business experience in implementing an advanced telemonitoring service
TRANSCRIPT

Dr. Bernardo Valdivieso Martinez,
Quality Manager & Planning Director
Department of Health La Fe, Valencia, Spain
The Challenge:“Improving Care Condition”

Implementing an Advanced
Chronic Disease Management
Service
- Business Experience -

Sumary
The introduction
The problem
The solution
Lessons & learnt

An introduction
Valencia land
Population: 4.396.318
> 65 years old: 17,3%
Health System:
Hospitals: 28
Primary Care Centres: 500
Budget: (million €)
3.074 (36,9%)
Spain

An introduction
• Atraction 52%
• Population: 260.000
• > 65 years old: 17,3%
• Health System
• Hospital: 1
• Primary Care Team: 13
• Budget (million €)
• 540 total
• 260 “capitation”
Valencia land Health Department LA FE

An introduction
Concepts Expenses %
Personal costs 371.962.870,10 68,3%
Operating costs 110.761.052,67 20,4%Arrendamientos 2.618.677,60 0,5%
Reparaciones 6.625.557,57 1,2%
Material oficina e informática 1.619.786,59 0,3%
Consumos energéticos, telefonía y ostales 9.416.549,05 1,7%
Vestuario y lencería 370.835,45 0,1%
Ptos. Farmacéuticos y de laboratorio 41.376.621,87 7,6%
Mat sanitario fungible 18.373.486,69 3,4%
Otros suministros de material 3.270.195,82 0,6%
Otros gastos 1.427.326,23 0,3%
Trabajos otras empresas 25.359.426,80 4,7%
Dietas personal 302.589,01 0,1%
Investments 6.189.361,29 1,1%
Concerts costs 30.399.165,41 5,6%
Prosthesis and stents costs 14.962.901,26 2,7%
Others costs 10.000.000,00 1,8%
Total 544.275.350,73 100,0%
Capitation

Sumary
The introduction
The problem
The solution
Lessons & learnt

The problem

The problem

Current Health Systems
The problem

Current Health Systems
The problem

Sumary
The introduction
The problem
The solution
Lessons & learnt

Models
Policies
Best practices
Scientific evidence

1. Identify and stratify population
2. Planning and coordinate care within all health care levels, using
case management methodology
3. Specific guidelines and protocols for each disease
4. Specific educational disease programmes
5. Integrated Information Systems
6. Evaluate and improve quality, cost and service
7. Align resources and incentives
Key elements

1. Identify and stratify population
2. Planning and coordinate care within all health care levels, using
case management methodology
3. Specific guidelines and protocols for each disease
4. Specific educational disease programmes
5. Integrated Information Systems
6. Evaluate and improve quality, cost and service
7. Align resources and incentives
Key elements

CASE MANAGEMENT
DISEASE MANAGEMENT
SELF CARE
HEALTH PROMOTION AND DISEASE PREVENTION
Population stratification
60%
40%
5 %
15%
80%

CASE MANAGEMENT
DISEASE MANAGEMENT
SELF CARE
HEALTH PROMOTION AND DISEASE PREVENTION
Population stratification
15
75
≥ 3 admissions
≤ 2 admissions
675 No admissions
2.500
13.000
115.500
Department LA FE: 260.000 population

1. Identify and stratify population
2. Planning and coordinate care within all health care levels, using
case management methodology
3. Specific guidelines and protocols for each disease
4. Specific educational disease programmes
5. Integrated Information Systems
6. Evaluate and improve quality, cost and service
7. Align resources and incentives
Key elements

The New Model
TRADITIONAL CARE MODEL
• Care is Proactive
• Care delivered by a health care
team
• Care integrated across time, place
and conditions
• Care delivered in group
appointments, nurse clinics,
telephone, internet, e-mail, remote
care technology
• Self-management support a
responsibility and integral part of the
delivery system
CHRONIC CARE MODEL
Deal with
Acute Attack
of Disease
Counsel re:
Lifestyle
ChangesReview
LabsAccess
Social/Other
Services
Reassure
Diagnose
General
Referral
Reviwe/Adjus
t Rx and Tx Routine
Preventive
Care
Modify and/or
Negotiate
Care Plans
Review
History
Review
Care
Plan
Complete
Forms
Talk with
Family
Reinforce
Positive
Health
Behaviours
Consultation
10 minutes

se
lf ca
re
Sase
management
Disease
management
Self care
support/
management
Level 3 High complexity
Level 2 High risk
Level 1 Low risk
Level 0, Healthy
60%
40% Healthy promotion
The New Model

