case management. case m.r. 59/m married roman catholic from cavite unemployed
TRANSCRIPT

Case Management

Case
• M.R.• 59/M• Married• Roman Catholic• From Cavite• Unemployed

Chief Complaint
Fever

Profile
• Diagnosed with Liver disease in July 2011 – Presentation: bipedal edema , abdominal enlargement,
and icteresia lost to ff-up until Sept. 2011 consult with private MD and given Silymarin and Vitamin B complex for the liver as maintenance meds
• Non-diabetic, Non-hypertensive, Non-asthmatic and no known allergies to foods and drugs

History of Present Illness
• 11 days PTA: (+) Fever 38-39oC with associated hypogastric tenderness private MD, UA done, A> UTI – Given: Cotrimoxazole 800/160 mg/tab 1 tab BID and
Paracetamol 500 mg PRN for fever with temporary lyses of fever.
• 7 days PTA: (+) developed maculopapular rashes initially on bilateral UE chest and trunk area; continued on Cotri, and still with on and off fever

History of Present Illness
• 5 days PTA: skin lesions generalized– (+) pruritus and erythema with involvement of the face
about the same time he developed deepening icteresia and jaundice, (+) conjunctival suffusion, (+) dry skin beginning flaking of old lesions
– Discontinued TMP-SMX as advised by a relative (-)
blisters/bullae formation

History of Present Illness• 2 days PTA:– (+) development of lip crusting and cracking– (+) anorexia– (+) irritable with difficulty sleeping– (+) soft stools, non-melenic, non-bloody, non-mucoid,
yellowish = 2-3 x/day– (+) cough, non-productive– Still with on and off fever– Still allegedly with good urine output but with tea colored
urine– Consult with private MD advised referral to Derma
•

History of Present Illness
• 1 day PTA: Consult at PGH-Derma– A> ADR sec. to Cotri, cannot fully commit to SJS/EM.
Skin biopsy done and was given Momethasone furoate, Montelukast, levociterizine, Hydroxyzine PRN -> sent home’
• Day of admission: – (+) fever (Tmax 40 oC)with chills– (+) generalized weakness– (+) drowsy ER Admission
Review of Systems• (-) headache (-) weight loss• (-) BOV (-) d/c (-) tinnitus (-) gum bleeding• (-) dyspnea (+) cough (-) sputum (-) hemoptysis• (-) chest pain (-) PND (-) 2 P orthopnea (-) claudication• (-) abdominal tenderness (-) diarrhea (-) constipation( (-)
hematochezia• (+) dysuria (-) hematuria (-) proteinuria (-) oliguria• (-) polyphagia (-) polydipsia (-) polyuria (-) heat and cold
intolerance• (-) edema (+) jaundice (-) ecchymosis (-) petechiae (-)
hematoma

Past Medical History
• (-) DM, HPN, PTB, BA, Cancer, Kidney, liver and heart diseases
• Denies allergies• (-) Previous surgeries
– Allegedly, had liver problem last July 2011 after presenting with jaundice Abd. UTZ done showing normal findings, AST and ALT done were also normal, started on Silymarin, and Vitamin B Complex

Family Medical History
• (-) DM, HPN, BA, PTB, Cancer, Kidney, liver and heart diseases
• Allergies

Personal and Social
• 40 pack year smoker• Moderate alcoholic beverage drinker, 3-4x/wk• Denies illicit drug use

Date PE Assessment Plan
1/4/12DEMS
110/60, 92, 24, 37.9(+) congested sclerae, PC, (-) NVE/CLAD(+) lip desquamationECE, (+) crackles R mid-basal LFAP, DHS, NRRR, (-) murmursAbdomen flat, soft, non-tenderFEP, PNB, (-) edema
CAP, MR SJS 2o to Cotrimoxazole
Dxtics: CBC, Electrolytes (Na, K, Cl, Ca, P, Mg), Crea, Albumin, ALT, AST, UA, Blood GS/CS x 2Blood Typing Txts: Diphenhydramine 50 mg IVCeftriaxone 2 g IVAzithromycin 500 mg/tabPacetamol 300 mg IV PRN for T> 38.50
Course at the ER


