chest.ppt
DESCRIPTION
kjbhjgbjTRANSCRIPT

بسم الله الرحمن الرحيم

CHEST

Indications for Chest X-ray• Cough• Haemoptysis• Fever• Chest pain• Trauma• Pre-operative• Check up• Metastatic work & Staging

NORMAL CHEST X-RAY
ViewsPA – Lateral – Supine
Deep Inspiration
Centeringmedial ends of clavicle equidistant from spine

PA VIEW

LAT VIEW
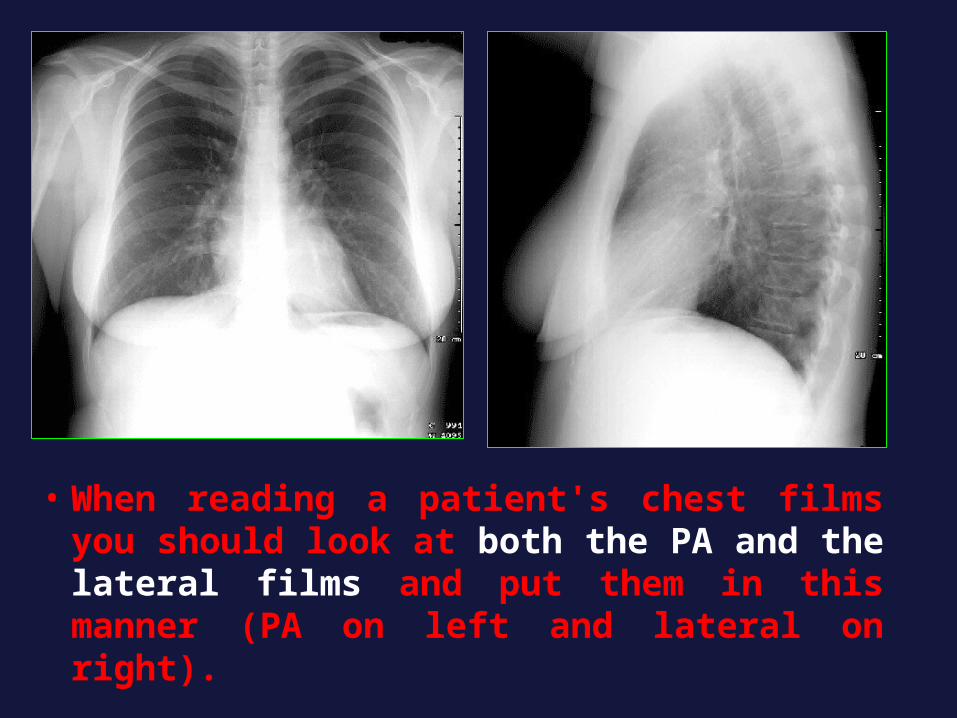
• When reading a patient's chest films you should look at both the PA and the lateral films and put them in this manner (PA on left and lateral on right).

This image outlines the specific anatomy of the PA chest x-ray.

HEART
How to read the chest X ray?from the periphery towards the centre
Via 4 circles

1st circle = outside the bony thorax (skin, soft tissues, breasts and sub-diaphragmatic area)

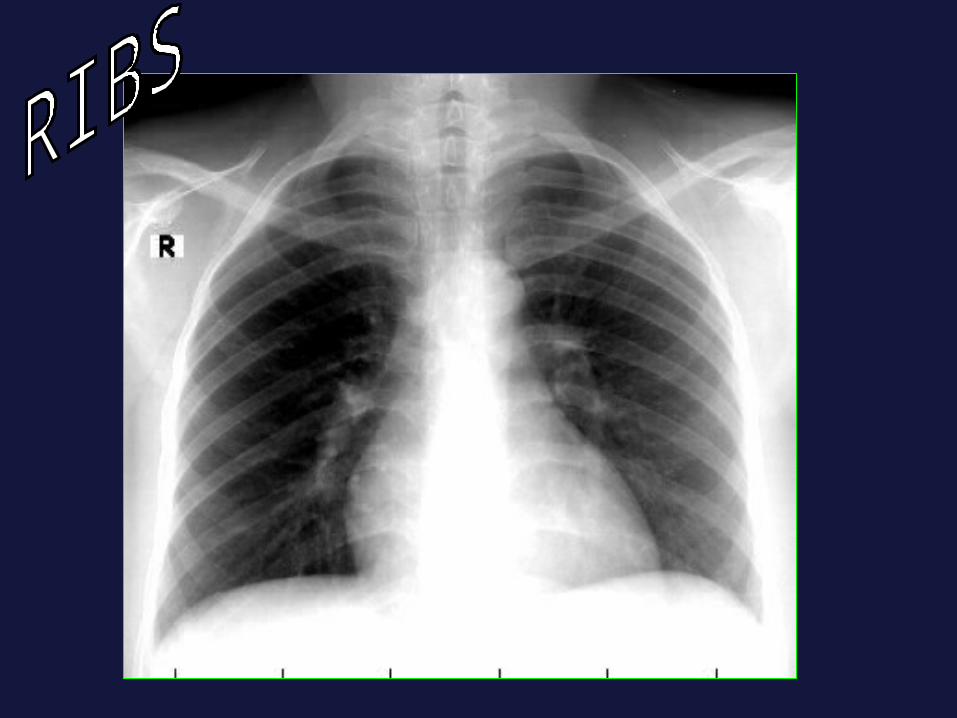
2nd circle = the bony thorax and diaphragms
AA

• 3rd circle =
Pleura: Fissures, AnglesLungs: translucency vascular markings
Read the lung parenchyma « from top to bottom and from left to right ».

• 4th circle = Mediastinum
Trachea. Heart. Vessels. Nodes.

Chest Radiographic Findings • Focal pulmonary lesion.• Diffuse pulmonary lesion.• Pleural diseases.• Cardiomediastinal abnormalities.• Lymphadenopathy.• Bone and soft tissue abnormalities.• Below the diaphragm.

localization
2nd
4th

Answer the following questions
• Is there a lesion?• Where is the lesion localization?• What is the character of the lesion?
WhiteBlack
White & Black

White
Mass or nodule
Mediastinal
Pleural
Chest wall
lungs ill defined Not a mass
Collapse or fibrosis infilterative
Alveolar Interstitial
Air bronchogram
silhouetteNodular / Reticular
Well defined
Loss of volume
Single or multiple

Black
Emphysema
Bulla
pneumothorax
Air cyst
White & Black
AbscessBronchiectasis
cavitationDiaphragm
PleuraAchalasia

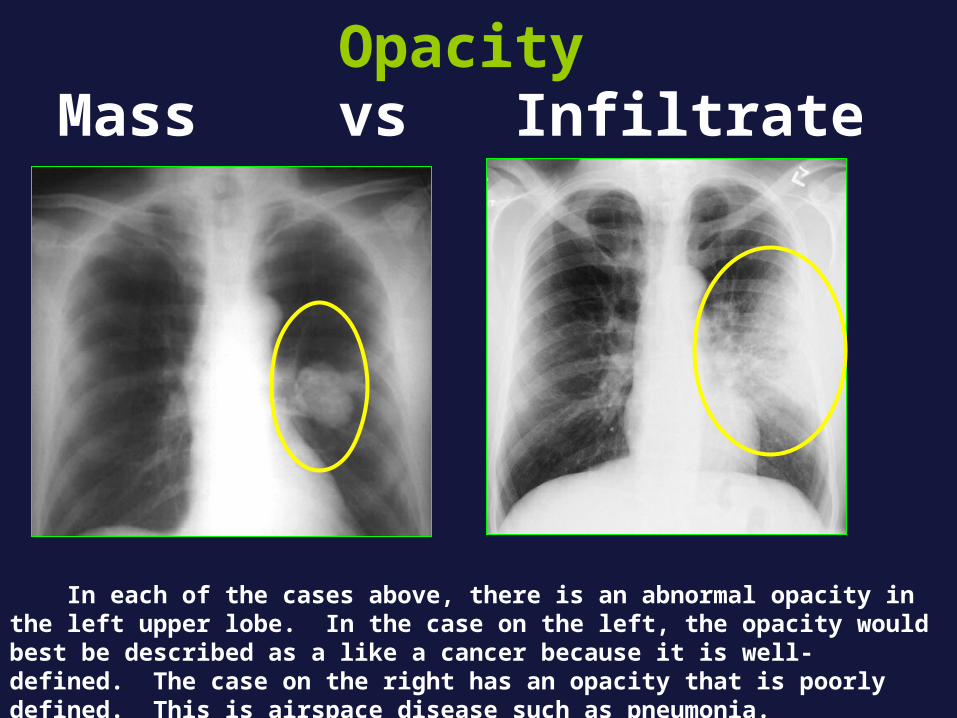
Opacity Mass vs Infiltrate
In each of the cases above, there is an abnormal opacity in the left upper lobe. In the case on the left, the opacity would best be described as a like a cancer because it is well-defined. The case on the right has an opacity that is poorly defined. This is airspace disease such as pneumonia.

