change in corneal microstructure with rigid gas permeable contact lens use following collagen...
TRANSCRIPT

Change in corneal microstructure with rigid gaspermeable contact lens use following collagencross-linking: an in vivo confocal microscopy studySri V Sehra, Jeewan S Titiyal, Namrata Sharma, Radhika Tandon, Rajesh Sinha
Dr Rajendra Prasad Centre forOphthalmic Sciences, All IndiaInstitute of Medical Sciences,New Delhi, India
Correspondence toProfessor Jeewan S Titiyal,Cornea and Refractive Surgeryservices, Dr. Rajendra PrasadCentre for OphthalmicSciences, All India Institute ofMedical Sciences, AnsariNagar, New Delhi 110026,India; [email protected]
Received 29 June 2013Revised 12 November 2013Accepted 1 December 2013Published Online First24 December 2013
To cite: Sehra SV, Titiyal JS,Sharma N, et al. Br JOphthalmol 2014;98:442–447.
ABSTRACTAim To study corneal microstructural changes withuse of rigid gas permeable contact lenses (CLs) inkeratoconus patients following collagen cross-linking(CXL).Methods In a prospective, non-randomised,comparative case series, keratoconus patients withdocumented progression were offered CXL (365 nm,3 mW/cm2, 30 min with 0.1% riboflavin). Patients whorefused CXL were fitted with CL and followed up for6 months (keratoconus (KL)-CL; 25 eyes). Patients whounderwent CXL were either fitted with CL 3 months afterthe procedure (CXL-CL; 26 eyes) or followed up withonly spectacle correction (CXL-SL; 21 eyes). Outcomemeasures of over-refraction and corneal microstructure(confocal microscopy) were evaluated at time of CXL and1, 2, 3, 4, 6 and 9 months after CXL.Results There was a myopic shift in over-refraction by0.37 D in CXL-CL (p=0.00), and 16/26 eyes requiredprescription of spectacles over CL to provide optimumvision; change in over-refraction was not seen in KC-CL.Patients using CL (CXL-CL and KC-CL) showed evidenceof epithelial cell stress with increase in the superficialepithelial cell size and decrease in basal epithelial celldensity. They also had a decrease in corneal sub-basalnerve plexus (CSNP) density and branching. Patientsusing spectacles after CXL showed regeneration of thesub-basal nerve plexus. Stromal keratocyte regenerationwas unaffected with CL use.Conclusions CL use after CXL is associated with adelay in the regeneration of the CSNP and epithelialcell stress.
INTRODUCTIONCorneal collagen cross-linking (CXL) with riboflavinfor keratoconus was introduced by Wollensak et al1
in 2003. This is a promising modality which helps tostabilise disease progression and improve uncorrectedvisual acuity.1–3 Studies have reported a post-CXLregression in keratometry by 0.9–2.3 D over afollow-up of 3–90 months.1–7 Confocal microscopystudies have demonstrated apoptosis of keratocytes inthe anterior stroma and absence of the corneal sub-basal nerve plexus (CSNP) following CXL. This isfollowed by a gradual keratocyte repopulation andsubsequent regeneration of the CSNP.8–10
Most patients require optical correction afterCXL; rigid gas permeable contact lenses (CLs) arecommonly used for this purpose. It is not known ifuse of CL affects microstructural recovery of thecornea after CXL. In this comparative study, weevaluated changes in the corneal microstructure
using in vivo confocal microscopy in patients fittedwith CL after CXL.
MATERIALS AND METHODSWe conducted a prospective non-randomised com-parative study between May 2010 and January 2012at Dr. Rajendra Prasad Centre for OphthalmicSciences, All India Institute of Medical Sciences,New Delhi, India. The study was started afterethical clearance from the Institutional EthicsCommittee.
Study populationPatients with stage II or higher keratoconus(Amsler–Krumeich classification11) and documentedprogression with decrease in corrected distancevisual acuity were recruited. All patients were16 years or older and none of them had a history ofCL use. Written informed consent was taken fromall patients. Patients with corneal thickness <400microns or those with the presence of centralcorneal scar, history of herpetic eye disease, severedry eye, corneal infection, history of autoimmunedisease and prior corneal surgery were excluded.After apprising patients of the benefits and sideeffects, CXL was offered to all recruited patients.Patients who refused the procedure were fitted withCL (Rose K, Menicon, Nagoya, Japan) and followedup as the keratoconus (KL)-CL group. A standardcross-linking procedure was performed in the rest.
