canadian diagnosis 2015
TRANSCRIPT

Fetalalcoholspectrumdisorder:CanadianguidelinesfordiagnosisAlbertE.Chudley,JulianneConry,JocelynnL.Cook,ChristineLoock,TedRosales,NicoleLeBlancAbstract THE DIAGNOSIS OF FETAL ALCOHOL SPECTRUM DISORDER (FASD) is complex and guidelines are warranted. A subcommittee of the Public Health Agency of Canada’s National Advisory Committee on Fetal Alcohol Spectrum Disorder reviewed, analysed and integrated current approaches to diagnosis to reach agreement on a standard in Canada. The purpose of this paper is to review and clarify the use of current diagnostic systems and make recommendations on their application for diagnosis of FASD-related disabilities in people of all ages. The guidelines are based on widespread consultation of expert practitioners and partners in the field. The guidelines have been organized into 7 categories: screening and referral; the physical examination and differential diagnosis; the neurobehavioural assessment; and treatment and follow-up; maternal alcohol history in pregnancy; diagnostic criteria for fetal alcohol syndrome (FAS), partial FAS and alcohol-related neurodevelopmental disorder; and harmonization of Institute of Medicine and 4-Digit Diagnostic Code approaches. The diagnosis requires a comprehensive history and physical and neurobehavioural assessments; a multidisciplinary approach is necessary. These are the first Canadian guidelines for the diagnosis of FAS and its related disabilities, developed by broad-based consultation among experts in diagnosis. Inthisdocument,wediscussthediagnosticapproachtodisabilitiesassociatedwithprenatalalcoholexposure.Fetalalcoholspectrumdisorder(FASD),alongwithitsmostvisiblepresentation,fetalalcoholsyndrome(FAS),isaserioushealthandsocialconcerntoCanadians.FASDisanumbrellatermdescribingtherangeofeffectsthatcanoccurinanindividualwhosemotherdrankalcoholduringpregnancy.Theseeffectsmayincludephysical,mental,behaviouralandlearningdisabilitieswithlifelongimplications.ThetermFASDisnotintendedforuseasaclinicaldiagnosis. FASDistheresultofmaternalalcoholconsumptionduringpregnancyandhasimplicationsfortheaffectedperson,themother,thefamilyandthecommunity.SinceFASwasfirstdescribedin1973,1ithasbecomeapparentthatitiscomplex;affectedpeopleexhibitawiderangeofexpression,fromseveregrowthrestriction,intellectualdisability,birthdefectsandcharacteristicdysmorphicfacialfeaturestonormalgrowth,facialfeaturesandintellectualabilities,butwithlifelongdeficitsinseveraldomainsofbrainfunction.FASDrequiresamedicaldiagnosisinthecontextofamultidisciplinaryassessment.FASDitselfisnotadiagnosticterm.ThepurposeofthispaperistoreviewandclarifytheuseofthecurrentdiagnosticsystemsandmakerecommendationsontheirapplicationfordiagnosisofFASD-relateddisabilitiesinpeopleofallages.ForadescriptionofthecharacteristicsandthenaturalcourseofFASD,consultsomeofthebroaderreviews.2-7 Epidemiology of FASD TheprevalenceofFASintheUnitedStateshasbeenre-portedas1–3per1000livebirthsandtherateofFASDas9.1per1000livebirths.8-11However,diagnosismayoftenbedelayedormissedentirely.2 TherearenonationalstatisticsontheratesofFASDinCanada,althoughstudieshaveestimateditsprevalenceinsmallpopulations.InanisolatedAboriginalcommunityinBritishColumbia,FASDprevalencewas190per1000livebirths.12InnortheasternManitoba,anincidenceofabout7.2per1000livebirthswasfound.13InanotherManitobastudyinaFirstNationscommunity,14theprevalenceofFASandpartialFASwasestimatedtobe55–101per1000.Intheirsurvey,AsanteandNelms-Matzke15estimatedtherateofFASandrelatedeffectsat46per1000nativeCanadianchildrenintheYukonand25per1000innorthernBritishColumbia.BasedonreferralstoadiagnosticclinicinSaskatchewan,therateofFASwasestimatedat0.589per1000livebirthsin1988–1992and0.515per1000in1973–1977.16However,noneofthesedatashouldbegeneralizedtoothercommunities,otherpopulationsortheCanadianpopulationingeneral.

Risk factors AcommonmisconceptionisthatFASDisassociatedwithethno-culturalbackground.However,thedatasuggestthatriskfactorsforprenatalalcoholexposureincludehighermaternalageandlowereducationlevel,prenatalexposuretococaineandsmoking,custodychanges,lowersocioeconomicstatusandpaternaldrinkinganddruguseatthetimeofpregnancy;17andreducedaccesstoprenatalandpostnatalcareandservices,inadequatenutritionandapoordevelopmentalenvironment(e.g.,stress,abuse,neglect).18 Ina5-yearfollow-upstudyofbirthmothersofchildrenwithfullFAS,Astleyandcolleagues19foundthatthesewomencamefromdiverseracial,educationalandeconomicbackgrounds.Theywereoftenchallengedbyuntreatedorunder-treatedmentalhealthconcerns,theyweresociallyisolated,theywerevictimsofabuseandtheyhadhistoriesofseverechildhoodsexualabuse. Becausetherearenolarge-scalestudiesofriskfactorsandbecauserisksareinterrelatedandcouldbedifferentfordifferentpopulations,itisdifficulttoprovideaccuratefiguresforrelativerisk.However,themostimportantriskfactorforFASDisrelatedtohighblood-alcoholconcentration:thetimingofexposureduringfetaldevelopment,thepatternofconsumption,i.e.,bingedrinking(4ormoredrinksperoccasion)andthefrequencyofuse.Althoughthereseemstobenodefinitethresholdofexposure,thereappearstobeadose-responserelation.17,20,21 Importance of early diagnosis Anearlydiagnosisisessentialtoallowaccesstointerventionsandresourcesthatmaymitigatethedevelopmentofsubsequent“secondarydisabilities”(e.g.,unemployment,mentalhealthproblems,troublewiththelaw,inappropriatesexualbehaviour,disruptedschoolexperience)amongaffectedpeople.22Furthermore,anearlydiagnosiswillalsoal-lowappropriateintervention,counsellingandtreatmentforthemotherandmaypreventthebirthofaffectedchildreninthefuture.23Itmayalsopromptcaregiverstoseekdiagnosisandsupportforpreviouslyundiagnosedsiblings.AreviewofmedicalandbehaviouralmanagementofthosewithFASDcanbefoundinothersources.3,24AstleyandClarren25suggestthataccurateandtimelydiagnosisisessentialtoimproveoutcome,asmisclassificationleadstoinappropriatepatientcare,increasedriskofsecondarydisabilities,missedopportunitiesforpreventionandinaccurateestimatesofincidenceandprevalence.Together,theseinaccuraciescouldhindereffortstoallocatesufficientsocialandhealthcareservicestothevulnerablepopulationsandprecludeaccurateassessmentofprimarypreventionefforts. Becauseoflimitedcapacityandexpertiseandtheneedtoinvolveseveralprofessionalsinacomprehensivemulti-disciplinarydiagnosticevaluation,onlyafractionofthoseaffectedcurrentlyreceiveadiagnosis.Results26fromtheCanadiannationalsurveyregardingknowledgeandattitudesofhealthprofessionalssuggestthatstandardizedguidelinesfordiagnosisandfurtherprofessionaleducationandtrainingareneededforpractitionerstoparticipateindiagnosis.Inresponsetotheseconcerns,HealthCanada’sNationalAdvisoryCommitteeonFASD,alongwithexpertsandpractitionersinFASdiagnosisandtreatment,presentthefollowingguidelinesfordiagnosis. Process of guideline development Theseguidelinesaretheresultofmorethan10face-to-faceconsultationswithCanadianandAmericanexpertsinthediagnosisofFASanditsrelateddisabilities(Appendix1).ManyoftheparticipantsarecurrentlyprovidingdiagnosticservicesacrossCanada.Reviewandfeedbackwereprovidedbyadiversegroupofindividuals;professionalorganizationsandsocieties;andprovincial,territorialandfederallevelsofgovernment.Guidelinesarepresentedin6areasrelatedtothediagnosticprocess:1.screeningandreferral;2.thephysicalexaminationanddifferentialdiagnosis;3.neurobehaviouralassessment;4.treatmentandfollow-up;5.maternalalcoholhistoryinpregnancy;and6.diagnosticcriteriaforFAS,partialFASandalcohol-relatedneurodevelopmentaldisorder.Wealsoincluderecommendationsforharmonizationofthe2mainapproachestodiagnosis. Therearemultipleapproachestodiagnosis,andtheworkinggroupsoughttointegratethesetoachieveconsistentdiagnosesacrossCanada.Currentknowledgeofthecomplexityofthedisabilitiesassociatedwithprenatalalcoholexposuredictatesthatacomprehensive,multidisciplinaryassessmentisnecessarytomakeanaccuratediagnosisandproviderecommendationsfor

