chapter five environmental aspects of human health · chapter five environmental aspects of human...
TRANSCRIPT

81
C H A P T E R F I V E
Environmental Aspectsof Human Health
Environmental factors play a funda-mental role in human health and dis-
ease. From polluted air and water to toxicsubstances in soil and food, environmen-tal pollutants can pose both direct andindirect threats to human health. Theirimpact on health is often complex andmay be influenced by a variety of factors,including exposure patterns, geneticmakeup, nutritional habits, and psycho-logical well-being. Correlations betweenan environmental hazard and an adversehealth effect may not, standing alone,establish that the former is the cause ofthe latter. Nevertheless, reducing expo-sures to environmental hazards, wherecausal links are established or likely, is animportant component in protecting pub-lic health.
Over the past 25 years, federal, state,and local government efforts to ensuresafe supplies of food and water, to managesewage and municipal waste, and toimprove air quality have contributed sub-stantially to human health improvementsin the United States. The past 25 yearsalso have seen an improvement in the dis-semination of information about healthrisks from environmental degradation.Two primary challenges today are to con-tinue making progress in reducing envi-ronmental risks, and to improve the exist-
ing regulatory system in order to achievethe greatest public health protection atthe lowest cost. A further and related chal-lenge is to improve scientific understand-ing about the links between environmentand health, so that policy decisions can bemade with the best information available.
Major new legislation, including theSafe Drinking Water Act Amendments of1996 and the Food Quality Protection Actof 1996, will improve and streamline theregulatory process while keeping healthconcerns paramount. New regulations toprotect air quality have shown that healthstandards can be met without sacrificingeconomic growth and that the health andeconomic benefits of reducing emissionscan be substantial.
The Clinton Administration has beenworking toward greater transparency inhow it evaluates health risks and formu-lates policy. The reevaluation of dioxinand its effects, for example, was a novelapproach in how risk assessments are con-ducted—incorporating both scientificexpertise and broad public input into theprocess. The Administration has also beenactively involved in working toward agreater understanding of the health risksfrom emerging threats such as endocrinedisruptors and global climate change.
This chapter highlights some of theseefforts and provides an overview of envi-ronmental health hazards, particularlythe contamination of drinking water, air,and food. Even so, it only touches on afew environmental risks to humanhealth. Other risks, such as those associat-ed with occupational hazards, accidents,noise, behavioral or lifestyle choices, andinfectious diseases, are also important.
DRINKING WATER QUALITY
Current Trends
EPA and the states are responsible forregulating approximately 200,000 publicwater systems, including 58,000 commu-nity water systems that serve over 240 mil-lion people. The concentration of conta-minants in drinking water supplies fromthese systems is controlled by standardsestablished to minimize risk to humanhealth. Contaminants found in drinking
water can cause myriad health effects,ranging from stomach upset and diarrhea(as with Cryptosporidium or Giardia) tochronic health effects such as liver andkidney damage, neurological disorders,and cancer (i.e., from heavy metals andpesticides). When violations of health-based standards occur, water systems arerequired to take action to remove thecontaminants from the drinking watersupply and notify the public about theviolation.
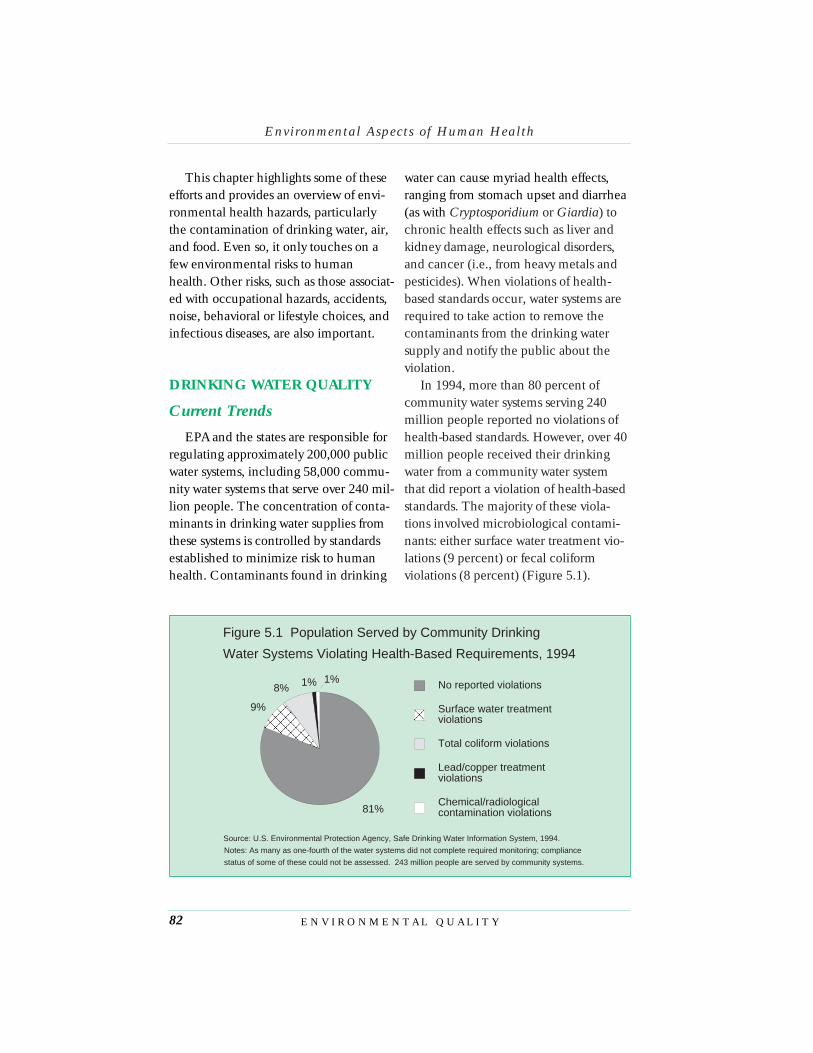
In 1994, more than 80 percent ofcommunity water systems serving 240million people reported no violations ofhealth-based standards. However, over 40million people received their drinkingwater from a community water systemthat did report a violation of health-basedstandards. The majority of these viola-tions involved microbiological contami-nants: either surface water treatment vio-lations (9 percent) or fecal coliformviolations (8 percent) (Figure 5.1).
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y82
81%
9%
8% 1% 1% No reported violations
Surface water treatmentviolations
Total coliform violations
Lead/copper treatmentviolations
Chemical/radiologicalcontamination violations
Figure 5.1 Population Served by Community Drinking
Water Systems Violating Health-Based Requirements, 1994
Source: U.S. Environmental Protection Agency, Safe Drinking Water Information System, 1994.
Notes: As many as one-fourth of the water systems did not complete required monitoring; compliance
status of some of these could not be assessed. 243 million people are served by community systems.

About 69 million people are served bydrinking water systems that have startedto institute mitigation measures (such ascorrosion control treatment) to reducepotential lead contamination at con-sumers’ taps. These systems are requiredto act because initial monitoring,required under EPA’s lead and copperrule, at high risk consumer taps foundlead levels that exceeded the regulatoryaction level for lead (Figure 5.2).Although exposure to lead can comefrom many other sources (e.g., frompaint, from contaminated soil, andthough the air), lead in drinking waterremains a significant risk to the publicand a large problem for water systems.
In addition to improved regulations,technological innovation can reduce the
amount of wastewater generated bydeveloping new water conservation tech-nologies and cleaner industrial technolo-gies. For example, the Department ofEnergy is supporting research to improvethe efficiency of water pipe galvanization.New “hot-dipped” galvanized water pipesemit four orders of magnitude less leadthan the conventional technology, whichleaves lead on the finished product.
Regulatory Background
The Clean Water Act of 1972 estab-lished a body of law and regulationsbacked by federal financial support toensure that the nation’s surface waters aresafe for fishing and swimming and assources of drinking water. In 1974, Con-
Environmental Aspects o f Human Health
C H A P T E R F I V E 83
15-30 31-60 81-130 >1300
10
20
30
40
50po
pula
tion
(mill
ions
)
lead action level exceedance (ppb)
Figure 5.2 Population Served by Drinking Water Systems
Exceeding Lead Action Levels, 1995
Source: U.S. Environmental Protection Agency, Safe Drinking Water Information System, 1995.
Note: Data are the results ot lead testing in high-risk households. A water system is found to exceed
the action level if more than 10 percent of its high-risk households contain lead levels above 15 ppb.