CXL procedureCXL was performed under topical anaesthesia with0.5% proparacaine hydrochloride administeredtwice 15 min before the procedure. A lid speculumwas inserted, followed by removal of the centralcorneal epithelium (7 mm diameter) using a bluntspatula. Commercially available isotonic riboflavin(0.1% riboflavin with 20% dextran; Medio-Cross,Italy) eye drops were administered every 5 min forhalf an hour. The UV device (UV-X, IROC, Zurich,Switzerland) was used to deliver ultraviolet A lightof 365 nm wavelength and 3 mW/cm2 irradiance viaa 9 mm aperture, at a distance of 5 cm from theapex of the cornea, for 30 min. After irradiation,the eye was rinsed with a sterile saline solution, onedrop of moxifloxacin hydrochloride (0.5%;Vigamox, Alcon Laboratories, Fort Worth, Texas,USA) was applied, and a bandage soft CL(PureVision; Bausch & Lomb, Rochester, New York,USA) was inserted and retained for 4 days.After cross-linking, patients were advised not to
use CL for 3 months. After 3 months, patients wereoffered the option of CL (Rose K). Patients who
442 Sehra SV, et al. Br J Ophthalmol 2014;98:442–447. doi:10.1136/bjophthalmol-2013-303934
Clinical science
group.bmj.com on October 5, 2014 - Published by bjo.bmj.comDownloaded from

underwent CL fitting were recruited into the CXL-CL group;patients who refused to be fitted with CL and were using specta-cles were recruited into the spectacle correction (CXL-SL) group.
EvaluationKC-CL group was evaluated at baseline and at 1, 3 and 6 monthsafter CLs were fitted. Patients who underwent CXL were evalu-ated before the procedure and then at monthly intervals till4 months, at 6 months and 9 months. Patients were asked to dis-continue CL on the night before the scheduled examination visit.A detailed ophthalmological examination including visual assess-ment, cycloplegic refraction, over-refraction, slit-lamp biomicro-scopy, basal Schirmer test, Goldmann tonometry and a dilatedfundus examination were performed at all follow-up visits. Studyvariables included over-refraction and corneal confocal micros-copy (Confoscan 4.0, NIDEK, Gamagori, Japan).
Confoscan 4.0 equipped with an Achroplan non-applanating40× immersion objective lens (Zeiss, Oberkochen, Germany) wasused. Each examination was performed according to a standardprocedure;12 before the examination, a drop of topical anaesthetic0.5% proparacaine hydrochloride (Paracaine; Sunways India,Mumbai, India) was instilled in the lower conjunctival fornix ofeach eye. One drop of polyacrylic gel (GenTeal Gel, NovartisFarma, Varese, Italy) was then applied onto the objective tip toserve as an immersion fluid. The patient was positioned in thechin and forehead rest, and when a stromal image appeared on themonitor of the confocal microscope, the recording button waspressed. Several scans of the entire depth of the central corneawere automatically taken. Illumination intensity was kept constantfor all cases. The standard dimension of each image produced was340×255 μm (area 0.132 mm2), with an optical section thicknessof 5.5 μm. The last clear and centred frame of the superficial epi-thelium was chosen. The manual micrometer in the software pro-vided with the instrument was used to measure individual cellsizes. Superficial epithelial cell size was calculated by averaging thecell sizes of 10 randomly selected cells.13 Basal epithelial celldensity was calculated by manually counting the cells in the basalepithelium in a region of fixed area (0.01 mm2). Cells overlappingwith the boundary box were counted only in the superior and leftside.14–16 The CSNP nerve fibre and nerve branch density werecalculated in the best-focused image.13 Anterior 10%, intermediate33%–66% and the posterior 10% of the corneal stroma weredetermined using the z-line in the instrument; the anterior, inter-mediate and posterior stromal keratocyte nuclei count was calcu-lated using the manual counter in the software provided. Nuclei in
Table 1 Mean over-refraction in CXL-CL group and KC-CL groupat the time of fitting contact lenses and at follow-up visits
Over-refraction (D) CXL-CL (n=26) KC-CL (n=25) p Value
At time of fitting CL 0.08±0.18 0.07±0.18 0.691 month after CL −0.07±0.31 0.07±0.19 0.043 months after CL −0.27±0.46 0.06±0.33 0.016 months after CL −0.28±0.47 0.10±0.38 0.01p Value 0.02 0.95
CL, rigid gas permeable contact lenses.
