chemical sensitivity based on biopsy studies
TRANSCRIPT

Hypothesis for Induction and Propagation ofChemical Sensitivity Based on Biopsy StudiesWilliam J. MeggsDepartment of Emergency Medicine, East Carolina University School ofMedicine, Greenville, North Carolina
The reactive airways dysfunction syndrome (RADS), the reactive upper airways dysfunctionsyndrome (RUDS), the sick building syndrome (SBS), and the multiple chemical sensitivitysyndrome (MCS) are overlapping disorders in which there is an intolerance to environmentalchemicals. The onset of these illnesses is often associated with an initial acute chemicalexposure. To understand the pathophysiology of these conditions, a study of the nasal pathologyof individuals experiencing these syndromes was undertaken. Preliminary data indicate that thenasal pathology of these disorders is characterized by defects in tight junctions between cells,desquamation of the respiratory epithelium, glandular hyperplasia, lymphocytic infiltrates, andperipheral nerve fiber proliferation. These findings suggest a model for a relationship between thechronic inflammation seen in these conditions and an individual's sensitivity to chemicals. Apositive feedback loop is set up: the inflammatory response to low levels of chemical irritants isenhanced due to the observed changes in the epithelium, and the epithelial changes are
propagated by the inflammatory response to the chemicals. This model, combined with theconcept of neurogenic switching, has the potential to explain many aspects of RADS, RUDS,SBS, and MCS in a unified way. - Environ Health Perspect 105(Suppl 2):473-478 (1997)
Key words: rhinitis, asthma, sick building syndrome, multiple chemical sensitivity syndrome,reactive airways dysfunction syndrome, reactive upper airways dysfunction syndrome,neurogenic inflammation, neurogenic switching
IntroductionThat chemical exposures can produceinflammation and that sensory nerves areinvolved in this process have been recog-nized since the early 1900s. In 1910 Brucedemonstrated that the inflammatoryresponse to chemical irritants can be abol-ished by ablation of sensory nerves (1).This response is widely known. The redeyes, nasal congestion, and sinus headachesthat arise from being stuck in the fumes ofrush-hour traffic, sitting in a smoky bar, orpainting with organic solvent-based paintsare examples of inflammation from expo-sures to chemical irritants. This reactivityto chemicals can be altered in some people,and it is recognized that some people havea heightened inflammatory response to
chemical irritants. A role for neurogenicinflammation in chemical sensitivity hasbeen reviewed (2). This altered reactivityto chemicals is best known in rhinitis andasthma, with airway inflammation beingtriggered by chemical irritants. Hence,understanding chemical sensitivity in theairway may hold the key to understandingchemical sensitivity in general and themultiple chemical sensitivity syndrome.My colleagues and I propose to study
the nasal pathology of individuals withallergic and chemical irritant rhinitis,chemical sensitivity, and the multiplechemical sensitivity syndrome. Many of usbelieve, however, that chemical sensitivityis a major public health problem that is
This paper is based on a presentation at the Conference on Experimental Approaches to Chemical Sensitivityheld 20-22 September 1995 in Princeton, New Jersey. Manuscript received at EHP 6 March 1996; manuscriptaccepted 10 October 1996.
The author thanks Drs. Tarik Elsheik, W. James Metzger, Marcus Albernaz, and Richard M. Bloch for theirongoing support and collaboration. This research was supported by the North Carolina Chapter of the AmericanLung Association.
Address correspondence to Dr. W.J. Meggs, Room 4W54, Brody Building, Department of EmergencyMedicine, East Carolina University School of Medicine, Greenville, NC 27858. Telephone: (919) 816-2954.Fax: (919) 816-3589.
Abbreviations used: ETS, environmental tobacco smoke; MCS, multiple chemical sensitivity; RADS, reactiveairways dysfunction syndrome; RUDS, reactive upper airways dysfunction syndrome; SBS, sick buildingsyndrome; VIP, vasoactive intestinal polypeptide.
related to the epidemics of inflammatoryconditions such as asthma and arthritis inindustrialized countries. Understanding theasthma epidemic and understanding themultiple chemical sensitivity syndrome maybe related, and the key to this process isunderstanding how an acute chemical expo-sure can produce ongoing inflammation inthe airway and at other sites.
