causes and treatment of chronic respiratory failure
TRANSCRIPT

1
UMEÅ UNIVERSITY MEDICAL DISSERTATION
New series No 1142 ISSN 0346-6612 ISBN 987-91-7264-455-7
From the Department of Public Health and Clinical Medicine Respiratory Medicine and Allergy
Umeå University, Sweden
Causes and Treatment of Chronic Respiratory Failure
Experience of a National Register
Torbjörn Gustafson
Umeå 2007

2
Copyright © 2007 by Torbjörn Gustafson
ISSN 0346-6612, ISBN 987-91-7264-455-7
Printed by: Solfjädern Offset AB, Umeå Cover: Blå Jungfrun, Kalmarsund
Department of Public Health and Clinical Medicine
Respiratory Medicine and Allergy Umeå University
SE-901 85 Umeå, Sweden

3
To Jonas, Helena, Emma and Ulla, my dear family!

4
TABLE OF CONTENTS
Abstract .................................................................................................................... 5
Swedish summary ..................................................................................................... 6
Original papers ......................................................................................................... 9
Abbreviations .......................................................................................................... 10
Introduction ............................................................................................................. 11
Aims ........................................................................................................................ 21
Material and methods ............................................................................................. 22
Study design ..................................................................................................... 22
Study populations ............................................................................................. 22
Data analyses ..................................................................................................... 25
Statistical methods ........................................................................................... 25
The individual papers ...................................................................................... 27
Results ..................................................................................................................... 40
Sex-related differences in LTOT in COPD (Paper I) ....................................... 40
Occupation and pulmonary fibrosis (Paper II) ................................................. 44
Ventilation or oxygen in kyphoscoliosis (Paper III) ......................................... 49
Quality in long-term oxygen therapy (Paper IV) .............................................. 52
Discussion of methodology ...................................................................................... 55
Discussion of main results ....................................................................................... 57
Conclusions ............................................................................................................. 70
Future perspectives ................................................................................................. 71
Acknowledgements .................................................................................................. 73
References ............................................................................................................... 75
Papers I – IV ............................................................................................................. 86

5
ABSTRACT Causes and treatment of chronic respiratory failure - experience of a national register Long-term oxygen therapy (LTOT) or home mechanical ventilation (HMV) can improve survival time in chronic respiratory failure. A national quality register could be an aid to identifying risk markers and optimizing therapy for respiratory failure.
Aims: ▪To identify risk markers for chronic respiratory failure, especially when triggered by chronic obstructive pulmonary disease (COPD) and idiopathic pulmonary fibrosis (IPF). ▪To predict sex-related differences in the future need of LTOT for COPD and to study sex related survival rate in COPD patients starting LTOT. ▪To investigate if HMV is more effective than LTOT alone in treating chronic respiratory failure caused by kyphoscoliosis. ▪To evaluate the use of quality indicators in LTOT.
Methods: Swedish national registers for LTOT and HMV were established in 1987 and 1996 respectively. They were reconstructed in 2004 to form the web-based register Swedevox. Indications for LTOT were based on the guidelines from the Swedish Society for Respiratory Medicine. The incidence and prevalence of LTOT for COPD were measured annually from 1987 to 2000, and the future need for LTOT was estimated on the basis of the frequency of ever smoking in Sweden in 2001 in different age groups. A postal questionnaire on occupational exposures was completed by 181 patients with severe pulmonary fibrosis who started LTOT between 1997 and 2000, and by 757 controls. Odds ratios (ORs) were calculated. Time to death was evaluated in kyphoscoliotic patients starting HMV or LTOT alone in 1996-2004. Ten quality indicators were defined and evaluated based on data from patients starting LTOT in 1987-2005.
Results: The incidence each year of LTOT in COPD patients increased more rapidly in women than in men (from 2.0 and 2.8/100,000 in 1987 to 7.6 and 7.1/100,000 in 2000 respectively, (p < 0.001)). Women ran a 1.9 times higher risk than men to develop chronic hypoxemia from COPD and had a higher survival rate during LTOT. In men, IPF was associated with exposure to birch dust with an OR 2.7, (95% confidence interval (CI) 1.30–5.65) and with hardwood dust, OR 2.7 (95% CI 1.14–6.52). Patients with kyphoscoliosis showed a better survival rate with HMV than with LTOT alone with a hazard ratio of 0.30 (95%CI 0.18-0.51), adjusted for age, sex, concomitant respiratory diseases, and blood gas levels. There were improvements in the following eight quality indicators for LTOT: access to LTOT, PaO2 ≤ 7.3 kPa without oxygen, no current smoking, low number of thoracic deformity patients without concomitant HMV, LTOT > 16 hours of oxygen/day, mobile oxygen equipment, reassessment of hypoxemia when LTOT was not started in a stable state COPD, and avoidance of continuous oral steroids in COPD. There was a decline in the indicator PaO2 > 8 kPa on oxygen. First-year survival rate in COPD was unchanged.
Conclusions: The incidence and prevalence of LTOT increase more rapidly in women than in men. Survival rate during LTOT in COPD is better in women than in men. Exposure to birch and hardwood dust may contribute to the risk of IPF in men. Survival rate in patients with kyphoscoliosis was three times better with HMV than with LTOT alone. The national quality register for LTOT showed improvements in eight out of ten quality indicators. Levels for excellent quality in the indicators are suggested. Key words: Chronic obstructive pulmonary disease; pulmonary fibrosis; kyphoscoliosis; respiratory failure; sex; smoking; occupation; survival; long-term oxygen therapy; mechanical ventilation.

6
SAMMANFATTNING PÅ SVENSKA Vid kronisk andningssvikt är tiden för överlevnad kort, men den kan förlängas med långtids behandling med syrgas (LTOT) eller hemrespiratorbehandling (HMV). Det är därför viktigt att identifiera riskfaktorer och att optimera behandlingen. Rökning, den huvudsakliga riskfaktorn för kroniskt obstruktiv lungsjukdom (KOL), har blivit vanligare hos kvinnor än hos män. Exponeringar i yrkesmiljö kan delvis ligga bakom utveckling av idiopatisk lungfibros (IPF), ett tillstånd med allvarlig ärrbildning i lungorna, vars orsak till stor del är okänd. Vid andningssvikt på grund av kyfoskolios spelar underventileringen på grund av deformeringen av bröstkorgen stor roll. Trots att mycket talar för att HMV är effektivare än enbart LTOT mot andningssvikt vid kyfoskolios, så erhåller en hel del kyfoskoliospatienter enbart LTOT. Det finns välkända svårigheter att få riktlinjer för LTOT genomförda. Ett nationellt kvalitetsregister kan tjäna som grund för utvärdering och förbättring av urval av patienter till samt genomförande av syrgasbehandling.
Målsättning: ▪ Att identifiera riskmarkörer för kronisk andningssvikt orsakad av kroniskt obstruktiv lungsjukdom (KOL) eller idiopatisk lungfibros (IPF). ▪ Att förutsäga könsrelaterade skillnader vad gäller behov av LTOT mot KOL inom en nära framtid och att studera könsrelaterade skillnader i överlevnad hos KOL-patienter, vilka påbörjar LTOT. ▪ Att studera om HMV är effektivare än enbart LTOT vid behandling av kronisk andningssvikt orsakad av kyfoskolios. ▪ Att utvärdera effekten av ett nationellt kvalitetsregister och att föreslå utmärkt kvalitet på kvalitetsindikatorer vid LTOT.
Metoder: Svenska nationella kvalitetsregister för LTOT och HMV etablerades respektive 1987 och 1996. Dessa rekonstruerades 2004 till att bilda det webbaserade registret Swedevox. Indikationerna för LTOT baseras på riktlinjer från Svensk Lungmedicinsk Förening. Dessa säger att LTOT är indicerat vid svår kronisk syrebrist, eller måttlig kronisk syrebrist komplicerad med högerhjärtsvikt eller förhöjt antal röda blodkroppar. Grundsjukdomen skall ha varit stabil i minst tre veckor. I vissa fall behöver dock LTOT påbörjas under en försämringsepisod av KOL och då skall skälet till LTOT omprövas de närmaste tre månaderna. Rökstopp är ett krav för att påbörja syrgasbehandling. Påbörjade LTOT och pågående LTOT på grund av KOL mättes varje år från 1987 till 2000 och det framtida behovet av LTOT hos män respektive kvinnor beräknades på basen av rökning någonsin i Sverige under 2000 i olika åldersgrupper. En postenkät om yrkesexponeringar fylldes i av 181 patienter med svår lungfibros, vilka påbörjade LTOT mellan 1997 och 2000, samt av 757 kontrollpersoner. Oddskvoter (OR) beräknades avseende riskmarkörer. Tiden till död utvärderades hos kyfoskoliospatienter som påbörjade HMV eller enbart LTOT under 1996-2004. Tio kvalitetsindikatorer definierades och utvärderades baserat på data från patienter, som påbörjade LTOT från 1987 till och med 2005.
Resultat: Det årliga antalet påbörjade LTOT hos KOL-patienter ökade snabbare hos kvinnor än hos män (från 2,0 och 2,8/100 000 under 1987 till 7,6 och 7,1/100,000 under 2000 respektive (p < 0,001)). Kvinnor löpte en 1,9 gånger högre risk än män att utveckla kronisk syrebrist på grund av KOL. Allt fler kvinnor med KOL beräknas påbörja LTOT under de närmaste åren och ännu fler kommer att ha pågående LTOT på grund av KOL. Hos män var IPF associerat med exponering för björkdamm, OR 2,7, (95 % konfidensintervall (CI) 1,30–5,65) och med damm av ädelträ, OR 2,7 (95 % CI 1,14–6,52). Patienter med kyfoskolios, vilka erhöll HMV, hade bättre överlevnadsgrad än de som behandlades med enbart syrgas med en riskkvot på 0,30 (95 % CI 0,18–0,51), korrigerat för ålder, kön, samtidig luftvägssjukdom samt blodgasnivåer. Det blev förbättring i följande åtta kvalitetsindikatorer
7
för LTOT: Tillgång till LTOT, arteriellt syretryck (PaO2) ≤ 7,3 kPa med luftandning, ingen pågående rökning, HMV till alla kyfoskoliospatienter som erhåller LTOT, > 16 timmar med syrgas per dygn, portabel syrgasutrustning, omprövning av indikationen för LTOT, om den har påbörjats när KOL inte var i stabil fas samt undvikande av underhållsbehandling med kortisontabletter vid KOL. Det blev minskning i indikatorn PaO2 > 8 kPa vid andning av syrgas. Överlevnadsgraden första året vid KOL var oförändrad. Under 2005 förmådde > 80 % av länen uppfylla fyra kriterier för LTOT.
Slutsatser: Påbörjade behandlingar med LTOT och pågående LTOT ökar snabbare hos kvinnor än hos män. Överlevnaden vid LTOT på grund av KOL är bättre hos kvinnor än hos män. Exponering för damm av björk och ädelträ kan bidra till ökad risk för IPF hos män. Kyfoskoliospatienter hade tre gånger bättre överlevnad med HMV än med enbart syrgas. Det nationella kvalitetsregistret för LTOT visade förbättring i åtta av tio kvalitetsindikatorer. Nivåer föreslås för utmärkt kvalitet för de tio indikatorerna.

8

9
CAUSES AND TREATMENT OF CHRONIC RESPIRATORY FAILURE – EXPERIENCE OF A NATIONAL REGISTER
ORIGINAL PAPERS
I Franklin KA, Gustafson T, Ranstam J, Ström K. Survival and future need of long-term oxygen therapy for chronic obstructive pulmonary disease - gender differences.
Respir Med 2007; 101:1506-1511
II Gustafson T, Dahlman-Höglund A, Nilsson K, Ström K, Tornling G, Torén K. Occupational exposure and severe pulmonary fibrosis.
Respir Med 2007; 101:2207-2212
III Gustafson T, Franklin KA, Midgren B, Pehrsson K, Ranstam J, Ström K. Survival of
patients with kyphoscoliosis receiving mechanical ventilation or oxygen at home.
Chest 2006; 130:1828-1833
IV Gustafson T, Löfdahl K, Ström K. A model of quality assessment in patients on long-term oxygen therapy.
Manuscript Permission to print the original papers in this thesis has been granted from the Editorial epartments of Respiratory Medicine and Chest The Tables 2 and 3 and the Figures 8-12 in this thesis were published in Respiratory Medicine, Volume 101, Franklin KA, Gustafson T, Ranstam J, Ström K, Survival and future need of long-term oxygen therapy for chronic obstructive pulmonary disease - gender differences, Page 1506-1511, Copyright Elsevier (2007). The Tables 4, 5 and 8-11 and the Figure 4 in this thesis were published in Respiratory Medicine, Volume 101, Gustafson T, Dahlman-Höglund A, Nilsson K, Ström K, Tornling G, Toren K, Occupational exposure and severe pulmonary fibrosis, Page 2207-2212, Copyright Elsevier (2007). The Tables 6, 12 and 13 and the Figures 13-15 in this thesis were published in Chest, Volume 130, Gustafson T, Franklin KA, Midgren B, Pehrsson K, Ranstam J, Ström K. Survival of patients with kyphoscoliosis receiving mechanical ventilation or oxygen at home, Page 1828- 1833. Copyright American College of Chest Physicians (2006).

10
ABBREVIATIONS
ATS American Thoracic Society
CI Confidence interval
COPD Chronic obstructive pulmonary disease
ERS European Respiratory Society
FEV1 Forced expiratory volume in one second
FVC Forced vital capacity
HMV Home mechanical ventilation
HR Hazard ratio
IPF Idiopathic pulmonary fibrosis
ILD Interstitial lung disease
kPa kilopascal
LTOT Long-term oxygen therapy
MRC Medical Research Council
NOTT Nocturnal Oxygen Therapy Trial
OR Odds Ratio
PaCO2 Arterial carbon dioxide tension
PaO2 Arterial oxygen tension
PF Pulmonary fibrosis
SD Standard deviation

11
INTRODUCTION
Chronic respiratory failure
Chronic respiratory failure (arterial partial pressure of oxygen (PaO2) < 8.0 kPa, with or
without arterial partial pressure of carbon dioxide (PaCO2) > 6.7 kPa while breathing air at
sea level),1 is a serious complication of several pulmonary diseases, chronic obstructive
pulmonary disease (COPD) being the most common of them.2-5 Other major causes include
interstitial lung disease (ILD), pulmonary vascular disease and damage to the lungs and
bronchi after pulmonary tuberculosis.2-5 Chronic respiratory failure can also be caused by
thoracic deformity, such as kyphoscoliosis and sequelae after pulmonary tuberculosis. In
thoracic deformity, hypoventilation with carbon dioxide retention requires special
attention.2,3,6 Hypoxemia, the main component of respiratory failure, is the result of various
combinations of four mechanisms: ventilation-perfusion inequality, hypoventilation, diffusion
impairment and shunt, of which ventilation-perfusion inequality is the most important.7,8
Hypoxemia is dangerous, since it results in tissue hypoxia, causing damage to the internal
organs.7
Long-term oxygen therapy
The consequence of chronic hypoxemia in COPD is a poor prognosis with reduced time to
death.9 Oxygen has been used in the treatment of pulmonary diseases since the 1920s.10,11
Long-term administration of oxygen (LTOT) to COPD patients with respiratory failure was
introduced in the 1950s, based on the results of some largely observational studies with small
numbers of subjects.12,13
The results of two large randomised controlled studies confirmed the improvements in
survival time after LTOT in COPD patients with severe chronic hypoxemia.14,15 The
Nocturnal Oxygen Therapy Trial (NOTT) from the US randomised 203 patients with COPD
and hypoxemia (PaO2 ≤ 7.3 kPa or PaO2 ≤ 7.9 kPa together with pulmonary hypertension or
polycythemia) to nocturnal oxygen of 12 hours per 24 hours or continuous oxygen for 24
hours per day. After a mean of 19 months (range 12-24 months), the mortality was 1.94 times
higher (p = 0.01) in the nocturnal oxygen group vs. continuous oxygen.
In the British study from the Medical Research Council (MRC), oxygen for at least 15 hours
per day at a flow rate of 2 l/min or higher if required to reach a PaO2 of > 8 kPa was

INTRODUCTION
12
compared with no oxygen at all in 87 COPD patients with PaO2 between 5.3 and 8.0 kPa.
Most patients were men and 37% were smokers. At 5 years of follow-up, 19/42 patients had
died in the oxygen group vs. 30/45 patients in the control group. There was no effect on
mortality in men within 500 days.
Later, a study in Poland demonstrated that LTOT had no influence on survival time in COPD
patients with mild-moderate hypoxemia, which so far is the only performed study in that
area.16 There was no difference in cumulative survival time over three years between LTOT
and no oxygen in 135 COPD patients with PaO2 between 7.4 and 8.7 kPa.
These controlled trials on hypoxemic COPD constitute the scientific evidence for several
recommendations on the use of LTOT.1,17-21
Long-term oxygen therapy is one of the two interventions with positive prognostic effects in
COPD, the other being smoking cessation.22-25 LTOT actually doubles survival time when
administered continuously to severely hypoxemic COPD patients.14,15 In contrast, a large
recently published study did not clearly show that the combination of inhaled steroid and
long-acting beta-2-agonist had life-prolonging effects on COPD.26
There is no evidence that LTOT has effects in terms of survival time in other underlying
conditions with chronic hypoxemia than COPD. Still, oxygen is believed to reduce dyspnoea
and to attenuate the harmful effect of hypoxemia on the internal organs.27 Therefore oxygen is
recommended when hypoxemia occurs in patients with idiopathic pulmonary fibrosis (IPF)
and pulmonary hypertension (PAH) or other disease processes with similar indications as in
COPD.2,21,28
Despite the doubling of survival time with LTOT administered for chronic severe hypoxemia
in COPD, survival time during LTOT is poor, particularly in pulmonary fibrosis and
pulmonary hypertension.3-5 In COPD, the excess mortality attributable to hypoxemia is
eliminated by LTOT29 but the mortality attributable to severe obstruction and cardiovascular
disease associated with COPD remains.30 Therefore, identifying risk markers for chronic
respiratory failure and hypoxemia is an important task for improving prevention.
Furthermore, the survival time benefit is only observed in patients with severe hypoxemia.14-16
Therefore, it is essential to have adequate patient selection criteria for LTOT. The survival