Figure 1 Change in superficialepithelial cell size with follow-up.(A) Comparison of epithelial cell size inCXL-CL and CXL-SL after collagencross-linking and fitting of contactlenses in CXL-CL; (B) Change inepithelial cell size after fitting contactlenses in CXL-CL and KC-CL. p*, t testbetween CXL-CL and CXL-SL. p#,repeated measures analysis of variancewithin a group.
Sehra SV, et al. Br J Ophthalmol 2014;98:442–447. doi:10.1136/bjophthalmol-2013-303934 443
Clinical science
group.bmj.com on October 5, 2014 - Published by bjo.bmj.comDownloaded from
two images in each region of interest were counted and theaverage of the two readings was taken.13–16
Statistical analysisQuantitative data were expressed as a mean±SD and qualitativedata expressed as a percentage. For parametric data, one-wayanalysis of variance (ANOVA) was used to compare inter-groupmeans and Bonferroni correction was used to analyse post-testresults. Kruskal–Wallis test was used for inter-group comparisonfor non-parametric data and Mann–Whitney U test was used forpost-test analysis. Longitudinal analysis within a group over thefollow-up period was done using repeated measures ANOVAand pair-wise post-test comparison was done with Bonferronicorrection for parametric data; non-parametric data were ana-lysed using the Freidman test and Wilcoxon matched pairs test.The level of statistical significance was set at p<0.05.
RESULTSIn all, 26 eyes of 18 patients were recruited in the CXL-CLgroup, 21 eyes of 18 patients were recruited in the CXL-SLgroup and 25 eyes of 16 patients were recruited in the KC-CLgroup.
The mean age of patients in CXL-CL, CXL-SL and KC-CL was19.88±3.75 years (range 16–26), 22.95±5.05 years (range 16–29) and 20.92±4.48 years (range 16–33), respectively; the groupswere comparable in their age distributions (p=0.07). Each grouphad three patients (six eyes) who were below 18 years of age. Thegroups were also comparable in their sex distribution: CXL-CLhad 15 male (57.7%) and 11 female (42.3%) eyes; CXL-SL had
12 male (57.1%) and nine female (42.9%) eyes; KC-CL had 15male (60%) and 10 female (40%) eyes.
CL parameters and over-refractionCL parameters were comparable in the groups fitted with CL.The mean base curve was 6.63±0.51 mm in CXL-CL and 6.69±0.69 mm in KC-CL (p=0.73), mean overall diameter was8.86±0.16 mm in CXL-CL and 8.89±0.24 mm in KC-CL(p=0.06) and mean power was −8.12±4.25 D in CXL-CL and−6.62±4.76 D in KC-CL (p=0.10).
Over-refraction was comparable between CXL-CL andKC-CL at the time of fitting CL; 6 months after fitting CL, thetwo groups had significantly different over-refraction values(table 1). There was a myopic shift in over-refraction inCXL-CL from 0.08±0.18 D to −0.28±0.47 D over 6 months(p=0.02) which was not seen in KC-CL. Sixteen eyes had to beprescribed spectacles lenses to be worn over CL to provideoptimum vision. CLs were well tolerated by all patients andthere were no drop-outs.
Intraocular pressureThe pre-CXL procedure mean intraocular pressure was 10.21±2.53 mm Hg in CXL-CL and 10.82±2.77 mm Hg in CXL-SL(p=0.43). After CXL, an increase in intraocular pressure wasnoted in both groups; however, this increase over pre-CXLvalues was not significant. Further, no significant difference wasnoted between CXL-CL and CXL-SL at any time. At the lastfollow-up visit, the intraocular pressure was 11.24±3.22 mm Hgin CXL-CL and 11.56±3.42 mm Hg in CXL-SL (p=0.74).