management.Wearerecommendingsuchamultidisciplinaryapproach.ThisapproachwillalsoallowforcollectionofCanadiandataforestimatingincidenceandprevalenceofFASD.Thisinformationisessentialtoidentifytheneedforandthedevelopmentofappropriatepreventionandinterventionprogramsandservices. Background and terminology for the diagnosis of FAS ThefirstrecognitionofavarietyofbirthdefectsanddevelopmentaldisabilitiesinoffspringborntoalcoholicparentsisattributedtoLemoineandcolleagues.27AspecificpatternofbirthdefectsfollowingmaternalalcoholexposurewasdescribedintheUnitedStates.1,28Thespecificpattern,referredtoasFAS,consistsoffacialabnormalities(smoothphiltrum[thespacebetweentheupperlipandthenose],thinvermilionborder[theexposedmucosal,orredpart,oftheupperlip],shortpalpebralfissures),impairedprenatalorpostnatalgrowth(orboth)andcentralnervoussystemorneurobehaviouraldisorders.Alcoholprobablyactsthroughmultiplemechanismsandarangeofdisabilitieshasbeenobservedintheabsenceofdysmorphicfeaturesreflectingvaryingdegreesofdamageduringfetaldevelopment;undoubtedly,timinganddegreeofexposureareimportantvariablesthatcontributetothevariation.Thus,theterm“suspectedfetalalcoholeffects”(FAE)wascreated.29These“effects”werefurtherdelineatedbytheUnitedStates’InstituteofMedicine(IOM),whichpublishedrecommendationsin1996fordiagnosisofFASinconsultationwithapanelofexperts.4 Thediagnosticcategoriespresentedwere:FASwithandwithoutaconfirmedhistoryofalcoholexposure,partialFAS,alcohol-relatedbirthdefects(ARBD),andalcoholrelatedneurodevelopmentaldisorder(ARND)(Table1). Inthelate1990s,anotherdiagnosticstrategywasdevelopedbyAstleyandClarren.25,30Theycreateda4-DigitDiagnosticCodeusingdatafromtheWashingtonStateFetalAlcoholSyndromeDiagnosticandPreventionNetworkofclinics.Thesystemusesquantitative,objectivemeasurementscalesandspecificcasedefinitions.The4digitsinthecodereflectthemagnitudeofexpressionorseverityofthe4keydiagnosticfeaturesofFASinthefollowingorder:growthdeficiency;theFASfacialphenotype;centralnervoussystemdamageordysfunction;gestationalexposuretoalcohol.Themagnitudeofexpressionofeachfeatureisrankedindependentlyona4-pointLikertscalewith1reflectingcompleteabsenceofthefeatureand4reflectingitsextremeexpression.The4-DigitDiagnosticCodeisnowbeingusedfordiagnosis,screeningandsurveillanceinclinicsthroughouttheUnitedStatesandCanada.TerminologyfromAstley’s2004revisionofthe4-DigitDiagnosticCodeareusedinthisarticle.* Althoughtheapproachesaredifferent,theunderlying,fundamentalcriteriaoftheIOMandthe4-DigitDiagnosticCodearesimilar.Someclinicsarechoosingtointegratethediagnostictoolsandprecisionreflectedinthe4-DigitDiagnosticCodewiththediagnosticcategoriesandlanguagerecommendedbytheIOMcommittee.AlthoughbothIOMcriteriaandthe4-DigitDiagnosticCodehavebeenpublished,manycliniciansstillusethelessdesirableandpotentiallymisleadinggestaltapproach(Table2). The diagnostic process Thediagnosticprocessconsistsofscreeningandreferral,thephysicalexaminationanddifferentialdiagnosis,theneurobehaviouralassessmentandtreatmentandfollow-up.Becauseofthecomplexityandtherangeofexpressionofdysfunctionrelatedtoprenatalalcoholexposure,amulti-disciplinaryteamisessentialforanaccurateandcomprehensivediagnosisandtreatmentrecommendations.Theassessmentprocessbeginswithrecognitionoftheneedfordiagnosisandendswithimplementationofappropriaterecommendations.Themultidisciplinarydiagnosticteamcanbegeographic,regionalorvirtual;itcanalsoacceptreferralsfromdistantcommunitiesandcarryoutanevaluationusingtelemedicine. Thecoreteammayvaryaccordingtothespecificcontext,butideallyitshouldconsistofthefollowingprofessionalswithappropriatequalifications,trainingandexperienceintheirparticulardiscipline: *AstleySJ. Diagnostic Guide for Fetal Alcohol Spectrum Disor- ders: The 4-Digit Diagnostic Code (3rd edition). Seattle: Uni- versity of Washington Publication Services; 2004.

•Coordinatorforcasemanagement(e.g.,nurse,socialworker). •PhysicianspecificallytrainedinFASDdiagnosis.•Psychologist.•Occupationaltherapist.•Speech-languagepathologist. Additionalmembersmayincludeaddictioncounsellors,childcareworkers,culturalinterpreters,mentalhealthworkers,parentsorcaregivers,probationofficers,psychiatrists,teachers,vocationalcounselors,nurses,geneticistsordysmorphologists,neuropsychologists,familytherapists. Comments Clearly,fundingfordevelopment,trainingandmaintenanceofmultidisciplinarydiagnosticteamsisnecessarysothatmajorcentreswillhavetheexpertiseandcapacitytoservetheircommunities.Tooptimizetheoutcomeofthediagnosis,thecommunityandthefamilymustbeprepared,readytoparticipatein,andbeinagreementwiththediagnosticassessment.Thediagnosticprocessshouldbesensitivetothefamily’sandthecaregiver’sneeds.Ineachcommunity,referralsmustbeevaluatedandtheirlevelofpriorityestablished.Thefamilyandguardianmustbeinagreementonthepurposeofdiagnosis.TheymustbemadeawareofthepotentialpsychosocialconsequencesofadiagnosisofFASD(e.g.,increasingasenseofguiltandanger,especiallywiththebirthmother,orpotentialstigmatizationofthechild).Thefamilyorguardianwilllikelyneedhelptomoveconfidentlythroughthediagnosticprocess.ThishelpmightincludesomepreparatoryeducationconcerningFASDandlinkingthemwithcommunitysupportsandresources. Informationfrommultiplesources(e.g.,schoolrecords,hospitalrecords,socialservices,previousassessments)shouldbeobtained;thismightinvolvemeetingswithrelevantprofessionalswhoknowthepatient(e.g.,teachers,physicians,socialworkers,psychologists).Otherrelevantdocumentationwouldincludebirthandpregnancyrecords,medicalandhospitalrecords,adoptionrecords,academicrecords,achievementtests,developmentalassessments,psychologicalandpsychometricassessments,legalreportsanddocumentationofthefamilyhistory. Thecomprehensiveassessmentbythediagnosticteamprovidesimportantinformationabouttheindividual’suniqueneedsandallowsinterventionstobetailoredtohisorherstrengthsandchallenges.Thepost-diagnosticreportshouldstatethebasisforthediagnosisbyincludingthehistoryofalcoholuse,thephysicalcriteriaandthepsychologicaldatathatsupportit. Multidisciplinaryteamsworkwithcommunitypartnersandresourcestodevelopandimplementmanagementplanstomaximizethepotentialoftheaffectedindividual.Followingassessment,areportcontainingrecommendationsshouldbemadeavailabletocaregivers,educators,andbiologicalfamilies,aswellasotherappropriateindividualswhoworkwiththechild(i.e.,daycareworkers,earlyinterventionworkers,socialworkers,etc).Theteamfindingsshouldbediscussedwiththeguardian.Olderchildrenwhohavethecognitiveabilityshouldhavetheopportunitytolearnabouttheirdiagnosisfromtheteam.Theteammightalsotakeontheresponsibilityforfacilitatingandprovidingfollow-upwiththefamilyandcom-munityresourcesregardingoutcomesoftherecommendations.Ultimately,thediagnosticprocesswillresultinconcretemanagementrecommendationstoimprovethelivesoftheaffectedindividuals,theirfamiliesandthecommunities. Canadaisalargecountrywithvastdistancesbetweencommunities,someofwhichareremoteandisolated.SpecialistsprovidingconsultationtoremoteareasrequirespecializedtraininginFASDassessmentandneedtolinkwithcentresthathavemultidisciplinaryteamstoassistinthediagnosticprocess.Anumberoftoolsmaybeusefulfordistantdiagnosis.Morefrequentuseoftelemedicine,forexample,willallowassessmentofchildrenindistantcommunities.31Otherexamplesincludetheuseofdigitalphotographs32,33and3-Dlasersurfacescanning34,35sentelectronicallytoteamsinlargercentres. WerecognizethatthereiscurrentlyalimitedcapacityeveninsomelargecommunitiesinCanadatoprovideamultidisciplinaryteam-basedapproachtoFASdiagnosis.Professionalsshouldmakethebestuseofavailableresourcesandexpertisetoprovideanaccurateassessmentandtreatmentplanforaffectedindividualsandtheirfamilies,recognizingthekeyroleofpsychology. 1. Screening and referral Recommendations

1.1Allpregnantandpost-partumwomenshouldbescreenedforalcoholusewithvalidatedscreeningtools(i.e.,T-ACE,TWEAK)byrelevanthealthcareproviders.Womenatriskforheavyalcoholuseshouldreceiveearlybriefintervention(i.e.,counselling). 1.2Abstinenceshouldberecommendedtoallwomenduringpregnancy,asthemother’scontinueddrinkingduringpregnancywillputthefetusatriskforeffectsrelatedtoprenatalalcoholexposure. 1.3ReferralofindividualsforapossibleFASD-relateddiagnosisshouldbemadeinthefollowingsituations: Table 1: Institute of Medicine diagnostic criteria for fetal alcohol syndrome and alcohol-related effects4 Fetal alcohol syndrome (FAS)
1. FAS with confirmed maternal alcohol exposure* 1. Confirmed maternal alcohol exposure* 2. Evidence of a characteristic pattern of facial anomalies that includes features such
as short palpebral fissures and abnormalities in the premaxillary zone (e.g., flat upper lip, flattened philtrum and flat midface)
3. Evidence of growth retardation, as in at least one of the following: • low birth weight for gestational age • decelerating weight over time not due to nutrition • disproportional low weight-to-height ratio
4. Evidence of central nervous system neurodevelopmental abnormalities, as in at least one of the following: • decreased cranial size at birth • structural brain abnormalities (e.g., microcephaly, partial or complete agenesis of the corpus callosum, cerebellar hypoplasia) • neurologic hard or soft signs (as age appropriate), such as impaired fine motor skills, neurosensory hearing loss, poor tandem gait, poor eye-hand coordination
2. FAS without confirmed maternal alcohol exposure B, C, and D as above 3. Partial FAS with confirmed maternal alcohol exposure A. Confirmed maternal alcohol
exposure* B. Evidence of some components of the pattern of characteristic facial anomalies Either C or D or E C. Evidence of growth retardation, as in at least one of the following: • low birth weight for gestational age • decelerating weight over time not due to nutrition • disproportionally low weight-to-height ratio
4. Evidence of CNS neurodevelopmental abnormalities, e.g., • decreased cranial size at birth • structural brain abnormalities (e.g., microcephaly, partial or complete agenesis of the corpus callosum, cerebellar hypoplasia) • neurologic hard or soft signs (as age appropriate) such as impaired fine motor skills, neurosensory hearing loss, poor tandem gait, poor eye–hand coordination
5. Evidence of a complex pattern of behaviour or cognitive abnormalities that are inconsistent with developmental level and cannot be explained by familial background or environment alone: e.g., learning difficulties; deficits in school performance; poor impulse control; problems in social perception; deficits in higher level receptive and expressive language; poor capacity for abstraction or metacognition; specific deficits in mathematical skills; or problems in memory, attention or judgment.
1. Presenceof3characteristicfacialfeatures(shortpalpebralfissures,smoothorflattenedphiltrum,thinvermilionborder).
2. Evidenceofsignificantprenatalexposuretoalcoholatlevelsknowntobeassociatedwithphysicalorde-velopmentaleffects,orboth.
3. Presenceof1ormorefacialfeatureswithgrowthdeficitsplusknownorprobablesignificantprenatalalcoholexposure.
4. Presenceof1ormorefacialfeatureswith1ormorecentralnervoussystemdeficitsplusknownorprob-ablesignificantprenatalalcoholexposure.

