children's grand round final 4x3 -...
TRANSCRIPT
5/26/16
1
2 | © 2015
• This presentation will take approximately one hour to complete.
VIEWING TIME
3 | © 2015
• This presentation is designed for primary care physicians.
• Other health care professionals working with patients and their families may also find this program of interest.
TARGET AUDIENCE
4 | © 2015
• It is the policy of Children’s Hospitals and Clinics of Minnesota to ensure balance, independence, objectivity and scientific rigor in all its educational programs. Our faculty have been asked to disclose to our program audience any real or apparent conflicts of interest related to the content of their presentations.
• They have also been requested to let you know when any products mentioned in their presentations are not labeled for the use under discussion or are still under investigation.
FACULTY DISCLOSURE
5 | © 2015
• Katy Schalla Lesiak, MSN/MPH, APRN; Catherine Wright, PsyD, MS, LPCC; and Dr. Julie Rabb, Psy.D. have disclosed no actual or apparent conflict of interest in relation to this educational activity.
• During this educational activity they will not be discussing the off-label use of commercial or investigational products not approved by the FDA.
SPEAKER FACULTY DISCLOSURE
Early Childhood Adversity and Toxic Stress: Practical tools for the primary care clinician
Grand Rounds May 19, 2016 Katy Schalla Lesiak, MSN/MPH, APRN Catherine Wright, PsyD, MS, LPCC Dr. Julie Rabb, Psy.D.
5/26/16
2
7 | © 2015
After completing this course, you will be able to:
1. Identify actions to take in a primary care setting to
promote healthy social-emotional development and
identify concerns that need more attention
2. Identify resources for referral, using a family-
centered approach
3. Recognize the benefit and availability of early
childhood mental health services within Children’s
and throughout Minnesota
Objectives
8 | © 2015
Children’s Disclaimers • Children's makes no representations or warranties about the accuracy, reliability,
or completeness of the content. Content is provided "as is" and is for informational use only. It is not a substitute for professional medical advice, diagnosis, or treatment. Children’s disclaims all warranties, express or implied, statutory or otherwise, including without limitation the implied warranties of merchantability, non-infringement of third parties’ rights, and fitness for a particular purpose.
• This content was developed for use in Children’s patient care environment and may not be suitable for use in other patient care environments. Children’s does not endorse, certify, or assess third parties’ competency. You hold all responsibility for your use or nonuse of the content. Children’s shall not be liable for claims, losses, or damages arising from or related to any use or misuse of the content.
• Please ask if you have any questions about these disclaimers.
9 | © 2015
Children’s Confidentiality Protections • This content and its related discussions are privileged and confidential under
Minnesota’s peer review statute (Minn. Stat. § 145.61 et. seq.). Do not disclose unless appropriately authorized. Notwithstanding the foregoing, content may be subject to copyright or trademark law; use of such information requires Children’s permission.
• This content may include patient protected health information. You agree to comply with all applicable state and federal laws protecting patient privacy and security including the Minnesota Health Records Act and the Health Insurance Portability and Accountability Act and its implementing regulations as amended from time to time.
• Please ask if you have any questions about these confidentiality protections.
10 | © 2015
• Children’s Hospitals and Clinics of Minnesota is accredited by the Minnesota Medical Association to provide continuing medical education for physicians.
• Children’s Hospitals and Clinics of Minnesota designates this educational activity for a maximum of 1 AMA PRA Category 1 Credit™
• Physicians should only claim credit commensurate with the extent of their participation in the activity.
• Children’s Hospitals and Clinics of Minnesota takes responsibility for the content, quality and scientific interest of these activities.
Accreditation
11 | © 2015
• It is the policy of Children’s Medical Education program that we cannot offer to retain CME records for physicians attending or viewing the online CME activity.
• The Minnesota Medical Association designates that physicians are responsible for maintaining their own CME records.
Retention of CME Records
12 | © 2015
• To receive CME credit, you must view the entire program. When the program is completed, click the Post Test button on the interface to access the Post Test.
• You must successfully pass the Post Test to receive CME credit.
Receiving CME Credit

5/26/16
3
Early Childhood Adversity and Toxic Stress:
Prac%cal tools for the primary care clinician
Katy Schalla Lesiak, MSN/MPH, APRN Minnesota Department of Health Catherine Wright, PsyD, MS, LPCC
Minnesota Department of Human Services
Children’s of Minnesota Grand Rounds 5/19/2016
Disclosure
• We have no disclosures to provide.