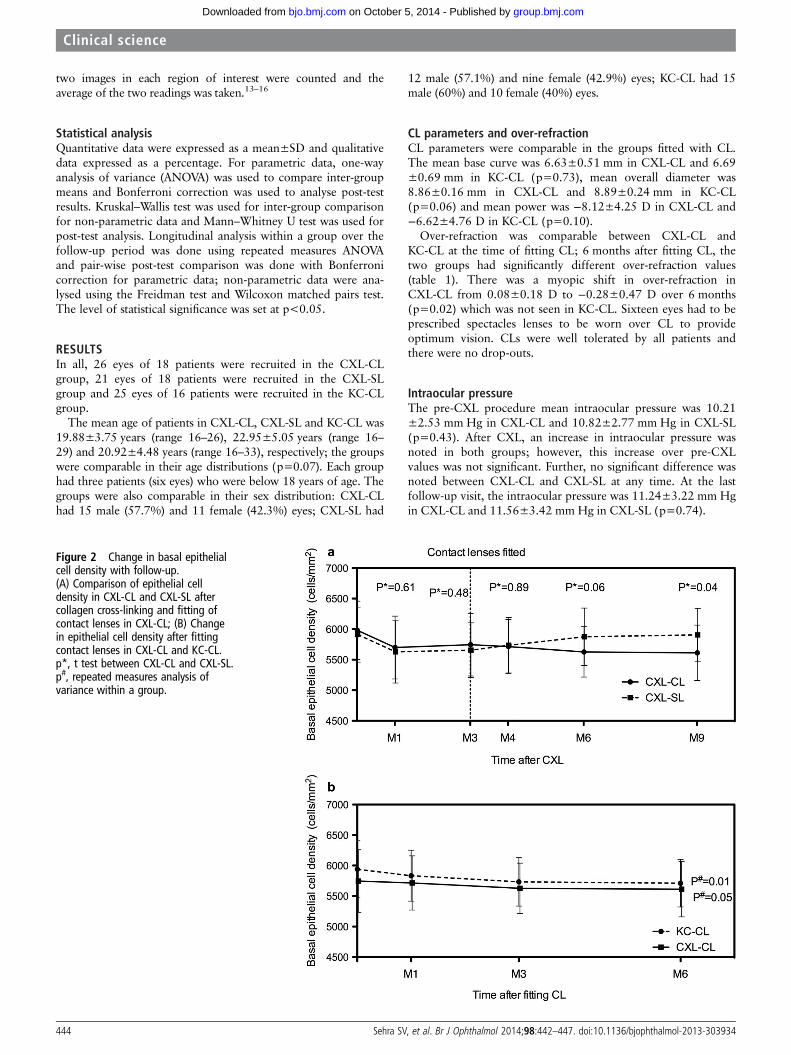
Figure 2 Change in basal epithelialcell density with follow-up.(A) Comparison of epithelial celldensity in CXL-CL and CXL-SL aftercollagen cross-linking and fitting ofcontact lenses in CXL-CL; (B) Changein epithelial cell density after fittingcontact lenses in CXL-CL and KC-CL.p*, t test between CXL-CL and CXL-SL.p#, repeated measures analysis ofvariance within a group.
444 Sehra SV, et al. Br J Ophthalmol 2014;98:442–447. doi:10.1136/bjophthalmol-2013-303934
Clinical science
group.bmj.com on October 5, 2014 - Published by bjo.bmj.comDownloaded from

Confocal microscopyAn increase in superficial epithelial cell size was noted 1 monthafter CXL and 3 months after CXL, the epithelial cell sizedecreased in both groups. Decrease in cell size continued inCXL-SL over the 9-month follow-up period while in CXL-CLthe superficial epithelial cell size increased after CLs were fitted(figure 1A). The mean cell size between CXL-CL and CXL-SLwas significantly different 1 month after fitting CL (p=0.02)and the difference increased over follow-up. A significantincrease in superficial epithelial cell size was also seen in KC-CL(figure 1B). Basal epithelial cell density decreased after CXL(figure 2A). Recovery of basal epithelial cell density was haltedafter CLs were fitted in CXL-CL. Cell density also decreased inKC-CL (figure 2B). The CSNP nerve fibre branching anddensity decreased 1 month after CXL to undetectable levels andthen recovered by 3 months (figure 3A and figure4A, respect-ively). Nerve fibre regeneration was halted after CLs were fittedin CXL-CL. CSNP nerve fibre branching and density alsodecreased in KC-CL (figures 3B and 4B, respectively).