Reactive airways dysfunction syndrome(RADS) is a chronic asthmalike illness withonset related to an acute chemical exposure(3). Reactive upper airways dysfunctionsyndrome (RUDS) is chronic rhinitis withonset related to an acute chemical exposure(4,5). The distinction between these syn-dromes and the multiple chemical sensitiv-ity syndrome (MCS) is that MCS patientshave symptoms at sites other than the air-way. This paper updates the progress ofour nasal biopsy research program. Basedon biopsy specimens of individuals withchemical sensitivity, a hypothetical modelhas been developed of the process by whichan acute chemical exposure can lead tochronic inflammation. In essence, a singlechemical exposure can induce a chronicdisease. After a few general comments, pre-liminary biopsy findings and this modelwill be presented.
General CommentsChemical sensitivity to inhalants refers toan abnormal sensitivity to a class ofinhalants that is different from allergy toprotein aeroallergens. Examples of this classof inhalants are given in Table 1. A numberof case definitions have been given for
Table 1. Examples of inhalants associated withchemical sensitivity.
Products of combustionCigarette and cigar smokeFurnace fumesGas cook stove and water heater fumesWood smokeGasoline-powered vehicle exhaustDiesel-powered vehicle exhaustKerosene heater exhaust
Perfumes and fragrancesPerfumesDetergents (grocery store soap aisle syndrome)
Products for cleaningPesticidesPetrochemical derivativesSolventsGlues and adhesivesFresh paintFresh printing inkBuilding material outgassing
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 473

W.J. MEGGS
chemical sensitivity syndromes (6), butwhat is constant throughout all descriptionsis the inhalants involved. These inhalantsare often complex mixtures that are ubiqui-tous in the environment of industrializedcountries. Typically, these inhalants containone or more odorous, low molecular weight,volatile organic chemicals. They are toxins,but the doses causing problems in chemi-cally sensitive individuals are lower than thedoses associated with classic toxicity.
In the early descriptions of chemicalsensitivity, disease states associated withinflammation were prominent. Randolphdescribed patients with arthritis, rhinitis,asthma, inflammatory bowel disease, andother inflammatory conditions that became
ARespiratory epithelium
-------- -- Basement membrane
Glands
Sensory nerve fibers
BRespiratory epithelium:tight junction defectsand desquamation
-___---_-__-_-_----- Basement membrane:thickening
" a Glands: hyperplasialymphocytic infiltrates
**/ Sensory nerve fibers:A
proliferation
Figure 1. (A) Schematic of the elements of the normalrespiratory epithelium showing the epithelial cell layerand the basement membrane. Glandular structures andsensory nerves are found in the subepithelial tissue.(B) Schematic of the deviations frorh normal seen inbiopsy specimens of persons developing chemical sen-sitivity associated with rhinitis after a chemical expo-sure (9). There are defects in the tight junctionsbetween respiratory epithelial cells, focal desquama-tion of the epithelial cells in places, hypertrophy ofglandular structures, lymphocytic infiltrates, and prolif-eration of sensory nerve fibers.
asymptomatic when patients were fasted onspring water with control of both inhalantsand ingestants in an environmental controlunit (7). In addition, mental symptomssuch as hallucinations, depression, andmania were described as improving whenthese patients were removed from the chem-ical environment. Elimination routinesincluded both inhalants and ingestants.Symptoms were provoked by reexposure tofoods and chemicals.
It is natural to consider neurogenicinflammation as a possible mechanism ofchemical sensitivity. For many decades ithas been known that sensory neurons areinvolved in an inflammatory process, andthat this neurogenic inflammation is trig-gered by chemicals that stimulate thesesensory neurons. For most people, thesereactions are mild and fleeting and areresolved with the individual's removal tofresh air. For some people, exposures suchas these can trigger debilitating illness withreactions lasting several days.
