necessary.
$50,000 No max plan coverage amount
No Yes
Yes Yes
$12 $12
$0 $0
$0 $0
$12 $12
Page 16 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
7B Routine Chiropractic
7C Occupational Therapy
7D Physician Specialist
7E
Mental Health-Individual sessions (includes intensive
outpatient mental health treatment-auth required)
7E
Mental Health-Group sessions (includes intensive
outpatient mental health treatment-auth required)
7F Podiatry (Medicare Covered)
7F Routine Podiatry
7G
Other Health Care (Physician Assistants, Nurse
Practitioners, etc..)
7H Psychiatric-Individual
7H Psychiatric-Group
7I PT and SP
8A Diagnostic Procedures/Tests
8A Lab Services
8B Diagnostic Radiological Services (MRI, CT, PET)
8B Therapeutic Radiological Services (radiation therapy)
8B X-Ray Services
9A Hospital Outpatient Services
9B Ambulatory Surgical Center (ASC)
9C
OP Substance Abuse-Individual (includes intensive
outpatient treatment-auth required)
9C
OP Substance Abuse-Group (includes intensive
outpatient treatment-auth required)
9D Outpatient Blood Services
10A Ambulance - Ground
10A Ambulance - Air
10B Transportation
11A DME
11B Prosthetics
11B Medical Supplies
11C
Diabetic Supplies
Coverage of meters and supplies is limited to
preferred manufacturers. Non-preferred brand
diabetic test strips & monitors are not covered.
Members are eligible for one glucose monitor
every two years and 200 glucose test strips per
30-day period. (Not applicable for Lacera)
11C Diabetic Therapeutic Shoes or Inserts
12 Renal Dialysis
13A Acupuncture and Other Therapies
13B OTC Items (Max Monthly Coverage)
13B
Does unused max coverage amount carry
forward to next period?
13C Meal Benefit
13C How many weeks does your Meal Benefit last?
13C
What is the maximum number of meals the
benefit provides?
13D/E/F Home Safety Devices benefit (max coverage)
13D/E/F Healthy Rewards/Choices
13D/E/F Additional Medical Nutritional Therapy
14A Medicare Covered Preventive services
14B Annual Physical Exam
14C Health Education
14C Nutritional/Dietary Benefit*
14C Additional Smoking & Tobacco Use Cessation
14C Fitness Benefit* (Silver & Fit)
14C Enhanced Disease Management
14C Tele-Monitoring Services*
14C
Remote Access Technologies (including Web/
Phone Based Technologies & Nursing Hotline)*
14C Bathroom Safety Devices*
14C Counseling Services
14C In-Home Safety Assessment
M4P2 M4P2
Arizona Arizona
4185-Viad
4123-Lacera
Contract Jul 1, 2016 - Jun 30, 2017
H0354-804 H0354-805
HMO HMO
Confirmed Confirmed
$12 per visit for up to 12 routine visits per
year
$12 per visit for up to 12 routine visits per
year
$12 $12
$12 $12
$12 $12
$12 $12
$12 $12
$12 $12
In PCP office - $0
In Specialist office - $12
In PCP office - $0
In Specialist office - $12
$12 $12
$12 $12
$12 $12
$0 $0
$0 $0
mammography and ultrasound-$0
CMG/ASC/HospOP - $125
non-cardiac nuclear studies - $0
cardiac nuclear studies - $12
routine stress test - $12
CMG - $100
ASC/HospOP - $150
non-cardiac nuclear studies - $0
cardiac nuclear studies - $12
routine stress test - $12
$12 $12
$0 $0
$0 for colorectal screenings
All else-$12
$12
$0 for colorectal screenings
All else-$12
$12
$12 $12
$12 $12
$0 with deductible waived for first three pints $0 with deductible waived for first three pints
$0 $0
$0 $0
Not covered Not covered
$0 $0
$0 $0
$0 $0
$0 $0
$0 $0
$12 $12
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$0 $0
Not covered $0
Not covered $0
Not covered $0
Not covered Not covered
$0 $0
Not covered Not covered
Not covered Not covered
$0 $0
Not covered Not covered
Not covered Not covered
Not covered Not covered
Page 17 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
14C Personal Emergency Response System (PERS)
14C Medical Nutrition Therapy (MNT)
14C
Post discharge In-home Medication
Reconciliation
14C Re-admission Prevention
14C Wigs for Hair Loss Related to Chemotherapy
14C Weight Management Programs
14C Alternative Therapies*
14D Kidney Disease Education Services
14E Glaucoma Screening
14E Diabetes Self Management Training
15
Part B Drugs Including Chemotherapy Drugs and
Office Injectables
15
Provide Part D home infusion drugs as part
of a bundled service under Part C
16 Type of Dental Benefit
16A Preventive Dental Benefit
16A
Maximum Coverage Amount for Preventive
Dental
16B Comprehensive Dental Benefit
16B
Comp Dental: Non-routine Services Cost
Sharing
16B Comp Dental: Diagnostic Services Cost Sharing
16B
Comp Dental: Restorative Services Cost
Sharing
16B
Comp Dental:
Endodontics/Periodontics/Extractions Cost
Sharing
16B
Comp Dental: Prosthodontics, Other
Oral/Maxillofacial Surgery, Other Services Cost
Sharing
16B
Maximum Coverage Amount for
Comprehensive Dental
16B Comprehensive Dental (Medicare-Covered)
17A Eye Exams (Medicare covered)
17A Routine Eye Exams
17A
Maximum Coverage Amount for Routine Eye
Exams
17B Eye wear (Medicare covered)
17B Routine Eye Wear Coverage
17B
Max Coverage Amount for Routine Eye Wear
Coverage
18A Hearing Exams (Medicare covered)
18A Routine Hearing Exams
18A Fitting/Evaluation for Hearing Aids
18A Max Coverage for Routine Hearing Exams
18B Hearing Aids Frequency
18B Maximum Coverage for Hearing Aids
Section Rx Part D
Section Rx Type of Benefit-Part D
Section Rx Formulary
Section Rx Does plan utilize floor pricing?