Objec=ves
ParNcipants will be able to… 1. IdenNfy acNons to take in their seSng to promote
healthy social-‐emoNonal development and idenNfy concerns that need more aUenNon
2. IdenNfy resources for referral, using a family-‐centered approach
3. Recognize the benefit and availability of early childhood mental health services within Children’s and throughout Minnesota
Social-‐emo=onal development (Infant and early childhood mental health)
The developing capacity of the child to • Experience, regulate and express emoNons • Form close and secure interpersonal relaNonships • Explore the environment and learn
…all in the context of family, community and culture www.zerotothree.org
What is early childhood mental health?
• Refers to children birth to five years • Interwoven with young child’s development and overall health
• Early intervenNon is the key to reverse the effects of adverse early experiences hUp://developingchild.harvard.edu/iniNaNves/council/
Promo=ng healthy social-‐emo=onal development in primary care • Recognize parent/primary caregiver as the infant’s most important partner in healthy development
• Model and encourage reciprocal communicaNon (serve and return) and responsive parenNng
• Talk, read, play with your baby • Promote posiNve parenNng
www.cdc.gov/ncbddd/childdevelopment/posiNveparenNng/index.html
• Provide anNcipatory guidance about development • Provide standardized screening to idenNfy and address concerns early

5/26/16
4
Strengthening Families www.cssp.org/reform/strengtheningfamilies/about
ProtecNve factors for healthy development • Parental resilience • Social connecNons • Knowledge of parenNng and child development • Concrete support in Nmes of need • Social and emoNonal competence of children
What can nega=vely impact development? • Exposure to trauma, significant loss with primary care givers
• DisrupNons in relaNonships with primary care givers because of parental mental illness, substance abuse, domesNc violence
• Biological Reasons • GeneNc inheritance; exposure to injury, infecNon, toxicants, nutriNonal deficiencies (in-‐utero or ader)
• Social/Environmental Stressors • Living in high risk neighborhoods; discriminaNon and racism; prolonged family stress due to death, divorce, extreme economic hardship, etc.
Ø Neurons to Neighborhoods, 2000 Ø ACE study (ongoing)-‐ www.acestudy.org
ADVERSE CHILDHOOD EXPERIENCES (ACE) STUDY
http://www.cdc.gov/ace/index.htm
22
ACEs in Minnesota (BRFSS 2011)
23
Minnesotans with more ACEs are more likely to have poor health
Toxic stress
• What is it? • Excessive or prolonged acNvaNon of the physiologic stress response systems
• Without buffering protecNve relaNonships • In contrast to posiNve or tolerable stress