gress enacted the Safe Drinking WaterAct, further developing a legislative basisto protect water quality. The Safe Drink-ing Water Act is intended to ensure thatevery public water system consistentlyprovides water that is safe to drink. Theact, which was substantially amended in1986, required EPA to establish nationaldrinking water safety standards that incor-porate enforceable maximum contami-nant levels or treatment techniques,underground injection control regula-tions to protect underground sources ofdrinking water, and grant programs forthe administration of state wellhead pro-tection area programs. The states were tobe delegated responsibility to ensure thatsafety standards were met.
Despite the progress made in improv-ing drinking water quality in the UnitedStates, both natural processes and humanactivities continue to exert pressures ondrinking water quality. For instance, pop-ulation growth, newly identified andemerging microorganisms, changes inchemical usage, and outdated and deteri-orating water systems present significantchallenges to the long-term safety of thenation’s drinking water supplies. Thesetrends are further exacerbated by shrink-ing budgets and resources at all levels ofgovernment. In 1995, EPA’s ScienceAdvisory Board (SAB) released a report,Safe Drinking Water: Future Trends andChallenges, which identified significanttrends affecting the nation’s drinkingwater, including population growthimpacts, public demand for better water,a changing contaminant profile, andchanges in drinking water productionand treatment. The report recommended
improved management of waterresources, consolidation of smaller sys-tems, accelerated research in risk assess-ment methodologies, and establishmentof an alert system for emergingpathogens.
Also in 1995, EPA Administrator CarolBrowner launched a reassessment ofEPA’s drinking water program andreleased EPA’s “white paper,” Strengthen-ing the Safety of Our Drinking Water: AReport on Progress and Challenges andan Agenda for Action. The white paperprovided an overview of drinking watersafety in the United States and identifiedfive agenda items for improving drinkingwater protection:
• provide Americans with more infor-mation about the nation’s drinkingwater;
• focus standards on the most serioushealth risks;
• provide technical assistance to pro-tect source water and help small sys-tems;
• reinvent federal/state partnershipsto improve drinking water safety; and
• invest in community drinking waterfacilities to protect human health.
The white paper estimated that sub-stantial health benefits could be achievedif existing standards were fully attained,including reduced exposure to lead foran estimated 50 million people (with pro-tection for 200,000 children againstunacceptable blood lead levels); preven-tion of more than 100,000 cases annuallyof gastrointestinal and other illnessesattributed to microorganisms; reduced
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y84

exposure for millions of people to dozensof contaminants that may cause illness,including compromised reproductivecapabilities, malfunction of vital organs,“blue baby” syndrome, and nervous sys-tem damage; and over 100 excess cancercases avoided per year.
The Safe Drinking Water ActAmendments of 1996
On August 6, President Clintonsigned the Safe Drinking Water Act(SDWA) amendments of 1996. The newlaw will help achieve many of the goalsoutlined in both the SAB and the EPAreports. It will: (1) establish a strong newemphasis on preventing contaminationproblems through source water protec-tion and enhanced water system manage-ment; (2) move greater responsibility tothe states and expand their role in creat-ing and focusing prevention programsand helping water systems improve oper-ations and avoid contamination prob-lems; and (3) set up a state revolvingfund (SRF) system to provide money tocommunities to improve their drinkingwater facilities.
The SRF is authorized at $1 billionfor each of fiscal years 1995 to 2003. Thestates may use set-asides from the SRF topay for programs such as source waterassessments; voluntary source water qual-ity protection partnerships with publicwater systems, local governments, andprivate companies; and capacity develop-ment and implementation efforts. Statesalso will have more flexibility in estab-lishing water quality monitoring require-ments.
The 1996 amendments recognize theimportance of community right-to-knowabout potential threats to drinking waterquality. Within 2 years of enactment, thelaw requires EPA to issue regulationsrequiring all community water systems toprepare at least annually a report withinformation about the system’s sourcewater and the level of contaminants inthe drinking water supply. In addition,public water systems must give notice ofany violation of a national drinking waterstandard “that has the potential to haveserious adverse effects on human healthas a result of short-term exposure” within24 hours after the violation.
The new law repeals the currentrequirement that EPA promulgate stan-dards for 25 additional contaminantsevery 3 years. These requirements, insti-tuted by Congress as part of the 1986SDWA amendments, have divertedresources from science-based priorities,and have been impossible to meet withinthe mandated time frames. Efforts tomeet all of the statute’s remaining stan-dard-setting requirements had detractedfrom the development of soundly ana-lyzed, well-supported standards for thehighest-risk drinking water contaminants,such as microbes. Under the 1996amendments, the agency’s decisionsabout new standards are informed by acost-benefit analysis.
Other provisions of the 1996 amend-ments include the establishment of a pri-ority list of unregulated contaminants andrequire that EPA promulgate rules onarsenic, enhanced surface water treatmentincorporating standards for Cryptosporidi-um, and a new multimedia approach to
Environmental Aspects o f Human Health
C H A P T E R F I V E 85

reducing risks from radon. EPA is alsodirected to conduct research on sensitivesubpopulations that may experiencegreater adverse health effects from drink-ing water contaminants than the generalpopulation (see also Chapter 6, “Environ-mental Justice”).
Other Programs
In addition to the 1996 SDWAamendments, many other programs areunder way to address drinking water qual-ity. In 1993, the Surface Water TreatmentRule (SWTR) went into effect. TheSWTR requires water systems using sur-face water sources to install filters formicrobiological contaminants that causedisease, such as Giardia lamblia,Legionella, and viruses. Compliance withthe rule will dramatically reduce theprobability of human exposure to harm-ful levels of microbiological contami-nants from surface water sources.
To protect sources of drinking watereven before water is withdrawn by adrinking water supplier, EPA has estab-lished the Source Water Protection andWellhead Protection Programs under theSDWA. The Source Water ProtectionProgram emphasizes preventing contami-nation of drinking water resources andincludes wellhead protection and “solesource aquifer” designations. The Well-head Protection Program protects sup-plies of groundwater that will providedrinking water in the future from conta-mination by chemicals and other haz-ards, including pesticides, nutrients, andother agricultural chemicals. The pro-gram is based on the concept that local
or state governments that adopt land useplans and other preventive measures canprotect groundwater. Currently, 39 stateshave an EPA-approved wellhead protec-tion program.
The Comprehensive State GroundWater Protection Program (CSGWPP),established by EPA in 1991, coordinatesall federal, state, and tribal and local pro-grams that address groundwater quality.States have the primary role in designingand implementing CSGWPPs in accor-dance with local needs and conditions.EPA has approved programs in 6 states,and plans from an additional 13 states areunder review.
The Administration is also working todevelop a comprehensive approach towater resource management to addressthe myriad water quality problems thatexist today from nonpoint and pointsources as well as from habitat degrada-tion. The Watershed ProtectionApproach is a management approach formore effectively protecting and restoringaquatic ecosystems and protectinghuman health. The watershed protectionapproach recognizes that water qualitymanagement must embrace human andecosystem health and that managing forone without considering the other can bedetrimental to both. It has four major fea-tures: targeting priority problems, stake-holder involvement, integrated solutions,and measuring success. The watershedprotection approach is not a new pro-gram that competes with or replacesexisting water quality programs; rather, itis a framework within which ongoingprograms can be integrated effectively.
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y86

AIR QUALITY
Ambient Air Quality
Over the past three or four decades,there have been important advances inthe understanding of how air pollutantsaffect human health. Air pollutants maycause lung cell damage, inflammation,acute changes in lung function and respi-ratory symptoms, as well as more long-term lung cell changes. Acute and chron-ic exposure to air pollutants is alsoassociated with increased mortality andmorbidity. Yet much remains to beunderstood, including, for instance, therole of air pollution in observed increasesin asthma cases and deaths from lung dis-ease. Table 5.1 summarizes the majorhealth effects of the six pollutants moni-tored by EPA.
In 1963, the United States took thefirst step toward healthier air by passingthe Clean Air Act. Amended in 1970 andagain in 1990, the Clean Air Act requiresEPA to set National Ambient Air QualityStandards (NAAQS) for pollutants con-sidered harmful to public health and theenvironment and to ensure that these airquality standards are met through strate-gies to control air emissions from sourcessuch as automobiles, power plants, andfactories. As a result of these measures, airquality in the United States improved sig-nificantly (see Chapter 10, “Air Quality”).
Despite these improvements, in 1994approximately 62 million people stilllived in counties where air quality levelsexceeded the national air quality stan-dards for at least one of the six principalpollutants. Ozone is the most commonlyviolated NAAQS, affecting 50 million
people in 1994. According to the currentozone standards established by EPA,ozone levels exceeding 0.12 parts per mil-lion can be detrimental to public health.During the high smog season extendingfrom June to early September, those lev-els are regularly exceeded in major citiesacross the United States, including NewYork and Los Angeles. Scientific evi-dence indicates that ozone affects notonly people with impaired respiratory sys-tems, such as asthmatics, but also healthyadults and children. Even exposures torelatively low concentrations of ozonehave been found to temporarily reducelung function and induce respiratoryinflammation in normal, healthy people,especially during exercise. EPA is cur-rently reviewing the NAAQS and hasagreed to complete its review and issuerevised standards by June 28, 1997. EPAmay propose more stringent ambient airquality standards for ozone if the datasupport those changes.
In addition, more than 13 million peo-ple live in counties where the currentEPA standard for particulate levels isexceeded. On the basis of studies ofhuman populations exposed to high con-centrations of particulates and laboratorystudies of animals and humans, it hasbeen determined that particulates posemajor concerns for human health. Theseinclude effects on breathing and respira-tory symptoms, aggravation of existingrespiratory and cardiovascular disease,alterations in the body’s defense systemsagainst foreign materials, damage to lungtissue, carcinogenesis, and prematuredeath. Two recent epidemiological stud-ies (Douglas Dockery, et.al., and C.
Environmental Aspects o f Human Health
C H A P T E R F I V E 87

Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y88
Table 5.1Air Pollutants and their Impacts on Health
Carbon MonoxideSources: Carbon monoxide is a colorless, odorless, poisonous gas formed when carbon in fuels isnot burned completely. It is a byproduct of motor vehicle exhaust, which contributes more than two-thirds of all CO emissions nationwide.
NAAQS: 9 ppm (measured over 8 hours)
Health Effects: Carbon monoxide enters the bloodstream and reduces oxygen delivery to the body’sorgans and tissues. Exposure to elevated CO levels is associated with visual impairment, reducedwork capacity, reduced manual dexterity, poor learning ability, and difficulty in performing complextasks.
LeadSources: Smelters and battery plants are the major sources of lead in air. Indoors, lead can be foundin old buildings from paint on walls.
NAAQS: 1.5 ug/m3 (measured as a quarterly average)
Health Effects: Lead accumulates in the body in blood, bone and soft tissue. Because it is not readilyexcreted, lead can also affect the kidneys, liver, nervous system, and other organs. Excessive expo-sure to lead may cause anemia, kidney disease, reproductive disorders, and neurological impair-ments such as seizures, mental retardation, and/or behavorial disorders.
Nitrogen DioxideSources: Nitrogen oxides form when fuel is burned at high temperatures, and come principally frommotor vehicle exhaust and stationary sources such as electric utilities and industrial boilers.
NAAQS: 0.053 ppm (measured as an annual average)
Health Effects: Nitrogen dioxide can irritate the lungs and lower resistence to respiratory infectionssuch as influenza. The effect of short-term exposure are still unclear, but continued or frequent expo-sure to concentrations that are typically much higher than those normally found in the ambient airmay cause increased incidence of acute respiratory illness in children.
OzoneSources: Unlike other pollutants, ozone is not emitted directly into the air but is created by sunlightacting on NOx and VOC emissions in the air. There are literally thousands of sources of these gases,from gasoline vapors to chemical solvents.
NAAQS: 0.12 ppm (measured at the highest hour during the day)
Health Effects: Exposure to ozone significantly reduces lung function and induces respiratory inflam-mation in normal, healthly people during periods of moderate exercise. It can be accompanied bysymptoms such as chest pain, coughing, nausea, and pulmonary congestion.
Sulfur Dioxide (SO2)Sources: Formed when fuel containing sulfur (mainly coal and oil) is burned, and during metal smelt-ing and other industrial processes.
NAAQS: 0.03 ppm (annual average) .14 ppm (over 24 hours)
Health Effects: SO2 can affect breathing, respiratory illness, alterations in pulmonary defenses, andaggravation of existing cardiovascular disease.
Particulate Matter (PM-10) (PM-10 refers to particles with a diameter of 10 micrometers or less)
Sources: Particulate matter is the term for solid or lliquid particles found in the air. Particles originatefrom a variety of mobile, stationary, and natural sources (diesel trucks, wood stoves, power plants,dust, etc.), and their chemical and physical compositions vary widely.
NAAQS: 50 ug/m3 (annual average) 150 ug/m3 (daily average)
Health Effects: Major concerns for human health from exposures to PM-10 are: effects on breathingand respiratory systems, damage to lung tissue, cancer, and premature death. The elderly, children,and people with chronic lung disease, influenza, or asthma tend to be especially sensitive to particu-late matter.
Source: U.S. Environmental Protection Agency (EPA), Air Quality Trends (EPA, Office of Air Quality, Planning & Stan-dards, Research Triangle Park, N.C., September 1995)

Arden Pope III, et. al.) have linked partic-ulate pollution to excess morbidity andmortality in U.S. cities, providing strikingevidence of the impact of energy-relatedtransportation and industrial emissionsupon human health and longevity.
As with ozone, EPA is considering therevision of its particulate standards.Ambient air standards for total suspendedparticulate matter were first set in 1971.Since 1987, however, EPA has used theindicator PM-10, which includes onlythose particles with aerodynamic diame-ter of 10 micrometers or less. Thesesmaller particles are likely responsible formost of the adverse health effects of par-ticulate matter because of their ability toreach the thoracic or lower regions of therespiratory tract. Further investigations byEPA may develop standards down to thePM-2.5 scale.
Most of the smaller particles under 2.5microns in diameter are from fossil-fuelbased energy-related emissions such asthose from power plants, vehicles (espe-cially diesel), and industry. Fortunately,initiatives intended to address other ener-gy-related air pollution problems, such asozone, acid rain, air toxics, and global cli-mate change, can also yield substantialreductions in fine particle pollutionwhile increasing energy efficiency anddecreasing costs.
In addition to evaluating standards,the Administration has been working withfederal agencies, the states, and industryto develop innovative and cost-effectiveprograms to reduce emissions under theClean Air Act. Market-based programssuch as emissions trading provide incen-tives for industry to develop new pollu-
tion control technologies or pollutionprevention approaches. In May 1996,EPA completed a draft study on benefitsand costs of the Clean Air Act during the1970–90 period. The analysis, whichmust still undergo review and possiblerevision by the EPA Science AdvisoryBoard, found that spending for Clean AirAct programs had yielded benefits that faroutweigh the costs due to the impact oflead and particulate matter controls (seeChapter 1, “America and the Environ-ment: A 25-Year Retrospective” andChapter 10, “Air Quality”).
There have also been government-wide efforts to find innovative solutions toair pollution problems. For example, theDepartment of Energy (DOE) has mademuch progress both in research and indeployment of technologies to mitigatethe urban heat islands that can negativelyaffect air quality. DOE is working to helpdevelop and identify the best roofing andpaving materials, to use computer modelsto determine the optimal approach tocooling a city, and to disseminate infor-mation around the nation. DOE esti-mates that over a 20-year period, trees canbe planted cheaply and roads, roofs, andparking lots replaced with cooler surfaces,with considerable savings in energy andenvironmental costs.
In many cities and regions, localefforts to reduce air pollution are alsobearing fruit. In Los Angeles, the combi-nation of cars, industries, weather, andnatural topography contributes to theworst air pollution problems in the Unit-ed States. To meet federal health stan-dards by 2010, a regional air pollutioncontrol board has devised an elaborate
Environmental Aspects o f Human Health
C H A P T E R F I V E 89

local air quality management plan thattargets industry, transportation, and con-sumers and relies on both current tech-nologies and some that are just nowbeing developed. The estimated healthbenefits would be substantial. In Chat-tanooga, Tennessee, a collaborative effortamong the city’s political, business, andenvironmental leaders managed to endthe severe air pollution problems thatplagued the city only two decades ago.When confronted with federal standardsin the Clean Air Act requiring localindustries to install air pollution equip-ment, the city translated these require-ments into economic growth, generatingnearly $40 million in locally manufac-tured air pollution control equipment.
Hazardous Air Pollutants
In addition to the six criteria pollu-tants monitored under NAAQS, EPA alsomonitors hazardous air pollutants such asbenzene, chlorine, and heavy metals,from stationary and urban area sources.Hazardous air pollutants are believed topose a significant threat to human health.Estimates by EPA suggest that as many as2,500 cancer cases per year may resultfrom outdoor exposure to 45 of the 189hazardous air pollutants listed under theClean Air Act Amendments of 1990.However, the scientific basis for estimat-ing risks from outdoor exposure to haz-ardous air pollutants is currently frag-mented and sparse (Figure 5.3). EPA is
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y90
Inadequate Suggestive Fair or better0
20
40
60
80
100
120
140
160
num
ber
of p
ollu
tant
s
Emissions data
Ambient concentrations
Noncancer data
Cancer data
Figure 5.3 Adequacy of Available U.S. Data on 189 Hazardous
Air Pollutants
Source: K. Sexton, "Science and Policy in Regulatory Decision Making: Getting the Facts Right about Haz-
ardous Air Pollutants," Environmental Health Perspectives, Vol. 103, Supplement 6 (1995), pp. 213-222.

