cancer services prioritization guidelines for covid-19...breast cancer visit prioritization for...
TRANSCRIPT

Cancer Services
Prioritization Guidelines for COVID-19
Updated 4/6/20

Cancer Services Prioritization Guidelines for COVID-19
Table of Contents
Patient Prioritization Definitions Page 3
Breast Care Center Page 4
Colorectal Surgery Page 7
Endocrine Neoplasia Page 8
Genitourinary Urologic Oncology Page 9
Gynecologic Surgical Oncology Page 13
Hepatobiliary & Pancreas Oncology Page 18
HPB / Surgical Oncology Page 24
NET Program Page 26
Orthopedic Oncology Page 27
Head & Neck Surgery Page 28
Neuro-Oncology Page 31
Thoracic & Sarcoma Oncology Page 34
Melanoma & Skin Cancer Program Page 38
Radiation Oncology Page 41

Patient Prioritization Definitions
Priority A • Deemed critical (unstable, unbearable suffering, and/or whose condition is
immediately life threatening) and for whom there is effective treatment. • Their immediate need is greatest and we must find ways (either in the
geographic area of the pandemic or elsewhere) where treatment can be instituted or continued.
Priority B • Deemed to be non-life threatening who can be deferred and services that may
be discontinued during a wave of the pandemic event. • Physicians will determine that these patients are not put at undue risk. If their
priority changes, they will be moved to priority A and treated at a cancer center or other appropriate facility somewhere in the province or country.
Priority C • Services may be discontinued during the entire pandemic event (multiple waves
of 6-8 weeks). • These patients are, for the most part, undergoing routine follow-up or screening
and can reasonably wait until the pandemic is over.

Breast Cancer Visit Prioritization for COVID 19
Priority A- In-person visits: New diagnosis invasive cancer
For new diagnoses: prioritize in person visits for neoadjuvant therapy (need exam), and new metastatic patients
Follow-up patients Early stage or metastatic patients receiving active chemotherapy Complex and symptomatic patients better served by in-person assessment Study patients on IV therapy, or those on experimental oral agents that require in person visits
Priority B - Video visits: Early stage breast cancer
Low risk new patients who have had surgery and need hormone therapy
New early stage post surgery who need additional testing, such as genomic testing, in order to make decisions about treatment
Early stage patients in follow up on hormone therapy or adjuvant antibody therapy (although these patients must come in for GnRH agonists, or infusions)
Metastatic disease Patients with stable metastatic disease on oral therapy (with laboratory tests performed locally
or at UCSF)Second opinion new or follow-up consultations
Early and late stage disease
Priority C - Reschedule in 3+ months:
Same day mammogram and survivorship visits (mammo being rescheduled so ok to reschedule both to keep synchronized)
Early stage breast cancer for routine follow-up, not on medications or not recently started on new therapy
Patients unable to do video visit

M emo: COVID plan for Breast Team
From: Laura Essermanand Breast Surgery Faculty, Residents,Admin and Nursing team
Steps being instituted to reduce chance of transmission
Surgical W orkforce and Caseload
1) Keep surgeons working at one hospital
a. SFGH: We will cancel our cases (3 non cancer cases) and clinic for this week. We
are happy to see any urgent cancer patientsat Mission Bay in the coming
weeks. Next week (3/24), our schedule was already closed due to planned
fellowsh ip interviews. We will re-evaluat ethis plan next week to see where we
are and discuss how we can best care for our patientsmoving forward. There wi ll
be a conference call at the end of t his week to determine how best to triage
urgent cancer casesat SFGH to M B. Jasmine has alreadybeen in touch wit h
SFGHand they approve this plan.
b. Mt Zion: Effectiveimmediately, no cases will be performed at Mt Zion. The
cancer cases scheduled for Wednesdayand Thursday will either be postponed or
moved to MB. Merisa Piper is cancelling her electiveprocedures and so we will
have capacity for the urgent cases
2) Cancel all elective surgical cases
a. Any casethat is not cancer will be postponed for at least 1 month
3) Safely delay cancer cases when ever possible
a. We already use a neoadjuvant approach for our high risk cancer cases. Those
patients that have complete d that therapy will be prioritized for comp letingtheir
surgical treatment. The I-SPY2 TRIALwill remain open for t hosepatients at
highestrisk. Borderline patients will get neoadjuvanttherapy, but off study to
minimize exposure for addit ionalimaging. We will get crit icalimaging to assist
optimalcare both on and off t rial.
b. Those patientsnewly diagnosedwi ll be placed on neoadjuvant therapy, even if
lower risk. All hormone therapy patientscan have 1-2 months of adjuvant
hormonal therapy safely- this will give us informat ion about response to
t reatment . All patients will be contacted
c. We have 2 research studiesthat can help us to mitigate anxiety about waitingfor
surgery for patients with DCIS. For hormone positivepatients, we havean active
surveillance protocol that allows DCIS pat ients to be placed on hormonal
therapy. Fort unate ly, we have treated 100 patientsth is way and know that it is
safe to wait 3 months. There is a protocol for women wit h high risk and
hormone negative DCIS w here we are injecting pembro into the lesions. We
have treate d 13 patientsto date and all but 1 has had a robust immune infiltrate,
suggesitng that a 2-3 month delaymay be beneficial here.
d. I have alreadycontactedthe breast radiolo gy leadership,as well as the MRI
study leadership,that we will need to monitor t hesepatients with MRI. We will
work with themto provide screeningand help everyone safely add on imaging
11 BCC Response Strategy

studies to make sure we are givingpatients optimal care. Aldea will work with
me to provide a plan to support COVID screeningfor the imaging side of our
practice
All SPECIALTIES
4) Reduce in person visits to diminish exposure for patientsand providers and staff
a. Second opinion patientswillbe asked if they just want assurance that their
current plans are suffic ient- these willbe converted to video visits. Our breast
surgery fellows will help to complete those calls
b. All follow -ups will be moved forward by 3 months (there is no essential follow-up
at this t ime except for people who aresymptomatic). We are callingpatients and
moving their visits out.
c. Patients undergoing active treatment who have essential visits and consults or
those with new cancers who need treatment started will beseen in person
d. Routine screening (non-cancer and post cancer t reat ment) will be postponed for
3 months
e. Evaluation of mild breast pain and any bilatera l breast pain will be postponed for
1-2 months
f. New breast masses willstill be booked for in clinic evaluation
5) Radiation Oncology recommendsthat we delay the start of radiation therapy for 3
months postoperatively. Video visits for evaluation and reassurance will be conducted.
6) Any cases where patients have marginal if any benefit from adjuvant radiation, surgery,
or systemic therapy will be counseled and advised to defer or avoid treatment.
Telehealth visits can be used for all such consults
7) Additional protection for Faculty and staff who are immunocomprom ised
a. Anyone wit h an underlyingcondition lowering their immune system will be
advised to stay home and work from home. THIS INCLUDES WOMEN IN THEIR
THIRD TRIMESTER OF PREGNANCY. I would suggest that this be standard policy
across the board.
8) We were able to tr iage 26 surgical cases for the last 2 weeks of March. We will meet as
a team to review the next month's schedule and send in a more extended list for the
entire month. We will work as a teamto determine the best way to deploy resources in
a multidisciplinary way to keep patients and staff as safe as possible duringthis period
of time.
21 BCC Response Strategy