• Why does it maUer? • Long-‐term effect on brain development, learning, behavior, physical & mental health
• Short-‐term vs. chronic stress responses Ø AAP (2011). Early childhood adversity, toxic stress and the role of the pediatrician: TranslaNng Developmental Science into Lifelong Health. Pediatrics.
5/26/16
5
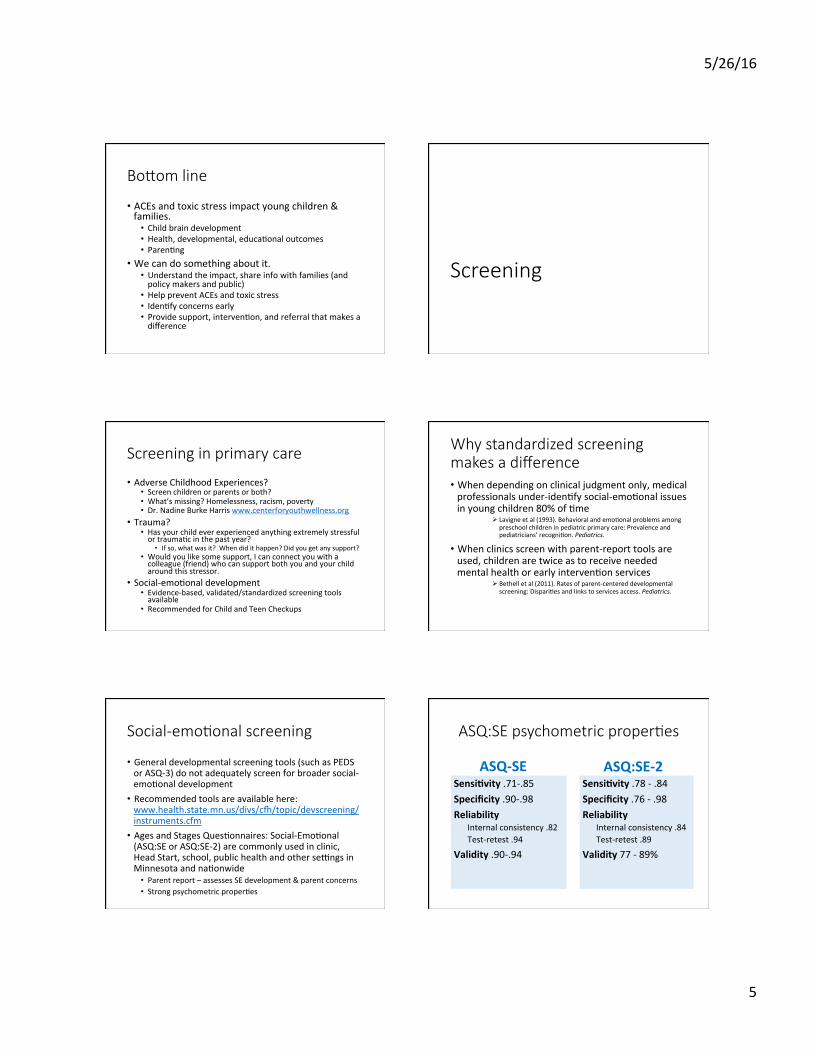
Bo[om line
• ACEs and toxic stress impact young children & families.
• Child brain development • Health, developmental, educaNonal outcomes • ParenNng
• We can do something about it. • Understand the impact, share info with families (and policy makers and public)
• Help prevent ACEs and toxic stress • IdenNfy concerns early • Provide support, intervenNon, and referral that makes a difference
Screening
Screening in primary care
• Adverse Childhood Experiences? • Screen children or parents or both? • What’s missing? Homelessness, racism, poverty • Dr. Nadine Burke Harris www.centerforyouthwellness.org
• Trauma? • Has your child ever experienced anything extremely stressful or traumaNc in the past year?
• If so, what was it? When did it happen? Did you get any support? • Would you like some support, I can connect you with a colleague (friend) who can support both you and your child around this stressor.
• Social-‐emoNonal development • Evidence-‐based, validated/standardized screening tools available
• Recommended for Child and Teen Checkups
Why standardized screening makes a difference • When depending on clinical judgment only, medical professionals under-‐idenNfy social-‐emoNonal issues in young children 80% of Nme
Ø Lavigne et al (1993). Behavioral and emoNonal problems among preschool children in pediatric primary care: Prevalence and pediatricians’ recogniNon. Pediatrics.
• When clinics screen with parent-‐report tools are used, children are twice as to receive needed mental health or early intervenNon services
Ø Bethell et al (2011). Rates of parent-‐centered developmental screening: DispariNes and links to services access. Pediatrics.
Social-‐emo=onal screening
• General developmental screening tools (such as PEDS or ASQ-‐3) do not adequately screen for broader social-‐emoNonal development
• Recommended tools are available here: www.health.state.mn.us/divs/cl/topic/devscreening/instruments.cfm
• Ages and Stages QuesNonnaires: Social-‐EmoNonal (ASQ:SE or ASQ:SE-‐2) are commonly used in clinic, Head Start, school, public health and other seSngs in Minnesota and naNonwide
• Parent report – assesses SE development & parent concerns • Strong psychometric properNes
ASQ:SE psychometric proper=es
ASQ-‐SE Sensi+vity .71-‐.85 Specificity .90-‐.98 Reliability