INTRODUCTION
13
benefit was doubled when continuous oxygen therapy was administered, as compared with
nocturnal treatment. Adequate LTOT, including hours of oxygen use and oxygenation, is also
essential to obtain maximum benefit. Adequate LTOT is also decisive to obtain improvements
in quality of life.31
A small improvement in quality of life is obtained with LTOT in hypoxemic COPD, but
quality of life remains poor during LTOT.31-34 To obtain the benefit of improving quality of
life, mobile equipment is decisive for patients active outside home.31 Dyspnoea at exertion
can be incapacitating in respiratory failure and oxygen has a limited effect on this symptom.35-
38
The aims of this thesis were to study sex as a risk factor for hypoxemic COPD and
occupational exposure as a risk factor for pulmonary fibrosis with severe hypoxemia, to
identify whether HMV or LTOT is the best treatment in kyphoscoliosis with respiratory
failure and to evaluate quality indicators for LTOT. The quality indicators were based on
existing evidence and guidelines and our experience of a national register on LTOT.
Sex-related differences in COPD
Tobacco smoking and occupational risk factors, as well as malnutrition, poor water supply,
sanitation, personal and domestic hygiene, unsafe sexual behaviour, alcohol use,
hypertension, physical inactivity, illegal drugs, and air pollution have been identified as major
risk factors for death and disability worldwide.39
Tobacco smoking is the dominant risk factor for COPD,19,40,41 after age.42 Smoking is
increasing in a global perspective.43 The cigarette consumption per capita worldwide is slowly
decreasing, but total smoking has increased continuously over the last decades, mainly owing
to population growth. Cigarette consumption is still higher per capita in developed countries,
but it is increasing dramatically in the developing part of the world.43 Chronic obstructive
pulmonary disease is expected to rise from the twelfth to the fifth leading cause of disability
from 1990 to 2020 and from the sixth to the third leading cause of death from 1990 to 2020.44
The tobacco industry has studied smoking patterns and preferred tobacco products among
women in detail, and has used this information to make tobacco products specially designed
to support recruitment of female smokers.45,46 Tobacco advertising contributes to initiation of
INTRODUCTION
14
smoking in the population.47-50 It is believed that deaths attributable to tobacco use would
continue to rise even if comprehensive tobacco control policies were immediately
implemented worldwide.43
Women are more sensitive than men to the harmful effects of tobacco smoke, according to
several studies,24,51-53 and may also be more disposed to developing severe form of COPD.54
Moreover, in severe COPD the prognosis is worse for women than for men.55,56 The effects of
long-term oxygen on survival time in women with severe COPD have been less studied than
among men. Only 21%-24% of the patients included in previous studies of LTOT and
survival time were women.14-16
For many years, the prevalence of COPD has been higher for men than for women. This
pattern has been changing in recent years.57 In Sweden, smoking has decreased gradually
since 1980 and since 1990 fewer men than women smoke. In 2005, 14% of men and 18% of
women in Sweden were current smokers, or less than 16% of the adults in total.58 The ratio in
a country of prevalence of smoking in younger women to that of older women is thought to be
an indicator of the future prevalence of smoking in that country.59
The mechanism behind pulmonary fibrosis
Idiopathic pulmonary fibrosis (IPF) is the most common disorder in the group of idiopathic
interstitial pneumonias which, in turn, is a subgroup of the diffuse parenchymal lung
diseases.60 The histological pattern is usual interstitial pneumonia (UIP), not specific for IPF.
It is a serious disease with poor response to treatment.61 Idiopathic pulmonary fibrosis is
clinically comparable to diffuse interstitial pneumonia (DIP) and nonspecific interstitial
pneumonia (NSIP), which carry less severe prognoses than IPF. These are the main
alternative interstitial lung diseases (ILD) to IPF.62,63 The recommended procedure for
differentiation of IPF from the other ILDs is surgical lung biopsy. When it is not possible to
perform, the differential diagnosis may rest on accepted major and minor criteria, based on
non-invasive techniques.61 In reality, open lung biopsy is only performed in a small
proportion of patients with PF.64,65
The mortality in IPF is high and is increasing.62,66,67 Median survival time is 3-5 years after
diagnosis and there is evidence that mortality rates may now be higher than in several

INTRODUCTION
15
malignancies.61,67 When PF is complicated by respiratory failure, survival time is
considerably shorter than in COPD with respiratory failure.3,5
Figures for prevalence/incidence are not entirely reliable, owing to a shortage of reports, a
low proportion of biopsy verifications of the diagnosis, and reclassification.61 The previous
highest prevalence (20.2 per 105 in men and 14.3 per 105 in women) and incidence (10.7 per
105 in men and 7.4 per 105 in women per year) was found in a New Mexico county.68 A
recent survey demonstrated a more than doubling of the incidence between 1990 and 2003 in
the United Kingdom.64 This increase could not be explained in terms of ageing in the
population or improved diagnostic accuracy.
There are several risk factors for IPF, including genetic predisposition and environmental
agents.61 The knowledge about potentially harmful occupational exposures is largely based on
six case-control studies in three countries.69-74 According to a meta-analysis of these studies,65
there are significant associations between six types of exposure and IPF: ever smoking (1.58
[1.27–1.97]), agriculture/farming (1.65 [1.20–2.26]), livestock (2.17 [1.28–3.68]), wood dust
(1.94 [1.34–2.81]), metal dust (2.44 [1.74–3.40]), and stone/sand (1.97 [1.09–3.55]). There is
no study from northern Europe on occupational exposure in patients with PF where, for
example, occupational exposure to soft wood may be frequent.
Respiratory failure in kyphoscoliosis
In respiratory failure, ventilation-perfusion mismatch, reduced area for gas diffusion and
alveolar hypoventilation contribute in varying proportions to this physiological disturbance,
depending on the underlying disease.7,8 Kyphoscoliosis causes impaired ventilatory
mechanics, which may result in considerable alveolar hypoventilation, especially during
sleep.75-79 It has been demonstrated that breathing at low lung volumes often leads to airway
obstruction.80-82 Many of these patients therefore have both a restrictive and obstructive
respiratory disorder and may develop both hypercapnia and hypoxemia in varying
combinations. Therefore, the selection criteria for both LTOT and for HMV are often
fulfilled. The respiratory and cardiac failure caused by kyphoscoliosis results in a poor
prognosis.
Several studies suggest that early initiation of HMV in kyphoscoliotic patients may prevent
the onset of overt respiratory failure.83,84 The mechanisms for the effect seem to be improved
respiratory drive,85,86 improved respiratory muscle function,87-89 but not necessarily affecting
of sleep architecture.90 Consequently, there is a positive effect on daytime blood gases from

INTRODUCTION
16
HMV during the night to patients with hypoventilation, which is observed early in the
treatment.91 The benefits of HMV as compared with LTOT has recently been shown in a
small retrospective follow-up by Buyse et al..92
Earlier studies comparing LTOT with HMV in patients with severe thoracic spine deformity
are either short-term or retrospective, and small in terms of number of subjects. Randomised
controlled trials on this issue are generally considered ethically difficult to justify.92
According to figures from quality registers in Sweden and France, LTOT is prescribed for a
substantial number of patients with respiratory failure caused by kyphoscoliosis.3,5,6 In the
Swedish Oxygen Register the annual number of new patients with kyphoscoliosis registered
when starting LTOT remained stable since 1987. This was a matter of concern, since the
Swedish Society of Respiratory Medicine has recommended HMV for these patients since
1993. Since several patients with severe thoracic spine deformity are prescribed LTOT
without concomitant HMV we found it important to compare the impact on survival time of
the different treatment modes in a large patient group.
Quality in long-term oxygen therapy
The main goal of LTOT in relation to hypoxemic COPD is to improve survival time. To attain
this goal, patient selection and performance are of utmost importance. Long-term oxygen
therapy is effective in COPD with severe hypoxemia. This treatment method is complicated,
and the portable oxygen is fairly expensive. Therefore, it is important to assure the quality of
LTOT with use of a number of appropriate quality parameters, and guidelines constitute the
first step in this direction.
Guidelines on LTOT
The indications for LTOT are described in a number of guidelines, among them the Global
Strategy for the Diagnosis, Management, and Prevention of COPD, and in the statement from
the American Thoracic Society (ATS) and the European Respiratory Society (ERS).1,19
Guidelines consist of patient selection criteria and criteria for performance of LTOT.
According to the guidelines from the Swedish Society of Respiratory Medicine, LTOT is
indicated for patients with:17,18,20,21
• chronic hypoxemia owing to COPD or other diseases,

INTRODUCTION
17
• a stable disease course on optimum medical therapy for at least three weeks, and
• arterial oxygen tension (PaO2) when breathing room air ≤ 7.3 kPa (< 7.0-7.5 kPa before
1993) or signs of cor pulmonale or haematocrit > 50 % plus
room air PaO2 of 7.4-8 kPa (around 7.5 kPa before 1993).
The prescription of LTOT to current smokers is discouraged.
Arterial blood gas samples are taken with the patient at rest and after having breathed air for a
minimum of 20 minutes. Arterial blood gas samples are taken on oxygen after having
breathed the prescribed flow of oxygen for a minimum of twenty minutes.
Performance of LTOT
According to the Swedish guidelines, oxygen should be prescribed as many hours as possible
per day, preferably 24 hours.21 A resting PaO2 of above 8 kPa when breathing oxygen is
recommended.
The stationary oxygen supply through the concentrator should be supplemented with mobile
equipment in patients with outdoor activity.
Reassessment of the indication for LTOT should be performed after one and three months,
when LTOT is initiated owing to an exacerbation of COPD.20
Quality indicators
Patient selection criteria
Access to LTOT – Given above, it is important to identify and provide LTOT to patients who
fulfil the selection criteria. In the mid 1980s there were large variations in the number of
LTOT patients among the different counties in Sweden, which caused concern among
respiratory physicians and was the rationale for the start of the Swedish Oxygen Register in
1987.2
Level of hypoxemia – Contrary to severe hypoxemia, patients with mild to moderate
hypoxemia should not be prescribed long-term oxygen, unless the hypoxemia is accompanied
by pulmonary hypertension or raised haematocrit levels.1,17-19 Consequently, the selection of
appropriate patients should be essential in LTOT.14-16
Smoking - According to the Swedish guidelines for LTOT, current smoking is an obstacle to
prescription of LTOT, because of the risk that ongoing smoking will jeopardize the treatment

INTRODUCTION
18
results. Cigarette smoking has been shown to inhibit the benefits of oxygen on secondary
polycythemia,93 and a previous study demonstrated association between continued smoking
during LTOT and increased mortality.3 There is also a risk of fire accidents, of which there
are a few reports.94-96
Kyphoscoliosis - Since alveolar hypoventilation is an important pathophysiological
mechanism when kyphoscoliosis is the reason for chronic hypoxemia,75-79 oxygen alone is
insufficient as therapy in these patients. Instead, HMV during the night is often recommended
as the first treatment,97 since it has favourable physiological effects, including improved
daytime blood gases.83-89,91 Many patients with kyphoscoliosis and respiratory failure receive
supplemental oxygen2,3,5,6 especially those who also have concomitant respiratory disease, but
the mortality is higher when oxygen is given without concomitant HMV, according to data
from a large French register and a Belgian retrospective follow-up study.5,92
Performance of LTOT
Correction of hypoxemia – The target for resting arterial oxygen tension is chosen from the
procedure in the NOTT and the MRC studies, where the subjects were given a flow rate of
oxygen sufficient to reach PaO2 60-80 mmHg (equal to 5.3-8.0 kPa) and 60 mmHg,
respectively.14,15 The level of oxygen in the arterial blood has to be raised to alleviate hypoxia
in the body tissues, and the results of LTOT thus depend on adherence to adequate
achievement of arterial oxygenation. In some patients, retention of carbon dioxide can make it
difficult to reach adequate oxygenation with the oxygen supply.27
Treatment time per day – Appropriate duration of treatment with oxygen per day is also
important for the outcome of LTOT, according to the findings in the NOTT and the MRC
studies.14,15 Oxygen should be supplied for at least 15 hours per day, and the effects on
survival time are increased if the treatment time is extended beyond that, up to 24 hours per
day.
Portable oxygen equipment – The possibilities of reaching appropriate treatment time
increases if the patient has suitable equipment. For this purpose, addition of portable oxygen
equipment to the stationary equipment has a positive effect in patients who spend time outside
their home.31,98,99

INTRODUCTION
19
Reassessment of LTOT after initiation during COPD exacerbation – It is often necessary to
start LTOT during recovery from an exacerbation of COPD instead of awaiting the stable
level of oxygenation. Some patients will then experience improved arterial oxygen levels
during a three-month period, making LTOT no longer needed. Under those circumstances,
recent guidelines recommend a recheck of arterial blood gases after 30-90 days.19,100,101
Concomitant treatment
Avoidance of continuous oral glucocorticosteroids in COPD – Temporary treatment with oral
glucocorticosteroids in acute exacerbations has beneficial effects on recovery time, lung
function and hypoxemia1,19 but long-term treatment with oral glucocorticosteroids is not
recommended in COPD, because no treatment effects have been shown and there are serious
side effects.1 An association has been found between oral steroid medication and increased
mortality in female LTOT patients3,102 and higher mortality in LTOT patients with high body
mass index receiving oral glucocorticosteroids has also been demonstrated.103
Results of treatment
Survival time – According to the results from the NOTT and MRC studies, LTOT can double
survival time in COPD patients with severe hypoxemia.14,15 Those studies were performed on
selected patients, who were younger and had fewer co-morbidities than the average patients
who have later received LTOT.104 The survival time in COPD patients may be lower in
clinical practice than in the randomised controlled trials,14,15 according to the findings of an
Australian study,104 where the patients were older and had multiple co-morbidities. However,
when selected according to similar criteria as in the NOTT and MRC studies, survival time in
Swedish COPD patients receiving LTOT was similar.102,105
Implementing guidelines for management of LTOT are recognized as being difficult.106,107
Adherence to the LTOT guidelines varies in different countries and different areas in the
countries.3,98,108-110 A national register provides a basis for evaluation and subsequent
improvement.

20

21
AIMS
The objectives of this thesis were to identify possible strategies for the prevention and
postponement of the development of chronic respiratory failure as well as to assure the quality
of treatment of chronic respiratory failure.
The specific aims were
- To identify risk markers for chronic respiratory failure, particularly female sex in chronic
obstructive pulmonary disease and occupational exposure in pulmonary fibrosis.
- To predict the future incidence and prevalence of chronic hypoxemia in chronic obstructive
pulmonary disease on the basis of sex-related prevalence in smoking.
- To study sex related survival time in COPD patients who start LTOT.
- To identify the best treatment of chronic respiratory failure caused by kyphoscoliosis,
comparing home mechanical ventilation or long-term oxygen alone.
- To evaluate the effects of a national quality assurance register and to suggest levels for
excellent quality for quality indicators in long-term oxygen therapy.
22
MATERIAL AND METHODS
STUDY DESIGN
Paper I: Register study of cohorts as well as cross-sectional data
Paper II: Retrospective case control study
Paper III: Cohort study
Paper IV: Prevalence study on county level and national level
STUDY POPULATIONS
The Swedish Oxygen Register
The Swedish Oxygen Register was established in 1987 with the two main purposes of gaining
knowledge of treatment effects and long-term prognosis in LTOT and improving the quality
of LTOT in chronic hypoxemia. The principal quality aspects were to optimize: access to
therapy, adherence to national guidelines for LTOT and performance of LTOT. The register is
used for a prospective cohort study of patients receiving oxygen for chronic hypoxemia at the
start of LTOT, including patients who were already on LTOT when the register was
established. The LTOT patients are reported from the responsible physicians at the Swedish
centers for LTOT, one or more in each Swedish county. Follow up is recorded one year after
inclusion.
Specially trained physicians and nurses are responsible for the LTOT in each county, which is
the relevant unit. Annual meetings are held for reporting of the results from the register, for
training, and thereby to achieve gradual improvements in LTOT. The statistics from the
register are also annually distributed in written forms.
A large number of variables for each patient are were registered at inclusion, when their
LTOT is started. A selection of these variables has been registered since the start of the
Register and others during limited periods.

MATERIAL AND METHODS
23
Table 1. Registered data in patients receiving LTOT (selection)
Inclusion record form Follow up record form Swedish census registration number Swedish census registration number Sex County County Number of in-hospital days Arterial blood gas tensions Reason of withdrawal of oxygen PaO2 (air) Date for withdrawal of oxygen PaCO2 (air) PaO2 (oxygen) PaCO2 (oxygen) Cause(s) of hypoxemia Smoking history Current medication Presence of ankle oedema WHO performance status FEV1 and FVC Oxygen therapy Equipment Prescribed flow rate Prescribed daily treatment time FEV1: forced expiratory volume in one second; FVC: forced vital capacity
Figure 1. Causes of hypoxemia in patients receiving LTOT 1987-2005 according to sex.
MATERIAL AND METHODS
24
Register coverage
Sweden had a population of 8.4 million in 1987 and 9.1 million in 2006. The register covers
approximately 85% of the LTOT patients.2 The coverage is internally validated with surveys
to the reporting centers about every other year. Four of the 24 counties were unable to report
all LTOT patients to the register, owing to shortages of staff during some part of the period
1987-2000.111 Data from the Swedish Oxygen Register were used in Papers I-IV
The Swedish Home Ventilator Register
The Swedish HMV Register was established 1996 with the purpose of allowing international
and national comparisons of indications, dissemination of methods and results. All the
Departments of Respiratory Medicine and all other medical units prescribing oxygen or home
mechanical ventilation in all Swedish counties report all patients who start HMV, and they are
then followed prospectively with survival time as a primary outcome. Among the data
registered is Swedish census registration number, sex, arterial blood gas tensions when
breathing air, and presence of a concomitant respiratory disease.
Register coverage
The Register covers at least 90% of the Swedish patients treated with HMV according to
repeated internal validations.
Data from the Swedish HMV Register were used in Paper III.
In November 2004, the Swedish Oxygen Register and the Swedish HMV Register were
reconstructed and merged to form the Swedevox Register, which is entirely web-based.
The Swedish Oxygen Register and the Swedish HMV Register were approved by all regional
ethic committees and by the Swedish Data Inspection Board. The registers were funded by the
Swedish National Board of Health and Welfare as national quality assurance registers.
The Causes of Death Register is kept by the Swedish National Board of Health and Welfare,
and comprises all deceased Swedish citizens during a calendar year. Among the information
in the register are Swedish census registration numbers, cause or causes of death, time of
MATERIAL AND METHODS
25
death and results of autopsy if performed. The International Classification of Diseases (ICD)
is used for classification of causes of death.
Official statistics in Sweden are produced by the government agency Statistics Sweden, or
Statistiska centralbyrån (SCB), housing the Swedish Population Register, which also contains
information about date of death for people living in Sweden.
Data analyses
In Paper I, we analysed data from the Swedish Oxygen Register, comparing this data with the
dates of death from the Swedish Causes of Death Register.
In Papers III and IV, we analysed data from the Swedish Oxygen and HMV registers with
dates of death from the Swedish Population Register. In the COPD patients in Paper IV, we
investigated the survival rates during the first year of LTOT, adjusted for age and sex. We
also analysed the age-adjusted overall survival according to the year of starting LTOT and
sex.
Statistical methods
The Chi-squared test was used in Papers I and III for comparisons of categorical data.
The Student’s t-test was used in Paper I for comparisons of continuous data.
Analyses of variance were used in Paper III for comparison analyses of continuous data.
Cox regression analysis was used in Paper I to analyse time to death adjusted for age, in Paper
III to assess the effects of treatment method on survival rate and in Paper IV to assess first-
year and overall survival rates standardised for sex and age 70 years.
The Mantel-Haenszel chi-squared test was used in Paper II to calculate odds ratios for PF and
IPF.
Linear regression analyses were used for adjustment of age and other confounders in time-
trend analyses of continuous variables in Paper I.
Logistic regression analysis was used in Paper I for age-adjusted analyses of category
variables and in Paper II to adjust for overlapping exposures between occupations.

