chest pain, weakness, and elevated cardiac enzymes: how ... · though you have ruled out anemia and...
TRANSCRIPT
118 VOL 55, NO 2 / FEBRUARY 2006 THE JOURNAL OF FAMILY PRACTICE
F E A T U R E E D I T O R S
Audrey Paulman, MD, MMM,
and Paul Paulman, MD,
University of Nebraska Collegeof Medicine, Omaha
C O R R E S P O N D E N C E
Edward Onusko, MD, 825 West Locust Street,Wilmington OH [email protected]
Chest pain, weakness, andelevated cardiac enzymes:How would you treat?
Edward Onusko, MD,
and Osawaru Omoruyi,
MDClinton Memorial Hospital /University of Cincinnati FamilyPractice Residency Program
FAMILY MEDICINE GRAND ROUNDS
You are making rounds in the hospital one Saturday morning when you receive acall from the emergency department saying a 68-year-old man is having chest pain,weakness, and “positive cardiac enzymes.” His electrocardiogram (ECG) reading isreported as unremarkable. Because it is the weekend and no cardiology consultation is available at your hospital, the family medicine resident wants to know if you wouldlike to admit the patient to your service or transfer him to a larger hospital. You decidethat you can best make this decision by going to the emergency department and personally evaluating the patient.
History of present illness
• Approximately 4 weeks of generalizedextremity pain and weakness; left-sided, nonexertional chest pain, whichis much less severe than his extremitypains
• Symptoms are most prominent in theproximal upper extremities, especiallywith movement; the right side is moreeffected than the left
• Dyspnea on exertion• Seen twice in local urgent care facilities
in the past 10 days; diagnosed withcongestive heart failure; treated withfurosemide, digoxin, and an unknownantibiotic without relief
• 20- to 30-pound weight loss over thepast year
Other medical history
• No chronic medical problems ormedications
• Until this past month, last seen by aphysician about 3 or 4 years prior
Review of systems
• Up to the day of admission has beenambulatory and able to care for himselfdespite his weakness
• No fever, chills, or rash; but has nightsweats
• Smokes; does not drink alcohol• Retired; lives with his wife
Physical examination
• Alert, appears mildly uncomfortable• Temperature 101ºF, respirations 32,
blood pressure 164/72, pulse 80• 3/5 strength in proximal upper and
lower extremities (can barely lift armsand legs off the bed; movement alsolimited by pain)
• Normal distal strength (hand grips anddorsi/plantar flexion of foot)
• Normal sensation, reflexes, cranialnerves, and mental status; no neckweakness
• No abnormal joint findings; has pinkdiscoloration over extensor surface of
0206FMGrandRounds.FinalREV2 1/25/06 2:51 PM Page 118
MCP joint, which patient dismisses asscars from previous abrasions thathave been present “for a long time”
• Heart, lungs unremarkable; no peri-pheral edema
Laboratory studies completed
in the emergency department
• ECG: normal• Chest x-ray: bibasilar peribronchial
infiltrates• Hemoglobin/hematocrit: normal• White blood count: 27,000 with 92%
neutrophils• Erythrocyte sedimentation rate: normal• Urinalysis: negative for blood• Brain natriuretic peptide: normal• Creatine kinase (CK): 2205 IU/L
(normal range 35–232)• Troponin-I: 0.6 ng/mL.
[Reference range:<0.05 = Negative
0.05–0.09 = Equivocal0.10–0.49 = Suspicious0.50 = Consistent with
myocardial injury]
Chest pain, weakness, and elevated cardiac enzymes ▲
Elevated cardiacenzymes have ahigh specificity for myocardialdamage, but it ismuch lower foracute ischemiccardiac disease
VOL 55, NO 2 / FEBRUARY 2006 119w w w. j f p o n l i n e . c o m
FAST TRACK
Q: What is your presumptive diagnosis? What is your management plan?