in the process of using its research capa-bilities and testing authorities to respondto this gap in scientific knowledge. InJune 1996, EPA proposed a test ruleunder the Toxic Substances Control Actto acquire needed inhalation toxicity dataon 21 hazardous air pollutants.
The Administration has also taken asteady and aggressive stance on increas-ing the amount of information availableto the public about toxics in their com-munities, their homes and their work-places. The Federal Right-to-Know Pro-gram, for example, assures thatcommunities have easy access to criticalenvironmental information about thereleases of toxic chemicals within theircommunities. In 1995, the number ofchemicals covered by the Right-to-KnowProgram of Toxics Release Inventoryincreased from 300 to over 600. In 1996,EPA proposed to require the miningindustry, utilities, hazardous waste han-dlers and other industrial sectors to alsodisclose basic toxic emissions data.Reporting from these industries wouldbegin in 1997.
In addition, the 1990 Clean Air Actamendments introduced important inno-vations for controlling air toxics. Prior topassage of the 1990 amendments, EPAhad regulated directly only seven of thehundreds of toxic air pollutants emittedfrom industries. Under the 1990 amend-ments, EPA must identify categories of“major” sources that emit any of the 189hazardous air pollutants listed specificallyunder the act. This modification willallow EPA to better protect humanhealth from hazardous air pollutants.These major sources of toxic air pollu-
tants also will provide a roadmap forDOE pollution prevention efforts, whichare targeted at the responsible industrialsectors.
Indoor Air Quality
Modern indoor environments containan array of chemical and biologicalsources of air pollution, including syn-thetic building materials, consumer prod-ucts, and dust. Common indoor pollu-tants include lead, radon, tobacco smoke,volatile organic compounds, combustiongases, particles, and mold. This sectionhighlights three indoor air problems:lead, radon, and environmental tobaccosmoke.
Lead. In the United States, children’smean blood lead levels have decreasedmore than 75 percent since the 1970s.This reduction is primarily the result ofthe phaseout of lead in gasoline andreductions in other sources and pathwaysof exposure, such as lead in soldered cansand paint (see Chapter 6, “Environmen-tal Justice”). With the reduction of leadin gasoline and foods, the remainingmajor sources of lead are lead-basedpaint, dust and soil, drinking water, andoccupational exposures.
While lead is not solely an “indoorair” issue, lead-based paint is currentlythe largest source of high-dose lead expo-sure for children. Approximately 1.7 mil-lion children still have blood lead levelsabove 10 micrograms per deciliter, theaccepted level set by the Centers for Dis-ease Control and Prevention, with thehighest rates of blood lead levels foundamong poor, urban, African American,
Environmental Aspects o f Human Health
C H A P T E R F I V E 91

and Hispanic children. Although lead wasbanned from residential paint in 1978, itis estimated that 83 percent of all housingunits built before 1980 contain somelead-based paint. Older, deterioratingbuildings with peeling paint pose thegreatest lead risk. The Department ofHousing and Urban Development(HUD) estimates that about two out ofthree homes occupied by young childrenhave lead paint and dust hazards, poten-tially affecting their mental and neuraldevelopment. In adults, lead in the bloodcan interfere with hearing, increase bloodpressure, and, at high levels, cause kidneydamage and anemia.
In response to this environmentalhealth threat, several U.S. agencies havemade reducing lead exposure to childrena top priority. Under the Toxic Sub-stances Control Act and the ResidentialLead-Based Paint Hazard Reduction Actof 1992, many new rules have been orwill be developed to help reduce leadexposures. These rules incorporate leadhazard identification programs, lead dis-closure and consumer education, andrenovation and remodeling procedures toreduce lead hazards. Since 1992, HUDhas awarded a total of $279 million ingrants to reduce lead hazards in low-income housing. The grant program sup-ports activities such as public education(using local media and community-basedorganizations to ensure widespread dis-semination in the neighborhoods wherelead poisoning is most prevalent), paintinspection and risk assessments, low-costinterim controls, and lead abatement.EPA and the National Institute of Envi-ronmental Health Sciences (NIEHS) also
have programs researching the healthrisks from lead exposures as well as reduc-ing lead exposures.
Radon. Radon is a cancer-causing,radioactive gas that comes from the natur-al breakdown of uranium in soil, rock,and water. Odorless and colorless, radonis believed to be a leading cause of lungcancer in the United States today. Radonis estimated to cause about 14,000 deathsper year. However, this number couldrange from 7,000 to 30,000 deaths peryear. The links between radon and cancerare based largely on high-level dose-riskrelationships developed from early studiesof uranium miners, but the degree towhich residential exposure to radon rep-resents an actual risk of lung cancer is notknown. Despite the uncertainty about theexact toll on human health, all majorhealth organizations (e.g., the Centers forDisease Control and Prevention, theAmerican Lung Association, and theAmerican Medical Association) agreewith estimates that radon causes thou-sands of preventable lung cancer deathsevery year.
Radon gets into buildings from thesoil, moving up through the ground intobuildings through cracks in floors andwalls, construction joints, gaps aroundservice pipes, and well water. Nearly 1 outof every 15 homes in the United States isestimated to have indoor radon levels ator above EPA’s current action level of 4picocuries per liter. Typically, mitigationsystems to lower radon levels cost lessthan $2,000. With these systems, radonlevels can be lowered in virtually allhomes to below 4 picocuries per liter, and
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y92

in 70 percent of those homes the levelswill be below 2 picocuries per liter.
EPA has taken action on many frontsto address this hazard to human health.For example, EPA has developed a pro-gram that evaluates the proficiency ofcontractors who conduct radon testingand those who install mitigation systemsfor homes and buildings. The names ofproficient contractors are availablethrough states, and 20 states have addedtheir own certification programs for thesecontractors. EPA’s Office of Air and Radi-ation has been educating the publicabout the dangers of radon and aboutways to address it. This outreach programinforms communities about how simplemeasures such as sealing cracks in floorsand walls can help to reduce radon. Withthe assistance of EPA and other collabo-rative groups, state agencies are also com-ing up with innovative outreach pro-grams. For example, in Kentucky, thestate’s medical history forms were amend-ed to include a question about whetherpatients had tested their homes for radon.If not, a public health nurse would thenexplain radon risks and present abrochure on how to test a home cheaplyand quickly for radon. With one simplechange in a form, some 70,000 Kentuckycitizens are now being reached everyyear.
In the 6 years of the program, EPAestimates that more than 9 million homeshave been tested for radon and mitigationsystems have been installed in 300,000homes. In addition, on the basis of EPA’snational school survey and discussionswith states, it is estimated that about 20
percent of U.S. schools have been testedfor radon.
On the research front, DOE is spon-soring research at the Lawrence BerkeleyLaboratory’s Center for Building Sciencethat has found ways to prevent radonfrom entering homes. In addition,Lawrence Berkeley Laboratory is workingwith the U.S. Geological Survey to devel-op radon concentration maps.
Environmental Tobacco Smoke.Smoking is the number one cause oflung cancer in the United States, andone of the greatest public health threats.Many government agencies are activelypursuing policies, from education cam-paigns to regulatory instruments, to edu-cate the public about the health hazardsof smoking and to get people to put downtheir cigarettes.
Tobacco smoke can also be hazardousto the health of the nonsmoker. Environ-mental tobacco smoke, also known assecondhand smoke, includes mainstreamsmoke, which is exhaled by the smoker,and sidestream smoke, which is thesmoke that comes from the end of aburning cigarette, pipe, or cigar.
EPA estimates that environmentaltobacco smoke is responsible for approxi-mately 3,000 lung cancer deaths eachyear. EPA warns that environmentaltobacco smoke can be especially harmfulto children and estimates that on anannual basis it is responsible for 150,000to 300,000 cases of lower respiratory tractinfection, such as pneumonia and bron-chitis, in infants and children under 18months of age and a worsening of thecondition of 200,000 to 1 million asth-matic children.
Environmental Aspects o f Human Health
C H A P T E R F I V E 93

Many new laws, regulations, and ordi-nances restrict or ban public smoking.On the federal level, the General Ser-vices Administration imposed regulationsrestricting smoking to designated areas infederal office buildings. By law, smokingis prohibited on almost all domestic air-line flights and, by regulation, on allinterstate bus travel. In 1995, the UnitedStates entered into an internationalagreement banning smoking on all non-stop flights between the United States,Canada, and Australia. Currently, nearlyevery state has some form of legislation toprotect nonsmokers; some states requireprivate employers to enact policies thatprotect employees who do not smoke. Inaddition to state legislation, more than560 local jurisdictions have enacted ordi-nances addressing nonsmokers’ rights,and most are more restrictive than theirstate counterparts.
On August 23, 1996, President Clin-ton established the nation’s first-evercomprehensive program to protect chil-
dren from the dangers of tobacco and alifetime of nicotine addiction with thepublication of the Food and DrugAdministration’s final rule on tobaccoand children, and with FDA’s initiationof a process to require tobacco companiesto educate children and adolescents —using a national multimedia campaign— about the dangers of cigarettes andsmokeless tobacco.
The plan is intended to reduce tobac-co use by children and adolescents by 50percent in seven years. It builds on previ-ous actions taken by Congress and otherssuch as the ban on television advertisingand state laws to prohibit the sale or useof tobacco by children. It follows recom-mendations by the American MedicalAssociation and the National Academy ofScience’s Institute of Medicine. Expertshave consistently recommended that thekeys to achieving the goal are reducingaccess and limiting the appeal to chil-dren. This initiative accomplishes thatobjective while preserving the availabilityof tobacco products for adults.
CONTAMINATED FOOD ANDFISH
Pesticide Residues in Food
Pesticides are used widely in agricul-ture in the United States. The use of pes-ticides has contributed to dramaticincreases in yields for most major fruitand vegetable crops by controlling harm-ful pests. Their use has led to substantialimprovements over the past 40 years inthe quantity and variety of the U.S. dietand thus in the health of the public. The
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y94
1987 1989 1991 19930
1
2
3
4
5
% o
f sur
reill
ance
sam
ples
Domestic Imported
Figure 5.4 Pesticide Violations
in Food Samples, 1987-1994
Source: See Part III, Table 76.
cont
aini
ng v
iola
tive
resi
dues

