chapter 9 growth hormones and the...
TRANSCRIPT
Chapter 9
Growth Hormones and
the Somatomedins
Nam Deuk Kim, Ph.D.
1
1. Endocrine Control of Growth
• Growth depends on growth hormone but is
influenced by other factors as well
– Genetic determination of an individual’s
maximum growth capacity
– An adequate diet
– Freedom from chronic disease and stressful
environmental conditions
– Normal levels of growth-influencing hormones
2
Growth Rate
• Not continuous
• Factors responsible for promoting growth
are not the same throughout growth period
• Fetal growth
– Promoted largely by hormones from placenta
– GH plays no role in fetal development
• Postnatal growth spurt
– Displayed during first two years of life
• Pubertal growth spurt
– Occurs during adolescence
3
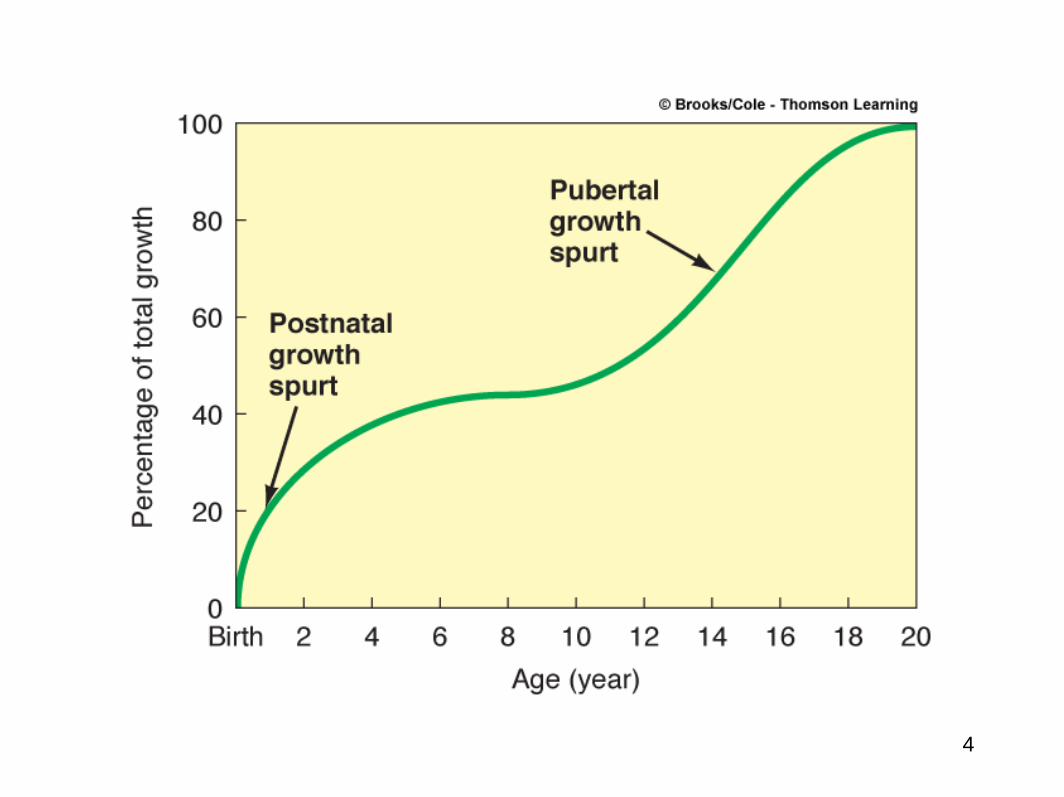
Normal Growth Curve
4
2. Growth Hormone and the Somatomedins • Primarily promotes growth indirectly by stimulating liver’s
production of somatomedins
– Primary somatomedin is insulin-like growth factor (IGF-1)
• 70 amino acids
• Acts directly on bone and soft tissues to bring about most
growth-promoting actions
• Stimulates protein synthesis, cell division, and lengthening
and thickening of bones
• IGF-2: 67 amino acids polypeptide with less well known
function
• Exerts metabolic effects not related to growth
– Increases fatty acid levels in blood by enhancing breakdown
of triglyceride fat stored in adipose tissue
– Increases blood glucose levels by decreasing glucose uptake
by muscles
5
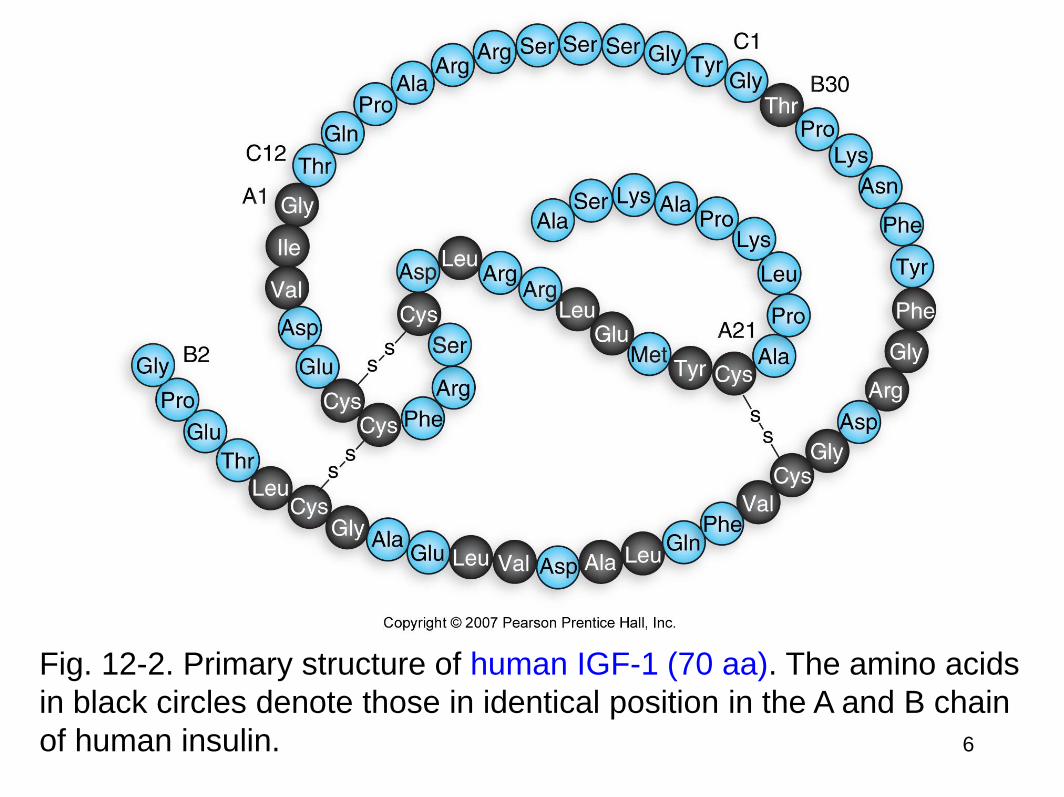
Fig. 12-2. Primary structure of human IGF-1 (70 aa). The amino acids
in black circles denote those in identical position in the A and B chain
of human insulin. 6
INSULIN-LIKE GROWTH FACTOR 1 (IGF-1)
Synthesized mainly by liver in response to GH - somatomedin
Mediates effects of GH on bone and cartilage
85% homology with proinsulin
Continuous peptide chain unlike insulin
Starvation or illness blocks IGF-1 formation in response to GH –
growth ceases during severe illness
Does it make sense that starvation activates GHRH release?
YES – in starvation GH exerts glucagon-like effects