Pulmonary Lesions
Focal:• Patchy area• Nodular opacity• Mass lesion• Cavitary lesion
Diffuse:• Reticular• Nodular• Ground glass veiling• Cystic

Patchy area
• Pneumonia• Infarct

RUL pneumonia

Right Lower Lobe PneumoniaRight Lower Lobe Pneumonia

Pulmonary infarct

Embolus in right pulmonary artery

Multiple pulmonary infarctions

Nodules and Masses
Single or multiple Size Border definition Calcification Location

Pulmonary Nodule 1. Tuberculoma.2. Hamartoma.3. Peripheral Br. CA.4. Metastasis.5. AVM.
Pulmonary Mass 1. Br. CA.2. Metastasis.3. Hydatid (Cystic)

Pulmonary Nodule
A nodule that is unchanged for two years is almost benign.
If the nodule is completely calcified or has central or stippled calcium it is benign.
Less than 3 cm is a nodule
Larger than 3cm is a mass

MassMass
CalcificationCalcification
Well-DefinedWell-Defined
Ill-DefinedIll-Defined

Apical TBApical TB

Lesion character
Lesion location
Lesion pathology
Pulm AVMPulm AVM


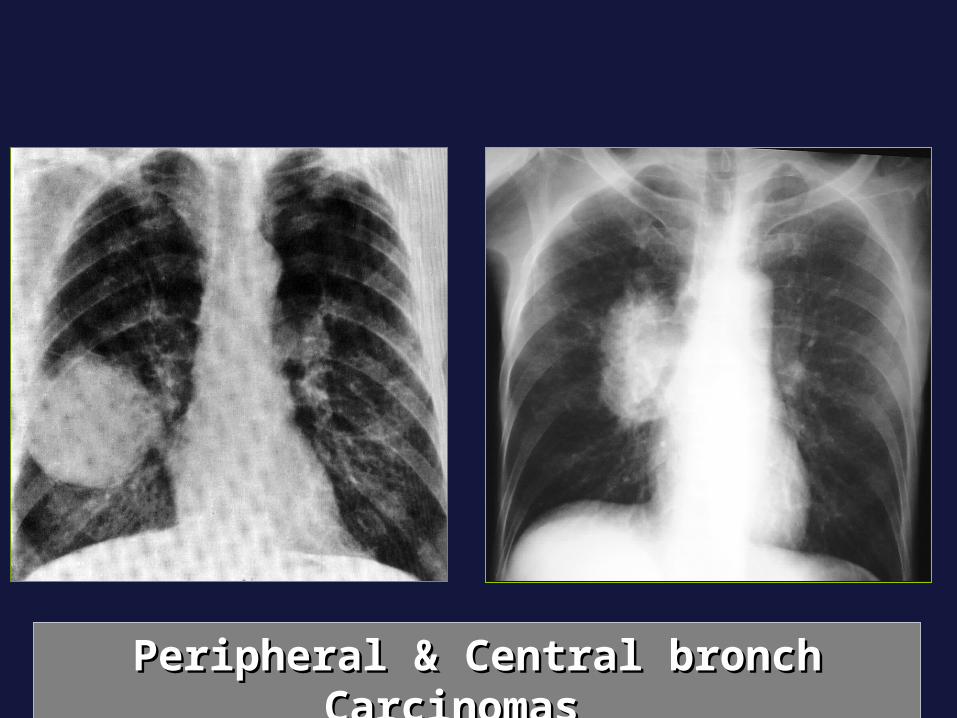
Peripheral & Central bronch Carcinomas Peripheral & Central bronch Carcinomas
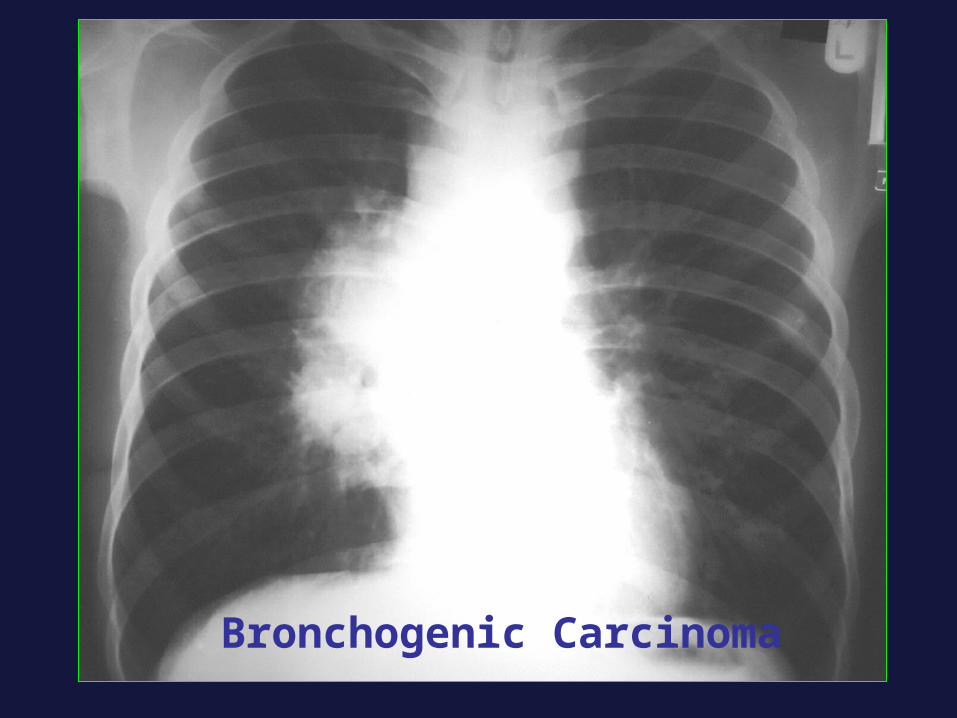
Bronchogenic Carcinoma



Alveolar Lung Diseases
• Pneumonia• Pulmonary edema• Pulmonary hemorrhage• Aspiration

Pulmonary edema
• Fluffy
• Indistinct margins, Confluent
• In both upper lobes
• air bronchograms.
• This is an alveolar (airspace) disease,
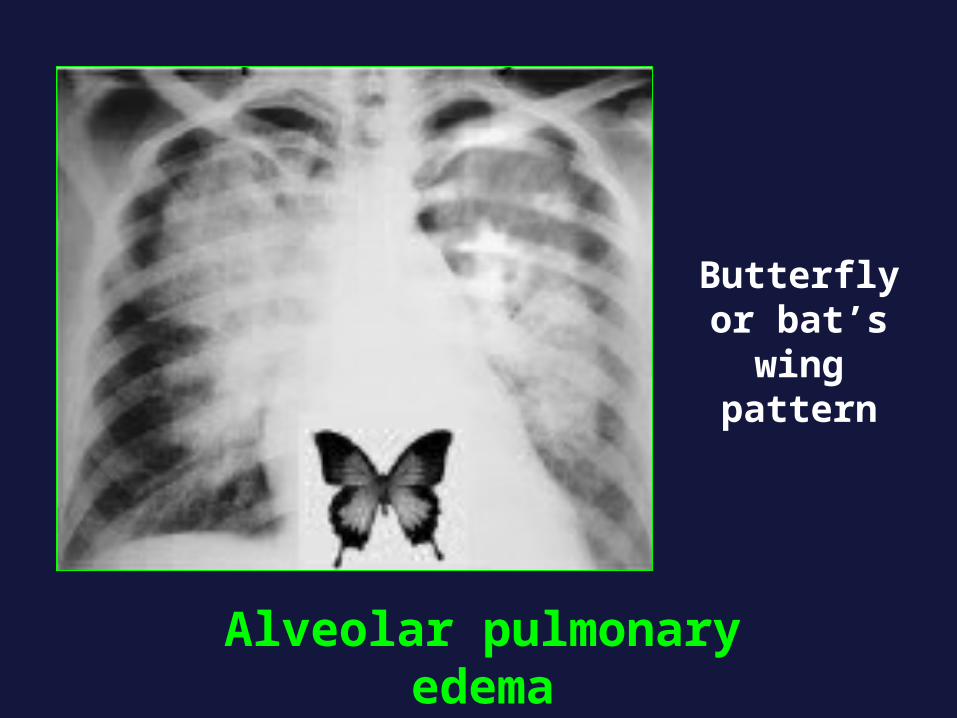
Alveolar pulmonary edema
Butterfly or bat’s wing
pattern

Pulmonary Lesions
Focal:• Patchy area• Nodular opacity• Mass lesion• Cavitary lesion
Diffuse:• Reticular• Nodular• Ground glass veiling• Cystic

Cysts & Cavities• Abnormal pulmonary parenchymal space.
• Not containing lung but filled with air and/or fluid.
• Congenital or acquired.
• Wall thickness greater than 1 mm
Cavitary Lung Lesions Carcinoma TB Abscess. Bulla Pneumatocele Thickness of the wall
Inner margin Air-fluid level Number