The work of Bascom and her collabora-tors is significant. A physiological responseto inhalant chemicals was demonstratedin challenge studies with environmentaltobacco smoke (ETS). As Bascom pointedout, this response is consistent with neuro-genic inflammation (8).
My research in this area began whenpatients with chemical sensitivity werereferred to an allergy clinic. These patientscomplained of an intolerance to chemicalsassociated with exposures to solvents or pes-ticides. Physical examination, particularlywhen supplemented with fiberoptic rhino-laryngoscopy, revealed severe inflammationof the upper airway in these patients.Findings included edema, abnormal mucus,cobblestoning (lymphoid hyperplasia), andfriability of the mucosa. One puzzling find-ing that we consistently saw was focal areasof white mucosa with prominent blood ves-sels (4). Initially we thought this mightrepresent atrophy of the mucosa, but biop-sies performed for clinical diagnosis inselected patients revealed no atrophy, andno difference between the white and redareas of the mucosa. To our surprise, therewas chronic inflammation of the mucosawith lymphocytic infiltrates in the biopsyspecimens. A preliminary research studywith controls was undertaken. The picturethat is emerging is depicted schematically inFigure 1. Figure 1A is a schematic of theanatomy of normal respiratory epithelium.
Abnormalities of the nasal mucosa sug-gested by this study were lymphocytic infil-trates, glandular hyperplasia, proliferationof peripheral nerve fibers, gaps in the tight
Figure 2. The nasal mucosa from a subject with chemical sensitivity associated with rhinitis is shown in an elec-tron micrograph. Three epithelial cells are seen on the right with defects in the tight junctions between the cells.To the left, there is desquamation of the epithelial cell layer. The basement membrane appears to be thickened.
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997
..... ..... ..... ...
474
PATHOLOGY OF CHEMICAL SENSITIVITY
junctions between epithelial cells, and focalareas of desquamation of the epithelium (9).These abnormalities are depicted schemati-cally in Figure 1B. An example of an elec-tron micrograph of a patient is shown inFigure 2, with defects in tight junctionsbetween respiratory epithelial cells anddesquamation of epithelial cells visible.Attempts to study the distribution of sub-stance P and vasoactive intestinal poly-peptide (VIP) in these specimens withimmunoperoxidase stains specific for thesesubstances were unsuccessful because cur-rently available reagents stain multiple sitesin tissue specimens in a nonspecific pattern.
In the study by Meggs et al. (9), thepresence of inflammation in patients rela-tive to controls was statistically significant(p<O.05). This study did not have thepower to verify statistically the nerve fiberproliferation that was seen in chemicallysensitive subjects relative to that in controls.
The challenge studies of Bascom et al.and Willes et al. (8,10) and these biopsystudies are complementary and supportedby other evidence that airway inflamma-tion is involved in chemical sensitivity. In acontrolled study of patients with chemicalsensitivity, Doty et al. (11) found signifi-cant increases in airway resistance in thechemically sensitive group. Welch (12)found significant exacerbations of preexist-ing allergic disease and new onset ofasthma in patients with chemical sensitivitydeveloping in association with carpetinstallation. Witorsch et al. (13) found that100% of 61 patients meeting the Cullencriteria for the multiple chemical sensitivitysyndrome had respiratory symptoms.Meggs and Cleveland (4) found that 100%of 10 consecutive patients referred to anallergy clinic with complaints of chemicalsensitivity, all ofwhom met the Cullen cri-teria, had severe inflammation demon-strated by fiber optic rhinoscopy even ifthey denied upper respiratory symptoms.
It is easy to understand how chemicalirritants trigger inflammation in the airway,and in fact the majority of patients withasthma and rhinitis report exacerbationsrelated to these same irritants (14,15). Inasthma, associations have been verified forperfume and tobacco smoke (14,16).Bascom et al. and Willies et al. verify anassociation between ETS and an inflamma-tory response in the upper airway (8,10).