but its ability to promote IGF-I synthesis and secretion is blocked
7
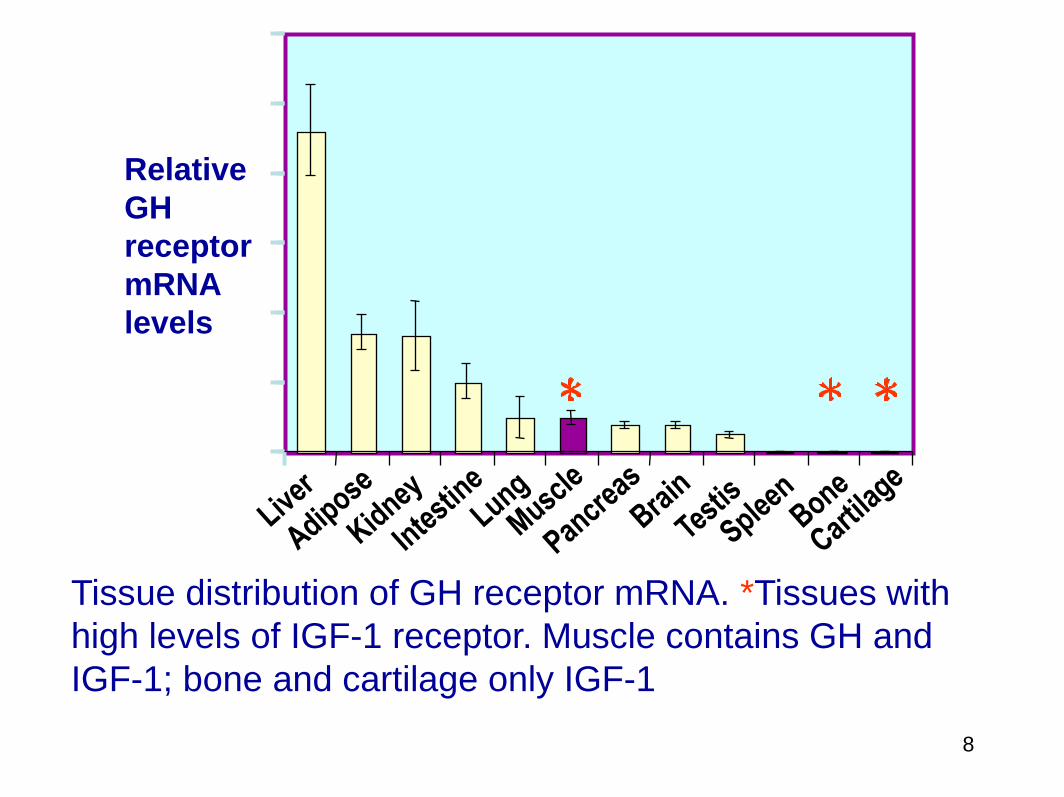
Relative
GH
receptor
mRNA
levels
Tissue distribution of GH receptor mRNA. *Tissues with
high levels of IGF-1 receptor. Muscle contains GH and
IGF-1; bone and cartilage only IGF-1
8
Summary of GH and IGF-1 effects
Direct effects of GH include
Muscle amino acid uptake resulting in protein synthesis
Glucose use peripherally (anti-insulin)
Glucose output from liver (anti-insulin)
Fat mobilization (anti-insulin) Ketogenesis in liver (anti-insulin)
IGF-I release from liver
Direct effects of IGF-1 include
Cartilage/bone growth
Muscle growth/proliferation
9
IGF-1 mechanism of action – similar to insulin in that
signaling is via receptor tyrosine kinase
Insulin and IGF-1 bind to each other’s receptors but only at
high concentration
IGF-1 receptor mainly mediates mitogenic/growth effects
Different physiological roles of insulin and IGF-1 accounted
for by cellular distribution of their receptors
IGF-1 vs. INSULIN
10
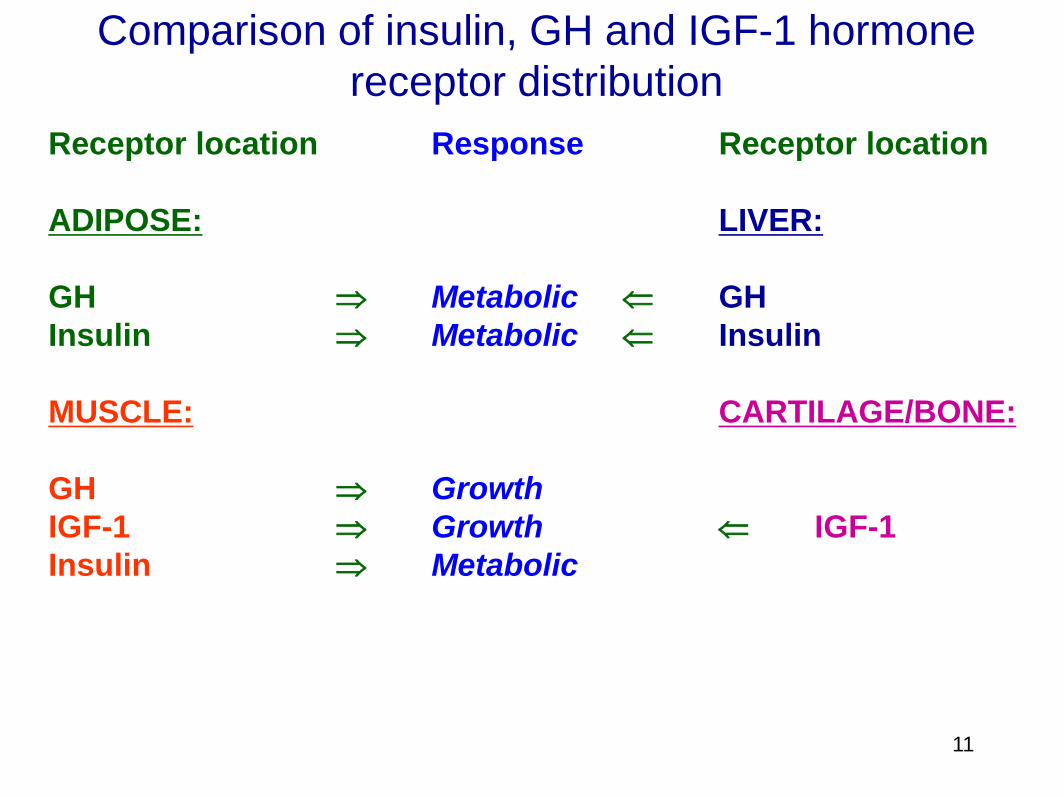
Comparison of insulin, GH and IGF-1 hormone
receptor distribution
Receptor location Response Receptor location
ADIPOSE: LIVER:
GH Metabolic GH
Insulin Metabolic Insulin
MUSCLE: CARTILAGE/BONE:
GH Growth
IGF-1 Growth IGF-1
Insulin Metabolic
11
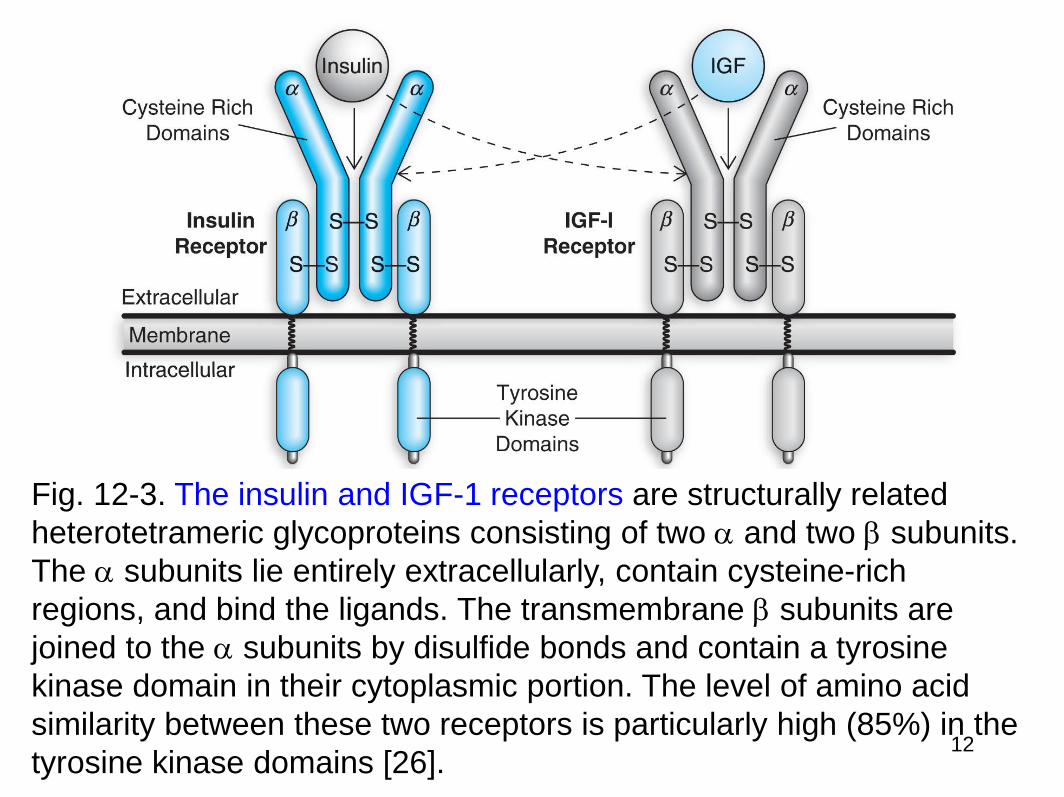
Fig. 12-3. The insulin and IGF-1 receptors are structurally related
heterotetrameric glycoproteins consisting of two and two subunits.
The subunits lie entirely extracellularly, contain cysteine-rich
regions, and bind the ligands. The transmembrane subunits are
joined to the subunits by disulfide bonds and contain a tyrosine
kinase domain in their cytoplasmic portion. The level of amino acid
similarity between these two receptors is particularly high (85%) in the
tyrosine kinase domains [26]. 12
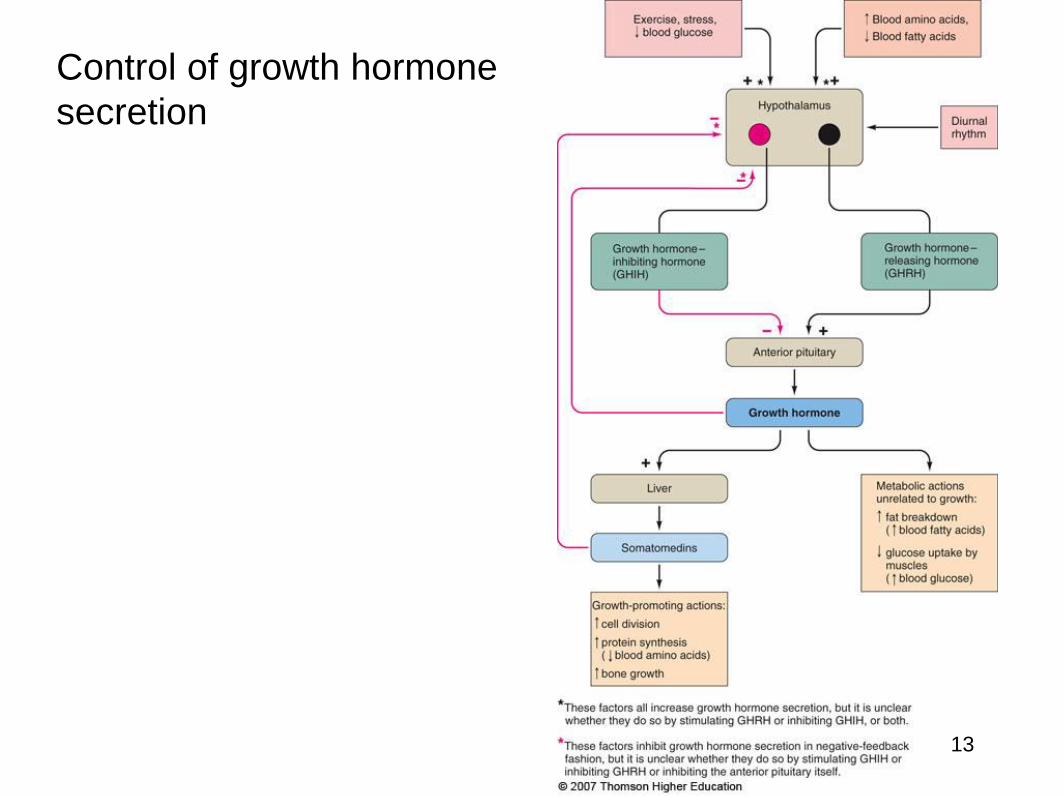
Control of growth hormone
secretion
13
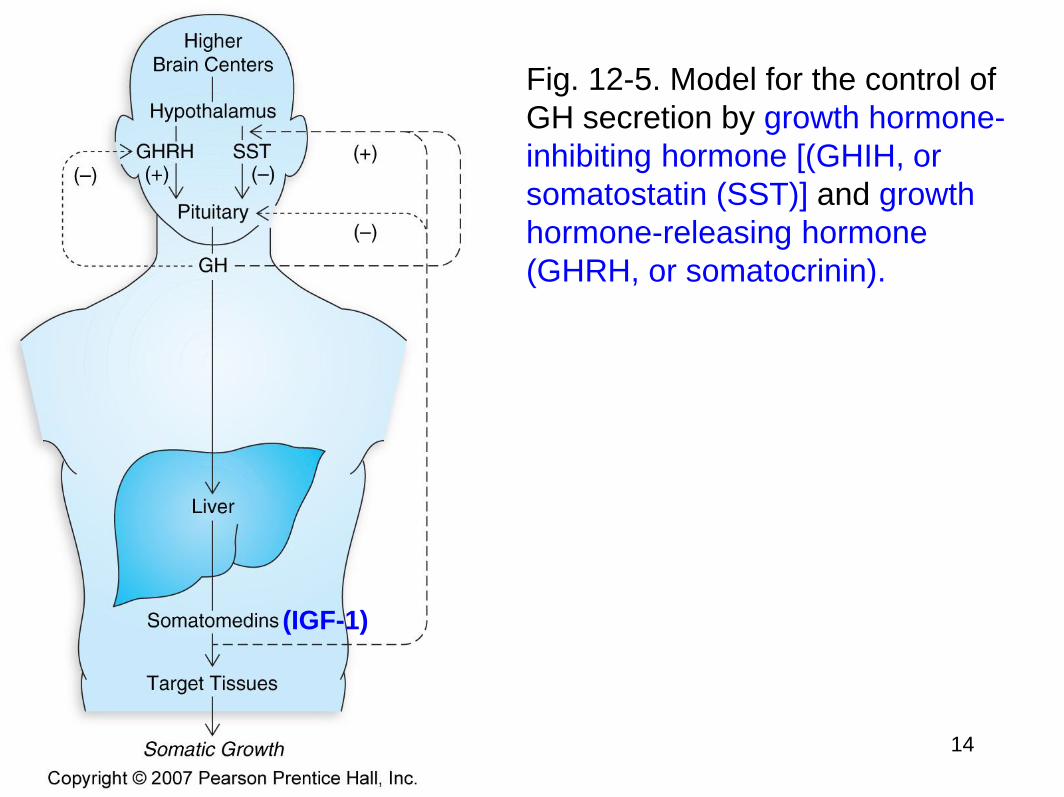
Fig. 12-5. Model for the control of
GH secretion by growth hormone-
inhibiting hormone [(GHIH, or
somatostatin (SST)] and growth
hormone-releasing hormone
(GHRH, or somatocrinin).