MATERIAL AND METHODS
26
The photograph in the printed version has been removed in the electronic version
Figure 2. Young girls smoking cigarettes

MATERIAL AND METHODS
27
PAPER I – Sex-related differences in LTOT in COPD
Patient population
We included all LTOT patients aged 18 and over with hypoxemia attributable to COPD who
were registered between 1 January 1987 and 31 December 2000 (n=5,689). We acquired the
vital statistics on each patient through 31 December 2003 and the dates of death from the
Causes of Death Register at the Swedish National Board of Health and Welfare.
Women were slightly younger than men at the start of LTOT (p < 0.001). The mean age of
both sex increased during the study years. In 1987, the mean age of the women was 66 ± 8
years and that of the men 67 ± 9 years. In 2000, the mean age of women had increased to 73 ±
9 years (p < 0.001) and the mean age of men to 74 ± 8 years (p < 0.001). Seventy-three per
cent of the women and 70% of the men had PaO2 < 7.3 kPa at the onset of oxygen therapy.
Three hundred and ninety-four patients were excluded since they were registered in the four
counties that withdrew from the study for part of the time. They did not differ in age and sex
from the included patients.
Mean arterial PaO2 was slightly lower and mean PaCO2 was higher in women than in men
when starting oxygen therapy. Mean PaCO2 at the start of treatment gradually decreased in
men from 1987 to 2000, but remained stable in women.
Table 2. Baseline characteristics of COPD patients at start of LTOT.
Women n = 2,894
Men n = 2,795 p-value
Age (years) 70 ± 9 72 ± 9 < 0.001
PaO2 (kPa) 6.6 ± 1.0 6.7 ± 0.9 < 0.001
PaCO2 (kPa) 6.6 ± 1.2 6.1 ± 1.2 < 0.001
PaO2 (oxygen) (kPa) 9.0 ± 1.1 9.0 ± 1.2 0.95
PaCO2 (oxygen) (kPa) 6.9 ± 1.2 6.4 ± 1.2 < 0.001
FEV1 (liters) 0.6 ± 0.3 1.0 ± 0.5 < 0.001
FVC (liters) 1.4 ± 0.5 2.1 ± 0.9 < 0.001
Peripheral oedema (%) 58 52 < 0.001 Smoking history (%) Current Past Never
4 85 11
3 90 6
< 0.001
Values are presented in per cent or as the means ± SD

MATERIAL AND METHODS
28
The predicted incidence and prevalence of the need for LTOT was calculated from the
frequency of ever smoking in Sweden in 2001 in different age groups, according to Statistics
Sweden:
Table 3. Ever smoking in men and women according to age in 2001.
Ever smoking (%)
Age Men Women
16-24 23.5 30.1
25-34 33.6 37.9
35-44 43.4 52.4
45-54 63.9 59.5
55-64 69.9 54.0
65-74 64.1 41.8
75-84 66.3 30.3
In the prediction of future need for LTOT, we assumed that age at the start of treatment for
men and women would be the same as in 2000 and that the relation between the prevalence
and incidence would continue to be the same as from 1987 to 2000.
The incidence of LTOT was calculated as in the following example:
The mean percentage of ever smoking in Sweden in women in the age group of 64-84 years
old of was 36.4% in 2001. This age group corresponds closely to the age range of women
receiving oxygen in 2000 (73 ±9 years). Five years later, in 2006, there would thus be 41.8%
of women who had ever smoked among women in the age group for starting LTOT, and the
incidence of LTOT was therefore calculated as being 1.15 times higher (41.8/36.4) in 2006
than in 2000 (when the incidence was 7.65 per 100,000) which would have been 8.78 per
100,000. Fifteen years later, in 2016, the incidence would be 1.48 times higher (54.0/36.4)
than in 2000.
Prevalence of LTOT was calculated as in the following example:
We first calculated the annual quotient between prevalence and incidence which, in women,
was 2.76 per 100,000 in 1988 and 3.47 per 100,000 in 2000. The mean increase for every year

MATERIAL AND METHODS
29
was 0.054. The prevalence of oxygen in the year of 2006 was therefore calculated as the
predicted incidence in 2006 (in women: 8.78 per 100,000) multiplied by the expected quotient
in 2006 i.e. the quotient in 2000 plus 6 x 0.054 (in women 3.79 per 100,000). This gave an
expected prevalence of 8.78 x 3.79 = 33.28 per 100,000 in women in the year of 2006.
The mathematical model is therefore: Expected prevalence year X = expected incidence year
X x ((prevalence year 2000/incidence year 2000) + (X-2000 x ((prevalence year
2000/incidence 2000) – (prevalence year 1987/incidence 1987))/13)).

MATERIAL AND METHODS
30
The photograph in the printed version has been removed in the electronic version
Figure 3. Inside a timber industry.

MATERIAL AND METHODS
31
PAPER II - Occupation and pulmonary fibrosis
We included as cases all patients (n=241) registered when starting LTOT for chronic
hypoxemia triggered by PF between 1 February 1997 and 4 April 2000. In the analysis, we
divided the cases into two groups, namely all cases (the PF sample), and a restricted sample of
cases (the IPF sample), after exclusion of all subjects with known aetiology of their fibrosis.
The data from the Oxygen Register and the questionnaires did not allow verification of IPF
according to accepted major and minor criteria.61 When identifying the IPF patients we
therefore excluded all patients with host susceptibility or known external agents. We then
assumed that the remaining patients had IPF, being the largest group of the idiopathic
interstitial pneumonias serious enough to cause chronic respiratory failure.
We selected as controls a random sample (n=1,000) from the general population of Sweden
with the same age range as the cases. We sent an extensive postal questionnaire to the cases
and the controls, described below.
The questionnaire was completed by 193 PF patients (cases). Twelve (6%) were excluded due
to erroneous diagnosis in the Oxygen Register. Hence, 181 subjects were included in the PF
sample. From this sample we excluded 27 subjects because of rheumatoid arthritis (n=14),
scleroderma (n=4), Sjögren’s syndrome (n=2) and other diseases such as systemic sclerosis
and systemic lupus erythematosus (n=7). An additional 14 cases were excluded because of
known aetiology, viz. asbestosis (n=6), silicosis (n=5), and irradiation or drug-induced PF
(n=3). Hence, 140 cases were included in the IPF sample. Of the 1,000 controls being sent the
questionnaire, 757 responded.
For each patient answering the questionnaire, the responsible physician was sent a
questionnaire about drugs used the ten years before debut of the disease, any irradiation
treatment, year of first symptoms and diagnosis, investigations performed, grounds for
diagnosis and the physician’s opinion of the possible aetiology of the PF. In the IPF sample,
75 had been examined with high resolution computer tomography of the lungs and ten had
lung biopsy, open or video assisted.
MATERIAL AND METHODS
32
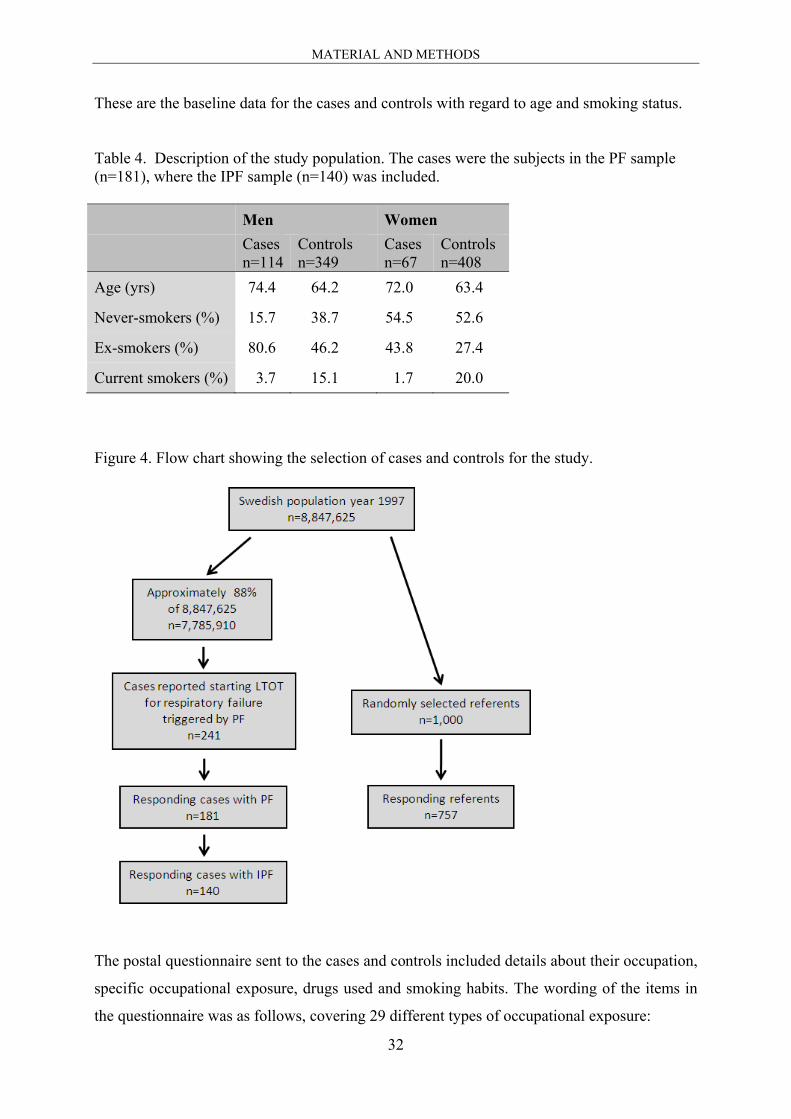
These are the baseline data for the cases and controls with regard to age and smoking status.
Table 4. Description of the study population. The cases were the subjects in the PF sample (n=181), where the IPF sample (n=140) was included. Men Women
Cases n=114
Controls n=349
Cases n=67
Controls n=408
Age (yrs) 74.4 64.2 72.0 63.4
Never-smokers (%) 15.7 38.7 54.5 52.6
Ex-smokers (%) 80.6 46.2 43.8 27.4
Current smokers (%) 3.7 15.1 1.7 20.0
Figure 4. Flow chart showing the selection of cases and controls for the study.
The postal questionnaire sent to the cases and controls included details about their occupation,
specific occupational exposure, drugs used and smoking habits. The wording of the items in
the questionnaire was as follows, covering 29 different types of occupational exposure:

MATERIAL AND METHODS
33
Table 5. Questions about occupational exposure in the questionnaire.
Have you ever been exposed to welding fumes? mineral dust? coal dust or graphite dust? man-made mineral fibres? ceramics dust? asbestos? grain dust? flour dust? dust from pine or fir? dust from birch? dust from hardwood? paper dust? textile dust? radiation? fire fumes? engine exhausts? irritating gases (ammonia, chlorine dioxide, chlorine gas, sulphur dioxide)? environmental tobacco smoke? Have you worked with grinding, polishing, milling, turning or other processing of metals? soldering? blasting? chrome-platering or nickel-platering? birds? moldy hay or straw? solvents? cutting oils/fluids? rapid glues (Loctite, cyanoacrylates or Omnifit)? Have you worked as a dentist, dental technician or dental nurse?
The cases and referents were divided into the following three groups according to year of
birth: 1906–1923, 1924–1936 and 1937–1969. The cases were diagnosed in 1968–1999. We
further divided them into three groups according to their year of diagnosis, as follows: 1968–
1986 (41%), 1987–1993 (28%) and 1994–1999 (31%).
Relevant exposure was exposure that had occurred before the onset of PF, approximated as
the year of diagnosis. It was also necessary to define an anchor point in time for each control.
Hence, in each birth year group the controls were randomly assigned to a year of diagnosis
group. The number of controls allocated to each year of diagnosis group was weighted by the
number of actual cases. Each control was then assigned the mid-year in his or her year of
diagnosis group as the anchor year.

MATERIAL AND METHODS
34
Subjects had to report exposure five years or more before diagnosis to be classified as
exposed. Consequently, exposure occurring during the 5-year period immediately prior to the
diagnosis was not included in the analysis. Exposures were merged into five categories in the
final analysis: occupational, organic dust, wood dust, inorganic dust, and metal dust.
Two groups of cases were analysed, the whole group of cases (the PF sample) and the
restricted sample (the IPF sample). The cases and controls were stratified for sex, age group,
and birth year group. Odds ratios (ORs) were calculated. Only exposure categories with five
or more exposed cases were considered in the final analysis.
The photograph in the printed version has been removed in the electronic version
Figure 5. A woman with kyphoscoliosis.

MATERIAL AND METHODS
35
PAPER III – Ventilation or oxygen in kyphoscoliosis
All men and women with respiratory failure caused by non-paralytic kyphoscoliosis, i.e.
scoliosis not related to neuromuscular disorders, registered when starting LTOT or HMV
between 1 January 1996 and 31 December 2004 were included (n=244). We acquired the vital
statistics before 15 February 2006 and the dates of death from the Swedish Population
Register.
The mean age of all patients was 69 ± 11 years. One hundred and sixty-seven were women
and 77 were men. Twenty-seven of the 100 patients who received HMV also received
supplementary oxygen therapy. Three patients were ventilated via tracheostomy and the rest
with nasal or oro-nasal masks. Mechanical ventilation was prescribed during sleep, i.e. for
less than eight hours to 75% of the patients and for more than 12 hours to only two per cent of
patients. All of 144 patients who received oxygen therapy alone were prescribed oxygen for
16 to 24 hours per day. Five patients who started with oxygen alone and later received
supplementary mechanical ventilation were grouped according to the initial treatment.
Table 6. Baseline characteristics of patients with kyphoscoliosis starting treatment with home mechanical ventilation or oxygen in Sweden, 1996-2004.
Characteristics HMV (n = 100)
LTOT alone (n = 144) p-value
Age (years) 62.4±12.7 73.5±8.9 < 0.001
Women (%) 68 69 0.95
Concomitant respiratory disease (%) 33 65 < 0.001
PaO2 (kPa) 7.5±1.7 6.4±0.9 < 0.001
PaCO2 (kPa) 7.6±1.2 6.9±1.3 0.002

MATERIAL AND METHODS
36
The photograph in the printed version has been removed in the electronic version
Figure 6. A man with portable oxygen equipment.

MATERIAL AND METHODS
37
PAPER IV - Quality in long-term oxygen therapy
We prospectively followed all registered adults starting LTOT for chronic hypoxemia before
1 January 2006 until death or 31 December 2006 (n=12,187). We did not include patients
receiving LTOT for a short period as part of palliative treatment for cancer of the lung,
whether primary or secondary.
Our quality indicators
Patient selection criteria
From 1987 and onwards:
- Access to LTOT as the number of LTOT patients per 100,000 inhabitants
- Percentage of patients with PaO2 ≤ 7.3 kPa when breathing air, daytime at rest
- Percentage of patients who are not current smokers
From 1993 and onwards:
- Small number of patients with thoracic deformity without concomitant HMV
Performance of LTOT
From 1987 and onwards:
- Percentage of patients with PaO2 > 8 kPa when breathing oxygen
- Percentage of patients with prescribed dosage of oxygen > 16 hours per day
1989-2004:
- Percentage of patients with access to mobile oxygen equipment, registered at follow-up after
one year
From 2002 and onwards:
- Percentage of COPD patients with reassessment of hypoxemia when breathing air if LTOT
was not started in a stable state, registered at follow up after one year
Concomitant treatment:
1987-1989 and from 1995 and onwards:
- Percentage of COPD patients without continuous oral glucocorticosteroids
Result of treatment: First-year survival rate in COPD
1987-2004:
- First-year survival rate among COPD patients

MATERIAL AND METHODS
38
Use of quality indicators
The county level of achievement for each quality indicator was given for comparisons with
the national level reached by all participating centers in the annual reports and from the start
of the web-based Swedevox register. With the individual levels obtained from these centers as
guidance, a recommended level of achievement was chosen as a marker of excellent quality,
according to the individual levels obtained from the centers, e.g. XX% of patients have PaO2
> 8 kPa when breathing oxygen (Table 14).
Each quality indicator was analysed by comparing data from 1987 and 2005, or at some other
start and end year, as described above.
Table 7. Baseline characteristics of patients starting LTOT 1987-2005.
Characteristic
No patients 12 187
% men 49
Age, years 71+9
Cause(s) of hypoxaemia, no patients
COPD 8446
Pulmonary fibrosis 1431
Thoracic deformity 605
Pulmonary vascular disease 461
Sequelae of pulmonary tuberculosis 262
Other causes 982
Arterial blood gas tensions, kPa
PaO2 (air) 6.6+1.0
PaCO2 (air) 6.2+1.3
PaO2 (oxygen) 9.0+1.3
PaCO2 (oxygen) 6.5+1.3

