carbohydrates monosaccharides d-glucosed-galactose
Post on 21-Dec-2015
229 views
TRANSCRIPT

CarbohydratesCarbohydrates
• Monosaccharides
D-glucose D-galactose

Reducing substance: hydroxyl group near an aldehyde or ketone group can react with Cu2+, converting it to Cu+
D-glucose D-fructose

• Disaccharides
Lactose
reducingend

Maltose
reducingend

Sucrose not a reducingsubstance

• Polysaccharides
Cellulose
reducingend

Glycogenbranches every8-12 glucose units
Amylopectinbranches about every24-30 linear linkages

Intestinal absorption of carbohydrates
Jejunum villimicrovilli

Intestinal absorption of carbohydrates
Starch
Glycogen
-amylase
saliva andpancreaticjuice
maltose
sucrose
lactose
galactose
GUTMICROVILLIBRUSHBORDER
BLOOD
glucose
fructose
galactose
glucose
fructose
Monosaccharides
1
2
3

Glucose Production Glucose Consumption
Glycogen (75%)
Glucose
Bloodglucose
125g
50g
50g
brain
rbcwbc
muscle
fat cell

Glucose transportersName Tissue Function
GLUT1 (erythrocyte) wide distribution, esp. brain, kidney, colon, fetal tissues
Basal glucose transport
GLUT2 (liver) Liver, -cells of pancreas, small intestine, kidney
Non-rate-limiting glucose transport
GLUT3 (brain) Wide distribution, esp. neurons, placenta, testis
Glucose transport in neurons
GLUT4 (muscle) Skeletal muscle, cardiac muscle, adipose tissue
Insulin-stimulated glucose transport*
GLUT5 (small intestine) Small intestine, kidney, skelatal muscle, brain, adipose tissue
Fructose transport
*insulin low…GLUT4 in intracellular compartments; insulin high…GLUT4 translocates to membrane

Glucose Production Glucose Consumption
Glycogen (75%)
Glucose
Bloodglucose
125g
50g
50g
pyruvatelactate (10-15%)
certainamino acids (10-15%)
glycerol (2%)
CO2
CO2
brain
rbcwbc
muscle
fat cell

Regulation of blood glucose
• Glycogenesis: glucose glycogen
(liver, muscle)
• Glycogenolysis: glycogen glucose
• Gluconeogenosis:
non-CHO sources glucose
• Glycolysis: glucose CO2 + H2O + ATP
• Renal threshold: proximal convoluted tubule
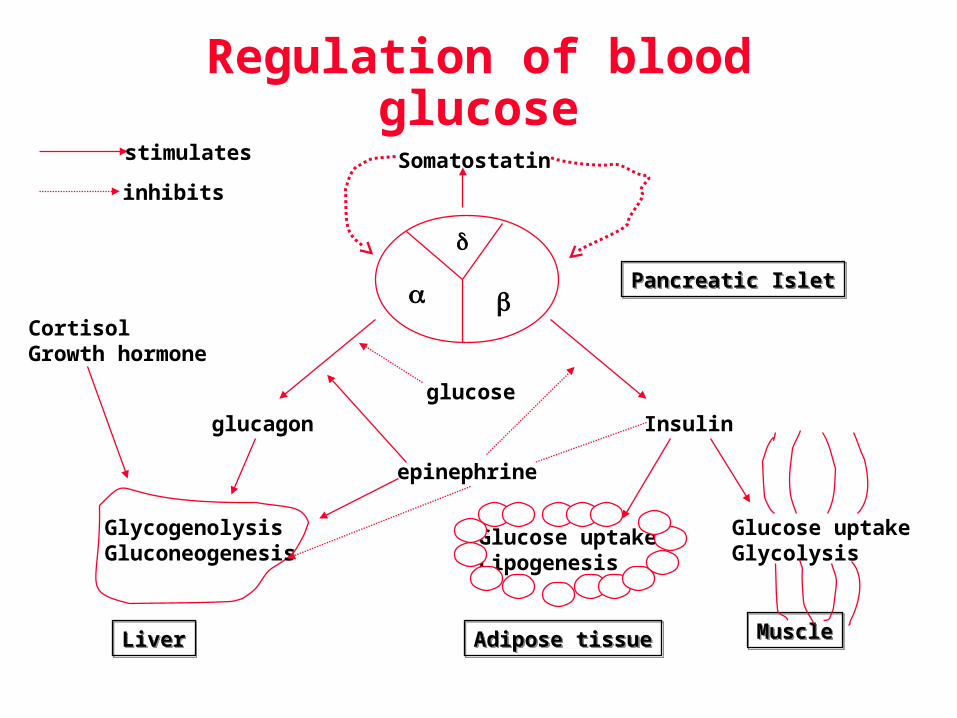
Regulation of blood glucose
Glucose uptakeLipogenesis
Glucose uptakeGlycolysis
Insulin
Pancreatic IsletPancreatic Islet
Somatostatin
glucose
epinephrine
glucagon
CortisolGrowth hormone
GlycogenolysisGluconeogenesis
LiverLiver Adipose tissueAdipose tissue MuscleMuscle
stimulates
inhibits