Colorectal Surgery Case Prioritization definitions/examples
1. Priority A : (urgent) diagnoses/cases that should be done within 7 days or the patient will potentially suffer adverse consequences
a. Obstructing colon cancer b. Obstructing rectal cancer (diversion needed to start therapy) c. Active sepsis from intraabdominal pathology (crohns, UC, diverticulitis,
iatrogenic and referred) d. Perianal sepsis with pain, active abscess e. Ulcerative colitis that is sick and not responding to tx (inpatient)
2. Priority B: (non-urgent but priority) diagnoses/cases that should be done within 1
month or the patient will potentially suffer adverse consequences a. Colon cancer b. Rectal cancer and has completed neoadjuvant tx c. Ulcerative colitis that is sick and not responding to tx (outpatient but high level
of sickness-weight loss anemia malaise etc) d. Diverticulitis that is actively symptomatic (colovesical fistula, colon stricture
causing LBO, untreatable abscess, phlegmon) e. Crohns disease with ileal/colonic stricture or abscess who has failed medical
therapy or cant go on biologics due to sepsis and is sick(cant leave hospital)
3. Priority C: (elective) can wait several months if not more depending on case a. Rectal cancer new diagnosis—encourage total neoadjuvant therapy b. Staging right hemi for appendiceal ca or polyp that is removed and need LN c. FAP that does not have clear cancer d. Loop ileostomy takedown for any diagnosis e. Colostomy takedown (diverticultis, perforation, etc) f. Stoma revision for any reason g. Diverticulitis h. Ulcerative colitis for dysplasia or steroids that are not weaned i. Crohns disease with ileal/colonic stricture failed medical therapy and is NOT sick j. Serial anal fistula surgery (if seton in place and drained well) k. Rectourethral fistula that is diverted l. Rectovaginal fistula m. Rectal prolapse

Endocrine Neoplasia priority cases (which need to be going within 4 weeks), also called ‘High’ priority, or Tier 3 CMS:
Adrenal: Adrenocortical cancer, or rapidly growing tumors Hypercortisolism of adrenal origin that cannot be controlled medically Pheochromocytoma or paraganglioma that cannot be controlled medically
Parathyroid: HPT with life-threatening hypercalcemia that cannot be controlled medically
Thyroid: Life-threatening or severely symptomatic Graves’ that cannot be controlled medically Goiter causing airway compromise Thyroid cancers that are threatening the life or the health of the patient such as those
with short double timings, locally aggressive, or aggressive recurrences. Open biopsy to confirm a suspected diagnosis of anaplastic thyroid cancer or thyroid
lymphoma in order to direct appropriate treatment Pediatric thyroid cancer
General: Endocrine disorders in pregnant patients that are dangerous to the health of the mother
or fetus that cannot be controlled medically (i.e. hypercalcemia, or severe functional thyroid disorder which are not controllable medically)

GU Medical Oncology Patient Prioritization Definitions
Priority A • Condition deemed critical (unstable, unbearable suffering, and/or whose
condition is immediately life threatening) and for whom there is effective treatment.
• Their immediate need is greatest and we must find ways (either in the geographic area of the pandemic or elsewhere) where treatment can be instituted or continued.
• E.g., patients with locally advanced/metastatic prostate cancer, patients with germ cell tumor receiving systemic potentially curative treatment, new brain metastasis, failing SOC therapy and need clinical trial option, need for palliative surgery or radiation; curative surgery or radiation in high-risk patient
Priority B • Condition deemed non-life threatening whose services can be deferred or
continued with adjusted frequency during a wave of the pandemic event. • Physicians will determine that these patients are not put at undue risk. If their
priority changes, they will be moved to priority A
• E.g., patients with castration-sensitive prostate cancer currently responding to ADT – can potentially delay/lengthen LHRH analog treatment intevals, space out laboratory evaluations
Priority C • Condition deemed stable whose services may be discontinued or deferred during
the entire pandemic event (multiple waves of 6-8 weeks). • These patients are, for the most part, undergoing routine follow-up or screening
and can reasonably wait until the pandemic is over. • E.g., germ cell tumor patients on long-term surveillance

GU Medical Oncology Patient Priorities
Priority Category
Patient Category
Delivery of Care Comments
Priority A
Condition critical: life- threatening, unstable
Established Patients
- Clinic appt: Convert to video if appropriate
- Treatment: Continue IV treatment. Ship oral drugs to patient home if possible; refer to surgery and radiation if palliative or potentially curative treatment required
- Clinical trials: Utilize SOC option if one exists. Prioritize trial enrollment for pts without other treatment options. Ship oral clinical trial drugs to patient home if at all possible
- Consider lowest frequency dosing schedule of infusions, e.g. q 4-6 month Lupron, q 6 week pembrolizumab
New Patients
- Clinic appt: Discuss urgency with provider, schedule for appt, video if appropriate.
- Treatment: Start treatment - Clinical trials: Utilize SOC option if
one exists. Prioritize trial enrollment for pts without other treatment options.
- Patients with active malignancy requiring active treatment for which UCSF is primary oncology provider
- Patients seeking clinical trial options with limited/no SOC options available
Priority B
Condition stable: non- life- threatening
Established Patients
- Clinic appt: Delay or convert to video if appropriate
- Treatment: Continue treatment - Procedure: Refer to
surgery/radiation when appropriate, potentially defer referral if referral is for palliation of mild symptoms
- Clinical trials: Utilize SOC option if
- Consider lowest frequency dosing schedule of infusions e.g. q 6 month Lupron

one exists. Prioritize trial enrollment for pts without other treatment options.
New Patients
- Clinic appt: Discuss urgency with provider, schedule for appt, video if appropriate
- Clinical trials: Utilize SOC option if one exists. Prioritize trial enrollment for pts without other treatment options.
- Patients with metastatic cancer currently progressing and/or requiring clinical trial options
Priority C
Condition stable
Established Patients
- Clinic appt: Postpone - Surveillance scan: Postpone
- Triage urgency – if active issue, consider video visit rather than further delay
New Patients
- Clinic appt: Waitlist for future scheduling
- Surveillance scan: Postpone
- Stable patients seeking second opinions without current evidence of disease progression

GU Surgery Cancellation Guidelines Stage 1:
First cancellations
DSU (vas, circs, scrotal,
cyst, cystoscopy)
Possible RARP's
(depending on trust
cancer decision)
GA TP Biopsies
Benign nephrectomy /
Partial Nephrectomy
Andrology cases
Brachytherapy
Functional /
Reconstruction
Elective URS / PCNL
TURP / Holep / BPH
Ureterolysis
Stage 2: Secondary
cancellations
Cystectomy (lower risk
cancer) [ITU]
LA TP Biopsies (high
PSA)
TURBT (low cancer risk)
RARPs (h i gh ca ncer risk)
Nephroureterectomy
(low cancer risk)
Stage 3:
Last to be cancelled
Cystectomy (high risk
cancer) [ITU]
Nephrectomy (time
sensitive)
TURBT (high risk)
Orchidectomy
Nephroureterectomy
(high risk)
URS with stents or
ureteric stones
IVC invasive
nephrectomy [ITU]
Stage 4:
Emergency Cases only
Obstructed kidneys/
infection
Emergency urology -
abscesses / washout s
etc.
Torsion