5. Presenceof1ormorefacialfeatureswithpre-orpost-natalgrowthdeficits,orboth(atthe10thpercentileorbelow[1.5standarddeviationsbelowthemean])and1ormorecentralnervoussystemdeficitsplusknownorprobablesignificantprenatalalcoholexposure.
1.4Individualswithlearningorbehaviouraldifficulties,orboth,withoutphysicalordysmorphicfeaturesandwithoutknownorlikelyprenatalalcoholexposureshouldbeassessedbyappropriateprofessionalsorspecialtyclinics(i.e.,developmentalpediatrics,clinicalgenetics,psychiatry,psychology)toidentifyandtreattheirproblems. Comments Screeningshouldnotbeequatedwithdiagnosis.Weknowthatinsomeplaceswithnodiagnosticservices,screeningtoolshavebeeninappropriatelyusedinlieuofaproperdiagnosis.OnepurposeofscreeningistoidentifyandreferpregnantwomenwhomaybeatriskforanalcoholusedisorderandwhomayplacetheirchildatriskforFASD.Severalalcoholscreeningtoolshavebeenfoundtobeeffectiveinidentifyingproblemdrinkinginaprimary Table 1: continued Alcohol-related effects Clinical conditions in which there is a history of maternal alcohol exposure,*† and where clinical or animal research has linked maternal alcohol ingestion to an observed outcome. There are 2 categories, which may co-occur. If both diagnoses are present, then both diagnoses should be rendered. 4. Alcohol-related birth defects (ARBD) Congenital anomalies, including malformations and dysplasias Cardiac Atrial septal defects Ventricular septal defects Skeletal Hypoplastic nails Shortened fifth digits Radioulnar synostosis Flexion contractures Camptodactyly Renal Aplastic, dysplastic, hypoplastic kidneys Horseshoe kidneys Ocular Strabismus Retinal vascular anomalies Auditory Conductive hearing loss Other Virtually every malformation has been described in some patient with FAS. The etiologic specificity of most of these anomalies to alcohol teratogenesis remains uncertain. 5. Alcohol-related neurodevelopmental disorder (ARND) Presence of A or B or both.
1. Evidence of CNS neurodevelopmental abnormalities, as in any one of the following: • decreased cranial size at birth • structural brain abnormalities (e.g., microcephaly, partial or complete agenesis of the corpus callosum, cerebellar hypoplasia) • neurologic hard or soft signs (as age appropriate), such as impaired fine motor skills, neurosensory hearing loss, poor tandem gait, poor eye-hand coordination
2. Evidence of a complex pattern of behaviour or cognitive abnormalities that are inconsistent with developmental level and cannot be explained by familial background or environment alone; e.g., learning difficulties; deficits in school performance; poor impulse control; problems in social perception; deficits in higher level receptive and expressive language;

poor capacity for abstraction or metacognition; specific deficits in mathematical skills; or problems in memory, attention or judgment.
*A pattern of excessive intake characterized by substantial, regular intake or heavy episodic drinking. Evidence of this pattern may include frequent episodes of intoxication, development of tolerance or withdrawal, social problems related to drinking, legal problems related to drinking, engaging in physically hazardous behaviour while drinking or alcohol-related medical problems such as hepatic disease. †Asfurther research is completed and as, or if, lower quantities or variable patterns of alcohol use are associated with ARBD or ARND, these patterns of alcohol use should be incorporated into the diagnostic criteria. caresetting(e.g.,TWEAK,T-ACE,CAGE,AUDIT,S-MAST,B-MAST).2,36-38 Thereismoderateevidence37,38tosupporttheuseofT-ACEandTWEAKtoidentifywomenwhowouldbenefitfrominterventionforalcoholuseduringpregnancy.Ifthewomancannotabstain,sheshouldreceivesupportandbereferredtoappropriatecounsellingandtreatment.Stoppingdrinkingatanypointduringthepregnancywillimprovetheoutcomeforthebaby.Researchisbeingcarriedouttodevelopgenderandculturallyappropriateinstrumentsforthescreeningofallwomenduringtheirchild-bearingyears.38 Thepurposeofscreeningindividualsatriskfortheeffectsofprenatalalcoholexposureistodeterminewhetherapatternoflearningandbehaviouralproblemsmayberelatedtoprenatalalcoholexposure.Thescreeningcouldbeconductedthroughtheeducationsystem,thementalhealthsystem,thejudicialsystemorsocialservices.Thepurposeofscreeningshouldbetofacilitatereferraltoadiagnosticclinicandhighlighttheneedforreferralandsupportforthebirthmother. TheFASDiagnosticandPreventionNetworkhashadencouragingresultsinapplyingtheFASfacialphoto-graphicscreeningtoolinfosterchildrenandschool-agechildrenpopulations.39However,inthewidearrayofFASDs,facialdysmorphologyisoftenabsentand,inthefinalanalysis,haslittleimportancecomparedwiththeimpactofprenatalalcoholexposureonbrainfunction.However,itisimportanttonotethatthefacialphenotypeisamidlinedefectthatisthemostsensitiveandspecificmarkerforalcohol-relatedbraindamage. Allthosesuspectedofhavingbraindysfunctionshouldbereferredtoanappropriateprofessionalorclinicforassessment(i.e.,developmentalpediatrics,clinicalgenetics,psychiatry,psychology).BecauseofthespecificityofFASDclinicsinaddressingissuesrelatedtoprenatalalcoholexposure,thosewithnoprenatalalcoholexposureshouldbereferredtoanappropriateprofessionalorclinicforassessment,treatmentandfollow-up. 2. The physical examination and differential diagnosis Thepurposeofdysmorphologyassessmentistoidentifythosewithfeaturesrelatedtoprenatalalcoholexposureandalsotoidentifychildrenwithdysmorphicfeaturesduetoothercauses.Occasionally,childrenwithprenatalalcoholeffectsmayhaveanothergeneticsyndromeasaco-morbidity.Whenindoubtandiffeasible,ageneticdysmorphologyassesmentisadvisable. Ageneralphysicalandneurologicexamination,includingappropriatemeasurementsofgrowthandheadsize,assessmentofcharacteristicfindingsanddocumentationofanomalies(e.g.,cleftpalate,congenitalheartdefects,epicanthicfolds,higharchedpalate,poorlyalignedorabnormalteeth,hypertelorism,micrognathia,abnormalhairpatterning,abnormalpalmarcreases,skinlesions)isrequiredtoexcludethepresenceofothergeneticdisordersormulti-factorialdisordersthatcouldleadtofeaturesmimickingFASorpartialFAS(Table3). Somechildrenwillhavesignificantneurologicdeficits,suchasdeafness,blindnessorseizures,andtheseshouldbe Table 2: 4-Digit Diagnostic Code criteria for FASD Rank Growth deficiency 4 Significant Height and weight below 3rd percentile 3 Moderate Height and weight
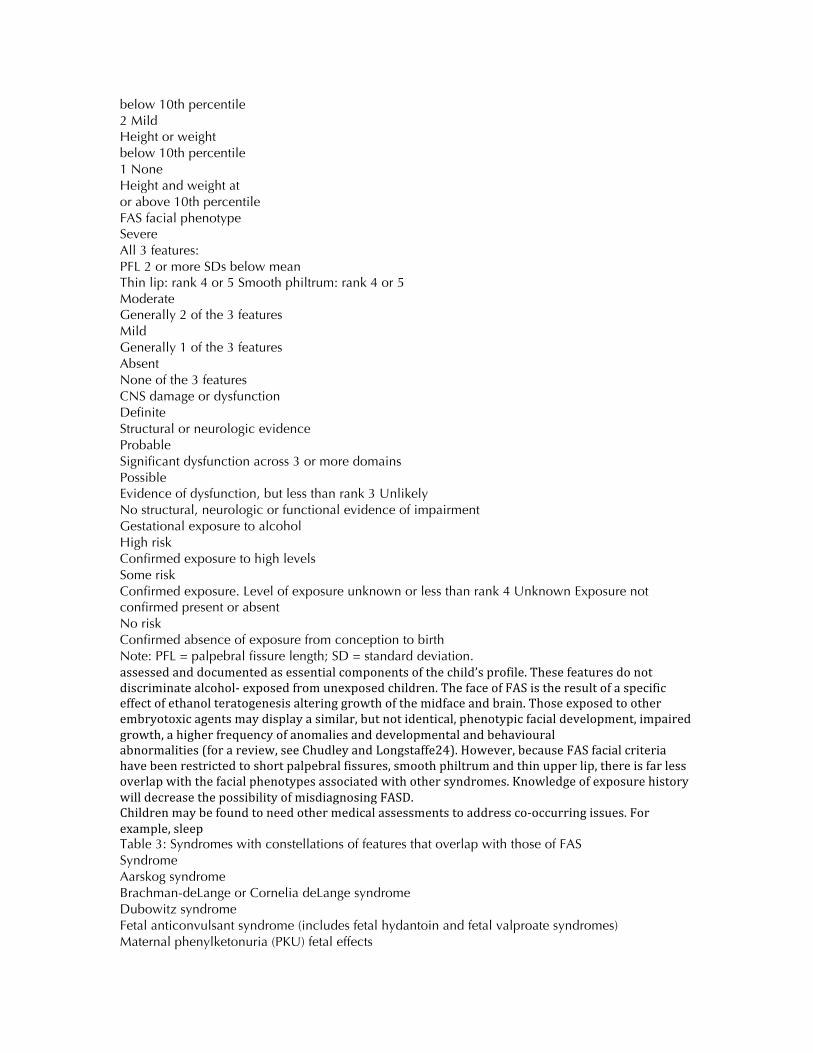
below 10th percentile 2 Mild Height or weight below 10th percentile 1 None Height and weight at or above 10th percentile FAS facial phenotype Severe All 3 features: PFL 2 or more SDs below mean Thin lip: rank 4 or 5 Smooth philtrum: rank 4 or 5 Moderate Generally 2 of the 3 features Mild Generally 1 of the 3 features Absent None of the 3 features CNS damage or dysfunction Definite Structural or neurologic evidence Probable Significant dysfunction across 3 or more domains Possible Evidence of dysfunction, but less than rank 3 Unlikely No structural, neurologic or functional evidence of impairment Gestational exposure to alcohol High risk Confirmed exposure to high levels Some risk Confirmed exposure. Level of exposure unknown or less than rank 4 Unknown Exposure not confirmed present or absent No risk Confirmed absence of exposure from conception to birth Note: PFL = palpebral fissure length; SD = standard deviation. assessedanddocumentedasessentialcomponentsofthechild’sprofile.Thesefeaturesdonotdiscriminatealcohol-exposedfromunexposedchildren.ThefaceofFASistheresultofaspecificeffectofethanolteratogenesisalteringgrowthofthemidfaceandbrain.Thoseexposedtootherembryotoxicagentsmaydisplayasimilar,butnotidentical,phenotypicfacialdevelopment,impairedgrowth,ahigherfrequencyofanomaliesanddevelopmentalandbehavioural abnormalities(forareview,seeChudleyandLongstaffe24).However,becauseFASfacialcriteriahavebeenrestrictedtoshortpalpebralfissures,smoothphiltrumandthinupperlip,thereisfarlessoverlapwiththefacialphenotypesassociatedwithothersyndromes.KnowledgeofexposurehistorywilldecreasethepossibilityofmisdiagnosingFASD. Childrenmaybefoundtoneedothermedicalassessmentstoaddressco-occurringissues.Forexample,sleep Table 3: Syndromes with constellations of features that overlap with those of FAS Syndrome Aarskog syndrome Brachman-deLange or Cornelia deLange syndrome Dubowitz syndrome Fetal anticonvulsant syndrome (includes fetal hydantoin and fetal valproate syndromes) Maternal phenylketonuria (PKU) fetal effects

