case discussion 1. management of head injury … discussion .pdf · case discussion 1. management...
TRANSCRIPT

CASE DISCUSSION 1.
MANAGEMENT OF HEAD INJURY
IN PRE-HOSPITAL CARE
Dr. Jalil IshakConsultant Family Medicine SpecialistKlinik Kesihatan Jasin, Melaka
Dr. Zainab KusiarFamily Medicine SpecialistKlinik Kesihatan Mantin, Negeri Sembilan
1

History
• A 68-year-old male presented to health clinic alone at about 9.00 am, half an hour after falling from his motorbike at an unknown speed.
• He was not wearing a helmet at the time; however he gave no history of LOC.
• He sustained a few minor abrasion wound on his right knee & right elbow, right side of forehead & broke his reading glasses during the fall.
2

History-2
• A known case of hypertension & IHD
• On several types of antihypertensives & other medications which patient’s not able to describe
• No history of vomiting, severe headache or limb weakness after the fall
• No history of palpitation, chest pain or shortness of breath at the time of fall from motorbike
3

Physical examination
• Walking, alert, able to communicate & answer questions
• Vital signs:▫ Blood Pressure: 150/95 mmHg
▫ Pulse rate: 80 bpm
▫ Pulse: Regular, normal volume
▫ Resp rate: 20 per minute, normal, regular
▫ Resp quality: Equal air entry bilaterally
4

Physical examination-2
• Head: A small mild abrasion wound on right side of forehead with no active bleeding
• Eyes: No conjunctival hemorrhage, or hyphema. Pupils are equal. • Nose: No bleeding• Ears: No bleeding• Neck: No pain. Full range of movement• Chest: No visible wound, non-tender on palpation• CVS: DRNM• Lungs: Clear• Abdomen: No visible wound, soft, non-tender • Pelvis: No visible wound, no tenderness on gentle palpation• Extremities: Superficial abrasion wounds over the right elbow &
right knee, no deformity• HI is assessed by GCS Score.
5

6

Answer 1a
7

• The score is the cumulative sum of the scale in each component. GCS score: E4V5M6 = 15
• The levels of HI severity are classified as:
8
Answer 1a

Answer 1b
• Head injury is defined as blunt &/or penetrating injury to the head (above the neck) &/or brain due to external force* with temporary or permanent impairment in brain function which may or may not result in underlying structural changes in the brain.
*The external forces may include any of the following events: ▫ the head being struck by an object▫ the head striking an object▫ the brain undergoing an acceleration/deceleration movement
without direct external trauma to the head▫ a foreign body penetrating the brain▫ forces generated from events such as blast or explosion
9

Basic investigations
• ECG: Sinus rhythm, rate 80
• Blood glucose: 6.1 mmol/l
• FBC: Hb 12.0 gm% TW: 6,000PLT: 250,000
Q2. What is the management for this patient?
10
Answer 2
• Management in Klinik Kesihatan▫ Wound dressing & ATT
▫ Paracetamol for musculoskeletal pain
▫ Discharge advice form regarding danger signs of HI
11
12

Answer 3
• Verbal & written discharge advice to patient or care givers & ensure patient/care giver understand the content & sign the document.
13

Answer 3
14

Answer 3
15

16

Answer 4
17
18

Answer 5
19

History (cont.)
• Patient was discharged - TCA PRN
• At 7.00 pm on the same day, the man came back to the clinic but this time he was brought by his neighbour.
• He had severe headache, vomiting, & appeared drowsy & weak.
• He fell backwards while walking in his neighbour’s house compound.
20

Clinical assessment
• BP: 90/60 mmHg
• Pulse rate: 58 bpm
• Pulse rhythm: Regular
• Respiratory rate: 12 per minute
• Respiratory quality: Equal air entry bilaterally
• SpaO2: 90%
94% (on oxygen supplementation)
21

Clinical assessment-2
• Other findings were similar as before except for the following:▫ Head: Small haematoma (2x3) cm at occipital area
• He was only opening eyes to pain & mumbling when asked question.
• He was not obeying command but able to push away the hand when applying pressure on the eyebrow.
Q6. What is the GCS score of this patient?
22

Eye Response
Spontaneous eye opening 4 points
Opens to verbal command, speech, or shout 3 points
Opens to pain, not applied to face 2 points
No eye opening 1 point
Verbal Response
Alert and oriented 5 points
Confused conversation, but able to answer questions 4 points
Inappropriate responses, jumbled phrases, but discernible words 3 points
Incomprehensible speech 2 points
No sounds 1 point
Motor Response
Obeys commands for movement fully 6 points
Localises to noxious stimuli 5 points
Withdraws from noxious stimuli 4 points
Abnormal flexion, decorticate posturing 3 points
Extensor response, decerebrate posturing 2 points
No response 1 point
GCS score: E2 V2 M5 = 9
Answer 6
23

Answer 6
• The score is the cumulative sum of the scale in each component.
• The levels of head injury severity are classified as:
24