Determination of glucose• Specimens used
– whole blood
» used with home glucose monitoring units
» cellular use of glucose gives 7% decrease/hour
» NaF preserves glucose 24 hr, RT
• cannot use such a specimen for enzyme assays, especially urease
» lithium iodoacetate preserves glucose; does not interfere with urease
» capillary blood = fasting venous level + 5 mg/dL
– plasma, serum
» 10-15% higher level than whole blood glucose
» RI: 70-105 mg/dL
– CSF
» RI: 60-70% plasma glucose = 40-70 mg/dL
– urine
» RI: <30 mg/dL random; <500 mg/24 hr

Glucose MethodsGlucose Methods• hexokinase
glucose + ATP gluc-6-PO4 + ADP
gluc-6-PO4 + NAD+ 6-phosphogluconate + NADH + H+
INT + NADH + H+ formazan + NAD+
– most widely used
– reference method against which others are compared
– serum, plasma and urine
– avoid hemolysis
HK
G6PD
PMS

Glucose MethodsGlucose Methods• glucose oxidase
glucose + O2 gluconic acid + H2O2
H2O2 + reduced dye oxidized dye + H2O• peroxidase reaction interference by uric acid, vitamin C, bilirubin
• suitable for spinal fluid
measure O2 consumption via pO2 electrode• suitable for all body fluids
measure H2O2 production via H2O2 electrode• suitable for plasma, serum, whole blood
GO
POD

• glucose dehydrogenase
glucose + NAD+ D-gluconolactone + NADH + H+ » highly specific as “GDH-NAD”, with little interference, EXCEPT…
• Pyrroloquinolinequinone (“GDH-PQQ”)
– 2005 FDA warning
– giving false increased glucose readings when patient is receiving maltose, icodextrin (dialysis), galactose, d-xylose
Glucose MethodsGlucose Methods
GDH
Manufacturer Proper Name Sugar
Octapharma Immune Globulin Intravenous (Human)
Maltose10%
Talecris Immune Globulin Intravenous (Human)
Maltose9-11%
Cangene Rho(D) Immune Globulin Intravenous (Human)
Maltose10%
Cangene) Vaccinia Immune Globulin (Human Maltose10%
NERL Diagnostic d-Xylose Usual dose 25g
Baxter Peritoneal dialysis soln (icodextrin) 7.5 mg/dL icodextrin

• glucose dehydrogenase
glucose + NAD+ D-gluconolactone + NADH + H+ » highly specific as “GDH-NAD”, with little interference, EXCEPT…
• Pyrroloquinolinequinone (“GDH-PQQ”)
– 2005 FDA warning
– giving false increased glucose readings when patient is receiving maltose, icodextrin (dialysis), galactose, d-xylose
» Coulometry• http://www.medisense.com/au
• FreeStyle glucometer, Abbott Laboratories
• Electrons released in the reaction are measured as a current
• Allows very small volume (0.3 uL) to be used, with results in 15 seconds
Glucose MethodsGlucose Methods
GDH

• oxidation-reduction reactions Fe3+ Fe2+ or Cu2+ Cu1+
• least specific for glucose
Glucose MethodsGlucose Methods
Clinical Significance
• Hyperglycemia– diabetes mellitus
– endocrine disorders
» acromegaly: incr. growth hormone
» Cushing’s syndrome: incr. cortisol
» thyrotoxicosis: incr. T4
» pheochromocytoma: incr. epinephrine
– drugs
» certain anesthetics
» steroids