Keratocyte nuclei count in the anterior corneal stromadecreased significantly 1 month after CXL followed by gradualrepopulation over 3 and 6 months. Use of CL did not alter theregeneration of the keratocytes; there was no significant differ-ence between CXL-CL and CXL-SL at any follow-up.Significant change in anterior stromal keratocyte nuclei countwas also not seen in KC-CL (p=0.65). The intermediate andposterior stromal keratocyte nuclei counts did not show signifi-cant change in any group.
DISCUSSIONCXL is a promising modality to halt the progression of kerato-conus, The optical correction after CXL may be in the form ofspectacles or CL fitting.17–19 In studies which have evaluatedresults of CXL, some authors have excluded patients usingCL,6 20–22 others have discontinued CL wear 2–4 weeks priorto follow-up visits,5 23–25 and some authors have discontinuedCL the night before the follow-up visit.26 Koppen et al27 hadevaluated the influence of CL use post-CXL on corneal topog-raphy, while no study has evaluated confocal changes with CLuse after CXL. In our comparative study, we prospectively evalu-ated changes in over-refraction and corneal microstructure usingconfocal microscopy in eyes that had been fitted with CL3 months after CXL. We compared these changes with patientsusing CL who had not undergone CXL and patients who werenot using CL after CXL.
There was a significant myopic shift in over-refraction by 0.37D over 6 months in eyes fitted with CL post-CXL (p=0.02),which was not seen in eyes that had not undergone CXL.Sixteen eyes had a drop in visual acuity because of this change;they had to be prescribed spectacles lenses to be worn over CLto provide optimum vision. This myopic change in over-refraction may be attributed to progressive keratometric flatten-ing that is seen after CXL. This is a significant finding andpatients need to be counselled in this regard.
On examination of the corneal microstructure, a normalcorneal healing process was seen after CXL in eyes that werenot using CL (figure 5). Mazzotta et al8 9 first studied long term
Figure 3 Change in CSNP nerve fibredensity with follow-up. (A) Comparisonof nerve fibre density in CXL-CL andCXL-SL after collagen cross-linking andfitting of contact lenses in CXL-CL;(B) Change in nerve fibre density afterfitting contact lenses in CXL-CL andKC-CL. p*, t test between CXL-CL andCXL-SL. p#, repeated measures analysisof variance within a group. CSNP,corneal sub-basal nerve plexus.
Sehra SV, et al. Br J Ophthalmol 2014;98:442–447. doi:10.1136/bjophthalmol-2013-303934 445
Clinical science