Internal consistency .82 Test-‐retest .94
Validity .90-‐.94
ASQ:SE-‐2 Sensi+vity .78 -‐ .84 Specificity .76 -‐ .98 Reliability
Internal consistency .84 Test-‐retest .89
Validity 77 -‐ 89%
5/26/16
6
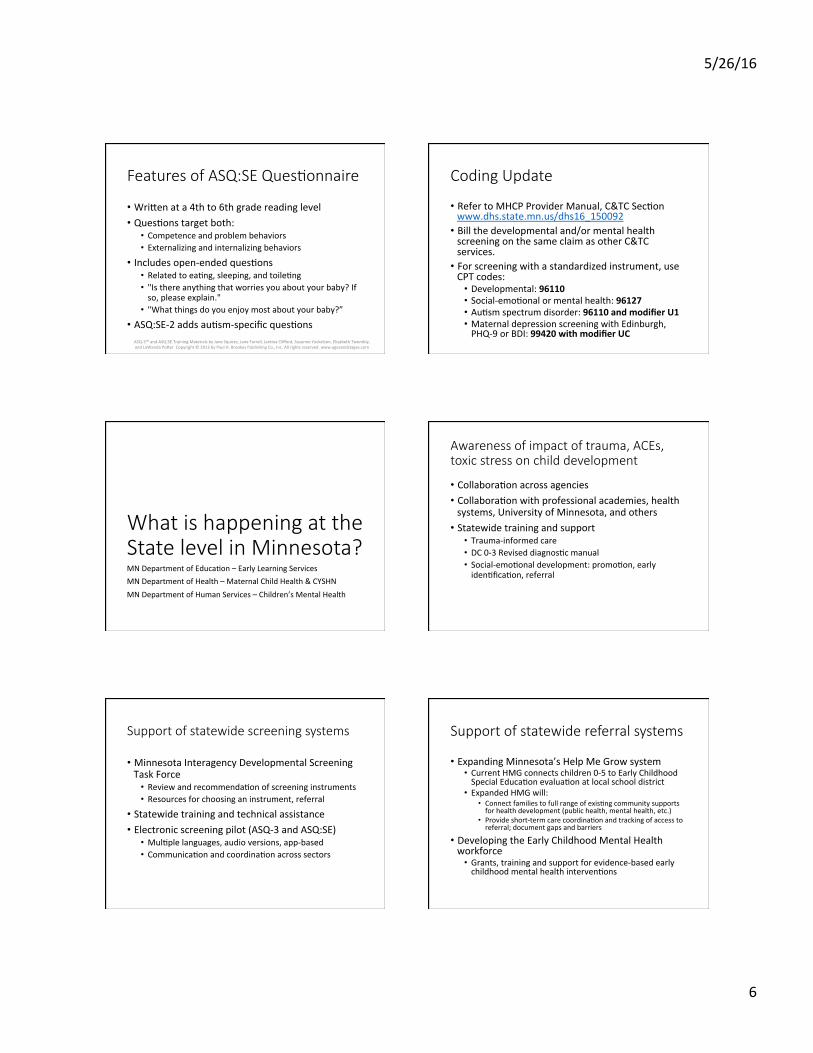
Features of ASQ:SE Ques=onnaire
• WriUen at a 4th to 6th grade reading level • QuesNons target both:
• Competence and problem behaviors • Externalizing and internalizing behaviors
• Includes open-‐ended quesNons • Related to eaNng, sleeping, and toileNng • "Is there anything that worries you about your baby? If so, please explain."
• "What things do you enjoy most about your baby?”
• ASQ:SE-‐2 adds auNsm-‐specific quesNons ASQ-‐3™ and ASQ:SE Training Materials by Jane Squires, Jane Farrell, JanNna Clifford, Suzanne Yockelson, Elizabeth Twombly, and LaWanda PoUer Copyright © 2013 by Paul H. Brookes Publishing Co., Inc. All rights reserved. www.agesandstages.com
Coding Update
• Refer to MHCP Provider Manual, C&TC SecNon www.dhs.state.mn.us/dhs16_150092
• Bill the developmental and/or mental health screening on the same claim as other C&TC services.
• For screening with a standardized instrument, use CPT codes:
• Developmental: 96110 • Social-‐emoNonal or mental health: 96127 • AuNsm spectrum disorder: 96110 and modifier U1 • Maternal depression screening with Edinburgh, PHQ-‐9 or BDI: 99420 with modifier UC
What is happening at the State level in Minnesota? MN Department of EducaNon – Early Learning Services MN Department of Health – Maternal Child Health & CYSHN MN Department of Human Services – Children’s Mental Health
Awareness of impact of trauma, ACEs, toxic stress on child development
• CollaboraNon across agencies • CollaboraNon with professional academies, health systems, University of Minnesota, and others
• Statewide training and support • Trauma-‐informed care • DC 0-‐3 Revised diagnosNc manual • Social-‐emoNonal development: promoNon, early idenNficaNon, referral
Support of statewide screening systems
• Minnesota Interagency Developmental Screening Task Force
• Review and recommendaNon of screening instruments • Resources for choosing an instrument, referral
• Statewide training and technical assistance • Electronic screening pilot (ASQ-‐3 and ASQ:SE)
• MulNple languages, audio versions, app-‐based • CommunicaNon and coordinaNon across sectors
Support of statewide referral systems
• Expanding Minnesota’s Help Me Grow system • Current HMG connects children 0-‐5 to Early Childhood Special EducaNon evaluaNon at local school district
• Expanded HMG will: • Connect families to full range of exisNng community supports for health development (public health, mental health, etc.)
