cervical cancer khabele tpca 7-09.ppt - … indicated after total hysterectomy ... certain hpv types...
TRANSCRIPT

1
Cervical Cancer Screening -Improving PAP Rates
Dineo Khabele, MD, FACOG, FACS
Assistant Professor
Division of Gynecologic Oncology
Vanderbilt University Medical Center
Objectives
1. Review the current guidelines for cervical cancer screeningcancer screening.
2. Review human papillomavirus (HPV) testing and vaccination.
3. Discuss disparities in cervical cancer screening and prevention.

2
Cervical Cancer
• 11, 070 new cases and 3,870 deaths from cervical cancer in the US in 2009
• 50 million women undergo Pap testing in the U.S./ year
• 3.5 million (7%) are diagnosed with a cytological abnormality requiring additional follow-up or evaluation
• Approximately 500 000 new cases in the world mainly in• Approximately 500,000 new cases in the world, mainly in developing countries
• 273,500 deaths worldwide
Jemal, CA Cancer J Clin. 2009
Wright, JAMA. 2002
Cervical Cancer: Risk Factors
• Persistent high risk human papilloma virus (HPV) infection
• Three or more lifetime sexual partnersThree or more lifetime sexual partners
• First sexual intercourse before age of 18
• Smoking
• Maternal DES (diethylstilbesterol) exposure during pregnancy
A i b l P• A previous abnormal Pap smear
• Never having had a Pap or not having one in the previous 5-10 years
3
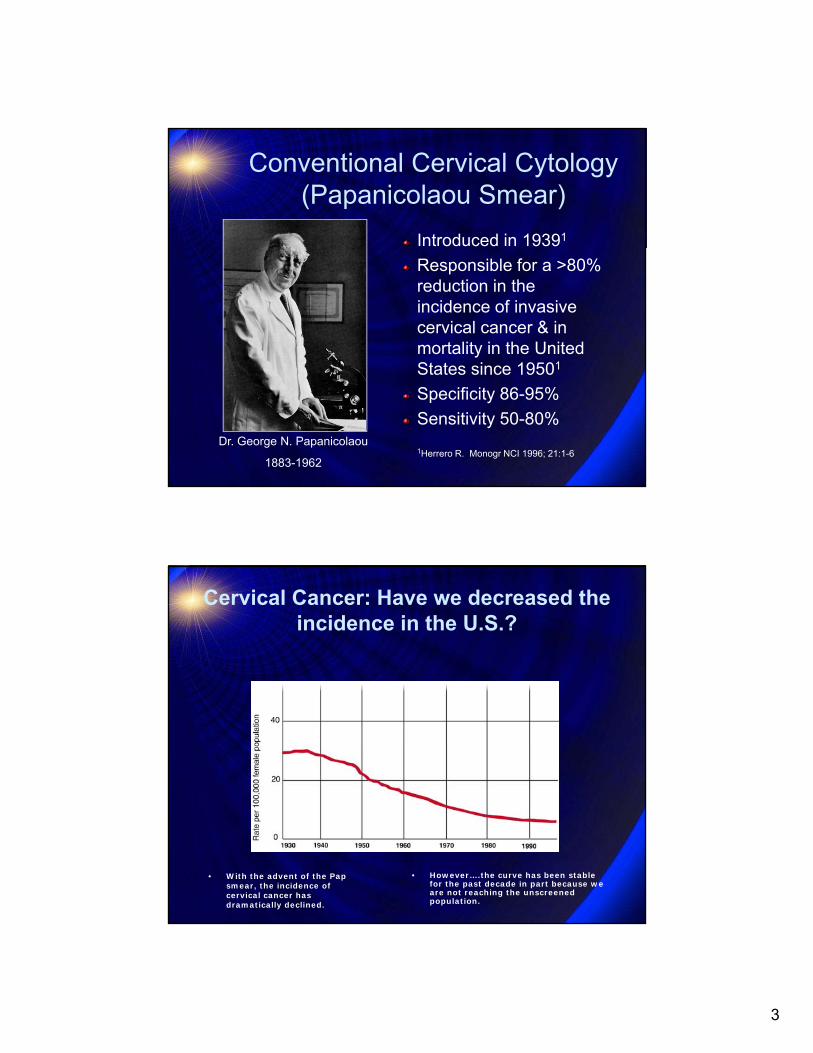
Conventional Cervical Cytology (Papanicolaou Smear)
Introduced in 19391
Responsible for a >80% reduction in the incidence of invasive cervical cancer & in mortality in the United States since 19501States since 19501
Specificity 86-95%
Sensitivity 50-80%
1Herrero R. Monogr NCI 1996; 21:1-6Dr. George N. Papanicolaou
1883-1962
Cervical Cancer: Have we decreased the incidence in the U.S.?
• However….the curve has been stable for the past decade in part because we are not reaching the unscreened population.
• With the advent of the Pap smear, the incidence of cervical cancer has dramatically declined.