Section Rx Does plan utilize ceiling pricing?
Section Rx Number of Tiers
Section Rx Formulary Exception Tier
Section Rx Part D deductible amount
Section Rx ICL amount
M4P2 M4P2
Arizona Arizona
4185-Viad
4123-Lacera
Contract Jul 1, 2016 - Jun 30, 2017
H0354-804 H0354-805
HMO HMO
Confirmed Confirmed
Not covered Not covered
Not covered $0
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$0 $0
$0 $0
$0 $0
Flu and Pneumonia shots - $0
Hepatitis B shots - $0
Oral Part B Drugs - 20%
Chemotherapy drugs - $0
Office Injectables - $0
SVN Meds - $0
All Other Part B - $0
Flu and Pneumonia shots - $0
Hepatitis B shots - $0
Oral Part B Drugs - 20%
Chemotherapy drugs - $0
Office Injectables - $0
SVN Meds - $0
All Other Part B - $0
Yes Yes
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
Not covered Not covered
$12 $12
$0 for diabetic retinal exams
$12 for all other Medicare-covered vision
services
$12
$0 for one routine exam every year $0 for one routine exam every year
No max plan coverage amount No max plan coverage amount
$0 $0
Contact Lenses: unlimited
Eye Glasses (Lenses and Frames): one
every year
Eye Glass Lenses: one every year
Eye Glass Frames: one every year
Contact Lenses: unlimited
Eye Glasses (Lenses and Frames): one
every year
Eye Glass Lenses: one every year
Eye Glass Frames: one every year
$50 every year $50 every year
$12 $12
$0 $0
$0 $0
No max plan coverage amount No max plan coverage amount
Unlimited Unlimited
$200 per unit $200 per unit
OPTION P2
Defined Standard with Wrap Defined Standard with Wrap
Formulary 5 Cigna Formulary 5 Cigna
No No
No No
5 5
4 4
$0 $0
Standard Part D ICL Amount -$3700 Standard Part D ICL Amount -$3310
Page 18 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
Section Rx Tier Label Description
Section Rx Tier Drug Types
Section Rx
Standard Retail Pharmacy Cost Share – Daily
Supply
Section Rx
Standard Retail Pharmacy Cost Share – One
Month Supply
Section Rx
Standard Retail Pharmacy Cost Share – Two
Month Supply
Section Rx
Standard Retail Pharmacy Cost Share – Three
Month Supply
M4P2 M4P2
Arizona Arizona
4185-Viad
4123-Lacera
Contract Jul 1, 2016 - Jun 30, 2017
H0354-804 H0354-805
HMO HMO
Confirmed Confirmed
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drug
Tier 5: Specialty
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Preferred Brand
Tier 4: Non-Preferred Drug
Tier 5: Specialty
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Non-Preferred Generic and Preferred
Brand
Tier 4: Non-Preferred Generic and Non-
Preferred Brand
Tier 5: Generic and Brand
Tier 1: Preferred Generic
Tier 2: Generic
Tier 3: Non-Preferred Generic and Preferred
Brand
Tier 4: Non-Preferred Generic and Non-
Preferred Brand
Tier 5: Generic and Brand
Tier 1: $0.00
Tier 2: $0.33
Tier 3: $1.50
Tier 4: $3.17
Tier 1: $0.00
Tier 2: $0.33
Tier 3: $1.50
Tier 4: $3.17
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $20
Tier 3: $90
Tier 4: $190
Tier 5: Not Available
Tier 1: $0
Tier 2: $20
Tier 3: $90
Tier 4: $190
Tier 5: Not Available
Tier 1: $0
Tier 2: $30
Tier 3: $135
Tier 4: $285
Tier 5: Not Available
Tier 1: $0
Tier 2: $30
Tier 3: $135
Tier 4: $285
Tier 5: Not Available
Page 19 of 20

Cigna HealthCare of Arizona
Medicare Advantage Employer Group Plans
2017BENEFIT OPTION
Region
Plan Name
Contract and ID #
Plan Type
Account Renewal Status
PBP Category
Section Rx
Preferred Retail Pharmacy Cost Share – Daily
supply
Section Rx
Preferred Retail Pharmacy Cost Share – One
Month Supply
Section Rx
Preferred Retail Pharmacy Cost Share – Two