MATERIAL AND METHODS
39
Figure 7. Age of COPD patients at the start of LTOT according to starting year and sex.
40
RESULTS
PAPER I – Sex-related differences in LTOT in COPD
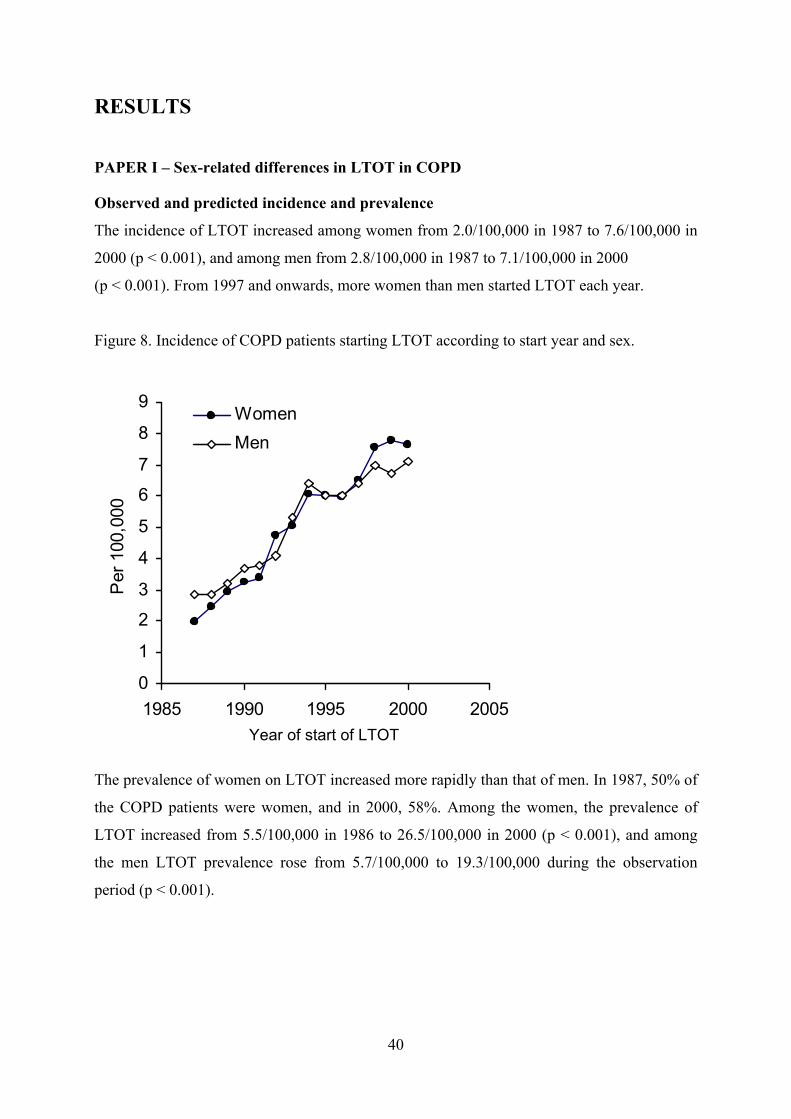
Observed and predicted incidence and prevalence
The incidence of LTOT increased among women from 2.0/100,000 in 1987 to 7.6/100,000 in
2000 (p < 0.001), and among men from 2.8/100,000 in 1987 to 7.1/100,000 in 2000
(p < 0.001). From 1997 and onwards, more women than men started LTOT each year.
Figure 8. Incidence of COPD patients starting LTOT according to start year and sex.
0
1
2
3
4
5
6
7
8
9
1985 1990 1995 2000 2005
Per
100
,000
WomenMen
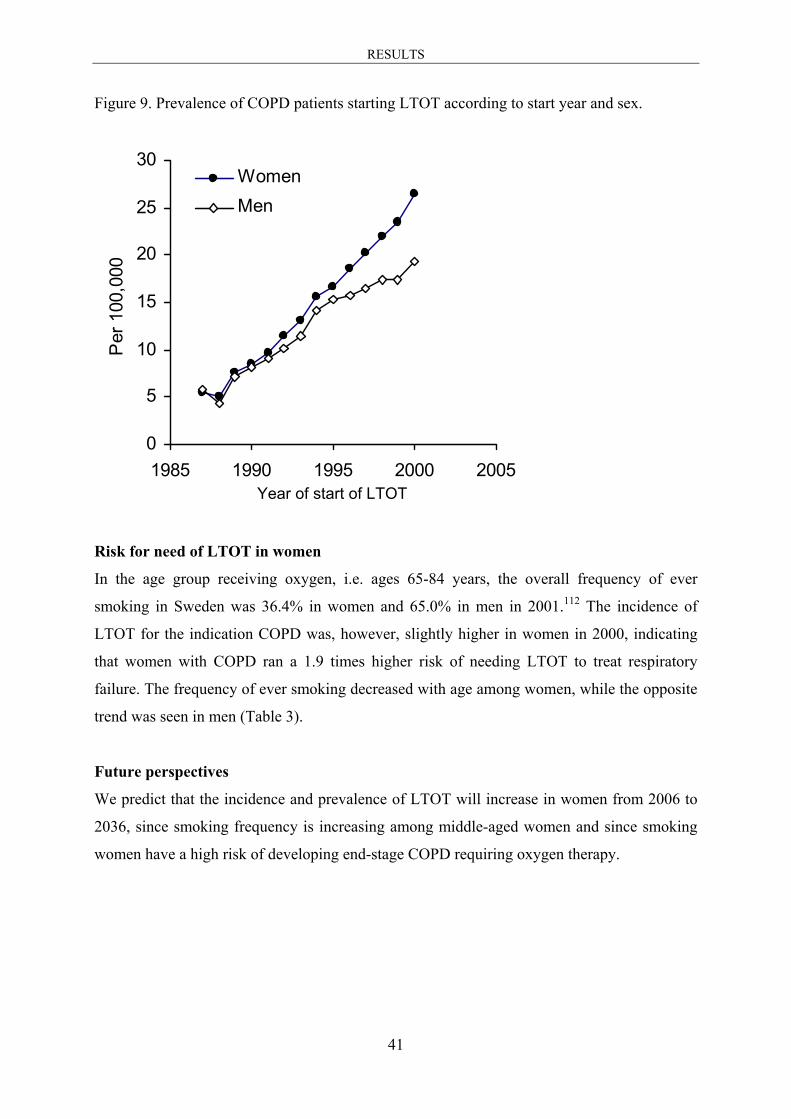
The prevalence of women on LTOT increased more rapidly than that of men. In 1987, 50% of
the COPD patients were women, and in 2000, 58%. Among the women, the prevalence of
LTOT increased from 5.5/100,000 in 1986 to 26.5/100,000 in 2000 (p < 0.001), and among
the men LTOT prevalence rose from 5.7/100,000 to 19.3/100,000 during the observation
period (p < 0.001).
Year of start of LTOT
RESULTS
41
Figure 9. Prevalence of COPD patients starting LTOT according to start year and sex.
0
5
10
15
20
25
30
1985 1990 1995 2000 2005
Per
100
,000
WomenMen
Risk for need of LTOT in women
In the age group receiving oxygen, i.e. ages 65-84 years, the overall frequency of ever
smoking in Sweden was 36.4% in women and 65.0% in men in 2001.112 The incidence of
LTOT for the indication COPD was, however, slightly higher in women in 2000, indicating
that women with COPD ran a 1.9 times higher risk of needing LTOT to treat respiratory
failure. The frequency of ever smoking decreased with age among women, while the opposite
trend was seen in men (Table 3).
Future perspectives
We predict that the incidence and prevalence of LTOT will increase in women from 2006 to
2036, since smoking frequency is increasing among middle-aged women and since smoking
women have a high risk of developing end-stage COPD requiring oxygen therapy.
Year of start of LTOT
RESULTS
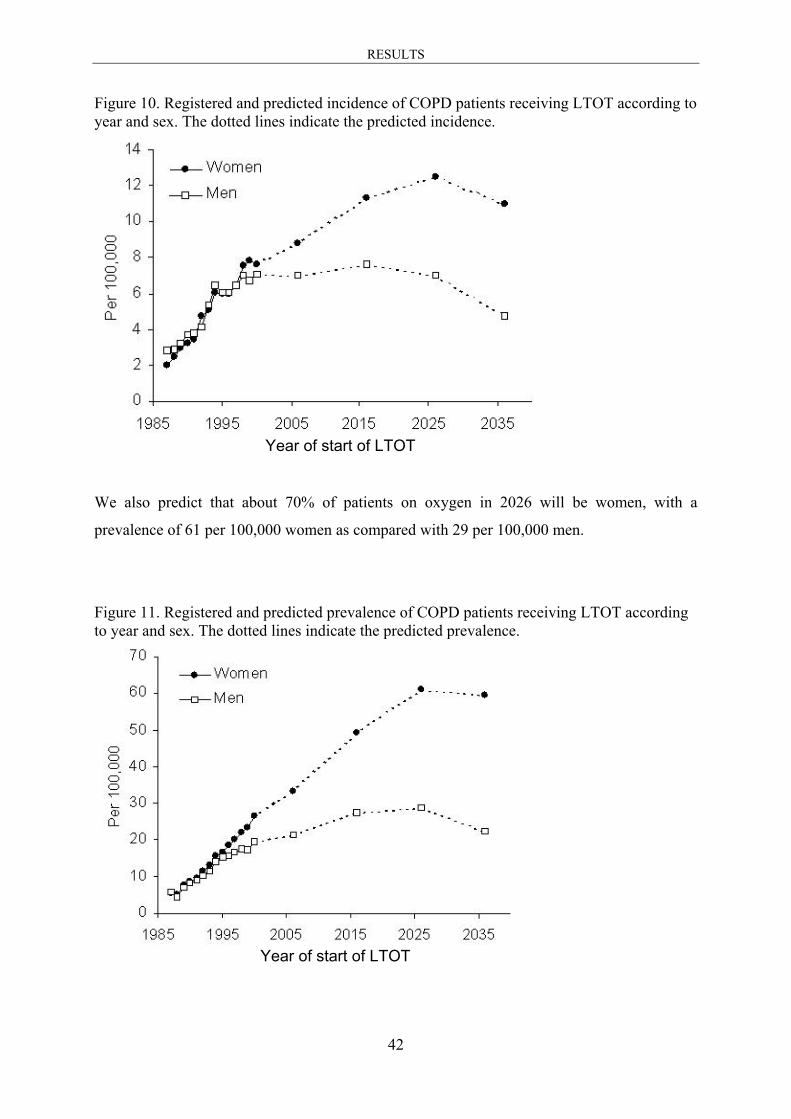
42
Figure 10. Registered and predicted incidence of COPD patients receiving LTOT according to year and sex. The dotted lines indicate the predicted incidence.
We also predict that about 70% of patients on oxygen in 2026 will be women, with a
prevalence of 61 per 100,000 women as compared with 29 per 100,000 men.
Figure 11. Registered and predicted prevalence of COPD patients receiving LTOT according to year and sex. The dotted lines indicate the predicted prevalence.
Year of start of LTOT
Year of start of LTOT

RESULTS
43
Hours of oxygen and survival time
In 1987, 42% of patients were prescribed oxygen from compressed gas cylinders and 58%
were prescribed oxygen from concentrators. The percentage of patients using concentrators
rose rapidly, to 97% in 2000. Liquid oxygen was prescribed in 2-3% of patients after 1993,
when it was introduced in Sweden. Slightly more men than women were prescribed oxygen
for > 20 hours per day, p=0.041. Two per cent of women were prescribed oxygen for less than
15 hours per day, 60% for 15-17 hours per day, 9% for 18-19 hours per day and 29% for 20-
24 hours per day. In the case of men, 2% were prescribed oxygen for less than 15 hours per
day, 59% for 15-17 hours per day, 8% for 18-19 hours per day and 31% for 20-24 hours per
day.
The median (1st and 3rd quartile) survival time after the start of treatment was 2.8 (2.6-2.9)
years in women and 2.0 (1.9-2.1) years in men (Figure 12). First-year survival rate was 77%
(95% CI 75-79%) in women and 69% (95% CI 67-71%) in men. The relative risk of death for
men vs. women was 1.21 (95% CI 1.14-1.28) according to a Cox regression adjusted for age.
In patients who were withdrawn from LTOT within one year from the start of treatment, death
was the reason for withdrawal in 88% of women and 91% of men. Improvement in
oxygenation breathing ambient air, and non-compliance were other reasons for withdrawal
during the first year of treatment.
Figure 12. Survival rate in men and women receiving LTOT 1987 -2000.

RESULTS
44
PAPER II - Occupation and pulmonary fibrosis
Subjects with occupational exposure had an increased risk for PF, but not for IPF. Exposure
to wood dust increased the risk for PF but not for IPF. There was no increased risk for either
PF or IPF in relation to exposure to metal dust.
Table 8. Odds ratio, stratified by sex, year of diagnosis, birth year and smoking, for the PF sample (n=181) and the IPF sample (n=140) according to occupational exposure. Exposure PF sample IPF sample
n* OR 95% CI n* OR 95% CI
Any occupational exposure 123 1.6 1.06–2.37 86 1.1 0.71–1.72
Organic dust 69 1.4 0.98–2.12 49 1.1 0.74–1.76
Wood dust 34 1.7 1.03–2.95 22 1.2 0.65–2.23
Inorganic dust 57 1.2 0.79–1.97 35 0.9 0.53–1.49
Metal dust 37 1.0 0.62–1.69 25 0.9 0.51–1.59
When stratifying the analyses for sex, we observed the highest risks of developing PF among
men. Exposure to wood dust among men doubled the risk of developing PF.
Table 9. Odds ratio, stratified by year of diagnosis, birth year and smoking, for the PF sample divided into men (n=114) and women (n=67), according to occupational exposure. Exposure Men, PF Women, PF
n* OR 95% CI n* OR 95% CI
Any occupational exposure 89 1.7 0.95–3.12 34 1.5 0.84–2.55
Organic dust 54 1.7 1.04–2.70 15 1.1 0.56–2.10
Wood dust 33 2.1 1.18–3.65 – n.a. –
Inorganic dust 54 1.4 0.84–2.23 – n.a. –
Metal dust 34 1.1 0.62–1.79 – n.a. –
We then analysed the risks of developing PF and IPF according to all the detailed exposures.
These analyses were performed in men and women together, and were restricted to exposures
affecting five or more cases. The exposure categories are not mutually exclusive. An
increased risk of PF was associated with exposure to mineral dust, birds, flour dust, dust from
pine or fir, birch dust, hardwood dust and fire fumes. In cases of IPF the exposures giving

RESULTS
45
increased risk were only birch dust and hardwood dust. The OR for flour dust and IPF were
just below significance level.

46
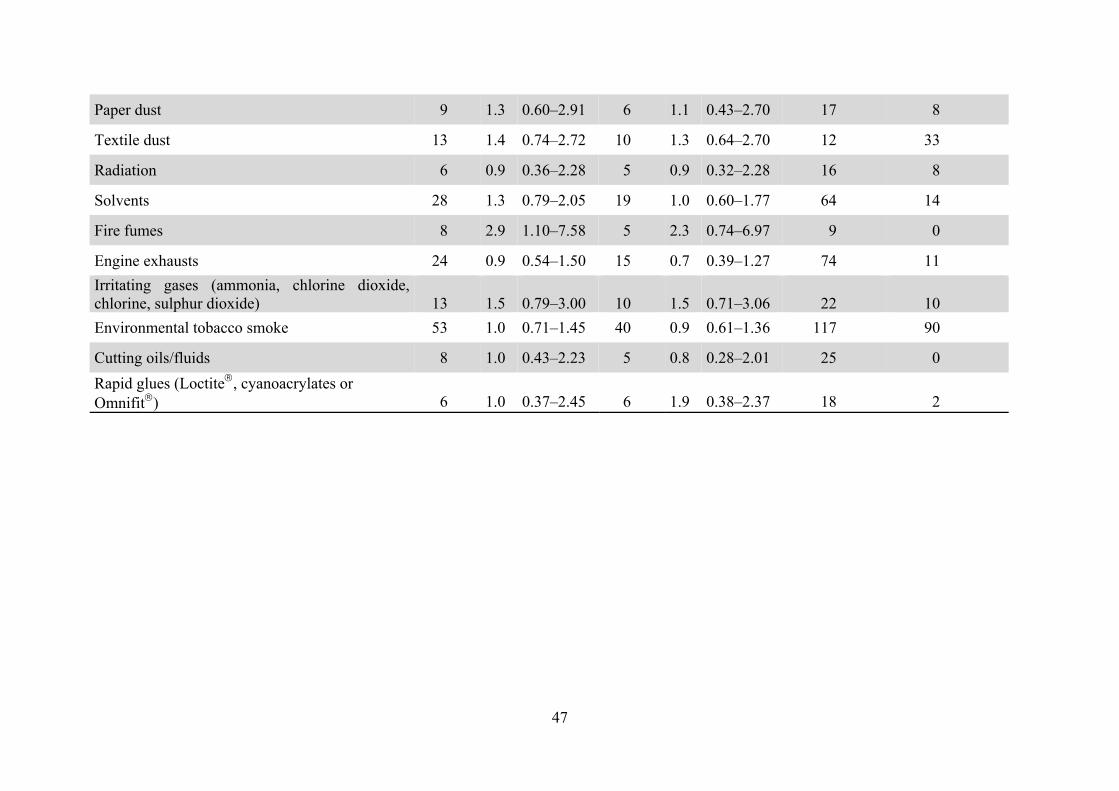
Table 10. Odds ratio for the PF sample and the IPF sample according to occupational exposure, stratified by sex. Only exposures with five or more exposed cases were considered. Number of controls exposed for each occupational exposure, divided into men and women. Exposure PF
(n=181) IPF
(n=140) Controls, men
(n=349) Controls, women (n=408)
n OR 95% CI n OR 95% CI n n
Welding fumes 24 1.1 0.64–1.78 15 0.8 0.42–1.42 70 1 Grinding, polishing, milling or turning or other processing of metals
22
1.0
0.57–1.64
15
0.8
0.43–1.44
62
13
Soldering 13 0.9 0.47–1.65 9 0.7 0.31–1.38 44 8
Blasting 7 3.2 1.10–9.32 – n.a. – 7 0
Mineral dust 27 2.4 1.39–4.06 14 1.4 0.74–2.72 39 2
Coal dust or graphite dust 11 1.8 0.83–3.82 9 1.8 0.80–4.07 18 3
Artificial mineral fibres 22 1.2 0.67–2.00 14 0.8 0.45–1.57 60 4
Asbestos 26 1.2 0.72–2.00 15 0.8 0.44–1.47 66 6
Birds 16 2.3 1.22–4.34 10 1.7 0.82–3.62 11 22
Moldy hay or straw 12 1.4 0.68–2.68 8 1.1 0.50–2.48 23 10
Grain dust 17 1.3 0.70–2.21 12 1.1 0.57–2.15 32 22
Flour dust 18 2.1 1.14–3.76 13 1.9 0.98–3.74 19 18
Pine or fir dust 32 2.1 1.31–3.47 20 1.4 0.82–2.52 48 9
Birch dust 16 2.6 1.32–5.18 13 2.4 1.18–4.92 18 4
Hardwood dust 10 2.4 1.05–5.69 9 2.5 1.06–5.89 12 2
47
Paper dust 9 1.3 0.60–2.91 6 1.1 0.43–2.70 17 8
Textile dust 13 1.4 0.74–2.72 10 1.3 0.64–2.70 12 33
Radiation 6 0.9 0.36–2.28 5 0.9 0.32–2.28 16 8
Solvents 28 1.3 0.79–2.05 19 1.0 0.60–1.77 64 14
Fire fumes 8 2.9 1.10–7.58 5 2.3 0.74–6.97 9 0
Engine exhausts 24 0.9 0.54–1.50 15 0.7 0.39–1.27 74 11 Irritating gases (ammonia, chlorine dioxide, chlorine, sulphur dioxide)
13
1.5
0.79–3.00
10
1.5
0.71–3.06
22
10
Environmental tobacco smoke 53 1.0 0.71–1.45 40 0.9 0.61–1.36 117 90
Cutting oils/fluids 8 1.0 0.43–2.23 5 0.8 0.28–2.01 25 0 Rapid glues (Loctite, cyanoacrylates or Omnifit)
6
1.0
0.37–2.45
6
1.9
0.38–2.37
18
2