group.bmj.com on October 5, 2014 - Published by bjo.bmj.comDownloaded from
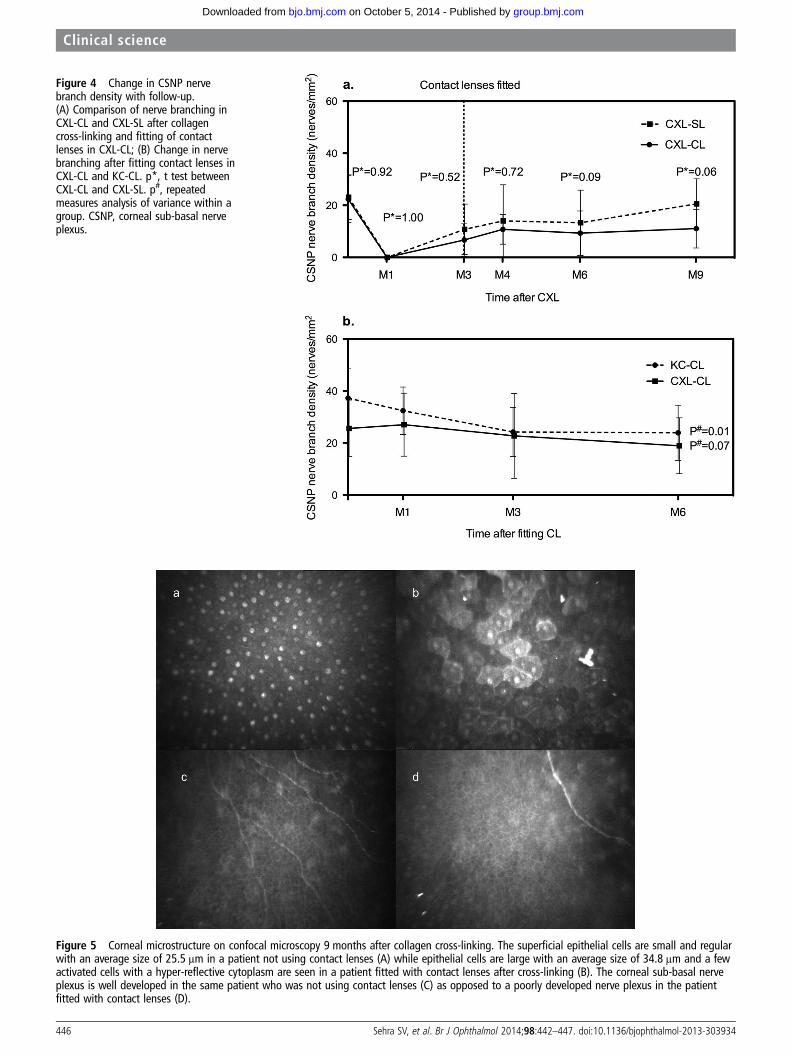
Figure 4 Change in CSNP nervebranch density with follow-up.(A) Comparison of nerve branching inCXL-CL and CXL-SL after collagencross-linking and fitting of contactlenses in CXL-CL; (B) Change in nervebranching after fitting contact lenses inCXL-CL and KC-CL. p*, t test betweenCXL-CL and CXL-SL. p#, repeatedmeasures analysis of variance within agroup. CSNP, corneal sub-basal nerveplexus.
Figure 5 Corneal microstructure on confocal microscopy 9 months after collagen cross-linking. The superficial epithelial cells are small and regularwith an average size of 25.5 μm in a patient not using contact lenses (A) while epithelial cells are large with an average size of 34.8 μm and a fewactivated cells with a hyper-reflective cytoplasm are seen in a patient fitted with contact lenses after cross-linking (B). The corneal sub-basal nerveplexus is well developed in the same patient who was not using contact lenses (C) as opposed to a poorly developed nerve plexus in the patientfitted with contact lenses (D).
446 Sehra SV, et al. Br J Ophthalmol 2014;98:442–447. doi:10.1136/bjophthalmol-2013-303934
Clinical science
group.bmj.com on October 5, 2014 - Published by bjo.bmj.comDownloaded from

confocal microscopy changes post-CXL. They have qualitativelydocumented regeneration of corneal sub-basal nerves followedby establishment of the normal CSNP anatomy and a gradualkeratocyte repopulation over follow-up.
We found that in patients fitted with CL after CXL, there wasa halting and reversal of CSNP regeneration (figure 5). Therewas also an increase in the superficial epithelial cell size anddecrease in the basal epithelium cell density; however, thestroma was unaffected. Similar changes in the epithelium andCSNP were also noted in eyes fitted with CL that had notundergone CXL.
Lema et al28 have demonstrated that CL use is associated withincreased levels of inflammatory cytokines on the ocular surface.Inflammation may lead to epithelial cell stress, increase in cellsize, decrease in cell density and may alter the CSNP architecture.This hypothesis is further supported by similar corneal micro-morphological changes, which have been observed secondary toocular surface inflammation in patients with vernal keratocon-junctivitis.13 Another reason for these changes could beCL-induced epithelial hypoxia. It is difficult to comment on thesignificance of these changes as we were unable to demonstrate ifthey were reversible. Our patients were dependent on CL andwere not willing to discontinue them for prolonged periods.
