cigarette smoking and depression comorbidity: systematic ... · cigarette smoking and depression...
TRANSCRIPT

Cigarette smoking and depression comorbidity:systematic review and proposed theoretical model
Amanda R. Mathew1, Lee Hogarth2, Adam M. Leventhal3, Jessica W. Cook4,5 & Brian Hitsman1
Department of Preventive Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL, USA,1 School of Psychology, University of Exeter, Exeter, UK,2
Departments of Preventive Medicine and Psychology, University of Southern California Keck School of Medicine, Los Angeles, CA, USA,3 University of Wisconsin-Madison School of Medicine and Public Health, Madison, WI, USA4 and William S. Middleton Memorial Veterans Hospital, Madison, WI, USA5
ABSTRACT
Background and Aims Despite decades of research on co-occurring smoking and depression, cessation rates remainconsistently lower for depressed smokers than for smokers in the general population, highlighting the need for theory-drivenmodels of smoking and depression. This paper provides a systematic reviewwith a particular focus upon psycholog-ical states that disproportionately motivate smoking in depression, and frame an incentive learning theory account ofsmoking-depression co-occurrence. Methods We searched PubMed, Scopus, PsychINFO and CINAHL to December2014, which yielded 852 papers. Using pre-established eligibility criteria, we identified papers focused on clinical issuesand motivational mechanisms underlying smoking in established, adult smokers (i.e. maintenance, quit attempts andcessation/relapse) with elevated symptoms of depression. Two reviewers determined independently whether papers metreview criteria. We included 297 papers in qualitative synthesis. Results Our review identified three primary mecha-nisms that underlie persistent smoking among depressed smokers: low positive affect, high negative affect and cognitiveimpairment. We propose a novel application of incentive learning theory which posits that depressed smokers experiencegreater increases in the expected value of smoking in the face of these three motivational states, which promotesgoal-directed choice of smoking behavior over alternative actions. Conclusions The incentive learning theory accountsfor current evidence on how depression primes smoking behavior and provides a unique framework for conceptualizingpsychological mechanisms of smoking maintenance among depressed smokers. Treatment should focus upon correctingadverse internal states and beliefs about the high value of smoking in those states to improve cessation outcomes fordepressed smokers.
Keywords Depression, nicotine dependence, review, smoking, smoking cessation, treatment.
Correspondence to: Amanda R. Mathew, Northwestern University Feinberg School of Medicine, Department of Preventive Medicine, 680 North Lake ShoreDrive, Suite 1400, Chicago, IL 60611, USA. E-mail: [email protected] 22 January 2016; 29 April 2016; final version accepted 5 September 2016
INTRODUCTION
Individuals with depression are more likely to smoke,smoke more cigarettes per day and are less likely to quitsmoking successfully than individuals without depression,and this health disparity is an important clinical and publichealth concern. Recent epidemiological data show that thesmoking rate for clinically depressed individuals is approx-imately twice the rate in the general population [1–6]. Fur-ther, smokers with depression report greater nicotinewithdrawal symptoms [7,8], due in part probably togreater nicotine dependence among depressed versusnon-depressed smokers [9–12]. Although depressedsmokers endorse levels of motivation to quit that are
similar to, or even higher than, smokers in the generalpopulation [13–15] and attempt to quit at similar rates[16], odds of successful abstinence at 1 month are30–50% lower for those with current depression andelevated depressive symptoms [16].
As smoking prevalence continues to decline in thegeneral population, those with mental illness are over-represented increasingly among smokers and constitutean important tobacco use disparity group [17]. Those withmental illness die up to 25 years earlier than those inthe general population, due largely to chronicillnesses associated with smoking (e.g. cardiovascular dis-ease [18–20]). Given that smoking cessation improvesboth mental [21–26] and physical health outcomes [27],
© 2016 Society for the Study of Addiction Addiction
REVIEW doi:10.1111/add.13604

even among smokers with chronic health conditions, de-velopment of smoking cessation interventions targeted tothose with various forms of mental illness (i.e. mood andanxiety disorders, substance use disorders, serious mentalillness) are greatly needed. Herein, we focus our reviewon continuous depressive symptomatology [28–30], rang-ing from subsyndromal levels of depression to clinical disor-ders (i.e. current or past diagnosis of major depression).
Although promising cessation treatments exist (e.g.[31]), no treatment has been shown to attenuate fullythe elevated relapse risk associated with depression, andfurther innovations in treatment development are needed.One major limitation to advances in treatment of comorbidsmoking–depression has been a lack of comprehensivetheories of the psychology of nicotine dependence and de-pression. Identifying the psychological mechanisms thatunderlie smoking persistence among those with elevateddepressive symptoms is critical for (1) a comprehensivecharacterization of the causal connection betweendepression and smoking and (2) developing innovative,theory-based and effective treatment strategies whichtarget these psychological mechanisms specifically indepressed smokers.
This systematic review provides an update of the cur-rent state of evidence on the topic of co-occurring smokingand depression and proposes a novel application of incen-tive learning theory to conceptualize smoking persistenceamong depressed smokers. As detailed below, the incentivelearning account has gained considerable empirical sup-port in the study of drug dependence [32–40], and offersa unique lens through which to view the clinical problemof smoking and depression. In particular, incentivelearning theory proposes that specific states drive goal-directed selection of smoking behavior over alternatechoices for depressed smokers. We believe that the incen-tive learning theory accounts for current evidence onhow depression primes smoking and identifies novelpsychological targets to optimize smoking cessationtreatment for depressed smokers.
MATERIALS AND METHODS
Data sources and searches
We searched the PubMed, Scopus, PsycINFO and CINAHLdatabases to December 2014, using Medical SubjectHeadings or Major Concept search terms when available.We combined smoking-related (i.e. smoking, tobacco,nicotine, smoking cessation, tobacco use, tobacco usedisorder, tobacco use cessation) and depression-relatedterms (i.e. depression, depressive, major depression).Search delimiters were ‘adult’, ‘human’ and ‘Englishlanguage’. We also performed manual searches ofreference lists of pertinent papers.
Study eligibility
Two authors reviewed abstracts and full-text publicationsindependently. Inclusion criteria stipulated that studiesexamine clinical issues relevant to established, adultsmokers (age ≥ 18 years), such as causes and correlatesof smoking maintenance, willingness to quit andcessation/relapse among established smokers, rather thansmoking initiation or progression to regular smoking. Thereview included both current/past major depression andelevated depressive symptoms. Studies not assessingdepression through clinical diagnostic instrument or vali-dated, continuous scale (i.e. by self-reported diagnosis orsingle-item only) were excluded. Studies of specialpopulations of smokers (e.g. psychiatric, medical) withoutmajor depression were excluded. We includedqualitative/quantitative reviews and clinical trial, humanlaboratory-based, observational and epidemiological studydesigns. Non-peer-reviewed publications and case studieswere excluded.
We excluded publications that both reviewers agreeddid not meet eligibility criteria. Authors resolved disagree-ments by consensus.
RESULTS
Results of literature searches
Our searches of databases identified 852 unique citations(Fig. 1). We screened 852 records by abstract and 453full-text papers. Of these, 297 papers were included in thequalitative synthesis. Publications incorporated in thenarrative review were those which contributed mostdirectly to our theoretical framework.
PSYCHOLOGICAL MECHANISMSPROMOTING SMOKING MAINTENANCEAND RELAPSE IN DEPRESSED SMOKERS
Affective processes
While depression is characterized by a wide range of affec-tive, cognitive, behavioral and somatic features [41],evidence is mounting that the affective disturbances indepression may play a qualitatively unique role indepression–smoking comorbidity over and above mostnon-affective depressive symptoms [15,42,43]. Indeed,symptom-level analyses have shown that high negativeaffect (NA; experience of subjective distress) and low posi-tive affect (PA; low engagement with the environment[44,45]) are associated uniquely with nicotine dependenceseverity [46,47], smoking heaviness [48] and smokingrelapse risk [42,49–53]. Moreover, low PA accounts forindependent variance in relapse risk, above and beyondhigh NA [42,49], suggesting that these two processesreflect unique etiological influences on smoking.