use of pesticides can also reduce spoilageand health risks from biological contami-nants. In general, pesticide residues infood have remained at low levels formany years. In 1994, only about 1 per-cent of domestic food samples (55 out of5,366 samples) contained illegal pesti-cide residues that exceeded establishedtolerance levels. In imported food sam-ples, the frequency was 3.6 percent (197out of 5,488 samples). In 1987, 1.5 per-cent of domestic samples and 3.4 percentof imported samples exceeded tolerancelevels (Figure 5.4).
However, many pesticides are harmfulto the environment and may negativelyaffect human health. Historically, EPAhas regulated pesticides under two majorfederal statutes: the Federal Insecticide,Fungicide and Rodenticide Act (FIFRA)and the Federal Food, Drug, and Cos-metic Act (FFDCA). FIFRA prohibitsthe sale or use of pesticides not registeredby EPA for use in the United States andprescribes labeling and other regulatoryrequirements to prevent unreasonableadverse effects on health or the environ-ment. Under FFDCA, EPA establishestolerances (maximum legally permissiblelevels) for pesticide residues in food. Tol-erances are enforced by the Departmentof Health and Human Services’ Food andDrug Administration for most foods andby the U.S. Department of Agriculture’sFood Safety and Inspection Service formeat, poultry, and some egg products.
For over two decades, there have beenefforts to update and resolve inconsisten-cies in the two major pesticide statutes,but consensus on necessary reforms hasbeen elusive. In 1993, the Administration
published a “Pesticide Reform Agenda”with proposals for reform. In August1996, Congress unanimously passed andPresident Clinton signed a landmark pes-ticide food safety bill, the Food QualityProtection Act of 1996, which incorporat-ed these proposals, to better protect peo-ple from food contamination. The actrepresents a major breakthrough, amend-ing both FIFRA and FFDCA to establisha more consistent, protective regulatoryscheme, grounded in sound science. Itmandates a single, health-based standardfor all pesticides in all foods; providesspecial protection for infants and chil-dren; expedites approval of safer pesti-cides; creates incentives for the develop-ment and maintenance of effective cropprotection tools for American farmers;and requires periodic reevaluation of pes-ticide registrations and tolerances toensure that the scientific data supportingpesticide registrations will remain up todate.
A significant provision of the FoodQuality Protection Act is that it substi-tutes a single strong health-based limita-tion on risks presented by pesticides infood for the inconsistent standards in theDelaney clause. The Delaney clause,contained in the section on food addi-tives of the FFDCA, states that no addi-tive will “be deemed safe if it is found toinduce cancer when ingested by man oranimal” and directs EPA not to approvesuch food additives. Its language wasinterpreted to mean a “zero risk” stan-dard for any cancer-causing food additive,including residues from pesticides foundin processed foods. However, on rawfoods the law requires that EPA use a
Environmental Aspects o f Human Health
C H A P T E R F I V E 95

negligible risk standard, in the belief thatif the cancer risk is outweighed by severalfactors such as the ability of the pesticideto help in the production of an adequate,wholesome, and economical food supply,the safe use of the pesticide is warranted.Thus, the Delaney clause presented regu-lators with the problem of conflictingstandards for pesticides in raw versusprocessed foods. The application of theDelaney clause criteria limited the intro-duction of lower-risk pesticides that couldreplace older and potentially more haz-ardous compounds. Furthermore, theDelaney clause approach was undulynarrow, because it singled out one healthendpoint—cancer—and did not coversubstances causing birth defects, nervedamage, or immune system failures.
These “paradoxes” now no longer existfor pesticides in food. A new standardthat requires that all tolerances be safe, inboth raw and processed foods, is nowused. Safety is defined as “a reasonablecertainty that no harm will result fromaggregate exposure,” and the requirementapplies to both raw and processed food,not just for cancer risks, but for all risks.This revision will allow EPA and othersto address any risks presented by food as itis consumed as well as to devoteresources that had been consumed byDelaney-related activities to higher- prior-ity public health and environmental pro-tection activities, including mandatessecured in the Food Quality ProtectionAct of 1996: protecting children andother sensitive subpopulations, imple-menting Consumer Right-to-Know provi-sions regarding pesticide risks, and evalu-
ating and reducing risks from pesticidesthat may be endocrine disruptors.
Contaminated Fish
Last year, 46 contaminants, from diox-in to chlordane, were found in fish. Thenumber of lakes, rivers, and other U.S.waterways where consumers have beenadvised to avoid or limit consumption oftrout, salmon, or other species because ofchemical contamination rose from 1,278in 1993 to 1,740 in 1995 (Figure 5.5).
While EPA provides guidance on lev-els of contamination, primary responsibil-ity for protecting residents from thehealth risks of consuming noncommer-cial contaminated fish and wildlife lieswith the states, the District of Columbia,and the four U.S. territories. They issueconsumption advisories to the publicwhen high concentrations of chemicalcontaminants have been found in localwildlife and freshwater fish. A completedatabase of these advisories—the Nation-
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y96
Others
DDT
Dioxins
Chlordane
PCBs
Mercury
0 500 1,000 1,500number issued per pollutant
1993
1994
1995
Figure 5.5 Contaminated Fish
Advisories, 1993-1995
Source: U.S. Environmental Protection Agency (EPA),
Update: National Listing of Fish and Wildlife Consump-
tion Advisories (EPA, Office of Water, 1996).

al Listing of Fish and Wildlife Consump-tion Advisories—is maintained by EPA’sOffice of Water to help water quality offi-cials and the public identify where fishcontamination is a concern. The data-base contains information on the types ofadvisories and bans in effect (e.g.,whether the advisory applies to the popu-lation in general or only to sensitive sub-populations such as pregnant women andchildren), the species and size range ofpiscivorous (fish-eating) fish in the wild,the chemical contaminant identified inthe advisory (e.g., mercury, PCBs, chlor-dane, dioxins, or DDT), the geographiclocation and area covered by each adviso-ry, and the date the advisory was issued.
The database is designed primarily tohelp federal, state, and local governmentagencies and Native American tribesassess the potential for human healthrisks associated with the consumption ofchemical contaminants in noncommer-cial fish and wildlife. The increase inadvisories issued between 1993 and 1995reflects an increase in the number ofassessments of the levels of chemical con-taminants in fish and wildlife tissues.These additional assessments were con-ducted as a result of increased awarenessof health risks associated with the con-sumption of chemically contaminatedwildlife and freshwater fish. The numberof advisories decreases if states determinethat the monitored concentrations ofchemical contaminants in wildlife orfreshwater fish tissues have decreased andno longer pose a risk to human health.
Mercury, PCBs, chlordane, dioxins,and DDT were responsible for almost 95percent of all fish consumption advisories
in effect in 1995. In 463 cases, the advi-sories recommended that everyone avoideating a certain species of fish; in 1,393instances, children, pregnant women, orother vulnerable groups were warned torestrict or eliminate their freshwater fishconsumption.
For commercial fish, EPA and FDAalso set limits for levels of chemical cont-amination to protect human health.
Case Study: The DioxinReassessment
Since the early 1970s, dioxins haveoften been referred to as one of the mosttoxic groups of chemical compoundsknown. Dioxins are inadvertently createdthrough a number of activities, includingcombustion, certain types of chemicalmanufacture, chlorine bleaching of pulpand paper, and other industrial processes.The main pathway for exposure tohumans is via airborne emissions of diox-in that settle on plants and are passed onand accumulated through the foodchain. While dioxin is produced in verysmall quantities in comparison with otherpollutants (equivalent to around 30pounds of the most toxic member of theclass annually), its high toxicity and prop-erties of bioaccumulation and persistencein the environment have led EPA to treatdioxin as a major public health threat.EPA first took action against dioxinregarding the herbicide 2,4,5-T in 1979and since then has expanded its dioxincontrol efforts to each of its major pro-grams.
In 1985, EPA published a scientificreview of the health effects of 2,3,7,8-
Environmental Aspects o f Human Health
C H A P T E R F I V E 97

