carl van laer
TRANSCRIPT

www.nkokleinbrabant.beCarl Van Laer
Jorn Potvin



Multidisciplinair en complex
VS


Vertigo vs duizeligheid, ijlhoofdigheid, instabiliteit, nausea,…
Synoniemen (draailoos?)
Vertigo
Tinnitus

Klassieke - maar niet zo praktische - indeling: perifeer vs centraal


Eén enkele episode van verlengde vertigo
Neuritis vestibularis
Hersenstam en cerebellaire laesies (CVA, TIA,..)
Eerste aanval van vestibulaire migraine
Eerste aanval van Menière
Praktische – maar niet zo gekende indeling - : obv symptomatologie

Recurrente vertigo en duizeligheid
Recurrente vertigo
Vestibulaire migraine
Benigne recurrente vertigo
Meniere
Vertebrobasilaire TIA
Vestibulaire paroxysmie of recurrente vestibulopathie (neurovasculaire compressie)
Perilymfe fistel
Recurrente duizeligheid
Orthostatische hypotensie
Hartritmestoornis
Psychogene duizeligheid
Medicatie geïnduceerde duizeligheid

Chronische duizeligheid
Patienten met voorgeschiedenis van vertigo
Psychogene vertigo
Visuele vertigo
Chronische migraineuze vertigo
Eind stadium Meniere
Patienten met progressieve onevenwicht
Bilateraal verlies vestibulaire functie
Neurologische oorzaken

Orthostatisch hypotensie
“maar mijn bloeddruk is normaal dokter ! “
-> orthostatische hypotensie kan evengoed bij perfect normale of goed gecontroleerde bloeddruk

Hyperventilatie

Vertigo: anamneseanamnese
• SO STONED Mnemonic:
• Symptoms: Describe the symptoms. (vertigo, instability, dizziness, drunken sensation, tendency to fall, falling over, etc.)
• Occurrence: How often do the symptoms occur? (Daily, weekly, monthly, irregular, etc.)
• Since: When did the symptoms occur? (Several weeks ago, several months ago, after a flu, after a fall, fifteen years ago, etc.)
• Triggers: What causes symptoms or aggravates them? (Head movements, bending over, looking up, laying down, turning over in bed, walking down the isles of a supermarket, watching vigorous movement, nothing in particular/spontaneously.)
• Otological symptoms: Are there any ear related symptoms possibly accompanied by head symptoms? (E.g. tinnitus, hearing loss, a sensation of fullness in the ear, ear pressure, hyperacusis or sensitivity to sound.)
• Neurological symptoms: Are there any neurological symptoms, possibly accompanied by head symptoms? (E.g. headache, migraine, light flashes, photophobia, phonophobia, difficulties in speech, loss of consciousness, syncope, tingling.)
• Evolution: How did and how do the symptoms evolve? (E.g. worse in the beginning then better, worsening, constant, ups and downs.)
• Duration: How long does the dizziness last? (Seconds, minutes, hours, days, continuously.)
Prof F Wuyts

Vertigo: klinisch onderzoekKlinisch onderzoek
Klinisch perifeer vestibulair onderzoek (Frenzelonderzoek)spontane of blikrichtingsnystagmusoogvolgbewegingenDix-Hallpike

Vertigo: klinisch onderzoekKlinisch onderzoek
VOR = Vestibulo Oculaire Reflex-> te testen via HIT (head impuls test)

Vertigo: klinisch onderzoekKlinisch onderzoek
Klinisch perifeer vestibulair onderzoek (Frenzelonderzoek)spontane of blikrichtingsnystagmusoogvolgbewegingenHIT (head impulse test): correctiesaccade?

HIT (head impulse test): correctiesaccade?= head thrust test-> aangedane kant = kant met correctiesaccade

Vertigo: klinisch onderzoekKlinisch onderzoek
Nystagmus: complex !!

Vertigo: spoed vertigo: sneltestAcuut?? Cerebellair CVA (PICA)
MRI >>> CT

Stroke?
HINTS?
Head-Impulse
Nystagmus
Test-of-Skew
INFARCT?
Impulse Normal
Fast-phase Alternating
Refixation on Cover Test
Kattah JC • Talkad AV • Wang DZ • Hsieh YH • Newman-Toker DEHINTS to diagnose stroke in acute vestibular syndrome: bedside oculomotor examination more sensitive than early MRI DWI
Stroke. 2009 Nov;40(11):3504-10

Vertigo: ENG (electronystagmografie) is nu VNG (videonystagmografie)ENG
VOR? Nystagmi? Oogvolgbewegingen? Dix Hallpike? Opto- en oculometrie? +Calorische testen: hypofunctie?