BenignBenign Cavities : Cavities :CryptococcusCryptococcus
• max wall thickness max wall thickness 4 mm4 mm• minimally irregular inner liningminimally irregular inner lining

Indeterminate CavitiesIndeterminate Cavities
• max wall thickness 5-15 mmmax wall thickness 5-15 mm• mildly irregular inner liningmildly irregular inner lining

MalignantMalignant Cavities: Squamous Cell Ca Cavities: Squamous Cell Ca• max wall thickness max wall thickness 16 mm16 mm• Irregular inner liningIrregular inner lining

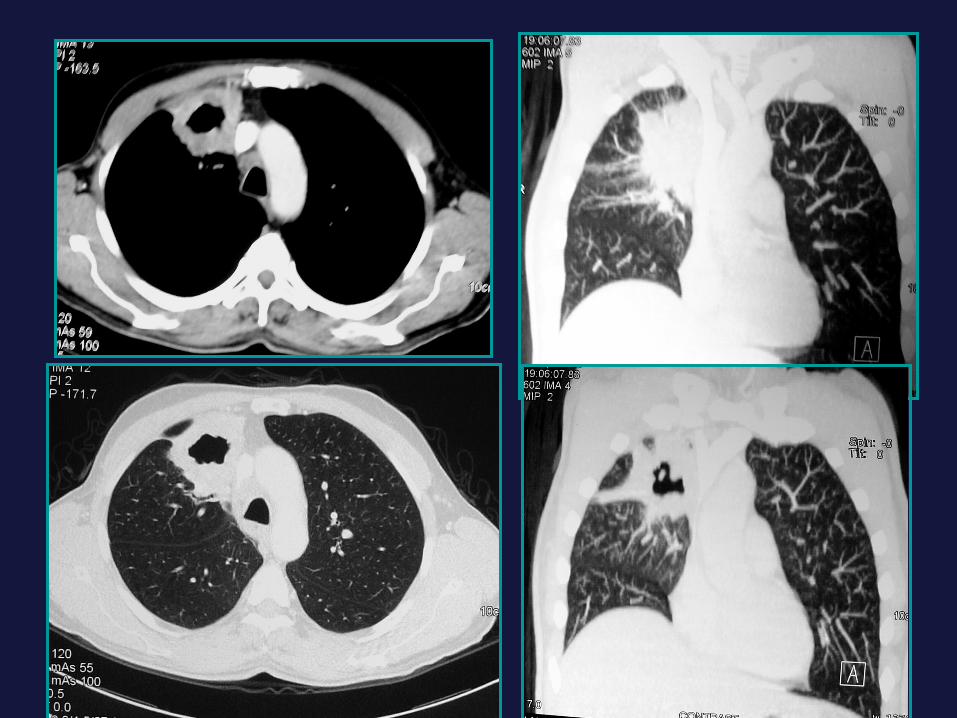
Thick-wall with nodular inner margin carcinoma of left lower lobe

Thin-walled with smooth inner margins RUL Tuberculosis


Carcinoma
TB
Abscess
Thickness ofWall Inner Margin A|F Level
Thick
Thick
Thin
Nodular
Smooth
Smooth
No
Yes
+/-
Cavities

COPD• Emphysema is loss of elastic recoil of the
lung with irreversible destruction of alveolar septa .
• It is caused most often by cigarette smoking and less commonly by alpha-1 antitrypsin deficiency.

X-Ray findings are:
• Diffuse hyperinflation• Flattened diaphragms • Increased retrosternal space (barrel
shaped chest) • Altered cardiac configuration (ribbon
shaped heart)• Attenuated peripheral vasculature


• Bullae (lucent, air-containing spaces that have no vessels), small or involve the whole hemithorax, infected (air-fluid level)
• Enlargement of PA (cor pulmonale) • Chronic bronchitis commonly occurs
in patients with emphysema and is associated with bronchial wall thickening.

Bullae

Atelectasis • Atelectasis is collapse or incomplete
expansion of the lung or part of the lung.
• It is most often caused by an endobronchial lesion, such as mucus plug or tumor. It can also be caused by extrinsic compression centrally by a mass such as lymph nodes or peripheral compression by pleural effusion.
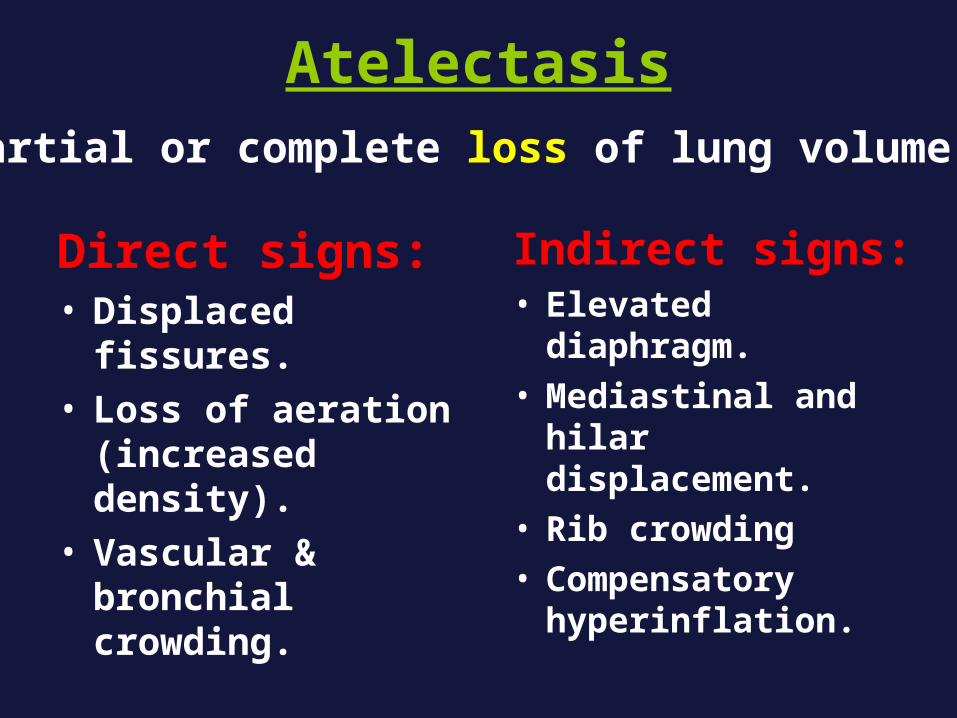
Atelectasis
Direct signs:• Displaced fissures.• Loss of aeration
(increased density).• Vascular &
bronchial crowding.
Indirect signs:• Elevated diaphragm.• Mediastinal and
hilar displacement.• Rib crowding• Compensatory
hyperinflation.
Partial or complete loss of lung volume.
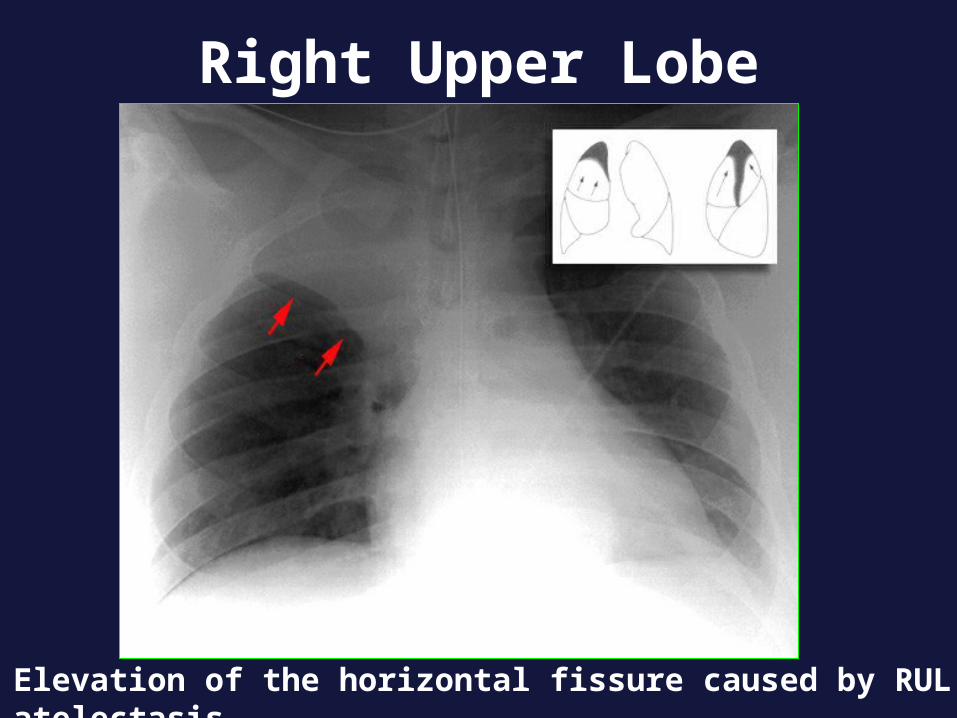
Elevation of the horizontal fissure caused by RUL atelectasis.
Right Upper Lobe