Course at the ERDate Findings Assessment Plan
1/4/12POD
Seen drowsy, not in distress, moves all extremitiesBP 110/60, HR 104, RR 18, Temp. 36.2Dirty icteric sclerae, hyperemic palpebral conjunctivae, (+) lip desquamation, (-) oral ulcer, (+) crackles on right mid LF, (+) generalized maculopapular rashes slightly with pustules, (+) jaundice
CAP-MRAdverse Drug Event to TMP-SMXt/c Stevens Johnsons Syndrome 2o to TMP-SMXJaundice prob. 2o to viral hepatitist/c Anemia of Chronic diseaset/c UTI
Ceftriaxone 2 g IV ODAzithromycin 500 mg/tab 1 tab ODParacetamol 500 mg/tab 1 tab q4 for fever > 38 oCMomethasone fucoate ? 0.1%, apply once a day on affected surfaceLeveciterizine + Montelukast 5/con ? 1 tab ODHydroxyzine 10 mg/tab 1 tab ODHS

Course at the ERDate Findings Assessment Plan
1/4/12DERMA
(+) icteric sclerae(+) eye redness(+) lip fissures and crusting(+) multiple generalized erythematous and slightly coalescing to pustules(+) slightly globular abdomen(+) RUQ tendernessIntact Traube’s space
ADR prob. 2o to TMP-SMXSJS unlikely at this time (must fullfill criteria of at least 2 mucosal sites)T/c drug hypersensitivity syndrome
Ceftriaxone 2 g IV ODAzithromycin 500 mg/tab 1 tab ODParacetamol 500 mg/tab 1 tab q4 for fever > 38 oCMomethasone fucoate ? 0.1%, apply once a day on affected surfaceLeveciterizine + Montelukast 5/con ? 1 tab ODHydroxyzine 10 mg/tab 1 tab ODHSWet lips with pNSSStart Hyddrocortisone 100 mg IV q8Emollients ad libido

Course at the ERDate Findings Assessment Plan
1/4/12ALLERGY
arousable, oriented(+) hyperemic conju/(+) conjunctival suffusion (-) matting eyelids, (+) icteresia (+) dry, crusty lips,(+) ronchi on BLLF, (+) crackles right base(+) tenderness at periumbilical to hypogastric area(+) generalized erythematous maculopapular rashes coalescing into plaques wiuth dry desquamation, (-) bullae, blisters
ADR to CotriSJS less likely atthis timet/c CAPt/c UTIt/c CLD sec to ALD r/o chronic hepatitis t/c cholestatic jaundice, r/o drug induced hepatitisr/o Hepatic encepth IAnemia from Chronic DiseaseAKI from poor intake
CONTINUE PREVIOUS MEDICATIONS
Course at the ERDate Findings Assessment Plan
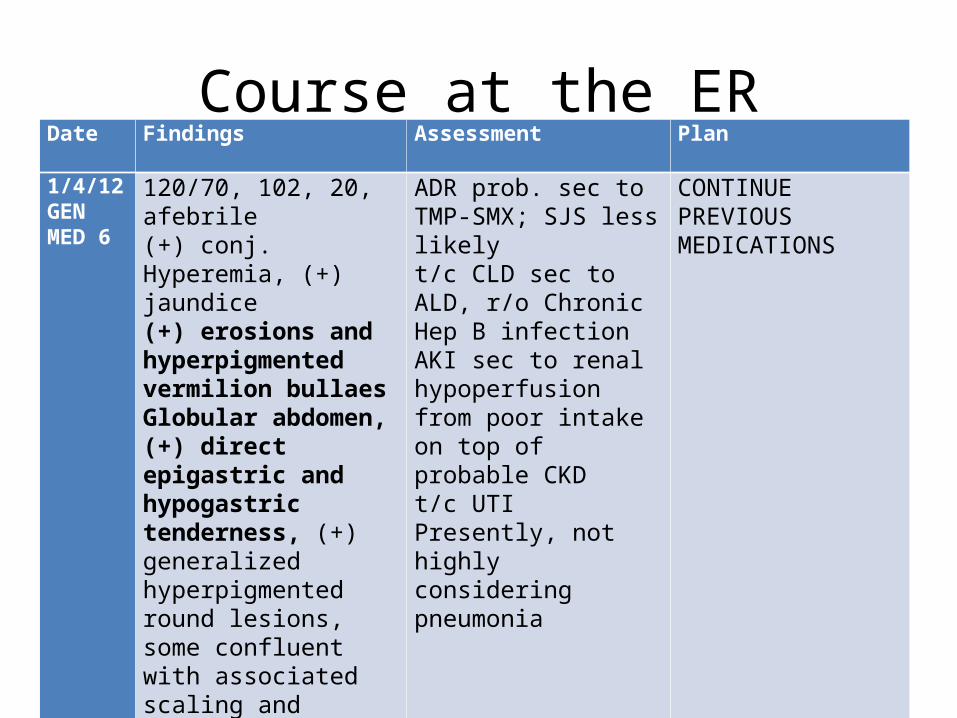
1/4/12GEN MED 6
120/70, 102, 20, afebrile(+) conj. Hyperemia, (+) jaundice(+) erosions and hyperpigmented vermilion bullaesGlobular abdomen, (+) direct epigastric and hypogastric tenderness, (+) generalized hyperpigmented round lesions, some confluent with associated scaling and erosions (-) discharge (-) blisters
ADR prob. sec to TMP-SMX; SJS less likelyt/c CLD sec to ALD, r/o Chronic Hep B infectionAKI sec to renal hypoperfusion from poor intake on top of probable CKDt/c UTIPresently, not highly considering pneumonia
CONTINUE PREVIOUS MEDICATIONS