4
Disparities in cervical cancer mortalitiy.
All White African American
Asian American/
American Indian/
Hispanic/ LatinoAmerican American/
Pacific Islander
Indian/Alaskan Native
Latino
2.7 2.4 5.1
(TN = 7.2)
2.7 2.6 3.5
Pap screening in African-American women is underutilized
• Current Pap test screening rates (~84%) fall h t f th H lth P l 2010 short of the Healthy People 2010
objective:screening of 90% of age-appropriate women
• The rate of not having had a Pap test in the past 3 years remains unchanged at approximately 16% for African American womenwomen
BRFSS, 2006

5
CLINICAL MANAGEMENT GUIDELINES FOR OBSTETRICIAN—GYNECOLOGISTS
NUMBER 45, AUGUST 2003 (Replaces Committee Opinion Number 152, March
1995)
Cer ical C tologCervical Cytology Screening
ACOG Screening Guidelines:When to Start
3 yrs after onset of intercourse & no later than age 21age
Earlier screening might over-diagnose lesions that would regress spontaneously, leading to over intervention
Cancer rarely seen 19Only 1.7% adolescents estimated to harbor HSIL70-90% HPV regression rates within 3 years1,2
80 90% LSIL regression in 13 21 yo (50 80% in adult80-90% LSIL regression in 13-21 yo (50-80% in adult women)1
1Moscicki AB. J Pediatr 1998; 132:277-2842Ho GY. NEJM 1998; 338:423-428

6
ACOG Screening Guidelines:When to Stop
Difficult to set an upper age limit for screeningACS Guideline – Discontinue After Age 70ACS Guideline – Discontinue After Age 70USPSTF Guideline – Discontinue After Age 65
Cervical cancer in older women almost entirely among unscreened & underscreenedScreening in women over 50 may be less efficient
Continue routine screening if:Remains sexually active w/ multiple partnersRemains sexually active w/ multiple partnersHas previous Hx of abnormal pap smears
ACOG Screening Guidelines:After Hysterectomy
Not indicated after total hysterectomy (includes removal of cervix) for benign(includes removal of cervix) for benign gynecologic disease
1.1% vaginal paps after hysterectomy abnormal1
Mean length of time after hysterectomy 19 years1
663 vaginal paps needed to detect one case of vaginal dysplasia2
1Pearce KF. NEJM 1996; 335:1559-622Piscitelli JT. Am J Ob Gyn 1995; 173:424-30

7
ACOG Screening Guidelines:After Hysterectomy
w/ CIN 2/3 prior to or at time of hysterectomy, p y yannually until 3 consecutive normal smears
w/ history DES exposure or Cervical Cancer, screen indefinitely while in reasonably good health
Increased risk for vaginal cancer
Error on side of screening if accurate information unavailable
ACOG Screening Guidelines:Screening Interval
After age 30 & 3 consecutive normalAfter age 30 & 3 consecutive normal smears, may screen every 2-3 years
Unless new partner, HIV (+), DES, chronic steroid use, or immunocompromisedWomen w/ prior abnormal results not considered screening (surveillance group)
M l bi ith HPV t ti t t dMay also combine with HPV testing to extend interval to 3 years
1Frame PS. J Am Board Fam Pract 1998; 11:87-952Sawaya GF. ASCCP March 2002. Abstract

8
Pap Diagnoses Preceding Histologic High-Grade
Neoplasia
AGCAGC
LSILLSIL ASCASC20%20%
10%10%
31%31%
39%39%
HSILHSIL
Modified from Kinney W, et al. Obstet Gynecol. 1998;91: 973-976.
Natural History of HPV Infection
0 to 2 Year 0 to 3 Years Up to 20 Years0 to 2 Year 0 to 3 Years Up to 20 Years
InitialHPV
InfectionCIN 1
Cervical Cancer
CIN 2/3 or AIS
ContinuingInfection
E6 & E7 interference E6 & E7 interference
w/ p53 & pRBw/ p53 & pRBCIN 1
Cleared HPV Infection Type SpecificImmunity
w/ p53 & pRBw/ p53 & pRB