Neurogenic SwitchingHow is it possible that stimulation ofrespiratory receptors by airborne chemicalscan lead to involvement of other organ
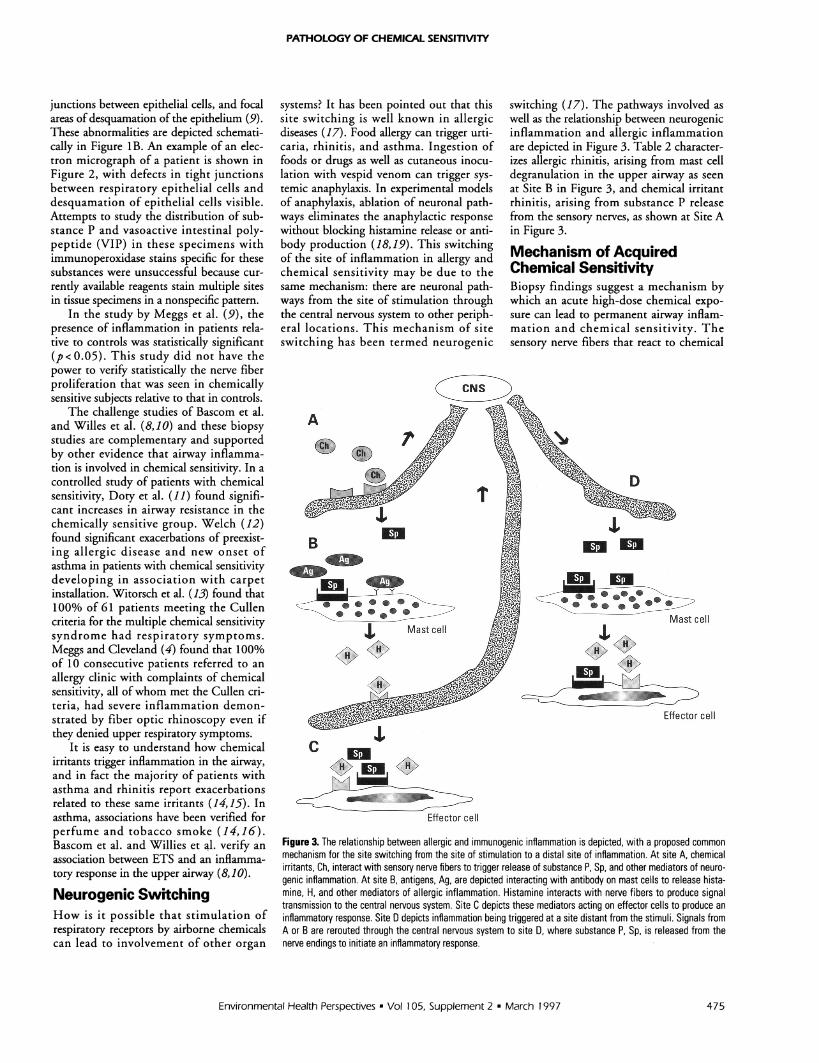
systems? It has been pointed out that thissite switching is well known in allergicdiseases (17). Food allergy can trigger urti-caria, rhinitis, and asthma. Ingestion offoods or drugs as well as cutaneous inocu-lation with vespid venom can trigger sys-temic anaphylaxis. In experimental modelsof anaphylaxis, ablation of neuronal path-ways eliminates the anaphylactic responsewithout blocking histamine release or anti-body production (18,19). This switchingof the site of inflammation in allergy andchemical sensitivity may be due to thesame mechanism: there are neuronal path-ways from the site of stimulation throughthe central nervous system to other periph-eral locations. This mechanism of siteswitching has been termed neurogenic
A
40 Mast coll_ _~
.A_ _lkh
c'A
_ _~~~~MOP
Effector cell
switching (17). The pathways involved aswell as the relationship between neurogenicinflammation and allergic inflammationare depicted in Figure 3. Table 2 character-izes allergic rhinitis, arising from mast celldegranulation in the upper airway as seenat Site B in Figure 3, and chemical irritantrhinitis, arising from substance P releasefrom the sensory nerves, as shown at Site Ain Figure 3.