RESULTS
48
When we analyzed men and women separately with five or more exposed subjects to a group,
risks remained increased for IPF in men exposed to birch dust (OR 2.7, 95% CI 1.30–5.65)
and hardwood dust (OR 2.7, 95% CI 1.14–6.52). Men with IPF also had an increased OR
associated with birds (OR 2.7, 95% CI 1.00–7.06). There was no increased risk for any of the
exposure subgroups in women.
Ten patients with PF reported occupational exposure to hardwood dust. There was also
information about occupations in the questionnaire. The occupations with the longest duration
of exposure to hardwood dust were wood products machine operator, forester, cabinet
makers, machine operator, telephone service worker and blacksmith. There were also two
carpenters and two subjects who did not report their occupation.
We also analysed the material using a latency period of 10 years instead of 5 years, with
similar results. The same exposures were associated with increased risks, but the risks were
slightly higher. In order to explore a cohort effect, we ran the analyses with the population
divided into two groups according to the mean birth year, 1930. We found no clear indication
of any cohort effect.
With the logistic regression models, we observed similar results. Exposure to organic dust
(and wood dust) increased the risk of PF, especially among men. No significant associations
were found when we modelled IPF as the dependent outcome.
Table 11. Logistic regression models for the PF sample giving odds ratios (and 95% confidence intervals) adjusted for sex, smoking, year of birth and year of diagnosis.
Predictor All PF patients (n=181) Men Women
Inorganic dust 1.1 (0.70–1.68) 1.1 (0.70–1.83) 0.55 (0.12–2.53)
Organic dust 1.5 (1.00–2.15) 1.7 (1.06–2.8) 1.2 (0.60–2.22)
Metal dust 0.98 (0.61–1.58) 0.97 (0.58–1.63) 0.82 (0.17–3.82)
Wood dust 1.9 (1.12–3.15) 2.1 (1.22–3.75) 0.50 (0.06–4.11)

RESULTS
49
PAPER III – Ventilation or oxygen in kyphoscoliosis
More patients started LTOT alone than HMV during the whole study period (Figure 13).
Figure 13. The annual number of patients starting HMV or LTOT 1996-2004.
Thirty-two of the 100 (32%) patients on home mechanical ventilation and 110 of the 144
(76%) patients on oxygen therapy alone had died at follow-up. Age above 70 years, suffering
from concomitant respiratory disease, low PaO2 and low PCO2 were related to an increased
risk of early death in the univariate analysis.
Table 12. Univariate analysis of relative risk of death among patients with kyphoscoliosis. Hazard ratio 95% CI p-value Mechanical ventilation vs. oxygen therapy alone 0.22 0.15-0.33 < 0.001
Age > 70 years 3.34 2.31-4.82 < 0.001
Concomitant respiratory disease 2.43 1.72-3.44 < 0.001
Female sex 1.33 0.93-1.93 0.118
PaO2 (mm Hg)* 0.97 0.96-0.99 < 0.001
PaCO2 (mm Hg)* 0.98 0.96-0.99 < 0.01 *Continuous variables

RESULTS
50
Table 13. Multivariate analyses of relative risk of death among patients with kyphoscoliosis.
Hazard ratio 95% CI p-value
Oxygen therapy alone 1
Home mechanical ventilation 0.30 0.18-0.51 < 0.001
Age > 70 years 2.63 1.74-3.98 < 0.001
Female sex 1.27 0.85-1.92 0.24
Concomitant respiratory disease 1.43 0.96-2.12 0.078
PaO2 (mm Hg) 0.99 0.97-1.02 0.70
PaCO2 (mm Hg) 0.99 0.98-1.02 0.95
Patients treated with HMV experienced better survival rate than patients treated with oxygen
alone, even when adjusting for age, sex, concomitant respiratory diseases and blood gases.
Figure 14. Cumulative proportion of surviving patients receiving HMV or LTOT alone.

RESULTS
51
Survival time was longer in patients with a concomitant disease receiving mechanical
ventilation than in patients without a concomitant respiratory disease on oxygen therapy
(p=0.03):
Figure 15. Cumulative proportion of surviving patients receiving HMV or LTOT alone, subdivided according to the presence of concomitant respiratory disease.

RESULTS
52
PAPER IV - Quality in long-term oxygen therapy
Quality indicators at national level
We found improvements in eight of the ten quality indicators. The achievement of adequate
oxygenation (PaO2 > 8 kPa) when breathing oxygen was impaired and first-year survival rate
was unchanged.
Table 14. Achieved performance at national level in ten quality indicators according to the proposed levels for excellent quality, first and latest-year of use of indicator.
Quality indicator Proposed excellent quality level
Achieved performance level first-year cohort and latest-year cohort Year Level
Patient selection criteria
1. Access to LTOT (patients/100,000 inhabitants) > 30 1987) 7 2005) 31
2. PaO2 ≤ 7.3 kPa (% of patients) > 85 1987) 76 2005) 85
3. Non-smokers (% of patients) ≥ 95 1987) 96 2005) 99
4. LTOT patients with thoracic wall deformity without HMV (n) None 1993) 30
2005) 5 Performance of LTOT
5. PaO2 > 8 kPa on oxygen (% of patients) > 90 1987) 86 2005) 80
6. More than 16 hours per day (% of patients) > 95 1987) 91 2005) 97
7. Mobile oxygen equipment (% of patients) > 50 1989) 48 2004) 65
8. Reassessment of LTOT one to three months after initiation during a COPD exacerbation (% of patients) > 95 2002) 0
2005) 30 Concomitant treatment 9. Avoidance of continuous oral glucocorticosteroids in COPD (% of patients) ≥ 80 1987) 54
2005) 81 Result of treatment
10. First-year survival rate in COPD patients > 0.65 1987) 0.73 2004) 0.75
Access to therapy increased in terms of the number of patients on LTOT and there was a
decrease in the variations among the counties. On 1 January 1987, the number of ongoing
patients on LTOT varied between 1.3 and 19.6 per 100,000 (a factor of 15) in the different
counties, whereas on 31 December 2005 it varied between 21.0 and 76.0 per 100,000 (a factor

RESULTS
53
of 3.6.) At national level, the total number of LTOT cases increased from 565 to 2,871 per
these dates.
The dominant underlying diseases for respiratory failure were COPD and PF.
Figure 16. Number of new patients (n) with long-term oxygen therapy in 1987-2005 divided by reasons for hypoxemia. : Chronic obstructive pulmonary disease; : Pulmonary fibrosis; : Thoracic cage deformity; : Other diseases.
The first-year survival rate in COPD patients did not change.
Figure 17. First-year survival rate in patients with COPD according to year of start of LTOT.
RESULTS
54
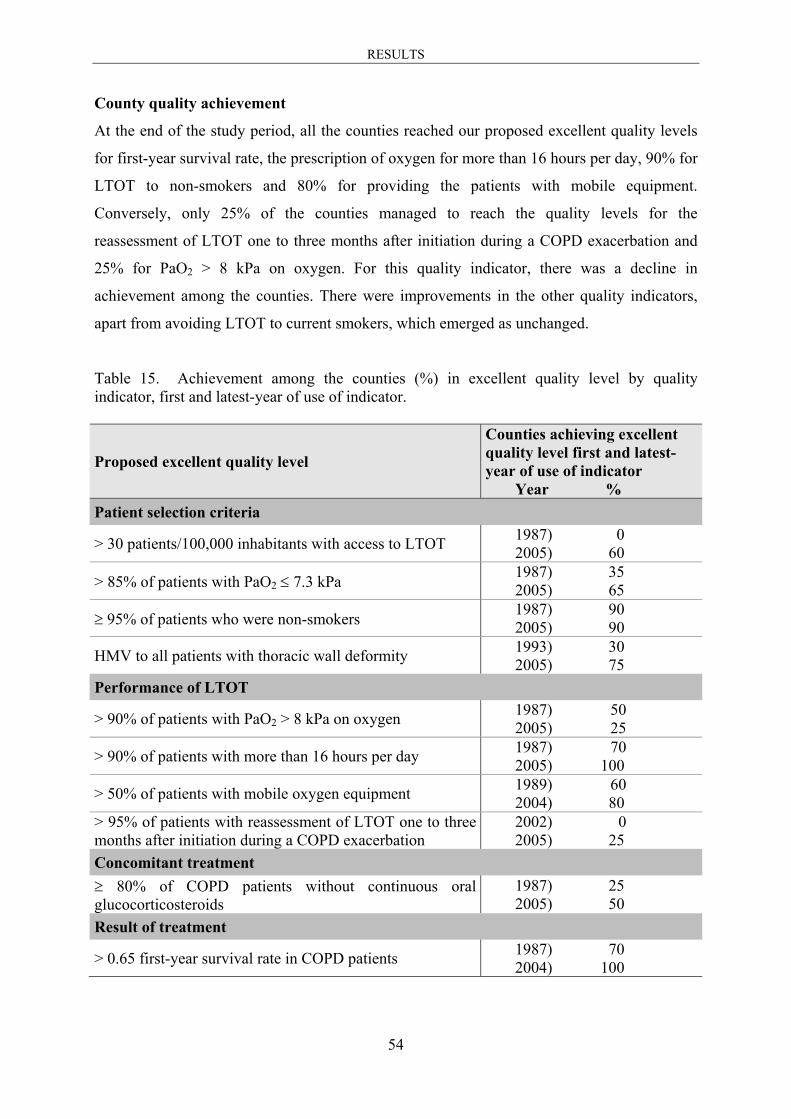
County quality achievement
At the end of the study period, all the counties reached our proposed excellent quality levels
for first-year survival rate, the prescription of oxygen for more than 16 hours per day, 90% for
LTOT to non-smokers and 80% for providing the patients with mobile equipment.
Conversely, only 25% of the counties managed to reach the quality levels for the
reassessment of LTOT one to three months after initiation during a COPD exacerbation and
25% for PaO2 > 8 kPa on oxygen. For this quality indicator, there was a decline in
achievement among the counties. There were improvements in the other quality indicators,
apart from avoiding LTOT to current smokers, which emerged as unchanged.
Table 15. Achievement among the counties (%) in excellent quality level by quality indicator, first and latest-year of use of indicator.
Proposed excellent quality level
Counties achieving excellent quality level first and latest-year of use of indicator Year %
Patient selection criteria
> 30 patients/100,000 inhabitants with access to LTOT 1987) 0 2005) 60
> 85% of patients with PaO2 ≤ 7.3 kPa 1987) 35 2005) 65
≥ 95% of patients who were non-smokers 1987) 90 2005) 90
HMV to all patients with thoracic wall deformity 1993) 30 2005) 75
Performance of LTOT
> 90% of patients with PaO2 > 8 kPa on oxygen 1987) 50 2005) 25
> 90% of patients with more than 16 hours per day 1987) 70 2005) 100
> 50% of patients with mobile oxygen equipment 1989) 60 2004) 80
> 95% of patients with reassessment of LTOT one to three months after initiation during a COPD exacerbation
2002) 0 2005) 25
Concomitant treatment ≥ 80% of COPD patients without continuous oral glucocorticosteroids
1987) 25 2005) 50
Result of treatment
> 0.65 first-year survival rate in COPD patients 1987) 70 2004) 100

55
DISCUSSION OF METHODOLOGY
A national quality assurance register, as the Swedish Oxygen Register and the Swedish Home
Mechanical Ventilation Register, now merged to become Swedevox, offers the advantage of
following the diagnosis and treatment outcome in the vast majority of patients over a long
period of time, making it possible to compare the medical service among the reporting units.
There are two major drawbacks to register studies: patients are not randomised to treatment
mode and there is no control group. The treatments among the patients in a register are
decided on the basis of the preferences of the doctor and patient. However, there is also an
advantage: the patients in the registers do not represent a small selected group, but rather the
majority of the Swedish patients as in this case treated with LTOT and HMV. Therefore, a
study based on data from the Swedish Oxygen Register gives different information than the
NOTT and MRC studies,14,15 since many of our patients would have been excluded from
those studies.
A quality register runs the risk of bias from under-reporting. For the Oxygen Register, an
external validation comparing patient registrations with data from manufacturers and
pharmacies was performed in 1986-1987.2 This validation showed that the coverage of the
register was 85%. Later, an internal validation of the coverage of registration was performed
approximately every second year by sending questionnaires to participating clinics.
We do not believe that there were selective reporting losses to the Oxygen Register, since the
interruptions in reporting applies to the entire counties, and were caused by shortages of staff.
For example from 1987 until 2000, in periods there were no reports from four counties. We
have not performed any analysis of dropout rates, but we advised the units against reporting
only surviving patients, when average coverage reporting resumed from a county.
The unique Swedish census registration numbers enable linkage with other registers that are
important for follow up and analyses, especially the Swedish Population Register for vital
status.113 This system may not altogether cover follow up correctly, owing to some difficulties
in the census registration number system. Statistics Sweden estimates, for example, that some
4,000 personal identification numbers are annually “recycled” from a small number of
persons. Also, some people emigrate without informing the authorities. Consequently, it is

DISCUSSION
56
sometimes difficult to obtain the correct date of death. Before the introduction of the web-
based registration system in 2004, the register forms occasionally contained an erroneous
census registration number. The patients have been known and followed by the reporting
clinic, which have reported the date of death or date of withdrawal for other reasons for these
patients. The number of erroneous census registration numbers was less than 1%. In all, we
believe that the cases without follow up have been few and may only have resulted in
negligible errors. Data collection is promoted by the uniformly organised medical care system
in Sweden and by the good quality of official statistics related to medical diagnoses,
treatments and causes of deaths.
How to improve quality of LTOT
One of the main objectives for a quality assurance register is to promote the improvement of
quality of care, e.g. patient selection and performance of treatment by feed back to the
reporting centers. To achieve this goal we have held annual meetings for the responsible
physicians and nurses since the start of the Swedish Oxygen Register 1987, where they also
received reports on the Swedish Home Mechanical Ventilation Register since its start in 1996.
Since 2004, data from the merged register Swedevox is entirely web-based, and the reporting
clinics have continuous access to their reported data. The annual reports and quality indicators
are accessible to each participating clinic and, when relevant, to the public. Some indicators
from small counties are subject to large annual variation and are therefore not accessible to
the public on an annual basis.

57
DISCUSSION OF MAIN RESULTS
Sex-related differences in LTOT in COPD
Our results indicate that over the next 20 years there will be an increasing female dominance
in patients receiving LTOT for chronic hypoxemia attributable to COPD. We estimate that in
Sweden in 2026, more than twice as many women as men will be on LTOT to treat COPD
with chronic hypoxemia. This assumption is based on our findings that incidence and
prevalence of LTOT increased among women as compared with men over 15 years, and on
the present smoking habits of middle-aged women and men. We believe that the increase in
prevalence of LTOT in women as compared with men will be more pronounced than the
increase in incidence, since we found significantly lower mortality after start of LTOT in
women than men in our study.
Several studies have demonstrated that women are more sensitive than men to the harmful
effect of tobacco smoke.51,54,114-116 It has long been known that there are sex-related
differences in the natural behaviour of the airways during a person’s life span, both in
biological and socio-cultural respects.117 Starting smoking in childhood is especially serious,
since it increases the likelihood of becoming a persistent adult smoker, and thus the risk of
developing obstructive airway disease.115 Moreover, lung function develops more slowly in
smoking girls than in smoking boys, and women who begin to smoke in childhood experience
a greater risk of lung function reduction and obstructive airway disease later than men who
smoke from childhood.114,115
Women may also be more susceptible than men to the development of severe COPD.
A study of patients with severe, early onset COPD revealed that current or ex-smoking female
first-degree relatives of these patients had a greater risk of reduction of FEV1 and of relevant
response to bronchodilator than male relatives.54 Analysis of data in two independent
population studies showed that smoking women ran a higher risk than smoking men of
needing admittance to hospital for COPD,51 but this finding was not reproduced in the
Confronting COPD International Survey.118 A Spanish investigation of COPD patients who
attended a pulmonary clinic, 53 FEV1-matched men and women, showed that the women
were younger and smoked less than the men.119 The women had more exacerbations in the
last year, poorer performance in walking distance and worse quality-of-life scores than the
DISCUSSION
58
men. Our new finding indicates that smoking women are substantially more likely than
smoking men to develop respiratory failure that necessitates LTOT.
We found a higher survival rate in women than in men after the start of LTOT. First-year
survival rate was 77% (95% CI 75–79%) and 69% (95% CI 67–71%), respectively, and
median survival rate was 2.8 years in women and 2.0 years in men. Similar survival data were
noted in an Australian study of 249 men and 256 women with COPD or chronic airflow
limitation treated with long-term oxygen.104 Their overall first-year survival rate was 75% and
median survival rate was 28 months in women and 22 months in men. Three other studies
reported higher survival rates after the onset of oxygen therapy. Miyamoto et al. found, in a
large study, a mean survival rate of 5.2 ± 0.2 years among women and 4.8 ± 0.2 in men after
the start of LTOT.4 Their first-year survival rates were 93.3% for women and 90.0% for men.
In a study by Chailleux et al. on the French quality register ANTADIR Observatory, the mean
survival time for COPD patients on LTOT was three years.5 Machado et al. found, in contrast
to several other authors, a higher risk of death among women than men with oxygen-
dependent COPD.56
When interpreting these results, patient selection and sex distribution among patients should
be taken into account. Women represented 51% of the subjects both in our study and in the
study by Crockett at al., while only 25% of the participants were women in the Japanese
study.4,104
The similarity in the results between our study and the Australian study104 can partly be
explained by the fact that all patients receiving LTOT were included in these studies, in
contrast to the studies by Chailleux et al and Miyamoto et al., who excluded patients for
various reasons and had higher survival rates.4,5
When patients with a poor WHO performance status were excluded from the Swedish
Oxygen Register, similar survival time as in the randomized controlled studies14,15 and in the
studies on Japanese and French LTOT patients4,5 was found.105
On the other hand, the daily hours of oxygen use should also affect the survival time,
according to the results in the “NOTT” study, where treatment 24 hours per day was more
effective than 12 hours per day.14 In the Japanese study, 63% of the patients were prescribed
oxygen for at least 20 hours per day,4 as compared with only 30% of the patients in our study.
This could very well contribute to the lower survival rate for our patients. The lower survival