9
HPV ClearanceMost HPV infections are transient
In women 15–25 years of age, ~80% of HPV infections resolve spontaneously1infections resolve spontaneously1
In 608 college women, 70% of new HPV infections cleared within 1 year and 91% within 2 years3
Median duration of infection = 8 months3
Certain HPV types are more likely to persist (eg,Certain HPV types are more likely to persist (eg, HPV 16 and HPV 18)
1. Meijer CJLM, et al. Histopathology. 1998;33:83–6.2. Schiffman M, Kjaer SK. J Natl Cancer Inst Monogr. 2003;31:14–9.3. Ho GYF, et al. N Engl J Med. 1998;338:423–8.
10
30%
Any HPV)
10%
15%
20%
25% Any HPV
High-risk HPV
Per
cen
tag
eH
PV
(+
)
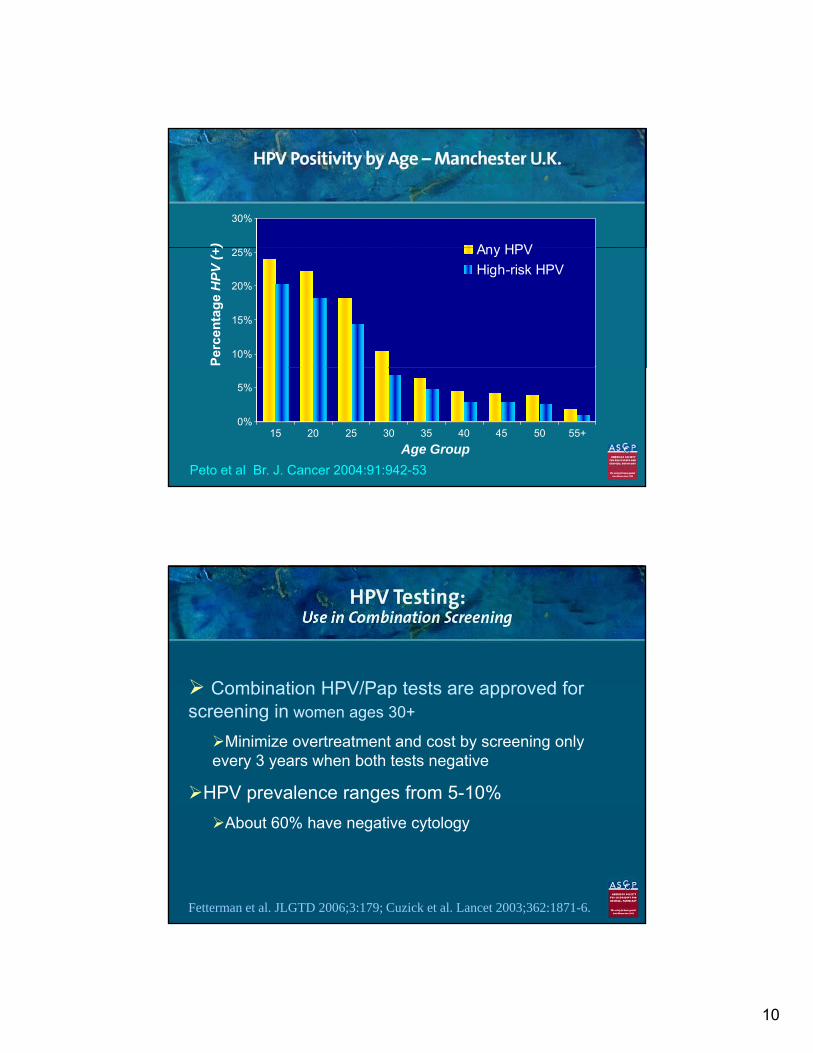
Peto et al Br. J. Cancer 2004:91:942-53
0%
5%
15 20 25 30 35 40 45 50 55+
Age Group
Combination HPV/Pap tests are approved for Combination HPV/Pap tests are approved for screening in women ages 30+
Minimize overtreatment and cost by screening only every 3 years when both tests negative
HPV prevalence ranges from 5-10%
About 60% have negative cytology
Fetterman et al. JLGTD 2006;3:179; Cuzick et al. Lancet 2003;362:1871-6.