Mechanism of AcquiredChemical SensitivityBiopsy findings suggest a mechanism bywhich an acute high-dose chemical expo-sure can lead to permanent airway inflam-mation and chemical sensitivity. Thesensory nerve fibers that react to chemical
D
Mast cellI
...A J6%FW.
e_0__ _
_~~~~Efco cel
Figure 3. The relationship between allergic and immunogenic inflammation is depicted, with a proposed commonmechanism for the site switching from the site of stimulation to a distal site of inflammation. At site A, chemicalirritants, Ch, interact with sensory nerve fibers to trigger release of substance P, Sp, and other mediators of neuro-genic inflammation. At site B, antigens, Ag, are depicted interacting with antibody on mast cells to release hista-mine, H, and other mediators of allergic inflammation. Histamine interacts with nerve fibers to produce signaltransmission to the central nervous system. Site C depicts these mediators acting on effector cells to produce aninflammatory response. Site D depicts inflammation being triggered at a site distant from the stimuli. Signals fromA or B are rerouted through the central nervous system to site D, where substance P, Sp, is released from thenerve endings to initiate an inflammatory response.
Environmental Health Perspectives - Vol 105, Supplement 2 * March 1997 475
WJ. MEGGS
Table 2. Characterization of allergic rhinitis and chemical irritant rhinitis.
Allergic rhinitis Chemical irritant rhinitis
Trigger Protein aeroallergens Chemical inhalantsTarget cell Mast cell Sensory nerve cellMediator released Histamine Substance PRecruited cell Eosinophil LymphocyteSensation Itching BurningSymptoms Rhinorrhea Congestion
Sneezing Headache
irritants to produce inflammation arelocated beneath the epithelial cell layer, asseen in Figure 1. This cell layer acts as abarrier between chemicals in the airway andthe nerve cells. It is reasonable to assumethat a high-dose exposure can penetrate thisbarrier to trigger inflammation and can alsodamage this layer so that there is a loss ofthe epithelial layer. When the epithelialbarrier is lost, neurogenic inflammationmay be triggered at much lower doses.Hence, there is ongoing inflammation,which in turn continues the damage to theepithelial barrier. A proliferation of nervefibers would mean that there are morereceptors for chemical irritants and moreinflammatory mediators to be released. Theintegrity of the tight junctions betweenepithelial cells is lost, and tumor necrosisfactor is known to produce similar defectsin tight junction integrity. One form oftumor necrosis factor is produced by lym-phocytes, and lymphocytic infiltrates areseen in this patient population.
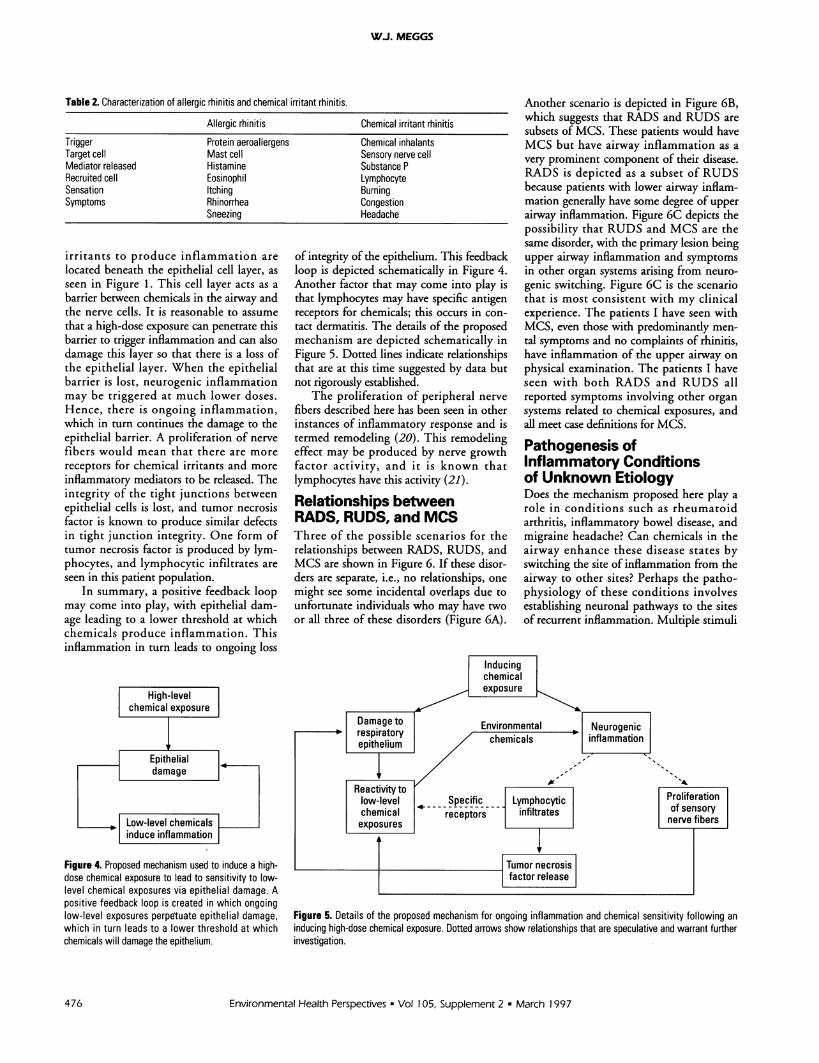
In summary, a positive feedback loopmay come into play, with epithelial dam-age leading to a lower threshold at whichchemicals produce inflammation. Thisinflammation in turn leads to ongoing loss