A limitation in our study was that we started fitting CL atleast 3 months post-CXL, while previous authors have fitted CLas soon as the epithelial defect heals, as early as 1 week afterCXL.27 Given the fact that CLs are affecting corneal healingprocess after CXL, the ideal time for fitting CL post-CXLremains uncertain.
Silicone hydrogel mini-scleral CLs are an existing alternativeoption to rigid gas permeable CLs for optical correction afterCXL. Severinsky et al29 had evaluated visual, refractive andtopographical outcomes after fitting silicone hydrogelmini-scleral CL post-CXL. Overall, 90% of their study groupwas successfully fitted with lenses and the mean Snellen visualacuity was 6/9. Further research could be directed towardsevaluating confocal microscopy changes in these patients; thiswould help to determine the optimal means of optical correc-tion after CXL.
To the best of our knowledge, this is the first study that hascomparatively evaluated corneal microstructure changes with invivo confocal microscopy in keratoconus patients fitted with CLafter CXL. We found that CL use is associated with significantchanges in CSNP regeneration and leads to epithelial stress.
Contributors All authors contributed towards planning, data collection, analysisand reporting the work in this study.
Competing interests None.
Ethics approval All India Institute of Medical Sciences Ethics Committee.
Patient consent Written informed consent was taken before enrolment.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking
for the treatment of keratoconus. Am J Ophthalmol 2003;135:620–7.2 Raiskup-Wolf F, Hoyer A, Spoerl E, et al. Collagen crosslinking with riboflavin and
ultraviolet-A light in keratoconus: long-term results. J Cataract Refract Surg2008;34:796–801.
3 Grewal DS, Brar GS, Jain R, et al. Corneal collagen crosslinking using riboflavin andultraviolet-A light for keratoconus: one-year analysis using Scheimpflug imaging.J Cataract Refract Surg 2009;35:425–32.
4 Hoyer A, Raiskup-Wolf F, Spörl E, et al. Collagen cross-linking with riboflavin andUVA light in keratoconus. Results from Dresden. Ophthalmologe 2009;106:133–40.
5 Vinciguerra P, Albè E, Trazza S, et al. Intraoperative and postoperative effects ofcorneal collagen cross-linking on progressive keratoconus. Arch Ophthalmol2009;127:1258–65.
6 Caporossi A, Mazzotta C, Baiocchi S, et al. Long-term results of riboflavinultraviolet a corneal collagen cross-linking for keratoconus in Italy: the Siena eyecross study. Am J Ophthalmol 2010;149:585–93.
7 Goldich Y, Marcovich AL, Barkana Y, et al. Clinical and corneal biomechanicalchanges after collagen cross-linking with riboflavin and UV irradiation in patientswith progressive keratoconus: results after 2 years of follow-up. Cornea2012;31:609–14.
8 Mazzotta C, Balestrazzi A, Traversi C, et al. Treatment of progressive keratoconus byriboflavin-UVA-induced cross-linking of corneal collagen: ultrastructural analysis byHeidelberg Retinal Tomograph II in vivo confocal microscopy in humans. Cornea2007;26:390–7.
9 Mazzotta C, Traversi C, Baiocchi S, et al. Corneal healing after riboflavinultraviolet-A collagen cross-linking determined by confocal laser scanningmicroscopy in vivo: early and late modifications. Am J Ophthalmol2008;146:527–33.
10 Kymionis GD, Diakonis VF, Kalyvianaki M, et al. One-year follow-up of cornealconfocal microscopy after corneal cross-linking in patients with post laser in situkeratosmileusis ectasia and keratoconus. Am J Ophthalmol 2009;147:774–8.
11 Alió JL, Shabayek MH. Corneal higher order aberrations: a method to gradekeratoconus. J Refract Surg 2006;22:539–45.
12 Brugin E, Ghirlando A, Gambato C, et al. Central corneal thickness: z-ring cornealconfocal microscopy versus ultrasound pachymetry. Cornea 2007;26:303–7.
13 Leonardi A, Lazzarini D, Bortolotti M, et al. Corneal confocal microscopy in patientswith vernal keratoconjunctivitis. Ophthalmology 2012;119:509–15.
14 Vanathi M, Tandon R, Sharma N, et al. In-vivo slit scanning confocal microscopy ofnormal corneas in Indian eyes. Indian J Ophthalmol 2003;51:225–30.