2 Amanda R. Mathew et al.
© 2016 Society for the Study of Addiction Addiction

The notion that two distinct affective processes promotesmoking is consistent with multi-dimensional models ofpsychopathology and personality which purport that lowPA and high NA are empirically distinct overarchingpsychological dimensions that have unique psychosocialand biological etiologies [54–56]. The low PA dimensionincludes constructs related to appetitive emotion, includingdiminished pleasure, interest, expectancy, motivation andreinforcement learning [54,57]), whereas the NA dimen-sion includes constructs related to aversive emotion includ-ing sadness, irritability, anxiety, low distress tolerance andneuroticism [54]. In the proposed theoretical model, lowPA and high NA represent distinct states that each worsenmore rapidly following abstinence for depressed versusnon-depressed smokers [58,59] and serve to augmentsmoking motivation.
First, as nicotine dependence increases, low PA signalsthe greater reinforcement value of smoking. In the overallpopulation of smokers and non-smokers, nicotine moder-ately improves PA and reward responsivity [60]. Crucially,smokers with prominent symptoms of anhedonia (i.e. thedecreased capacity to experience pleasure) experiencefrequent bouts of low PA and endorse greater nicotine-induced increases in PA and reward responsivity followingsmoking [61]. While smoking itself is more reinforcing inthe anhedonic state, a greater experience of reward mayalso be derived from other non-nicotine reinforcers, suchas music, and contribute to the greater net value ofsmoking in the anhedonic state [62]. Following acute
withdrawal, regular smokers show moderate-sized reduc-tions in PA and reward responsivity [51,59,63], whileanhedonic smokers exhibit greater reductions in PA,reward responsivity and urge to smoke to enhance PA[64–67]. Potentially, pre-existing deficits in hedonic experi-ence among depressed smokers may be unmasked andexacerbated by nicotine withdrawal, producing strongmotivation to resume smoking to end a temporary ‘timeout’ in reward experience and obtain smoking’s positivereinforcing effects [57]. Thus, low PA is established as asignal for the increased reinforcement value of smoking,particularly among depressed smokers with prominentsymptoms of anhedonia.
Secondly, elevated NA also serves as a motivationalstate driving smoking maintenance among depressedsmokers. Although escape or avoidance of NA is thoughtto be the pre-potent motive for addictive drug use [68],the relationship between smoking and NA is complex.Nicotine is thought to have antidepressant proper-ties [69–72] and experience of NA is shown, reliably, todecrease latency to smoke and increase number of puffsconsumed [73]. However, while smoking reverseswithdrawal-induced NA [74–77], there is little evidencethat it alleviates experimentally induced NA [77–82].
Depressed smokers probably fail to distinguish NAprovoked by withdrawal versus other sources (i.e. environ-mental stressors), and thus seek out smoking in response toboth states. Nicotine withdrawal is characterized by amarked increase in NA among smokers in the
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram: summary of search and selection
Smoking and depression 3
© 2016 Society for the Study of Addiction Addiction

generalpopulation [83,84]. Depression-prone smokersexperience even greater deprivation-induced increases inNA [85–87], which could reflect an unmasking of a pro-pensity towards negative affective states [57]. Accordingly,depressed smokers [88] and individuals prone to depression[89] are especially likely to smoke for affect regulationmotives. NA thus provides a reliable signal for the greaterreinforcement value of smoking and becomes establishedas a motivational state which primes smoking behavior,particularly in depressed smokers.
Cognitive impairment
In addition to affective disturbances, depression is charac-terized by non-specific cognitive deficits that span domainsof attention, memory, processing speed and all aspects ofexecutive functioning [90–96]. Although the aggregatedeffect size estimates of cognitive deficits in major depressionare small to medium [93,97], these deficits are clinicallysignificant [93,97], functionally impairing [98–100] andmay persist even after an acute depressive episode hasabated [90]. Crucially, cognitive impairment associatedwith depression is similar to that observed during nicotinewithdrawal, particularly in domains of executive function-ing and attention [101–103]. In a general population ofsmokers, smoking abstinence is associated with impairedsustained attention, working memory and response inhibi-tion [104], and biases cognition towards the perceived sa-lience of smoking-related stimuli ([105,106], but also see[107]). Depressed smokers are shown to experience evengreater withdrawal-induced deficits in cognitive perfor-mance [108], which may reflect the overlap (or perhapsadditive effect) of cognitive deficits in depression withcognitive deficits induced by smoking abstinence. Accord-ingly, depressed smokers may maintain smoking behaviorin order to attenuate cognitive deficits, especially whenengaged in effortful or cognitively demanding tasks[109,110]. Importantly, cognitive deficits are associatedprospectively with smoking relapse for both smokers inthe general population [111,112] and depression-pronesmokers [113]. Thus, background cognitive deficits indepression may summate with acute withdrawal-relatedcognitive deficits to prime smoking [108].
Our theoretical model posits that cognitive impairmentcomes to signal the additional reinforcement of smokingproduced by the resulting improvement in cognitive func-tioning. However, far fewer studies have examined cogni-tive versus affective processes underlying smokingmaintenance in depressed smokers, limiting the definitiveconclusions that can be drawn. Preliminary evidencesuggests that depressed smokers endorse smoking in partto manage negative intrusive thoughts and facilitateconcentration and problem-solving [114]. Additionally,depressed versus non-depressed smokers showed improved
reaction-time performance after smoking, suggesting thatthey experienced greater cognitive enhancementcompared to baseline [115]. Further studies are neededto test whether depressed versus non-depressed smokersexperience greater reinforcement value of smoking in theface of cognitive impairment, as suggested by an incentivelearning theory account.
Proposed incentive learning model of smoking anddepression and distinction from negativereinforcement-based models
Negative reinforcement models may be divided into threecategories based upon the proposed mechanisms by whichadverse states promote drug use. All three categories makethe common prediction that depressed smokers experiencefrequent bouts of high NA, low PA and cognitive impair-ment, which intensify rapidly during acute abstinenceand function to promote smoking maintenance andrelapse [80–83]. The distinction between the three catego-ries of negative reinforcement accounts lies in their depic-tion of the learning processes by which these adversestates acquire control over smoking behavior. The earlynegative reinforcement accounts referred to the adversestates as internal instrumental discriminative stimuli(or SDs for short) because they ‘set the occasion’ or providethe context [116] in which smoking is more reinforcing;but exactly how these internal SDs prime smoking behaviorwas not specified fully [117,118].
The later wave of negative reinforcement theories[119], allostasis theories [120,121] andmore recent incen-tive habit theories [122] have sought to specify howadverseinternal states prime smoking behavior. These theories fol-low Hull’s [123] stimulus–response/reinforcement view ofinstrumental discrimination learning, according to whichadverse internal stimuli (S) form a direct association withsmoking response sequences (R) as a result of reinforce-ment from smoking. The S–R association between adversestates and smoking responses is especially strong becausesmoking is more reinforcing in the adverse states, whichstrengthens the S–R association. This learning enables ad-verse states to elicit smoking behavior directly, without re-trieving knowledge of the consequences of the behavior.Accordingly, S–R-based control of smoking has been calledautomatic, unconscious, pre-conscious, habitual and com-pulsive. Such S–R accounts are attractive because they canexplain howadverse internal states could promote smokingbehavior bypassing the individual’s intentions to remainabstinent, which could account for depressed smokers’elevated rates of smoking cessation failure, despite highmotivation to quit. These accounts ascribe to internalstimuli the same form of direct control over response selec-tion that ‘standard’ habit theories of addiction haveascribed to external drug-related cues [124–126].
4 Amanda R. Mathew et al.
© 2016 Society for the Study of Addiction Addiction

However, S–R accounts of action control by internalstates have been challenged on logical grounds by re-searchers from the behavior-analyst tradition [127–130].The grounds for this challenge are that the behavioralsequences needed to yield nicotine reinforcement differvastly depending on the context (e.g. purchasing cigarettesfrom a store versus from a machine; smoking during abreak versus in a bar). Internal states on their own arenot sufficiently discriminating to elicit the responsesequence that is required to produce nicotine reinforce-ment in these various external contexts via simpleS–R/reinforcement learning [127–130]. Instead, from thebehavior-analyst perspective, adverse internal states func-tion as motivating operations (or MOs) because they pre-dict that smoking has greater reinforcement valueindependently of the external context and the responsecurrently required to produce that reinforcer. MOs arethought to motivate behavior by interacting with theexternal SDs. Specifically, by virtue of signaling that asmoking reinforcement has a greater value, MOs lowerthe threshold of activation required for external SDs to elicitthe specific response sequences required to producesmoking reinforcement in the external context. On thisaccount, adverse states do not elicit smoking directly(as predicted by S–R theories) but, rather, modulate theability of external discriminative stimuli to evoke smokingbehavior through S–R learning. The main weakness of thisaccount is that it does not explain fully the nature of theinteraction which allows adverse states (MOs) to modulatecontrol by external stimuli over response selection.