Vertigo: Beeldvorming: MRI (> CT), indicatiestelling

Vertigo: ziektebeelden
Acuut?? Cerebellair CVA (PICA)

Vertigo type
Spell duration
Spell frequency
Triggers
Associated symptoms
Rotational vertigo or dizziness
Minutes to hours
Daily, weekly
Spontaneous, visual
Photofobia, phonophobia, scotoma, photopsia, …Headache doesn’t have to occur simultaneouslyPersonal or family history of migraine
Vestibular migraine
Thomas Brandt • Michael Strupp • Marianne DieterichFive keys for diagnosing most vertigo, dizziness, and imbalance syndromes: an expert opinion
J Neurol (2014) 261:229–231

Vestibulaire migraineVertigo: vestibulaire migraine

• Vestibular migraine• A. At least 5 episodes with vestibular symptoms of moderate to severe intensity, lasting 5 minutes to 72 hours
• B. Current or previous history of migraine with or without aura according to the International Classification of Headache Disorders (ICHD).
• C. One or more migraine features symptoms with at least 50% of the vestibular episodes: (1) headache with at least two of the following characteristics: one sided location, pulsating quality, moderate or severe pain intensity, aggravation by routine physical activity; (2) photophobia and phonophobia; (3) visual aura
• D. Not better accounted for by another vestibular or ICHD diagnosis.
• Probable vestibular migraine• A. At least 5 episodes with vestibular symptoms of moderate or severe intensity, lasting 5 min to 72 hours.
• B. Only one of the criteria B and C for vestibular migraine is fulfilled (migraine history or migraine features during the episode).
• C. Not better accounted for by another vestibular or ICHD diagnosis.
Vestibular Migraine (VM) criteria
Lempert T et al. Vestibular migraine: diagnostic criteria. J Vestib Res. 2012;22(4):167-72.

Vertigo type
Spell duration
Spell frequency
Triggers
Associated symptoms
Rotational vertigo
< 1 minute
Only when triggered
Head movements
Thomas Brandt • Michael Strupp • Marianne DieterichFive keys for diagnosing most vertigo, dizziness, and imbalance syndromes: an expert opinion
J Neurol (2014) 261:229–231
Positionele vertigo: canalo- of cupulolithiasisBPPV

BPPV: Benigne Paroxismale Positie Vertigo
BPPV is een vorm van positionele vertigo en wordt gekenmerkt door acute draaiduizeligheid die ontstaat bij bewegingen, bijvoorbeeld bij omhoog kijken (hyperextensie van de nek) en omdraaien in bed.
De draaiduizeligheid kan heftig zijn, maar duurt gewoonlijk maar een tiental seconden.
De klachten zijn uitputbaar, dat wil zeggen dat herhaling van de hoofdbewegingen de klachten doet verminderen of verdwijnen. Van dit laatste wordt gebruik gemaakt voor de behandeling.
Deze positionele klachten moeten onderscheiden worden van orthostatische hypotensie (orthostatisme) en cervicogene vertigo.
Eerste aanval kan zich presenteren als een acuut vestibulair syndroom (acute vertigo - tot en met zelfs braken soms -duurt kort maar patiënten voelen zich nog 1 à 2 dagen ongemakkelijk)

Thomas Brandt • Michael Strupp • Marianne DieterichFive keys for diagnosing most vertigo, dizziness, and imbalance syndromes: an expert opinion
J Neurol (2014) 261:229–231
BPPV: Benigne Paroxismale Positie Vertigo
www.nkokleinbrabant.be Praktische info
Nuttige documenten Positionele vertigo type BPPV

Vertigo type
Spell duration
Spell frequency
Triggers
Associated symptoms
Rarely rotational vertigo
Minutes to hours
Positional
Head movements not related to SCC axis
Cervicalgia, tension in the neck, headache
Proprioceptive cervicogenic vertigo
Dario Yacovino • Timothy C. HainClinical Characteristics of Cervicogenic-Related Dizziness and Vertigo
Semin Neurol 2013;33:244–255