A:
� Is this acute non-ST elevation myocardial infarction (NSTEMI)?
The American College of Cardiology andthe American Heart Association definemyocardial infarction primarily as elevatedcardiac-specific enzymes troponin-I and tro-ponin-T in the appropriate clinical setting.1,2
Elevated cardiac troponins have a sensitivi-ty approaching 100% for myocardial dam-age. Specificity is much lower for acuteischemic cardiac disease, however, particu-larly for patients with a low pretest proba-bility (45% false-positive rate in one seriesof 1000 consecutive patients presenting to alarge urban emergency department withsymptoms of acute coronary ischemia).3
Mechanisms other than atheroscleroticcoronary artery disease that can elevatecardiac troponins:
• Increased cardiac demand (eg, sepsis,hypovolemia)
• Nonatherosclerotic ischemia (eg,cocaine or other sympathomimeticagents, coronary vasospasm)
• Direct myocardial injury (eg, cardiaccontusion, myocarditis)
• Myocardial strain (eg, congestive heart
failure, pulmonary embolus)• Chronic renal insufficiency (mechanism
unclear).4
In light of this patient’s history andphysical exam findings, you doubt he’shaving an acute cardiac event. The mostremarkable features are his weakness, muscle pain, and markedly elevated CK.
Though you have ruled out anemiaand several other possibilities, the differen-tial diagnosis of weakness is still broad.You decide to explore the differential diagnosis of elevated CK, a more specificfinding in this case.
Pursuing the differential
You consult UpToDate, searching under“creatine kinase,” and find an article entitled “Muscle enzymes in the evaluationof neuromuscular disease.”5 You concludethat the most likely cause of your patient’sproblems is an idiopathic inflammatorymyopathy: polymyositis, dermatomyositis,or inclusion-body myositis.6
Other possibilities include post-viralmyositis and myositis associated with connective tissue disease, hypothyroidism,or drug reactions.
0206FMGrandRounds.Final 1/23/06 1:28 PM Page 119
D-penicillamine, zidovudine (AZT),and viral or bacterial infection may pro-duce inflammatory myopathy similar topolymyositis.7 A history of exposure tomyotoxic drugs (such as statins) and toxinshas been excluded.
The absence of a family history forneuromuscular disease and the relativelyrecent onset of symptoms rule out aninherited muscular dystrophy or congeni-tal muscle enzyme deficiency.
Myasthenia gravis presents withextraocular muscle involvement. Guillain-Barré syndrome is characterized by ascend-ing muscle weakness. Lyme disease maycause weakness secondary to peripheralneuropathy but it does not produce evidence of muscle inflammation such as
elevation of the CK. West Nile virusencephalitis may present with muscleweakness and flaccid paralysis.8
Trichinellosis may also cause muscleinflammation with weakness and elevationof CK, but it is rare in the United States.
You repeat parts of your physicalexam and confirm that his proximal upperextremity muscles are much weaker thanhis distal muscles.
In practice settings where specialty consultation is not always immediatelyavailable, your diagnostic skills may bechallenged by uncommon presentations ofdisease. In this case, the challenge is “chestpain and positive cardiac enzymes” in apatient who does not appear to have a pri-mary cardiac problem.
Know the extramuscularsigns/symptomscommon withmyopathies
120 VOL 55, NO 2 / FEBRUARY 2006 THE JOURNAL OF FAMILY PRACTICE
FAMILY MEDICINE GRAND ROUNDS
FAST TRACK
Q: What is your management plan at this point?
A:
■ DTaP approachWhen confronted with a difficult clinicalproblem, you may find it useful to organ-ize the management plan according to theacronym “DTaP,” which for this patientwould include:
DDiagnostic plan: serial ECGs and car-diac enzymes: an echocardiogramTTherapeutic plan: pain control; antibi-otics for possible pneumonia; considersteroidsAAssistance from consultants (who areyou going to ask for help?): physiatristconsult for electromyography (EMG);cardiology consult; neurology consultPPatient education (explain to the patient and his family the current diag-nostic possibilities and your manage-ment plan)PProvider education (learn more aboutmyopathies!).