Month Supply
Section Rx
Preferred Retail Pharmacy Cost Share – Three
Month Supply
Section Rx Retail Pharmacy days supply
Section Rx
Standard Mail Order Pharmacy Cost Share –
Daily Supply
Section Rx
Standard Mail Order Pharmacy Cost Share -
One Month Supply
Section Rx
Standard Mail Order Pharmacy Cost Share –
Three Month Supply
Section Rx Standard Mail Order Pharmacy Days Supply
Section Rx Out of Network Pharmacy Cost Share
Section Rx Out of Network Pharmacy Days Supply
Section Rx LTC Pharmacy Cost Share – Daily Supply
Section Rx LTC Pharmacy Cost Share – One Month Supply
Section Rx LTC Pharmacy days supply
Section Rx Gap coverage
Section Rx OOP Threshhold Type
Section Rx OOP Threshhold Tiers
M4P2 M4P2
Arizona Arizona
4185-Viad
4123-Lacera
Contract Jul 1, 2016 - Jun 30, 2017
H0354-804 H0354-805
HMO HMO
Confirmed Confirmed
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
Tier 1: $
Tier 2: $
Tier 3: $
Tier 4: $
30 days for one month supply
60 days for two month supply
90 days for three month supply
(60 and 90 day excludes Tier 5)
30 days for one month supply
60 days for two month supply
90 days for three month supply
(60 and 90 day excludes Tier 5)
Tier 1: $0.00
Tier 2: $0.33
Tier 3: $1.50
Tier 4: $3.17
Tier 1: $0.00
Tier 2: $0.33
Tier 3: $1.50
Tier 4: $3.17
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $30
Tier 3: $135
Tier 4: $285
Tier 5: Not Available
Tier 1: $0
Tier 2: $30
Tier 3: $135
Tier 4: $285
Tier 5: Not Available
30 days for a one month supply
90 days for three month supply
(90 day excludes Tier 5)
30 days for a one month supply
90 days for three month supply
(90 day excludes Tier 5)
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
30 days for one month supply 30 days for one month supply
Tier 1: $0.00
Tier 2: $0.32
Tier 3: $1.45
Tier 4: $3.06
Tier 1: $0.00
Tier 2: $0.32
Tier 3: $1.45
Tier 4: $3.06
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
Tier 1: $0
Tier 2: $10
Tier 3: $45
Tier 4: $95
Tier 5: 33%
31 days for one month supply 31 days for one month supply
All tiers: Full coverage All tiers: Full coverage
Medicare-defined post threshold cost shares -
$4950
Medicare-defined post threshold cost shares -
$4850
All Tiers All Tiers
Preventive services covered under Medicare will have a zero office visit cost share if the only
service being performed during the office visit is the preventive service. If the preventive service is
performed in conjunction with other services in the same office visit, then the applicable office visit
copayment may be charged. Also, the office visit copay may be charged for these services that
are diagnostic in nature (if applicable).
Copays/Coinsurance incurred by customers for covered benefits shown on this chart apply to the out-
of-pocket maximum. Cost incurred for non-covered services are not covered. For example, if a
customer exhausts the SNF days and continues to remain in the facility, costs incurred by the member
for non-covered days in the SNF do not apply to the OOP maximum. Also, Part D copays apply to the
Part D out-of-pocket limit (TrOOP).
Separate Office Visit will apply if diagnostic services provided in conjunction with an office visit. Office
visit copay will not apply if no office visit was incurred.
Copyright© 2017 Cigna HealthCare of Arizona, Inc. all rights reserved. This material may not be
reproduced, in whole or in part, without the expressed written permission of the owner, Cigna
HealthCare of Arizona, Inc. Use and distribution is limited solely to authorized personnel.
Page 20 of 20