Gyn Onc Patient Priorities (Draft 3/27/20)
Priority Category
Patient Category
Delivery of Care Exclusions / Comments
Priority A
Cancer patients on treatment
New patients with aggressive cancer diagnosis
Established Patients
- Clinic Appt: Convert to video visits when possible
- Treatment: Continue treatment;
- Procedure: Schedule for surgery
- Clinical trials: Treatment protocols at discretion of attending provider. CRC’s are not allowed to be on campus. There are no biobanking services.
- OK for inpatient chemotherapy
admissions at this time.
- For infusion patients and no issues/complaints, prefer Video visit in advance of Infusion. If issues/symptoms, can be seen in person.
- Consider chemo modifications within standard of care. 21d regimens versus weekly. Growth factor support for high risk patients.
- Oral antineoplastic regimen patients (PARPi, Letrozole/Everolimus) should be seen by Video visit.
- Orders need to be done by EMR or Docusign 2 days prior to treatment. Monday for Wednesday. Wednesday for Friday. Friday for Monday.
- Patients being seen treated by outside providers should be seen by Video visit.
- Asymptomatic recurrence patients should be seen by Video visit.
- Rad Onc treatment plans for cure or palliation should

proceed as needed, including brachytherapy procedures
New Patients
- Clinic Appt: Schedule for an appointment
- Treatment: Start treatment
- Procedure: Schedule for surgery
- Clinical Trials: Treatment protocols at discretion of attending provider
- We will continue to see new patients with a new diagnosis of cancer or a high suspicion for cancer.
- Atypical hyperplasia/FIGO grade 1 endometrial CA: all pathology must be reviewed at UCSF. If we do not yet have UCSF review, OK to see new patient as Video appointment.
- Pelvic mass: providers will review patients for Zoom versus in person appointments.
- Anyone who is a surgical candidate will need to be seen in person.
- All new surgical cases need to be submitted by Division Chief to Dr. Lobo before they will be scheduled by perioperative administration. 3a cases will be prioritized for surgery.
- Pre-op & Post-op patients should be seen by Video. Consents should be written out and reviewed at Video visit and then signed in Pre-op.
- Atypical hyperplasia & FIGO grade 1 endometrial carcinoma surgeries are considered 2a/2b. Suggested management of atypical

hyperplasia versus FIGO grade 1 endometrial carcinoma. If pathology recent, recommend progestin therapy (Megace, Levonorgestrol IUD). If pathology not recent, recommend repeat endometrial biopsy & imaging. Patients who are symptomatic despite progestins, or if progestins are contraindicated may be considered for hysterectomy. (3a)
- Second opinions can be deferred if they have primary oncologists/surgeons/radiation oncologists. We are available for direct consultation with their providers if needed. Consider Grand Rounds for other 2nd opinions.
Priority B
New patients with less suspicious pelvic masses, low malignant potential diagnoses
Established Patients
- Clinic Appt: Delay appointments if possible
- Treatment: Convert to video visits when possible
- Clinical Trials: Treatment protocols at discretion of attending provider
- Rad Onc treatment plans for adjuvant may be deferred.
New Patients
- Clinic Appt: Possible to be scheduled at a later date
- Determine the urgency to be seen
- Pelvic mass: providers will
review patients for Zoom versus in person appointments.

- Asymptomatic low risk pelvic mass surgeries will be deferred (1a or 1b)
- Atypical hyperplasia/FIGO grade 1 endometrial CA: all pathology must be reviewed at UCSF. If we do not yet have UCSF review, OK to see new patient as Video appointment.
-
Priority C Established - Clinic Appt: Postpone
- Treatment: Postpone
- Procedure: Postpone
- Postpone surveillance visits
(any 3 months or beyond). Reschedule in 3 months or offer NP.
- Radiology remains open but requires Covid-urgent assessment. Otherwise will be deferred. Consider outside facilities.
- Clinic patients with active issues will be seen by triaged for need of Video visit versus in person evaluation.
- Genetic Testing Station remains open for scheduling video visits and testing by mail.
Patients Asymptomatic
surveillance
patients
Cancer Risk
patients
Dysplasia
patients
New Patients
- Clinic Appt: Waitlist for future scheduling
- Treatment: Postpone
- Procedure: Postpone
-
- Cancer Risk new patients and RRSO surgeries will be deferred. Cancer Risk patients with symptoms of abdominal bloating or pelvic pain should be triaged for evaluation.

- High grade dysplasia and
AIS patients will be referred to Dysplasia clinic. If surgery indicated, patients will be referred back to Gyn Onc.
-

Hepatobiliary and Pancreatic Cancer Priority Scheme during the COVID-19 Pandemic
Diagnosis
CT scans will be prioritized in staging of patients as this will help determine the treatment course. If diagnostic endoscopic ultrasound (EUS) is not available, CT-guided core biopsy may be considered. EUS will be considered
on a case to case basis for diagnostic purposes.
Tumor markers such as CA 19-9, CEA and AFP should be obtained at diagnosis to evaluate future treatment response.
If patients require ERCP for biliary obstruction, they will be considered on a case by case basis.
ERCP interval for biliary stent exchanges will be longer than the 6-8 weeks’ timeline.
Treatment Planning New cases will be triaged similar to the workflow prior to the pandemic by the nurse navigators. If there is a surge that may
result in limited number of staff/provider (due to illness or due to work in other areas), cases with existing oncologists may not be seen as a formal consult (but, potentially a conversation with the primary oncologist can be considered).
Cases will be discussed during the multidisciplinary Tumor Board to determine the best treatment course.o The list of patients discussed during the Tumor Board meetings will be compiled weekly in a spreadsheet. This
spreadsheet will note the plan for surgery, systemic therapy or radiation therapy as the next step. o Tumor Board consensus will be recorded in a standardized note template using the Team Conference note type in
APeX. This note will be written by the primary APP or the MD of the patient who present the patient’s case. o These lists will be followed closely to determine if treatment recommendations are followed or need to be modified
during future multidisciplinary tumor board meetings.
Monitoring Treatment Response
If possible, CT scans may be delayed if there is a dependable tumor marker that can be followed monthly.
CT scans will be obtained when patient is being considered to surgical resection and radiation therapy.