Right middle lobe atelectasis can be difficult to detect in the PA film. The right heart border is indistinct on the PA film. The lateral shows marked decrease in the distance between the horizontal and oblique fissures.
Right Middle Lobe
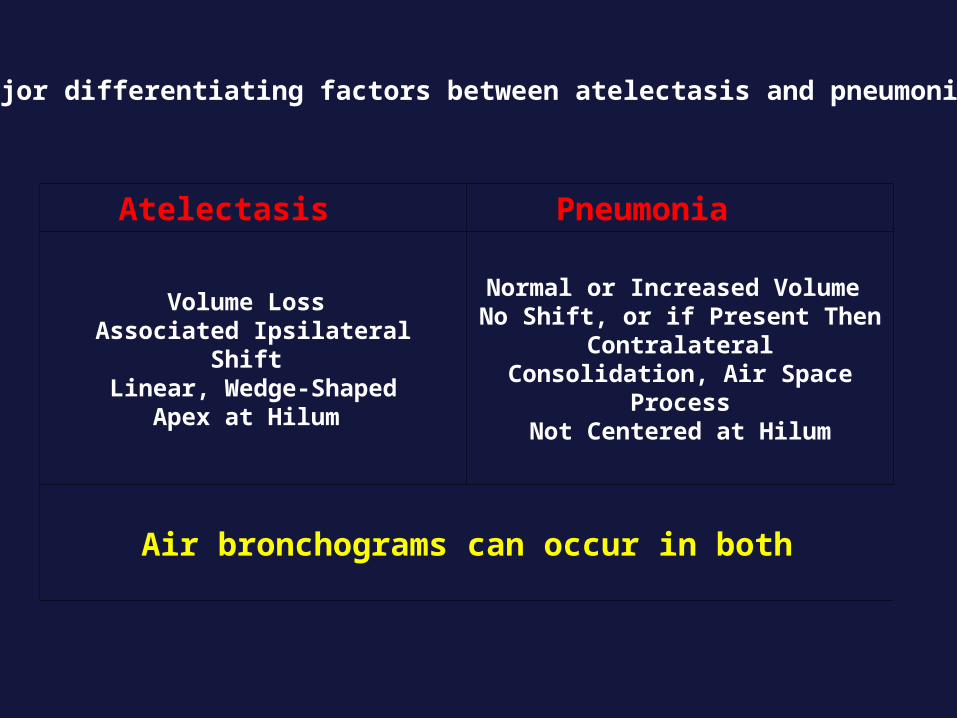
Major differentiating factors between atelectasis and pneumonia
Atelectasis Pneumonia
Volume Loss Associated Ipsilateral Shift
Linear, Wedge-ShapedApex at Hilum
Normal or Increased Volume No Shift, or if Present Then
ContralateralConsolidation, Air Space Process
Not Centered at Hilum
Air bronchograms can occur in both

Tuberculosis (TB)• Mycobacterium tuberculosis.Primary TB:The organism settle in an alveolus
anywhere and spread to regional LN (Ghon’s focus)
Post primary TB:Due to reinfection rather than
reactivation.

Pulmonary changes:1ry:PRIMARY COMPLEX• Ghon’s focus• Ipsilateral lymphadenopathy• Pleural effusionPost 1ry:• Consolidation in the apical segments of the
lower lobe, patchy, and may be bilateral• Fibrosis and volume loss, pulled trachea• Cavities (single or multiple, small or large)• Calcification may occur

• Tuberculous bronchopneumonia:Patchy nodular infiltrations.• Miliary TB:1-2 mm discrete, small nodules
(haematogenous spread)• Tuberculmoa:Localized granuloma, commonly
calcified.• Airway involvement:Collapse by LN or bronchial stenosis




Bronchiectasis
• Abnormal and permanent dilatation of the bronchi, most often secondary to an infectious process.
Types• Cylindrical (Tubular)• Varicose • Cystic (Saccular)

Etiology:• Cystic fibrosis • Bronchial wall weakness • Infection.• Obstruction (e.g neoplasms, foreign body)• Inhalation and aspiration (e.g ammonia,
gastric aspiration, heroin overdose) • Impaired host defense (e.g allergic
bronchopulmonary aspergillosis).• Inflammation (e.g bronchiolitis obliterans)

BronchiectasisBronchiectasis

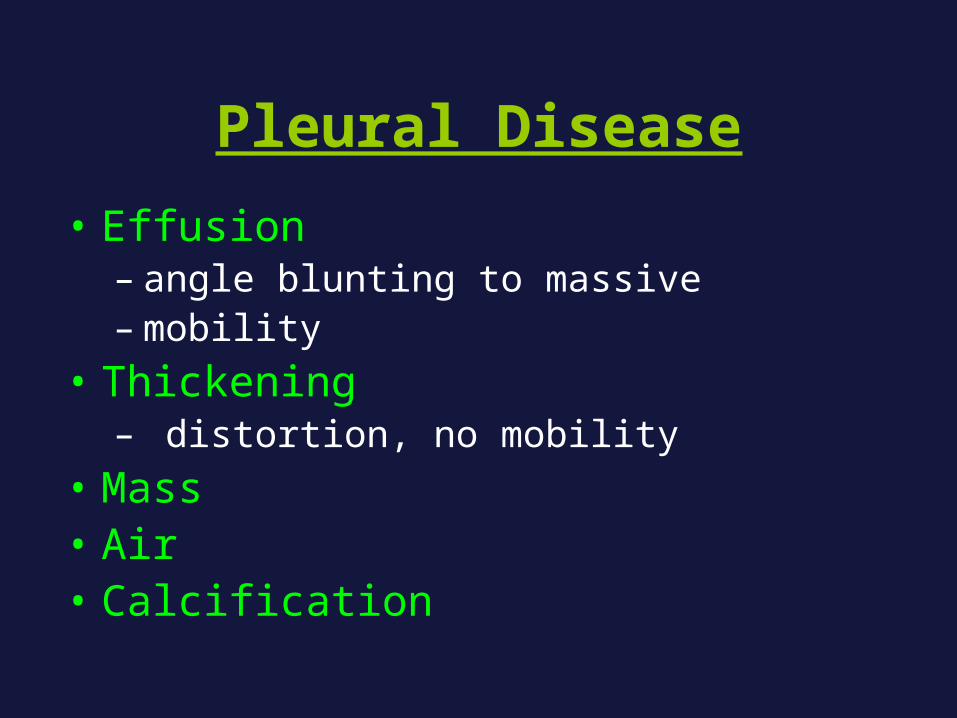
Pleural Disease• Effusion
– angle blunting to massive– mobility
• Thickening– distortion, no mobility
• Mass• Air• Calcification

Pleural effusion
• Transudate:• Cardiac failure• Hepatic failure• Nephrotic syndrome• Meig’s syndrome
• Exudate• Infection• Malignancy• Pulmonary infarction• Collagen vascular
diseases.• Subphrenic abscess• Pancreatitis

• Haemprrhagic:• Bronchogenic ca.• Trauma• Pulmonary infarction• Bleeding disorders
• Chylous:• Obstructed thoracic
duct• Traumatic injury to
the thoracic duct




Empyema

Subpulmonic EffusionSubpulmonic Effusion

Pneumothorax • Spontaneous• Traumatic• Secondary to
pneumomediastinum & pneumoperitoneum
• Secondary to lung dis (emphysema, cystic fibrosis, neoplasms)


PNEUMOTHORAX

PNEUMOTHORAX
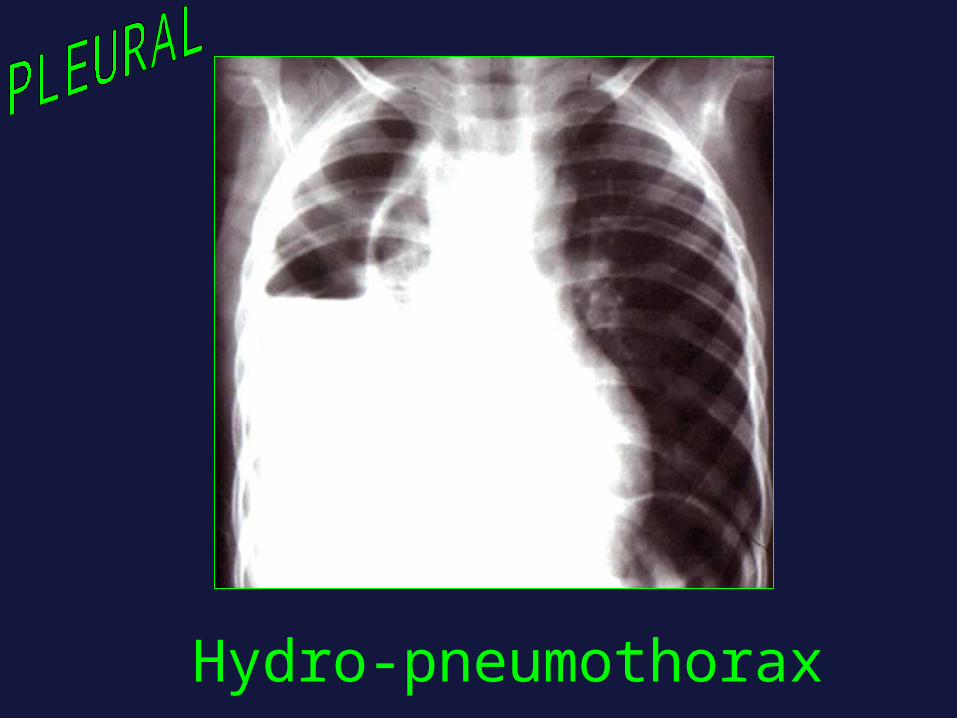
Hydro-pneumothorax

Hydro-pneumothorax

Pleural CalcificationPleural Calcification

Pleural masses
• Loculated pleural effusion• Metastases• Malignant mesothelioma• Pleural fibroma


