case report breast metastasis from hepatocellur carcinoma ... · pdf filebreast metastasis...
TRANSCRIPT
Int J Clin Exp Med 2017;10(2):3850-3854www.ijcem.com /ISSN:1940-5901/IJCEM0043535
Case Report
Breast metastasis from hepatocellur carcinoma: a case report and literature review
Jianbo Han1*, Fengwei Kong2*, Chunying Wang2*, Hai Ding1, Yufeng Zhang1, Junmao Liu1, Duxian Liu3, Yongxiang Yi1
Departments of 1Hepatobiliary Surgery, 3Pathology, The Second Hospital of Nanjing, Affiliated to Southeast University, Nanjing 210003, China; 2Department of General Surgery, Xuzhou Infectious Disease Hospital, Xuzhou 221000, China. *Equal contributors.
Received November 3, 2016; Accepted December 8, 2016; Epub February 15, 2017; Published February 28, 2017
Abstract: The incidence of breast metastasis from extramammary malignancy was rare. A case of breast metastasis from hepatocellular carcinoma (HCC) after partial hepatectomy and radical lymphadenectomy in a 49-year-old wom-an was reported. The breast metastasis from HCC was confirmed by immunohistochemistry. Therefore, metastatic breast HCC as end stage should be considered for patients who had liver cancer history and newly diagnosed breast lesions. And pre-operative biopsy was recommended to avoid unnecessary hepatectomy, as the patient attenuated quickly after surgery.
Keywords: Hepatocellular carcinoma (HCC), breast metastasis
Introduction
The incidence of intramammary metastasis from extramammary malignancy was rare, and the most common metastatic origins were mel-anoma and gastric carcinoma while pathologi-cal and clinical features may be helpful for the differential diagnosis [1, 2]. Metastases from extramammary malignancies to breast en- counter 0.5% of all breast tumors [3]. Besides, the incidence of extrahepatic metastasis of HCC was approximately 13% at 5 years after medical treatment, and the most common extrahepatic metastatic site was lung [4, 5]. Herein, a rare case of breast metastasis from HCC was presented and related literatures were reviewed.
Case presentation