(IGF-1)
14
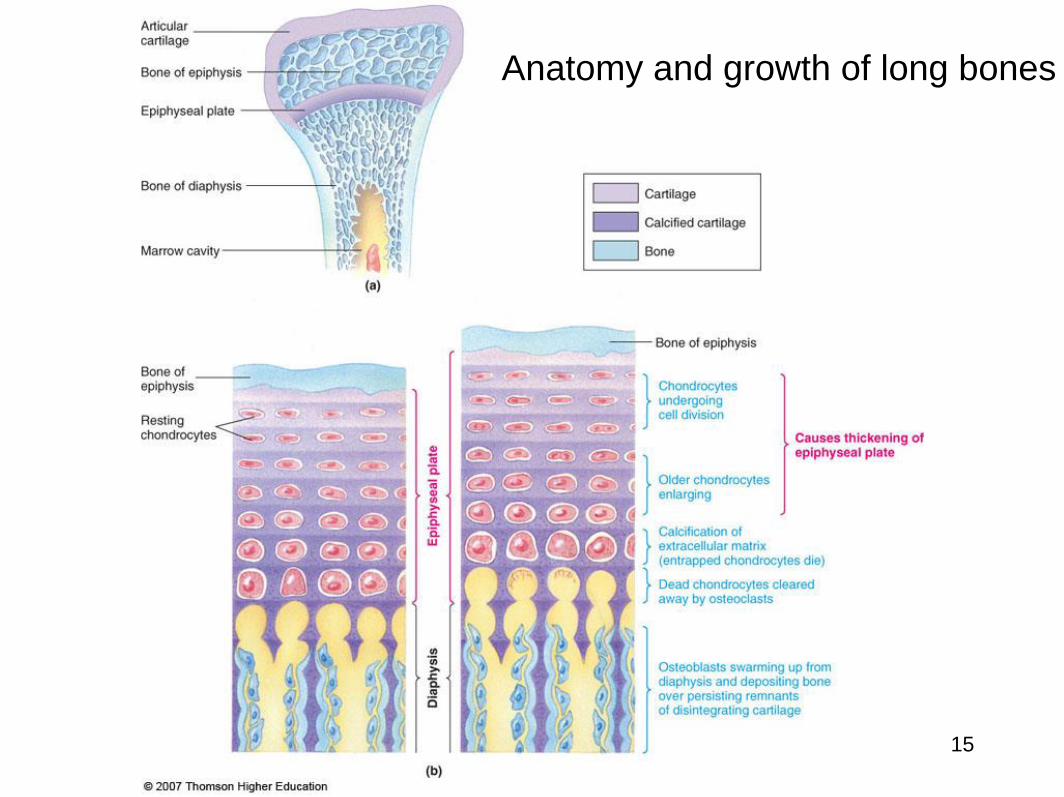
Anatomy and growth of long bones
15
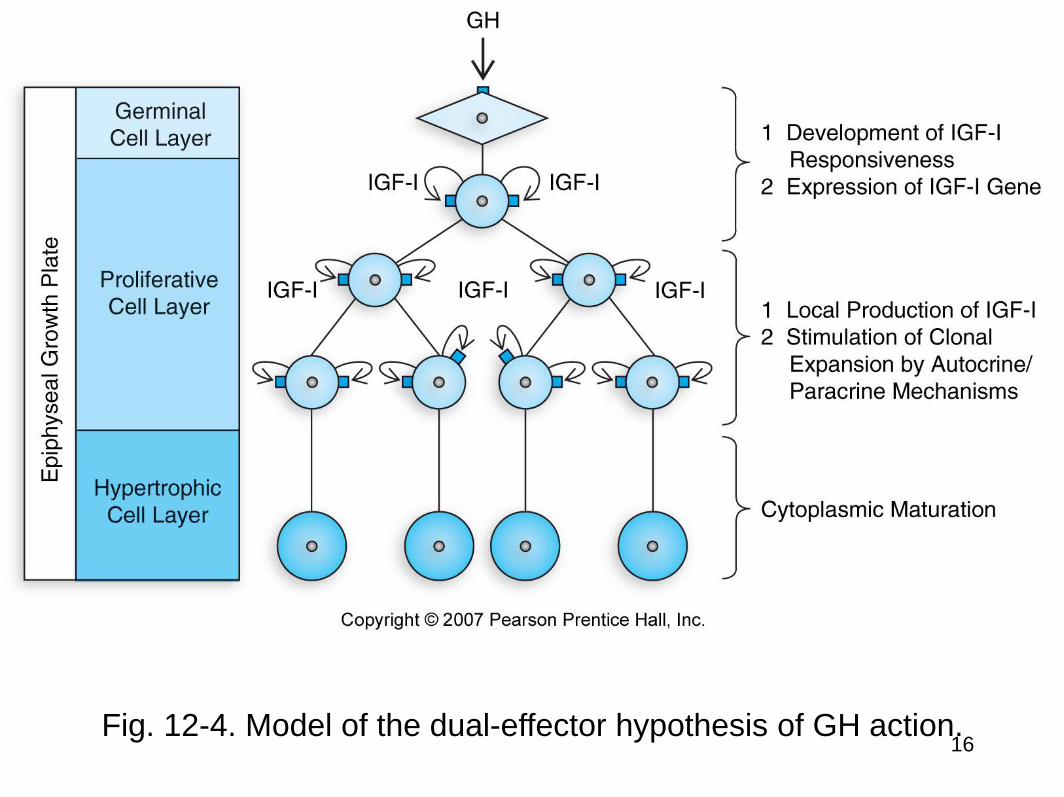
Fig. 12-4. Model of the dual-effector hypothesis of GH action. 16
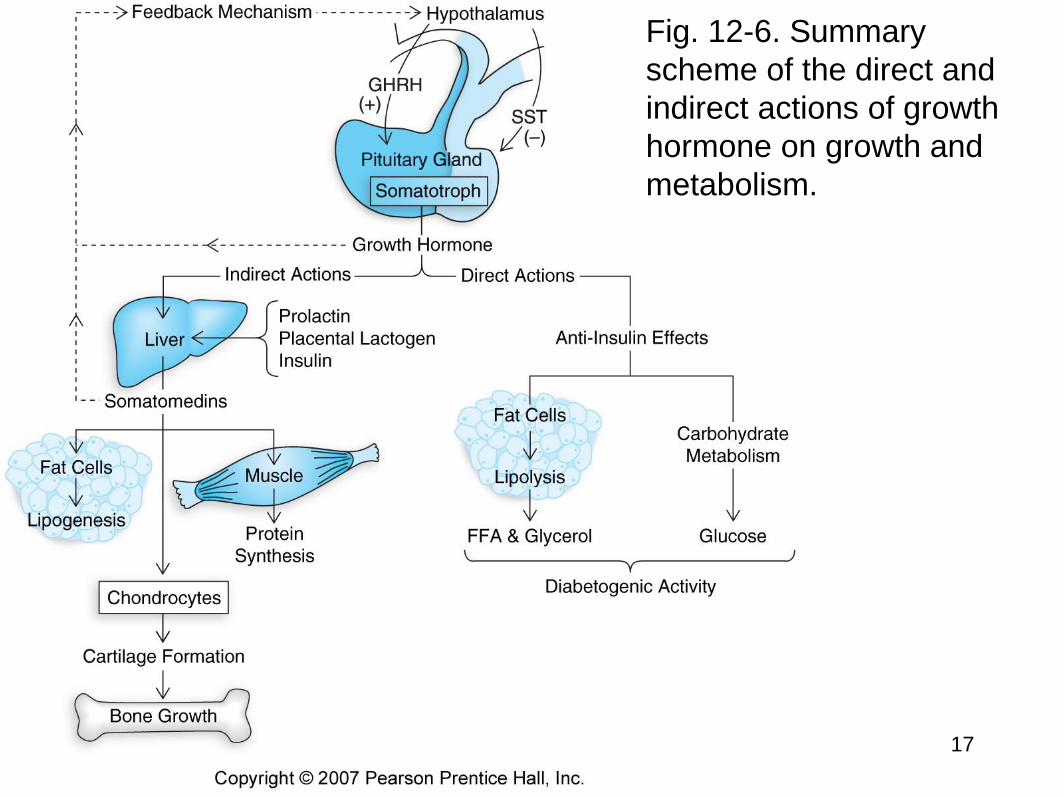
Fig. 12-6. Summary
scheme of the direct and
indirect actions of growth
hormone on growth and
metabolism.
17

Targeting IGF-1R Pathway in Cancer
• 키 클수록 소득 높다
• 키 클수록 암 발생 위험도 함께 커진다.
• 남성: 5cm 커질수록 5%씩 증가
• 여성: 5cm 커질수록 7%씩 증가
• 베르그만(Bergmann) 법칙: 항온동물의 경우 같은 종이라도 추운 곳에 사는 것이 더운 곳에 사는 것보다 몸집이 더 크다는 법칙. 더운 곳에서는 몸의 열을 발산해야 하지만 추운 곳에서는 체온 유지를 위해 몸 표면적을 줄여 열 손실을 막아야 한다. 몸의 길이가 두배가 되면 표면적은 4배(22)로, 부피는 8배(23)로 늘어난다. 몸집이 커지면서 부피에 대한 표면적의 비율이 줄어드는 것이다. 사람도 북유럽인이 남유럽인 보다 더 크다.
• AMGEN Oncology - 2009
18
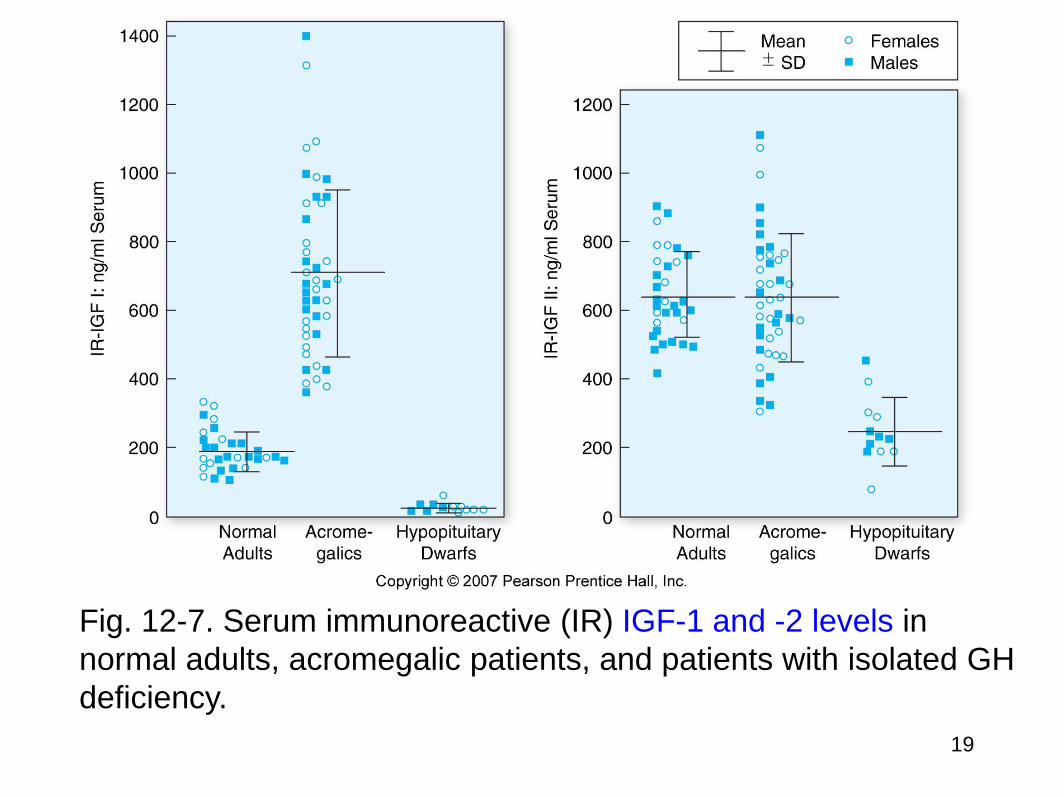
Fig. 12-7. Serum immunoreactive (IR) IGF-1 and -2 levels in
normal adults, acromegalic patients, and patients with isolated GH
deficiency.