Opaque Hemi thorax• Pleural effusion• Atelectasis• Post Pneumonectomy• Pneumonia• Mass

• In atelectasis, there is s shift toward the side of the opacification
• In pleural effusion, there is a shift away from the side of the opacification
• In pneumonia, there is no shift, There may be an air bronchogram sign present
• In pneumonectomy, the 5th rib is usually absent

Which is this?

Which is this?

Which is this?
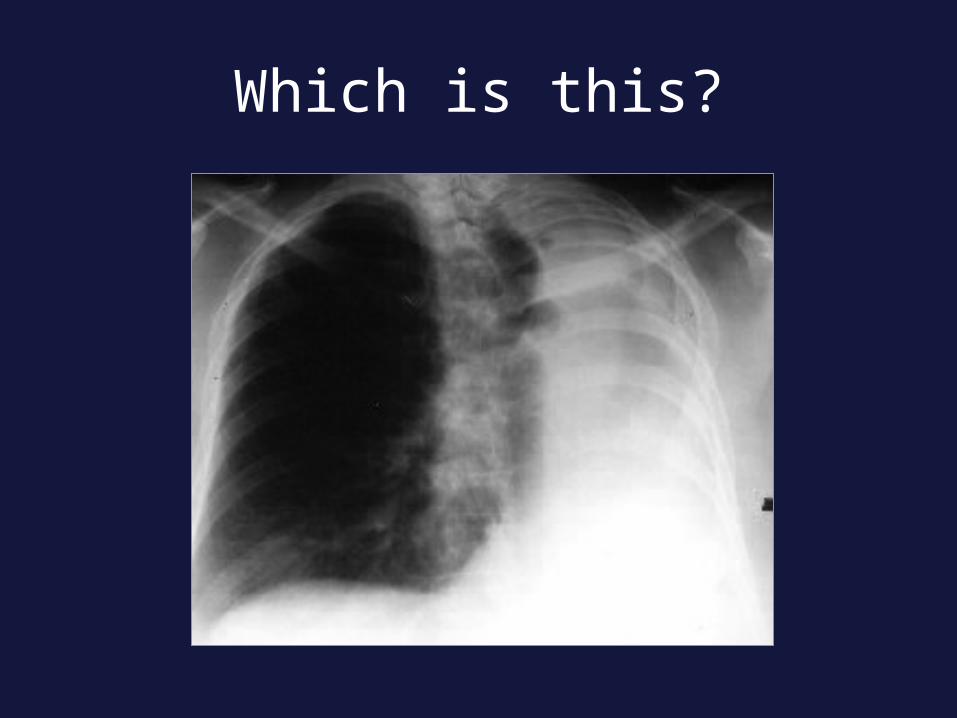
Which is this?

Lymphadenopathy
Non-specific presentations: mediastinal widening hilar prominence
Specific patterns: particular station enlargement


Right Paratracheal Right Paratracheal LymphadenopathyLymphadenopathy

Right Hilar LANRight Hilar LAN
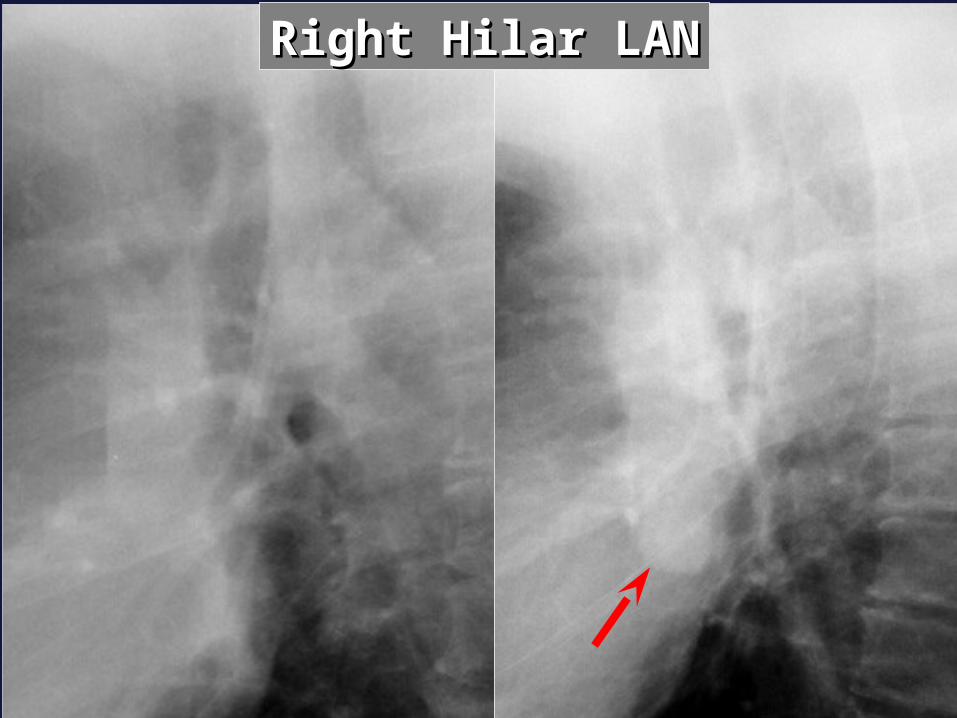
Right Hilar LANRight Hilar LAN

Left Hilar LANLeft Hilar LAN

Subcarinal LANSubcarinal LAN
*
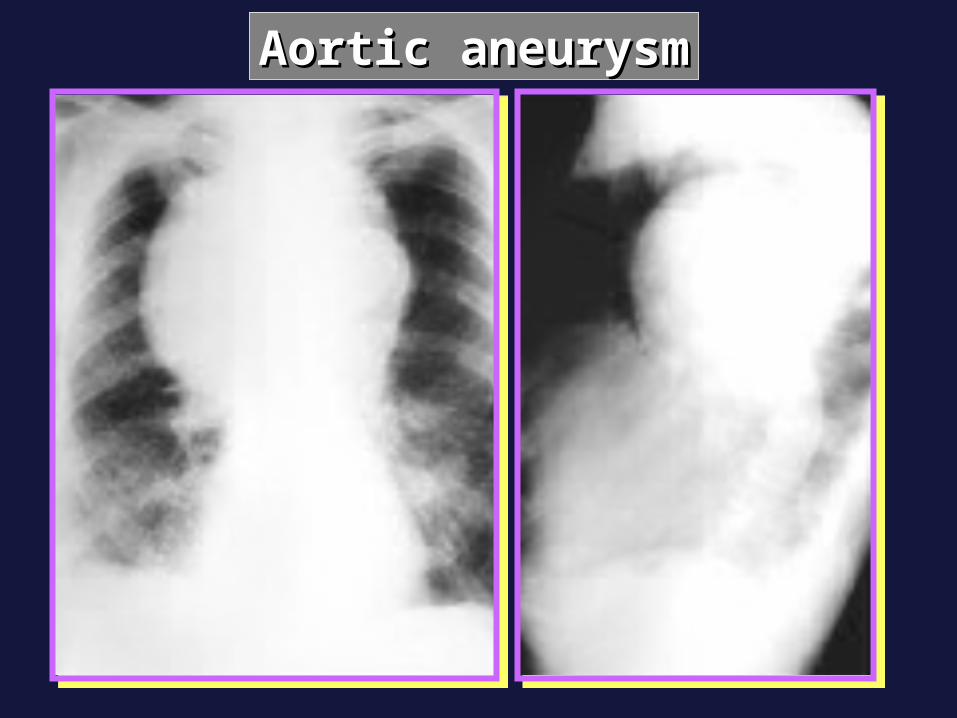
Aortic aneurysmAortic aneurysm

TRAUMA

Pulmonary trauma (laceration) Pleural trauma (haemo,
pneuomthorax). Skeletal trauma (ribs, sternum,
spine, scapula, joints).