Management at KK (2nd visit)• Patient was attended immediately:
▫ Vital signs & GCS scoring done▫ O2 via oxygen mask given▫ IVD normal saline commenced▫ Cervical collar to immobilise cervical spine put on
• Patient was sent to the radiology unit for skull X-ray in view of occipital haematoma & it was done within half an hour.
• He was then immediately sent to the nearby hospital & accompanied by a medical officer.
Q7. Is skull X-ray indicated in this patient?
25
Answer 7
• The plain skull x-ray is ineffective screening tool in predicting ICH in MHI with a mean sensitivity of 50.0% (ranges from 13.0% to 75.0%) & a mean specificity of 97.0% (ranges from 91.0% to 99.5%).55
Thus,1. The patient should be sent immediately to hospital without
wasting time doing skull X-ray.2. The skull X-ray has no value on further management.
55. Hofman PA, et al. J Neurol Neurosurg Psychiatry. 2000 68(4):416-422
26
27

Answer 8
28

29

Answer 9
30
31

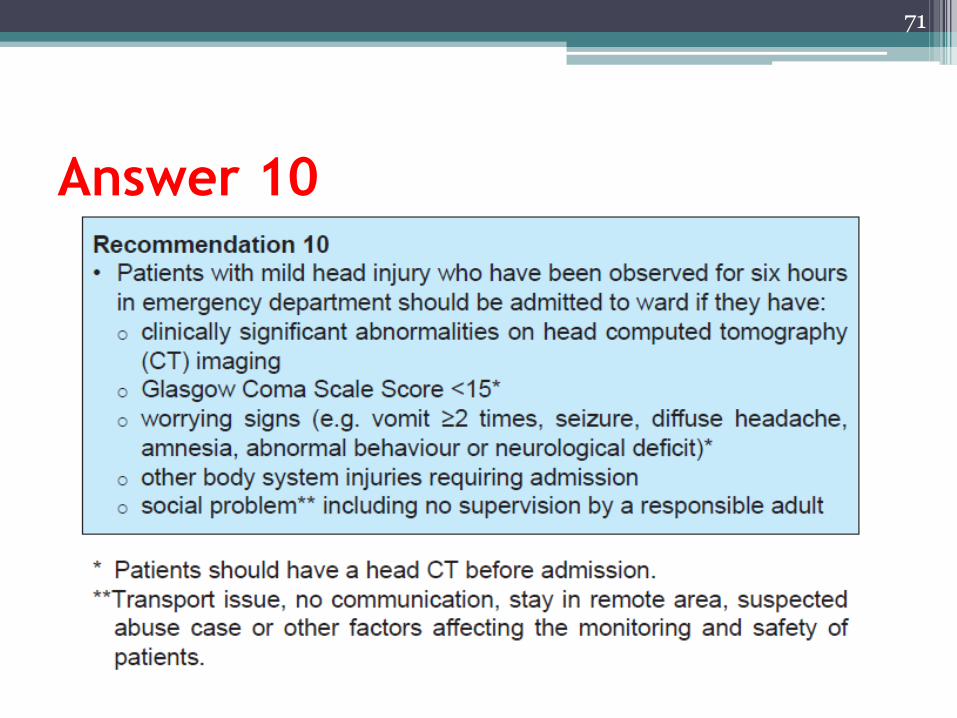
Answer 10
• Patient’s GCS was <15
32
33
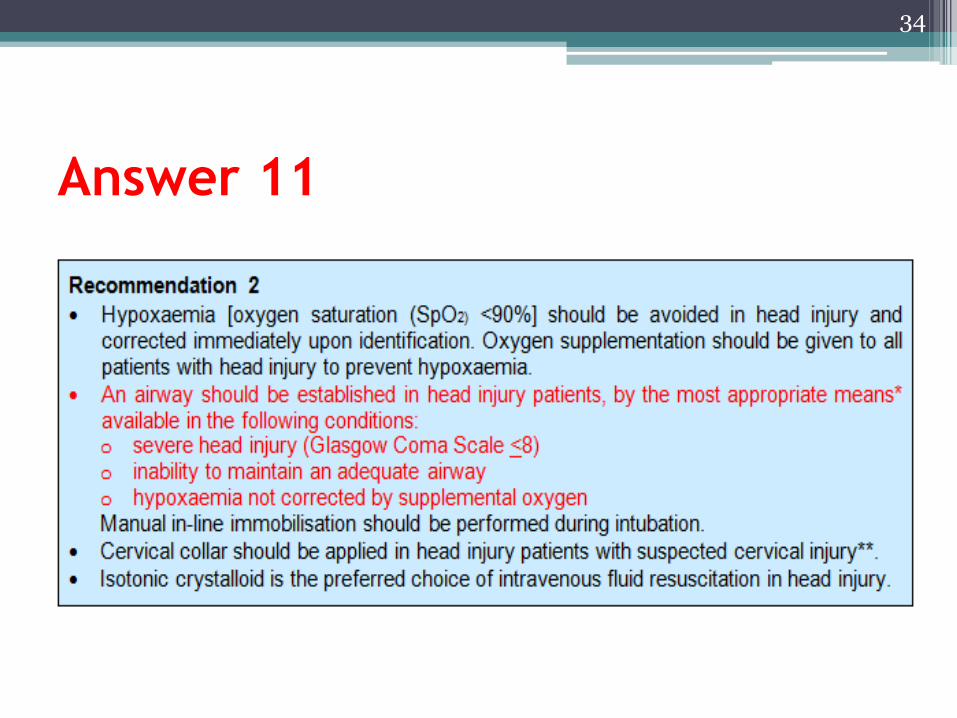
Answer 11
34