19
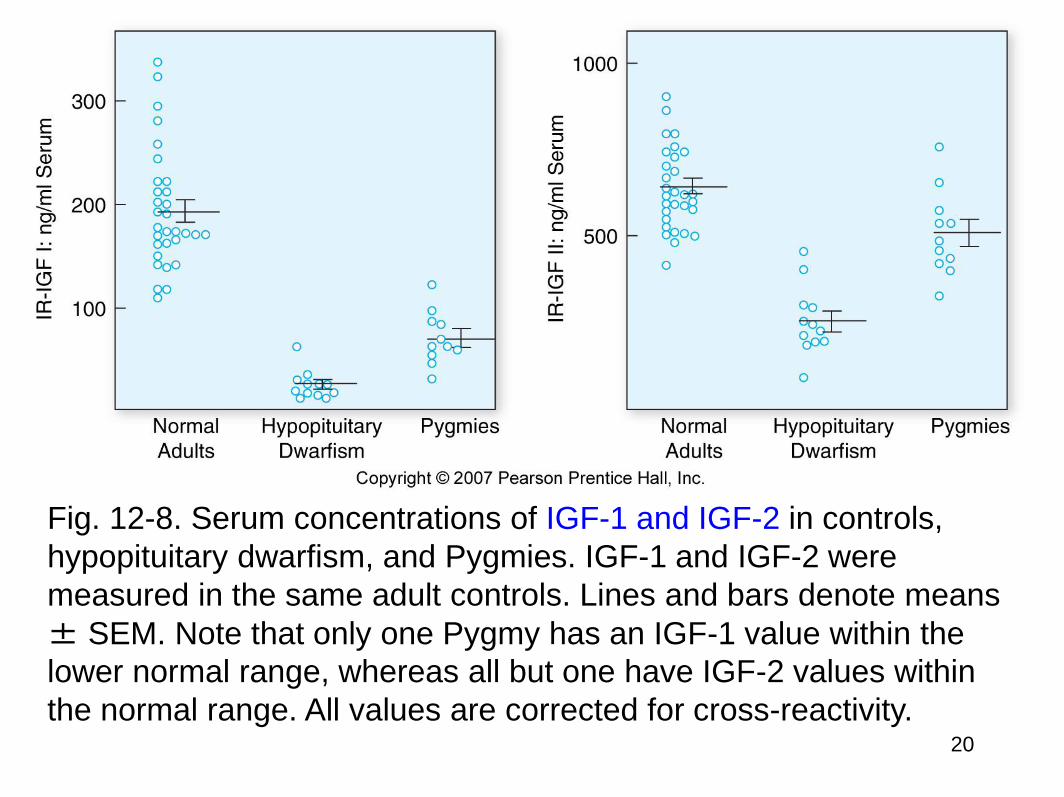
Fig. 12-8. Serum concentrations of IGF-1 and IGF-2 in controls,
hypopituitary dwarfism, and Pygmies. IGF-1 and IGF-2 were
measured in the same adult controls. Lines and bars denote means
± SEM. Note that only one Pygmy has an IGF-1 value within the
lower normal range, whereas all but one have IGF-2 values within
the normal range. All values are corrected for cross-reactivity. 20
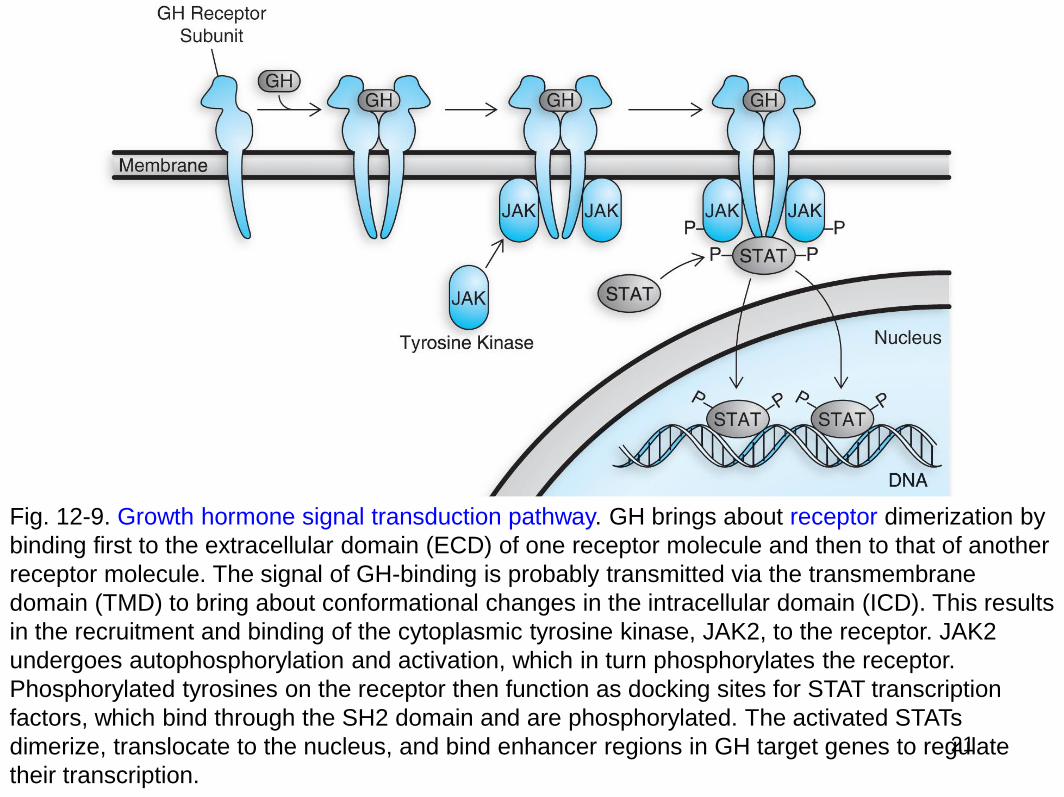
Fig. 12-9. Growth hormone signal transduction pathway. GH brings about receptor dimerization by
binding first to the extracellular domain (ECD) of one receptor molecule and then to that of another
receptor molecule. The signal of GH-binding is probably transmitted via the transmembrane
domain (TMD) to bring about conformational changes in the intracellular domain (ICD). This results
in the recruitment and binding of the cytoplasmic tyrosine kinase, JAK2, to the receptor. JAK2
undergoes autophosphorylation and activation, which in turn phosphorylates the receptor.
Phosphorylated tyrosines on the receptor then function as docking sites for STAT transcription
factors, which bind through the SH2 domain and are phosphorylated. The activated STATs
dimerize, translocate to the nucleus, and bind enhancer regions in GH target genes to regulate
their transcription.
21

Laron syndrome
• Laron-type dwarfism, is
an autosomal recessive
disorder characterized by
an insensitivity to growth
hormone (GH), caused by
a variant of the growth
hormone receptor.
• Defect in the GH receptor
• It causes short stature and
a resistance to diabetes
and cancer.
22
23
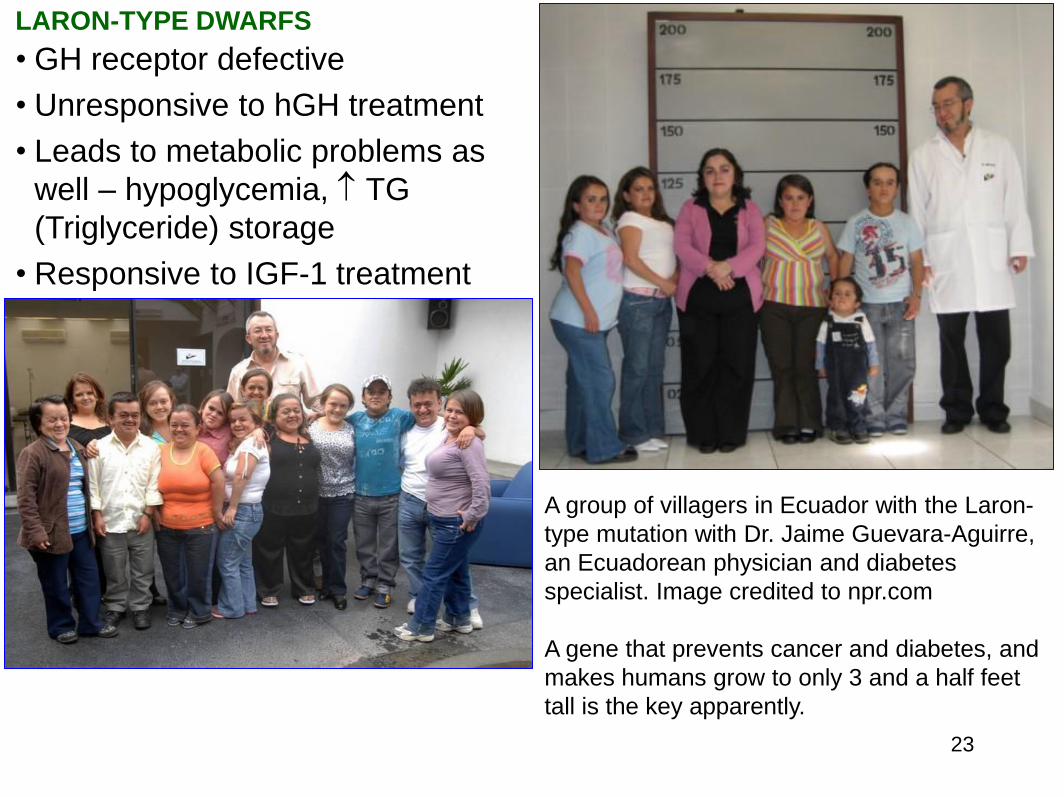
LARON-TYPE DWARFS
• GH receptor defective
• Unresponsive to hGH treatment
• Leads to metabolic problems as
well – hypoglycemia, TG
(Triglyceride) storage
• Responsive to IGF-1 treatment
A group of villagers in Ecuador with the Laron-
type mutation with Dr. Jaime Guevara-Aguirre,
an Ecuadorean physician and diabetes
specialist. Image credited to npr.com
A gene that prevents cancer and diabetes, and
makes humans grow to only 3 and a half feet
tall is the key apparently.