DISCUSSION
59
rate in our material probably depends both on the inclusion of all patients, regardless of
performance status, and the shorter treatment time with oxygen per 24 hour period.
The mathematical model used to predict the future incidence and prevalence of LTOT in
COPD is based on two assumptions: the age at the start of LTOT is stable and quitting
smoking will not affect the model. The mean age at the start of LTOT increased gradually in
the period 1987-2005. We are happy enough to have a high smoking cessation rate.58 A high
cessation rate in patient cohorts reaching the age of 60-80 years during the period 2007-2035
will probably reduce or postpone the onset of chronic hypoxemia and need of LTOT in this
group.
As previously mentioned, the national ratio of prevalence of smoking in younger women to
that of older women is thought to be an indicator of the future prevalence of smoking in that
country.59 Despite this uncertainty, the increased sensitivity of the female lung to tobacco
smoke and the high numbers of smoking women will lead to an increased need for LTOT in
the future, which will probably be even more pronounced worldwide than in Sweden, if our
predictions prove correct.43,44,120
Methodological considerations
The future incidence and prevalence of LTOT in COPD may develop in other directions than
predicted if various conditions turn out to be other than anticipated using our method. Lower
incidence and prevalence may occur if smoking decreases more rapidly than we believe and if
prevention and treatment of COPD improves more rapidly than it has so far. The prevalence
of LTOT may increase if cardiovascular mortality continues to decrease,121,122 if the attention
to respiratory failure increases and if the LTOT becomes more effective with increased hours
of oxygen per day.14

DISCUSSION
60
Occupation and pulmonary fibrosis
We report the association in men between IPF and exposure to birch dust and hardwood dust
as the main finding in our case-control study. The risk of IPF with these exposures was more
than doubled, and the risk of PF, without exclusion of cases with other probable reason for
fibrosis, was doubled in men with exposure to unspecified wood dust. In addition to birch
dust and hardwood dust, the patients with PF, men and women together, also had increased
odds ratios for blasting, mineral dust, birds, flour dust, and dust from pine or fir and fire
fumes.
We studied a different selection of cases than in the previous case-control studies, namely
severe PF including IPF as the largest subgroup. In this procedure, we could estimate the risk
of the studied exposures in the patients with already known external cause of their PF,
asbestos being the most common, and other diseases known to be associated with PF,
rheumatoid arthritis being the largest group. The previous case-control studies on risk of
environmental exposures did not include patients with other forms of ILD than IPF.69-74 We
found associations with more exposures in PF than in IPF, namely: blasting, mineral dust,
birds, flour dust, dust from pine or fir, birch dust, hardwood dust and fire fumes. The
increased odds ratios for blasting and mineral dust might represent undiagnosed silicosis. It is
also possible that some of the patients with known cause of PF actually had IPF, since IPF is
the most common of the idiopathic interstitial pneumonias.63,123 The cohort we studied was a
national sample of PF patients in advanced stage with chronic hypoxemia. They represent 8-
9% of the Swedish patients with ongoing LTOT for chronic hypoxemia, the second largest
group after COPD. As expected, the majority of the PF patients in our study, 77%, had
IPF.63,123 The fibrosis in PF patients was explained by external agents in 8% and by
association with other disease in 15%. Yet it is possible that some of the remaining 23% also
had IPF, since IPF is not only the most common ILD but also the most serious one.123 The
diagnosis of IPF was based on other data than lung biopsy in the majority of our patients, as
in a recent study from the UK on incidence and mortality of IPF.64
The main difference between our results and those of previous studies of environmental
exposure in IPF was that we did not find an increased risk with exposure to metal dust as was
found in five other case-control studies.69-71,73,74 In a UK study on standardised mortality
ratios, no association with exposure to metal dust was found.124 The patients in our cohort
may have been less severely exposed to dust from hard metal and they may have had less

DISCUSSION
61
harmful working environments than the patients in previous studies. A difference in patient
selection may also have played a role. Our patients represented a national sample and were
not recruited from a specific region, as in two of the other case-control studies.69,71
Methodological considerations
The cases in the PF sample, which included the IPF sample, were selected in the sense that
they represented a late stage in the disease and that current smoking was an exclusion
criterion, when they were prescribed LTOT. On the other hand, the cases were recruited from
the whole country, and can thus be assumed to be representative of Swedish patients with IPF,
with knowledge of the poor prognosis of that disease. In a retrospective case-control study
like this one, there is a risk of recall bias. People with a disease may be more inclined to recall
certain exposures than control persons without the disease.125 This problem could be solved
by interviews from experts to achieve higher accuracy, but for practical and financial reasons
that is not possible in a large study like this.126 Among people with respiratory disorders,
higher sensitivity and lower specificity have been demonstrated than in persons without
respiratory problems to self-reported dust or gas exposure.127 For common exposures, as in
our study, bias in terms of sensitivity is more important than bias specificity to cause
misclassification.128 We have found support for the validity of the self-reported exposures
when comparing with details about occupations among the ten patients who reported exposure
to dust from hardwood. An even more accurate check of validity of the reported exposures
could be achieved by using a job exposure matrix, as in a recent study on adult asthma
incidence.129

DISCUSSION
62
Ventilation or oxygen in kyphoscoliosis
The results of our prospective study from two national quality assurance registers suggest that
HMV is a more effective improver of survival rates than LTOT alone in patients with
respiratory failure owing to kyphoscoliosis. Our results also indicate that survival rate is not
influenced by the degree of hypoxemia or hypercapnia, once corrected with HMV or a
combination of HMV with LTOT. The presence of concomitant respiratory disease, in 66% of
the patients, mainly COPD, does not seem to have as negative an impact on survival time as
found in two previous studies.5,6
There is abundant documentation on the effectiveness and uses of mechanical ventilation in
kyphoscoliosis.83,89,92,130 It’s utility has also been demonstrated in a French survey.5
Consequently, home mechanical ventilation and not LTOT is the recommended treatment for
hypercapnic respiratory failure, as seen in kyphoscoliosis.97 There is no documentation that
supports treatment with oxygen to these patients. The reasons for which a considerable
proportion of the Swedish kyphoscoliotic patients are treated with LTOT instead of HMV
might be that the responsible physicians have assessed the concomitant disease as mainly
responsible for the respiratory failure, and the hypoxemia has been regarded as more serious
than the hypercapnia. However, our results show that this treatment strategy is erroneous in
patients with kyphoscoliosis and respiratory failure. The hypoventilation or impending
hypoventilation is the greatest risk factor and should always be corrected first.
Concomitant respiratory disease is common in patients with kyphoscoliosis5,6 and this may be
partly explained as an airway complication attributable to small lung volume.80,81 Recent
research demonstrates that a restriction of lung volume and chronic breathing at low lung
volumes might increase the rate of stress generation in airway smooth muscle,82 as has also
been demonstrated in mechanical strain in cultured airway smooth muscle cells.131 In obese
patients there is an increased prevalence of wheezing and airway hyperresponsiveness81,132-134
and several studies have observed an association between high body mass index and
asthma.135-141 Patients with kyphoscoliosis breathe at low lung volumes, which might explain
the high frequency of airway disease in patients with kyphoscoliosis and respiratory failure,80
as in patients with lung function affected by chronic cervical spinal cord injury.142
Furthermore, airway obstruction in kyphoscoliosis can also be caused by bronchial torsion
secondary to the thoracic deformity.143
DISCUSSION
63
Among the kyphoscoliotic patients treated with LTOT, 54% had a diagnosis of COPD, and
only 75% of these patients with kyphoscoliosis and COPD had ever smoked. This finding
supports the hypothesis that the kyphoscoliosis or relatively low lung volumes might explain
some of the airways disease diagnosed as COPD and thought to motivate LTOT.80
Improvement in vital capacity and arterial blood gas oxygen has been shown to occur when
patients with kyphoscoliosis are treated with nocturnal nasal intermittent positive pressure
ventilation.92
The strongest confounding factor in our study was the older mean age in the LTOT group.
When entered in a multiple regression analysis, age and treatment turned out to have
independent impacts on survival time. When considered alone, hypoxemia and concomitant
respiratory disease was associated with poorer survival time, but since these factors were
closely related to advanced age, they lost their statistical significance when entered in the
multivariate analysis. Moreover, survival time was not affected by levels of carbon dioxide or
vital capacity. No effect of initial PaO2 is expected, since both therapies aim at correcting
hypoxemia. Since nocturnal mechanical ventilation corrects daytime hypercapnia,91 which
was most pronounced in the HMV groups, any negative effect of hypercapnia on survival
time is abolished by this treatment. The prognosis for patients with a combination of HMV
and LTOT was about the same as with HMV alone, which is in accordance with the results of
Buyse et al. in a study on a smaller patient material.92
Methodological considerations
A joint register would have strengthened our results, but since the two registers have been
supervised by the same scientific society and in most instances receive reports from the same
clinicians, we believe that our results give a true description of the outcome for the two
treatment modalities. Our study is not randomised or controlled, which would probably not be
ethically possible in relation to this problem.92 The patients were actually selected for one of
the studied treatment methods. Patients prescribed LTOT and HMV differed at the start of
treatment for respiratory failure, the main difference being that patients prescribed LTOT had
a mean age of twelve years older. They also had more pronounced hypoxemia and less
hypoventilation or hypercapnia than the patients prescribed HMV. They also had slightly
higher vital capacity. Clearly, LTOT was selected for a subset of patients with more
hypoxemia than explained by hypoventilation only, and hypercapnia was an indication for
starting HMV. Yet the results of this study demonstrate that when the main disease is a severe

DISCUSSION
64
thoracic spine deformity, patients receiving HMV have a better outcome than patients on
LTOT, and our results add support to the consensus statement on therapy in kyphoscoliosis.97

DISCUSSION
65
Quality in long-term oxygen therapy
We found improvement in eight of the ten quality indicators which we had selected for follow
up during the 19 years of quality registration. Patient selection was improved regarding access
to therapy, and there was an increase in the proportion of patients with severe hypoxemia and
a decrease in the proportion of current smokers. There were improvements both on the
national level and in the individual counties. Yet, there was a worsening in terms of achieving
the treatment goal of oxygenation with supplementary oxygen. That quality indicator was
poorly fulfilled at the end of the observation period as was the activity of reassessment of
LTOT when it was started during an exacerbation of COPD. However, the latter quality
indicator was introduced late in the observation period and improvement might have been
slow. From the start of the study the register data was used for feed back to the responsible
physicians and nurses in annual reports and at training meetings. In this way, the register has
served as a benchmarking tool for quality assurance, as can be seen in that there were
improvements in most of the quality indicators.
Patient selection in LTOT
Initiation of LTOT increased considerably during the study, almost entirely on the indication
of COPD. The reason for this is probably increased attention to patients requiring LTOT and
the time course of smoking habits rather than selection of patients with doubtful indications,
since the proportion of patients with severe hypoxemia increased. A Danish study showed
increased prevalence of LTOT to COPD patients from 27 per 100,000 inhabitants in 1994 to
42 per 100,000 in 2000.144 The highest prevalence was found in the counties where general
practitioners took part in the prescription of LTOT, and the adherence to the criteria for the
treatment was lower in those counties. In our study, all responsible physicians, mainly
pulmonologists, were specially trained for LTOT. We found a fourfold variation between the
counties in the incidence of LTOT prescriptions in 2005. Differences in attention could
possibly contribute to this, but the differences are probably caused by variations in respiratory
failure owing to smoking related diseases, as can be seen by the fact that there was also a
fourfold variation in the incidence of lung cancer in Sweden, according to the Cancer Register
of the National Board of Health and Welfare.145
There was an adherence to the indicator severe hypoxemia when breathing room air of 76% in
the patients who were prescribed LTOT from the beginning of the study, and this rose to 85%.
The adherence to the Swedish guidelines for LTOT is likely to have been higher, since some

DISCUSSION
66
of the patients with PaO2 > 7.3 kPa probably had pulmonary hypertension or polycythemia as
an additional reason for LTOT. In a Danish study on COPD patients receiving LTOT, 462 of
822 (56%) patients had adherence to the criteria for hypoxemia.146 There were no data on
PaO2 on room air in 169 of the patients and there was adherence to the hypoxemia criteria in
70.6% of the other 653 patients. The limit at which LTOT is effective in treating hypoxemia
is addressed as a research field in a recent NHLBI workshop report.36 The report emphasizes
that the average use of oxygen was only 13.5 hours per day in the study by Górecka et al.,
which may have lowered the possibility of establishing an effect on survival time in mild to
moderate hypoxemia, and that LTOT might have other effects than prolonged survival time in
these patients.
The Swedish guidelines include a strong recommendation that LTOT should be avoided in
patients who have not stopped smoking. The reason is that smoking probably interferes with
the treatment result and that there is a risk of fire accidents.94-96 Current smokers have
increased mortality during LTOT,3 but it is still possible that LTOT is beneficial on survival
time in these patients. This is an ethical issue for further investigation according to the
NHLBI workshop.36
At the end of our study, as many as 99% of the patients were non-smokers when starting
LTOT. This adherence to guidelines for LTOT has varied in other countries between 49% in
the US and 93% in Turkey.147,148 Other examples of proportion of non-smoking LTOT
patients are 79% in Denmark and 86% in Scotland.108,110
When respiratory failure is caused by deformity of the thoracic cage, LTOT is often
prescribed, especially when there is a concomitant respiratory disorder.2,3,5,6,149 However,
HMV is physiologically more effective in these patients.83-89 Home mechanical ventilation
alone is sufficient in some cases, but LTOT alone results in a poorer survival rate.92,149
After the presentation of the results of Paper III, the prescription of LTOT alone to patients
with deformity of the thoracic cage dwindled to a few registered cases annually in Sweden.
Performance of LTOT
Attaining the desired level of PaO2 when breathing oxygen was the only quality indicator that
decreased during the study (from 86% to 80%). This was not explained by insufficient PaO2
in the patients with PF, in whom it can otherwise be difficult to reach appropriate oxygenation
levels. Nor was it explained by an increase in the mean PaCO2 from 1987 to 2005 on oxygen

DISCUSSION
67
in the LTOT patients. Yet another explanation could be insufficient titration of the oxygen
dosage, owing to shortening of the times for in-hospital treatment. In previous studies, the
adherence to improvement of the arterial oxygenation guidelines when breathing oxygen was,
for example, 45% in a Scottish study and 90% in an Australian study.110,150
Prescription of oxygen for more than 16 hours per day was high from the start in our study,
and improved further. It is possible that this was influenced by increased usage of portable
oxygen equipment.98,99,151 In a Greek study, only 27% of the patients with LTOT used oxygen
for more than 15 hours daily, as compared with 65% of the patients in a Danish study.99,152
We have studied the prescribed treatment time per day, rather than use of oxygen in reality,
since compliance has been deemed too difficult to follow in our large patient material, and
would seriously affect the possibilities for the staffs to report to the register. In an early
observation in the Swedish Oxygen Register, measuring of oxygen cylinder use and reading
of concentrator meters showed that approximately 70% of patients used oxygen for 15 hours
or more per day.3 Compliance of 65% with the treatment time > 15 hours per day was
demonstrated in both a Danish and a Dutch study.99,153 The use of mobile oxygen equipment
influenced compliance in both of these studies.
Adequate treatment time per day is important to the effects of LTOT in terms of survival
times,14,15 and mobile oxygen equipment has been shown to be important to enable patients
with outdoor activity, to have improved compliance.98 The use of mobile oxygen equipment
increased from 48% to 65% of the patients in our study between 1989 and 2004. The
corresponding figures have been between 20% and 67% in other countries.153-155 During the
same period, the oxygen equipment has also undergone developments, with lightweight
cylinders and demand pulsing delivery devices, making it easy to handle.156 We did not
measure the patients’ use of their mobile equipment, but according to the results in previous
studies, there is reason to suppose some degree of reduced compliance with the use of the
equipment.151,153
When severe hypoxemia occurs during an exacerbation of COPD, it may often be necessary
to initiate LTOT despite there not being a stable phase in the underlying disease. Reversal of
hypoxemia may take several weeks so initiating LTOT earlier has become more common
with earlier discharges from hospital.19,100,101 This early LTOT has been prescribed in such
cases for several years, and lately it has also been recommended in some guidelines.19,20

DISCUSSION
68
When LTOT is started during an exacerbation of COPD, it is recommended that the
indication be reassessed after one to three months.19,20 During the few years when we
registered adherence to the guidelines for this indicator, it increased from zero to 30% of the
relevant patients. In a Danish study from 1995, only 39% of the patients were followed up
properly after initiation of LTOT108 and the corresponding figure was 61% in a localised
British district in 1986-1987.157 Those studies dealt with all patients who received LTOT, and
to our knowledge, there is no other study of the follow up of only patients starting LTOT
during an exacerbation of COPD.
Concomitant treatment
A few studies have demonstrated increased mortality in COPD patients, associated with
maintenance therapy with oral glucocorticosteroids.102,103,158 In the study by Ström, female
COPD patients had increased mortality; in Ringbaek’s study the increased mortality was
limited to overweight COPD patients, while the increase in mortality was found to be dose
dependent for oral steroids in the study by Schols. Attention has been paid to this risk since
many years in Swedish COPD patients and the use of oral glucocorticosteroids decreased
from 46% to 19% during our study period. In some of these elderly patients, the indication for
corticosteroid maintenance therapy may well be other diseases than COPD.
Results of treatment
In our 19 year observation of COPD patients receiving LTOT, we found a stable level of the
first-year survival rate. We chose that measure for practical reasons. When comparing with
the national Causes of Death Register data, we did not find any significant change in overall
survival. It might be expected that improvements over the years in the performance of LTOT
would lead to somewhat improved survival times. One explanation for the fact that this did
not occur is probably that the patients have become steadily older at start of LTOT, which
could, in turn, be a result of improved overall care, with postponement of respiratory failure.
The decrease of smoking in the population during recent decades can also have influenced the
later start of respiratory failure. It is also possible that the prescription of oxygen for a
minimum of 16 hours per day results in many patients not striving to use oxygen for up to 24
hours per day. A continuous treatment 23-24 hours per day probably improves survival times
more than 15-16 hours per day in COPD patients with severe hypoxemia.14,15 Patients in our
study were older and patients with a very poor performance status or concomitant disease

DISCUSSION
69
were not excluded as in the NOTT and MRC studies,14,15,159 a fact that probably affected our
survival statistics.
Methodological considerations
We chose the ten quality indicators as a proposed instrument for accessing improvement of
LTOT, based on published evidence: PaO2 ≤ 7.3 kPa on air,14-16 HMV to patients with
thoracic deformity,92,97,149 PaO2 > 8 kPa on oxygen,14-16 more than 16 hours of oxygen per
day3,14,15 and reassessment of LTOT if started during a COPD exacerbation,19,100,101 and early
results on data from our register concerning access to LTOT,2 non-smoking status3 and
avoidance of continuous oral glucocorticosteroids in COPD.102,103,158 The suggested levels for
excellent quality of the indicators are based on the results in the individual counties and
reflect the current disease panorama and guidelines. Changes in epidemiology and scientific
progress will lead to a need for revision of the levels for excellent quality.36
70
CONCLUSIONS
Our results contribute to knowledge for preventing and postponing chronic obstructive
pulmonary disease (COPD) and idiopathic pulmonary fibrosis (IPF) and to improved quality
of treatment of respiratory failure.
Specific conclusions:
- Women with COPD experience a more rapid increase in incidence and prevalence for long-
term oxygen therapy (LTOT) than men with COPD.
- Exposure to wood dust, especially dust from birch and hardwood, may be a risk marker in
men for developing IPF.
- A substantial increase in the need for oxygen therapy will probably occur in women in the
immediate coming years.
- When they receive LTOT for COPD with severe hypoxemia, women have better survival
rates than men.
- Patients with kyphoscoliosis treated with home mechanical ventilation have better survival
rate than those treated with oxygen alone.
- We found improvements in eight of our ten quality indicators during 19 years of quality
registration. We propose a model for the quality assurance of LTOT, using indicators with
levels for excellent quality, based on our estimation of current knowledge.