You request specialty consultations:Neurology: possible polymyositis; rec-
ommends rheumatology consultation,multiple labs (most of which are sent outto a reference lab and return only sever-al days later)
Cardiology: ECG normal; cardiologistdoes not see evidence for congestiveheart failure or coronary artery disease
Physical medicine and rehabilitation:EMG performed; findings consistentwith inflammatory myopathy
Rheumatology: recommends proceed-ing with muscle biopsy to differentiatepolymyositis and inclusion-body myositis
Surgery: performs muscle biopsy whichis sent to a regional neuropathologist;reveals inflammatory myopathy withprominent perivascular lymphocyticinflammation strongly suggestive of dermatomyositis.
0206FMGrandRounds.FinalREV 1/24/06 3:06 PM Page 120
� Further case managementand resolution
You administer solumedrol intravenously1 g/d for 3 days, then change to prednisoneorally 1 mg/kg/d.
The patient improves steadily with 3months of oral steroid therapy. He tests
changes can occur. Dermatomyositis maypresent with skin lesions alone (dermato-myositis sine myositis) or rarely withmyopathy alone (dermatomyositis sinedermatitis). In our case, multiple examin-ers failed to detect any classic dermato-logic abnormalities, though the pinkishskin changes over the extensor aspect ofthe MCP joints were, in retrospect, sug-gestive of dermatomyositis. The weak-ness associated with this disease may bemild, moderate, or severe enough toresult in quadriparesis. Dermatomyositisusually occurs alone but may be presentwith scleroderma and mixed connectivetissue disease.
Chest pain, weakness, and elevated cardiac enzymes ▲
VOL 55, NO 2 / FEBRUARY 2006 121w w w. j f p o n l i n e . c o m