What are the pitfalls in the management
of this patient?
Patient should be admitted in the first scene as…1. Patient was 68 years old (>65 years) & had history
of falling from a motorbike.
2. The history of medication for heart disease e.g. aspirin & warfarin was not elicited in the first visit
3. The social history was not properly taken• Patient was staying alone - nobody to supervise him• Patient had difficulty to read without a reading glasses
4. Verbal explanation regarding discharge advicewas not given• Patient misunderstood that he should come to clinic only
when headache is severe
35

What are the pitfalls in the
management of this patient?-2
• In those aged ≥60 years, irrespective of motor scale component of GCS, total GCS score & head AIS score, is an independent risk factor for the mortality.13
• Patients with pre-injury use of antiplatelet agents (e.g. clopidogrel & aspirin) are at an increased risk for mortality with blunt traumatic ICH.76
13. Timmons SD, et al. J Trauma. 2011;71(5):1172-1178
76. Wong DK,e t al. J Trauma. 2008;65(6):1303-130
36

37
Thank You

CASE DISCUSSION 2.
MANAGEMENT AT
EMERGENCY & TRAUMA DEPARTMENT
Dr. Nik Ahmad Shaiffudin Nik Him
Consultant Emergency Physician
Universiti Sultan Zainal Abidin, Terengganu
Dr. Cecilia Anthonysamy
Emergency Physician
Hospital Serdang, Selangor
38

History
• A 65-year-old gentleman had a history of slip & fall in the bathroom.
• He was brought into the Emergency & Trauma Department (ED) by his neighbour for superficial L/W at the temporal parietal area.
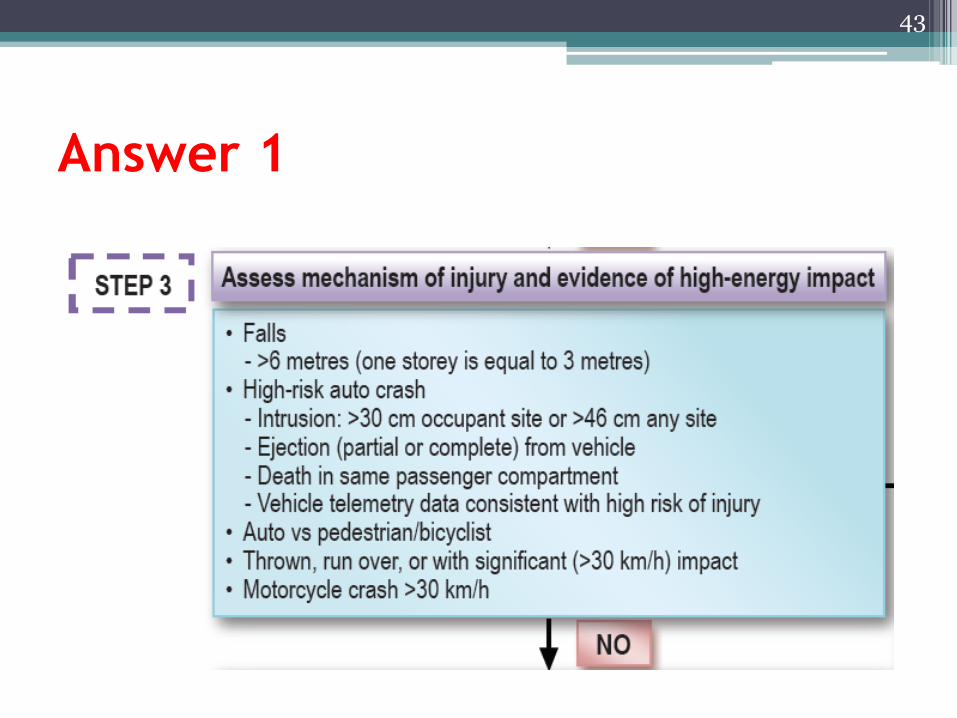
Q1. What are the triage criteria for
patient with HI in ED?
39
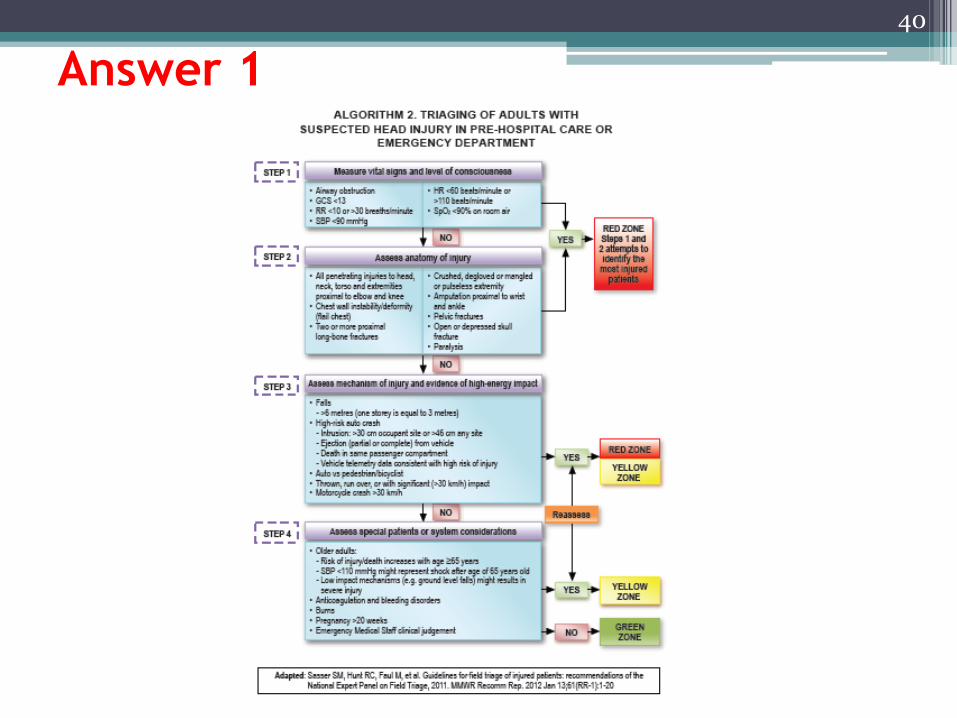
Answer 1
40