• Provide short-‐term care coordinaNon and tracking of access to referral; document gaps and barriers
• Developing the Early Childhood Mental Health workforce
• Grants, training and support for evidence-‐based early childhood mental health intervenNons

5/26/16
7
Training MH clinicians on appropriate methods for diagnosis of young children
• Since 2004, CMH division has trained 1000 mental health professionals in the use of the DC:0-‐3R
• Developmentally appropriate diagnosNc process for children ages 0-‐4 years
• CMH provides ongoing mentoring support to clinicians on the use of DC:0-‐3R through a monthly case consultaNon.
• CMH partnered with the Minnesota Department of Health to idenNfy clinicians able to diagnosis and treat young children based on our list of 1000
• Over 350 clinicians across the state will see children under 5
Early Childhood Mental Health clinicians are trained in evidence-‐based treatments:
• Parent Child InteracNon Therapy (PCIT) Ages 3 – 7 years
• Trauma Informed-‐ Child Parent Psychotherapy (TI-‐CPP) Ages birth – 6 years
• AUachment Bio-‐behavioral Catch-‐up (ABC) Ages 6 months – 3 years
Referrals to EC MH (all ages, 0-‐5)
0%
5%
10%
15%
20%
25%
30%
Family County Other MH Provider
Head Start
Primary Care
EC Teacher
Special Ed Public Health Nurse
2011 2014
*Each of the following sources accounted for 1% or less of the referrals: IEIC, ECFE, Home Visitor, Rehabilitation, Crisis, County
What does our data say? Type of diagnos=c assessment: DC:03 and DSM
18.7% 15.9% 9.7%
5.0% 3.0%
76.0% 79.2% 85.8%
91.1% 92.6%
0.0% 10.0% 20.0% 30.0% 40.0% 50.0% 60.0% 70.0% 80.0% 90.0%
100.0%
2011 2012 2013 2014 2015
DSM DC:03R
Diagnosis Frequency Percent (%) 1 Adjustment disorder 778 17.9 2 Regulation Disorders of Sensory Processing 682 15.7 3 Anxiety Disorders 639 14.7 4 No DA information identified (code missing) 401 9.2 5 Posttraumatic Stress Disorder 347 8.0 6 Other Disorders of Childhood 182 4.2 7 Disruptive Behavior Disorders 174 4.0 8 Deprivation/Maltreatment Disorder 147 3.4 9 No Diagnosis Identified (code incorrect) 133 3.1 10 Other Disorders 112 2.6 11 Mixed Disorder of Emotional Expressiveness 94 2.2 12 Pervasive Developmental Disorder 88 2.0 13 Sensory Stimulation-Seeking 83 1.9 14 Disorder of Relating and Communicating 54 1.2 15 Anxiety Disorder NOS 52 1.2 16 Hypersensitive Type A: Negative Defiant 45 1.0 17 Disorders of Affect 34 0.8 18 Diagnosis on Axis I Deferred 27 0.6 19 Hypersensitive Type A: Fearful 25 0.6 20 Multisystem Developmental Disorder 23 0.5