Drug Oct Nov Dec Jan 24 25 26 27 28 29 30 31 1 Liveraid B Comp TMP-SMX
=
Para
(+) maculopapular rashes, trunk then becoming generalized

Present Working Impression• ADR to TMP-SMX• t/c CLD prob 2o to
1. Chronic Hepa B infection2. Alcoholic liver Disease
• AKI from Renal Hypoperfusion from sepsis, poor oral intake, third spacing from hypoalbuminimea
• UTI• Not highly considering CAP-MR
- Patient is for admission

Medications on Board
•Ceftriaxone 2 g IV OD•Hydroxyzine 10 mg/tab 1 tab ODHS•Montelukast + Levocetirizine 5/10 mg/tab OD•Momethasone furoate 0.1% lotion apply on affected areas once day•Paracetamol 500 mg/tab 1 tab q4 prn for T>38oC•Petroleum jelly lotion ad libidum•Lactulose 30 cc TID to make 3-4 BM/day
Course at the WardsDate Findings Assessment Plan
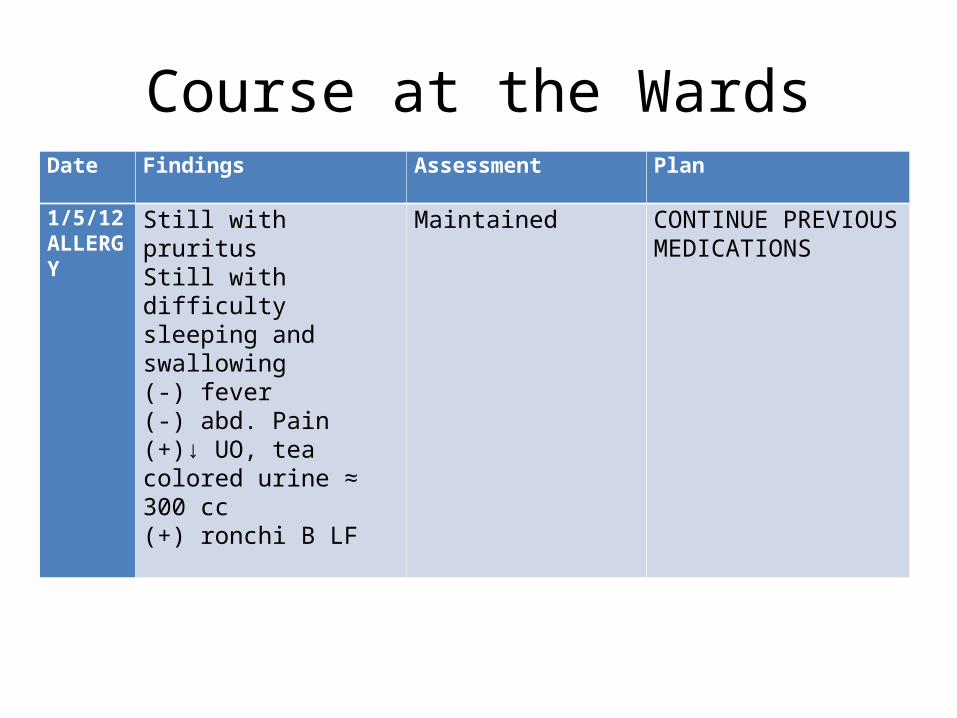
1/5/12ALLERGY
Still with pruritusStill with difficulty sleeping and swallowing(-) fever(-) abd. Pain(+)↓ UO, tea colored urine ≈ 300 cc (+) ronchi B LF
Maintained CONTINUE PREVIOUS MEDICATIONS