Proprioceptive cervicogenic dizziness
Dario Yacovino • Timothy C. HainClinical Characteristics of Cervicogenic-Related Dizziness and Vertigo
Semin Neurol 2013;33:244–255
Cervicogene duizeligheid
Er zijn vele synoniemen voor deze ‘cervicogenic dizziness’, waarbij duizeligheid of andere evenwichtsklachten gerelateerd is bij nekbewegingen bij patiënten met klachten van de nek (bv bij artrose van de nek, na whiplash trauma,…). Het is een uitsluitingsdiagnose: eerst moeten alle andere diagnoses uitgesloten worden. Er zijn verschillende theorieën, waarvan de meest bekende de veranderde proprioceptieve input van de nekspieren naar het evenwichtsorgaan is. Cervicogeneduizeligheid moet gedifferentieerd worden van vertebrobasilaire insufficiëntie (VBI), waarbij er bij VBI meestal andere klachten zijn zoals visusproblemen (minder zicht, dubbelzicht), hoofdpijn, vallen

Orthostatische hypotensie
Bij orthostatische hypotensie is er meestal enkele seconden na opstaan (van zit naar staan of van lig naar staan) een licht, instabiel, duizelig gevoel (soms met zwarte vlekken). Bij (snel) opstaan gaat het bloed met zwaartekracht naar de benen en is er een reflex van de spieren rond de bloedvaten van de benen om het bloed snel terug naar het hoofd te duwen om alert te blijven. Bij orthostatisme is deze reflex wat vertraagd, vaak gewoon door wat ouder te worden. Het is belangrijk om te weten dat dit even goed kan voorkomen bij patiënten met een normale bloeddruk.

Vertigo type
Spell duration
Spell frequency
Triggers
Associated symptoms
Rotational vertigo
> 20 minutes to 12 hours
Weekly, monthly
Spontaneous
Unilateral SNHL, feeling of pressure, tinnitus
Ménière’s disease
Thomas Brandt • Michael Strupp • Marianne DieterichFive keys for diagnosing most vertigo, dizziness, and imbalance syndromes: an expert opinion
J Neurol (2014) 261:229–231

• Certain• Definite Ménière’s disease + histopathologic confirmation
• Definite• ≥ 2 definitive spontaneous episodes of vertigo ≥ 20 minutes to 12 h
• audiometrically documented low- to medium-frequency sensorineural hearing loss at least one occasion before, during or after one of the episodes of vertigo
• fluctuating aural symptoms (hearing, tinnitus or fullness) in the affected ear
• Probable• two or more episodes of vertigo or dizziness, each lasting 20 minutes to 24 hours
• audiometrically documented hearing loss at least one occasion
• fluctuating aural symptoms (hearing, tinnitus or fullness) in the affected ear
• Possible• episodic vertigo of the Ménière type without documented hearing loss and/or
• sensorineural hearing loss, fluctuating or fixed, with disequilibrium but without definitive episodes
Ménière’s Disease (MD) criteria
Lopez-Escamez JA et al. Diagnostic criteria for Menière's disease. J Vestib Res. 2015;25(1):1-7.

Vertigo type
Spell duration
Spell frequency
Triggers
Associated symptoms
Vertigo, nausea, vomitus
Uren tot een dag hele zieke patient, nadien elke dag stap per stap beter
éénmalig
Geen (stress?, viraal?)
Erg zieke (anders gezonde) patient zonder enige neurologische uitval enhorizontale nystagmus altijd naar dezelfde kant
Thomas Brandt • Michael Strupp • Marianne DieterichFive keys for diagnosing most vertigo, dizziness, and imbalance syndromes: an expert opinion
J Neurol (2014) 261:229–231
Vestibular neuritis (neuritis vestibularis)

neuritis vestibularis
Neuritis vestibularis RECHTS
=
Valneiging (lateropulsie) naar RECHTS
=
Nystagmus naar LINKS (omdat ‘de richting’ van een nystagmus per conventie wordt benoemd naar zijn ‘snelle kan’)

Stroke or neuritis?
anterior inferior cerebellar artery
= AICA
posterior inferior cerebellar artery
= PICA