Family physician’s commentary
This case illustrates the importance of not letting dramatic laboratory abnormal-ities—for this patient, an elevated CK enzyme level—unduly influence your
investigative focus. The patient’s history and physical exam findings provided alarger context in which the diagnosis of acute coronary insufficiency becameunlikely. Balanced consideration of the patient’s muscle pain and weakness and ele-vated CK level narrowed the diagnostic possibilities appropriately.
positive for anti-Jo antibodies but his pulmonary symptoms resolve. He under-goes an outpatient evaluation for cancerscreening. Colonoscopy, esophogastro-duodenoscopy and chest/abdominal/pelviccomputed tomography scans are negativefor evidence of malignancy.
� Other ways in which you may encounter inflammatory myopathies
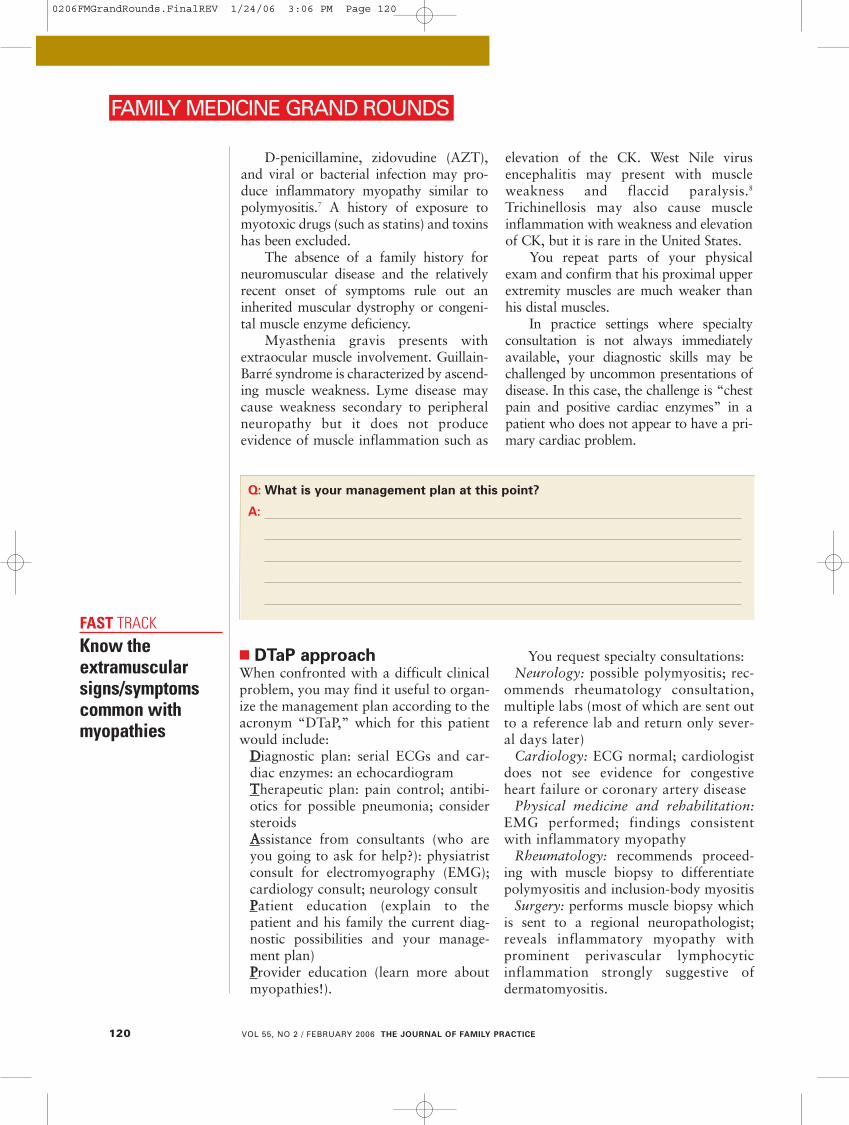
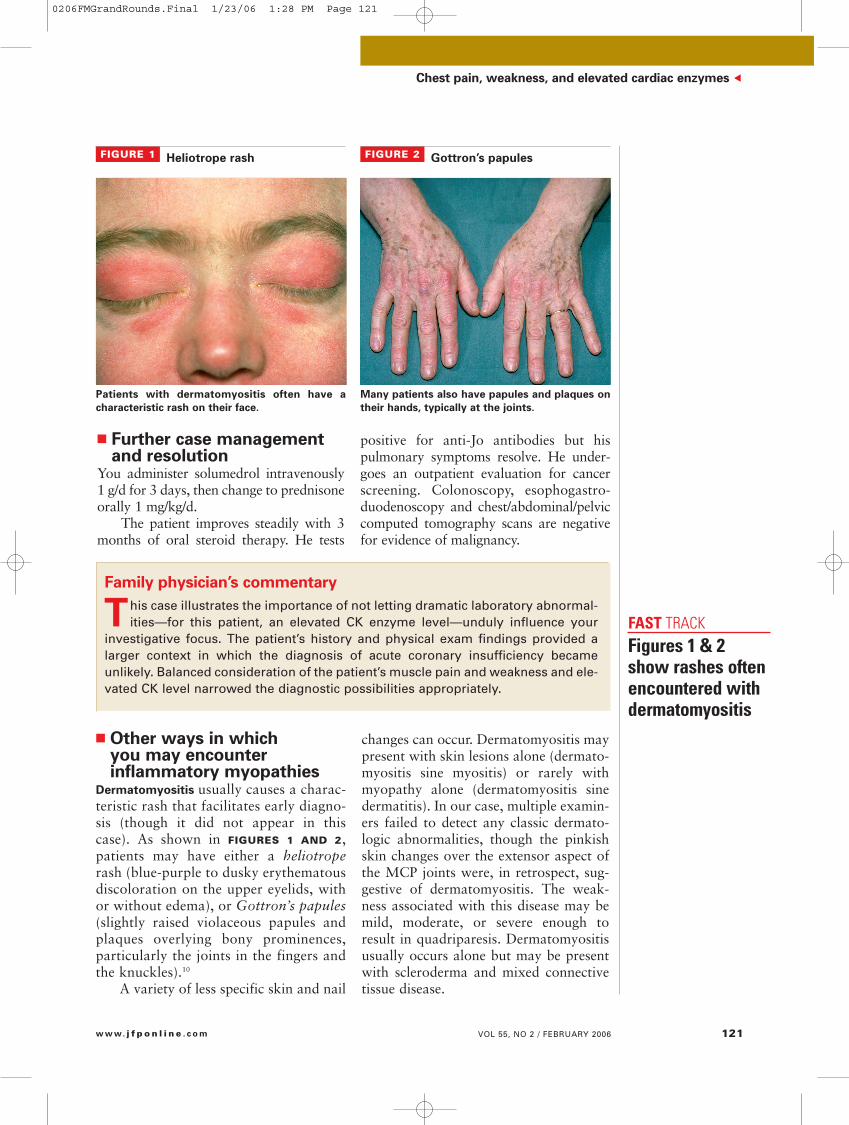
Dermatomyositis usually causes a charac-teristic rash that facilitates early diagno-sis (though it did not appear in thiscase). As shown in FIGURES 1 AND 2,patients may have either a heliotroperash (blue-purple to dusky erythematousdiscoloration on the upper eyelids, withor without edema), or Gottron’s papules(slightly raised violaceous papules andplaques overlying bony prominences,particularly the joints in the fingers andthe knuckles).10
A variety of less specific skin and nail
FIGURE 1 Heliotrope rash
Patients with dermatomyositis often have a
characteristic rash on their face.
FIGURE 2 Gottron’s papules
Many patients also have papules and plaques on
their hands, typically at the joints.
Figures 1 & 2show rashes oftenencountered withdermatomyositis