Date Findings Assessment Plan
1/5/12GEN MED 6
(+) with flank pain(+) decrease urine output(+) tea colored urine90/60, 70, 20, 37oC(+) dry, cracked vermillion border of lips with areas of hyperpigmentations, (+) apthous ulcers(+) cracklesGlobular abdomen, non-tender, non-palpable liver edge
Maintained
However upon consultation with Allergy senior resident and referral to consultant:Dx: Stevens Johnson Syndrome with Nephritis
Due to:1. Involvement of buccal mucosa2. Probable Interstitial nephritis
CONTINUE PREVIOUS MEDICATIONSTxt: Give hydrocortisone 250 mg IV q6H x 48 hours then taper Ranitidine 50 mg IVq 8o

Course at the WardsDate Findings Assessment/Lab Results Plan
1/5/12WAPOD
Referred for bloody NGT aspirate, ~ 80 cc fresh blood, (-) melena, (-) dyspnea, (-) dec. sensorium100/70 88 20 99%
Gastric Ulceration/BPUD vs. BEV
WBC: 19.7 6.9Hgb: 92 105Hct: 0.24 0.298Plt: 45 69Neut: 0.80 0.56Lymph: 0.070.20Mono: 0.12 0.04 BUN: 28.10 26.7Crea: 476 375BCR: 14.58CrCl: 12.55
Omeprazole drip 40 mg in 100 cc pNSSCold saline lavage
Transfuse 6 units platelet concentrateTransfuse 1 unit pRBC PTXM x 4-6Standby 1-2 u pRBC

Course at the WardsDate Findings Assessment Plan
1/6/12RENAL
I: 1300O: 450Restless, lethargic, afebrile, Blood tinged output per NGTECE, tachypneic, (+) cracklesTachycardic(+) muddy brown urine
Azotemia prob. from AKI prob. from Acute Tubular Necrosis cannot rule out acute nephritis Associated Renal hypoperfusion from 1. Systemic inflammatory state with febrile episodes 2. Recent UGIB and acute blood loss
CONTINUE PREVIOUS MEDICATIONS
ABGRepeat UA, may do urine eosinophilSuggest Sepsis work-up: blood GS/CS, Urine GS/CS

Course at the WardsDate Findings Assessment Plan
1/6/12GEN MED 6
I: 1360O: 450 (+) UGIB, fresh blood/NGT = 500 ccStill with decrease urine outputStill with decrease sensoriumBM x 2 since yesterday
Encephalopathy, Considerations:Hepatic from CLDUremic prob. sec to AKI sec to Allergic interstitial diseaseSepticUGIB prob sec :Uremic gastritisBEV from portal hpn sec to CLDSteroid-induced gastritisGI mucosal involvement from SJS ADR to TMP-SMXt/c Complicated UTI
Shift Hydrocortisone to Pip-Tazo 2.75 g IvHold Hydrocortisone for nowDiscontinue Ranitidine

Course at the WardsDate Findings Assessment Plan
1/6/12ANES
Referred for IntubationPre-Intubation: 80/60, tachycardicET tube size 8.0 inserted at level 19Secretions suctioned O2 sats post intubation: 97% HR: 95 70/50
Maintained