of integrity of the epithelium. This feedbackloop is depicted schematically in Figure 4.Another factor that may come into play isthat lymphocytes may have specific antigenreceptors for chemicals; this occurs in con-tact dermatitis. The details of the proposedmechanism are depicted schematically inFigure 5. Dotted lines indicate relationshipsthat are at this time suggested by data butnot rigorously established.
The proliferation of peripheral nervefibers described here has been seen in otherinstances of inflammatory response and istermed remodeling (20). This remodelingeffect may be produced by nerve growthfactor activity, and it is known thatlymphocytes have this activity (21).
Relationships betweenRADS, RUDS, and MCSThree of the possible scenarios for therelationships between RADS, RUDS, andMCS are shown in Figure 6. If these disor-ders are separate, i.e., no relationships, onemight see some incidental overlaps due tounfortunate individuals who may have twoor all three of these disorders (Figure 6A).
Another scenario is depicted in Figure 6B,which suggests that RADS and RUDS aresubsets of MCS. These patients would haveMCS but have airway inflammation as avery prominent component of their disease.RADS is depicted as a subset of RUDSbecause patients with lower airway inflam-mation generally have some degree of upperairway inflammation. Figure 6C depicts thepossibility that RUDS and MCS are thesame disorder, with the primary lesion beingupper airway inflammation and symptomsin other organ systems arising from neuro-genic switching. Figure 6C is the scenariothat is most consistent with my clinicalexperience. The patients I have seen withMCS, even those with predominantly men-tal symptoms and no complaints of rhinitis,have inflammation of the upper airway onphysical examination. The patients I haveseen with both RADS and RUDS allreported symptoms involving other organsystems related to chemical exposures, andall meet case definitions for MCS.
Pathogenesis ofInflammatory Conditionsof Unknown EtiologyDoes the mechanism proposed here play arole in conditions such as rheumatoidarthritis, inflammatory bowel disease, andmigraine headache? Can chemicals in theairway enhance these disease states byswitching the site of inflammation from theairway to other sites? Perhaps the patho-physiology of these conditions involvesestablishing neuronal pathways to the sitesof recurrent inflammation. Multiple stimuli
Figure 4. Proposed mechanism used to induce a high-dose chemical exposure to lead to sensitivity to low-level chemical exposures via epithelial damage. Apositive feedback loop is created in which ongoinglow-level exposures perpetuate epithelial damage,which in turn leads to a lower threshold at whichchemicals will damage the epithelium.
