case presentation surgery grand round - denver, colorado · case presentation • right chest tube...
TRANSCRIPT

Case PresentationSurgery Grand Round
Amid Keshavarzi, MDUCHSC 4/9/2006
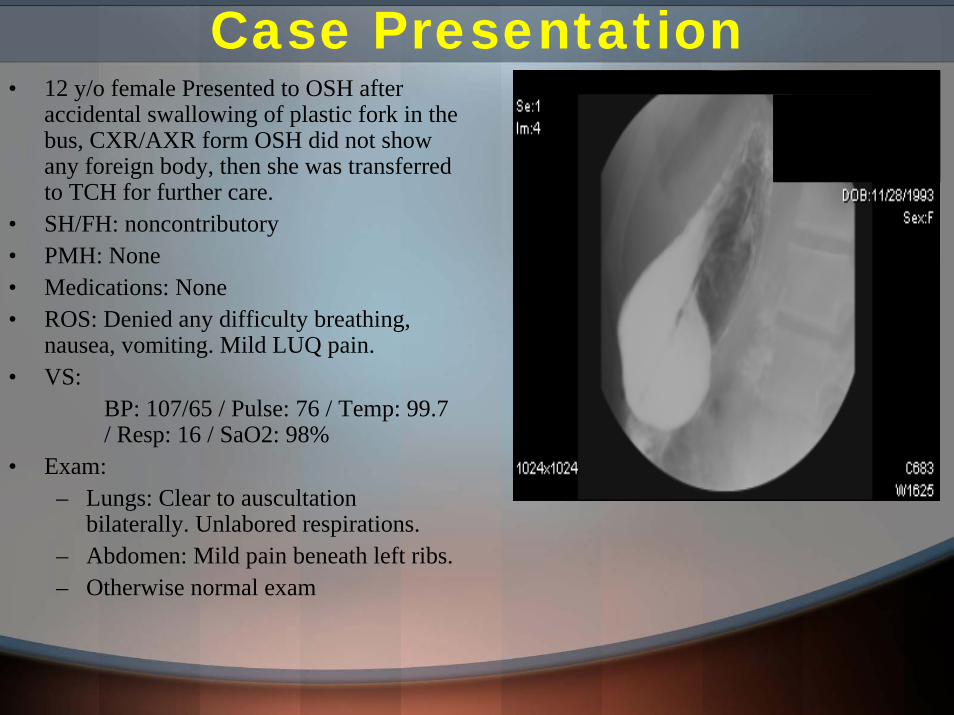
Case Presentation• 12 y/o female Presented to OSH after
accidental swallowing of plastic fork in the bus, CXR/AXR form OSH did not show any foreign body, then she was transferred to TCH for further care.
• SH/FH: noncontributory• PMH: None• Medications: None• ROS: Denied any difficulty breathing,
nausea, vomiting. Mild LUQ pain.• VS:
BP: 107/65 / Pulse: 76 / Temp: 99.7 / Resp: 16 / SaO2: 98%
• Exam: – Lungs: Clear to auscultation
bilaterally. Unlabored respirations. – Abdomen: Mild pain beneath left ribs.– Otherwise normal exam

• Initial CXR normal
• Initial esophagram negative for leak.
• Patient underwent gastroesophagoscopy.
• Following removal of the fork, repeat endoscopy revealed several areas of abrasion of both the stomach and esophagus, without significant bleeding or obvious perforation.
• Patient recovered form anesthesia and transferred to PACU.
Case Presentation

Case Presentation
• Right chest tube was placed, and esophagram was repeated.
•In the PACU, found to be agitated, and on exam, she was tachypneic, decrease BS in the right chest, with right chest wall and neck crepitus.

• Patient admitted to PICU.
• Initial VS: Temp: 99.7 / HR: 76 / RR: 16 / BP: 107/65
• HD #1: Temp: 38.7 / HR 120’s / RR 20’s, WBC 18 / BP 112/49
Hospital Coarse
OR for exploration.
Underwent right thoracotomy, debridment of pleural cavity, repair of esophageal perforation with pleural patch.
Found to have 1.5 cm vertical perforation of right lateral mid-esophagus, behind the azygus vein, with moderate pleural soiling and mediastinitis.
Reinforced primary repair was performed using pleural patch.