Priority Category Patient Category Delivery of Care Exclusions / Comments
High Priority (treatment within 2 weeks)
Established Patients
Patients on systemic therapy, esp 1st line in first 6 mos of tx, or actively progressing and requiring subsequent line therapy
Patients on active treatment with radiation for sarcoma, gastric cancer, or pancreatic malignancies for whom surgery is indicated
- Clinic Appt: Convert to video visits when possible (should be possible for large majority, potentially with infusion center APP backup if vital signs off)
- Treatment: Evaluation of treatment response can be made by following tumor markers (when tumors expressed
Borderline Resectable Pancreatic Cancer Continue with neoadjuvant chemotherapy with consideration of surgical resection.
Locally Advanced Pancreatic Cancer - Continue with neoadjuvant chemotherapy up to 12 cycles. - If the patient has completed 12 cycles at the time of pandemic, surgery can be considered. - If surgical resection is not possible, consider radiation therapy in discussion with the multidisciplinary team.
Metastatic Pancreatic Cancer
- Surgery will be considered for patients already enrolled in neoadjuvant protocols in whom delay could negatively impact their outcome by allowing for recovery of residual cancer and thus losing the benefit invested in the neoadjuvant approach.
- Surgery will be considered for emergent and very aggressive tumors and/or tumors causing life-threatening complications including bleeding, fistulas, cholangitis, pancreatitis and perforations.

- Consideration for clinical trials will be
delayed until the clinical trials are active. - Systemic therapy will be continued. A therapy break can be considered if the patient has maximum response, has low volume of disease or has cumulative toxicity from the chemotherapy. - When possible and if applicable, 5FU maintenance can be considered in the form of capecitabine.
New Patients - Clinic Appt: Convert to video visits when possible (should be possible for large majority)
- Treatment: Borderline Resectable Pancreatic Cancer - Start with neoadjuvant chemotherapy (up to 12 cycles) prior to consideration of surgical resection. Radiation therapy can be considered as a potential bridge prior to surgery (will be determined case by case).
Locally Advanced Pancreatic Cancer - Start with neoadjuvant chemotherapy (up to 12 cycles). Consideration of potential surgery or
- Initial diagnosis of GI cancers requiring biliary drainage procedures, additional diagnostic evaluation via IR-guided biopsies, and preoperative preconditioning procedures (PVE, TACE/TARE).
- Patients with new diagnosis of GI cancer with symptomatic complications (bleeding, obstruction, infection or perforation) requiring treatment/hospitalization
- Patients should be prioritized by disease biology/ tumor aggressive and limited medical therapies (i.e Periampullary cancers, primary liver cancers).

radiation therapy can be evaluated at
the time of restaging scans.
Metastatic Pancreatic Cancer - Consideration for clinical trials will be delayed until the clinical trials are active. - Systemic therapy will be initiated without delay.
- Surgery is considered for emergent and very aggressive tumors and/or tumors causing life-threatening complications including bleeding, fistulas, and perforations.
Mod Priority (treatment within 2-6 weeks)
Established Patients Clinic Appt: - Convert to video visits when possible.
Treatment as above. - Patients not tolerating systemic therapies, or those completing neoadjuvant treatment plans will consider moving to high priority.
- Pts stable on neoadjuvant treatments that can receive additional cycles (i.e. MCR liver mets, pancreas, gastric cancers, and GIST)
- Patients with high risk premalignant conditions (i.e. Main duct IPMN)
- After a minimum of 2 weeks and a maximum of 6 weeks, patient’s priority will be re-evaluated.
- Surgery: Patients with known malignancies in whom delay in surgery beyond 2-6 weeks may reasonably increase risk of metastasis or necessitate change in surgical approach, AND for whom surgery outweighs the risk

of COVID-19 exposure in an
inpatient setting.
New Patients - Clinic Appt: - Convert to video visits
- Treatment: - As above - Appointments for patients who have primary oncologists may be delayed if they are being considered for clinical trials.
- Patients with new diagnosis of GI cancers/ retroperitoneal malignancies for whom surgery is indicated
- When appropriate, consider initiating neoadjuvant systemic chemotherapy, radiation or local regional therapies prior to definitive surgery.
- These patients should be presented at TB and treatment plan approved by all services involved.
- After a minimum of 2 weeks and a maximum of 6 weeks, patient’s priority will be re-evaluated.
Low Priority (treatment may be postponed for 6 weeks or longer)
Established Patients - Clinic Appt: Postponing appointments of patients who are on surveillance may be considered. - Patients on surveillance for premalignant conditions (i.e. IPMN, duodenal polyps, small < cm GIST). - Post-op surveillance alone
- Includes surgical treatment of ground glass opacities, mixed density nodules, typical carcinoids, thymomas, and patients with esophageal cancers who received induction chemoRT