TCDD, the most toxic of the dioxin fami-ly of compounds. In the 1985 assessment,EPA concluded that dioxin is a provenanimal carcinogen and a probablehuman carcinogen and began using thatassessment as the scientific basis for diox-in risk estimates for all EPA programs. In1988, EPA prepared a draft reassessment,as well as a draft exposure document thatpresented procedures for conducting site-specific exposure assessments. However,questions about the scientific methodolo-gy, dioxin’s toxicity, and possible healtheffects remained.
In 1991, EPA announced that it wouldconduct a scientific reassessment of thehealth risks of exposure to dioxin anddioxinlike compounds, drawing on signif-icant advances in the scientific under-standing of mechanisms of dioxin toxici-ty, new studies of dioxin’s carcinogenicpotential in humans, and increased evi-dence of other adverse health effects. InSeptember 1994, EPA released its final“public review draft” of the dioxinreassessment. The dioxin reassessmentbreaks new ground—not only by provid-ing policymakers with the most compre-hensive assessment of dioxin to date, butalso by establishing a new, participatorymodel of how a risk assessment should beconducted.
The dioxin reassessment process isnoteworthy for several reasons. First, EPAhas worked to make each phase of thedioxin reassessment an open and partici-patory process. More than 100 scientistsfrom academia, government, and indus-try have collaborated throughout thereassessment process by providing data,writing chapters, and reviewing drafts. In
addition, EPA has held several publicmeetings to gather comments onprogress, and it published earlier draftsfor public comment and review. Second,unlike the 1985 report, which consideredonly the compound 2,3,7,8-TCDD, the1994 draft report also investigates thehealth impacts of dioxin-related com-pounds. Thus, other chemicals thatbehave like dioxins (i.e., chemicals thathave a similar structure to dioxin andbind to a cellular protein called the “Ahreceptor”) were also considered in the1994 report.
Third, the 1994 draft report is alsounique in that it attempted to provide acomprehensive inventory of emissionsources. It found that waste combustionaccounts for a large percentage of allknown emissions, yet acknowledged thelikelihood that there are a number ofunidentified sources of dioxin in theUnited States. The sources of dioxin arestill under review, and EPA is still in theprocess of collecting additional informa-tion and data about sources and emissionlevels.
Finally, unlike the 1985 report, whichfocused exclusively on cancer risks, the1994 draft report evaluates dioxin’s non-cancer effects as well. These effects mayinclude developmental and reproductiveeffects, immune suppression, and disrup-tion of hormones that regulate normalbiological functions. In addition, thereassessment reaffirmed with greater con-fidence that dioxin is a proven animalcarcinogen and a probable human car-cinogen.
Until the final report is released in1997, EPA’s efforts to control dioxin risks
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y98

will not change. Indeed, during thereassessment process, efforts to imple-ment dioxin control programs have con-tinued. In December 1995, EPA Admin-istrator Carol Browner announcedpromulgation of air standards for newand existing municipal waste combustors.The rule specifies technology-based per-formance standards, which would reducedioxin and other organic chemical emis-sions by 95 to 99 percent from a numberof existing municipal waste combustorsand all new plants. In addition, EPA hasproposed similar regulations for medicalwaste incinerators. EPA has continued toadminister programs to limit dioxin con-tamination of U.S. waters by developingtechnology-based effluent limitationguidelines for pulp and paper mills, bydeveloping ambient water quality criteriaguidance, and by prohibiting the dis-charge of dredged material that is conta-minated with dioxin in violation of statewater quality standards. The Safe Drink-ing Water Program, the Superfund Pro-gram, and the Pesticides and ToxicChemicals Program also all have activepollution prevention and control pro-grams for dioxins and furans. Once thefinal report is released, EPA will begin anextensive review of policies developed tomanage dioxin risks, again relying heavilyon early public input into the policy eval-uation process.
EMERGING CHALLENGES
The Endocrine Disruptor Debate
There have been many reports thatdomestic animals and wildlife have suf-
fered adverse reproductive and otherhealth effects from exposure to environ-mental chemicals that interact with theendocrine system, often called endocrinedisruptors or environmental hormones.These problems have primarily beenidentified in animals and humansexposed to relatively high levels of certainorganic chemicals. Whether similareffects are occurring in the generalhuman or wildlife populations fromambient environmental levels is current-ly unknown.
While many uncertainties existregarding the effects that environmentalhormones have on humans and animals,the issue must be taken seriously. Hor-mones play a major role in the function-ing of all organ systems, and small distur-bances in endocrine function inlaboratory animals, at critical stages ofdevelopment, have been shown to pro-duce profound and lasting effects. Inaddition, people are exposed to a com-plex mixture of many natural and syn-thetic compounds, which may have syn-ergistic effects. Further, some chemicalsthat have been identified as endocrinedisruptors, such as PCBs, persist in theenvironment for a long time.
Most of the effects associated withexposure to endocrine-disrupting chemi-cals, such as reproductive dysfunctionand sexual abnormalities, have beenobserved in wildlife populations receivingrelatively high levels of exposure consist-ing mainly of persistent chlorinated com-pounds, such as DDT. Examples includereproductive problems in wood ducksfrom Bayou Meto, Arkansas; embryonicdeformities in Great Lakes fish-eating
Environmental Aspects o f Human Health
C H A P T E R F I V E 99

birds; feminization and demasculiniza-tion in gulls; developmental effects inGreat Lakes snapping turtles; and devel-opmental dysfunction in lake trout in theGreat Lakes. In each case, detectableconcentrations of chemicals with knownendocrine-disrupting effects have beenreported in the animals or their environ-ment, but a cause-and-effect link hasbeen established for only a few of theseobservations.
For human populations, some studieshave suggested that endocrine-disruptingchemicals may be responsible for report-ed increases in certain cancers andadverse reproductive effects. The hypoth-esis that endocrine disruptors can causecancer in humans is based largely on theclear association between exposure ofpregnant women to diethylstilbestrol(DES), a drug taken to avoid miscarriage,and reproductive organ cancers in theirdaughters. In addition, cancer trend datafor the 1973–91 period show increases inthe incidence of some cancers associatedwith hormones (female breast, 24 per-cent; testicular, 41 percent; prostate, 126percent). So far, because there are insuf-ficient supporting data, the linkagebetween the incidence of human cancersand an endocrine (hormonal) disruptionmechanism remains a working hypothe-sis. Most of these increases in incidencemay be attributed to improvements indetection and early diagnosis, or otherfactors. In the case of breast cancer, forexample, epidemiological studies havedetermined a variety of risk factors, suchas oral contraceptives, estrogen replace-ment therapy, family history, smoking,and alcohol use.
There have been documented cases ofreproductive problems in humansexposed accidentally to high doses ofendocrine-disrupting chemicals as well asreports of declines in the quality andquantity of sperm production in humansover the last four decades. Several stud-ies, such as a 1992 study by Carlsen et al.and a 1995 study by Auger et al., haveprovided evidence that there have beendeclines in sperm count in their selectedpopulations. However, other studies, suchSuominen and Vierula’s review of severalstudies published between 1958 and1992, and clinical studies by Fisch et al.and Paulsen et al., have concluded thatthere were no decreases in sperm countor semen volume. Thus, while there maybe reductions in some specific locations,more research is needed concerningpotential reductions in sperm productionin the general population.
While there is much scientific uncer-tainty and debate about this issue, thereis resounding agreement that additionaldata and research are needed. The pub-lic and private sectors have recognizedthis need and have established researchprograms. Several federal agencies arecurrently engaged in a wide range ofresearch activities relating to endocrinedisruptors, which include studies of expo-sure and effects, as well as the mecha-nisms of endocrine-disrupting chemicals.The National Science and TechnologyCouncil’s Committee on Environmentaland Natural Resources identified thisissue as an initiative in November 1995,and has established an interagency work-ing group of scientists to identify researchneeds related to the health and ecologi-
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y100

cal effects of endocrine-disrupting chemi-cals and to develop an interagencyresearch plan. The National Academy ofSciences is also conducting an assess-ment. The Environmental ProtectionAgency has recently completed an agen-cywide draft on the state of the scienceentitled “Environmental Endocrine Dis-ruption: An Effects Assessment andAnalysis Document,” which has beensubmitted to the Risk Assessment Forumand the Science Policy Council forapproval. EPA is also forming a commit-tee (the Endocrine Disruptor Screeningand Testing Advisory Committee) toadvise the agency on the development ofa strategy for screening and testing chem-icals and pesticides for their potential todisrupt the endocrine system. Theseefforts, and others, will lead the way to abetter understanding of endocrine disrup-tors and their potential impacts and ulti-mately will provide the tools needed tomake informed policy decisions aboutthis issue.
Ozone and Climate Change
Ozone. In 1994, the World Meteoro-logical Organization (WMO) in collabo-ration with the National Oceanic andAtmospheric Administration (NOAA),National Aeronautics and Space Admin-istration (NASA), and the United NationsEnvironment Programme (UNEP)released its scientific assessment of ozonedepletion. The report, Scientific Assess-ment of Ozone Depletion: 1994, includesa review of potential health impacts fromstratospheric ozone depletion.
The assessment reports that the accu-mulation of certain human-made gasesin the upper atmosphere or stratos-phere—from the widespread use of vari-ous halocarbons for refrigeration, insulat-ed packaging, and in industry andagriculture—has resulted in a sustaineddecline in stratospheric ozone concentra-tions. The major consequence of thisstratospheric ozone depletion is reducedshielding of Earth’s surface againstincoming solar ultraviolet radiation; thus,a continuing depletion of stratosphericozone would increase the amount ofultraviolet radiation that reaches Earth’ssurface. These increases would be experi-enced, mostly, in the middle and highlatitudes, where the majority of the globalpopulation is concentrated. Indeed, Unit-ed Nations projections indicate that asozone depletion reaches its peak beforethe year 2000, mid-latittudes in theNorthern Hemisphere may experience a15 percent increase in UV-B exposureduring winter and spring. The assessmentfound that UV-B radiation increased by 2percent for every 1 percent decrease inthe ozone layer.
Although the amount of UV-B strikingEarth’s surface can vary routinely by asmuch as 20 percent, scientists havewarned that if the current trend were tocontinue, radiation would reach levelshigh enough to increase the incidence ofskin cancer and cataracts in humans.The assessment, assuming no change inexposure patterns in the general popula-tion, projected that a sustained 10 to 15percent depletion of stratospheric ozoneover several decades could result in anestimated 15 to 20 percent increase in
Environmental Aspects o f Human Health
C H A P T E R F I V E 101