Incentive learning theory addresses this limitation bysuggesting that adverse states promote smoking behaviorthrough a conjunction of explicit desire and goal-directedinstrumental knowledge [32–34]; see also [35]. On thisview, adverse states function as motivational states (likeMOs) which, by virtue of predicting the greater reinforce-ment value of smoking, come to elicit an expectation ofthe greater reinforcement value of smoking (i.e. greatersubjective desire to smoke). Smokers also acquire explicitgoal-directed instrumental knowledge of the specificresponse sequences that yield nicotine reinforcement indifferent external contexts. These two forms of knowledgeare then synthesized in a cognitive inference. The experi-ence of an adverse state generates an expectation of thegreater reinforcement value of smoking which is combinedwith goal-directed instrumental knowledge of the responsesequence required to produce the desired smokingoutcome given the specific external context [36–39]. Theincentive learning account is unique among the categoriesof negative reinforcement theory in predicting that adverseinternal states prime smoking behavior via a conjunctionof subjective desire to smoke and instrumental knowledgeof the responses required to produce that outcome in thecurrent context.
Proposed theory
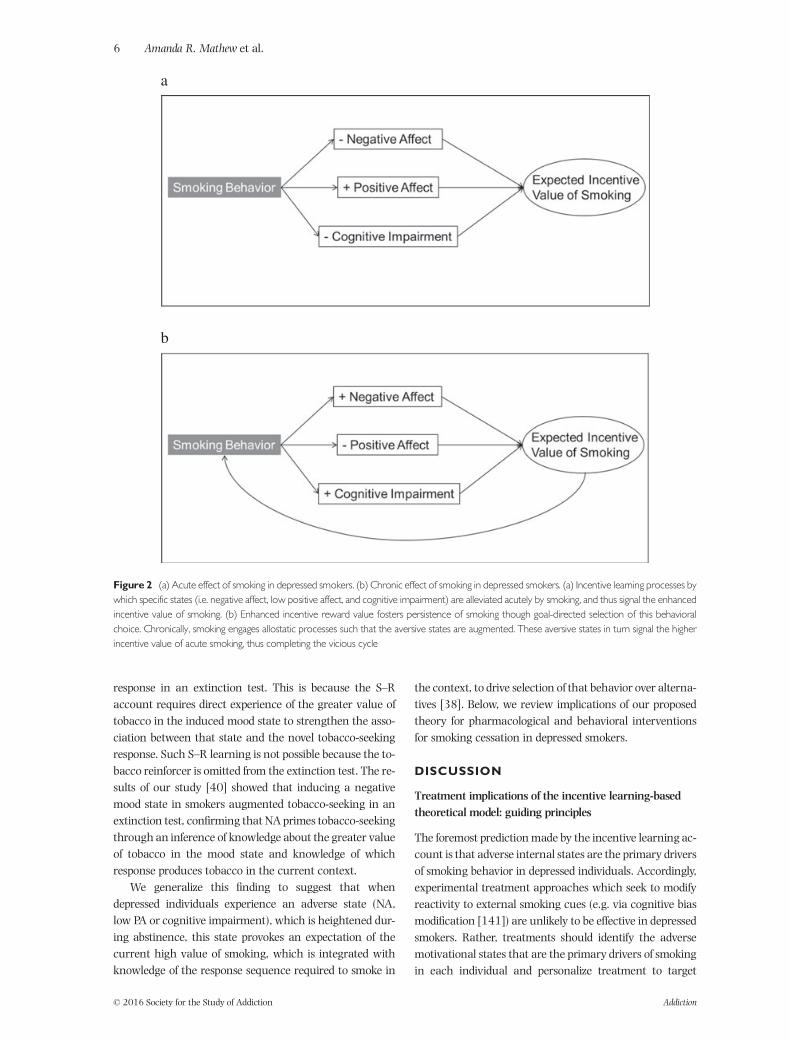
As shown in Fig. 2, we propose a novel application of theincentive learning account to co-occurring smoking anddepression. Figure 2a illustrates the acute smoking phasein which depressed smokers develop an expectation ofgreater reinforcement value of smoking in three specificmotivational states: NA, low PA and cognitive impairment.As smoking persists, Fig. 2b displays the role of chronicsmoking in worsening NA, low PA and cognitive impair-ment over time due to frequent bouts of nicotinewithdrawal. Belief about the high reward value of smokingin these motivational states, particularly during absti-nence, is conceptualized as the primary trigger for smokingmaintenance and relapse following a quit attempt indepressed smokers.
Although this theoretical framework is relevant tosmokers in the general population, we believe that themotivational states are especially effective in depressedsmokers. First, those with depression experience moreintense adverse states and greater reinforcement value ofsmoking in these states, so these states become morepowerful motivators of smoking. Secondly, depression isassociated with a more severe withdrawal syndrome,adding further intensity to the adverse states as motivatorsof smoking behavior. Lastly, depression is thought to coun-ter acute satiety, so depressed smokers sustain a greater ex-pected value of smoking even immediately after smoking.
The unique prediction of the incentive learningaccount(compared to the S–R account) is that subjective desire tosmoke prompted by adverse states and goal-directed instru-mental knowledge of the effective smoking response ineach context are integrated to drive smoking behavior.One source of support for this claim is the finding thatexperimental induction of stress or NA provoke increasesin both smoking desire and smoking behavior[79,82,131–139]. Although the mood-induced increasein smoking desire may cause the smoking behavior, asanticipated by incentive learning theory, S–R-basednegative reinforcement accounts would argue that theincrease in smoking desire is actually epiphenomenal inrelation to smoking behavior. The causal status of subjec-tive desire in controlling behavior remains an unresolvedscientific question [34,140].
We recently reported direct empirical evidencesupporting the incentive learning account over the S–Raccount of how negative mood provokes smoking [40]. Aunique prediction of the incentive learning account is thatinduced negative mood should be able to augment a noveltobacco-seeking response in an extinction test throughintegration of (1) expected high value of tobacco and(2) knowledge of the instrumental response required toproduce that outcome in the context. By contrast, theS–R account predicts that an induced negative moodshould not be able to augment a novel tobacco-seeking
Smoking and depression 5
© 2016 Society for the Study of Addiction Addiction
response in an extinction test. This is because the S–Raccount requires direct experience of the greater value oftobacco in the induced mood state to strengthen the asso-ciation between that state and the novel tobacco-seekingresponse. Such S–R learning is not possible because the to-bacco reinforcer is omitted from the extinction test. The re-sults of our study [40] showed that inducing a negativemood state in smokers augmented tobacco-seeking in anextinction test, confirming that NA primes tobacco-seekingthrough an inference of knowledge about the greater valueof tobacco in the mood state and knowledge of whichresponse produces tobacco in the current context.
We generalize this finding to suggest that whendepressed individuals experience an adverse state (NA,low PA or cognitive impairment), which is heightened dur-ing abstinence, this state provokes an expectation of thecurrent high value of smoking, which is integrated withknowledge of the response sequence required to smoke in
the context, to drive selection of that behavior over alterna-tives [38]. Below, we review implications of our proposedtheory for pharmacological and behavioral interventionsfor smoking cessation in depressed smokers.
DISCUSSION
Treatment implications of the incentive learning-basedtheoretical model: guiding principles
The foremost prediction made by the incentive learning ac-count is that adverse internal states are the primary driversof smoking behavior in depressed individuals. Accordingly,experimental treatment approaches which seek to modifyreactivity to external smoking cues (e.g. via cognitive biasmodification [141]) are unlikely to be effective in depressedsmokers. Rather, treatments should identify the adversemotivational states that are the primary drivers of smokingin each individual and personalize treatment to target
Figure 2 (a) Acute effect of smoking in depressed smokers. (b) Chronic effect of smoking in depressed smokers. (a) Incentive learning processes bywhich specific states (i.e. negative affect, low positive affect, and cognitive impairment) are alleviated acutely by smoking, and thus signal the enhancedincentive value of smoking. (b) Enhanced incentive reward value fosters persistence of smoking though goal-directed selection of this behavioralchoice. Chronically, smoking engages allostatic processes such that the aversive states are augmented. These aversive states in turn signal the higherincentive value of acute smoking, thus completing the vicious cycle
6 Amanda R. Mathew et al.
© 2016 Society for the Study of Addiction Addiction

those states. Further, effective intervention strategiesshould address smokers’ beliefs about the high rewardvalue of smoking in these motivational states. In sum,our theory suggests that treatments which (1) attenuateadverse internal states and (2) reverse positive expectan-cies associated with smoking are most likely to achievecessation among depressed smokers.