5/26/16
8
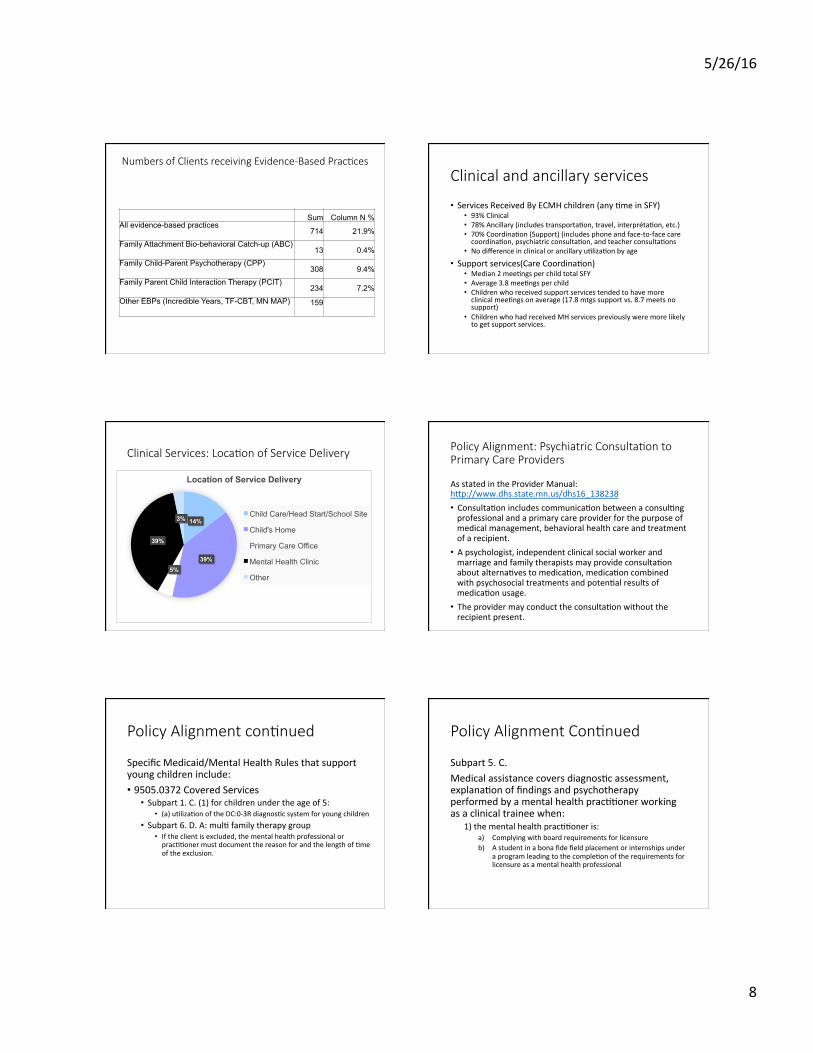
Numbers of Clients receiving Evidence-‐Based Prac=ces
Sum Column N % All evidence-based practices 714 21.9% Family Attachment Bio-behavioral Catch-up (ABC) 13 0.4% Family Child-Parent Psychotherapy (CPP) 308 9.4% Family Parent Child Interaction Therapy (PCIT) 234 7.2% Other EBPs (Incredible Years, TF-CBT, MN MAP) 159
Clinical and ancillary services
• Services Received By ECMH children (any Nme in SFY) • 93% Clinical • 78% Ancillary (includes transportaNon, travel, interprétaNon, etc.) • 70% CoordinaNon (Support) (includes phone and face-‐to-‐face care coordinaNon, psychiatric consultaNon, and teacher consultaNons
• No difference in clinical or ancillary uNlizaNon by age • Support services(Care CoordinaNon)
• Median 2 meeNngs per child total SFY • Average 3.8 meeNngs per child • Children who received support services tended to have more clinical meeNngs on average (17.8 mtgs support vs. 8.7 meets no support)
• Children who had received MH services previously were more likely to get support services.
Clinical Services: Loca=on of Service Delivery
14%
39% 5%
39%
3%
Location of Service Delivery
Child Care/Head Start/School Site
Child's Home
Primary Care Office
Mental Health Clinic
Other
Policy Alignment: Psychiatric Consulta=on to Primary Care Providers
As stated in the Provider Manual: hUp://www.dhs.state.mn.us/dhs16_138238 • ConsultaNon includes communicaNon between a consulNng professional and a primary care provider for the purpose of medical management, behavioral health care and treatment of a recipient.
• A psychologist, independent clinical social worker and marriage and family therapists may provide consultaNon about alternaNves to medicaNon, medicaNon combined with psychosocial treatments and potenNal results of medicaNon usage.
• The provider may conduct the consultaNon without the recipient present.
Policy Alignment con=nued
Specific Medicaid/Mental Health Rules that support young children include: • 9505.0372 Covered Services
• Subpart 1. C. (1) for children under the age of 5: • (a) uNlizaNon of the DC:0-‐3R diagnosNc system for young children
• Subpart 6. D. A: mulN family therapy group • If the client is excluded, the mental health professional or pracNNoner must document the reason for and the length of Nme of the exclusion.