AFRICAN PYGMIES
• Normal GH and IGF-I binding
• Defect is post-receptor
• Tissue resistance to IGF-1 leads to short stature
24
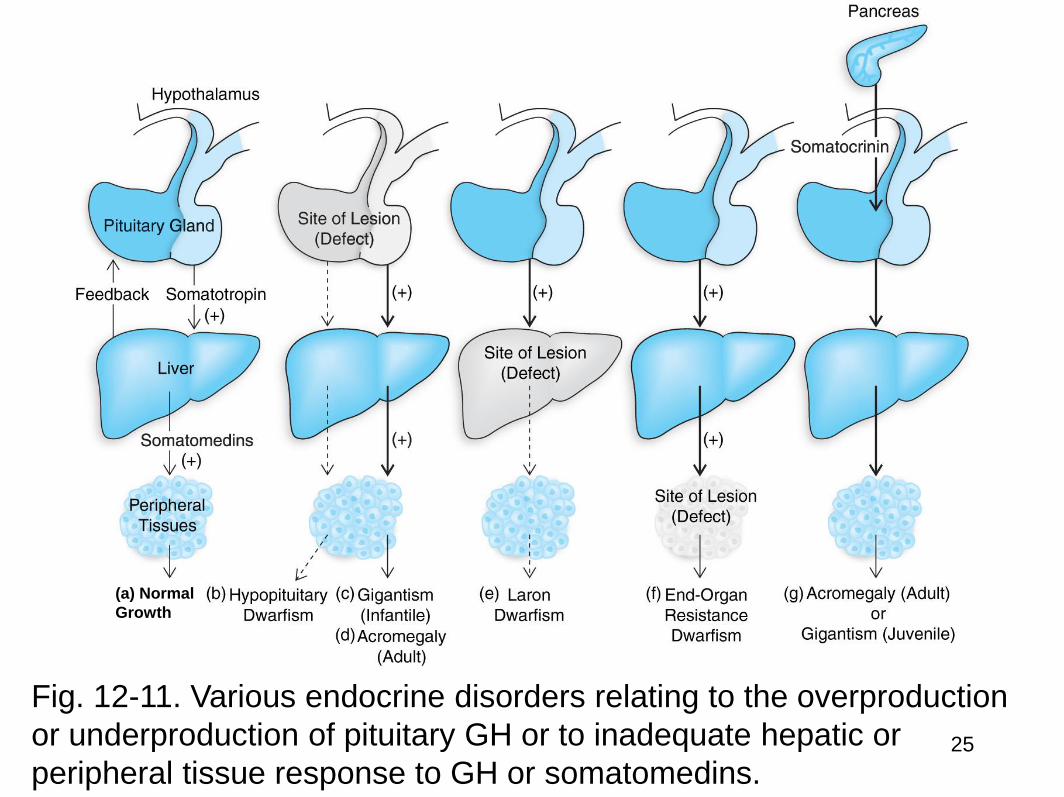
(a) Normal
Growth
Fig. 12-11. Various endocrine disorders relating to the overproduction
or underproduction of pituitary GH or to inadequate hepatic or
peripheral tissue response to GH or somatomedins. 25
3. Other Hormones for Growth
• Other hormones besides growth hormone are essential for normal growth
– Thyroid hormone
• Growth severely stunted in hypothyroid children
• Hypersecretion does not cause excessive growth
– Insulin
• Deficiency often blocks growth
• Hyperinsulinism often spurs excessive growth
– Androgens
• Play role in pubertal growth spurt, stimulate protein synthesis in many organs
• Effects depend on presence of GH
– Estrogens
• Effects of estrogen on growth prior to bone maturation are not well understood poorly
26
4. Growth Hormone Abnormalities • Growth hormone deficiency
– Due to pituitary defect or hypothalamic dysfunction
– Hyposecretion of GH in child is one cause of dwarfism
– Deficiency in adults produces relatively few symptoms
• Growth hormone excess
– Most often caused by tumor of GH-producing cells of anterior
pituitary
– Symptoms depend on age of individual when abnormal
secretion begins
• Gigantism
– Caused by overproduction of GH in childhood before epiphyseal
plates close
• Acromegaly
– Occurs when GH hypersecretion occurs after adolescence
27
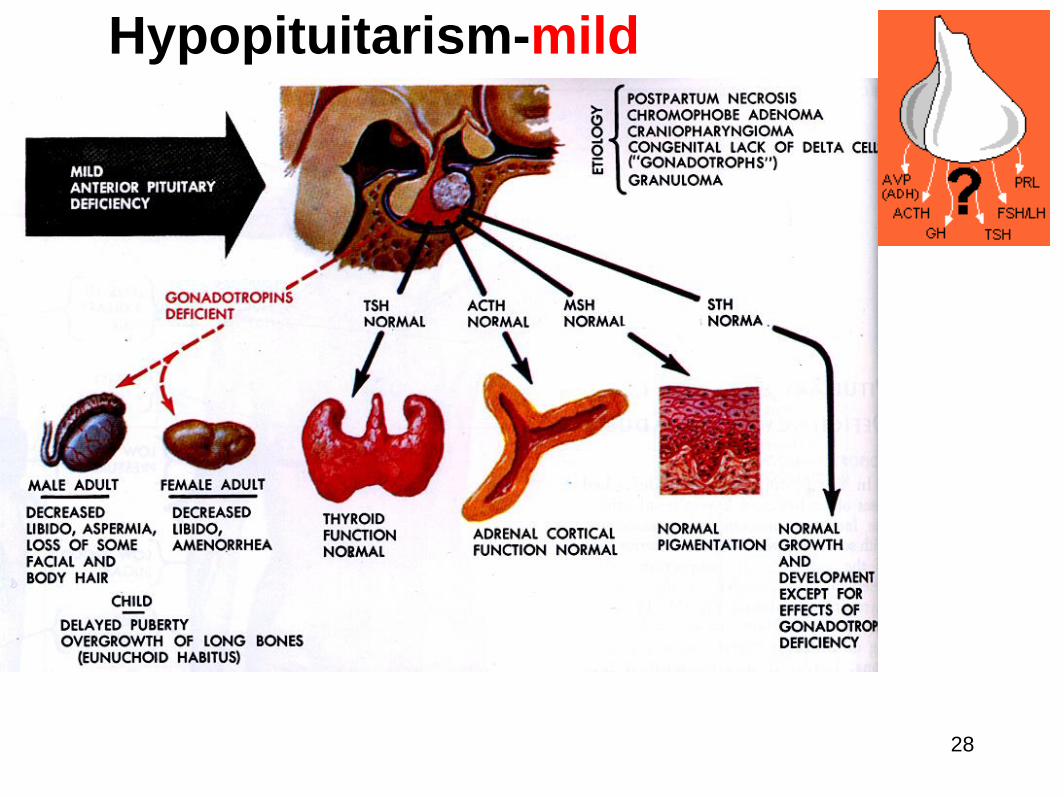
Hypopituitarism-mild
28
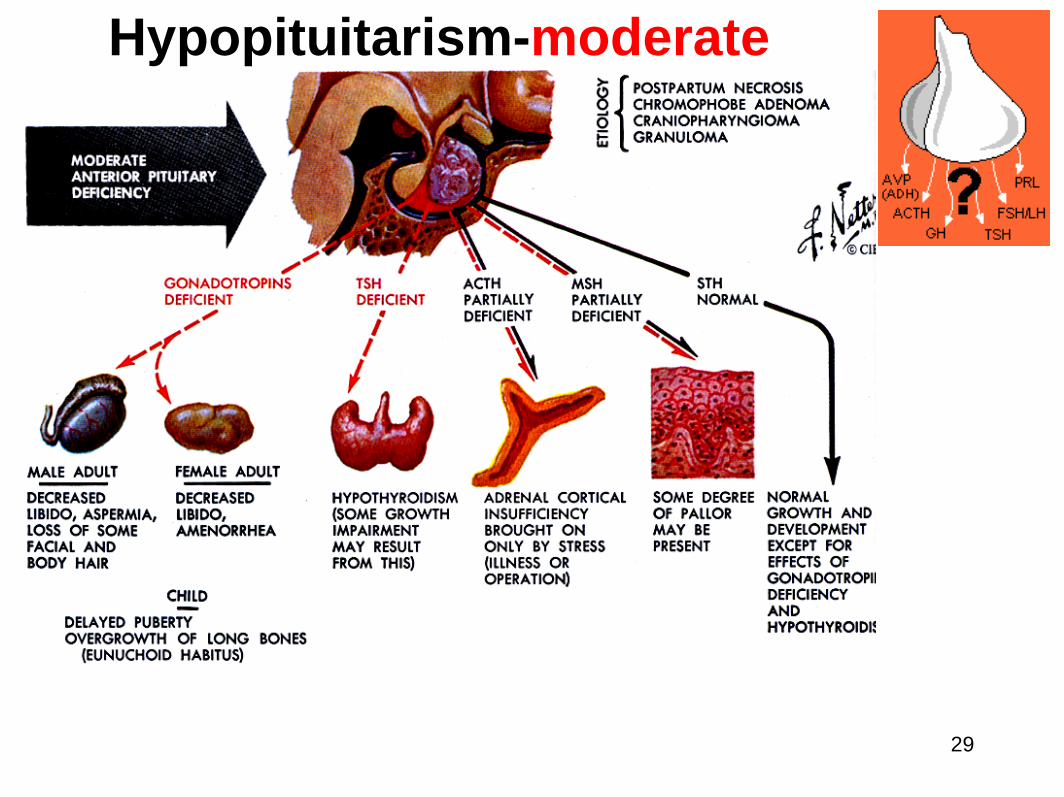
Hypopituitarism-moderate
29
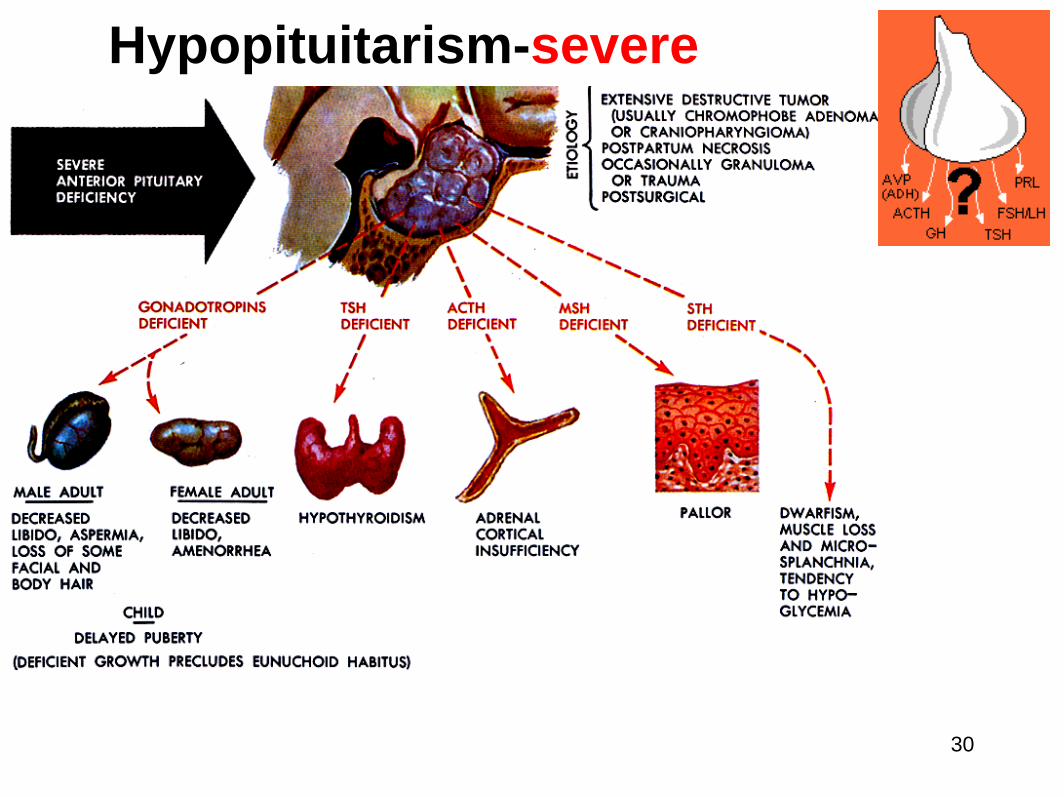
Hypopituitarism-severe