Targeted pharmacological interventions
Consistent with our theory, pharmacological interventionsmay be particularly effective in depressed smokers by ame-liorating the motivational states which raise the expectedvalue of smoking: high NA, low PA and cognitive impair-ment. In particular, varenicline has cognitive-enhancingeffects in both treatment-motivated smokers [142] andnon-smokers [143], and reduces the cognitive impairmentthat accompanies withdrawal [144]. Bupropion is alsoshown to be an effective pharmacological interventionamong depressed smokers [145,146], possibly through itseffects on affective functioning [88,147]. Further, giventhat multiple withdrawal-related motivational states mayinteract or summate to motivate smoking among de-pressed smokers, combination pharmacotherapy (i.e. com-bined varenicline and bupropion or combination nicotinereplacement therapy [148–150] may be particularly war-ranted for this population to address each state optimally.As studies of pharmacological agents have focused largelyupon cessation outcomes rather than mediating variables,future research testing the effects of medications on themotivational states identified in this review could help toguide pharmacological treatment for depressed smokers.
Targeted behavioral interventions
To date, NA has been the primary component of depressiontargeted characteristically by behavioral interventions insmokers with comorbid depression [151–154]. Expandingbehavioral interventions to also target low PA explicitlycould improve smoking outcomes for smokers with depres-sion. Behavioral activation—an efficacious treatment formajor depressive disorder that increases engagement in re-inforcing activities congruent with a person’s goals [155]—may counteract withdrawal-related anhedonia andincrease quit rates by increasing exposure to alternativesources of non-smoking reinforcement [156].
Our model states further that relations between moti-vational states and goal-directed smoking behavior are me-diated by expectancies that smoking will improve thesestates. Behavioral interventionswhich address these expec-tancies (i.e. by challenging maladaptive beliefs about thelong-term mood regulating effects of nicotine) could helpto break the link between cognitive/affective deficits andsmoking maintenance among depressed smokers.
Although smokers with depression believe commonly thatsmoking helps to regulate their negative mood states[157,158], evidence suggests that smoking actually leadsto worsening of mental health symptoms over time and,conversely, quitting leads to improved mental health status[159]. Thus, behavioral interventions should emphasizethe distinction between withdrawal reversal and truemood improvement to allow smokers to learn that the ben-efits of smoking are short- but not long-term, and restrictedto the withdrawal syndrome and not environmentalstressors. Novel strategies incorporating self-monitoringand personalized feedback could help to improve thesalience and credibility of this message, particularly amongdepressed smokers.
Conclusions
Our proposed theory posits that smoking is maintainedamong depressed smokers through the expectation thatsmoking will alleviate specific states, in integration withthe goal-directed choice of smoking over alternate behav-iors. Drawing from a systematic review of the smoking-depression literature, we propose high NA, low PA andcognitive impairment as the three motivational states thatdrive this process. While we have chosen a narrativereview format in order to frame our conceptual model, thisapproach limited our ability to systematically assess for riskof bias and strength of evidence across studies. As the treat-ment literature on smoking and depression expands, it willbe increasingly important for future reviews of this topic toinclude both qualitative and quantitative methods ofanalysis.
Our review identifies several directions for futureresearch. First, it remains unclear how awareness of cogni-tive deficits interacts with awareness of affective states (i.e.low PA and high NA) to provide the motivational signalpromoting goal-directed smoking behavior. Studies thatcharacterize each of these withdrawal-related statesamong depressed smokers, as well as their unique andshared contribution to tobacco-seeking behavior, areneeded. Secondly, although our theory holds that expec-tancies play a causal role in smoking maintenance, it hasnot been specified fully how knowledge of reward valuesand context-dependent response requirements translateinto actual action selection. Thirdly, cognitive processesamong depressed smokers have received relatively little re-search attention, but we believe cognitive impairment rep-resents a key motivational state maintaining smokingbehavior in this population [160]. Future research shouldelucidate further the extent to which depressed smokerssmoke for cognitive enhancement motives, benefit differen-tially from smoking in terms of functional cognitive out-comes and respond to pro-cognitive agents as part of asmoking cessation intervention. Lastly, as depression and
Smoking and depression 7
© 2016 Society for the Study of Addiction Addiction

smoking co-occur commonly with other mental healthconcerns (i.e. substance use disorders, anxiety disorders)[161–163], identifying the unique versus shared incentivestates underlying each of these conditions in order to guideintegrated treatment is an important priority.
Declaration of interests
Dr. Histman has served on a scientific advisory board forPfizer and receives study medication and placebo free ofcharge from Pfizer for use in ongoing National Institutesof Health funded clinical trials.
Acknowledgments
This work is supported by the National Cancer Instituteand National Institute on Drug Abuse of the UnitedStates National Institutes of Health (Grant NumbersF32DA036947 and R01CA184211). J.W.C. is supportedby Merit Review Award 101CX00056 from the US Depart-ment of Veterans Affairs. We thank Dr Robert West forfeedback on an earlier draft of this manuscript.
References
1. Grant B. F., Hasin D. S., Chou S. P., Stinson F. S., Dawson D. A.Nicotine dependence and psychiatric disorders in the UnitedStates: results from the national epidemiologic survey onalcohol and related conditions. Arch Gen Psychiatry 2004;61: 1107–15.
2. Hall S. M., Prochaska J. J. Treatment of smokers withco-occurring disorders: emphasis on integration in mentalhealth and addiction treatment settings. Annu Rev ClinPsychol 2009; 5: 409–31.
3. Lasser K., Boyd J. W., Woolhandler S., Himmelstein D. U.,McCormick D., Bor D. H. Smoking and mental illness: apopulation-based prevalence study. JAMA 2000; 284:2606–10.
4. Lawrence D., Mitrou F., Zubrick S. R. Smoking and mentalillness: results from population surveys in Australia and theUnited States. BMC. Public Health 2009; 9: 285.
5. Ziedonis D., Hitsman B., Beckham J. C., Zvolensky M.,Adler L. E., Audrain-McGovern J. et al. Tobacco useand cessation in psychiatric disorders: National Instituteof Mental Health report. Nicotine Tob Res 2008; 10:1691–715.
6. Cook B. L., Wayne G. F., Kafali E. N., Liu Z., Shu C., Flores M.Trends in smoking among adults with mental illness andassociation between mental health treatment and smokingcessation. JAMA 2014; 311: 172–82.
7. Breslau N., Kilbey M. M., Andreski P. Nicotine withdrawalsymptoms and psychiatric disorders: findings from an epide-miologic study of young adults. Am J Psychiatry 1992; 149:464–9.
8. Weinberger A. H., Desai R. A., McKee S. A. Nicotine with-drawal in U.S. smokers with current mood, anxiety, alcoholuse, and substance use disorders. Drug Alcohol Depend2010; 108: 7–12.
9. Goodwin R. D., Zvolensky M. J., Keyes K. M., Hasin D. S.Mental disorders and cigarette use among adults in theUnited States. Am J Addict 2012; 21: 416–23.
10. Grant B. F., Hasin D. S., Chou S., Stinson F. S., Dawson D. A.Nicotine dependence and psychiatric disorders in the UnitedStates: results from the national epidemiologic survey on al-cohol and relatedconditions. Arch Gen Psychiatry 2004; 61:1107–15.
11. Khaled S. M., Bulloch A., Exner D. V., Patten S. B. Ciga-rette smoking, stages of change, and major depression inthe Canadian population. Can J Psychiatry 2009; 54:204–8.
12. Khaled S. M., Bulloch A. G., Williams J. V., Lavorato D. H.,Patten S. B. Major depression is a risk factor for shortertime to first cigarette irrespective of the number of ciga-rettes smoked per day: evidence from a nationalpopulation health survey. Nicotine Tob Res 2011; 13:1059–67.