11

12
Natural History of HPV
20514 women in Kaiser Permanente HPV 16+Kaiser Permanente Portland, OR followed for 10 years
Cumulative incidence rates of ≥CIN3
17 2 % for HPV 16+
HPV 16+
HPV 18+
HC2+17.2 % for HPV 16+
13.6% for HPV 18+
3.0% for 11/13 HC2+
0.8% for HC2-
HC2-
From Khan MJ, et al. JNCI 2005; 97:1072From Khan MJ, et al. JNCI 2005; 97:1072--99
HPV
Seattle, Washington college studentscollege students
36 month cumulative risk of CIN2-3
Any incident HPV 10%
Incident HPV 16/18 27%27%
Median time to detection of CIN2-3 was only 14 mo after HPV detection
From Winer, et al. J Inf Diseases 2005From Winer, et al. J Inf Diseases 2005

13
HPV Vaccines
HPV 16 and 18 Prevalence by Cytology Sentinel Surveillance (2003-2004)
80
HPV 18
HPV 16
10
20
30
40
50
60
70
80
Pre
vale
nce
(%
)
0
10
Anyabnormality
ASCUS LSIL HSIL
Centers for Disease Control and Prevention, preliminary/unpublished data. Modified from CIP. June 2006. Available at http://www.cdc.gov/nip/ACIP/slides/mtg-slides-jun06.htm#hpv. Accessed on March 3, 2007.

14
Most Prevalent HPV Types That Cause Cervical Squamous Cancer
HPV 1658%60
>70% of cases HPV 16
HPV 18
HPV 45
HPV 31
HPV 33
-infe
cted
pat
ients
(%
)
50
40
30
20
>70% of cases of cervical cancerare associated with HPV 16 or 18
HPV 16 HPV 18 HPV 45 HPV 31 HPV 33
N=1918 patients.Munoz et al. N Engl J Med. 2003;348:518-527. Based on a worldwide survey.
13%
5% 4% 3%All H
PV
-
10
0
Most Prevalent HPV Types That Cause Cervical Adenocarcinoma
60
n (%)
32%
43%
20
30
40
50
ence
of
HPV
typ
e in
aden
ocar
cinon
ma
(
8%4%
0
10
HPV 16 HPV 18 HPV 45 Multiple types
HPV DNA was detected in 93% of patients with cervical adenocarcinoma.Castellsague X et al. J Natl Cancer Inst. 2006;98:303-315.
Pre
val
case
s of

15
Prevalence of HPV in Genital Warts
>90% of cases of genital wartsgenital wartsare associated with HPV types 6 and 111
1.4 Million annual visits to physicians
1. Brown DR et al. J Clin Microbiol. 1999;37:3316-3322.
Natural History of HPV Infection
0 to 2 Year 0 to 3 Years Up to 20 Years0 to 2 Year 0 to 3 Years Up to 20 Years
InitialHPV
InfectionCIN 1
Cervical Cancer
CIN 2/3 or AIS
ContinuingInfection
E6 & E7 interference E6 & E7 interference
w/ p53 & pRBw/ p53 & pRBCIN 1
Cleared HPV Infection Type SpecificImmunity
w/ p53 & pRBw/ p53 & pRB

16
Immunization Against HPV
Studies suggest type-specific immunity to HPV1immunity to HPVType-specific neutralizing antibodies2
Virus-like particles (VLPs) are recombinant viral capsids that induce type-specific neutralizing
tib di 2antibodies2
Self assembled L1 proteinVLPs are highly immunogenic2
Photo courtesy of Margaret Stanley.1. Viscidi RP et al. Cancer Epidemiol Biomarkers Prev. 2004;13:324-327.2. Schiller JT et al. Nat Rev Cancer. 2004;2:343-347.
Quadrivalent L1 VLP Vaccine
Prevention of HPV 6/11/16/18
Infection & Disease

17
100%
Prevention of HPV 16/18-related Abnormal Cervical Cytology by Quadrivalent L1 VLP Vaccine†
(Women 16 – 26 years)
93% 8 cases Vaccine
25%
50%
75%93%
95% CI
85 - 97
8 cases Vaccine108 cases Placebo
0%N (Vaccine)= 1021N (Placebo)= 1023
†ASC-US (positive by high risk probe), LSIL, or worse