Vascular trauma (dissection, rupture). Diaphragmatic trauma (rupture, hernia) Oesophygeal trauma (rupture,
laceration, FB)
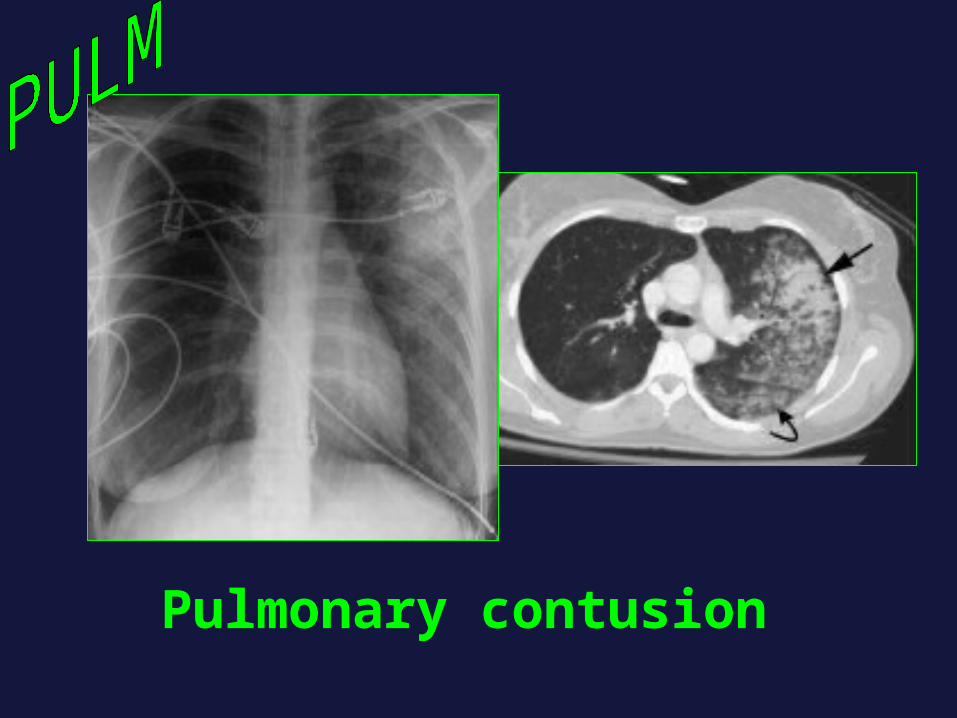
Pulmonary contusion

Pulmonary laceration

PNEUMOTHORAX
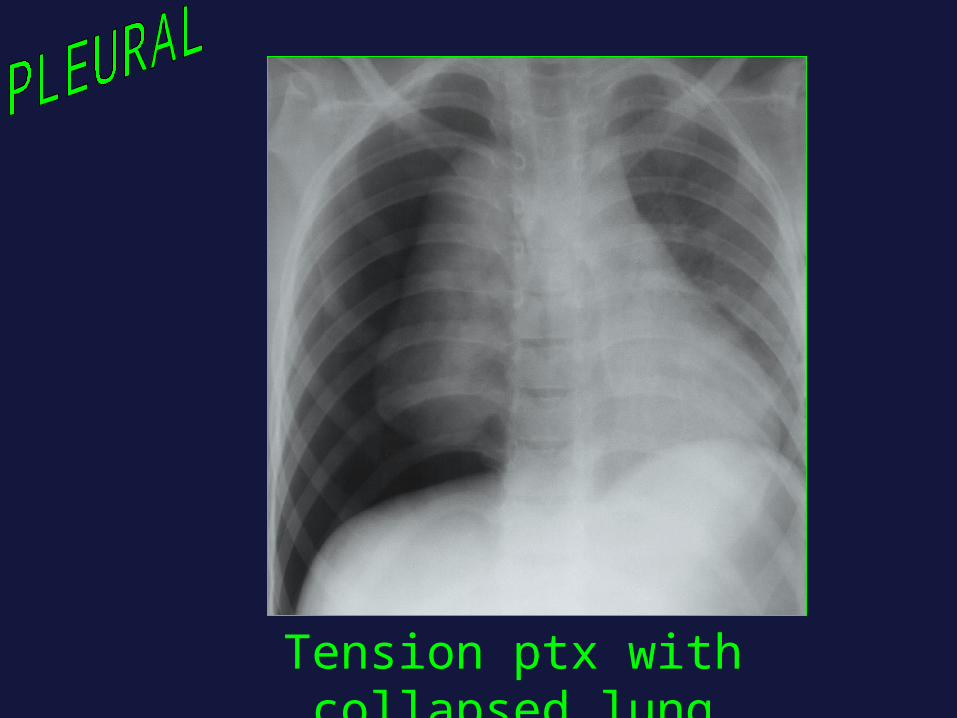
Tension ptx with collapsed lung

SC emphysema caused by multiple rib fractures

aortic dissection – contrast-enhanced CT

Fracture ribs
Flair rib
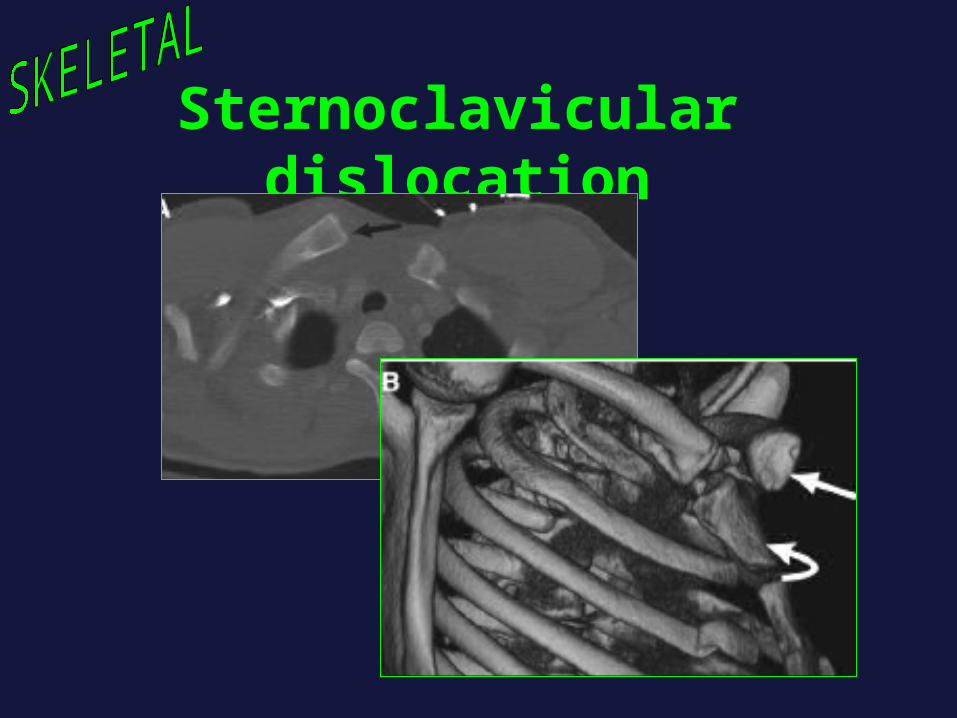
Sternoclavicular dislocation
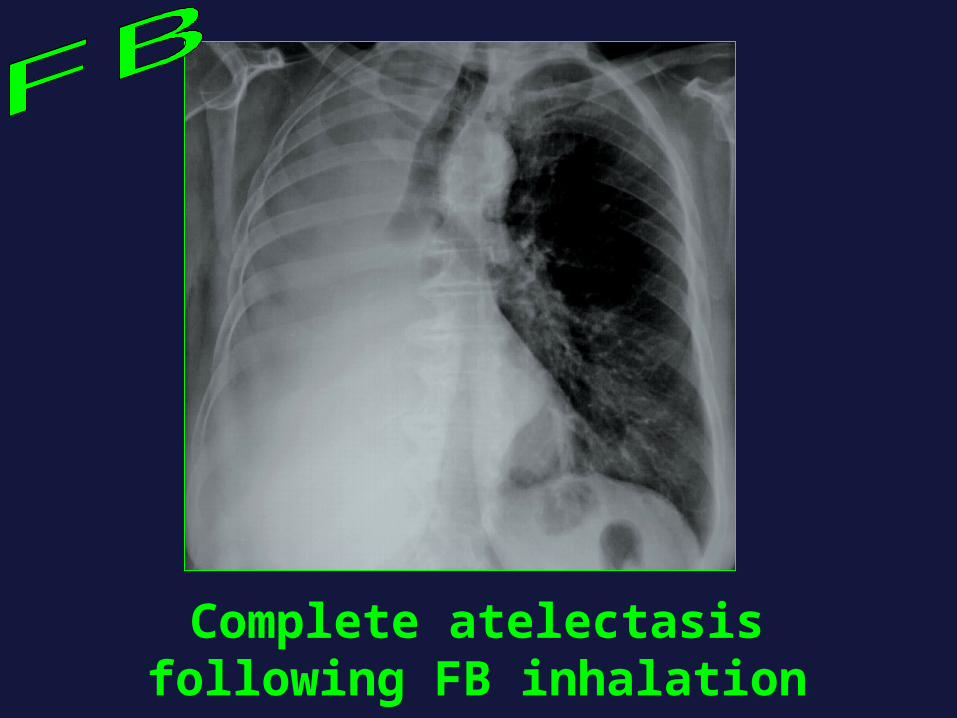
Complete atelectasis following FB inhalation
How to investigate case of chest
Plain X ray.CT (MSCT, CTA).U/S (effusion, echo).Techniques (angio, Ba).Intervention (drainage, biopsy, embo).