A 49-year-old woman was admitted for a focal liver lesion detected by the ultrasound. Routine tests for hepatic, renal and coagulation func-tions were normal. Besides, the HBV test revealed positive serum HBsAg, HBeAg and HBcAb. HBV-DNA copies was 2.3 × 106 IU/ml. In addition, the serum level of alpha-fetoprotein (AFP) was slightly elevated as 21.9 ng/ml (nor-mal AFP < 10.9 ng/ml), and the other tumor
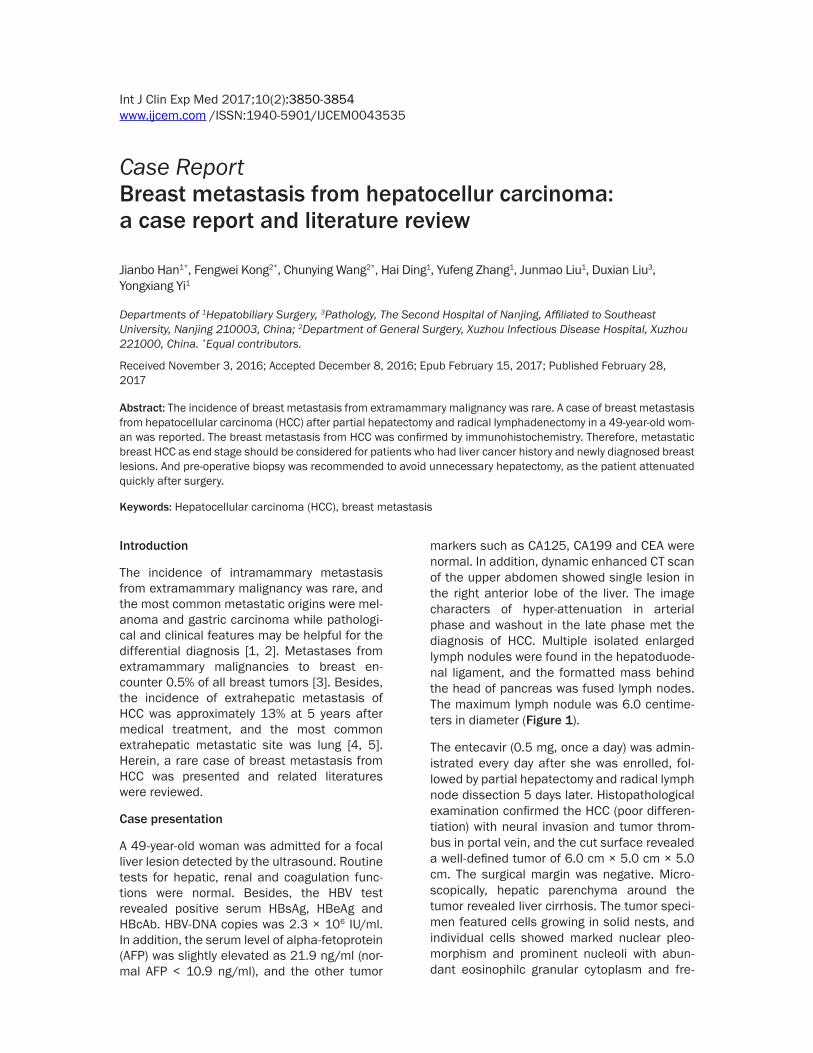
markers such as CA125, CA199 and CEA were normal. In addition, dynamic enhanced CT scan of the upper abdomen showed single lesion in the right anterior lobe of the liver. The image characters of hyper-attenuation in arterial phase and washout in the late phase met the diagnosis of HCC. Multiple isolated enlarged lymph nodules were found in the hepatoduode-nal ligament, and the formatted mass behind the head of pancreas was fused lymph nodes. The maximum lymph nodule was 6.0 centime-ters in diameter (Figure 1).
The entecavir (0.5 mg, once a day) was admin-istrated every day after she was enrolled, fol-lowed by partial hepatectomy and radical lymph node dissection 5 days later. Histopathological examination confirmed the HCC (poor differen-tiation) with neural invasion and tumor throm-bus in portal vein, and the cut surface revealed a well-defined tumor of 6.0 cm × 5.0 cm × 5.0 cm. The surgical margin was negative. Micro- scopically, hepatic parenchyma around the tumor revealed liver cirrhosis. The tumor speci-men featured cells growing in solid nests, and individual cells showed marked nuclear pleo-morphism and prominent nucleoli with abun-dant eosinophilc granular cytoplasm and fre-
Breast metastasis from hepatocellur carcinoma
3851 Int J Clin Exp Med 2017;10(2):3850-3854
quent mitotic figures (Figure 2). Besides, the immunohistochemical analysis indicated posi-tive Ki67 (>80%), VEGF, EGFR, VILLIN, CK19, and negative CK7, CK20, CD34, Hep-1 and GPC-3. The lymph nodules behind the head of pancreas were metastatic HCC; however, lymph nodes in the hepatoduodenal ligament were negative. Then she was discharged 14 days after operation, and Sorafenib (400 mg, twice a day) was administrated 21 days after the surgery.