13. Acton G. S., Kunz J. D.,WilsonM., Hall S. M. The construct ofinternalization: conceptualization, measurement, andprediction of smoking treatment outcome. Psychol Med2005; 35: 395–408.
14. Prochaska J. J., Rossi J. S., Redding C. A., Rosen A. B., Tsoh J.Y., Humfleet G. L. et al. Depressed smokers and stage ofchange: implications for treatment interventions. Drug Alco-hol Depend 2004; 76: 143–51.
15. Buckner J. D., Farris S. G., Zvolensky M. J., Shah S. M.,Leventhal A. M., Minnix J. A. et al. Dysphoria and smokingamong treatment seeking smokers: the role of smoking-related inflexibility/avoidance. Am J Drug Alcohol Abuse2015; 41: 45–51.
16. Cooper J., Borland R., McKee S. A., Yong H. H., Dugué P. A.Depression motivates quit attempts but predicts relapse:differential findings for gender from the InternationalTobacco Control study. Addiction 2016; 111: 1438–47.
17. Williams J. M., Stroup T. S., Brunette M. F., Raney L. E. Inte-grated care: tobacco use and mental illness: a wake-up callfor psychiatrists. Psychiatr Serv 2014; DOI: 10.1176/appi.ps.201400235.
18. Druss B. G., Zhao L., Von Esenwein S., Morrato E. H., MarcusS. C. Understanding excess mortality in persons with mentalillness: 17-year follow up of a nationally representative USsurvey. Med Care 2011; 49: 599–604.
19. Colton C., Manderscheid R. Congruencies in increasedmortality rates, years of potential life lost, and causes ofdeath among public mental health clients in eight states.Prev Chronic Dis 2006; 3: A42.
20. Tiihonen J., Lönnqvist J., Wahlbeck K., Klaukka T., NiskanenL., Tanskanen A. et al. 11-year follow-up of mortality inpatients with schizophrenia: a population-based cohortstudy (fin11 study. Lancet 2009; 374: 620–7.
21. Kahler C. W., Spillane N. S., Busch A. M., Leventhal A. M.Time-varying smoking abstinence predicts lower depressivesymptoms following smoking cessation treatment. NicotineTob Res 2011; 13: 146–50.
22. Mathew A. R., Robinson J. D., Norton P. J., Cinciripini P. M.,Brown R. A., Blalock J. A. Affective trajectories before andafter a quit attempt among smokers with current depressivedisorders. Nicotine Tob Res 2013; 15: 1807–15.
23. Taylor G., McNeill A., Girling A., Farley A., Lindson-Hawley N., Aveyard P. Change in mental health aftersmoking cessation: systematic review and meta-analysis.BMJ 2014; 348: g1151.
24. Berlin I., Chen H., Covey L. S. Depressive mood, suicide idea-tion and anxiety in smokers who do and smokers who do notmanage to stop smoking after a target quit day. Addiction2010; 105: 2209–16.
8 Amanda R. Mathew et al.
© 2016 Society for the Study of Addiction Addiction

25. McDermott M. S., Marteau T. M., Hollands G. J., Hankins M.,Aveyard P. Change in anxiety following successful andunsuccessful attempts at smoking cessation: cohort study.Br J Psychiatry 2013; 202: 62–7.
26. Bakhshaie J., Zvolensky M. J., Goodwin R. D. Cigarettesmoking and the onset and persistence of depression amongadults in the United States: 1994–2005. Compr Psychiatry2014; DOI: 10.1016/j.comppsych.2014.10.012.
27. US Department of Health and Human Services (USDHHS).The Health Consequences of Smoking—50 Years of Progress: AReport of the Surgeon General. Atlanta, GA: USDHHS, Centersfor Disease Control and Prevention, National Center forChronic Disease Prevention and Health Promotion, Officeon Smoking and Health; 2014.
28. Bowins B. Depression: discrete or continuous? Psychopathol-ogy 2015; 48: 69–78.
29. Angst J., Sellar R., Merikangas K. R. Depressive spectrumdiagnoses. Compr Psychiatry 2000; 41: 39–47.
30. Ayuso-Mateos J. L., Nuevo R., Verdes E., Naidoo N., ChatterjiS. From depressive symptoms to depressive disorders: the rel-evance of thresholds. Br J Psychiatry 2010; 196: 365–71.
31. Anthenelli R. M., Morris C., Ramey T. S., Dubrava S. J.,Tsilkos K., Russ C. et al. Effects of varenicline on smokingcessation in adults with stably treated current or past majordepression: a randomized trial. Ann Intern Med 2013; 159:390–400.
32. DickinsonA., Balleine B.W. The cognitive/motivational inter-face. In: KringelbachM. L., Berridge K. C., editors. Pleasures ofthe Brain. The Neural Basis of Taste, Smell and Other Rewards.Oxford, UK: Oxford University Press; 2010, pp. 74–84.
33. Balleine B. W., Ball J., Dickinson A. Benzodiazepine-inducedoutcome revaluation and the motivational control ofinstrumental action in rats. Behav Neurosci 1994; 108:573–89.
34. Heyes C., Dickinson A. The intentionality of animal action.Mind Lang 1990; 5: 87–103.
35. Pittenger S. T., Bevins R. A. Interoceptive conditioning witha nicotine stimulus is susceptible to reinforcer devaluation.Behav Neurosci 2013; 127: 465–73.
36. Bradfield L. A., Balleine B.W. Hierarchical and binary associ-ations compete for behavioral control during instrumentalbiconditional discrimination. J Exp Psychol Anim BehavProcess 2013; 39: 2–13.
37. Trask S., Bouton M. Contextual control of operant behavior:Evidence for hierarchical associations in instrumental learn-ing. Learn Behav 2014; 42: 281–8.
38. Hogarth L., Troisi J. R. 2nd. A hierarchical instrumental de-cision theory of nicotine dependence. In: Balfour D. J. K.,Munafò M. R., editors. The Neurobiology and Genetics of Nico-tine and Tobacco. Current Topics in Behavioral Neurosciences.Gewerbestrasse, Switzerland: Springer International Pub-lishing; 2015, pp. 165–91.
39. Hogarth L., Retzler C., Munafò M. R., Tran D. M. D., Troisi J.R. 2nd, Rose A. K. et al. Extinction of cue-evoked drug-seeking relies on degrading hierarchical instrumental expec-tancies. Behav Res Ther 2014; 59: 61–70.
40. Hogarth L., He Z., Chase H. W., Wills A. J., Troisi J. R. 2nd,Leventhal A. M. et al. Negative mood reverses devaluationof goal-directed drug-seeking favouring an incentive learn-ing account of drug dependence. Psychopharmacology(Berl) 2015; 232: 3235–47.
41. American Psychiatric Association (APA). Diagnostic and Sta-tistical Manual of Mental Disorders (DSM-5®). Arlington, VA:American Psychiatric Publishers; 2013.
42. Leventhal A. M., Ramsey S. E., Brown R. A., LaChance H. R.,Kahler C. W. Dimensions of depressive symptoms andsmoking cessation. Nicotine Tob Res 2008; 10: 507–17.
43. Haas A. L., Munoz R. F., Humfleet G. L., Reus V. I., Hall S. M.Influences of mood, depression history, and treatmentmodality on outcomes in smoking cessation. J Consult ClinPsychol 2004; 72: 563–70.
44. Watson D., Clark L. A., Tellegen A. Development and valida-tion of brief measures of positive and negative affect: thePANAS scales. J Pers Soc Psychol 1988; 54: 1063.
45. Watson D., Weber K., Assenheimer J. S., Clark L. A.,Strauss M. E., McCormick R. A. Testing a tripartite model:I. Evaluating the convergent and discriminant validity ofanxiety and depression symptom scales. J Abnorm Psychol1995; 104: 3–14.
46. Leventhal A. M., Kahler C. W., Ray L. A., Zimmerman M.Refining the depression–nicotine dependence link: patternsof depressive symptoms in psychiatric outpatients withcurrent, past, and no history of nicotine dependence. AddictBehav 2009; 34: 297–303.
47. Mickens L., Greenberg J., Ameringer K. J., Brightman M.,Sun P., Leventhal A. M. Associations between depressivesymptom dimensions and smoking dependence motives.Eval Health Prof 2011; 34: 81–102.