Noonan syndrome Toluene embryopathy Williams syndrome Other chromosome deletion and duplication syndromes Overlapping features Widely spaced eyes, small nose with anteverted nares, broad philtrum, mid-facial recession Long philtrum, thin vermilion border of upper lip, depressed nasal bridge, anteverted nares, microcephaly Short palpebral fissures, widely-spaced eyes, epicanthal folds, variable ptosis (droopy eyes) and blepharophimosis, microcephaly Widely-spaced eyes, depressed nasal bridge, mid-facial recession, epicanthal folds, long philtrum, thin vermilion border of upper lip Epicanthal folds, short palpebral fissures, long poorly formed philtrum, thin vermilion border of upper lip, microcephaly Low nasal bridge, epicanthal folds, wide spaced eyes, long philtrum Short palpebral fissures, mid face hypoplasia, smooth philtrum, thin vermilion border upper lip, microcephaly Short palpebral fissures, anteverted nares, broad long philtrum, maxillary hypoplasia, depressed nasal bridge, epicanthic folds, microcephaly Many have short palpebral fissures, mid-facial hypoplasia, smooth philtrum. Features of this syndrome that differentiate it from FAS Round face, downslanted palpebral fissures, widow’s peak, prominent “lop” ears, specific contracture of digits on extension. Inherited as an x-linked trait. Molecular defect identified. Single eyebrow across eyes and forehead (synophrys), long eyelashes, downturned corners of mouth, short upper limbs particularly involving ulnar side, very short stature. Molecular defect identified. Shallow suprorbital ridges, broad nasal tip, clinodactyly Bowed upper lip, high forehead, small mouth Prominent glabella, small up turned nose, round face Down-slanted palpebral fissures, wide mouth with well-formed philtrum, protruding upper lip. Molecular defect identified. Large anterior fontanelle, hair patterning abnormalities, ear anomalies Wide mouth with full lips and pouting lower lip, stellate pattern of iris, periorbital fullness, connective tissue dysplasia, specific cardiac defect of suprvalvar aortic stenosis in many. Chromosome deletion on FISH (fluorescent in situ hybridization) probe analysis of 7q. Chromosomal analysis by standard analysis and some select syndromes by specific FISH probe analysis disturbanceiscommonwithprenatalalcoholexposureandmedicalproblemsrelatedtoobstructivesleepapneamayhavebeenoverlookedpreviously.Atypicalseizuresmayalsobepresentandendocrinopathiesmayexistasacomor-bidreasonforgrowthdeficiency.Theseindividualsshouldbeassessedbyappropriatehealthprofessionals. 2a. Growth Recommendations 2.1Growthshouldbemonitoredtodetectdeficiency.Presenceofpre-orpost-natalgrowthdeficiency,definedasheightorweightatorbelowthe10thpercentile(1.5standarddeviationsbelowthemean)oradisproportionatelylowweight-to-heightratio(atorbelowthe10thpercentile)usingappropriatenorms.Todeterminethatachildisgrowthdeficientrequirestakingintoconsiderationconfoundingvariablessuchasparentalsize,geneticpotentialandassociatedconditions(e.g.,gestationaldiabetes,nutritionalstatus,illness). Comments Childrenaffectedbyprenatalalcoholexposuremayhaveprenatalorpostnatalgrowthdeficits.Theycanbesmallforgestationalageinuteroandremainbelowaveragethrough-outtheirliveswithrespecttoheadcircumference,weightandheight.Manychildrencanhavenormalgrowth

parameters,butbeatriskinlaterdevelopmentforclinicallysignificantlearning,behaviouralandcognitivedeficits.Ifthereisnoalcoholexposureinthethirdtrimester,thegrowthparameterscanbenormal.Gestationaldiabetescanleadtoincreasedfetalsize,whichcanmasktheeffectsofgrowthretardationfromprenatalalcoholexposure.Furthermore,iftheinfantisbornintoafamilyoracommunitywhere“normal”sizeisabovetheaverageforthegeneralpopulation,growthimpairmentmaybemaskedifthechildiscomparedwithstandardgrowthparametersratherthancommunitynorms.14Growthdeficienciesmaynotpersistwithage,andinfantgrowthrecordsmaynotbeavailableforadultscominginforassessmentforthefirsttime.ThereisaneedtoestablishgrowthnormsfortheCanadianpopulationandsubpopulationsthatdifferfromthegeneralpopulation. 2b. Facial features Recommendations 2.2The3characteristicfacialfeaturesthatdiscriminateindividualswithandwithoutFASare:
• Shortpalpebralfissures,atorbelowthe3rdper-centile(2standarddeviationsbelowthemean).
• Smoothorflattenedphiltrum,4or5onthe5-pointLikertscaleofthelip-philtrumguide.25,39
•Thinvermilionborderoftheupperlip,4or5onthe5-pointLikertscaleofthelip-philtrumguide. 2.3Associatedphysicalfeatures(abnormalitiessuchasmidfacehypoplasia,micrognathia,abnormalpositionorformationoftheears,higharchedpalate,hyper-telorism,epicanthicfolds,limbandpalmarcreaseab-normalitiesandshort-upturnednose)shouldberecordedbutdonotcontributetoestablishingthediagnosis. 2.4Facialfeaturesshouldbemeasuredinallagegroups.Ifapatient’sfacialfeatureschangewithage,thediagnosisofthefacialfeaturesshouldbebasedonthepointintimewhenthefeaturesweremostseverelyexpressed.Whendiagnosingadults,itcanbehelpfultoviewchild-hoodphotographs. Comments AcharacteristiccraniofacialprofileassociatedwithFASwasfirstdescribedbyJonesandSmith40in1975andlaterrefinedbyAstley,Clarrenandothers.25,32,39IndividualswithFAShaveshortpalpebralfissures,athinupperlipandan Fig. 1: Lip-philtrum guide. A 5-point pictorial scale for measuring philtrum smoothness and upper lip thinness. Features are measured independently; for example, an individual can have a rank 5 philtrum and a rank 1 upper lip. indistinctphiltrum(Fig.1).Palpebralfissurelength,philtrumandupperlipdifferwithraceandage.Growthandfacialanthropometricdataareneededforthespecificpopulation,assensitivityandspecificityoftheassessmentwillbeloweredwithouttheuseofappropriatenorms.SomediscriminatingcharacteristicfeaturesinFAS(i.e.,up-perliporphiltrum)maybecomelessrecognizablewithage,makingaccuratediagnosismoredifficultinoldergroups,butfacialfeaturesshouldalwaysbemeasured.MorelongitudinalresearchisneededtocorrelatechangesinthesecharacteristicphysicalfindingsinadolescentsandadultsdiagnosedwithFASorpartialFAS. Palpebralfissurelength(Fig.2)isdifficulttomeasureaccuratelywithouttraining.Thomasandco-workers41havepublishednormsforpalpebralfissurelengthat29weeksgestationto14years.Thereareanumberofopinionsaboutwhichnormsareappropriate,41-44butitisgenerallyagreedthatallareflawedinsomerespect. TwographsofpalpebralfissurelengtharepresentedinAppendix2.Somediscrepanciesexist.BothstudiesusedNorthAmericanwhitesubjects;standardsforotherpopu-lationsinCanadaarenotcurrentlyavailable.Appendix2-1maybemorereliablewhenmeasuringpalpebralfissurelengthusingaplasticruler(intheexperienceofoneoftheauthors);Appendix2-2maybemorereliableifslidecalipersareused(intheexperienceofoneoftheauthors).Percentileranksforbothgraphsseemtobeinagreementuntilage7years,afterwhichAppendix2-2showslongerpalpebralfissuresinolderchildrenandadolescentsthanAppendix2-1.Webelievethismaybeduetodifferencesinmeasurementtechnique.Becausecalipersarenotacom-montoolinmostmedicalclinics,werecommendtheuseofaclearflexibleplasticruler.