Lt. lower lobe pneumonia

Rt. Middle lobe pneumonia


TB

Pulmonary infarct
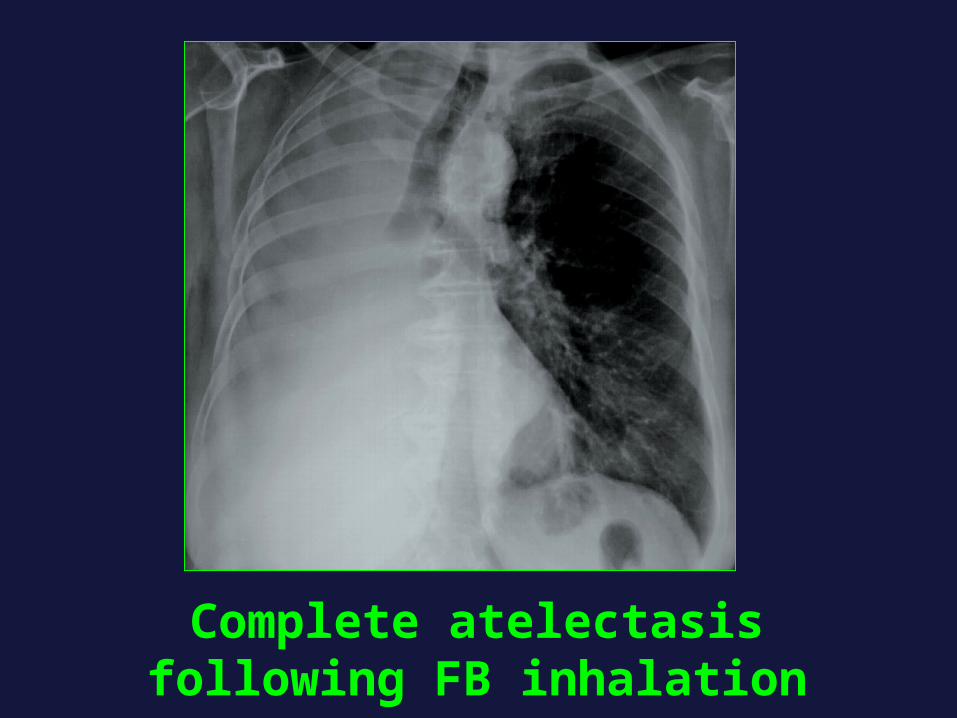
Complete atelectasis following FB inhalation




Radiological signs
Silhouette sign Air bronchogram Noduleopacity / Mass Atelectasis Pneumonia

Silhouette Sign
When two objects of the same When two objects of the same density touch each other, the edge density touch each other, the edge between them disappears between them disappears
A B

Using the Silhouette SignRight middle lobe silhouettes right
heart borderLingula silhouettes left heart borderRight lower lobe silhouettes right
hemidiaphragmLeft lower lobe silhouettes left
hemidiaphragm
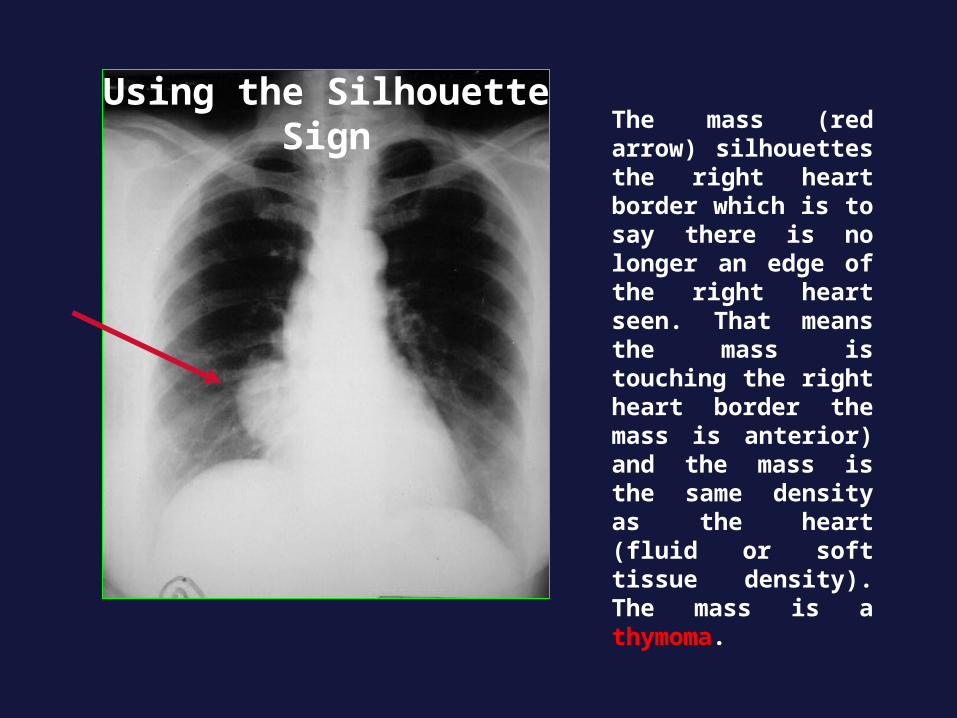
The mass (red arrow) silhouettes the right heart border which is to say there is no longer an edge of the right heart seen. That means the mass is touching the right heart border the mass is anterior) and the mass is the same density as the heart (fluid or soft tissue density). The mass is a thymoma.
Using the Silhouette Sign
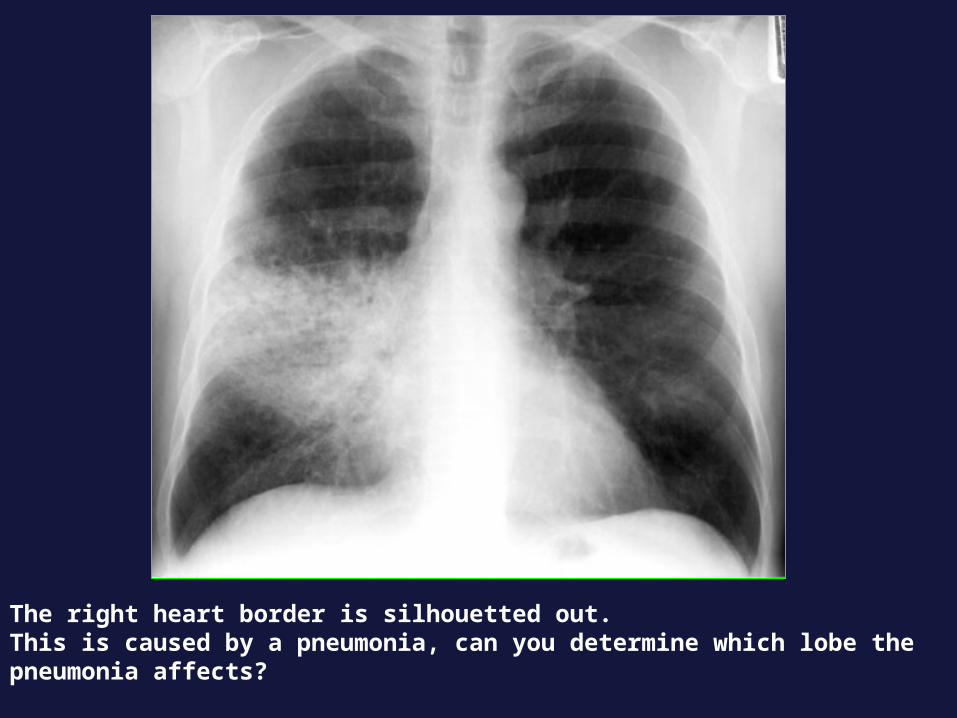
The right heart border is silhouetted out. This is caused by a pneumonia, can you determine which lobe the pneumonia affects?

Air Bronchogram • An air bronchogram is a tubular outline of an
airway made visible by filling of the surrounding alveoli by fluid or inflammatory exudates.
• Causes of air bronchogram: :– lung consolidation– Pulmonary edema– Non obstructive pulmonary atelectasis– Severe interstitial disease– Neoplasm– Normal expiration.

The black branching structures are the result of air in the bronchi, now visible because density other than air surrounds them (in this case it is inflammatory exudate from a pneumonia).