• Hypoglycemia– insulin overdose
– drugs
» sulfonylureas
» antihistamines
– alcoholism (long term)
– insulinoma
– galactosemia
– glycogen storage diseases
Clinical Significance

• Diagnosis of Diabetes Mellitus– Symptoms of diabetes mellitus
» Polyuria
» Polydipsia
» Unexplained weight loss
– Any TWO of the following tests, on different days
» Casual plasma glucose > 200 mg/dL
» Fasting plasma glucose (FPG) > 126 mg/dL
» 2hr Post prandial glucose (PPG) > 200 mg/dL after a meal with 75g glucose load
Expert Committee on the Diagnosis Expert Committee on the Diagnosis and Classification of DM - 2005and Classification of DM - 2005
• Type 1– Type 1a
» characterized by beta cell destruction caused by an autoimmune process, usually leading to absolute insulin deficiency
» patients must take insulin to survive
» usually young, with acute onset (days to weeks)
» islet-cell antibodies usually present
– Type 1b
» idiopathic
Expert Committee on the Diagnosis Expert Committee on the Diagnosis and Classification of DM - 2005and Classification of DM - 2005

Expert Committee on the Diagnosis Expert Committee on the Diagnosis and Classification of DM - 2005and Classification of DM - 2005
• Type 2– insulin resistance in peripheral tissue and an insulin
secretory defect of the beta cell
– variable [insulin]
– highly associated with a family history of diabetes, older age (>40), obesity and lack of exercise
– more common in
» Women
» African American
» Hispanics
» Native Americans

• “Other specific types” – pancreatic, hormonal disease
– Pancreatitis, cystic fibrosis
– Acromegaly (GH), Cushing’s syndrome (cortisol)
– drug/chemical toxicity
– insulin receptor abnormalities
– no renal or retinal complications
Expert Committee on the Diagnosis Expert Committee on the Diagnosis and Classification of DM - 2005and Classification of DM - 2005

• Gestational diabetes mellitus– pregnancy
– frequent but transitory glucose intolerance
– greater risk of perinatal complications
– placental lactogen?
– > 140 mg/dL one hour after 50-g glucose load screening
– TWO of four results abnormal in 100 g glucose load test:
– fasting plasma glucose > 105 mg/dL
– > 195 mg/dL at 1 hr
– > 165 mg/dL at 2 hrs
– > 145 mg/dL at 3 hrs
Expert Committee on the Diagnosis Expert Committee on the Diagnosis and Classification of DM - 2005and Classification of DM - 2005

National Diabetes Association National Diabetes Association 20032003
• Pre-diabeteshttp://diabetes.niddk.nih.gov/dm/pubs/diagnosis/index.htm
http://www.diabetes.org/pre-diabetes.jsp
Fasting Plasma Glucose Diagnosis Result (mg/dL)
70 – 99 Normal
100 to 125 Pre-diabetes(impaired fasting
glucose)
126 and above Diabetes mellitus**Confirmed by repeating the test on a different day.

• Glucose tolerance test (still used for gestational diabetes diagnosis)– patient preparation
» normal diet three days prior to test
» no food after regular evening meal on day before test
» take fasting blood, urine specimen
» drink 100 g glucose load within 5 minutes
» allow water, but no food, chewing gum, smoking, exercise during test
» specimens taken 1, 2, 3 hours after ingestion
Clinical Significance
Plasma glucose (mg/dL)
Minutes after glucose ingestion60 120 180
100
200
Normal
Diabetic

• Other conditions, tests associated with diabetes mellitus– white cell antigens
» HLA types DR3, DR4, DQB1*0302
» Note that diabetes resistance genes = DR2, DQB1*0602
– lipid studies
» hyperlipoproteinemia type IV• increased TG
– microalbuminuria
– microangiopathies
» retinal, renal, neural
Clinical Significance

Management of diabetes mellitus
• Glycated hemoglobin (A1)
COOH
COOH
COOH COOH
COOH
COOH
H2N
H2N
H2N
H2N H2N H2N
N N
gluglu
non-enzymatic process conversion of HbA into HbA1 at N-terminal valine