Answer 1
41

Answer 1
42
Answer 1
43

Answer 1
44
Answer 1
• The purpose of triage is to ensure the right patient receives appropriate timely treatment in the right place before he/she deteriorates.34
• A systematic method ensures quick work flow process.34
34. Pearson WS, et al. Prehospital Emergency Care. 2012;16(3):323- 328
45

Answer 1
46
History (cont.)
• Patient was triaged as Green & attended by a medical officer.
• On examination:• GCS 15/15, BP 180/90 mmHg, HR 65, RR 16• L/W over right temporal parietal region (6 x 1 x 0.5) cm
• Management:• T&S• Allow discharge home with cap. mefenamic acid 500
mg PRN
Q2. Is the management adequate? Documentation?
47
Issues:1. Not following 4-step triage algorithm
(co-morbidities & age 65 year old)
2. GCS 15/15 (was documentation sufficient?)
3. BP 180/90 mmHg (any action or treatment required?)
4. L/W at right temporal parietal region of (6 x 1 x 0.5) cm in dimension (any underlying skull fracture?)
5. Discharge home (any care giver?)
48
Answer 2. Management Issues

49
• MHI is in danger of being underdiagnosed in ED.
• A study of patients who had a HI suggested that patients with a low risk of dying i.e. patients with MHI are at the greatest risk of inadequate diagnosis & treatment.
Answer 2. Underdiagnosis of MHI
in ED

50

51
Answer 3. Performing GCS

Answer 3. Documentation of GCS
• Documentation of GCS has 3 parts
1. What is the individual score?
2. Explanation (what did you see?)
3. What is the total score ?
• Example:
E2 eye open to pain, V3 response with sound,
M5 localising pain
GCS 10/15
52

History (cont.)
• Further history from neighbour:
▫ Patient stays alone & has history of DM, MR secondary to rheumatic heart disease & hypertension.
▫ He is on atenolol, glibenclamide & aspirin.
Q4. State your triage category & give your
reasons.
53

Answer 4
54
Triage category:
Yellow Zone
Reasons:1. Older adults
• Risk of injury/death increases after age 65
2. Anticoagulation & bleeding risk

55

Answer 5
• Initial management of patients with HI should be
performed according to primary survey of
trauma patients as recommended by Advanced
Trauma Life Support guidelines:• Airway patency & cervical spine protection
• Breathing
• Circulation & haemorrhage control
• Disability
• Exposure
56

Answer 5
57

Answer 5
58

Answer 5
59

History (cont.)
• Patient was brought in again to ED within 4 hours post-discharge for persistent vomiting & headache.
• His GCS was 11/15 (E3V3M5), hence planned for immediate plain head CT.
Q6. Where should this patient be triaged
now?
60