48. Leventhal A. M., Zvolensky M. J., Schmidt N. B.Smoking-related correlates of depressive symptom dimen-sions in treatment-seeking smokers. Nicotine Tob Res 2011;13: 668–76.
49. Leventhal A. M., Piper M. E., Japuntich S. J., Baker T. B., CookJ. W. Anhedonia, depressed mood, and smoking cessationoutcome. J Consult Clin Psychol 2014; 82: 122–9.
50. Cook J., Spring B., McChargue D., Doran N. Effects ofanhedonia on days to relapse among smokers with ahistory of depression: a brief report. Nicotine Tob Res2010; 12: 978–82.
51. Cook J.W., Piper M. E., Leventhal A. M., SchlamT. R., FioreM.C., Baker T. B. Anhedonia as a component of the tobaccowithdrawal syndrome. J Abnorm Psychol 2015; 124: 215–25.
52. Hitsman B., Pingitore R., Spring B., Mahableshwarkar A.,Mizes J. S., Segraves K. A. et al. Antidepressant pharmaco-therapy helps some cigarette smokers more than others. JConsult Clin Psychol 1999; 67: 547–54.
53. Schnoll R. A., Leone F. T., Hitsman B. Symptoms ofdepression and smoking behaviors following treatmentwith transdermal nicotine patch. J Addict Dis 2013; 32:46–52.
54. Clark L. A., Watson D. Tripartite model of anxiety anddepression: psychometric evidence and taxonomic implica-tions. J Abnorm Psychol 1991; 100: 316–36.
55. Elliot A. J., Thrash T. M. Approach–avoidance motivation inpersonality: approach and avoidance temperaments andgoals. J Pers Soc Psychol 2002; 82: 804–18.
56. Lane R. D., Reiman E. M., Bradley M. M., Lang P. J., Ahern G.L., Davidson R. J. et al. Neuroanatomical correlates ofpleasant and unpleasant emotion. Neuropsychologia 1997;35: 1437–44.
57. Leventhal A. M., Zvolensky M. J. Anxiety, depression, andcigarette smoking: a transdiagnostic vulnerability frame-work to understanding emotion-smoking comorbidity.Psychol Bull 2015; 141: 176–212.
58. Audrain-McGovern J., Wileyto E. P., Ashare R., Cuevas J.,Strasser A. A. Reward and affective regulationin depression-prone smokers. Biol Psychiatry 2014; 76:689–97.
Smoking and depression 9
© 2016 Society for the Study of Addiction Addiction

59. Pergadia M. L., Der-AvakianA., D’SouzaM. S., Madden P. A.,Heath A. C., Shiffman S. et al. Association between nicotinewithdrawal and reward responsiveness in humans and rats.JAMA Psychiatry 2014; 71: 1238–45.
60. Dawkins L., Powell J. H., West R., Powell J., Pickering A. Adouble-blind placebo controlled experimental study ofnicotine: I—effects on incentive motivation. Psychopharma-cology (Berl) 2006; 189: 355–67.
61. Cook J. W., Spring B., McChargue D. Influence of nicotine onpositive affect in anhedonic smokers. Psychopharmacology(Berl) 2007; 192: 87–95.
62. Perkins K. A., Karelitz J. L. Reinforcement enhancing effectsof nicotine via smoking. Psychopharmacology (Berl) 2013;228: 479–86.
63. Leventhal A. M., Waters A. J., Moolchan E. T., Heishman S.J., Pickworth W. B. A quantitative analysis of subjective,cognitive, and physiological manifestations of the acutetobacco abstinence syndrome. Addict Behav 2010; 35:1120–30.
64. Leventhal A. M., Munafo M., Tidey J. W., Sussman S.,Monterosso J. R., Sun P. et al.Anhedonia predicts altered pro-cessing of happy faces in abstinent cigarette smokers.Psychopharmacology (Berl) 2012; 222: 343–51.
65. Leventhal A., TrujilloM., Ameringer K., Tidey J., Sussman S.,Kahler C. Anhedonia and the relative reward value of drugand nondrug reinforcers in cigarette smokers. J AbnormPsychol 2014; 123: 375–86.
66. Leventhal A. M., Waters A. J., Kahler C. W., Ray L. A.,Sussman S. Relations between anhedonia and smokingmotivation. Nicotine Tob Res 2009; 11: 1047–54.
67. Cook J. W., Spring B., McChargue D., Hedeker D. Hedoniccapacity, cigarette craving, and diminished positive mood.Nicotine Tob Res 2004; 6: 39–47.
68. Baker T. B., Piper M. E., McCarthy D. E., Majeskie M. R., FioreM. C. Addiction motivation reformulated: an affectiveprocessing model of negative reinforcement. Psychol Rev2004; 111: 33–51.
69. Balfour D. J., Ridley D. L. The effects of nicotine on neu-ral pathways implicated in depression: a factor innicotine addiction? Pharmacol Biochem Behav 2000; 66:79–85.
70. Tizabi Y., Overstreet D. H., Rezvani A. H., Louis V. A., Clark E.Jr., Janowsky D. S. et al. Antidepressant effects of nicotine inan animal model of depression. Psychopharmacology (Berl)1999; 142: 193–9.
71. Vázquez-Palacios G., Bonilla-Jaime H., Velázquez-Moctezuma J. Antidepressant effects of nicotine and fluoxe-tine in an animal model of depression induced by neonataltreatment with clomipramine. Prog NeuropsychopharmacolBiol Psychiatry 2005; 29: 39–46.
72. Mineur Y. S., Picciotto M. R. Biological basis for theco-morbidity between smoking and mood disorders. J DualDiagn 2009; 5: 122–30.
73. Heckman B. W., Carpenter M. J., Correa J. B., Wray J. M.,Saladin M. E., Froeliger B. et al. Effects of experimentalnegative affect manipulations on ad libitum smoking: ameta-analysis. Addiction 2015; 110: 751–60.
74. Hatsukami D. K., Hughes J. R., Pickens R. W., Svikis D.Tobacco withdrawal symptoms: an experimental analysis.Psychopharmacology (Berl) 1984; 84: 231–6.
75. Hughes J. R., Hatsukami D. K., Pickens R. W., Krahn D.,Malin S., Luknic A. Effect of nicotine on the tobacco with-drawal syndrome. Psychopharmacology (Berl) 1984; 83:82–7.
76. Parrott A. C. Stress modulation over the day in cigarettesmokers. Addiction 1995; 90: 233–44.
77. Perkins K. A., Karelitz J. L., Conklin C. A., Sayette M. A.,Giedgowd G. E. Acute negative affect relief from smokingdepends on the affect situation and measure but not onnicotine. Biol Psychiatry 2010; 67: 707–14.
78. Perkins K. A., Ciccocioppo M., Conklin C. A., Milanak M.E., Grottenthaler A., Sayette M. A. Mood influences onacute smoking responses are independent of nicotineintake and dose expectancy. J Abnorm Psychol 2008;117: 79.
79. Conklin C. A., Perkins K. A. Subjective and reinforcing effectsof smoking during negative mood induction. J AbnormPsychol 2005; 114: 153–64.
80. Kassel J. D., Shiffman S. Attentional mediation of cigarettesmoking’s effect on anxiety. Health Psychol 1997; 16:359–68.
81. Kassel J. D., Unrod M. Smoking, anxiety, and attention:support for the role of nicotine in attentionally mediatedanxiolysis. J Abnorm Psychol 2000; 109: 161–6.
82. Willner P., Jones C. Effects of mood manipulation on subjec-tive and behavioural measures of cigarette craving. BehavPharmacol 1996; 7: 355–63.
83. Hughes J. R. Effects of abstinence from tobacco: Etiology,animal models, epidemiology, and significance: a subjectivereview. Nicotine Tob Res 2007; 9: 329–39.
84. Piper M. E. Withdrawal: Expanding a key addiction con-struct. Nicotine Tob Res 2015; 17: 1405–15.
85. Leventhal A. M., Ameringer K. J., Osborn E., Zvolensky M. J.,Langdon K. J. Anxiety and depressive symptoms and affec-tive patterns of tobacco withdrawal. Drug Alcohol Depend2013; 133: 324–9.
86. Gilbert D. G., McClernon F. J., Rabinovich N. E., Dibb W. D.,Plath L. C., Hiyane S. et al. EEG, physiology, and task-related mood fail to resolve across 31 days of smokingabstinence: relations to depressive traits, nicotineexposure, and dependence. Exp Clin Psychopharmacol1999; 7: 427–43.