18
80
Reduction in Any Abnormal Pap tests Regardless of Causal HPV type by Quadrivalent L1 VLP Vaccine
20
40
60
↓23%↓16%
↓35%↓43%
0ASC-US HR + LSIL ASC-H HSIL
Cases Placebo 359 1000 89 41Cases Vaccine 285 864 59 24
W Huh, SGO 2008
Adverse Events in HPV 6/11/16/18 Studies
Injection-site reactions (pain, redness, swelling) most commonMost common general adverse events were fever and nausea
No difference between vaccine & placeboSAEs occurred in <0.1% of both groupsAmong women becoming pregnant on trial
Incidence fetal loss similar between groups (38% vsIncidence fetal loss similar between groups (38% vs. 40%)Incidence congenital anomalies similar (15 vs. 16)
includes pyloric stenosis, congenital megacolon, congenital hydronephrosis, hip dysplasia, and club foot

19
Gardasil Vaccine Reports to VAERSGardasil Vaccine Reports to VAERShttp://www.cdc.gov/vaccinesafety/vaers/gardasil.htmhttp://www.cdc.gov/vaccinesafety/vaers/gardasil.htm
GuillainGuillain--Barré Syndrome (GBS)Barré Syndrome (GBS)GBS occurs in 1GBS occurs in 1--2 out of every 100,000 people in their teens2 out of every 100,000 people in their teensThere has been no indication that Gardasil increases the There has been no indication that Gardasil increases the rate of GBS in girls and women above the rate expected in rate of GBS in girls and women above the rate expected in the general populationthe general population
Blood ClotsBlood ClotsRarely, people have reported blood clots after GardasilRarely, people have reported blood clots after GardasilMost had a risk of getting blood clots, such as taking oral Most had a risk of getting blood clots, such as taking oral contraceptivescontraceptives
DeathsDeathsAs of December 31, 2008, there have been 32 U.S. reports of As of December 31, 2008, there have been 32 U.S. reports of death among females who have received the vaccinedeath among females who have received the vaccineThere was no common pattern to the deaths that would There was no common pattern to the deaths that would suggest that they were caused by the vaccinesuggest that they were caused by the vaccine
Page last reviewed: March 29, 2009Page last reviewed: March 29, 2009Page last updated: March 3, 2009Page last updated: March 3, 2009Content source: Content source: Immunization Safety Office,Immunization Safety Office, Office of the Chief Science OfficerOffice of the Chief Science Officer
Subjects Exposed to Any Vaccine HPV Type at Enrollment
Baseline HPV Status
Efficacy Studies—Combined Population
20%
Baseline HPV Status
Naïve to all 4 types
Positive to 1 type
Positive to 2 types
Positive to 3 types
93% of subjects were naïve to ≥3 vaccine HPV types (6, 11, 16, or 18) at enrollment.
6%
73%
• Among subjects who were positive to a vaccine HPV type, most were positive to only 1 type.• Exclusion criteria: 6 or more sexual partners
Positive to 4 types 1.2%
0.1%

20
Indications and Use:Quadrivalent L1 VLP Vaccine
Indicated in girls and women 9 to 26 years of age for the prevention of the diseases caused byage for the prevention of the diseases caused by HPV types 6, 11, 16, and 18:
Cervical cancer
Genital warts (condyloma acuminata)
Dysplastic lesions:Cervical AISCervical AIS
CIN grades 2 and 3
VIN grades 2 and 3
VAIN grades 2 and 3
CIN grade 1
* 3 IM injections: 0, 2 and 6 months3 IM injections: 0, 2 and 6 months
Gardasil® Package Insert
“Shots for Girls Stir Early-Sex Concerns” - June 2006
The TennesseanThe Tennessean
I would love to hear how to “separate out the moral issues” to a nine year old who is questioning why she needs such a vaccine Theyear old who is questioning why she needs such a vaccine. The laws and commands of God cannot and should not be “separated” for any reason. We have forgotten that He gave us laws and commands for our own good! Dr. Khabele failed to consider there would be little need for this vaccine if we taught biblical principles of sex.” www.apologeticspress.org

21
Where can we intervene to close the gaps?BEDSIDE (Patient and Provider)
•Access to Care•Education and Awareness
•Knowledge, Attitudes and Beliefs
COMMUNITY (Policy & Public Health)•Health Access to Care
•Education and Awareness•Knowledge, Attitudes and Beliefs
RESEARCH•Clinical Trials
•Health Services and Health Outcomes Research
•Bench Research
Conclusions
1. Management guidelines exist for cervical cancer screeningcancer screening
2. HPV vaccines have been developed to protect against the most common HPV types1. Quadrivalent vaccine protects against HPV 6, 11, 16,
18
2. Bivalent vaccine protects against HPV 16, 18p g ,
3. A multi-pronged approach is needed to reduce disparities in cervical cancer screening, prevention, incidence and mortality