by prof.dr. kamal mahmoud ahmad head of the cardiology & angiology unit medical research...
TRANSCRIPT


BYPROF.DR.KAMAL
MAHMOUDAHMAD
HEAD OF
THE CARDIOLOGY &
ANGIOLOGY UNITMEDICAL RESEARCH
INSTITUTEALEXANDRIA UNIVERSITY
SUDDEN CARDIAC DEATH IN YOUNG ATHLETES
A competitive athlete
is one who participates
in an organized team
or individual sport that
requires regular
competition against
others and requires
vigorous training

What do these elite athletes look like?
athletes had a 46% larger left ventricle than non-conditioned
people .They also had a 33%increase in
stroke volume. Resting heart rates is low

How do we measure the Athletes Heart?a
The size of the left ventricle when fully expanded, the thickness of its walls, and the amount of blood it pumps with each beat, (called stroke volume) are all key stats in assessing the heart. A technique using ultra sound technology called echocardiography allows doctors to watch the heart in action, freeze the image, and then take measurements to establish the athlete’s heart.

DEMOGRAPHICS
Sudden cardiac death occurs most frequently during basketball and football
Majority of deaths occur in menMost athletes are of high school age at the
time of deathMajority of the athletes who incur sudden
death have been free of cardiovascular symptoms
Collapse is usually associated with intense physical exertion and most commonly occur in the afternoon and early evening hours

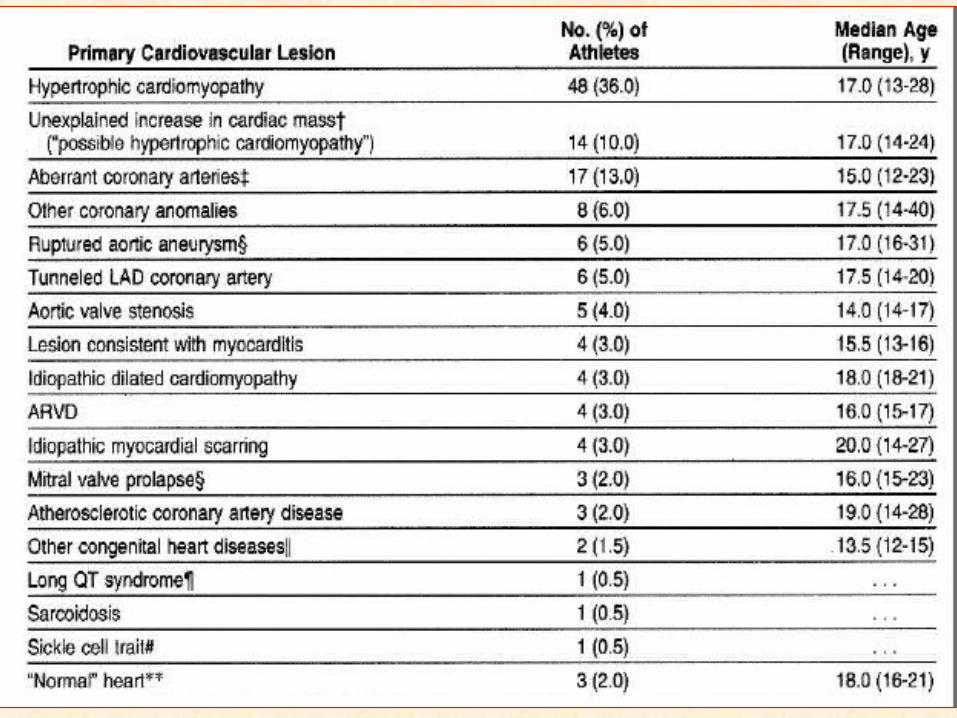
Cause of Death
85% died of cardiovascular causes
15% died of non cardiovascular causes -