The New Model
09-30-00044-Departamento La Fe- Modelo de crónicos 02-VF4
Página 96 de 142
En resumenModelo de gestión de enfermedades crónicas del departamento La Fe de la Agencia Valenciana de Salud:
Paciente / Cuidador
• Autocuidado• Automonitorización• Telemonitorización• Uso adecuado de los recursos y de la
medicación
Actor
Actividades más importantes
Equipo de Atención Primaria
• Formación e información• Atención domiciliaria y ambulatoria
programada y urgente• Elaboración plan de cuidados con
UHD• Comprobar inclusión en el programa
Gestora de casos
• Formación e información• Seguimiento del paciente• Resolución de dudas del paciente• Coordinación con todos los recursos
asistenciales
Unidad Médica de Corta Estancia
Servicios Especialidad
• Información y formación al paciente• Seguimiento de la evolución del
paciente• Atención en consulta programada
Nivel 3
Autocuidado, Automonitorización. Telemonitorización
• Formación e información• Seguimiento de 6 meses • Resolución de dudas • Coordinación recursos
asistenciales
Nivel 2
Autocuidado, Automonitorización. Telemonitorización
Nivel 1
Hábitos de vida saludables
Nivel 0
Unidad de Hospitalización Domiciliaria
• Formación en domicilio (3 dias) y evaluación inicial del paciente
• Elaborar el plan de cuidados con AP • Medico de enlace• Atencion a domicilio en crisis de PP
• Evaluación del riesgo de PP• Atencion crisis de PP• Soporte a especialistas en la
asistencia de PP• Derivación de pacientes
• Formación e información• Atención domiciliaria y
ambulatoria programada y urgente
• Comprobar inclusión en el programa
• Seguimiento de la evolución del paciente
• Atención en consulta programada
• Medico de enlace• Atención a domicilio en
crsis de PP
• Evaluación del riesgo de PP• Atencion crisis de PP• Soporte a especialistas en
la asistencia de PP• Derivación de pacientes
• Formación e información• Atención domiciliaria y
ambulatoria programada y urgente
• Comprobar inclusión en el programa
• Información y formación al paciente
• Atención en consulta programada
• Formación e información• Atención domiciliaria y
ambulatoria programada y urgente
DES
CO
MP
EN
SA
CIO
N
–PP – Paciente Pluripatológico
Coordinated & Integrated Care
PrimaryCare
Hospital at Home
CaseManager
PacientCarer
Sec
undar
yC
are
Specialist
Acute Geriatric
Prim
ary
Car
e

Nurse “Case manager”
The New Model

Involve patient and family
The New Model

1. Identify and stratify population
2. Planning and coordinate care within all health care levels, using
case management methodology
3. Specific guidelines and protocols for each disease
4. Specific educational disease programmes
5. Integrated Information Systems
6. Evaluate and improve quality, cost and service
7. Align resources and incentives
Key elements

“Innovando los Cuidados de las Condiciones Crónicas”
Guidelines and protocols
Educative interventions
Factors that exacerbate disease
Exacerbation symptoms recognition
Knowledge about disease and treatment
Therapeutic compliance
Guidelines and protocols

1. Identify and stratify population
2. Planning and coordinate care within all health care levels, using
case management methodology
3. Specific guidelines and protocols for each disease
4. Specific educational disease programmes
5. Integrated Information Systems
6. Evaluate and improve quality, cost and service
7. Align resources and incentives
Key elements

Healthcare Integrates - ERP -

The New Model
Nurse “Case manager”
Involve patient and family
Telemonitoring Services

Telemonitoring Services (Pilot phase)

1. Identify and stratify population
2. Planning and coordinate care within all health care levels, using
case management methodology
3. Specific guidelines and protocols for each disease
4. Specific educational disease programmes
5. Integrated Information Systems
6. Evaluate and improve quality, cost and service
7. Align resources and incentives
Key elements