the incidence of skin cancer in fair-skinned populations. Solar ultravioletlight is an important cause of squamous-cell carcinoma of the eye. Increased UV-B radiation can also interfere with thebody’s immune system; this constitutesone of the most potentially dangerouseffects of UV-B because of the possibilitythat immunity to infectious diseases maybe compromised.
Climate Change. As discussed inChapter 12, “Climate Change,” theinternational scientific community, repre-sented by the 2,500 scientists of the Inter-governmental Panel on Climate Change(IPCC), reported in its latest assessmentin 1995 that human activities are havinga discernible influence on global climate.The models used by the IPCC predict anincrease in average global temperature ofabout 1o to 3.5o C (1.4o to 6.3o F) by2100. A change of this magnitude willlikely produce alterations both in physi-cal systems (e.g., higher temperatures,heavier rainfall, and rising sea level) andin ecosystems (e.g., forests, agriculture,marine ecologies, and the habitats of var-ious insects and animals), with profoundimplications for human health.
In its chapter on human health, theIPCC reports that climate change, byaltering local weather patterns and by dis-turbing life-supporting natural systemsand processes, may affect the health ofhuman populations and that adverseeffects are likely to outweigh beneficialeffects. The range of health effects wouldbe diverse, often unpredictable in magni-tude, and sometimes slow to emerge.Researchers believe that both direct risks(e.g., death in heat waves or floods) and
indirect risks (e.g., changes in food pro-duction or the distribution and incidenceof vector-borne diseases) to human healthwill emerge.
Estimating health impacts of climatechange is still a relatively new field of sci-entific study, and it remains controver-sial. There are inevitable, multipleuncertainties involved in trying to projectpotential health impacts in relation tofuture scenarios of climate change. Inaddition, actual health impacts will varydramatically by region depending onenvironmental circumstances, the exist-ing health infrastructure, social and eco-nomic resources, and the baseline healthstatus of the population. Many of theanticipated adverse health impacts of cli-mate change are expected in the world’sless-developed regions; in many of thosecountries, there already exists a highprevalence of undernutrition, chronicexposure to infectious disease agents, andinadequate access to social and physicalinfrastructure. Nevertheless, humanhealth in the United States may beadversely affected in several ways: by anincrease in heat-related mortality, espe-cially in urban areas; by an increase inthe frequency and severity of extremeweather events such as flooding; and byan increase in the potential for the spreadof diseases such as malaria, dengue,cholera, and salmonellosis. In addition,demographic trends including popula-tion aging and increasing levels of disabil-ity, chronic illness, and coastal retire-ment may increase the vulnerability ofthe U.S. population to adverse healthimpacts related to climate change.
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y102

Cases of heat-stress mortality, particu-larly in vulnerable individuals such as thevery young and the very old, couldincrease because of climate change.Recent analyses of concurrent meteoro-logical and mortality data in cities in theUnited States, Canada, the Netherlands,China, and the Middle East show thatoverall death rates rise during heat waves,particularly when the temperature andhumidity rise above the local popula-tion’s threshold value. One model sug-gests that the annual number of heat-
related deaths would approximately dou-ble by 2020 and would increase several-fold by 2050. For a city like Atlanta,Georgia, that could increase the numberof heat-related deaths from the currentaverage of about 80 each summer tonearly 200 in 2020 and closer to 300 in2050 (see Table 5.2). These estimates arebased on myriad assumptions and involvea large amount of uncertainty. Neverthe-less, in very large cities with populationssensitive to heat stress, climate change
Environmental Aspects o f Human Health
C H A P T E R F I V E 103
Table 5.2
Total Summer Heat-related Deaths in Selected Cities:Current Mortality and Estimates of Future Mortality Under the
GFDL89 Climate Change Scenario
GFDL89 climate change scenario
Year 2020 Year 2050
Present No Acclimatized No AcclimatizedCity mortality1 acclimatization population acclimatization population
average number of summer-season heat-related deaths
United States Atlanta 78 191 96 293 147Dallas 19 35 28 782 618Detroit 118 264 131 419 209Los Angeles 84 205 102 350 174New York 320 356 190 879 494Philadelphia 145 190 142 474 354San Francisco 27 49 40 104 85
CanadaMontreal 69 121 61 245 124Toronto 19 36 0 86 1
ChinaShanghai 418 1,104 833 2,950 1,033
EgyptCairo 281 476 na 830 na
Source: A.H. McMichael, A.Haines, R.Sloof and S, Kovats, eds. Climate Change and HumanHealth, p. 57 (World Health Organization and United Nations Environment Program, Geneva,1996).
Notes: 1raw mortality data. na=not applicable.

could cause significant increases in extraheat-related deaths annually.
Climate change will also likelyincrease the frequency and severity ofsome extreme weather events such asflooding. Flash flooding is currently aleading cause of weather-related mortali-ty in the United States. In addition todirect deaths from drowning and otheraccidents, flooding could also facilitatethe spread of infectious diseases by dam-aging homes and displacing residents, aswell as contaminating water sources withfecal material or toxic chemicals. Weath-er-related disasters often overwhelm localpublic health facilities and water and san-itation infrastructure, further affectinghuman health.
A third area in which climate changecan affect human health in the UnitedStates is by changing the distribution ofdisease vectors. Infectious agents andtheir vector organisms are sensitive to fac-tors such as temperature, surface water,humidity, wind, soil moisture, andchanges in forest distribution. Net cli-mate-change-related increases in the geo-graphic distribution (altitude and lati-tude) of the vector organisms ofinfectious diseases (e.g., malarial mosqui-tos, schistosome-spreading snails) andchanges in the life-cycle dynamics ofboth vector and infective parasites would,in aggregate, increase the potential trans-mission of many vector-borne diseases.Malaria, a mosquito-borne disease thatcurrently afflicts an estimated 1 in 20people in the world, provides an apt
example. Models reported on by theIPCC suggest that with the predicted cli-mate change, the proportion of theworld’s population living within thepotential malaria transmission zonecould increase from around 45 to around60 percent by the latter half of the nextcentury. Although this predicted increasein potential transmission encroachesmostly into temperate regions, actual cli-mate-related increases in malaria inci-dence would occur primarily in tropical,subtropical, and less well protected tem-perate zone populations currently at themargins of endemically infected areas.
Addressing the Issues. The UnitedStates has been an active participant inboth the Montreal Protocol and the Cli-mate Convention. On December 31,1995, the industrialized nations of theworld officially ended their production ofozone-depleting chlorofluorocarbons(CFCs), except for a few essential uses.The U.S. role in this effort and theAdministration’s continued work towardreducing greenhouse gas emissions arediscussed in detail in Chapter 11,“Stratospheric Ozone” and Chapter 12,“Climate Change.”
On the health side, the Administrationis working closely with the scientific com-munity to further investigate the linksbetween ozone depletion and climatechange and human health. The develop-ment of advanced remote sensing andGIS technologies will help in facilitatinglarge-scale data collection and analysis.
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y104

Environmental Aspects o f Human Health
C H A P T E R F I V E 105
REFERENCES
Auger, J., et al., “Decline in Semen Quality Among Fertile Men in Paris During the Past 20Years,” New England Journal of Medicine, Vol. 332 (1995), pp. 281–285.
Browner, Carol M., “Environmental Tobacco Smoke: EPA’s Report,” EPA 175-N-93-027, EPAJournal (Fall 1993).
Carlsen, E., et al., “Evidence for Decreasing Quality of Semen During Past Fifty Years,” BritishMedical Journal, Vol. 304 (1992), pp. 609–613.
Center for the Study of Environmental Endocrine Effects, “Environmental Endocrine Effects:An Overview of the State of Scientific Knowledge and Uncertainties,” discussion draft (Centerfor the Study of Environmental Endocrine Effects, Washington, DC, September 1995).
Colburn, Theo, Dianne Dumanoski, and John Peterson Myers, Our Stolen Future: Are WeThreatening Our Fertility, Intelligence, and Survival - A Scientific Detective Story (Dutton, NewYork, 1996).
Cushman, John, Jr., “E.P.A. Plans Radical Change in Calculation of Cancer Risk,” The NewYork Times, April 16, 1996, pp. A1, A18.
“Dioxins and Dioxin-like Chemicals,” Environmental Health Monthly, Vol. 7, No. 6 (March1995).
Dockery, Douglas W., et al., “An Association Between Air Pollution and Mortality in Six U.S.Cities,” The New England Journal of Medicine, Vol. 329, No. 24 (December 1993), pp.1753–1759.
Farland, William H., “EPA’s Scientific Reassessment of Dioxin,” Health and EnvironmentDigest, Vol. 5, No. 12 (March 1992).
Fisch, H., et al., “Semen Analyses in 1,238 Men from the United States over a 25-Year Period:No Decline in Fertility,” Fertility and Sterility, Vol. 65 (1996), pp. 1009–1014.
Folinsbee, Lawrence J., “Human Health Effects of Air Pollution,” Environmental Health Per-spectives, Vol. 100 (1992), pp. 45–56.
Food and Drug Administration (FDA), Pesticide Program Residue Monitoring 1994 (FDA,Washington, DC, 1994).
Hileman, Bette, “Health Effects of Electromagnetic Fields Remain Unresolved,” Chemicaland Engineering News (November 8, 1993).
Institute of Medicine, Emerging Infections: Microbial Threats to Health in the United States(National Academy Press, Washington, DC, 1992).
Intergovernmental Panel on Climate Change, Climate Change 1995: Impacts, Adaptations,and Mitigation Summary for Policy Makers, Contribution of Working Group II to the SecondAssessment Report (Intergovernmental Panel on Climate Change, Washington, DC, 1995).
Kavlock, R.J., et al., “Research Needs for the Risk Assessment of Health and EnvironmentalEffects of Endocrine Disruptors: A Report of the U.S. EPA-sponsored Workshop,” Environmen-tal Health Perspectives, Vol. 104, Supplement 4 (1996).

Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y106
Lee, Gary, “Clean Air Regulations Are Paying Off, EPA Says,” The Washington Post (June 10,1996), p. A17.
Lee, Gary, “Hospitalizations Tied to Ozone Pollution,” The Washington Post (June 21, 1996),p. A3.
McMichael, A.J., A. Hains, R. Sloof, and S. Kovats, eds., Climate Change and Human Health(World Health Organization, World Meteorological Organization, and United Nations Envi-ronment Programme, Geneva, 1996).
National Research Council, The Epidemiological Transition: Policy and Planning Implicationsfor Developing Countries (National Academy Press, Washington, DC, 1993).
National Research Council, Measuring Lead Exposure in Infants, Children, and Other Sensi-tive Populations (National Academy Press, Washington, DC, 1993).
National Research Council, Pesticides in the Diets of Infants and Children (National AcademyPress, Washington, DC, 1993).
National Science and Technology Council and Institute of Medicine, Conference on HumanHealth and Global Climate Change: Summary of the Proceedings (National Academy Press,Washington, DC, 1996).
Natural Resources Defense Council, Breathtaking: Premature Mortality due to Particulate AirPollution in 239 American Cities (Natural Resources Defense Council, New York, May 1996).
Nichols, Mary, “Lessons from Radon,” EPA 175-N-93-027, EPA Journal (Fall 1993).
Office of Technology Assessment, Identifying and Controlling Immunotoxic Substances: Back-ground Paper (Office of Technology Assessment, Washington, DC, 1991).
Office of Technology Assessment, Researching Health Risks (Office of Technology Assessment,Washington, DC, 1993).
Ozone ACTION, “Human Health Effects: Ozone Depletion and Climate Change,” FactSheet (Ozone ACTION, Washington, DC, 1996).
Patz, Jonathan A., et al., “Global Climate Change and Emerging Infectious Diseases,” Journalof the American Medical Association, Vol. 275, No. 3 (January 17, 1996), pp. 217–223.
Paulsen, C.A., N.G. Berman, and C. Wang, “Data from Men in Greater Seattle Area RevealsNo Downward Trend in Semen Quality: Further Evidence That Deterioration of SemenQuality Is Not Geographically Uniform,” Fertility and Sterility, Vol. 65 (1996), pp. 1015–1020.
Physicians for Social Responsibility and Environmental Defense Fund, Putting the Lid onDioxins: Protecting Human Health and the Environment (PSR and EDF, Washington, DC,1994).
Pope, Andrew, “Indoor Allergens: A Report,” EPA 175-N-93-027, EPA Journal (Fall 1993).
Pope, C. Arden, III, et al., “Particulate Air Pollution as a Predictor of Mortality in a ProspectiveStudy of U.S. Adults,” American Journal of Respiratory Critical Care Medicine, Vol. 151(1995), pp. 669–674.
The President’s Council on Sustainable Development, Sustainable America: A New Consen-sus for Prosperity, Opportunity, and a Healthy Environment for the Future (Government Print-ing Office, Washington, DC, 1996).

Environmental Aspects o f Human Health
C H A P T E R F I V E 107
Sexton, Ken, “An Inside Look at Air Pollution,” EPA 175-N-93-027 EPA Journal (Fall 1993).
Sexton, Ken, “Science and Policy in Regulatory Decision Making: Getting the Facts RightAbout Hazardous Air Pollutants,” Environmental Health Perspectives, Vol. 103, Supplement 6(1995), pp. 213–222.
Suominen, J., and M. Vierula, “Semen Quality of Finnish Men,” British Medical Journal, Vol.306 (1993), p. 1579.
U.S. Department of Agriculture (USDA), Water Quality, NRCS/RCA Issue Brief 9 (USDA,Natural Resources Conservation Service, Washington, DC, March 1996).
U.S. Department of Commerce, “We Asked . . . You Told Us: Source of Water and SewageDisposal,” Census Questionnaire Content, 1990 CQC–28 (Department of Commerce, Wash-ington, DC, February 1995).
U.S. Department of Health and Human Services, Healthy People 2000 Review (Department ofHealth and Human Services, Washington, DC, 1994).
U.S. Environmental Protection Agency (EPA), Air Quality Trends, EPA-454/F-95-003 (EPA,Washington, DC, September 1995).
U.S. Environmental Protection Agency (EPA), Environmental Indicators of Water Quality inthe United States, EPA 841-R-96-002 (EPA, Office of Water Washington, DC, June 1996).
U.S. Environmental Protection Agency (EPA), “EPA’s On-Going Regulatory Program,” Diox-in Facts (EPA, Office of Communications, Education, and Public Affairs, Washington, DC,September 1994).
U.S. Environmental Protection Agency (EPA), “For Your Information: Major Issues in theFood Quality Protection Act of 1996,” FYI Brief (EPA, Office of Prevention, Pesticides, andToxic Substances, Washington, DC, August 1996).
U.S. Environmental Protection Agency (EPA), “For Your Information: The Food Quality Pro-tection Act of 1996,” FYI Brief (EPA, Office of Prevention, Pesticides, and Toxic Substances,Washington, DC, August 1996).
U.S. Environmental Protection Agency (EPA), National Drinking Water Program RedirectionStrategy (EPA, Washington, DC, June 1996).
U.S. Environmental Protection Agency (EPA), “The Reassessment Process,” Dioxin Facts(EPA, Office of Communications, Education, and Public Affairs, Washington, DC, Septem-ber 1994).
U.S. Environmental Protection Agency (EPA), “The Safe Drinking Water Act Amendments of1996: Strengthening Protection for America’s Drinking Water,” draft paper (EPA, Office ofWater, Washington, DC, August 1996).
U.S. Environmental Protection Agency (EPA), Science Advisory Board Report: Safe DrinkingWater, Future Trends and Challenges, EPASAB-DWC-95002 (EPA, Washington, DC, 1995).
U.S. Environmental Protection Agency (EPA), “Scientific Highlights from Draft Reassess-ment,” Dioxin Facts (EPA, Office of Communications, Education, and Public Affairs, Wash-ington, DC, September 1994).
Environmental Aspects o f Human Health
E N V I R O N M E N T A L Q U A L I T Y108
U.S. Environmental Protection Agency (EPA), “Statement of Lynn Goldman, M.D., AssistantAdministrator for Prevention, Pesticides, and Toxics: September 13, 1994,” press release (EPA,Office of Communications, Education, and Public Affairs, Washington, DC, September 1994).
U.S. Environmental Protection Agency (EPA), Update: National Listing of Fish and WildlifeConsumption Advisories, Fact Sheet, EPA-823-F-96-006 (EPA, Office of Water, Washington,DC, June 1996).
U.S. Environmental Protection Agency (EPA), Watershed Protection: A Statewide Approach(EPA, Office of Water, Washington, DC, March 1996).
U.S. Environmental Protection Agency (EPA), “White Paper,” Strengthening the Safety of OurDrinking Water: A Report on Progress and Challenges and an Agenda for Action (EPA, Washing-ton, DC, March 1995).
Vogt, Donna U., The Delaney Clause Effects on Pesticide Policy, Congressional Research Ser-vice Report for Congress 95-514 SPR (Congressional Research Service, Washington, DC,1995).
The World Commission on Environment and Development (The Brundtland Commission),Our Common Future (Oxford University Press, Oxford, 1987).
World Meteorological Organization (WMO) in collaboration with the National Oceanic andAtmospheric Administration (NOAA), National Aeronautics and Space Administration(NASA), and the United Nations Environment Programme (UNEP), Scientifc Assessment ofOzone Depletion: 1994, Global Ozone Research and Monitoring Project - Report No. 37(WMO, NOAA, NASA, UNEP, Geneva, 1995).
World Resources Institute in collaboration with the United Nations Environment Programme,the United Nations Development Programme, and the World Bank, World Resources 1996–97(Oxford University Press, New York, 1996).