71
FUTURE PERSPECTIVES
The two most important therapeutic implications of our studies are:
- Do not treat patients with respiratory failure due to kyphoscoliosis with oxygen alone.
- Encourage COPD patients with chronic hypoxemia to use the oxygen for as many hours as
possible during the every day and night.
The demonstrated female dominance in the increase of incidence and prevalence of LTOT
together with the increase in smoking in women as compared with men will constitute a
strong argument for increased efforts regarding smoking prevention and cessation. It is
important to target women for information and other measures to counteract the efforts by the
tobacco industry to recruit female smokers.160 Our model for prediction of future need for
LTOT can be validated by analyzing the future incidence and prevalence of LTOT.
The finding of wood dust as a probable risk marker for idiopathic pulmonary fibrosis (IPF)
will contribute to relevant preventive actions in manufacturing industries as well as in
handicrafts and private carpentries. It will be important to follow the future incidence of IPF,
and if it rises, it may be justifiable to repeat a case control study based on quality resister data
on risk markers for IPF. We also aim to evaluate cigarette smoking as a risk marker for IPF
by studying data on IPF patients reported to the Swedevox Register.161
Home mechanical ventilation (HMV) is the first line treatment when respiratory failure occurs
in patients with kyphoscoliosis. In selected cases, this treatment may be supplemented with
oxygen. After the presentation of Paper III to the participating centers the number of new
patients prescribed LTOT without HMV dropped to a few elderly patients who could not
learn to accept HMV. However, it is necessary to use data from the Swedevox Register to
assure that the prescription of LTOT without HMV to kyphoscoliotic patients stays on a low
level.
Evaluation of the implementation of the quality indicators for LTOT will serve as an
instrument for improvement of performance and outcome of LTOT. Scientific re-evaluation
of several of the indicators must be undertaken regularly to decide whether they should
remain as indicators or whether adjustments are needed.36 The optimal treatment time per 24

72
hours and the possible effect of LTOT in mild to moderate hypoxemia are areas that would
need further evidence.
Impaired health related quality of life is a very important aspect of respiratory failure and the
effect of LTOT has, so far, only been explored in a sample of our LTOT patients.31 Since
2006 we have included a short generic instrument for health related quality of life
measurement at the start and after the end of the first year of LTOT. The development of a
Swedish version of a specific instrument for health related quality of life in respiratory failure
will facilitate a better evaluation of the impact of treatment including the impact on LTOT in
this aspect.
The levels for excellent quality also need continuous updating according to new knowledge
and the changing epidemiology of respiratory failure.
73
ACKNOWLEDGEMENTS
First I want to express my gratitude to all those who developed the Swedish Oxygen Register and allowed me to analyze data from the Register - Kerstin Ström, my tutor, who developed the Register as one of the national quality registers, supported by the Swedish Board of Health and Welfare. You have generously supported me during many years, and you have shared your deep knowledge about long-term oxygen therapy with me. It has been a privilege for me to work with the register data under your supervision. Thank you for all enjoyable work meetings in Karlskrona, and for your and Thomas’ hospitality in your home at Långö! - The Swedish Society of Respiratory Medicine, the owner of the Register - The Swedish Heart-Lung Foundation, who supported the first Register and the transition of the Oxygen and HMV Registers to the web-based Swedevox Register - Jacob Boe, who initiated the Oxygen Register with a planned duration of five years - All colleagues in the Swedish Society of Respiratory Medicine and all “oxygen nurses” in Sweden who enthusiastically filled in all those report forms Karl Franklin, my co-supervisor, for all your generous support and for all the valuable advice in different aspects of my postgraduate studies. It is a pleasure to experience a speedy and effective transformation of a message in a text or a slide with your guidance Kjell Torén, my co-supervisor, for all your generous support and for everything you have taught me about occupational influences in pulmonary diseases. I have had several exciting weeks, working with our project at your institution. Thank you for all the lovely dinners in your home! Kurt Boman, my co-supervisor, for your all your generous support and helpful advice given at short notice whenever needed during work with my thesis. You introduced me to the science of magnesium in skeletal muscle many years ago. These studies were not possible to develop further, but we did not give up on my postgraduate studies Leif Rosenhall, my former Head of the Respiratory Department, for introducing me to respiratory medicine, for your wonderful leadership and for your friendship. Posthumous gratitude, I miss you very much Thomas Sandström, the head of the Umeå University Division of Respiratory Medicine and Allergy, for all your generous support and encouragement during this project and during my earlier study on magnesium and asthma Bengt Midgren, for co-authorship and for everything you have taught me in association with the Home Ventilator Register, nowadays Swedevox Kenneth Nilsson, for co-authorship and for all your generous support during many years of clinical work with interstitial lung diseases
74
Jonas Ranstam, for co-authorship and invaluable statistical advice Anna Dahlman-Höglund and Göran Tornling and Kerstin Löfdahl, for co-authorship Katarina Nylén, for all the encouragement you have given me to go on with this project, and for the care of many respiratory problems in our Department during my periods of absence Ellinor Ädelroth, the Head of the Department of Public Health and Clinical Medicine, for your periods providing back-up for me at our Outpatient Department, and for all your encouragement during this project and during many years prior to this All colleagues on the Department of Respiratory Medicine and Allergy at Umeå University Hospital, for your work with the respiratory problems in patients at Skellefteå hospital during my project. A special thanks to Håkan Törnqvist, for your periods of back-up for me at our Outpatient Department and to Eva Norrman; investigations around patients with tuberculosis can generate a lot of work Jan-Håkan Jansson, for all your much appreciated support on both details in this project as well as help in the clinical work Lars Johansson, for your generous support on details in this project and the many times that I have had computer problems Eva Åberg, the Head of Department of Medicine and Geriatrics, for allowing to me work with this project, for encouragement, and for working the years we have worked together in our Department Jeanette Kliger, Linda Schenck and Karin Axell, for your excellent linguistic revision Karin Burman and Lena Åström, for your important help with all practical items My dear family: Ulla, Jonas, Helena and Emma, for your patience with my absence from home in person or mentally. This was not a new phenomenon, but it has this time been worse than usual. The apartment on Språkgränd in Umeå has been a nice second home for me during the post graduate courses This work was generously supported by grants from the Swedish Heart-Lung Foundation, from the Västerbotten County Council and from the Foundation of Medical Research in Skellefteå The papers in this thesis have also been supported by grants from the Swedish National Board of Health and Welfare, the Blekinge County Council, and BREAS Medical AB.

75
REFERENCES
1 GOLD Executive Committee. Global Initiative for Chronic Obstructive Lung Disease,
2006. Available from: http://goldcopd.com/ (accessed 5 December, 2007)
2 Strom K, Boe J. A national register for long-term oxygen therapy in chronic hypoxia: preliminary results. Eur Respir J 1988; 1:952-958
3 Strom K, Boe J. Quality assessment and predictors of survival in long-term domiciliary oxygen therapy. The Swedish Society of Chest Medicine. Eur Respir J 1991; 4:50-58
4 Miyamoto K, Aida A, Nishimura M, et al. Gender effect on prognosis of patients receiving long-term home oxygen therapy. The Respiratory Failure Research Group in Japan. Am J Respir Crit Care Med 1995; 152:972-976
5 Chailleux E, Fauroux B, Binet F, et al. Predictors of survival in patients receiving domiciliary oxygen therapy or mechanical ventilation. A 10-year analysis of ANTADIR Observatory. Chest 1996; 109:741-749
6 Strom K, Pehrsson K, Boe J, et al. Survival of patients with severe thoracic spine deformities receiving domiciliary oxygen therapy. Chest 1992; 102:164-168
7 West J. Pulmonary pathophysiology – the essentials. Baltimore: Williams & Wilkins, 1987; 157-171
8 Corbridge T, Irvin CG. Pathophysiology of chronic obstructive pulmonary disease with emphasis on physiologic and pathologic correlations. In: Casaburi R, Petty TL, eds. Principles and practice of pulmonary rehabilitation. Philadelphia: W.B. Saunders Company, 1993; 18-32
9 Burrows B, Earle RH. Prediction of survival in patients with chronic airway obstruction. Am Rev Respir Dis 1969; 99:865-871
10 Barach A. The therapeutic use of oxygen. JAMA 1922; 79:693-699
11 Openbrier DR, Hoffman LA, Wesmiller SW. Home oxygen therapy. Evaluation and prescription. Am J Nurs 1988; 88:192-197
12 Petty TL, Finigan MM. Clinical evaluation of prolonged ambulatory oxygen therapy in chronic airway obstruction. Am J Med 1968; 45:242-252
13 Petty TL. Historical perspective on long-term oxygen therapy. In: O’Donohue W, ed. Long-term oxygen therapy. Scientific basis and clinical application. NewYork, NY: Marcel Dekker, 1995; 1-23
14 Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Nocturnal Oxygen Therapy Trial Group. Ann Intern Med 1980; 93:391-398

76
15 Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Report of the Medical Research Council Working Party. Lancet 1981; 1:681-686
16 Gorecka D, Gorzelak K, Sliwinski P, et al. Effect of long-term oxygen therapy on survival in patients with chronic obstructive pulmonary disease with moderate hypoxaemia. Thorax 1997; 52:674-679
17 Alton M, Andersson R, Boe J, et al. Pulmonell hypertension vid obstruktiva lungsjukdomar - orsaker, utredning och behandling. Läkartidningen 1985; 82:4399-4411
18 Dellborg M, Leksell L, Midgren B, et al. [Oxygen--when, why, how? Treatment of chronic hypoxia and other lung diseases]. Lakartidningen 1993; 90:3077-3078, 3083-3078
19 Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J 2004; 23:932-946
20 Nationellt vårdprogram för KOL, Kroniskt Obstruktiv Lungsjukdom, 2002. Available from: http://www.slmf.se/ (accessed 5 December, 2007)
21 Lofdahl K, Gustafson T, Franklin KA, et al. [Need of integrated guidelines for home oxygen therapy]. Lakartidningen 2007; 104:1902-1904
22 Fletcher C, Peto R, Tinker R, et al. The natural history of chronic bronchitis and emphysema. Oxford: Oxford University Press, 1976
23 Lange P, Groth S, Nyboe GJ, et al. Effects of smoking and changes in smoking habits on the decline of FEV1. Eur Respir J 1989; 2:811-816
24 Xu X, Weiss ST, Rijcken B, et al. Smoking, changes in smoking habits, and rate of decline in FEV1: new insight into gender differences. Eur Respir J 1994; 7:1056-1061
25 Sherrill DL, Enright P, Cline M, et al. Rates of decline in lung function among subjects who restart cigarette smoking. Chest 1996; 109:1001-1005
26 Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007; 356:775-789
27 Ström K. Respiratorisk insufficiens vid KOL. In: Larsson K, ed. KOL – Kroniskt obstruktiv lungsjukdom. Lund: Studentlitteratur, 2006; 385-392
28 McLaughlin VV, Presberg KW, Doyle RL, et al. Prognosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 2004; 126:78S-92S
29 Anthonisen NR, Wright EC, Hodgkin JE. Prognosis in chronic obstructive pulmonary disease. Am Rev Respir Dis 1986; 133:14-20
30 Sin DD, Man SF. Chronic obstructive pulmonary disease as a risk factor for cardiovascular morbidity and mortality. Proc Am Thorac Soc 2005; 2:8-11

77
31 Andersson A, Strom K, Brodin H, et al. Domiciliary liquid oxygen versus concentrator treatment in chronic hypoxaemia: a cost-utility analysis. Eur Respir J 1998; 12:1284-1289
32 Heaton RK, Grant I, McSweeny AJ, et al. Psychologic effects of continuous and nocturnal oxygen therapy in hypoxemic chronic obstructive pulmonary disease. Arch Intern Med 1983; 143:1941-1947
33 Lahdensuo A, Ojanen M, Ahonen A, et al. Psychosocial effects of continuous oxygen therapy in hypoxaemic chronic obstructive pulmonary disease patients. Eur Respir J 1989; 2:977-980
34 Okubadejo AA, Paul EA, Jones PW, et al. Does long-term oxygen therapy affect quality of life in patients with chronic obstructive pulmonary disease and severe hypoxaemia? Eur Respir J 1996; 9:2335-2339
35 Bradley JM, O'Neill B. Short-term ambulatory oxygen for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2005:CD004356
36 Croxton TL, Bailey WC. Long-term oxygen treatment in chronic obstructive pulmonary disease: recommendations for future research: an NHLBI workshop report. Am J Respir Crit Care Med 2006; 174:373-378
37 Nonoyama ML, Brooks D, Lacasse Y, et al. Oxygen therapy during exercise training in chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2007:CD005372
38 Nonoyama ML, Brooks D, Guyatt GH, et al. Effect of oxygen on health quality of life in patients with chronic obstructive pulmonary disease with transient exertional hypoxemia. Am J Respir Crit Care Med 2007; 176:343-349
39 Michaud CM, Murray CJ, Bloom BR. Burden of disease--implications for future research. Jama 2001; 285:535-539
40 Facts about chronic obstructive pulmonary disease (COPD). Centers for Disease Control and Prevention. Available from: http://www.cdc.gov/nceh/airpollution/copd/copdfaq.htm (accessed 5 December, 2007)
41 Pauwels RA, Buist AS, Calverley PM, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med 2001; 163:1256-1276
42 Lindberg A, Jonsson AC, Ronmark E, et al. Prevalence of chronic obstructive pulmonary disease according to BTS, ERS, GOLD and ATS criteria in relation to doctor's diagnosis, symptoms, age, gender, and smoking habits. Respiration 2005; 72:471-479
43 Guindon G, Boisclair. Past, current, and future trends in tobacco use: The World Bank, 2003. Available from: http://www1.worldbank.org/tobacco/publications.asp (accessed 5 December, 2007)
78
44 Murray C, Lopez A. Alternative visions of the future: projecting mortality and disability, 1990-2020. In: Murray C, Lopez A, eds. The Global Burden of Disease. The Harvard School of Public Health, on behalf of the World Health Organization and the World Bank, 1996; 361-395
45 Toll BA, Ling PM. The Virginia Slims identity crisis: an inside look at tobacco industry marketing to women. Tob Control 2005; 14:172-180
46 Carpenter CM, Wayne GF, Connolly GN. Designing cigarettes for women: new findings from the tobacco industry documents. Addiction 2005; 100:837-851
47 Warner KE, Goldenhar LM, McLaughlin CG. Cigarette advertising and magazine coverage of the hazards of smoking. A statistical analysis. N Engl J Med 1992; 326:305-309
48 Richmond RL. How women and youth are targeted by the tobacco industry. Monaldi Arch Chest Dis 1997; 52:384-389
49 Audrain-McGovern J, Rodriguez D, Patel V, et al. How do psychological factors influence adolescent smoking progression? The evidence for indirect effects through tobacco advertising receptivity. Pediatrics 2006; 117:1216-1225
50 DiFranza JR, Wellman RJ, Sargent JD, et al. Tobacco promotion and the initiation of tobacco use: assessing the evidence for causality. Pediatrics 2006; 117:e1237-1248
51 Prescott E, Bjerg AM, Andersen PK, et al. Gender difference in smoking effects on lung function and risk of hospitalization for COPD: results from a Danish longitudinal population study. Eur Respir J 1997; 10:822-827
52 Langhammer A, Johnsen R, Gulsvik A, et al. Sex differences in lung vulnerability to tobacco smoking. Eur Respir J 2003; 21:1017-1023
53 Gan WQ, Man SF, Postma DS, et al. Female smokers beyond the perimenopausal period are at increased risk of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Respir Res 2006; 7:52
54 Silverman EK, Weiss ST, Drazen JM, et al. Gender-related differences in severe, early-onset chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2000; 162:2152-2158
55 Wise RA. Changing smoking patterns and mortality from chronic obstructive pulmonary disease. Prev Med 1997; 26:418-421
56 Machado MC, Krishnan JA, Buist SA, et al. Sex differences in survival of oxygen-dependent patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2006; 174:524-529
57 Soriano JB, Maier WC, Egger P, et al. Recent trends in physician diagnosed COPD in women and men in the UK. Thorax 2000; 55:789-794
58 Daily smokers. Statistics Sweden 2007. Available from: http://www.scb.se/ (accessed 5 December, 2007)