CRADIOVASCULAR CAUSES
Cardiac History ScreeningCardiac History Screening
Previous murmur or high BPPrevious murmur or high BPFamily history of early MI or sudden deathFamily history of early MI or sudden deathExercise-related symptomsExercise-related symptoms

CASE PRESENTATION




TIMING OF SCD IN ATHLETES
90% of deaths among young athletes occur during training or competition
These observations substantiate the finding that in the presence of certain cardiovascular diseases, vigorous physical exertion represents a trigger for lethal arrhythmias and sudden death on the athletic field

Many of the athletes who've died playing their sport either had very subtle symptoms they didn't understand,or they didn't appreciate the risk.
The events are sudden and tragic. There are cardiac programs
specifically designed for these athletes to catch their condition before it's too late.

In SCA, the heart suddenly stops beating normally. The electrical impulses that control the rhythm of the heart become so disorganized that the heart can no longer effectively pump oxygenated blood to the brain and the body's vital organs, and death occurs

Etiology of life threatening arrhythmias and sudden cardiac death
Coronary artery disease. (MI) Heart failure.Cardiomyopathies. Hypertrophic cardiomyopathy (HCM) Dilated cardiomyopathy (DCM) Arrhytythmogenic RV cardiomyopathy (ARVD)Primary electrophysiologic disorders. Long QT syndrome Brugada syndrome Aortic stenosis Anomalous origin of coronary arteries

Coronary artery disease.
8o % of fatal arrhythmias and SCDThe culprit arrhythmia is;VT/VF in 95% and Asystole in 5 %

Predictors of arrhythmias
LARGE infarction.Impaired LV systolic function.Presence of occluded artery.

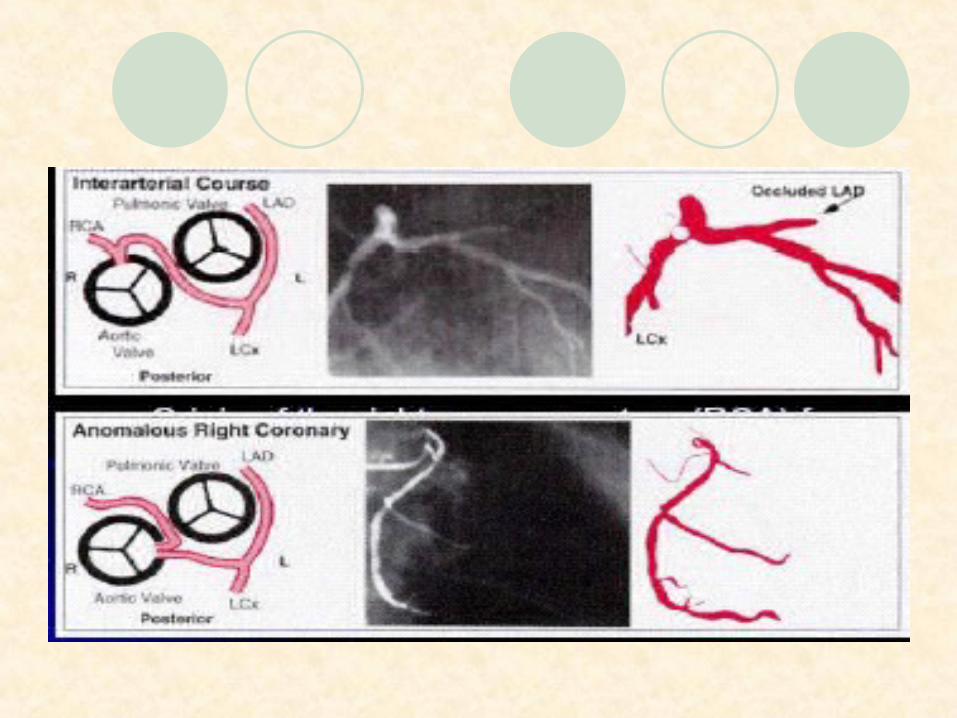
Anomalous Coronary arteries
Type of Anomalous Coronary arteries
Origin of the left main coronary artery (LMCA) from the right or non coronary sinus
Origin of the right coronary artery (RCA) from the left coronary sinus.
Both coronary arteries arising from the same coronary ostium .
Absent right coronary artery in one case.