Course at the WardsDate Findings Assessment Plan
1/6/12GEN MED 6GI
(+) persistent decrease in sensorium(+) fresh blood/NGT(+) melena/diaper
Abd. UTZ: (+) cirrhotic liver, (+) splenomegaly, (+) renal parenchymal disease, (+) contracted gallbladder
Conferred with Derma: Provisional Biopsy Result: Vacuolar intergface dermatitis, drug reaction may be considered
t/c Acute Fulminant Hepatitis prob. drug induced
Start Somatostan 3 g in D5W 250 cc X 12 RTCFor BTIdeally, for liver transplantFor possible EGD and RBL once stabilized
Facilitate BTStart dopamine, if still hypotensive start noradrenaline

Course at the WardsDate Findings Assessment
1/6/12GEN MED 6
Drowsy, intubated withdraws to painBP 140/80 on Dopa at 12 mcg/hrHR 7620 CAB, O2 sat 99%
Acute fulminant hepatitis prob. drug induced (Co-trimoxazole) on top of CLD prob sec to 1. ALD, 2. PNC sec to Chronic Hepatitis, in hepatorenal syndrome Type IIShock prob. sec to 1. Hypovolemic sec to blood loss 2. Septic from urosepsisEncephalopathy 1. Hepatic St. 3-4, 2. Septic UGIB prob. sec to 1. BEV, 2. BPUD, 3. SRMI, 4. Steroid inducedCLD prob. sec to 1. ALD, 2. FNC sec to Chronic Hep B Complicated UTIADR to Cotri-moxazole

Labs
• PT: 14.0/90.8/0.10/8.74• PTT: 30.6/>245 • UA: dark, yellow, cloudy, pH 5.5 SG 1.015, (-)
CHON, CHO, RBC abundant, WBC 1-3, +2 bacteria, EC few, fine granular cast 0.3, bil +2, leukocyte trace, NO2 (-), Hgb + 3
• Urine GS (-) PMN, (-) organisms

• 1/6/12: 7:50 PM• Patient’s son signed DNR, to consume meds and no blood/
blood products to be given to the patient, and to stop all IV fluids of the patient
• 10:58: WAPOD– Patient referred for BP=0, HR=O– Noted DNR status– ECG done: asystole– Time of death: 10.53 PM
• PCOD: Hypovolemic shock sec to blood loss prob. from 1. Bleeding esophageal varices from CLD, 2. Bleeding peptic ulcer disease, 3. Stress related mucosal injury

Problem List
1.Generalized body rash with fever– Considerations: ADR to TMP-SMX; SJS
2. Increasing abdominal girth, jaundice, increasing liver enzymes, hyperbilirubinemia
– Chronic liver disease from Hep B infection– Hepatitis sec. to hypersensitivity reaction to TMP-SMX
3. Oliguria, tea colored urine, hyaline cast, increase BUN, increase creatinine
– Dehydration from poor intake– Allergic interstitial nephritis
4. Bilateral pulmonary crackles– Infection? (pneumonia)– Acute pulmonary congestion from AKI

Stevens-Johnson Syndrome
• Signs and Symptoms– Facial swelling– Tongue swelling– Hives– Skin pain– A red or purple skin rash that spreads within hours to days– Blisters on your skin and mucous membranes, especially in your
mouth, nose and eyes– Shedding (sloughing) of your skin– If you have Stevens-Johnson syndrome, several days before the
rash develops you may experience:• Fever, Sore throat, Cough, Burning eyes

Stevens-Johnson Syndrome• Exact cause can't always be identified. Usually, the condition is
an allergic reaction in response to medication, infection or illness.
• Medication causes:– Anti-gout medications, such as allopurinol– Nonsteroidal anti-inflammatory drugs (NSAIDs), often used to treat pain– Penicillins– Anticonvulsants– Infectious causes:
• Herpes (herpes simplex or herpes zoster), Influenza, HIV, Diphtheria, Typhoid, Hepatitis
• Physical stimuli, such as radiation therapy or ultraviolet light.

• Diagnosis is based on thorough medical history, physical exam and the disorder's distinctive signs and symptoms.
• To confirm the diagnosis: skin (biopsy)
Stevens-Johnson Syndrome

• Stopping medication causes• Supportive care• Fluid replacement and nutrition• Wound care• Eye care• Immunoglobulin intravenous (IVIG• Skin grafting
Stevens-Johnson Syndrome

• Medications– Pain meds– Antihistamines : itching– Antibiotics , when needed– Topical steroids to reduce skin inflammation– Intravenous corticosteroids for adults
Stevens-Johnson Syndrome