Acuut vestibulair syndroom (AVS)
Stroke or neuritis?
7.4% AICA infarction presents like a labyrinthitis
17% PICA infarction without associated neurological symptoms
Brain CT has 16% sensitivity to detect posterior circulation stroke
Nut CT ??? Medicolegaal, uitsluiten bloeding,…

Vertigo type
Spell duration
Spell frequency
Triggers
Associated symptoms
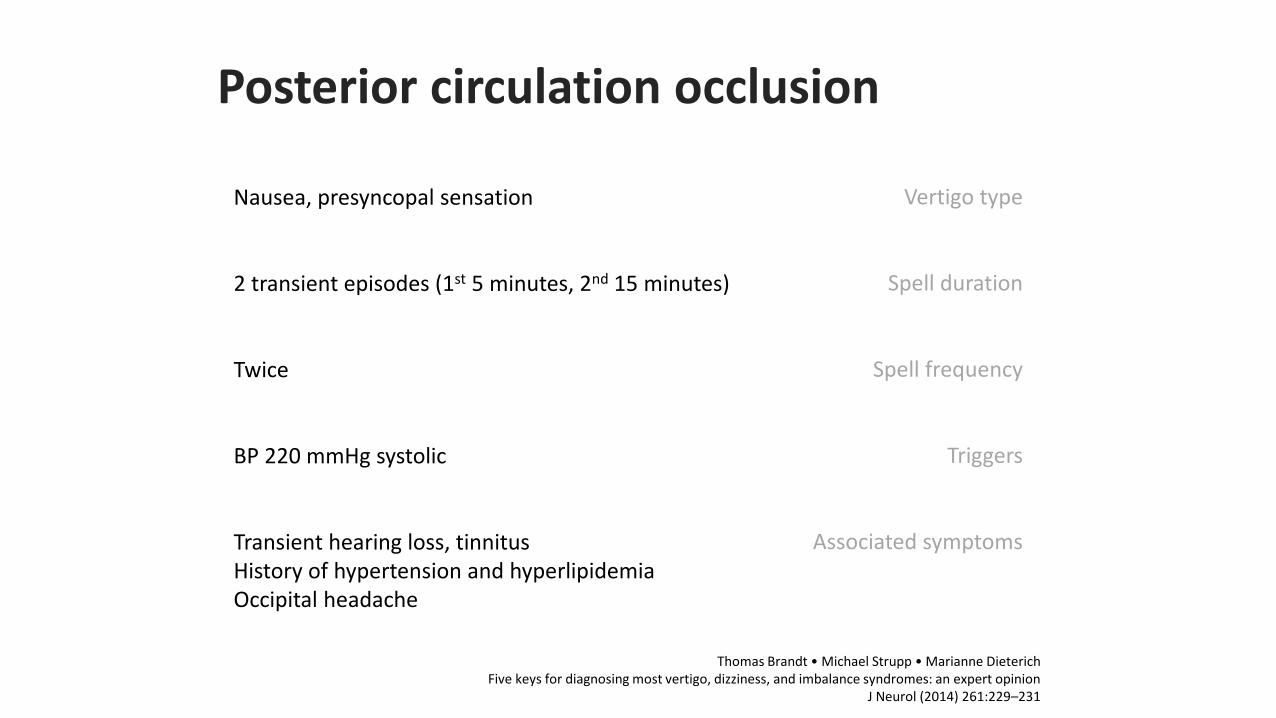
Nausea, presyncopal sensation
2 transient episodes (1st 5 minutes, 2nd 15 minutes)
Twice
BP 220 mmHg systolic
Transient hearing loss, tinnitusHistory of hypertension and hyperlipidemiaOccipital headache
Thomas Brandt • Michael Strupp • Marianne DieterichFive keys for diagnosing most vertigo, dizziness, and imbalance syndromes: an expert opinion
J Neurol (2014) 261:229–231
Posterior circulation occlusion

Posterior circulation ischemic events incl. approx. 20% to 25% of all strokes and TIAs
TIAs can present with isolated vertigo episodes weeks-months prior to a completed infarction
Approximately 5% of TIA patients suffer a stroke within 48 hours and rapid treatment reduces stroke risk by up to 80%
Patients with posterior circulation TIA have an even higher stroke risk than those with anterior circulation spells
Dizziness is the most common presenting symptom of vertebral artery dissection which affects younger patients, mimics migraine, and is easily misdiagnosed.
Posterior circulation occlusion
Newman-Toker DE et al. TiTrATE - A Novel, Evidence-Based Approach to Diagnosing Acute Dizziness and Vertigo.
J Neurol (2014) 261:229–231