30

Hypopituitarism-panhypopituitarism
31
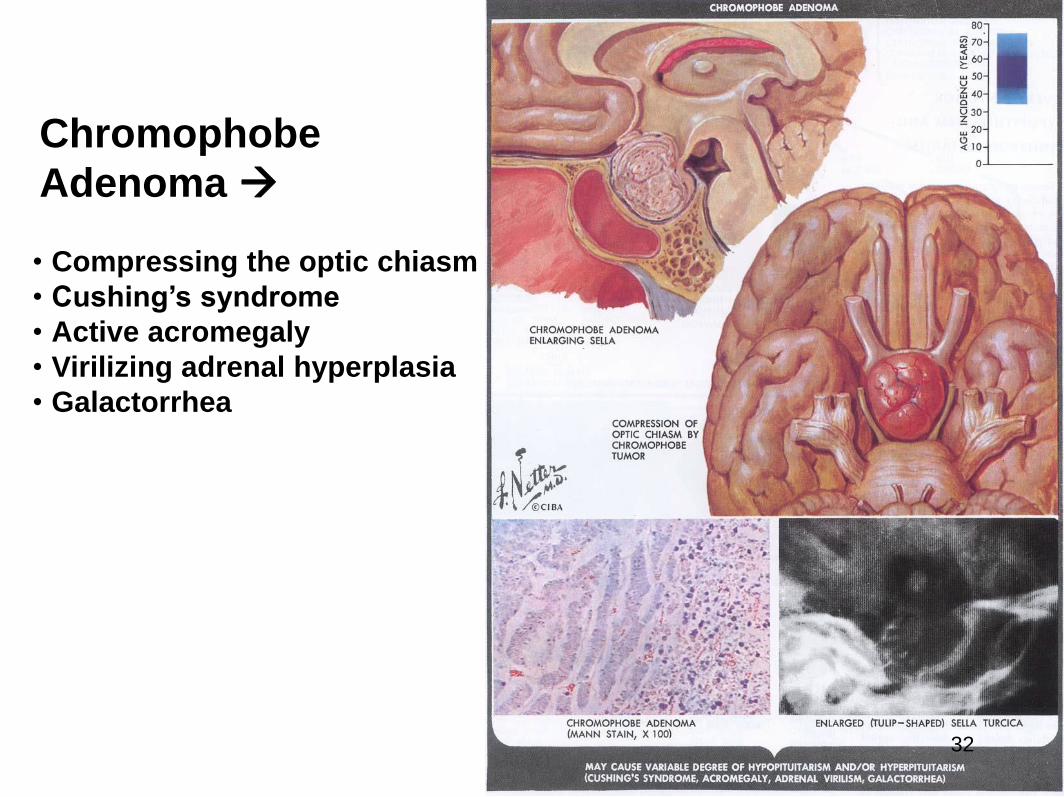
Chromophobe
Adenoma
• Compressing the optic chiasm
• Cushing’s syndrome
• Active acromegaly
• Virilizing adrenal hyperplasia
• Galactorrhea
32
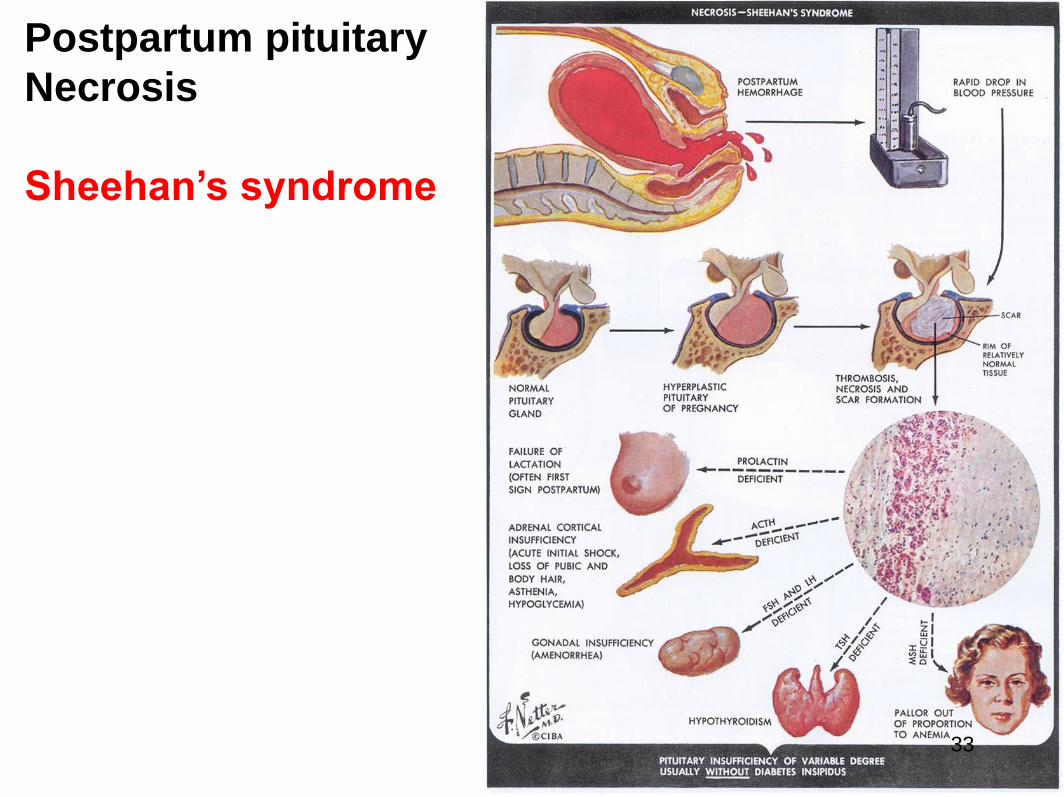
Postpartum pituitary
Necrosis
Sheehan’s syndrome
33
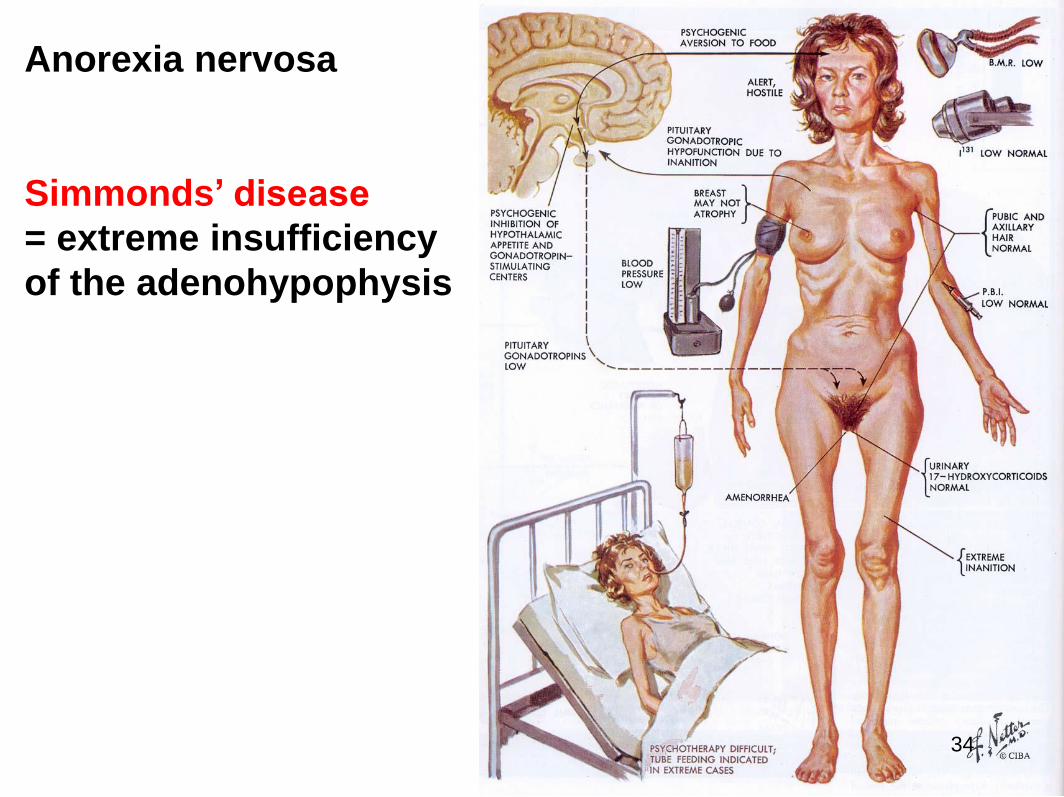
Anorexia nervosa
Simmonds’ disease
= extreme insufficiency
of the adenohypophysis
34
Dwarfism • Targets of GH therapy: 20%
• 10~15% of dwarfism is effective
on GH therapy
35
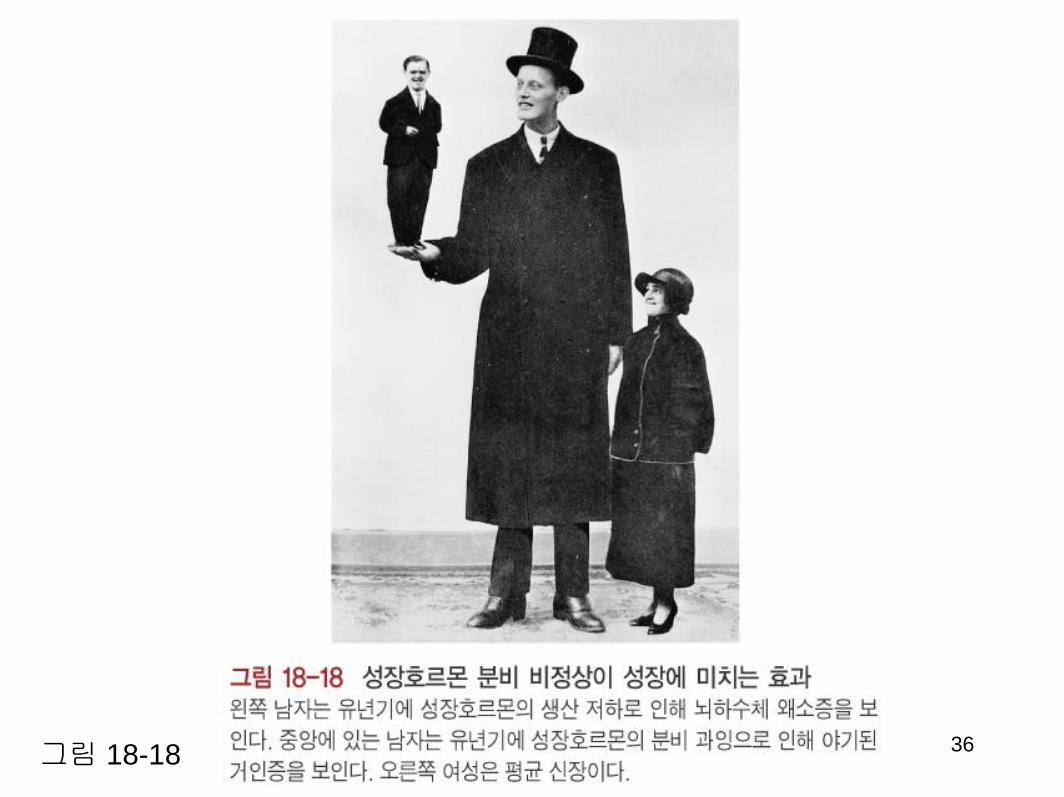
그림 18-18 36

Hyperpituitrism
GH secreted in excess causing acromegaly, gigantism
PRL secreted in excess causing galactorrhea
ACTH secreted in excess causing Cushing's syndrome
TSH secreted in excess causing hyperthyroidism
37
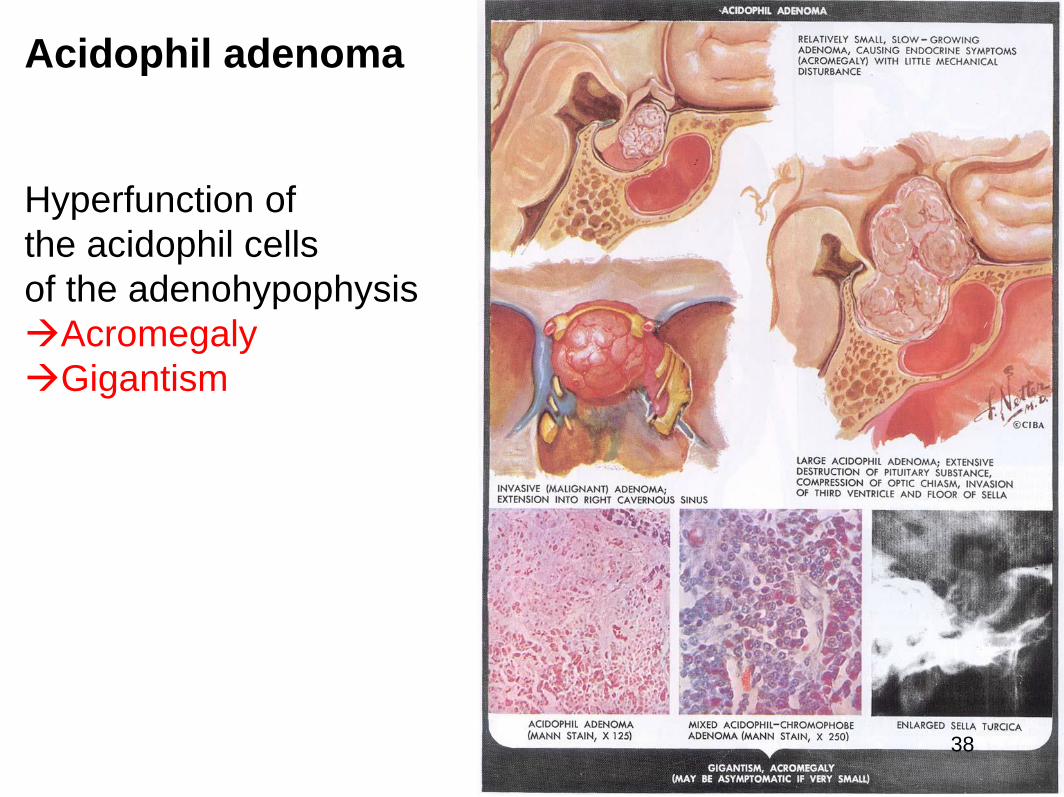
Acidophil adenoma
Hyperfunction of
the acidophil cells
of the adenohypophysis
Acromegaly
Gigantism
38

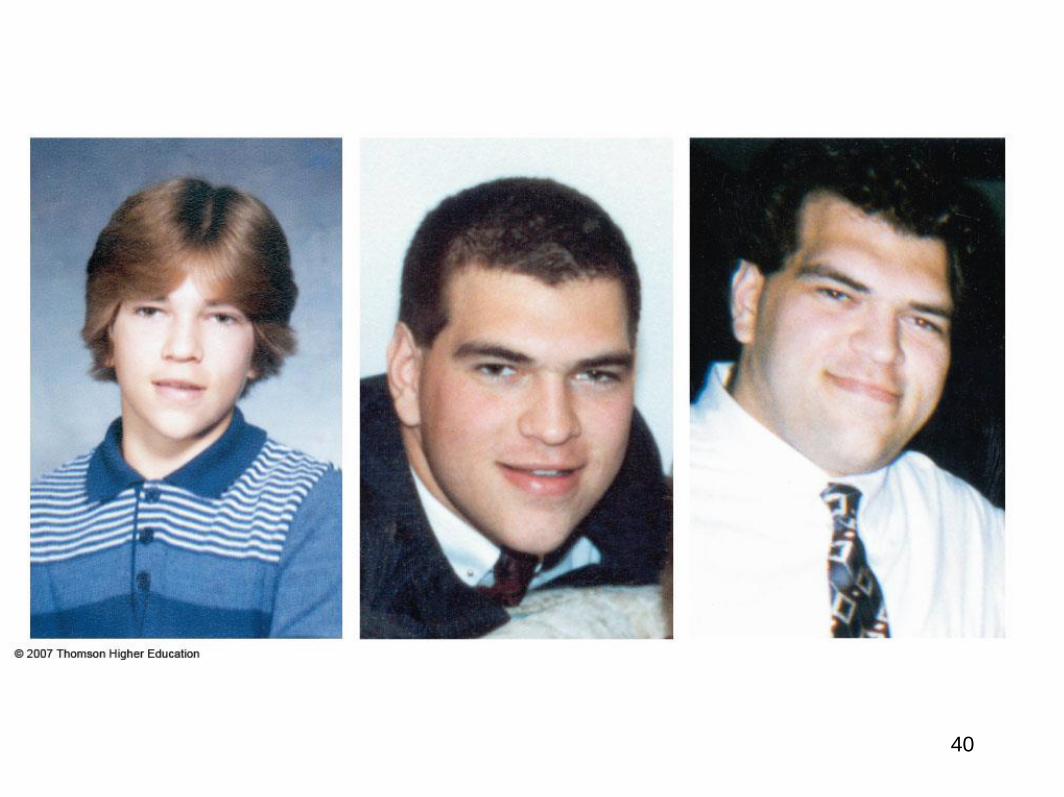
Acromegaly
Typical symptoms of acromegaly
• coarsening of facial features
• enlarged hands and feet
• thickening of the soft tissue in the
palms and soles of the feet
• carpal tunnel syndrome (tingling
feeling or pains in the hands)
• excessive sweating and oily skin
• headaches
• vision disturbance
• sleep apnoea
• general tiredness
• (amenorrhoea) - adult females
• impotence - adult males
• reduced fertility
39
40
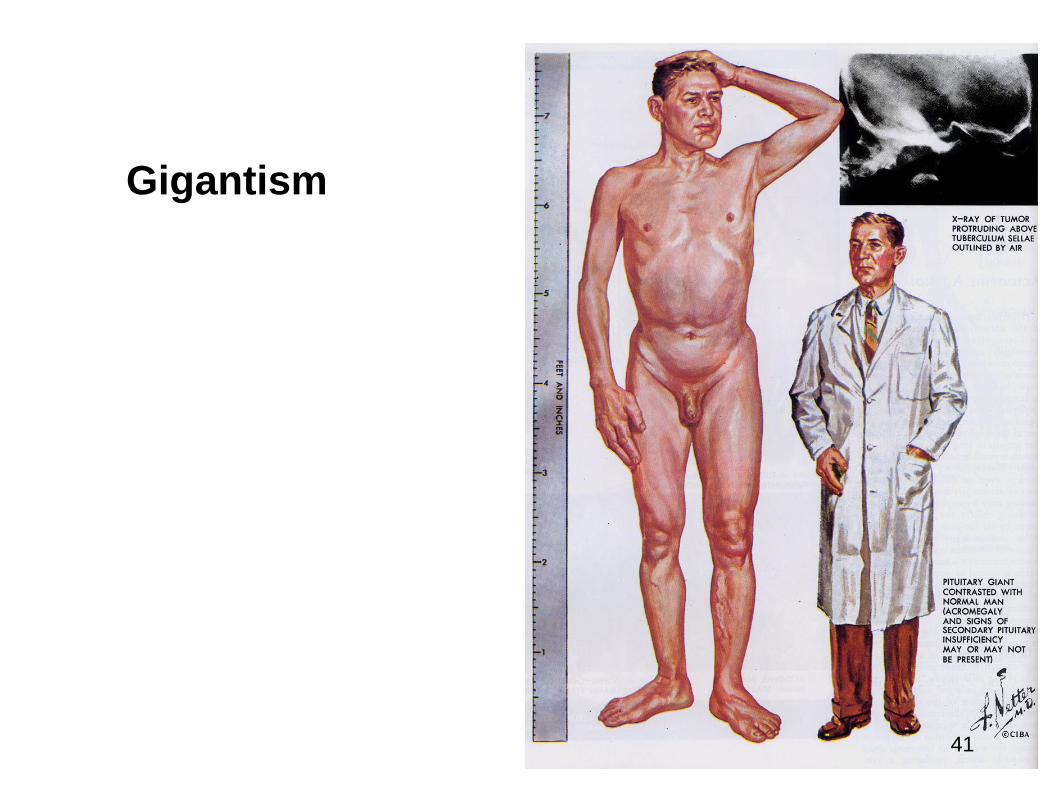
Gigantism
41
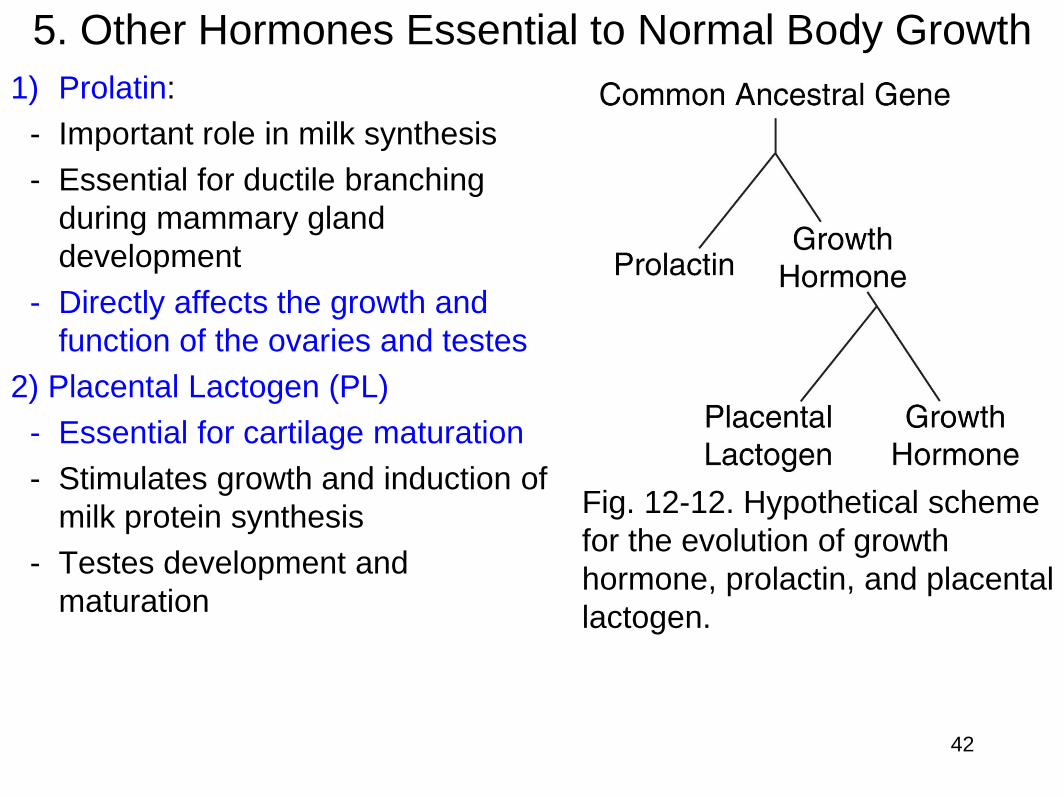
Fig. 12-12. Hypothetical scheme
for the evolution of growth
hormone, prolactin, and placental
lactogen.
5. Other Hormones Essential to Normal Body Growth
1) Prolatin:
- Important role in milk synthesis
- Essential for ductile branching
during mammary gland
development
- Directly affects the growth and
function of the ovaries and testes
2) Placental Lactogen (PL)
- Essential for cartilage maturation
- Stimulates growth and induction of
milk protein synthesis
- Testes development and
maturation
42
3) Neurotropic growth factors
• Several peptide growth factors regulate the differentiation and
growth of both CNS and PNS.
• Nerve growth factor (NGF) promotes survival of peripheral
sympathetic and spinal neurons during development.
- NGF is one member of a family of neurotropins.
- NGF is a small secreted protein that is important for the growth,
maintenance, and survival of certain target neurons (nerve cells).
- It also functions as a signaling molecule.
- Other members of the neurotrophin family that are well
recognized include Brain-Derived Neurotrophic Factor (BDNF),
Neurotrophin-3 (NT-3), and Neurotrophin 4/5 (NT-4/5).
43
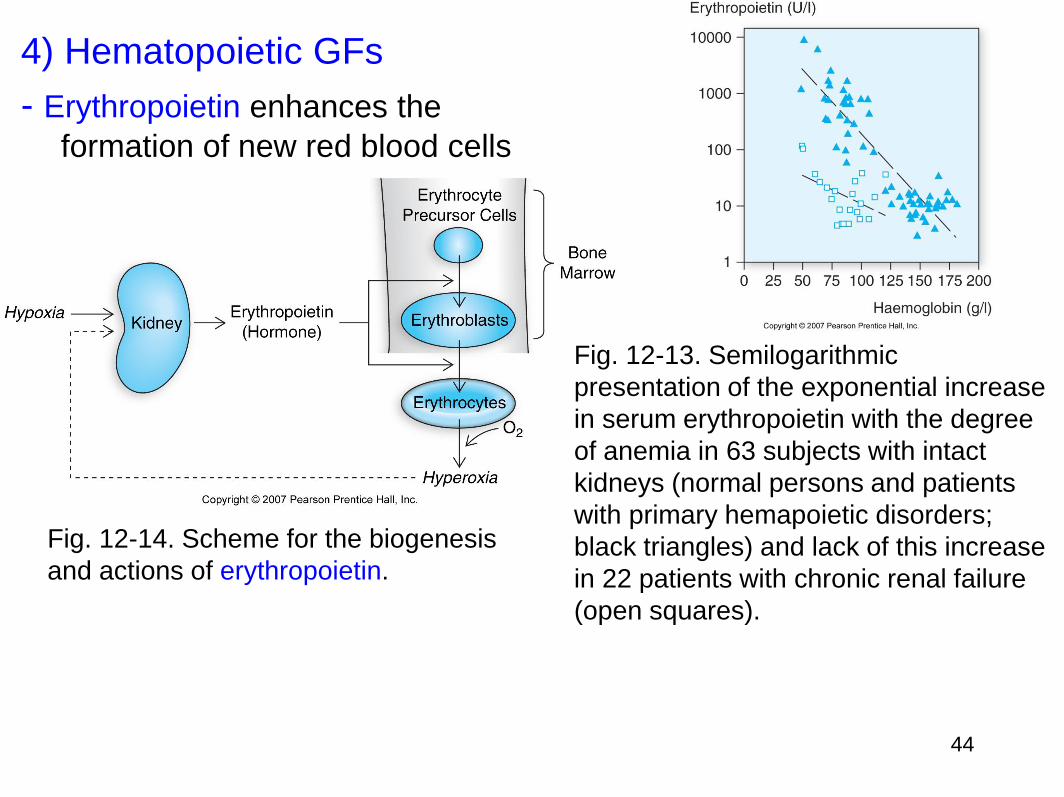
4) Hematopoietic GFs
- Erythropoietin enhances the
formation of new red blood cells
Fig. 12-14. Scheme for the biogenesis
and actions of erythropoietin.
44
Fig. 12-13. Semilogarithmic
presentation of the exponential increase
in serum erythropoietin with the degree
of anemia in 63 subjects with intact
kidneys (normal persons and patients
with primary hemapoietic disorders;
black triangles) and lack of this increase
in 22 patients with chronic renal failure
(open squares).

Fig. 12-17. Primary structure of bovine thymosin 1.
5) Thymic hormones stimulate maturation of T lymphocytes
• Thymosins are small proteins present in many animal tissues.