Hospital Coarse• POD # 1:
– Gastric feed started, HD stable, WBC: 14
• POD # 2:– Chest tubes were placed to waterseal, WBC: 10.8
• POD # 3:– Anterior chest tube D/C’s, WBC: 7.5
• POD # 4: – No major event
• POD # 5:– Esophagram negative for leak– Postosterior chest tube D/C’d– NGT D/C’d– Diet advanced
• POD # 6: – Discharged home

Esophageal Perforation: Historical Facts
• Esophageal perforation was first described ~ 250 years ago.
• In 1723, Herman Boerhaave first described barogenic esophageal rupture.
• In 1947, first reports of successful esophageal repair were performed by Barrett, Olsen and Clagett, separately.
• In 1952, Satinsky and Kron performed the first successful esophagectomy for perforation.
• In 1965, Mengoli and Klasser were the first described the conservative management.

Esophageal Perforation
0%10%20%30%40%50%60%
Instru
mentat
ion
Forei
gn Bod
y
Operat
ive In
jury
Others
Etiology
Etiology of Esophageal Perforation
• Esophageal perforations are associate with 15-30% mortality.• Extremely high mortality before the era of antibiotics.• Increase in frequency of iatrogenic injuries (60-70%) due to more frequent instrumentation in
last 40 years.• Most common site are areas of anatomic narrowing.
Abdominal
Cervical
Brinster CJ et al. : Ann Thorac Surg (2004) 77: 1475-83

Esophageal Perforation• Diagnosis:
– Contrast esophagography:• Gastrographin study positive in 50% of cervical
perforations and 75-80% of esophageal perforations
• Contrast studies have overall false negative rate of 10%.
– CT– Flexible esophagoscopy– Pleural effusion sampling
• Surgical options:– Primary repair– Reinforced primary repair– Esophagectomy– T-tube drainage– Exclusion and diversion– Thoracoscopic repair– Delay primary repair
• Criteria for non-surgical treatment:– Early diagnosis.– Contained leak within neck or
mediastinum.– Drainage into esophageal lumen.– Injury not related to neoplasm, in
abdomen and not proximal to obstruction.
– No sign or symptom of sepsis.– Availability experienced radiologist and
CT surgeon.
S. Hasan et al. Eur J CT Surgery 28 (2005) 7-10 Brinster CJ et al. : Ann Thorac Surg (2004) 77: 1475-83

Brinster CJ et al. : Ann Thorac Surg (2004) 77: 1475-83
Esophageal Perforation

Conservative management of iatrogenic esophageal perforation – a viable option
• Retrospective study, over 10 years.• 9/26 had carcinoma and 17/26 had benign
pathology.• 22/26 diagnosed within 6 h, and 4/26 over 24 h.• Treatment plan : NPO, IVF, and Abx• 22/26 (84.6%) success rate with this regimen.• All four death (15.3%) was caused by other
cases than mediastinitis, but all had contamination of pleural cavity.
• 46% of patient complicated with empyema.• Conservative management give comparable to
or better result than surgical intervention. • Perforations which involves pleural or
peritoneal cavity carries the worst prognosis.
S. Hasan et al. Eur J CT Surgery 28 (2005) 7-10
Clinical Findings in Iatrogenic Esophageal Perforation
0 20 40 60 80 100
Chest pain
Pyrexia
Neck Emphysema
Back pain
Shock
X-Ray Findings
0% 10% 20% 30% 40% 50% 60%
LME
Pneu
momed
iastin
um
Pneu
mothora
x
Pneu
moperi
toneiu
m
Subd
iaph.
Exrav
asati
on
Extra
vasa
tion t
o pleu
ra

Algorithm for Management of Esophageal Perforation
Huber-Lang M et al. : Surg Today (2006) 36:332–340 Brinster CJ et al. : Ann Thorac Surg (2004) 77: 1475-83
Conclusion
• Conservative management of esophageal perforation is a viable option but mostly dependent on patients pre-existing conditions.
• Primary repair of esophageal perforations with or without reinforcement is the best therapeutic approach.

References:
• Huber-Lang M, et al. : Esophageal perforation: principles of diagnosis and surgical management. Surg Today. 2006;36(4):332-40.
• Chambers AS, et al. : A new management approach for esophageal perforation. J ThoracCardiovasc Surg. 2005 Nov;130(5):1470-1.
• Richardson JD et al. : Management of esophageal perforations: the value of aggressive surgical treatment. Am J Surg. 2005 Aug;190(2):161-5.
• Hasan S, et al. : Conservative management of iatrogenic oesophageal perforations--a viable option. Eur J Cardiothorac Surg. 2005 Jul;28(1):7-10.
• Eroglu A, et al. : Esophageal perforation: the importance of early diagnosis and primary repair. Dis Esophagus. 2004;17(1):91-4.
• Brinster CJ, et al. : Evolving options in the management of esophageal perforation. Ann Thorac Surg. 2004 Apr;77(4):1475-83.