How much of AVS is caused by non-vestibular and non-cerebrovascular causes? 50%
• Alcohol, opiates
• Phenytoin, carbamazepine, phenobarbital, benzodiazepines, lithium
• SSRI withdrawal
• Volatile hydrocarbons (toluene, pesticides, etc.)
• CO
• Electrolyte abnormalities
• Hypoglycaemia
• Thiamine (vit. B1) insuff
Stroke or neuritis?

Frequent dizziness and instability spellsFrequent duizelig en instabiel-> “ de NKO-speciallekes”
- vestibulaire paroxysmie- superior semicirculair kanaal dehiscentie- vestibulair schwannoom (acousticusneurinoom)

Vertigo type
Spell duration
Spell frequency
Triggers
Associated symptoms
Rotational vertigo or ataxia
Seconds to minutes
Up to 30 episodes each day
Spontaneous, hyperventilation, head and body position
Hearing loss, tinnitus
Vestibular paroxysmia
Thomas Brandt • Michael Strupp • Marianne DieterichFive keys for diagnosing most vertigo, dizziness, and imbalance syndromes: an expert opinion
J Neurol (2014) 261:229–231
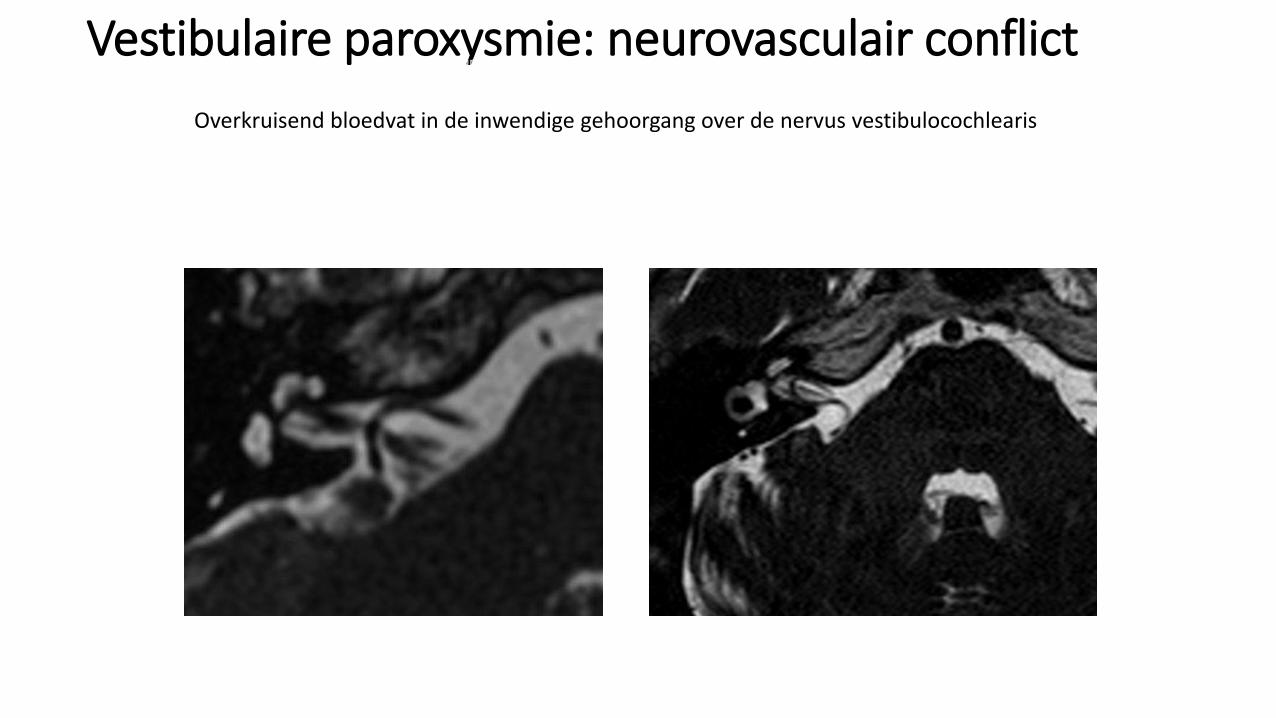
Vestibulaire paroxysmie: neurovasculair conflictVestibulaire paroxysmie
Overkruisend bloedvat in de inwendige gehoorgang over de nervus vestibulocochlearis