- Treatment:
Patients who have indolent disease may be considered a therapy break.
- Surgery: Patients with known malignancies for whom surgery may be postponed 6 weeks or longer without appreciably increasing risk of metastasis or necessitate change in surgical approach, OR for whom the post-operative risk of COVID-19 exposure in an inpatient setting outweighs the expected benefit from surgery.
- After a minimum of 6 weeks, patient’s priority will be re- evaluated.
New Patients - Clinic Appt: Postponing appointments may be considered for patients who have primary oncologists and are currently receiving therapy.
- Surgery: Patients with newly diagnosed malignancies for whom surgery may be postponed 6 weeks or longer without appreciably increasing risk of metastasis or necessitate change in surgical approach, OR for whom the post-operative risk of COVID-19 exposure in an inpatient setting outweighs the expected benefit from surgery.
- After a minimum of 6 weeks, patient’s priority will be re- evaluated.
- Non- symptomatic benign conditions discovered on imaging (i.e. hepatic hemangioma or cysts).
- Patients referred for evaluation for pre-malignant conditions Symptomatic benign conditions (hepatic hemangiomas, Hepatic cyst disease, chronic pancreatitis).
- Transfer center referrals for bile duct injuries should be assessed and temporized for definitive surgical Tx in a few weeks.
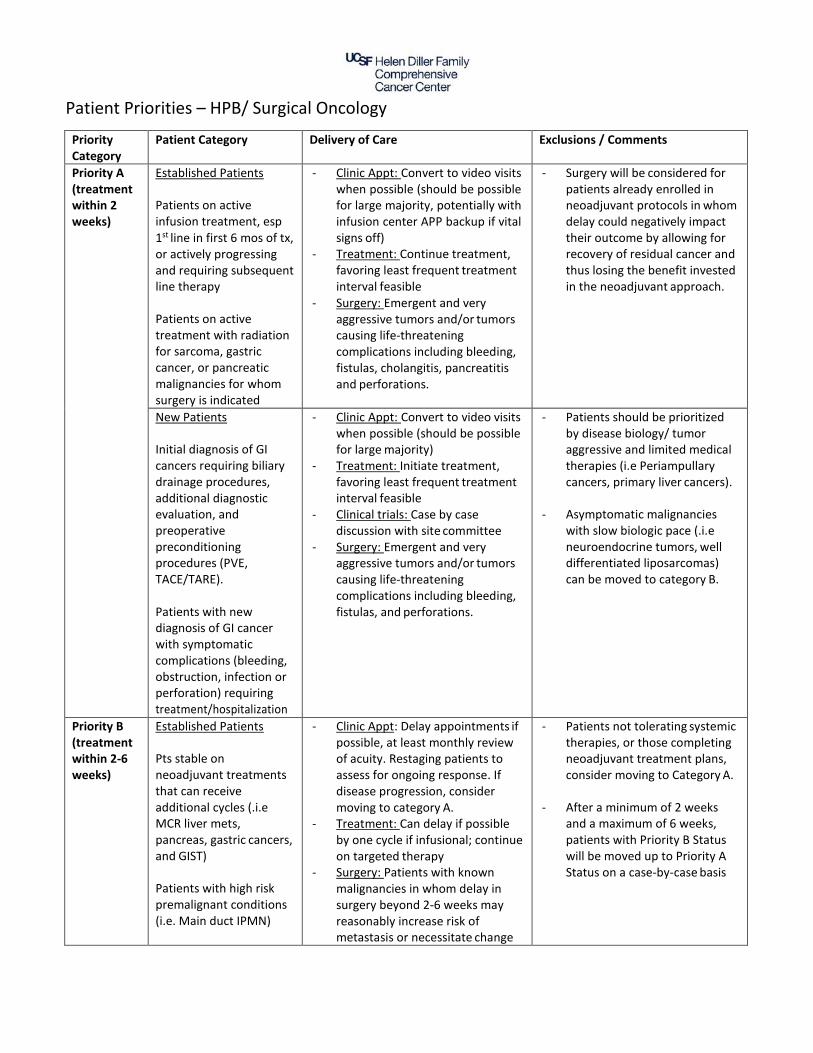
Patient Priorities – HPB/ Surgical Oncology
Priority Category
Patient Category Delivery of Care Exclusions / Comments
Priority A (treatment within 2 weeks)
Established Patients
Patients on active infusion treatment, esp 1st line in first 6 mos of tx, or actively progressing and requiring subsequent line therapy
Patients on active treatment with radiation for sarcoma, gastric cancer, or pancreatic malignancies for whom surgery is indicated
- Clinic Appt: Convert to video visits when possible (should be possible for large majority, potentially with infusion center APP backup if vital signs off)
- Treatment: Continue treatment, favoring least frequent treatment interval feasible
- Surgery: Emergent and very aggressive tumors and/or tumors causing life-threatening complications including bleeding, fistulas, cholangitis, pancreatitis and perforations.
- Surgery will be considered for patients already enrolled in neoadjuvant protocols in whom delay could negatively impact their outcome by allowing for recovery of residual cancer and thus losing the benefit invested in the neoadjuvant approach.
New Patients
Initial diagnosis of GI cancers requiring biliary drainage procedures, additional diagnostic evaluation, and preoperative preconditioning procedures (PVE, TACE/TARE).
Patients with new diagnosis of GI cancer with symptomatic complications (bleeding, obstruction, infection or perforation) requiring treatment/hospitalization
- Clinic Appt: Convert to video visits when possible (should be possible for large majority)
- Treatment: Initiate treatment, favoring least frequent treatment interval feasible
- Clinical trials: Case by case discussion with site committee
- Surgery: Emergent and very aggressive tumors and/or tumors causing life-threatening complications including bleeding, fistulas, and perforations.
- Patients should be prioritized by disease biology/ tumor aggressive and limited medical therapies (i.e Periampullary cancers, primary liver cancers).
- Asymptomatic malignancies with slow biologic pace (.i.e neuroendocrine tumors, well differentiated liposarcomas) can be moved to category B.
Priority B (treatment within 2-6 weeks)
Established Patients
Pts stable on neoadjuvant treatments that can receive additional cycles (.i.e MCR liver mets, pancreas, gastric cancers, and GIST)
Patients with high risk premalignant conditions (i.e. Main duct IPMN)
- Clinic Appt: Delay appointments if possible, at least monthly review of acuity. Restaging patients to assess for ongoing response. If disease progression, consider moving to category A.
- Treatment: Can delay if possible by one cycle if infusional; continue on targeted therapy
- Surgery: Patients with known malignancies in whom delay in surgery beyond 2-6 weeks may reasonably increase risk of metastasis or necessitate change
- Patients not tolerating systemic therapies, or those completing neoadjuvant treatment plans, consider moving to Category A.
- After a minimum of 2 weeks and a maximum of 6 weeks, patients with Priority B Status will be moved up to Priority A Status on a case-by-case basis

in surgical approach, AND for whom surgery outweighs the risk of COVID-19 exposure in an inpatient setting.
New Patients
Patients with new diagnosis of GI cancers/ retroperitoneal malignancies for whom surgery is indicated
- Clinic Appt: Delay appointments if possible, at least monthly review of acuity. Convert to video visits for most
- Treatment: Postpone in most cases
- Surgery: Patients with newly diagnosed malignancies in whom delay in surgery beyond 2-6 weeks may appreciably increase risk of metastasis or necessitate change in surgical approach, AND for whom surgery outweighs the post- operative risk of COVID-19 exposure in an inpatient setting.
- When appropriate, consider initiating neoadjuavant systemic chemotherapy, radiation or local regional therapies prior to definitive surgery.
- These patients should be presented at GI TB and treatment plan approved by all services involved.
- After a minimum of 2 weeks and a maximum of 6 weeks, patients with Priority B Status will be moved up to Priority A Status on a case-by-case basis
Priority C (treatment may be postponed for 6 weeks or longer)
Established Patients
Patients on surveillance for premalignant conditions (i.e. IPMN, duodenal polyps, small < cm GIST).
Post-op surveillance alone
- Clinic Appt: Postpone - Treatment: Postpone - Surgery: Patients with known
malignancies for whom surgery may be postponed 6 weeks or longer without appreciably increasing risk of metastasis or necessitate change in surgical approach, OR for whom the post- operative risk of COVID-19 exposure in an inpatient setting outweighs the expected benefit from surgery.
- Includes surgical treatment of ground glass opacities, mixed density nodules, typical carcinoids, thymomas, and patients with esophageal cancers who received induction chemoXRT
- After a minimum of 6 weeks, patients with Priority C Status may be moved up to Priority A or B Status on a case-by-case basis
New Patients
Patients referred for evaluation for pre- malignant conditions
Symptomatic benign conditions (hepatic hemangiomas, Hepatic cyst disease, chronic pancreatitis).
Transfer center referrals for bile duct injuries should be assessed and temporized for definitive surgical Tx in a few weeks.
- Clinic Appt: Postpone - Treatment: Postpone - Surgery: Patients with newly
diagnosed malignancies for whom surgery may be postponed 6 weeks or longer without appreciably increasing risk of metastasis or necessitate change in surgical approach, OR for whom the post-operative risk of COVID-19 exposure in an inpatient setting outweighs the expected benefit from surgery.
- After a minimum of 6 weeks, patients with Priority C Status may be moved up to Priority A or B Status on a case-by-case basis
- Non- symptomatic benign
conditions discovered on imaging (i.e. hepatic hemangioma or cysts).