FAST TRACK
0206FMGrandRounds.Final 1/23/06 1:28 PM Page 121

Inclusion-body myositis is often mis-diagnosed as polymyositis or dermato-myositis until identified by muscle biopsyfindings (see How inflammatorymyopathies develop), although suspicion israised with a poor response to steroid ther-apy.9 Some patients report falling as aresult of quadriceps weakness. On occa-sion the weakness can be asymmetric ordistal (rare with dermatomyositis orpolymyositis). Diagnosis is always madeby muscle biopsy. Disease progression isslow but steady and most patients end uprequiring a walker or assistive device.
Polymyositis is a sub-acute inflamma-tory myopathy affecting adults and,rarely, children. In most cases the actualonset of polymyositis is not easily deter-mined as patients tend to delay seekingmedical evaluation.
Other muscular disorders, as discussedin the case presentation, need to beexcluded.
� Commonly associated clinical findings
Extramuscular manifestations of inflamma-
tory myopathies. Dermatomyositis is a sys-temic inflammatory disorder that mayextend beyond the dermatologic and mus-cular systems, and patients can exhibitsuch symptoms as fever, malaise, and
weight loss.Arthralgia and Raynaud’s phenome-
non may occur with associated connectivetissue disease.
Dysphagia indicates involvement ofthe oropharyngeal striated muscles and theupper esophagus.
Cardiac disturbances include atrioven-tricular conduction defects, tachyarrhyth-mias, myocarditis, heart failure, and possi-bly hypertension from long-term steroiduse. The elevated troponin-I seen in ourindex case may have been evidence of amild myocarditis, though the echocardio-gram was normal.