Models
Policies
Best practices
Scientific evidence
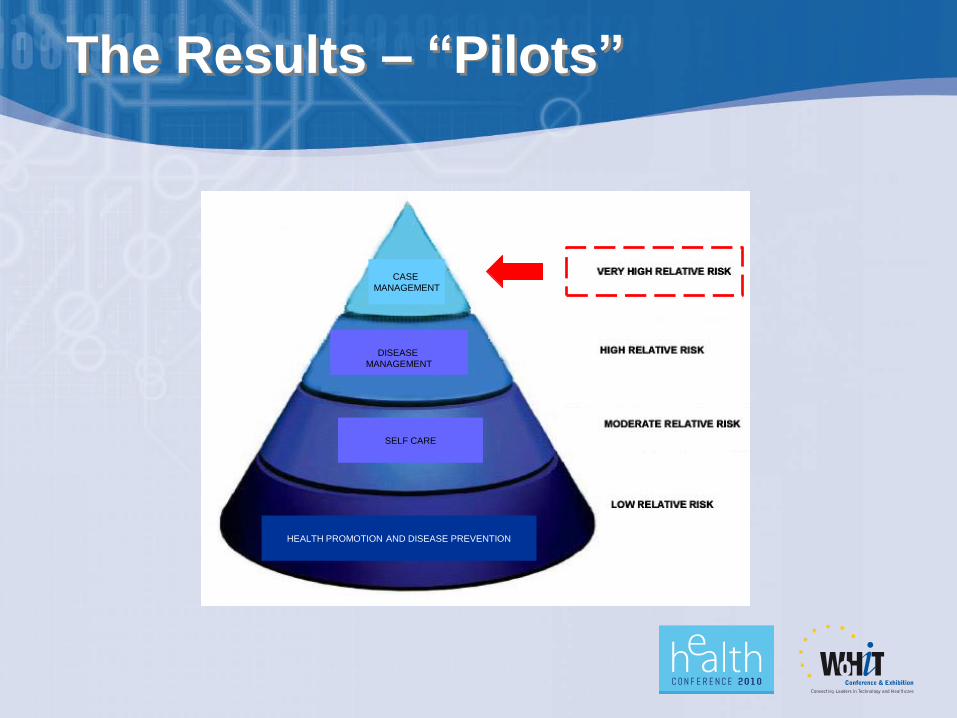
The Results – “Pilots”
CASE
MANAGEMENT
DISEASE
MANAGEMENT
SELF CARE
HEALTH PROMOTION AND DISEASE PREVENTION

The results: CHF Pilot
Comparative analysis
RESOURCES Pre Manag
Average admissions CHF per patient 1,5 0,4 73,3%
Density admissions CHF 4,2 1,0 76,2%
Average stays per patient 11,4 2,6 77,2%
Density stays 43,9 8,6 80,4%

“Innovando los Cuidados de las Condiciones Crónicas”
The results: CHF Pilot
Comparative analysis
RESOURCES Pre Manag
Average care atention all causes 3,6 1,4 61,1%
Average care atention CHF 1,9 0,4 78,9%
Density incidents urgency (all) 9,8 4,7 52,0%
Density incidents urgency (CHF) 5,3 1,3 75,5%

“Innovando los Cuidados de las Condiciones Crónicas”
Comparative analysis
RESULTS %
Exitus location at Home 74,2 %
Exitus location in Hospital 25,7 %
Sedation exitus at home 23,0 %
Hospital readmision 2,7 %
Derived to HML 3,4 %
The results: Palliative Care Pilot

1. Identify and stratify population
2. Planning and coordinate care within all health care levels, using
case management methodology
3. Specific guidelines and protocols for each disease
4. Specific educational disease programmes
5. Integrated Information Systems
6. Evaluate and improve quality, cost and service
7. Align resources and incentives
Key elements

Align resources and incentives
Strategic Map - Departament Health LA FE
To develop the human potential
Population and Society Financials
Pioneering development of the portfolio of services
Impel the use and security of
the TIC
To align the investments
with the strategy
Potenciar docencia e
investigaciónTo innovate the
attention of chronic
conditions
To guarantee services of health that satisfy the necessities and
the expectations with the population
To guarantee the economic sustainability of the system
To implant a System of
Recognitions
To manage alliances with agents nails
To impel the organizational
change
To plan the RR.HH for the
change
9
12
1614
2218 19
Improve the availability of the
strategic intelligence
15
to innovate the portfolio of
services
10
Clinically appropriate attendance
To harness clinical
security
7
Development of the knowledge
Suitable use of resources and optimized processes
Promotion of the health
Guarantee the
prevention
To harness thedomiciliary attention
and thehospitalizationalternatives
To make the promotion of
healthful habits
To present the system
1
2
4
3 To adapt pharmaceutical
prescription
6
To orient investigation
with the activity in line
11
Patients
To incorporate the
sharpshooting knowledge
21
To impel the use of the
best practices
8
13
To orient the organization to
the strategy17
Rational useof diagnose
tests
5
To order teaching to increase its
impact
12
To improve the satisfaction of professionals
20
C. To improve the health results
D. To generate confidence and security in the system
E. To respect environment
F. Improve the accessibility
G. Lend decisive attendance
H. Harness personalization
I. Increase to fidelización and attraction
J. To maximize income
and to manage the investments
K. To optimize the costs
L. Improve the productivity
BA