NET Prioritization Plan during COVID-19
Top priority
New patient lives in SF, no other provider-- new NEC (local or mets). New patient lives in SF, no other provider-- new functional or o/w symptomatic metastatic NET Follow up patient on therapy (we are main provider) -- needs ongoing care Follow up patient with new symptoms (we are main provider)--needs ongoing care (e.g. debulking, LDT, PRRT)
(New Patient or follow up-- Lives regionally- SBO from symptomatic primary--will have surgery here)
Middle priority
New Patient lives in SF, no other provider, metastatic well diff nonfunctional NET Progressing patients who have local provider, but we have been part of care team--follow up visit. (e.g. pt has had ongoing f/u here) New Patient new NEC (local or mets) has local provider- wants advice about treatment (2nd opinion)---Case by case-- (e.g. contra costa patient has greater need than someone already seeing NET specialist at another site) New Patient new functional or o/w symptomatic metastatic NET has local provider-- wants advice about treatment (2nd opinion)- Case by case-- (e.g. contra costa patient has greater need than someone already seeing NET specialist at another site) Follow up patient on surveillance (we are main provider) -- needs restaging. (case by case) NP, ACC resected-- question of adjuvant therapy
New Patient, localized NET, primary in place- needs to see surg onc
NEXT New Patient lives in SF, no other provider, resected localized well diff nonfunctional NET New Patient lives in SF, no other provider, small NET--left in place New Patient, progressing patient who has local provider (e.g. Kaiser, cpmc, Stanford)-- second opinion about next steps. (CASE BY CASE as some patients don’t have access to NET expertise in their local area)
Lowest priority New Patient lives in SF, no other provider, small NET resected Stable patients with local provider, on or off therapy ( and we have been part of care team)-- follow up visit. (e.g. pt has had ongoing f/u here)---????? (or one level above?) New Patient, Stable patients with local provider, on or off therapy -wants second opinion here New Patient, has other provider, resected localized well diff nonfunctional NET New Patient, has other provider, small NET--left in place

Orthopedic Oncology Case Cancellation Algorithm
First Cancellation s: Benign non-aggre ssive or su specte d-benignnon-aggressive bone and soft
ti ssue tumors and tumor-like conditions
Excision of benign tumors, ie lipoma, ALTs, schwan nomas, ost eochondromas
Im plant lengthening
Implant revision/ exchange fo r non-inf ectious causes, ie poly wear
Stage 1 or 2 osseointegrat ion cases
UBC st eroid inj ect ion
Second Cancellation s: Benign aggressive or suspected-benign aggressive bone and soft tissue
tumor s and tumor-like conditions
Giant cell t umor not amenable to denosumab tempor izat ion
Aneurys mal bone cyst not amenable to inject ion
Chondroblastoma large / sympt omat ic
Impending pathologic fr act ur e not amenable to denosumab/ radia t ion/ act ivit y modificat ion
t em por izat ion
Third Cancellation s: Malignant or suspected-malignant bone and soft tissue tumors and
tumor-like conditions
Sarcoma resection (high priority for cases wit hin a chemo window)
Biopsy for a high-risk suspected malignancy or to determine treat ment
Pat ho logic or per i-prosthetic fr act ure
PJI or o t h e r soft t issue infect ion
Neurologic compromise

Head & Neck Surgery Patient Priorities
Priority Category Patient Category
Delivery of Care Exclusions / Comments
Priority A
Disease Conditions: Upper aerodigestive cancers, sinonasal cancer, erosive or regionally metastatic skin cancers, medullary/poorly differentiated/ anaplastic thyroid cancer, aggressive salivary cancers, lymphoma, sarcoma, evolving metastatic disease
Established Patients
- Clinic Appt: Convert to video visits when possible - Treatment: Continue treatment; - Procedure: Schedule for surgery, radiotherapy,
systemic therapy - Clinical trials: Therapeutic interventional studies
permitted when the clinician believes they are the best option for the patient and comply with restrictions on participation by study personnel. Observational or non-interventional studies that may be conducted remotely and off site (e.g. quality of life, surveys, retrospective) may proceed.
- In person evaluation if concern for recurrence for diagnostic examination
- Continue to perform needed therapeutic and diagnostic surgeries/procedures
- Postpone supportive care 6-8 weeks unless immediately essential for basic health, e.g. dental oncology, speech language pathology, nutrition, gastrostomy placements, psycho-oncology
New Patients
- Clinic Appt: Schedule for an appointment – video if possible
- Treatment: Start treatment - Procedure: Schedule for surgery, radiotherapy,
systemic therapy - Clinical trials: Therapeutic interventional studies
permitted when the clinician believes they are the best option for the patient and comply with restrictions on participation by study personnel. Observational or non-interventional studies that may be conducted remotely and off site (e.g. quality of life, surveys, retrospective) may proceed.
- Second opinions should be offered as video visits only
- In person evaluation for diagnostic exam when needed to accurately stage patient
- Continue to perform needed therapeutic and diagnostic surgeries/procedures
- Streamline all treatments when feasible e.g. hypofractionation of radiation therapy, lower number of systemic therapy infusions
- Postpone supportive care 6-8 weeks unless immediately essential for determination of appropriate therapy, e.g. dental oncology, speech language pathology, nutrition, gastrostomy placements, psycho-oncology

Priority B
Disease Conditions: well differentiated thyroid cancer, presumed benign parotid tumors, early skin cancer, stable metastatic disease
Established Patients
- Clinic Appt: Delay appointments if possible, video visits acceptable
- Treatment: Convert to video visits when possible - Procedure: defer 6-8 weeks
Clinical trials: Therapeutic interventional studies permitted when the clinician believes they are the best option for the patient and comply with restrictions on participation by study personnel, but treatment will be delayed when safe an feasible like SOC interventions for category B patients. Observational or non-interventional studies that may be conducted remotely and off site (e.g. quality of life, surveys, retrospective) may proceed
- Convert to video visits or delay appointments depending on goals of the visit. Can triage if absolutely needs in person visit
- Delay surgery for 6-8 weeks – revisit if needs to be extended again
- Delivery of adjuvant therapies e.g. radiation and systemic therapy to be delayed until 8 weeks after surgery
New Patients
- Clinic Appt: Video visits only - Determine the urgency to be seen
- Convert to video visits or delay appointments depending on goals of the visit. Can triage if absolutely needs in person visit
- Delay surgery for 6-8 weeks - revisit if needs to be extended again
- Delivery of adjuvant therapies e.g. radiation and systemic therapy to be delayed until 8 weeks after surgery
Priority C
Disease Condition: parathyroid disease, obstructive salivary gland disease, other benign tumors such as lipoma,
Established Patients
- Clinic Appt: Postpone - Treatment: Postpone - Procedure: Postpone
-
New Patients
- Clinic Appt: Waitlist for future scheduling - Treatment: Postpone - Procedure: Postpone

keloid, erygium; any patient currently under observation or who can be safely observed for chronic condition

Neuro-Oncology Patient Priorities
Priority Category Patient Category
Delivery of Care Exclusions / Comments
Priority A
Newly diagnosed GBM
Recurrent GBM
Malignantly transformed LGG
Anaplastic Astrocytoma
Anaplastic Oligodendroglio ma
LGG on trial Malignant
Meningioma
Neurologically unstable patients
Establishe d Patients
- Clinic Appt: Convert to video visits when possible, except for those getting injections/infusi on of experimental possible
- Treatment: Continue treatment; of radiation and chemotherapy when able
- Procedure: Schedule for surgery when indicated
- Clinical trials: if added to SOC surgery or does not significantly increase risk of exposure to pandemic
-
New Patients
- Clinic Appt: Schedule for an appointment if treatment to be done at our Institution, (UCSF) case review if treatment to be done locally
- Second opinions can be deferred if they have primary oncologists/surgeons/radia tion oncologists, and all attempts will be made to review cases remotely via telemedicine or case review.