Policy Alignment Con=nued
Subpart 5. C. Medical assistance covers diagnosNc assessment, explanaNon of findings and psychotherapy performed by a mental health pracNNoner working as a clinical trainee when:
1) the mental health pracNNoner is: a) Complying with board requirements for licensure b) A student in a bona fide field placement or internships under
a program leading to the compleNon of the requirements for licensure as a mental health professional

5/26/16
9
Policy Alignment Con=nued:
2013 Changes to Minnesota Statutes/ benefits in the process of being created: • 256b.0625 Subd. 62: Mental health clinical care consultaNon.
• Allowing a treaNng mental health professional or clinical trainee to bill Medicaid for providing consultaNon to another professional about a child’s clinical needs.
• Example: Talking with a child’s childcare teacher, primary care physician, public health nurse to ensure mental health and other services are aligned.
• This benefit is for children ages birth to 21 with complex and chronic condiNons, including early childhood mental health condiNons.
• The State Plan Amendment to the Center for Medicaid Services and our legislature have approved this benefit. It is available as of January 1, 2015.
Policy Alignment Con=nued:
Changes to Minnesota Statutes/ benefits in process: 256B.0946 INTENSIVE TREATMENT IN FOSTER CARE-‐ • Providing holisNc therapeuNc services to a child in foster care (wrapping clinical, mental health services around the biological and foster family) in order to reduce disrupNons in placement and reduce negaNve outcomes on children.
• Services include helping children get an intensive clinical mental health service while sNll meeNng (respecNng) their permanency needs and rights
• Use current systems to increase access for children who need an intense level of mental health service
• Create more flexible, coordinated service delivery among all child’s team members (parents, foster parents and professionals)
• Strengthen treatment and permanency planning with consultaNon, psychoeducaNon and therapy services to support successful out-‐of-‐home placements
• Promote evidence based pracNces and outcome measures to improve results for children in foster care
Contact us with other ques=ons:
Katy Schalla Lesiak, MSN/MPH, APRN-‐CPNP Child and Teen Checkups (C&TC), Early Childhood Comprehensive Systems Coordinator Maternal Child health Minnesota Department of Health [email protected] Catherine Wright, PsyD, MS, LPCC Early Childhood Mental Health System Coordinator, Children’s Mental Health Minnesota Department of Human Services [email protected]
What’s happening at Children’s Hospitals and Clinics of Minnesota? Julie Rabb, PsyD, LP Clinical Psychologist – Psychological Services Children’s Hospitals and Clinics of Minnesota [email protected]
Children’s Early Childhood Ini=a=ves
1. Mosaic in Primary Care -‐ Teaming with medical providers -‐ Universal screening -‐ Brief in-‐clinic intervenNons -‐ Consistent follow-‐up
2. Research -‐ Toxic Stress and Health -‐ Partnership with Harvard Center for the Developing
Child and the University of MN
Children’s Early Childhood Ini=a=ves, con=nued 3. Psychology Services
-‐ Partnership with Children’s Hospital AssociaNon -‐ Increased capacity for services 0-‐6 -‐ Two generaNon model for intervenNons
4. Group Pilot -‐ Parents with children 0-‐3 -‐ Special Medical Needs -‐ AUachment and development
5/26/16
10
Early Childhood Mental Health clinicians are trained in evidence-‐based treatments:
• Parent Child InteracNon Therapy (PCIT) Ages 3 – 7 years
• Trauma Informed-‐ Child Parent Psychotherapy (TI-‐CPP) Ages birth – 6 years
• AUachment Bio-‐behavioral Catch-‐up (ABC) Ages 6 months – 3 years
Children’s Early Childhood Ini=a=ves, con=nued 3. Psychology Services
-‐ Partnership with Children’s Hospital AssociaNon -‐ Increased capacity for services 0-‐6 -‐ Two generaNon model for intervenNons
4. Group Pilot -‐ Parents with children 0-‐3 -‐ Special Medical Needs -‐ AUachment and development
Children’s Ini=a=ves -‐ Contact
Dr. Julie Rabb, Psy.D. Psychology Services
St. Paul 651-‐220-‐6815
Top 3 take away points:
1. Early childhood social-‐emoNonal and brain development maUers, and toxic stress and ACEs impact that development.
2. There’s something we can do: • Advocate and educate • Support parents/caregivers as babies’ most important developmental partner
• Screen, idenNfy concerns early, refer to appropriate resources
• Collaborate within and outside of your seSng for systems improvements
3. Resources are available and emerging over Nme.
To receive CME credit, please click
the “Post Test” button on the interface below, and complete the post test.
Thank you for viewing this presentation!