Figure 5. Details of the proposed mechanism for ongoing inflammation and chemical sensitivity following aninducing high-dose chemical exposure. Dotted arrows show relationships that are speculative and warrant furtherinvestigation.
Environmental Health Perspectives * Vol 105, Supplement 2 - March 1997476

PATHOLOGY OF CHEMICAL SENSITIVITY
A
CC
B RUDS= MCS
Figure 6. Venn diagrams depicting possible relation-ships between RADS, RUDS, and MCS.
such as chemicals in the airway, infections,allergies, and emotional stress could resultin excitation of these pathways.
Research NeedsMuch work is still to be done on thismodel, as summarized in Table 3. Basicscience needs include the elucidation of thechemoreceptors on the sensory nerves.These receptors are thought to be proteinson the sensory nerve membranes and needto be isolated so they can be sequenced andhave their structures studied. Clinically,there is a specificity to the response tochemicals. Some patients with severechemical sensitivities have been known totolerate substances that are devastating toothers. For example, not all patients withasthma are aversely affected by exposure to
Table 3. Basic science and clinical research needs.
Basic science needsIsolate chemoreceptorsSequence chemoreceptorsStudy structure of chemoreceptorsStudy mechanism of chemical specificity-chemoreceptors vs lymphocytes
Study mechanism of nerve fiber proliferationDetermine role of tumor necrosis factorStudy the neurological pathways of neurogenicswitching
Clinical science needsConduct further biopsy studies in RADS, RUDS,MCS, SBS
Expand control groupsDevelop experimental models of the induction andpropagation of chemical sensitivity
Conduct challenge studiesConduct studies of inflammatory conditions inenvironmental control units
Study treatment of chemical sensitivity
cigarette smoke; however, it can be devas-tating to other patients. Is there a chemore-ceptor specificity, or does the specificity liewith the lymphocytes? Chemical specificreceptors on lymphocytes are known tooccur in contact dermatitis, and a similarsituation may exist in the airway. What isthe mechanism of the peripheral nervefiber proliferation suggested in patients'biopsies? Do lymphocytes or nerves pro-duce a factor that causes this proliferation?What is the mechanism by which gap junc-tion integrity breaks down? Is tumornecrosis factor involved in this process?
Clinical science needs include furtherbiopsy studies in both humans and otherspecies. Larger control groups are needed,
including normal subjects, patients withallergic rhinitis and allergic asthma,patients with asthma and rhinitis related tochemical exposures, and chemically sensi-tive patients without rhinitis. Biopsystudies should be combined with challengestudies to aid in assigning patients togroups. The problem of nonspecific stain-ing of monoclonal antibodies to substanceP, VIP, and neutral endopeptidase shouldbe addressed, and functional assays maybe necessary to establish the role of thesesubstances in chemical sensitivity.
The role of chemical sensitivity ininflammatory conditions of unknown eti-ology such as inflammatory bowel disease,rheumatoid arthritis, and other collagenvascular diseases should be elucidated. Thiswork can only be done in environmentalcontrol units because adapatative phenom-ena and masking are so prominent in thesepopulations under study.
Most importantly, clinical research mustbe done to improve treatment of chemicallysensitive patients. Do anti-inflammatorymedications such as nonsteroidal anti-inflammatory drugs and topical steroidshave roles in the treatment of chemical sen-sitivity patients? Do the substance Pinhibitors now in clinical trial have roles inthe management of chemical sensitivity?Does avoidance of chemical inhalantsreduce reactivity to chemical irritants? Doesthe nasal epithelium heal if the patient isremoved from the chemical environment?Does this healing result in the patienthaving decreased reactivity to chemicals?
REFERENCES
1. Bruce AN. Uber die Beziehung der Sensiblen Nervenendigungenzum Enzundungsvorgang. Arch Exp Pathol Pharmakol 63:424(1910).