15 Weed KH, MacEwen CJ, Cox A, et al. Quantitative analysis of corneal microstructurein keratoconus utilising in vivo confocal microscopy. Eye (Lond) 2007;21:614–23.
16 Ali Javadi M, Kanavi MR, Mahdavi M, et al. Comparison of keratocyte densitybetween keratoconus, post-laser in situ keratomileusis keratectasia, anduncomplicated post-laser in situ keratomileusis cases. A confocal scan study. Cornea2009;28:774–9.
17 Jhanji V, Sharma N, Vajpayee RB. Management of keratoconus: current scenario.Br J Ophthalmol 2011;95:1044–50.
18 Snibson GR. Collagen cross-linking: a new treatment paradigm in cornealdisease—a review. Clinical & Experimental Ophthalmology 2010;38:141–53.
19 Ashwin PT, McDonnell PJ. Collagen cross-linkage: a comprehensive review anddirections for future research. British Journal of Ophthalmology 2009;94:965–70.
20 Caporossi A, Baiocchi S, Mazzotta C, et al. Parasurgical therapy for keratoconus byriboflavin-ultraviolet type A rays induced cross-linking of corneal collagen:preliminary refractive results in an Italian study. J Cataract Refract Surg2006;32:837–45.
21 Coskunseven E, Jankov MR 2nd, Hafezi F. Contralateral eye study of cornealcollagen cross-linking with riboflavin and UVA irradiation in patients withkeratoconus. J Refract Surg 2009;25:371–6.
22 Henriquez MA, Izquierdo L Jr, Bernilla C, et al. Riboflavin/ultraviolet A cornealcollagen cross-linking for the treatment of keratoconus: visual outcomes andScheimpflug analysis. Cornea 2011;30:281–6.
23 Koller T, Iseli HP, Hafezi F, et al. Scheimpflug imaging of corneas after collagencross-linking. Cornea 2009;28:510–15.
24 Vinciguerra P, Albè E, Trazza S, et al. Refractive, topographic, tomographic, andaberrometric analysis of keratoconic eyes undergoing corneal cross-linking.Ophthalmology 2009;116:369–78.
25 Hersh PS, Greenstein SA, Fry KL. Corneal collagen crosslinking for keratoconus andcorneal ectasia: one-year results. J Cataract Refract Surg 2011;37:149–60.
26 Wittig-Silva C, Whiting M, Lamoureux E, et al. A randomized controlled trial ofcorneal collagen cross-linking in progressive keratoconus: preliminary results.J Refract Surg 2008;24:S720–5.
27 Koppen C, Gobin L, Mathysen D, et al. Influence of contact lens wear on the resultsof ultraviolet A/riboflavin cross-linking for progressive keratoconus. Br J Ophthalmol2011;95:1402–5.
28 Lema I, Durán JA, Ruiz C, et al. Inflammatory response to contact lenses in patientswith keratoconus compared with myopic subjects. Cornea 2008;27:758–63.
29 Severinsky B, Wajnsztajn D, Frucht-Pery J. Silicone hydrogel mini-scleral contactlenses in early stage after corneal collagen cross-linking for keratoconus:a retrospective case series. Clin Exp Optom 2013;96:542–6.
Sehra SV, et al. Br J Ophthalmol 2014;98:442–447. doi:10.1136/bjophthalmol-2013-303934 447
Clinical science
group.bmj.com on October 5, 2014 - Published by bjo.bmj.comDownloaded from

doi: 10.1136/bjophthalmol-2013-303934December 24, 2013
2014 98: 442-447 originally published onlineBr J Ophthalmol Sri V Sehra, Jeewan S Titiyal, Namrata Sharma, et al. microscopy studycollagen cross-linking: an in vivo confocalgas permeable contact lens use following Change in corneal microstructure with rigid
http://bjo.bmj.com/content/98/4/442.full.htmlUpdated information and services can be found at:
These include:
References http://bjo.bmj.com/content/98/4/442.full.html#ref-list-1
This article cites 29 articles, 2 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(548 articles)Ocular surface � (460 articles)Cornea �
Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on October 5, 2014 - Published by bjo.bmj.comDownloaded from