Thereisaneedtoestablishupdatednormsforallagesandsubpopulations.AstleyandClarren25,39havedevelopednormsfortheassessmentofthelipandphiltrumusingtheirpictorialguide.Lip-philtrumguidesweredevelopedforuseinCaucasianandAfrican-Americanpopulations,butnostandardsarecurrentlyavailableforotherpopulations. 3. Neurobehavioural assessment Recommendations 3.1Thefollowingdomainsshouldbeassessed:
1. Hardandsoftneurologicsigns(includingsensory-motorsigns).
2. Brainstructure(occipitofrontalcircumference,magneticresonanceimaging,etc.).
3. Cognition(IQ).4. Communication:receptiveandexpressive.5. Academicachievement.6. Memory.7. Executivefunctioningandabstractreasoning.8. Attentiondeficit/hyperactivity.
i.Adaptivebehaviour,socialskills,socialcommunication. 3.2Theassessmentshouldincludeandcomparebasicandcomplextasksineachdomain,asappropriate. 3.3Thedomainsshouldbeassessedasthoughtheywereindependententities,butwherethereisoverlapexperiencedclinicaljudgmentisrequiredtodecidehowmanydomainsareaffected. 3.4Adomainisconsidered“impaired”whenonastandardizedmeasure: a.Scoresare2standarddeviationsormorebelowthemean,or b.Thereisadiscrepancyofatleast1standarddeviationbetweensubdomains.Forexample:i.Verbalv.non-verbalabilityonstandardIQtests,ii.Expressivev.receptivelanguage, iii.Verbalv.visualmemory,orc.Thereisadiscrepancyofatleast1.5–2standarddeviationsamongsubtestsonameasure,takingintoaccountthereliabilityofthespecificmeasureandnormalvariabilityinthepopulation. 3.5Inareaswherestandardizedmeasurementsarenotavailable,aclinicaljudgmentof“significantdysfunction”ismade,takingintoconsiderationthatimportantvariables,includingthechild’sage,mentalhealthfactors,socioeconomicfactorsanddisruptedfamilyorhomeenvironment(e.g.,multiplefosterplacements,historyofabuseandneglect),mayaffectdevelopmentbutdonotindicatebraindamage. 3.6Evidenceofimpairmentin3domainsisnecessaryforadiagnosis,butacomprehensiveassessmentrequiresthateachdomainbeassessedtoidentifystrengthsandweaknesses. 3.7Thediagnosisshouldbedeferredforsomeat-riskchildren(e.g.,preschool-age)whohavebeenexposedtoalcohol- Fig. 2: Palpebral fissure length. To measure palpebral fissure length, identify the inner corner or encanthion (en) and outer corner or excanthion (ex) for each eye. Have the patient look up so that ex can be seen clearly. With a clear flexible ruler held in the horizontal plane, measure the length of each ex-en interval immediately below the eye, being careful not to touch the eye or eyelashes. Plot the result on an appropriate nomo-gram chart to determine the percentile or standard deviation for each eye. Childrencanbeexposedtoprenatalalcoholbutmaynotyetdemonstratemeasurabledeficitsinthebraindomainsormaybetooyoungtobetestedinallthedomains.However,developmentalassessmentshouldidentifyareasforearlyintervention. ExamplesofteststhataremostwidelyusedtoassessthedomainsandtheircriteriaareprovidedinAppendix3. Comments Researchreportshavedocumentedarangeofcognitiveandbehaviouraloutcomesassociatedwithprenatalalcoholexposure.Contemporarystudieshavereportedsomeoftheseoutcomesinthe

absenceofFASphysicalfeatures.Currently,nomodalprofileofabilitieshasbeenfoundtobeuniquetoalcoholexposure,isobservedinallthosewithprenatalalcoholexposure,orcanbedistinguishedfromthatobservedwithsomeotherneurobehaviouraldisorders.Furthermore,noteverydeficitthatwemayidentifyinachildwithprenatalexposuretoalcoholmaybesolelytheresultofalcoholexposure.AnexpertanalysisofneurodevelopmentaldeficitscausedbyarangeofteratogensandcongenitaldisordersfailedtoresultinaconsensusoncoredeficitsassociatedonlywithFASD.4 ResearchandexperiencehasshownthatfeaturesofFASDarecomplexandmultifaceted,originatingwithorganicbraindamagecausedbyalcohol,butinteractingwithgeneticandotherinfluences.Overthelifespanoftheaffectedperson,thesefeaturesmaybeexacerbatedormitigatedbyenvironmentalexperiences. TomakethediagnosisofFAS,featuressuchasmicrocephaly,structuralabnormalities(asmaybedetectedonbrainscans)andhardneurologicsignsaretakenasstrongevidenceoforganicbraindamage.Webelievethatlowaveragetoborderlineintelligenceandsoftneurologicsignsaloneareinsufficientevidenceofbraindamagebecausetheyarefrequentlyfoundinthegeneralpopulation.Featuressuchaslearningdifficulties,attentiondeficit/hyperactivitydisorderanddeficitsinadaptiveskills,memory,higher-levellanguageandabstractthinkingarefrequentlyseeninchildrenwithprenatalalcoholexposure,butalsoamongthosewithotheretiologies.Thesedeficitscanbemultifactorialinetiologyandcanalsobeattributedtogeneticsorpostnatalexperiences. The4-DigitDiagnosticCodeevaluationoftheFASDbrainisbasedonlevelsofcertainty,inthejudgementoftheclinician,thattheindividual’scognitiveandbehaviouralproblemsreflectbraindamage.Ahigherratingmayreflectamoresevereexpressionoffunctionaldisability,asynchronouspatternsacrossdomainsorcertaintybasedondeficitsinmultipledomains.Thedeterminationisbasedonobjectiveevidenceof“substantialdeficienciesordiscrepanciesacrossmultipleareasofbrainperformance.”25,39 TheIOM4alsorequires“evidenceofacomplexpatternofbehaviororcognitiveabnormalitiesthatareinconsistentwithdevelopmentallevelandcannotbeexplainedbyfamilialbackgroundorenvironmentalone,suchaslearningdifficulties;deficitsinschoolperformance;poorimpulsecontrol;problemsinsocialperception;deficitsinhigherlevelreceptiveandexpressivelanguage;poorcapacityforabstractionormetacognition;specificdeficitsinmathematicalskills;orproblemsinmemory,attention,orjudgment,”butismuchlessspecificthanthe4-DigitDiagnosticCodewithregardtothecriteriafordeterminingthedeficit. Wehaveadaptedthemethodofthe4-DigitDiagnosticCodewithregardtoidentifyingdomainsandseverityofimpairmentorcertaintyofbraindamage.CurrentresearchshowsoverlapbetweentheneurobehaviouraloutcomesinFASandARNDdiagnosticgroupswhenneuropsychologicdataarecompared.45Inaddition,webelievethatasinglefeaturesuchasmicrocephalyisnotasufficientindicatorofbraindamageforthepurposesofanFASdiagnosisbecauseitmayreflectgeneticorethnicdifferencesnotreflectedincurrentlyavailablephysicalnorms.Ourconcernisthattheremaybeanover-diagnosisofFASifevidenceofbraindamageisbasedonasingleindicatorasallowedbyboththe4-DigitDiagnosticCodeandtheIOMmodels.Anindividualshowinghardneurologicsignsorstructuralbrainabnormalities(i.e.,truebraindamage)willlikelyshowadditionalfunctionaldeficitsinthelisteddomains.AdiagnosisoffullFASwillnotbedeniedbycombiningthecriteriaforfullFASandARNDinthisharmonizedsystem. Althoughthedomainsareconsideredtobeseparateandindependententities,thereisobviouslyoverlap.Forexample,adiscrepancybetweenverbalandnon-verbalscoresonanIQtest(takingintoaccountnormalvariabilityinthepopulation)maybereflectingaspecificlanguagedisability.Iflanguageisdeficient,candeficitsinverbalmemorybeconsideredanadditionaldomain?Doesalanguagedeficitrepresentbraindamageifthechildhasexperiencedaprolongedperiodofsocialdeprivation?Thecut-offof2standarddeviationsbelowthemeanonstandardizedtestsisrecommendedtoincreaseconfidencethatabilitiesinthedomainareimpairedasaresultofbraindamageandarescoredas“3”(significantdysfunction)onthe4-DigitDiagnosticCode.With3suchdomains,thebrainrankis3:“probablebraindysfunction.” Werealizethatinstandardneuropsychologicpractice,1.5standarddeviationsbelowthemeanmayindicatesubtleimpairments.Usingthe4-DigitDiagnosticCode,thedomainswouldbescoredas“moderatedysfunction”andmayresultinabrainrankof2:“possiblebraindysfunction.”Thesemoresubtlefindingsareanimportantpartoftheindividual’sprofile.Forthepurposeofdiagnosis,