Calcinosis (deposition of calcium inthe skin or muscles) occurs in up to 40%of children with dermatomyositis but isunusual in adults.10
Pulmonary symptoms may be due toweakness of the thoracic muscles, intersti-tial lung disease, or aspiration. One retro-spective study of 156 consecutive patientswith dermatomyositis/polymyositis basedon clinical criteria found a 23.1% inci-dence of interstitial lung disease.11
Malignant disorders. The frequency ofcancer is increased in association withthese diseases. Studies have placed thehighest risk of concomitant malignancywith dermatomyositis and the least risk with polymyositis. (The relative risk for malignancy in dermatomyositis as compared with polymyositis was 2.4.)Malignancy associated with dermato-myositis or polymyositis is twice as likelyin women than in men.12
Risk of associated malignancy washighest within the first year of diagnosis.Therefore, consider a diagnostic evalua-tion for malignancy at the time myopathyis diagnosed. The optimal diagnostic regi-men in this setting is unknown. In one ret-rospective French study of 40 consecutiveadult patients with inflammatory myopa-thy (33 with dermatomyositis and 7 withpolymyositis) between the years 1981 and2000, malignancy was present at the timeof myopathy diagnosis in 16 patients (13with dermatomyositis and 3 withpolymyositis).12 An Australian population-
Serologic testsare commonlydone but their clinical usefulness is uncertain
122 VOL 55, NO 2 / FEBRUARY 2006 THE JOURNAL OF FAMILY PRACTICE
FAMILY MEDICINE GRAND ROUNDS
FAST TRACK
Inflammatory myopathies: Scope of the problem
The main categories of idiopathic acquired inflammatory
myopathy are polymyositis, dermatomyositis, and inclusion-body myositis. They cause moderate-to-severeweakness and inflammation of muscles.6 The prevalence ofthese disorders is unclear because diagnosis has not consis-tently been based on uniform, reliable criteria. But the incidence is believed to be 1 per 100,000 of the general population, with dermatomyositis being the most commonand polymyositis the least common of these myopathies.9
Inclusion-body myositis is the most common form of inflammatory myopathy in patients older than 50 years.Polymyositis is generally seen after the second decade oflife. Both children and adults may be affected by dermato-myositis. There have been rare familial occurrences.
0206FMGrandRounds.Final 1/23/06 1:28 PM Page 122
based, retrospective cohort study of 537individuals with biopsy-proven idiopathicinflammatory myopathy from 1981–1995demonstrated 116 cases of malignancy in104 patients.13 The risk was highest in der-matomyositis (standardized incidence ratio[SIR] 6.2), next highest in inclusion-bodymyositis (SIR 2.4), and lowest inpolymyositis (SIR 2.0).
� Diagnosis: What helps, what doesn’t
Suspect inflammatory myopathy by theconstellation of clinical findings; confirm itby looking for elevated muscle enzymesand characteristic findings on EMG andmuscle biopsy (see How inflammatorymyopathies develop).
The most sensitive muscle enzyme forinflammatory myopathy is CK, levels ofwhich usually parallel disease activity andmay be used to assess response to thera-py.6,10 Needle EMG demonstrates increasedspontaneous activity with fibrillations;complex repetitive discharges; positivesharp waves; and voluntary motor unitsconsisting of low-amplitude polyphasicunits of short duration.6 EMG findingsalone are not diagnostic.
Serologic tests are commonly donebut their clinical usefulness is controver-sial.10 Antinuclear antibodies are found inabout 80% of cases but are nonspecificand not clinically useful.14 Myositis-specific antibodies (MSAs) have beendescribed in about 30% of idiopathicinflammatory myopathies but are also ofuncertain diagnostic and pathogenicimportance.14 The most prevalent MSA,anti-Jo, is present in only about 20% ofcases and correlates with interstitial lungdisease, but has uncertain usefulness in differentiating between dermatomyosi-tis, polymyositis, and inclusion-body myositis.6,10,11,14,15
Differentiate between the inflamma-tory myopathies based on characteristicpathological findings on muscle biopsy(previously discussed). Muscle biopsy isthe definitive test for establishing the
diagnosis. In our case presentation, theregional neuropathologist thought thebiopsy result was most consistent withdermatomyositis despite the clinicalpaucity of skin abnormalities, thoughour consulting neurologist favored adiagnosis of polymyositis on clinicalgrounds.