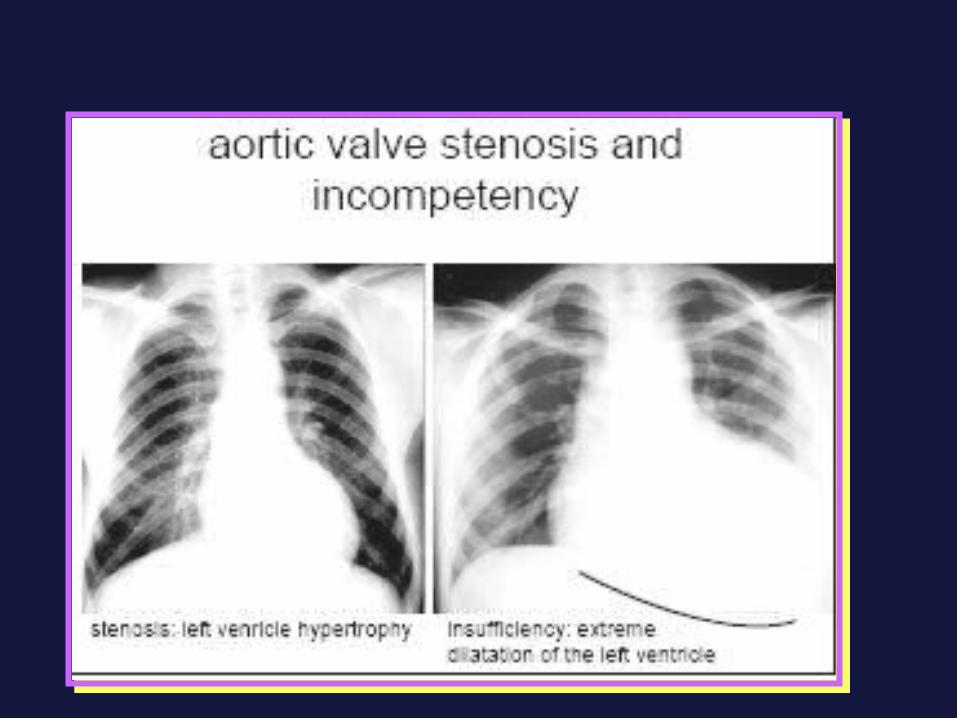
HEART

ANATOMY
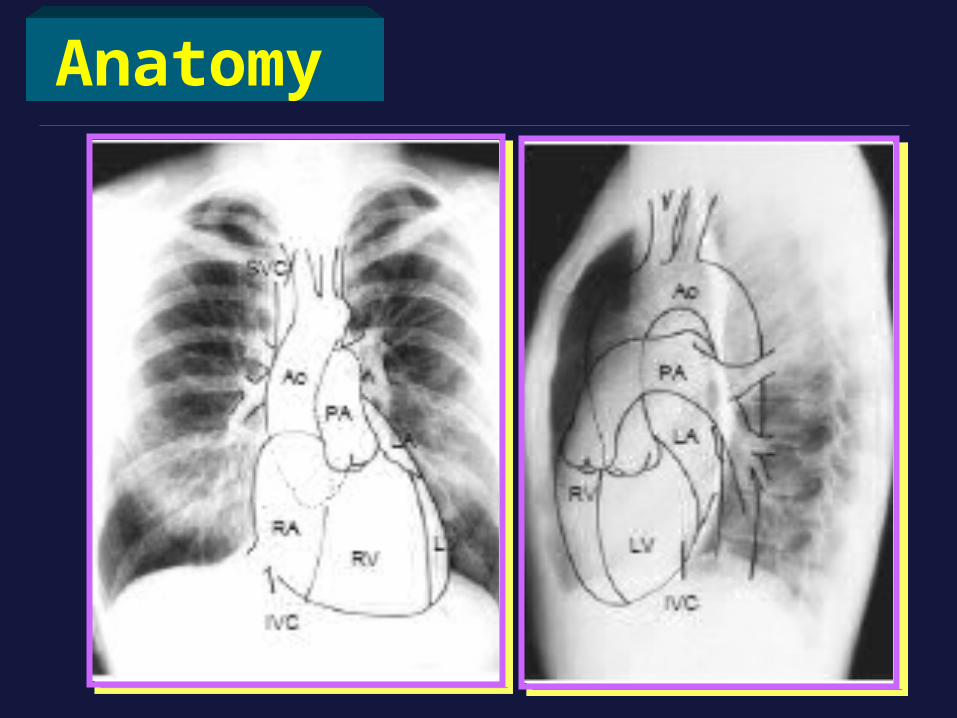
Anatomy

Size
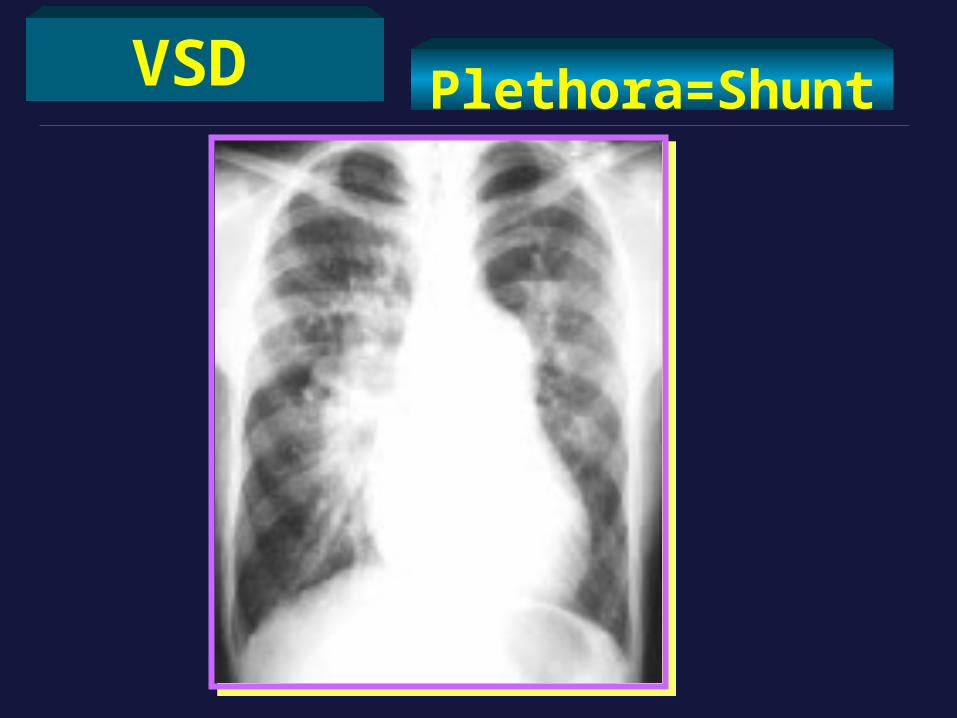
VSD Plethora=Shunt
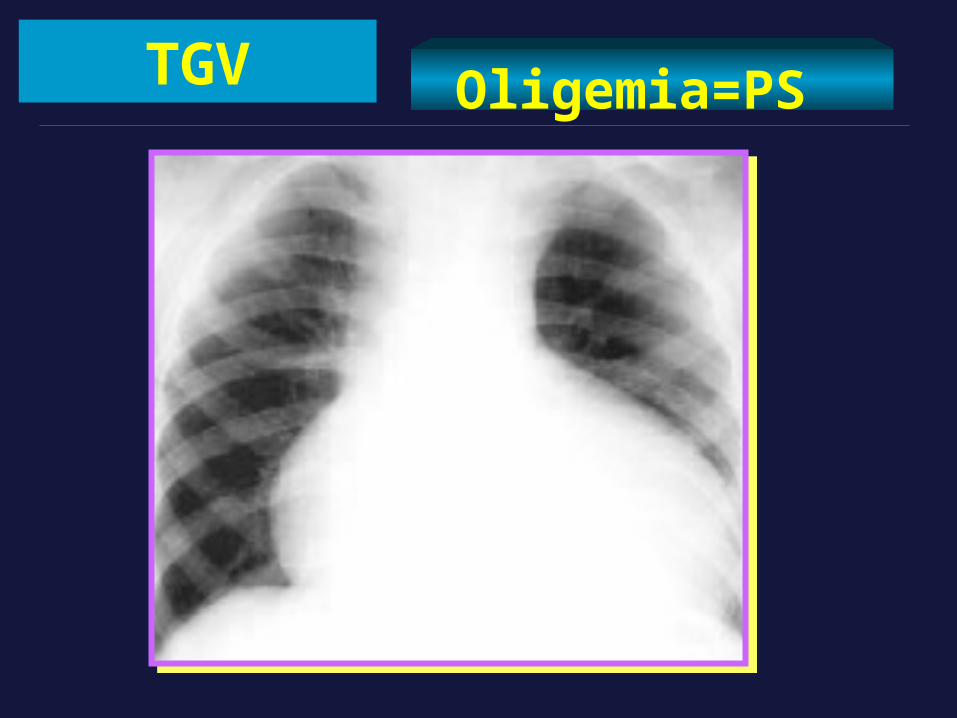
TGV Oligemia=PS