87. Audrain-McGovern J., Wileyto E. P., Ashare R., Cuevas J.,Strasser A. A. Reward and affective regulation indepression-prone smokers. Biol Psychiatry 2014; 76:689–97.
88. LermanC., Audrain J., Orleans C.T., BoydR.,GoldK.,MainD.et al. Investigation of mechanisms linking depressed mood tonicotine dependence. Addict Behav 1996; 21: 9–19.
89. Brody C. L., Hamer D. H., Haaga D. A. Depressionvulnerabil-ity, cigarette smoking, and the serotonin transporter gene.Addict Behav 2005; 30: 557–66.
90. Bora E., Harrison B., Yücel M., Pantelis C. Cognitive impair-ment in euthymic major depressive disorder: a meta-analysis. Psychol Med 2013; 43: 2017–26.
91. Trivedi M. H., Greer T. L. Cognitive dysfunction in unipolardepression: implications for treatment. J Affect Disord 2014;152–154: 19–27.
92. Hammar A., Ardal G. Cognitive functioning in majordepression—a summary. Front Hum Neurosci 2009; 3: 26.
93. Lee R. S., Hermens D. F., Porter M. A., Redoblado-HodgeM. A. A meta-analysis of cognitive deficits in first-episodemajor depressive disorder. J Affect Disord 2012; 140:113–24.
94. Murrough J. W., Iacoviello B., Neumeister A., Charney D. S.,Iosifescu D. V. Cognitive dysfunction in depression:neurocircuitry and new therapeutic strategies. NeurobiolLearn Mem 2011; 96: 553–63.
10 Amanda R. Mathew et al.
© 2016 Society for the Study of Addiction Addiction

95. Austin M.-P., Mitchell P., Goodwin G. M. Cognitive deficits indepression possible implications for functional neuropathol-ogy. Br J Psychiatry 2001; 178: 200–6.
96. Millan M. J., Agid Y., Brüne M., Bullmore E. T., Carter C. S.,Clayton N. S. et al. Cognitive dysfunction in psychiatricdisorders: characteristics, causes and the quest for improvedtherapy. Nat Rev Drug Discov 2012; 11: 141–68.
97. McIntyre R. S., Cha D. S., Soczynska J. K.,Woldeyohannes H.O., Gallaugher L. A., Kudlow P. et al. Cognitive deficits andfunctional outcomes in major depressive disorder: determi-nants, substrates, and treatment interventions. DepressAnxiety 2013; 30: 515–27.
98. Evans V. C., Chan S. S., Iverson G. L., Bond D. J., Yatham L.N., Lam R. W. Systematic review of neurocognition andoccupational functioning in major depressive disorder.Neuropsychiatry 2013; 3: 97–105.
99. Buist-Bouwman M., Ormel J., de Graaf R., de Jonge P., vanSonderen E., Alonso J. et al.Mediators of the association be-tween depression and role functioning. Acta Psychiatr Scand2008; 118: 451–8.
100. Jaeger J., Berns S., Uzelac S., Davis-Conway S.Neurocognitive deficits and disability in major depressivedisorder. Psychiatry Res 2006; 145: 39–48.
101. Jacobsen L. K., Krystal J. H., Mencl W. E., Westerveld M.,Frost S. J., Pugh K. R. Effects of smoking and smoking absti-nence on cognition in adolescent tobacco smokers. BiolPsychiatry 2005; 57: 56–66.
102. Jacobsen L. K., Mencl W. E., Constable R. T., Westerveld M.,Pugh K. R. Impact of smoking abstinence on working mem-ory neurocircuitry in adolescent daily tobacco smokers.Psychopharmacology (Berl) 2007; 193: 557–66.
103. Mendrek A., Monterosso J., Simon S. L., Jarvik M., Brody A.,Olmstead R. et al. Working memory in cigarette smokers:comparison to non-smokers and effects of abstinence. AddictBehav 2006; 31: 833–44.
104. McClernon F. J., Addicott M. A., Sweitzer M. M. Smokingabstinence and neurocognition: implications for cessationand relapse. Curr Top Behav Neurosci 2015; 23: 193–227.
105. Freeman T. P., Morgan C. J., Beesley T., Curran H. V. Drugcue induced overshadowing: selective disruption of natu-ral reward processing by cigarette cues amongstabstinent but not satiated smokers. Psychol Med 2012;42: 161–71.
106. Waters A. J., Carter B. L., Robinson J. D., Wetter D. W., LamC. Y., Kerst W. et al. Attentional bias is associated withincentive-related physiological and subjective measures.Exp Clin Psychopharmacol 2009; 17: 247–57.
107. Canamar C. P., London E. Acute cigarette smoking reduceslatencies on a smoking Stroop test. Addict Behav 2012; 37:627–31.
108. Ashare R., Strasser A. A., Wileyto E. P., Cuevas J., Audrain-McGovern J. Cognitive deficits specific to depression-pronesmokers during abstinence. Exp Clin Psychopharmacol2014; 22: 323–31.
109. Hartlage S., Alloy L. B., Vázquez C., Dykman B. Automaticand effortful processing in depression. Psychol Bull 1993;113: 247–78.
110. Gotlib I. H., Joormann J. Cognition and depression: currentstatus and future directions. Annu Rev Clin Psychol 2010;6: 285–312.
111. Patterson F., Jepson C., Loughead J., Perkins K., Strasser A.A., Siegel S. et al. Working memory deficits predict short-term smoking resumption following brief abstinence. DrugAlcohol Depend 2010; 106: 61–4.
112. Powell J., Dawkins L.,West R., Powell J., PickeringA. Relapseto smoking during unaided cessation: clinical, cognitive andmotivational predictors. Psychopharmacology (Berl) 2010;212: 537–49.
113. Kassel J. D., Yates M., Brown R. A. Baseline reaction timepredicts 12-month smoking cessation outcome informerly depressed smokers. Psychol Addict Behav 2007;21: 415–9.
114. Malpass D., Higgs S. How is cigarette smoking maintained indepression? Experiences of cigarette smoking in people diag-nosed with depression. Addict Res Theory 2009; 17: 64–79.
115. Malpass D., Higgs S. Acute psychomotor, subjective andphysiological responses to smoking in depressed outpatientsmokers and matched controls. Psychopharmacology (Berl)2007; 190: 363–72.
116. Skinner B. F. The Behavior of Organisms: An ExperimentalAnalysis. Oxford, UK: Appleton-Century; 1938.
117. Pomerleau O. F., Pomerleau C. S. Neuroregulators and thereinforcement of smoking: towards a biobehavioral explana-tion. Neurosci Biobehav Rev 1984; 8: 503–13.
118. Carmody T. P. Affect regulation, tobacco addiction, andsmoking cessation. J Psychoact Drugs 1989; 21: 331–42.
119. Baker T. B., Piper M. E., McCarthy D. E., Majeskie M. R., FioreM. C. Addiction motivation reformulated: an affective pro-cessing model of negative reinforcement. Psychol Rev2004; 111: 33–51.
120. Koob G. F. Neurobiological substrates for the dark side ofcompulsivity in addiction. Neuropharmacology 2009; 56:18–31.
121. Koob G. F., Volkow N. D. Neurocircuitry of addiction.Neuropsychopharmacology 2010; 35: 217–38.
122. Belin D., Belin-Rauscent A., Murray J. E., Everitt B. J. Addic-tion: failure of control over maladaptive incentive habits.Curr Opin Neurobiol 2013; 23: 564–72.
123. Hull C. L. Principles of Behavior. New York:Appleton-Century-Crofts; 1943.
124. Miles F. J., Everitt B. J., Dickinson A. Oral cocaine seeking byrats: action or habit? Behav Neurosci 2003; 117: 927–38.
125. Dickinson A., Wood N., Smith J. W. Alcohol seeking by rats:action or habit? Q J Exp Psychol B 2002; 55: 331–48.
126. Corbit L. H., Nie H., Janak P. H. Habitual alcohol seeking:time course and the contribution of subregions of the dorsalstriatum. Biol Psychiatry 2012; 72: 389–95.
127. Dougher M. J., Hackbert L. Establishing operations, cogni-tion, and emotion. Behav Anal 2000; 23: 11–24.
128. Michael J. Establishing operations. Behav Anal 1993; 16:191–206.
129. Laraway S., Snycerski S., Olson R., Becker B., Poling A. Themotivating operations concept: current status and criticalresponse. Psychol Rec 2014; 64: 601–23.