Answer 6
• Red zone
61

62
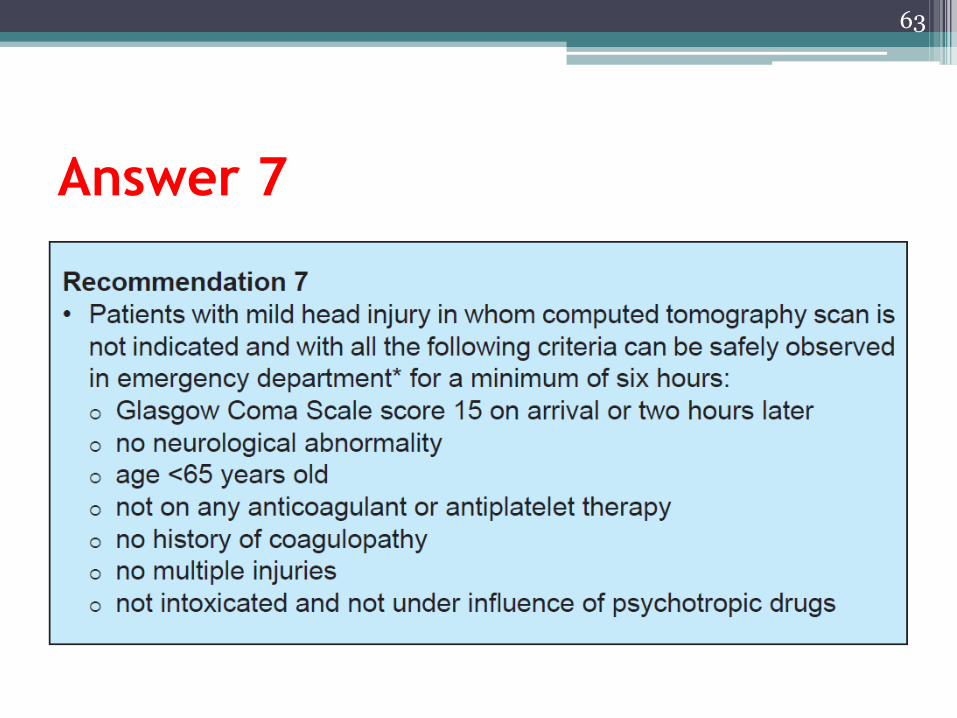
Answer 7
63

64

• Head chart
• CT scan of head & cervical spine
• Refer to neurosurgeon
65
Answer 8

66
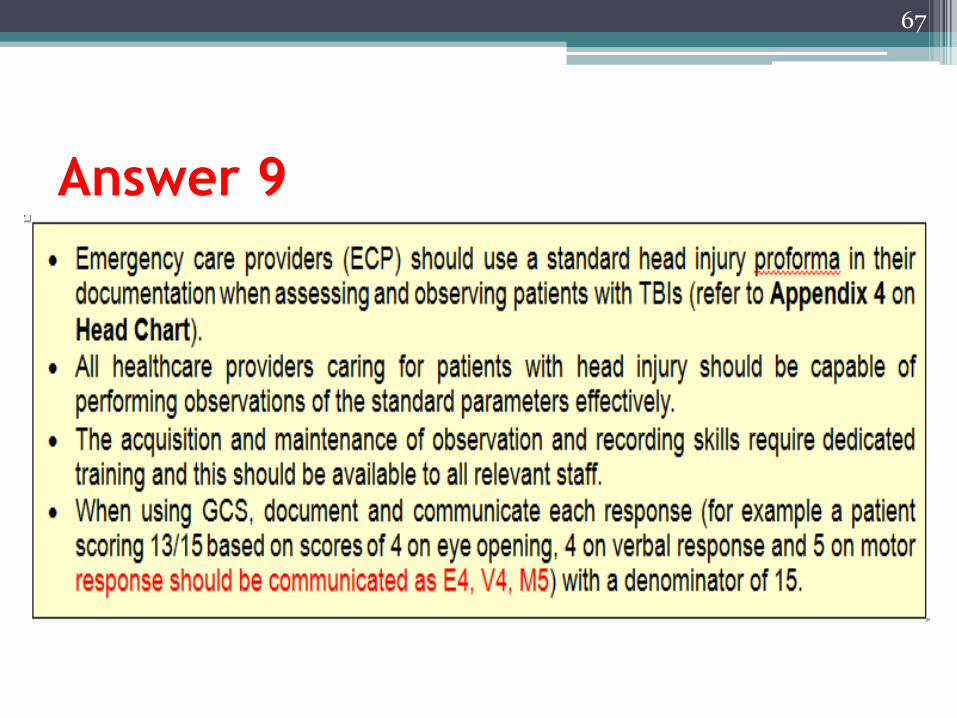
Answer 9
67
Answer 9
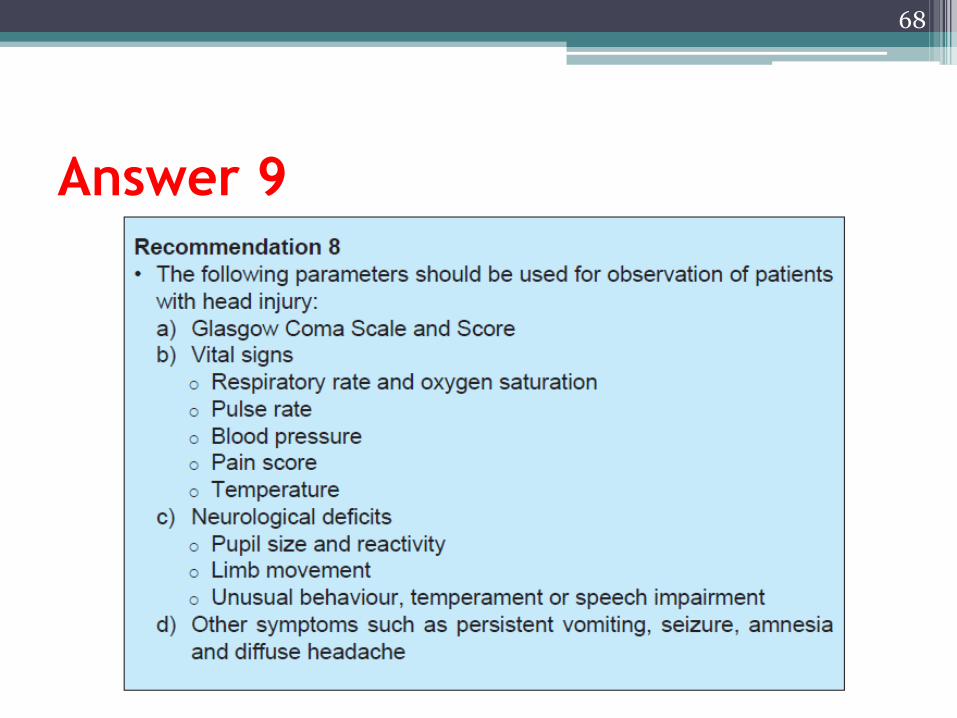
68