79
59 2001 Surgeon General's Report—Women and Smoking, 2001. Available from: http://www.cdc.gov/tobacco/index.htm (accessed 5 December, 2007)
60 American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am J Respir Crit Care Med 2002; 165:277-304
61 American Thoracic Society. Idiopathic pulmonary fibrosis: diagnosis and treatment. International consensus statement. American Thoracic Society (ATS), and the European Respiratory Society (ERS). Am J Respir Crit Care Med 2000; 161:646-664
62 du Bois R, Wells A. Cryptogenic fibrosing alveolitis/idiopathic pulmonary fibrosis. Eur Respir J 2001; 18:Suppl. 32, 43s–55s
63 Noth I, Martinez FJ. Recent advances in idiopathic pulmonary fibrosis. Chest 2007; 132:637-650
64 Gribbin J, Hubbard RB, Le Jeune I, et al. Incidence and mortality of idiopathic pulmonary fibrosis and sarcoidosis in the UK. Thorax 2006; 61:980-985
65 Taskar VS, Coultas DB. Is idiopathic pulmonary fibrosis an environmental disease? Proc Am Thorac Soc 2006; 3:293-298
66 Hubbard R, Johnston I, Coultas DB, et al. Mortality rates from cryptogenic fibrosing alveolitis in seven countries. Thorax 1996; 51:711-716
67 Olson AL, Swigris JJ, Lezotte DC, et al. Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003. Am J Respir Crit Care Med 2007; 176:277-284
68 Coultas DB, Zumwalt RE, Black WC, et al. The epidemiology of interstitial lung diseases. Am J Respir Crit Care Med 1994; 150:967-972
69 Scott J, Johnston I, Britton J. What causes cryptogenic fibrosing alveolitis? A case-control study of environmental exposure to dust. Bmj 1990; 301:1015-1017
70 Iwai K, Mori T, Yamada N, et al. Idiopathic pulmonary fibrosis. Epidemiologic approaches to occupational exposure. Am J Respir Crit Care Med 1994; 150:670-675
71 Hubbard R, Lewis S, Richards K, et al. Occupational exposure to metal or wood dust and aetiology of cryptogenic fibrosing alveolitis. Lancet 1996; 347:284-289
72 Mullen J, Hodgson MJ, DeGraff CA, et al. Case-control study of idiopathic pulmonary fibrosis and environmental exposures. J Occup Environ Med 1998; 40:363-367
73 Baumgartner KB, Samet JM, Coultas DB, et al. Occupational and environmental risk factors for idiopathic pulmonary fibrosis: a multicenter case-control study. Collaborating Centers. Am J Epidemiol 2000; 152:307-315
80
74 Miyake Y, Sasaki S, Yokoyama T, et al. Occupational and environmental factors and idiopathic pulmonary fibrosis in Japan. Ann Occup Hyg 2005; 49:259-265
75 Mezon BL, West P, Israels J, et al. Sleep breathing abnormalities in kyphoscoliosis. Am Rev Respir Dis 1980; 122:617-621
76 Guilleminault C, Kurland G, Winkle R, et al. Severe kyphoscoliosis, breathing, and sleep: the "Quasimodo" syndrome during sleep. Chest 1981; 79:626-630
77 Sawicka EH, Branthwaite MA. Respiration during sleep in kyphoscoliosis. Thorax 1987; 42:801-808
78 Pehrsson K, Bake B, Larsson S, et al. Lung function in adult idiopathic scoliosis: a 20 year follow up. Thorax 1991; 46:474-478
79 Pehrsson K, Larsson S, Oden A, et al. Long-term follow-up of patients with untreated scoliosis. A study of mortality, causes of death, and symptoms. Spine 1992; 17:1091-1096
80 Irvin CG. Lung volume: a principle determinant of airway smooth muscle function. Eur Respir J 2003; 22:3-5
81 Litonjua AA, Sparrow D, Celedon JC, et al. Association of body mass index with the development of methacholine airway hyperresponsiveness in men: the Normative Aging Study. Thorax 2002; 57:581-585
82 McClean MA, Matheson MJ, McKay K, et al. Low lung volume alters contractile properties of airway smooth muscle in sheep. Eur Respir J 2003; 22:50-56
83 Zaccaria S, Ioli F, Lusuardi M, et al. Long-term nocturnal mechanical ventilation in patients with kyphoscoliosis. Monaldi Arch Chest Dis 1995; 50:433-437
84 Masa JF, Celli BR, Riesco JA, et al. Noninvasive positive pressure ventilation and not oxygen may prevent overt ventilatory failure in patients with chest wall diseases. Chest 1997; 112:207-213
85 Annane D, Quera-Salva MA, Lofaso F, et al. Mechanisms underlying effects of nocturnal ventilation on daytime blood gases in neuromuscular diseases. Eur Respir J 1999; 13:157-162
86 Dellborg C, Olofson J, Hamnegard CH, et al. Ventilatory response to CO2 re-breathing before and after nocturnal nasal intermittent positive pressure ventilation in patients with chronic alveolar hypoventilation. Respir Med 2000; 94:1154-1160
87 Bach JR, Robert D, Leger P, et al. Sleep fragmentation in kyphoscoliotic individuals with alveolar hypoventilation treated by NIPPV. Chest 1995; 107:1552-1558
88 Piper AJ, Sullivan CE. Effects of long-term nocturnal nasal ventilation on spontaneous breathing during sleep in neuromuscular and chest wall disorders. Eur Respir J 1996; 9:1515-1522

81
89 Gonzalez C, Ferris G, Diaz J, et al. Kyphoscoliotic ventilatory insufficiency: effects of long-term intermittent positive-pressure ventilation. Chest 2003; 124:857-862
90 Ferris G, Servera-Pieras E, Vergara P, et al. Kyphoscoliosis ventilatory insufficiency: noninvasive management outcomes. Am J Phys Med Rehabil 2000; 79:24-29
91 Laub M, Midgren B. The effects of nocturnal home mechanical ventilation on daytime blood gas disturbances. Clin Physiol Funct Imaging 2006; 26:79-82
92 Buyse B, Meersseman W, Demedts M. Treatment of chronic respiratory failure in kyphoscoliosis: oxygen or ventilation? Eur Respir J 2003; 22:525-528
93 Calverley PM, Leggett RJ, McElderry L, et al. Cigarette smoking and secondary polycythemia in hypoxic cor pulmonale. Am Rev Respir Dis 1982; 125:507-510
94 Muehlberger T, Smith MA, Wong L. Domiciliary oxygen and smoking: an explosive combination. Burns 1998; 24:658-660
95 Chang TT, Lipinski CA, Sherman HF. A hazard of home oxygen therapy. J Burn Care Rehabil 2001; 22:71-74; discussion 70-71
96 Lacasse Y, LaForge J, Maltais F. Got a match? Home oxygen therapy in current smokers. Thorax 2006; 61:374-375
97 Clinical indications for noninvasive positive pressure ventilation in chronic respiratory failure due to restrictive lung disease, COPD, and nocturnal hypoventilation--a consensus conference report. Chest 1999; 116:521-534
98 Pepin JL, Barjhoux CE, Deschaux C, et al. Long-term oxygen therapy at home. Compliance with medical prescription and effective use of therapy. ANTADIR Working Group on Oxygen Therapy. Association Nationale de Traitement a Domicile des Insuffisants Respiratories. Chest 1996; 109:1144-1150
99 Ringbaek T, Lange P, Viskum K. Compliance with LTOT and consumption of mobile oxygen. Respir Med 1999; 93:333-337
100 Levi-Valensi P, Weitzenblum E, Pedinielli JL, et al. Three-month follow-up of arterial blood gas determinations in candidates for long-term oxygen therapy. A multicentric study. Am Rev Respir Dis 1986; 133:547-551
101 Guyatt GH, Nonoyama M, Lacchetti C, et al. A randomized trial of strategies for assessing eligibility for long-term domiciliary oxygen therapy. Am J Respir Crit Care Med 2005; 172:573-580
102 Strom K. Survival of patients with chronic obstructive pulmonary disease receiving long-term domiciliary oxygen therapy. Am Rev Respir Dis 1993; 147:585-591
103 Ringbaek TJ, Viskum K, Lange P. BMI and oral glucocorticoids as predictors of prognosis in COPD patients on long-term oxygen therapy. Chron Respir Dis 2004; 1:71-78

82
104 Crockett AJ, Cranston JM, Moss JR, et al. Survival on long-term oxygen therapy in chronic airflow limitation: from evidence to outcomes in the routine clinical setting. Intern Med J 2001; 31:448-454
105 Ström K. Experience with an oxygen registry in Sweden. In: O’Donohue W, ed. Long-term oxygen therapy – scientific basis and clinical application. New York: Marcel Dekker, Inc., 1995; 331-337
106 Heffner JE, Ellis R. The guideline approach to chronic obstructive pulmonary disease: how effective? Respir Care 2003; 48:1257-1266; discussion 1267-1258
107 MacNee W, Calverley PM. Chronic obstructive pulmonary disease . 7: Management of COPD. Thorax 2003; 58:261-265
108 Ringbaek TJ, Lange P, Viskum K. Geographic variation in long-term oxygen therapy in Denmark : factors related to adherence to guidelines for long-term oxygen therapy. Chest 2001; 119:1711-1716
109 Gorecka D, Sliwinski P, Zielinski J. Adherence to entry criteria and one year experience of long-term oxygen therapy in Poland. Eur Respir J 1992; 5:848-852
110 Morrison D, Skwarski K, MacNee W. Review of the prescription of domiciliary long term oxygen therapy in Scotland. Thorax 1995; 50:1103-1105
111 Franklin KA, Gustafson T, Ranstam J, et al. Survival and future need of long-term oxygen therapy for chronic obstructive pulmonary disease--gender differences. Respir Med 2007; 101:1506-1511
112 Living conditions. Report No 105. Health related habits of life 1980–2002: Statistics Sweden, 2004
113 Population statistics. Statistics Sweden. Available from: http://www.scb.se/ (accessed 5 December, 2007)
114 Gold DR, Wang X, Wypij D, et al. Effects of cigarette smoking on lung function in adolescent boys and girls. N Engl J Med 1996; 335:931-937
115 Patel BD, Luben RN, Welch AA, et al. Childhood smoking is an independent risk factor for obstructive airways disease in women. Thorax 2004; 59:682-686
116 Watson L, Vonk JM, Lofdahl CG, et al. Predictors of lung function and its decline in mild to moderate COPD in association with gender: results from the Euroscop study. Respir Med 2006; 100:746-753
117 Becklake MR, Kauffmann F. Gender differences in airway behaviour over the human life span. Thorax 1999; 54:1119-1138
118 Watson L, Vestbo J, Postma DS, et al. Gender differences in the management and experience of Chronic Obstructive Pulmonary Disease. Respir Med 2004; 98:1207-1213

83
119 de Torres JP, Casanova C, Hernandez C, et al. Gender and COPD in patients attending a pulmonary clinic. Chest 2005; 128:2012-2016
120 Mannino DM. COPD: epidemiology, prevalence, morbidity and mortality, and disease heterogeneity. Chest 2002; 121:121S-126S
121 Koster M, Andersson J, Carling K, et al. [Mortality after myocardial infarction has decreased in nearly all Swedish counties during the 1990's. Greatest improvement seen in those counties with the worst initial results]. Lakartidningen 2003; 100:2838-2844
122 MONICAs hjärtinfarktregister 2007. Available from: http://www.umu.se/phmed/medicin/monica/ (accessed 5 December, 2007)
123 Raghu G, Weycker D, Edelsberg J, et al. Incidence and prevalence of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 2006; 174:810-816
124 Harris JM, Cullinan P, McDonald JC. Occupational distribution and geographic clustering of deaths certified to be cryptogenic fibrosing alveolitis in england and wales. Chest 2001; 119:428-433
125 Dawson B, Trapp RG. Basic & Clinical Biostatitics. New York: McGraw Hill, 2004; 338
126 Fritschi L, Siemiatycki J, Richardson L. Self-assessed versus expert-assessed occupational exposures. Am J Epidemiol 1996; 144:521-527
127 Bakke PS, Hanoa R, Gulsvik A. Relation of occupational exposure to respiratory symptoms and asthma in a general population sample: self-reported versus interview-based exposure data. Am J Epidemiol 2001; 154:477-483
128 Flegal KM, Brownie C, Haas JD. The effects of exposure misclassification on estimates of relative risk. Am J Epidemiol 1986; 123:736-751
129 Kogevinas M, Zock JP, Jarvis D, et al. Exposure to substances in the workplace and new-onset asthma: an international prospective population-based study (ECRHS-II). Lancet 2007; 370:336-341
130 Robert D, Gerard M, Leger P, et al. [Permanent mechanical ventilation at home via a tracheotomy in chronic respiratory insufficiency]. Rev Fr Mal Respir 1983; 11:923-936
131 Smith PG, Roy C, Dreger J, et al. Mechanical strain increases velocity and extent of shortening in cultured airway smooth muscle cells. Am J Physiol 1999; 277:L343-348
132 Pelosi P, Croci M, Ravagnan I, et al. Respiratory system mechanics in sedated, paralyzed, morbidly obese patients. J Appl Physiol 1997; 82:811-818
133 Ray CS, Sue DY, Bray G, et al. Effects of obesity on respiratory function. Am Rev Respir Dis 1983; 128:501-506
134 Shaheen SO. Obesity and asthma: cause for concern? Clin Exp Allergy 1999; 29:291-293

84
135 Fluge O, Omenaas E, Eide GE, et al. Fish consumption and respiratory symptoms among young adults in a Norwegian community. Eur Respir J 1998; 12:336-340
136 Shaheen SO, Sterne JA, Montgomery SM, et al. Birth weight, body mass index and asthma in young adults. Thorax 1999; 54:396-402
137 Camargo CA, Jr., Weiss ST, Zhang S, et al. Prospective study of body mass index, weight change, and risk of adult-onset asthma in women. Arch Intern Med 1999; 159:2582-2588
138 Romieu I, Avenel V, Leynaert B, et al. Body mass index, change in body silhouette, and risk of asthma in the E3N cohort study. Am J Epidemiol 2003; 158:165-174
139 Beckett WS, Jacobs DR, Jr., Yu X, et al. Asthma is associated with weight gain in females but not males, independent of physical activity. Am J Respir Crit Care Med 2001; 164:2045-2050
140 Chen Y, Dales R, Jiang Y. The association between obesity and asthma is stronger in nonallergic than allergic adults. Chest 2006; 130:890-895
141 Chen Y, Dales R, Tang M, et al. Obesity may increase the incidence of asthma in women but not in men: longitudinal observations from the Canadian National Population Health Surveys. Am J Epidemiol 2002; 155:191-197
142 Grimm DR, Arias E, Lesser M, et al. Airway hyperresponsiveness to ultrasonically nebulized distilled water in subjects with tetraplegia. J Appl Physiol 1999; 86:1165-1169
143 Al-Kattan K, Simonds A, Chung KF, et al. Kyphoscoliosis and bronchial torsion. Chest 1997; 111:1134-1137
144 Ringbaek TJ, Lange P. The impact of the Danish Oxygen Register on adherence to guidelines for long-term oxygen therapy in COPD patients. Respir Med 2006; 100:218-225
145 The National Board of Health and Welfare. The Swedish Cancer Registry. Available from: http://www.socialstyrelsen.se/Statistik/statistik_amne/Cancer/index.htm (accessed 5 December, 2007)
146 Ringbaek TJ, Viskum K, Lange P. Does long-term oxygen therapy reduce hospitalisation in hypoxaemic chronic obstructive pulmonary disease? Eur Respir J 2002; 20:38-42
147 Oba Y, Salzman GA, Willsie SK. Reevaluation of continuous oxygen therapy after initial prescription in patients with chronic obstructive pulmonary disease. Respir Care 2000; 45:401-406
148 Atis S, Tutluoglu B, Bugdayci R. Characteristics and compliance of patients receiving long-term oxygen therapy (LTOT) in Turkey. Monaldi Arch Chest Dis 2001; 56:105-109

85
149 Gustafson T, Franklin KA, Midgren B, et al. Survival of patients with kyphoscoliosis receiving mechanical ventilation or oxygen at home. Chest 2006; 130:1828-1833
150 Cranston JM, Nguyen AM, Crockett AJ. The relative survival of COPD patients on long-term oxygen therapy in Australia: A comparative study. Respirology 2004; 9:237-242
151 Vergeret J, Brambilla C, Mounier L. Portable oxygen therapy: use and benefit in hypoxaemic COPD patients on long-term oxygen therapy. Eur Respir J 1989; 2:20-25
152 Katsenos S, Froudarakis ME, Charisis A, et al. Long-term oxygen therapy in Ioannina. Respiration 2004; 71:619-624
153 Kampelmacher MJ, Van Kesteren RG, Alsbach GP, et al. Prescription and usage of long-term oxygen therapy in patients with chronic obstructive pulmonary disease in The Netherlands. Respir Med 1999; 93:46-51
154 Restrick LJ, Paul EA, Braid GM, et al. Assessment and follow up of patients prescribed long term oxygen treatment. Thorax 1993; 48:708-713
155 Schaanning J, Strom K, Boe J. Do patients using long-term liquid oxygen differ from those on traditional treatment with oxygen concentrators and/or compressed gas cylinders? A comparison of two national registers. Respir Med 1998; 92:84-87
156 Tiep B. Portable oxygen therapy with oxygen conserving devices and methodologies. Monaldi Arch Chest Dis 1995; 50:51-57
157 Walshaw MJ, Lim R, Evans CC, et al. Prescription of oxygen concentrators for long term oxygen treatment: reassessment in one district. Bmj 1988; 297:1030-1032
158 Schols AM, Wesseling G, Kester AD, et al. Dose dependent increased mortality risk in COPD patients treated with oral glucocorticoids. Eur Respir J 2001; 17:337-342
159 Ström K, Boman G, Herala M. Quality assurance based on the Swedish Oxygen Register of home oxygen therapy. In: Kira S, Petty TL, eds. Progress in Domiciliary respiratory Care - Current Status and perspectives. New York: Elsevier Science B.V, 1994; 161-168
160 Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet 2007; 370:765-773
161 Baumgartner KB, Samet JM, Stidley CA, et al. Cigarette smoking: a risk factor for idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 1997; 155:242-248