- Treatment: Start treatment
- Procedure: Schedule for surgery
- Clinical Trials: - if added to SOC
surgery or does not significantly increase risk of exposure to pandemic
Priority B
Stable malignant tumors on surveillance Newly diagnosed LGG
Establishe d Patients
- Clinic Appt: Delay appointments if possible
- Treatment: Convert to video visits when possible
- Procedure: Schedule for surgery when indicated
- Clinical Trials: None at this time
-
New Patients
- Clinic Appt: Possible to be scheduled at a later date
- Determine the urgency to be seen, and do case reviews and telemedicine visits
-
Priority C
Stable LGG and benign tumors
Establishe d Patients
- Clinic Appt: Postpone
- Treatment: Postpone
-

- Procedure: Postpone
New Patients
- Clinic Appt: Waitlist for future scheduling, or remote case review or telemedicine
- Treatment: Postpone
- Procedure: Postpone
-

Patient Priorities – Thoracic and Sarcoma Oncology
Priority Category
Patient Category Delivery of Care Exclusions / Comments
Priority A (treatment within 2 weeks)
Established Patients
Patients on active infusion treatment, esp. 1st line in first 6 mos. of tx, or actively progressing and requiring subsequent line therapy
Patients with known diagnosis of thoracic malignancy for whom surgery or radiation is indicated
- Clinic Appt: Convert to video visits when possible (should be possible for large majority, potentially with infusion center APP backup if vital signs off)
- Treatment: Continue treatment, favoring least frequent treatment interval feasible
- Clinical trials: Case by case discussion with site committee
- Surgery: Emergent and very aggressive tumors and/or tumors causing life-threatening complications including bleeding, fistulas, and perforations.
- Radiation: For emergencies e.g. SVC syndrome, bleeding, airway obstruction, spinal cord compression.
- For pts on maintenance immunotherapy > 6 mos., maintenance chemo > 6 mos. priority B (very likely to tolerate missing at least one dose)
- For pts on maintenance immunotherapy > 2 years with stable disease priority C (no evidence base for further tx)
- Surgery will be considered for patients already enrolled in neoadjuvant protocols in whom delay could negatively impact their outcome by allowing for recovery of residual cancer and thus losing the benefit invested in the neoadjuvant approach.
- Radiation will be hypofractionated to greatest degree possible e.g. 1-5 fractions preferred
New Patients
Initial diagnosis of metastatic thoracic cancer, esp demographics favoring actionable driver mutations and small cell lung cancer
Patients with new diagnosis of thoracic malignancy for whom surgery or radiation is indicated
- Clinic Appt: Convert to video visits when possible (should be possible for large majority)
- Treatment: Initiate treatment, favoring least frequent treatment interval feasible
- Clinical trials: Case by case discussion with site committee
- Surgery: Emergent and very aggressive tumors and/or tumors causing life-threatening complications including bleeding, fistulas, and perforations.
- Radiation: For emergencies e.g. SVC syndrome, bleeding, airway obstruction, spinal cord compression.
- Second opinions can/should be deferred if pts have primary oncologist already, but provider time permitting, can be done to help guide local oncologist—pts should be advised in advance they will not be transferred to our care during the pandemic event
- Asymptomatic metastatic carcinoid and metastatic thymoma can move to priority B
- Radiation will be hypofractionated to greatest degree possible e.g. 1-5 fractions preferred
Priority B (treatment within 2-6 weeks)
Established Patients
Pts on maintenance immunotx > 6 mos., maintenance chemo > 6 mos.
Pts stable on targeted therapy
- Clinic Appt: Delay appointments if possible, at least monthly review of acuity. Restaging for targeted therapy patients in ongoing response and without symptoms can probably be extended from the standard 2-3 mos. to 4 mo. Convert to video visits for most
- Includes surgical treatment of most solid lung tumors and patients with esophageal cancers who did not undergo induction chemotherapy
- After a minimum of 2 weeks and a maximum of 6 weeks, patients with Priority B Status

Patients with known diagnosis of thoracic malignancy for whom surgery or radiation is indicated
- Treatment: Can delay if possible by one cycle if infusional; continue on targeted therapy
- Clinical Trials: Case by case discussion with site committee
- Surgery: Patients with known malignancies in whom delay in surgery beyond 2-6 weeks may reasonably increase risk of metastasis or necessitate change in surgical approach, AND for whom surgery outweighs the risk of COVID-19 exposure in an inpatient setting.
- Radiation: Locoregionally advanced tumors with low probability of response to neoadjuvant systemic therapy and high risk of progression within 2-6 weeks, primary tumors that can be cured with short-course fractionation and/or SBRT and have high risk of progression within 6 weeks.
will be moved up to Priority A Status on a case-by-case basis
- Radiation will be hypofractionated to greatest degree possible e.g. <5-20 fractions preferred
New Patients
Post-op, indication for adjuvant therapy (can likely be safely delayed 1- 3 mos. without compromise or efficacy)
Patients with new diagnosis of thoracic malignancy for whom surgery or radiation is indicated
- Clinic Appt: Delay appointments if possible, at least monthly review of acuity. Convert to video visits for most
- Treatment: Postpone in most cases
- Clinical Trials: Case by case discussion with site committee
- Surgery: Patients with newly diagnosed malignancies in whom delay in surgery beyond 2-6 weeks may appreciably increase risk of metastasis or necessitate change in surgical approach, AND for whom surgery outweighs the post- operative risk of COVID-19 exposure in an inpatient setting.
- Radiation: Locoregionally advanced tumors with low probability of response to neoadjuvant systemic therapy and high risk of progression within 2-6 weeks, primary (not metastatic or oligometastatic) tumors that can be cured with short-course fractionation and/or SBRT and have high risk of progression within 6 weeks.
- Includes surgical treatment of most solid lung tumors and patients with esophageal cancers who did not undergo induction chemotherapy
- After a minimum of 2 weeks and a maximum of 6 weeks, patients with Priority B Status will be moved up to Priority A Status on a case-by-case basis
- Radiation will be hypofractionated to greatest degree possible e.g. <5-20 fractions preferred