• Glycated hemoglobin– irreversible reaction occurring throughout the 120-day
life span of rbc
– reflects timed average [glucose] over previous 4-8 weeks
– HbA1c = 80% total glycohemoglobin
– reference range: 3-6% total Hgb
– uncontrolled diabetes mellitus: 12-20% total Hgb
– controlled: 9-12% total Hgb
• Considerations when measuring HbA1c
– abnormal hemoglobins can also be glycated
– variability in levels of “labile fraction” (intermediates)
Management of diabetes mellitus

For every 1% decrease in HbA1c, risk of microvascular complications is reduced by 35%
Diabetes Care 2000, 23: S27-S31
Management of diabetes mellitus

• Manual Methods for HbA1c compared
Management of diabetes mellitus
Ion-exchangechromatography
AffinityChromatography
PrincipleHbA HbA1c
++
+ ++
++
+
+
-- - - - - -- - - - - - - - - -- -- - -
“Fast fraction” HbA1c
elutes firstpba
pba
pbapba
HbA--Val--N | CH2
| C=O | HOCH | HCOH | HCOH | CH2OH
HbA1c
elutes last
Phenylboronic acid

• Manual Methods for HbA1c compared– other non-glycated Hb measured
» IEC: HbF and any others with charge like A1
» AC: none– time
» IEC: 2-3 hrs» AC: 15 minutes
– glycated hemoglobins measured» IEC: A1a, 1b, 1c only» AC: any glycated hemoglobin, including
abnormals– temperature sensitive?
» IEC: yes» AC: no
Management of diabetes mellitus

• Automated Method for HbA1c
– High pressure liquid chromatography (HPLC)
– Cation exchange method
» the eluant must be __________________
» The first form of hemoglobin eluting from the column must be _________________________
» The last form of hemoglobin eluting from the column must be __________________________
Management of diabetes mellitus


• Attempts to convert HbA1c value to “mean blood glucose” value– Nathan et al, 1984 using linear regression on data
from 21 patients
– 33.3 (%HbA1c) – 86
– Examples: 6.0% = ~115 mg/dL 7.5% = ~165 mg/dL 9.0% = ~215 mg/dL
Management of diabetes mellitus


• Revised calculation, effective 3/21/05– Rohlfing et al, 2002 using comparison data from
1500 patients
– (35.6 x %HbA1c) – 77.3
– Examples: 6.0% = ~136 mg/dL 7.5% = ~190 mg/dL 12.0% = ~350 mg/dL
– Only valid for A1c values between 6 and 12%
Management of diabetes mellitus

• Glycated serum proteins– albumin (“fructoseamine”)
– turnover = 2-3 weeks
– rapid method using tetrazolium dye reduction
colored product
Management of diabetes mellitus
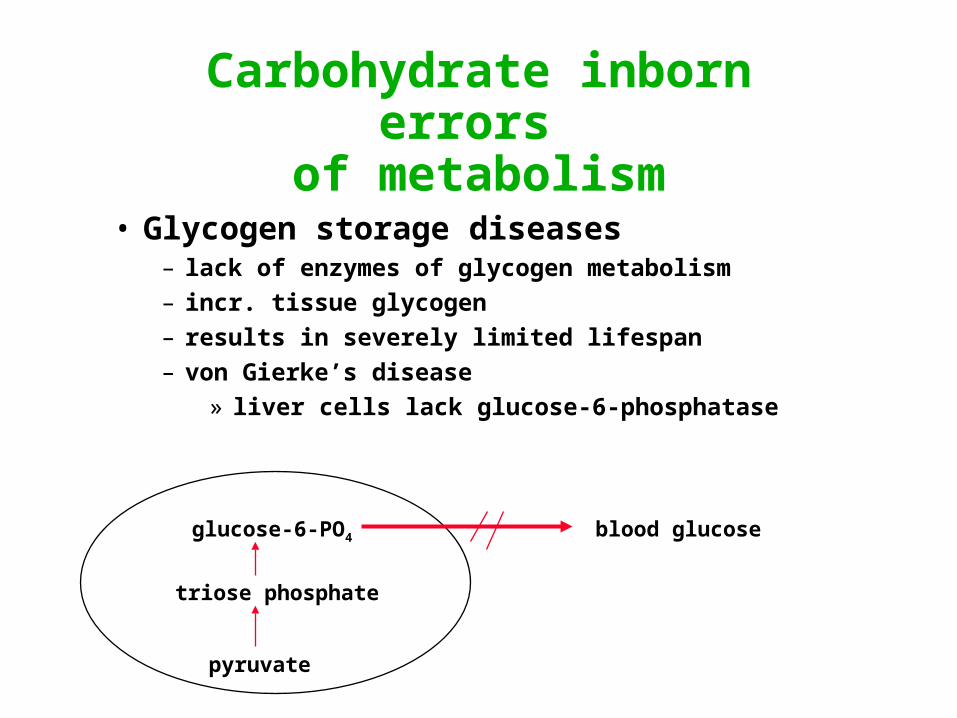
Carbohydrate inborn errors of metabolism
• Glycogen storage diseases– lack of enzymes of glycogen metabolism
– incr. tissue glycogen
– results in severely limited lifespan
– von Gierke’s disease
» liver cells lack glucose-6-phosphatase
pyruvate
triose phosphate
glucose-6-PO4 blood glucose