however,andthecertaintythatthescoresrepresentinjurycausedbyalcohol,themoreextremecutoffisrecommended.Themultidisciplinaryteam,reviewingthedataandusingexperiencedclinicaljudgement,iscriticalinmakinganaccuratediagnosisasqualitativeaspectsofperformancearealsoimportant.Thediagnosticprofileisdynamicandmaychangeovertime;thusindividualsaffectedorsuspectedtobeaffectedmayrequireseveralassessmentsovertime.Servicesshouldnotbebasedonthediagnosisitself,butratherontheprofileofbrainfunction-dysfunction.4. Treatment and follow-up Recommendations
1. 4.1EducationofthepatientandfamilymembersonfeaturesofFASDiscrucial.Thepotentialpsychosocialtensionsthatmightbeexpectedtodevelopwithinthefamilyasaresultofthediagnosisshouldalsobediscussed.Thismustbedoneinaculturallysensitivemannerusingappropriatelanguage.
2. 4.2Amemberofthediagnosticteamshouldfollow-upout-comesofdiagnosticassessmentsandtreatmentplanswithinareasonablelengthoftimetoassurethattherecommendationshavebeenaddressed.
3. 4.3Diagnosedindividualsandtheirfamiliesshouldbelinkedtoresourcesandservicesthatwillimproveout-come.However,whereservicesarelimitedinthecom-munity,anindividualshouldnotbedeniedanassessmentfordiagnosisandtreatment.Oftenthediagnosisintheindividualistheimpetusthatleadstothedevelopmentofresources.
4. 5. Maternal alcohol history in pregnancy Recommendations
1. 5.1Prenatalalcoholexposurerequiresconfirmationofalcoholconsumptionbythemotherduringtheindexpregnancybasedonreliableclinicalobservation,self-report,reportsbyareliablesourceormedicalrecordsdocumentingpositivebloodalcohol,alcoholtreatmentorothersocial,legalormedicalproblemsrelatedtodrinkingduringthepregnancy.
2. 5.2Thenumberandtype(s)ofalcoholicbeveragesconsumed(dose),thepatternofdrinkingandthefrequencyofdrinkingshouldallbedocumentedifavailable.
3. 5.3Hearsay,lifestyle,otherdruguseorhistoryofalcoholexposureinpreviouspregnanciescannot,inisolation,beinformativeofdrinkingpatternsintheindexpregnancy.However,co-occurringdisorders,significantpsychosocialstressorsandprenatalexposuretoothersubstances(e.g.,smoking,licitorillicitdrugs)intheindexandpreviouspregnanciesshouldstillberecorded,basedonknowninteractiveeffectsofthesevariablesontheseverityofpregnancyoutcomesforboththemotherandheroffspring.
4. Comments Gatheringreliableinformationaboutmaternaldrinkingiskeytoestablishinganaccuratediagnosis.Specialattentionmustbepaidtoinquiringaboutmaternalalcoholusebeforethewomanrecognizedthatshewaspregnant.Somewomendonotconsiderthattheirpriordrinkingisimportantandmanyunderreportit.Trainingisrequiredinhowtoobtainthisinformationinanon-threatening,non-judgmentalway. Canadiansurveydatasuggestthatthenumberofwomenwhoreportdrinkingduringpregnancyhasdecreased.TheNationalPopulationHealthSurvey,1994–199546andNationalLongitudinalSurveyofChildrenandYouth,1994–199547re-portedthat17–25%ofwomendrankalcoholatsomepointduringtheirpregnancyand7–9%drankalcoholthrough-outtheirpregnancy.AccordingtotheNationalLongitudinalSurveyofChildrenandYouth,1998–19994814.4%ofwomendrankatsomepointduringtheirpregnancyand4.9%drankthroughouttheirentirepregnancy(3%reportedbingedrinkingduringpregnancy).IntheFall2002SurveyofFirstNationsPeopleLivingonReserve,4953%oftherespondentssaidthatcuttingdownorstoppingalcoholusewasimportantforwomentohaveahealthybaby. Theevaluationof“significantalcoholexposure”isoftenconfusing.TheIOMdescribessignificantalcoholexposureas“apatternofexcessiveintakecharacterizedbysubstantial,regularintakeorheavyepisodicdrinking”4(theNationalInstituteonAlcohol,Alcoholism,andAlcoholAbusedefines

heavyalcoholuseasdrinking5ormoredrinksperoccasionon5ormoredaysinthepast30days36).Evidenceofthispatternmayincludefrequentepisodesofintoxication,developmentoftoleranceorwithdrawal,socialproblemsrelatedtodrinking,legalproblemsrelatedtodrinking,engaginginphysicallyhazardousbehaviourwhiledrinking,oralcohol-relatedmedicalproblemssuchashepaticdisease.Asfurtherresearchiscompletedandas,orif,lowerquantitiesorvariablepatternsofalcoholuseareassociatedwithalcohol-relatedbirthdefects(ARBD)orARND,thesepatternsofalcoholuseshouldbeincorporatedintothediagnosticcriteria.4 6. Diagnostic criteria for FAS, partial FAS and ARND Recommendations 6.1Thecriteriaforthediagnosisoffetalalcoholsyndrome,afterexcludingotherdiagnoses,are:A.Evidenceofprenatalorpostnatalgrowthimpairment,asinatleast1ofthefollowing:a.Birthweightorbirthlengthatorbelowthe 10thpercentileforgestationalage.b.Heightorweightatorbelowthe10thpercentile forage.c.Disproportionatelylowweight-to-heightratio (=10thpercentile).Simultaneouspresentationofall3ofthefollowingfacialanomaliesatanyage:a.Shortpalpebralfissurelength(2ormorestandarddeviationsbelowthemean).b.Smoothorflattenedphiltrum(rank4or5onthelip-philtrumguide). c.Thinupperlip(rank4or5onthelip-philtrumguide). C.Evidenceofimpairmentin3ormoreofthefollowingcentralnervoussystemdomains:hardandsoftneurologicsigns;brainstructure;cognition;communication;academicachievement;memory;executivefunctioningandabstractreasoning;attentiondeficit/hyperactivity;adaptivebehaviour,socialskills,socialcommunication. D.Confirmed(orunconfirmed)maternalalcoholexposure. 6.2Thediagnosticcriteriaforpartialfetalalcoholsyndrome,afterexcludingotherdiagnoses,are:A.Simultaneouspresentationof2ofthefollowingfacialanomaliesatanyage:
1. Shortpalpebralfissurelength(2ormorestandarddeviationsbelowthemean).2. Smoothorflattenedphiltrum(rank4or5onthelip-philtrumguide).3. Thinupperlip(rank4or5onthelip-philtrumguide).
B.Evidenceofimpairmentin3ormoreofthefollowingcentralnervoussystemdomains:hardandsoftneurologicsigns;brainstructure;cognition;communication;academicachievement;memory;executivefunctioningandabstractreasoning;attentiondeficit/hyperactivity;adaptivebehaviour,socialskills,socialcommunication. C.Confirmedmaternalalcoholexposure.
3. 6.3Thediagnosticcriteriaforalcohol-relatedneurodevelopmentaldisorder,afterexcludingotherdiagnoses,are:A.Evidenceofimpairmentin3ormoreofthefollowingcentralnervoussystemdomains:hardandsoftneurologicsigns;brainstructure;cognition;communication;academicachievement;memory;executivefunctioningandabstractreasoning;attentiondeficit/hyperactivity;adaptivebehaviour,socialskills,socialcommunication. B.Confirmedmaternalalcoholexposure.
4. 6.4Thetermalcohol-relatedbirthdefects(ARBD)shouldnotbeusedasanumbrellaordiagnosticterm,forthespectrumofalcoholeffects.ARBDconstitutesalistofcongenitalanomalies,includingmalformationsanddysplasiasandshouldbeusedwithcaution (Table1).
Comments OurdefinitionofpartialFASdiffersfromthepublishedIOMcriteria.4Wheresignificantprenatalalcoholexposureisknownandthereissignificantgrowthretardationandsignificantindicativefacialfeaturesbutnoevidenceofbraininvolvement,adiagnosisofpartialFAScouldbemadeusingtheIOMcriteria.Itisourviewthat,usingthetermpartialFASintheabsenceofmeasurablebraindeficits

couldbeharmfulfortheindividualbecausethediagnosisofpartialFASimpliesbraindysfunction.Ifsomecharacteristicfacialfeaturesandgrowthimpairment,withoutsignificantdevelopmentalorbehaviouralproblems,arefoundinchildrenunder6yearsofage,itwouldbeprudenttosaythatthechildmaybeatriskoflearningandbehaviourproblemsatalatertimeduetoprenatalalcoholexposure.Noalcohol-relateddiagnosisshouldbemade,butthechildmustbemonitoredbythefamilyphysicianorhealthcareworkeranddeficitsshouldbedocumentedusinganeu-rodevelopmentalassessment. Theterm“partial”inpartialFASdoesnotimplythattheseindividualsarelessseverelyimpairedinday-to-dayfunctioningthanthosewithadiagnosisofFAS,asthedeficitsinbrainfunctionmaybesimilar. 7. Harmonization of the Institute of Medicine (IOM) and 4-Digit Diagnostic Code approaches Recommendations 7.1Theapproachidentifiedinthe4-DigitDiagnosticCodeshouldbeusedtodescribe,assessandmeasureobjectivelyalcoholexposure,growth,facialfeaturesandbraindamage.The4-DigitDiagnosticCodeshouldberecordedforeachassessmentandmaybeusefulforsurveillanceandresearchpurposes. 7.2TheterminologyintheIOMcriteriashouldbeusedtodescribethediagnosis. Comments Table4andTable5illustratehowwerecommendharmonizingtheIOMand4-DigitDiagnosticCodecriteria.TheARBDcategoryhaslimitedutilityinthediagnosis,butwedorecognizethatalcoholisteratogenicandmayberesponsibleforbirthdefectsifexposureoccursduringcriticalperiodsofdevelopment.However,intheabsenceofotherfeaturesofFASorbraindeficits,itisdifficulttoat-tributecausation. Future research related to diagnostic guidelines Thelackorunavailabilityofevidenceanddatainkeyareaslimitstheeffectivenessofthediagnosticprocess,ingeneral.SuchkeyareasincludethedevelopmentofCanadiangrowthandanthropometricnormsforallagesandethno-culturalgroups.Thereisalsoaneedforthedevelopmentandvalidationofscreeningtoolsthatarespecificandsensitivetoprenatalalcoholexposure.Thesetoolsshouldbeadaptableforuseinvariouscontexts,theyshouldbeculturallyappropriateandtheyshouldleadtoaccuratereferralsfordiagnosisandassessment.Emerging issues Biomarkers Often,womenwillnotaccuratelyrecalltheamountorfrequencyofalcoholconsumptionduringpregnancy.Somewomenmayalsounderestimateconsumptionlevelordenythattheydrankalcoholduringpregnancy.Medicalrecordsareknowntobeincompletewithrespecttomaternalalcoholhistory.Currently,therearenoreliablemeanstocon-firmmaternaldrinkingusingbiochemicalmarkersinpregnancy.Highlevelsofwholeblood-associatedacetaldehyde,carbohydrate-deficienttransferrin,gamma-glutamyltranspeptidaseandmeanredbloodcellvolumemaybeusefulmarkersinpregnantwomen.50 Studiesareunderwaytodeterminetheutilityoffattyacidethylestersinmeconiumasmarkersforprenatalexposuretoalcohol.51-53Thismarkerwillonlybeusefulifitcanbeestablishedthatfattyacidethylesterlevelsinmeconiumarepredictiveofdevelopmentaloutcome.Meconiumtestingcouldalertcaregiverstoinfantswhomightbeatriskforalcoholeffectsandleadtoappropriatemonitoring,interventionandprevention.Ethicalissuesregardinginformedconsentsurroundtheuseofbiologicalmarkersinthebabythatmayindicatematernaldrinking. Recentinnovationshaveledtothedevelopmentoflasersurfacescanning,anon-invasivemethodforacquiring3-dimensionalimages.33,34Thistechniqueispromisingintheanalysisoffacialfeaturesassociatedwithprenatalalcoholexposure,but,atpresent,isaresearchtoolonly. Remote and rural areas