2. Meggs WJ. Neurogenic inflammation and sensitivity to envi-ronmental chemicals. Environ Health Perspect 101:234-238(1993).
3. Brooks SM, Weiss MA, Bernstein IL. reactive airways dysfunc-tion syndrome (RADS): persistent asthma syndrome after highlevel irritant exposure. Chest 88:376-384 (1985).
4. Meggs WJ, Cleveland CH Jr. Rhinolaryngoscopic examinationof patients with the multiple chemical sensitivity syndrome.Arch Environ Health 48:14-18 (1992).
5. Meggs WJ. RADS and RUDS: the toxic induction of asthmaand rhinitis. Clin Toxicol 32:367-371 (1994).
6. Miller CS. White paper: chemical sensitivity: history and phe-nomenology. ToxicolInd Health 10:253-276 (1994).
7. Randolph TG, Moss RW. An Alternative Approach toAllergies, Rev ed. New York:Harper and Row, 1989.
8. Bascom R, Kulle T, Kagey-Sobotka A, Proud D. Upper respira-tory tract environmental tobacco smoke sensitivity. Am RevRespir Dis 143:1304-1311 (1991).
9. Meggs WJ, Elsheik T, Metzger WJ, Albernaz M, Bloch RM.Nasal pathology and ultrastructure in patients with chronic air-way inflammation (RADS and RUDS) following an irritantexposure. J Toxicol Clin Tox 34:383-396 (1996).
10. Willes SR, Fitzgerald TK, Bascom R. Nasal inhalation chal-lenge studies with sidestream tobacco smoke. Arch EnvironHealth 47:223-230 (1992).
11. Doty R, Deems DA, Frye RE, Pelberg R, Shapiro A. Olfactorysensitivity, nasal resistance, and autonomic function in patientswith multiple chemical sensitivities. Arch Otolaryngol HeadNeck Surg 114:1422-1427 (1988).
12. Welch LS, Sokas R. Development of multiple chemical sensi-tivity after an outbreak of sick-building syndrome. Toxicol IndHealth 8:47-50 (1992).
13. Witorsch P, Ayesu K, Balter NJ, Schwartz SL. Multiple chemi-cal sensitivity: clinical features and causal analysis in 61 cases(abstract). Clin Toxicol 33:524-525 (1995).
14. Shim C, Williams MH Jr. Effect of odors in asthma. Am JMed 80:18-22 (1986).
15. Meggs WJ. Health effects of indoor air pollution. NC Med J53:354-358 (1992).
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 477

WJ. MEGGS
16. Danuser B, Weber A, Hartmann AL, Krueger H. Effects ofbronchoprovocation challenge test with cigarette sidestreamsmoke on sensitive and healthy adults. Chest 103:353-358(1993).
17. Meggs WJ. Neurogenic switching: a hypothesis for a mecha-nism for switching the site of inflammation in allergy andchemical sensitivity. Environ Health Perspect 103:54-56(1995).
18. Levy RM, Rose JE, Johnson JS. Effect of vagotomy on anaphy-laxis in rat. Clin Exp Immunol 24:96-101 (1976).
19. Leslie CA, Mathe AA. Modification of guinea pig lung anaphy-laxis by central nervous system (CNS) perturbations. J AllergyClin Immunol 83:94-101 (1989).
20. Stead RH, Kosecka-Janiszewska U, Oestreicher AB, Dixon MF,Bienenstock J. Remodeling of B-50 (GAP-43) and NSE-immu-noreactive mucosal nerves in the intestines of rats infected withHippostrongylus brasiliensis. J Neurosci 11:3809-3821 (1991).
21. Gozes Y, Moskowitz MA, Strom TB, Gozes I. Conditionedmedia from activated lymphocytes maintain syjpathetic neu-rons in culture. Brain Res 282:93-97 (1982).
478 Environmental Health Perspectives a Vol 105, Supplement 2 * March 1997