Answer 9
69

70
Answer 10
71

72
Answer 11
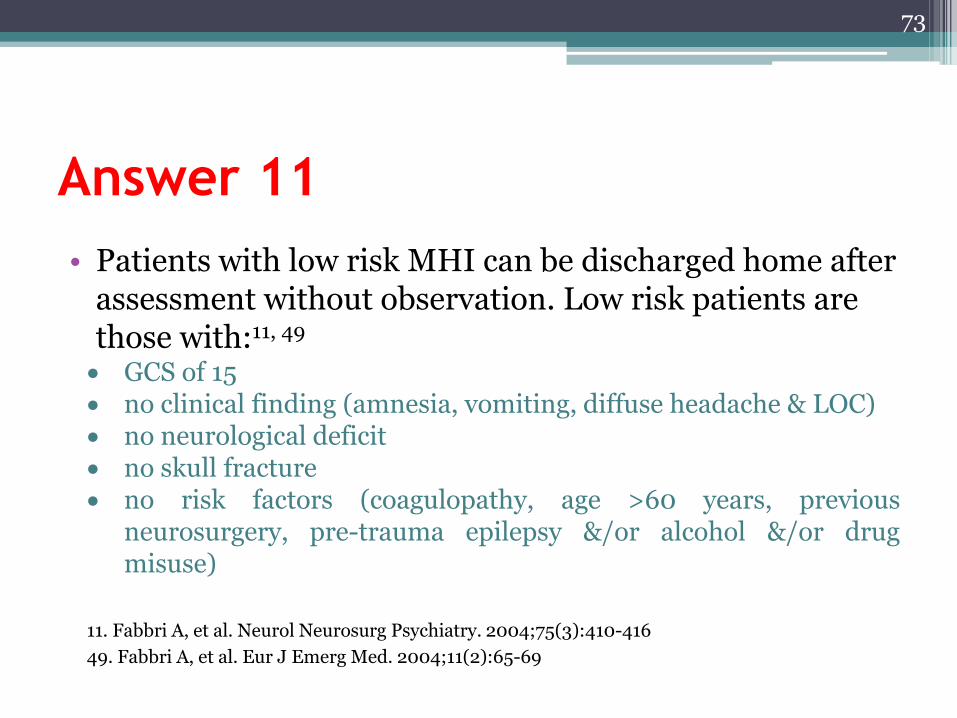
• Patients with low risk MHI can be discharged home after assessment without observation. Low risk patients are those with:11, 49
GCS of 15 no clinical finding (amnesia, vomiting, diffuse headache & LOC) no neurological deficit no skull fracture no risk factors (coagulopathy, age >60 years, previous
neurosurgery, pre-trauma epilepsy &/or alcohol &/or drugmisuse)
11. Fabbri A, et al. Neurol Neurosurg Psychiatry. 2004;75(3):410-416
49. Fabbri A, et al. Eur J Emerg Med. 2004;11(2):65-69
73

74

Answer 12
75

Answer 12
76
77
Thank You
CASE DISCUSSION 3.
SAFE TRANSFER
Dr. Tony Yong Yee Khong
General Surgeon, Hospital Sultanah Aminah, Johor
Dr. Mohd. Sofan Zenian
Neurosurgeon, Hospital Queen Elizabeth, Sabah
Dr. Zarina Yakof
Radiologist, Hospital Sungai Buloh, Selangor
78

History
• An 18-years-old motorcyclist, with h/o bikeskidded & fell, & was brought to hospital lessthan half an hour later▫ helmet was not buckled, sustained brief LOC, could
obey simple command, opened eye spontaneously &disorientated towards place
• He had scalp laceration on right frontal region,which was sutured.
• Vital signs - BP 122/80, PR 76• Primary survey showed no life threatening
injuries.
79