Furthermore, she was re-admitted 1 month later because of aggravated backache. Her serum level of AFP was 24 ng/ml, and the CT scan showed no mass except multiple enlarged retroperitoneal lymph nodes (Figure 3A). Local three-dimensional conformal radiotherapy (lin-ear accelerator 6MV photons, 36 Gy/18 times) was adjusted, and then the back pain of the patient was relieved gradually. Additionally, 4 months after the surgery, a breast mass was indicated by CT scan. Routine blood test was normal, and the liver function tests showed ALT 35.5 IU/L, AST 52.0 IU/L, TBIL 29.3 µmol/L, DBIL 12.0 µmol/L, GGT 277.5 U/L, ALB 27.6 g/L, and the Child-Pugh grade of hepatic reserve was B (8 points), and the serum level of AFP was 31.7 ng/ml. The chest CT scan indi-cated multiple mediastinal lymph nodes under the left clavicle and around the parasternal, additionally, small amount of pericardial effu-sion and a mass about 2.0 cm × 2.0 cm × 1.5 cm in the upper inner quadrant of the left breast was also indicated (Figure 4). Besides, abdominal CT scan showed multiple new mass-es in the liver and small amount of ascites
nohistochemical tests did not indicate primary breast cancer, a clinical diagnosis of metastatic HCC was made. The liver function of the patient was deteriorated gradually, and she received only supportive treatment. Then the patient was died from hepatorenal syndrome five month after the operation.
Discussion
The diagnosis rate of early HCC was low because of its ambiguous symptoms, and extrahepatic metastases may be presented as the initial manifestation [6]. Metastatic tumor in breast was usually single, round and painless [1]. It can be misdiagnosed as benign tumor. Unilateral left-sided and upper outer quadrant of the breast was the most frequently metastatic location [2]. Similarly, the breast lesion in this case was located in the upper inner quadrant of left breast.
Intrahepatic lymph drainage into hepatic por- tal lymph node via the portal triads was the usual pathway of local regional spread of HCC. And treatment of extrahepatic metastases in selected HCC patients who have good hepatic reserve, intrahepatic tumor stage (T0-T2), and are free of portal venous invasion may improve survival [7]. In this case, the peripancreatic lymph nodes were involved synchronously with HCC. The exact metastatic pathway to breast from HCC is still unknown, and more studies are needed. The prognosis of patients with lymph nodes involvement was poor, and the median survival time was 7.4 months even after hepatic resection and radical lymphade-nectomy [7].
Figure 1. Dynamic enhanced CT scan of the upper abdomen showed single lesion in the right anterior lobe. The mass behind the head of pancreas was fused lymph nodes. The chest CT scan showed no lesion in mediastinum and breast.
(Figure 4), and retroperitone- al lymph nodes were shrunk obviously (Figure 3B). The breast mass was resected for biopsy, and the pathological examination showed meta-static cancer invasion and the cytology revealed poorly dif-ferentiated carcinoma. Imm- unohistochemical analysis in- dicated positive C-erbB-2, Villin, AE1/AE3, and negative CK7, CK20, ER, PR, CA125, TTF-1, Naspin A, GATA-3, GPC-3, Arg-1 and GCDFP15. The tumor was similar to the HCC microscopically. As the immu-

Breast metastasis from hepatocellur carcinoma
3852 Int J Clin Exp Med 2017;10(2):3850-3854
Accurate diagnosis of metastatic breast cancer is important for selection of appropriate treat-ment to avoid unnecessary or even harmful therapy. Routine pathologic examination and immunohistochemical study may be helpful to confirm the diagnosis in most cases. The tumor markers such as AFP for HCC, CK7/20 for gas-tric carcinoma, thyroid transcription factor (TTF-1) for lung cancer, ER/PR/BRSR-2 for breast cancer and PSA for prostate cancer were help-ful in differential diagnosis [2]. If immunohisto-chemical study showed negative breast cancer marker and positive extramammary cancer marker, the diagnosis of metastatic breast car-cinoma should be considered.