Cardiomyopathies
Cardiomyopathies are defined by the World Health Organization
(WHO) as Diseases of the myocardium which
result in cardiac dysfunction.

The WHO Classification of Cardiomyopathies Includes:
HYPERTROPHIC.DILATED.RESTRICTIVE.
AndArrhythmogenic right ventricular
cardiomyopathies.
HYPERTROPHIC CM
Prevalence and Genetics
Most common cause of sudden death in young athlete Prevalence: 0.2% (1:500) in the adult general population
Most common genetic cardiovascular disease
< 1% of patient in cardiology practice
Genetics: autosomal dominant trait, caused by mutations in genes encoding proteins of the cardiac sarcomeres





In hypertrophic Cardiomyopathy
The ventricular walls are
hypertrophied.
The cavity is small.
The ventricular function is
normal or hyperkinetic.




Hypertrophic CM
Fatal arrhythmias and SCD can occur throughout life particularly in young patients.

Hypertrophic CM
The disease is the most common cause of sudden death in atheletes, and the genetic defects responsible may have a prevalence in the population as high as 1 in 2000..

Hypertrophic CM
The consequences of the heart muscle thickening are restriction of blood flow into and out of the heart, interruption of the heart's own blood supply, the development of heart rhythm irregularities.

Predictors of FA & SCD IN HOCM
symptoms such as chest pain, headaches and black-outs.
Next attempts are made to distinguish those patients who may be at risk for sudden death from those who are not

Predictors of FA & SCD IN HOCM
Family history of SCD.Syncope.IVS > 30 mm.Non sustained VT.Sustained VT & VF.

ARVDARVD
Normal heart tissue is replaced by Normal heart tissue is replaced by fibrofatty tissue fibrofatty tissue
Dilatation or formation of aneurysms in the Dilatation or formation of aneurysms in the right ventricular wall right ventricular wall

THE ATHELETES HEART
LEFT VENTRICULAR DD >45 mm.MAXIMAL DIASTOLIC WALL
THICKNESS < 15mmNO FAMILY HISTORYNO LEFT ATRIAL ENLARGEMENT.NORMAL DIASTOLIC FUNCTION.

Athletic HEART
Habitual physical activity reduces the overall risk of myocardial infarction and sudden coronary death by preventing development and progression of atherosclerotic coronary artery disease.

Athletic HEART
However vigorous exertion increases the incidence of acute coronary events in individuals who did not exercise regularly.

Athletic HEART
Sport acts as a trigger of cardiac arrest in those athletes who are affected by silent cardiovascular conditions;
Cardiomyopathy, premature coronary artery disease and congenital coronary anomalies, which predispose to life-threatening ventricular arrhythmias during physical exercise

cigarette smoking
continued cigarette smoking is associated with a significant increase in the risk of life-threatening tachyarrhythmias and SCD
The Impacts of Smoking on Diving
The effects of smoking are especially significant for persons who participate in scuba diving.
A review of scientific literature about the body's reaction to smoking and nicotine illustrates how smoking can effect diving performance

The Impacts of Smoking on Diving
Nicotine promotes platelet aggregation and fibrinogen formation, which are precursors to the clots that obstruct small blood vessels. An obstruction initiates negative repercussions that increases the risk of diving and decompression. The heart rate increases, elevating oxygen consumption and the shrinking of small blood vessels increases total peripheral resistance , increased blood pressure and poor circulation in the periphery of the body.

The Impacts of Smoking on Diving
Peripheral circulation involves the miles of very small blood vessels all over the body. The vessels are problematic in efficient inert gas elimination. For example, the extremities contain numerous areas of reduced circulatory efficiency such as the joints (responsible for the majority of decompression sickness). When divers begin to get chilled, a natural reduction in blood circulation to the peripheral system occurs to maintain a reasonable core temperature.