Question 1
• What is the initial GCS?
• What other important history should be taken/clinical signs to be noted?
• Does he need an immediate CT scan on presentation?
80
Answer 1• Initial GCS - 14 (E4V4M6)
• Medical/drug history whether he is on antiplatelet/anticoagulant.
• Whether he has been vomiting repeatedly or has other signs of increase ICP.
• Assess that he did not have focal neurological deficit, including cranial nerve deficit & no signs of base of skull fracture.
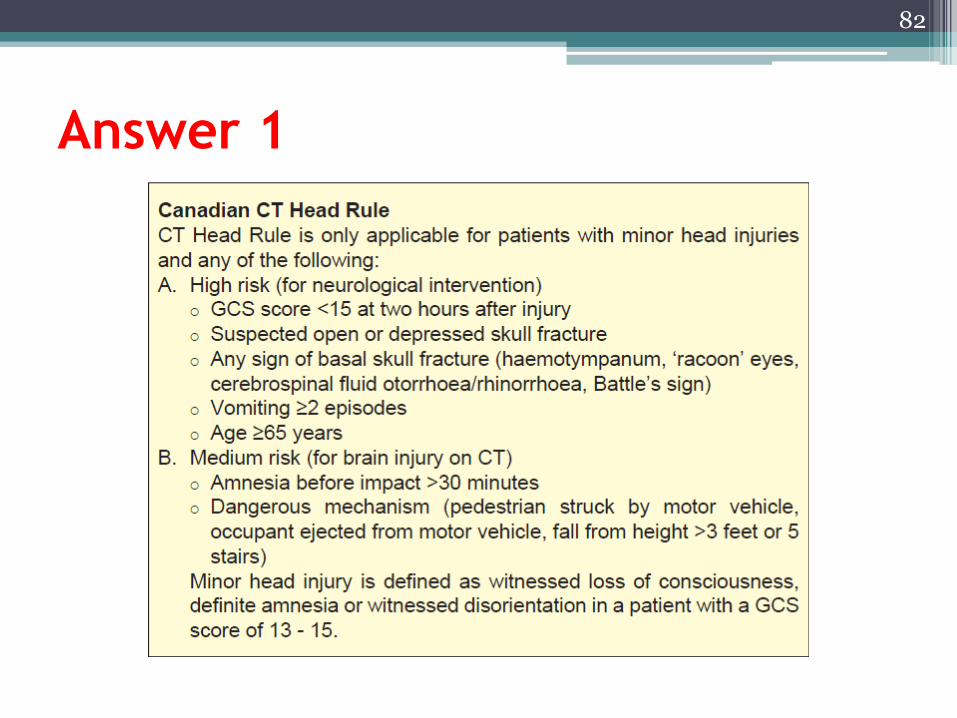
• No he does not need an immediate CT scan.• Based on CCHTR
▫ he needs to be observed until 2 hours post-injury
▫ if GCS is still <15 for head CT
81
Answer 1
82
History (cont.)
• He was seen in a district hospital without CT scan.
• GCS was still 14/15 at 2 hours post-injury.
• A CT head was indicated based on CCTHR
Q2. What should the attending doctor do?
83

Answer 2
• The doctor should call up the neurosurgical/surgical doctor of the receiving hospital with CT & neurosurgical/surgical service to transfer the patient with hospital ambulance & escorted by a doctor/paramedic.
84
History (cont.)
• This patient with GCS 14/15 had been put on cervical collar since pre-hospital management. Neck tenderness could not be elicited on examination.
Q3. Should you image the cervical spine?
What imaging modality would you
choose?
85

Answer 3
• Cervical collar should be kept because cervical injury cannot be cleared without a full GCS. In this case, since there is an indication for CT head, CT cervical is the imaging modality of choice.
86

History (cont.)
• On arrival to hospital with CT, BP dropped to 80/40 mm Hg with PR 110 just before head CT.
• Abdomen was soft, non tender.
• FAST scan revealed positive free fluid.
• Patient did not respond to resuscitation.
• GCS dropped to 10/15.
Q4. What should you do?
87

Answer 4
• Proceed to laparotomy
• CT scan can be performed later.
• CT scan brain/cervical should be done immediately after all source of life threatening bleed has been addressed & patient adequately resuscitated.
88

History (cont.)
• CT brain showed a frontoparietal SDH (thickness 1 cm) with midline shift.
• Definite neurosurgical intervention is required.
• While waiting for transfer, the staff nurse noticed patient’s pupils were unequal (Rt: 2 mm & reactive, Lt: 4 mm & sluggish to light).
• BP remained stable & no signs of Cushing’s reflex.
Q5. What should be done while
waiting transfer?
89

Answer 5
90

91

Answer 6
• Safe transfer practice include:▫ Ensure haemodynamic optimisation
▫ Secure ongoing bleeding prior to transfer
▫ Intubation
▫ Cervical immobilisation
▫ Necessary investigation results
▫ Transfer team should be trained in neuro-trauma management
▫ Reliable communication equipment
▫ Complete transfer checklist for neurosurgical patients
92

93

Answer 7• Transfer monitoring will include pupil size & reaction to
light, cardiac monitoring, BP, pulse oximetry, capnography (if available) ± urine output.
• Targeted parameters:▫ MAP >80 mmHg, PaO2 >97.5 mmHg, PaCO2 35 to 40 mmHg,
SpO2 > 90%
94

95

Answer 8
• Effective communication between referring hospital & neurosurgical centre plays very important role in managing this patient:▫ Allows accurate & reliable information to be conveyed,
& patient worsening clinical condition continuously updated during transfer
▫ Minimises the transit time in ED▫ Allows anaesthetist & OT to be ready & prepared
earlier▫ Allows operation to be executed ASAP once patient
reach the neurosurgical centre
96

97
Thank You
CASE DISCUSSION 4.
SPECIAL CONSIDERATION
Dr. Vanitha Sivanaser
Anaesthesiologist
Hospital Kuala Lumpur, Kuala Lumpur
98