Theavailabilityofdiagnosticservicesislimitedinruralandremoteareas.Acommunitymaynothaveaccesstoadiagnosticteamorresourcesandservices.Untilregionallybaseddiagnosticteamsareestablished,theuseoftelemedicinefordistantdiagnosis,consultationandtrainingmaybehelpful.31Recentadvancesusingdigitalimagingandcomputer-assistedanalysisforthediagnosisofcharacteristicfeaturesofFAShaveshownpromiseforanalysisoffacialfeaturesassociatedwithprenatalalcoholexposure.32,33,44 Table 4: Harmonization of Institute of Medicine (IOM) nomenclature and 4-digit diagnostic code ranks for growth, face, brain and alcohol history 4-digit diagnostic code ranks IOM nomenclature FAS (with confirmed exposure) FAS (without confirmed exposure) Partial FAS (with confirmed exposure)* ARND (with confirmed exposure) Growth deficiency 2, 3 or 4 2, 3 or 4 1, 2, 3 or 4 1, 2, 3 or 4 FAS facial phenotype 3 or 4 3 or 4 2, 3 or 4 1 or 2 CNS damage or dysfunction 3 or 4 3 or 4 3 or 4 3 or 4 (2 for < 6 years) Gestational exposure to alcohol 3 or 4 2 3 or 4 3 or 4 Note: ARND = alcohol-related neurodevelopmental disorder; CNS = central nervous system; FAS = fetal alcohol syndrome. Source: Developed by Kwadwo Asante and Julianne Conry *Any final 4-digit code that can be made with these combinations of numbers and that is not also an FAS code signifies partial FAS. Combinations of face 2 that include two significant facial features also meet criteria for partial FAS. Table 5: Comparison of Institute of Medicine (IOM) and 4-Digit Diagnostic Code methods in the diagnosis of FAS Feature Facial characteristics Number of features required Thin (flat) upper lip Flattened philtrum Flat midface Short palpebral fissures Other features Growth Number of features required Low birth weight alone Decelerating weight over time Low weight-to-height ratio Low height and low weight IOM Not specified Yes Yes Yes Yes ? 1 Yes, percentile not specified

Yes Yes No 4-Digit Diagnostic Code 3 of 3 Yes Yes No Yes No 1 No No No Yes, ʺ 10th percentile 1 structural or neurologic feature OR 3 domains of significant impairment in function Yes, ʺ 3rd percentile Yes Yes No Central nervous system dysfunction Number of features required Structural features may include: Microcephaly at birth Structural abnormalities Hard neurologic signs Sof
Adult diagnosis Diagnosisofadultscreatesspecialchallengesinallaspectsofthediagnosis.Physicalfeaturesmaychangeovertime,theremaybecatch-upgrowth,andcumulativeenvironmentalinfluencesmaydistorttheevaluationofbrainfunction.Theadult’shistorymayincludeadditionaltraumaticheadinjury,alcoholanddrugabuse,andmentalhealthproblems.Althoughtestsforthevariousdomainsarereadilyavailable,cliniciansworkingwiththeadultFASDpopulationfindthatthetestsareoftennotsensitivetoreal-lifeissues.Inadditiontothedatarequiredforthediagnosis,anassessmentmustincludeadditionalcomponentssuchasfunctionalliteracyandnumeracy,employabilityandqualityoflife,whichfallwithinthedomainofadaptiveskills.Theclinicianshouldnotrelysolelyontheself-reportoftheindividualwhoisalcohol-affected;thehistoryandabilitiesoftheindividualmustbeverifiedbyareliablesource. Conclusion Theassessmentforprenatalalcoholexposureisadiagnosisfortheaffectedperson,thebirthmotherandpossiblyaffectedsiblings.Ratherthanlabeling,adiagnosisprovidesablueprintforearlyintervention.Treatmentplanningandimplementation,specificallytargetedtowardtheuniqueneedsoftheindividualandthefamily,formalargepartofthediagnosis. TheseguidelinesandrecommendationshavebeendevelopedinparallelandinconsultationwithaUnitedStatescommitteechargedwiththesametask.54ThechallengesforpreventionanddiagnosisofFASDandinterventiontoassistthoseaffectedbythisdisorderareevolvinganddynamic.Researchisongoingtodeterminewhethertools,suchasnovelbrainimagingtechniques,biomarkersandDNAmicro-arraytechniques,mightenhanceaccurateandreliablealcohol-relateddiagnosesandtreatment. Wehopethattheseguidelinesandrecommendationswillbeusedtofacilitatetrainingofhealthprofessionals,improveaccesstodiagnosticservicesandfacilitatereferralforinterventionortreatmentforallpeopleandfamilieslivingwiththisdisability. Thisarticlehasbeenpeerreviewed. FromtheChildren’sHospital,HealthSciencesCentre,DepartmentsofPediatricsandChildHealthandBiochemistryandMedicalGenetics,UniversityofMani-toba,Winnipeg,Man.(Chudley);theDepartmentofEducationalandCounsellingPsychologyandSpecialEducation,UniversityofBritishColumbia;AsanteCentreforFetalAlcoholSyndrome,MapleRidge,B.C.(Conry);theDepartmentofOb-stetricsandGynecology,UniversityofOttawa,Ottawa,Ont.(Cook);theDepart-mentofPediatrics,UniversityofBritishColumbia,BCChildren’sHospital,Van-couver,B.C.(Loock);theProvincialMedicalGeneticsProgram;theDepartmentofPediatrics,MemorialUniversityofNewfoundland,St.John’s,Nfld.(Rosales);andtheDepartmentofPediatrics,GeorgesDumontHospital,Moncton,N.B.(LeBlanc). Competing interests: Nonedeclared.