In this case, the immunostaining of breast mass showed negative AFP, ER/PR and slightly positive C-erbB-2. Pathological comparison of the mass and the personal family history, clini-cal medical history was useful to differentiate primary and metastatic cancer. The value of
patients with invasion of the portal vein, he- patic vein, or inferior vena cava, intrahepatic metastases, and tumor stage between patients with intra- and extrahepatic metastases [8]. Metastasis to the breast from an extramam-mary neoplasm usually indicates disseminated metastatic disease and a poor prognosis [2]. It was reported that the frequent metastatic sites from HCC were lung, bone and lymph node. The median survival time and 1-year survival rate of HCC with extrahepatic metastases were 7 months and 24.9% [9]. Surgical resection (SR) for metastatic lesions can provide survival ben-efits for carefully selected patients with 1 or 2 isolated extrahepatic metastases and succe- ssful treatment of intrahepatic HCC, in addi-tion, surgical intervention was shown to lead to relative prolongation of the survival time for HCC patients with brain metastasis, especially in those with preserved hepatic function [10, 11]. Control of intrahepatic tumor and good hepatic reserve function were the only two sig-
Figure 2. The breast mass showed pathological resemblance of the liver cancer. A. Primary HCC (hematoxylin-eosin, × 400); B. Metastatic HCC in the breast (hematoxylin-eosin, × 400); C. Specimen of metastatic breast mass from HCC.
Figure 3. Multiple enlarged lymph nodes in retroperitoneal were detected one month later after she was discharged from hospital (A). The lymph nodes were shrunk obviously after local three-dimensional conformal radiotherapy (B).
AFP declined after the sur-gery, and 4 month later, it was elevated after the breast mass, multiple enlarged ly- mph nodules and recurrent HCC was detected. The breast mass showed histological structural resemblance to HCC, and the diagnosis of breast metastasis from HCC was confirmed through patho-logical comparison of previ-ously diagnosed cancer and metastatic lesion.
There were significant diff- erences in proportions of

Breast metastasis from hepatocellur carcinoma
3853 Int J Clin Exp Med 2017;10(2):3850-3854
nificant predictors of survival in patients with extrahepatic metastases from HCC, and thera-peutic approaches to control intrahepatic tumors were important for survival improve-ment [12]. A variety of interventional-based liv-er-directed therapies and more recently sys-temic therapy with sorafenib are available to treat unresectable tumors, and long-term sur-vival may be achieved from resecting metasta-sis at sites of the abdominal lymph node, adre-nal gland, lung, and peritoneum for selected cases with limited isolated metastasis, pre-served liver function and the primary tumor has been adequately controlled [13]. However, only 1 month was indicated for the presenting patient due to poor hepatic function reserve, as the patient attenuated quickly after surgery regardless of best supportive treatment. On the other hand, the therapeutic role of mastec-tomy for patients with breast metastasis from HCC was unknown [10, 11].
In conclusion, metastatic breast cancer should be considered when a patient had liver cancer history and newly diagnosed breast mass and pre-operative fine needle biopsy of metastatic foci was recommended, because the patient might not benefit from radical hepatectomy and mastectomy, then personalized multidisci-plinary therapy should be critically selected according to the general status and hepatic reserve of the patients.
Acknowledgements
This study was supported by Nanjing Medical Science and Technique Development Founda- tion, Nanjing Department of Health (Grant:
QRX11235 and Grant: ZDX12008), and Jiang- su Science and Technology Project of Clini- cal Medicine Foundation, Science and Tech- nology Department of Jiangsu Province (Grant: BL2014005).
Disclosure of conflict of interest
None.
Address correspondence to: Yongxiang Yi, Depart- ment of Hepatobiliary Surgery, The Second Hospital of Nanjing, Affiliated to Southeast University, 1-1 Zhongfu Road, Nanjing 210003, Jiangsu, China. Tel: +86-25-83626203; E-mail: [email protected]
References
[1] Koch A, Richter-Marot A, Wissler MP, Baratte A, Mathelin C. Mammary metastasis of extrama-mmary of cancers: current knowledge and di-agnostic difficulties. Gynecol Obstet Fertil 2013; 41: 653-9.