• They are named thymosins because they were originally isolated
from the thymus, but most are now known to be present in many
other tissues.
• Thymosins have diverse biological activities, and two in particular,
thymosins α1 and β4, have potentially important uses in medicine,
some of which have already progressed from the laboratory to the
clinic.
• In relation to diseases, thymosins have been categorized as
biological response modifiers.
45

Fig. 12-18. Primary structure of bovine thymosin 4. Residues
31–43 are aligned with residues 18–30 to indicate regions of
internal duplication.
46
6) Platelet-derived growth factor (PDGF) acts locally on injured
blood vessels.
• Platelet-derived growth factor (PDGF) is one of the numerous growth
factors, or proteins that regulate cell growth and division.
• In particular, it plays a significant role in blood vessel formation
(angiogenesis), the growth of blood vessels from already-existing blood
vessel tissue. Uncontrolled angiogenesis is a characteristic of cancer.
• In chemical terms, platelet-derived growth factor is dimeric glycoprotein
composed of two A (PDGF-AA) or two B (PDGF-BB) chains or a
combination of the two (PDGF-AB).
• PDGF is a potent mitogen for cells of mesenchymal origin, including
smooth muscle cells and glial cells.
• In both mouse and human, the PDGF signaling network consists of four
ligands, PDGFA-D, and two receptors, PDGFR-α and PDGFR-β.
• All PDGFs function as secreted, disulphide-linked homodimers, but only
PDGFA and B can form functional heterodimers.
47
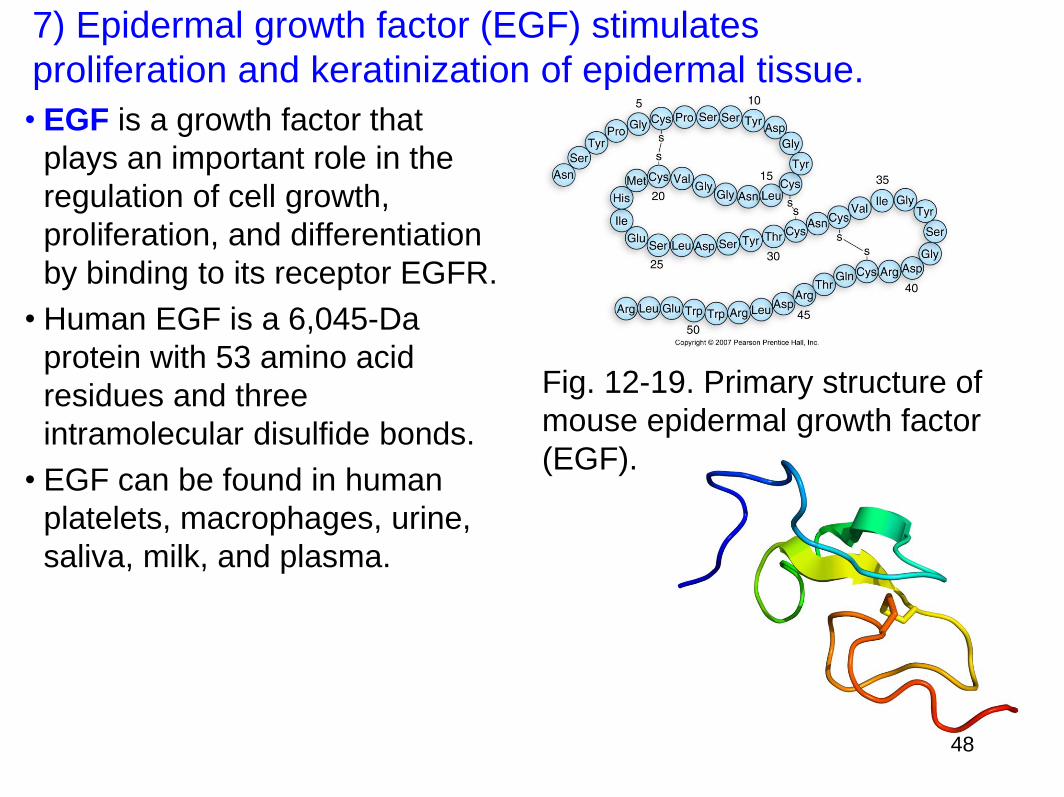
7) Epidermal growth factor (EGF) stimulates
proliferation and keratinization of epidermal tissue.
• EGF is a growth factor that
plays an important role in the
regulation of cell growth,
proliferation, and differentiation
by binding to its receptor EGFR.
• Human EGF is a 6,045-Da
protein with 53 amino acid
residues and three
intramolecular disulfide bonds.
• EGF can be found in human
platelets, macrophages, urine,
saliva, milk, and plasma.
Fig. 12-19. Primary structure of
mouse epidermal growth factor
(EGF).
48
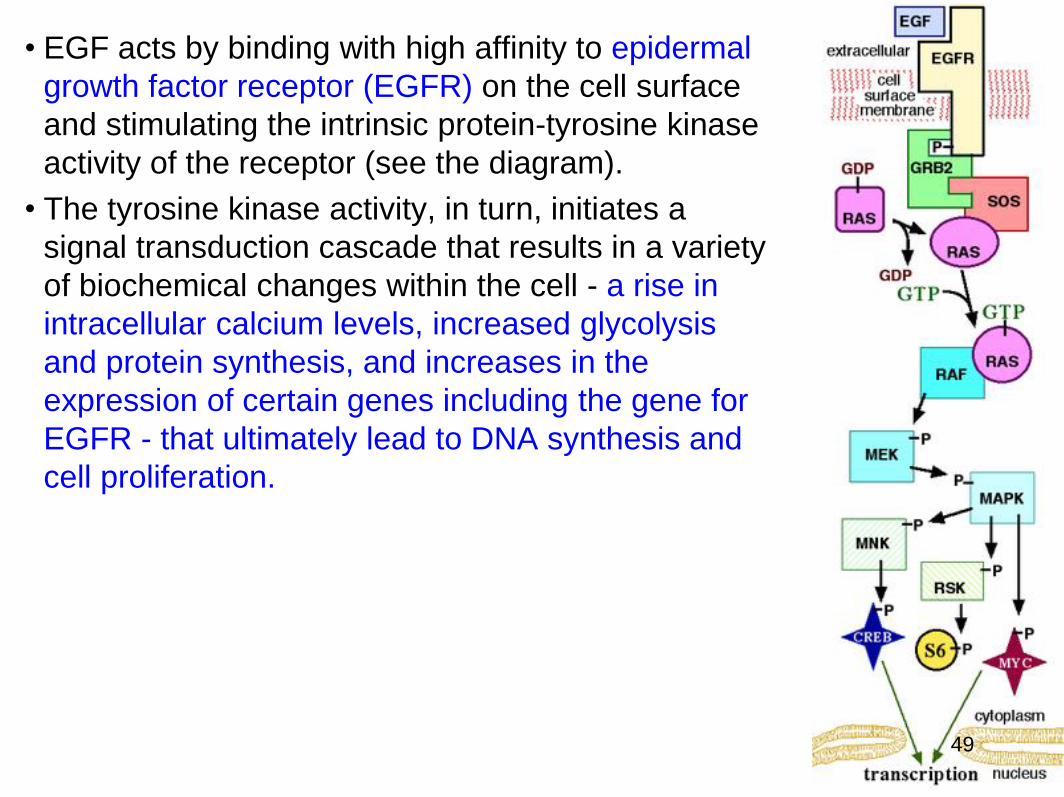
• EGF acts by binding with high affinity to epidermal
growth factor receptor (EGFR) on the cell surface
and stimulating the intrinsic protein-tyrosine kinase
activity of the receptor (see the diagram).
• The tyrosine kinase activity, in turn, initiates a
signal transduction cascade that results in a variety
of biochemical changes within the cell - a rise in
intracellular calcium levels, increased glycolysis
and protein synthesis, and increases in the
expression of certain genes including the gene for
EGFR - that ultimately lead to DNA synthesis and
cell proliferation.
49

• EGF is the founding member of the EGF-
family of proteins.
• Members of this protein family have
highly similar structural and functional
characteristics.
• Besides EGF itself other family
members include:
- Heparin-binding EGF-like growth factor
(HB-EGF)
- transforming growth factor-α (TGF-α)
- Amphiregulin (AR)
- Epiregulin (EPR)
- Epigen
- Betacellulin (BTC)
- neuregulin-1 (NRG1)
- neuregulin-2 (NRG2)
- neuregulin-3 (NRG3)
- neuregulin-4 (NRG4).
• All family members contain one or
more repeats of the conserved amino
acid sequence:
• CX7CX4-5CX10-13CXCX8GXRC
• Where X represents any amino acid.
• This sequence contains 6 cysteine
residues that form three intramolecular
disulfide bonds.
• Disulfide bond formation generates
three structural loops that are essential
for high-affinity binding between
members of the EGF-family and their
cell-surface receptors.
50
• EGF therapy:
• Because of the increased risk of cancer by EGF, inhibiting it
decreases cancer risk.
• Such medications are so far mainly based on inhibiting the EGF
receptor. Monoclonal antibodies are potential substances for this
purpose.
• Gefitinib (INN) (trade name Iressa) is a drug used in the treatment
of certain types of cancer.
• Gefitinib is an EGFR inhibitor, like erlotinib, which interrupts
signaling through the epidermal growth factor receptor in target
cells.
• It is marketed by AstraZeneca and Teva.
51

8) Fibroblast Growth Factors
• Fibroblast growth factors, or FGFs, are a family of
growth factors involved in angiogenesis, wound healing,
and embryonic development.
• The FGFs are heparin-binding proteins and interactions
with cell-surface associated heparan sulfate
proteoglycans have been shown to be essential for FGF
signal transduction.
• FGFs are key players in the processes of proliferation
and differentiation of wide variety of cells and tissues.
52

FGF Family • In humans, 22 members of the FGF family have been identified, all of
which are structurally related signaling molecules:
• Members FGF1 through FGF10 all bind fibroblast growth factor receptors
(FGFRs). FGF1 is also known as acidic, and FGF2 is also known as basic
fibroblast growth factor.
• Members FGF11, FGF12, FGF13, and FGF14, also known as FGF
homologous factors 1-4 (FHF1-FHF4), have been shown to have distinct
functional differences compared to the FGFs. Although these factors
possess remarkably similar sequence homology, they do not bind FGFRs
and are involved in intracellular processes unrelated to the FGFs. This
group is also known as "iFGF”.
• Members FGF16 through FGF23 are newer and not as well characterized.
FGF15 is the mouse ortholog of human FGF19 (hence there is no human
FGF15).
• Human FGF20 was identified based on its homology to Xenopus FGF-20
(XFGF-20).
• In contrast to the local activity of the other FGFs, FGF15/FGF19, FGF21
and FGF23 have more systemic effects. 53
9) Transforming Growth Factors
• Transforming growth factor (sometimes referred to as
Tumor growth factor, or TGF) is used to describe two
classes of polypeptide growth factors, TGFα and TGFβ.
• The name "Transforming Growth Factor" is somewhat
arbitrary, since the two classes of TGFs are not structurally
or genetically related to one another, and they act through
different receptor mechanisms.
• Furthermore, they do not always induce cellular
transformation, and are not the only growth factors that
induce cellular transformation.
54
Types of TGF
TGFα is upregulated in some human cancers. It is
produced in macrophages, brain cells, and keratinocytes,
and induces epithelial development.
TGFβ exists in three known subtypes in humans, TGFβ1,
TGFβ2, and TGFβ3.
- These are upregulated in Marfan's syndrome and some
human cancers, and play crucial roles in tissue
regeneration, cell differentiation, embryonic development,
and regulation of the immune system.
- Isoforms of transforming growth factor-beta (TGF-β1) are
also thought to be involved in the pathogenesis of pre-
eclampsia.
- TGFβ receptors are single pass serine/threonine kinase
receptors.
55
Function of TGF
• These proteins were originally characterized by their
capacity to induce oncogenic transformation in a
specific cell culture system, rat kidney fibroblasts.
• Application of the transforming growth factors to
normal rat kidney fibroblasts induces the cultured cells
to proliferate and overgrow, no longer subject to the
normal inhibition caused by contact between cells.
56