� Treatment recommendationsCorticosteroids are the most efficacioustreatment for dermatomyositis (strengthof recommendation [SOR]: BB).10 Oneempirical regimen is to give prednisone 1 mg/kg/d as initial therapy; maintainthis therapy for 1 month after symptomsand CK have normalized; then slowlytaper (SOR: CC).10 Twenty-five percent of
Chest pain, weakness, and elevated cardiac enzymes ▲
VOL 55, NO 2 / FEBRUARY 2006 123w w w. j f p o n l i n e . c o m
How inflammatory myopathies develop
Evidence suggests the inflammatory myopathies areautoimmune disorders.6 They are often associated with
connective tissue diseases and other systemic autoimmuneconditions. Viral infections such as coxsackie, influenza,paramyxovirus, mumps, cytomegalovirus, and Epstein-Barrhave been indirectly associated with chronic and acutemyositis and may trigger the autoimmune process.
Specific muscle or capillary target antigens havenot been identified, and the agents that initiate self-sensiti-zation are still unknown. Other features of these disordersare their association with auto-antibodies, certain histocompatibility genes, T-cell–mediated myocytotoxicity,and complement-mediated microangiopathy.6
Dermatomyositis appears to be primarily a B-cellmediated microangiopathy. Antibodies directed against theendothelium of the endomysial capillaries lead to the primary histological changes in the blood vessels.9 Thedisease manifests when the complement system is activat-ed to form the membrane attack complex (MAC).
Polymyositis and inclusion-body myositis appearto result from a cytotoxic T-cell response directed specifi-cally against muscle fibers.9 CD-8+ cells are induced via T-cell activation to invade MHC-I antigen-expressing musclecells.6 Usually most muscle cells do not express MHC ClassI or II antigens. Histology demonstrates infiltration of indi-vidual muscle fibers by inflammatory cells. Inclusion-bodymyositis is differentiated from polymyositis by the presence of nuclear and cytoplasmic vacuoles.
0206FMGrandRounds.Final 1/23/06 1:28 PM Page 123

patients will not respond to steroids; others will not tolerate the side effects ofsteroid therapy.10
Immunosuppressive drugs such asazothioprine, methotrexate, cyclosporine,mycophenolate mofetil and cyclophos-phamide may be used as second-linetreatment (SOR: CC).6 Intravenousimmunoglobulin may have some efficacy(SOR: BB).16 Plasmapheresis does notappear to be effective (SOR: BB).17
� Determinants of prognosisMost patients will improve over severalweeks or months with therapy, althougha third or more are left with mild tosevere muscle damage. Dermatomyositisresponds better than polymyositis; inclu-sion-body myositis is the most difficult totreat.10 Poor prognostic factors includeolder age, association with cancer, pul-monary fibrosis, dysphagia with aspira-tion pneumonia, cardiac involvement,steroid-resistant disease, and calcinosis indermatomyositis.6,10 Studies have demon-strated 5-year survival rates between77% and 92%.18,19 The main causes ofdeath were related to malignancy andcardiac or pulmonary complications. ■
R E F E R E N C E S
1. Alpert JS, Thygesen K, Antman E, et al. Myocardialinfarction redefined—a consensus document of theJoint European Society of Cardiology/AmericanCollege of Cardiology Committee for the redefinitionof myocardial infarction. J Am Coll Cardiol 2000;36:959–969.