Vestibulaire paroxysmie
A. Short vertiginous spells
B. One or several of the next triggers: • Rest, head position or changes in position
C. One or several of the following characteristics:• No other symptoms, disturbance of stance, disturbance of gait,
unilateral tinnitus, unilateral aural fullness, unilateral reduced hearing
D. One or several of the following additional criteria:• Neurovascular conflict with the VIII cranial nerve, hyperventilation-
induced nystagmus, increase of vestibular deficit measured by ENG, treatment response to anti-epileptics
E. Symptoms can not be explained by other diseases
1 Jannetta et al. Surg. Forum, 1975. 2 Hufner et al. Neurology 2013.
1 Jannetta et al. Surg. Forum, 1975. 2 Hufner et al. Neurology 2013.

Superior semicircular canal dehiscenceSymptoms at baseline• Autophony
present 10/10• Pulsatile tinnitus
present 8/10• Hyperacusis of bone conducted sounds present 7/10• Tullio phenomenon present 4/10• Pressure-induced vertigo present 3/10• C-VEMP (verlaagde drempels, verhoogde amplitude

Symptom at baseline• SSCD
• Autophonypresent 9/9
• Pulsatile tinnitus present 7/9
• Hyperacusis of bone conducted sounds present 6/9• Tullio phenomenon
present 4/9• Pressure-induced vertigo
present 3/9
fat plug
bone paté

Vestibular schwannoma
A vestibular schwannoma is a benign primary intracranial tumor of the myelin-forming cells of the vestibulocochlear nerve (8th cranial nerve). A type of schwannoma, this tumor arises from the Schwann cells responsible for the myelin sheath that helps keep peripheral nerves insulated.[1]
Although it is commonly called an acoustic neuroma, this a misnomer for two reasons. First, the tumor usually arises from the vestibular division of the vestibulocochlear nerve, rather than the cochlear division.
Second, it is derived from the schwann cells of the associated nerve, rather than the actual neurons (neuromas)

Intracanalicular
Small (1-10 mm)
Medium (11-20 mm)
Moderate (21-30 mm)
Large (31-40 mm)
Giant (>40 mm)

vestibular schwannoma
cochlear nerve
vestibular nerve
caudal cranial
facial nerve

Ménière’s disease + vestibular migraine
Vestibular migraine + vestibular paroxysmia
Ménière’s disease + vestibular migraine + vestibular paroxysmia
Superior semicircular canal dehiscence + vestibular paroxysmia
Superior semicircular canal dehiscence + vestibular migraine
Bilateral areflexia + proprioceptive cervicogenic dizziness
Vestibular schwannoma + vestibular migraine
…
Vallen buiten beschouwing: duizeligheid bij de geriatrische patiënt en cardiale problematiek (aritmieën,...)
Combo

Vestibular migraineonderhoudsmedicatie: flunarizine 10mg voor slapen (<6maanden, gewichtstoename), propranolol,
amitriptyline (redomex), pizotifen, topiramaatacuut: sumatriptan, dimenhydrinate, diazepam,..,
BPPVrepositiomanoeuvres
Ménière’s diseaseAcuut: vestibulaire suppresiva (bv aggyrax), Onderhoudsmedicatie: betahistine en diuretica (co-amiloride, dytenzide is uit de handel), low-salt diet,
caffeine-restriction, intratympanale gentamycine of corticosteroïdenVestibular paroxysmia
(ox)carbamazepine, neurovasculaire decompressie (weinig evidentie)
Superior semicircular canal dehiscenceheelkunde
proprioceptive cervicogenic dizzinessfysiotherapie, kine, osteopathie, fysische geneeskunde, NSAID,…
Vestibular schwannoma wait and scan, heelkunde, gammaknife radiotherapie
Posterior circulation occlusion: neurologie
TLC, psychologische behandeling,
Behandeling

www.nkokleinbrabant.beCarl Van Laer
Jorn Potvin