Priority C (treatment may be postponed for 6 weeks or longer)
Established Patients
Pts on maintenance immunotherapy >2 years
Post-op surveillance alone
- Clinic Appt: Postpone - Treatment: Postpone - Surgery: Patients with known
malignancies for whom surgery may be postponed 6 weeks or longer without appreciably increasing risk of metastasis or necessitate change in surgical approach, OR for whom the post- operative risk of COVID-19 exposure in an inpatient setting outweighs the expected benefit from surgery.
- Radiation: Patients with metastatic or oligometastatic disease, patients for whom radiation may be safely delayed for at least 8 weeks.
- Includes surgical treatment of ground glass opacities, mixed density nodules, typical carcinoids, thymomas, and patients with esophageal cancers who received induction chemoXRT
- Includes patients who can safely delay initiation of radiation e.g. minimally invasive lung cancers with low risk of progression in 6 weeks, patients who have had operation for non-small cell lung cancer and may receive postoperative chemotherapy before starting radiation, patients who have had operations for less aggressive thymic malignancy or carcinoid or salivary gland tumors who can safely start radiation at 8 weeks from surgery with minimal risk of relapse.
- After a minimum of 6 weeks, patients with Priority C Status may be moved up to Priority A or B Status on a case-by-case basis
- Radiation will be hypofractionated to greatest degree possible e.g. <5-20 fractions preferred
New Patients
Post-op, no indication for adjuvant therapy
Second opinions with established oncologist
- Clinic Appt: Postpone - Treatment: Postpone - Surgery: Patients with newly
diagnosed malignancies for whom surgery may be postponed 6 weeks or longer without appreciably increasing risk of metastasis or necessitate change in surgical approach, OR for whom the post-operative risk of COVID-19 exposure in an inpatient setting outweighs the expected benefit from surgery.
- Radiation: Patients with metastatic or oligometastatic disease, patients for whom radiation may be safely delayed for at least 8 weeks.
- Includes surgical treatment of ground glass opacities, mixed density nodules, typical carcinoids, thymomas, and patients with esophageal cancers who received induction chemoXRT
- Includes patients who can safely delay initiation of radiation e.g. minimally invasive lung cancers with low risk of progression in 6 weeks, patients who have had operation for non-small cell lung cancer and may receive postoperative chemotherapy before starting radiation, patients who have had operations for less aggressive

thymic malignancy or carcinoid
or salivary gland tumors who can safely start radiation at 8 weeks from surgery with minimal risk of relapse.
- After a minimum of 6 weeks, patients with Priority C Status may be moved up to Priority A or B Status on a case-by-case basis
- Radiation will be hypofractionated to greatest degree possible e.g. <5-20 fractions preferred

Melanoma & Skin Cancer Program Medical Oncology - Patient Prioritization Definitions
Priority A • Condition deemed critical (unstable, unbearable suffering, and/or whose
condition is immediately life threatening) and for whom there is effective treatment.
• Their immediate need is greatest and we must find ways (either in the geographic area of the pandemic or elsewhere) where treatment can be instituted or continued.
• E.g., patients with stage IV disease, brain metastasis, failing SOC therapy and need clinical trial option, need for palliative surgery or radiation
Priority B • Condition deemed non-life threatening whose services can be deferred or
continued with adjusted frequency during a wave of the pandemic event. • Physicians will determine that these patients are not put at undue risk. If their
priority changes, they will be moved to priority A
• E.g., patients with stage III disease requiring adjuvant therapy start or patients currently on adjuvant therapy, patients with stage IV disease known to be responding
Priority C • Condition deemed stable whose services may be discontinued or deferred during
the entire pandemic event (multiple waves of 6-8 weeks). • These patients are, for the most part, undergoing routine follow-up or screening
and can reasonably wait until the pandemic is over. • E.g., asymptomatic patients with stage II or III disease not on adjuvant therapy
v 3.27.2020

Melanoma & Skin Cancer Program Medical Oncology Patient Priorities
Priority Category
Patient Category
Delivery of Care Comments
Priority A
Condition critical: life- threatening, unstable
Established Patients
- Clinic appt: Convert to video if appropriate
- Treatment: Continue treatment - Procedure: Refer to
derm/surgery/radiation - Clinical trials: Utilize SOC option if
one exists. Prioritize trial enrollment for pts without other treatment options.
- Consider lowest frequency dosing schedule of infusions
New Patients
- Clinic appt: Discuss urgency with provider, schedule for appt, video if appropriate.
- Treatment: Start treatment - Procedure: Refer to
derm/surgery/radiation - Clinical trials: Utilize SOC option if
one exists. Prioritize trial enrollment for pts without other treatment options.
- Prioritize metastatic disease requiring treatment over stable second opinions.
Priority B
Condition stable: non- life- threatening
Established Patients
- Clinic appt: Delay or convert to video if appropriate
- Treatment: Continue treatment - Procedure: Refer to
derm/surgery/radiation - Clinical trials: Utilize SOC option if
one exists. Prioritize trial enrollment for pts without other treatment options.
- Consider lowest frequency dosing schedule of infusions
New Patients
- Clinic appt: Discuss urgency with provider, schedule for appt, video if appropriate
- Clinical trials: Utilize SOC option if one exists. Prioritize trial enrollment for pts without other treatment options.
- Prioritize patients requiring treatment start over stable second opinions
v 3.27.2020

Priority C
Condition stable
Established Patients
- Clinic appt: Postpone - Procedure/treatment: Discuss
urgency, triage referral to derm/surgery/radiation
- Surveillance scan: Postpone
- Triage urgency – if active issue, consider video visit rather than further delay
New Patients
- Clinic appt: Waitlist for future scheduling
- Procedure/treatment: Discuss urgency, triage referral to derm/surgery/radiation
- Surveillance scan: Postpone
* Further reference: NCCN guidelines on melanoma care during COVID 19
v 3.27.2020

Radiation Oncology Program
Radiation Oncology Patient Priorities A, B, C*
Priority Description Examples
Priority A1 All emergent and urgent patients where alternative management to radiotherapy is not possible.
Patients already on treatment (not limited to RT) where treatment break would yield compromised outcomes
Non-surgical spinal cord compression
Airway obstruction
Brain metastases
Cancer-related bleeding
Post-operative/Post-induction malignancies where package time important (HN, Lung, HGG, GI, Sarcoma)
Priority A2 Patients with higher risk malignancies where treatment delays would compromise outcomes
Symptomatic metastases refractory to medical management
HN
Lung
HGG
Peds
Sarcoma
GI
Lymphoma
Gyn
High risk breast/prostate without induction/maintenance options
Priority B Patients with asymptomatic metastatic disease for RT- prophylaxis/consolidation
Patients who can have RT deferred for weeks to months where observation and/or induction/maintenance regimens available
Oligometastases
Asymptomatic skeletal/visceral metastases
Lower risk/lower stage primary malignancies (e.g. prostate, breast, subset of A2 above)
Priority C Patients with benign disease who can be delayed for radiotherapy beyond 3-6 months with limited impact on outcome
Benign meningioma
Pituitary adenoma
Trigeminal Neuralgia
Desmoid/Dupuytren’s
*In all cases, hypofractionation and less resource-intensive (simpler modality) approaches should be considered where evidence supported.
Triage for treatment delay should be determined on a case by case basis with emphasis to minimize any harm to the patient.