Potassium disorders
Potassium disorders (hyperkalemia & hypokalemia ) may precipitate cardiac arrhythmias or cardiopulmonary arrest.
They are an anticipated complication in
patients with renal failure, but may also occur in patients with no previous history of renal disease.
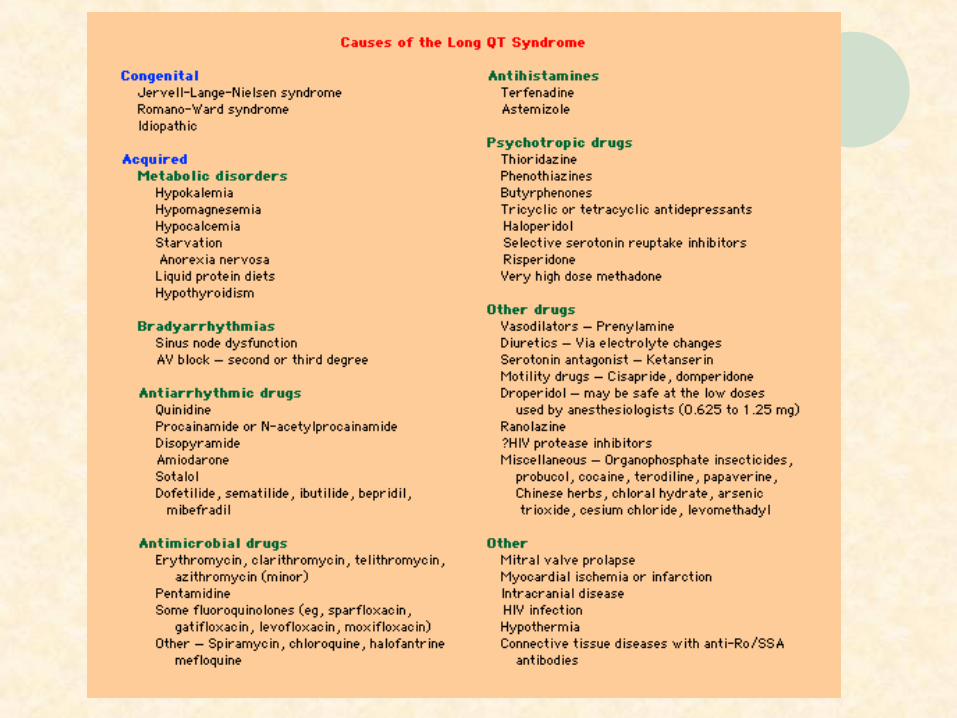
long QT syndrome
Occurring especially during conditions of increased sympathetic activity.
mortality is high among untreated, symptomatic individuals