2. Braunwald E, Antman EM, Beasley JW, et al.ACC/AHA 2002 guideline update for the manage-ment of patients with unstable angina and no-ST-segment elevation myocardial infarction—summaryarticle: a report of the American College ofCardiology/American Heart Association task force onpractice guidelines (Committee on the Managementof Patients With Unstable Angina). J Am Coll Cardiol2002; 40:1366–1374.
3. Ng SM, Krishnaswamy P, Morrisey R, et al. Mitigationof the clinical significance of spurious elevations ofcardiac troponin I in settings of coronary ischemiausing serial testing of multiple cardiac markers. Am JCardiol 2001; 87:994–999.
4. Jeremias A, Gibson C. Narrative review: Alternativecauses for elevated cardiac troponin levels when acutecoronary syndromes are excluded. Ann Intern Med2005; 142:786–791.
5. Miller M. Muscle enzymes in the evaluation of neu-
romuscular disease. In UpToDate [database].Available at www.uptodate.com. Accessed onJanuary 10, 2005.
6. Dalakas C, Hohlfeld R. Polymyositis and dermato-myositis. Lancet 2003; 362:971–982.
7. Rowland LP. Polymyositis, inclusion body myositis,and related myopathies. In: Merritt’s Neurology. 10thed. Philadelphia, Pa: Lippincott, Williams & Wilkins;2000:765–769.
8. Peterson LZR, Marfin AA. West Nile virus: a primerfor the clinician. Ann Intern Med 2002; 137:173–179.
9. van der Meulen MFG, Bronner I, et al. Polymyositis:An overdiagnosed entity. Neurology 2003;61:316–321.
10. Callen J. Dermatomyositis. Lancet 2000; 355:53–57.
11. Marie I, Hachulla E, Cherin P, et al. Interstitial lungdisease in polymyositis and dermatomyositis.Arthritis Rheum 2002; 47:614–622.
12. Sparsa A, Liozon E, Herrmann F, et al. Routine vsextensive malignancy search for adult dermato-myositis and polymyositis. Arch Dermatol 2002;138:885–890.
13. Buchbinder R, Forbes A, Hall S, Dennett X, Giles G.Incidence of malignant disease in biopsy-proveninflammatory myopathy. Ann Intern Med 2001;134:1087–1095.
14. Hengstman GJD, Brouwer, Egberts WT, et al. Clinicaland serological characteristics of 125 Dutch myositispatients: Myositis specific antibodies aid in the dif-ferential diagnosis of the idiopathic inflammatorymyopathies. J Neurol 2002; 249:69–75.
15. Schmidt WA, Wetzel W, Friedlander R, et al. Clinicaland serological aspects of patients with anti-Jo-1antibodies—an evolving spectrum of disease mani-festations. Clin Rheumatol 2000; 19:371–377.
16. Dalakis M, Illa I. A controlled trial of high-dose intra-venous immune globulin infusions as treatment fordermatomyositis. N Engl J Med 1993; 329:1993–2000.
17. Miller FW, Leitman SF, Cronin M, et al. Controlledtrial of plasma exchange and leukapheresis inpolymyositis and dermatomyositis. N Engl J Med1992; 326:1380–1384.
18. Marie I, Hachulla E, Hatron PY, et al. Polymyositisand dermatomyositis: Short term and longterm out-come, and predictive factors of prognosis. JRheumatol 2001; 28:2230–2237.
19. Danko K, Ponyi A, Constantin T, Borgulya G, SzegediG. Long-term survival of patients with idiopathicinflammatory myopathies according to clinical fea-tures: A longitudinal study of 162 cases. Medicine(Baltimore) 2004; 83:35–42.
124 VOL 55, NO 2 / FEBRUARY 2006 THE JOURNAL OF FAMILY PRACTICE
FAMILY MEDICINE GRAND ROUNDS
Corticosteroidsare the preferredtreatment for dermatomyositis;immune systemsuppressing drugsmay be useful as a second-linetreatment
FAST TRACK
0206FMGrandRounds.Final 1/23/06 1:28 PM Page 124