Departamento de Salud nº 7
.........................
MANAGEMENT
AGREEMENT
.........................DEPARTAMENT LA FE 20%
Align resources and incentives

Home
Care
Ambulatorry
Care
Emergnecy
Acute
Stay
Hospitalitation
Amulatory
Care
Complex
SECUNDARY CAREPRIMARY CARE
Align resources and incentives
Em
erg
ency

Home
Care
Ambulatorry
Care
Emergnecy
Hospital
at
Home
Ambulatoriy
Care
Specialist
Em
erg
ency
Hospital Support Team
Case Managers
Acute
Stay
Hospitalitation
Amulatory
Care
Complex
SECUNDARY CARE
Acute
Geriatric
Unit
Mediium & Long
Stay
Unit
PRIMARY CARE
Case
management
Disease
management
Self care
support/
management
Align resources and incentives

Resources “care proactive” 2011
Primary Care Team
Doctor 1 / 1.500
Nurse 1 / 2.000
Hospital Home Unit Team
Doctor 1 / 20.000
Nurse 1 / 10.000
Case Managers * 1 / 125
Align resources and incentives
*Chronic Level 1 High complex

Resources “care reactive” 2011
Hospital Support Teams 2
Acute Geriatric Unit 45
Medium Stay Unit 56
Convalescence
Palliatives Care
Long Stay Unit 28
Mental Health Unit 28
“Innovando los Cuidados de las Condiciones Crónicas”
Align resources and incentives

e-Chronic Disease Management Service
Align resources and incentives

CASE MANAGEMENT
DISEASE MANAGEMENT
SELF CARE
HEALTH PROMOTION AND DISEASE PREVENTION
60%
40%
5 %
15%
80%
Align resources and incentives
1.500 € year / user
2.000 Case management
3.000.000 € year
e-CDM Service

Sumary
The introduction
The problem
The solution
Lessons & learnt

Lessons & learnt
20% Technologicaland
80% cultural

HIS
E-CDM Service
Lessons learnt
2
1
3

CASE MANAGEMENT
DISEASE MANAGEMENT
SELF CARE
HEALTH PROMOTION AND DISEASE PREVENTION
60%
40%
5 %
15%
80%
Align resources and incentives
1.500 € year / user
2.000 Case management
3.000.000 € year
260.000 population
e-Health & e-Disease
Management
3.000.000 € year
e-CDM Service

An introduction
Concepts Expenses %
Personal costs 371.962.870,10 68,3%
Operating costs 110.761.052,67 20,4%Arrendamientos 2.618.677,60 0,5%
Reparaciones 6.625.557,57 1,2%
Material oficina e informática 1.619.786,59 0,3%
Consumos energéticos, telefonía y ostales 9.416.549,05 1,7%
Vestuario y lencería 370.835,45 0,1%
Pharmaceutical and laboratory products 41.376.621,87 7,6%
health products and consumables 18.373.486,69 3,4%
Otros suministros de material 3.270.195,82 0,6%
Otros gastos 1.427.326,23 0,3%
Trabajos otras empresas 25.359.426,80 4,7%
Dietas personal 302.589,01 0,1%
Investments 6.189.361,29 1,1%
Concerts costs 30.399.165,41 5,6%
Prosthesis and stents costs 14.962.901,26 2,7%
Others costs 10.000.000,00 1,8%
Total 544.275.350,73 100,0%
Capitation
↓ 10%

Lessons & learnt
20% Technological
and
80% cultural

Departamento de Salud nº 7
Lessons & learnt

Lessons & learnt

Departamento de Salud nº 7
Lessons & learnt

Lessons & learnt