[2] Lee SK, Kim WW, Kim SH, Hur SM, Kim S, Choi JH, Cho EY, Han SY, Hahn BK, Choe JH, Kim JH, Kim JS, Lee JE, Nam SJ, Yang JH. Characteris-tics of metastasis in the breast from extrama-mmary malignancies. J Surg Oncol 2010; 101: 137-40.
[3] Lakhani SR. International agency for research on cancer and World health organization. WHO classification of tumours of the breast. Lyon: International agency for research on cancer; 2012.
[4] Terada T, Maruo H. Unusual extrahepatic met-astatic sites from hepatocellular carcinoma. Int J Clin Exp Pathol 2013; 6: 816-820.
[5] Kanda M, Tateishi R, Yoshida H, Sato T, Masu-zaki R, Ohki T, Imamura J, Goto T, Yoshida H, Hamamura K, Obi S, Kanai F, Shiina S, Omata
Figure 4. A mass about 2.0 cm × 2.0 cm × 1.5 cm in the upper inner quadrant of the left breast was detected (A). The imaging of the mass was enhanced peripherally in arterial phase. CT scan of chest showed multiple enlarged lymph nodes in the mediastinum, under the left clavicle and around the parasternal (B). CT scan of abdomen showed multiple new masses in the liver (C).
Breast metastasis from hepatocellur carcinoma
3854 Int J Clin Exp Med 2017;10(2):3850-3854
M. Extrahepatic metastasis of hepatocellular carcinoma: incidence and risk factors. Liver Int 2008; 28: 1256-1263.
[6] Helal Tel A, Radwan NA, Shaker M. Extrahe-patic metastases as initial manifestations of hepatocellular carcinoma: an Egyptian experi-ence. Diagn Pathol 2015; 10: 82.
[7] Uka K, Aikata H, Takaki S, Shirakawa H, Jeong SC, Yamashina K, Hiramatsu A, Kodama H, Takahashi S, Chayama K. Clinical features and prognosis of patients with extrahepatic metas-tases from hepatocellular carcinoma. World J Gastroenterol 2007; 13: 414-20.
[8] Yang Y, Nagano H, Ota H, Morimoto O, Naka-mura M, Wada H, Noda T, Damdinsuren B, Marubashi S, Miyamoto A, Takeda Y, Dono K, Umeshita K, Nakamori S, Wakasa K, Sakon M, Monden M. Patterns and clinicopathologic fea-tures of extrahepatic recurrence of hepatocel-lular carcinoma after curative resection. Sur-gery 2007; 141: 196-202.
[9] Natsuizaka M, Omura T, Akaike T, Kuwata Y, Yamazaki K, Sato T, Karino Y, Toyota J, Suga T, Asaka M. Clinical features of hepatocellular carcinoma with extrahepatic metastases. J Gastroenterol Hepatol 2005; 20: 1781-1787
[10] Chan KM, Yu MC, Wu TJ, Lee CF, Chen TC, Lee WC, Chen MF. Efficacy of surgical resection in management of isolated extrahepatic metas-tases of hepatocellular carcimoma. World J Gastroenterol 2009; 15: 5481-88.
[11] Han MS, Moon KS, Lee KH, Cho SB, Lim SH, Jang WY, Jung TY, Kim IY, Jung S. Brain metas-tasis from hepatocellular carcinoma: the role of surgery as a prognostic factor. BMC Cancer 2013; 13: 567.
[12] Jung SM, Jang JW, You CR, Yoo SH, Kwon JH, Bae SH, Choi JY, Yoon SK, Chung KW, Kay CS, Jung HS. Role of intrahepatic tumor control in the prognosis of patients with hepatocellular carcinoma and extrahepatic metastases. J Gastroenterol Hepatol 2012; 27: 684-9.
[13] Chua TC, Morris DL. Exploring the role of resec-tion of extrahepatic metastases from hepato-cellular carcinoma. Surg Oncol 2012; 21: 95-101.