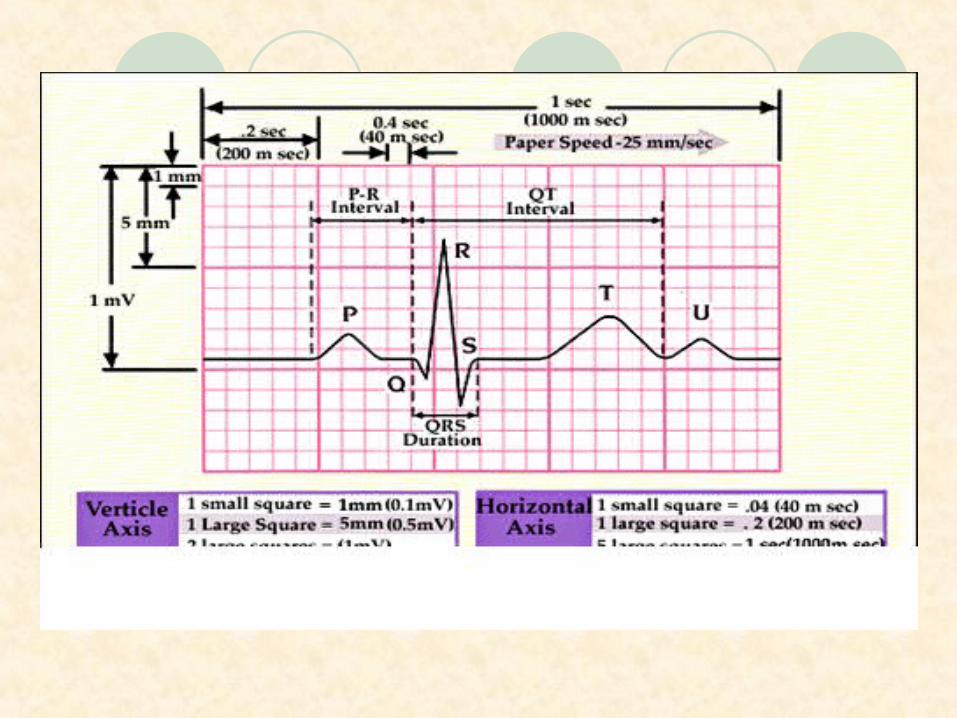
QTc = QT interval ÷ square root of the RR interval (in msec)

long QT syndrome
Congenital long QT syndrome (LQTS) is a genetic disorder characterized by prolongation of the QT interval on the electrocardiogram and by life-threatening cardiac arrhythmias.


Short QT syndrome
Short QT syndrome is an inheritable primary electrical disease of the heart that was discovered in 1999.
The disorder is characterized by an abnormally short QT interval (<300 ms) and a propensity to atrial fibrillation, sudden cardiac death or both.
so far two relevant genetic mutation has been identified that can lead to a short QT interval on the ECG

AWAY FROM THE HEART
Food Additives And The Artificial Sweetener Aspartame
there is one mechanism that's getting no attention at all: the excitotoxin damage caused by food additives and the artificial sweetener aspartame.
An alarming number of SCD, in high schools and colleges as well as among professional athletes.
IT was thought that food additives, cause their damage in the cardiovascular centers in the brain stem and/or by over-stimulating sympathetic centers in the hypothalamus of the brain.

herbal remedies
Extracts from the plant Aconitum species have been used as anti-inflammatory and analgesic agents.
Many of these alkaloids are extremely potent cardiotoxins resulting in various fatal arrhythmias as ;
severe bradycardia, sinus inactivity, AV dissociation with idiojunctional rhythm and LBBB resulting in hypotension and syncope.
Prevention of Fatal Arrhythmias by Fish Oil
Fatty Acid Intake
The long-chain n-3 fatty acids in fish have been demonstrated to have antiarrhythmic properties in experimental models and to prevent sudden cardiac death in a randomized trial of post–myocardial infarction patients.
Circulation. 2005;112:2762-2768.)
Melatonin
The pineal secretory product, melatonin, is known to be a potent free radical scavenger, antioxidant and can inhibit the intracellular calcium overload. ischemia-reperfusion injury.
Incidence of SCD is high in the morning hours.
It has been shown that melatonin levels are significantly low at these times and patients with coronary heart disease have lower levels than normal individuals.

Melatonin
These findings thought that melatonin would be valuable to test in clinical trials for prevention of possible ischemia-reperfusion-induced injury, especially life threatening arrhythmias and infarct size,
Anadolu Kardiyol Derg. 2006 Jun;6(2):

Better understanding of the interaction among various functional, structural, and genetic factors underlying the susceptibility to, and initiation of, fatal arrhythmias is a major goal and will provide new tools for the prediction, prevention, and therapy of SCD

To initiate A program that combines cardiology and sports medicine.
These clinics not only treat athletes with obvious symptoms but test those without as well.



السالم عليكم ورحمة الله وبركاته