Contributors: Allauthorscontributedequallytothismanuscript.Allauthorscontributedsubstantiallytoconceptionanddesign,oracquisitionofdata,oranalysisandinterpretationofdataanddraftedthearticleorreviseditcriticallyforimportantintellectualcontent.Theygavetheirfinalapprovaloftheversionsubmittedtobepublished. Acknowledgements: ThisworkissupportedbytheFASDTeamsofthePublicHealthAgencyofCanadaandtheFirstNationsandInuitHealthBranch,HealthCanada.Theauthorswouldliketothankthemanycliniciansandindividualswhohelpeddevelop,reviewandprovidefeedbackontheseguidelines,especiallythePublicHealthAgencyofCanada’sNationalAdvisoryCommitteeonFASD;Drs.FredBoland,SusanAstleyandSterlingClarren;andtheCentersforDiseaseCon-trolandPrevention’sscientificworkinggroupondiagnosis.Thisworkwassup-portedbythePublicHealthAgencyofCanadaandtheFirstNationsandInuitHealthBranch,HealthCanada. References 1.JonesKL,SmithDW.Recognitionofthefetalalcoholsyndromeinearlyin-fancy.Lancet1973;2(7836):999-1001. 2.SokolRJ,Delaney-BlackV,NordstromB.Fetalalcoholspectrumdisorder.JAMA2003;290(22):2996-9. 3.StreissguthAP.Fetalalcoholsyndrome:aguideforfamiliesandcommunities.Bal-timore:PaulH.Brookes;1997. 4.StrattonK,HoweC,BattagliaFC.Fetalalcoholsyndrome:diagnosis,epidemiol-ogy,prevention,andtreatment.Washington:InstituteofMedicineandNationalAcademyPress;1996.Available:www.nap.edu/books/0309052920/html/index.html(accessed2004Oct29). 5.StreissguthAP.Maternaldrinkingandtheoutcomeofpregnancy:implica-tionsforchildmentalhealth.AmJOrthopsychiatry1977;47(3):422-31. 6.Jointstatement:preventionoffetalalcoholsyndrome(FAS)fetalalcoholef-fects(FAE)inCanada.Ottawa:HealthCanada;1996. 7.RobertsG.,NansonJ.Bestpracticesfetalalcoholsyndrome/fetalalcoholeffectsandtheeffectsofothersubstanceuseduringpregnancy.Ottawa:HealthCanada;2003. 8.ChavezGF,CorderoJF,BecerraJE.Leadingmajorcongenitalmalforma-tionsamongminoritygroupsintheUnitedStates,1981-1986.MMWRMorbMortalWklyRep1988;37(3):17-24. 9.SokolRJ,ClarrenSK.Guidelinesforuseofterminologydescribingtheimpactofprenatalalcoholontheoffspring.AlcoholClinExpRes1989;13(4):597-8.10.SampsonPD,BooksteinFL,BarrHM,StreissguthAP.Prenatalalcoholex- posure,birthweight,andmeasuresofchildsizefrombirthtoage14years.Am JPublicHealth1994;84(9):1421-8.11.SampsonPD,StreissguthAP,BooksteinFL,LittleRE,ClarrenSK,Dehaene P,etal.Incidenceoffetalalcoholsyndromeandprevalenceofalcohol-related neurodevelopmentaldisorder.Teratology1997;56(5):317-26.12.RobinsonGC,ConryJL,ConryRF.ClinicalprofileandprevalenceoffetalalcoholsyndromeinanisolatedcommunityinBritishColumbia.CMAJ1987; 137(3):203-7.13.WilliamsRJ,OdaiboFS,McGeeJM.Incidenceoffetalalcoholsyndromein northeasternManitoba.CanJPublicHealth1999;90(3):192-4.14.SquareD.FetalalcoholsyndromeepidemiconManitobareserve.CMAJ 1997;157(1):59-60.15.AsanteKO,Nelms-MaztkeJ.Reportonthesurveyofchildrenwithchronichandi- capsandfetalalcoholsyndromeintheYukonandNorthwestBritishColumbia. Whitehorse:CouncilforYukonIndians;1985.16.HabbickBF,NansonJL,SnyderRE,CaseyRE,SchulmanAL.Foetalalcohol syndromeinSaskatchewan:unchangedincidenceina20-yearperiod.CanJ PubHealth1996;87(3):204-7.17.SoodB,Delaney-BlackV,CovingtonC,Nordstrom-KleeB,AgerJ,Templin T,etal.Prenatalalcoholexposureandchildhoodbehavioratage6to7years: I.dose-responseeffect.Pediatrics2001;108(2):E34.18.BingolN,SchusterC,FuchsM,IosubS,TurnerG,StoneRK,etal.Thein-
fluenceofsocioeconomicfactorsontheoccurrenceoffetalalcoholsyndrome. AdvAlcoholSubstAbuse1987;6(4):105-18.19.AstleySJ,BaileyD,TalbotC,ClarrenSK.Fetalalcoholsyndrome(FAS)pri- marypreventionthroughFASdiagnosis:I.Identificationofhigh-riskbirthmothersthroughthediagnosisoftheirchildren.AlcoholAlcohol2000;35(5):499-508. 20.JacobsonJL,JacobsonSW.Prenatalalcoholexposureandneurobehavioraldevelopment:whereisthethreshold?AlcoholHealthResWorld1994;18:30-6. 21.JacobsonJL,JacobsonSW.Drinkingmoderatelyandpregnancy.Effectsonchilddevelopment.AlcoholResHealth1999;23(1):25-30. 22.StreissguthA,BarrH,KoganJ,BooksteinF.Primaryandsecondarydisabili-tiesinfetalalcoholsyndrome.In:StreissguthAP,KanterJ,editors.Thechal-lengeoffetalalcoholsyndrome:overcomingsecondarydisabilities.Seattle:Univer-sityofWashingtonPress;1997.pp25-39. 23.AstleySJ,BaileyD,TalbotT,ClarrenSK.Fetalalcoholsyndrome(FAS)pri-marypreventionthroughFASdiagnosis:II.Acomprehensiveprofileof80birthmothersofchildrenwithFAS.AlcoholAlcohol2000;35(5):509-19.
24. ChudleyAE,LongstaffeSE.Fetalalcoholsyndromeandfetalalcoholspec-trumdisorder.In:CassidyS,AllansonJ,editors.Managementofgeneticsyn-dromes.2nded.NewYork:JohnWileyandSons;2004.
25. AstleySJ,ClarrenSK.Diagnosticguideforfetalalcoholsyndromeandrelatedcon-ditions:the4-DigitDiagnosticCode.2nded.Seattle:UniversityofWashingtonPublicationServices;1999.
26. ClarkeME,ToughSC.Anationalsurveyregardingknowledgeandattitudesofhealthprofessionalsaboutfetalalcoholsyndrome.Ottawa:HealthCanada;2003.
27. LemoineP,HarousseauH,BorteyruJP,MenuetJC.Lesenfantsdeparentsal-cooliques-anomaliesobservées:àproposde127cas.OuestMed1968;21:476-82.
28. JonesKL,SmithDW,UllelandCN,StreissguthAP.Patternofmalformationinoffspringofchronicalcoholicmothers.Lancet1973;1(7815):1267-71.
29. ClarrenSK,SmithDW.Thefetalalcoholsyndrome.Lamp1978;35(10):4-7.30. AstleySJ,ClarrenSK.Diagnosingthefullspectrumoffetalalcohol-exposedindi-
viduals:introducingthe4-DigitDiagnosticCode.AlcoholAlcohol2000;35(4):400-10.31. BenoitT,BowesMD,BowmanN,CantinD,ChudleyA,CrollyD,etal.Telemedicinediagnosis
forfetalalcoholsyndrome-theManitobaexperience.PediatrChildHealth2002;7:147-51.
32. AstleySJ,StachowiakJ,ClarrenSK,ClausenC.Applicationofthefetalalco-holsyndromefacialphotographicscreeningtoolinafostercarepopulation.JPediatr2002;141(5):712-7.
33. AstleySJ,ClarrenSK.Measuringthefacialphenotypeofindividualswithprenatalalcoholexposure:correlationswithbraindysfunction.AlcoholAlcohol2001;36(2):147-59.
34. HennessyRJ,KinsellaA,WaddingtonJL.3Dlasersurfacescanningandgeo-metricmorphometricanalysisofcraniofacialshapeasanindexofcerebro-cran-iofacialmorphogenesis:initialapplicationtosexualdimorphism.BiolPsychiatry2002;51(6):507-14.
35. DaSilveiraAC,DawJLJr,KusnotoB,EvansC,CohenM.Craniofacialap-plicationsofthree-dimensionallasersurfacescanning.JCraniofacSurg2003;14(4);449-56.
36. USDepartmentofHealthandHumanServices.NationalInstituteonAlco-holAbuseandAlcoholism.10thspecialreporttotheUSCongressonalcoholandhealth:highlightsfromcurrentresearch.Washington:TheInstitute;2000.
37. BradleyKA,Boyd-WickizerJ,PowellSH,BurmanML.Alcoholscreeningquestionnairesinwomen:acriticalreview.JAMA1998;280(2):166-71.
38. RussellM,MartierSS,SokolRJ,MudarP,BottomsS,JacobsonS,etal.Screeningforpregnancyrisk-drinking.AlcoholClinExpRes1994;18(5):1156-61.
39. AstleySJ,ClarrenSK.Acasedefinitionandphotographicscreeningtoolforthefacialphenotypeoffetalalcoholsyndrome.JPediatr1996;129(1):33-41.

40. JonesKL,SmithDW.Thefetalalcoholsyndrome.Teratology1975;12(1):1-10.41. ThomasIT,GaitantzisYA,FriasJL.Palpebralfissurelengthfrom29weeks
gestationto14years.JPediatr1987;111:267-8.42.HallJG,Froster-IskeniusUG,AllansonJE,editors.Handbookofnormalphysi-calmeasurements.Oxford:OxfordUniversityPress;1989.pp.149-50. 43.FarkasLG.Anthropometryoftheheadandface.2nded.NewYork:RavenPress;1994. 44.MooreES,WardRE,JamisonPL,MorrisCA,BaderPI,HallBD.Newper-spectivesonthefaceinfetalalcoholsyndrome:whatanthropometrytellsus.AmJMedGenet2002;109(4):249-60. 45.MattsonSN,RileyEP,GramlingL,DelisDC,JonesKL.Heavyprenatalal-coholexposurewithorwithoutphysicalfeaturesoffetalalcoholsyndromeleadstoIQdeficits.JPediatr1997;131(5):718-21. 46.Nationalpopulationhealthsurvey,1994-1995.Ottawa:StatisticsCanada;1995.Available:stcwww.statcan.ca/english/sdds/5004.htm(accessed2004Oct29).47.Nationallongitudinalsurveyofchildrenandyouth,1994-1995.Ottawa:Sta- tisticsCanada;1995.48.Nationallongitudinalsurveyofchildrenandyouth,1998-1999.Ottawa:Sta- tisticsCanada;1999.49.Fall2002surveyofFirstNationspeoplelivingonreserve.Ottawa:EKOSRe- search;2002.50.StolerJM,HuntingtonKS,PetersenCM,DanielP,AboagyeKK,Lieberman E,etal.Theprenataldetectionofsignificantalcoholexposurewithmaternal bloodmarkers.JPediatr1998;133(3):346-52.51.MooreC,JonesJ,LewisD,BuchiK.Prevalenceoffattyacidethylestersin meconiumspecimens.ClinChem2003;49(1):133-6.52.BearerCF.Meconiumasabiologicalmarkerofprenatalexposure.AmbulPediatr 2003;3(1):40-3.53.ChanD,Bar-OzB,PellerinB,PaciorekC,KleinJ,KapurB,etal.Population baselineofmeconiumfattyacidethylestersamonginfantsofnon-drinking womeninJerusalemandToronto.TherDrugMonit2003;25(3):271-8.54.NationalCenteronBirthDefectsandDevelopmentalDisabilitiesCentersforDiseaseControlandPreventionDepartmentofHealthandHumanServices.FetalAlcoholSyndrome:GuidelinesforReferralandDiagnosis:NationalTaskForceonFetalAlcoholSyndromeandFetalAlcoholEffect;2004 http://www.cdc.gov/ncbddd/fas/documents/FAS_guidelines_accessible.pdf Correspondence to: Dr. Jocelynn L. Cook, FASD Team, Public Health Agency of Canada, Division of Childhood and Adolescence, Jeanne Mance Bldg. 9th flr, Tunney’s Pasture, Address Locator 1909C2, Ottawa ON K1A 0K9; [email protected]