History
• A 69-years-old man with medical problems▫ He was a pillion rider & had a fall from a motorbike.
▫ He sustained bruises on his upper limbs & an abrasion on his scalp.
▫ He was brought into the ED by ambulance.
99

Past medical history
• Medical problems - coronary artery disease, hypertension & hyperlipidaemia
• He is on regular follow-up with the cardiologist & compliant to his medical therapy of tab. aspirin 150 mg OD & tab. clopidogrel 75 mg OD.
• He takes tab. amlodipine 10 mg OD for his hypertension control.
• His hyperlipidaemia control is obtained by tab. atorvastatin 20 mg OD.
100

Examination at ED
• His GCS was E4V5M6.
• Abrasion wound was oozing but did not require suture.
• Pupils were bilaterally reactive 3+/3+.
• Limb movements were symmetrical.
101

Investigations
• FBC: ▫ Hb 12 gm/dL
▫ Platelet 250,000
• PT - 12 secs
• PTT 0 - 35
• INR - 1.2
102
Q1. What is your next step of
management?a. Skull x-ray (KIV discharge)
b. CT Scan brain (KIV discharge)
c. Admission with or without imaging
d. No imaging
e. ……?
103

• Skull X-ray in a patient with HI on antiplatelet therapy▫ A normal skull x-ray does not exclude ICH & may miss
a fracture.
104
Answer 1. Pitfall 1

Answer 1. Pitfall 2• CT scan in a patient with injury on antiplatelet
therapy▫ Risk factors for urgent scan
Age >65 years old
A history of bleeding/clotting disorder or on anticoagulant &/or antiplatelet (Algorithm 3)
105

History (cont.)
• CT scan brain showed small punctate haemorrhage. Othwersie rest of the findings were normal.
• The patient has a good caregiver, stays 5 minute drive from the hospital with transportation available.
Q2. Do you admit or discharge the
patient?
106

Answer 2
107

History (cont.)
• He was referred to the neurosurgeon & physician for further input & management.
• Ix reviewed:▫ Hb 12 gm/dL, platelet 250,000, PT - 12 secs, PTT 0 -
35, INR - 1.2
• Attending doctor ordered:▫ Continued antiplatelet
▫ Allowed discharge
Q3. What are your comments?
108

Answer 3. Pitfall 3
109
• To continue or withhold antiplatelet therapy in a patient with HI on antiplatelet therapy▫ Physician advised to continue.
• Patients with pre-injury use of antiplatelet agents (e.g. clopidogrel & aspirin) are at an increased risk for mortality with blunt traumatic ICH.76
• Achieving rapid control of haemorrhage is important as the haemorrhagic expansion in traumatic ICH occurs within the first 24 hours after injury77 & is an independent predictor of mortality.78
• Conclusion:▫ Antiplatelet need to be withold if any abnormal CT findings
present.
76. Wong DK, et al. J Trauma. 2008;65(6):1303-1308
77. Narayan RK, et al. J Neurotrauma. 2008;25(6):629-639
78. Davis SM, et al. Neurology. 2006;66(8):1175-1181

History (cont.)
• Attending doctor ordered:▫ Withold antiplatelet
▫ To transfuse 4 units of platelets & discharge after platelets transfusion
Q4. What are your comments?
110

Answer 4. Pitfall 4
• Transfusion of platelet concentrates in a patient with HI on antiplatelet therapy.▫ Attending doctor asked to transfuse platelets.
• Platelet transfusion in adults with pre-injury aspirin & traumatic ICH showed inadequate evidence to support the routine use of platelet transfusion in the ED. There was higher mortality among these patients.80
80. Nishijima DK, et al. J Trauma Acute Care Surg. 2012;72(6):1658-1663
111

History (cont.)
• No bed available in ward. Patient was observed in ED.
Q5. How long should the patient be
observed?
112

Answer 5.Pitfall 5
• Duration of observation in ED of patient with HI on antiplatelet therapy.▫ Patients with MHI (GCS 15), >65 years old, on low
dose aspirin with systolic BP <150 mmHg & presenting with initial negative primary head CT, should have a routine repeat head CT within 12 - 24 hours to accurately identify HI or such patients should be subjected to a prolonged hospital observation for at least 48 hours.45
45. Tauber M, et al. J Trauma. 2009 ;67(3):521-5
113

114

Answer 6. Pitfall 6
115
• Discharge criteria in a patient with HI on antiplatelet therapy.
• Antiplatelet therapy has to be sorted out.• Brain CT imaging has to be done.• Adequate observation in hospital.• Presence of responsible adult to monitor at home.
• Discharge instructions to patients & care giver should highlight the following alarming features:99
▫ GCS <15 (unable to open eye spontaneously, disorientated or unable to obey command)
▫ vomiting
▫ headache
▫ amnesia
▫ seizure
▫ neurological deficit 99. Fung M, et al. Brain Inj. 2006;20(9):889-894

History (cont.)
• If the same patient came in to hospital, had a drop of GCS & a positive Brain CT finding of a ICH requiring surgery.
Q7. What should you do?
116
Answer 7
• Antiplatelet therapy would have to be stopped.
• Transfusion of platelets pre-operative procedure should commence.
• Further ordering of platelets in OT.
117
118
Thank You