130. Troisi J. R. 2nd. Sensation within the skin. ACS ChemNeurosci 2015; 6: 209–10.
131. Spring B., Pingitore R., McChargue D. E. Reward value ofcigarette smoking for comparably heavy smoking schizo-phrenic, depressed, and nonpatient smokers. Am JPsychiatry 2003; 160: 316–22.
132. Audrain-McGovern J., Wileyto E. P., Ashare R., Cuevas J.,Strasser A. A. Reward and affective regulationin depression-prone smokers. Biol Psychiatry 2014; 76:689–97.
133. Leventhal A. M., Trujillo M., Ameringer K. J., Tidey J. W.,Sussman S., Kahler C.W. Anhedonia and the relative rewardvalue of drugand nondrug reinforcers in cigarette smokers. JAbnorm Psychol 2014; 123: 375–86.
Smoking and depression 11
© 2016 Society for the Study of Addiction Addiction

134. Brandon T. H.,Wetter D.W., Baker T. B. Affect, expectancies,urges and smoking: do they conform to models of drugmotivation and relapse? Exp Clin Psychopharmacol 1996; 4:29–36.
135. Perkins K. A., Karelitz J. L., Giedgowd G. E., Conklin C. A.Negative mood effects on craving to smoke in women versusmen. Addict Behav 2013; 38: 1527–31.
136. Vinci C., Copeland A. L., CarriganM. H. Exposure to negativeaffect cues and urge to smoke. Exp Clin Psychopharmacol2012; 20: 47–55.
137. Payne T. J., Schare M. L., Levis D. J., Colletti G. Exposure tosmoking-relevant cues: Effects on desire to smoke and topo-graphical components of smoking behaviour. Addict Behav1991; 16: 467–79.
138. Fucito L. M., Juliano L. M., Toll B. A. Cognitive reappraisaland expressive suppression emotion regulation strategies incigarette smokers. Nicotine Tob Res 2010; 12: 1156–61.
139. Hitsman B., Spring B., Pingitore R., Munafò M., HedekerD. Effect of tryptophan depletion on the attentionalsalience of smoking cues. Psychopharmacology (Berl)2007; 192: 317–24.
140. Dennett D. C. Content and Consciousness. London, UK:Routledge; 2010.
141. Wiers R. W., Gladwin T. E., Hofmann W., Salemink E.,Ridderinkhof K. R. Cognitive bias modification and cognitivecontrol training in addiction and related psychopathologymechanisms, clinical perspectives, and ways forward. ClinPsychol Sci 2013; DOI: 10.1177/2167702612466547.
142. Rhodes J. D., Hawk L. W. Jr., Ashare R. L., Schlienz N. J.,Mahoney M. C. The effects of varenicline on attention andinhibitory control among treatment-seeking smokers.Psychopharmacology (Berl) 2012; 223: 131–8.
143. Mocking R. J., Patrick Pflanz C., Pringle A., Parsons E.,McTavish S. F., Cowen P. J. et al. Effects of short-termvarenicline administration on emotional and cognitiveprocessing in healthy, non-smoking adults: a randomized,double-blind, study. Neuropsychopharmacology 2013; 38:476–84.
144. Patterson F., Jepson C., Strasser A. A., Loughead J., PerkinsK. A., Gur R. C. et al. Varenicline improves mood and cogni-tion during smoking abstinence. Biol Psychiatry 2009; 65:144–9.
145. Lerman C., Niaura R., Collins B. N., Wileyto P.,Audrain-McGovern J., Pinto A. et al. Effect of bupropion ondepression symptoms in a smoking cessation clinical trial.Psychol Addict Behav 2004; 18: 362–6.
146. Catley D., Harris K. J., Okuyemi K. S., Mayo M. S., Pankey E.,Ahluwalia J. S. The influence of depressive symptoms onsmoking cessation among african americans an arandomized trial of bupropion. Nicotine Tob Res 2005; 7:859–70.
147. Niaura R., Britt D. M., Shadel W. G., Goldstein M., AbramsD., Brown R. Symptoms of depression and survival experi-ence among three samples of smokers trying to quit.Psychol Addict Behav 2001; 15: 13–17.
148. Piper M. E., Smith S. S., Schlam T. R., Fiore M. C., Jorenby D.E., Fraser D. et al. A randomized placebo-controlled clinicaltrial of 5 smoking cessation pharmacotherapies. Arch GenPsychiatry 2009; 66: 1253–62.
149. Smith S. S., McCarthy D. E., Japuntich S. J., Christiansen B.,Piper M. E., Jorenby D. E. et al. Comparative effectiveness of
5 smoking cessation pharmacotherapies in primary careclinics. Arch Intern Med 2009; 169: 2148–55.
150. Ebbert J. O., Hatsukami D. K., Croghan I. T., Schroeder D.R., Allen S. S., Hays J. T. et al. Combination vareniclineand bupropion sr for tobacco-dependence treatment incigarette smokers: a randomized trial. JAMA 2014; 311:155–63.
151. Brown R. A., Kahler C. W., Niaura R., Abrams D. B., Sales S.D., Ramsey S. E. et al. Cognitive–behavioral treatment fordepression in smoking cessation. J Consult Clin Psychol2001; 69: 471–80.
152. Brown R. A., NiauraR., Lloyd-Richardson E. E., StrongD. R.,Kahler C.W., Abrantes A. M. et al. Bupropion and cognitive–behavioral treatment for depression in smoking cessation.Nicotine Tob Res 2007; 9: 721–30.
153. Gierisch J. M., Bastian L. A., Calhoun P. S., McDuffie J. R.,Williams J. W. Jr. Smoking cessation interventions forpatients with depression: a systematic review andmeta-analysis. J Gen Intern Med 2012; 27: 351–60.
154. van der Meer R. M., Willemsen M. C., Smit F., Cuijpers P.Smoking cessation interventions for smokers with current orpast depression. Cochrane Database Syst Rev 2013; Issue 8.Art. No.: CD006102. DOI: 10.1002/14651858.CD006102.pub2.
155. Dimidjian S., Hollon S. D., Dobson K. S., Schmaling K.B., Kohlenberg R. J., Addis M. E. et al. Randomized trialof behavioral activation, cognitive therapy, and antide-pressant medication in the acute treatment of adultswith major depression. J Consult Clin Psychol 2006; 74:658–70.
156. MacPherson L., Tull M. T., Matusiewicz A. K., Rodman S.,Strong D. R., Kahler C. W. et al. Randomized controlled trialof behavioral activation smoking cessation treatment forsmokers with elevated depressive symptoms. J Consult ClinPsychol 2010; 78: 55–61.
157. Kassel J. D., Stroud L. R., Paronis C. A. Smoking, stress, andnegative affect: correlation, causation, and context acrossstages of smoking. Psychol Bull 2003; 129: 270–304.
158. Brandon T. H. Negative affect as motivation to smoke. CurrDir Psychol Sci 1994; 3: 33–7.
159. Piper M. E., Rodock M., Cook J. W., Schlam T. R., Fiore M. C.,Baker T. Psychiatric diagnoses among quitters versus con-tinuing smokers 3 years after their quit day. Drug AlcoholDepend 2013; 128: 148–54.
160. Hall F. S., Der-Avakian A., Gould T. J., Markou A., ShoaibM., Young J. W. Negative affective states and cognitiveimpairments in nicotine dependence. Neurosci BiobehavRev 2015; 58: 168–85.
161. McClaveA. K., Dube S. R., Strine T.W., Kroenke K., CaraballoR. S., Mokdad A. H. Associations between smoking cessationand anxiety and depression among U.S. Adults. Addict Behav2009; 34: 491–7.
162. Mykletun A., Overland S., Aaro L. E., Liabo H. M., Stewart R.Smoking in relation to anxiety and depression: Evidencefrom a large population survey: the HUNT study. Eur Psychi-atry 2008; 23: 77–84.
163. Berg C. J., Wen H., Cummings J. R., Ahluwalia J. S., Druss B.G. Depression and substance abuse and dependency in rela-tion to current smoking status and frequency of smokingamong nondaily and daily smokers. Am J Addict 2013; 22:581–9.
12 Amanda R. Mathew et al.
© 2016 Society for the Study of Addiction Addiction