• Lactose intolerance– deficiency in intestinal mucosal lactase
– GTT done as baseline
– 2nd day, give lactose instead of glucose
– normal: normal GTT curve
– abnormal: flat curve ( and much pain!)
Carbohydrate inborn errors of metabolism

• Galactosemia(1) galactose galactose-1-PO4
galactilol
(2) galactose-1-PO4 UDP-galactose
(3) UDP-galactose UDP-glucose cataracts
(4) UDP-glucose glucose-1-PO4
– deficiency in uridyl transferase *
– results in galactosuria, retardation, cataracts, no conjugation of bilirubin
– urine tests
Carbohydrate inborn errors of metabolism
galactose + O2 galactose dialdehyde + H2O2
gal. oxidase
*

• Complication of uncontrolled diabetes mellitus– Acid-base imbalance
– Can be life-threatening
– Acetone, acetoacetate, -hydroxybutyrate
Ketones
fatty acids amino acidsacetyl CoA
TCA cycleCO2
H2O
ATP
Ketones acetoacetate B-hydroxybutyrate acetate
Bloodketones

• Complication of uncontrolled diabetes mellitus– Sodium nitroprusside
– B-hydroxybutyrate dehydrogenase
Ketones
fatty acids amino acidsacetyl CoA
TCA cycleCO2
H2O
ATP
Ketones acetoacetate B-hydroxybutyrate acetate
Bloodketones

Extra slides

Glycogenesis, glycogenolysis
• Hormones involved– fed: insulin from pancreatic beta cells (Islets of Langerhans)
» preproinsulin proinsulin (A, B and C peptides)
insulin + C-peptide
» anabolic (synthesis)
» promotes cellular uptake of glucose
» increased:
• lipogenesis
• protein synthesis
• glycogenesis
» decreased:
• lipolysis
• ketone formation
• gluconeogenesis
• glycogenolysis

• Hormones involved– fasting: glucagon from pancreatic alpha cells
» catabolic
» liver: glycogen converted to glucose, released into blood
» muscle: glycogen converted to glucose-6-PO4, remains in the muscle cell for its own energy needs
– “fight or flight” : epinephrine from adrenal medulla
» action similar to glucagon
Glycogenesis, glycogenolysis

• Stimulation of insulin release– glucose
– leucine, arginine, histidine, phenylalanine
– sulfonylureas (tolbutamides)
– ACTH, GH
• Inhibition of insulin release– thiazide diuretics
– dilantin (antiseizure)
– human placental lactogen (diabetes of pregnancy)
• Decreased tissue response to insulin– glucocorticoids obesity
– estrogens inactivity
– progestins low CHO diet
Glycogenesis, glycogenolysis

Gluconeogenesis
• cortisol (hydrocortisone)– from adrenal cortex
– inhibits glucose entry into muscle, connective tissue, lymphoid tissue
– stimulates release of gluconeogenic amino acids from muscle
– promotes conversion of amino acids into glucose by liver
– stimulates lipolysis in adipose cells, releasing glycerol for conversion to glucose by liver
• ACTH– from anterior pituitary
– stimulates production of cortisol

• NOTE!!– if serum/plasma is not separated from cells soon after
collection, cellular use of glucose will continue, causing a falsely decreased glucose result
• proximal convoluted tubule– reabsorbs all glucose if <180 mg/dL
– glycosuria results if blood glucose >180 mg/dL
Glycolysis
Renal Threshold